Embed Size (px)
Citation preview

Future drugs for patients not tolerating or
progressing under Sorafenib
Fabio Piscaglia
Internal Medicine
University of Bologna, Italy

DICHIARAZIONE DI CONFLITTO DI INTERESSI ULTIMI 2 ANNI
Fabio Piscaglia
• Bayer (speaker and advisory board fee)
• Bracco (speaker fee)
• Eisai (advisory board)
• Esaote (research grants)

PER QUALI PAZIENTI I FARMACI DOPO SORAFENIB?CONDIZIONI ALLA SOSPENSIONE DI SORAFENIB
Quali pazienti stanno attualmente andando nei trial di 2a linea e quali potremo trattare in futuro nella pratica clinica?
Reig M, Hepatology 2013;58, 2023-2031
Per trial arruolabili 19%, nella vita reale almeno 50%

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
Hallmarks consolidati

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
Hallmarks consolidatiTarget dei TKI anti-angiogenici (es. Sorafenib)

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
Hallmarks consolidatiTarget dei TKI anti-fattori di crescita
MET is the only known tyrosine kinase receptor for hepatocyte-growth factor (HGF) and is involved in cancer progression and metastasis

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
Regorafenib
Tivantinib

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
Cell 2013, 144:646-674
Hallmarks di recente identificazione

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
Cell 2013, 144:646-674
Hallmarks di recente identificazione
Target non utili per terapie oncologiche

Hanahan & Weinberg, Cell 2013, 144:646-674
POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI

2015 2019
Apatinibvs placebo In 2nd line HCC
Q3 2019 data readout
2016
Regorafenib in 2 nd-lineHCC (RESORCE)
Q2 2016
Nivolumab in 2 nd-line HCC(extend ph I/II to 500) Q4 2018 data readout
(could be earlier)
Pembrolizumab in 2 nd-line HCC (KEYNOTE-240)Q4 2018 data readout
2018
Y90 +/- Nexavar ® in HCC (SORAMIC)
~ 1H 2016 recruitment ? 2018 data readout
Y90 vs TACE in advanced HCC
Q2 2018 data readout
Nivolumab vs Nexavar ®
in 1 st -line HCCQ2 2018 data readout
Donafenib vs Nexavar ®
In 1st line HCC Q3 2019 data readout
1L Competitor data
2L Competitor data
Nexavar® data
2017
Cabozantinibin 2 nd-line HCC
Q1 2017 data readout
Ramucirumabin 2 nd-line HCC (REACH II)
Q1 2017 data readout
Tivantinib in 2 nd-line(METIV-HCC)
Q1 2017 data readout
Lenvatinib vs Nexavar ® in 1st-line (REFLEX)
Q1 2017 data readout
HCC - Evolving Systemic Therapy Landscape
Ramuricumab in 2 nd line in HCC (LY3009806)
Q3 2019 data readout

Hanahan & Weinberg, Cell 2013, 144:646-674
POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
LENVATINIBDONAFENIBAPATINIB

Lenvatinib (Lenvima, Eisai, Inc.)
BID, twice daily; HCC, hepatocellular carcinoma; NCI-CTCAE, National Cancer Institute Common Toxicity Criteria for Adverse Events; PO, orally
Ganten TM, et al. Presented at the 2014 European Society of Medical Oncology(ESMO) meeting. Poster 5545
Dosing Trial RR-DTC
Patients
2
Plus Pembrolizumab in selected solid tumours1a/2
Plus Everolimus in advanced or mRCC1
In anaplastic thyroid cancer2
Refractory to gemcitabine-based unresectablebiliary tract cancer2
Refractory, unresectable Stage III/IV melanoma2
Phase
• MOA: multi-targed, TKI that inhibits VEGFR-1, 2, 3; FGFR-1, 2, 3, and 4; PDGFR-alpha, KIT, and RET
• Administered: orally
• Approved indications: progressive radioactive-iodine refractory DTC
Meccanismo di azione simile a Sorafenib e Regorafenib. Difficle prevedere se gli eventi avversi siano così diversi da permettere trattamento a chi non tollera Sorafenib. Attualmente non in valutazione in seconda linea

Lenvatinib (Lenvima, Eisai, Inc.)multi-targed, TKI that inhibits VEGFR-1, 2, 3; FGFR-1, 2, 3, and 4;
PDGFR-alpha, KIT and RET. Oral.
R
• A multicenter, randomized, open-label, phase 3 trial to compare the efficacy and safety of lenvatinib (E7080) vs Nexavar ® in 1L treatment of patients with unresectable HCC
• 145 centers: Belgium (3); France (14); Germany (9); Italy (7); Poland (3); Russian Federation (5); Spain (5); United Kingdom (6)
954
Primary endpoint:• OS
Main secondary endpoints:• PFS
• TTP, ORR, HRQoL
Select patient criteria:• Unresectable HCC
per AASLD*
• Child-Pugh class A
• ECOG PS 0-1
• No prior systemic therapy for HCC
Lenvatinib12 mg (or 8 mg) QD
Nexavar ®
400 mg PO BID
Until PD orunacceptable
toxicity
1:1
*AASLD criteria, including cirrhosis of any etiology or with chronic hepatitis B or C infection criteria.
1L, first-line; AASLD, American Association for the Study of Liver Diseases; ECOG PS, Eastern Cooperative Oncology Group performance status; QD, once a day; BID, twice a day; OS, overall survival; PFS, progression-free survival; TTP, time to progression; ORR, objective response rate; HRQoL, health-related quality of life.
https://clinicaltrials.gov/ct2/show/NCT01761266
• Study start date: March 2013• Estimated primary completion date: April 2016• This study is ongoing, but no more recruiting participants
Arruolamento chiuso. In attesa dei dati definitivi di sopravvivenza fine 2016

R
• A multicenter, randomized, open-label, phase 3 trial to compare the efficacy and safety of lenvatinib (E7080) vs Nexavar ® in 1L treatment of patients with unresectable HCC
• 145 centers: Belgium (3); France (14); Germany (9); Italy (7); Poland (3); Russian Federation (5); Spain (5); United Kingdom (6)
954
Primary endpoint:• OS
Main secondary endpoints:• PFS
• TTP, ORR, HRQoL
Select patient criteria:• Unresectable HCC
per AASLD*
• Child-Pugh class A
• ECOG PS 0-1
• No prior systemic therapy for HCC
Lenvatinib12 mg (or 8 mg) QD
Nexavar ®
400 mg PO BID
Until PD orunacceptable
toxicity
1:1
*AASLD criteria, including cirrhosis of any etiology or with chronic hepatitis B or C infection criteria.
1L, first-line; AASLD, American Association for the Study of Liver Diseases; ECOG PS, Eastern Cooperative Oncology Group performance status; QD, once a day; BID, twice a day; OS, overall survival; PFS, progression-free survival; TTP, time to progression; ORR, objective response rate; HRQoL, health-related quality of life.
https://clinicaltrials.gov/ct2/show/NCT01761266
• Study start date: March 2013• Estimated primary completion date: April 2016• This study is ongoing, but no more recruiting participants
Arruolamento chiuso. In attesa dei dati definitivi di sopravvivenza fine 2016Meccanismo di azione simile a Sorafenib. Difficle pre vedere che gli eventi
avversi siano così diversi da permettere trattament o a chi non tollera Sorafenib. Attualmente non in valutazione in seconda linea
Lenvatinib (Lenvima, Eisai, Inc.)multi-targed, TKI that inhibits VEGFR-1, 2, 3; FGFR-1, 2, 3, and 4;
PDGFR-alpha, KIT and RET. Oral.

DONAFENIB in studio in prima linea vs SORAFENIB
APATINIB in studio in seconda linea vs Placebo
Tutti studi all-comers(non selezione molecolare dei pazienti)

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674RAMUCIRUMAB

RAMUCIRUMABRecombinant IgG1 monoclonal Ab inhibiting VEGF-R2. Intravenous
Zhu AX, Lancet Oncol 2015;16:859-870
AFP >400 AFP <400
Phase-3: Ramucirumab vs Placebo in 2nd line HCC progressing on Sorafenib with AFP>400

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
TIVANTINIB

highly selective MET inhibitor . Also displays cytotoxic activity via molecular mechanisms that are independent from its ability to bind MET. Administrated orally
Tivantinib – METIV-HCC (NCT01755767)

Tivantinib For Second-line Treatment of Advanced He patocellular Carcinoma: A Randomised, Placebo-controlled Phase 2 Study
Santoro et al, Lancet Oncology 2013;14:55-63
Unchanged OS in c-MET (-)Unchanged TTP in c-MET (-)

HR: 0.38 (95% CI: 0.18-0.81) Log Rank: P=0.01
Median OS Patients Events
Tivantinib 7.2 mos 22 17
Placebo* 3.8 mos 15 15
Santoro et al, Lancet Oncology 2013;14:55-63
Improved OS in c-MET (+)Improved TTP in c-MET (+)
Tivantinib For Second-line Treatment of Advanced He patocellular Carcinoma: A Randomised, Placebo-controlled Phase 2 Study

• A phase III , randomized, double-blind study of tivantinib (ARQ 197) in subjects with c-MET diagnostic-high inoperable HCC treated with one prior systemic therapy
• 113 centers: Europe (79)
• C-Met high status on tumor tissue always to be confirmed centrally in double testing
• Study start date: December 2012• Estimated study completion date: June 2017• Estimated primary completion date: March 2017
• Enrolment concluded and follow up is ongoing. Final analysis still to be performed
N=368
Primary endpoint:• OS
Main secondary endpoints:• PFS• Safety
Select patient criteria:• Histologically confirmed
HCC inoperable and not eligible for local treatment
• MET diagnostic-high tissue
• At least 4 weeks of one prior Nexavar® treatment
• ECOG PS 0-1
PlaceboPO BID
1:1
Tivantinib120 mg PO BID(240 mg/day)
Tivantinib – METIV-HCC (NCT01755767)
ECOG PS, Eastern Cooperative Oncology Group performance status; PO, orally; BID, twice a day.
https://clinicaltrials.gov/ct2/show/NCT01755767
R Until PD orunacceptable
toxicity

Hanahan & Weinberg, Cell 2013, 144:646-674
POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
CABOZANTINIB

R
• A phase III, randomized (1:1), double-blind , controlled study of cabozantinib (XL184) vs placebo in subjects with HCC who have received prior Nexavar ®
• 102 centers: Europe (43); United Kingdom (5)
N=760
Primary endpoint:• OS
Main secondary endpoints:• PFS
• ORR
Select patient criteria:• HCC that has progressed
following 1-2 systemic treatments
• Received prior Nexavar®
• ECOG PS 0-1
• Child-Pugh class A
1:1
Cabozantinib – CELESTIAL (NCT01908426)
ECOG PS, Eastern Cooperative Oncology Group performance status; PO, orally; QD, once daily; PD, progressive disease; PFS, progression-free survival; ORR, objective response rate.
https://clinicaltrials.gov/ct2/show/NCT01908426
Cabozantinib60 mg tablet PO QD
Placebo PO QD
• Study start date: August 2013• Estimated primary completion date: October 2016
• This study is currently recruiting participants
Until PD orunacceptable
toxicity
• tyrosine kinase inhibitor inhibits the action of VEGFR-1, -2, -3; RET, and MET
Sia 2a che ulteriore lineaTripla azione

Hanahan & Weinberg, Cell 2013, 144:646-674
POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
NIVOLUMABIPILIMUMABTREMELIMUMAB

NIVOLUMAB
human IgG4 anti-PD-1 monoclonal antibody. Inhibitory ligand blocking antibody (blocks the interaction between PD-1 and PD-L1/PD-L2,1) against the programmed death; allows the immune system to attack the tumor as an example of immune checkpoint blockade. Intravenous infusion. Approved indications: US treatment of melanoma (Dec 2014); EU metastatic melanoma as a monotherapy (Apr 2015)
MHC
PD-L1
PD-1
PD-1
T-cellreceptor
PD-L2
T cell
NFκB
Other
PI3K
Tumor cell
IFNγ
IFNγR
Shp-2
Nivolumab
1.Topalian SL, et al. N Engl J Med. 2012;366:2443-2454

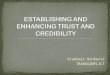
Nivolumab Phase 1/2. Maximal Change in Target Lesions From Baseline
120
100
80
60
40
20
0
-20
-40
-60
-80
-100
Patients (N = 40) †
Cha
nge
in T
arge
t Les
ion
Fro
m B
asel
ine,
%
Uninfected
HCV
HBV
Confirmed response*
* ** * * *
* *†2 uninfected patients not shown: 1 had disease progression before the first assessment; 1 had a maximal change of +23%‡Patient with resolved HCV infection
‡
AB. El-Khoueiry,1 et al. Presented at ASCO Annual meeting 2015. Abstract LBA 101
Phase 1/2 Safety and Antitumor Activity of Nivoluma b in Patients With Advanced Hepatocellular Carcinoma (HCC): CA209-040
AB. El-Khoueiry,1 et al. Presented at ASCO Annual meeting 2015. Abstract LBA 101

Protocol ongoing. Currently expansion phase:1L randomized Nivolumab 3mg/kg vs Sorafenib (open randomization)Infusion once a week for 3 weeks out of 4
2L different combined dosages (Nivolumab ± Ipilimumab) (Phase I/II).
NIVOLUMAB ( ± IPILIMUMAB in 2L)

NIVOLUMAB
R
• A randomized, multi-center phase III study of nivolumab vs Nexavar® as first-line treatment in patients with advanced HCC
• 103 centers: Belgium (3); Czech Republic (2); France (8); Germany (5); Poland (3); Spain (4); United Kingdom (4)
• Study start date: November 2015• Estimated primary completion date: June 2019
• This study is currently recruiting participants
N=726
Primary endpoint:• TTP• OS
Main secondary endpoints:• PFS• ORR• Programmed death L1
expression
Select patient criteria:• Histologically confirmed,
unresectable, advanced HCC
• Not eligible for LRT
• ECOG PS 0-1
• Child-Pugh class A
1:1
Nivolumab3 mg/kg IV2,*
Nexavar ®
400 mg PO BID
*3 mg/kg IV dose is based on Phase 1/II study findings. BID, twice daily; ECOG PS, Eastern Cooperative Oncology Group performance status; IV, intravenously; LRT, locoregional therapy; PO, orally; PD, progressive disease; PFS, progression-free survival; ORR, objective response rate.
1. https://clinicaltrials.gov/ct2/show/NCT02576509. 2. El-Khoueiry AB, et al. J Clin Oncol 2015 (Suppl; Abstr LBA101).
Until PD orunacceptable
toxicity

TREMELIMUMAB
Sangro, J Hepatol, 2013; 59: 81-88
• Intravenous every 3 months• Pilot study, Only 17 pazient assessed for tumor response• Partial response was 17.6% and disease control rate was 76.4%. • Time to progression was 6.5 Months

Hanahan & Weinberg, Cell 2013, 144:646-674
Cell 2013, 144:646-674
VACCINATION
POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI

Pexa-Vec (JX-594, Polaris)a vaccinia virus engineered to express granulocyte-macrophage colony
stimulating factor (GM-CSF), thereby stimulating direct oncolysis, tumor vascular disruption and anti-tumor immunity
R
• A phase 3 randomized, open-label study to determine whether treatment with vaccinia virus based immunotherapy (Pexa-Vec ) followed by Nexavar ® increases survival compared to Nexavar ® in patients with advanced HCC who have not received prior systemic therapy
• 4 centers: United States (3); New Zealand (1)
• Administration: intratumoural (IT) or intravenous (IV)
• Study start date: October 2015• Estimated study completion date: October 2019• Estimated primary completion date: October 2017• This study is currently recruiting participants
N=600
Primary endpoint:• OS
Secondary endpoints:• TTP
• PFS, ORR, DCR
• Safety
Select patient criteria:• Unresectable HCC
Advanced HCC (i.e., BCLC stage C or B per AASLD criteria*)
• Child-Pugh class A
• ECOG PS 0-1Nexavar ®
400 mg BID starting Day 1
1:1
*AASLD criteria, including cirrhosis of any etiology or with chronic hepatitis B or C infection criteria.
BCLC, Barcelona Clinic Liver Cancer; AASLD, American Association for the Study of Liver Diseases; ECOG PS, Eastern Cooperative Oncology Group performance status; IT, intratumoral; PFU, plaque forming units; BID, twice a day; PD, progressive disease; OS, overall survival; PFS, progression-free survival; TTP, time to progression; ORR, objective response rate; DCR, disease control rate.
https://clinicaltrials.gov/ct2/show/NCT02562755
PexaVec 3, IT injectionsof 1e9 PFUs � Nexavar ®
400 mg BID
P P P SDay 1 Week 2 Week 4 Week 6
Until P
D or
unacceptable toxicity
Attualmente testato solo in 1L quindi i risultati non influenzeranno chi è in progression o intollerante a Sorafenib

Immunoterapia. Studio coreano in adiuvante dopo RF o PEI

POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI
Hanahan & Weinberg, Cell 2013, 144:646-674
Cell 2013, 144:646-674

• A randomized, double-blind, multi-center phase III study of ADI-PEG 20 plus best supportive care (BSC) vs placebo plus BSC in subjects with advanced HCC who have failed prior systemic therapy
• Study start date: July 201173 centers: Italy (10); United Kingdom (10)
• Results presented in abstract form and NEGATIVE (no survival advantage)
N=636
Primary endpoint:• OS
Main secondary endpoints:• TTP• PFS• ORR• Safety and tolerability
Select patient criteria:• Advanced HCC
• Child-Pugh grade B7
• ECOG PS<2
PlaceboIM weekly + BSC
1:1
ADI-PEG 20 + BSC(arginine deiminase with
polyethylene glycol) 18 mg/m2 IM weekly
ADI-PEG 20 (NCT01287585)Arginine deiminase (ADI) formulated with polyethylene glycol (PEG). IM injection
ECOG PS, Eastern Cooperative Oncology Group performance status; IM, intramuscular; PD, progressive disease; OS, overall survival; TTP, time to progression; PFS, progression-free survival; ORR, objective response rate.
https://clinicaltrials.gov/ct2/show/NCT01287585
R Until PD orunacceptable
toxicity
• ADI degrades arginine, an amino acid crucial to tumor cell metabolism and growth of certain cancers (ie, melanoma, HCC, pancreatic, prostate cancer). Depletion of arginine by ADI from the blood can control tumor growth and even eliminate arginine-requiring cancers without damage to normal tissue cells.

Hanahan & Weinberg, Cell 2013, 144:646-674
POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI

Drug Target Selection % Patients Phase
Ramucirumab VEGFR2 AFP>400 44 III
Refametinib MEK RAS mutations
<5 II
Tivantinib MET MET-high 48 III
MSC2156119J MET MET-high 48 I/II
BLU-554 FGFR4 FGF19 6 FGFR4 Amp
I/II
RO5137382 Glypican-3 Glypican-3 II
Terapia su bersaglio

Drug Target Selection % Patients Phase
Ramucirumab VEGFR2 AFP>400 44 III
Refametinib MEK RAS mutations
<5 II
Tivantinib MET MET-high 48 III
MSC2156119J MET MET-high 48 I/II
BLU-554 FGFR4 FGF19 6 FGFR4 Amp
I/II
RO5137382 Glypican-3 Glypican-3 II
Terapia su bersaglio
Selezione su liquid biopsy (prelievo).Studio terminato con insufficiente arruolamento

Drug Target Selection % Patients Phase
Ramucirumab VEGFR2 AFP>400 44 III
Refametinib MEK RAS mutations
<5 II
Tivantinib MET MET-high 48 III
MSC2156119J MET MET-high 48 I/II
BLU-554 FGFR4 FGF19 6 FGFR4 Amp
I/II
RO5137382 Glypican-3 Glypican-3 II
Terapia su bersaglio

Hanahan & Weinberg, Cell 2013, 144:646-674
POSSIBILI TARGET FARMACEUTICI IN RELAZIONE AI MECCANISMI DI CANCEROGENESI

Regorafenib – RESORCE (NCT01774344)
Eur J Cancer, 2013;49:3412-3419
Best individual patient response Regorafenib. Studio concluso di fase 2 in HCC

• A randomized, double-blind, placebo-controlled, multicenter phase 3 study of regorafenib in patients with advanced HCC who have progressed on Nexavar ® treatment
• 178 centers: Austria (3), Belgium (2), Czech Republic (3), France (21), Germany (14), Hungary (4), Italy (19), Netherlands (3), Spain (12), Switzerland (3), United Kingdom (5)
Primary endpoint:• OS
Secondary endpoints:• TTP• PFS• ORR• DCR
Stratification: Geographical region, ECOG PS, AFP levels, EHS/MVI
Regorafenib160 mg PO QD (3 weeks
on, 1 week off) + BSC(4 weeks/cycle)
Placebo QD(3 weeks on, 1 week off) + BSC (4 weeks/cycle)
ST
RA
TIF
ICA
TIO
NN
=57
3R
AN
DO
MIZ
AT
ION
2:
1
Select patient criteria:• Advanced, unresectable
HCC per AASLD
• Child-Pugh class A
• ECOG PS 0-1
• Failed Nexavar®
• Tolerated Nexavar®
Regorafenib – RESORCE (NCT01774344)
Inclusion criterion: Sorafenib terminated <4 weeks

Regorafenib – RESORCE (NCT01774344)
Data will be presented for the first time end of Ju ne
Possible reasons for the success:
- Refined stratification , not only geography but also ECOG PS, AFP levels, EHS/MVI- Inclusion criteria : patients tolerant to Sorafenib and having terminated it by no longer
than 4 weeks and with documented radiological progression
Exclusion of slow progressors and of “practical” first liners (patients with early discontinuation of Sorafenib due to adverse events).
Press release

I risultati dello studio RESORCE avranno importanti implicazioni per il disegno delle future sperimentazioni:
- Regorafenib dovrebbe diventare reference standard d i paragone per gli studi di 2L trials
- Lo studio RESORCE ci ha insegnato che i pazienti de bbono essere stratificati meglio all’inclusione per tipologia e tempistica di progressione.
- Disegnare sperimentazioni per pazienti poco tollera nti al Sorafenib diventerà più difficile (richiede molti centri).
- Se qualcuno degli studi di 2L in corso prima dell’u scita di Regorafenib per HCC risulterà positivo sarà complesso decidere quale sia il trattamento di riferimento per la pratica clinica o negli studi
Il futuro delle terapie farmacologiche

Il futuro delle terapie farmacologiche
- La variabilità del decorso dell’HCC non è ancora be n compresa (forse anche per le limitate conoscenze molecolari / istologiche) e questo può impattare il disegno dei trial
- Non ci sono all’orizzonte farmaci che verosimilment e andranno bene per TUTTI i pazienti con HCC (all-comers)
- Le strategie terapeutiche in campo oncologico si st anno diversificando rispetto alla sola terapia antiangio genica e si disegnano studi “arricchiti” per caratteristiche mo lecolari
- In futuro possibili vaccini individualizzati?
- Pressochè tutte le nuove sperimentazioni richiedono campioni di tessuto per escludere forme miste / colangioCa e so prattutto per cercare marcatori di risposta (meglio biopsia recen te)

Il futuro delle terapie farmacologiche
L’evoluzione delle terapie dell’HCC richiederà :
- Centri che gesticano bene gli eventi avversi da Reg orafenib
- Capacità organizzative (imaging, biopsie, visite, a rchiviazione dati in CRF elettroniche) all’altezza dei trial di 2L vs Regorafenib 3L
- La nuova normativa Italiana a seguito di quella Eur opea richiede ora regole molto stringenti per accreditamente stud i Fase 1 (in vigore da luglio 2016)
Pertanto sarà sempre più importante l’interazione co n o l’affidamento a centri di riferimento

Grazie per l’attenzione
NB: il documento con le ”RACCOMANDAZIONI MULTISOCIETARIE ITALIANE(AISF, AIOM, IT-IHBPA, SIC, SIRM, SITO) PER LA GESTIONE CLINICA INTEGRATA DEL PAZIENTE CON EPATOCARCINOMA” sarà
accessibile e scaricabile dai siti delle società scientifiche entro l’estate 2016www.webaisf.org