Embed Size (px)
DESCRIPTION
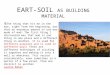
G rown U p C ongenital H eart (disease). 1965. 1500.000. ↑ 5% anno. 1250.000. 1000.000. 750.000. 500.000. 250.000. 1970. 1980. 1990. 2000. 2010. JACC 2001 Warnes JACC 2006 Williams. 2005. %. RVEF. Millane JACC 2000. Vander Velde Eur J Epidemiol 2005. - PowerPoint PPT Presentation
Citation preview

Grown
Up
Congenital
Heart (disease)

70
30
Ad. Pat Ped. Pat
1965

250.000
500.000
750.000
1000.000
1500.000
1970 1980 1990 2000 2010
1250.000
↑ 5% anno
JACC 2001 Warnes JACC 2006 Williams

40
60
Ad. Pat Ped. Pat
2005


0
10
20
30
40
50
60
70
8 10 12 14 16 18 20 22 24 26 ys
%RVEF
Millane JACC 2000

Vander Velde Eur J Epidemiol 2005

ACE/ARB treatment
Ramipril … 17 pts Therrien InT J Card 08
Losartan .. 37 pts Dore Circ 2005
Enalapril …. 9 pts Robinson Ped Card 2002
Losartan … 7 pts Lester AmJ C 2001
Enalapril ….. 14 pts Hecther AmJC 2001
No high-quality data support the use
Beta/Blocker treatment
…..31 pts Doughan Am J Card 2007
…. 14 pts Bouallal Card Young 2010
… 8 pts Josephson Can J Card 2006
It is difficult to conclude that B/blockade is beneficial

Type of procedure at risk
Cardiac conditions at highest risk

0
2
4
6
8
10
12
14
16
18
20
SVT VT Endocardits CVA
%
Engelfriet Eur H J 2005

The principal reasons for 373 medical admissions to the Royal Brompton Hospital GUCH unit in 1997.
Sommerville Heart 2002

0
5
10
15
20
25
30
35
40
Arr Ac HF Inf Sync TE Chestpain
Hem Ao An Card Arr Oth
%
Kaemmerer Am JC 2008

The updated recommendations dramatically change long established practice for primary care physicians,cardiologists, dentists, and their patients. For ethical reasons, these practitioners need to discuss the potential benefit and harm of antibiotic prophylaxis with their patients before a final decision is made. Following informed review and discussion, some patients (and also physicians) may wish to continue with routine prophylaxis in the individual case, and these views should be respected.

Br Med Bull. 2008;85:151-80.Adult congenital heart disease: a 2008 overview.
Bédard E, Shore DF, Gatzoulis MA.
SourceAdult Congenital Heart Center and Center for Pulmonary Arterial
Hypertension, Royal Brompton Hospital, Sydney Street, London SW3 6NP, UK
Current ACC/AHA GL are much more restrictive concernig the use of prophylactic antibiotics. However , we advocate a prudent approach for endocarditis prohylaxis in patients with CHD

Good oral hygiene and regular dental review have an essential role inreducing the risk of IE.
Transient bacteraemia occurs frequently in the context of these daily routine activities
It appears plausible that a large proportion of IE-causing bacteraemia may derive from daily routine activities such as tooth brushing, flossing….
In the majority of patients, no potential index procedure preceding the first clinical appearance of IE can be identified

Atrial septal defect
Interventional options:surgery or device closure
Unresolved issues:surgery vs device closure

0
5
10
15
20
25
30
< 20 21-30 31-40 41-50 51-60 61-70 > 70 ys
Mayo
Toronto
%
JACC 2001 Warnes

0
5
10
15
20
25
30
35
40
ASD VSD ToF CoAo TGA Marfan Fontan Cyan. Def
Engelfriet Eur H J 2005
Y
21
79
> 50 y < 50 y

Ebstein’s anomaly RV to PA conduits

0
5
10
15
20
25
30
35
40
45
50
Normali
NormaliNYHA I
NYHA IINYHA III
NYHA I
NYHA II
NYHA III
GUCH età media 33 y
Pazienti HF età media 59 y
VO2 ml/kg/m
…….all should have a measurement of exercise physiology.all should have a measurement of exercise physiology
Diller Circulation 2005

65% 18%
17%
Non cardiac Peri op CV
Am J Cardiol 2000 Oechslin
Analyzing the mortality causes in Analyzing the mortality causes in GUCH pts it appears that GUCH pts it appears that cardiovascular death is the most cardiovascular death is the most frequent: 65% of all deaths, excluding frequent: 65% of all deaths, excluding the perioperative cardiac surgery the perioperative cardiac surgery deaths. deaths.
26%
21%18%
18%
17%
Non cardiac Peri op Other CV HF SD
The most common mode is SD, followed The most common mode is SD, followed
by progressive HFby progressive HF

ICD therapy in adult patients with ToFWitte Europace 2008
...inappropriate anti-tachycardia pacing delivery (20%) and inappropriate cardioversion (25 %) ...Conclusion :Tetralogy of Fallot patients have a higher risk of inappropriate therapies …..
ICD in Tetralogy of Fallot Khairy Circ 2008
36 patients (29.8%) experiencedcomplications, of which 6 (5.0%) were acute, 25 (20.7%) were late lead-related, and 7 (5.8%) were late generator-related complications. Conclusions:…late lead-related complications are common.
14 patients (37.8%) experienced complications: 5 (13.5%) acute, 1 (2.7%) late generator related, and 12 (32.4%) late lead related.
SD and ICD in TGA With Intra-atrial Baffles: A Multicenter Study Khairy Circ Arr 2008
Specific criteria for ICD implantation for primary prevention have not been well defined yet

GUCHGUCHCardiologo pediatra
Cardiologo dell’adulto

RETE INTERAZIENDALE per la GESTIONE dei GUCH
ICLAS
IGG
ASl 3GUCHCardiologo Pediatra Cardiologo dell’Adulto
Ambulatorio per i GUCH ASL 3 - Nervi

RETE INTERAZIENDALE per la GESTIONE dei GUCH
ICLAS
IGG
ASl 3
GUCHCardiologo Pediatra Cardiologo dell’Adulto
Ambulatorio per i GUCH ASL 3 - Nervi