Embed Size (px)
Citation preview

1
Functional Outcome After Total Hip Replacement: The Effect of Race and Ethnicity
Among Medicare Beneficiaries
A dissertation presented
By
Sonya L. Larrieux
To
School of Public Policy and Urban Affairs
In partial fulfillment of the requirements for the degree of
Doctor of Philosophy
In the field of
Law and Public Policy
Northeastern University
Boston, Massachusetts
May 2017

2
FUNCTIONAL OUTCOMES AFTER TOTAL HIP REPLACEMENT: THE EFFECT OF
RACE AND ETHNICITY AMONG MEDICARE BENEFICIARIES
A dissertation presented
By
Sonya L. Larrieux
ABSTRACT OF DISSERTATION
Submitted in partial fulfillment of the requirements
for the degree of Doctor of Philosophy in Law and Public Policy
in the College of Social Science and Humanities of
Northeastern University
May 2017

3
Abstract
Racial/ethnic disparities have been a long-standing problem associated with minority
healthcare and health status. The consequences and ramification of persistent disparate
healthcare is expressed in the overall poorer health status of minority groups in comparison to
non-minority groups. The source of poor minority health status has been attributed to various
causes, including inherent genetic inferiority, iatrophobia, and a wide array of impeding social
determinants such as poor education, poor healthcare literacy, poverty/SES, racism and implicit
bias.
The purpose of this study was to address the paucity of empirical studies examining the
relationship between race/ethnicity and the post-surgical functional outcomes of individuals who
had a total hip replacement (THR). This study differs from previous ones in its’ focus on
functional rather than the surgical outcome or medical issues related to this surgical procedure.
Specifically, this research was conducted to examine whether there were similar functional
outcomes across racial/ethnic CMS beneficiary groups who underwent a common elective
surgical orthopedic procedure (THR) and received post-acute care physical rehabilitation through
a Medicare certified home health care agency.
The socioecological model (SEM) was the theoretical framework used for this study.
This model proposes consideration of the research inquiry from some of the five interactive
components of SEM (intrapersonal, interpersonal, community, organization/institutional,
structural) The CMS data set that was utilized provides the opportunity to consider the outcomes
directly to some of the levels of the model and suggest how other findings might better be
explained from a different perspective.
This was a retrospective cohort research design study based on secondary analysis of
Centers for Medicare and Medicaid Services (CMS) administrative claims and assessment data

4
files of 21, 448 beneficiaries who underwent a total hip replacement in 2012 and were discharged
from the acute care hospital to their homes with post-acute physical rehabilitation through a
CMS certified home health care agency. Analysis of functional outcomes, based upon the
beneficiaries transfer and ambulatory status as assessed within one episode of home health care
services (60 days) using the Outcome and Assessment Information Set (OASIS),
Descriptive statistics as well as bivariate analysis, multivariate and multinomial logistic
regression analyses were conducted to examine the effect of each individual variable on the
outcomes of interest (transfer and ambulation ability). Race/ethnicity was the one factor that was
consistently found to have a statistically significant impact on transfer and ambulation outcomes.
When all variables were considered in the multivariate analyses for ambulation, minority groups
were 1.3 to 2.6 times more likely to be moderately to totally dependent in their
ambulation/locomotion abilities. These results confirm racial/ethnic disparities in the functional
outcomes of this study sample and support the need for a culturally competent, patient cantered,
health care system to better address inequitable patient outcomes.

5
Acknowledgements
I take this opportunity to express by sincere gratitude to the co-chairs of my dissertation
committee co-chairs, Dr. Judith Barr and Dr. Alisa Lincoln who along with committee members
Dr. Gia Barboza and Dr. Gary Young for their unwavering support and guidance throughout the
dissertation process. Your thought provoking questions and feedback on the several drafts of the
manuscript kept me focused and directed towards my successful outcome.
A very special thank you to my dear friends, extended family and colleagues who
cheered me on, and provided an attentive listening ear as I related yet another rendition of my
proposed research. To everyone who was much more confident than I was, that I could complete
this task, I truly thank you.
To my immediate family, despite all the writing I have been doing recently, I don’t think
I can ever find the words to thank you enough for your immeasurable emotional support,
encouragement, prayers, and positive thoughts that were instrumental in sustaining along the
PhD journey. Our sons, Eric and Alex, without any words other than those of encouragement
and undaunting confidence in my ability to attain my goal made it clear that I most certainly had
to practice what I preached. Their belief in me, gave me the confidence to persevere whenever I
was doubtful of the results. Last, but by no means least, merci beaucoup to my husband, Jean-
Robert, for his love, patience and faith in me. I am very fortunate to have such loving family
and friends.

6
~Dedication~
This academic achievement is dedicated in loving memory of my parents
Enid (Née Hobbs) & Gerald Welch
who inspired and instilled in me
the importance of education
&
the value of perseverance in attaining ones’ ultimate goals

7
TABLE OF CONTENTS Abstract 4
Acknowledgments 5
Dedication 6
Table of Contents 7
Lists of Abbreviations, Figures and Tables 8
Chapters
Chapter One – Introduction 10
Chapter Two – Literature Review 17
Chapter Three – Linking Theory to the Research Model 68
Chapter Four – Methodology and Research Design 74
Chapter Five – Results 92
Chapter Six – Summary, Conclusion, Future Studies, and Recommendations 119
References 149
Appendix 1: Figures 163
Appendix 2: Tables 167
Appendix 3: OASIS Worksheet Variable Selection and justification 204
Appendix 4: OASIS C 215
Appendix 5: National Standards for Culturally and Linguistically Appropriate Services 239

8
List of Abbreviations, Figures and Tables
List of Abbreviations
AAAL Arthritis - Attributable Activity
ADL Activities of Daily Living
AHRQ Agency for Healthcare Research and Quality
APTA American Physical Therapy Association
BiDIL Isosorbide Dinitrate/Hydralazine HCI
CAPTE Commission on Accreditation in Physical Therapy Education
CDA Cumulative Disadvantage
CDC Center for Disease Control & Prevention
CLAS National Standards for Culturally and Linguistically Appropriate Services
CMS Center for Medicare & Medicaid Services
DHHS Department of Health & Human Services
DUA Data Use Agreement
EMTALA Emergency Medical Treatment &Active Labor Law
FPL Federal Poverty Level
GDP Gross Domestic Product
Ha Alternative Hypothesis
HHA Home Health Agency
HHC Home Health Care
HHS Health & Human Services
HIPAA Health Insurance Portability & Accountability Act
Ho Null Hypothesis
ICD – 9 International Classification of Diseases & Related Health Problems
IMD Implantable Medical Device
IOM Institute of Medicine
IRB Internal Review Board
IRF In-patient Rehabilitation Facility
LBW Low Birth Weight
NCMHD National Center on Minority Health
NIH National Institute of Health
OASIS Outcome and Assessment Information Set
OBQI Outcome-Based Quality Improvement
pt. Patient
P.T. Physical Therapist
QMB Qualified Medicare Beneficiary
ResDAC Research Data Assistance Center
RIF Research Identifiable Files
SEM Social Ecological Model
SNF Skilled Nursing Facility
THA Total Hip Arthroplasty
TJR Total Joint Replacement
TKR Total Knee Replacement
USSC United States Supreme Court
VA Veterans Administration
WHO World Health Organization

9
List of Figures
Figure 1.1 Population by Race and Hispanic Origin: 2012 and 2060
Figure 1.2 Key Components of the Social Ecological Model
Figure 2.1 The Social Ecological Model: Theoretical Model Applied to this Study
Figure 2.2 Beneficiaries’ Discharge Disposition Following Orthopedic IMD Admission, by
procedure, 2003 – 2009.
Figure 5.1 Study Universe Flowchart
List of Tables
Table 2.1 Definitions of Health Disparities, Health Inequities, and Health Equity
Table 2.2 Definitions of Health Care Disparities and Health Care Equity
Table 2.3 Social Ecological Model: Conceptual Theoretical Model Applied to this Study
Table 2.4 Racial/ethnic Population & Incarceration Rate Within the United States
Table 2.5 An Overview of Racial/e\Ethnic Disparities in Physical Therapy
Table 3.1 Donabedian’s Structure, Process, Outcome: Conceptual Model Applied to this
Study
Table 4.1 Characteristics of CMS Claims & Assessment Files Used for Data Sources
Table 4.2.1 Pilot Study Data Objective 1
Table 4.2.2 Pilot Study Data Objective 2
Table 4.3 Structural and process Variables of the Study Defined
Table 5.1 Study Sample Characteristics/Donabedian Structural variables
Table 5.2 Study Sample Characteristics: Donabedian Process variables by Race/Ethnicity
Table 5.3.1: Study Sample Characteristics: Transfer Ability Outcome by race/ethnicity
Table 5.3.2: Study Sample Characteristics Donabedian Ambulation/Locomotion Outcome by
race/ethnicity
Table 5.4 Functional Outcome Measures and Race/Ethnicity: Transfer
Ambulation/Locomotion
Table 5.4.1 Functional Outcome Measures, Age
Table 5.4.2 Functional Outcome Measures, Gender
Table 5.4.3 Functional Outcome Measures, Comorbidities
Table 5.4.4. Functional Outcome Measures, Rural/Urban
Table 5.4. 5 Functional Outcome Measures, Socioeconomic
Table 5.4.6 Functional Outcome Measures, Length of Stay
Table 5.4.7 Functional Outcome Measures and Physical Therapy Charge Amount
Table 5.4.8 Functional Outcome Measures and Number of Days to Discharge Assessment
Table 5.5 Odds Ratio Estimate – Transfer Status: Crude, Adjusted& Relative Importance
Table 5.6 Multinomial Logistic Regression Odds Ration for Transfer Ability:
Reference = Independent
Table 5.7 Multinomial Logistic Regression Odds Ratio for Transfer Ability:
Reference equals Minimal Dependence
Table 5.8 Odds Ratios Estimate – Crude and Adjusted for Ambulation/Locomotion
Table 5.9 Impact of Independent Variable on Process: Physical therapy Charge Amount
Table 5.10 Impact of Independent Variables on Process: Length of Stay
Table 5.11 Impact of Independent Variables on Length of Home Health Care Services

10
CHAPTER 1
“Of all the forms of inequity, injustice in health care is the most shocking and inhumane”
Martin Luther King Jr.
Introduction /Background
Disparities in healthcare, the “racial or ethnic differences in the quality of healthcare
that are not due to access-related factors or clinical needs, preferences and appropriateness of
intervention” (Smedley, 2003), have been a matter of record in the United States for more
than a century. In 1906, W.E.B. DuBois, as reported by Gamble & Stone (2006), used data
from census reports, vital statistics and insurance company records to document the health
disparity between black and white Americans. Technological advances in science and
medicine have greatly improved the health status of Americans in aggregate. However,
although all have seen some improvement, it is not shared equally. Morbidity and mortality
indicators document the persistence of disparities across racial and ethnic populations. The
prevalence of asthma, cancer, diabetes, HIV, hypertension, obesity, preterm births, and
smoking is greater among the minority than non-minority population (Isaac, 2013). Mortality
rates for coronary heart disease and strokes, homicide, and infant mortality are generally more
prevalent among all minorities when compared to non-minorities. There are however
exceptions such as whites exceeding American Indian & Alaska Native (AIAN) and Asian
Pacific Islanders (API) in regard to coronary heart disease (CHD) and Hispanics having lower
death rates for both CHD and strokes than whites (Isaac, 2013).
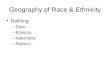
As illustrated in Figure1, the demographics of the United States are changing and
trending towards the emergence of a “majority minority” population defined as the point at
which the combined racial and ethnic minority populations will be greater than 50 percent.
According to the US Census 2014 National Projections, this transition will occur in 2044,

11
when 50.3 percent of all Americans are projected to be self-identified as a member of any
group other than non-Hispanic white (Colby & Ortman, 2014). Five states or equivalents
(Hawaii, District of Columbia, California, New Mexico, and Texas) already have attained a
majority-minority demographic profile. The aging of both the American born or native “baby
boomer” generation and the rising non-white foreign-born population will yield an increase in
the population of the older adult (age 65 and older). Should the current health disparity trends
persist, the majority of the population will be those of poorer health and suffer greater
morbidity and mortality rates than the expected new minority – non-Hispanic whites.
Regardless of the distribution across racial or ethnic lines, any such inequity is a matter of
social injustice. However, there are also potentially huge fiscal ramifications if the current
health care systems and the minority health status remain unchanged. The cost to Medicare
for the older adult and health care cost under the Affordable Health Care Act for those
younger than 65 will be increased due to the projected larger majority- minority segment of
the US population who as noted above, are those with greater morbidity issues than their non-
Hispanic white counterparts.
Figure 1.1

12
The potential effect of a nation where the majority of the population is in poor or
substandard health is daunting. Accounting for 17 percent of the gross domestic product
(GDP), the 2014 national health expenditure was $3.0 trillion or $9,523 per capita. Health
spending is projected to grow 1.3 percentage points faster than the GDP per year during the
ten-year period between 2015 and 2025 (CMS.gov). In a study commissioned by the Joint
Center for Political and Economic Studies and conducted between 2003 and 2006, LaVeist et
al (2009) estimated the economic burden of health disparities via direct medical cost, indirect
cost of health inequalities and the cost of premature death. Their report projected medical
care and lost productivity cost due to racial disparities in health amounted to a $309 billion
annual loss to the U.S. economy. By eliminating minority health inequalities, indirect cost
associated with illness and premature death would have been reduced in excess of $1trillion
during the period of their study. Hence, a population predominantly in substandard health,
challenged with continued rising health care cost, does not bode well for the future of our
country.
The historical and social determinants of disparities in both health care and health
status currently seen in the United States have been well documented throughout health care
literature (Heckler, 1985) (Smedley, 2003) (AHRQ, 2015) (Healthy People, 2020) (Healthy
People, 2010) and will be addressed in greater detail in the Chapter Two: Literature Review of
this dissertation. Many disparities in health and health care have been well documented (ibid)
(Isaac, 2013) as have an array of social determinants such as social economic status, racism,
implicit bias, the built environment in which people live, etc. (LaVeist, 2005) (Williams,
2010). However little of this work considers the plausible factors of disparities in the context
of standardized measures of the individual’s functional outcome explicitly by race/ethnicity as
related to rehabilitation intervention; specifically that of physical therapy (PT) services. This

13
dissertation will focus on the utilization and functional outcomes of Medicare beneficiaries
who have undergone a primary total hip replacement (THR) and received PT through home
care following discharge from the acute care hospital setting.
1.2 Focus Statement: Statement of the problem
The total joint replacement (TJR) – specifically a total hip replacement (THR) is a
surgical procedure to alleviate pain and impaired functional limitations commonly associated
with osteoarthritis. There is extensive existing literature examining the racial/ethnic patterning
of utilization of these procedures and some associated outcomes; i.e. length of stay in the
acute care setting, mortality rates, post-operative hospital readmission, etc. (Dunlop et al,
2003) (Ibrahim, 2010) (Inneh, 2016) (Pierce, 2015) (Shahid, 2016). However, there is a
paucity of research regarding post-operative ambulation and/or other activities of daily living.
The goal of my research is to build on the existing literature examining disparities in minority
health status and health care specifically by analyzing the impact of race and ethnicity on the
functional outcomes of Medicare beneficiaries who underwent this common orthopedic
surgery.
1.3 The Theoretical Framework
In order to examine the impact of race and ethnicity on the functional outcomes of
individuals who have undergone a THR, I will draw upon the social ecological model (SEM).
This model provides a format that facilitates a multi-level perspective helpful in
understanding multifaceted problems associated with health disparities. The SEM affords the
ability to examine and understand the dynamic interrelations between the individual and the
environmental factors and the ways in which these factors impact health outcomes of interest.
Although this model originated within the fields of psychology and sociology as a
framework for prevention, it has been adapted in accordance to the discipline for which it is

14
being used and/or the problem being examined. However, the overarching common
characteristic of this model /theoretical framework is the emphasis on the fundamental concept
that there exist a reciprocal causation between the multiple levels of the model, such that the
individual or issue at the core of the model both shapes and is shaped by the multiple levels
within the model.
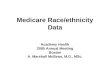
Figure 1.2 Key components of the Social Ecological Model
Source: “Reciprocal Causation” Winch, P (2012) Ecological models & multilevel interventions.
Johns Hopkins Bloomberg School of Public Health. PPT available at http://ocw.jhsph.edu/courses/healthbehaviorchange/PDFs/C14_2011.pdf. Accessed 6/9/12/15.
This research will apply these principles as the theoretical framework upon which utilization of
rehabilitation and functional outcome following a total hip replacement is considered. A more
detailed discussion of this framework is presented in the literature review chapter of this
dissertation.
1.4 Research Focus, Questions & Hypotheses
The overarching goal of this study is to build on the existing body of research and
literature addressing the existence of racial/ethnic disparities in health care and status. Given the
plethora of overall research on disparities and inequities in health and healthcare, I will focus on
whether the same issues exist for those receiving physical therapy rehabilitation services. The
differences in functional outcomes between minority and non-minority cohorts of Medicare

15
beneficiaries’ status following a common orthopedic procedure will be examined to assess health
status disparity. This study is designed to increase the understanding of racial/ethnic disparities
though the examination of outcome measures for those who have undergone a total hip
replacement (THR), also known as and interchangeably referred to as a total hip arthroplasty
(THA).
The principal research question – Are there disparities in the functional outcomes of a
racial/ethnically diverse national study population of Medicare beneficiaries who were
discharged to their home with Physical Therapy rehabilitation through homecare subsequent to a
THR?
Using Medicare claims and assessment data, the main research hypotheses to be examined are:
1: There are racial/ethnic differences in acute hospital length of stay following THR
2: There are racial/ethnic differences in utilization of rehabilitation [Physical Therapy]
during acute hospitalization.
3: There are racial/ethnic differences in functional outcome measures among those who
underwent a THR and subsequently received physical therapy rehabilitation in a home
health care environment.
Secondary analysis of the claims and assessment data is used in this research study to
address these hypotheses. The assessment of the individual’s functional ability will be
measured based on their capability to perform activities of daily living (ADLs) related to
mobility activities needed to function within a community, specifically, the ability to transfer
into and out of a variety of positions and ambulation/locomotion.
1.5 Summary
Disparities in the health care and status between minority and non-minority sub-
populations remain a persistent public health issue. These disparities are most often described in

16
terms of health and healthcare indicators that confirm racial and ethnic minorities have poorer
access to care, higher infant mortality rates, greater prevalence of disease etc. Less is found in
analysis of the impact of race/ethnicity on functional outcome following a common surgical
procedure. In this study, I propose to contribute to the existing health disparities literature by
determining whether racial/ethnic inequities are found in functional outcomes as assessed
through a standardized assessment tool (OASIS) and reported in Medicare data files. Given that
health equity has been described as the “principle underlying a commitment to reduce – and
ultimately, eliminate – disparities in health and its determinants, including social determinants”
(Braveman, 2014), based on my research findings, a second goal of my research is to propose
policy that will promote incentives for the provision of quality care that yield equitable
functional outcomes and decreases disparities in individual health status.
The rest of this dissertation is organized as follows. Chapter Two presents the literature
review. Chapter Three serves as the bridge between the literature and the methodology used in
this research. Chapter Four provides the methodology and the research model used for this
study. The results of the study are presented in Chapter Five and Chapter Six completes this
dissertation with conclusions, recommendations and proposed topics for future research.

17
Chapter 2 Review of the Literature
2.1 Introduction
Racial and ethnic disparities in health and health care persist despite the many advances
in modern technology and medical innovations provided over the past several decades. The
overall United States population’s health has improved; however, however, it has improved at a
lower rate for racial/ethnic minorities. For centuries, optimal health status and health care have
been vastly different across racial/ethnic lines. These differences are a well acknowledged,
evidenced-based, compelling issue that continues to plague minorities nationwide (AHRQ, 2015)
(Satcher, 2005), (Smedley, 2003). Racial/ethnic disparities in health status and health care are the
focus of this literature review. This review begins with a discussion of the terms associated with
health disparities and is followed by social issues associated with disparities found to be related
to health status and healthcare in general as well as in terms of physical rehabilitation
specifically related to the total hip arthroplasty. The Social Ecological Model is introduced as
the theoretical framework for this research. Next, I discuss the historical perspective of the
cross-racial relations resulting in social differences between European/American colonialists and
enslaved Africans, highlighting the ways that history provides context for understanding racial
and ethnic health disparities today. Finally, some of the key structural laws and policies related
to the current state of distinctive differences in minority vs. non-minority health are considered.
2.1.1 Disparities, Equality, Equity: A Discussion of the Terms
Several terms are associated with the differences seen in health status and health care
utilization and outcomes among US sub-populations. Commonly used terms include disparities,
inequalities and inequities in reference to differences among diverse racial and ethnic groups in
comparison to those of non-Hispanic white origins. In some cases, these terms are used

18
interchangeably in discussion associated with the variances in health status and health care seen
across various racial and /or ethnic populations. It is therefore helpful to define these terms.
As noted by Isaac (2013), there is not a clear or universal definition or uniformity of
measurement, of how we typically reference the study of race, ethnicity and health status or
differences in healthcare outcomes. While in the United States the more common terminology is
racial and ethnic health disparities, the most common global nomenclatures are health
inequalities and health inequities. There is reportedly no consensus regarding the terminology
(ibid). Table 2.1, of the Appendix, taken from Isaac publication based on the work of Braveman
(2006) and Carter-Pokras and Baquet (2002), provides a summary of the definitions used by
different government agencies as well as authors conducting research in this aspect of health and
health care. A review of the definitions reveals a common characteristic: all indicate that there
are differences in health outcomes and health status among populations. Each health status or
health care definition suggests that something is unjust and needs to be fixed (Isaac, 2013).
Table 2.2, of the Appendix also adapted by Isaac from Braveman’s work (2006), summarizes
health care disparities and quality. These tables have been chosen because they summarize both
the breadth of definitions and the nuances among these commonly used terms in the literature
related to health and healthcare differences.
2.1.2 Racial/Ethnic Disparities in Health: An Overview
Health is defined by the World Health Organization as “a state of complete physical,
mental and social well-being and not merely the absence of disease or infirmity” (WHO,
1948). For many measures of health across the lifespan, African Americans, and in some
cases members of other racial and ethnic groups, consistently fair worse than the non-

19
Hispanic white majority segment of the United States population. Key statistical findings
from the most recent CDC Health Disparities and Health Inequalities Report - United States,
2013 notes four indicators that are related to some of the health disparities seen in our
country. First, the primary cause of death, cardiovascular disease, is at least 50 percent more
probable as a cause of premature death due to heart disease or stroke in non-Hispanic black
adults than their non-Hispanic white equivalents. Second, type 2 diabetes is more prevalent
among Hispanics, non-Hispanic blacks, and those with interracial profiles than among non-
Hispanic whites and Asians. Diabetes is also higher among adults without college degrees
and those with lower household incomes. Third, the infant mortality rate of non-Hispanic
blacks is more than twice the rate of non-Hispanic whites. In contrast, people who identify
as Asian and Pacific Islander had fewer deaths than expected and as such are a good example
of lower than anticipated minority disparities. Geographic location was also found to be an
influential factor of this indicator, in that rates of infant mortality were found to be higher in
the South and Midwestern parts of the country compared to other regions. Fourth, suicide
was found to be highest among American Indians/Alaska Natives and non-Hispanic whites.
However, regardless of race or ethnicity, men were found more likely to commit suicide than
women, (CDC 2013)
Trends in cancer mortality and morbidity in the US demonstrate the persistence of
racial/ethnic disparities in health in spite of overall advances in medical technology yielding
overall improvement in health. Minorities die from cancer at a disproportionally higher rate
than their non-minority counterparts. This has found to be especially true as related to
African Americans who have a one-third greater risk of dying from cancer than their white
counterparts. Despite overall cancer deaths decreasing, racial/ethnic disparity across groups

20
persists and prevalence remains higher among African Americans with men having a higher
death rate than women (Isaacs, 2013) (CDC, 2013). Similar to mortality data, the chronic
disease morbidity data also reveals that minorities fare worse than whites; specifically,
blacks/African Americans present with the highest incidence for diabetes, HIV, hypertension,
preterm births and obesity (ibid). Thus, overall collective individual health status, as
exemplified via several morbidity and mortality indexes, is poorer within the minority
community when compared to the non-minority population.
A myriad of factors across several disciplines have been found to be associated with the
aforementioned differences in health status and health care among the diverse racial and ethnic
groups of the United States population. Therefore, I review empirical and theoretical research,
as well as literature relevant to health disparities and inequities to address this very complex
problem. Sources of reference included in this dissertation come from healthcare, medicine,
history, sociology, psychology, law and policy.
As the above referenced tables and discussion indicate, there is a rather wide range of
and variation in definitions of the terms. In this dissertation, I specifically examine
racial/ethnic health disparities as differences in post-orthopedic surgical functional outcomes
in transfer and ambulation abilities based upon social and demographic variables (e.g., gender,
race/ethnicity, age) of the individuals within the Medicare beneficiary population studied.
The process by which health care is delivered to the study sample (i.e., length of hospital stay
or number of days of care) represents health care disparities, while racial and ethnic
differences in the level of functional outcomes of Medicare beneficiaries studied addresses
whether the attained outcome is equitable across racial/ethnic population groups.

21
2.2 Theoretical Framework
The Social Ecological Model (SEM) provides the theoretical framework used to
understand the dynamic interrelations among the individual, interpersonal, and the environmental
factors as well as the structural laws and policies related to the primary research question of this
dissertation: whether there are racial/ethnic disparities in the functional outcomes of CMS
beneficiaries discharged with home care subsequent to a THR. The theoretical framework is
also offered to give the reader the context for policy recommendations.
The causes of racial/ethnic health disparities that have been documented over the
centuries in healthcare and health status cannot realistically be attributed to any single factor.
Disparities in this realm are certainly a multifaceted problem. Persistence of this issue can be
credited to problems of multiple origins and/or viewed and assessed from various
perspectives. The SEM is a framework that provides a lens that facilitates a multi-level
approach to studying disparities in health status for the cohort that will be examined in this
dissertation.
The determinants of health include the myriad of personal, social, environmental and
economic factors that impact health status. Among the broad categories of health
determinants are: biological/genetic composition, individual behavior, social interaction and
norms, the physical environment, economic status and access to health services. Stress,
obesity, birth defects, discrimination, housing conditions, unemployment and education are
all examples of determinants that can positively or negatively impact health. Laws and
policies that regulate any factors within the broad realm of health determinants will also have
an effect on health status (Healthy People, 2020). Examples of the latter would include
taxation on tobacco products and consequently the impact such tax has on access to these

22
products by the indigent due to prohibitive cost. The United States Supreme Court’s June 28,
2012 upholding of the Patient Protection and Affordable Care Act and its individual mandate
represents a legislative measure that impacts access to health care (Oberlander and Perreira,
2012). Each of these factors can be expressed from the standpoint of the SEM which
provides a means to organize the various determinants of health.
This model evolved from the work of Urie Bronfenbrenner (1977) who proposed the
ecology of human development as a means to consider child development from the child’s
perspective of his/her environment, the actual environment in which the child exists and the
interaction between the individual and the environment. (Reifsnider 2005). Bronfenbrenner’s
ecological development model was based upon the premise that understanding human
development should not rely solely on direct behavior observation, but rather requires
“examination of multiperson systems of interaction” in various settings to account for the
impact of the environment in which the child/individual is developing (op. cit.
Bronfenbrenner 1977). Thus, his model can be seen as a lifelong reciprocal interaction
between the growing individual and the changing environment. Bronfenbrenner’s ecological
model is composed of four interactive components that are embedded within each other. The
microsystem is the inner most level of the developmental model and holds the mother and
child. The mesosystem includes interrelations of the developing individual at a specific point
in their life. For example this system includes family, friends, sports teams for the child,
while for their parents, it may include their work environment or their child’s daycare center.
As Bronfenbrenner succinctly states, “a mesosystem is a system of microsystems.” The third
component defined-the exosystem is an extension of the mesosystem and includes the social
systems in which the developing individual and/or parent is not necessarily an active

23
participant, but include society’s institutions that have an impact on individuals within the
given environment, i.e. “the neighborhood, media, local, state & federal government agencies,
distribution of goods and services, transportation” (Bronfenbrenner, 1977; Reifsnider, 2005).
The final component of the ecology of human development model is the macrosystem and
refers to the “overarching institutional patterns of the culture or subculture.” This component
contains the “blueprint” or prototype for the culture and affords consistency such that there is
a general similarity within for example, the school systems, how the court system operates,
and the official language (ibid).
Although the SEM originated from the field of developmental psychology, it is widely
accepted and utilized as a framework across many disciplines of public health where it is often
linked to prevention of illness and/or health and wellness promotion. Later models of health
promotion proposed by McLeroy (1988), and Stokols (1992, 1996) originate from
Bronfenbrenner’s model and combine the individual’s intrapersonal attributes (attitudes,
knowledge skills, biological factures, sex, beliefs perceptions etc.) with interpersonal,
organizational/community and public policy to take into consideration the interactions of the
various potential factors that are interrelated and span diverse populations and several
environmental factors related to health and illness (Stokols,1996).
As presented by Dr. Kristine Gebbie at a 2003 Institute of Medicine workshop, “Who
will Keep the Public Healthy?”, the ecological model is “a model of health that emphasizes
the linkage and relationships among multiple factors (or determinants) affecting health”
(Hernandez, 2003). This definition acknowledges a dynamic interplay across the many factors
influencing health and wellness in contemporary times. SEM considers the influence and
interdependence of five dimensional levels: the individual, interpersonal/microsystem,

24
organizational/mesosystem, community/ecosystem and policy/macrosystem level. At the core
of this model is the individual, who is surrounded by the remaining four factors, which will
potentially impact the functional outcome of individuals who in the case of this research, have
undergone a THR. Using the SEM lens this research will examine hypothesized disparities in
the functional outcome of CMS beneficiaries who have under gone the relatively common
surgical orthopedic procedure, THR.
Table 2.3 The Social Ecological Model
Social Ecological Model Level
Description
Individual/ Intrapersonal Individual characteristics that influence ones behavior, including but not limited to: gender, age, racial/ethnic identity, SES, knowledge , attitudes , skills, self-efficacy, religious identity, health literacy, expectations.
Interpersonal Social support systems of the individual (both formal & informal) that can influence the individuals’ behavior and provide identity. Examples include family, friends, peers, religious networks, customs, traditions etc.
Organizational/Institutional The formal and informal rules and regulations policies and structures that regulate the behavior or operation of social institutions and organizations.
Community Norms and regulations, includes the built environment [i.e. parks], village or tenant associations, community leaders, businesses.
Structural/ Laws, Policy Laws, policies at the local, state, federal or global level that regulate and support actions and practices.
Adapted : from Winch, P (2012) Ecological models & multilevel interventions. Johns Hopkins Bloomberg School of Public Health. PPT available at http://ocw.jhsph.edu/courses/healthbehaviorchange/PDFs/C14_2011.pdf. Accessed 6/9/12/15
Drawing upon the SEM, and as illustrated in Table 2.3, there are several potential
intrapersonal factors(e.g., the number and severity of comorbidities, socioeconomic status, age,
gender, racial/ethnic identity, health literacy, expectations) that may impact individual utilization
of rehabilitation services and postoperative functional outcome subsequent to a THR. At the
microsystem/interpersonal level, social support systems, both formal and informal, are the most
intimately linked level of the model to the individual, and as such are in position to directly
influence individual behaviors and outcomes. Social support of family and friends as well as

25
personal relationships between the individual and those involved in his or her care, i.e. healthcare
providers, are factors of critical importance at this level. The community level includes
institutional rules and regulations for the operation of systems or organizations that are executed
at the mesosystemic/organizational level. The focus at this level relates to how characteristics of
a given organization can influence behavior. Consequently, factors implemented at this level
may negatively or positively affect the individual. In the case of this study, the efficiency of
community home health care agencies has the potential to facilitate or hinder the individual’s
functional outcome. Access to and affordability of resources within the exosystem/community
of the individual’s built environment (i.e., transportation, healthcare systems, informational
networks) each have the potential to impact the individual as well. The macrosytem/social and
political level is the outer most of the tier of the SEM and, as it relates to this specific study, is
concerned with laws and policies across all governmental levels regarding allocation of
resources, guidelines for accreditation of institutions, the criteria for initial issuance and renewal
of professional licensing, as well as Medicare (CMS) regulations. Within the confines of the
Medicare data obtained, this research will examine levels of the SEM as the theoretical
framework upon which utilization of rehabilitation and functional outcome following a total hip
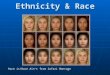
replacement is considered. Figure 2.1 illustrates aspects of the SEM levels specifically
considered relative to in this dissertation.

26
Figure 2.1 The Social Ecological Model. Adapted from the Centers for Disease Control and Prevention (CDC), The Social Ecological Model: A Framework for Prevention, http://www.cdc.gov/violenceprevention/overview/social-ecologicalmodel.html (retrieved April 21, 2014).
2.3 A Historical Background/Perspective
“If you want to understand today, you have to search yesterday”- Pearl S. Buck
2.3.1 The Antebellum Period
Historically, health disparities in the United States can be rooted back to the
rationalizations and prevalent beliefs held by colonial Americans and entrepreneurial
Europeans during the era of slavery. The formal and informal beliefs can be viewed as the
foundation upon which the interpersonal racial basis of slavery was justified.
Although the initial workforce was comprised of indentured servants and convicts, their
relatively limited number compared to the vastness of the land to be colonized was not
sufficient. In addition, as this labor force was Caucasian, it was difficult to distinguish this
cohort from the free segment of the population. Unsuccessful attempts to enslave the Native
Americans led to participation in the African slave trade to increase the colonial workforce.
STRUCTURAL/Laws / Policy Black Codes , Jim Crow laws
•CMS: Healthy People 2020 , health care professional licensing & accredidation
Organizations/Institutional Slavery, post emacipation segregation
Community
Built environment; Rural/Urban location
Interpersonal/SOCIAL SUPPORTIplicit Biasis, impact of incarceration on minority family structure & support, patient/healthcare professional
relationships
IndividualAge, gender, racial/ethnic identity, intenalized racism,
health status, # of comorbidities, surgical expectations

27
The initial shipment of slave labor arrived in Jamestown VA in 1619, and afforded colonial
settlers the advantage of a color coding system that made it easier to identify runaway slaves
(Krieger, 1987).
Justification for the enslavement of Africans ranged from the supposed support of biblical
scripture to pseudo-scientific research. From the perspective of the former, it was interpreted
that God allowed non-believers to be enslaved. It was discerned that since Africans were
infidels, they met God’s criteria for enslavement. As such, the Africans were the perfect
source of labor needed to develop the colonies in the New World for the “greater glory of
God and King” (ibid, Krieger pg. 261). However, non-believers could be converted and to
evade this paradox of Christianity-invoked slavery, the Europeans sought and found a
solution to this dilemma via their interpretation from the Book of Genesis related to Noah’s
son Ham. Their conlusion was that due to color “Africans were the decedents of Ham, cursed
son of Noah, consigned by God to a fate of perpetual servitude” (Ibid). “Scientific” support
of enslavement was derived from Southern physicians, many of whom benefitted from the
slave trade by rendering medical service to plantations as well as being compensated for
auction block inspection of slaves to see if they were fit to be sold (Kreiger, 1987)
(Washington, 2006). Rather than honest considerations of the impact of the substandard
living and inhumane working conditions to which the enslaved were subjected, doctors
attributed the observed racial health disparities (i.e. greater infant mortality among African
children or the twice as many blacks than whites who died of tuberculosis) to race The
enslaved were considered to have abhorrent maternal behaviors such as “destroying their
offspring”, or innate deficiencies such as inability to adjust to the “temperate climate” of the
South. In sum Pendleton and his medical peers, as reported by Krieger, ascribed health

28
related issues to the “peculiar constitution” of blacks instead of the “peculiar institution” of
the South (Op Cit).
Scientific racism in the form of non-anesthetic experimental surgical procedures, medical
experimentation and conscription for post mortem dissection were used as mechanisms to
validate Anglo-European ethnocentrism (Washington, 2006) (Krieger, 1987). These invasive
pseudoscientific procedures were supposedly conducted as a means of confirming the
biological differences and cognitive inferiority of blacks, and therefore were actions to
substantiate the rationale for their enslavement. The biblical and “scientific evidence”
through the mid-nineteenth century “proved” racial differences and confirmed black
inferiority and white supremacy as the duplicitous rationalization for slavery.
Enslaved Africans were considered the same as any other personal property of the slave
owner; their treatment was equivalent to that given to other proprietary investments such as
livestock (Washington, 2006 -pg. 48). An excerpt of the court’s opinion presented by Chief
Justice Taney in reference to, the United States Supreme Court’s Dred Scott decision [1857],
succinctly summarizes the continuous sentiment of black inferiority:
“They had for more than a century before been regarded as beings of an inferior order, and altogether unfit to associate with the white race, either in social or political relations; and so far inferior, that they had no rights which the white man was bound to respect; and that the negro might justly and lawfully be reduced to slavery for his benefit. He was bought and sold, and treated as an ordinary article of merchandise and traffic, whenever a profit could be made by it” (Taney, 1857).
2.3.2 Postbellum Period
Laws implemented following emancipation demonstrate white farmers’ and political
leaders’ attempts to rebuild racial order. State legislatures passed a series of Acts known as Black
Codes (Oshinsky,1996). Under the Black Codes, enforced in the mid 1860’s black people were

29
free in their person and property, but not socially or politically equal to whites. These laws
effectively upheld racism and white supremacy following emancipation. The strict enforcement of
Black Codes became a way to reestablish the master-slave dynamic between former slaves and
slave-owners.
At the turn of the 20th century, a vast majority of states (primarily in the south) enforced
segregation via state and local Jim Crow laws that stemmed from the Black Codes. States
imposed legal punishments for black people who interacted with white people. Like the Black
Codes, these laws criminalized black people for being present in certain spaces and aiming to
achieve goals of a free person. This explicit form of legally enforced segregation persisted until it
was outlawed a century after emancipation during the Civil Rights era. Both Black Codes and
Jim Crow laws represent forms of social exclusion that facilitated the persistence of segregation
and racism of earlier historical periods.
The innate destiny of an involuntary workforce was legally terminated with the
Emancipation Proclamation. Nonetheless, the eugenics movement of the early 20th century
was the source of the unremitting search for evidence to classify blacks among the inferior.
The profile of “eugenic misfits” included those with psychomotor impairments, who were
indigent, black, uneducated, criminals, recent immigrants, whereas those who were highly
educated and of good social class were representative of the eugenically superior
(Washington, 2006).
Perhaps one of the more notorious examples of egregious medical mistreatment of humans is
found in the Tuskegee Syphilis Study conducted under the auspices of the U.S. Public Health
Services [1932-1972]. This study deceitfully recruited 600 black men infected with syphilis to
be treated, when in fact they were being used to study the natural progression of this disease

30
without treatment over the forty-year period. Only 7.5% or 30 men of the study’s participants
managed to circumvent obstacles put in place to obstruct their ability to avail themselves of the
effective pharmacological treatment – penicillin – which became available in 1943, almost 30
years before the Tuskegee study was terminated. Iatrophobia among many blacks can be
understood by the aforementioned social and medical actions as well as the continued refinement
of surgical techniques from gynecological procedures of the 1860s for vesicovaginal fistula to
cardiac procedures in 2001 with the Abio-Cor artificial heart using black “subjects”
(Washington, 2006). Among examples of other social and medical circumstances that may have
contributed to some of the mistrust by minorities in the health care system are: being the subjects
for non-consensual sterilization, radiation (plutonium) experimentation, “black only”
pharmaceuticals for heart failure (BiDIL), the Central Intelligence Agency’s release of disease-
carrying mosquitoes into black communities in the 1950s and 1960s, and the random intravenous
transfusion of artificial blood (PolyHeme) to severely injured and usually unconscious
emergency department patients in Detroit (Ibid).
There is little, if any, substantial rational basis to utilize race for much other than a
phenotypic marker of an individual. M.F. Ashley Montagu (1941) explained more than 70 years
ago that the idea of race can be traced back to the “scholastic naturalization of Aristotle’s work,
’Predictables of Genus, Species, Difference, Property and Accident’, and then onward “to the
early stages of the Age of Enlightenment when Linnaeus considered the concepts of Class,
Species and Genus from the theologians to serve as systematic tools. The term race was actually
first introduced into the literature of Natural History by Buffon who in the year 1749 used it to
describe six groups of man” (Montagu, pg 244). The word race was used as a term of
“convenience” to identify a subdivision of the same human species of different geographic

31
regions. Gene variability and genetic mutation along with many secondary factors were
explained as the evolutionary basis of the changes seen in people and account for several
significant features of identification such as variations in skin pigmentation, eye color, facial
features or hair texture, all of which are expressions of genetic traits within various components
of the same human race, but characteristics of different species. Without scientifically based
evidence to prove otherwise, it is difficult to accept the variations among humans as much more
than just that, a variance in traits or characteristics. No weakness has been identified that would
make an individual more susceptible to greater morbidity or mortality on the basis of race alone
(La Veist, 2005). However, several social conditions associated with race can subject one to a
plethora of social conditions which can expose an individual to the discriminatory social mores
in vogue at the time. The literature identifies these types of conditions, largely socio-economic
in nature, to be associated with risk factors for and vulnerability to many problematic
health/medical conditions.
The “conceptual model of race” developed by LaVeist in 1994, is also referred to as the
physiognomy model of race and health. This model indicates that the individual’s phenotype is
used as the default trait of identification - race. LaVeist explains the route to racial/ethnic
disparities as a function of both social and cultural or behavioral factors a group of people are
subjected to based primarily on their phenotype. The former (social) includes those
characteristics or conditions that are beyond the scope of the individual. Examples include
substandard conditions of the built environment often associated with minority populations, poor
sanitation and other city services, race differences in the receipt of quality medical care, poor
quality housing, discrimination or racism. LaVeist defines the social risk factors as those which
are generally beyond direct individual control. The cultural factors include the behavioral

32
component of the conceptual model of race. These characteristics at the individual level of
ethnic groups affect health or illness and ultimately individual health status, i.e. dietary practices,
the use of tobacco and/or alcohol products, response to stress. Societal factors are linked to
health and illness behaviors as a means to account for the racial differences seen in health status.
Consideration of race in isolation of social and behavioral factors may result in the assumption
that health status is the outcome of the phenotypic attribute when the issue is actually one of
social class (LaVeist, 2002) (LaVeist, 2005). In sum as succinctly defined by Moya and Markus,
“Race…is a complex system of ideas and practices regarding how some visible characteristics of
human bodies such as skin color, facial features, and hair texture relate to people’s character,
intellectual capacity, and patterns of behavior” (Moya and Markus, 2010 pg 62). Nonetheless
the rationalization of ante and postbellum treatment of the non-white racial/ethnic component of
the population hinged on white/European supremacy. The result can be seen as a source of
breakdown of the interpersonal relations at the second SEM level as it relates to racial/ethnic
health disparities.
2.3.3 The Historical Legacy of Racism and Health
One perspective of examining the persistence of the racial and ethnic health disparities
within today’s healthcare system considers the issue as merely a byproduct of the historical
foundation upon which the United States was built. As noted by Jones, (2000) race can be used
to represent onesculture, socioeconomic status, genetic profile etc. However, racial (and ethnic)
classification has historically had, and continues to have, a profound impact that goes well
beyond the phenotypic classification of the individual. “[T]he variable ‘race’ is not a biological
construct that reflects innate differences, but a social construct that precisely captures the impacts
of racism” (Ibid pg 1212). Three levels of racism (institutional, personally mediated and

33
internalized) are considered as the plausible link to the well-documented disparities in health
status, health care and health outcomes that overall are often strikingly poorer within the
minority population in comparison to the non-Hispanic white or majority population.
2.3.3.1 Institutional Racism: SES, Segregation, and the Criminal Justice System
A term coined by Stokely Carmichael, “[i]nstitutional racism relies on the active and
pervasive operation of anti-black attitudes and practices. A sense of superior group position
prevails: whites are 'better' than blacks; therefore, blacks should be subordinate to whites. This is
a racist attitude and it permeates the society, on both the individual and institutional level,
covertly and overtly” (Carmichael, 1967). This form of racism is characterized by differential
access to “goods, services, and opportunities of society by race”; it can be legalized, and
commonly presents as “inherited disadvantage” that may be executed by acts of omission or
commission (Jones, 2000). The historical subjugation of black Americans and other United
States ethnic minorities is inherent and conducive to our nation’s economic system. The history
of emancipation and post-emancipation racialized laws exemplify conscious forms of
institutional efforts to maximize profits, even when it results in the demise of minority health,
and/or socioeconomic conditions.
Socioeconomic status (SES) is most commonly measured by poverty, income, education,
occupation, wealth and any combination of these sub-factors. It is a key factor in explaining the
health disparities existing in the racial/ethnic minority sector of the United States population.
Slaves lived under abject poverty conditions with entire families in one room log or wood and
dirt cabins with dirt floors. Food was plentiful though nutritional value was questionable (Berlin,
Favreau, & Miller,1998 pp 48-49; 132-133; 80). The post-emancipation period was not much
better, nor relatively speaking are the conditions of the present day impoverished minority sub-

34
population. As discussed by LaVeist (2005), members of minority populations disproportionally
experience the lower of all measures used to define an individual’s socioeconomic status.
Whether it is education, level of poverty, occupation or wealth, minorities are at the lowest end
of each dimension. Examination of minority status along these measures reveals that in most
instances, minorities fare far worse when compared to the non-minority population (whites). As
discussed un the introduction, health status varies among the minority sub-group, with some
racial/ethnic groups performing worse than others depending upon the determinant being
measured. However, the minority/non-minority gap is blatantly obvious regardless of the
measure assessed. There is a linear relationship between socioeconomic status and health such
that as one's SES decreases so does one's health (LaVeist, 2005). Thus it is the minority sector
of the population (those with lower education, at the lower poverty levels, poor public school
districts, with the least prestigious jobs, lower paying “blue collar" occupations) that in general
have the worse health. Socioeconomic status is a factor that impacts health at both the individual
and between racial levels as access to health care within the community may be sparse.
Although there is a correlation between SES and poor health among minority
populations, health status is not an exclusive expression of poor health. As demonstrated in data
of the U.S. Department of Health & Human Services and reported by LaVeist, (2005), self-
identification of fair or poor health exists among individuals classified from across the income
spectrum from poor to high income levels. However, while people in all income groups report
fair or poor health the percentage of poor or near poor adults reporting poor health is more than
twice that of middle income and as much as four times or greater than high income adults;
however, many other factors also are significant to health status. Thus it would be inaccurate to
state that poor health is solely a reflection of poor SES (ibid, chapter 8). This inaccuracy is

35
further supported in research which concluded that “ethnic and racial minorities experience a
lower quality of health services and are less likely to receive routine procedures that white
Americans” (Satcher, 2005; Smedley, 2003). In a 2011 study that examined racial disparities
nationally reported to be most prevalent among minorities, disparities were significantly
decreased or completely eliminated when evaluated within a racially integrated, low income
community of southwest Baltimore, Maryland. The higher nationally reported statistics for
hypertension, diabetes and obesity morbidities among blacks were either decreased or erased
when social factors and medical care for black and white Americans were equalized. When
whites are exposed to the same health risks found in urban neighborhoods, their health status was
compromised, similar to that of blacks who more frequently reside in such neighborhoods (La
Veist, 2011)
Racial residential segregation, “the physical separation of the races in residential
contexts” (Williams, Collins 2001), has been identified as another aspect of institutional racism
that can impact minority health. Examples of common characteristics found in minority
communities include high cost groceries of lesser quality that can yield poor nutrition, decreased
recreational facilities and perceived unsafe neighborhoods that are not conducive to physical
exercise, and unequal access to a wide range of municipal amenities as political leaders are more
likely to cut spending and services in poor rather than affluent neighborhood.
The criminal justice system is yet another factor (at the organizational/institutional third
SEM level) which directly or indirectly has the potential to impact disparities in health. Simply
stated, “nowhere are racial disparities more than in the criminal justice system” (Markus, Moya,
2010). A review of racial/ethnic population demographics and incarceration statistics speaks
volumes in regard to the potential impact of mass incarceration on loss of social support within

36
the minority family structure. As seen in Table 2.4, imprisonment is disproportionally higher
among the black, Hispanic and North American Native minority populations relative to their
percentage of the United States population. Per the U.S. 2010 Census reports (vintage 2015),
blacks, Hispanics and North American Native represent 13.3, 17.8 and 0.9 percent of the national
population respectively (U.S. Census, 2015). However, based on National Prison Statistics data,
these three subdivisions of the population account for 37.8, 33.6 and 2.0 percent of the federally
imprisoned (Federal Bureau of Prisons, year?). The mass incarceration of these racial/ethnic
minority populations yields the potential foundation for fractured family and community
structure within these minority groups.
Many aspects of individual, interpersonal and institutional components of racism are
related to the foundation and continuation of the racial/ethnic health disparities. SES impacts
health (via conditions of their built environment, i.e. housing, access to community health care
and /or medical facilities, available healthy food resources etc.). While SES is highly correlated
with race, it is not the sole explanation for health disparities (Williams, Sternthal, 2014) ( Diez,
Mair, 2010). Upon controlling for SES from many outcomes, differences in health status may
still persist across racial/ethnic lines. Therefore, other factors such a s racism, either personally
mediated or internalized, should also be considered.
2.3.3.2 Personally mediated racism
The level of personally mediated racism includes prejudice and discrimination, where
prejudice means differential assumptions about the abilities, motives, and intentions of others
according to their race, and discrimination means differential actions toward others according to
their race. This form of racism can be intentional or non-intentional (Jones 2000) and is
demonstrated via a lack of respect, failure to communicate options, suspicion, devaluation,

37
scapegoating and dehumanization. Multiple studies have focused on implicit bias as an
important covert factor that may influence some healthcare providers in succumbing to providing
unequal treatment to certain racial and ethnic cohorts of their total patient population. Implicit
bias is described as attitudes, thoughts and feelings that often exist outside of conscious
awareness, and thus are difficult to consciously acknowledge and control. These attitudes are
often automatically activated and can influence human behavior without conscious volition
(Gordon et al., 2015). Much of the justification for minority/majority interactions during the
colonial and post-emancipation periods in history (i.e scientific racism, pseudoscientific surgical
procedures, Eugenics, Tuskegee studies etc.) are examples of this thinking rationale.
Research has found that evidence of implicit racial/ethnic bias exists within the current
medical workforce. In a 2007 study, Green et al. asked physicians to evaluate symptoms of a
hypothetical patient admitted to the hospital emergency department with complaints of chest
pain. All patient characteristics with the exception race were identical. Upon completion of
their medical decisions in regard to recommended treatment for the hypothetical patient, the
physicians were given three Implicit Association Tests, which measured implicit bias. Those
who showed unconscious preference for whites were twice as likely to have recommended
lifesaving treatment (i.e. blood clotting drugs) for white than for black patients. The ramification
had this been a live rather than hypothetical patient population would be that blacks with
symptoms of heart attacks would be two times as likely to die due to their doctors’ failure to
prescribe the appropriated treatment.
van Ryn and Burke discovered that physician perceptions of patients were “influenced by
[the] patients’ race and socioeconomic status.” Physicians rated patients of color as less
intelligent than white patients. This was the case even when confounding variables such as sex,

38
age, income and education were controlled. Physicians also reported “fewer affiliative feelings
toward black patients.” Generally, patients of lower SES were given lower ratings on personality
characteristics in terms of self-control and irrationality and perceived intelligence (van Ryn,
2002). The findings also suggest a shared culture in the medical system that transcends
racial/ethnic traits of physicians, as the racist/discriminatory findings were not found solely
among non-minority doctors, who may have found themselves in Jones’ third and final level of
racism, internalized
2.3.3.3 Internalized racism
The third level of Jones’ theoretical framework related to levels of racism is the
internalized racism which is defined as acceptance by members of the stigmatized races of
negative messages about their own abilities and self-worth. This level is characterized by not
believing in others who look like them and not believing in themselves. In this stage the
stigmatized individual accepts limitations to their own full humanity, including their dreams,
rights to self-determination and allowable self-expression, and facilitates embracing “whiteness”.
In sum, it is identified by Jones as a stage of self-hate (ibid).
Frantz Fanon, a psychiatrist native of the West Indies, as discussed by White (2011),
suggests that due to what he dubbed colonialized mentality, people who are marginalized will
adopt the same perception of themselves as their oppressor. “They will themselves come to
believe that their oppressors are indeed smarter, more talented, and more accomplished, while
they are inferior and less capable.” In an attempt to deal with the situation, the marginalized
individual adopts the beliefs, behaviors, attitudes of the oppressor and even belittles and
identifies with him/her by way of a psychological defense mechanism. This self-hatred
paradigm is both “deeply ingrained and largely unconscious” (White, p 167).

39
2.4 Stress and Coping Mechanisms for Racism
Day to day stress may come across as a mere inconvenience to many Americans.
However, research of public health scholars has found biological support that the daily
stresses that ethnic minorities are subjected have psychological/behavioral impacts which
ultimately contribute to health status deterioration and resultant disparities. Response to any
given stressor is likely dependent upon a myriad of factors such the environment; the
intensity, duration of the stressor; and personal characteristics of the stigmatized individual.
Stress levels have been found to cause the brain to trigger endocrine organs to release
hormones such as cortisol and epinephrine to levels that can modify immune function and/or
cause inflammation. Repetitive or prolong exposure to these hormones may “produce ‘wear
and tear’ on organs and precipitate chronic diseases such as diabetes and heart disease”
(McKewen & Gianaros, 2010). Research that studies innate changes in gene
expression(epigenetics) indicates that both the social and physical environment can activate
gene expression and in so doing determine whether a disease develops. The epigenetic trait
can be passed on to children and impact the occurrence of disease in more than one
generation (Braveman et al., 2011).
Examples of health status disparities that are the result of psychological/behavioral
discrimination are high levels of hypertension and low birth weight of infants in ethnic
minority communities and described in the following two hypotheses.
2.4.1 Weathering Hypothesis & Cumulative Disadvantage (CDA) Perspectives
The Weathering Hypothesis, proposed in the 1990s by Professor Arline Geronimus,
indicates that during the early adult years the health status of minorities begins to
prematurely deteriorate. This premature aging, which Geronimus refers to as weathering,

40
occurs in response to long-term exposure to persistent social and financial stress and the
attempt to actively cope with stressful circumstances (Geronimus, 1992, 1996). Weathering
has been supported through research that has assessed the biological wear and tear impact of
repeated exposure and adaptation to stressors via the comparison of allostatic load scores and
found them to be higher in blacks than in whites (Geronimus et al., 2006). The outcome of
this repeated and chronic stress is premature aging that impacts women’s health status or
health behaviors, such as lower life expectancy and early onset of degenerative chronic
conditions among racial/ethnic minorities, especially African Americans. As a consequence
of increases in lower life expectancy and early onset of degenerative chronic conditions
among ethnic minorities, infants of African American women had an increased risk of low
birth weight (LBW) as their mothers increased in age. As mothers increased in age the
white/black disparity in LBW widens. Although the concept of weathering was originally
developed to explain racial differences in minority LBW and infant mortality, it has since
been used and correlated with an explanation for reproductive health and hypertension.
Thus, the theoretical framework serves as a plausible means of understanding why some
minorities have earlier onset of various health conditions when compared to non-minorities.
Dannefer (2003) describes Cumulative Disadvantage (CDA) as “the systematic tendency
for inter-individual divergence in a given characteristic (e.g. money, health, or status) with
the passage of time” (pg S327). An example would be the cumulative effect of obesity,
which one may see expressed later in life through a heart attack. A health issue may arise
when the body can no longer compensate and at that critical point, the system malfunctions
or goes into an acute crisis. The acute response is due to a cumulative buildup over time, and

41
issues typically occur at middle age or later in life. Unequal social and economic conditions
as well as differential access to various resources accumulate and adversely influence health.
2.4.2 John Henryism
A similar hypothesis that seeks to explain the disproportionately high number of ethnic
minorities who suffer from increased heart rate and higher systolic blood pressure is that it is due
to John Henryism, a term coined by Doctor Sherman James (James, 1994) in reference to a black
American folk hero who symbolizes strength and determination. According to black American
folklore, John Henry, an ex-slave, was renowned for his physical strength and skill as a steel-
driving man, requiring that he use a nine-pound hammer to drive the stakes that held the railroad
tracks in place. He accepted a challenge to compete against a mechanical steam drill. Swinging a
hammer in each hand, John Henry was actually able to perform faster and more efficiently than
the machine, and won the contest. Unfortunately, moments after the contest ended, John Henry
dropped dead from absolute physical and mental exhaustion. As noted by James, “‘John
Henryism’ is a synonym for prolonged, high-effort coping with difficult psychosocial
environmental stressors” (James 1994, pg 167). This story is applicable to the day to day
stressors that many ethnic minorities endure purely because of their phenotypic profile.
The John Henryism hypothesis:
“assumes that lower socioeconomic status individuals in general, and African-Americans in particular, are routinely exposed to psychosocial stressors (e.g., chronic financial strain, job insecurity, and subtle or perhaps not so subtle social insults linked to race or social class) that require them to use considerable energy each day to manage the psychological stress generated by these conditions” (James, 1994).
However, James (ibid) takes into account the fact that not all people of a lower social status who
are exposed to these stressors will respond equally. Some will sustain cognitive and emotional
engagement, while others will be more apathetic, passive and eventually give up. Therefore,

42
James distinguishes people into two groups: “those strongly predisposed to cope actively with
psychosocial stressors (high John Henryism group) and those less predisposed to active coping
(low John Henryism group)” (ibid pg 168). The highest mean blood pressure would be expected
in those individuals who are simultaneously categorized by low socioeconomic status and high
John Henryism.
2.5 Racial/Ethnic Disparities in Health: An Examination of Physical Therapy
Under the auspices of the United States Department of Health and Human Services, the
Healthy People initiative to address national health promotion and disease prevention. One of
the overarching goals of Healthy People 2020 is to create social and physical environments that
promote good health for all (Healthy People, 2020). However, each level of racism previously
discussed has the potential to serve as a barrier that can impede the individual’s access to health
care services. As discussed by Northbridge (2003) the most concrete access-related factors that
have potential impact on health and disparate outcomes are seen when considering the built
environment in which many minorities live. Poor neighborhoods with high incidences of crime
are not areas where residents will likely feel safe to walk or jog for exercise. Such
neighborhoods are also less likely to have health clubs or gyms that would be an alternative to
engage in healthy lifestyle activities. Morland (2002) describes how poor environs do not have
large grocery stores or farmer’s markets with readily available access to healthy food choices.
Instead these areas have a greater number of fast food restaurants and small convenient food
stores stocked largely with less expensive and less nutritious foods. The stressors of living under
these circumstances that are commonly associated with minorities at the lower socioeconomic
level also have a negative effect on health (Williams, 2001). The conditions and circumstances
counter the cited overarching goal of the Healthy People 2020. None reflect the social or

43
physical environmental conditions conducive to the healthy lifestyle that facilitates good health
nor the prevention or management of chronic conditions, nor recovery from injury or surgical
intervention.
However racial/ethnic disparities have been found to persist even when the same social
and physical environmental conditions existed when physical rehabilitation was provided.
Horner et al. (2003) conducted a secondary data analysis of the Veterans Administration Stroke
study involving patients who were hospitalized at any of the nine Veterans Administration (VA)
hospitals that participated in the nationwide prospective cohort study. The authors examined the
process and outcomes of stroke rehabilitation across the VA facilities, “an equal access
healthcare system.” Investigators concluded that racial disparities existed both in the
rehabilitation process and the outcomes of the patients studied. Blacks at the lower income level
experienced a delayed start of rehabilitation and had worse post-stroke functional recovery. The
subjects (black or white) were referred to rehabilitation based on the severity of their stroke and
degree of cognitive impairment; however, premorbid status was not discussed.
The presence and access to rehabilitation facilities and utilization of PT services are
critical aspects of the built environment. Within a limited geographic location and a relatively
small sample size, McCallum (2010) found disparities related to physical therapy services in
three community health care clinics in Ohio that serve “medically underserved adults.” Data
collected in the study included interviews with health care providers, patient surveys, and
documents (e.g., service records, organizational records, maps, charts, community health
indicators, demographics, and socio-economic information) to determine community and patient
characteristics.. In addition, available community resources and knowledge of the scope of
physical therapy practice was considered. The outcomes of McCallum’s (2010) research

44
indicates that access to physical therapy services by those within the identified community was
negatively influenced by three primary factors: an insufficient number of physical therapists to
meet the needs of the population studied; a poor understanding by both patient and physician
regarding the scope of practice of physical therapy; and the lack of a “standardized screening or
assessment processes related to physical mobility problems for patients with chronic health
conditions.” These factors consequently yielded a decreased patient referral of those who may
either be at risk for disability or by those who are already in need of physical therapy services.
Racial/ethnic disparities in the access, utilization and functional outcomes have been
found across various PT practice patterns. Table 2.5 provides an overview of some of these
disparities specifically linked to physical therapy rehabilitation services provided to those with
neurological and orthopedic impairment.
This section provided an overview of some of the key health disparities more commonly
found across the various practice patterns of PT. However, as this dissertation specifically
addresses disparities related to the functional outcomes following the THR, a discussion of this
surgical procedure and associated post-operative physical therapy rehabilitation is indicated and
presented.

45
2.6 Total Hip Replacement
First performed in the United States during the late 1960s, total hip replacement (THR), also
known as a total hip arthroplasty (THA), is an elective orthopedic surgical procedure that
involves joint reconstruction (arthroplasty) where pieces of a joint are replaced with artificial
implants--or prostheses (https://www.hss.edu/). Total hip replacement is one of the most common
surgical procedures in the United States (Lermonth,2007) (H-CUP, 2014). As reported by
Kremers et al. (2015), the 2010 prevalence of THR among the total U.S. population was
estimated at 0.83%. The July 6, 2016 CDC updates of the 2010 National Hospital Discharge
Survey, indicated 332,000 total hip arthroplasty procedures done in the United States. (CDC,
2016)
The primary indication for a THR is osteoarthritis with symptomatic complaints of pain
and locomotor limitations. The most important pre-operative expectations of THR cited by
prospective surgical candidates are improved mobility and decreased pain (Scott et al., 2012).
Although the procedure is performed on individuals from mid-adolescence and throughout
senescence, the greatest prevalence is found in those in the sixth through eighth decades of life
and the frequency is greater in women than men (Hootman, 2016), (Kremers et al., 2015)
(Learmonth et al., 2007). As reported by Hootman et al. (2016), one in five adults (18 yo or
greater) or 52.5 million people in the United States have been medically diagnosed with arthritis
and 2.7 million report diagnosis-related limitations. Although the rate of disease progression and
perception of pain will vary from patient to patient, this chronic disease condition affects all
racial and ethnic groups and is noted as the most common cause of disability (CDC, MMWR,
2016). By 2040, doctor-diagnosed arthritis is projected to increase by 49% and will include

46
78.8 million or 25% of all adults; those adults with arthritis attributable activity limitations will
increase 52% to 34.6 million or 11.4% of the adult population (Hootman et al., 2016).
Total joint replacements (TJR), specifically THR and total knee replacements (TKR), are
reported as the most common inpatient surgical procedure for Medicare beneficiaries (CMS.gov)
with more than 60% of all THR procedures performed on Medicare enrollees (Cram et al., 2011).
In a systematic review of the literature, Santaguida et al. (2008) examined patient characteristics
that impacted the prognosis of individuals who underwent a TJR. The patient characteristics of
interest included age, sex, race, body weight, socioeconomic status and work status. The impacts
of these characteristics were reported relative to post-operative THR outcomes of post-operative
mortality, surgical revision of the arthroplasty, post-operative pain and function. The results of
this review indicated that following a TJR there was an increased mortality risk associated with
older males; greater revision was associated with younger males; older age was related to worse
function (especially for women); and postoperative pain was not influenced by either age or pain.
All subgroups were deemed to have benefitted from this surgical procedure. However, although
noted as a patient characteristic of interest affecting prognosis, results were not given relative to
the influence of race.
The aging of the “baby boomer” generation (those born 1946-1964), the ability to
diagnose and treat advanced arthritis more readily, and the demand for improved mobility and
higher quality of life are all factors that will keep total joint replacements in continued high
demand (Kremers, 2015). In a systematic literature review of cost effectiveness analyses of TJR,
Daigle et al. (2012) found that the literature indicated that for those where it is medically
indicated, total joint replacements are a highly cost-effective intervention that “offer(s) good
value for the money spent” (Daigle et al., 2012 pg 655). Studies analyzing projections for joint

47
arthroplasties in the United States between 2005 and 2030 have projected that the demand for
THA will grow by 174 percent to 572,000 (Kurtz, 2007).
Qasim and Andrews (2013) reviewed 2000 and 2009 post-surgical outcomes data of a
nation-wide sample of patients from low- and high-income areas in the United States, to
determine the rates of mortality and post-surgical patient safety outcomes for eight procedures:
abdominal aortic aneurysm repair, coronary artery bypass graft, carotid endarterectomy,
craniotomy, esophageal resection of cancer, hip replacement, pancreatic resection for cancer
and percutaneous coronary intervention. Results indicate that almost all post-operative outcomes
improved for both the low- and high-income communities across the nine-year period. However,
disparities in surgical outcomes from these procedures were persistent; those patients living in
low-income communities fared significantly worse than those who lived in high-income
communities. Of particular interest as it relates to this dissertation, the risk-adjusted mortality
rate for hip replacement was 26 percent higher in 2009 for patients from low-income areas than
those from high-income areas. The researchers indicated that residents from low-income
communities “are more likely than those who are better off to be either covered by Medicaid or
uninsured and to belong to a racial or ethnic minority group. These characteristics have been
shown to be associated with poorer surgical outcomes” (ibid pg 1777).
The prevalence of arthritis in the American adult population is disproportionally greater
among the minority population when compared to non-minority population (Oliver, 2014)
(Dunlop, 2003). Arthritis-attributable activity limitations (AAAL) either with or without
doctor-diagnosed arthritis is also greater across the minority population (Barbour, 2013)
(Helmick, 2008), However, despite the well-documented benefits of TJR and THR,
utilization of this surgical intervention is approximately two thirds less common among

48
minorities in comparison with non-minorities (Dunlop, 2003). In a recent longitudinal study
Singh and colleagues (2013) found both a lesser utilization as well as poorer post-operative
outcomes as assessed by post-operative 30 day hospital readmission rates across an 18-year
period. In a review of the literature addressing the racial and ethnic disparities in total hip and
knee arthroplasties, Irgit & Nelson (2011) noted the “incidence rate of activity-related OA
among African Americans and Hispanics is at least equal to, if not greater than among non-
Hispanic whites”. Their review of the literature found no medically justified reason for the
lower utilization rate of TJR among the minority population. However, other plausible
reasons mentioned for the lower utilization by blacks and minorities included lower
expectations and decreased trust in the medical system based on prior historical unethical
medical abuse.
In a study to evaluate the implications of health conditions and economic access as a means
to understand the minority vs. non-minority differences in joint arthroplasty of those 70 years of
age and older, Dunlop and colleagues (2003) analyzed the 1993 and 1995 public-use data from
the Asset and Health Dynamics Among the Oldest Old (AHEAD), a prospective study of people
70 years of age and older. This study monitors changes in physical and functional health
“assessed from physical and daily functional task limitation” such as ambulation and activities of
daily living (ADLs) (Dunlop, 2003 pg 290), as well as economic resources and healthcare
demand. Health need was based upon the number of medical conditions and functional health
issues noted. Due to a greater prevalence of arthritis among minority than non-minority persons,
the health need was greater in the former. Nonetheless the non-minority cohort still had a lesser
TJR utilization rate. The disparity remained even when economic and medical status were

49
statistically controlled. Thus, neither differences in health conditions nor economic inequities
explained the lesser utilization use of TJR among minorities.
Using 1998-2002 data from the US Health and Retirement Study, Steel et al. (2008)
prospectively examined the prevalence of those identified as in need of a TJR to those who
actually received a TJR within the subsequent two years of identified need. Self-
classification of being in need was based on the response of 14,807 patients' response to 5
questions that indicated “disabling symptoms despite medical therapy.” The questions
represented criteria “indicating chronic discomfort & significant functional impairment” for
which National Institutes of Health (NIH) consensus panels considered THR an option.
Although the need was greater for participant who were black (and those who were poorer,
older, women or obese or did not have a college education), they received 50 percent fewer
THRs than those who held traits and characteristics of their antithetic counterparts.
The research by both Dunlop (2003) and Steel et al. (2008) examined study populations of
more than 10 and 20 years old respectively and technology has improved TJR considerably
during that time span. However, the results of their research remain important given the
continued and very similar present day status of minority health where disparities in healthcare
access, utilization and surgical/medical outcomes remain. One of the four overarching goals of
the country’s Department of Health and Human Services’ (HSS) Healthy People 2020 program
is to “Achieve health equity, eliminate disparities, and improve the health of all groups.”
2.7 Research Question within the Content of Law and Policy: Evolution and Interaction
among Legislative, Regulatory, and Judiciary Actions
Racial and ethnic health status and health care disparities have been long-standing issues of
concern in the United States. Acknowledging these differences and improving the health of the

50
underserved have been objectives of our government for several decades (Heckler, 1985)
(Smedley, 2003) (Washington, 2006). This section of the literature review provides a
chronological development of the policies and legislation that fall within the fifth level of the
SEM.
2.7.1 Title VI of the 1964 Civil Rights Act
Title VI prohibits recipients of federal funds from discriminating on the basis of race,
ethnicity, or national origin [42 U.S.C. § 2000d (2000)]. Through enforcement by the
Department of Health, Education and Welfare (HEW) now under Department of Health and
Human Services (DHHS), Title VI has helped eliminate discriminatory practices such as denial
of admitting privileges to black American physicians, refusal to admit patients who are not cared
for by attending physicians with staff privileges, high prepayment requirements for black
American patients, and discriminatory routing of ambulances (Smith, 2016). Title VI’s coverage
of entities that receive federal assistance includes hospitals and other healthcare facilities that,
since 1965, receive Medicare or Medicaid payments.
Despite major victories against intentional discrimination in healthcare, such as
segregated hospitals and/or hospital wards, Title VI has limitations. Title VI is “ill-suited in its
current form to battle the more subtle problem of racial disparities in medical treatment that are
caused by caregivers’ implicit cognitive bias” (Watson, 2001). Plaintiffs have attempted to
utilize sections 601 and 602 of Title VI as a mechanism for redressing these subtler forms of
discrimination. Title VI’s disparate-treatment provision states that “[n]o person in the United
States shall, on the ground of race, color, or national origin, be excluded from participation in, be
denied the benefits of, or be subjected to discrimination under any program or activity receiving
Federal financial assistance” [42 U.S.C. § 2000d (2000).] However, individuals seeking redress

51
under section 601 have mostly been unsuccessful due to the challenge of proving perceived
discrimination as intentional. In Alexander v. Sandoval the Supreme Court established that
section 601 prohibits only explicit, intentional discrimination, which makes the section
inapplicable to cases in which disparate treatment is caused by implicit cognitive bias.
[Alexander v. Sandoval, 532 U.S. 275, 280-81 (2001)].
Section 602 of Title VI permits federal agencies to “effectuate the provisions of [section
601] … by issuing rules, regulations, or orders of general applicability.” [42 U.S.C. § 2000d-1
(2000)]. There has yet to be a Supreme Court ruling explicitly stating that section 602 prohibits
only intentional discrimination. Consequently, “most federal agencies have adopted regulations
pursuant to section 602 that bar the use of federal funds for programs that have a disparate
impact on minorities (Shin, 2002). Despite the potential utility section 602 stands to offer, the
“Supreme Court’s ruling in Alexander v. Sandoval severely limits the scope of section 602 and
greatly limits any ability it previously might have had to protect against racial disparities in
medical treatment” (ibid Shin, 2002).
A state court in its decision concerning South Camden Citizens in Action v. New Jersey
case dealt yet another blow to communities that attempted to use Title VI as a means to acquire a
preliminary injunction against industrial construction such as waste facilities, food processing
companies, automotive shops, and a petroleum coke transfer station that allegedly would cause a
racially disparate adverse impact [South Camden Citizens in Action v. New Jersey. 274 F.
3d771, 775 (2001)]. The plaintiffs in South Camden sought to “enforce a prohibition on disparate
impact discrimination that does not appear explicitly in Title VI, but rather is set forth in EPA
regulations. They contend[ed] that the regulations are a valid interpretation of Title VI” (Ibid pg
780). The court sought to resolve the issue of “whether disparate impact regulations promulgated

52
pursuant to section 602 may, and if so do, create a right that may be enforced through a section
1983 action…[S]ection 1983 provides a remedy for deprivation under color of state law of ‘any
rights … secured by the Constitution and laws (Ibid pg 779).
The state court’s analysis held that South Camden Citizens in Action did not present any
federal right to enforce, and therefore the district court erred in granting relief on the basis of
section 1983 (Ibid). This ruling dealt yet another serious blow to those attempting to utilize both
the legislature and judicial system as a mechanism to address racial health disparities.
In summation, legislation and the judicial system do not appear to hold the ultimate
answer to the persistent matters of disparities in health care and health status. If that alone were
the solution, a markedly lower prevalence of disparities would possibly be seen where legislation
affords individuals with equal access to the healthcare system, such as Medicare. Unfortunately,
disparities are found within this population as well. Thus racial/ethnic disparities continue to
prevail in health care despite legislative and policy intervention at the macrosystem/social &
political level of the SEM.
2.7.2 Original Medicare and Medicaid and Its Current Configuration and Coverage
In 1965, Congress passed legislation under the auspices of title XVIII and XIX of the Social
Security Act establishing Medicare and Medicaid respectively. Administrative responsibilities
for Medicare and the federally funded component of Medicaid are now entrusted to the Centers
for Medicare and Medicaid Services (CMS) under the Department of Health and Human
Services. CMS is the single largest payer for health care in the United States. It now provides
benefits to more than 120 million Americans through federally financed health care benefits to
55,056,521 million Medicare, 65,011,874 million Medicaid, and 8,129,426 State Children's
Health Insurance Program (SCHIP) beneficiaries (CMS.gov).

53
Medicare was legislated as “a health insurance program for aged persons to complement
the retirement, survivors and disability benefit under Title II of the Social Security Act.” This
legislation was implemented in 1966 and covered most adults 65 years old or greater (Public
Law 96-510).
In its original legislation, Medicare had two primary components, Part A and Part B: the
former assisting with the payment for in-patient, home health agency, skilled nursing facility and
hospice care and the latter paying for physician, outpatient hospital, home health agency and
other services. Part A services are rendered without premium to most eligible people, while care
and services provided under Part B are covered by a monthly premium which is paid by or on
behalf of the beneficiary. As an outcome of the Balanced Budget Act of 1997 (Public Law 105-
33), a third component of Medicare–Part C (also known as Medicare +Choice) was established
and later modified via PL 108-173 – the Medicare Prescription Drug, Improvement and
Modernization Act of 2003 and renamed as the Medicare Advantage program. Part C/Medicare
Advantage affords Medicare beneficiaries access to health care plans within the private sector.
Effective in 2006, the fourth component of Medicare health insurance is Part D, effective in
2006, that provides subsidized voluntary prescription drug insurance coverage for Medicare
beneficiaries who pay a drug benefit premium. Premium and cost sharing subsidies are available
for low-income enrollees through Part D.
Medicare is our country’s largest health care insurance program, and after Social
Security, the second largest social insurance program. As noted this program covers most of the
aged population in the United States, including those who receive disability benefits from Social
Security. In 2014, Part A covered more than 53 million enrollees with benefit payments of
$264.9 billion; Part B covered over 49 million enrollees with payments of $261.9 billion; Part D

54
covered greater than 40 million enrollees with benefit payments of $77.7 billion (Klees et al.,
2015).
Medicaid was established in response to the perceived inadequacy of welfare medical
care under public assistance. This program falls under the aegis of Title XIX of the Social
Security Act and is a federal and state entitlement program provides medical assistance to
certain individuals and families with low income and resources. Under broad national guidelines
of federal statues, regulations, and policies, each state functions autonomously in terms of
beneficiary eligibility standards and the type, amount, duration and scope of assistance the state
provides. Each state administers its own program, resulting in state to state inconsistency in
eligibility, services offered, and reimbursement in accordance with the state legislatures. In
order to receive federal matching funds, states must offer medical assistance for certain basic
services to most categorically needy populations. Among the services included (but not limited)
are: inpatient and outpatient services, physician services, vaccines for children, laboratory and x-
ray services and home health care for persons eligible for skilled nursing services. Also federal
matching funds are available for states to provide certain optional services, including
“rehabilitation and physical therapy services” pertinent to the topic of this dissertation. The 2014
Medicaid combined payments to health care vendors for services provided to 59.3 million
beneficiaries averaged $7,038 per person. (Klees, 2015)
2.7.2.1 Medicaid – Medicare Relationship
Medicare beneficiaries with low incomes and limited resources may also receive
assistance from Medicaid. The form of assistance varies in accordance with the need. For those
who fall under this category and are eligible for full Medicaid coverage, the Medicare health care
coverage is supplemented by services available under the state’s Medicaid program (i.e. nursing

55
care greater than Medicare 100-day limit). For beneficiaries who are dually enrolled in both
programs, services covered by Medicare are paid by that program before any payments by the
Medicaid program. Other Medicare beneficiaries who receive help with Medicare premiums and
or cost-sharing payments through their state Medicaid programs are the Qualified Medicare
Beneficiaries (QMB) with financial resources at or below the Social Security Insurance
limitation and incomes at or below 100 percent of the Federal Poverty Level (FPL) and Specified
Low Income Medicare Beneficiaries (SLMB) with resources similar to the QMBs but with
higher incomes and for whom Medicaid pays only for a portion of the Part B premium. As
Medicaid no longer provides drug benefits for Medicare beneficiaries, the final common means
of assistance that was implemented in 2006 with the inception of the Medicare prescription drug
benefit is a low-income subsidy for the Medicare drug plan premiums and assistance with cost
sharing for prescriptions (Klees et al 2015).
Since the implementation of Medicare, Medicare payment for medical health services
was contingent on non-segregated patient hospitalization as well as other implicit and explicit
forms of discrimination (Smith, 2016). Therefore, the Medicare regulations have played a
significant role in the reduction of race based health disparities. To be funded, hospital
administration had to comply with the non-biased and equal medical treatment of their minority
patients. Thus, Medicare was prohibiting the racial discrimination that was overtly present and
yielded disparate racial/ethnic healthcare delivery and poorer health status. Adherence to the
standards set forth by Medicare theoretically promotes uniform standards for it beneficiaries.
Given the above expectations, CMS data was selected as the source of my study
population. All beneficiaries would be expected to be the recipient of uniform frequency of care,
to be monitored by a uniform quality assessment system, and whose health records are collected

56
through a nationally uniform data system. Therefore, the impact of a social construct such as
one's racial/ethnic identity should not impede a uniform functional outcome.
2.7.3 The Heckler Report and Its Impact on Minority
For more than a quarter of a century, several key federal reports and initiatives have
attempted to bring the problem of disparate minority health to the attention of the American
people. National attention was most markedly elevated with release of the U.S. Department’s
of Health, Education, and Welfare1985 – Report of the Secretary’s Task Force on Black &
Minority Health, which clearly detailed the numerous differences between the health of blacks
and whites (Heckler, 1985). This report sparked the birth of several federal initiatives in the
1990s (Kennedy, 2005). By the year 2000, Healthy People 2010 identified the elimination of
disparate health care as one of the country’s primary public health goals for the decade
(USDHHS, 2000). Healthy People continues as a science-based federal program that aims to
improve the health of all Americans via decennial set goals and objectives.
Key legislation such as “The Minority Health and Health Disparities Research and
Education Act of 2000” (PL 106-525) was instrumental in laying the foundation for the
National Institutes of Health’s (NIH) goal to decrease and ultimately eliminate health
disparities. The overarching goal was to promote health for all Americans. On November 22,
2000, President George W. Bush signed this law and the National Center on Minority Health
and Health Disparities (NCMHD)was instituted. This federal agency was established to foster,
coordinate and assess the progress of all NIH sponsored research activities related to minority
health and other health disparities. Several reports resulted from NIH funded research to
examine and address the apparently inefficient healthcare market where health equity was not
found across all sectors of the United States diverse population (Atrash, 2006). In a seminal

57
2003 report, the Institute of Medicine’s (IOM) Unequal Treatment: Confronting Racial &
Ethnic Disparities in Healthcare documented and affirmed the prevalence of disparities in
health care throughout the country and provided recommendations for their amelioration
(Smedley 2003).
Mandated by the Healthcare Research & Quality Act of 1999 [PL 106-129], the
Agency for Healthcare Research and Quality (AHRQ) has provided annual reports to
Congress since 2003 on the quality of, and disparities in, healthcare delivery to members of
the population of the United States. The recent 2015 edition of this report, which incorporates
more than 250 measures of quality and disparities, notes many quality improvements such as:
decrease in hospital-acquired conditions, 1.3 percent less incidents of harm to patients,
approximately 50,000 lives saved and 12 billion dollars in cost saving, improvements in
person-centered care as reflected by better patient-provider communication, and increases in
effective treatments as demonstrated by better hospital pneumonia care and the doubling of
adolescent immunization rates between 2008 and 2012 (AHRQ, 2015). As such these quality
improvements have positively impacted overall population health. However, as detailed
above (Sections 2.1.1 and 2.50) racial disparities persist and can perhaps be most succinctly
referenced by the fact that blacks have a higher mortality rate than any other racial or ethnic
group in 80 percent of the ten leading causes of death (Kelly, 2015).
Legislation, specifically the 2010 Patient Protection and Affordable Care Act [PL 111-
148], has been associated with better access to care. Following what had been a 10.2 percent
increase of people unable or delayed in securing necessary medical, dental or prescription
medicines due to insufficient monetary or insurance resources between the years of 2002
(61.2 percent) and 2010 (71.4 percent), these unmet needs stabilized and declined between

58
2012 and 2014 (AHRQ, 2015). The level of uninsured continues to drop and at the end of the
first quarter of 2016 the rate of the uninsured fell to a record low of less than nine percent
when it was recorded at 8.9 percent (CDC.gov). Differences remain such that the indigent
generally encounter less access to healthcare and the care received, and when accessed, is of
suboptimum quality (AHRQ, 2015).
2.7.4 Emergency Medical Treatment and Active Labor Act
In 1986, Congress enacted The Emergency Medical Treatment and Active Labor Act
(EMTALA). This statute, which is often referred to as the “patient dumping” statute, “requires
federally funded hospitals (e.g., those that participate in Medicare or Medicaid) that operate
emergency rooms to screen all emergency room patrons for ‘emergency medical conditions’
regardless of patients’ ability to pay, and to provide stabilizing treatment for emergency
conditions” (Smedley et al., 2003 pg 156). Consequently, under this statute, health care facilities
cannot discriminate against the poor. The only circumstance where a hospital does not need to
adhere to these guidelines is when the medical benefits of transferring the individual to another
facility outweigh the risks to the individual (42U.S.C. § 1395dd(a) (2000). EMTALA’s
enforcement provisions subject a violating hospital to: (1) a monetary penalty of up to fifty-
thousand dollars per violation; (2) a private cause of action against the hospital; and (3) any
appropriate equitable relief [§ 1395dd(d0(1)-(3)].
Roberts v. Galen of Virginia, Inc. is a Supreme Court case that opened the door for
plaintiffs with claims based on unintentional racial disparity in medical treatment [Roberts v.
Galen of Virginia Inc. 525 U.S. 249.253 (1999)] “Under Roberts, any patient may state a claim
under EMTALA if he or she demonstrates that the hospital provided disparate treatment, instead
of providing appropriate medical screening” (Shin, 2002). However, EMTALA is still limited in

59
the sense that the essential element of a claim is the question of whether the hospital conducted
an appropriate medical screening. Unfortunately for plaintiffs, a number of circuit courts have
held that EMTALA’s mandatory emergency screening examination “need not meet national
standards of care, but instead must only comply with the screening hospital’s regular practices.”
(Shin, 2002).
2.7.5 Tort Law
Medical malpractice law, also known as tort law, is a prime example of how litigation is
limited in its efforts to eradicate racial health status disparities. There is such a wide variation in
clinical practice patterns and “[w]ithout high-quality data about the efficacy of alternatives
approaches, physician-experts cannot provide testimony that distinguishes scientifically between
‘correct’ and ‘incorrect’ clinical practice variations” (Schmedley et al., 2003 pg 155). Plaintiffs
who claim they were victims of racial discrimination via medical malpractice “would have a
difficult time proving causation-in-fact absent well maintained data concerning the efficiency of
alternative approaches that would resolve disparity in clinical outcomes” (Bloche, 2001 as
quoted by Smedley et al., 2003 pg.156). Consequently, a very small proportion of medical
malpractice suits yield settlements or judgments directed at reducing disparities (Smedley et al,
2003). Moreover, “poor people and members of disadvantaged minority groups are less likely
than other Americans to sue their doctors [making] [m]edical malpractice law…of weak utility
as a mechanism to address racial and ethnic discrimination” (ibid).
2.7.6 Legal and Regulatory Policy Summation The use of the United States judicial and regulatory systems has been found to be of little
use as mechanisms to combat and eventually eradicate racial health status disparities. Case law
proves and legal scholars agree that these mechanisms are inadequate by themselves to address

60
discriminatory practices. These legal remedies are implemented only when facing overt and
explicit instances of race-based healthcare discrimination obstacles. Furthermore, the legal and
regulatory systems focus the majority of their attention on eradicating healthcare disparities
(disparities in the frequency of and quality of delivery of healthcare services) and not general
disparities in health status. The utilization of data large cohorts of the national Medicare
population provides the platform to further consider racial/ethnic disparities in health status via
specific measures of functional outcomes as they are related to physical rehabilitation
2.8 The Role of Physical Rehabilitation Medicine in Total Hip Replacement
Physical therapy is component of the rehabilitation process for individuals who will be
undergoing or have undergone a THR. The preoperative goal is to educate the prospective
patient regarding what to expect from surgery and to provide the patient with exercises to
condition the body before surgery. At this preoperative stage this will generally include
flexibility and strengthening for the lower extremities, how the patient will use assistive devices
afterwards as well as any post-surgical precautions. Rooks et al. (2006) found that a 6-week pre-
operative exercise program had several positive effects which included: increased strength, and
increased functional status prior to surgery and that the pre-operative program decreased the
odds for needing in-patient post-operative rehabilitation. A systematic literature review of
eighteen trials through 2012 was analyzed. The format and the type of intervention (i.e.
strengthening, balance, stretching, land based and/or aquatic programs) varied among the studies
as did the delivery and composition of the pre-operative rehabilitation provided and included
individual as well as group sessions with 3-4 or 6-10 participants per groups. The conclusion of
the analysis indicated pre-operative exercise-based interventions is an option that can reduce pain

61
and improve physical function for people awaiting hip replacement surgery (Gill & McBurney,
2013).
During the 3-5 days of post THR acute-care recovery, the therapist instructs patients
how to safely execute bed mobility, transfer out of bed to a chair, perform basic
strengthening and range of motion exercises and ambulate with the appropriate assistive
devise for short distances.
During the next 4-6 weeks, depending upon the patient’s support at home and their
ability to stay safe, sub-acute care will be delivered in either a short-term care rehabilitation
facility, the patient's home with home care assistance, or at home with outpatient services.
During this sub-acute stage of recovery, the patient continues to work on ambulation and
stair negotiation, balance, muscle strengthening and full movement of the involved leg. Full
functional independence and return to pre-surgical abilities is the long-term goal of this stage.
However, based on a pilot study with a convenience sample of the 207 members of
the American Physical Therapy Association with a special interest in TJR rehabilitation,
Gorman and Curry (2010) determined that variability in current physical therapy practices
does exist. There was a relatively low response rate of 12-18% and (n=25 – 39) to the online
administered survey. Not all facilities offer a preoperative program for their prospective
patients and there is variation among those who do so in terms of who conducts the pre-
operative programs (i.e. nurses, physical therapist (PT), PT case managers, occupational
therapist (OT)), and the frequency and content of the classes. Post-operative initiation of
patient rehabilitation also varies in regard to initial examination (i.e. day of surgery, 1-day
post-op etc.) as well as the content of the post-operative rehabilitation program which varies
from assisting the patient to sitting at the edge of the bed to ambulation within the room or in

62
the hospital hallway. The study did provide “preliminary information regarding current
practices related to rehabilitation in the acute care setting of persons” following a TJA and
was a start in describing practice trends at the time of the survey.
Vissers et al. (2011) conducted a systematic review and meta-analysis of the literature
to examine recovery of physical function following THA. Physical functioning is
operationally defined as a construct that includes three primary aspects: 1) perceived
problems in daily functions that were measured via the assessment of answers to a validated
questionnaire; 2) functional capacity to perform activities either in a lab setting or outpatient
clinic as measured with capacity tests that assessed the subjects’ ambulatory abilities on
level surfaces and with stair negotiation or a gait analysis; and 3) actual daily activity that
were measured with pedometers or activity monitors. The results of the 31 studies included
in this review and meta-analysis found increased physical functioning across all 3 measures
subsequent to a THA by 80 – 84% compared to the control group who didn’t have a THR,
(age matched health individuals) within 6-8 months post-surgery. Considering that surgeons
typically use a two year window as measure of surgical outcome, this measure of
approximately 20 percent less than maximum outcome is commendable.
All of the above may impact individual health status and health care among the many
subsectors of the United States population. All are among the mechanisms that help us
understand and explain health disparities. However, much of the literature regarding disparities
in health status and healthcare that results in inequity in patient outcomes centers on medicine
and physician-to-patient interactions. There is a paucity of literature regarding the impact of
physical rehabilitation, specifically physical therapy, in relation to patient functional outcomes
across racially and ethnically diverse populations.

63
Physical therapists are members of the healthcare team who are intimately involved with
the care of a selective cohort of patients. They play a key role in the rehabilitation of individuals
with various physical impairments as well as to those recovering from acute injury or subsequent
to surgical intervention. Although it would be tempting to infer that what has been found
regarding physician and resultant health process and outcome disparities is the same for all
components and members of the healthcare team, it would be far from a conclusive or an
evidence based assumption.
Research addressing post-acute care patient outcomes subsequent to rehabilitation for
elective surgical procedures such as total joint replacements, have had small sample sizes (Kim,
2010) (Mallinson et al., 2011) (Mahomed et al., 2008). Studies that included larger samples (i.e.
greater than 1000 participants) lacked diversity among the participants (de Pablo, 2004). In a
longitudinal study that examined clinical characteristics and outcomes of the more than 1.4
million patients who underwent a total hip arthroplasty between 1991 and 2008, no functional
patient outcome measures were reported. Data stratified by race and ethnicity was limited to the
proportion of the study population represented by white, black, other or not available (Cram et
al., 2011). Studies assessing functional differences among racial/ethnic groups have been found
to have similar limitations as noted above. The retrospective population-based study of a diverse
THR cohort as examined for this dissertation allows for the comparison of functional outcome
measures across racial and ethnic identities for a designated diagnosis–THR.
Outcomes have been defined as the “consequences attributable to antecedent care”
(Donabedian, 2003, pg. 52). Measuring individual functional outcome among Medicare
beneficiaries who have undergone a total joint arthroplasty affords my research a valuable gauge
of the quality of health care delivered. This research provides the opportunity to examine health

64
equity for the growing senior citizen sector of the population. As large numbers of the "baby
boomer generation” enter into senescence, they will become the recipients of physical therapy
services for common orthopedic elective surgical procedures such as total hip replacements.
Examination of functional outcomes for this designated cohort offers the opportunity to assess
racial/ethnic disparity in an area of health care where the issue has been less studied. Such
evaluation can set the foundation for potential policy changes to assure equity in functional
outcomes for this growing population.
2.9 Home Health Agency
The Medicare beneficiaries examined in this study are those who were discharged from
an acute care setting to their homes with services to be provided by a home health care agency
(HHA). Medicare Part A covers the first 100 visits following a 3-day hospital stay and Part B
covers any visits beyond the initial 100-day period (Klees et al. 2015).
Although some patients who have undergone THRs are discharged to in-patient
rehabilitation facilities (IRFs) after their acute care hospitalization for the surgical procedure, the
majority either go directly home or receive home health care services or outpatient therapy.
Others are discharged to skilled nursing facilities (SNFs) for the delivery of post-acute
rehabilitation.
The described pattern of rehabilitation services is the result of a 2004 Centers for
Medicare and Medicaid Services (CMS) policy change. Policy at that time eliminated unilateral
TJRs from Medicare’s list of qualifying diagnoses (CMS-13) eligible for the intense and
expensive inpatient rehabilitation services which was more prevalent prior to this policy change.
CMS determined that “patients could achieve similar outcomes in a less expensive setting…”
(Hartley & Camilo, 2012). TJRs are among the thirteen medical conditions that CMS requires

65
60% of patients must have in order to be admitted to an IRF. Medicare coverage for IRF
services following acute hospitalization for TJR is limited to patients with three complicating
conditions: 1) have undergone bilateral TJR; 2) have a body mass index of 50 or greater; or 3) be
85 years of age or older. Some Medicare beneficiaries after TJR remain in need of medical
monitoring although they do not require or are unable to adhere to the intensity (3 hours/day) of
(IRF) rehabilitation services. Consequently, these patients are typically discharged to skilled
nursing facilities (SNF) (Ibid).
Hospital admissions rates for TJR have steadily increased for CMS beneficiaries over the
course of the recent years. Those admitted for THR have increased from 29 to 37 per 10,000
beneficiaries representing an annual 4.1 percent increase between 2003 and 2009. The discharge
disposition for this cohort of beneficiaries has increasingly been to home with home health care
services instead of rehabilitation facilities. The results of a 2012 Government Accountability
Office (GAO) report as illustrated in Figure 2.3 below, show discharge to home with home care
to have increased by 14 percent, while discharge to rehabilitative facilities has declined by 12
percent (GAO-12-583R). Thus under the assumption of this trend continuing along the same
trajectory, the population chosen for this dissertation study was those individuals who were
discharged home with home care subsequent to acute hospitalization for a primary THR.

66
Figure 2.2 Beneficiaries’ Discharge Disposition Following Orthopedic Implantable Medical Device Admissions, by Procedure, 2003-2009
As accessed from GAO Report # 12-583R
2.10 Summary
The historical overview of some of the social and medical conditions to which African
Americans and other minority groups have endured from the period of slavery through
contemporary period provides a baseline for understanding some of the poorer health status
found within the minority population in comparison to the non-minority population.
As exemplified by the above noted studies, disparities related to access and utilization of
physical therapy services have been identified and documented. However, few examine causes
for these differences and whether the noted disparities are associated with any differences in
patient functional outcomes typically measured through PT. Although less is known about
disparities in PT than in some other areas, my analysis based on several prior studies, historical
6062
5956
5349 48
2023
2528
3033 34
1814 15 14
16 17 16
0
10
20
30
40
50
60
70
2003 2004 2005 2006 2007 2008 2009
Percentage
of beneficiaries
Year
Total Hip Replacement
Rehabilitative Facility Home Health Care Home or Self‐Care

67
perspectives, social and policy analyses suggest that similar racial/ethnic findings are likely to be
found in this aspect of healthcare as well.
Projections of the country’s changing demographics indicates that the current minority
population will become the majority in less than a quarter of a century. This should raise
concern regarding the potential consequence for the health of both national and international
populations. A country where the majority of its population is in less than optimal health is not
one that can lead or competitively compete within the global market. Acknowledgement and
national consensus regarding the root cause(s) of this public health issue is critically important in
order to effectively address the problem.
As discussed in Section 2.8, CMS legislation emerged from the Social Security Act and
was designed to promote access to healthcare for senior citizens and the poor and in the process,
reduce disparities. A direct relationship of this dissertation to law and public policy stems from
the fact that Medicare insurance regulations were designed to address disparities. The
implications of this dissertation research will be developed in the discussion.

68
Chapter 3 Linking Theory to the Research Model
3.0 Introduction
My review of the literature indicates that health disparities exists in several aspects of the
health of the population and that these disparities are influenced by many social, economic and
environmental factors. They exist not only in the manifestation of disease and poor health status
(e.g., infant mortality, diabetes, cerebral vascular accidents), but also are found in the differential
intensity of care that has been documented in delivery sites (e.g., hospital emergency
departments) and within the same clinical conditions (e.g., heart attacks, strokes). Few studies
have examined the existence of health disparities in the process and outcome of physical therapy
(PT) services and none have been found by this researcher that specifically questioned if health
disparities exist in 1) the provision of these services following surgical hip replacement and
follow-up PT care provided through a home health agency (HHA) and 2) the functional
outcomes of these patients at the conclusion of HHA PT services.
To operationalize these question, I combine the factors identified from the health
disparity theoretical models presented in Chapter 2 with measures of intensity of PT process
of care to create a research design that examines if health disparities exist in functional
outcomes following a hip replacement. I have selected Donabedian’s quality of care model
(Donabedian, 2005) (Donabedian, 2003) consisting of three elements: “structure”, “process”
and “outcome” as the conceptual framework for the analytical model of this study.
The measures, as discussed by Donabedian are not elements of quality, but
mechanisms to assess quality. There is an assumed interrelationship among these methods of
judging quality of care and each has the potential to influence the other.

69
Briefly, structure refers to “how” care is delivered; it is the way in which the health care
system is set up or structured to deliver care. Included within the realm of structure are the
material resources (the facilities, equipment, traits and individual characteristics of the
workforce or patients), their organizational characteristics (i.e. performance review, types of
supervision, methods of paying for care), and the rules and regulations that govern how the
care is dispensed. For this analytic model, the demographic characteristics are also included
as structural variables; they don’t change and are part of the “structural” components within
which care is delivered. Process conveys what is done; this typically involves the actions
that comprise health care such as steps in diagnosis, patient education, treatment,
rehabilitation etc. According to this assessment approach, process also includes other
contributions to care such as the support offered by family and friends. Donabedian’s third
approach for quality assessment is that of outcome which references the results. These are the
changes seen in individuals and populations that are credited to health care. Specifically, this
form of assessment includes changes in health status, patient knowledge, patient and/or family
behavior as well as their satisfaction with the care received and its outcomes. Quality of care
is the result of numerous factors that fall within the domain of the three aforementioned
assessment measures. The analytical model used for this study will link structural theories of
health disparities (demographic, social and economic characteristics) with intensity of PT
process of care and then examine whether health disparities exist in their individual and
collective impact on post – hip replacement patient outcomes.
3.1 Study population
Hip arthroplasty is a surgical procedure frequently needed by the older adult to address
pain and functional limitations commonly associated with arthritis. Therefore, the Medicare

70
population, primarily consisting of individuals 65 years and older, is ideal for this research.
Incorporating uniform coding for individual patient demographic and clinical variables as well as
procedural codes, billing information and patient outcome information, Medicare data files
provide a rich source of standardized data for this research.
One aspect of the Medicare program makes the use of its data particularly relevant for
this research. This year marks the fiftieth year anniversary of the implementation of Medicare.
The legislation signed into effect by Presidnt Lyndon Johnson guaranteed health insurance for all
Americans sixty-five years of age and older. This legislation was one year subsequent to the
Title VI of the Civil Rights Act which prohibited discrimination based on racial and/or national
origin by any program receiving federal funding. Medicare required that hospitals eliminate
discrimination and segregation to receive payment from the Medicare program. Examples of
practices outlawed by Medicare included private hospitals restricted to whites with primary
county hospital for blacks, racially segregated hospital wards, denial of physicians’ admission
and/or surgical privileges as specific racial/ethnic or religious health care institutions. Hospitals
that continued these practices would not be eligible for government funded Medicare support.
As reported by Smith (2016), compliance with the Medicare hospital desegregation regulations
would afford hospitals more than fifty percent of their revenues. In most cases, during the
1960’s hospitals had daunting deficits as the cost of the health care they provided increased
while the ability of patients (about half of whom were age sixty-five and older) decreased.
Voluntary health insurance for high users of care (the elderly) was prohibitive for most hospitals.
Thus the financial implications of non-adherence to the requirements of Medicare outweighed
the preference to maintain a segregated hospital facility. Consequently, the “Golden Rule”
prevailed; “Those with the gold ruled”. In this case, the government’s monetary support via the

71
Medicare insurance plan ultimately not only reduced racial/ethnic discrimination but also was the
difference between “expanded services and increased profitability or decline, insolvency and
closure (Smith, 2016 pg 131).
3.2 The Analytic Research Model
The Medicare data set provides data elements that will be incorporated into statistical
models to determine if health disparities exist in patient outcomes (outcome variables –
ambulation and transfer) subsequent to hip replacement, for those Medicare patients followed by
physical therapy through a home health agency and if these disparities can be explained by
structural variables (conceptualized here as patient demographics and economic conditions)
and/or process variables (intensity of care).
The following Medicare patient data elements (and the characteristic for which it serves
as a proxy) have been incorporated into the analytic statistical model. Table 3.1 summarizes and
defines the variables included in the analytic statistical model.
3.2.1 Structural variables
For this analytic statistical model, the independent demographic variables of the study
population (personal structural characteristics such as age, gender, race/ethnicity and
comorbidities) will capture components of the theoretical models of health disparities. Also,
social economic status as measured by dual enrollment Medicare and Medicaid and cost share
with low income subsidy status is used as social indicator and urban or rural residence indicate
the geographical component of the structural variables of the Medicare beneficiary.
3.2.2 Process variables

72
The length of hospital stay, the total amount charged for PT service in the acute hospital
setting and the total number of PT visits during home health care were the data elements used to
measure this variable.
3.3.3 Outcome variables
Two variables assessing activities of daily living (ADL) were used as measures of
functional outcome in this study. Transferring outcome variable evaluated the patients’ ability
to move safely from bed to chair or the ability to turn and position self in bed if the individual is
bedfast. Ambulation/locomotion outcome variable assessed the patients’ ability to walk safely,
once in a standing position, or use a wheelchair, once in a seated position, on a variety of
surfaces (i.e. level or uneven). Both functional outcomes were measures of the patients’
rehabilitation status upon discharge within one 60-day episode of HHA services
3.4 Summary
Table 3.1 describes the structure-process-outcome variables as operationalized in this
study.

73
Table 3.1 Donabedian’s Structure – Process – Outcome Model: Analytic Model Applied to this Study
Structure Variable Means of Measurement CMS File Source
Personal Characteristics
Race/Ethnicity White, Black, Hispanic, Asian, North American Native, Unknown, Other MBSF Age 65 and/or older MBSF Sex Male, Female MBSF Co-morbidities Number between 1 – 25 MBSF
Social SES
According to health insurance status: Medicare Part “A” & “B” Dual Enrollment: Medicare/Medicaid status Cost Share – Low Income Subsidy status
MBSF
Geographic Beneficiary’s residence Urban or Rural MBSF Process Variable Means of Measurement CMS File Source Acute hospital length of
stay # / count of days in acute hospital LOS_DAY_CNT
MedPAR
Inpatient PT services Total charge amount for inpatient PT services PHYS_THRPY_CHRG_AMT
MedPAR
Home Health PT services
Number of HHA visits/ 1 episode of care (60 days) TOT VST CNT
HHA
Outcomes Variable Means of Measurement CMS File Source
M1850 - Transferring 00 = Able to independently transfer. 01 = Able to transfer with minimal human assistance or with use of an assistive device. 02 = Able to bear weight and pivot during the transfer but unable to transfer self. 03 = Unable to transfer self and is unable to bear weight or pivot when transferred by another person. 04 = Bedfast, unable to transfer but is able to turn and position self in bed. 05 = Bedfast, unable to transfer and is unable to turn and position self.
OASIS
M1860 – Ambulation/Locomotion
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device). 01 = With the use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or without railings. 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces. 03 = Able to walk only with the supervision or assistance of another person at all times. 04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.
OASIS

74
CHAPTER 4 Methods
4.1 Study Overview
The purpose of this study is to examine if differences exist in the utilization of physical therapy
rehabilitation services and in functional outcome abilities of a national, representative sample of
racially and ethnically diverse Medicare beneficiaries discharged from an acute care hospital to
their home with home health care rehabilitation following total hip replacement (THR).
4.1.1 Primary research questions:
After controlling for identified and obtainable confounding variables, are there
racial/ethnic disparities in functional outcomes as assessed by:
o Differences in transfer abilities as evaluated via OASIS variable M1850?
o Differences in ambulation/locomotion abilities as evaluated by OASIS variable
M1860?
4.1.2 Secondary research questions:
After controlling for identified and obtainable confounding variables, are there
racial/ethnic disparities in process characteristics of the quality of care model for the study
sample as measured by the:
o acute hospital length of stay
o acute hospital PT charges
o number days from hospital discharge to final home health care discharge
assessment (within 1 60-day episode of care)?
4.1.3 Descriptive questions:
What are the demographics of the study sample as assessed by the following variables?
o race/ethnicity,

75
o age,
o sex,
o geographical location,
o number of co-morbidities,
o Social Economical Status
4.1.4 Hypotheses: null (HO) and alternative (Ha)
Five hypotheses are used to examine whether racial/ethnic and/or the process by which physical
rehabilitation administered to the Medicare beneficiaries in this study sample impacted their
functional outcome.
1. HO There are not racial/ethnic disparities in functional outcome of the study sample
as measured by M1850 – Transferring ability of Medicare beneficiaries who were
discharged to their home with Physical Therapy rehabilitation under the auspices of a
CMS certified home health agency subsequent to a total hip replacement.
Ha There are racial/ethnic disparities in functional outcome of the study sample as
measured by M1850 – Transferring ability of Medicare beneficiaries who were
discharged to their home with Physical Therapy rehabilitation under the auspices of a
CMS certified home health agency subsequent to a total hip replacement.
2. HO There are not racial/ethnic disparities in functional outcome of the study sample as
measured by M1860 - Ambulation/locomotion ability of Medicare beneficiaries who
were discharged to their home with Physical Therapy rehabilitation under the
auspices of a CMS certified home health agency subsequent to a total hip
replacement.

76
Ha There are racial/ethnic disparities in functional outcome of the study sample as
measured by M1860, Ambulation/locomotion ability of Medicare beneficiaries who
were discharged to their home with Physical Therapy rehabilitation under the
auspices of a CMS certified home health agency subsequent to a total hip
replacement.
3. HO There are not racial/ethnic disparities in process characteristics of the quality of
care model of the study sample as measured by the acute hospital length of stay of
Medicare beneficiaries who were discharged to their home with Physical Therapy
rehabilitation under the auspices of a CMS certified home health agency subsequent
to a total hip replacement.
Ha There are racial/ethnic disparities in process characteristics of the quality of care
model for the study sample as measured by the acute hospital length of stay Medicare
beneficiaries who were discharged to their home with Physical Therapy rehabilitation
under the auspices of a CMS certified home health agency subsequent to a total hip
replacement.
4. HO There are not racial/ethnic disparities in process characteristics of the quality of
care model for the study sample as measured by the PT charge amount to Medicare
beneficiaries who were discharged to their home with Physical Therapy rehabilitation
under the auspices of a CMS certified home health agency subsequent to a total hip
replacement.
Ha There are racial/ethnic disparities in process characteristics of the quality of care
model for the study sample as measured by the PT charge amount to Medicare
beneficiaries who were discharged to their home with Physical Therapy rehabilitation

77
under the auspices of a CMS certified home health agency subsequent to a total hip
replacement.
5. HO There are not racial/ethnic disparities in process characteristics of the quality of
care model for the study sample as measured by the number days from hospital
discharge to final home health care discharge assessment (within 1 60-day episode of
care) of Medicare beneficiaries who were discharged to their home with Physical
Therapy rehabilitation under the auspices of a CMS certified home health agency
subsequent to a total hip replacement.
Ha There are racial/ethnic disparities in process characteristics of the quality of care
model for the study sample as measured by the number days from hospital discharge
to final home health care discharge assessment (within 1 60-day episode of care) of
Medicare beneficiaries who were discharged to their home with Physical Therapy
rehabilitation under the auspices of a CMS certified home health agency subsequent
to a total hip replacement
4.2 Data and Population Source
Administrative data from CMS Chronic Conditions Data Warehouse via the Research Data
Assistance Center (Res DAC), a CMS contractor based at the University of Minnesota, were
used in the study. The data request was for the cohort of Medicare beneficiaries, who in the
2012 calendar year, underwent an elective primary THR identified with codes 81.51 and 81.52 of
The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
The data files include information regarding but not limited to beneficiary diagnosis, socio-
demographic, environmental, health status and functional status attributes of adult (non-
maternity) patients. The specific CMS assessment and claims data files used in this study were

78
Medicare Provider Analysis and Review (MedPAR), Master Beneficiary Summary File (MBSF),
Home Health Agency File (HHA), and the Outcome and Assessment Information Set (OASIS).
Table 4.1 provides the relevant characteristics of the four 2012 CMS files used to access data for
the research questions.
Table 4.1 Characteristics of CMS Claims & Assessment Files Used for Data Sources*
Reference: https://www.resdac.org/cms-data/files/mbsf: accessed 12/17/2016
File Name Abbreviation Function
Medicare Provider Analysis and Review
MedPAR
Addresses Medicare utilization Contains inpatient hospital and skilled nursing facility (SNF)
final stay records. Includes: diagnosis & procedure codes (ICD-9), dates of
service, reimbursement amount, beneficiary demographic information.
Source used to identify the CMS beneficiaries with THR
Master Beneficiary Summary
MBSF
Includes several segments of information. The following were used for this study: Base A/B/D segment is the source for beneficiary enrollment
information, reasons for entitlement and monthly and yearly manage care indicators.
Chronic Conditions segment includes administrative data linked by a unique identifier allowing researchers to analyze information across the continuum of care,
Cost & Utilization segment includes summarized information about the service utilization and Medicare payment amounts by file type.
Home Health Agency HHA
Holds final actions, fee for service claim submitted by HHA providers:
Includes number and type of visit (i.e. skilled-nursing care, PT, OT, SpT health aide, medical social services) .
Holds final actions, fee for service claim submitted by HHA providers:
Includes number & type of visit (i.e. skilled-nursing care, PT, OT, SpT health aide, medical social services).
Outcome & Assessment Information Set
OASIS
Contains data items developed for measuring patient outcomes for the purpose of performance improvement in home health care.
Medicare certified home care agencies are required to conduct patient-specific comprehensive assessments at specified times. The data are collected at start of care, 60-day follow-ups, and discharge .
OASIS variable selection & justification worksheet must be completed to indicate & select which of the 500 plus variables are needed to carry out the study.
Source for functional outcome measures M 1850 & M1860 used in this study.

79
4.2.1 Security Issues
The nature of my research focuses on a specific cohort of CMS beneficiaries (a national
cohort of Medicare beneficiaries who received a THR in 2012) so a customized data file was
required. Thus, the requested files are classified as research identifiable files (RIF). Limited data
files are available only as 100% files or 5% random samples. Consequently, more information
than necessary would be provided if the 100% files were requested; while a 5% random file
would not necessarily afford me the minority representation needed for a statistically significant
analysis across racial/ethnic lines (variables).
Acquisition RIF files from a division of the federal government such as CMS requires the
researcher to assure that adherence to CMS regulations for acquisition and storage of the data can
and will be met. At the time of applying for the necessary files, my university did not have the
information technology infrastructure that satisfied the CMS requirements. Consequently, it was
necessary to seek an alternative. Fortunately, I was granted permission to store the requested CMS
data on a Health Insurance Portability and Accountability Act (HIPAA) secure server housed at
Boston University Department of Medicine. Its Technology Department maintains a data storage
and processing environment designed to meet the requirements of HIPAA for research purposes.
The data are stored under the aegis of the Boston Rehabilitation Outcomes Center on a protected
network on a storage solution that may only be accessed and manipulated through virtual desktops.
I have been provided with a Boston University [BU] login/username which allows me access to a
HIPAA secure server housed at BU where the requested CMS data are stored. This password
protected virtual desktop provides external security controls specially designed to meet the security
features required by HIPAA in a way that preserves a researcher-friendly environment that does not
unduly impede my work as an investigator.

80
Northeastern University Institutional Review Board granted IRB approval per IRB# 13-
06-12. Centers of Medicare and Medicaid granted DUA renewal through 10/31/2017 per DUA#
277708.
4.3 Pilot Study
A pilot study was conducted to assure that the planned request for a national Medicare
beneficiaries file would contain sufficient numbers to detect a difference, if it was present, in
THR outcome-based on racial/ethnic disparities. A request was made to the CMS contractor,
the Research Data Assistance Center at the University of Minnesota (ResDAC), for the
California-only Medicare data file that contained Medicare frequency and discharge destination
data for beneficiaries who underwent a total hip replacement (THR) in California during 2010.
California was selected as the pilot site after the following steps: 1) Analyses were
conducted to determine which states had the greatest population density of individuals age
65year old and older, the largest minority population, and the most diverse minority population.
The 2010 State by State Demographics: Race/Ethnicity/Gender table from the Administration on
Aging was used to identify these criteria. Those states in which the 65 year and older population
consisted of greater than 20 percent minorities were selected. 2) From that cohort, the frequency
of Medicare beneficiaries receiving a THR by state was examined. California was identified as
the state with the largest and most diverse minority senior citizen populations; it had a
cumulative total hip replacement frequency of 21,233 in 2010. If a statistically significant
difference could be found in outcomes based on racial/ethnic disparities in California, then it was
assumed that the power of the research study would be furthered strengthened when additional
states meeting these criteria were included.

81
The data were analyzed to address three objectives related to differences in the treatment
and functional outcomes among Medicare California patients with THR.
4.3.1 Pilot Study Objective 1
1.Examine the association between White and Non – White patients and five discharge
destinations (home/self-care; skilled nursing facility [SNF], home/home care [HHC], in-patient
rehabilitation facility [IRF], and all other destinations combined) for all patients who underwent
a THR (Table 4.1). Using a total sample size of 21,233 and the frequencies reported in the
Medicare data, there was 100.0% power to detect a difference in discharge destination across
White/Non-White groups using a chi-square test of association and a significance level equal to
0.05
Table 4.2 Pilot Study Data2
OBJECTIVE 1: Distribution of total hip replacement discharge destination by race/ethnicity
Home/Self-care SNF HHC IRF Other White 2000 8754 5219 993 580
Non-White 386 1867 973 313 148
Chi-Square Test Power Analysis — Numeric Results for Chi-Square Test
Power N W Chi-Square DF Alpha Beta 1.0 21,233 0525 68.5681 4 0.05000 0.00000
4.3.2. Pilot Study Objective
Among patients who underwent a total hip replacement, examine comparisons in five discharge
destinations by type of ethnicity group. Three pairwise comparisons were considered: White vs.
African-American, White vs. Asian/Pacific Islander, and White vs. Hispanic. Since multiple
comparisons were made, a Bonferroni correction for three comparisons to adjust the significance
level, alpha, to equal 0.05/3 = 0.017 was used to decrease the possibility of the results occurring
by chance. With the frequencies reported in the Medicare database, there is 97% power to detect

82
a difference between White/African-American; 100% power to detect a difference between
White/Asian; and 99.7% power to detect a difference between White/Hispanic using separate
chi-square tests with alpha for each test equal to 0.017. (Table “B”) Calculations were
performed using NCSS/PASS software.
Table 4.2 Pilot Study Data Continued
OBJECTIVE 2: Pairwise Comparison of Total Hip Replacement Discharge Designation Objective 2a - Frequency Table (White vs. African-American). Effect size = 0.034506; DF=4.
Home/Self-care SNF HHC IRF Other White 2000 8754 5219 993 580
African American
113 405 273 51 53
Objective 2b - Frequency Table (White vs. Asian). Effect size = 0.075867; DF=4.
Home/Self-care SNF HHC IRF Other White 2000 8754 5219 993 580 Asian 59 420 147 96 38
Objective 2c - Frequency Table (White vs. Hispanic). Effect size = 0.040638; DF=4. Home/Self-care SNF HHC IRF Other
White 2000 8754 5219 993 580 Hispanic 181 908 456 148 52
From this analysis, based on a sample size of 21,233 Medicare total hip replacement patients
from California, the sample size was sufficient to detect a difference in post-discharge
placement across racial/ethnic groups with 100% power to detect an effect size (W) of
0.0525 using a 4 degrees of freedom Chi-Square Test with a significance level (alpha) of
0.05000.
4.3.3 Pilot Study Objective 3
Among patients who were discharged with home health care (HHC), compare functional
outcomes across race/ethnicity groups. The transfer outcome is categorical and scored from 0-5;
the ambulation outcome is scored from 0-6. In California, there were 6,192 Medicare THR

83
patients who were discharged to home care. Approximately 80% of these patients were White
and 20% were all other ethnicities combined. Assuming 30% in the White group were
discharged with home health care, a total sample size of 6,125 achieves power of 100.0% to
detect a difference of one unit in the functional outcome scales assuming a standard deviation of
1.5. Calculations were conducted using PS software (Dupont and Plummer, 1997) with a two-
group t-test and two-sided alpha equal to 0.052
The pilot study conducted on a sample from one state (CA) of the study universe
indicates that the data have the power to detect significant racial/ethnic difference in discharge
destination between white and three other racial/ethnic Medicare beneficiary groups (African
Americans, Asians, and Hispanic) who had a THR during 2010. Differences in functional
outcomes measured by transfer and ambulation abilities scored from 0-5 and 0 -6 respectively
were also found. Based on the results of the pilot study it was determined that a dissertation
study of an even larger national population examining the same variables would yield significant
results, if differences were present.
4.4 Dissertation Study
This study examined functional outcome and process measures of Medicare beneficiaries
who received a THR during the 2012 calendar year.
4.4.1 Study Sample
The initial study universe included 249,060 Medicare patients who had a hip
replacement in 2012. As the data were reviewed and pertinent criteria were stipulated, the study
sample was decreased to include a final number of 21,448 CMS beneficiaries. Several
considerations were made that yielded the final cohort for this study. Table 4.2 summarizes the
process yielding the final study sample.

84
4.4.2 Sample Selection: Inclusion & Exclusion Criteria
Consideration was given to the invasiveness of the surgical procedure and its expected
impact on recovery time. Therefore, only those Medicare beneficiaries who received a THR
(ICD – 9 code = 81.51) were included in this study. Those who received a partial hip
replacement (ICD-9 code 81.52) (N=51,231) were excluded as the latter, less extensive surgical
procedure could afford a shorter recovery with a quicker attainment of functional abilities and
could possibly skew the results.
A key factor of interest was functional outcome in relation to racial and/or ethnic identity.
Therefore, per the options available in the Medicare data base, only those identified as (1)
white, (2) black, (3) other, (4) Asian, (5) Hispanic, or (6) North American Native were included
in the study. The results of those who were noted with “unknown” race/ethnicity were excluded
(N=243).
In an effort to assure a representative study sample of states that would provide adequate
racial and ethnic diversity (as well as a more urban than rural subject), only beneficiaries from
the 11 states that met the following criteria were included: 1) states where the THR frequency
was greater than 1500/state and 2) states where the proportion of THR was equal to or greater
than 3.0 percent of African American/blacks and/or 2.5 percent of at least one other minority
including “other”. Beneficiaries of the following continental states met the criteria and were
included in the analysis: CA, FL, GA, IL, MI, NC, NY, OH, PA, TX and VA. Beneficiaries
who resided in states or territories other than the ones identified were excluded.

85
Thus, the final study samples included patients who had total hip surgery, were 65 years
old or older, discharged to home with home care, were in one of the 11 identified states, and had
a race/ethnic classification code from 1-6.
Figure 4.4.1 illustrates the breakdown of the population following the application of each
criterion to refine the study sample.
4.4.3 Additional inclusion and exclusion criteria
Social economic status was also a factor considered in this analysis. Two proxies were
used for low income status: 1) whether a beneficiary was dually enrolled in Medicare and
Medicaid and/or 2) whether the beneficiary was the recipient of a limited income subsidy as part
of the Medicare Part “D” cost share group benefits.
A final critical feature for this study was a cut-off measure for the duration of home
health services. For the purposes of this research, post-surgical beneficiaries discharged from
home health care within one episode of care or 60 days were included in this study. Those
whose episode of home care was met during their acute hospital stay before discharge or that
extended into a second episode of care (i.e. within 120 days) were excluded from this study
4.4.4 Instrumentation
Data used to measure patient outcomes is drawn from the Outcome and Assessment
Information Set - OASIS, which is the home health assessment instrument. Implemented in
1999 and used by CMS to assess home health quality of care and to compute and report
measures from standardized data elements, OASIS assessment and documentation is used as a
payment basis for each home health sixty day episode of care delivered to Medicare
beneficiaries. The OASIS “C” is the most recent version of this outcome assessment tool and has
been in effect since January 2010. As noted on the CMS web site for OASIS, “Outcomes have

86
been defined in many ways, but those derived from OASIS items have a very specific definition:
they measure changes in a patient’s health status between two or more time points” CMS (1).
The instrument was designed to provide the necessary data items to measure both outcomes and
patient risk factors. The data elements of this instrument:
1. Represent core items of a comprehensive assessment for an adult home care patient; and
2. Form the basis for measuring patient outcomes for purposes of outcome-based quality
improvement (OBQI)”. (cms.gov)
An “OASIS Workbench Variable Selection & Justification Worksheet” must be completed to
indicate and provide rationalization for which of the 500 plus variables are being requested for
inclusion in the data output. Please see Appendix A for this document and Appendix B for the
OASIS “C” assessment tool.
4.5 Definition of variables
After examining the frequency distributions of the variables in the final data set of the
study sample, variables were defined as follows for statistical analyses:
4.5.1 Demographic/independent/ predictor variables
4.5.1.1 Race/ethnicity consists of three categories -- white, black, and others. The latter
category, consisting of those who self-identified as “other”, Asian, Hispanic, and /or North
American Native, was necessary because of small sample sizes in these populations. For
purposes of the analysis, the reference category in this study is white.
4.5.1.2 Gender is represented by two categories -- (1) male or (2) female.
4.5.1.3 Age is represented by the chronological age as of the end of the reference year (2012).
This variable is organized continuously in the model of analysis associated with the secondary
research question that focuses on processes and as such a linear regression analysis model is

87
used. However, age is organized in three categories (65-74, 75-84, and 85+ years) when
examining the primary research questions relative to functional outcome measures. The values
for these outcomes are categorical measures of ability regarding transfer from point “A” to “B”
on a scale of 00-05 and/or ambulation/locomotion on a scale of 00-06.
4.5.1.4 Geographic location is represented by two categories - (1) urban or (2) rural as identified
by beneficiary zip code and data indicator regarding urban or rural designation.
4.5.1.5 Socioeconomic status (SES) is represented by two categorical proxies (“yes” or “no”) in
response to two questions related to health insurance status indicative of whether or not the
beneficiary has 1) dual Medicare and Medicaid enrollment and/or 2) Cost Share Group with
Limited Income subsidy for Medicare Part D. A “yes” answer for either of the two is a proxy for
lower SES.
4.5.1.6 The number of co-morbidities is a proxy to measure the beneficiary’s overall burden of
disease. When continuous outcomes are concerned, it is characterized as a continuous variable
(range 1-25 co-morbidities). When examining categorical outcome variables, it is analyzed as a
categorical variable consisting of four levels roughly representative of quartile distribution of the
number of co-diagnoses (1- 4, 5-7, 8-11, and 12 or more).

88
Table 4.3 Structural and Process Variables of Study Sample Defined
Primary Analysis
Influences on Process and Outcome Dependent Variable Independent Variables
% predicted of dependent and relative contribution of dependent
Outcome # 1
Current Transfer Group A/Independent = 00 & 01 Group B/Dependent = 02 -05 or > 02
1-Race/Ethnicity: White; Black/African American Other as self-identified: Other’ including self-identified other, North American Native, Asian, Hispanic North American Native 2- Age: 65-74; 75-84; 85+ 3. Sex 4- Diagnosis Count 1-4; 5-7; 8-11 & 12+ 5 -Residence ‐ Urban ‐ Rural 6 – Length of Stay [LOS]: Quartile grouping 7 – Total PT Charge Amount: Quartile grouping 8 – Days_ Disch_2_assess: Quartile grouping
YES
Outcome # 2
Ambulation/Locomotion Group A/Independent = 00 & 01 Group B/Dependent = 02 -05 or > 02
1-Race/Ethnicity: White; Black/ African American Other as self-identified: Other’ including self-identified, Asian, & No American ; Asian; Hispanic No American Native 2- Age Continuous 65 – oldest beneficiary 3- Sex 4- Diagnosis Count -Continuous 1 – 25 -Categorical: 0-4; 5-7; 8-11 & 12+ 5 -Residence ‐ Urban ‐ Rural 6 – Length of Stay [LOS]: Quartile grouping 7 – Total PT Charge Amount: Quartile grouping 8 – Days_ Disch_2_assess: Quartile grouping
YES

89
Table 4.3 Structural and Process Variables of Study Sample Defined (Continued)
Secondary Analysis: Effect of Structural on Process Variables90
Influences on Process and Outcome Dependent Independent
% predicted of dependent and relative contribution of dependent
LOS Race/Ethnicity; Age; Sex; Diagnosis count; Residence
Total PT Charge Amount Race/Ethnicity; Age; Sex; Diagnosis count; Residence
Days_ Disch_2_assess Race/Ethnicity; Age; Sex; Diagnosis count; Residence
4.5.2 Process Variables
Three process variables are examined relative to their impact on the functional outcome
measures. Those examined include:
4.5.2.1 Length of acute hospital stay (LOS) is defined as the number of days the beneficiary is in
the hospital. It is measured continuously per hour and in fractions of the hour from admission to
discharge from the hospital.
4.5.2.2 Physical Therapy Charge amount is defined as a continuous dollar and cent numeration
representing the total claims charge per each beneficiary for PT services during the beneficiary’s
acute hospital stay.
4.5.2.3 The number of days from discharge to assessment represents the calculated number of
days between discharge from the acute care hospital to the final home health agency assessment
within one episode of care (60 days) for code 09 (discharged from HHA services). This
continuous variable serves as a proxy for the amount of HHC rendered to the post – surgical
patient.

90
4.5.3 Outcome/Dependent variables
4.5.3.1 Transfer (M1850). This measures the post-surgical patients’ current ability to
move freely from bed to chair, or ability to turn and position self in bed if patient is bedfast. This
variable assessed as one of five options as identified in Table 4.5.1.
Table 4.5.1 Outcome # 1: M – 1850 Current Transfers
00= Able to independently transfer. 01 = Able to transfer with minimal human assistance or with use of an assistive device. 02 = Able to bear weight and pivot during the transfer but unable to transfer self. 03 = Unable to transfer self and is unable to bear weight or pivot when transferred by another person. 04 = Bedfast, unable to transfer but is able to turn and position self in bed. 05 = Bedfast, unable to transfer and is unable to turn and position self.
4.5.3.2 Ambulation/locomotion (M1860) is used to assess the current ability to walk safely, once
in a standing position, or use a wheelchair, once in a seated on a variety of surfaces. This
variable assessed as one of six options as identified in Table 4.5.2.
Table 4.5.2 outcome # 2: M – 1860 Ambulation & Locomotion
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device). 01 = With the use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or without railings. 02=Requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces. 03 = Able to walk only with the supervision or assistance of another person at all times. 04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.
4.6 Analysis:
This was a retrospective cohort research design study based on secondary analysis of
Centers for Medicare and Medicaid Services (CMS) administrative claims and assessment data

91
files of beneficiaries who were admitted for and received a THR in 2012 calendar year in 11
selected states.
Descriptive statistical analysis was used to characterize the demographic variables
incorporated into statistical models. The analysis included measures of the means, standard
deviations and ranges of scores as appropriate (e.g., ranges of rating values for OASIS scores
that measure transferring and ambulation abilities). The two categorical outcome variables
examined levels of transfer abilities and ambulation/locomotion status. Our key predictors were
race/ethnicity, age, gender, number of co-morbidities, length of hospital stay, urban vs rural
place of residence, PT charge amount, number of days from hospital discharge to home health
care discharge, and socioeconomic status.
A logistic regression model that included four categories for race and ethnicity was used
in this analysis. Due to their relatively small percentage of the study sample, three of the original
racial/ethnic group classifications were included in the “Other” racial group: self-identified other,
Asian and North American Native. The Hispanic group devoid of any accompanying racial
classification was kept as the only ethnic form of identity. The CMS data used did not include
options for more than one form of identification and therefore racial/ethnic identification in this
research included these four classifications: white, black, Hispanic and “Other “as defined above.
The Statistical Analysis System (SAS) Version 9.3 (SAS Institute, Cary NC) was used
for all data analyses. Chi Square test with Fisher exact test, when appropriate, was used to assess
the association between important predictors and the 2 study outcomes. Logistic regression
models were used to calculate the crude and adjusted odds ratios with confidence intervals.
Multivariate linear regressions were also used for continuous process variables (e.g., length of
acute hospital stay.

92
Chapter 5 Results
5.1 Evolution of Study Population
The study universe consisted of 249,060 Medicare beneficiaries who underwent surgery
for hip replacement in the U.S. and its territories during 2012. Based on inclusion/exclusion
criteria summarized in Chapter 4 and Figure 5.1, this number was reduced to yield the study
sample. The primary source of exclusion (N=142,247) was of those who were discharged to
destinations other than to the study’s specified location, a CMS certified home health agency for
post-operative physical rehabilitative care. This study included only those medically classified as
having had a primary THR (ICD - 9 code 81.51). Consequently 51,239 individuals who
underwent surgical hip replacement under any other classification (i.e. partial hip replacement,
ICD – 9 code 81.52) were excluded from this study.
A primary focus of this research was to examine the relationship between race/ethnicity
and the post-surgical outcomes of CMS beneficiaries who had a THR. Consequently, states with
larger diverse populations were chosen in an effort to attain a representative racial and ethnic
diverse study sample. As a result, 16,402 who were not from the eleven selected states were
excluded from this study. An additional5.14% of the original total population was excluded due
to missing data, being less than 65 years of age, not having an identified racial or ethnic
classification indicated on record, or not having a discharge assessment within sixty days of
discharge from the acute care hospital. The final study sample included 21,448 individuals from
the 11 selected states who were discharged from an acute care hospital following a primary THR
(ICD-9 code 81.51) to a Medicare certified home health care agency (Figure 5.1).

93
Figure 5.1 Study Universe Flowchart

94
5.2 Characteristics of Study Variables Used in Analytic Modeling
The demographic and clinical characteristics of the study sample structural variables (i.e.
age, gender etc.), the process variables (i.e. length of hospital stay) and the primary outcomes
(transfer and/or ambulation ability) are presented in Tables 5.1, 5.2, 5.3.1 and 5.3.2 respectively.
5. 2.1 Demographic and Clinical Characteristics of the Study Sample: Structural Variables
The study sample was predominantly non-Hispanic white (93.27%), female (56.20%) and
resided in urban areas of the 11 selected states (83.49%). Five states (California, Florida,
Pennsylvania, Texas and North Carolina) accounted for 60 % (N=12,965) of the sample.
Although the data set included those who ranged in age between 65 and 109 years, the majority
(63.23%) who underwent this procedure were between 65 and 74 years old. Fifty-five percent of
the study sample had between 1 and 7 co-morbidities. Socioeconomic status as measured via
dual status (full or restricted enrollment in Medicare and Medicaid or cost share group status for
Medicare part D with full or low-income subsidy) was less than 3 and 4 percent respectively. A
review of Table 5.1 (below) reveals that in most instances, the structural variables of racial and
ethnic groups follow the same trends of the total study sample. An exception is noted for gender
which was equally distributed within the self-identified “Other” group.

95
Table 5.1 Study Sample Characteristics/Donabedian Structural variables by **
Variables Total Study Population
White Black Other Self-identified
Asian Hispanic North American Native
N 21448 20048 (93.47%) 1011 (4.71%) 193 (0.90%) 94 (0.44%) 91 (0.42) 11 (0.05%)
Age Group 65-74 Y.O. 13631 (63.55%) (63.55%) 717 (70.92%) 141(73.06%) 52 (55.32%) 56 (61.54%) ** 75- 84 Y.O. 6969 (32.49%) 6591 (32.88%) 271 (26.81%) 48 (24.87) 32 (34.04%) 23 (25.27%) ** 85 + Y.O. 848 (3.95%) 799 (3.99%) 23 (20.27%) ** 10 (10.64%) 12 (13.19%) Mean 73.06 73.12 71.95 72.89 74.4 74.37 Median 72.00 72.00 71.00 71.50 73.00 72.00 Standard Deviation
5.73 5.73 5.35 5.99 7.17 7.50
Sex Male 9444 (44.03%) 8871(44.25%) 400 (39.56%) 96 (49.74%) 33 (33.67%) 39 (42.86%) ** Female 12004(55.97%) 11177(55.75%) 611 (60.44%) 97 (50.26%) 65 (66.33%) 52 (57.14%) ** Dx Count 0-4 4859 (22.65%) 4538 (22.64%) 238 (23.54%) 38 (19.69%) 23 (24.47%) 19 (20.88%) ** 5 - 7 7098 (33.09%) 6629 (33.07%) 344 (34.03%) 60 (31.09%) 31 (32.98%) 33 (36.26%) ** 8 - 11 6063 (28.27%) 5662 (28.24%) 280 (27.70%) 63 (32.64%) 29 (30.85%) 23 (27.47%) ** 12+ 3428 (15.98 %) 3219 (16.06%) 149 (14.74%) 32 (16.58%) 11 (11.70%) 14 (15.38%) Residence Urban 17909 (83.49%) 16665(83.13%) 896 (88.63%) 169 (87.56%) 87 (92.55%) 82 (90.11%) **
Rural 3541 (16.51%) 3383 (16.87%) 115 (11.37%) 24 (12.44%) 7 (7.45%) 9 (9.89%) **
** Per CMS requirements results with N < 10 are not reported

96
Table 5.1 Study Population Characteristics/Donabedian Structural variables** (Continued)
State ID (selected)
Total Study Population
N (%/study pop)
White N (%/State)
(%/study pop)
Black N (%/State)
(%/study pop)
Other N (%/State)
(%/study pop)
Asian N (%/State)
(%/study pop)
Hispanic (N (%/State)
(%/study pop)
No. American Native
N (%/State) (%/study pop)
N 21448 20048 (93.47%) 1011 (4.71%) 193 (0.90%) 94 (0.44%) 91 (0.42) 11(0.05%)
CA 3616 (16.86%)
3320 (16.56%) (91.81%)
119 (11.77%) (3.29%)
81 (41.97%) (2.24%)
55 (58.51%)(1.52%)
37 (40.66%)(1.02)
**
FL 3543 (16.52%) 3428 (17.10%) (96.75)
70 (6.92%) (1.97%)
25 (12.95%) (0.70%)
** 14 (15.38%)(0.39%)
-----
GA 1113 (5.19%) 965 (4.81%) (86.70%)
137 (13.55%) (12.3%)
** ** ** -----
IL 1504 (7.01%) 1407 (7.02%) (93.55%
81 (8.01%) (5.38%)
** ** ** -----
MI 1491 (6.95%) 1393 (6.95%) (93.42%)
85 (8.41%) (5.70%)
10 (5.18%) (0.67%)
** ** -----
NC 1749 (8.15%) 1570 (7.83%) (89.76%)
157 (15.53%) (8.97%)
13 (6.74%) (8.97%)
** ** **
NY 1566 (7.30%) 1495 (7.46%) (95.46%)
53 (5.24%) (3.38%)
** ** ** **
OH 1285 (5.98%) 1211 (6.04%) (94.46%)
54 (5.34%) (4.21%)
** ** -----
PA 2287 (10.66%) 2207 (11.01%) (96.50%)
65 (6.43%) (2.84%)
12 (6.22%) (0.52%)
** **
**
TX 1770 (8.25%) 1663 (8.30%) (93.95%)
66 (6.53%) (3.72%)
14 (7.25%) (0.79%)
**
22 (24.18%) (1.24%)
VA 1527 (7.12%) 1389 (6.93%) (90.96%)
124 (12.27%) (8.12%)
8 (4.15%) (0.52%)
** ** **
** Per CMS requirements results with N < 10 are not reported

97
Table 5.1 Study Sample Characteristics/Donabedian Structural variables** (Continued) Socioeconomic Status — 1-Dual Status Medicare/Medicaid Full or Restricted
No (0) 20838 (97.16%) 19615 (97.84%) 904 (89.42%) 180 (93.26%) 75 (79.79%) 56 (61.54%) ** Yes (1)
610 (2.84%) 433 (1)2.16 107 (10.58%) 13 (6.74%) 19 (20.21%) 35 (38.46%) **
Socioeconomic Status — 2-CSG Status Dual entry/LIS Full or low Income Subsidy (LIS)
No 20645 (96.26%) 19489 (97.06) 870 (86.05%) 179 (92.75%) 74 (78.72%) 55 (60.44%) ** Yes
803 (3.74%) 589 (2.94) 141 (13.95%) 7.25%) 20 (21.28%) 36 (39.56%) **
** Per CMS requirements results with N < 10 are not reported

98
5.2.2 Characteristics of the Study Sample: Process Variables
As noted in Table 5.2 (below), descriptive process variables are measured via three
factors: the length of stay in the acute hospital where THR was performed, the total charge
amount for physical therapy while in the acute care hospital, and the number of days between
discharge from the acute care hospital and the home health care agency. Patients in the total
study sample spent an average of 2.9 days in the acute care hospital; the range across all racial
and ethnic groups was between 2.89 and 3.19 days. The median charge amount for physical
therapy services in the acute care hospital was between $1110 and $1190 for white, black and
others of the study population, but was $1413 for Hispanics. The number of days between
discharge from the acute hospital setting and the discharge assessment within one episode of care
(60 days) from the home health care agency was the proxy used for the number of days spent in
home health care after hospital discharge process. The median length of post-acute home health
care was 20 days for the total study sample, while the median for blacks and Hispanics was 23
and 24 days respectively.

99
Table 5.2 Study Sample characteristics: Donabedian Process Variables by Race/Ethnicity
Length of Stay/day count In hospital
Total Study Population N = 21448
White N = 20048
Black N = 1011
Other (Self-identified, Asian, N. American Native) N = 298
Hispanic N = 91
Mean 2.90 2.89 3.05 3.00 3.19
Median 3.0 3.0 3 3.00 3
Standard Deviation 1.84 1.68 1.30 1.71 1.56
Hospital PT charge amount ($)
Mean 1405.89 1407.97 1310.31 1510.05 1667.98
Median 1179.00 1184.00 1110.00 1190.50 1413.00
Standard Deviation 1020 1012 978.89 1391 1552
Days Hospital Discharge – Home Health Agency Discharge
Mean 22.63 22.47 25.09 23.27 28.96
Median 20.00 20.00 23.00 20.00 24.00
Standard Deviation 10.77 10.67 11.56 11.48 16.19

100
5.2.3 Characteristics of the Study Sample: Outcome Variables
Tables 5.3.1 and 5.3.2 summarize the level of performance of the four racial/ethnic
groups for the two variables (transfer ability and ambulation/locomotion) used to assess post-
operative functional ability at termination of home health care rehabilitation services. Greater
than 99% of the total study sample was found to be either independent or in need of minimal
assistance to transfer from one surface or position to another. The results were similar across
each of the four racial/ethnic groups of the study sample, and as such the data at the descriptive
level essentially indicated no true variance for transfer ability, when the outcome was stratified
into two groups (Tables 5.4.1 - 5.4.9). The independent group included those who were
independent and minimally dependent. The dependent included those whose status ranged from
moderately dependent to totally dependent. Because independent group included ninety-nine
percent of the study sample, it was decided to further stratify this group into two: fully
independent and minimally dependent. Therefore, the final analysis that examined transfer
ability was conducted with three groups: Independent, Minimal dependence, and those with
Moderate through Total dependence. A total of 69 percent of both the total study sample and
white group were independent with transfer ability compared to 62 percent of those who were
black, 55 percent Hispanic and 67 percent classified as “Other”. Both the total study sample and
those who were identified as white included thirty percent who could transfer with minimal
dependence, compared to 32 percent of those who were classified as other, 37 who were black
and 42 percent who were Hispanic. Less than half of one percent of either the total study sample
or any of the racial/ethnic groups were moderately to totally dependent in their transfer abilities
(Table 5.3.1).

101
Table 5.3.1 Study Sample characteristics: Donabedian Transfer Ability Outcome Variable by Race/Ethnicity**
Current Transfer Ability
Total Study Population N = 21448
White N = 20048
Black N = 1011
Other N = 298
Hispanic N = 91
00 : transfers independently
14821 (69.10%)
13943 (69.55%) 629 (62.22%) 199 (66.77%) 50 (54.95%)
01: transfers with minimal human assistance or with use of an assistive device
6541 (30.50%)
6029 (30.07%) 377 (37.29%) 97 (32.55%) 38 (41.76%)
02: bear weight and pivot during the transfer but unable to transfer self.
74 (0.35%) 65 (0.32%) ** ** **
03: Unable to transfer self and is unable to bear weight or pivot when transferred by another person
** ** 0 (0.00%) 0 **
04: Bedfast, unable to transfer but is able to turn and position self in bed
** ** 0 (0.00%) 0 0 (0.00%)
05: Bedfast, unable to transfer and is unable to turn and position self
2 ( 0.01%) 2 (0.01%) 0 (0.00%) 0 0 (0.00%)
NOTE: “Other” = Self-identified as other, Asian, and North American Native ** Per CMS requirements results with N < 10 are not reported5.3. Bivariate Analyses
The bivariate analysis examined each variable individually as a predictor for the two
functional outcomes measured – transferring and ambulation/locomotion. The results of the chi
square analysis presented in Tables 5.4.1-5.4.9 reveals several variables with p-values indicating
statistical significance in the difference in levels of that variable and both the transfer and
ambulation/locomotion outcomes. Race/ethnicity, socioeconomic status, length of acute hospital
stay, the charges for physical therapy during the acute hospital stay, and the number of days to
discharge assessment from home health care were all found to be statistically significant with p
values of < 0.0001- 0.0114. However, although this statistic confirms a difference, it does not
specify where the difference exists. For instance, the p-value of 0.0080 indicates a statistically
significant difference in transfer ability that can be attributed to race/ethnicity. There is also a

102
statistically significant difference in the ambulatory/locomotion abilities among racial/ethnic
groups (p-value < 0.0001). However, it was not apparent where the difference lay.
5.4 Outcomes for Transfer Ability
To determine where differences lay, a multivariate logistic regression was performed to
assess the difference in outcomes among groups.
The crude and adjusted odds ratios for transfer abilities are presented in Table 5.5
(below). The same independent variables identified in the chi square analysis were found to be
significant when the crude odds ratios were calculated. However, compared to the white
reference group, the Hispanic group was the only non-white racial/ethnic group that showed
significant difference with transfer ability: OR 8.95 (2.774, 28.939). The observed difference
persisted after adjusting for all the other variables: OR 5.201 (1.424, 18.989); Hispanics were
five times more likely to be dependent compared to whites. The wide confidence interval also
indicates a low precision of the odds ratio which might be due to the small number (n=91) in the
Hispanic group. However, race/ethnicity persisted as key predictor of the difference in transfer
outcome when a multinomial logistic regression analysis was performed using three level
stratification of assessment for transfer ability (Table 5.6). Blacks were 1.38 times
(approximately 40%) more likely to be minimally dependent compared to whites: OR 1.386
(1.211, 1.585).

103
Table 5.5 Odds Ratio Estimate – Transfer Status: Crude, Adjusted & Relative Importance
**LOHHC - Length of home health care services equals the number of days from hospital discharge to discharge from home health care.
Variables Crude Odds Ratio
(95% Confidence Limits)Adjusted Odds Ratio
(95% Confidence Limits)
Relative Importance (amount of weight/variable
on Transfer status)
Race/Ethnicity Reference = White
Black 1.306 (0.527, 3.235) 1.23 (0.496, 3.167) * Hispanic 8.959 (2.774, 28.939) 5.201 ( 1.424, 18.989) 3.06%
Other 1.776 (0.434, 7.263) 1.621 (0.389, 6.754) * Age Groups
Reference = 85+
65 – 74 vs 85+ 0.546 (0.216, 1.380) 0.680 (0.264, 1.751) * 75 – 84 vs 85+ 0.900 (0.353, 2.296) 1.040 (0.403, 2.683) *
Gender Reference = Male
Female 1.204 (0.781, 1.857) 1.132 (0.729, 1.758) * Residential Location
Reference = Urban
Rural Area 1.247 (0.733, 2.123) 1.399 (0.811, 2.413) * Comorbidities
Reference = 12+
0 – 4 0.580 (0.285, 1.178) 0.774 (0.372, 1.611) * 5 -7 0.766 (0.285, 1.178) 0.947 (0.507, 1.767) *
8 – 11 0.931 (0.509, 1.703) 1.049 (0.569, 1.934) * Continuous 1.042 (0.993, 1.093)
**LOHHC Reference = 1st Quartile 1-15 days
16 – 30 (2nd Quartile) 0.516 (0.282, 0.946) 0.440 (0.239, 0.810) -0.2011 (10.44%) 31 – 45 (3rd Quartile) 0.412 (0.204. 0.833) 0.322 (0.158, 0.656) -0.2614 (13.57%) 46 – 60 ( 4th Quartile) 1.392 (0.837, 2.315) 0.871 (0.508, 1.492) * PT Charge Amount $
Reference = 1st Quartile $0 - 754
2nd Quartile $755 – 1179) 1.664 (0.801, 3.457) 1.539 (0.734, 3.227) *
3rd Quartile $ 1180 - 1771 1.614 (0.794, 3.284) 1.438 (0.694, 2.980) *
4th Quartile $ 1772 – 15,740
2.974 (1.524, 5.735) 2.236 (1.116, 4.478) 0.1915 (9.94%)
Hospital Length of Stay Reference = 0-6
2nd Quartile 7 – 12days 1.796 (0.989, 3.259) 1.522 (0.823, 2.813) * 3rd Quartile 13 - 18 days 4.299 (2.227, 8.301) 3.118 (1.543, 6.300) 0.2007 (10.42%)
4th Quartile 19-24 days 3.960 (1.775, 8.835) 2.482 (1.038, 5.936) 0.1164 (6.04%)

104
Table 5.5 Odds Ratio Estimate – Transfer Status: Crude, Adjusted & Relative Importance (Continued)
When examining the effect of the length of home care services on transfer ability, the
second and third quartile (16-30 and 31-45 days of care respectively compared to 1-15 days)
were more likely to need assistance with transfers: OR 0.516 (0.282, 0.946) and 0.412 (0.201,
0.833) respectively. This suggests that on average those in the second or third quartile are 50%
more likely to be dependent with transfer ability than those in the first quartile. The OR estimate
for the fourth quartile was not significant (Table 5.5). The multinomial logistic regression
analysis indicated that whether the reference group was independent (Table 5.6) or minimally
dependent (Table 5.7), the results were consistent with the above findings: the longer the stay in
home health care, the more likely you are to be dependent. For example, with the independent
group as the reference, the moderate to totally dependent group of second and third quartiles
were more likely to need assistance with transfers: OR 0.390 (0.212, 0.717) and 0.272 (0.133,
0.554) respectively (Table 5.6).
Variables Crude Odds Ratio
(95% Confidence Limits)
Adjusted Odds Ratio
(95% Confidence Limits)
Relative Importance (amount of weight/variable
on Transfer status)
Socioeconomic Status Reference : Medicare
Only
Dual Status (Medicare & Medicaid) 3.539 (1.702, 7.358) 7.478 (0.473, 118.141)
Cost Share Group (Low Income Subsidy) 2.653 (1.277, 5.512) 0.282 (0.018, 4.453)

105
Table 5.6 Multinomial Logistic Regression Odds Ration for Transfer Ability: Reference = Independent Table 5.6 Multinomial Logistic Regression Odds Ration for Transfer Ability: Reference
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Race/Ethnicity Comorbidity Count Reference = 12+
Black – Moderate -total Dependence
1.417 (0.560, 3.583) 0 – 4 Moderate -total Dependence
0.682 (0.328, 1.420)
Black – Minimal Dependence
1.386 (1.211,1.585) 0 – 4 Minimal Dependence
0.697 (0.632, 0.769)
Hispanic Moderate -total Dependence
6.155 (1.665, 22.753) 5 -7 Moderate -total Dependence
0.866 (0.464, 1.617)
Hispanic Minimal Dependence
1.516 (0.982, 2.339) 5 – 7 Minimal Dependence
0.784 (0.717, 0.857)
Other Moderate -total Dependence
1.677 (0.401, 7.009) 8 – 11 Moderate -total Dependence
0.981 (0.523, 1.811)
Other Minimal Dependence
1.108 (0.865, 1.421) 8 – 11 Minimal Dependence
0.838 (0.766, 0.917)
Age Groups
Days Acute Hospital Discharge – to Home Health Agency Discharge (days) Reference = 1st Quartile 1-15 days
65 – 74 vs 85+ Moderate -total Dependence
0.611 (0.237, 1.576) 16 – 30 (2nd Quartile) Moderate -total Dependence
0.390 (0.212, 0.717)
65 – 74 vs 85+ Minimal Dependence
0.748 (0.645, 0.868) 16 – 30 (2nd Quartile) Minimal Dependence
0.707 (0.655, 0.763)
75 – 84 vs 85+ Moderate -total Dependence
0.963 (0.373, 2.489) 31 – 45 (3rd Quartile) Moderate -total Dependence
0.272 (0.133, 0.554)
75 – 84 vs 85+ Minimal Dependence
0.816 (0.701, 0.949) 31 – 45 (3rd Quartile) Minimal Dependence
0.610 (0.562, 0.663)
Gender 46 – 60 ( 4th Quartile) Moderate -total Dependence
0.736 (0.428, 1.264)
Female Moderate -total Dependence
1.201 (0.773, 1.866) 46 – 60 ( 4th Quartile) Minimal Dependence
0.622 (0.568. 0.680)
Female Minimal Dependence
1.188 (1.119, 1.262)
Residential Location Reference = Urban
Rural Area Moderate -total Dependence
1.467 (0.850, 2.532)
Rural Area Minimal Dependence
1.143 (1.055, 1.238)

106
= Independent (Continued)
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Physical Therapy Charge Amount: Acute Care Hospital Stay ($) Reference = 1st Quartile $0 - 754
Socioeconomic Status
2nd Quartile $755 – 1179) Moderate -total Dependence
1.520 (0.724, 3.187)
Dual Status (Medicare & Medicaid) Moderate -total Dependence
8.184 (0.521, 128.502)
2 Quartile $755 – 1179 Minimal Dependence
0.970 (0.890, 1.057) Dual Status (Medicare & Medicaid) Minimal Dependence
1.261 (0.906, 1.757)
3rd Quartile $ 1180 – 1771 Moderate -total Dependence
1.427 (0.688, 2.959)
Cost Share Group (Low Income Subsidy) Moderate -total Dependence
0.305 (0.019, 4.765)
3rd Quartile $ 1180 – 1771 Minimal Dependence
0.980 (0.901, 1.066) Cost Share Group (Low Income Subsidy) Minimal Dependence
1.195 (0.892, 1.600)
4th Quartile $ 1772 – 15,740 Moderate -total Dependence
2.17 (1.085, 4.359)
4th Quartile $ 1772 – 15,740 Minimal Dependence
0.926 (0.848, 1.012)
Hospital Length of Stay 2nd Quartile 0 – 3 days Moderate -total Dependence
1.641 (0.887, 3.036)
2nd Quartile 0 – 3 days Minimal Dependence
1.272 (1.186, 1.364)
3rd Quartile 0 - 3 days Moderate -total Dependence
3.537 (1.748, 7.155)
3rd Quartile 0 - 3 days Minimal Dependence
1.471 (1.325, 1.632)
4th Quartile 3 – 24 days Moderate -total Dependence
3.141 (1.311, 7.525)
4th Quartile 3 – 24 Minimal Dependence
1.931 (1.686, 2.211)

107
Table 5.7 Multinomial Logistic Regression Odds Ratio for Transfer Ability: Reference = Minimal Dependence
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Race/Ethnicity Comorbidity Count Reference = 12+
Black – Moderate -total Dependence
1.023 (0.404, 2.592) 0 – 4 Moderate -total Dependence
0.979 (0.469, 2.040)
Black – Independent
0.722 (0.631, 0.826) 0 – 4 Independent
1.434 (1.301, 1.581)
Hispanic Moderate -total Dependence
4.061 (1.093, 15.087) 5 -7 Moderate -total Dependence
1.104 (0.590, 2.066)
Hispanic Independent
0.660 (0.428, 1.018) 5 – 7 Independent
1.275 (1.167, 1.394)
Other Moderate -total Dependence
1.513 (0.360, 6.360) 8 – 11 Moderate -total Dependence
1.171 (0.633, 2.164)
Other Independent
0.902 (0.704, 1.157) 8 – 11 Independent
1.193 (1.090, 1.305)
Age Groups
Days Acute Hospital Discharge – to Home Health Agency Discharge (days) Reference = 1st Quartile 1-15 days
65 – 74 vs 85+ Moderate -total Dependence
0.817 (0.316, 2.111) 16 – 30 (2nd Quartile) Moderate -total Dependence
0.551 (0.299, 1.0160
65 – 74 vs 85+ Independent
1.336 (1.152, 1.549) 16 – 30 (2nd Quartile) Independent
1.414 (1.310, 1.526)
75 – 84 vs 85+ Moderate -total Dependence
1.181 (0.456, 3.059) 31 – 45 (3rd Quartile) Moderate -total Dependence
0.445 (0.218, 0.910)
75 – 84 vs 85+ independent
1.226 (1.054, 1.427) 31 – 45 (3rd Quartile) Independent
1.639 (1.509,1.779)
Gender 46 – 60 ( 4th Quartile) Moderate -total Dependence
1.184 (0.687, 2.038)
Female Moderate -total Dependence
1.011 (0.650, 1.573) 46 – 60 ( 4th Quartile Independent
1.608 (1.470, 1.760)
Female Independent
0.842 (0.792, 0.894)
Residential Location: Reference = Urban
Rural Area Moderate -total Dependence
1.284 (0.743, 2.219)
Rural Area Independent
0.875 (0.808,0.948)

108
Table 5.7 Multinomial Logistic Regression Odds Ratio for Transfer Ability: Reference = Minimal Dependence (Continued)
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Physical Therapy Charge Amount: Acute Care Hospital Stay ($) Reference = 1st Quartile $0 - 754
Socioeconomic Status
2nd Quartile $755 – 1179) Moderate -total Dependence
1.567 (0.746, 3.292)
Dual Status (Medicare & Medicaid) Moderate -total Dependence
6.48, (0.411, 102.304)

109
The odds ratios for other variables such as age, gender and comorbidity count were not
significant relative to their impact on transfer ability when analyzed. The crude and adjusted OR
for those 65-74 and 75-84 years old were: OR 0.546 (0.216, 1.380) and 0.9 (0.353, 2.296)
[reference group: 85 years and older] respectively. However, when examined using the
multinomial logistic regression with “independent” as the reference group, the 65-74 and 75-84
age groups were 20 to 30% more likely to be minimally dependent: OR 0.748 (0.645, 0.868) and
OR 0.816 (0.701, 0.949) respectively. [Table 5.6].
5.5 Outcomes for Ambulation/Locomotion
Greater variance was observed in the ambulation/locomotion outcome among the total
study sample (Table 5.3.2). Thus the final analysis of ambulation/locomotion ability was
conducted with two groups: Group 1/Independent & minimal dependence and Group
2/moderately to totally dependent. At discharge, seventy-five percent of both the total study
2 Quartile $755 – 1179 Independent
1.031 (0.946, 1.124) Dual Status (Medicare & Medicaid) Independent
0.793 (0.569, 1.104)
3rd Quartile $ 1180 – 1771 Moderate -total Dependence
1.456 (0.701, 3.024)
Cost Share Group (Low Income Subsidy) Moderate -total Dependence
0.255 (0.016, 4.002)
3rd Quartile $ 1180 – 1771 Independent
1.020 (0.938, 1.110) Cost Share Group (Low Income Subsidy) Independent
0.837 (0.625, 1.121)
4th Quartile $ 1772 – 15,740 Moderate -total Dependence
2.348 (1.169, 4.715)
4th Quartile $ 1772 – 15,740 Independent
1.080 (0.988, 1.180)
Hospital Length of Stay 2nd Quartile 0 – 3 days Moderate -total Dependence
1.291 (0.697, 2.391)
2nd Quartile 0 – 3 days Independent
0.786 (0.733, 0.843)
3rd Quartile 0 - 3 days Moderate -total Dependence
2.405 (1.186, 4.877)
3rd Quartile 0 - 3 days Independent
0.680 (0.613, 0.755)
4th Quartile 3 – 24 days Moderate -total Dependence
1.67 (0.678, 3.905)
4th Quartile 3 – 24 Independent
0.518 (0.452, 0.593)

110
sample and those identified as white were found to be either independent or require minimal
assistance with ambulation (Group 1), compared to the ambulatory/locomotion status of blacks,
Other and Hispanic which ranged between 47 and 71 percent. Moderate to total dependency in
ambulation locomotion was greater for the black, Hispanic and Other groups (28 to 48%)
compared to the total study sample or white groups (25%). Less than one percent of all
racial/ethnic groups were chairfast or totally dependent.
Table 5.3.2 Study Sample characteristics: Donabedian Ambulation/Locomotion Outcome Variable by Race/Ethnicity**
Note: “Other” = self-identified as other, Asian, of North American Native ** Per CMS requirements results with N < 10 are not reported
Table 5.8 displays the crude and adjusted odds ratios with their 95% confidence intervals
and relative importance for the independent structural and process variables. Both bivariate and
Current Ability Ambulation/Locomotion
Total Study Population N = 21448
White N = 20048
Black N = 1011
Other N = 298
Hispanic N = 91
00 : independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
4174 (19.46%) 3988 (19.89%)
130 (12.86%)
44 (14.77%)
12 (13.18%)
01: Ambulates with use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
11926 (55.60%) 11148 (55.61%)
587 (58.06%)
156 (52.35%)
35 (38.46%)
02: Requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces
5186 (24.18%) 4764 (23.67%)
288 (28.49%)
95 (31.88%
39 (42.85%)
03: Able to walk only with the supervision or assistance of another person at all times
154 (0.72%)
141 (0.70 %)
** ** **
04: Chairfast, unable to ambulate but is able to wheel self independently
** ** ** 0 0
05: Chairfast, unable to ambulate and is unable to wheel self
** ** 0 0 0
06: Bedfast, unable to ambulate or be up in a chair
** ** 0 0 0

111
multivariate analyses were performed and there was not much difference in the effect size
between the two estimates. For example, compared to White, in bivariate analysis, the Black,
Hispanic, and Other racial/ethnic groups were found to be one to two and a half times more
likely to be moderately to totally dependent in their ambulatory or locomotion abilities at the
time of their discharge assessment from home care. Specifically, when adjusted, blacks were
33% more likely to be dependent compared to whites adjusted: OR1.33 (1.152, 1.544) and
Hispanics were 2.5 times more likely to be dependent when compared to whites, adjusted: OR
2.75 (1.668, 3.975).
Other key findings relative to their impact on ambulation/locomotion included age,
number of comorbidities and the length of hospital stay after the THR (Table 5.8). Although age
groups were statistically significant, they had a weak measurable effect when compared to the
older age group (85 years old or older). Those in the younger age groups (65-74 and 75-84 years
old) were less likely to be dependent: OR 0.459 (0.395,0.534) and 0. 599 (0.514, 0.699)
respectively. Compared to THR patients with twelve or more comorbidities, those with the
lowest number of comorbidities were less likely to be dependent; i.e. OR 0.549 (0.494, 0.610)
for those with 0-4 additional diagnoses. Longer hospital length of stay was associated with an
increased likelihood of dependency. Those who had a post-surgical hospital stay of 3 to 24 days,
were two times more likely to be dependent in ambulation/locomotion in comparison to those
discharged within a maximum of 6 days: OR 2.130 (1.842, 2.463).

112
Table 5.8 Odds Ratios Estimate (Crude and Adjusted) for Ambulation/Locomotion: by Donabedian Structure and Process Variables
Variables Crude Odds Ratio 95% Confidence Limits
Adjusted Odds Ratio 95% Confidence Limits
Relative Importance (amount of weight/variable on Ambulation/Locomotion status)
Race/Ethnicity Reference = White
Black 1.264 (1.099, 1.453) 1.333 (1.152, 1.544) 0.0336 2.04% Hispanic 2.882 (1.908, 4.353) 2.575 (1.668, 3.975) 0.0339 2.06% Other 1.510 (1.183, 1.927) 1.538 (1.193, 1.982) 0.0278 1.69%
Age Groups Reference = 85+
65 – 74 vs 85+ 0.486 (0.421, 0.562) 0.459 (0.395, 0.534) 0% significant: non-measurable effect
75 – 84 vs 85+ 0.628 (0.542, 0.729) 0.599 (0.514, 0.699) 0% significant: non-measurable effect Gender: Reference = Male Female 1.492 (1.400, 1.590) 1.582 (1.481, 1.691) 0.1256 7.64% Residential Location Reference = Urban
Rural Area 1.162 (1.071, 1.260) 1.283 (1.178, 1.398) 0.0511 3.11% Comorbidities (Dx Count) Reference = 12+
0 - 4 0.534 (0.486, 0.594) 0.549 (0.494, 0.610) -0.1384 8.42% 5 -7 0.658 (0.601, 0.720) 0.668 (0.608, 0.735) -0.1045 6.36% 8 – 11 0.775 ( 0.707, 0.849) 0.777 (0.707, 0.855) -0.0625 3.80%

113
Table 5.8 Odds Ratios Estimate ( Crude and Adjusted )for Ambulation/Locomotion: by Donabedian Structure and Process Variables (Continued)
Variables Crude Odds Ratio 95% Confidence Limits
Adjusted Odds Ratio 95% Confidence Limits
Relative Importance (amount of weight/variable on Ambulation/Locomotion status)
Days Acute Hospital Discharge – to H H A Discharge (days) Reference = 1st Quartile 1-15
16 – 30 (2nd Quartile) 0.571 (0.528, 0.618) 0.495 (0.456, 0.537) -0.1724 10.68% 31 – 45 (3rd Quartile) 0.471 (0.432, 0.514) 0.378 (0.345, 0.414) -0.2246 13.67% 46 – 60 ( 4th Quartile) 0.521 (0.471, 0.572) 0.358 (0.324, 0.396) -0.2150 13.09% Physical Therapy Charge Amount Acute Care Hospital Stay ($) Reference = 1st quartile ($0-754)
2nd Quartile $755 – 1179) 0.916 (0.837, 1.002) 0.891 ( 0.811, 0.979) -0.0266 1.61% 3rd Quartile $ 1180 - 1771 0.915 (0.840, 0.997) 0.875 (0.798, 0.959) -0.0329 2.00% 4th Quartile $ 1772 – 15,740 1.030 (0.944, 1.123) 0.902 (0.820, 0.993) -0.0245 1.19% Hospital Length of Stay Reference = 1st Quartile
2nd Quartile 0 – 3 days 1.432 (1.332, 1.540) 1.502 (1.390, 1.623) 0.1121 6.82% 3rd Quartile 0 - 3 days 1.820 (1.642, 2.018) 1.853 (1.657, 2.072) 0.1088 6.62% 4th Quartile 3 – 24 days 2.130 ( 1.868, 2.429) 2.130 (1.842, 2.463) 0.0968 5.89% Socioeconomic Status Reference =Medicare only
Dual Status (Medicare & Medicaid)
1.820 (1.540, 2.151) 1.171 (0.828, 1.656)* 0.0145 0.883%
Cost Share Group (Low Income Subsidy)
1.743 (1.504, 2.020 1.417 (1.043, 1.923) 0.0364 2.21%
* = Not Significant ** = Negative Standardized Estimate (negative effect)

114
5.6 Impact of Independent Variables on Process
A linear regression analysis was performed to determine the impact of structural variables
(i.e. race, gender socioeconomic status) on process variables: PT charge amount (Table 5.9),
hospital amount, the length of acute hospital stays (Table 5.10) and the number of days between
hospital and home health care discharges (Table 5.11) as dependent variables. The standardized
estimate (standardized betas) identified two independent variables, age and health status, to have
the highest relative importance of the variables examined. More comorbidities (the sicker) and
older beneficiaries were associated with longer acute hospital stays, greater amounts charged for
physical therapy, and more days of home health care services.. Age and the number of
comorbidities accounted for 18 to 20 and 16 percent respectively of the physical therapy charge
amount and the duration of home health care services within one episode of care (Tables 5.9 and
5.11). Race/ethnicity, socioeconomic status and gender each accounted for less than 10 percent
of the effect on the physical therapy charge amount (Table 5.9). Comorbidities were responsible
for 50 percent and age for 19 percent for the effect on hospital length of stay. Both
race/ethnicity and socioeconomic status variables each accounted for less than 10 percent of the
observed impact on the hospital length of stays (Table 5.10). Comorbidities and gender (female)
each accounted for 16 percent of the observed effect on the number of days beneficiaries were in
receipt of home health care services. However, age had the greatest impact (20%) as an
independent variable; it was the key factor that accounted for longer time spent with home health
care. (Table 5.11)

115
Table 5.9 Impact of Independent Structure Variables on Physical Therapy Charge Amount Process Dependent Variable
Variable Regression Coefficient P- Value Relative Importance Race: Reference (White) Black/African American -112.78030 0.0006 -0.02343 (8 %) Hispanic 184.91952 0.0855 0.01178 (4 %) Other 76.73917 0.1949 0.00881 (3.%) Age (No Reference) 8.80304 <.0001 0.04950 (18.%) Gender: Reference (Male) Female 32.80819 0.0187 0.01597 (5.%) Geographic Location: Reference (Urban)
Rural -274.86195 <.0001 -0.10004 (36.%) Comorbidity Count (No reference) 11.20715 <.0001 0.04460 (16.%) Socioeconomic Status Dual Status: Full or Restricted 114.61237 0.1588 0.01868 (6.%) Cost Share Group: full Dual or Low Income subsidy
7.36602 0.9176 0.00137 (4.%)

116
Table 5.10 Impact of Independent Structure Variables on Length of Hospital Stay Process Dependent Variable
Variable Regression Coefficient p-value Relative Importance Race: Reference (White) Black/African American 2.38117 <.0001 0.04683 (8.96%) Hispanic 4.43093 <.0001 0.02672 (5.12%) Other 0.45790 <.0001 0.00497 (0.95%) Age (No Reference) 0.19930 <.0001 0.10609 (20.31%) Gender: Reference (Male) Female 1.82191 <.0001 0.08393 (16.07%) Geographic Location: Reference (Urban)
Rural 2.34243 <.0001 0.08070 (15.45%) Comorbidity Count (No reference) 0.21779 <.0001 0.08204 (15.70%) Socioeconomic Status Dual Status: Full or Restricted 1.31899 0.1191 0.02035 (3.89%)
Cost Share Group: full Dual or Low Income subsidy
4.00795 <.0001 0.07060 (13.51%)

117
Table 5.11 Impact of Independent Structure Variables on Length of Home Health Care Process Dependent Variable ****
****Length
of home health care process equals the number of days from hospital discharge to discharge from home health care.
Variable Regression Coefficient p-value Relative Importance Race: Reference (White) Black/African American 2.38117 <.0001 0.04683 (8.96%) Hispanic 4.43093 <.0001 0.02672 (5.12%) Other 0.45790 <.0001 0.00497 (0.95%) Age (No Reference) 0.19930 <.0001 0.10609 (20.31%) Gender: Reference (Male) Female 1.82191 <.0001 0.08393 (16.07%) Geographic Location: Reference (Urban)
Rural 2.34243 <.0001 0.08070 (15.45%) Comorbidity Count (No reference) 0.21779 <.0001 0.08204 (15.70%) Socioeconomic Status Dual Status: Full or Restricted 1.31899 0.1191 0.02035 (3.89%)
Cost Share Group: full Dual or Low Income subsidy
4.00795 <.0001 0.07060 (13.51%)

118
5.7 Summary
Race and ethnicity influence the functional outcomes (transfer and ambulation) of individuals
who have had a THR. However, the processes of care (length of hospital stays, number of
comorbidities, and charge amount for PT services during the acute hospital stay) are also
impacted by structural variables. Those with the greatest impact on processes examined were not
found to be race or ethnicity, but rather older age and poorer health. Thus, both structure and
process variables are associated with differences seen in the post-surgical outcomes analyzed in
this representative study sample.

119
Chapter 6 Discussion and Conclusion Introduction
Racial/ethnic disparities in health and health care have long been experienced by minority
patients. Documentation throughout history has shown that minority populations have had
disparate access to medical healthcare when compared to non-minority populations. These
differences have been highlighted from biblical times, and in the US, throughout the ante-bellum
and post-bellum periods, the civil rights movement of the 1960s, and they remain prevalent in
this first quarter of the twenty-first century. The consequences and ramification of persistent
disparities in health and health care are seen in the overall poorer health status of minority groups
in comparison to non-minority groups. Minority groups have been found to have higher
incidences of most leading causes of death and chronic illness such as cardiovascular disease,
diabetes, cancer and infant mortality rates. Poor minority health status has been attributed to
various causes over time, including inherent genetic inferiority, iatrophobia, and a wide array of
social determinants such as poor education, poor healthcare literacy, poverty/SES, racism and
implicit provider bias.
The purpose of this study was to address the paucity of empirical studies examining the
impact of patient race/ethnicity on physical therapy outcomes, particularly on post-surgical
functional outcomes of individuals who had a hip replacement and had been discharged to
physical therapy rehabilitation associated with a home care agency. This study differs from
previous ones in its focus on functional rather than surgical outcomes or medical issues related to
this surgical procedure. Specifically, this research was conducted to examine whether there are
similar functional outcomes across racial/ethnic CMS beneficiary groups that undergo a common
elective surgical orthopedic procedure (THR) and receive post-acute care physical rehabilitation
through a Medicare-certified home health care agency. The concise answer was found to be:

120
”No, the differences are NOT similar across groups. Differences in functional outcomes as
measured by the transfer and ambulation/locomotion abilities were observed in the comparison
of minority and non-minority groups. More specifically a difference was found between black
and white patients after controlling for potentially confounding factors such as comorbidities,
age, gender and/or SES. Racial/ethnic difference were most clearly seen when examining the
impact of specific independent variables on functional ambulation/locomotion abilities. Few
disparities were seen in the impact of structural variables on the independent transfer outcome
variable.
6.1 Discussion of Results
The data used for the statistical analysis was CMS administrative claims (MedPAR,
MBSF & HHA) and assessment (OASIS) files of Medicare beneficiaries who received a THR in
the 2012 calendar year. The aim was to examine if racial/ethnic disparities documented in other
healthcare delivery and health status studies held true for this component of physical
rehabilitation.
The descriptive characteristics of this study sample was similar to that in other research
analyses such as that of Irgit & Nelson (2011). In particular, the study sample was
predominantly white (93%). The remaining 7% included all other racial and ethnic groups as
identified in the CMS files utilized: white, black, Hispanic, Asian, North American Native and
other. The largest component of the minority sample was composed of blacks (4.71%). The
THR procedure was also found to be more prevalent in women than men; this is consistent with
the results of others such as Hootman, (2016), Kremers et al., (2015) and Learmonth et al.,
(2007). However, in this study, the primary focus on functional outcomes, as opposed to the

121
post-operative surgical outcomes more commonly discussed in the literature, women were also
found to be more dependent regarding ambulation (28.17%) when compared to men (20.82%).
The bivariate analysis examined the relationship between each structural variable and the
outcomes of interest (transfer and ambulation/locomotion ability). Four independent variables
(i.e., structural and process variables, the latter used as independent variables) were significant
predictors of the patient's transfer ability within the maximum 60 days with home care services:
Hispanic ethnicity OR = 8.9; the length of HHC services for those in the 2nd and 3rd quartiles, OR
.516 and.412 respectively; PT charge amount to those in the 4th quartile for acute hospital care,
OR, 2.94 and length of hospital stay for those in the 3rd and 4th quartiles OR, 4.2 and 3.9
respectively. Not found to be significant predictors of transfer ability were the patients’ gender,
urban or rural residency, and number of comorbidities. Due to small sample size in the several
levels of transfer dependency, the relationship between the independent variables (structural and
process variables when both used as independent variables) and transfer functional outcomes was
examined by collapsing the five levels into two: independent and minimal dependence vs
moderate to total dependence. Ninety nine percent of the study sample was identified as
independent in their transfer abilities.
A similar analysis of the relationship between a patient’s ambulation/locomotion ability
found that all variables were statistically significant predictors of the level of the patient’s
functional dependency (ie independent defined as independent and requires minimal assistance
or dependent defined as moderate assistance to totally dependent). Examples of these
relationships as seen in Table 5.8 include race/ethnicity (OR,1.2 – 2.8), and hospital length of
stay (OR, 1.4 – 2.1)

122
As previously noted all three process variables (length of hospital stay, the PT charge
amount and the duration of home health care as measured by the number of days from hospital
discharge to HHA discharge) were found to be positive predictors of dependency for each of the
outcomes: transfer, OR, and ambulation/locomotion abilities; (Tables 5.5., 5.8). However,
except for the length of the hospital stay, the adjusted odds ratio (multivariate analysis) indicates
that the process variables are of minimal relative importance in predicting the level of
dependency for ambulation /locomotion ability. The length of hospital stay accounted for 6 to
7% of relative importance associated with the level of dependence in ambulation and clinically
supports the need for a longer hospital stay due to poorer performance with ambulatory mobility.
Age and the number of comorbidities were predictors of the two primary outcomes of
interest: transfers and ambulation/locomotion. Age had a relative importance of 18-20% related
to predicting each of the three process variables. The number of comorbidities had 16% relative
importance as a predictor of PT charges and the number of days spent in one 60-day episode of
home health care and a 50% impact on the length of hospital stay. As such the older and the
graver the patient’s state of health, the longer the hospital stay, the greater the charges for PT
rehabilitation and the more days of home health care services utilized (Tables 5.9-5.11), the
lower the patient’s transfer/ambulation ability.
In a secondary analysis examining the effect of the structural independent variables on
processes (length of hospital stay, charge amount for physical therapy, and the number of days
from hospital discharge to home health care discharge when these were defined as dependent
variables), race/ethnicity and socioeconomic status had a minimal impact on the cost of PT
services provided, and the durations of the hospital stay or length of home care services.
Minority status appears to be associated with lower expenditure on those services. The one

123
exception was for beneficiaries with dual Medicare/Medicaid status or those who received a low-
income subsidy and had higher utilization of home health rehabilitation services. Poor
preoperative function due to delaying a needed THR and delaying the procedure due to fear have
been reported as plausible reasons that minorities and individuals with low socioeconomic status
mayneed more intensive post-operative care (Lavernia et al. ,2004) (Lavernia et al., 2010). The
consequence of deferred surgical intervention suggests that non-white patients may be more
seriously or chronically ill when care is accessed to address their impairment (Brega et al, 2005).
As such, recovery and functional outcomes may be worse than the average results.
The bulk of published research on racial/ethnic differences does not address patients’
functional abilities. Instead, it tends to address disparities regarding medical and surgical
outcomes. Examples of the latter include, but are not limited to, nonwhites compared to whites
having a the lower prevalence of surgical intervention despite a diagnostic need (Steel et al.,
2008); a greater likeliness of being discharged to a non-home facility after surgery (Keswani et
al., 2016) (Inneh, 2016); and a higher 90-day readmission rate after surgery (Clair et al., 2016).
The clinical characteristics of minority groups, such as greater disease severity, more
comorbidities, poorer socio-economic characteristics and patient expectations, have found to be
associated with a lower rate of undergoing this surgical procedure (Groeneveld et al., 2008). In
an eighteen-year, national longitudinal study of total joint replacement among CMS
beneficiaries, Singh and colleagues (2013) found a persistent disparity in arthroplasty usage and
poorer post-operative outcomes. Although there was no difference in post-operative mortality,
Singh found that when compared to Caucasians, African-Americans had inferior outcomes such
as longer hospital stays, higher rates of readmission, lower likelihood of being discharged home
(than to rehabilitation facilities). This dissertation only analyzed beneficiaries who were

124
discharged home with home care and did not assess readmission rates. However, the median
length of hospital stay was 3 days across all racial/ethnic groups studied.
Less common in the literature, although the focus of this study, was the impact of
race/ethnicity on the functional outcomes. However, Brega et al (2005) examined racial/ethnic
disparities in the functional outcomes using OASIS records of a national representative sample
of 105, 160 elderly home health care recipients in the calendar year 2001. Their results found
non - Hispanic whites experienced substantially better functional outcomes than did home health
care recipients of other racial/ethnic backgrounds and the disparity was most pronounced
between non-Hispanic whites and African Americans/blacks. Similar results were found in this
dissertation study, where race/ethnicity was the one factor that was consistently found to have a
statistically significant impact on functional ADL outcomes as measured by the transfer and
ambulation ability (and to a more limited degree, transfer ability when analyzed in two levels of
function – independent versus other levels) at the end of one episode of HHC. Approximately
one and a half percent (1.46%) of the minority group (black, Hispanic and other) were found to
be dependent in transfer abilities compared to approximately a third of one percent of whites
(0.38%).
To determine if homogeneity of the two level transfer analyses was masking differences,
the transfer outcome variable was reexamined using a three-level multinominal approach. Now
Blacks were found to be 1.4 times more likely to be minimally to totally dependent when
compared to whites who were independent. They were only 0.72 times as likely to be
independent when compared to minimally dependent whites' transfer ability. Hispanics were
also found to be more dependent when comparing their transfer ability to that of whites.

125
However, the wide confidence intervals suggest an unstable estimate, likely due to the small
sample size (N= 91).
For the ambulation outcome, when all the variables were considered in the multivariate
analyses, compared to whites, minority groups were 1.3 to 2.6 times more likely, to be
moderately to totally dependent with functional ability meaning the need to use a two-handed
device such as a walker to being bedfast, unable to ambulate or be upright in a chair.
It is expected for individuals to have different rates of recovery related to some structural
or process variables. For instance, due to age and the overall developmental changes that occur
across the lifespan, older patients may fare worse than younger ones; it is also expected that the
less healthy one is, the slower one's recovery may be due to the additional stress that post-
surgical recovery may place on the body systems. It has also been found that when blacks and
whites live under similar socioeconomic, social and environmental conditions, “the racial
disparity we normally see in national samples was attenuated or completely erased” (LaVeist et
al 2011). However, Pollack et al. (2013) found that when net worth – the sum of all assets minus
the sum of debts--is examined in relation to self-rated health, older and younger blacks and
whites as well as older Hispanics in the lowest quartile of wealth were found to have 3-5 times
higher odds of self-reporting as being in fair to poor rather than good health.
Race and/or ethnicity are social constructs, and "race" is in large part a social rather than
a biological category” (Cooper et al,, 2003) (Williams & Sternthal, 2010). Although they may
exist, differences in functional outcomes should not be expected based on racial or ethnic
classification, but rather examined as an expression of the social root causes of variations that are
found in humanity.

126
6.2 Results and the Socioecological Model (SEM)
The socioecological model was the theoretical framework used for this study. This
model proposes consideration of the research question – are there racial /ethnic differences in
functional outcomes--from some of the five interactive components of SEM. The CMS data set
that was utilized provides the opportunity to assess the impact of various SEM levels on
functional outcomes. However, as noted in each section below, some important variables were
not available in the CMS data set.
6.2.1 The Individual/Intrapersonal
The individual is at the core of the SEM. The structural variables included in the study
analysis are: racial/ethnic identity, age, gender, socioeconomic status, number of comorbidities
and the patient’s residential location (rural or urban). These variables were examined to
determine if they had a differential effect on study outcomes. The literature indicates that there
is a greater prevalence of arthritis and functional limitation of older minority groups in black and
Hispanic minority groups compared to whites (Steele et al., 2008). However, despite a need for
joint replacement in this group due to the greater functional limitations caused by arthritis, these
minority groups are less likely to receive this surgical procedure (ibid).
Some key factors that would have been of value for a more patient-centered analysis of
outcomes at this level of the SEM were either not part of the data files or not in the information
collected during the OASIS assessment: i.e. patient’s prior ambulatory status and patient’s post-
operative expectations. Data that captured the latter would have afforded a more patient-
centered assessment by comparing concordance between the patient’s functional expectations
prior to surgery and their clinical functional outcomes reported in OASIS at the point of
discharge from home health care services. Simply put, there would have been data regarding

127
whether the attained functional abilities were at, below, or above the patient's expectations- a
measure of patient satisfaction.
6.2.2 The Interpersonal SEM Level
This level of the SEM addresses the formal and informal social support systems available
to the individual that can potentially influence the individual's outcomes. Although 20 of the
nearly 600 OASIS variables (N=592) address this aspect of the model, many other variables
(specifically M0340- M0350) were generally missing from the OASIS files in this dataset.
Consequently, there was no information regarding whether the individuals in the study sample
lived alone, with family members or others, or received some form of primary care assistance.
6. 2.3 The Community SEM Level
Other than data indicating whether individuals in the sample study resided in a rural or
urban geographic location, information that addressed regulation of social institutions or
organizations was not available for, nor a focal point of, this study. However, although not
measurable in the context of this study, it is acknowledged that the resources (i.e., the number of
PTs) of the home health care agency within the patient's community will impact HHA
efficiency, which will in turn have a direct effect on the study sample’s functional outcomes.
6.2.4 Organizational/Institutional SEM Level
The institutional rules and regulations may impact the number and strategic locations of
community home health care agencies, which ultimately may impact patient coverage; however,
the operation of the community’s home health agencies is governed at the outer ring of the SEM,
the social/political level. At the institutional level of this research, as illustrated in Figure 2.1,
are the ramifications and long-term impacts of historical, social and psychological conditions
such as slavery, implicit bias, and an underrepresented minority health care workforce. Although

128
presented in the literature review (Chapter 2), they were beyond the scope of this study but are a
focal point for some policy recommendations discussed at the end of this chapter.
6.2.5 Structural /Laws, Policy Level
This final level of the SEM considers the laws and policies across all governmental
levels. These are the strutures Medicare, Medicaid and other polies The dataset used for this
research includes the process variables, such as the number of days spent in acute hospital care,
the monetary charges for physical therapy services during hospitalization and the number of days
spent in post-acute physical therapy through a home health agency. All are factors examined in
this study that fall under this level of the SEM. They are assessed relative to the influence they
have on the two functional outcomes of the study sample.
6.3 Strengths and Limitations
This was a retrospective cohort research study to investigate functional outcome
differences among a sample of Medicare beneficiaries who had a primary THR in the 11 selected
states. My study targeted Medicare beneficiaries age 65 and older.The initial dataset likely
included most patients who had a THR during the 2012 calendar year, as more than 98 percent of
adults of this age range are enrolled in Medicare (ResDAC, 2012). Therefore, use of CMS
administrative claims and assessment data provided access to a large pool of beneficiaries (N =
21,448) for analysis that captured a close approximation of the universe of US citizens over the
age of 65 receiving a total hip replacement in 2012.
6.3.1 Strengths
The data file for this dissertation include pertinent information regarding any CMS-
covered service that the beneficiary used: admission and discharge dates from hospital and home
health care, diagnoses, source of care and procedure codes. In addition, demographic data (i.e.

129
gender, date of birth, race/ethnicity) was also included. Although not used in this study, CMS
administrative files can be linked to other external files (e.g., US Census, Surveys, cancer
registries etc.). Outcome variables were obtained from the linked OASIS file. Although the
OASIS assessment tool was not developed as a comprehensive assessment instrument, it was
intended as a basic set of patient outcome measures that were considered essential for assessment
of the beneficiaries’ health and changes overtime. As such, it is a standardized matrix by which
to compare individuals who receive home health care following post-acute discharge (Goldberg
et al. 2011). Additionally, this assessment tool is both valid and reliable. Variables such as
ambulation and transfers, “generally had higher validity compared to the ‘gold standards’ or
expert opinion”…and that “accuracy seemed to be better for discharge compared to admission”
(O’Connor and Davitt, 2012 pg 295)
6.3.2 Limitations
This study was, cross-sectional, a “snapshot” at one point in time during the 2012
calendar. Therefore, the opportunity to take note of trending changes over any period was not
available. The focus of the study was on those discharged to home health care for the immediate
post-acute physical rehabilitation. Therefore, the functional outcomes of 57 percent of the study
universe who were discharged home or to other faculties such as skilled nursing or in-patient
rehabilitation facilities were not captured by this study. In addition, analyses were conducted on
home health care results that occurred within one episode of care (60 days). Consequently, it is
not known if there racial/ethnic differences found in functional outcomes for patients of HHC is
consistent with Medicare beneficiaries who received post-operative rehabilitation in other
facilities (i.e SNF, IRF). Also, although there are Medicare beneficiaries who are less than 65
years old, who have had THRs, it was decided to include only those who were Medicare patients

130
equal to or greater than 65 years to standardize the age for subjects in this study. Consequently,
any racial/ethnic differences in younger Medicare beneficiaries with a primary THR were not
evaluated.
The CMS data used in this study did not include the information needed to assess patient
social and instrumental support (i.e. living arrangements and/or the informal assistance of family
members, friends who could help the patient as needed once discharged home). However,
clinical experience suggests that individuals of low socioeconomic status may be less likely to
have the necessary support to get to an out-patient clinic for PT services because other household
member are working or otherwise not available to assist the patient in getting to appointments
that are typically during regular business hours. There may also be limited outpatient physical
therapy facilities within poor neighborhoods. To compensate for this limited access, the PT may
extend home care so that the patient receives the physical therapy necessary. Unfortunately, the
impact of social support could not be assessed in this study
A limitation that may have impacted my research is the exclusion of variables due to
excessive missing data in certain variables that would have been useful for the analysis. To
prevent unreliable data, these variables, while useful for the understanding of the outcomes, were
not included in this analysis. Some of the social variables originally intended to be included to
characterize social support (i.e. lives alone, with attendant, conditions of housing etc.) or pre-
operative status (at risk for falls or prior ambulatory status) were missing from all or the greater
majority of the study sample. In addition, as the analysis relied on CMS administrative data,
patient satisfaction was not captured. This study also relied upon proxies for SES (i.e. dual
Medicare/Medicaid enrollment) as opposed to more traditional measure such as educational and
income levels. Having some of this information would have provided a more holistic or

131
ecological appreciation of the study sample's characteristics, critical to the core-intrapersonal
level of the SEM as well as the interpersonal level in terms of social support.
Limitations were also found regarding the sensitivity of the OASIS measures used to
describe functional ability. Unlike continuous variables such as “distance walked”, the OASIS
five transfer and six ambulatory categories are subjectively rated and less precise than
continuous measures. of functional performance.
Information regarding the racial/ethnic identity of the healthcare provider was also not
available in this data set. Therefore this study was unable to confirm or refute other research
(Poma,2017) (Sweeney, 2016) (Sullivan, 2004) (LaViest, 2002) that have addressed the impact
concordance or non-concordance between patients and their health care providers may have
processes and outcomes of care.
Finally, the study sample was a cohort of CMS beneficiaries who lived in the 11
designated states (CA, FL, GA, IL, MI, NC, NY, OH, PA, TX, VA), not randomly selected from
the national study population Thus the research cannot be generalized to the entire population of
individuals with total hip replacements.
6.4 Summary conclusions, and implications: Law and Public Policy Implications
Race/ethnicity was a predictor of greater functional dependency for the two primary
outcomes examined in this study of Medicare beneficiaries discharged home with home health
care following a THR in 2012. The observed differences persisted in both multivariate and
multinomial regression analyses when other factors were controlled (i.e. age, socioeconomic
status, rural or urban residence etc.). The Medicare study sample consisted of those who had
undergone this surgical intervention for the relief of pain and the expectation of improved
function. Given this common indication for THR shared by the study sample, and yet

132
inequitable functional outcomes, the question is: What should be done to facilitate more
equitable outcomes across racial/ethnic groups? Consideration of the country’s rapidly changing
demographics and arguments for social justice further complicates the matter.. There are several
plausible and integrated approaches to address this consistently recurring issue of disparities in
healthcare and minority health status.
6.4.1 Acknowledging the “Elephant in the Room”
Ample research data have been noted over the last several decades that racial/ethnic
disparities are a compelling issue of health care that needs to be addressed. Acknowledgement
of this as an issue and addressing the root causes of those differences is a huge step in a positive
direction in terms of eliminating racial/ethnic disparities due to race-related social biases.
6.4.2 Self-awareness: Implicit Provider Bias
Several studies of implicit bias of medical doctors (MD) have found that on average,
physicians hold an implicit “pro-white/anti-black patient bias” and this preference affects the
care provided to their patients. A study by Green et al. (2007), examined racial/ethnic bias of
physicians based on their medical decisions made after reading a vignette of a randomly assigned
black or white patient presenting with symptoms of an acute coronary syndrome to the
emergency department. Although physicians reported no explicit preference of black versus
white patients, nor difference in perceived cooperativeness in their questionnaire responses, the
results of their Implicit Association Tests (IAT) indicated preference for white in contrast to
black patients. As the physicians’ implicit preference scores for whites increased, so did their
likelihood to treat the white patient with the more appropriate anti-blood clotting medication
(thrombolysis) with less appropriate use of the same medication for the black patient.

133
Based on IAT tests, MDs reveal a strong implicit racial preference for white Americans
over black Americans among all test takers. When stratified by MD race and ethnicity, implicit
preference for white Americans was strong among all MD groups except for African American
MDs. White MDs showed the strongest implicit preference for whites, while African American
MDs, on average, did not show an implicit preference for either (Sabin et al., 2009)). When
measuring the implicit racial bias of physicians and their general perceptions of their patients
based on race, physicians reported less affiliative feeling toward black patients and rated them as
less intelligent than their white counterparts (Burke & van Ryn, 2000). When measuring the
perception of care among black patients, clinicians with higher pro-white IAT scores were
ranked lower by black patients on quality of care (Blair et al., 2013). Physicians with a pro-white
IAT score also generally believe that black patients do not adhere to medical recommendations,
which in turn skews their delivery of medical advice (Cooper et al., 2012). Acknowledgment
and realization of these unintentional biases is critically important in the improvement of patient
provider communication and ultimately the most equitable patient care.
The focus of much of the implicit bias research addresses physicians; however, in a
systematic review of the literature, Hall et al. (2015) examined implicit bias of healthcare
professionals and examined the impact of their implicit attitudes about racial/ethnic groups on
healthcare outcomes. In addition to medical doctors of various sub-specialties, medical students
as well as students in nursing and pharmacy were also included. The results indicate that of the
fifteen studies included in the review, fourteen found low to moderate levels of implicit bias
among health professionals that had a negative impact on patients of color. In general, physical
therapists, and especially those who provide physical rehabilitation in the home of their patients
work closely in a unique environment in an effort to assist them attain optimal function.

134
However, as implicit biases are attitudes beyond conscious awareness and not typically in
synchrony with explicit behavior, it is important that healthcare providers be aware of the
potential negative effect these attitudes can have (i.e. prejudiced behaviors) which typically
surface when very busy, or under pressure or are fatigued. Such attitudes are clearly
counterintuitive to the intent of physical rehabilitation. Thus, self-awareness and substantive
change is critical to address the matter and provide equitable patient-centered care.
6.4.3 Patient-Centered Care
Patient-centered care “is care that is respectful of and responsive to individual patient
preferences, needs, and values, and ensuring that patient values guide all clinical decisions”
(IOM, 2001) and is fundamental to assuring that not only the desired, but correct care, is
provided to individual (Epstein et al., 2010). Therapeutic alliance (or simply alliance) is an
important component of patient-centered care. Positive therapeutic alliance between the health
provider and patient has been found to be associated with the patients’ compliance with
treatment and positive outcomes, such as improved pain and treatment satisfaction (Hall et al.
2010) (Ferreira et al. 2013) (Fuentes et al., 2014) (O’Keeffe, et al. 2016). This format of medical
care fosters a collaborative patient-to-healthcare-provider relationship that affords a more
tailored, rather than purely generic diagnosis-based, care. Successful delivery of healthcare
under this format demands a culturally competent healthcare provider who fulfills his or her
professional duty to care for patients regardless of the patients' health status or response to
treatment (Epstein, 2010). Overall, patient-centered care has been found to promote self-
efficacy due to reducing anxiety and indirectly building trust and social support and overall well-
being empowered by effective professional patient/provider relationship.

135
As presented by Jette, (2017) in a recent editorial, the Baby Boomer generation is
projected to be approximately 20 percent of the United States population by 2030. This
inevitable demographic change suggests that we not only deliver patient-centered care, but that
we also consider a paradigm shift to also consider family-centered health care. As Jette notes,
the care of those 65 and older largely relied on families to shoulder the majority of the long-term
services and support (LTSS). This will continue to be the pattern of care, although the LTSS
system is complicated by shorter hospital stays causing elderly hospitalized family members to
return home needing more complex care. However, families are now smaller and the home now
has less supportive infrastructure to provide the more intensive care.
The findings of this dissertation indicated that minority groups were 1.3 to 2.5 times more
likely to be dependent than their white counterparts in their ambulation and, depending upon
living arrangements, would likely require some initial family support or assistance upon
returning home post-surgically. The transition to family-centered care will involve training that
will help health and rehabilitation care providers to better recognize and engage family
caregivers. Jette identifies the building of a workforce with competencies to accommodate this
shift from person- to family-centered care. One of the five key factors noted for the success of
this transition will be making cultural competence a care aspect of provider competencies in
working with family caregivers (Ibid).
Consideration of patient/family centered care is a central component of the Patient -
Centered Outcomes Research Institute (PCORI) that was introduced as an element of the US
Patient Protection and Affordable Care Act of 2010. The prime intent of PCORI is to expand the
focus of patient-centered health care to be inclusive of the results from healthcare research.
PCORI seeks to take advantage of the unique perspective of patients in an effort to improve

136
clinical research questions beyond that of the research and/or medical and scientific realms by
including the vantage point of those who are ultimately most impacted by the medical and
technological advances and interventions that stem from research – the patient, who is in the end-
, the key stakeholder. As summated by Frank et al. (2014, pg 1514) “Patient-centered outcomes
research is poised to substantially change how clinical questions are asked, how answers are
pursued, and how those answers are used”.
6.4.4 Cultural Competence
The Health Policy Institute (2004) succinctly defines cultural competence as the ability of
providers and organizations to effectively deliver healthcare that meets the social, cultural and
linguistic needs of patients. Throughout the literature this attribute is discussed as an on-going
journey rather than a finite destination. Development and refinement of the skills that yield the
ideal clinician-patient relationship requires the integration of a wide range of knowledge,
attitudes and eventual skill (Betancourt et al., 2003). The goal of cultural competency is to
create a healthcare system and workforce capable of delivering the highest quality care to every
patient regardless of race, ethnicity, and culture of language proficiency (Betancourt, 2005).
Several factors result in a culturally competent healthcare environment, including a certain level
of political correctness by not using inappropriate terms that are potentially offensive; visual
affirmation in the healthcare setting with artwork and literature that is reflective of other cultures
and not just those of the mainstream population. This simple gesture affirms a conception of a
value for the person not just as a patient or consumer of the healthcare services, but as a person
inclusive of their culture (Rose, 2013)
Eliminating or minimizing communication barriers is another key component of cultural
competency. In 2000 the national standards of culturally and linguistically appropriate services

137
(CLAS) were adopted by the Department of Health and Human Services. Fourteen standards
were developed to eliminate racial and ethnic disparities by promoting more effective
communication and in so doing also improve the quality of care for the entire nation. The
specific purposes of the CLAS standards “are to address the inequities that exist in the provision
of health care and to make services more responsive to the individual needs, on a cultural and
linguistic basis, of patients/consumers/clients served” (Rose, 2013 pg. 170). The standards are
organized within three categories: culturally competent care (1-3); language access services (4-7)
and organizational supports for cultural competence (8-14). Four of the standards (4-7) that
focus on “Language Access Services” are mandatory and required of all federal funded
recipients. The remaining ten standards are defined as guidelines or recommendations (Chun,
2009).
As summarized by Rose (ibid) the two overarching features of CLAS are to:
Provide a common understanding and consistent definitions of culturally and
linguistically appropriate services in health care
Offer a practical framework for the implementation of services and organizational
structures that can help healthcare organizations and providers be responsive to
the cultural and linguistic issues presented by diverse populations
The means for implementing the standards in CLAS vary greatly among healthcare
professional organizations and accrediting bodies. Standardized measurement tools and
guidelines for the implementation strategies that best meet the needs of all people was lacking.
Thus in 2013 the Office of Minority Health (OMH) under the auspices of the federal department
of Health and Human Services released the “National Standards for Culturally and Linguistically
Appropriate Services (CLAS) in Health and Health Care. This enhanced version of the 2000

138
CLAS standards includes broader definitions of culture beyond race and ethnicity and expands
health to include mental as well as physical health. A 2014 addition to the 2013 version of
CLAS provides the overarching principal standard, which succinctly states the primary goal of
the rest of the document: “Provide effective, equitable, understandable, and respectful quality
care and services that are responsive to diverse cultural health beliefs and practices, preferred
languages, health literacy, and other communication needs.” The remaining fourteen standards
are subdivided among three categories: Governance, Leadership and Workforce; Communication
and Language Assistance; and Engagement, Continuous Improvement and Accountability (Koh
et al., 2014).
The rapidly changing demographic in our country arguably makes cultural competency
more important than ever. The U.S. Census Bureau estimates that by the year 2050, over half of
the population will comprise a diverse mix of ethnic and racial groups. This means the issue of
cultural competence will require continued vigilance to attain the overarching goal of health
equity across the myriad of diverse racial/ethnic groups that will be represented throughout the
country; and a critical component of cultural competency is diversity.
6.4.5 Diversification of the Workforce
Increasing the diversification of the healthcare workforce has been identified as a means
of closing the health disparities gap (Sullivan, 2004). Racial/ethnic diversity of health
professionals has also been associated with improved access to and quality of healthcare in
underserved and increasingly diverse groups of the population (Grumback, 2008) (USHHS,
2006).
6.4.5.1 The Health Workforce Data

139
A recent update regarding the diversity of the health workforce (Snyder et al., 2016),
based on an annual nationally representative household survey, was conducted by the US Census
Bureau. It was based on a comparative analysis of data between 2004 and 2013 and focused on
41 selected occupations listed in the 2000 Standard Occupational Classifications System. The
results indicated that the 2013 health workforce had greater racial diversity than the US
population. Among the non-Hispanic group, the health workforce had a greater percentage of
African Americans (18.2%) and Asian/Pacific Islanders (8.1%) but a lower percentage of Whites
(70.9%) when compared to the US population: 14.9%, 6.2% and 75.3% respectively. However,
in 2013, there was considerably less of the Hispanic group in the 2013 health workforce
compared to their its representation in the US population (10.9 vs 17.1%).
Although the physician workforce saw minimal advances in diversity, there was a notable
increase in the diversity of the overall health workforce between 2004 and 2013 compared to the
0.8% increase for other racial/ethnic groups (African Americans 1.3%; Hispanic group 2.4 %).
Thus, the trend is on an upward trajectory, with the five most racially diverse occupations being:
nursing, psychiatric and home health aides; personal & home care; health
technologist/technicians; licensed practical nurses and licensed vocational nurses; and social
workers. People who identified as Hispanic were found most prevalent in the following five
occupations: dental assistants; medical assistants and other support occupations; personal and
home care aides; medical, dental and ophthalmic laboratory technician; and opticians,
dispensing. The physician and surgeon workforce in 2013 was composed of 70.6% white/non-
Hispanic, 10% Hispanic, 5.8% African American and 0.1% American Indian/Alaskan Native
(Snyder et al., 2016).
6.4.5.2 Benefits of Workforce Diversity

140
As discussed by Ayanian (2007), there are several ways in which a more diverse
healthcare workforce can help to decrease disparities. It is likely that healthcare professionals of
minority groups have either personally experienced healthcare disparities or done so vicariously
through a family member or friends. Such an experience can imprint a lasting effect that
motivates the professional to address disparities within their organization. Secondly, by sharing
their insights about how racial and ethnic disparities can arise with colleagues of non-minority or
international origins, they can work together to facilitate more equitable care. Finally, a more
diverse workforce can afford minority patients the opportunity to be treated by a clinician of the
same racial or ethnic group if it is preferred because of common culture or language. As
discussed, racial/ethnic concordance between patients and their healthcare provider has been
associated with greater patient centered care and satisfaction. Unfortunately given the lack of
racial/ethnic identification of the health care team in this study, this relationship was not able to
be examined.
6.5 Title VII, Part B of the Public Health Service Act Programs and Others
When searching for ways to increase the number of underrepresented minority (URM) groups
in the healthcare workforce, the lack of diversity in healthcare educational institutions must be
addressed. Healthcare pipeline programs focusing on the high-school-to-college
transition among minority students attempt to facilitate academic and professional interest in the
health sciences (Patterson & Carline, 2006). These programs expose students to the sciences and
work to cultivate a strong interest in science and research as a necessary foundation for pursuing
post-secondary education in healthcare. Pipeline programs enhance opportunities for racial and
ethnic minority and disadvantaged students to gain a better understanding of options in
healthcare beyond medicine, nursing, and dentistry (USDHHS, 2009).

141
Several Health Resource and Services Administration (HRSA) programs support
diversity of the health workforce through concentration on professional health training under the
guidelines of Title VII, part B or the PHS Act. The common denominator of these programs (i.e.
Centers of Excellence, Scholarships for Disadvantaged Students, Health Careers Opportunity
Program and the Faculty Loan Repayment Program) is to attract prospective students into fields
of medicine and health care with the goal of growing the URM workforce to a level
representative of those racial/ethnic groups’ existence within the national population. These
programs seek to recruit and retain URMs via targeted recruitment, mentoring, financial
assistance, and career development curricula.
6.5.1 Primary and Secondary Education
At the community level, programs at primary, secondary and post-secondary academic
levels seek to introduce young people to healthcare and provide a deeper exploration of more
than the commonly known fields of medicine. Fourth grade students at a private school in
suburban Boston, MA were introduced to disability and rehabilitation medicine (primarily PT) in
a program called “Understanding Handicaps” by this author during the early 1990s. That
program introduced young students to motor functions: why and how motor abilities are lost or
never develop, and how therapeutic exercise can help to improve or compensate for the
impairments. This program provided the children with the opportunity to experience how
physical therapists teach people of all ages to uses adaptive equipment (walkers, crutches, cane
and/or wheelchairs) to attain their maximal functional mobility.
Middle and high school children are often introduced to a wide variety of future careers
and professions through summer enrichment programs and job fairs during the school year or

142
high school curricula with a healthcare focus. One example of the latter is Edward M. Kennedy
Academy for Health Careers (EMK) that aims to foster minority interest in healthcare through its
curriculum, its Shadow Day, and its partnership with Northeastern University (NU). This
Shadow Day program for tenth-grade students aims to maintain their interest in the health
sciences. They observe and interact in a college-level class on a topic related to healthcare over
the course of one school day. The day consists of attending the class, which varies every year,
lunching with student mentors from NU’s Bouvé College of Health Sciences, and writing their
reflections on the day. It is proposed that the EMK academic curriculum, partnership with
Northeastern University and programs such as the NU/EMK Shadow Day provide exposure to
and awareness of various health and medical professions. This awareness could potentially
facilitate the development of student interest in healthcare as a future profession. Analysis of
student reflections following the shadow day found that 52.14 percent responded positively to
the experience. Continuation of such experiences that introduce students to the health care fields
and yield positive experiences can widen student perspectives of future options in the healthcare
and potentially foster development of an under representative minority workforce (Larrieux et
al., 2012).
6.5.2 The Law: A Call for State Healthcare Antidiscrimination Law
As discussed in the review of the literature (Chapter 2), the United States judicial and
regulatory systems have been relatively unhelpful as a means to successfully contest and
eventually eradicate racial health status disparities. Given the many factors associated with
health disparities (poor minority health status, institutional racism in healthcare, and inadequate
legal protection), case law has proven that these mechanisms are inadequate by themselves to
address discriminatory practices. In 1946, the Hill Burton Act [41 U.S.C. §§291 291O

143
(2002)] required hospitals and facilities that received funding under this act for construction and
modernization to provide uncompensated care and services to persons unable to pay as well as
for persons living in the area. Since 1965, federal laws such as Title VIII and XIX of the Social
Security Act that implemented Medicare and Medicaid respectively, mandate that providers and
facilities abide by Title VI of the Civil Rights Act which prohibits discrimination based on race,
color, or national origin in all programs and activities that receive federal financial assistance.
Thus, the legal and regulatory systems primarily focus upon eradicating healthcare disparities
(disparities in the frequency of and quality of delivery of healthcare services) and not general
disparities in health status.
The only federal law explicitly related to eliminating racial discrimination in healthcare
delivery is Title VI of the Civil Rights Act. Specifically, section 601of Title VI states:
“No person in the United States, shall, on the grounds of race, color, or national origin, be excluded from participation in, be denied the benefits of, or be subject to discrimination under any program or activity receiving federal financial assistance” [Title VI of the 1964 Civil Rights Act. Pub. L. No. 99-352, 378 252 (codified at 42 U.S.C.) 2000d-2000d-4 (1982)] However, because the Supreme Court interpreted section 601 to be related only to intentional
discrimination and regulatory agencies interpreted Title VI to exclude doctors in private practice,
cases brought before the court system have not been successfully litigated as they have been
deemed to have occurred due to unintentional bias. Furthermore, little data have been provided
regarding Title VI compliance by the Office of Civil Rights (Randall, 2007).
Consequently, health care disparities remain a problem as findings of the United States
Commission on Civil Rights as reported by Randall (ibid pg 183 - 184) clearly reports:
“There is substantial evidence that discrimination in healthcare delivery, financing and research continues to exits. Such evidence suggests that Federal laws designed to address inequality in healthcare have not been adequately enforced by federal agencies. [Such failure has] resulted in a failure to remove the historical barriers to access to quality healthcare for women and minorities, which in turn has perpetuated these barriers”

144
Therefore, Randall (ibid pg 184 -187) proposed “A HealthCare Antidiscrimination Act”
be enacted as a legislative measure to better address health disparities which Title VI of Civil
Rights Act does not effectively address. The proposed law would focus on six critical criteria
that would:
Recognize multiple forms of discrimination, including overt and implicit
Authorize and fund testers and testing organizations
Send individuals of different races, but with the same symptoms or medical
complaints, to healthcare providers or facilities to determine if patients of certain
races receive different treatment
Assure fines and regulatory enforcement
Require health scorecards/report for health agency providers, or facilities
Require data collection and reporting
As Randall insists, the current Civil Rights Act does not adequately address racial disparity in the
healthcare system. For “effective public health policy to be established, appropriate state and
federal laws must be available to eliminate discriminatory practices in healthcare” (Op cit pg.
188).
6.6 Conclusion and Policy Recommendations
This study identified disparities in the functional outcomes between Medicare minority
and non-minority beneficiaries who had a THR and were discharged home with home health care
physical rehabilitation services. Despite the commonality of surgical intervention and post-acute
care discharge destination with home health care for physical rehabilitation, racial/ethnic
differences were consistently found in the level of functional independence, when all other
factors of the model were controlled by a statistical model. The implications of these findings

145
suggest a persistent racial/ethnic inequity in healthcare that merits educational policy
recommendations.
Related specifically to the health professions delivering post-acute physical rehabilitation
to those receiving homecare, it is noted that the accrediting body for physical therapy education,
the Commission on Accreditation in Physical Therapy (CAPTE), requires both cultural
competency standards and linguistic competency as components for all physical therapy
education curricula. There are nine criteria in total that must be met by the PT programs and the
criteria must be clearly stated in course(s) of the program's curriculum. However, there is not a
designated format for adhering to this requirement and it may be satisfied differently depending
on the school and/or state. Although encouraged as a matter of professional duty, there is
currently no known cultural competency post-graduate requirement linked to licensure renewal
for physical therapists.
To date, the four federal mandates of the CLAS Standards in Health and Health Care and
Title VI of the Civil Rights Act (1964) remain laws at the federal level governing cultural and
linguistic matters of health and racial/ethnic discrimination respectively. In addition, Executive
Order 13166 signed August 11, 2000 by president Clinton, further explains Title VI by stressing
the need to improve access for persons with limited English proficiency (Chun, 2009). Thus,
from the federal perspective, the matter is an issue of equal access to health services.
However, a more holistic approach that addresses the several factors that have been found
related to the racial/ethnic disparities in minority health status and healthcare is being addressed
through cultural competence, and its components of diversity, and patient centered care. Over
the course of the last twelve years, some state legislatures have addressed the matter of health
disparities with cultural competency as a required regulation for licensed practice in their states.

146
For instance, New Jersey’s Bryant Law, enacted and passed in March 2005 mandates that all
medical students complete cultural competency training in order to practice as a licensed
physician in that state; the California Bill AB 1195 requires the accrediting body responsible for
continuing medical education to include curriculum in cultural competency for all coursework
that includes direct patient care; and effective 2008, in the state of Washington, SB 6194
required all health professional educational programs to include multicultural health in their
curricula (Chun, 2009).
The effect of cultural competency education was evaluated by Horvat et al (2014) in the
United States, Canada, and the Netherlands based on a systematic review of five studies in the
literature. Although the studies varied in how the cultural education was provided and which
outcome measures were used for assessment, evidence indicated improved improvements in the
involvement of culturally and linguistically diverse (minority) patients. Similarly, in a
systematic review of seven studies, five in the United States, one from Canada and one from
Scotland, Govere et al. (2016) concluded that despite various formats and duration of training
and different cultural assessment tools, cultural competency training was significantly associated
with increases in five of the seven patient satisfaction items used to assess the effects of cultural
competency training for health professionals. Although no generalizable conclusions could be
drawn, results showed that the cultural competence training of the health professionals was
associated with increased patient involvement and satisfaction.
The outcomes of these studies are representative of patient-centered care and are aligned
with the principal standard of the CLAS Health and Health Care. As such they can be considered
as the rationale for the development and implementation of a two-pronged cultural competency
mandate for all health care professionals. The first component of the recommended policy would

147
be for a generic but standardized transdisciplinary core cultural competency education module
applicable to all healthcare providers. The second component of this process should be of
discipline-specific relevance. In as much as cultural competence is a process, it is suggested that
the cultural competency education become an integral component of the routine professional
licensing process required in all states as a required condition of license renewal. As discussed
by Govere et al., such a process should be based upon “valid and reliable standardized cultural
competence assessment tools specific to the competencies of a given health profession.” In
addition, “applying valid and reliable standardized patient satisfaction assessment tools specific
to the culturally competent care given to the patient…may improve correlation between care and
patient satisfaction” (ibid pg 409). The combination of self-awareness of bias, acknowledgement
of health disparities, mandated cultural competency and the previously discussed programs to
improve the diversification of the healthcare workforce bode well for the delivery of optimal and
equitable health services to people of all ethnic and racial origins and for the potential of each
patient to attain their best functional outcome.
6.7 Future Research
Given the findings of this research, racial/ethnic disparities as measured by the transfer
and ambulatory ability of a study sample at the point of termination of home health care services
do exist. Less obvious is why these disparities exist. Future research should consider
examination of the number of comorbidities or the severity of sickness verses racial /ethnic
identity. It is possible, that the source of the disparity found in this study was related to poorer
health status of minority groups, however this was not factored into the model. As noted this
study captured functional outcomes at a specific point of care – the termination of HHC. It
would be beneficial to collect a medical baseline and include prognosis for all participants as a

148
mandatory component within the OASIS so that future health disparities research in this field
could control for these characteristics. It is also not known whether the surgical and functional
outcomes met the patients’ expectations. Linking the CMS data set to patient satisfaction
surveys would be helpful in finding whether the patient was satisfied or not irrespective of the
surgical outcomes. Including measures of these potential influential factors could afford a more
comprehensive understanding of racial/ethnic disparities in functional outcomes. Continued
research and innovative actions to address inequitable racial/ethnic outcomes is an important
component in the effort to resolve the multifaceted problem of health care disparities among
marginalized groups of the population.

149
References:
2014 National Healthcare Quality and Disparities Report. Rockville, MD: Agency for Healthcare Research and Quality; May 2015. AHRQ Pub. No. 15-0007.
Atrash, H., & Hunter, M. (2006). Health Disparities in the United States: A continuing
Challenge. In D. Satcher, & R. Pamies, (Eds.), Multicultural Medicine and Health Disparities. New York, NY: McGraw-Hill Medical Publishing Division.
Ayanian, J., Williams, R., (2007). Principles for Eliminating Racial and Ethnic Disparities in
Healthcare. In R. Williams (Ed.), Eliminating Healthcare Disparities in Americ: Beyond the IOM Report. (pp 377 – 385). Totowa, N.J. Humana Press.
Banaji, M., Greenwald, A. (2013) Blond Spot: Hidden Biases of Good People. New York:
Bantam Books. Barbour, K. E., Helmick, C. G., Theis, K. A., Murphy, L. B., Hootman, J. M., Brady, T. J., &
Cheng, Y. J. (2013). Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation—United States. Morbidity and Mortality Weekly Report, 62(44), 869-873.
Benz, Jennifer. Espinosoa, O., Welsh, V., Fontes, A. (2011). Awareness of racial and ethnic
health disparities has improved only modestly over a decade. Health Affairs. 30 (10) 1860-1867.
Berlin, I., Favreau, M., Miller, S. (1998). Remembering Slavery. New York: The New Press. Betancourt, J., Green, A., Carrillo,J. Park,E., (2005). Cultural competence and healthcare
disparities:key perspectives and trends. Health Affairs. 24 (2); 499-505 Bhandari, Vijay, Kushel, M., Price, L., Schillinger, D. (2005). Racial disparities in
outcomes of inpatient stroke rehabilitation. Archives of Physical Medicine and Rehabilitation. 86, 2081-2086.
Blair I, Steiner J, Fairclough D, Hanratty R, Price D, Hirsh H, & Havranek E. 2013).
Clinicians’ implicit ethnic/racial bias and perceptions of care among black and latino patients. Annals of Family Medicine. 11(1):43 - 52.
Bloche, M. G. (2001). Race and Discretion in American Medicine, Yale Journal of Health
Policy, Law, and Ethics . 95 - 131. Braveman, Paula (2006). Health disparities and health equity: Concepts and measurement.
Annual Review of Public Health, 27, 167-194. Braveman, P., Sgerter, S., Williams, D. (2011). The social determinants of health: coming of

150
age. Annual Reviews of Public Health. 32, 381-398. Braveman, Paula, (2014). What are health disparities and health equity? We need to be clear.
Public Health Reports. 129 (suppl 2) 5-8. Brega, A., Goodrich,G., Powell,. Grigsby, J. (2005). Racial and ethnic disparities in the
outcomes of elderly home care recipients. Home Health Care Services Quarterly. 24 (3), 1 – 21.
Bronfenbrenner, U. (1977) Toward an experimental ecology of human development. American
Psychologist. July, 513 – 531. Burke J, Van Ryn M. (2000) The effect of patient race and socioeconomic status on physicians’
perceptions of patients. Social Science & Medicine. 50 (6), 813 - 828. Carmichael, S. (1967). Black Power: The Politics of Liberation in America. London: Penguin Books. Carter-Pokras, O., Baquet, C. (2002). What is a “health disparity”? Public Health Reports. 117
(5), 426-434. Carter, S., Rizzo, J. (2007). Use of outpatient physical therapy services by people with
musculoskeletal conditions. Physical Therapy. 87(5). 497-512. Center for Disease Control and Prevention; Morbidity and Mortality Weekly Report (2009).
Prevalence and Most Common Causes of Disability Among Adults---United States, 2005. 58 (16), 421-426.
Center for Disease Control and Prevention ; Morbidity and Mortality Weekly Report (2013)
Prevalence of Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation – United States, 2010-2012. 62 (44), 871-873.
Center for Disease Control and Prevention. National Hospital Discharge Survey: 2010 table,
Procedures by selected patient characteristics – Number by procedure category and age. “Number of all-listed procedures for discharges from short-stay hospitals, by procedure category and age: United States, 2010” updated 7/6/2016. Available at: http://www.cdc.gov/nchs/data/nhds/4procedures/2010pro4_numberprocedureage.pdf accessed: 7/11/2016
Center of Medicare and Medicaid Services (1) available at
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/OASIS/DataSet.html
Center of Medicare and Medicaid Services (2) available at
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/OASIS/Background.html

151
Center of Medicare and Medicaid Services Comprehensive Care for Joint Replacement Model
available at: https://inn.ovation.cms.gov/initiatives/cjr Center of Medicare and Medicaid Services (3): (7/15/2016 last modified) NHE Fact Sheet.
Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NHE-Fact-Sheet.html Accessed 7/12/16.
Chan, L., Wang, H., Terdiman, J., Hoffman, J., Ciol, M., Lattimore, B., Sidney,
S.,…Sandel, M. (2009) Disparities in outpatient and home health service utilization following stroke: results of a 9-year cohort study in northern california. (2009). Physical Medicine and Rehabilitation. 1 (11); 997 - 1003,
Chun, M., (2009). Cultural competency compliance issues in health care: an overview of
federal and state mandates and suggested tools and resources. Journal of Health Care Compliance. 11 (5); 27-32.
Clair,A., Evangelista, P., Lajam, C., Slover, J., Bosco, J., Iorio, R., Cost analysis of total
arthroplasty readmissions in a bundled payment care improvement initiative. The Journal of Arthroplasty. Article in Press 1-4.
Colby, S. L., Ortman, J.M. (2014). Projections of the Size and Composition of the U.S.
Population: 2014 to 2060, Current Population Reports, P25-1143, U.S. Census Bureau, Washington, DC.
Cooper, R., Kaufman, J., Ward, R., (2003). Race and Genomics. New England Journal of Medicine. 348 (1166 – 1170). Cooper L, Roter D, Inui T,Carson,K., Beach, M., Sabin,J., Greenwald, A., Inui,T., (2012). The
associations of clinicians' implicit attitudes about race with medical visit communication and patient ratings of interpersonal care. American Journal of Public Health. 102(5): 979 - 987.
Cram, P., Lu, X., Kaboli, P., Vaughan-Sarrazin, M., Cai, X., Wolf, B., & Li, Y. (2011).
Clinical characteristics and outcomes of Medicare patients undergoing total hip arthroplasty, 1991-2008. Journal of American Medical Association. 305(15), 1560-1567.
Daigle, M., Weinstein, S., Katz, J., Losina, E. (2012). The cost-effectiveness of total joint
arthroplasty: a systemic review of published literature. Best Practice & Research Clinical Rheumatology. 26. 649-658.
Dannefer, INITIAL?. (2003) Cumulative advantage /disadvantage and the life course: cross-
fertilizing age and social science theory. Journal of Gerontology: Social Sciences. 58B (6). S3327 – S337.

152
Dahodwala, N., Ming, X., Noll, E., Siderowf, A., Mandell, D. (2009). Treatment of disparities
in Parkinson’s disease. Annals of Neurology. 66(2). 142-145. dePablo, P., Losina, E., Phillips, C., Fossel, A., Nizar, M., Lingard, E., & Katz, J. (2004)
Determinants of discharge destination following elective total hip replacement. Arthritis & Rheumatism. 51(6), 1009-1017.
Diez, R., Mair, C. (2010) Neighborhoods and health. Annals of the New York Academy of
Sciences. 1186, 125-145. Donabedian, A. (2003). An Introduction to Quality Assurance in Health Care. New York:
Oxford University Press. Donabedian, A. (2005). Evaluating the quality of medical care. The Milbank Quarterly. 83 (4),
691-720. Dunlop, D., Song, J., Manheim, L., Chang, R. (2003). Racial disparities in joint replacement
use among older adults. Medical Care. 41: (2) 288-298. Dupont, W.D., Plummer, W.D. (1997). PS power and sample size program available for free on
the Internet. Controlled Clin Trials: 18:274 Ellis, C., Egede, L., (2009). Racial/ethnic differences in poststroke rehabilitation utilization in
the USA. Expert Review of Cardiovascular Therapy. 7(4). 405-410. Epstein, R., Fiscella, K., Lesser, C., Stange, K., (2010). Why the nation needs a policy push on
patient-centered health care. Health Affairs. 29, (8), 1489-1495. Federal Bureau of Prisons. Inmate Statistics. Available at:
https://www.bop.gov/about/statistics/statistics_inmate_race.jsp Accessed 12/30/2016. Ferreira, P., Ferreira, M., Maher, C., Refshauge, K., Larimer,J., Adams,R. (2013). The
therapeutic alliance between clinicians and patients predicts outcome in chromic low back pain. Physical Therapy. 93 (4): 470 – 478.
Frank L, Basch E, Selby J., (2014). The PCORI perspective on patient-centered outcomes
research. Journal of the American Medical Association. 312 (15):1513-1514. Fricke J. (2012). Activities of Daily Living. In: J.H. Stone, M. Blouin, editors. International
Encyclopedia of Rehabilitation. Available online: http://cirrie.buffalo.edu/encyclopedia/en/article/37/
Fuentes, J., Armijo-Olivo,S., Funabashi, M., Miciak,, M., Dick, B., Warren, S., Rashiq, S.,
Magee, D., Gross, D. (2014). Enhanced therapeutic alliance modulates pain intensity

153
and muscle [pain sensitivity in patients with chronic low back pain: an experimental controlled study. Physical Therapy. 94 (4). 477 - 489.
Gamble, V., Stone, D. (2006). U.S. policy on health inequities: the interplay of politics and
research. Journal of Health Politics, Policy and Law, 93(122), 99-106. Gebbie, K., Rosenstock, L., Hernandez, L. Eds. Institute of Medicine (2003). Who will keep the Public Healthy? Educating Public Health Professionals for the 21st Century. CITY:
National Academy Press. Geronimus, A. (1992). The weathering hypothesis and the health of African-American women
and infants: evidence and speculations. Ethnicity and Disease. 2 (3), 207-221. Geronimus, A. (1996). Black/White differences in the relationship of maternal age to
birthweight: a population-based test of the weathering hypothesis. Social Science and Medicine. 42 (4), 589-597.
Geronimus, A., Hicken, M., Keene, D. Bound, J. (2006). “Weathering” and age patterns of
allostatic load scores among blacks and whites in the United States. American Journal of Public Health. 96 (5), 826-833.
Gill, S., McBurney, H. (2013) Does exercise reduce pain and improve physical function before
hip or knee replacement surgery? A systematic review and meta-analysis of randomized controlled trials. Achieves of Physical Medicine and Rehabilitation. 94 (1) 164-176.
Goldberg, J., Johnson, M., Pajerowski,W., Tanamor, M., Ward, A., (2011). Home Health Study
Report (Report No. HHSM- 500-2021-00072C). Baltimore, MD: L & M Policy Research, LLC.
Gorman, S., Curry, A. (2010) A Pilot Study Exploring the Variability of Physical Therapy
Practices of Members of the Total Joint Replacement Listserv. Journal of Acute Care Physical Therapy: 1 (2), 46-55.
Govere, L., Govere, E. (2016) How effective is cultural competence training of healthcare
providers on improving patient satisfaction of minority groups? A systematic review of the literature. Evidenc Based Nursing. 13 (6); 402-410.
Green, A. Carney, D., Pallin, D., Ngo, L., Raymond, K., Iezzoni, L., Banaji, M. (2007)
Implicit bias among physicians and its prediction of thrombolysis decisions for black and white patients. Journal of Internal Medicine. 22 (9); 1231-1238.
Groeneveld, P., Kwoh. K., Mor, M., Appelt,C., Geng, M,. Gutierrez, J., Wessel, D., Ibrahim,
S. (2008) Racial differences in expectation of joint replacement surgery outcomes. Arthritis Care and Research. 59 (5); 730 -737.

154
Grumbach, K., & Mendoza, R. (2008). Disparities in human resources: addressing the lack of
diversity in the health professions. Health Affairs, 27 (2): 413-422. Hall, A., Ferreira, P., Maher.C., Latimer,J., Ferreira.M. (2010). The influence of the therapist-
patient relationship on treatment outcome in physical rehabilitation: a systematic review. Physical Therapy. 90 (8); 1099 – 1110).
Hall, W., Chapman,M., Lee, K., Merino, Y., Thomas, T., Payne,B., Eng, E., Day, S., Coyne-
Beasley, T., (2015) Implicit racial/ethnic bias among healthcare professional and it influence on health care outcomes: a systematic review. American Journal of Public Health. 105 (12) e60 – e76.
Harada, N., Chun, A., Chiu, V., Pakalniskis, A. (2000). Patterns of rehabilitation utilization
after hip fracture in acute hospitals and skilled nursing facilities. Medical Care. 38(11). 1119-1130.
Hartley, G.W., Camilo, S. (2012). Patient management in postacute inpatient settings. In A.
Guccione, R. Wong, & D. Avers. (Eds). Geriatric Physical Therapy, (3rd ed., pp. 482-499). St Louis, MO: Elsevier. .
Healthy People 2020.gov. Social Determinants of Health. Available at:
https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health. Accessed 9/1/2016.
Heckler, M.M. U.S. Department of Health and Human Services (1985) Report of the
Secretary’s Task Force Report on Black and Minority Health Volume I: Executive Summary. Other. Government Printing Office, Washington, DC.
Helmick, C., Felson, D., Lawrence, R., Gabriel, S., Hirsch, R., Kwoh, C.,……Stone, J. (2008).
Estimates of the prevalence of arthritis and other rheumatic conditions in the United States part I. Arthritis and Rheumatism. 58 (1). 15-25.
Hernandez, L. (editor) (2003) Who will keep the public healthy? – Workshop Summary. Committee on Educating Public Health Professionals for the 21st Century Board on Health Promotion and Disease. Institute of Medicine of the National Academies. Available at: http://www.nap.edu/catalog/10759.html
Hintze, J. (2011). PASS 11. NCSS, LLC. Kaysville, Utah. Available at: www.ncss.com. Hootman, J., HeIlmick, C., Barbour, K., Theis, K., Boring, M. (2016) Updated projected
prevalence of self-reported doctor-diagnosed arthritis and arthritis-attributable activity limitation among US. adults, 2015-2014. Arthritis and Rheumatology. 68 (7). 582-1587.
Horn, S., Deutscher, D. Smout, R., DeJong, G. & Putman, K. (2010). Black-White differences in patient characteristics, treatments, and outcomes in inpatient stroke rehabilitation.

155
Archives of Physical Medicine and Rehabilitation. 91. 1712 – 1721. Horner, R., Swanson, J., Bosworth, H., Matcher, D. (2003). Effects of race and poverty on the
process and outcome of inpatient rehabilitation services among stroke patients. Stroke. 34. 1027-1031.
Horvat, L., Horey, D., Romios, P., Kis-Rigo, J., ( 2014). Cultural competence education for
health professionals (Review). Cochrane Database Systematic Reviews. 2014 May 5;(5):CD009405. doi: 10.1002/14651858.CD009405.pub2.
HSS.gov, “Key Features of the Affordable Care Act By Year” Available at:
https://www.hhs.gov/healthcare/facts-and-features/key-features-of-aca-by-year/index.html# Accessed 12/23/2016.
Hospital for Special Surgery website. “Hip Replacement” available at: https://www.hss.edu/condition-list_hip-replacement.asp Accessed 6/7/2016.
Ibrahim, S. (2010). Racial variations in the utilization of knee and hip joint replacement: an
introduction and review of the most recent literature. Current Orthopedic Practice. 21 (2). 126-131.
Inneh, I.A., Clair, A.J., Slover, J.D., Lorio, R. (2016). Disparities in discharge destination after
lower extremity joint arthroplasty: analysis of 7,924 patients in an urban setting. The Journal of Arthroplasty. Doi: 10.1016/j.arth.2016
Irgit, K., Nelson, C. (2011). Defining racial and ethnic disparities in THA and TKA. Clinical
Orthopedic and Related Research. 469; 1817-1823. Isaac, L. (2013). Defining Health Care Disparities and Examining Disparities Across the Life
Span. In La Veist & L. Isaac (Eds.), Race, Ethnicity and Health: A Public Health Reader (11-31). San Francisco, CA: Jossey-Bass.
James, S. A. (1994). John Henryism and the health of African-Americans. Culture, Medicine
and Psychiatry. 18; 163-182 Jette, A. (2017). From person – centered to family – centered health care. Physical Therapy. 97
(2); 157 – 158. Jones, C. (2000). Levels of racism: a theoretical framework and the gardener’s tale. American
Journal of Public Health. 90; 1212-1215. Kennedy, E. (2005). The role of the federal government in eliminating health disparities. Health
Affairs. 24(2), 452-458. Kim, T., Gordes, K., Alon, G. (2010). Utilization of physical therapy in home health care under
the prospective payment system. Journal of Geriatric Physical Therapy. 33(1). 2-9.

156
Keswani,a., Tast, M., Fields,A., Lovy., A., Moucha. C,. Bozic, k., (2016). Discharge destination after total joint arthroplasty an analysis of postdischarge outcome, placement risk factors, and recent trends. The Journal of Arthroplasty. 31. 1155 – 1162.
Klees, B., Wolfe, C., Curtis, C. “Brief Summaries of Medicare & Medicaid as of November 16, 2015.” Office of the Actuary, Centers for Medicare & Medicaid Services, Department of Health and Human Services Available online at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/MedicareProgramRatesStats/Downloads/MedicareMedicaidSummaries2015.pdf,
Koh, H., Gracia, N., Alvarez, M., (2014) Culturally and linguistically appropriate services-
advancing health with CLAS. New England Journal of Medicine.37 (3); 198 – 201. Kremers, W., Washington, R., Steiner, C., …Berry,D. (2015). Prevalence of total hip and knee
replacement in the United States. Journal of Bone and Joint Surgery. 97-A (17). 1386-1397.
Krieger, N. (1987) Shades of difference: theoretical underpinnings of the medical controversy
on black/white differences in the United States, 1830-1870. International Journal of Health Services. 17 (2) 259-278.
Kurtz, S., Ong, K., Lau, E., Mowat, F., Halpern, M. (2007). Projections of primary and revision
hip and knee arthroplasty in the United States from 2005 to 2030. The Journal of Bone and Joint Surgery. 89-A (4) 780-785.
LaVeist, T. (1994). Beyond Dummy Variables and Sample Selection: What health services
researchers ought to know about race as a variable. In T.A. LaVeist (Ed.), Race, Ethnicity and Health (pp115-128). San Francisco: Jossey-Bass. (2002).
LaVeist,T., Nuru-Jeter, A., (2002). Is doctor-patient race concordance associated with greater
satisfaction with care? (2002). Journal of Health and Social Behavior. 43 (3). 296 – 306.
LaVeist, T. (2005) Conceptual Issues in Race/Ethnicity and health (chapter 2). In T. La Veist
(Ed.), Minority Populations and Health-An Introduction to Health Disparities in the United States (pp. 15-29). San Francisco: Jossey-Bass.
LaVeist, T. (2005). Theories of Racial/Ethnic Differences in Health (chapter 7). In T. LaVeist
(Ed.), Minority Populations and Health-An Introduction to Health Disparities in the United States (pp. 133-156). San Francisco: Jossey-Bass.
LaVeist, T. (2005). Socioeconomic Status and Racial/Ethnic Differences in Health (chapter 8).
In T. La Veist (Ed.), Minority Populations and Health-An Introduction to Health Disparities in the United States (pp. 157-179). San Francisco: Jossey-Bass.

157
LaVeist, T., Gaskin D., Richard P. (2009). The economic burden of health inequities in the United States. Washington DC: Joint Center for Political and Economic Studies.
LaVeist, T., Pollack, K., Thorpe, R., Fesahazion, R., Gaskin, D. (2011). Place, not race:
disparities in southwest Baltimore when blacks and whites live under similar conditions. Health Affairs. 30(10). 1880-1887.
Lavernia CJ, Lee D, Sierra RJ, Gomez-Marin O. (2004). Race, ethnicity, insurance coverage,
and preoperative status of hip and knee surgical patients. J Arthroplasty. 19: 978–85. Lavernia CJ, Alcerro JC, Rossi MD. (2010). Fear in arthroplasty surgery: the role of race. Clin
Orthop Relat Res 468: 547–54. Learmonth, I.D., Young, C., Rorabeck, C. (2007) The operation of the century: total hip
replacement. Lancet. 370. Oct 27, 1508-1519 Available at: www.thelancet.com Accessed: 6/20/16.
Leland, N., Gonzalo, P., Christian, T., Bynum, J., Mor, V., Weile, T., Teno, J. (2015). An
examination of the first 30 days after patients are discharged to the community from hip fraction postacute care. Medical Care. 53 (10) 879-887.
Mahomed, N., Davis, A., Hawker, G., Badley, E., Davey, R., Syed, K.,…Wright, J. (2008)
Inpatient compared with home-based rehabilitation following primary unilateral total hip or knee replacement: a randomized controlled trial. The Journal of Bone and Joint Surgery. 90-A (8). 1673-1680.
Mallinson, T., Bateman, J., Hsiang-Yi, T., Manheim, L., Almagor, O., Deutsch, A., Heinemann,
A. (2011) A comparison of discharge functional status after rehabilitation in skilled nursing, home health, and medical rehabilitation settings for patients after lower-extremity joint replacement surgery. Archives of Physical Medicine and Rehabilitation. 92. 712-720.
McCallum, C. (2010). Access to physical therapy services among medically underserved adults:
a mixed-method study. Physical Therapy 90(5). 735-747. McEwen, B., Gianaros, J. (2010) Central role of the brain in stress and adaptation: links to
socioeconomic status, health and disease. Annals of the New York Academy of Sciences: Issues the Biology of Disadvantage. 1186. 190-222
McLeroy, K., Bibeau, D., Steckler, A., Glanz, K. (1988). An ecological perspective on health
promotion programs. Health Education Quarterly 15 (4). 351 – 377. Montagu, M.F. ( 1941) The concept of race in the human species in the light of genetics. The
Journal of Heredity. 32 (8). 243-248.

158
Morland, K., Wing, S., Diez, R., Poole, C. (2002) Neighborhood characteristics associated with the location of food stores and food service places. American Journal of Preventative Medicine. 22(1). 23-9.
Markus, H., Moya, P. (2010). Doing Race: 21 Essays for the 21st Century. New York
W.W. Norton. National Center for Health Statistics. (2012). Health, United States, 2011: With Special Feature
on Socioeconomic Status and Health. Hyattsville, MD. National Hospital Discharge Survey: 2009 table, Procedures by selected patient characteristics-
Number by procedure category and age. Available at: http://www.cdc.gov/nchs/data/nhds/4procedures/2009pro4_numberprocedureage.pdf
National Partnership for Action. (2011). HHS Action Plan to Reduce Racial and Ethnic Health
Disparities, 2011; and The National Stakeholder Strategy for Achieving Health Equity. Available from: http://minorityhealth.hhs.gov/npa Accessed [6/26/2012].
National Prevention and Health Promotion Strategy. (June 2011). The National Prevention
Strategy: America’s Plan for Better Health and Wellness. Available from: http://www.healthcare.gov/prevention/nphpphc/strategy/report.html Accessed
[6/26/2012]. Nelson, A.R. (2002). Unequal Treatment: Confronting Racial and Ethnic Disparities in
Healthcare (1st ed.). CITY: National Academies Press. Northbridge, M.E, Sclar, E.D., Biswas, P. (2003). Sorting out the connections between the built
environment and health: a conceptual framework for navigating pathways and planning healthy cities. Journal of Urban Health, 8(4), 556-568.
O’Connor, M., Davitt, J., (2012). The outcome and assessment information set (OASIS): a
review of validity and reliability. Home Health Care Services Quarterly, 31 (4), 267-301. O’Keeffe, M., Cullinane,P., Hurley, J., Leahy. I., Bunzli, S., O’Sullivan, P., O’Sullivan,. (2016).
What influences patient-therapist interaction in musculoskeletal physical therapy? Qualitative systematic review and meta-synthesis. Physical Therapy. 96 (5): 609 - 622.
Oliver, M.N., Wells, K.M., Joy-Gaba, J.A., Hawkins, C.B., Nosek, B.A. (2014) Do physicians'
implicit views of African Americans affect clinical decision making? Journal of The American Board of Family Medicine, 27(2), 177-188.
Ortman, J., Guarneri, C., (2014). United States Population Projections: 2000 to 2050, available
at: https://www.census.gov/population/projections/files/analytical-document09.pdf accessed 10/11/16.
Oshinsky, D. (1996). Worse Than Slavery: Parchman Farm and the Ordeal of Jim Crow Justice.

159
New York: Free Press. Patterson, D., Carline, J., Promoting minority access to health careers through health profession-
public school partnerships: a review of the literature. Academic Medicine. 81 (6); S5=S10.
Pierce, T., Elmallah, R., Lavernia, C., Chen, A., Harwin, F., Thomas, C., Mont, M. (2015).
Racial disparities in lower extremity arthroplasty outcomes and use. Orthopedics. 38 (12), e1139-e1146.
Pollack, C., Cubbin, C., Sania, A., Hayward, M., Vallone, D., Flaherty, B., Braveman, P., (2013). Do wealth disparities contribute to health disparities within racial/ethnic groups? Journal
of Epidemiology and Community Health. 67 (5), 439 - 445. Poma, P. A. (2017). Race/Ethnicity concordance between patients and physicians. Journal of
the National Medical Association, 109 (1), 6-8. Preamble to the Constitution of the World Health Organization as adopted by the International
Health Conference, New York, 19-22 June, 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948.
Qasim, M., Andrews, R. (2013). Despite overall improvement in surgical outcomes
since 2000, income-related disparities persist. Health Affairs. 32 (10), 1773-1780. Reifsnider, E., Gallagher, M., Forgione, B. (2005). Using ecological models in research on health
disparities. Journal of Professional Nursing. 4 (July-August), 216-222. Rooks, D., Huang, J., Bierbaum, B., Bolus, S., Rubano, B., Connolly, C., …Katz, J. (2006)
Effect of preoperative exercise on measures or functional status in men and women undergoing total hip and knee arthroplasty. Arthritis & Rheumatism (Arthritis Care & Research). 55 (5), 700-7-8.
Roux, A., Mair, C. (2010). Neighborhoods and health. Annals of the New York Academy of
Sciemces. 1186, 125=145.
Sabin JA, Nosek BA, Greenwald AG, Rivara FP. (2009) Physicians’ implicit and explicit attitudes about race by md race, ethnicity, and gender. Journal of Health Care for the Poor and Underserved . ; 20(3):896-913.
Santaguida, P., Hawker, G., Hudak, P., Glazier, R., Mahaomed, N., Kreder, H., …Wright, J.
(2008). Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review. Canadian Journal of Surgery. 51 (6), 428 – 436.
Satcher, D., Fryer, G., McCann, J., Troutman, A., Woolf, S., Rust, G. (2005). "What if we were equal? a comparison of the black-white mortality gap in 1960 and 2000." Health Affairs.
19(4), 459-464.

160
Schneider,J., Barkauskas,V., Keenan,G., (2008). Evaluating home care nursing outcomes with
oasis and noc. Journal of Nursing Scholarship. 40(1), 76-82. Scott, C., Bugler, K., Clement, N., MacDonald, D., Howie, C., Biant. L. (2012). Patient
expectation of arthroplasty of the hip and knee. The Bone & Joint Journal Br. 94 (7) 974-981.
Shahid, H., Singh, J. Racial/ethnic disparity in rates and outcomes of total joint arthroplasty.
(2016). Current Rheumatology Reports. 18 :20 DOI 10.1007/s11926-016-0570-3. Available at http://link.springer.com/article/10.1007/s11926-016-0570-3/fulltext.html
Shin, M.S. (2002). Redressing Wounds: Finding a Legal Framework to Remedy Racial Disparities in Medical Care. California Law Review, 90, 2047.
Singh, J., Lu, X., Rosenthal, G., Ibrahim, S., Cram, P. (2013) Racial disparities in knee and hip
total joint arthroplasty: an 18-yeaar analysis of national Medicare data. Annals of the Rheumatic Diseases. 73 (12). 2107-2115.
Smedley, B., Stith, A., Nelson, A.C. (2003). Unequal Treatment: Confronting Racial and Ethnic
Disparities in Health Care. Washington, DC: National Academies Press. Smith, D. (2016) The Power to Heal: Civil Rights, Medicare, and the Struggle to Transform
America’s Health Care System. Nashville, TN: Vanderbilt University Press. Snyder, C., Stover, B., Skillman, S., Frogner, B., (2016). Supporting diversity in the health
professions. Council on Graduate Medical Education. Available at: https://www.hrsa.gov/advisorycommittees/bhpradvisory/cogme/Publications/diversityresourcepaper.pdf Accessed : 2/19/2017.
Steel, N., Clark, Q., Lang, I., Wallace, R., Melzer, D. (2008). Racial disparities in receipt of hip
and knee joint replacements are not explained by need: the health and retirement study 1998-2004. Journal of Gerontology: Medical Sciences. 61A (6). 629-634.
Stokols, D. (1996). The social ecology of health promotion: implications for research and
practice. American Journal of Health Promotion, Inc. 10 (4), 247-257. Stokols, D. (1996). Translating social ecological theory into guidelines for community health
promotion. American Journal of Health Promotion, Inc. 10 (4), 282-298. Stokols, D. (1992). Establishing and maintaining healthy environments toward a social ecology
of health promotion. American psychologist. 47 (1), 6-22. Sullivan Commission on Diversity in the Health Workforce. (2004) Missing Persons:
Minorities in the Health Professions. Washington, DC.

161
Sweat, M.D., Denison, J.A., (1995). Reducing HIV incidence in developing countries with structural and environmental interventions. AIDS. 9 (suppl A), S251-257.
Sweeney, C. ., Zinner, D., Rust, G., & Fryer, G. E. (2016). Race/Ethnicity and Health Care
Communication: Does Patient-Provider Concordance Matter? Medical care, 54(11), 1005-1009.
Taney, C.J.R. (1857). Dred Scott v. Sandford. Available at:
http://cdn.constitutionreader.com/files/pdf/constitsky,ution/ch86.pdf Accessed 6/20/16. Tullai-McGuinness, S., Madigan, E., Fortinsky, R., (2009). Validity testing the outcomes and
assessment information set (oasis). Home Health Care Services Quarterly. 28 (1) U.S. Census Bureau (3/3/2015). News Release: New Census Bureau Report Analyzes U.S.
Population Projections. Available at: https://www.census.gov/newsroom/press-releases/2015/cb15-tps16.html Accessed: 7/12/2016.
United States Census Bureau (2012). News Release: Most Children Younger than Age 1 are Minorities, Census Bureau Reports. 5/17/2012. Available at: https://www.census.gov/newsroom/releases/archives/population/cb12-90.html Accessed: 7/12/2016.
United States Census Bureau Quick Facts: United States Available at:
https://www.census.gov/quickfacts/table/PST045215/00. Accessed 12/30/2016 U.S. Department of Health and Human Services, Health Resources and Services Administration,
Bureau of Health Professions. (2006). The rationale for diversity in the health professions: A review of the evidence. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/diversityreviewevidence.pdf
United States Department of Health and Human Services. (2011) HHS Action Plan to Reduce
Racial and Ethnic Disparities: A Nation Free of Disparities in Health and Health Care. Washington, DC. Available at: [http://minorityhealth.hhs.gov/npa/files/Plans/HHS/HHS_Plan_complete.pdf ] Accessed [6/26/2012]
United States Department of Health and Human Services. Office of Disease Prevention and
Health Promotion. Healthy People 2020. Washington, DC. Available at: [http://www.healthypeople.gov/2020/about/DOHAbout.aspx]. Accessed [6/26/2012].United States Government Accountability Office. (2012). Trends in Beneficiaries Served and HospitalResources Used in Implantable Medical Device Procedures (GAO-12-583R). Washington, DC: James Cosgrove. Retrieved from http://www.gao.gov/products/GAO-12-583R
Valentine, P., Wynn, J., & McLean, D. (2016). Improving diversity in the health
professions. North Carolina medical journal, 77(2), 137-140.

162
vanRyn, M., Burke., J. (2002). The effect of patient race and socioeconomic status on
physicians' perceptions of patients. In T. LaVeist (Ed.), A Public health Reader: Race, Ethnicity and Health (pp. 547-574). San Francisco: Jossey-Bass.
Vernig, B. Strengths and Limitations of CMS Administrative Data in Research. Research Data
Assistance Center (ResDAC), 28, Aug. 2012. https://www.resdac.org/resconnect/articles/156 . Accessed 19 Feb. 2017
Vissers, M., Bussmann, J., Verhaar, J., Arends, L., Furlan, A., Reijman, M. (2011). Recovery of
physical functioning after total hip arthroplasty: systematic review and meta-analysis of the literature. Physical Therapy. 91 (5), 615 – 629.
Washington, H. (2006). Medical Apartheid – The Dark History of Medical Experimentation on
Black Americans from Colonial Times to the Present. New York: Harlem Moon. Watson, S.D. (2001). Race, Ethnicity and Quality of Care: Inequalities and Incentives. Race,
Ethnicity and Quality of Care: Inequalities and Incentives, 27, 218-219.
White, A.A., Chanoff, D. (2011). Seeing Patients: Unconscious Bias in Health Care. Cambridge, MA: Harvard University Press.
White-Means, S., Dong,Z., Hufstader, M., Brown., (2009). Cultural Competency, Race, and skin
tone bias among pharmacy, nursing, and medical students. Medical Care Research and Review. 66 (4). 436 – 455.
Williams, D.R., Collins, C. (2001). Racial residential segregation: a fundamental cause of racial
disparities in health. Public Health Reports. 116(5). 404-416. Williams, D.R., Sternthal, M. (2010). Understanding racial-ethnic disparities in health:
sociological contributions. Journal of Health and Social Behavior. 51(s). s15-s27. Winch, P. (2012). Ecological models and multilevel interventions [PDF PowerPoint slides].
Retrieved from http://ocw.jhsph.edu/courses/healthbehaviorchange/PDFs/C14_2011.pdf World Health Organization, 1948. Preamble to the Constitution of WHO as adopted by the
International Health Conference, New York, 19 June - 22 July 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of WHO, no. 2, p. 100) and entered into force on 7 April 1948. Available at : http://apps.who.int/gb/bd/PDF/bd48/basic-documents-48th-edition-en.pdf#page=7 : Page I of the WHO Constitution

163
Figure 1.1
Figure 1.2 Key components of the Social Ecological Model
Source: “Reciprocal Causation” Winch, P (2012) Ecological models & multilevel interventions.
Johns Hopkins Bloomberg School of Public Health. PPT available at http://ocw.jhsph.edu/courses/healthbehaviorchange/PDFs/C14_2011.pdf. Accessed 6/9/12/15.

164
Figure 2.1 The Social Ecological Model: Theoretical Model Applied to this Study
Reference: Adapted from the Centers for Disease Control and Prevention (CDC). The Social Ecological Model: A Framework for Prevention, http://www.cdc.gov/violenceprevetntil/overview/social-ecologicalmodel.html (retrieved April 21, 2014)

165
Figure 2.2 Beneficiaries’ Discharge Disposition Following Orthopedic IMD Admissions, by Procedure, 2003-2009
Source: GAO analysis of Healthcare and Utilization Project Nationwide Impatient Sample Data
As accessed from GAO Report # 12-583R
6062
5956
5349 48
2023
2528
3033 34
1814 15 14
16 17 16
0
10
20
30
40
50
60
70
2003 2004 2005 2006 2007 2008 2009
Percentage
of beneficiaries
Year
Total Hip Replacement
Rehabilitative Facility Home Health Care Home or Self‐Care

166
Figure 5.1 Study Universe Flowchart

167
Table 2.1 Definitions of Health Disparities, Health Inequities, and Health Equity
Health Disparities Agency or Author Definition
Secretary’s Task force on Black and Minority Health, 1985 (U.S. Department of Health and Human Services)
“…the statistical technique of ‘excess deaths’; that is, the difference between the number of deaths observed in the majority populations and the number of deaths which would have been expected if the minority populations had the same age and sex-specific death rate as the nonminority populations.”
Minority Health and Health Disparities Research and Education Act
“A population is a health disparity population if there is significant disparity in the overall rate of disease incidence, prevalence, morbidity, mortality or survival rates in the population as compared to the health status of the general population.”
Centers for Disease Control and Prevention (2000)
Health disparities as discussed in Healthy People 2010 include “differences…by gender, race or ethnicity, education or income, disability, geography location, or sexual orientation.”
National Institutes of Health, 1999 (2007)
“Health disparities are difference in the incidence, prevalence, mortality, and burden of diseases and other adverse health conditions that exist among specific population groups in the United States.”
National Institutes of Health, 12003 (2007)
“Health Disparities Research (HD) includes basic, clinical and social sciences studies that focus on identifying, understanding, preventing, diagnosing, and treating health conditions such as diseases, disorders, and other conditions that are unique to, more serious, or more prevalent in subpopulations in socioeconomically disadvantaged (I.e., low education level, live in poverty) and medically underserved, rural, and urban communities.”
National Cancer Institute (2008)
Defined “as adverse differences in cancer incidence (new cases), cancer prevalence (all existing cases), cancer death (mortality), cancer survivorship, in the United States. These population groups may be characterized by age, disability, education, ethnicity, gender, geographic location, income, or race. People who are poor, lack health insurance, and are medically underserved (have limited or no access to effective health care)-regardless of ethnic and racial background-often bear a greater burden of disease than the general population."
Center for Disease Control and Prevention (2011)
A “particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage. Health disparities adversely affect groups of people who have systematically experienced greater obstacles to health based on their racial or ethnic groups; religion; socioeconomic status; gender; age; mental health; cognitive, sensory, or physical disability; sexual orientation or gender identity; geographic location; or other characteristics historically linked to discrimination of exclusion.”
U.S. Department of Health and Human Services, Office of Minority Health, National Partnership for Action (2011)
“A particular type of health difference that is closely linked with social or economic disadvantage. Health disparities adversely affect groups of people who have systematically experienced greater social and/or economic obstacles to health and/or a clean environment based on their racial or ethnic group; religion; socioeconomic status; gender; age; mental health; cognitive, sensory, or physical disability; sexual orientation; geographic location; or other characteristics historically linked to discrimination or exclusion."
Flaskerud (2002) The “gap between the health of socio-economically advantaged and disadvantaged populations.” Aldelson (2005) The “indicators of a relative disproportionate burden of disease on a particular population.”
Fink (2009)
The “difference in a measurement of a health variable between an individual or group with specific defining characteristics disproportionate to a defined measure for another individual or group when other variables have been controlled (genetics, sociocultural beliefs and values, personal choice, and other variation from the normative measure).”

168
Table 2.1 Definitions of Health Disparities, Health Inequities, and Health Equity (Continued)
Health Inequalities Agency or Author Definition
Whitehead (1991)
Health inequalities are differences in health that are ‘avoidable,’ ‘unjust,’ and ‘unfair.’ Equity in health means that all persons have fair opportunities to attain their full health potential, to the extent possible.”
Murray, Gakidou, & Frank (1999)
These authors regard health inequalities as any avoidable differences in health among any individuals, who should not be grouped a priori according to social characteristics (except possibly geographical location).
Graham (2004) Health inequalities are “systematic differences in the health of groups and communities occupying unequal positions in society.”
Health Equity Agency or Author Definition
World Health Organization, 1996 (Braveman, 2006)
Equity means that people’s needs, rather than their social privileges, guide the distribution of opportunities for well-being. In virtually every society in the world, social privilege is reflected by differences in socioeconomic status, gender, geographical location, racial/ethnic/religious differences and age. Pursuing equity in health means trying to reduce avoidable gaps in health status and health services between groups with different levels of social privilege.
World Health Organization, 1995 (Braveman & Gruskin, 2003a)
Equity in health is operationally defined as “minimizing avoidable disparities in health and its determinants – including but not limited to healthcare – between groups of people who have different levels of underlying social advantage”
Starfield (2001)
Equity in health is “the absence of systemic and potentially remediable differences in one or more aspects of health across populations or population subgroups defined socially, economically, demographically, or geographically."
Braveman & Gruskin (2003a)
For the purposes of measurement and operationalization, equity in health is the absence of systematic disparities in health (or in the major social determinants of health) between groups with different levels of underlying social advantage/disadvantage-that is, wealth, power, or prestige. Inequities in health systematically put groups of people who are already socially disadvantaged (for example, by virtue of being poor, female, and /or members of a disenfranchised racial, ethnic, or religious group) at further disadvantage with respect to their health; health is essential to well-being and to overcome other effects of social disadvantage. “Assessing health equity requires comparing health and its social determinants between more and less advantaged social groups.”
Asada (2005) Health inequity exists where health distribution is not “spread equally to every unit of the analysis in the population.”
U.S. Department of Health & Human Services, Office of Minority Health (2011)
“Health equity is attainment of the highest level of for all people. Achieving health equity requires valuing everyone equally with focused and ongoing social efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities.”

169
Table 2.2 Definitions of Health Care Disparities and Health Care Equity
Health Care Disparities Agency or Author Definition
Institute of Medicine report, Unequal Treatment (Smedley, Stith, & Nelson, 2003)
Defined “as racial or ethnic differences in the quality of healthcare that are not due to access related factors of clinical needs, preferences, and appropriateness of intervention.”
National Healthcare Disparities Report, Agency for Healthcare Research and Quality (2003)
Defined “as any differences among populations that are statistically significant and differ from the reference group by at least 10 percent.”
Fink (2009)
Defined as the “difference in a measurement of access to or quality of health care services between an individual or group possessing a defined characteristic when other variables have been controlled, such as individual health choices, disease courses, and other variation from the normative measure.”
Health Care Equity Agency or Author Definition
Mooney (1983) Horizontal equity requires equal treatment for equal need.
Aday, Fleming & Anderson (1984) Health care is equitable when resource allocation and access are determined by health needs.
Culyer & Wagstaff (1993) Equity in health care can mean equal utilization, distribution according to need, equal access, equal health outcomes.

170
Table 2.3 The Social Ecological Model: Conceptual Theoretical Model Applied to this
Study
Social Ecological Model Level Description
Individual/ Intrapersonal
Individual characteristics that influence ones behavior, including but not limited to: gender, age, racial/ethnic identity, SES, knowledge , attitudes , skills, self-efficacy, religious identity, health literacy, expectations.
Interpersonal Social support systems of the individual (both formal & informal) that can influence the individuals’ behavior and provide identity. Examples include family, friends, peers, religious networks, customs, traditions etc.
Organizational/Institutional The formal and informal rules and regulations policies and structures that regulate the behavior or operation of social institutions and organizations.
Community Norms and regulations, includes the built environment [i.e. parks], village or tenant associations, community leaders, businesses.
Structural/ Laws, Policy Laws, policies at the local, state, federal or global level that regulate and support actions and practices.
Adapted from: Winch, P. 2012 Winch, P (2012) Ecological models & multilevel interventions. Johns Hopkins
Bloomberg School of Public Health. PPT available at http://ocw.jhsph.edu/courses/healthbehaviorchange/PDFs/C14_2011.pdf. Accessed 6/9/12/15
Table 2.4 Racial/Ethnic Population & Incarceration Rate Within the United States
Sources:
1. Incarceration Rates: Federal Bureau of Prisons available at: https://www.bop.gov/about/statistics/statistics_inmate_race.jsp
2. U.S. Population Census: The United States Census Bureau, Quick Facts, available at: https://www.bop.gov/about/statistics/statistics_inmate_race.jsp
Ethnicity/Race # of Inmates % of Inmates % of US Population Hispanic 63,856 33.6% 17.8%
Asian 2,800 1.5% 5.6%
Black 71,904 37.8% 13.3%
Native American 3,879 2.0% 0.9%
White 111,593 58.7% White alone: 77.1%
White-Non-Hispanic/Latino: 61.6%

171
Table 2.5 An Overview of Racial/Ethnic Disparities in Physical Therapy
Authors Title Methods Population Key Findings
Ellis & Egede (2009)
Racial/ethnic differences in post stroke rehabilitation utilization in the US
Systemic literature review of 82 studies
363,540 analyzed racial/ethnic differences in utilization of rehabilitation services among individuals following a stroke
Blacks and other racial minorities receiving post stroke rehabilitation services, had longer acute hospital stays than those not identified as an individual of racial/ethnic minority heritage, but received fewer occupational, physical or speech therapy rehabilitation services during their stay.
Chan et al., (2009)
Disparities in outpatient and home health service utilization following stroke: results of a 9-year cohort study in Northern California.
A nine-year retrospective study that examined differences in the use of outpatient and home care post stroke rehabilitation services
11,119 patients hospitalized for a stroke between 1996 and 2003 and followed for 1 year
Contrary to other studies, Chan concluded that the hypothesized racial disparities did not exist among this northern California cohort. In fact, non-whites in this cohort received greater rehabilitation services in both outpatient and via home health care services.
Bhandari et al., (2005)
Racial disparities in outcomes of inpatient stroke rehabilitation.
Retrospective cohort study.
1002 post stroke pat admitted to a community-based inpatient rehabilitation facility between 1995 and 2001.
Black patients attained less functional improvement (–1.9 FIM points, P=.02) compared to whites over the course of their inpatient rehabilitation as assessed using the individual scores on the FIM(TM) 1 – a rehabilitation assessment tool to measure the degree of “disability and amount of assistance required to perform activities of daily living. Despite lower functional scores blacks were more likely to be discharged to home (adjusted odds ratio=1.7; 95% confidence interval, 1.1–2.5).
Horn et al (2010)
Black-White differences in patient characteristics, treatments, and outcomes in inpatient stroke rehabilitation.
Multicenter prospective observational cohort study of post stroke rehabilitation
732 black and white patients with moderate or severe strokes across six inpatient rehabilitation facilities
Black subjects with moderate strokes were younger, included more women than men, and had more co-morbidities such as diabetes, hypertension and obesity than their white counterpart. White subjects received more minutes a day of OT, although black subjects had significantly longer median PT and OT session duration. However, there were no cross racial disparities in patients’ functional outcomes.

172
Table 2.5 An Overview of Racial/Ethnic Disparities in Physical Therapy (Continued)
Authors Title Methods Population Key Findings
Dahodwala et al (2009)
Treatment of disparities in Parkinson’s disease
Retrospective cohort study.
307 incident Parkinson Disease cases
Blacks were “four times less likely than whites to receive any PD treatment which included PD medication commonly prescribed for patients with PD (i.e. l-dopa, bromocriptine, perolide, ropinirole), medication or physical therapy, or a second visit for PD. Disparity in treatment plans remained even after controlling for potential influential demographic and clinical factors.
Carter & Rizzo (2007)
Use of outpatient physical therapy services by people with musculoskeletal conditions
Retrospective cohort study that analyzed responses in the Medical Expenditure Panel Survey from 1996 to 2000.
18,546 adult survey participants who had at least one musculoskeletal condition
A non-northeast geographic location and minority racial/ethnic status (African American or Hispanic) were negatively correlated with the use of outpatient physical therapy services.
Leland et al (2015)
An examination of the first 30 days after patients are discharged to the community from hip fraction post-acute care
Retrospective cohort study.
880,779 Medicare fee-for-service beneficiaries 75 years of age and older who experienced their first hip fracture between 1999–2007
Blacks were 16% less likely than their white equivalents to attain this outcome. Blacks were also admitted at a higher proportion to hospital facilities ranked in the lowest quartile than the highest quartile and as such had one-day longer length of hospital stay, 3% greater intensive care unit utilization and had more hospital complications.

173
Table 3.1 Donabedian’s Structure – Process – Outcome Model: Analytic Model Applied to this Study
Structure Variable Means of Measurement CMS File Source
Personal Characteristics
Race/Ethnicity White, Black, Hispanic, Asian, North American Native, Unknown, Other MBSF Age 65 and/or older MBSF Sex Male, Female MBSF Co-morbidities Number between 1 – 25 MBSF
Social SES
According to health insurance status: Medicare Part “A” & “B” Dual Enrollment: Medicare/Medicaid status Cost Share – Low Income Subsidy status
MBSF
Geographic Beneficiary’s residence Urban or Rural MBSF Process Variable Means of Measurement CMS File Source Acute hospital length of
stay # / count of days in acute hospital LOS_DAY_CNT
MedPAR
Inpatient PT services Total charge amount for inpatient PT services PHYS_THRPY_CHRG_AMT
MedPAR
Home Health PT services
Number of HHA visits/ 1 episode of care (60 days) TOT VST CNT
HHA
Outcomes Variable Means of Measurement CMS File Source
M1850 - Transferring 00 = Able to independently transfer. 01 = Able to transfer with minimal human assistance or with use of an assistive device. 02 = Able to bear weight and pivot during the transfer but unable to transfer self. 03 = Unable to transfer self and is unable to bear weight or pivot when transferred by another person. 04 = Bedfast, unable to transfer but is able to turn and position self in bed. 05 = Bedfast, unable to transfer and is unable to turn and position self.
OASIS
M1860 – Ambulation/Locomotion
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device). 01 = With the use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or without railings. 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces. 03 = Able to walk only with the supervision or assistance of another person at all times. 04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.
OASIS

174
Table 4.1 Characteristics of CMS Claims & Assessment Files Used for Data Sources*
Reference: https://www.resdac.org/cms-data/files/mbsf: accessed 12/17/2016
File Name Abbreviation Function
Medicare Provider Analysis and Review
MedPAR
Addresses Medicare utilization Contains inpatient hospital and skilled nursing facility (SNF)
final stay records. Includes: diagnosis & procedure codes (ICD-9), dates of
service, reimbursement amount, beneficiary demographic information.
Source used to identify of the CMS beneficiaries with THR
Master Beneficiary Summary
MBSF
Includes several segments of information; the following were used for this research: Base A/B/D segment is the source for beneficiary enrollment
information, reasons for entitlement and monthly& monthly manage care indicators
Chronic Conditions segment includes administrative data linked by a unique identifier allowing researchers to analyze information across the continuum of care
Cost & Utilization segment includes summarized information about the service utilization and Medicare payment amounts by file type.
Home Health Agency HHA
Holds final actions, fee for service claim submitted by HHA providers:
Includes number & type of visit (i.e. skilled-nursing care, PT, OT, SpT health aide, medical social services)
Holds final actions, fee for service claim submitted by HHA providers:
Includes number & type of visit (i.e. skilled-nursing care, PT, OT, SpT health aide, medical social services)
Outcome & Assessment Information Set
OASIS
Contains data items developed for measuring patient outcomes for the purpose of performance improvement in home health care
Medicare certified home care agencies are required to conduct patient-specific comprehensive assessments at specified times. The data are collected at start of care, 60-day follow-ups, and discharge
OASIS variable selection & justification worksheet must be completed to indicate & select which of the 500 plus variables are needed to carry out the study
Source for functional outcome measures M 1850 & M1860 used in this study

175
Table 4.2 Pilot Study Data to Determine if Sufficient Racial/Ethnic Diversity OBJECTIVE 1: Distribution of total hip replacement discharge destination by race/ethnicity
Home/Self-care SNF HHC IRF Other White 2000 8754 5219 993 580
Non-White 386 1867 973 313 148
Chi-Square Test Power Analysis — Numeric Results for Chi-Square Test
Power N W Chi-Square DF Alpha Beta 1.0 21,233 0525 68.5681 4 0.05000 0.00000
Table 4.2.2 OBJECTIVE 2: Pairwise Comparison of Total Hip Replacement Discharge Designation Objective 2a - Frequency Table (White vs. African-American). Effect size = 0.034506; DF=4.
Home/Self-care SNF HHC IRF Other White 2000 8754 5219 993 580
African American
113 405 273 51 53
Objective 2b - Frequency Table (White vs. Asian). Effect size = 0.075867; DF=4.
Home/Self-care SNF HHC IRF Other White 2000 8754 5219 993 580 Asian 59 420 147 96 38
Objective 2c - Frequency Table (White vs. Hispanic). Effect size = 0.040638; DF=4. Home/Self-care SNF HHC IRF Other
White 2000 8754 5219 993 580 Hispanic 181 908 456 148 52

176
Table 4.3 Structural and Process Variables of Study Sample Defined
Primary Analysis
Influences on Process and Outcome Dependent Variable Independent Variables
% predicted of dependent and relative contribution of dependent
Outcome # 1
Current Transfer Group A/Independent = 00 & 01 Group B/Dependent = 02 -05 or > 02
1-Race/Ethnicity: White; Black/African American Other as self-identified: Other’ including self-identified other, North American Native, Asian, Hispanic North American Native 2- Age: 65-74; 75-84; 85+ 3. Sex 4- Diagnosis Count 1-4; 5-7; 8-11 & 12+ 5 -Residence ‐ Urban ‐ Rural 6 – Length of Stay [LOS]: Quartile grouping 7 – Total PT Charge Amount: Quartile grouping 8 – Days_ Disch_2_assess: Quartile grouping
YES
Outcome # 2
Ambulation/Locomotion Group A/Independent = 00 & 01 Group B/Dependent = 02 -05 or > 02
1-Race/Ethnicity: White; Black/ African American Other as self-identified: Other’ including self-identified, Asian, & No American ; Asian; Hispanic No American Native 2- Age Continuous 65 – oldest beneficiary 3- Sex 4- Diagnosis Count -Continuous 1 – 25 -Categorical: 0-4; 5-7; 8-11 & 12+ 5 -Residence ‐ Urban ‐ Rural 6 – Length of Stay [LOS]: Quartile grouping 7 – Total PT Charge Amount: Quartile grouping 8 – Days_ Disch_2_assess: Quartile grouping
YES

177
Table 4.3 Variables Defined (Continued)
Secondary Analysis: Effect of Structural on Process Variables90
Influences on Process and Outcome Dependent Independent
% predicted of dependent and relative contribution of dependent
LOS Race/Ethnicity; Age; Sex; Diagnosis count; Residence
Total PT Charge Amount Race/Ethnicity; Age; Sex; Diagnosis count; Residence
Days_ Disch_2_assess Race/Ethnicity; Age; Sex; Diagnosis count; Residence

178
Table 5.1 Study Sample Characteristics/Donabedian Structural variables by Race/Ethnicity **
Variables Total Study Population
White Black Other Self-identified
Asian Hispanic North American Native
N 21448 20048 (93.47%) 1011 (4.71%) 193 (0.90%) 94 (0.44%) 91 (0.42) 11 (0.05%)
Age Group 65-74 Y.O. 13631 (63.55%) (63.55%) 717 (70.92%) 141(73.06%) 52 (55.32%) 56 (61.54%) ** 75- 84 Y.O. 6969 (32.49%) 6591 (32.88%) 271 (26.81%) 48 (24.87) 32 (34.04%) 23 (25.27%) ** 85 + Y.O. 848 (3.95%) 799 (3.99%) 23 (20.27%) ** 10 (10.64%) 12 (13.19%) Mean 73.06 73.12 71.95 72.89 74.4 74.37 Median 72.00 72.00 71.00 71.50 73.00 72.00 Standard Deviation
5.73 5.73 5.35 5.99 7.17 7.50
Sex Male 9444 (44.03%) 8871(44.25%) 400 (39.56%) 96 (49.74%) 33 (33.67%) 39 (42.86%) ** Female 12004(55.97%) 11177(55.75%) 611 (60.44%) 97 (50.26%) 65 (66.33%) 52 (57.14%) ** Dx Count 0-4 4859 (22.65%) 4538 (22.64%) 238 (23.54%) 38 (19.69%) 23 (24.47%) 19 (20.88%) ** 5 - 7 7098 (33.09%) 6629 (33.07%) 344 (34.03%) 60 (31.09%) 31 (32.98%) 33 (36.26%) ** 8 - 11 6063 (28.27%) 5662 (28.24%) 280 (27.70%) 63 (32.64%) 29 (30.85%) 23 (27.47%) ** 12+ 3428 (15.98 %) 3219 (16.06%) 149 (14.74%) 32 (16.58%) 11 (11.70%) 14 (15.38%) Residence Urban 17909 (83.49%) 16665(83.13%) 896 (88.63%) 169 (87.56%) 87 (92.55%) 82 (90.11%) **
Rural 3541 (16.51%) 3383 (16.87%) 115 (11.37%) 24 (12.44%) 7 (7.45%) 9 (9.89%) **
** Per CMS requirements results with N < 10 are not reported

179
Table 5.1 Study Population Characteristics/Donabedian Structural variables** (Continued)
State ID (selected)
Total Study Population
N (%/study pop)
White N (%/State)
(%/study pop)
Black N (%/State)
(%/study pop)
Other N (%/State)
(%/study pop)
Asian N (%/State)
(%/study pop)
Hispanic (N (%/State)
(%/study pop)
No. American Native
N (%/State) (%/study pop)
N 21448 20048 (93.47%) 1011 (4.71%) 193 (0.90%) 94 (0.44%) 91 (0.42) 11(0.05%)
CA 3616 (16.86%)
3320 (16.56%) (91.81%)
119 (11.77%) (3.29%)
81 (41.97%) (2.24%)
55 (58.51%)(1.52%)
37 (40.66%)(1.02)
**
FL 3543 (16.52%) 3428 (17.10%) (96.75)
70 (6.92%) (1.97%)
25 (12.95%) (0.70%)
** 14 (15.38%)(0.39%)
-----
GA 1113 (5.19%) 965 (4.81%) (86.70%)
137 (13.55%) (12.3%)
** ** ** -----
IL 1504 (7.01%) 1407 (7.02%) (93.55%
81 (8.01%) (5.38%)
** ** ** -----
MI 1491 (6.95%) 1393 (6.95%) (93.42%)
85 (8.41%) (5.70%)
10 (5.18%) (0.67%)
** ** -----
NC 1749 (8.15%) 1570 (7.83%) (89.76%)
157 (15.53%) (8.97%)
13 (6.74%) (8.97%)
** ** **
NY 1566 (7.30%) 1495 (7.46%) (95.46%)
53 (5.24%) (3.38%)
** ** ** **
OH 1285 (5.98%) 1211 (6.04%) (94.46%)
54 (5.34%) (4.21%)
** ** -----
PA 2287 (10.66%) 2207 (11.01%) (96.50%)
65 (6.43%) (2.84%)
12 (6.22%) (0.52%)
** **
**
TX 1770 (8.25%) 1663 (8.30%) (93.95%)
66 (6.53%) (3.72%)
14 (7.25%) (0.79%)
**
22 (24.18%) (1.24%)
VA 1527 (7.12%) 1389 (6.93%) (90.96%)
124 (12.27%) (8.12%)
8 (4.15%) (0.52%)
** ** **
** Per CMS requirements results with N < 10 are not reported

180
Table 5.1 Study Sample Characteristics/Donabedian Structural variables** (Continued)
Socioeconomic Status — 1-Dual Status Medicare/Medicaid Full or Restricted No (0) 20838 (97.16%) 19615 (97.84%) 904 (89.42%) 180 (93.26%) 75 (79.79%) 56 (61.54%) ** Yes (1)
610 (2.84%) 433 (1)2.16 107 (10.58%) 13 (6.74%) 19 (20.21%) 35 (38.46%) **
Socioeconomic Status — 2-CSG Status Dual entry/LIS Full or low Income Subsidy (LIS)
No 20645 (96.26%) 19489 (97.06) 870 (86.05%) 179 (92.75%) 74 (78.72%) 55 (60.44%) ** Yes
803 (3.74%) 589 (2.94) 141 (13.95%) 7.25%) 20 (21.28%) 36 (39.56%) **
** Per CMS requirements results with N < 10 are not reported

181
Table 5.2 Study Sample characteristics: Donabedian Process Variables by Race/Ethnicity
Length of Stay/day count In hospital
Total Study Population N = 21448
White N = 20048
Black N = 1011
Other (Self-identified, Asian, N. American Native) N = 298
Hispanic N = 91
Mean 2.90 2.89 3.05 3.00 3.19
Median 3.0 3.0 3 3.00 3
Standard Deviation 1.84 1.68 1.30 1.71 1.56
Hospital PT charge amount ($)
Mean 1405.89 1407.97 1310.31 1510.05 1667.98
Median 1179.00 1184.00 1110.00 1190.50 1413.00
Standard Deviation 1020 1012 978.89 1391 1552
Days Hospital Discharge – Home Health Agency Discharge
Mean 22.63 22.47 25.09 23.27 28.96
Median 20.00 20.00 23.00 20.00 24.00
Standard Deviation 10.77 10.67 11.56 11.48 16.19

182
Table 5.3.1 Study Sample characteristics: Donabedian Transfer Ability Outcome Variable by Race/Ethnicity**
Current Transfer Ability
Total Study Population N = 21448
White N = 20048
Black N = 1011
Other N = 298
Hispanic N = 91
00 : transfers independently
14821 (69.10%)
13943 (69.55%) 629 (62.22%) 199 (66.77%) 50 (54.95%)
01: transfers with minimal human assistance or with use of an assistive device
6541 (30.50%)
6029 (30.07%) 377 (37.29%) 97 (32.55%) 38 (41.76%)
02: bear weight and pivot during the transfer but unable to transfer self.
74 (0.35%) 65 (0.32%) ** ** **
03: Unable to transfer self and is unable to bear weight or pivot when transferred by another person
** ** 0 (0.00%) 0 **
04: Bedfast, unable to transfer but is able to turn and position self in bed
** ** 0 (0.00%) 0 0 (0.00%)
05: Bedfast, unable to transfer and is unable to turn and position self
2 ( 0.01%) 2 (0.01%) 0 (0.00%) 0 0 (0.00%)
NOTE: “Other” = Self-identified as other, Asian, and North American Native ** Per CMS requirements results with N < 10 are not reported

183
Table 5.3.2 Study Sample characteristics: Donabedian Ambulation/Locomotion Outcome Variable by Race/Ethnicity**
Note: “Other” = self-identified as other, Asian, of North American Native ** Per CMS requirements results with N < 10 are not reported
Current Ability Ambulation/Locomotion
Total Study Population N = 21448
White N = 20048
Black N = 1011
Other N = 298
Hispanic N = 91
00 : independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
4174 (19.46%) 3988 (19.89%)
130 (12.86%)
44 (14.77%)
12 (13.18%)
01: Ambulates with use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
11926 (55.60%) 11148 (55.61%)
587 (58.06%)
156 (52.35%)
35 (38.46%)
02: Requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces
5186 (24.18%) 4764 (23.67%)
288 (28.49%)
95 (31.88%
39 (42.85%)
03: Able to walk only with the supervision or assistance of another person at all times
154 (0.72%)
141 (0.70 %)
** ** **
04: Chairfast, unable to ambulate but is able to wheel self independently
** ** ** 0 0
05: Chairfast, unable to ambulate and is unable to wheel self
** ** 0 0 0
06: Bedfast, unable to ambulate or be up in a chair
** ** 0 0 0

184
Table 5.4 .1 Functional Outcome Measures and Race/Ethnicity: Transfer & Ambulation/Locomotion
Transfer N (%) p-value* 0.0080*
Ambulation/Locomotion p-value* <.0001 Race Independent Dependent Independent Dependent
White N = 20048
19972 (99.62%) 76 (0.38%) 15136 (75.50%) 4912 (24.50%)
Black N = 1011
1006 (99.51%) ** 717 (70.92%) 294 (29.08%)
Hispanic N = 91
88 (96.70%) ** 47 (51.65%) 44 (48.35%)
Other: Self-identified, Asian & No. American Native N = 298
296 (99.33%) ** 200 (67.11%) 98 (32.89%)
TOTAL: 21,448
21,362 (99.60%) 86 (.40%) 16,100 (75.07%) 5,348 (24.93%)
*Fisher’s Exact Test ** Per CMS requirements results with N < 10 are not reported
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times. 04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

185
Table 5.4.2 Functional Outcome Measures, (Transfer & Ambulation/Locomotion) by Age
Transfer N (%) p-value* 0.0553
Ambulation/Locomotion p-value* <.0001 Age Independent Dependent Independent Dependent
65 -74 years of age 13587 (99.68%) 44 (0.32%) 10526 (77.22%) 3105 (22.78%)
75 84 years of age 6932 (99.47%) 37 (0.53%) 5046 (72.41%) 1923 (27.59%)
85 + years of age 843 (99.41%) ** 528 (62.26%) 320 (37.74%) *Fisher’s Exact Test ** Per CMS requirements results with N < 10 are not reported
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

186
Table 5.4.3 Functional Outcome Measures, (Transfer & Ambulation/Locomotion) by Gender
Transfer N (%) p-value* 0.3999
Ambulation/Locomotion p-value <.0001 Gender Independent Dependent Independent Dependent
Male 9410 (99.64%) 34 (0.36%) 7478 (79.18%) 1966 (20.82%) Female 11952 (99.57%) 52 (0.43%) 8622 (71.83%) 3382 (28.17%)
*Fisher’s Exact Test
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

187
Table 5.4.4 Functional Outcome Measures, (Transfer & Ambulation/Locomotion) by Comorbidities
Transfer N (%) p-value* 0.3978
Ambulation/Locomotion p-value* <.0001 Diagnosis Count Independent Dependent Independent Dependent
0 - 4 4845 (99.71) 14 (0.29) 0 - 4 4845 (99.71)
5 - 7 7071 (99.62) 27 (0.38) 5 - 7 7071 (99.62)
8 - 11
6035 (99.54)
28 (0.46) 8 – 11
6035 (99.54)
12 + 3411 (99.50} 17 (0.50) 0 - 4 4845 (99.71)
*Fisher’s Exact Test
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

188
Table 5.4.5 Functional Outcome Measures, Rural/Urban
Transfer N (%) p-value* 0.4149
Ambulation/Locomotion p-value* 0.0003 Rural/Urban Independent Dependent Independent Dependent
Urban 17838 (99.61%) 69 (0.39%) 13527 (75.54%) 4380 (24.46%) Rural 3524 (99.52%) 17 (0.48%) 2573 (72.66%) 968 (27.34%)
*Fisher’s Exact Test Transfer Ability
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

189
Table 5.4. 6 Functional Outcome Measures, (Transfer & Ambulation/Locomotion) by Socioeconomic Status
Transfer N (%) p-value* 0.3978
Ambulation/Locomotion p-value* <.0001 SES Indepen
dent Dependent Independent Dependent
Dual Status (Full or Restricted Medicaid)-No
20760 (99.63%)
78 (0.37 %) 15717 (75.42%) 5152 (24.58%)
Dual Status (Full or Restricted Medicaid)-Yes
602 (98.69%)
8 (1.31 %) 383 (62.79%) 227 (37.21%)
p-value* 0.0152
p-value* <.0001
Cost Share Group (Full dual entry or low income subsidy) - No
20567 (99.62%)
78 (0.38%) 15587 (75.50%) 5058 (24.50%)
Cost Share Group (Full dual entry or low income subsidy) - Yes
795 (99.00%)
8 (1.00%) 513 (63.89%) 290 (36.11%)
*Fisher’s Exact Test
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

190
Table 5.4.7 Functional Outcome Measures, (Transfer & Ambulation/Locomotion) by Length of Stay
Transfer N (%) p-value* <.0001
Ambulation/Locomotion p-value* <.0001 Length of Stay Independent Dependent Independent Dependent
1st Quartile
7223 (99.79) 15 (0.21)
5811 (80.28) 1427 (19.72)
2nd Quartile 10459 (99.63) 39 (0.37) 7766 (73.98) 2732 (26.02) 3rd Quartile 2464 (99.12) 22 (0.88) 1718 (69.11) 768 (30.89) 4th Quartile 1216 (99.18) 12 (0.82) 805 (65.66) 421 (34.34)
*Fisher’s Exact Test
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

191
Table 5.4.8 Functional Outcome Measures (Transfer & Ambulation/Locomotion) by Physical Therapy Charge in Acute Care Hospital
Transfer N (%) p-value* 0.0036
Ambulation/Locomotion p-value* <0.0114 Physical Therapy
Charge Amount ($) Independent Dependent
Independent Dependent
1st Quartile: $0- 754
5386 (99.78) 12 (0.22)
4015 (74.38) 1383 (25.62)
2nd Quartile: $755 - 1179
4856 (99.63) 18 (0.37)
3705 (76.02) 1169 (23.98)
3rd Quartile: $1180- 1771
5838 (99.64) 21 (0.36)
4455 (73.04) 1404 (23.96)
4th Quartile: $1772 -15,740
5282 (99.34) 35 (0.66)
3925 (73.82) 1392 (26.18)
*Fisher’s Exact Test
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

192
Table 5.4.9 Functional Outcome Measures (Transfer & Ambulation/Locomotion) by Number of Days to Discharge Assessment from Home Health Agency
Transfer N (%) p-value* 0.0006
Ambulation/Locomotion p-value* <0.0001 Number of Days to
Discharge Assessment Independent Dependent
Independent Dependent
1st Quartile: 0 – 15 days
6987 (99.50) 35 (0.50)
4676 (66.59) 2346 (33.41)
2nd Quartile: 16-30 days
5802 (99.74) 15 (0.26)
4521 (77.72) 1296 (22.28)
3rd Quartile: 31 -45 days
4843 (99.79) 10 (0.21)
3925 (80.88) 928 (19.12)
4th Quartile: 46 -60 days
3730 (99.31) 26 (0.69)
2978 (79.29) 778 (20.71)
*Fisher’s Exact Test
Transfer Ability Independent
00= Able to independently transfer. 01 = Able to transfer with minimal human
assistance or with use of an assistive device. Dependent
02 = Able to bear weight and pivot during the transfer but unable to transfer self.
03 = Unable to transfer self, to bear weight or pivot when transferred by another person.
04 = Bedfast, unable to transfer but is able to turn and position self in bed.
05 = Bedfast, unable to transfer and is unable to turn and position self.
Ambulation/locomotion Ability Independent
00 = Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
01 = With the use of a one-handed assistive device able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
Dependent 02 = requires use of a two-handed device (e.g., walker or crutches) to walk alone on a
level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
03 = Able to walk only with the supervision or assistance of another person at all times.
04 = Chairfast, unable to ambulate but is able to wheel self independently. 05 = Chairfast, unable to ambulate and is unable to wheel self. 06 = Bedfast, unable to ambulate or be up in a chair.

193
Table 5.5 Odds Ratio Estimate – Transfer Status: Crude, Adjusted & Relative Importance
**LOHHC - Length of home health care services equals the number of days from hospital discharge to discharge from home health care.
Variables Crude Odds Ratio
(95% Confidence Limits)Adjusted Odds Ratio
(95% Confidence Limits)
Relative Importance (amount of weight/variable
on Transfer status)
Race/Ethnicity Reference = White
Black 1.306 (0.527, 3.235) 1.23 (0.496, 3.167) * Hispanic 8.959 (2.774, 28.939) 5.201 ( 1.424, 18.989) 3.06%
Other 1.776 (0.434, 7.263) 1.621 (0.389, 6.754) * Age Groups
Reference = 85+
65 – 74 vs 85+ 0.546 (0.216, 1.380) 0.680 (0.264, 1.751) * 75 – 84 vs 85+ 0.900 (0.353, 2.296) 1.040 (0.403, 2.683) *
Gender Reference = Male
Female 1.204 (0.781, 1.857) 1.132 (0.729, 1.758) * Residential Location
Reference = Urban
Rural Area 1.247 (0.733, 2.123) 1.399 (0.811, 2.413) * Comorbidities
Reference = 12+
0 – 4 0.580 (0.285, 1.178) 0.774 (0.372, 1.611) * 5 -7 0.766 (0.285, 1.178) 0.947 (0.507, 1.767) *
8 – 11 0.931 (0.509, 1.703) 1.049 (0.569, 1.934) * Continuous 1.042 (0.993, 1.093)
**LOHHC Reference = 1st Quartile 1-15 days
16 – 30 (2nd Quartile) 0.516 (0.282, 0.946) 0.440 (0.239, 0.810) -0.2011 (10.44%) 31 – 45 (3rd Quartile) 0.412 (0.204. 0.833) 0.322 (0.158, 0.656) -0.2614 (13.57%) 46 – 60 ( 4th Quartile) 1.392 (0.837, 2.315) 0.871 (0.508, 1.492) * PT Charge Amount $
Reference = 1st Quartile $0 - 754
2nd Quartile $755 – 1179) 1.664 (0.801, 3.457) 1.539 (0.734, 3.227) *
3rd Quartile $ 1180 - 1771 1.614 (0.794, 3.284) 1.438 (0.694, 2.980) *
4th Quartile $ 1772 – 15,740
2.974 (1.524, 5.735) 2.236 (1.116, 4.478) 0.1915 (9.94%)
Hospital Length of Stay Reference = 0-6
2nd Quartile 7 – 12days 1.796 (0.989, 3.259) 1.522 (0.823, 2.813) * 3rd Quartile 13 - 18 days 4.299 (2.227, 8.301) 3.118 (1.543, 6.300) 0.2007 (10.42%)
4th Quartile 19-24 days 3.960 (1.775, 8.835) 2.482 (1.038, 5.936) 0.1164 (6.04%)

194
Table 5.5 Odds Ratio Estimate – Transfer Status: Crude, Adjusted & Relative Importance (Continued)
Variables Crude Odds Ratio
(95% Confidence Limits)
Adjusted Odds Ratio
(95% Confidence Limits)
Relative Importance (amount of weight/variable
on Transfer status)
Socioeconomic Status Reference : Medicare
Only
Dual Status (Medicare & Medicaid) 3.539 (1.702, 7.358) 7.478 (0.473, 118.141)
Cost Share Group (Low Income Subsidy) 2.653 (1.277, 5.512) 0.282 (0.018, 4.453)

195
Table 5.6 Multinomial Logistic Regression Odds Ration for Transfer Ability: Reference = Independent
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Race/Ethnicity Comorbidity Count Reference = 12+
Black – Moderate -total Dependence
1.417 (0.560, 3.583) 0 – 4 Moderate -total Dependence
0.682 (0.328, 1.420)
Black – Minimal Dependence
1.386 (1.211,1.585) 0 – 4 Minimal Dependence
0.697 (0.632, 0.769)
Hispanic Moderate -total Dependence
6.155 (1.665, 22.753) 5 -7 Moderate -total Dependence
0.866 (0.464, 1.617)
Hispanic Minimal Dependence
1.516 (0.982, 2.339) 5 – 7 Minimal Dependence
0.784 (0.717, 0.857)
Other Moderate -total Dependence
1.677 (0.401, 7.009) 8 – 11 Moderate -total Dependence
0.981 (0.523, 1.811)
Other Minimal Dependence
1.108 (0.865, 1.421) 8 – 11 Minimal Dependence
0.838 (0.766, 0.917)
Age Groups
Days Acute Hospital Discharge – to Home Health Agency Discharge (days) Reference = 1st Quartile 1-15 days
65 – 74 vs 85+ Moderate -total Dependence
0.611 (0.237, 1.576) 16 – 30 (2nd Quartile) Moderate -total Dependence
0.390 (0.212, 0.717)
65 – 74 vs 85+ Minimal Dependence
0.748 (0.645, 0.868) 16 – 30 (2nd Quartile) Minimal Dependence
0.707 (0.655, 0.763)
75 – 84 vs 85+ Moderate -total Dependence
0.963 (0.373, 2.489) 31 – 45 (3rd Quartile) Moderate -total Dependence
0.272 (0.133, 0.554)
75 – 84 vs 85+ Minimal Dependence
0.816 (0.701, 0.949) 31 – 45 (3rd Quartile) Minimal Dependence
0.610 (0.562, 0.663)
Gender 46 – 60 ( 4th Quartile) Moderate -total Dependence
0.736 (0.428, 1.264)
Female Moderate -total Dependence
1.201 (0.773, 1.866) 46 – 60 ( 4th Quartile) Minimal Dependence
0.622 (0.568. 0.680)
Female Minimal Dependence
1.188 (1.119, 1.262)
Residential Location Reference = Urban
Rural Area Moderate -total Dependence
1.467 (0.850, 2.532)
Rural Area Minimal Dependence
1.143 (1.055, 1.238)

196
Table 5.6 Multinomial Logistic Regression Odds Ration for Transfer Ability: Reference = Independent (Continued)
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Physical Therapy Charge Amount: Acute Care Hospital Stay ($) Reference = 1st Quartile $0 - 754
Socioeconomic Status
2nd Quartile $755 – 1179) Moderate -total Dependence
1.520 (0.724, 3.187)
Dual Status (Medicare & Medicaid) Moderate -total Dependence
8.184 (0.521, 128.502)
2 Quartile $755 – 1179 Minimal Dependence
0.970 (0.890, 1.057) Dual Status (Medicare & Medicaid) Minimal Dependence
1.261 (0.906, 1.757)
3rd Quartile $ 1180 – 1771 Moderate -total Dependence
1.427 (0.688, 2.959)
Cost Share Group (Low Income Subsidy) Moderate -total Dependence
0.305 (0.019, 4.765)
3rd Quartile $ 1180 – 1771 Minimal Dependence
0.980 (0.901, 1.066) Cost Share Group (Low Income Subsidy) Minimal Dependence
1.195 (0.892, 1.600)
4th Quartile $ 1772 – 15,740 Moderate -total Dependence
2.17 (1.085, 4.359)
4th Quartile $ 1772 – 15,740 Minimal Dependence
0.926 (0.848, 1.012)
Hospital Length of Stay 2nd Quartile 0 – 3 days Moderate -total Dependence
1.641 (0.887, 3.036)
2nd Quartile 0 – 3 days Minimal Dependence
1.272 (1.186, 1.364)
3rd Quartile 0 - 3 days Moderate -total Dependence
3.537 (1.748, 7.155)
3rd Quartile 0 - 3 days Minimal Dependence
1.471 (1.325, 1.632)
4th Quartile 3 – 24 days Moderate -total Dependence
3.141 (1.311, 7.525)
4th Quartile 3 – 24 Minimal Dependence
1.931 (1.686, 2.211)

197
Table 5.7 Multinomial Logistic Regression Odds Ratio for Transfer Ability: Reference = Minimal Dependence
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Race/Ethnicity Comorbidity Count Reference = 12+
Black – Moderate -total Dependence
1.023 (0.404, 2.592) 0 – 4 Moderate -total Dependence
0.979 (0.469, 2.040)
Black – Independent
0.722 (0.631, 0.826) 0 – 4 Independent
1.434 (1.301, 1.581)
Hispanic Moderate -total Dependence
4.061 (1.093, 15.087) 5 -7 Moderate -total Dependence
1.104 (0.590, 2.066)
Hispanic Independent
0.660 (0.428, 1.018) 5 – 7 Independent
1.275 (1.167, 1.394)
Other Moderate -total Dependence
1.513 (0.360, 6.360) 8 – 11 Moderate -total Dependence
1.171 (0.633, 2.164)
Other Independent
0.902 (0.704, 1.157) 8 – 11 Independent
1.193 (1.090, 1.305)
Age Groups
Days Acute Hospital Discharge – to Home Health Agency Discharge (days) Reference = 1st Quartile 1-15 days
65 – 74 vs 85+ Moderate -total Dependence
0.817 (0.316, 2.111) 16 – 30 (2nd Quartile) Moderate -total Dependence
0.551 (0.299, 1.0160
65 – 74 vs 85+ Independent
1.336 (1.152, 1.549) 16 – 30 (2nd Quartile) Independent
1.414 (1.310, 1.526)
75 – 84 vs 85+ Moderate -total Dependence
1.181 (0.456, 3.059) 31 – 45 (3rd Quartile) Moderate -total Dependence
0.445 (0.218, 0.910)
75 – 84 vs 85+ independent
1.226 (1.054, 1.427) 31 – 45 (3rd Quartile) Independent
1.639 (1.509,1.779)
Gender 46 – 60 ( 4th Quartile) Moderate -total Dependence
1.184 (0.687, 2.038)
Female Moderate -total Dependence
1.011 (0.650, 1.573) 46 – 60 ( 4th Quartile Independent
1.608 (1.470, 1.760)
Female Independent
0.842 (0.792, 0.894)
Residential Location: Reference = Urban
Rural Area Moderate -total Dependence
1.284 (0.743, 2.219)
Rural Area Independent
0.875 (0.808,0.948)

198
Table 5.7 Multinomial Logistic Regression Odds Ratio for Transfer Ability: Reference = Minimal Dependence (Continued)
Variables
Odds Ratio 95% Confidence Limits Variables
Odds Ratio 95% Confidence Limits
Physical Therapy Charge Amount: Acute Care Hospital Stay ($) Reference = 1st Quartile $0 - 754
Socioeconomic Status
2nd Quartile $755 – 1179) Moderate -total Dependence
1.567 (0.746, 3.292)
Dual Status (Medicare & Medicaid) Moderate -total Dependence
6.48, (0.411, 102.304)
2 Quartile $755 – 1179 Independent
1.031 (0.946, 1.124) Dual Status (Medicare & Medicaid) Independent
0.793 (0.569, 1.104)
3rd Quartile $ 1180 – 1771 Moderate -total Dependence
1.456 (0.701, 3.024)
Cost Share Group (Low Income Subsidy) Moderate -total Dependence
0.255 (0.016, 4.002)
3rd Quartile $ 1180 – 1771 Independent
1.020 (0.938, 1.110) Cost Share Group (Low Income Subsidy) Independent
0.837 (0.625, 1.121)
4th Quartile $ 1772 – 15,740 Moderate -total Dependence
2.348 (1.169, 4.715)
4th Quartile $ 1772 – 15,740 Independent
1.080 (0.988, 1.180)
Hospital Length of Stay 2nd Quartile 0 – 3 days Moderate -total Dependence
1.291 (0.697, 2.391)
2nd Quartile 0 – 3 days Independent
0.786 (0.733, 0.843)
3rd Quartile 0 - 3 days Moderate -total Dependence
2.405 (1.186, 4.877)
3rd Quartile 0 - 3 days Independent
0.680 (0.613, 0.755)
4th Quartile 3 – 24 days Moderate -total Dependence
1.67 (0.678, 3.905)
4th Quartile 3 – 24 Independent
0.518 (0.452, 0.593)

199
Table 5.8 Odds Ratios Estimate (Crude and Adjusted) for Ambulation/Locomotion: by Donabedian Structure and Process Variables
Variables Crude Odds Ratio 95% Confidence Limits
Adjusted Odds Ratio 95% Confidence Limits
Relative Importance (amount of weight/variable on Ambulation/Locomotion status)
Race/Ethnicity Reference = White
Black 1.264 (1.099, 1.453) 1.333 (1.152, 1.544) 0.0336 2.04% Hispanic 2.882 (1.908, 4.353) 2.575 (1.668, 3.975) 0.0339 2.06% Other 1.510 (1.183, 1.927) 1.538 (1.193, 1.982) 0.0278 1.69%
Age Groups Reference = 85+
65 – 74 vs 85+ 0.486 (0.421, 0.562) 0.459 (0.395, 0.534) 0% significant: non-measurable effect
75 – 84 vs 85+ 0.628 (0.542, 0.729) 0.599 (0.514, 0.699) 0% significant: non-measurable effect Gender: Reference = Male Female 1.492 (1.400, 1.590) 1.582 (1.481, 1.691) 0.1256 7.64% Residential Location Reference = Urban
Rural Area 1.162 (1.071, 1.260) 1.283 (1.178, 1.398) 0.0511 3.11% Comorbidities (Dx Count) Reference = 12+
0 - 4 0.534 (0.486, 0.594) 0.549 (0.494, 0.610) -0.1384 8.42% 5 -7 0.658 (0.601, 0.720) 0.668 (0.608, 0.735) -0.1045 6.36% 8 – 11 0.775 ( 0.707, 0.849) 0.777 (0.707, 0.855) -0.0625 3.80%

200
Table 5.8 Odds Ratios Estimate ( Crude and Adjusted )for Ambulation/Locomotion: by Donabedian Structure and Process Variables (Continued)
Variables Crude Odds Ratio 95% Confidence Limits
Adjusted Odds Ratio 95% Confidence Limits
Relative Importance (amount of weight/variable on Ambulation/Locomotion status)
Days Acute Hospital Discharge – to H H A Discharge (days) Reference = 1st Quartile 1-15
16 – 30 (2nd Quartile) 0.571 (0.528, 0.618) 0.495 (0.456, 0.537) -0.1724 10.68% 31 – 45 (3rd Quartile) 0.471 (0.432, 0.514) 0.378 (0.345, 0.414) -0.2246 13.67% 46 – 60 ( 4th Quartile) 0.521 (0.471, 0.572) 0.358 (0.324, 0.396) -0.2150 13.09% Physical Therapy Charge Amount Acute Care Hospital Stay ($) Reference = 1st quartile ($0-754)
2nd Quartile $755 – 1179) 0.916 (0.837, 1.002) 0.891 ( 0.811, 0.979) -0.0266 1.61% 3rd Quartile $ 1180 - 1771 0.915 (0.840, 0.997) 0.875 (0.798, 0.959) -0.0329 2.00% 4th Quartile $ 1772 – 15,740 1.030 (0.944, 1.123) 0.902 (0.820, 0.993) -0.0245 1.19% Hospital Length of Stay Reference = 1st Quartile
2nd Quartile 0 – 3 days 1.432 (1.332, 1.540) 1.502 (1.390, 1.623) 0.1121 6.82% 3rd Quartile 0 - 3 days 1.820 (1.642, 2.018) 1.853 (1.657, 2.072) 0.1088 6.62% 4th Quartile 3 – 24 days 2.130 ( 1.868, 2.429) 2.130 (1.842, 2.463) 0.0968 5.89% Socioeconomic Status Reference =Medicare only
Dual Status (Medicare & Medicaid)
1.820 (1.540, 2.151) 1.171 (0.828, 1.656)* 0.0145 0.883%
Cost Share Group (Low Income Subsidy)
1.743 (1.504, 2.020 1.417 (1.043, 1.923) 0.0364 2.21%
* = Not Significant ** = Negative Standardized Estimate (negative effect)

201
Table 5.9 Impact of Independent Structure Variables on Physical Therapy Charge Amount Process Dependent Variable
Variable Regression Coefficient P- Value Relative Importance Race: Reference (White) Black/African American -112.78030 0.0006 -0.02343 (8 %) Hispanic 184.91952 0.0855 0.01178 (4 %) Other 76.73917 0.1949 0.00881 (3.%) Age (No Reference) 8.80304 <.0001 0.04950 (18.%) Gender: Reference (Male) Female 32.80819 0.0187 0.01597 (5.%) Geographic Location: Reference (Urban)
Rural -274.86195 <.0001 -0.10004 (36.%) Comorbidity Count (No reference) 11.20715 <.0001 0.04460 (16.%) Socioeconomic Status Dual Status: Full or Restricted 114.61237 0.1588 0.01868 (6.%) Cost Share Group: full Dual or Low Income subsidy
7.36602 0.9176 0.00137 (4.%)

202
Table 5.10 Impact of Independent Structure Variables on Length of Hospital Stay Process Dependent Variable
Variable Regression Coefficient p-value Relative Importance Race: Reference (White) Black/African American 2.38117 <.0001 0.04683 (8.96%) Hispanic 4.43093 <.0001 0.02672 (5.12%) Other 0.45790 <.0001 0.00497 (0.95%) Age (No Reference) 0.19930 <.0001 0.10609 (20.31%) Gender: Reference (Male) Female 1.82191 <.0001 0.08393 (16.07%) Geographic Location: Reference (Urban)
Rural 2.34243 <.0001 0.08070 (15.45%) Comorbidity Count (No reference) 0.21779 <.0001 0.08204 (15.70%) Socioeconomic Status Dual Status: Full or Restricted 1.31899 0.1191 0.02035 (3.89%)
Cost Share Group: full Dual or Low Income subsidy
4.00795 <.0001 0.07060 (13.51%)

203
Table 5.11 Impact of Independent Structure Variables on Length of Home Health Care Process Dependent Variable ****
****Length of home health care process equals the number of days from hospital discharge to discharge from home health care.
Variable Regression Coefficient p-value Relative Importance Race: Reference (White) Black/African American 2.38117 <.0001 0.04683 (8.96%) Hispanic 4.43093 <.0001 0.02672 (5.12%) Other 0.45790 <.0001 0.00497 (0.95%) Age (No Reference) 0.19930 <.0001 0.10609 (20.31%) Gender: Reference (Male) Female 1.82191 <.0001 0.08393 (16.07%) Geographic Location: Reference (Urban)
Rural 2.34243 <.0001 0.08070 (15.45%) Comorbidity Count (No reference) 0.21779 <.0001 0.08204 (15.70%) Socioeconomic Status Dual Status: Full or Restricted 1.31899 0.1191 0.02035 (3.89%)
Cost Share Group: full Dual or Low Income subsidy
4.00795 <.0001 0.07060 (13.51%)

Version 09/22/2015
Date:Requestor Name:
Requestor Institution:Study Title:
Check to request Variable Name and Location Not in CCW Use in Analysis
X HHA Assessment ID CMS Recommended Variable Original Assessment ID HHA Item Subset Code * HHA Submission ID *
X Facility Internal ID CMS Recommended VariableX Resident Internal ID * CMS Recommended VariableX State Code CMS Recommended Variable
X Submission Date
CMS Recommended Variable CMS assessments can be extracted based on either effective date or submission date.
HHA Submission Day *
X Effective Date
CMS Recommended Variable CMS assessments can be extracted based on either effective date or submission date.
Agency Document ID Code * Calculated Birth Date Submit Code Calculated CMS Certification Number (CCN) * Calculated Patient Age Number * Correction Number Create Timestamp * Create User ID * Item Set Version Code * HHA Correction Status Code * Processed Timestamp * Resident Match Criteria ID Software Product Name * Software Product Version Code
*** ATTENTION: This is the variable list for OASIS-C, implemented on 1/1/2010. Variable numbers in ( ) indicate previously established fields, e.g. (M0010). Some variables contain 2 numbers- one without ( ) and one with ( )- e.g. M1005 (M0180), indicating a new variable "M1005" similar to a past (no longer existing) variable "M0180." For further details, please refer to the user manual found at: http://www.cms.gov/HomeHealthQualityInits/14_HHQIOASISUserManual.asp
Directions: Indicate variables to include in the ouput and justify the need for each. For variable definitions see the OASIS data dictionary. Bolded variables indicate CMS recommended variables.
OASIS C Workbench Variable Selection & Justification Worksheet
204

Software Vendor ID CMS WILL NOT RELEASE Specification Version Code * Submitted HIPPS Code Submitted HIPPS Version Code Calculated HIPPS Code Calculated HIPPS Version Code Transaction Type Code * Update Timestamp Update User ID * M0010 CMS Certification Number (CCN) M0014 Branch State Code M0016 Branch ID M0018 NPI Physician ID M0018 NPI Physician ID Unknown M0020 Patient ID * M0030 Start of Care Date M0032 Resumption of Care Date M0032 Resumption of Care Date NA M0040 Patient First Name * CMS WILL NOT RELEASE M0040 Patient Last Name * CMS WILL NOT RELEASE M0040 Patient Middle Initial * M0040 Patient Suffix * M0050 Patient State of Residence M0060 Patient ZIP Code M0063 Patient Medicare Number * M0063 Patient No Medicare Number M0064 Patient Social Security Number * M0064 Patient Social Security Number Unknown M0065 Patient Medicaid Number * M0065 Patient Medicaid Number NA M0066 Patient Birth Date M0069 Patient Gender M0080 Discipline of Person Completing Assessment M0090 Date Assessment Completed M0100 Reason for Assessment M0102 Physician Ordered SOC or ROC Date M0102 Physician Ordered SOC or ROC Date NA M0104 Date Of Referral M0110 Episode Timing M0140 Race/Ethnicity: American Indian or Alaskan Native
205

M0140 Race/Ethnicity: Asian M0140 Race/Ethnicity: Black or African-American M0140 Race/Ethnicity: Hispanic or Latino M0140 Race/Ethnicity: Native Hawaiian or Other Pacific Islander M0140 Race/Ethnicity: White M0150 Medicaid Fee For Service Payment M0150 Medicaid HMO/Managed Care Payment M0150 Medicare Fee For Service Payment M0150 Medicare HMO/Managed Care Payment M0150 No Payment M0150 Other Government Payment M0150 Other Payment Source M0150 Private HMO/Managed Care Payment M0150 Private Insurance Payment M0150 Self-Pay Payment M0150 Title Programs Payment M0150 Unknown Payment Source M0150 Workers Compensation Payment M0903 Date of Last Home Visit M0906 Discharge/Transfer/Death Date M1000 Discharged Past 14 Days From LTCH M1000 Inpatient Discharge from IRF M1000 Inpatient Discharge from Nursing Facility M1000 Inpatient Discharge from Other M1000 Inpatient Discharge from Psychiatric Hospital Or Unit M1000 Inpatient Discharge from Short Stay Acute Hospital M1000 Inpatient Discharge from SNF/TCU Facility M1000 No Inpatient Discharge M1005 Inpatient Discharge Date Unknown M1005 Most Recent Inpatient Discharge Date M1010 Inpatient Diagnosis 1 ICD-9 CD M1010 Inpatient Diagnosis 2 ICD-9 CD M1010 Inpatient Diagnosis 3 ICD-9 CD M1010 Inpatient Diagnosis 4 ICD-9 CD M1010 Inpatient Diagnosis 5 ICD-9 CD M1010 Inpatient Diagnosis 6 ICD-9 CD M1011 Inpatient Diagnosis 1 ICD-10-C M * M1011 Inpatient Diagnosis 2 ICD-10-C M * M1011 Inpatient Diagnosis 3 ICD-10-C M * M1011 Inpatient Diagnosis 4 ICD-10-C M *
206

M1011 Inpatient Diagnosis 5 ICD-10-C M * M1011 Inpatient Diagnosis 6 ICD-10-C M * M1011 Inpatient Diagnosis ICD-10-C M Not Applicable * M1012 Inpatient Procedure 1 ICD-9 M1012 Inpatient Procedure 2 ICD-9 M1012 Inpatient Procedure 3 ICD-9 M1012 Inpatient Procedure 4 ICD-9 M1012 Inpatient Procedure ICD-9 Not Applicable M1012 Inpatient Procedure ICD-9 Unknown M1016 Regimen Change - Diagnosis 1 ICD-9 M1016 Regimen Change - Diagnosis 2 ICD-9 M1016 Regimen Change - Diagnosis 3 ICD-9 M1016 Regimen Change - Diagnosis 4 ICD-9 M1016 Regimen Change - Diagnosis 5 ICD-9 M1016 Regimen Change - Diagnosis 6 ICD-9 M1016 Regimen Change - Not Applicable ICD-9 Code M1017 Regimen Change - Diagnosis 1 ICD-10-C M * M1017 Regimen Change - Diagnosis 2 ICD-10-C M * M1017 Regimen Change - Diagnosis 3 ICD-10-C M * M1017 Regimen Change - Diagnosis 4 ICD-10-C M * M1017 Regimen Change - Diagnosis 5 ICD-10-C M * M1017 Regimen Change - Diagnosis 6 ICD-10-C M * M1017 Regimen Change - Not Applicable ICD-10-C M Code * M1018 Prior Condition - Disruptive Behavior M1018 Prior Condition - Impaired Decision-Making M1018 Prior Condition - Indwelling/Suprapubic Catheter M1018 Prior Condition - Intractable Pain M1018 Prior Condition - Memory Loss M1018 Prior Condition - None of the Above M1018 Prior Condition - Not Applicable M1018 Prior Condition - Unknown M1018 Prior Condition - Urinary Incontinence M1020 Primary Diagnosis ICD-9 Code M1020 Primary Severity Rating ICD-9 Code M1021 Primary Diagnosis ICD-10-C M Code * M1021 Primary Diagnosis Severity Rating ICD-10-C M Code * M1022 Other Diagnosis Code 1 ICD-9 M1022 Other Diagnosis Code 1 Severity ICD-9 M1022 Other Diagnosis Code 2 ICD-9 M1022 Other Diagnosis Code 2 Severity ICD-9
207

M1022 Other Diagnosis Code 3 ICD-9 M1022 Other Diagnosis Code 3 Severity ICD-9 M1022 Other Diagnosis Code 4 ICD-9 M1022 Other Diagnosis Code 4 Severity ICD-9 M1022 Other Diagnosis Code 5 ICD-9 M1022 Other Diagnosis Code 5 Severity ICD-9 M1023 Other Diagnosis Code 1 ICD-10-C M * M1023 Other Diagnosis Code 1 Severity ICD-10-C M * M1023 Other Diagnosis Code 2 ICD-10-C M * M1023 Other Diagnosis Code 2 Severity ICD-10-C M * M1023 Other Diagnosis Code 3 ICD-10-C M * M1023 Other Diagnosis Code 3 Severity ICD-10-C M * M1023 Other Diagnosis Code 4 ICD-10-C M * M1023 Other Diagnosis Code 4 Severity ICD-10-C M * M1023 Other Diagnosis Code 5 ICD-10-C M * M1023 Other Diagnosis Code 5 Severity ICD-10-C M * M1024 ICD-9 Case Mix Diagnosis: Primary, Column 3 M1024 ICD-9 Case Mix Diagnosis: Primary, Column 4 M1024 Other Payment Diagnosis 1 Multiple ICD-9 Code * M1024 Other Payment Diagnosis 2 Multiple ICD-9 Code * M1024 Other Payment Diagnosis 3 Multiple ICD-9 Code * M1024 Other Payment Diagnosis 4 Multiple ICD-9 Code * M1024 Other Payment Diagnosis 5 Multiple ICD-9 Code * M1024 Other Payment Primary Diagnosis 1 Code * M1024 Other Payment Primary Diagnosis 2 Code * M1024 Other Payment Primary Diagnosis 3 Code * M1024 Other Payment Primary Diagnosis 4 Code * M1024 Other Payment Primary Diagnosis 5 Code * M1025 Optional Diagnosis Code 1 ICD-10-C M * M1025 Optional Diagnosis Code 2 ICD-10-C M * M1025 Optional Diagnosis Code 3 ICD-10-C M * M1025 Optional Diagnosis Code 4 ICD-10-C M * M1025 Optional Diagnosis Code 5 ICD-10-C M * M1025 Primary Optional Diagnosis ICD-10-C M Code * M1025 Optional Diagnosis Multiple Code 1 ICD-10-C M * M1025 Optional Diagnosis Multiple Code 2 ICD-10-C M * M1025 Optional Diagnosis Multiple Code 3 ICD-10-C M * M1025 Optional Diagnosis Multiple Code 4 ICD-10-C M * M1025 Optional Diagnosis Multiple Code 5 ICD-10-C M * M1025 Primary Optional Diagnosis Multiple Codes ICD-10-C M *
208

M1030 Home Therapies - Enteral Nutrition M1030 Home Therapies - Intravenous or Infusion Therapy M1030 Home Therapies - None of the Above M1030 Home Therapies - Parenteral Nutrition M1032 Risk for Hospitalization - Frailty Indicators M1032 Risk for Hospitalization - History of Falls M1032 Risk for Hospitalization - Mental, Emotional or Behavioral Decline M1032 Risk for Hospitalization - Multiple Hospitalizations M1032 Risk for Hospitalization - None of the Above M1032 Risk For Hospitalization - Other M1032 Risk for Hospitalization - Taking Five or More Meds M1033 Risk For Hospitalization - Difficulty with Medical Instructions * M1033 Risk For Hospitalization - Exhaustion * M1033 Risk for Hospitalization - Fall History * M1033 Risk For Hospitalization - Mental, Emotional, Behavioral * M1033 Risk For Hospitalization - Multiple ER Visits * M1033 Risk For Hospitalization - Multiple Hospitalizations * M1033 Risk For Hospitalization - None of the Above * M1033 Risk For Hospitalization - Other * M1033 Risk For Hospitalization - Taking Five or More Meds * M1033 Risk For Hospitalization - Weight Loss * M1034 Overall Status M1036 Risk Factor - Alcohol Dependency M1036 Risk Factor - Drug Dependency M1036 Risk Factor - None of the Above M1036 Risk Factor - Obesity M1036 Risk Factor - Smoking M1036 Risk Factor - Unknown M1040 Influenza Vaccine Received from Agency M1041 Influenza Season * M1045 Influenza Vaccine - Reason Not Received M1046 Influenza Vaccine Received During Flu Season * M1050 Pneumococcal Vaccine Received In Agency M1051 Pneumococcal Vaccine Ever Received * M1055 Pneumococcal Vaccine - Reason Not Received M1056 Pneumococcal Vaccine - Reason Never Received * M1100 Patient Living Arrangement M1200 Vision M1210 Hearing M1220 Understand Verbal Content
209

M1230 Verbal Expression M1240 Formal Pain Assessment M1242 Frequency Of Pain Interfering With Activity M1300 Pressure Ulcer Assessment M1302 Risk Of Developing Pressure Ulcers M1306 Unhealed Pressure Ulcers at Stage II or Higher M1307 Oldest Stage II Pressure Ulcer Onset Date M1307 Status Oldest Stage II Pressure Ulcer Since SOC/ROC M1308 Number of Current Pressure Ulcers - Stage II M1308 Number of Current Pressure Ulcers - Stage III M1308 Number of Current Pressure Ulcers - Stage IV M1308 Number of Stage II Pressure Ulcers at SOC/ROC M1308 Number of Stage III Pressure Ulcers at SOC/ROC M1308 Number of Stage IV Pressure Ulcers at SOC/ROC M1308 Number of Unstageable Pressure Ulcers Due To Eschar or Slough M1308 Number of Unstageable Pressure Ulcers Due To Eschar or Slough at SOC/ROC M1308 Number of Unstageable Pressure Ulcers Due To Non-Removable Dsg M1308 Number of Unstageable Pressure Ulcers Due to Non-removable Dsg at SOC/ROC M1308 Number of Unstageable Pressure Ulcers Due To Deep Tissue Injury M1308 Number of Unstageable Pressure Ulcers Due To Deep Tissue Injury at SOC/ROC M1309 Number of Worsening Nonstageable Pressure Ulcers at SOC/ROC * M1309 Number of Worsening Stage II Pressure Ulcers at SOC/ROC * M1309 Number of Worsening Stage III Pressure Ulcers at SOC/ROC * M1309 Number of Worsening Stage IV Pressure Ulcers at SOC/ROC * M1310 Largest Pressure Ulcer Length M1312 Largest Pressure Ulcer Width M1314 Largest Pressure Ulcer Depth M1320 Status of Most Problematic (Observable) Pressure Ulcer M1322 Current Number Of Stage I Pressure Ulcers M1324 Stage Of Most Problematic Pressure Ulcer M1330 Stasis Ulcer Present M1332 Current Number of (Observable) Stasis Ulcer(s) M1334 Status of Most Problematic Stasis Ulcer M1340 Surgical Wound Present M1342 Status of Most Problematic Observable Surgical Wound M1350 Skin Lesion Or Open Wound M1400 When Is Patient Dyspneic or SOB M1410 Respiratory Treatment At Home - CPAP/BPAP M1410 Respiratory Treatment At Home - None of the Above M1410 Respiratory Treatment At Home - Oxygen
210

M1410 Respiratory Treatment At Home - Ventilator M1500 Heart Failure Present M1510 Heart Failure Follow-up - Change In Care Plan M1510 Heart Failure Follow-up - Emergency Treatment Advised M1510 Heart Failure Follow-up - No Action Taken M1510 Heart Failure Follow-up - Physician Contacted M1510 Heart Failure Follow-up - Physician Ordered Treatment M1510 Heart Failure Follow-up - Pt Educ or Clinical Intervention M1600 UTI Treatment M1610 Urinary Incontinence Or Catheter Presence M1615 Urinary Incontinence Timing M1620 Bowel Incontinence Frequency M1630 Ostomy For Bowel Elimination M1700 Cognitive Functioning M1710 When Confused Frequency M1720 When Anxious Frequency M1730 Depression Screening M1730 PHQ2 - Little Interest Or Pleasure In Doing Things M1730 PHQ2 Feeling Down, Depressed, or Hopeless M1740 Cog/Behav/Psych Sympt - Delusional M1740 Cog/Behav/Psych Sympt - Disruptive or Inappropriate M1740 Cog/Behav/Psych Sympt - Impaired Decision-Making M1740 Cog/Behav/Psych Sympt - Memory Deficit M1740 Cog/Behav/Psych Sympt - None of the Above M1740 Cog/Behav/Psych Sympt - Physical Aggression M1740 Cog/Behav/Psych Sympt - Verbal Disruption M1745 Frequency Of Disruptive Behavior Symptoms M1750 Receives Psychiatric Nursing Services M1800 Current Grooming M1810 Current Dress Upper Body M1820 Current Dress Lower Body M1830 Ability To Wash Body M1840 Current Toilet Transferring M1845 Current Toileting Hygiene M1850 Current Transferring M1860 Current Ambulation/Locomotion M1870 Current Feeding or Eating M1880 Current Plan/Prepare Light Meal M1890 Current Telephone Use M1900 Prior Functioning ADL/IADL - Ambulation
211

M1900 Prior Functioning ADL/IADL - Household Tasks M1900 Prior Functioning ADL/IADL - Self Care M1900 Prior Functioning ADL/IADL - Transfer M1910 Multi-Factor Fall Risk Assessment M2000 Drug Regimen Review M2002 Medication Follow-Up M2004 Medication Intervention M2010 Patient/Caregiver High Risk Drug Education M2015 Patient/Caregiver Drug Education Intervention M2020 Current Management Of Oral Medications M2030 Current Management Of Injectable Medications M2040 Prior Medication Management - Injectable Meds M2040 Prior Medication Management - Oral Meds M2100 Care Management - ADL Assistance M2100 Care Management - Advocacy or Facilitation M2100 Care Management - IADL Assistance M2100 Care Management - Management of Equipment M2100 Care Management - Medical Procedures/Treatments M2100 Care Management - Medication Administration M2100 Care Management - Supervision And Safety M2102 Care Assistance - ADL Assistance * M2102 Care Assistance - Advocacy Or Facilitation * M2102 Care Assistance - IADL Assistance * M2102 Care Assistance - Management of Equipment * M2102 Care Assistance - Medical Procedures/Treatments * M2102 Care Assistance - Medication Administration * M2102 Care Assistance - Supervision And Safety * M2110 Frequency Of ADL Or IADL Assistance From Caregiver M2200 Therapy Need - Number Of Visits M2200 Therapy Need - Not Applicable M2250 Plan Of Care Synopsis - Depression Intervention M2250 Plan Of Care Synopsis - Diabetic Foot Care M2250 Plan Of Care Synopsis - Fall Prevention M2250 Plan Of Care Synopsis - Pain Intervention M2250 Plan Of Care Synopsis - Parameters for Physician Notification M2250 Plan Of Care Synopsis - Pressure Ulcer Moist Treatment M2250 Plan Of Care Synopsis - Pressure Ulcer Prevention M2300 Emergent Care Since Last OASIS M2310 Emergent Care Reason - Acute Mental/Behavioral M2310 Emergent Care Reason - Cardiac Dysrhythmia
212

M2310 Emergent Care Reason - Dehydration/Malnutrition M2310 Emergent Care Reason - DVT, Pulmonary Embolus M2310 Emergent Care Reason - GI Issues M2310 Emergent Care Reason - Heart Failure M2310 Emergent Care Reason - Hypo/Hyperglycemia/Diabetes M2310 Emergent Care Reason - Improper Medication Administration M2310 Emergent Care Reason - Injury From Fall M2310 Emergent Care Reason - IV Catheter Infection M2310 Emergent Care Reason - Myocardial Infarction/Chest Pain M2310 Emergent Care Reason - Other M2310 Emergent Care Reason - Other Heart Disease M2310 Emergent Care Reason - Other Respiratory Problem M2310 Emergent Care Reason - Respiratory Infection M2310 Emergent Care Reason - Stroke (CVA) or TIA M2310 Emergent Care Reason - Uncontrolled Pain M2310 Emergent Care Reason - Unknown M2310 Emergent Care Reason - Urinary Tract Infection M2310 Emergent Care Reason - Wound Infection/Deterioration M2400 Synopsis - Depression Prevention M2400 Synopsis - Diabetic Foot Care M2400 Synopsis - Falls Prevention M2400 Synopsis - Pain Intervention M2400 Synopsis - Pressure Ulcer Moist Treatment M2400 Synopsis - Pressure Ulcer Prevention M2410 Admit Inpatient Facility Type M2420 Discharge Location M2430 Hospital Reason - Acute Mental/Behavioral M2430 Hospital Reason - Cardiac Dysrhythmia M2430 Hospital Reason - Dehydration, Malnutrition M2430 Hospital Reason - DVT, Pulmonary Embolus M2430 Hospital Reason - GI Issues M2430 Hospital Reason - Heart Failure M2430 Hospital Reason - Hypo/Hyperglycemia/Diabetes M2430 Hospital Reason - Improper Medication Administration M2430 Hospital Reason - Injury Caused by Fall M2430 Hospital Reason - IV Catheter Infection M2430 Hospital Reason - Myocardial Infarction/Chest Pain M2430 Hospital Reason - Other M2430 Hospital Reason - Other Heart Disease M2430 Hospital Reason - Other Respiratory Problem
213

M2430 Hospital Reason - Respiratory Infection M2430 Hospital Reason - Scheduled Treatment Or Procedure M2430 Hospital Reason - Stroke (CVA) Or TIA M2430 Hospital Reason - Uncontrolled Pain M2430 Hospital Reason - Unknown M2430 Hospital Reason - Urinary Tract Infect M2430 Hospital Reason - Wound Infection/Deterioration M2440 Admitted Nursing Home Reason - Hospice M2440 Admitted Nursing Home Reason - Other M2440 Admitted Nursing Home Reason - Permanent Placement M2440 Admitted Nursing Home Reason - Respite Care M2440 Admitted Nursing Home Reason - Therapy Services M2440 Admitted Nursing Home Reason - Unknown M2440 Admitted Nursing Home Reason - Unsafe At Home
214

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 1 of 24
Home Health Patient Tracking Sheet
(M0010) C M S Certification Number: __ __ __ __ __ __
(M0014) Branch State: __ __
(M0016) Branch I D Number: __ __ __ __ __ __ __ __ __ __
(M0018) National Provider Identifier (N P I) for the attending physician who has signed the plan of care:
__ __ __ __ __ __ __ __ __ __ ⃞ UK – Unknown or Not Available
(M0020) Patient I D Number: __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
(M0030) Start of Care Date: __ __ /__ __ /__ __ __ __
month / day / year
(M0032) Resumption of Care Date: __ __ /__ __ /__ __ __ __ ⃞ NA - Not Applicable
month / day / year
(M0040) Patient Name:
__ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
(First) (M I) (Last) (Suffix)
(M0050) Patient State of Residence: __ __
(M0060) Patient Zip Code: __ __ __ __ __ __ __ __ __
(M0063) Medicare Number: __ __ __ __ __ __ __ __ __ __ __ __ ⃞ NA – No Medicare (including suffix)
(M0064) Social Security Number: __ __ __ - __ __ - __ __ __ __ ⃞ UK – Unknown or Not Available
(M0065) Medicaid Number: __ __ __ __ __ __ __ __ __ __ __ __ __ __ ⃞ NA – No Medicaid
(M0066) Birth Date: __ __ /__ __ /__ __ __ __ month / day / year
(M0069) Gender:
⃞ 1 - Male
⃞ 2 - Female
(M0140) Race/Ethnicity: (Mark all that apply.)
⃞ 1 - American Indian or Alaska Native
⃞ 2 - Asian
⃞ 3 - Black or African-American
⃞ 4 - Hispanic or Latino
⃞ 5 - Native Hawaiian or Pacific Islander
⃞ 6 - White
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection instrument is 0938-0760. The time required to complete this information collection is estimated to average 0.7 minutes per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Baltimore, Maryland 21244-1850.
215

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 2 of 24
(M0150) Current Payment Sources for Home Care: (Mark all that apply.)
⃞ 0 - None; no charge for current services
⃞ 1 - Medicare (traditional fee-for-service)
⃞ 2 - Medicare (HMO/managed care/Advantage plan)
⃞ 3 - Medicaid (traditional fee-for-service)
⃞ 4 - Medicaid (HMO/managed care)
⃞ 5 - Workers' compensation
⃞ 6 - Title programs (e.g., Title III, V, or XX)
⃞ 7 - Other government (e.g., TriCare, VA, etc.)
⃞ 8 - Private insurance
⃞ 9 - Private HMO/managed care
⃞ 10 - Self-pay
⃞ 11 - Other (specify)
⃞ UK - Unknown
216

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 3 of 24
Outcome and Assessment Information Set
Items to be Used at Specific Time Points
Start of Care ----------------------------------------------------------------
Start of care—further visits planned
M0010-M0030, M0040- M0150, M1000-M1036, M1100-M1242, M1300-M1302, M1306, M1308-M1324, M1330-M1350, M1400, M1410, M1600-M1730, M1740-M1910, M2000, M2002, M2010, M2020-M2250
Resumption of Care -----------------------------------------------------
Resumption of care (after inpatient stay)
M0032, M0080-M0110, M1000-M1036, M1100-M1242, M1300-M1302, M1306, M1308-M1324, M1330-M1350, M1400, M1410, M1600-M1730, M1740-M1910, M2000, M2002, M2010, M2020-M2250
Follow-Up -------------------------------------------------------------------
Recertification (follow-up) assessment Other follow-up assessment
M0080-M0100, M0110, M1020-M1030, M1200, M1242, M1306, M1308, M1322-M1324, M1330-M1350, M1400, M1610, M1620, M1630, M1810-M1840, M1850, M1860, M2030, M2200
Transfer to an Inpatient Facility --------------------------------------
Transferred to an inpatient facility—patient not discharged from an agency Transferred to an inpatient facility—patient discharged from agency
M0080-M0100, M1040-M1055, M1500, M1510, M2004, M2015, M2300-M2410, M2430-M2440, M0903, M0906
Discharge from Agency — Not to an Inpatient Facility
Death at home --------------------------------------------------------- M0080-M0100, M0903, M0906 Discharge from agency ---------------------------------------------- M0080-M0100, M1040-M1055, M1230, M1242, M1306-
M1350, M1400-M1620, M1700-M1720, M1740, M1745, M1800-M1890, M2004, M2015-M2030, M2100-M2110, M2300-M2420, M0903, M0906
CLINICAL RECORD ITEMS
(M0080) Discipline of Person Completing Assessment:
⃞ 1-RN ⃞ 2-PT ⃞ 3-SLP/ST ⃞ 4-OT
(M0090) Date Assessment Completed: __ __ /__ __ /__ __ __ __
month / day / year
(M0100) This Assessment is Currently Being Completed for the Following Reason:
Start/Resumption of Care
⃞ 1 – Start of care—further visits planned
⃞ 3 – Resumption of care (after inpatient stay)
Follow-Up
⃞ 4 – Recertification (follow-up) reassessment [ Go to M0110 ]
⃞ 5 – Other follow-up [ Go to M0110 ]
Transfer to an Inpatient Facility
⃞ 6 – Transferred to an inpatient facility—patient not discharged from agency [ Go to M1040]
⃞ 7 – Transferred to an inpatient facility—patient discharged from agency [ Go to M1040 ]
Discharge from Agency — Not to an Inpatient Facility
⃞ 8 – Death at home [ Go to M0903 ]
⃞ 9 – Discharge from agency [ Go to M1040 ]
217

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 4 of 24
(M0102) Date of Physician-ordered Start of Care (Resumption of Care): If the physician indicated a specific start
of care (resumption of care) date when the patient was referred for home health services, record the date specified.
__ __ /__ __ /__ __ __ __ [ Go to M0110, if date entered ]
month / day / year
⃞ NA –No specific SOC date ordered by physician
(M0104) Date of Referral: Indicate the date that the written or verbal referral for initiation or resumption of care was
received by the HHA.
__ __ /__ __ /__ __ __ __
month / day / year
(M0110) Episode Timing: Is the Medicare home health payment episode for which this assessment will define a
case mix group an ―early‖ episode or a ―later‖ episode in the patient’s current sequence of adjacent Medicare home health payment episodes?
⃞ 1 - Early
⃞ 2 - Later
⃞ UK - Unknown
⃞ NA - Not Applicable: No Medicare case mix group to be defined by this assessment.
PATIENT HISTORY AND DIAGNOSES
(M1000) From which of the following Inpatient Facilities was the patient discharged during the past 14 days? (Mark all that apply.)
⃞ 1 - Long-term nursing facility (NF)
⃞ 2 - Skilled nursing facility (SNF / TCU)
⃞ 3 - Short-stay acute hospital (IPP S)
⃞ 4 - Long-term care hospital (LTCH)
⃞ 5 - Inpatient rehabilitation hospital or unit (IRF)
⃞ 6 - Psychiatric hospital or unit
⃞ 7 - Other (specify)
⃞ NA - Patient was not discharged from an inpatient facility [Go to M1016 ]
(M1005) Inpatient Discharge Date (most recent):
__ __ /__ __ /__ __ __ __
month / day / year
⃞ UK - Unknown
218

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 5 of 24
(M1010) List each Inpatient Diagnosis and ICD-9-C M code at the level of highest specificity for only those conditions
treated during an inpatient stay within the last 14 days (no E-codes, or V-codes):
Inpatient Facility Diagnosis ICD-9-C M Code
a. __ __ __ . __ __
b. __ __ __ . __ __
c. __ __ __ . __ __
d. __ __ __ . __ __
e. __ __ __ . __ __
f. __ __ __ . __ __
(M1012) List each Inpatient Procedure and the associated ICD-9-C M procedure code relevant to the plan of care.
Inpatient Procedure Procedure Code
a. __ __ . __ __
b. __ __ . __ __
c. __ __ . __ __
d. __ __ . __ __
⃞ NA - Not applicable
⃞ UK - Unknown
(M1016) Diagnoses Requiring Medical or Treatment Regimen Change Within Past 14 Days: List the patient's
Medical Diagnoses and ICD-9-C M codes at the level of highest specificity for those conditions requiring changed medical or treatment regimen within the past 14 days (no surgical, E-codes, or V-codes):
Changed Medical Regimen Diagnosis ICD-9-C M Code
a. __ __ __ . __ __
b. __ __ __ . __ __
c. __ __ __ . __ __
d. __ __ __ . __ __
e. __ __ __ . __ __
f. __ __ __ . __ __
⃞ NA - Not applicable (no medical or treatment regimen changes within the past 14 days)
(M1018) Conditions Prior to Medical or Treatment Regimen Change or Inpatient Stay Within Past 14 Days: If
this patient experienced an inpatient facility discharge or change in medical or treatment regimen within the past 14 days, indicate any conditions which existed prior to the inpatient stay or change in medical or treatment regimen. (Mark all that apply.)
⃞ 1 - Urinary incontinence
⃞ 2 - Indwelling/suprapubic catheter
⃞ 3 - Intractable pain
⃞ 4 - Impaired decision-making
⃞ 5 - Disruptive or socially inappropriate behavior
⃞ 6 - Memory loss to the extent that supervision required
⃞ 7 - None of the above
⃞ NA - No inpatient facility discharge and no change in medical or treatment regimen in past 14 days
⃞ UK - Unknown
219

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 6 of 24
(M1020/1022/1024) Diagnoses, Symptom Control, and Payment Diagnoses: List each diagnosis for which the
patient is receiving home care (Column 1) and enter its ICD-9-C M code at the level of highest specificity (no surgical/procedure codes) (Column 2). Diagnoses are listed in the order that best reflect the seriousness of each condition and support the disciplines and services provided. Rate the degree of symptom control for each condition (Column 2). Choose one value that represents the degree of symptom control appropriate for each diagnosis: V-codes (for M1020 or M1022) or E-codes (for M1022 only) may be used. ICD-9-C M sequencing requirements must be followed if multiple coding is indicated for any diagnoses. If a V-code is reported in place of a case mix diagnosis, then optional item M1024 Payment Diagnoses (Columns 3 and 4) may be completed. A case mix diagnosis is a diagnosis that determines the Medicare P P S case mix group. Do not assign symptom control ratings for V- or E-codes.
Code each row according to the following directions for each column:
Column 1: Enter the description of the diagnosis. Column 2: Enter the ICD-9-C M code for the diagnosis described in Column 1; Rate the degree of symptom control for the condition listed in Column 1 using the following scale: 0 - Asymptomatic, no treatment needed at this time 1 - Symptoms well controlled with current therapy 2 - Symptoms controlled with difficulty, affecting daily functioning; patient needs ongoing monitoring 3 - Symptoms poorly controlled; patient needs frequent adjustment in treatment and dose monitoring 4 - Symptoms poorly controlled; history of re-hospitalizations Note that in Column 2 the rating for symptom control of each diagnosis should not be used to determine the
sequencing of the diagnoses listed in Column 1. These are separate items and sequencing may not coincide. Sequencing of diagnoses should reflect the seriousness of each condition and support the disciplines and services provided.
Column 3: (OPTIONAL) If a V-code is assigned to any row in Column 2, in place of a case mix diagnosis, it may be necessary to complete optional item M1024 Payment Diagnoses (Columns 3 and 4). See OASIS-C Guidance Manual.
Column 4: (OPTIONAL) If a V-code in Column 2 is reported in place of a case mix diagnosis that requires multiple diagnosis codes under ICD-9-C M coding guidelines, enter the diagnosis descriptions and the ICD-9-C M codes in the same row in Columns 3 and 4. For example, if the case mix diagnosis is a manifestation code, record the diagnosis description and ICD-9-C M code for the underlying condition in Column 3 of that row and the diagnosis description and ICD-9-C M code for the manifestation in Column 4 of that row. Otherwise, leave Column 4 blank in that row.
(Form on next page)
220

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 7 of 24
(M1020) Primary Diagnosis & (M1022) Other Diagnoses (M1024) Payment Diagnoses (OPTIONAL)
Column 1 Column 2 Column 3 Column 4
Diagnoses (Sequencing of diagnoses should
reflect the seriousness of each condition and support the
disciplines and services provided.)
ICD-9-C M and symptom control rating for each
condition. Note that the sequencing of these ratings may not match
the sequencing of the diagnoses
Complete if a V-code is assigned under certain
circumstances to Column 2 in place of a case mix
diagnosis.
Complete only if the V-code in Column 2 is reported in
place of a case mix diagnosis that is a multiple
coding situation (e.g., a manifestation code).
Description ICD-9-C M /
Symptom Control Rating Description/ ICD-9-C M
Description/ ICD-9-C M
(M1020) Primary Diagnosis
a.
(V-codes are allowed)
a. (__ __ __ . __ __)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4
(V- or E-codes NOT allowed)
a.
(__ __ __ . __ __)
(V- or E-codes NOT allowed)
a.
(__ __ __ . __ __)
(M1022) Other Diagnoses
b.
(V- or E-codes are allowed)
b. (__ __ __ __ . __ __)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4
(V- or E-codes NOT allowed)
b.
(__ __ __ . __ __)
(V- or E-codes NOT allowed)
b.
(__ __ __ . __ __)
c. c. (__ __ __ __ . __ __)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4
c.
(__ __ __ . __ __)
c.
(__ __ __ . __ __)
d. d. (__ __ __ __ . __ __)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4
d.
(__ __ __ . __ __)
d.
(__ __ __ . __ __)
e. e. (__ __ __ __ . __ __)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4
e.
(__ __ __ . __ __)
e.
(__ __ __ . __ __)
f. f. (__ __ __ __ . __ __)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4
f.
(__ __ __ . __ __)
f.
(__ __ __ . __ __)
(M1030) Therapies the patient receives at home: (Mark all that apply.)
⃞ 1 - Intravenous or infusion therapy (excludes TPN)
⃞ 2 - Parenteral nutrition (TPN or lipids)
⃞ 3 - Enteral nutrition (nasogastric, gastrostomy, jejunostomy, or any other artificial entry into the
alimentary canal)
⃞ 4 - None of the above
(M1032) Risk for Hospitalization: Which of the following signs or symptoms characterize this patient as at risk for hospitalization? (Mark all that apply.)
⃞ 1 - Recent decline in mental, emotional, or behavioral status
⃞ 2 - Multiple hospitalizations (2 or more) in the past 12 months
⃞ 3 - History of falls (2 or more falls - or any fall with an injury - in the past year)
⃞ 4 - Taking five or more medications
⃞ 5 - Frailty indicators, e.g., weight loss, self-reported exhaustion
⃞ 6 - Other
⃞ 7 - None of the above
221

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 8 of 24
(M1034) Overall Status: Which description best fits the patient’s overall status? (Check one)
⃞ 0 - The patient is stable with no heightened risk(s) for serious complications and death (beyond those
typical of the patient’s age).
⃞ 1 - The patient is temporarily facing high health risk(s) but is likely to return to being stable without
heightened risk(s) for serious complications and death (beyond those typical of the patient’s age).
⃞ 2 - The patient is likely to remain in fragile health and have ongoing high risk(s) of serious complications
and death.
⃞ 3 - The patient has serious progressive conditions that could lead to death within a year.
⃞ UK - The patient’s situation is unknown or unclear.
(M1036) Risk Factors, either present or past, likely to affect current health status and/or outcome: (Mark all that apply.)
⃞ 1 - Smoking
⃞ 2 - Obesity
⃞ 3 - Alcohol dependency
⃞ 4 - Drug dependency
⃞ 5 - None of the above
⃞ UK - Unknown
(M1040) Influenza Vaccine: Did the patient receive the influenza vaccine from your agency for this year’s influenza season (October 1 through March 31) during this episode of care?
⃞ 0 - No
⃞ 1 - Yes [ Go to M1050 ]
⃞ NA - Does not apply because entire episode of care (SOC/ROC to Transfer/Discharge) is outside this
influenza season. [ Go to M1050 ]
(M1045) Reason Influenza Vaccine not received: If the patient did not receive the influenza vaccine from your agency during this episode of care, state reason:
⃞ 1 - Received from another health care provider (e.g., physician)
⃞ 2 - Received from your agency previously during this year’s flu season
⃞ 3 - Offered and declined
⃞ 4 - Assessed and determined to have medical contraindication(s)
⃞ 5 - Not indicated; patient does not meet age/condition guidelines for influenza vaccine
⃞ 6 - Inability to obtain vaccine due to declared shortage
⃞ 7 - None of the above
(M1050) Pneumococcal Vaccine: Did the patient receive pneumococcal polysaccharide vaccine (PPV) from your agency during this episode of care (SOC/ROC to Transfer/Discharge)?
⃞ 0 - No
⃞ 1 - Yes [ Go to M1500 at TRN; Go to M1230 at DC ]
(M1055) Reason PPV not received: If patient did not receive the pneumococcal polysaccharide vaccine (PPV) from your agency during this episode of care (SOC/ROC to Transfer/Discharge), state reason:
⃞ 1 - Patient has received PPV in the past
⃞ 2 - Offered and declined
⃞ 3 - Assessed and determined to have medical contraindication(s)
⃞ 4 - Not indicated; patient does not meet age/condition guidelines for PPV
⃞ 5 - None of the above
222

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 9 of 24
LIVING ARRANGEMENTS
(M1100) Patient Living Situation: Which of the following best describes the patient's residential circumstance and availability of assistance? (Check one box only.)
Living Arrangement
Availability of Assistance
Around the clock
Regular daytime
Regular nighttime
Occasional / short-term assistance
No assistance available
a. Patient lives alone ⃞ 01 ⃞ 02 ⃞ 03 ⃞ 04 ⃞ 05
b. Patient lives with other person(s) in the home ⃞ 06 ⃞ 07 ⃞ 08 ⃞ 09 ⃞ 10
c. Patient lives in congregate situation (e.g., assisted living) ⃞ 11 ⃞ 12 ⃞ 13 ⃞ 14 ⃞ 15
SENSORY STATUS
(M1200) Vision (with corrective lenses if the patient usually wears them):
⃞ 0 - Normal vision: sees adequately in most situations; can see medication labels, newsprint.
⃞ 1 - Partially impaired: cannot see medication labels or newsprint, but can see obstacles in path, and the surrounding layout; can count fingers at arm's length.
⃞ 2 - Severely impaired: cannot locate objects without hearing or touching them or patient nonresponsive.
(M1210) Ability to hear (with hearing aid or hearing appliance if normally used):
⃞ 0 - Adequate: hears normal conversation without difficulty.
⃞ 1 - Mildly to Moderately Impaired: difficulty hearing in some environments or speaker may need to increase volume or speak distinctly.
⃞ 2 - Severely Impaired: absence of useful hearing.
⃞ UK - Unable to assess hearing.
(M1220) Understanding of Verbal Content in patient's own language (with hearing aid or device if used):
⃞ 0 - Understands: clear comprehension without cues or repetitions.
⃞ 1 - Usually Understands: understands most conversations, but misses some part/intent of message. Requires cues at times to understand.
⃞ 2 - Sometimes Understands: understands only basic conversations or simple, direct phrases.
Frequently requires cues to understand.
⃞ 3 - Rarely/Never Understands
⃞ UK - Unable to assess understanding.
(M1230) Speech and Oral (Verbal) Expression of Language (in patient's own language):
⃞ 0 - Expresses complex ideas, feelings, and needs clearly, completely, and easily in all situations with no observable impairment.
⃞ 1 - Minimal difficulty in expressing ideas and needs (may take extra time; makes occasional errors in word choice, grammar or speech intelligibility; needs minimal prompting or assistance).
⃞ 2 - Expresses simple ideas or needs with moderate difficulty (needs prompting or assistance, errors in word choice, organization or speech intelligibility). Speaks in phrases or short sentences.
⃞ 3 - Has severe difficulty expressing basic ideas or needs and requires maximal assistance or guessing
by listener. Speech limited to single words or short phrases.
⃞ 4 - Unable to express basic needs even with maximal prompting or assistance but is not comatose or unresponsive (e.g., speech is nonsensical or unintelligible).
⃞ 5 - Patient nonresponsive or unable to speak.
223

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 10 of 24
(M1240) Has this patient had a formal Pain Assessment using a standardized pain assessment tool (appropriate to the patient’s ability to communicate the severity of pain)?
⃞ 0 - No standardized assessment conducted
⃞ 1 - Yes, and it does not indicate severe pain
⃞ 2 - Yes, and it indicates severe pain
(M1242) Frequency of Pain Interfering with patient's activity or movement:
⃞ 0 - Patient has no pain
⃞ 1 - Patient has pain that does not interfere with activity or movement
⃞ 2 - Less often than daily
⃞ 3 - Daily, but not constantly
⃞ 4 - All of the time
INTEGUMENTARY STATUS
(M1300) Pressure Ulcer Assessment: Was this patient assessed for Risk of Developing Pressure Ulcers?
⃞ 0 - No assessment conducted [ Go to M1306 ]
⃞ 1 - Yes, based on an evaluation of clinical factors, e.g., mobility, incontinence, nutrition, etc., without use
of standardized tool
⃞ 2 - Yes, using a standardized tool, e.g., Braden, Norton, other
(M1302) Does this patient have a Risk of Developing Pressure Ulcers?
⃞ 0 - No
⃞ 1 - Yes
(M1306) Does this patient have at least one Unhealed Pressure Ulcer at Stage II or Higher or designated as
"unstageable"?
⃞ 0 - No [ Go to M1322 ]
⃞ 1 - Yes
(M1307) The Oldest Non-epithelialized Stage II Pressure Ulcer that is present at discharge
⃞ 1 - Was present at the most recent SOC/ROC assessment
⃞ 2 - Developed since the most recent SOC/ROC assessment: record date pressure ulcer first identified:
__ __ /__ __ /____ __ __ month / day / year
⃞ NA - No non-epithelialized Stage II pressure ulcers are present at discharge
224

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 11 of 24
(M1308) Current Number of Unhealed (non-epithelialized) Pressure Ulcers at Each Stage: (Enter ―0‖ if none; excludes Stage I pressure ulcers)
Column 1
Complete at SOC/ROC/FU & D/C
Column 2
Complete at FU & D/C
Stage description – unhealed pressure ulcers Number Currently
Present
Number of those listed in Column 1 that were present on admission (most recent
SOC / ROC)
a. Stage II: Partial thickness loss of dermis presenting as a shallow open ulcer with red pink wound bed, without slough. May also present as an intact or open/ruptured serum-filled blister.
___ ___
b. Stage III: Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or muscles are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling.
___ ___
c. Stage IV: Full thickness tissue loss with visible bone, tendon, or muscle. Slough or eschar may be present on some parts of the wound bed. Often includes undermining and tunneling.
___ ___
d.1 Unstageable: Known or likely but unstageable due to non-removable dressing or device ___ ___
d.2 Unstageable: Known or likely but unstageable due to coverage of wound bed by slough and/or eschar.
___ ___
d.3 Unstageable: Suspected deep tissue injury in evolution. ___ ___
Directions for M1310, M1312, and M1314: If the patient has one or more unhealed (non-epithelialized) Stage III or IV pressure ulcers, identify the Stage III or IV pressure ulcer with the largest surface dimension (length x width) and
record in centimeters. If no Stage III or Stage IV pressure ulcers, go to M1320.
(M1310) Pressure Ulcer Length: Longest length ―head-to-toe‖ | ___ | ___ | . | ___ | (cm)
(M1312) Pressure Ulcer Width: Width of the same pressure ulcer; greatest width perpendicular to the length
| ___ | ___ | . | ___ | (cm)
(M1314) Pressure Ulcer Depth: Depth of the same pressure ulcer; from visible surface to the deepest area
| ___ | ___ | . | ___ | (cm)
(M1320) Status of Most Problematic (Observable) Pressure Ulcer:
⃞ 0 - Newly epithelialized
⃞ 1 - Fully granulating
⃞ 2 - Early/partial granulation
⃞ 3 - Not healing
⃞ NA - No observable pressure ulcer
225

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 12 of 24
(M1322) Current Number of Stage I Pressure Ulcers: Intact skin with non-blanchable redness of a localized area
usually over a bony prominence. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue.
⃞ 0 ⃞ 1 ⃞ 2 ⃞ 3 ⃞ 4 or more
(M1324) Stage of Most Problematic Unhealed (Observable) Pressure Ulcer:
⃞ 1 - Stage I
⃞ 2 - Stage II
⃞ 3 - Stage III
⃞ 4 - Stage IV
⃞ NA - No observable pressure ulcer or unhealed pressure ulcer
(M1330) Does this patient have a Stasis Ulcer?
⃞ 0 - No [ Go to M1340 ]
⃞ 1 - Yes, patient has BOTH observable and unobservable stasis ulcers
⃞ 2 - Yes, patient has observable stasis ulcers ONLY
⃞ 3 - Yes, patient has unobservable stasis ulcers ONLY (known but not observable due to non-removable
dressing) [ Go to M1340 ]
(M1332) Current Number of (Observable) Stasis Ulcer(s):
⃞ 1 - One
⃞ 2 - Two
⃞ 3 - Three
⃞ 4 - Four or more
(M1334) Status of Most Problematic (Observable) Stasis Ulcer:
⃞ 0 - Newly epithelialized
⃞ 1 - Fully granulating
⃞ 2 - Early/partial granulation
⃞ 3 - Not healing
(M1340) Does this patient have a Surgical Wound?
⃞ 0 - No [ Go to M1350 ]
⃞ 1 - Yes, patient has at least one (observable) surgical wound
⃞ 2 - Surgical wound known but not observable due to non-removable dressing [ Go to M1350 ]
(M1342) Status of Most Problematic (Observable) Surgical Wound:
⃞ 0 - Newly epithelialized
⃞ 1 - Fully granulating
⃞ 2 - Early/partial granulation
⃞ 3 - Not healing
(M1350) Does this patient have a Skin Lesion or Open Wound, excluding bowel ostomy, other than those described above that is receiving intervention by the home health agency?
⃞ 0 - No
⃞ 1 - Yes
226

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 13 of 24
RESPIRATORY STATUS
(M1400) When is the patient dyspneic or noticeably Short of Breath?
⃞ 0 - Patient is not short of breath
⃞ 1 - When walking more than 20 feet, climbing stairs
⃞ 2 - With moderate exertion (e.g., while dressing, using commode or bedpan, walking distances less
than 20 feet)
⃞ 3 - With minimal exertion (e.g., while eating, talking, or performing other ADLs) or with agitation
⃞ 4 - At rest (during day or night)
(M1410) Respiratory Treatments utilized at home: (Mark all that apply.)
⃞ 1 - Oxygen (intermittent or continuous)
⃞ 2 - Ventilator (continually or at night)
⃞ 3 - Continuous / Bi-level positive airway pressure
⃞ 4 - None of the above
CARDIAC STATUS
(M1500) Symptoms in Heart Failure Patients: If patient has been diagnosed with heart failure, did the patient exhibit symptoms indicated by clinical heart failure guidelines (including dyspnea, orthopnea, edema, or weight gain) at any point since the previous OASIS assessment?
⃞ 0 - No [ Go to M2004 at TRN; Go to M1600 at DC ]
⃞ 1 - Yes
⃞ 2 - Not assessed [Go to M2004 at TRN; Go to M1600 at DC ]
⃞ NA - Patient does not have diagnosis of heart failure [Go to M2004 at TRN; Go to M1600 at DC ]
(M1510) Heart Failure Follow-up: If patient has been diagnosed with heart failure and has exhibited symptoms indicative of heart failure since the previous OASIS assessment, what action(s) has (have) been taken to respond? (Mark all that apply.)
⃞ 0 - No action taken
⃞ 1 - Patient’s physician (or other primary care practitioner) contacted the same day
⃞ 2 - Patient advised to get emergency treatment (e.g., call 911 or go to emergency room)
⃞ 3 - Implemented physician-ordered patient-specific established parameters for treatment
⃞ 4 - Patient education or other clinical interventions
⃞ 5 - Obtained change in care plan orders (e.g., increased monitoring by agency, change in visit frequency, telehealth, etc.)
ELIMINATION STATUS
(M1600) Has this patient been treated for a Urinary Tract Infection in the past 14 days?
⃞ 0 - No
⃞ 1 - Yes
⃞ NA - Patient on prophylactic treatment
⃞ UK - Unknown [Omit ―UK‖ option on DC]
(M1610) Urinary Incontinence or Urinary Catheter Presence:
⃞ 0 - No incontinence or catheter (includes anuria or ostomy for urinary drainage) [ Go to M1620 ]
⃞ 1 - Patient is incontinent
⃞ 2 - Patient requires a urinary catheter (i.e., external, indwelling, intermittent, suprapubic)
[ Go to M1620 ]
227

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 14 of 24
(M1615) When does Urinary Incontinence occur?
⃞ 0 - Timed-voiding defers incontinence
⃞ 1 - Occasional stress incontinence
⃞ 2 - During the night only
⃞ 3 - During the day only
⃞ 4 - During the day and night
(M1620) Bowel Incontinence Frequency:
⃞ 0 - Very rarely or never has bowel incontinence
⃞ 1 - Less than once weekly
⃞ 2 - One to three times weekly
⃞ 3 - Four to six times weekly
⃞ 4 - On a daily basis
⃞ 5 - More often than once daily
⃞ NA - Patient has ostomy for bowel elimination
⃞ UK - Unknown [Omit ―UK‖ option on FU, DC]
(M1630) Ostomy for Bowel Elimination: Does this patient have an ostomy for bowel elimination that (within the last 14 days): a) was related to an inpatient facility stay, or b) necessitated a change in medical or treatment regimen?
⃞ 0 - Patient does not have an ostomy for bowel elimination.
⃞ 1 - Patient's ostomy was not related to an inpatient stay and did not necessitate change in medical or
treatment regimen.
⃞ 2 - The ostomy was related to an inpatient stay or did necessitate change in medical or treatment
regimen.
NEURO/EMOTIONAL/BEHAVIORAL STATUS
(M1700) Cognitive Functioning: Patient's current (day of assessment) level of alertness, orientation, comprehension, concentration, and immediate memory for simple commands.
⃞ 0 - Alert/oriented, able to focus and shift attention, comprehends and recalls task directions
independently.
⃞ 1 - Requires prompting (cuing, repetition, reminders) only under stressful or unfamiliar conditions.
⃞ 2 - Requires assistance and some direction in specific situations (e.g., on all tasks involving shifting of
attention), or consistently requires low stimulus environment due to distractibility.
⃞ 3 - Requires considerable assistance in routine situations. Is not alert and oriented or is unable to shift
attention and recall directions more than half the time.
⃞ 4 - Totally dependent due to disturbances such as constant disorientation, coma, persistent vegetative
state, or delirium.
(M1710) When Confused (Reported or Observed Within the Last 14 Days):
⃞ 0 - Never
⃞ 1 - In new or complex situations only
⃞ 2 - On awakening or at night only
⃞ 3 - During the day and evening, but not constantly
⃞ 4 - Constantly
⃞ NA - Patient nonresponsive
228

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 15 of 24
(M1720) When Anxious (Reported or Observed Within the Last 14 Days):
⃞ 0 - None of the time
⃞ 1 - Less often than daily
⃞ 2 - Daily, but not constantly
⃞ 3 - All of the time
⃞ NA - Patient nonresponsive
(M1730) Depression Screening: Has the patient been screened for depression, using a standardized depression screening tool?
⃞ 0 - No
⃞ 1 - Yes, patient was screened using the PHQ-2©* scale. (Instructions for this two-question tool: Ask
patient: ―Over the last two weeks, how often have you been bothered by any of the following problems‖)
Not at all 0 - 1 day
Several days
2 - 6 days
More than half of the
days 7 – 11 days
Nearly every day 12 – 14
days
N/A Unable to respond
PHQ-2©*
a) Little interest or pleasure in doing things ⃞0 ⃞1 ⃞2 ⃞3 ⃞na
b) Feeling down, depressed, or hopeless? ⃞0 ⃞1 ⃞2 ⃞3 ⃞na
⃞ 2 - Yes, with a different standardized assessment-and the patient meets criteria for further evaluation for
depression.
⃞ 3 - Yes, patient was screened with a different standardized assessment-and the patient does not meet
criteria for further evaluation for depression.
*Copyright© Pfizer Inc. All rights reserved. Reproduced with permission. (M1740) Cognitive, behavioral, and psychiatric symptoms that are demonstrated at least once a week (Reported
or Observed): (Mark all that apply.)
⃞ 1 - Memory deficit: failure to recognize familiar persons/places, inability to recall events of past 24 hours, significant memory loss so that supervision is required
⃞ 2 - Impaired decision-making: failure to perform usual ADLs or IADLs, inability to appropriately stop activities, jeopardizes safety through actions
⃞ 3 - Verbal disruption: yelling, threatening, excessive profanity, sexual references, etc.
⃞ 4 - Physical aggression: aggressive or combative to self and others (e.g., hits self, throws objects,
punches, dangerous maneuvers with wheelchair or other objects)
⃞ 5 - Disruptive, infantile, or socially inappropriate behavior (excludes verbal actions)
⃞ 6 - Delusional, hallucinatory, or paranoid behavior
⃞ 7 - None of the above behaviors demonstrated
(M1745) Frequency of Disruptive Behavior Symptoms (Reported or Observed) Any physical, verbal, or other disruptive/dangerous symptoms that are injurious to self or others or jeopardize personal safety.
⃞ 0 - Never
⃞ 1 - Less than once a month
⃞ 2 - Once a month
⃞ 3 - Several times each month
⃞ 4 - Several times a week
⃞ 5 - At least daily
229

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 16 of 24
(M1750) Is this patient receiving Psychiatric Nursing Services at home provided by a qualified psychiatric nurse?
⃞ 0 - No
⃞ 1 - Yes
ADL/IADLs
(M1800) Grooming: Current ability to tend safely to personal hygiene needs (i.e., washing face and hands, hair care, shaving or make up, teeth or denture care, fingernail care).
⃞ 0 - Able to groom self unaided, with or without the use of assistive devices or adapted methods.
⃞ 1 - Grooming utensils must be placed within reach before able to complete grooming activities.
⃞ 2 - Someone must assist the patient to groom self.
⃞ 3 - Patient depends entirely upon someone else for grooming needs.
(M1810) Current Ability to Dress Upper Body safely (with or without dressing aids) including undergarments, pullovers, front-opening shirts and blouses, managing zippers, buttons, and snaps:
⃞ 0 - Able to get clothes out of closets and drawers, put them on and remove them from the upper body
without assistance.
⃞ 1 - Able to dress upper body without assistance if clothing is laid out or handed to the patient.
⃞ 2 - Someone must help the patient put on upper body clothing.
⃞ 3 - Patient depends entirely upon another person to dress the upper body.
(M1820) Current Ability to Dress Lower Body safely (with or without dressing aids) including undergarments, slacks, socks or nylons, shoes:
⃞ 0 - Able to obtain, put on, and remove clothing and shoes without assistance.
⃞ 1 - Able to dress lower body without assistance if clothing and shoes are laid out or handed to the
patient.
⃞ 2 - Someone must help the patient put on undergarments, slacks, socks or nylons, and shoes.
⃞ 3 - Patient depends entirely upon another person to dress lower body.
(M1830) Bathing: Current ability to wash entire body safely. Excludes grooming (washing face, washing hands, and shampooing hair).
⃞ 0 - Able to bathe self in shower or tub independently, including getting in and out of tub/shower.
⃞ 1 - With the use of devices, is able to bathe self in shower or tub independently, including getting in and
out of the tub/shower.
⃞ 2 - Able to bathe in shower or tub with the intermittent assistance of another person:
(a) for intermittent supervision or encouragement or reminders, OR (b) to get in and out of the shower or tub, OR (c) for washing difficult to reach areas.
⃞ 3 - Able to participate in bathing self in shower or tub, but requires presence of another person
throughout the bath for assistance or supervision.
⃞ 4 - Unable to use the shower or tub, but able to bathe self independently with or without the use of
devices at the sink, in chair, or on commode.
⃞ 5 - Unable to use the shower or tub, but able to participate in bathing self in bed, at the sink, in bedside
chair, or on commode, with the assistance or supervision of another person throughout the bath.
⃞ 6 - Unable to participate effectively in bathing and is bathed totally by another person.
230

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 17 of 24
(M1840) Toilet Transferring: Current ability to get to and from the toilet or bedside commode safely and transfer on and off toilet/commode.
⃞ 0 - Able to get to and from the toilet and transfer independently with or without a device.
⃞ 1 - When reminded, assisted, or supervised by another person, able to get to and from the toilet and
transfer.
⃞ 2 - Unable to get to and from the toilet but is able to use a bedside commode (with or without
assistance).
⃞ 3 - Unable to get to and from the toilet or bedside commode but is able to use a bedpan/urinal
independently.
⃞ 4 - Is totally dependent in toileting.
(M1845) Toileting Hygiene: Current ability to maintain perineal hygiene safely, adjust clothes and/or incontinence pads before and after using toilet, commode, bedpan, urinal. If managing ostomy, includes cleaning area around stoma, but not managing equipment.
⃞ 0 - Able to manage toileting hygiene and clothing management without assistance.
⃞ 1 - Able to manage toileting hygiene and clothing management without assistance if supplies/implements are laid out for the patient.
⃞ 2 - Someone must help the patient to maintain toileting hygiene and/or adjust clothing.
⃞ 3 - Patient depends entirely upon another person to maintain toileting hygiene.
(M1850) Transferring: Current ability to move safely from bed to chair, or ability to turn and position self in bed if patient is bedfast.
⃞ 0 - Able to independently transfer.
⃞ 1 - Able to transfer with minimal human assistance or with use of an assistive device.
⃞ 2 - Able to bear weight and pivot during the transfer process but unable to transfer self.
⃞ 3 - Unable to transfer self and is unable to bear weight or pivot when transferred by another person.
⃞ 4 - Bedfast, unable to transfer but is able to turn and position self in bed.
⃞ 5 - Bedfast, unable to transfer and is unable to turn and position self.
(M1860) Ambulation/Locomotion: Current ability to walk safely, once in a standing position, or use a wheelchair, once in a seated position, on a variety of surfaces.
⃞ 0 - Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device).
⃞ 1 - With the use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or without railings.
⃞ 2 - Requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.
⃞ 3 - Able to walk only with the supervision or assistance of another person at all times.
⃞ 4 - Chairfast, unable to ambulate but is able to wheel self independently.
⃞ 5 - Chairfast, unable to ambulate and is unable to wheel self.
⃞ 6 - Bedfast, unable to ambulate or be up in a chair.
(M1870) Feeding or Eating: Current ability to feed self meals and snacks safely. Note: This refers only to the process of eating, chewing, and swallowing, not preparing the food to be eaten.
⃞ 0 - Able to independently feed self.
⃞ 1 - Able to feed self independently but requires:
(a) meal set-up; OR (b) intermittent assistance or supervision from another person; OR (c) a liquid, pureed or ground meat diet.
⃞ 2 - Unable to feed self and must be assisted or supervised throughout the meal/snack.
⃞ 3 - Able to take in nutrients orally and receives supplemental nutrients through a nasogastric tube or gastrostomy.
⃞ 4 - Unable to take in nutrients orally and is fed nutrients through a nasogastric tube or gastrostomy.
⃞ 5 - Unable to take in nutrients orally or by tube feeding.
231

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 18 of 24
(M1880) Current Ability to Plan and Prepare Light Meals (e.g., cereal, sandwich) or reheat delivered meals safely:
⃞ 0 - (a) Able to independently plan and prepare all light meals for self or reheat delivered meals; OR
(b) Is physically, cognitively, and mentally able to prepare light meals on a regular basis but has not routinely performed light meal preparation in the past (i.e., prior to this home care admission).
⃞ 1 - Unable to prepare light meals on a regular basis due to physical, cognitive, or mental limitations.
⃞ 2 - Unable to prepare any light meals or reheat any delivered meals.
(M1890) Ability to Use Telephone: Current ability to answer the phone safely, including dialing numbers, and effectively using the telephone to communicate.
⃞ 0 - Able to dial numbers and answer calls appropriately and as desired.
⃞ 1 - Able to use a specially adapted telephone (i.e., large numbers on the dial, teletype phone for the
deaf) and call essential numbers.
⃞ 2 - Able to answer the telephone and carry on a normal conversation but has difficulty with placing calls.
⃞ 3 - Able to answer the telephone only some of the time or is able to carry on only a limited conversation.
⃞ 4 - Unable to answer the telephone at all but can listen if assisted with equipment.
⃞ 5 - Totally unable to use the telephone.
⃞ NA - Patient does not have a telephone.
(M1900) Prior Functioning ADL/IADL: Indicate the patient’s usual ability with everyday activities prior to this current illness, exacerbation, or injury. Check only one box in each row.
Functional Area Independent Needed Some
Help Dependent
a. Self-Care (e.g., grooming, dressing, and bathing)
⃞0 ⃞1 ⃞2
b. Ambulation ⃞0 ⃞1 ⃞2
c. Transfer ⃞0 ⃞1 ⃞2
d. Household tasks (e.g., light meal preparation, laundry, shopping )
⃞0 ⃞1 ⃞2
(M1910) Has this patient had a multi-factor Fall Risk Assessment (such as falls history, use of multiple medications,
mental impairment, toileting frequency, general mobility/transferring impairment, environmental hazards)?
⃞ 0 - No multi-factor falls risk assessment conducted.
⃞ 1 - Yes, and it does not indicate a risk for falls.
⃞ 2 - Yes, and it indicates a risk for falls.
MEDICATIONS
(M2000) Drug Regimen Review: Does a complete drug regimen review indicate potential clinically significant
medication issues, e.g., drug reactions, ineffective drug therapy, side effects, drug interactions, duplicate therapy, omissions, dosage errors, or noncompliance?
⃞ 0 - Not assessed/reviewed [ Go to M2010 ]
⃞ 1 - No problems found during review [ Go to M2010 ]
⃞ 2 - Problems found during review
⃞ NA - Patient is not taking any medications [ Go to M2040 ]
(M2002) Medication Follow-up: Was a physician or the physician-designee contacted within one calendar day to
resolve clinically significant medication issues, including reconciliation?
⃞ 0 - No
⃞ 1 - Yes
232

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 19 of 24
(M2004) Medication Intervention: If there were any clinically significant medication issues since the previous OASIS
assessment, was a physician or the physician-designee contacted within one calendar day of the assessment to resolve clinically significant medication issues, including reconciliation?
⃞ 0 - No
⃞ 1 - Yes
⃞ NA - No clinically significant medication issues identified since the previous OASIS assessment
(M2010) Patient/Caregiver High Risk Drug Education: Has the patient/caregiver received instruction on special
precautions for all high-risk medications (such as hypoglycemics, anticoagulants, etc.) and how and when to report problems that may occur?
⃞ 0 - No
⃞ 1 - Yes
⃞ NA - Patient not taking any high risk drugs OR patient/caregiver fully knowledgeable about special
precautions associated with all high-risk medications
(M2015) Patient/Caregiver Drug Education Intervention: Since the previous OASIS assessment, was the
patient/caregiver instructed by agency staff or other health care provider to monitor the effectiveness of drug therapy, drug reactions, and side effects, and how and when to report problems that may occur?
⃞ 0 - No
⃞ 1 - Yes
⃞ NA - Patient not taking any drugs
(M2020) Management of Oral Medications: Patient's current ability to prepare and take all oral medications reliably and safely, including administration of the correct dosage at the appropriate times/intervals. Excludes injectable and IV medications. (NOTE: This refers to ability, not compliance or willingness.)
⃞ 0 - Able to independently take the correct oral medication(s) and proper dosage(s) at the correct times.
⃞ 1 - Able to take medication(s) at the correct times if:
(a) individual dosages are prepared in advance by another person; OR (b) another person develops a drug diary or chart.
⃞ 2 - Able to take medication(s) at the correct times if given reminders by another person at the
appropriate times
⃞ 3 - Unable to take medication unless administered by another person.
⃞ NA - No oral medications prescribed.
(M2030) Management of Injectable Medications: Patient's current ability to prepare and take all prescribed
injectable medications reliably and safely, including administration of correct dosage at the appropriate times/intervals. Excludes IV medications.
⃞ 0 - Able to independently take the correct medication(s) and proper dosage(s) at the correct times.
⃞ 1 - Able to take injectable medication(s) at the correct times if:
(a) individual syringes are prepared in advance by another person; OR (b) another person develops a drug diary or chart.
⃞ 2 - Able to take medication(s) at the correct times if given reminders by another person based on the
frequency of the injection
⃞ 3 - Unable to take injectable medication unless administered by another person.
⃞ NA - No injectable medications prescribed.
(M2040) Prior Medication Management: Indicate the patient’s usual ability with managing oral and injectable medications prior to this current illness, exacerbation, or injury. Check only one box in each row.
Functional Area Independent Needed Some
Help Dependent Not Applicable
a. Oral medications ⃞0 ⃞1 ⃞2 ⃞na
b. Injectable medications ⃞0 ⃞1 ⃞2 ⃞na
233

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 20 of 24
CARE MANAGEMENT
(M2100) Types and Sources of Assistance: Determine the level of caregiver ability and willingness to provide assistance for the following activities, if assistance is needed. (Check only one box in each row.)
Type of Assistance
No assistance needed in this area
Caregiver(s) currently provide
assistance
Caregiver(s) need training/
supportive services to
provide assistance
Caregiver(s) not likely to
provide assistance
Unclear if Caregiver(s) will provide assistance
Assistance needed, but
no Caregiver(s)
available
a. ADL assistance
(e.g., transfer/ ambulation, bathing, dressing, toileting, eating/feeding)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4 ⃞5
b. IADL assistance
(e.g., meals, housekeeping, laundry, telephone, shopping, finances)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4 ⃞5
c. Medication administration (e.g.,
oral, inhaled or injectable)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4 ⃞5
d. Medical procedures/ treatments (e.g.,
changing wound dressing)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4 ⃞5
e. Management of Equipment (includes
oxygen, IV/infusion equipment, enteral/ parenteral nutrition, ventilator therapy equipment or supplies)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4 ⃞5
f. Supervision and safety (e.g., due to
cognitive impairment) ⃞0 ⃞1 ⃞2 ⃞3 ⃞4 ⃞5
g. Advocacy or facilitation of
patient's participation in appropriate medical care (includes transporta-tion to or from appointments)
⃞0 ⃞1 ⃞2 ⃞3 ⃞4 ⃞5
234

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 21 of 24
(M2110) How Often does the patient receive ADL or IADL assistance from any caregiver(s) (other than home health agency staff)?
⃞ 1 - At least daily
⃞ 2 - Three or more times per week
⃞ 3 - One to two times per week
⃞ 4 - Received, but less often than weekly
⃞ 5 - No assistance received
⃞ UK - Unknown [Omit ―UK‖ option on DC]
THERAPY NEED AND PLAN OF CARE
(M2200) Therapy Need: In the home health plan of care for the Medicare payment episode for which this assessment
will define a case mix group, what is the indicated need for therapy visits (total of reasonable and necessary physical, occupational, and speech-language pathology visits combined)? (Enter zero [ ―000‖ ] if no therapy visits indicated.)
(__ __ __) Number of therapy visits indicated (total of physical, occupational and speech-language pathology combined).
⃞ NA - Not Applicable: No case mix group defined by this assessment.
(M2250) Plan of Care Synopsis: (Check only one box in each row.) Does the physician-ordered plan of care
include the following:
Plan / Intervention No Yes Not Applicable
a. Patient-specific parameters for notifying physician of changes in vital signs or other clinical findings
⃞0 ⃞1 ⃞na Physician has chosen not to establish patient-specific parameters for this patient. Agency will use standardized clinical guidelines accessible for all care providers to reference
b. Diabetic foot care including monitoring for the presence of skin lesions on the lower extremities and patient/caregiver education on proper foot care
⃞0 ⃞1 ⃞na Patient is not diabetic or is bilateral amputee
c. Falls prevention interventions ⃞0 ⃞1 ⃞na Patient is not assessed to be at risk for falls
d. Depression intervention(s) such as medication, referral for other treatment, or a monitoring plan for current treatment
⃞0 ⃞1 ⃞na Patient has no diagnosis or symptoms of depression
e. Intervention(s) to monitor and mitigate pain ⃞0 ⃞1 ⃞na No pain identified
f. Intervention(s) to prevent pressure ulcers ⃞0 ⃞1 ⃞na Patient is not assessed to be at risk for pressure ulcers
g. Pressure ulcer treatment based on principles of moist wound healing OR order for treatment based on moist wound healing has been requested from physician
⃞0 ⃞1 ⃞na Patient has no pressure ulcers with need for moist wound healing
235

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 22 of 24
EMERGENT CARE
(M2300) Emergent Care: Since the last time OASIS data were collected, has the patient utilized a hospital
emergency department (includes holding/observation)?
⃞ 0 - No [ Go to M2400 ]
⃞ 1 - Yes, used hospital emergency department WITHOUT hospital admission
⃞ 2 - Yes, used hospital emergency department WITH hospital admission
⃞ UK - Unknown [ Go to M2400 ]
(M2310) Reason for Emergent Care: For what reason(s) did the patient receive emergent care (with or without hospitalization)? (Mark all that apply.)
⃞ 1 - Improper medication administration, medication side effects, toxicity, anaphylaxis
⃞ 2 - Injury caused by fall
⃞ 3 - Respiratory infection (e.g., pneumonia, bronchitis)
⃞ 4 - Other respiratory problem
⃞ 5 - Heart failure (e.g., fluid overload)
⃞ 6 - Cardiac dysrhythmia (irregular heartbeat)
⃞ 7 - Myocardial infarction or chest pain
⃞ 8 - Other heart disease
⃞ 9 - Stroke (CVA) or TIA
⃞ 10 - Hypo/Hyperglycemia, diabetes out of control
⃞ 11 - GI bleeding, obstruction, constipation, impaction
⃞ 12 - Dehydration, malnutrition
⃞ 13 - Urinary tract infection
⃞ 14 - IV catheter-related infection or complication
⃞ 15 - Wound infection or deterioration
⃞ 16 - Uncontrolled pain
⃞ 17 - Acute mental/behavioral health problem
⃞ 18 - Deep vein thrombosis, pulmonary embolus
⃞ 19 - Other than above reasons
⃞ UK - Reason unknown
236

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 23 of 24
DATA ITEMS COLLECTED AT INPATIENT FACILITY ADMISSION OR AGENCY DISCHARGE ONLY
(M2400) Intervention Synopsis: (Check only one box in each row.) Since the previous OASIS assessment, were the
following interventions BOTH included in the physician-ordered plan of care AND implemented?
Plan / Intervention No Yes Not Applicable
a. Diabetic foot care including monitoring for the presence of skin lesions on the lower extremities and patient/caregiver education on proper foot care
⃞0 ⃞1 ⃞na Patient is not diabetic or is bilateral amputee
b. Falls prevention interventions ⃞0 ⃞1 ⃞na Formal multi-factor Fall Risk Assessment indicates the patient was not at risk for falls since the last OASIS assessment
c. Depression intervention(s) such as medication, referral for other treatment, or a monitoring plan for current treatment
⃞0 ⃞1 ⃞na Formal assessment indicates patient did not meet criteria for depression AND patient did not have diagnosis of depression since the last OASIS assessment
d. Intervention(s) to monitor and mitigate pain ⃞0 ⃞1 ⃞na Formal assessment did not indicate pain since the last OASIS assessment
e. Intervention(s) to prevent pressure ulcers ⃞0 ⃞1 ⃞na Formal assessment indicates the patient was not at risk of pressure ulcers since the last OASIS assessment
f. Pressure ulcer treatment based on principles of moist wound healing
⃞0 ⃞1 ⃞na Dressings that support the principles of moist wound healing not indicated for this patient’s pressure ulcers OR patient has no pressure ulcers with need for moist wound healing
(M2410) To which Inpatient Facility has the patient been admitted?
⃞ 1 - Hospital [ Go to M2430 ]
⃞ 2 - Rehabilitation facility [ Go to M0903 ]
⃞ 3 - Nursing home [ Go to M2440 ]
⃞ 4 - Hospice [ Go to M0903 ]
⃞ NA - No inpatient facility admission [Omit ―NA‖ option on TRN]
(M2420) Discharge Disposition: Where is the patient after discharge from your agency? (Choose only one answer.)
⃞ 1 - Patient remained in the community (without formal assistive services)
⃞ 2 - Patient remained in the community (with formal assistive services)
⃞ 3 - Patient transferred to a non-institutional hospice
⃞ 4 - Unknown because patient moved to a geographic location not served by this agency
⃞ UK - Other unknown
[ Go to M0903 ]
237

OMB #0938-0760 Expiration date 12/31/2014
OASIS-C: All Items Centers for Medicare & Medicaid Services August 2009 Page 24 of 24
(M2430) Reason for Hospitalization: For what reason(s) did the patient require hospitalization? (Mark all that apply.)
⃞ 1 - Improper medication administration, medication side effects, toxicity, anaphylaxis
⃞ 2 - Injury caused by fall
⃞ 3 - Respiratory infection (e.g., pneumonia, bronchitis)
⃞ 4 - Other respiratory problem
⃞ 5 - Heart failure (e.g., fluid overload)
⃞ 6 - Cardiac dysrhythmia (irregular heartbeat)
⃞ 7 - Myocardial infarction or chest pain
⃞ 8 - Other heart disease
⃞ 9 - Stroke (CVA) or TIA
⃞ 10 - Hypo/Hyperglycemia, diabetes out of control
⃞ 11 - GI bleeding, obstruction, constipation, impaction
⃞ 12 - Dehydration, malnutrition
⃞ 13 - Urinary tract infection
⃞ 14 - IV catheter-related infection or complication
⃞ 15 - Wound infection or deterioration
⃞ 16 - Uncontrolled pain
⃞ 17 - Acute mental/behavioral health problem
⃞ 18 - Deep vein thrombosis, pulmonary embolus
⃞ 19 - Scheduled treatment or procedure
⃞ 20 - Other than above reasons
⃞ UK - Reason unknown
[ Go to M0903 ]
(M2440) For what Reason(s) was the patient Admitted to a Nursing Home? (Mark all that apply.)
⃞ 1 - Therapy services
⃞ 2 - Respite care
⃞ 3 - Hospice care
⃞ 4 - Permanent placement
⃞ 5 - Unsafe for care at home
⃞ 6 - Other
⃞ UK - Unknown
[ Go to M0903 ]
(M0903) Date of Last (Most Recent) Home Visit:
__ __ /__ __ / __ __ __ __ month / day / year
(M0906) Discharge/Transfer/Death Date: Enter the date of the discharge, transfer, or death (at home) of the patient.
__ __ /__ __ / __ __ __ __ month / day / year
238

239
National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Health and Health Care
The CLAS standards are intended to advance health equity, improve quality, and help eliminate health care disparities by establishing a blueprint for health and health care organizations: Principal Standard 1. Provide effective, equitable, understandable, and respectful quality care and services that are responsive to diverse cultural health beliefs and practices, preferred languages, health literacy, and other communication needs. Governance, Leadership, and Workforce 2. Advance and sustain organizational governance and leadership that promotes CLAS and health equity through policy, practices, and allocated resources. 3. Recruit, promote, and support a culturally and linguistically diverse governance, leadership, and workforce that are responsive to the population in the service area. 4. Educate and train governance, leadership, and workforce in culturally and linguistically appropriate policies and practices on an ongoing basis. Communication and Language Assistance 5. Offer language assistance to individuals who have limited English proficiency or other communication needs, at no cost to them, to facilitate timely access to all health care and services. 6. Inform all individuals of the availability of language assistance services clearly and in their preferred language, orally and in writing. 7. Ensure the competence of individuals providing language assistance, recognizing that the use of untrained individuals or minors as interpreters should be avoided. 8. Provide easy-to-understand print and multimedia materials and signage in the languages commonly used by the populations in the service area. Engagement, Continuous Improvement, and Accountability 9. Establish culturally and linguistically appropriate goals, policies, and management accountability and infuse them throughout the organization’s planning and operations. 10. Conduct ongoing assessments of the organization’s CLAS-related activities and integrate CLAS-related measures into measurement and continuous quality improvement activities. 11. Collect and maintain accurate and reliable demographic data to monitor and evaluate the impact of CLAS on health equity and outcomes and to inform service delivery. 12. Conduct regular assessments of community health assets and needs and use the results to plan and implement services that respond to the cultural and linguistic

240
diversity of populations in the service area. 13. Partner with the community to design, implement, and evaluate policies, practices, and services to ensure cultural and linguistic appropriateness. 14. Create processes for conflict and grievance resolution that are culturally and linguistically appropriate to identify, prevent, and resolve conflicts or complaints. 15. Communicate the organization’s progress in implementing and sustaining CLAS National standards for culturally and linguistically appropriate services in health and health care: a blueprint for advancing and sustaining CLAS policy and practice. Washington,DC: Office of Minority Health, Department of Health and Human Services, April 2013.