Embed Size (px)
Citation preview

Functional Dyspepsia: A Case-Based Approach

Case Study
• Christina is a 32-year-old woman referred for the evaluation of a 1-year history of upper gastrointestinal discomfort.
• She describes a daily, persistent ache or discomfort that waxes and wanes.
– Occasional heartburn
• Eating seems to make the pain worse, and she feels very full even after eating only a modest-sized meal.
• Her weight has remained stable for the past year.

Case Study
• Previously healthy female– 2-3 glasses of wine/week; no tobacco
– High fiber diet
• PShx: Appendectomy (childhood)
• Meds: OCPs and occasional NSAIDS– H2RAs tried x 1 month: no benefit
• Family Hx: Gallstones; IBS
• Physical exam: Epigastric tenderness o/w normal

Symptoms which are consideredto originate from the gastroduodenal region
Symptoms which are consideredto originate from the gastroduodenal region
Uninvestigated dyspepsiaUninvestigated dyspepsia
Functional dyspepsiaFunctional dyspepsia
Organic dyspepsiaOrganic
dyspepsia
EndoscopyEndoscopy
DyspepsiaDyspepsiaDyspepsiaDyspepsia
1313
30%
70%

Dyspepsia: Epidemiology and Burden of Illness
• 25% of the adult US population experiences recurrent dyspepsia.
• Less than 50% of those with symptoms of dyspepsia seek medical care.
• Dyspepsia accounts for up to 5% of all family practice consultations.
• Dyspepsia has a significant impact on quality of life.
Talley NJ et al. Gastroenterology. 1998;114: 582-595.Tougas G et al. Am J Gastroenterol. 1999;94: 2845-2854.
Talley NJ et al. Gastroenterology. 1998;114: 582-595.Tougas G et al. Am J Gastroenterol. 1999;94: 2845-2854.

The Economics of Dyspepsia
• It is estimated that 10% of all healthcare expenditures in the United Kingdom go towards treating dyspepsia.
• In the United States, direct costs (diagnostic studies, emergency room visits, medications) and indirect costs (absenteeism, presenteeism) for dyspepsia amount to more than $2 billion/year.
Soo S et al. Cochrane Database Sys Rev. 2000;2;CD001960.American Gastroenterological Association. The Burden of Gastrointestinal Diseases. 2001.
Soo S et al. Cochrane Database Sys Rev. 2000;2;CD001960.American Gastroenterological Association. The Burden of Gastrointestinal Diseases. 2001.

Organic vs Functional Dyspepsia
Tack J et al. Gastroenterology. 2006;130:1466-1479.Tack J et al. Gastroenterology. 2006;130:1466-1479.
DyspepsiaDyspepsia
Identifiable cause for symptoms
• Peptic ulcer
• GERD (± esophagitis)
• Malignancy
• Pancreaticobiliary disease
• Medication
No identifiable explanation
• Unidentified pathophysiological or microbiological abnormality
• Abnormal motor or sensory function
– Altered gastric emptying– Fundic dysaccommodation– Gastroduodenal hypersensitivity
GERD, gastroesophageal reflux disease.

Disrupted gut–immune interactions
Altered brain–gut interactions
Saad RJ et al. Aliment Pharmacol Ther. 2006;24:475-492.Tack J et al. Gastroenterology. 2006;130:1466-1479.
Saad RJ et al. Aliment Pharmacol Ther. 2006;24:475-492.Tack J et al. Gastroenterology. 2006;130:1466-1479.
Visceral hypersensitivity
• abnormal sensitivity to acid
Geneticfactors
Psychosocialfactors
Abnormal upper motor
+ reflex function: Gastric emptying• Dysaccommodation
FunctionalFunctionalDyspepsiaDyspepsia
Proposed Pathophysiological Mechanisms Involved in Functional Dyspepsia

GI Motility Disturbances in Dyspepsia
Dysfunction of visceral afferents
Gastric myoelectrical dysrhythmias
Antroduodenal dyscoordination
Postprandial antral hypomotility
Impaired fundic accommodation
Diagram adapted from Quigley EM. Aliment Pharmacol Ther. 2004;20:56-60.Kellow JE. Med J Aust. 1992;157:385-388.
Diagram adapted from Quigley EM. Aliment Pharmacol Ther. 2004;20:56-60.Kellow JE. Med J Aust. 1992;157:385-388.
Delayed gastric emptying
Presenting symptoms
Upper abdominal pain
Postprandial abdominal bloating
Nausea Postprandial belching
Vomiting Anorexia
Early satiety

Options forUninvestigated Dyspepsia
Tack J et al. Gastroenterology. 1998;114:582-595.Tack J et al. Gastroenterology. 1998;114:582-595.
Test and treatfor H pylori
Prompt EGD• Age >45–50• Warning signs
Empirictherapy
Uninvestigateddyspepsia
Uninvestigateddyspepsia
EGD, esophagogastroduodenoscopy.

Endoscopy in Uninvestigated Dyspepsia• In patients younger than 55 diagnosed with
dyspepsia, the incidence of gastroesophageal malignancy was 1.06 per million population/year.1
• Gastric cancer was present in less than 1 per 1000 patients with dyspeptic symptoms without warning signs who underwent endoscopy.2
• No cases of gastric cancer were observed in 1886 patients with dyspepsia who underwent endoscopy; 61% of these cases were functional in nature (28% were acid related and 11% were non-acid related).3
1. Gillen D. Am J Gastroenterol. 1999;94:2329-2330; 2. Breslin NP et al. Gut. 2000;46:93-97; 3. Froelich JW et al. Am J Gastroenterol. 2001;96:.

Initial Management of Uninvestigated Dyspepsia: Pros and Cons of Immediate EGD
Cash BD et al. In: Hot Topics. 2003.Cash BD et al. In: Hot Topics. 2003.
Advantages Disadvantages Usefulness
• Provides reassurance to patient and doctor
• Allows targeted therapy and the potential for fewer prescriptions
• Expensive
• Invasive, with small risk for complications
• Lack of infrastructure to provide EGD to all patients with dyspepsia
• Patients with symptom onset after age 45 to 50 or with alarm features
• Nonresponders to initial test and treat, empiric therapy, or both

• Noninvasive
• Cure/symptomatic benefit in thosewith PUD
• Leads to similar outcomes compared with early EGD
• May reduce costs by reducing endoscopy workload and medication use
• Patients less satisfied with test and treatthan with endoscopy
• May avert endoscopy in only a minority of patients
• Curing H pylori improves symptoms in <50% of patients
• Effect on GERD?
• Young patients without alarm features in regions in which gastric cancer is rare
• Likely cost-effective in areas of highH pylori/ulcer prevalence
Initial Management of Uninvestigated Dyspepsia: Pros and Cons of Test and Treat
AdvantagesAdvantages DisadvantagesDisadvantages UsefulnessUsefulness
Cash BD et al. In: Hot Topics. 2003.Cash BD et al. In: Hot Topics. 2003.PUD, peptic ulcer disease.

Initial Management of Uninvestigated Dyspepsia: Pros and Cons of Empiric Therapy
OTC, over the counter; H2RA, histamine type-2 receptor antagonist; PPI, proton pump inhibitor.
• Widely available
• Excellent safety record
• Inexpensive for those with few recurrences
Advantages
• Can rarely mask serious disease
• May only postpone investigation
• Can result in chronic medication use
• ? Potential for AEs with long-term PPI use
Disadvantages
• First onset of dyspepsia ofshort duration
• Young patients with dyspepsia without alarm features
• Likely cost-effective in areas of low H pylori/ulcer prevalence
Usefulness
• OTC antacid
• OTC H2RAor PPI
• Prescription H2RA, PPI
Strategy
Cash BD et al. In: Hot Topics. 2003.Cash BD et al. In: Hot Topics. 2003.

Uninvestigated Dyspepsia: Summary
• One size does not fit all• Factors favor the cost-effectiveness of empiric
antisecretory therapy over test and treat in many parts of the United States.– Decreasing H pylori and PUD prevalence– Decreasing proportion of ulcers caused by H pylori– Decreasing PPI costs
• The cost-effectiveness of combining empiric therapy and test and treat deserves further study.– High H pylori prevalence: test and treat and PPI for
nonresponders?– Low H pylori prevalence: PPI and test and treat for
responders?

Case Study
• Treated with PPI (once daily)
• Labs normal except for + H pylori– Treated (triple therapy)
• Heartburn improved; epigastric pain worse– Post-prandial nausea, bloating, constipation, lower
abdominal pain develop
• EGD performed: non-specific erythema– Biopsies normal
• Diagnosed with Functional Dyspepsia

Presence of one or more of the following symptoms, thought to originate in the gastroduodenal region
Presence of one or more of the following symptoms, thought to originate in the gastroduodenal region
Rome III Criteria: Functional Dyspepsia
Tack J et al. Gastroenterology. 2006;130:1466-1479.Tack J et al. Gastroenterology. 2006;130:1466-1479.
No evidence of structural disease to explain the symptoms and
*Symptoms present for the past 3 months, withonset at least 6 months before diagnosis
*Symptoms present for the past 3 months, withonset at least 6 months before diagnosis
Epigastricburning
Epigastricburning
Bothersome postprandialfullness after
ordinary sized meals
Bothersome postprandialfullness after
ordinary sized meals
Early satiety that prevents
finishing a regularsized meal
Early satiety that prevents
finishing a regularsized meal
Epigastricpain
Epigastricpain
*New with Rome III criteria.*New with Rome III criteria.
Postprandial distress syndrome
(PDS): Meal-related FDEpigastric pain syndrome (EPS)

DyspepsiaGERD
IBSChronic
Constipation(CC)
Abdominal pain
Regurgitation
Heartburn
DiscomfortBelching
Bloating
Constipation
Locke 3rd, et al. Neurogastroenterol Motil. 2005;17(1):29–34Corazziari. Best Pract Res Clin Gastroenterol. 2004;18(4):613–31
Talley et al. Am J Gastroenterol. 2003;98(11):2454–9
Overlap of GI motility and sensory disorders
• Diagnosis can shift from one disorder to another over time

Functional Dyspepsia: Unclear Natural History
• 80% of patients have symptoms 18 to 24 months after diagnosis.1
• 74% of patients have symptoms 12 to 24 months later.2
• In contrast, some studies have shown that 30% to 50% of patients experience resolution of symptoms over the course of 12 to 24 months.3,4
1. Talley NJ et al. Am J Epidemiol. 1992;136:165-177.2. Jones R et al. Br J Clin Pract. 1992;46:95-97.
3. Bonnevie O et al. Scand J Gastroenterol. 1982;17:1073-1076. 4. Sloth H et al. Scand J Gastroenterol. 1989;24:440-444.

Questions to Ask
• What is your most bothersome symptom?
• What other symptoms do you experience frequently?
• How do your symptoms affect your life?
• How do you explain your symptoms to family or friends?
• Why do you think you developed these symptoms?
• What is your greatest concern about having dyspepsia?
• What other concerns do you have about your symptoms?

Case Study
• Desipramine begun (10 mg q.h.s.)– Epigastric discomfort improved; no other changes
• RUQ ultrasound, celiac abs: normal• Lactose free diet: no benefit• Desipramine increased (50 mg q.h.s.)
– Groggy, constipation worse
• Metoclopramide started/desipramine stopped– Nausea/bloating improve; constipation and
epigastric discomfort unchanged
• PEG started/ metoclopramide increased

Current Management of Functional Dyspepsia
• Lifestyle changes
• H pylori eradication
• Antisecretory therapy
• Prokinetics
• Antinociceptive agents
• Psychological therapies
Functional Dyspepsia
70%

Treatment of Functional Dyspepsia: Lifestyle Modifications
• No RCTs evaluate the role of diet or exercise.
• Smaller, more frequent meals may benefit some patients.
• Low-fat diets may lessen symptoms in some patients with FD.1,2
• Monitor medications, especially NSAIDs, ASA products, iron, and antibiotics.
1. Mullan A. Eur J Clin Nutr 1994;48:97-105. 2. Barbera RC et al. Eur J Gastroenterol Hepatol. 1995;7:1051-1057.
RCT, randomized-controlled trial; FD, functional dyspepsia;
ASA, acetylsalicylic acid.

Cochrane Collaboration Meta-Analysis of H pylori Cure for Functional Dyspepsia
• 12 RCTs (2903 patients)
• Mean response rate– Placebo, 29% (range, 7%-51%)
– H pylori cure, 37% (range, 21%-62%)
• Relative risk of symptoms remaining– 0.91 (95% CI, 0.86-0.95)
• NNT = 15 (95% CI, 10-28)
• Second meta-analysis of 10 RCTs in patients with FD followed up for 1 year after treatment for H pylori did not show any benefit in resolution of dyspepsia symptoms compared with placebo.
Moayyedi P et al. Am J Gastroenterol. 2003;98:2621-2626. Laine L et al. Ann Intern Med. 2001;134:361-369.
Moayyedi P et al. Am J Gastroenterol. 2003;98:2621-2626. Laine L et al. Ann Intern Med. 2001;134:361-369.NNT, number needed to treat.

H pylori Eradication in Functional Dyspepsia: The Bottom Line
• H pylori cure may offer benefit in a subset of patients with FD.– No reliable method exists to identify those likely to
respond.
– Overall benefits on a population basis are likely to be small.
– If a chemopreventive benefit of H pylori cure for gastric cancer can be demonstrated,1 the balance will clearly favor treatment.
1Uemura NEJM 20011. Uemura N. N Engl J Med. 2001;345:829-832.

Rationale for Antisecretory Therapy in Functional Dyspepsia• Overlap of GERD and dyspepsia symptoms
– Gastric acid secretion in patients with FD similar to that in controls1
• Acid hypersensitivity– Lowers threshold of mechanosensitive afferents2
– Increases nausea with duodenal acid infusion3
• Abnormal clearance from the duodenum3
– Decreases fasting clearance of exogenous acid
– Decreases fasting duodenal motor activity
1. Collen MJ. Dig Dis Sci. 1989;34:246-250.2. Sansom MS et al. Gastroenterology. 1999;116:515.
3. Coffin B et al. Am J Physiol Gastrointest Liver Physiol. 2001;280:G904-G909.

H2RAs for Functional Dyspepsia
• Meta-analysis (2001)
• 22 RCTs in patients with nonulcer dyspepsia
• 14 studies, parallel group; 8 studies, crossover
• 15 of 22 studies found H2RA superior to placebo at relieving epigastric pain but not global symptoms of dyspepsia
• Significant design flaws in many studies, including crossover design and inclusion of GERD-predominant patients
Redstone HA et al. Aliment Pharmacol Ther. 2001;15:1291-1299.

Cochrane Collaboration Meta-Analysis of PPI Therapy for Functional Dyspepsia
• 7 RCTs (3031 patients)
• PPI for 2 to 8 weeks was superior to placebo in relieving symptoms of nonulcer dyspepsia
• Relative risk of symptoms remaining– 0.86 (95% CI, 0.80-0.93)
• NNT = 9 (95% CI, 6-26)– Six RCTs (2032 patients) found no difference
between low-dose and standard-dose PPI for FD
Moayyedi P et al. Gut. 2003;52(suppl 1):A16.Moayyedi P et al. Gut. 2003;52(suppl 1):A16.

Which Functional Dyspepsia Patients Are Most Likely to Improve With PPI Therapy?
• Retrospective analysis of BOND and OPERA studies (826 patients randomly assigned to omeprazole 10 mg, 20 mg, or placebo)
• Treatment success defined as complete absence of symptoms on last 3 days of week 4
• Predictors of success– Fewer days with symptoms during week 1 of therapy
– Age older than 40
– Presence of heartburn
– Less bloating, epigastric pain, diarrhea
– Short duration of symptoms (<3 months) Moayyedi P et al. Aliment Pharmacol Ther. 2003;18:117.Moayyedi P et al. Aliment Pharmacol Ther. 2003;18:117.

Emerging Therapies for Functional Dyspepsia
• Antidepressants
• Serotonergic agents
• Dopaminergic agents
• CAM– Cognitive/hypnotherapy
– Capsaicin
– Herbals

Prokinetic Agents for the Treatment of Functional Dyspepsia
Physiological effects
AgentPrimary
mode of action AntiemeticGastric
emptyingVisceral
sensitivity
Gastric antral
motility
Gastric fundic
accommodation
MetoclopramideDopamine antagonist5-HT4 agonist ↑ ↓ ↑
DomperidoneDopamine antagonist ↑ ↓
Tegaserod 5-HT4 agonist ↑ ↓ ↑ ↑
LevosulpirideDopamine antagonist5-HT4 agonist ↑ ↓ ↑
Saad RJ. Aliment Pharmacol Ther. 2006;24:475-492.Saad RJ. Aliment Pharmacol Ther. 2006;24:475-492.

Antidepressants for Functional Dyspepsia• Reserved for moderate to severe symptoms
• Tricyclic antidepressants (TCAs)– Visceral and somatic perception are altered with TCAs.1
– Study in 7 patients found that amitryptiline improved symptoms but did not alter sensation of gastric distention.2
– Meta-analysis in patients with FGIDs found improvement of global symptoms (OR = 4.2; NNT = 3.2) and pain.3
• Selective serotonin reuptake inhibitors (SSRIs)– Paroxetine did not alter perception of gastric distention but
did enhance gastric accommodation in healthy volunteers.4
– No RCT findings have been published for FD.1. Gorelick AB et al. Am J Physiol. 1998;275:G460-G466.
2. Mertz H. Am J Physiol. 1998;93:160-165.3. Jackson JL et al. Am J Med. 2000;108:65-72.4. Tack J et al. Am J Physiol. 2003;17:603-608.
FGID, functional gastrointestinal disorder.

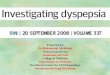
Desipramine vs Placebo for Moderate to Severe FGIDs
60
73
47 49
0
20
40
60
80
100
ITT n=201 PP n=153
Drossman DA et al. Gastroenterology. 2003;125:19-31.Drossman DA et al. Gastroenterology. 2003;125:19-31.
P = 0.13
P = 0.006NNT = 4
• Better response in patients with moderate symptoms
• Dose: 50-250 mg qhs
Re
sp
on
se
s,
%
Desipramine Placebo (12 weeks)

Desipramine for FGID: Moderate to Severe Adverse Effects
26
20
1613
1113
8
2
0
10
20
30
40
Dry Mouth Sleep Constipation Flush
• 8-fold increase in study dropouts with TCA• Multiple adverse effects common (mean, 3.5)
Desipramine (n = 135) Placebo (n = 55)
Drossman DA et al. Gastroenterology. 2003;125:19-31.Drossman DA et al. Gastroenterology. 2003;125:19-31.
Pa
tie
nts
, %

Alosetron for Functional Dyspepsia
Talley NJ et al. Aliment Pharmacol Ther. 2001;15:525-537.Talley NJ et al. Aliment Pharmacol Ther. 2001;15:525-537.*P < 0.05 compared with placebo.
*Total Women
Ad
eq
ua
te R
eli
ef,
%
Men
40
4651
4240
4954
4339 39
4340
0
10
20
30
40
50
60
Placebo n=66 0.5 mg n=59 1.0 mg n=67 2.0 mg n=65

Functional Dyspepsia: 5-HT4 Agonists
• Tegaserod improved preprandial and postprandial gastric accommodation in healthy volunteers.
• Global symptom improvement was noted in women with FD on 6 mg bid tegaserod.2
• In patients with delayed gastric emptying and FD, gastric emptying normalized in 80% of patients receiving 6 mg tid tegaserod compared with 50% receiving placebo (P < 0.058).3
1. Tack J et al. Gastroenterology. 2002;122:A453.2. Tack J et al. Gastroenterology. 2002;122:A20.
3. Tougas G et al. Gastroenterology. 2003;124:A54.

Tegaserod in Functional Dyspepsia:Days With Satisfactory Relief
Talley NJ et al. Presented at: ACG. 2006.Talley NJ et al. Presented at: ACG. 2006.
6.05% difference 3.16% difference
26.63
32.24
0
50
D2302
Da
ys
Wit
h S
ati
sfa
cto
ry R
eli
ef
(%)
Placebo (n=652)
Tegaserod 6 mg bid (n=651)
P=0.0662
29.3631.87
0
50
40
30
20
10
D2301
P=0.0002
Placebo(n=673)
Tegaserod 6 mg bid (n=680)
*
Da
ys
Wit
h S
ati
sfa
cto
ry R
eli
ef,
%
0
40
30
20
10

Tegaserod Removed From The Market
• March 30, 2007- FDA and Novartis removed tegaserod from the market
• 13 patients treated with tegaserod had cardiovascular events
– 4 patients - heart attack (1 died)
– 6 patients - severe chest pain/angina
– 3 patients - stroke
0
0.02
0.04
0.06
0.08
0.1
0.12
Per
cen
t o
f p
atie
nts
wit
h
card
iova
scu
lar
even
ts
Tegaserod Placebo
13
1
http://www.fda.gov. Accessed April 2, 2007.
29 Randomized, controlled trials of over 18,000 patients
N = 11,614 N = 7,031

Itopride Hydrochloride Effects on Gastric Motor and Sensory Function
• Dopamine D2 antagonist (similar to domperidone)
• Randomized, double-blind, placebo-controlled study
• Assessment of gastric function in 46 healthy persons– Before and after 7 days of tid therapy– No significant effects on gastric motor and sensory function
625516555
467512449
0
150
300
450
600
750
Total gastric volume (mL) Proximal gastric volume (mL)
Choung RS et al. Am J Gastroenterol. 2006;101:S487.Choung RS et al. Am J Gastroenterol. 2006;101:S487.
Placebo Itopride 100 mg Itopride 200 mg
Vo
lum
e,
mL
Vo
lum
e,
mL

Case Study
• Current tx: Omeprazole 20 mg q day, metoclopramide 20 mg q ac, PEG 17 gm q day– Nausea, bloating, heartburn improved
– Epigastric discomfort persists; now fatigued
• Domperidone 10 mg q.i.d. substituted for metoclopramide; PPI and PEG continued– Fatigue improves; epigastric pain persists
• Desipramine 25 mg q.h.s. reintroduced– Epigastric pain tolerable
– Agrees to cognitive behavioral therapy evaluation

Complementary Medicine in the United States
• Use of complementary medicine increased from 34% to 42% (1990-1997).1
• Relaxation techniques (16%), herbal remedies (12%), massage (11%) are its most common forms.1
• It is often used to treat chronic conditions.– Back pain, anxiety, depression, headache
– IBS the most commonly treated GI problem2
– >20% alternative medicine use among IBS/FD patients3
• $21.2 billion in 1997– $12.2 billion out of pocket
1. Eisenberg DM et al. JAMA. 1998;280:1569-1575.2. Smart HL et al. Gut. 1986;27:826-828.
3. Koloski NA et al. Aliment Pharmacol Ther. 2003;17:841-851.

CBT vs Education for Moderate to Severe FGID
7073
3741
0
20
40
60
80
100
ITT n=201 PP n=168
P < 0.001NNT=3
P < 0.001NNT=3
Drossman DA et al. Gastroenterology. 2003;125:19-31.Drossman DA et al. Gastroenterology. 2003;125:19-31.
CBT Education (12 weeks)
CBT, cognitive-behavioral therapy.
Res
po
nd
er r
ate,
%

Hypnotherapy for Functional Dyspepsia
*P < 0.05.Hypnotherapy associated with less drug use and fewer visits. Calvert EL et al. Gastroenterology. 2002;123:1778-1785.Calvert EL et al. Gastroenterology. 2002;123:1778-1785.
**
*
HT, n = 26 Support and placebo, n=24 Medical, n = 29
*
*59
73
424134
10
33
43
11
0
25
50
75
100
End of Rx (16 wks) Long-term (56 wks) QOL
% I
mp
rove
me
nt

Capsaicin for Functional Dyspepsia
Capsaicin, n = 15
*P < 0.05.One to two capsules red pepper powder q ac.Epigastric pain and fullness relieved.
Bortolotti M et al. Aliment Pharmacol Ther 2002;16:1075-1082.Bortolotti M et al. Aliment Pharmacol Ther 2002;16:1075-1082.
* * *
1 2 3 4 5B
0
1
2
3
4
5 Placebo, n = 15
Time, weeks
Sc
ore

Herbal Remedies for Functional Dyspepsia: A Systematic Review
• 17 RCTs of herbal remedies are included in the review (8 trials had a Jadad score >3).1
• Peppermint and caraway oil were the best-studied herbal remedies.– 4 RCTs show their benefits.
• Most studies were conducted with combinations – Effective ingredient and quality control were unclear.
• Iberogast®, a combination of 9 herbs, relieved symptoms compared with placebo in several European studies.2
1. Thompson Coon J. Aliment Pharmacol Ther. 2002;16:1689-1699.2. Gundermann KJ et al. Adv Ther. 2003;20:43-49.
1. Thompson Coon J. Aliment Pharmacol Ther. 2002;16:1689-1699.2. Gundermann KJ et al. Adv Ther. 2003;20:43-49.

Dyspepsia: Novel Therapies
• Mianserin (tetracyclic antidepressant)
• Clonidine
• Sumatriptan/buspirone
• Paroxetine (SSRIs)
• Neurokinin antagonists
• Corticotrophin-releasing factor (CRF) antagonists
• Opioid antagonists

Medical Strategies for Functional Dyspepsia
Therapeutic intervention Efficacy Notes
H pylori eradication 36% vs 30% placebo; NNT 18 Meta-analysis of 13 RCTs
PPIs 33% vs 23% placebo; NNT 9 Meta-analysis of 8 RCTs
H2-receptor antagonists
More effective than placebo only for epigastric pain + postprandial fullness
Meta-analysis of 11 RCTs
Antidepressants – TCAs
73% vs 49% placebo; NNT 4. Significant adverse effects
Single RCT only
Antacids No better than placebo 1 RCT only
Bismuth salts No better than placebo Meta-analysis of 5 RCTs
Sucralfate No better than placebo Meta-analysis of 2 RCTs
Saad RJ. Aliment Pharmacol Ther. 2006;24:475-492.Saad RJ. Aliment Pharmacol Ther. 2006;24:475-492.

ChallengingTreatable
Common
Poorly understood
Controversial
Chronic
FunctionalFunctionalDyspepsiaDyspepsia
Functional Dyspepsia Is…

Dyspepsia in Review
• Definition
• Epidemiology, natural history, and costs
• Underlying pathophysiology
• Diagnosis
• Treatment options
• Evidence to support current therapies

Functional Dyspepsia: Diagnosis
• Thorough history and physical examination
• Evaluation for warning signs/features– Unintentional weight loss, anemia, or dysphagia
– History of NSAID use
– Previous gastrointestinal bleeding or ulcer disease
– Recurrent vomiting
– Abnormal physical examination other than epigastric pain
• High-prevalence or low-prevalence Helicobacter pylori area?
NSAID, nonsteroidal antiinflammatory drug.

Functional DyspepsiaFunctional DyspepsiaFunctional DyspepsiaFunctional Dyspepsia
Epigastric pain syndrome (EPS):Epigastric pain
syndrome (EPS):
Postprandial distress syndrome (PDS): Meal-related
FD
Postprandial distress syndrome (PDS): Meal-related
FD Pain or burning
localized to the epigastrium of at least moderate intensity
Pain or burning localized to the epigastrium of at least moderate intensity
Postprandial fullness, after ordinary sized meals, at least several times per week, or
Early satiation that prevents finishing a regular meal, at least several times per week
Postprandial fullness, after ordinary sized meals, at least several times per week, or
Early satiation that prevents finishing a regular meal, at least several times per week
Tack J et al. Gastroenterology. 2006;130:1466-1479.Tack J et al. Gastroenterology. 2006;130:1466-1479.

H pylori Test and Treat: How, Who, and What to Do With the Results
Dyspepsia (uninvestigated)
Age >55 or alarm features
Age <55 No alarm features
H pylori prevalence <10%
EGDH pylori prevalence
>10%
PPI trialTest and treat
H pylori
Test and treat H pylori
PPI trial
Consider EGD
failsfails
fails fails
Talley NJ et al. Am J Gastroenterol. 2005;100:2324-2337.Talley NJ et al. Am J Gastroenterol. 2005;100:2324-2337.
How to test for H pylori
• C-13 urea breath test
• Stool antigen test
If positive
• Initiate triple therapy

Functional Dyspepsia: H pylori Eradication
• A single-center study demonstrated improvement in 21% of patients with H pylori eradication (PPI + abx) compared with 7% with PPI alone (P < 0.001).1
• Three multicenter RPCTs involving 759 patients did not find any significant relief of dyspepsia symptoms after H pylori eradication.2-4
1. McColl K et al. N Engl J Med. 1998;339:1869-1874.2. Talley NJ et al. BMJ. 1999;318:833-837.
3. Talley NJ et al. N Engl J Med. 1999;341:1106-1111.4. Froelich JW et al. Am J Gastro 2001; 96:_
RPCT, randomized placebo-controlled trial

Treatment of Dyspepsia (circa 1892)
• “Therapeutic measures may be divided into those which attempt to replace in the digestive juices important elements which are lacking…”
• “In the first group come hydrochloric acid and ferments, which are so freely employed in dyspepsia.”
• “Ewald recommend large doses of from 90-100 drops at intervals of 15 minutes after meals.”
Osler W. The Principles and Practice of Medicine. 1892.

Evidence for Prokinetic Therapies
• Metoclopramide – The most commonly used prokinetic in the treatment of FD. A recent meta-analysis failed to show any significant benefit above placebo.1
• Cisapride – Seventeen studies were reviewed. Earlier apparent favorable response might have been attributed to publication bias. Recent review of 17 studies did not show any significant benefit compared with placebo.1,2
1. Abraham NS et al. Aliment Pharmacol Ther. 2004;19:631-641.2. Soo S et al. Cochrane Database Sys Rev. 2000;2:CD001960.

Evidence for Prokinetic Therapies
• Domperidone – Eight studies were evaluated. Many had severe design flaws. Recent meta-analysis showed a slight benefit at improving symptoms compared with placebo.1
• Levosulpiride – A dopamine antagonist. Not available in the United States. Recent study showed benefit compared with cisapride, though no placebo group was included.2
1. Veldhuyzen van Zanten SJO et al. Am J Gastroenterol. 2001;96:689-696.2. Mearin F et al. Clin Gastroenterol Hepatol. 2004;2:301-308.

5-HT3 Antagonists for Functional Dyspepsia
• 5-HT3 antagonists may alter visceral perception.1
– Alosetron 1 mg bid did not alter perception of gastric distention compared with placebo in healthy volunteers.2
– Effects on visceral perception in FD patients have not yet been reported.
• 5-HT3 antagonists may be beneficial for nausea.3
• Do 5-HT3 antagonists have effects on gastric emptying?4
1Gershon Rev Gastro Dis 2003;3:S252Zerbib APT 1994;8:4033Hasler, Chey Gastroenterol 2003;125:18604Akkermans Gut 1988:29;1249
1. Gershon MD. Rev Gastroenterol Disord. 2003;3:S25-S34.2. Zerbib F et al. Aliment Pharmacol Ther. 1994; 8:403.
3. Hasler WL et al. Gastroenterology. 2003;125:1860-1867.4. Akkermans LM. Gut. 1988;29:1249-1252.

5-HT3 Antagonists for Functional Dyspepsia• In the only multicenter RPCT to date, 320 patients
with FD were randomly assigned to 3 doses of alosetron or placebo for a 12-week trial period.
• Primary efficacy variable was adequate relief of upper abdominal pain or discomfort.
• Fifty-five percent of patients receiving 1 mg bid alosetron experienced adequate improvement compared with 46% receiving placebo (P = 0.05). No difference was observed in patients receiving 0.5 mg bid or 2 mg bid alosetron.1
1. Talley NJ et al. Aliment Pharmacol Ther. 2001;15:525-537.
RPCT, randomized placebo-controlled trial

Effect of Tegaserod on Gastric Emptying, Gastric Accommodation, and Small Bowel Transit• In patients with dyspepsia and normal gastric emptying, tegaserod significantly
increased meal-induced gastric accommodation.1
*P < 0.008 vs placebo; †P < 0.002 vs placebo.
Tim
e,
min
Placebo Tegaserod 6 mg bid
†*
n = 40 (17 women).Randomized, placebo-controlled, crossover study
1. Tack J et al. Gastroenterology. 2005;128:A94.2. Degen L et al. Neurogastroenterol Motil. 2005;17:821-826.
(1/2)T
137
194
116128
0
200
Gastric emptying Small bowel transit
150
100
50

Interpersonal Psychotherapy for Refractory Functional Dyspepsia
14.8
10.9
8.7
13.112.4
9.3
0
2
4
6
8
10
12
14
16
Entry End of Rx 1 yr FU
To
tal
Sym
pto
m S
core
*P = 0.015.Seven visits in 12 weeks.Included patients with refluxlike symptoms.
Hamilton J. Gastroenterology. 2000;119:661-669.Hamilton J. Gastroenterology. 2000;119:661-669.
PI therapy, n = 37 Symptomatic, n = 36
*

Functional Dyspepsia: Summary
• Empiric antisecretory therapy is effective in a subset of patients with FD.
• Effective prokinetic therapy is eagerly awaited.
• The benefits of H pylori cure in FD, if present at all, are small.
• Agents that affect accommodation or visceral nociception may provide an alternative or may prove complementary to acid suppression therapy.
• Psychological therapies are effective in a subset of FD patients.
• Complementary strategies require further study.