Embed Size (px)
Citation preview

Future Role of Pharmacotherapy for Obesity
Management
VT Chetty MD FRCPC MSc
Associate Prof McMaster University
Medical Director Bariatric Clinic, HGH

Objectives
• Overview of background history • Principles of Pharmacotherapy in Obesity • Review medications for long term use• What does the future holds?

Rational & Principles of Pharmacotherapy in
Obesity

Obesity is a Chronic Disease
• Long-term therapy is required for successful long-term weight management.
• Drugs do not cure obesity
• Drugs do not work when they are not taken

Drugs cause Modest Weight Loss
• Weight loss of 5%–10% of total body weight is considered clinically important

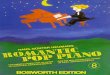
Modest Weight Loss Prevents Diabetes in Overweight and Obese Persons with Impaired
Glucose Tolerance
Diabetes Prevention Program Research Group. N Eng J Med 2002;346:393. Copyright © 2002. Massachusetts Medical Society. All rights reserved.
Cum
ulat
ive
Inci
denc
e of
Dia
bete
s (%
)
0
Year
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
Placebo
Lifestyle
58% (48-66%)

Effect of Weight Loss With Lifestyle Intervention on Risk of
Diabetes
Diabetes Care 2006

Comparison with other chronic diseases
1. Newly diagnosed Type 2 diabetes and hypertension respond very well to diet and exercise - but the primary treatments are drugs
2. The primary treatment for obesity is diet and exercise, drugs are an “adjunct”. Many patients must demonstrate that they have failed D&E before getting drugs or surgery

Phases of Obesity Treatment
Phase I(Weight Loss)
3-6 months
Phase II(Weight-Loss Maintenance)
Indefinitely
We
igh
t
www.drsharma.ca

“No one size fits all”
• Obesity is a heterogenous disorder with multiple etiologies
• “Obesities”-Foresight report

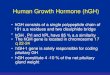
1. Mean responses describe how patients fare on average.2. The weight loss curves describe the tempo of weight loss.3. The placebo response indicates the strength of the behavioral
approach.
–8
–6
–4
–2
0
0 1 2 3 4 5 6 7 8 9 10 11 12
Mea
n C
hang
e in
Wei
ght
(%)
Drug
Placebo
Treatment MonthNoteunits
Noteplateau
Placebo response indicates behavioral program
Applying Pharmacotherapy Trials to the Practice Setting

Summary
• Obesity is a chronic disorder
• Heterogeneous
• Modest wt loss = clinical benefit
• Weight loss and Weight maintenance
• Clinical trials

History
• Many anti-obesity drugs in the past proved to have significant toxicity

“Lose 40 pounds in 4 weeks”: Regulating commercialweight-loss programs
Phenylpropanolamine

AmphetaminesDigitalis
“Rainbow pills”
AmphetaminesDigitalis
“Rainbow pills”
1940-60
1992
DexfenfluramineDexfenfluramine
1997
30% BMI<3014% BMI <27BRFSS
DinitrophenolThyroxine
DinitrophenolThyroxine
1933
Rimonabant approval in
Europe
Rimonabant approval in
Europe
2006-08
OrlistatOrlistat
1998
Sibutramine1997-2010
Sibutramine1997-2010
QnexaLocaserin
Not approved
QnexaLocaserin
Not approved
ContraveDec 2010 approvalFeb 2011 rejected
ContraveDec 2010 approvalFeb 2011 rejected
2010
AlliAlli

Food Intake and Appetite are Complex Processes
Nature, 2000;404:661-671

DRUGS FOR OBESITY:THE FUTURE

FDA 2007 draft guidance
Primary efficacy criteria (one of the following)• 5% greater (statistically significant) weight loss
than placebo at 1 year.• At least 35% patients achieving 5% weight loss
on drug and approximately double the proportion in the placebo-treated group.
Sample size• 3000 randomized to active dose of drug and no
fewer than 1500 on placebo for 1 year.
FDA Guidance for industry developing products for weight management, draft guidance, revision 1, Feb 2007

Emerging antiobesity drugs
• Drugs reporting phase III results• Lorcaserin (Arena)• Phentermine + topiramate (Vivus)• Bupropion + naltrexone (Orixegen)

Lorcaserin
• Activation of 5-HT2C receptor decreases food intake via POMC neurons.
• Fenfluramine and dexfenfluramine were agonists of both 5-HT2C and 5-HT2B.
• Selective 5-HT2C agonist.
Thomsen WJ et al., J Pharmacol Exp Ther 2008;325:577-87

Lorcaserin – main results
• Two phase III trials – BLOOM (2 yrs) and BLOSSOM (1yr)
• Weight change at 1 yr• -5.8% (lorcaserin 10 mg bid) vs -2.5%
(placebo)• 5% weight loss – 47%
• FDA defined valvulopathy• RR 1.07 (0.74, 1.55)
FDA briefing document, Advisory committee meeting for lorcaserin, 16 Sep 2010

Lorcaserin – FDA advisory committee meeting• Concerns
• Neoplams in rats (breast, brain, and other regions)
• Psychiatric and cognitive AEs
• Vote for approval• Yes = 5
• No = 9
• May 2012 voted 18-4 to recommend approval of benefits "outweigh the potential risks when used long term" in overweight and obese people.
FDA Endocrine and Metabolic Drugs Advisory Committee, 15 Sep 2010

Phentermine + topiramate
• Phentermine available since 1959 for short-term treatment of obesity.
• Topiramate has been well studied for obesity.– Consistently demonstrated dose-dependent weight loss efficacy
in numerous trials ranging from 6 months to more than a year in obese and overweight patients with and without type 2 diabetes and hypertension.
– Reduction of BP and improvement of glycaemic control.– Neuropsychiatric adverse events have hindered its further
development for treatment of obesity.
Bray GA et al., Obes Res 2003;11:722-33. Wilding J et al., Int J Obes 2004;28:1399-1410. Toplak H et al., Int J Obes 2007;31:138-46. Rosenstock J et al., Diabetes Care 2007;30:1480-6. Tonstad S et al., Am J Cardiol 2005;96:243-51. Stenlof K et al., Diabetes Obes Metab 2007;9:360-8.

Phentermine + topiramate efficacy pooled data
Tx group N Mean weight loss (%)
mean difference vs
placeboPlacebo 1477 -1.7
PHEN/TPM 3.75/23 234 -5.1 -3.2
PHEN/TPM 7.5/46 488 -8.4 -6.7
PHEN/TPM 15/92 1479 -10.6 -8.9
FDA briefing document, Endocrine and Metabolic Drugs Advisory Committee, 15 July 2010

PHEN/TPM – FDA advisory committee meeting
• Concerns• Teratogenicity with TPM in patients treated for
epilepsy• Psychiatric (depression, anxiety) and cognitive AEs• Decreased serum bicarbonate and potential
implications • Increase in heart rate (0.6 bpm for mid-dose, 1.6 bpm
for high-dose)
• Vote for approval• Yes = 6• No = 10
FDA Endocrine and Metabolic Drugs Advisory Committee, 15, July 210

• Vivus Inc., the manufacturer of Qnexa, submitted new data on the drug's psychiatric and cardiovascular side effects and an FDA advisory committee endorsed approval by a 20-2 vote in February.
• The FDA is expected to make a decision in July.

Bupropion + naltrexone
• Bupropion, primarily norepinephrine uptake inhibitor, is marked for treatment of depression and as a smoking cessation aid.
• Bupropion showed modest weight loss efficacy in three obesity trials.1
• Naltrexone, an opioid receptor antagonist, is marketed to treat alcoholism and opioid addiction.
• Animal studies suggest pharmacodynamic synergy.2
1Gadde KM et al., Exp Rev Neurother 2007;7:17-24. 2Greenway FL et al., Obesity 2009;17:30-39

Bupropion + naltrexone weight loss (%)
Study Placebo NB16 NB32
NB-301 -1.3 -5.0% -6.1
NB-302 -5.1 -9.3
NB-303 -1.2 -6.4*
NB-304(DM)
-1.8 -5.0
• Does not include data of rerandomised patients
•Greenway et al., Lancet, July 30, 2010; Wadden et al., Obesity June 2010; Orexigen presentation, July 2009

Contrave Feb 2011
• Initial approval by Advisory Committee-Dec 2010
• Concern about the cardiovascular safety profile of naltrexone/bupropion
• Orexigen decided not to pursue approval in the U.S.

Gastrointestinal Peptides That Regulate
Food Intake
• A. Glucagon-like peptide-1
• B. Peptide-YY
• C. Oxyntomodulin
• D. Amylin
• E. Ghrelin

L-cell(ileum + colon)
Proglucagon
GLP-1 [7-37]
GLP-1 [7-36NH2]
K-cell(jejunum)
ProGIP
GIP [1-42]
Synthesis and Secretion of GLP-1 and GIP

The family of incretin-based therapies
Human GLP-1 analogues
Exendin-basedtherapies, e.g. exenatide
GLP-1 receptor agonists
DPP-4 inhibitors, e.g. sitagliptin, vildagliptin
Incretin-basedtherapies

GLP-1 has multiple direct effects on human physiology
Brain Insulin secretion (glucose-dependent) and beta-cell sensitivity
Glucagon secretion (glucose-dependent)
Insulin synthesis
Beta-cell mass*
Pancreas
Liver Hepatic glucose output
Caloric intake*
GI tractDecreasedmotility
*in animal studies
Cardiac

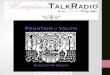
Fig 2 Meta-analysis of change in body weight (kg) in included trials after at least 20 weeks of treatment, using random effects model.
Vilsbøll T et al. BMJ 2012;344:bmj.d7771
©2012 by British Medical Journal Publishing Group
2.90kg (-3.59-2.22)

SSRI=Selective Serotonin Reuptake Inhibitor.
Selected Medications That Can Cause Weight Gain
• Psychotropic medications– Tricyclic antidepressants– Monoamine oxidase
inhibitors– Specific SSRIs– Atypical antipsychotics– Lithium– Specific anticonvulsants
-adrenergic receptor blockers
• Diabetes medications– Insulin
– Sulfonylureas
– Thiazolidinediones
• Highly active antiretroviral therapy
• Tamoxifen
• Steroid Hormones– Glucocorticoids
– Progestational steriods
35/26

Summary

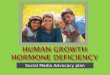
Obesity: Unmet Medical Needin Metabolic Disease Space%
of
Pat
ien
ts
Weight loss (%)
1015
50-
100-
0-
Pills
80-
5
Current goal
25 20 030
Surgery Future
Pharmacotherapy

Guide for Selecting Obesity Treatment
The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. October 2000, NIH Pub. No.00-4084
Treatment 25-26.9 27-29.9 30-34.9 35-39.9 >40
Diet, Exercise, Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
SurgeryWith co-
morbidities +
BMI Category (kg/mBMI Category (kg/m22))

Conclusions• Obesity is a chronic disease
• Modest weight loss (5% -10% of body weight) can have considerable medical benefits
• Lifestyle change (diet and physical activity) is the cornerstone of therapy
• Pharmacotherapy can be useful in properly selected patients

Discussion / QuestionsDiscussion / Questions






![Ttr Chetty Teachimpacts 0[1]](https://img.pdfslide.us/doc/110x75/577ccf011a28ab9e788ea161/ttr-chetty-teachimpacts-01.jpg)












![HGH &HS] M C](https://img.pdfslide.us/doc/110x75/628e4bb1ec00ee2bfd1ed2f4/hgh-amphs-m-c.jpg)