Embed Size (px)
Citation preview

EDITORIAL BOARD
EDITOR-IN-CHIEF Y. Chandrashekhar, MD, DM, Minneapolis, MN
EXECUTIVE EDITORS Christopher M. Kramer, MD, Charlottesville, VA
Leslee J. Shaw, PhD, New York, NY
DEPUTY EDITORS
Vasken Dilsizian, MD, Baltimore, MD
Thomas H. Marwick, MBBS, PhD, MPH,Melbourne, Australia
James K. Min, MD, New York, NY
William A. Zoghbi, MD, Houston, TX
ASSOCIATE EDITORS
Ron Blankstein, MD, Boston, MA
Frank A. Flachskampf, MD, PhD,Uppsala, Sweden
Paul A. Grayburn, MD, Dallas, TX
Farouc A. Jaffer, MD, PhD, Boston, MA
Raymond Y.K. Kwong, MD, MPH,Boston, MA
Eike Nagel, MD, PhD, Frankfurt, Germany
Koen Nieman, MD, PhD, Stanford, CA
Partho P. Sengupta, MD, Morgantown, WV
EMERITUS EDITOR-IN-CHIEF
Jagat Narula, MD, New York, NY
EXECUTIVE MANAGING EDITOR
Monica R. Payne-Emmerson, MS,Washington, DC
MANAGING EDITOR
Steven Glaros Washington, DC
GUEST EDITORS
Zahi A. Fayad, PhD, New York, NY
Harvey Hecht, MD, New York, NY
Jonathon Leipsic, MD, Vancouver, Canada
Sherif Nagueh, MD, Houston, TX
Dudley J. Pennell, MD, London, United Kingdom
Thomas H. Schindler, MD, St. Louis, MO
James D. Thomas, MD, Chicago, IL
James E. Udelson, MD, Boston, MA
Renu Virmani, MD, Gaithersburg, MD
CME/MOC/ECME EDITOR
Ragavendra R. Baliga, MD, Columbus, OH
SOCIAL MEDIA EDITOR
Andrew D. Choi, MD, Washington, DC
Jeffrey B. Geske, MD, Rochester, MN
STATISTICAL EDITOR
Paul L. Clopton, MS, San Diego, CA
SENIOR ADVISING EDITORS
Jeroen J. Bax, MD, PhD,Leiden, the Netherlands
Robert O. Bonow, MD, Chicago, IL
Eugene Braunwald, MD, Boston, MA
Pamela S. Douglas, MD, Durham, NC
EDITOR-IN-CHIEF, JACC
Valentin Fuster, MD, PhD, New York, NY
EDITOR-IN-CHIEF,
JACC: Cardiovascular Interventions
David J. Moliterno, MD, Lexington, KY
EDITOR-IN-CHIEF,
JACC: Heart Failure
Christopher M. O’Connor, MD,Falls Church, VA
EDITOR-IN-CHIEF,
JACC: Clinical Electrophysiology
David J. Wilber, MD, Chicago, IL
EDITOR-IN-CHIEF,
JACC: Basic to Translational Science
Douglas L. Mann, MD, St. Louis, MO
EDITOR-IN-CHIEF,
JACC: Case Reports
Julia Grapsa, MD, PhD, London, UK
EDITOR-IN-CHIEF,
JACC: CardioOncology
Bonnie Ky, MD, MSCE,Philadelphia, PA
VICE PRESIDENT, PUBLISHING
Kimberly Murphy, Washington, DC
DIRECTOR, PRODUCT MANAGEMENT,
DIGITAL PUBLISHING
Nandhini Kuntipuram,Washington, DC
SENIOR EDITORIAL CONSULTANTS
Eloisa Arbustini, MD, Pavia, Italy
Luigi P. Badano, MD, PhD, Padua, Italy
Daniel S. Berman, MD, Los Angeles, CA
Rebecca T. Hahn, MD, New York, NY
Harlan M. Krumholz, MD, SM, New Haven, CT
Warren J. Manning, MD,Boston, MA
Gregg W. Stone, MD,New York, NY
ETHICS COMMITTEE
Holly Atkinson, MD, New York, NY
Lawrence S. Cohen, MD, New Haven, CT
Kim Fox, MD, London, United Kingdom
Robert Frye, MD, Rochester, MN
Philip J. Landrigan, MD, New York, NY
Richard L. Popp, MD, Palo Alto, CA
Eric Prystowsky, MD, Indianapolis, IN
James Willerson, MD, Houston, TX

EDITORIAL CONSULTANTS
Stephan Achenbach, MD,Erlangen, Germany
Erick Alexánderson-Rosas, MD,Mexico City, Mexico
Andrew E. Arai, MD, Bethesda, MD
Rob S. Beanlands, MD,Ottawa, Canada
Frank Bengel, MD,Hannover, Germany
Michael J. Blaha, MD, MPH,Baltimore, MD
Jamieson M. Bourque, MD, MHS,Charlottesville, VA
Chiara Bucciarelli-Ducci, MD, PhD,Bristol, United Kingdom
Matthew J. Budoff, MD,Los Angeles, CA
Ignasi Carrio, MD, Barcelona, Spain
Hyuk-Jae Chang, MD, PhD,Seoul, South Korea
Robin P. Choudhury, DM,Oxford, United Kingdom
Benjamin J.W. Chow, MD,Ottawa, Canada
Milind Desai, MD, Cleveland, OH
Marc Dewey, MD, Berlin, Germany
Marcelo F. Di Carli, MD, Boston, MA
Erwan Donal, MD, PhD,Rennes, France
Rami Doukky, MD, MSc, Chicago, IL
Thor Edvardsen, MD, PhD,Oslo, Norway
Andrew J. Einstein, MD,New York, NY
Mark K. Friedberg, MD,Toronto, Canada
Matthias Friedrich, MD,Montreal, Canada
Henry Gewirtz, MD,Boston, MA
Thierry C. Gillebert, MD, PhD,Ghent, Belgium
Julia Grapsa, MD, PhD,London, United Kingdom
John P. Greenwood, MBChB, PhD,Leeds, United Kingdom
Jong-Won Ha, MD, PhD,Seoul, South Korea
Robert C. Hendel, MD,New Orleans, LA
Diwakar Jain, MD, Valhalla, NY
Michael Jerosch-Herold, PhD,Boston, MA
Philipp A. Kaufmann, MD,Zurich, Switzerland
Sanjiv Kaul, MBBS,Portland, OR
Paul Knaapen, MD, PhD,Amsterdam, the Netherlands
Juhani Knuuti, MD, Turku, Finland
Shelby Kutty, MD, PhD, MHCM,Baltimore, MD
André La Gerche, MBBS, PhD,Melbourne, Australia
Patrizio Lancellotti, MD, PhD,Liege, Belgium
Roberto M. Lang, MD,Chicago, IL
João A.C. Lima, MD,Baltimore, MD
Bin Lu, MD, Beijing, China
Girijanandan Mahapatra, MD,Mumbai, India
Gerald Maurer, MD,Vienna, Austria
Edward O. McFalls, MD, PhD,Minneapolis, MN
Todd D. Miller, MD,Rochester, MN
Satoshi Nakatani, MD,Osaka, Japan
Khurram Nasir, MD, MPH,Miami Beach, FL
Kazuaki Negishi, MD, PhD,Hobart, Australia
Stephen J. Nicholls, MBBS, PhD,Adelaide, Australia
Robin Nijveldt, MD, PhD,Nijmegen, the Netherlands
Yukio Ozaki, MD, PhD,Toyoake, Japan
Alan S. Pearlman, MD, Seattle, WA
Steffen E. Petersen, MD, DPhil,MPH, London, United Kingdom
Philippe Pibarot, DVM, PhD,Québec, Canada
Michael H. Picard, MD,Boston, MA
Gianluca Pontone, MD, PhD,Milan, Italy
Sanjay Rajagopalan, MD,Columbus, OH
Harry Rakowski, MD,Toronto, Canada
Carlos E. Rochitte, MD, PhD,São Paulo, Brazil
Michael Salerno, MD, PhD,Charlottesville, VA
Javier Sanz, MD,New York, NY
Erik Schelbert, MD, MS,Pittsburgh, PA
Jeanette Esther Schulz-Menger, MD,Berlin, Germany
Joseph B. Selvanayagam, MBBS(Hons), DPhil,Adelaide, Australia
Roxy Senior, MD, DM,London, United Kingdom
Robert J. Siegel, MD,Los Angeles, CA
Albert J. Sinusas, MD,New Haven, CT
Prem Soman, MD, PhD,Pittsburgh, PA
Masaaki Takeuchi, MD, PhD,Kitakyushu, Japan
Ahmed Tawakol, MD,Boston, MA
Paaladinesh Thavendiranathan,MD, SM, Toronto, Canada
Liza Thomas, MBBS, PhD,Sydney, Australia
Richard W. Troughton, MBChB, PhD,Christchurch, New Zealand
Todd C. Villines, MD,Bethesda, MD
Nathan D. Wong, PhD,Irvine, CA
Alistair A. Young, PhD,Auckland, New Zealand
Jose Zamorano, MD,Madrid, Spain
EMERGING EDITORIAL
CONSULTANTS
Amir Ahmadi, MD,New York, NY
Shehab Anwer, MBBCh,Cairo, Egypt
Lilit Baghdasaryan, MD,Yerevan, Armenia
Sorina Mihaila Baldea, MD, PhD,Bucharest, Romania
Tor Biering-Sørensen, MD, PhD,Copenhagen, Denmark
Matteo Cameli, MD, PhD,Siena, Italy
Raluca Elena Dulgheru, MD,Liege, Belgium
Basma Hammad, MD,Boston, MA
Akihisa Kataoka, MD, PhD,Tokyo, Japan
Asim Katbeh, MD,Damascus, Syria
Tomas Lapinskas, MD,Kaunas, Lithuania
Gina LaRocca, MD, MHSc,New York, NY
Savvas Loizos, MD, MSc, PhD,London, United Kingdom
Bła _zej Michalski, MD, PhD,Lodz, Poland
Marcelo Haertel Miglioranza, MD, PhD,Porto Alegre, Brazil
Sarah Moharem-Elgamal, MB BCh,MSc, MD, Giza, Egypt
Doralisa Morrone, MD, PhD,Pisa, Italy
Didem O�guz, MD, Rochester, MN
Toma�z Podlesnikar, MD,Leiden, the Netherlands
Fuad Samadov, MD,Baku, Azerbaijan
Rizwan Sarwar, MBBS, Oxford, UK
Nishant R. Shah, MD, MPH, MSc,Providence, RI
Hatem A. Soliman, MD, MSc, MRCP,London, United Kingdom
Carla Sousa, MD,Porto, Portugal
Elena Surkova, MD, PhD,London, United Kingdom
Francois Tournoux, MD, PhD,Montreal, Canada
Svetlin Tsonev, MD, PhD,Sofia, Bulgaria
Brandon M. Wiley, MD, MS,Rochester, MN

Howard “Bo” T. Walpole, Jr., MD, MBA, FACC, Treasurer
2019-2020 OFFICERS
Richard J. Kovacs, MD, FACC, PresidentAthena Poppas, MD, FACC, Vice President
Akshay Khandelwal, MD, FACC, Secretary and Board of Governors Chair
Timothy W. Attebery, DSc, MBA, FACHE, Chief Executive Officer
2019-2020 PUBLICATIONS AND
EDITORIAL COORDINATION
COMMITTEEViviany R. Taqueti, MD, MPH, FACC,Chair
Rhonda M. Cooper-DeHoff, MD, FACC,Annual Scientific Session Program Committee
Prasad C. Gunasekaran, MD,FIT Representative
Fadi G. Hage, MD, FACC
Fred M. Kusumoto, MD, FACC,Awards Committee
Renato D. Lopes, MD, PhD, FACC
Sandra M. Oliver-McNeil, DNP, ACNP-BC, AACC
James E. Tcheng, MD, FACC, (Ex Officio), Chair, Digital Steering Committee
John U. Doherty, MD, FACC
Syed Tanveer Rab, MBBS, MACC
William J. Oetgen, MD, MBA, FACC, ACC Executive Vice President, Science & Quality,
Education and Publications
Kimberly Murphy, ACC Division Vice President, Publishing
CORRESPONDENCE FOR
AMERICAN COLLEGE OF
CARDIOLOGY
All correspondence for the
College, other than that related to
JACC: Cardiovascular Imaging,
should be sent to Resource Center,
American College of Cardiology,
2400 N Street NW,
Washington, DC 20037

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E AM E R I C A N
C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
ORIGINAL RESEARCH
Selective Referral Using CCTA VersusDirect Referral for Individuals Referredto Invasive Coronary Angiographyfor Suspected CAD
A Randomized, Controlled, Open-Label TrialHyuk-Jae Chang, MD, PHD,a Fay Y. Lin, MD,b Dan Gebow, PHD,c Hae Young An, BS,a Daniele Andreini, MD, PHD,d
Ravi Bathina, MD,e Andrea Baggiano, MD,d Virginia Beltrama, MD,d Rodrigo Cerci, MD,f Eui-Young Choi, MD,g
Jung-Hyun Choi, MD,h So-Yeon Choi, MD,i Namsik Chung, MD, PHD,a Jason Cole, MD,j Joon-Hyung Doh, MD,k
Sang-Jin Ha, MD,l Ae-Young Her, MD,m Cezary Kepka, MD,n Jang-Young Kim, MD,o Jin-Won Kim, MD,p
Sang-Wook Kim, MD,q Woong Kim, MD,r Gianluca Pontone, MD, PHD,d Uma Valeti, MD,s Todd C. Villines, MD,t
Yao Lu, MS,b Amit Kumar, MS,b Iksung Cho, MD,q Ibrahim Danad, MD,b,u Donghee Han, MD,a,b Ran Heo, MD,v
Sang-Eun Lee, MD,a Ji Hyun Lee, MD,a,b Hyung-Bok Park, MD,w Ji-min Sung, PHD,a David Leflang, BA,c
Joseph Zullo, BA,c Leslee J. Shaw, PHD,b James K. Min, MDb
ABSTRACT
ISS
OBJECTIVES This study compared the safety and diagnostic yield of a selective referral strategy using coronary
computed tomographic angiography (CCTA) compared with a direct referral strategy using invasive coronary angiography
(ICA) as the index procedure.
BACKGROUND Among patients presenting with signs and symptoms suggestive of coronary artery disease (CAD), a
sizeable proportion who are referred to ICA do not have a significant, obstructive stenosis.
METHODS In a multinational, randomized clinical trial of patients referred to ICA for nonemergent indications, a se-
lective referral strategy was compared with a direct referral strategy. The primary endpoint was noninferiority with a
multiplicative margin of 1.33 of composite major adverse cardiovascular events (blindly adjudicated death, myocardial
infarction, unstable angina, stroke, urgent and/or emergent coronary revascularization or cardiac hospitalization) at a
median follow-up of 1-year.
RESULTS At 22 sites, 823 subjects were randomized to a selective referral and 808 to a direct referral strategy. At
1 year, selective referral met the noninferiority margin of 1.33 (p ¼ 0.026) with a similar event rate between the ran-
domized arms of the trial (4.6% vs. 4.6%; hazard ratio: 0.99; 95% confidence interval: 0.66 to 1.47). Following CCTA,
only 23% of the selective referral arm went on to ICA, which was a rate lower than that of the direct referral strategy.
Coronary revascularization occurred less often in the selective referral group compared with the direct referral to ICA
(13% vs. 18%; p < 0.001). Rates of normal ICA were 24.6% in the selective referral arm compared with 61.1% in the
direct referral arm of the trial (p < 0.001).
CONCLUSIONS In stable patients with suspected CAD who are eligible for ICA, the comparable 1-year major adverse
cardiovascular events rates following a selective referral and direct referral strategy suggests that both diagnostic
approaches are similarly effective. In the selective referral strategy, the reduced use of ICA was associated with a greater
diagnostic yield, which supported the usefulness of CCTA as an efficient and accurate method to guide decisions of ICA
performance. (Coronary Computed Tomographic Angiography for Selective Cardiac Catheterization [CONSERVE];
NCT01810198) (J Am Coll Cardiol Img 2019;12:1303–12) Published by Elsevier on behalf of the American College of
Cardiology Foundation.
N 1936-878X/$36.00 https://doi.org/10.1016/j.jcmg.2018.09.018

ABBR EV I A T I ON S
AND ACRONYMS
ACC = American College of
Cardiology
AHA = American Heart
Association
CAD = coronary artery disease
ICA = invasive coronary
angiography
CCTA = coronary computed
tomographic angiography
MACE = major adverse
cardiovascular event
PCI = percutaneous coronary
intervention
From the
Cardiovasc
Francisco,
India; fQu
University
Mobile, M
Gangwon-d
Warsaw, PqChung-An
Minnesota
Netherland
Seonam U
unrestricte
Program o
Chang and
Program th
Dr. Min is
no role in
research g
board of A
relationshi
Manuscrip
Chang et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Selective Referral to Cath J U L Y 2 0 1 9 : 1 3 0 3 – 1 2
1304
I nvasive coronary angiography (ICA) is acommonly performed diagnostic testfor evaluation of stable symptomatic pa-
tients with suspected coronary artery disease(CAD) to guide decisions of coronary revascu-larization (1–4). Although current profes-sional guidance documents offer directionfor appropriate selection of patients for elec-tive ICA, previous studies observed that mostindividuals who underwent nonemergentICA did not have actionable CAD (5,6). Forthese patients, ICA is an invasive, expensiveprocedure that may be unnecessary. WhenCAD is identified, ICA is frequently associ-ated with ad hoc percutaneous coronary
intervention (PCI) at the time of ICA, but whetherthis approach improves clinical outcomes is notclear (7–9).
SEE PAGE 1313
Coronary computed tomographic angiography(CCTA) is a noninvasive anatomic imaging methodthat enables identification and exclusion of CAD(10–12). Previous multicenter studies have consis-tently demonstrated the high diagnostic performanceof CCTA to exclude obstructive CAD by 99% to 100%, afinding that is associated with favorable outcomes.These data have advanced the concept of the use ofCCTA as a “gatekeeper” that more precisely selectsindividuals for ICA (6,13). For stable patients alreadyreferred for nonemergent ICA, it is not known how thesafety and downstream clinical outcomes of a selec-tive ICA referral strategy, informed by CCTA findings,
aSeverance Cardiovascular Hospital, Yonsei University Health
ular Imaging, New York-Presbyterian Hospital and Weill Corn
California; dCentro Cardiologico Monzino, IRCCS, Milan, Italy; e
anta Diagnostico Nuclear, Curitiba, Brazil; gGangnam Severanc
Hospital, Busan, South Korea; iAjou University Hospital, Gye
obile, Alabama; kInje University, Ilsan Paik Hospital, Gyeon
o, South Korea; mKangwon National University Hospital, Ga
oland; oWonju Severance Hospital, Gangwon-do, South Korea; pK
g University Hospital, Seoul, South Korea; rYeungnam Univer
, Minneapolis, Minnesota; tWalter Reed Medical Center, Bethesd
s; vAsan Medical Center, University of Ulsan College of Medicin
niversity College of Medicine, Gyeonggi-do, South Korea. Thi
d grant from GE Healthcare (Princeton, New Jersey) and the
f the National Research Foundation of Korea, Ministry of Scien
Chung were supported by a grant (Grant No. 2012027176) from
rough the National Research Foundation of Korea, funded by
supported by the Dalio Foundation, National Institutes of Healt
study design, data collection, data analysis, data interpretation,
rants and speaker fees from GE, Bracco, Bayer, Medtronic, and H
rineta and GE Healthcare; and has an equity interest in Cleerly.
ps relevant to the contents of this paper to disclose. Jagat Narula
t received August 15, 2018; revised manuscript received Septemb
compare to a direct ICA referral strategy, becausepatients would have otherwise undergone ICA.
The objective of the CONSERVE (CoronaryComputed Tomographic Angiography for SelectiveCardiac Catheterization) trial (NCT01810198) was tocompare the cardiovascular outcomes of a selectivereferral strategy, in which CCTA was performedbefore ICA, versus a direct referral strategy. The pri-mary hypothesis of the CONSERVE trial was that aselective referral strategy would be noninferior to adirect referral strategy for major adverse cardiovas-cular events (MACE).
METHODS
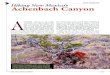
STUDY DESIGN. CONSERVE was a 1:1 randomized,controlled, open-label, international, multicentertrial at 22 hospitals and cardiology practices in NorthAmerica, East Asia, Europe, and India. The studyprotocol was approved at each enrolling site by thelocal institutional review board or ethics committee.After randomization to selective referral versus directreferral, ICA and CCTA performance and interpreta-tion were executed locally, and downstream clinicaldecision-making was at the sole discretion of the localphysicians. A total of 20 patients (14 in the selectivereferral and 6 in the direct referral arm) withdrewconsent and were not included in our analysis(Figure 1).
PATIENT ENROLLMENT. The study participants werestable patients with suspected but without knownCAD referred for nonemergent ICA based uponthe American College of Cardiology/American Heart
System, Seoul, South Korea; bDalio Institute of
ell Medicine, New York, New York; cMDDX, San
CARE Hospital and FACTS Foundation, Hyderabad,
e Hospital, Seoul, South Korea; hPusan National
onggi-do, South Korea; jCardiology Associates of
ggi-do, South Korea; lGangneung Asan Hospital,
ngwon-do, South Korea; nInstitute of Cardiology,
orea University Guro Hospital, Seoul, South Korea;
sity Hospital, Daegu, South Korea; sUniversity of
a, Maryland; uVU Medical Center, Amsterdam, the
e, Seoul, South Korea; and the wMyongji Hospital,
s trial was supported by an investigator-initiated
Leading Foreign Research Institute Recruitment
ce, ICT & Future Planning (Seoul, Korea). Drs. H-J.
the Leading Foreign Research Institute Recruitment
the Ministry of Science, ICT & Future Planning.
h, and GE Healthcare. The funder of the study had
or writing of the report. Dr. Pontone has received
eartflow. Dr. Min serves on the scientific advisory
All other authors have reported that they have no
, MD, served as Guest Editor for this paper.
er 4, 2018, accepted September 19, 2018.

FIGURE 1 Consort Diagram
n = 1,664
Randomized (n = 1,611)
Excluded (n = 33)♦ Not meeting inclusion criteria (n = 6)♦ Declined to participate (n = 21)♦ Unspecified (n = 6)Withdrew consent (n = 20)
Enrollment
Allocated to Selected Referral Strategy(n = 823)♦ Did not receive allocated test (n = 39) (26 patient decision, 2 physician decision, 11 unspecified)
Allocated to Direct Referral Strategy(n = 808)♦ Did not receive allocated test (n = 89) (71 patient decision, 3 physician decision, 15 unspecified)
Allocation
Lost to follow-up (n = 44)Completed 6 months of Follow-up (n = 769)
Completed 1 year of Follow-up (n = 672)
Lost to follow-up (n = 46)Completed 6 months of Follow-up (n = 703)
Completed 1-year of Follow-up (n = 606)
Follow-Up
n = 784 underwent CCTA n = 719 underwent ICA
Data Analysis
CONSORT diagram. CCTA ¼ coronary computed tomography angiography; ICA ¼ invasive coronary angiography.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Chang et al.J U L Y 2 0 1 9 : 1 3 0 3 – 1 2 Selective Referral to Cath
1305
Association (ACC/AHA) guidelines for coronary angi-ography (2), and included indications based onabnormal stress testing or suspected CAD symptoms.Patients were recruited during a clinic visit at thepoint of referral to ICA. Exclusion criteria includedknown history of CAD, ACC/AHA Class I or III indi-cation for ICA, known complex congenital heartdisease, planned ICA for reasons other thanCAD evaluation, or other reasons that precludedrandomization to either group for reasons of safety(Supplemental Appendix).
TRIAL RANDOMIZATION. After enrollment andbaseline data collection, block randomization strati-fied by Korean and non-Korean sites was performedwith 1:1 allocation to the selective referral or directreferral groups using web-based computer randomi-zation (MDDX, San Francisco, California). Subjects
and physicians were not blinded to allocation orstudy results.
TRIAL PROCEDURES. After receiving writteninformed consent, eligible patients were randomlyassigned to a selective referral or a direct referralstrategy. A selective referral strategy was defined byinitial performance of CCTA, with ICA performed atthe discretion of the local physician informed by theCCTA findings. A direct referral strategy allowedperformance of ICA as otherwise planned beforestudy enrollment.
An initial sample size calculation yielded a neces-sary and sufficient sample size of 1,463 patients,assuming a 10% dropout and an annualized event rateof 5.2% based on 80% power to detect a noninferioritymultiplicative margin of 1.33. A hypothesis of non-inferiority allowed us to evaluate the safety of a

TABLE 1 Downstream Procedural Use Following Randomization
Selective Referral (n ¼ 784Underwent Index CCTA)
Direct Referral (n ¼ 719Underwent Index ICA)
p ValueTotal % Total %
Invasive procedures
Invasive coronary angiography 179 23 30 4 <0.001
Fractional flow reserve 0 0 41 6 <0.001
Percutaneous coronary intervention 89 11 109 15 <0.001
Coronary artery bypass surgery 9 1 18 3 0.075
Revascularization 98 13 127 18 0.007
Noninvasive CAD tests
CCTA 3 0.4 1 1 <0.001
Exercise electrocardiography 108 14 79 11 0.12
Stress nuclear 14 2 10 1 0.67
Stress echocardiogram 9 1 9 1 0.95
Rest echocardiogram 281 36 95 13 <0.001
Overall % of downstream testing 1,204 153 199 29 <0.001
CAD ¼ coronary artery disease; CCTA ¼ coronary computed tomography angiography.
Chang et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Selective Referral to Cath J U L Y 2 0 1 9 : 1 3 0 3 – 1 2
1306
selective referral strategy compared with the stan-dard of care, that is, direct referral to invasive angi-ography. On October 22, 2015, we proposed to expandenrollment to a larger sample of a minimum of 1,600patients and to obtain a median follow-up time of 12months as reflective of the diagnostic episode of carefor initial referral to ICA. All changes to the protocol,including the sample size calculation, was performedunder the guidance of a Data Safety and MonitoringBoard.
All sites were instructed to perform ICA and CCTAin accordance with local site practice and societalguidelines. For both ICA and CCTA, presence orabsence of angiographic stenoses $50% using a So-ciety of Cardiovascular Computed Tomography coro-nary tree model was recorded by local site physicians,and the maximum on per-patient basis was used todefine obstructive CAD (14). Normal ICAs wereconsidered to be ICAs that demonstrated nostenosis $50%.
Data collection was performed prospectively in acentral electronic data capture system. We acquiredbaseline data related to demographic characteristics,clinical CAD risk factors, angina typicality, ACC/AHAguideline indication for ICA, and cardiovascularmedications. Follow-up was performed in person orby telephone communication at regular prescribedintervals, as well as last date of follow-up for thosewho did not reach 365 days at study closure. At eachfollow-up, patients were queried as to the occur-rence of any MACE. Further data were collected fordownstream invasive coronary and noninvasive car-diac procedures, as well as cardiovascular and all-cause hospitalizations. The primary endpoint wasanalyzed at 1 year of follow-up. Of event-free
survivors, 6-month follow-up was complete in 98%and 98% of patients in the selective and directreferral arms groups, respectively; similarly, 1-yearfollow-up (�1 month) was complete in 86% and84% of selective and direct referral patients,respectively (Figure 1).
MACEs. Independent investigators blinded to studyallocation adjudicated adverse events. The primaryendpoint was a composite of MACEs that includeddeath, nonfatal myocardial infarction, unstableangina, stroke, urgent or emergent coronary revas-cularization, and cardiovascular hospitalization(endpoint definitions provided in the SupplementalAppendix). Secondary clinical endpoints includedthe primary MACE endpoint plus major bleeding,need for urgent or emergent surgery due to hem-orrhage, major transfusion, and rates of test-relatedcomplications. The secondary endpoints alsoincluded evaluation of downstream resource use,including coronary revascularization, invasive andnoninvasive CAD diagnostic testing, and hospitali-zations. An independent clinical events committee,blinded to randomization assignment, adjudicatedall clinical endpoints. Supervision of the accrual andevaluation of all suspected endpoints was per-formed under the guidance of a Data Safety andMonitoring Board.
STATISTICAL METHODS. Statistical analyses werepre-specified. Baseline demographic, CAD riskfactors, angina typicality, and ACC/AHA guidelineindications for ICA were summarized as frequenciesand proportions for categorical variables and mean �SD for continuous variables. Categorical comparisonswere made using chi-square tests, whereas

TABLE 2 Baseline Characteristics of the Patients Enrolled in the CONSERVE Trial
SelectiveReferral Strategy
(n ¼ 784)
DirectReferral Strategy
(n ¼ 719)
Age, yrs 59.9 � 12.1 60.8 � 11.5
Sex
Female 378 (48.3) 316 (43.9)
Race/ethnicity
Asian 671 (85.6) 604 (84.0)
White 103 (13.1) 102 (14.2)
African American 4 (0.5) 10 (1.4)
Hispanic 4 (0.5) 3 (0.4)
Unknown 2 (0.3) 0 (0.0)
Body mass index (kg/m2) 25.6 � 4.0 25.7 � 4.0
Risk factors
Hypertension 446 (56.9) 424 (59.0)
Dyslipidemia 259 (33.0) 249 (34.6)
Diabetes 203 (25.9) 212 (29.5)
Current smoker (#3 months) 108 (13.8) 98 (13.6)
Former smoker (>3 months) 126 (16.1) 124 (17.2)
Premature family history of CAD 67 (8.5) 57 (7.9)
Pre-test likelihood of obstructive CAD, % 51 � 30 52 � 30
Angina type
Typical angina 243 (31.0) 216 (30.1)
Atypical angina 315 (40.2) 278 (38.7)
Noncardiac chest pain 18 (2.3) 10 (1.4)
Asymptomatic 90 (11.5) 76 (10.6)
Other symptoms 117 (14.9) 138 (19.2)
Dyspnea 106 (13.5) 127 (17.7)
Palpitations 5 (0.6) 6 (0.8)
Dizziness or syncope 6 (0.7) 4 (4.3)
Arrhythmia 0 (0.0) 1 (0.1)
Nonemergent indications for ICA
NIST findings 227 (29.0) 201 (28.0)
Symptomatic with abnormal NIST 183 (23.4) 165 (23.0)
Asymptomatic with >2 CAD risk factorsand an abnormal NIST
39 (5.0) 32 (4.5)
Worsening NIST 5 (0.6) 4 (0.6)
Symptoms 533 (68.0) 477 (66.3)
Persistent angina despite optimized medical therapy 201 (25.6) 205 (28.5)
Any angina, not evaluable by NIST 286 (36.5) 231 (32.1)
Heart failure with normal ejection fractionof unknown etiology
46 (5.9) 41 (5.7)
Other clinical indications 24 (3.1) 41 (5.7)
Low-risk surgery, stable angina, high-risksurgery with equivocal NIST or vascularsurgery with $2 risk factors
17 (2.2) 19 (2.6)
Asymptomatic, high-risk occupation orother miscellaneous
7 (0.9) 22 (3.1)
No. of vessels with obstructive CAD $50% onthe index procedure
No CAD 269 (34.4) 174 (24.2)
Nonobstructive CAD 294 (37.6) 265 (36.9)
1-vessel CAD 126 (16.1) 127 (17.7)
2-vessel CAD 52 (6.6) 82 (11.4)
3-vessel or left main stenosis 41 (5.2) 71 (9.9)
Values are mean � SD or n (%).
ICA ¼ invasive coronary angiography; NIST ¼ non-invasive stress testing; other abbreviations as Table 1.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Chang et al.J U L Y 2 0 1 9 : 1 3 0 3 – 1 2 Selective Referral to Cath
1307
continuous variables were compared using Student’st-tests.
The null hypothesis was that the ratio of hazardrates of the direct referral arm compared with theselective referral arm ($1.33). Additional comparisonsof the selective and direct referral arms used a time-to-first MACE analysis using a Cox proportional-hazards model. MACE-free survival probabilitieswere calculated using Kaplan-Meier survival curves.ICA normalcy was calculated using the first ICA thatoccurred within 1 year of enrollment. Modeled radi-ation dose (in millisieverts) was estimated for theinitial test using the dose�length product for CCTAand published survey data for ICA (15–17). Finally, wemodeled diagnostic cost using a hybrid approach inwhich utilization data (from Table 1) were multipliedby published cost estimates, including Medicarepayment rates for fiscal year 2016 (18). All analyseswere performed with SAS 9.4 (SAS Institute Inc., Cary,North Carolina).
RESULTS
DESCRIPTIVE STATISTICS. Enrollment was initiatedon December 2012 and completed on July 2015. A totalof 1,611 patients were randomized, with follow-updata available for 1,503 patients (90.3%) at the timeof study completion (Figure 1). Among the 823 pa-tients randomized to the selective referral strategy,784 underwent CCTA, and among the 808 patientsrandomized to the direct referral strategy, 719 un-derwent ICA. Additional analyses can found in theSupplemental Appendix.
The mean age of the study population was 60 � 12years; 46.2% were women (Table 2). CAD risk factorswere prevalent: 58% were hypertensive, 34% weredyslipidemic, 28% had diabetes, and 30% were cur-rent or former smokers. The pre-test likelihood ofCAD was largely intermediate risk. Most patientswere symptomatic, with typical and atypical anginareported in 31% and 40% of patients, respectively. Onthe index procedure, the prevalence of obstructiveCAD was 28% for CCTA and 39% for the direct referralto ICA arm (p < 0.001).
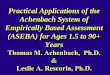
MACE RATES. The median follow-up was 12.3 months(interquartile range: 11.7 to 13.2 months). Duringfollow-up, 4.6% (n ¼ 36) of the selective referral armand 4.6% (n ¼ 33) of the direct referral arm experi-enced MACEs (p ¼ 0.99) (Table 3, Figure 2). For theprimary outcome, the hazard ratio was 0.99 (95%confidence interval: 0.66 to 1.47; p¼0.026 for the1-sided test of noninferiority). Pre-specified

TABLE 3 MACE Rate by Randomization to Selective Referral Versus Direct Referral to ICA
SelectiveReferral(n ¼ 784)
DirectReferral(n ¼ 719)
Hazard Ratio(95% CI) p Value
Any MACE (primary endpoint) 36 (4.6) 33 (4.6) 0.99 (0.62–1.58) 0.99
Death 2 (0.3) 1 (0.1)
Acute myocardial infarction 2 (0.3) 2 (0.3)
Unstable angina 9 (1.1) 8 (1.1)
Cardiac hospitalization 33 (4.2) 31 (4.3)
Stroke 2 (0.3) 2 (0.3)
Composite of MACE or major bleed 36 (4.6) 35 (4.9) 0.93 (0.58–1.48) 0.75
Major bleed 0 (0.0) 2 (0.3)
Need for major transfusion 0 (0.0) 1 (0.1)
Values are n (%) unless otherwise indicated.
CI ¼ confidence interval; MACE ¼ major adverse cardiovascular event; other abbreviation as in Table 2.
FIGURE 2 MACE-F
.00
0.0
0.2
0.4
0.6
0.8
1.0
Cum
ulat
ive
MAC
E-Fr
ee S
urvi
val
Kaplan-Meier major a
to selective referral
Chang et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Selective Referral to Cath J U L Y 2 0 1 9 : 1 3 0 3 – 1 2
1308
secondary clinical endpoints were rare, with majorbleeding occurring in 2 patients in the direct referralarm that required 1 major transfusion. No bleeding orrequirement for transfusion occurred in the selectivereferral arm (Table 3). There was no significant dif-ference in the secondary clinical endpoints (4.6% vs4.5%, p ¼ 0.48) (Supplemental Appendix).
FOLLOW-UP INVASIVE AND NONINVASIVE
TESTING. The rate of follow-up ICA was lower in theselective referral group; 23% of patients underwentfollow-up ICA compared with 100% of the directreferral patients. An additional 4% of patients in thislatter arm underwent repeat ICA (Table 1). Similarly,rates of PCI were lower in the selective referralpatients (11% vs. 15% in the direct referral arm;p < 0.001) (Table 1). In contrast, the proportion ofpatients who underwent any downstream exercise
ree Survival
.25 .50 .75 1.00 1.25 1.50Follow-Up Time (In Years)
Direct-Referral
Selective-Referral
dverse cardiovascular event (MACE)�free survival by randomization
versus direct referral to invasive coronary angiography (p ¼ 0.95).
electrocardiography, stress nuclear, or stress echo-cardiography was higher in the selective referral arm(14% vs. 11%; p ¼ 0.04). No differences were noted inthe proportion of patients who were reported as freefrom angina at the completion of follow-up (60% inthe selective referral arm vs. 62% in the direct referralarm, p ¼ 0.52).
DETECTION OF OBSTRUCTIVE CAD AT ICA. The ICAnormalcy rate, defined as no obstructive CAD, was25% (24 of 114 patients) in the selective referral armcompared with 61% (439 of 719 patients) in the directreferral arm (p < 0.001). Among the 219 patientsidentified with obstructive CAD by CCTA in the se-lective referral arm, only 52% went on to ICA duringfollow-up; a lower proportion of patients withobstructive CAD by the index study underwentrevascularization in the selective referral group (34%of 219 vs. 43% of 280; p ¼ 0.04). Of these patients,functional evaluation by stress testing or fractionalflow reserve was performed before revascularizationin 73 of 74 (99%) patients in the selective referralgroup compared with 113 of 121 (93%) patients in thedirect referral group (p < 0.001). Although higherrates of follow-up testing were reported in the se-lective referral arm, cumulative diagnostic test costsremained 57% lower in the selective referral arm,which was solely due to the higher upfront costsassociated with ICA (Figure 3).
RADIATION EXPOSURE. The median effective dosefor diagnostic ICA is 7 to 9 mSv (16,17). By compari-son, the observed CCTA median effective dose in theCONSERVE trial was 6.5 mSv.
DISCUSSION
The CONSERVE trial was a multinational, random-ized clinical trial with a pragmatic strategy design forpatients with stable but suspected CAD who wereeligible based on guideline indications of non-emergent ICA. In this trial, we observed that aselective referral strategy, in which decisions toproceed to ICA were informed by CCTA findings, metthe noninferiority multiplicative margin of 1.33(p ¼ 0.026), with similar MACE event rates of 4.6% inboth arms. However, additional observationsrevealed that compared with patients in the directreferral group, 77% of patients in the selectivereferral group avoided ICA, and, as such, diagnosticevaluation costs were reduced by 57%. In addition, astrategy of CCTA followed by selective ICA signifi-cantly improved the diagnostic yield, with animproved detection of obstructive CAD comparedwith those who underwent direct ICA. This enrichedyield of a CCTA arm was expected based on this

FIGURE 3 Diagnostic Procedural Cost
$582
$112
81% ↑
$500
$-
$1,000
$1,500
$2,000
$2,500
$3,000
Follow-Up Invasive
Invasive Test Cost Noninvasive Test Cost
$200 $94
53% ↑
$500
$-
$1,000
$1,500
$2,000
$2,500
$3,000
Follow-Up Noninvasive
Total Diagnostic Cost
$1,183
$2,755
57% ↓
$500
$-
$1,000
$1,500
$2,000
$2,500
$3,000
Total Diagnostic
Selective Referral Direct Referral
Follow-Up Test Cost
Index Test Cost
$500
$-
$1,000
$1,500
$2,000
$2,500
$3,000$2,549
$401
Index
84% ↓
Estimated cost for diagnostic procedures in the CONSERVE trial: a comparison of selective- versus direct-referral to invasive coronary angiography. Costs are presented
as average per patient costs on the index test, follow-up (invasive and noninvasive) testing, and total diagnostic costs. A comparison of costs in the selective referral
arm versus the direct referral arm is presented at the top of each set of the columns (e.g., index costs were 84% lower for the selective referral arm versus the direct
referral arm of the trial.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Chang et al.J U L Y 2 0 1 9 : 1 3 0 3 – 1 2 Selective Referral to Cath
1309
selective testing approach because patients pro-ceeding to ICA would be more often those with evi-dence of obstructive CAD.
COMPARATIVE EVIDENCE FROM OTHER TRIALS
AND REGISTRIES. These data supported that CCTAexhibits excellent diagnostic performance and pro-vides, for the first time, a demonstration of a strategyof care not previously illustrated in previous ran-domized trials. Previous pragmatic trials largelycompared CCTA with functional testing, such as theNational Institutes of Health-National Heart, Lung,and Blood Institute PROMISE (Prospective Multi-center Imaging Study for Evaluation of Chest PainTrial) and other trials (19–23). Our results contrastedwith previous trials, which generally demonstratedincreased revascularization in the CCTA groupscompared with functional testing. In contrast, theCONSERVE trial evaluated CCTA in higher risk pa-tient groups at a later stage in clinical decision-making (because most patients were enrolledfollowing an abnormal stress test or for persistent orworsening symptoms despite medical therapy) as a“gatekeeper” to identify candidates who might havesafely avoided ICA (19). A similar gatekeeper strategywas reported in the Cost-Effectiveness of functionalCardiac Testing in the diagnosis and management ofCAD trial that revealed ICA was reduced by 20% to25% in the 898 patients who underwent stress
imaging compared with direct referral to ICA. Inaddition, the single-center Coronary Artery DiseaseManagement trial of 340 patients also evaluatedCCTA as a gatekeeper to ICA for a narrower range ofindications restricted to a chest pain evaluation (24).This report by Dewey et al. (24) noted reductions inICA of >80%. However, they used a shorter durationof follow-up through only 48 h to assess near-termsafety of major procedural complications (p ¼ 1.00).Our trial could be contrasted with this previousfinding because we broadened enrollment to patientswith diverse indications and from multiple centersaround the world, and extended follow-up to 12months, which was a sufficient duration to capturethe entire episode of care.
Our low event rate was not atypical from current apriori designed clinical trials, but it did limit ourstrength of evidence and causal statements thatmight be inferred from the CONSERVE trial. Sug-gested inferences from our trial should support thedocumented similar safety profile for a selectivereferral strategy guided by CCTA findings comparedwith direct referral to ICA in largely lower risk pa-tients referred for nonemergent indications. Thereduction in the use of ICA in the selective referralarm guided by CCTA findings was noteworthy, and itsfindings might have applicability to current diag-nostic testing approaches. Moreover, our data were inaccord with randomized trials that examined the

Chang et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Selective Referral to Cath J U L Y 2 0 1 9 : 1 3 0 3 – 1 2
1310
safety of an initial trial of optimal medical therapyversus an angiographically-guided coronary revascu-larization strategy (9,25).
Often, a criticism of CCTA is the potential foroveruse of ICA, but in the CONSERVE trial, post-testmanagement relied upon ischemia-guided care andresulted in the use of stress testing to further selectcandidates for ICA and revascularization. Our studydemonstrated an overall 28% reduction in coronaryrevascularization rates in the selective referralgroup, with increased stress testing and decreasedrevascularization even among those with obstructiveCAD by the index study. This exhibited the “diag-nostic-therapeutic cascade,” in which the temporalcoupling of ICA with the ability to perform revascu-larization resulted in more liberal use of ad hocPCI (26).
ENRICHING THE DIAGNOSTIC YIELD GUIDED BY
CCTA. The CONSERVE trial had clinical applicabilityfor patients referred for nonemergent ICA because aselective strategy guided by CCTA could avoidapproximately 4 of 5 ICA procedures, and reduce therate of ICA normalcy by nearly two-thirds. We useda simple diagnostic test that was interpreted on siteby treating site physicians, required no central corelaboratory analysis, and was applicable to a widerpatient population who were referred for ICA. Froma policy perspective, implementation of a selectivereferral strategy might result in markedly fewerinvasive diagnostic and revascularization proced-ures, with increased noninvasive testing. Our resultsmight provide insights as to the potential magnitudeof impact of the updated United Kingdom NationalInstitute for Clinical Excellence (UK-NICE) guide-lines, which recommend CCTA as the first-line testfor coronary artery disease (27). We proposed thatresults from the CONSERVE trial are generalizable tocontemporaneous ICA for several reasons. First, thepatient indications used for inclusion were stillconsidered appropriate by contemporary profes-sional societal guidance documents, and reflectedcommon and routine practices across our variedenrolling centers (4). Moreover, post-CCTA oftenrelied on noninvasive stress testing to further refinethe selective referral arm and inform the use of ICA.Approximately 40% of patients in the ACC CathPCIregistry underwent ICA without previous stresstesting (28). This registry reported a high rate of noobstructive CAD and suggested that alternative ap-proaches should be used to avert unnecessary ICA, ifpossible. Our results also extended the findings fromthe PLATFORM (Prospective Longitudinal Trial ofFFR-CT: Outcome and Resource Impacts) study,
which was an observational registry that enrolled asubgroup of patients who were candidates for ICA(29). From the PLATFORM ICA cohort, a combinedstrategy of CCTA in addition to noninvasive frac-tional flow reserve resulted in an ICA cancellationrate of 61% and a marked reduction in the finding ofno obstructive CAD at ICA. However, in this study, aCCTA-alone arm was not evaluated. In this regard,the CONSERVE findings offered insight into theefficacy of CCTA alone, to serve as an efficientgatekeeper of ICA, with a 77% reduction in ICA anda similar 1-year safety profile of few reported majoradverse clinical events, as observed in the PLAT-FORM study. The present study results suggestedthat, at least for the purposes of guiding referral toICA, that CCTA alone might represent an effectiveapproach.
STUDY LIMITATIONS. Our pragmatic trial wasgeneralizable to real-world clinical practice patterns,with referral decisions to ICA and revascularizationbased on the overall judgment of site physiciansfrom a wide array of international sites, as opposedto protocolized care that would increase uniformitywithin the trial. Our trial was typical of most inwhich accrual of lower risk patients resulted in lowerthan expected MACE rates. We performed a post hocpower calculation, and based on the reported MACErate of 4.6%, the available power was 62% (a ¼ 0.05)to detect noninferiority between the randomizedarms of our trial. The CONSERVE trial was alsopowered to include “softer” endpoints; a trial for theuse of only “hard” clinical outcomes would haverequired a substantially larger sample size becauseof the identical frequency of adverse clinical eventsin each trial arm. For any trial, patients who are lostto follow-up are an important consideration. Wecompared those patients included in the presentanalysis and compared with those who were lost,which revealed similarities in presenting symptoms,risk factor prevalence, and pre-test likelihood ofCAD (Supplemental Appendix). The lower rate ofobserved obstructive CAD might challenge whetherdirect referral should have been an option, but in-dications for referral to ICA were in accordance tosocietal guidelines, and reflected the high rate ofnormal ICA often quoted in the published literature(5,30). Finally, because of the null results of theVeteran Affairs�sponsored Clinical Outcomes UsingRevascularization and Aggressive Drug Evaluationtrial, some might argue that direct referral should becompared with no testing rather than to a selectivereferral strategy. Further investigation now appearswarranted to address this question, (9).

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Evidence sup-
ports that most patients undergoing elective ICA do not have
obstructive CAD. We compared 1-year MACE-free survival and
downstream resource use of a selective referral strategy using
CCTA compared with a direct referral strategy to ICA. Our results
noted similar 1-year MACE rates (p ¼ 0.95). The selective referral
strategy was noninferior to the direct referral strategy at a
margin of 1.33 (p ¼ 0.026), albeit with reduced statistical power.
In patients who underwent initial CCTA or the selective referral
arm, we observed a marked reduction in the use of follow-up ICA
(by w80%) and diagnostic cost savings of 57%. These results
supported the use of CCTA as a front-line diagnostic procedure,
followed by selective referral to ICA of a greater proportion of
patients with obstructive CAD.
TRANSLATIONAL OUTLOOK: The CONSERVE trial aimed to
evaluate, in a randomized trial setting, the potential to safely shift
lower risk patients eligible for elective ICA to less expensive CCTA.
Because of the high rate of ICA across the United States, the
implications of findings from the CONSERVE trial could expedite a
patient’s diagnosis of CAD while providing for a prompt and
efficient diagnostic pathway guided by CCTA findings.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Chang et al.J U L Y 2 0 1 9 : 1 3 0 3 – 1 2 Selective Referral to Cath
1311
CONCLUSIONS
In this trial of stable patients with suspected CAD whowere referred for guideline-directed ICA, a selectivereferral strategy was found to result in similar MACErates at 1 year of follow-up compared with a direct-referral strategy. Growing evidence supports thatnoninvasive anatomic testing by CCTA alone, as agatekeeper procedure, may prove advantageous inpromptly and accurately identifying candidates fordownstream procedures. These data and similarlyrelevant findings from other randomized trials call forrevisions to the current ischemic heart diseaseguidelines for the evaluation of patients with stableischemic heart disease (3).
ADDRESS FOR CORRESPONDENCE: Dr. James K.Min, Department of Radiology and Medicine, DalioInstitute of Cardiovascular Imaging, Weill CornellMedicine, 413 E. 69th Street, Suite 108, New York,New York 10021. E-mail: [email protected] Dr. Hyuk-Jae Chang, Division of Cardiology,Severance Cardiovascular Hospital, Yonsei UniversityCollege of Medicine, 50-1 Yonsei-ro, Seodaemun-gu,Seoul 03722, South Korea. E-mail: [email protected],Twitter: @lesleejshaw.
RE F E RENCE S
1. Writing Group Members, Mozaffarian D,Benjamin EJ, et al. Heart disease and strokestatistics-2016 update: a report from the Amer-ican Heart Association. Circulation 2016;133:e38–60.
2. Scanlon PJ, Faxon DP, Audet AM, et al. ACC/AHA guidelines for coronary angiography. A reportof the American College of Cardiology/AmericanHeart Association Task Force on practice guide-lines (Committee on Coronary Angiography).Developed in collaboration with the Society forCardiac Angiography and Interventions. J Am CollCardiol 1999;33:1756–824.
3. Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for thediagnosis and management of patients with stableischemic heart disease: a report of the AmericanCollege of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines, andthe American College of Physicians, American As-sociation for Thoracic Surgery, Preventive Cardio-vascular Nurses Association, Society forCardiovascular Angiography and Interventions,and Society of Thoracic Surgeons. J Am Coll Car-diol 2012;60:e44–164.
4. Patel MR, Bailey SR, Bonow RO, et al.ACCF/SCAI/AATS/AHA/ASE/ASNC/HFSA/HRS/SCCM/SCCT/SCMR/STS 2012 Appropriate usecriteria for diagnostic catheterization: a reportof the American College of Cardiology Foun-dation Appropriate Use Criteria Task Force,
Society for Cardiovascular Angiography andInterventions, American Association forThoracic Surgery, American Heart Association,American Society of Echocardiography,American Society of Nuclear Cardiology, HeartFailure Society of America, Heart Rhythm So-ciety, Society of Critical Care Medicine, Societyof Cardiovascular Computed Tomography,Society for Cardiovascular Magnetic Reso-nance, and Society of Thoracic Surgeons. J AmColl Cardiol 2012;59:1995–2027.
5. Patel MR, Peterson ED, Dai D, et al. Low diag-nostic yield of elective coronary angiography.N Engl J Med 2010;362:886–95.
6. Chinnaiyan KM, Raff GL, Goraya T, et al. Coro-nary computed tomography angiography afterstress testing: results from a multicenter, state-wide registry, ACIC (Advanced Cardiovascular Im-aging Consortium). J Am Coll Cardiol 2012;59:688–95.
7. Tonino PAL, De Bruyne B, Pijls NHJ, et al.Fractional flow reserve versus angiography forguiding percutaneous coronary intervention.N Engl J Med 2009;360:213–24.
8. Al-Lamee R, Thompson D, Dehbi H-M, et al.Percutaneous coronary intervention in stableangina (ORBITA): a double-blind, randomisedcontrolled trial. Lancet 2018;391:31–40.
9. Boden WE, O’Rourke RA, Teo KK, et al. Optimalmedical therapy with or without PCI for stable
coronary disease. N Engl J Med 2007;356:1503–16.
10. Budoff MJ, Dowe D, Jollis JG, et al. Diagnosticperformance of 64-multidetector row coronarycomputed tomographic angiography for evalua-tion of coronary artery stenosis in individualswithout known coronary artery disease: resultsfrom the prospective multicenter ACCURACY(Assessment by Coronary Computed TomographicAngiography of Individuals Undergoing InvasiveCoronary Angiography) trial. J Am Coll Cardiol2008;52:1724–32.
11. Meijboom WB, Meijs MF, Schuijf JD, et al.Diagnostic accuracy of 64-slice computed to-mography coronary angiography: a prospective,multicenter, multivendor study. J Am Coll Cardiol2008;52:2135–44.
12. Miller JM, Rochitte CE, Dewey M, et al. Diag-nostic performance of coronary angiography by64-row CT. N Engl J Med 2008;359:2324–36.
13. Marwick TH, Cho I, Ó Hartaigh B, Min JK.Finding the gatekeeper to the cardiac catheteri-zation laboratory: coronary ct angiography orstress testing? J Am Coll Cardiol 2015;65:2747–56.
14. Raff GL, Abidov A, Achenbach S, et al. SCCTguidelines for the interpretation and reporting ofcoronary computed tomographic angiography.J Cardiovasc Comp Tomogr 2009;3:122–36.
15. Chen J, Einstein AJ, Fazel R, et al. Cumulativeexposure to ionizing radiation from diagnostic and

Chang et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Selective Referral to Cath J U L Y 2 0 1 9 : 1 3 0 3 – 1 2
1312
therapeutic cardiac imaging procedures: apopulation-based analysis. J Am Coll Cardiol2010;56:702–11.
16. Einstein AJ. Effects of radiation exposure fromcardiac imaging: how good are the data? J Am CollCardiol 2012;59:553–65.
17. Einstein AJ, Berman DS, Min JK, et al. Patient-centered imaging: shared decision making forcardiac imaging procedures with exposure toionizing radiation. J Am Coll Cardiol 2014;63:1480–9.
18. Mark DB, Federspiel JJ, Cowper PA, et al.Economic outcomes with anatomical versus func-tional diagnostic testing for coronary artery dis-ease. Ann Intern Med 2016;165:94–102.
19. Douglas PS, Hoffmann U, Patel MR, et al.Outcomes of anatomical versus functional testingfor coronary artery disease. N Engl J Med 2015;372:1291–300.
20. Scot-Heart Investigators. CT coronary angi-ography in patients with suspected angina due tocoronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet2015;385:2383–91.
21. Thom H, West NE, Hughes V, et al. Cost-effectiveness of initial stress cardiovascular MR,stress SPECT or stress echocardiography as agate-keeper test, compared with upfront invasivecoronary angiography in the investigation andmanagement of patients with stable chest pain:
mid-term outcomes from the CECaT randomisedcontrolled trial. BMJ Open 2014;4:e003419.
22. Foy AJ, Dhruva SS, Peterson B, Mandrola JM,Morgan DJ, Redberg RF. Coronary computed to-mography angiography vs functional stress testingfor patients with suspected coronary artery dis-ease: a systematic review and meta-analysis.JAMA Intern Med 2017;177:1623–31.
23. Jorgensen ME, Andersson C, Norgaard BL,et al. Functional testing or coronary computedtomography angiography in patients with stablecoronary artery disease. J Am Coll Cardiol 2017;69:1761–70.
24. Dewey M, Rief M, Martus P, et al. Evaluationof computed tomography in patients with atypicalangina or chest pain clinically referred for invasivecoronary angiography: randomised controlledtrial. BMJ 2016;355:i5441.
25. BARI 2D Study Group, Frye RL, August P, et al.A randomized trial of therapies for type 2 diabetesand coronary artery disease. N Engl J Med 2009;360:2503–15.
26. Lucas FL, Siewers AE, Malenka DJ,Wennberg DE. Diagnostic-therapeutic cascaderevisited: coronary angiography, coronary arterybypass graft surgery, and percutaneous coronaryintervention in the modern era. Circulation 2008;118:2797–802.
27. Moss AJ, Williams MC, Newby DE, Nicol ED.The updated NICE guidelines: cardiac ct as the
first-line test for coronary artery disease. CurrCardiovasc Imaging Rep 2017;10:15.
28. Abdallah MS, Spertus JA, Nallamothu BK,Kennedy KF, Arnold SV, Chan PS. Symptoms andangiographic findings of patients undergoingelective coronary angiography without prior stresstesting. Am J Cardiol 2014;114:348–54.
29. Douglas PS, Pontone G, Hlatky MA, et al.Clinical outcomes of fractional flow reserve bycomputed tomographic angiography-guideddiagnostic strategies vs. usual care in patientswith suspected coronary artery disease: the pro-spective longitudinal trial of FFR(CT): outcomeand resource impacts study. Eur Heart J 2015;36:3359–67.
30. Patel MR, Dai D, Hernandez AF, et al. Preva-lence and predictors of nonobstructive coronaryartery disease identified with coronary angiog-raphy in contemporary clinical practice. Am HeartJ 2014;167:846–852 e2.
KEY WORDS coronary computedtomographic angiography, invasive coronaryangiography, major adverse cardiac events,stable ischemic heart disease
APPENDIX For the list of participatingcenters, an expanded Methods section, and asupplemental table and figure, please see theonline version of this paper.

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
EDITORIAL COMMENT
CONSERVE Your Energy and Resources*
David E. Newby, DMSEE PAGE 1303
T here are a wide range of noninvasive investi-gations at our disposal for the assessment ofchest pain and suspected coronary heart dis-
ease. Current international guidelines recommendinvestigations depending on either the presentingcharacteristics of the patient or their pre-test proba-bility of obstructive coronary heart disease. A centralfeature of these guidelines is to refer high-riskpatients directly for invasive coronary angiographyor to use noninvasive testing to select outintermediate-risk patients who may need invasivecoronary angiography. For the latter, there havebeen many trials that have compared the perfor-mance of different noninvasive strategies to achievethis (1,2). However, there have been few trials thathave done the reverse: can we use a noninvasivetest to avoid unnecessary invasive coronary angiog-raphy in higher risk patients who should undergoguideline-directed invasive coronary angiography?This is important because rates of normal coronaryarteries in patients who have undergone invasivecoronary angiography continue to be unacceptablyhigh, and, in some institutions, these rates are>50% (3).
Coronary computed tomography coronary angi-ography (CCTA) is becoming an increasingly popularinvestigative strategy because it increases diag-nostic certainty, better risk stratifies patients,guides treatment decisions, and can reduce long-term rates of myocardial infarction (1,4,5). Particu-larly relevant here, CCTA also markedly reduces therate of normal coronary arteries identified at thetime of invasive coronary angiography (2,5). Thisreduction in rates of normal coronary angiography
ISSN 1936-878X/$36.00
*Editorials published in JACC: Cardiovascular Imaging reflect the views of
the authors and do not necessarily represent the views of iJACC or the
American College of Cardiology.
From the British Heart Foundation Centre for Cardiovascular Science,
University of Edinburgh, Edinburgh, Scotland, United Kingdom. Dr.
Newby has reported that he has no relationships relevant to the
contents of this paper to disclose.
occurs despite CCTA often overcalling the severityof coronary stenosis. The latter is, in part, related tobetter definition of coronary plaque, for whichpositive remodeling often means a cross-sectionalstenosis is >70%, whereas the luminal diameterstenosis on invasive coronary angiography canbe <50% because there is no visualization of theexpanded and remodeled coronary artery wall. Thealternative problem of under calling the degree ofstenosis is much less common and is often causedby CCTA interpretation in the presence of extensivecoronary calcification—the Achilles heel of CCTA.However, overall, CCTA is 3 times more likely toover call than under call a stenosis, which suggestsit is a relatively safe and conservative approach.Moreover, CCTA is robust in determining the pres-ence of any coronary heart disease, irrespective ofstenosis severity, giving it an excellent negativepredictive value for the exclusion of coronary heartdisease.
The CONSERVE (Coronary Computed TomographicAngiography for Selective Cardiac Catheterization)trial, reported by Chang et al. (6) in this issue ofiJACC, is an important contribution to the fieldbecause it has taken the bold step of investigatingwhether doing a CCTA first is better for higher riskpatients who are referred directly for invasive coro-nary angiography. The investigators asked the ques-tion of whether CCTA could avoid unnecessaryinvasive coronary angiography with its attendantrisks, and whether such a strategy is safe and non-inferior to direct invasive coronary angiography. Inkeeping with the higher risk population, the rates oftypical and atypical angina and subsequent identifi-cation of coronary heart disease were high, with morethan two-thirds of the study population classified inthis way. Marked differences were seen in the rates ofinvasive coronary angiography, with more than three-quarters of patients in the CCTA group no longerneeding invasive coronary angiography. Moreover,this marked reduction was also associated with a
https://doi.org/10.1016/j.jcmg.2018.10.009

Newby J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 3 1 3 – 5
1314
3-fold reduction in the rates of visualizing normalcoronary arteries or nonobstructive disease at thetime of invasive coronary angiography. This wasconsistent with previous studies that examined pa-tients hospitalized with acute chest pain, in whom therates of invasive angiography and normal coronaryangiograms were also markedly reduced (7). Thisreaffirms the excellent negative predictive value ofCCTA and its usefulness in being a “gate keeper” forthe cardiac catheterization laboratory. Such dramaticeffects were reflected in a decrease of 50% in overalldiagnostic costs, which suggested a favorable healtheconomic rationale for a CCTA first approach. Finally,and most importantly, this approach was safe, withidentical rates of major adverse coronary artery dis-ease events, which allowed the trial to meet its non-inferiority threshold.
Another important feature of the trial was theobserved reduction in coronary revascularizationprocedures with CCTA. Previous criticisms reportedthat CCTA leads to more coronary revascularizationsin intermediate-risk patients. However, recent evi-dence demonstrated that early increases were offsetby later reductions in the need for coronary revas-cularization (5), which suggested that CCTA betteridentified patients with coronary heart disease andled to earlier optimal treatment and prevention ofdownstream disease progression or recurrent pre-sentations. In the CONSERVE trial, there was areduction in early rates of coronary revascularization.Although this may, in part, be attributable to theCCTA group appearing to have slightly lower risk ofdisease, some of the benefit was likely to due to theimpetus to treat stenotic disease in the cardiac cath-eterization laboratory. The demonstration of 1- or 2-vessel disease, which does not carry a prognosticbenefit from coronary revascularization, means thatphysicians might be more prepared to treat patientswith medical therapy for longer periods of time ratherthan the interventional cardiologist proceeding topercutaneous coronary intervention at the time ofinvasive angiography—the so-called oculo-stenoticreflex.
Some limitations of the trial should be acknowl-edged. The CONSERVE trial was an open-label study,which is common for all CCTA studies. Some elementof patient bias was apparent because more patientsappeared to withdraw when assigned to the invasivecoronary angiography arm of the trial (71 patients vs.26 patients), which suggested a strong patient pref-erence for CCTA. This might have also influenced howkeen patients were to undergo invasive coronaryangiography when assigned to the CCTA arm. This
might have led to some over estimation of thereduction in subsequent rates of invasive coronaryangiography, although this alone was unlikely to ac-count for the overall dramatic difference. This effectmight also explain why there appeared to be morepatients with severe coronary artery disease in theinvasive coronary angiography arm. Those with moresevere symptoms might have had a preference forinvasive angiography and preferred to accept it,whereas those with mild symptoms might have had apreference for less invasive investigations. Thosewho withdrew from invasive coronary angiographywere at a much lower risk of disease with atypicalsymptoms.
Another important consideration was the domi-nance of cardiac hospitalizations in the primaryendpoint rather than the harder clinical endpoints ofmyocardial infarction or death. However, for cardiachospitalizations, a bias against CCTA would beanticipated if it was seen as being inferior to the goldstandard of invasive coronary angiography, becausepatients who have had a CCTA and present to thehospital with unclear symptoms are more likely to beadmitted to the hospital with possible unstableangina, as was seen in the PROMISE (ProspectiveMulticenter Imaging Study for Evaluation of ChestPain) trial (2). Overall, the rates of hard endpointswere low, and the duration of follow-up was short. Itoften takes more considerable durations of follow-upto demonstrate potential differences (5), and it will beinteresting to see if this is the case for the CONSERVEtrial if longer term follow-up is undertaken.
The CONSERVE trial addressed an important clin-ical question and lends further weight to theincreasing use of CCTA as a first-line test of choice inpatients being investigated for coronary heart dis-ease. It showed that even in those who are directlyreferred for invasive coronary angiography, CCTA is anoninferior alternative that reduces the need forinvasive angiography, decreases invasive procedures,and appears to result in similar short-term clinicaloutcomes. So now, the question is why would you gostraight for invasive coronary angiography? Shouldyou not CONSERVE your energy and resources, anduse CCTA instead?
ADDRESS FOR CORRESPONDENCE: Prof. David E.Newby, British Heart Foundation John WheatleyChair of Cardiology, British Heart Foundation Centrefor Cardiovascular Science, University of Edinburgh,Room SU314, Chancellor’s Building, 49 Little FranceCrescent, Edinburgh, Scotland EH16 4SA, UnitedKingdom. E-mail: [email protected].

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 NewbyJ U L Y 2 0 1 9 : 1 3 1 3 – 5 Editorial Comment
1315
RE F E RENCE S
1. The SCOT-HEART Investigators. CT coronaryangiography in patients with suspected angina dueto coronary heart disease (SCOT-HEART): anopen-label, parallel-group, multicentre trial. Lan-cet 2015;385:2383–91.
2. Douglas PS, Hoffmann U, Patel MR, et al.,PROMISE Investigators. Outcomes of anatomicalversus functional testing for coronary artery dis-ease. N Engl J Med 2015;372:1291–300.
3. Douglas PS, Patel MR, Bailey SR, et al. Hospitalvariability in the rate of finding obstructivecoronary artery disease at elective diagnostic
coronary angiography. J Am Coll Cardiol 2011;58:801–9.
4. Williams MC, Hunter A, Shah ASV, et al. Use ofcoronary computed tomographic angiography toguide management of patients with coronary dis-ease. J Am Coll Cardiol 2016;67:1759–68.
5. The SCOT-HEART Investigators. Coronary CTangiography and 5-year risk of myocardial infarc-tion. N Engl J Med 2018;379:924–33.
6. Chang H-J, Lin FY, Gebow D, et al. Selectivereferral using CCTA versus direct referral for in-dividuals referred to invasive coronary angiography
for suspected CAD: a randomized, controlled, open-label trial. J Am Coll Cardiol Img 2019;12:1303–12.
7. Dewey M, Rief M, Martus P, et al. Evaluation ofcomputed tomography in patients with atypicalangina or chest pain clinically referred for invasivecoronary angiography: randomised controlledtrial. BMJ 2016;355:i5441.
KEY WORDS coronary computed tomographicangiography, invasive coronary angiography,major adverse cardiac events, stable ischemicheart disease

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
ORIGINAL RESEARCH
Anatomical and FunctionalComputed Tomography forDiagnosing HemodynamicallySignificant Coronary Artery Disease
A Meta-AnalysisCsilla Celeng, MD, PHD,a Tim Leiner, MD, PHD,a Pál Maurovich-Horvat, MD, PHD, MPH,b Béla Merkely, MD, PHD,b
Pim de Jong, MD, PHD,a Jan W. Dankbaar, MD, PHD,a Hendrik W. van Es, MD, PHD,c Brian B. Ghoshhajra, MD, MBA,d
Udo Hoffmann, MD, MPH,d Richard A.P. Takx, MD, PHD, MSCa,c,d
ABSTRACT
ISS
Fro
Im
St.
Ma
OBJECTIVES This meta-analysis determined the diagnostic performance of coronary computed tomography (CT)
angiography (CTA), CT myocardial perfusion (CTP), fractional flow reserve CT (FFRCT), the transluminal attenuation
gradient (TAG), and their combined use with CTA versus FFR as a reference standard for detection of hemodynamically
significant coronary artery disease (CAD).
BACKGROUND CTA provides excellent anatomic, albeit limited functional information for the evaluation of CAD.
Recently, various functional CT techniques emerged to assess the hemodynamic consequences of CAD.
METHODS This meta-analysis was performed in adherence to the PRISMA (Preferred Reporting Items for Systematic
Reviews and Meta-Analyses) guidelines. PubMed, EMBASE, and Web of Science were searched from inception until
September 7, 2017. Bayesian random effects analysis was used to compute pooled sensitivity, specificity, and the
summary receiver-operating characteristic curve of the index tests and compare them with the FFR as a reference
standard. Analyses were performed on vessel and patient levels. Because CTA has excellent sensitivity, specificity was
considered most relevant. Individual FFRCT values were collected.
RESULTS Overall, 54 articles and 5,330 patients were included. At vessel level, pooled specificity of CTP (0.86; 95%
confidence interval [CI]: 0.76 to 0.93), FFRCT (0.78; 95% CI: 0.72 to 0.83) and TAG (0.77; 95% CI: 0.61 to 0.89) were
substantially higher than that of CTA (0.61; 95% CI: 0.54 to 0.68). The addition of FFRCT, CTP, and TAG to CTA resulted
in high to excellent specificities (0.80 to 0.92). The summary receiver-operating characteristic curve at vessel level
yielded superior diagnostic accuracy for CTP, FFRCT, and combined CTA and CTP, compared with CTA. A subanalysis of on-
site versus off-site FFRCT revealed no substantial differences between the sensitivity (0.84 vs. 0.85) and specificity (0.80
vs. 0.73) of the 2 techniques. In a second subanalysis, dynamic CTP showed higher sensitivity (0.85 vs. 0.72), but had a
lower specificity (0.81 vs. 0.90) than static CTP.
CONCLUSIONS CTP and FFRCT demonstrated a substantial improvement in the identification of hemodynamically
significant CAD compared with CTA; therefore, their integration to clinical workflow before revascularization is
recommended. (J Am Coll Cardiol Img 2019;12:1316–25) © 2019 by the American College of Cardiology Foundation.
N 1936-878X/$36.00 https://doi.org/10.1016/j.jcmg.2018.07.022
m the aDepartment of Radiology, University Medical Center Utrecht, Utrecht, the Netherlands; bMTA-SE Cardiovascular
aging Research Group Heart and Vascular Center, Semmelweis University, Budapest, Hungary; cDepartment of Radiology,
Antonius Hospital, Nieuwegein, the Netherlands; and the dCardiac MR PET CT Program, Department of Radiology,
ssachusetts General Hospital, Harvard Medical School, Boston, Massachusetts. Dr. Celeng has received grant support from

AB BR E V I A T I O N S
AND ACRONYM S
CTA = computed tomography
angiography
CAD = coronary artery disease
CTP = computed tomography
myocardial perfusion
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Celeng et al.J U L Y 2 0 1 9 : 1 3 1 6 – 2 5 Functional CT for Diagnosing CAD
1317
C omputed tomography angiography (CTA)has a high sensitivity in the evaluation ofcoronary artery disease (CAD) (1–4). Howev-
er, its specificity for the detection of hemodynamical-ly significant CAD is still moderate at best, especiallyin cases of intermediate coronary stenosis (30% to70% reduction in coronary lumen diameter) (5).
SEE PAGE 1326 FFR = fractional flow reserve
LR = likelihood ratio
MRI = magnetic resonance
imaging
FFRCT = fractional flow reserve
computed tomography
SROC = summary receiver-
operating curve
TAG = transluminal
attenuation gradient
Invasive fractional flow reserve (FFR) is the currentreference standard for determining the hemodynamicsignificance of CAD (6–8). FFR is calculated as theratio between the maximum achievable myocardialblood flow during hyperemia in the presence of astenosis and the maximum achievable myocardialblood flow in the absence of a stenosis (6). FFR has a“grey zone” of ischemic threshold value (between0.75 and 0.80) (7). Previous comprehensive trialsshowed that the use of FFR-guided revascularizationreduced the rate of composite endpoints (death,nonfatal myocardial infarction, repeat revasculariza-tion) and urgent revascularization (9,10). Computedtomography myocardial perfusion imaging (CTP) hasbeen proposed as an alternative to magnetic reso-nance imaging (MRI) and nuclear cardiology tech-niques for the diagnosis of hemodynamicallysignificant CAD (11). In addition, new noninvasive CTtechniques have emerged, which allow the assess-ment of potential hemodynamic changes attributableto CAD without modification of imaging protocols oran additional radiation dose. Advances in computa-tional fluid dynamics allow for determination of sig-nificant ischemia by computation of noninvasive FFRCT (FFRCT) or the transluminal attenuation gradient(TAG) (12–15). The aim of this study was to conduct ameta-analysis to determine the diagnostic perfor-mance of CTA, CTP, FFRCT, and TAG, and the com-bined use of these techniques with CTA versusinvasive FFR as the reference standard for thedetection of hemodynamically significant CAD in pa-tients with suspected or known CAD.
METHODS
This systematic review and meta-analysis was con-ducted in agreement with the PRISMA (PreferredReporting Items for Systematic Reviews and Meta-Analyses) statement (16). The protocol was published
the European Association of Cardiovascular Imaging. Dr. Ghoshhajra has been
Dr. Hoffman has received research grants from KOWA, MedImmune, Pfizer,
reported that they have no relationships relevant to the contents of this pap
Manuscript received January 17, 2018; revised manuscript received July 8, 2
online (PROSPERO 2015 CRD42015017148).PubMed, EMBASE, and Web of Science weresystematically searched from inception toSeptember 7, 2017. The search syntax is pre-sented in Supplemental Table 1. No searchrestrictions were imposed for language ordate of publication. A manual reference checkof included articles was performed to identifyadditional articles missed by our systematicsearch.
ELIGIBILITY CRITERIA. Two independentresearchers (C.C. and R.A.P.T.) applied pre-defined criteria to determine article eligi-bility. Articles were included based on thefollowing criteria: study domain–patientswith suspected or known CAD; index test–CTA, CTP, FFRCT, and TAG, and the combi-
nation of CTA and CTP, CTA, and FFRCT, and CTA andTAG; reference standard–invasive FFR for interme-diate coronary lesions; study result–agreement be-tween the index and reference standard; and studydesign–cross-sectional study. In cases of studies withoverlapping populations, the study with the largerpopulation sample was included. Discordances be-tween reviewers were resolved by consensus. Animalstudies, phantom studies, and case reports (n < 10)were not included.DATA EXTRACTION AND CRITICAL APPRAISAL.
Data were extracted by one reviewer (C.C.) and veri-fied by a second reviewer (R.A.P.T.). The followingdata categories were extracted from the includedstudies: study population characteristics, index testcharacteristics, and reference test characteristics.True positive, false positive, false negative, and truenegative numbers were obtained. The results weresummarized in 2-by-2 contingency tables. In cases ofcombined modalities, the reviewers included onlythose studies that judged the combined test positiveif both CTA and functional CT were positive for he-modynamically significant CAD. This means that pa-tients with a positive test on CTA but negative onfunctional CT, or a negative CTA and positive test onfunctional CT, were deemed as not having hemody-namically significant CAD. In cases of multiple imag-ing thresholds, the pre-defined primary endpoint wasselected. If the primary endpoint was not reported,the best performing threshold was chosen. In
a consultant for Siemens Healthcare and Medtronic.
Siemens, and HeartFlow, Inc. All other authors have
er to disclose.
018, accepted July 12, 2018.

Celeng et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Functional CT for Diagnosing CAD J U L Y 2 0 1 9 : 1 3 1 6 – 2 5
1318
addition, the performance of FFRCT was evaluated atvessel level by digitizing scatterplots or Bland-Altmanplots, in which invasive FFR was used as the refer-ence standard using a previously described methodby Cook et al. (17). Because individual points in ascatterplot can overlap, studies with >10% missingdata points were omitted from the analysis. If indi-vidual FFRCT values were listed in a table, then thosevalues were extracted. A threshold of invasive FFRof #0.80 was used as the cutoff for hemodynamicallysignificant CAD. Two independent reviewers (C.C.and R.A.P.T.) assessed the relevance and validity ofthe included studies using the QUADAS-2 (QualityAssessment of Diagnostic Accuracy Studies) criteria(18). Discrepancies were resolved by consensus. Themaximum time between noninvasive and invasivestenosis degree assessment was also recorded. If thisperiod was >2 months, the flow and timing of thestudy was scored as high bias.DATA SYNTHESIS AND ANALYSIS. Analyses wereperformed at both vessel and patient level. Possiblepublication bias per imaging technique was assessedgraphically by generating funnel plots for modalitiesthat included $10 studies. Sensitivity, specificity,positive likelihood ratio (þLR) and negative LR (�LR),and the log diagnostic odds ratio, including the95% confidence interval, were calculated. Pooledresults were used to calculate the summary receiver-operating curves (SROCs). Heterogeneity wasassessed by visual inspection of SROCs (19). Due toanticipated methodological heterogeneity, Bayesianrandom effects analysis was performed, because itprovides more robust results in cases of studies with arelatively small sample size. Furthermore, it alsotakes the potential sources of variation (e.g., impre-cision of sensitivity and specificity) into account (20–23). The logit link function was used. The penalizedcomplexity prior framework was applied, whichresulted in more precise estimates (23). The contrastwas chosen at p ¼ 0.05 (sigma >3), which corre-sponded to sensitivities or specificities within an in-terval of 0.5 to 0.95, with a 95% probability (22). Post-test probabilities per imaging technique were calcu-lated based on various pre-test probabilities and thepooled LRs. Subgroup analyses were performed toreveal potential performance differences between on-site FFRCT versus off-site FFRCT and dynamic CTPversus static CTP. For the subgroup analysis of indi-vidual FFRCT at vessel level, a graph was generatedthat displayed the sensitivity and specificity atdifferent FFRCT values. Youden’s index was used todetermine the optimal threshold (i.e., by identifica-tion of the threshold that maximizes the sum ofsensitivity plus specificity). In addition, the FFRCT
value was determined, at which sensitivity or speci-ficity was $90%. Agreement between invasive FFRand FFRCT values was considered when both testswere #0.80 or >0.80. All statistical analyses wereperformed with the statistical software R (version3.42, R Foundation for Statistical Computing, Vienna,Austria) and the package “meta4diag” (version 2.0.6,arXiv:1512.06220v2 [stat.AP]) and MedCalc (version18.5, Mariakerke, Belgium).
RESULTS
After removal of duplicates, the search retrieved 1,377potentially relevant articles. Full text review wasperformed in 150 articles that met our pre-definedinclusion criteria. Included studies were publishedbetween 2008 and 2017. From 54 studies (n ¼ 5,330),39 studies reported on CTA, 12 reported on CTP, 10assessed CTA and CTP, 6 reported on TAG, 4 reportedon CTA and TAG, 18 assessed FFRCT, and 3 reportedon CTA and FFRCT (Figure 1). The average weightedradiation exposure was 5.0 mSv for prospectivelygated CTA, 11.4 mSv for retrospectively gated CTA,and 6.9 mSv for stress CTP only (not including restCTA). Funnel plots did not reveal obvious publicationbias (Supplemental Figure 1). Study population char-acteristics, index test characteristics, and referencetest characteristics were retrieved and are listedin Supplemental Tables 2 to 4. Quality assessmentusing QUADAS-2 criteria showed that patient selec-tion specifically was a source of bias (Figure 2).
POOLED SENSITIVITY AND SPECIFICITY AT VESSEL
AND PATIENT LEVEL. At vessel level, pooled sensi-tivity was the best for CTA (0.87), followed by FFRCT
(0.85), CTA and CTP (0.82), CTP (0.81), CTA andFFRCT (0.76), CTA and TAG (0.70), and finally TAG(0.59). The highest pooled specificity was reached byCTA and TAG (0.92), followed by CTA and CTP (0.88),CTP (0.86), CTA and FFRCT (0.80), FFRCT (0.78), TAG(0.77), and CTA (0.61). More detailed diagnostic per-formances are listed in Table 1 and SupplementalFigure 2. The subanalysis of on-site (11 studies) versusoff-site (7 studies) FFRCT on vessel level revealedno substantial differences between the sensitivity(0.84 vs. 0.85) and specificity (0.80 vs. 0.73, respec-tively) of the 2 techniques (Supplemental Figure 3).The second subanalysis on dynamic CTP (7 studies)versus static CTP (5 studies) showed that dynamicCTP had higher sensitivity (0.85 vs. 0.72) but lowerspecificity (0.81 vs. 0.90) compared with static CTP(Supplemental Figure 4).
At patient level, pooled sensitivity was the best forCTA (0.94), followed by FFRCT (0.89), CTA and CTP(0.89), CTP (0.83), and TAG (0.69). The highest

FIGURE 1 Flowchart of Selection of the Included Studies
Potentially relevant articles identified throughPubMed (n = 404), Embase (n = 739) and Web
of Science (n = 976)
Studies reviewed for title and abstract(n = 1377)
Articles reviewed for full text (n = 150)
Studies included in the meta-analysis (n = 54)
CTA(n = 39)
CTP(n = 12)
CTA and CTP(n = 10)
TAG(n = 6)
CTA and TAG(n = 4)
FFRCT(n = 18)
CTA and FFRCT(n = 3)
Duplicates excluded (n = 742)
Studies excluded (n = 96)- No FFR as reference standard (n = 32)- Overlapping patient population (n = 23)- Animal study (n = 1)- Case report (n = 3)- Conference abstract (n = 16)- Review (n = 2)- Subgroup/not in domain (n = 19)
Studies excluded on basis of abstract(n = 1228)
Studies included based on referencecheck (n = 1)
Flowchart of selection of the included studies. CTA ¼ computed tomography angiography; CTP ¼ computed tomography perfusion; FFRCT ¼fractional flow reserve computed tomography; TAG ¼ transluminal attenuation gradient.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Celeng et al.J U L Y 2 0 1 9 : 1 3 1 6 – 2 5 Functional CT for Diagnosing CAD
1319
pooled specificity was reached by CTA and CTP (0.81),followed by CTP (0.79), FFRCT (0.76), CTA (0.48), andTAG (0.39). More detailed diagnostic performancesare listed in Table 2 and Supplemental Figure 5.
FIGURE 2 Quality of the Included Studies Assessed by QUADAS-2
Patient Selection
Index Test
Reference Standard
Flow and Timing
0% 25%
69%
56%
33% 6%
Low Bias
The chart illustrates that patient selection specifically is a potential sou
Studies.
POOLED DIAGNOSTIC ACCURACY. The SROC atvessel level demonstrated superior diagnostic accu-racy for CTP, FFRCT, and CTA in combination withCTP, compared with CTA. CTA in combination with
50%
61%
13%
28%
89%
19%
17%
11%
75% 100%
Unclear High Bias
rce of bias. QUADAS ¼ Quality Assessment of Diagnostic Accuracy

TABLE 2
Imaging M
CTA
CTP
CTA and C
FFRCT
CTA and F
TAG
CTA and T
Abbreviatio
TABLE 1 Outcome Summary Per Vessel
Imaging ModalityNumber ofVessels
Sensitivity (%)(95% CI)
Specificity (%)(95% CI) þLR (95% CI) �LR (95% CI)
LogDOR(95% CI)
CTA 6,400 0.87 (0.84–0.91) 0.61 (0.54–0.68) 2.27 (1.87–2.76) 0.21 (0.15–0.27) 2.40 (2.00–2.80)
CTP 2,118 0.81 (0.72–0.88) 0.86 (0.76–0.93) 6.28 (3.17–11.91) 0.23 (0.13–0.34) 3.29 (2.43–4.22)
CTA and CTP 1,785 0.82 (0.76–0.87) 0.88 (0.81–0.92) 6.97 (4.29–11.39) 0.21 (0.13–0.30) 3.49 (2.81–4.24)
FFRCT 2,432 0.85 (0.82–0.87) 0.78 (0.72–0.83) 3.86 (2.91–5.22) 0.20 (0.16–0.24) 2.97 (2.56–3.41)
CTA and FFRCT 362 0.76 (0.50–0.93) 0.80 (0.69–0.88) 4.00 (1.85–7.05) 0.31 (0.08–0.69) 2.64 (1.09–4.23)
TAG 726 0.59 (0.46–0.72) 0.77 (0.61–0.89) 2.89 (1.41–5.98) 0.53 (0.33–0.76) 1.64 (0.64–2.70)
CTA and TAG 327 0.70 (0.46–0.87) 0.92 (0.77–0.99) 15.98 (2.63–59.63) 0.33 (0.12–0.63) 3.56 (1.75–5.53)
CI ¼ confidence interval; CTA ¼ computed tomography angiography; CTP ¼ computed tomography perfusion; FFRCT ¼ fractional flow reserve CT; LogDOR ¼ log diagnostic odds ratio; þLR ¼positive likelihood ratio; �LR ¼ negative likelihood ratio; TAG ¼ transluminal attenuation gradient.
Celeng et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Functional CT for Diagnosing CAD J U L Y 2 0 1 9 : 1 3 1 6 – 2 5
1320
FFRCT, TAG, and CTA in combination with TAG wereassociated with wide confidence intervals due to thelimited number of studies; hence, the true diagnosticperformance was indeterminate (Figure 3A). In linewith these findings, a large change in post-testprobability was observed for functional CT over CTAalone, whereas TAG alone demonstrated only amodest change in post-test probability (Figure 4).Specifically, at a pre-test probability of 30%, in case ofa negative test, post-test probabilities were between8% and 11% for CTA, CTP, FFRCT, and the combina-tion of CTA and CTP as well as CTA and FFRCT. In caseof a positive result, CTA yielded a post-test proba-bility of 49%, whereas CTP achieved 73% and FFRCT
achieved 62%. On a patient level, the SROCs showedsimilar good diagnostic performance for CTP, CTA incombination with CTP, and FFRCT compared withCTA (Figure 3B). TAG had a lower diagnostic perfor-mance than CTA, with wide confidence intervals.
DIAGNOSTIC ACCURACY OF INDIVIDUAL FFRCT AT
VESSEL LEVEL. We extracted data on 1,370 vesselsfrom 14 studies (Supplemental Table 4) and found anoptimal FFRCT threshold of #0.80 using the Youdenindex, which resulted in an area under the curve of0.87, with a sensitivity of 84% (95% CI: 81% to 87%)and a specificity of 77% (95% CI: 74% to 80%). Using
Outcome Summary Per-Patient
odality NSensitivity (%)
(95% CI)Specificity (%)
(95% CI)
3,101 0.94 (0.91–0.97) 0.48 (0.37–0.59)
697 0.83 (0.71–0.92) 0.79 (0.68–0.87)
TP 619 0.89 (0.78–0.96) 0.81 (0.73–0.90)
1,069 0.89 (0.85–0.92) 0.76 (0.69–0.82)
FRCT NA NA NA
188 0.69 (0.22–0.97) 0.39 (0.07–0.82)
AG NA NA NA
ns as in Table 1.
pre-determined thresholds, we observed $90%sensitivity at a FFRCT value of >0.82 and $90%specificity at a FFRCT value of #0.74 (Figure 5A). Invessels with FFRCT values between 0.74 and 0.82,diagnostic agreement with invasive FFR was weak(54% in 316 vessels), whereas diagnostic agreementfor FFRCT values outside of this range was high (87%in 1,054 vessels). The distribution of the data alsopresented as the frequency of invasive FFR at adifferent FFRCT value (Figure 5B). The agreementbetween invasive FFR and FFRCT is displayed inFigure 5C.
DISCUSSION
This meta-analysis demonstrated the additionalvalue of functional CT over anatomic CTA alone forthe assessment of hemodynamically significantCAD. The main results of this investigation can besummarized as follows. 1) In line with previousobservations, CTA showed excellent sensitivity;however, it had limited specificity both on vessel andpatient levels. 2) Regarding the functional CT imagingtechniques, CTP and FFRCT yielded high to excellentsensitivity. Interestingly, the specificity of both theseimaging techniques, especially CTP, was high.
þLR (95% CI) �LR (95% CI)LogDOR(95% CI)
1.85 (1.48–2.36) 0.12 (0.06–0.19) 2.78 (2.13–3.51)
4.10 (2.46–7.01) 0.22 (0.09–0.40) 2.97 (1.98–4.02)
4.75 (3.16–6.99) 0.14 (0.04–0.30) 3.59 (2.54–4.78)
3.76 (2.76–5.21) 0.15 (0.10–0.21) 3.25 (2.70–3.84)
NA NA NA
1.55 (0.32–4.72) 1.36 (0.07–5.42) 0.45 (�2.70–3.61)
NA NA NA

FIGURE 3 SROC at Vessel and Patient Levels
CTA CTP CTA and CTP FFRCT
CTA and FFRCT TAG CTA and TAG
CTA CTP CTA and CTP FFRCT TAG
A
B
SROC
SROC
1−Specificity
Sens
itivi
ty
0 0.2 0.4 0.6 0.8 1
0
0.2
0.4
0.6
0.8
1
Sens
itivi
ty
0
0.2
0.4
0.6
0.8
1
1−Specificity0 0.2 0.4 0.6 0.8 1
Summary receiver-operating characteristic curve (SROC) at (A) vessel level and (B)
patient level. Each symbol represents an imaging modality and the corresponding circle
around the confidence intervals, except for CTA and FFRCT at vessel level and TAG at
patient level due to limited data points. Abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Celeng et al.J U L Y 2 0 1 9 : 1 3 1 6 – 2 5 Functional CT for Diagnosing CAD
1321
Evidence for TAG was limited and showed moderatesensitivity on both levels, whereas its specificityshowed substantial differences in performance atvessel and patient levels (0.77 vs. 0.39). Also, dis-crepancies in TAG could be dependent on the acqui-sition technique and scanner hardware, which mighthave resulted in differences in coronary contrastconcentrations and thus, could also have influencedTAG results (24). 3) With the combination of CTA andCTP as well as CTA and FFRCT, vessel-level sensitivityremained high, whereas CTA and TAG showed mod-erate sensitivity. The specificity of all the combinedtechniques was high to excellent. 4) Regarding thediagnostic accuracy on both vessel- and patient-levelall CT functional imaging techniques except TAGshowed better performance than CTA alone; however,on vessel-level the combination of CTA and FFRCT
as well as CTA and TAG showed wide confidenceintervals. Therefore, their true diagnostic accuracywas unclear. 5) Concerning the changes in the diag-nostic probability, at a pre-test probability of 30%, anegative test resulted in post-test probabilities of 8%to 11% for CTA, CTP, FFRCT, and the combination ofCTA and CTP as well as CTA and FFRCT. Hence, anegative test decreased the absolute probability ofdisease by w20%, although no improvement wasobserved over CTA alone. In cases of a positive result,CTA yielded a post-test probability of 49%, whereasCTP achieved 73% and FFRCT achieved 62%; thus,these techniques more accurately identified hemo-dynamically significant CAD. This meta-analysisdemonstrated that the use of functional CT imagingtechniques might aid the clinical management ofpatients with suspected or known CAD.
ADVANTAGES AND LIMITATIONS OF CTP. A previ-ous meta-analysis demonstrated that the perfor-mance of CTP was similar to MRI and positronemission tomography for the detection of hemody-namically significant CAD (25). In the present study,which included twice the number of vessels, weshowed that CTP yielded the same specificity. Despitethese advantages, the integration of CTP into clinicalworkflow is limited. A possible limitation, whichmight hamper the use of CTP, is the complexity of theimaging procedure. Currently, there are 3 acquisitionmethods for the detection and evaluation ofmyocardial perfusion defects: static single energy(myocardial contrast enhancement is obtained at theearly arterial phase); static dual energy (iodine ma-terial distribution map is created by using dual-energy acquisition); and dynamic CTP (myocardialcontrast enhancement is acquired several times dur-ing the first-pass) (26). The subanalysis of dynamic

FIGURE 4 Absolute Change in Post-Test Probability for the Various CT Techniques
Pre-Test Probability
Post
-Tes
t Pro
babi
lity
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
CTACTPCTA and CTP
TAG
Reference lineCTA and TAG
FFRCT
CTA and FFRCT
Absolute change in post-test probability of hemodynamically significant coronary artery disease by various pre-test probabilities. The
reference line shows no effect of the test on post-test probability. A large change in post-test probability was observed for functional CT over
CTA alone, whereas TAG alone demonstrated only a modest change in post-test probability. Abbreviations as in Figure 1.
Celeng et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Functional CT for Diagnosing CAD J U L Y 2 0 1 9 : 1 3 1 6 – 2 5
1322
CTP versus static CTP demonstrated that the sensi-tivity of dynamic CTP was higher, but its specificitywas lower than that of static CTP. Both static anddynamic CTP can be performed during rest and/orstress.
Based on our findings, most institutions use astress perfusion protocol with dynamic acquisition(53%) to improve the detection of perfusion defects(27,28). In terms of radiation exposure, static restCTP—in line with coronary CTA—requires a single-snapshot for the detection of contrast attenuationand is therefore associated with a lower radiationdose. We found that the weighted radiation exposureof stress CTP plus rest CTA leads to substantiallyhigher radiation (11.9 mSv) compared with that ofprospectively electrocardiographically triggered CTAalone (5.0 mSv). With use of low-kilovolt protocols,dynamic CTP is feasible at a lower radiation dose(29,30). Nevertheless, radiation exposure should belimited whenever feasible, and this might entail apreference for FFRCT.
ADDED VALUE OF FFRCT. Our meta-analysis showedthat the diagnostic performance of FFRCT was similar
to that of CTP; moreover, it did not require additionalradiation nor the administration of adenosine.Furthermore, it allows to estimate functional changesin coronary artery flow after stent implantation (31).Recently, Cook et al. (17) performed a systematic re-view, in which they included 5 FFRCT studies anddigitized plots to acquire individual correlations ofFFRCT and invasive FFR values. They concluded thatFFRCT around the cutpoint of 0.80 showed less cer-tainty, and that FFRCT values of >0.90 and #0.60provided almost complete certainty. In our meta-analysis, we performed a similar subanalysis on alarger number of vessels (1,370 vs. 908) and observedgood agreement with invasive FFR for FFRCT values>0.82 and #0.74. Of note, when evaluating valuesclose to a threshold (i.e., intermediate values), loweragreement will be observed, which is also true forrepeated measures of invasive FFR itself (32). Somediscrepancy between modeling and directlymeasured FFR is expected to be present, althoughwith advanced FFRCT algorithms, the use of machinelearning, and improvements in CT hardware, thisdiscrepancy is expected to decrease (33,34). Heart-Flow (Redwood City, California) FFRCT analysis was

FIGURE 5 Individual FFRCT Values
0
50
FFRCT
≤0.30
0.30-035
0.35-0.40
0.40-0.45
0.45-0.50
0.50-0.55
0.55-0.60
0.60-0.65
0.65-0.70
0.70-0
.75
0.75-0
.80
0.80-0.85
0.85-0.90
0.90-0.95
0.95-1.00
100
150
200
250
Freq
uenc
y
B
0
10
20
30
40
50
60
70
80
90
100
Compared to Invasive FFR
0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0FFRCT
(%)
Specificity
Sensitivity
A
40
50
60
70
80
90
100
0.3 0.4 0.5 0.6 0.7 0.8 1.00Average Between Invasive FFR and FFRCT
Agre
emen
t (%
)
0.9
C
(A) Sensitivity and specificity (with 95% confidence intervals) at different FFRCT values.
(B) The frequency of invasive FFR #0.80 (orange) and invasive FFR >0.80 (green) at
different FFRCT values. The dotted line represents the moving average trendline. (C) Per-
range agreement by plotting agreement against the average of invasive FFR and FFRCT
value. Abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Celeng et al.J U L Y 2 0 1 9 : 1 3 1 6 – 2 5 Functional CT for Diagnosing CAD
1323
the first commercially available software that wasable to compute a CT-derived FFR value. In recentyears, various vendors developed other FFRCT plat-forms. When using HeartFlow, CTA data are trans-mitted to an off-site location and are analyzed by anindependent laboratory. In case of on-site assess-ment, FFRCT data are analyzed at the local institution.Within the frame of this meta-analysis, we performeda subanalysis to determine the diagnostic accuracy ofoff-site FFRCT versus on-site FFRCT. Our results indi-cated that the performance of on-site FFRCT algo-rithms was as high as that of off-site FFRCT. Of note,on-site FFRCT post-processing might be desirablebecause it allows the physician to access functionaldata in a more timely manner. Nevertheless, mostFFRCT algorithms are proprietary, and the exactmechanism remains unclear.
COSTS ATTRIBUTABLE TO FUNCTIONAL CT IMAGING.
Because health care costs of noninvasive versusinvasive imaging are substantially different, severalstudies aimed to assess the cost-effectiveness ofnovel noninvasive imaging techniques for identifi-cation of patients with significant CAD. The clinicaland economic outcomes of FFRCT versus usual carewere investigated within the framework of 3comprehensive trials (DISCOVER-FLOW [Diagnosis ofISChemia-Causing Stenoses Obtained Via Noninva-sivE FRactional FLOW Reserve], HeartFlowNXT[HeartFlow analysis of coronary blood flow using CTangiography: NeXt sTeps] and PLATFORM [Prospec-tive LongitudinAl Trial of FFRct: Outcome andResource IMpacts]) (35–37). Beyond improved orequivalent clinical outcome (12% to 19% fewerevents at 1 year), the use of FFRCT resulted inreduced costs (30% to 33% lower) by more accuratelyidentifying patients for revascularization. Based onthese promising results, HeartFlow Inc. receivedFood and Drug Administration clearance inNovember 2014. In the United Kingdom, a studydemonstrated that the integration of HeartFlowFFRCT as a diagnostic strategy for stable chest painresulted in cost savings of £200 per patient (38),which led the National Institute for Health and CareExcellence to recommend the adoption of HeartFlowFFRCT into current practice (39). The National Insti-tute for Health and Care Excellence consideredHeartFlow FFRCT cost-effective at a list price of £700(excluding VAT) per analysis compared with thecurrent treatment pathway of all functional imagingtests, which includes single-photon emissioncomputed tomography, MRI, and echocardiography.In case of TAG, no studies were reported on theadditional cost of TAG software, because the analysis
can be performed on-site using a dedicated work-station, thus the costs are expected to be limited.The cost-effectiveness of CTP was evaluated only in1 study, which reported lower costs and an addi-tional gain in quality-adjusted life years when using

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE 1:
Current clinical guidelines do not encompass the
application of functional CT imaging techniques for
the detection of hemodynamically relevant ischemia in
patients with stable CAD.
COMPETENCY IN MEDICAL KNOWLEDGE 2: CTP
and FFRCT provide improved diagnostic accuracy
compared with coronary CTA alone, which has high
sensitivity but moderate specificity.
COMPETENCY IN PATIENT CARE AND PROCE-
DURAL SKILLS: Both functional CT imaging tech-
niques might refine the critical pathway of patients to
invasive catheterization.
COMPETENCY IN INTERPERSONAL AND
COMMUNICATION SKILLS: It is relevant to
assemble robust evidence to clarify the role of func-
tional CT techniques and to discuss the available op-
tions with patients who will undergo coronary CTA.
TRANSLATIONAL OUTLOOK: Further clinical trials
using sophisticated imaging protocols and machine-
learning algorithms are needed to validate the novel
functional CT tests in the clinical setting and to further
refine the probability of potential outcomes of pa-
tients with CAD.
Celeng et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Functional CT for Diagnosing CAD J U L Y 2 0 1 9 : 1 3 1 6 – 2 5
1324
dual-energy CT compared with single-photon emis-sion computed tomography (40).
STUDY LIMITATIONS. The results of our meta-analysis need to be considered in the context of theincluded studies, which were mainly performed atexpert centers and limited in number for some mo-dalities. CT radiation exposure was not reported in allincluded studies. Verification bias was an importantlimitation, which occurred when studies only per-formed the reference standard in those with a posi-tive initial test. This might result in a high pre-testprobability, which could increase the specificity of agiven imaging modality. Another limitation was theheterogeneity among studies (including differencesin diagnostic criteria), which might have influencedthe reported summary values of the different imagingmodalities. Finally, we were not able to obtain indi-vidual FFRCT values from all studies, including theNXT trial (41), because only 312 individual pointscould be identified in the Bland-Altman plot of the484 vessels included in the study. For the DeFACTO(Determination of Fractional Flow Reserve byAnatomic Computed Tomographic AngiOgraphy)data, a substudy (42) was used in which 150 vessels(407 in total in the original study population) of in-termediate stenosis on CTA were evaluated.
CONCLUSIONS
This meta-analysis indicated that despite recentdevelopments in CT hardware, the specificity ofCTA remains moderate for the detection of hemo-dynamically significant stenosis. The specificity offunctional CT imaging tests and their combined usewith CTA was high to excellent, except for TAG,which showed discrepancies in specificity on vesseland patient levels. CTP, FFRCT, and its combineduse with CTA yielded higher diagnostic performancethan CTA alone. The diagnostic performance ofindividual FFRCT at vessel level was good, witha relative narrow area of uncertainty aroundthe threshold of 0.80. CTP and FFRCT both havethe potential to improve identification of patients
with hemodynamically significant CAD at reducedhealth costs, therefore, their integration intothe routine clinical workflow is recommended. Dueto limited evidence the exact role of TAG isuncertain.
ADDRESS FOR CORRESPONDENCE: Dr. Csilla Celeng,Department of Radiology, University Medical CenterUtrecht, Heidelberglaan 100, 3584 CX Utrecht, theNetherlands. E-mail: [email protected].
RE F E RENCE S
1. Miller JM, Rochitte CE, Dewey M, et al.Diagnostic performance of coronary angiog-raphy by 64-row CT. N Engl J Med 2008;359:2324–36.
2. Vanhoenacker PK, Heijenbrok-Kal MH, VanHeste R, et al. Diagnostic performance of multi-detector CT angiography for assessment of
coronary artery disease: meta-analysis. Radiology2007;244:419–28.
3. Budoff MJ, Dowe D, Jollis JG, et al.Diagnostic performance of 64-multidetector rowcoronary computed tomographic angiography forevaluation of coronary artery stenosis in in-dividuals without known coronary artery disease:
results from the prospective multicenter ACCU-RACY (Assessment by Coronary Computed Tomo-graphic Angiography of Individuals UndergoingInvasive Coronary Angiography) trial. J Am CollCardiol 2008;52:1724–32.
4. Budoff MJ, Nakazato R, Mancini GB, et al. CTangiography for the prediction of hemodynamic

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Celeng et al.J U L Y 2 0 1 9 : 1 3 1 6 – 2 5 Functional CT for Diagnosing CAD
1325
significance in intermediate and severe lesions:head-to-head comparison with quantitative coro-nary angiography using fractional flow reserve asthe reference standard. J Am Coll Cardiol Img2016;9:559–64.
5. Rossi A, Papadopoulou SL, Pugliese F, et al.Quantitative computed tomographic coronaryangiography: does it predict functionally signifi-cant coronary stenoses? Circ Cardiovasc Imaging2014;7:43–51.
6. Pijls NH, De Bruyne B, Peels K, et al. Measure-ment of fractional flow reserve to assess thefunctional severity of coronary-artery stenoses.N Engl J Med 1996;334:1703–8.
7. De Bruyne B, Sarma J. Fractional flow reserve: areview: invasive imaging. Heart 2008;94:949–59.
8. Jeremias A, Kirtane AJ, Stone GW. A test incontext: fractional flow reserve: accuracy, prog-nostic implications, and limitations. J Am CollCardiol 2017;69:2748–58.
9. Tonino PA, De Bruyne B, Pijls NH, et al. Frac-tional flow reserve versus angiography for guidingpercutaneous coronary intervention. N Engl J Med2009;360:213–24.
10. De Bruyne B, Pijls NH, Kalesan B, et al. Frac-tional flow reserve-guided PCI versus medicaltherapy in stable coronary disease. N Engl J Med2012;367:991–1001.
11. Lubbers M, Coenen A, Kofflard M, et al.Comprehensive cardiac CT with myocardial perfu-sion imaging versus functional testing in sus-pected coronary artery disease: the multicenter,randomized CRESCENT-II trial. J Am Coll CardiolImg 2018;11:1625–36.
12. Grunau GL, Min JK, Leipsic J. Modeling offractional flow reserve based on coronary CTangiography. Curr Cardiol Rep 2013;15:336.
13. Choi JH, Min JK, Labounty TM, et al. Intra-coronary transluminal attenuation gradient incoronary CT angiography for determining coronaryartery stenosis. J Am Coll Cardiol Img 2011;4:1149–57.
14. Choi JH, Koo BK, Yoon YE, et al. Diagnosticperformance of intracoronary gradient-basedmethods by coronary computed tomographyangiography for the evaluation of physiologicallysignificant coronary artery stenoses: a validationstudy with fractional flow reserve. Eur Heart JCardiovasc Imaging 2012;13:1001–7.
15. Lu MT, Ferencik M, Roberts RS, et al. Nonin-vasive FFR derived from coronary CT angiography:management and outcomes in the PROMISE trial.J Am Coll Cardiol Img 2017;10:1350–8.
16. Liberati A, Altman DG, Tetzlaff J, et al. ThePRISMA statement for reporting systematic re-views and meta-analyses of studies that evaluatehealthcare interventions: explanation and elabo-ration. BMJ 2009;339:b2700.
17. Cook CM, Petraco R, Shun-Shin MJ, et al.Diagnostic accuracy of computed tomography-derived fractional flow reserve: a systematic re-view. JAMA Cardiol 2017;2:803–10.
18. Whiting PF, Rutjes AW, Westwood ME, et al.QUADAS-2: a revised tool for the quality assess-ment of diagnostic accuracy studies. Ann InternMedicine 2011;155:529–36.
19. Leeflang MM. Systematic reviews and meta-analyses of diagnostic test accuracy. Clin Micro-biol Infect 2014;20:105–13.
20. Ma X, Chen Y, Cole SR, Chu H. A hybridBayesian hierarchical model combining cohort andcase-control studies for meta-analysis of diag-nostic tests: accounting for partial verificationbias. Stat Methods Med Res 2016;25:3015–37.
21. Chu H, Guo H, Zhou Y. Bivariate random effectsmeta-analysis of diagnostic studies using gener-alized linear mixed models. Med Decision Making2010;30:499–508.
22. Guo J, Riebler A, Rue H. Bayesian bivariatemeta-analysis of diagnostic test studies withinterpretable priors. Stat Med 2017;36:3039–58.
23. Menten J, Boelaert M, Lesaffre E. Bayesianmeta-analysis of diagnostic tests allowing forimperfect reference standards. Stat Med 2013;32:5398–413.
24. Stuijfzand WJ, Danad I, Raijmakers PG, et al.Additional value of transluminal attenuationgradient in CT angiography to predict hemody-namic significance of coronary artery stenosis.J Am Coll Cardiol Img 2014;7:374–86.
25. Takx RA, Blomberg BA, El Aidi H, et al. Diag-nostic accuracy of stress myocardial perfusionimaging compared to invasive coronary angiog-raphy with fractional flow reserve meta-analysis.Circ Cardiovasc Imaging 2015;8.
26. Varga-Szemes A, Meinel FG, De Cecco CN,Fuller SR, Bayer RR 2nd, Schoepf UJ. CT myocar-dial perfusion imaging. AJR Am J Roentgenol2015;204:487–97.
27. Gould KL, Lipscomb K. Effects of coronarystenoses on coronary flow reserve and resistance.Am J Cardiol 1974;34:48–55.
28. Ko SM, Park JH, Hwang HK, Song MG. Directcomparison of stress- and rest-dual-energycomputed tomography for detection of myocar-dial perfusion defect. Int J Cardiovasc Imaging2014;30 Suppl 1:41–53.
29. Fujita M, Kitagawa K, Ito T, et al. Dosereduction in dynamic CT stress myocardial perfu-sion imaging: comparison of 80-kV/370-mAs and100-kV/300-mAs protocols. Eur Radiol 2014;24:748–55.
30. Kim SM, Kim YN, Choe YH. Adenosine-stressdynamic myocardial perfusion imaging using 128-slice dual-source CT: optimization of the CT pro-tocol to reduce the radiation dose. Int J CardiovascImag 2013;29:875–84.
31. Kim KH, Doh JH, Koo BK, et al. A novelnoninvasive technology for treatment planningusing virtual coronary stenting and computedtomography-derived computed fractional flowreserve. J Am Coll Cardiol Intv 2014;7:72–8.
32. Petraco R, Sen S, Nijjer S, et al. Fractionalflow reserve-guided revascularization: practicalimplications of a diagnostic gray zone and
measurement variability on clinical decisions. J AmColl Cardiol Intv 2013;6:222–5.
33. Itu L, Rapaka S, Passerini T, et al. A machine-learning approach for computation of fractionalflow reserve from coronary computed tomogra-phy. J Appl Physiol (1985) 2016;121:42–52.
34. Zreik M, Lessmann N, van Hamersvelt RW,et al. Deep learning analysis of the myocar-dium in coronary CT angiography for identifi-cation of patients with functionally significantcoronary artery stenosis. Med Image Anal 2017;44:72–85.
35. Hlatky MA, Saxena A, Koo BK, Erglis A,Zarins CK, Min JK. Projected costs and conse-quences of computed tomography-determinedfractional flow reserve. Clin Cardiol 2013;36:743–8.
36. Kimura T, Shiomi H, Kuribayashi S, et al. Costanalysis of non-invasive fractional flow reservederived from coronary computed tomographicangiography in Japan. Cardiovasc Interv Ther2015;30:38–44.
37. Douglas PS, De Bruyne B, Pontone G, et al. 1-Year Outcomes of FFRCT-guided care in patientswith suspected coronary disease: the PLATFORMstudy. J Am Coll Cardiol 2016;68:435–45.
38. Rajani R, Webb J, Marciniak A, Preston R.Comparative efficacy testing - fractional flowreserve by coronary computed tomography for theevaluation of patients with stable chest pain. Int JCardiol 2015;183:173–7.
39. National Institute for Health and Care Excel-lence. HeartFlow FFRCT for estimating fractionalflow reserve from coronary CT angiography.Available at: nice.org.uk/guidance/mtg32. AccessedSeptember 2, 2017.
40. Meyer M, Nance JW Jr., Schoepf UJ, et al.Cost-effectiveness of substituting dual-energy CTfor SPECT in the assessment of myocardialperfusion for the workup of coronary artery dis-ease. Eur J Radiol 2012;81:3719–25.
41. Norgaard BL, Leipsic J, Gaur S, et al. Diagnosticperformance of noninvasive fractional flowreserve derived from coronary computed tomog-raphy angiography in suspected coronary arterydisease: the NXT trial (Analysis of Coronary BloodFlow Using CT Angiography: Next Steps). J AmColl Cardiol 2014;63:1145–55.
42. Nakazato R, Park HB, Berman DS, et al.Noninvasive fractional flow reserve derived fromcomputed tomography angiography for coronarylesions of intermediate stenosis severity: resultsfrom the DeFACTO study. Circ Cardiovasc Imaging2013;6:881–9.
KEY WORDS coronary artery disease,computed tomography, fractional flowreserve, meta-analysis, myocardial perfusionimaging
APPENDIX For supplemental tables andfigures, please see the online version of thispaper.

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E A M E R I C A N
C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
EDITORIAL COMMENT
A New Decade of Old Questions
Steps Toward Demonstrating the Efficacy ofPhysiologic CAD Evaluation by CT*James K. Min, MD,a Farouc A. Jaffer, MD PHDb
A t the time of its introduction in 2005, coro-nary computed tomography angiography(CCTA) of $64 detector rows was broadly
evaluated in single and, subsequently, multicenterclinical trials for its diagnostic performance againstan invasive coronary angiography (ICA) referencestandard (1). The majority of these studies observedsimilar results, with CCTA exhibiting very high sensi-tivities and generally moderate specificities for iden-tification and exclusion of a $50% luminal diameterstenosis by ICA. Despite its similar specificity to stressimaging tests, such as those performed with single-photon emission computed tomography or stressechocardiography, CCTA was and is still consideredby many to be a method that excels at exclusion ofhigh-grade coronary stenosis, but not a method thatexcels at its specific and reliable identification.
Even though proponents of CCTA contended thatthe performance measures were sufficient to justifyits routine use in clinical care based on its negativepredictive value, large-scale clinical outcomes trialswith CCTA-guided strategies were lacking, and priorrandomized controlled trials such as COURAGE(Clinical Outcomes Utilizing Revascularization andAggressive Drug Evaluation) and BARI2D (Bypass
ISSN 1936-878X/$36.00
*Editorials published in JACC: Cardiovascular Imaging reflect the views of
the authors and do not necessarily represent the views of iJACC or the
American College of Cardiology.
From the aDepartment of Radiology and Medicine, Dalio Institute of
Cardiovascular Imaging, Weill Cornell Medical College and the New
York-Presbyterian Hospital, New York, New York; and the bDepartment
of Medicine, Massachusetts General Hospital and Harvard Medical
School, Boston, Massachusetts. Dr. Min has served on the advisory
boards for GE Healthcare and Arineta; has received research support
from GE Healthcare, the Dalio Foundation, and the National Institutes
of Health; and has equity interest in Cleerly. Dr. Jaffer has received
research grants from Canon and Siemens; served as a consultant to
Boston Scientific, Abbott Vascular, Siemens, and Philips; and owns
intellectual property related to intravascular imaging, with rights held
by Massachusetts General Hospital.
Angioplasty Revascularization Investigation in Type 2Diabetes) that used ICA stenosis to guide clinical de-cision making for revascularization did not observeimproved mortality with revascularization (2–4).Furthermore, given the traditional approach toemploy stress testing to guide physiologic-basedtreatment decisions of revascularization and medi-cal therapy for coronary artery disease (CAD), dis-cussion ensued as to which was the noninvasive“superior” approach for CAD assessment—CCTA orstress imaging. This disagreement and equipoiseamong the scientific community set the stage for theperformance of 2 large-scale multisite randomizedcontrolled trials assessing the performance of CCTA:PROMISE (Prospective Multicenter Imaging Study forEvaluation of Chest Pain) (n ¼ 10,003) and SCOT-HEART (Scottish Computed Tomography of theHeart) (n ¼ 4,146) (5,6). In PROMISE, CCTA was testedagainst any method of functional stress testing,and no differences were observed in major adversecardiac events between groups at a 25-monthfollow-up. In contrast, SCOT-HEART evaluated pa-tients undergoing a standard of care that often butnot always included stress electrocardiographictesting versus that standard plus CCTA. At a 1.7-yearfollow-up, the CCTA group experienced a near sig-nificant 38% reduction in fatal and nonfatal myocar-dial infarction (p ¼ 0.0527) that increased to asignificant 50% reduction at 3 years (p ¼ 0.02) (7).Germane to the latter study, the rates of ICA weresimilar among randomized groups, with no significantdifferences in coronary revascularization rates.Rather, the most notable difference between theCCTA and non-CCTA arm that appeared to drive thebenefit in the CCTA arm was a 4-fold increased use ofCAD preventive medical therapies in patients thatunderwent CCTA.
Since these seminal publications, the field of CCTAhas evolved additional tools that now enable physi-ologic evaluation of CAD beyond anatomical CCTA
https://doi.org/10.1016/j.jcmg.2018.08.002

SEE PAGE 1316
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Min and JafferJ U L Y 2 0 1 9 : 1 3 2 6 – 9 Editorial Comment
1327
detail, including vasodilator-mediated stress testingby computed tomography perfusion (CTP) by static,dual energy, or dynamic approaches; modelingof hyperemia for computation of fractional flowreserve from computed tomography (FFRCT) throughcomputational fluid dynamics; and quantification ofthe contrast opacity before and after a stenosis at aresting state to further understand the hemodynamicsignificance of a particular coronary lesion (trans-luminal attenuation gradient [TAG]) (8).
Each of these methods, as well as the differentapproaches within each method, differs significantly,and have important advantages and limitations. 1)CTP by static methods is subject to the same limita-tions as perfusion assessed by single-photon emissioncomputed tomography, in that it is a relative tech-nique that may be subject to false negative results inthe setting of balanced ischemia (9,10). Dual energyCTP suffers from higher radiation doses if performedin the projection domain, whereas dual energycomputed tomography in the image domain does notoffer the ability to perform actual material decom-position. Dynamic CTP offers an understanding ofabsolute blood flow at the myocardial level, but maybe associated with higher radiation exposure. 2)FFRCT aims to evaluate decrements in hyperemiccoronary pressure across a given coronary lesion and,in this regard, does not allow for determination of theeffects of a coronary lesion on myocardial blood flow.Two computational fluid dynamic methods currentlyexist that enable estimation of FFR by CT, including asoftware-as-a-service method that employs 3-dimen-sional modeling and on-site solutions that usereduced order computational fluid dynamic methodsto allow for calculations to be achievable on a tradi-tional standalone computer (11). One major limitationto both of these approaches is their reliance solely onthe luminal geometry, which alone is insufficient toreliably determine the lesion-causing nature of acoronary stenosis. 3) TAG contrasts with both CTPand FFRCT in that it can be performed on a restingCCTA and is represented by a linear regression coef-ficient between the opacification and axial distance ofany given location within a coronary artery. Earlystudies have demonstrated a positive relationshipof TAG to high-grade coronary stenosis, whichrepresented a surrogate of coronary ischemia, withlimited subsequent studies observing a similar rela-tionship to hyperemia-induced FFR (12,13). Notably,the capability of assessing resting differencesin coronary flow across the entire cardiac cycle inintermediate stenoses is generally antithetical toobservations in pre-clinical and clinical models that
demonstrate that resting flow disturbances occuronly in severe stenoses.
In this issue of iJACC, Celeng et al. (14) report asummary meta-analysis of these techniques—bothalone as well as in combination with CCTA—todiagnose ischemia. This well-performed study eval-uated 54 studies, wherein 5,330 patients wereincluded with a focus on per-vessel performanceagainst an invasive FFR reference standard. For anyphysiologic measure alone, CTP was demonstrated toexhibit the highest accuracy and specificity (86%) andwas superior to TAG and FFRCT, which performednearly identically (77% and 78%, respectively). Thesefindings were similar on a per-patient level, with CTPdemonstrating the highest specificity (79%) comparedwith TAG (39%) and FFRCT (76%). Interestingly, theaddition of CCTA information yielded mild improve-ments to CTP (sensitivity 81% to >82%, specificity86% to >88%), whereas this addition of CCTA infor-mation to FFRCT reduced its sensitivity (85% to 76%)and increased its specificity (78% to 80%). Comparedwith static CTP methods, dynamic CTP demonstratedhigher sensitivity (85% vs. 72%) with lower specificity(81% vs. 90%). For different methods of FFRCT, off-site versus on-site performed similarly (85% vs.84%). Importantly, the investigators also presentedan illustration of the high diagnostic performance ofFFRCT when the values are very low or very high, butmodest performance between the range of 0.74 and0.82 when the invasive FFR was in the intermediaterange.
Celeng et al. (14) should be commended for ananalysis that summarizes the current state of physio-logic CAD evaluation by CCTA and their study, as mosthigh-quality studies do, evoke numerous additionalquestions. This meta-analysis emphasizes what wecurrently know about physiologic CAD evaluation byCCTA but, more importantly, emphasizes how early onwe are in fully understanding the potential of CCTAand its associated tools for physiologic CAD evalua-tion, as has been described by Celeng et al. (14).Recently, novel methods of computing FFR usingdeep neural networks andmachine learning have beendeveloped to calculate FFR from CT using coronaryluminal topographies and geometries for calculationof FFR (15,16). Beyond the use of luminal measuresalone, Dey et al. (17) have integrated the entirety ofcoronary luminal and atherosclerotic plaque featuresconsidering plaque burden, composition, and locationwith outputs of coronary vessel ischemia determinedby a machine learning algorithm.

Min and Jaffer J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 3 2 6 – 9
1328
In their seminal paper, Fryback and Thornbury (18)describe a multistep process demonstrating theefficacy of diagnostic imaging wherein technicalevaluation and diagnostic accuracy—the current stateof physiologic CAD evaluation by CCTA—are followedby evaluation of the effect of the imaging test to in-fluence diagnostic work-up, patient management,and ultimately patient-centered and societal out-comes of improved event-free survival andcost-effectiveness. Based on this foundation, animportant question is whether it is possible to employthese techniques to assess the salutary effects ofmedical therapy; for example, for a symptomatic pa-tient with myocardial ischemia who is successfullytreated with antianginal medications, will the perfu-sion abnormalities on CTP normalize as they do withsuch techniques as single-photon emission computedtomography and positron emission tomography? Thesame question is important to understand for FFRCT,which by all methods relies on luminal geometryalone that is expectedly unaffected by medical ther-apy. Although seemingly poor performing for diag-nosis of ischemia, it is nevertheless curious whetherthe accuracy of TAG is affected in the setting ofreduced chronotropy, as might be expected for a pa-tient chronically treated with beta blockers.
For mainstream use of these techniques, however,clinical outcomes-based trials remain needed. Todate, no large-scale CT study has evaluated CADoutcomes when knowing both coronary “anatomy”and “physiology.” Though historical debate hasdefined these terms at a binary threshold of stenosisseverity or with the presence or absence of aperfusion abnormality, the present study data byCeleng et al. (14), as well as that related to athero-sclerosis information offered by CCTA, highlightthe oversimplification that comes from such
categorizations wherein “physiology” can representresting differences in contrast opacification, differ-ences in rest-stress myocardial perfusion, absolutemyocardial blood flow, or modeled differences inhyperemic pressure differences along a vessel. As thefield awaits the performance of well-performed clin-ical trials that address these issues, including thehighly awaited ISCHEMIA (International Study ofComparative Health Effectiveness With Medical andInvasive Approaches) trial (NCT01471522), whereinpatients with moderate-to-severe ischemia by stresstesting underwent CCTA, with one-half assigned tomedical therapy and the other one-half to medicaltherapy plus early invasive angiography with inten-ded revascularization. This study, though not usingCT alone to provide both anatomic and physiologicinformation, will nevertheless offer significant infor-mation gain as to the ideal approaches to CAD treat-ment in the setting of abnormal anatomy and/orphysiology. The field of CT would do well to considerthe ISCHEMIA trial as an example of high-qualityresearch based on patient-centered outcomes.Rather than simply identifying small differences inthe areas under receiver-operating characteristicscurve for discrimination of ischemia, assessment ofthese newer CCTA tools to guide therapy in a mannerthat improves clinical CAD outcomes and cost-effectiveness likely represents the next era ofresearch required to substantively advance the fieldof diagnostic imaging.
ADDRESS FOR CORRESPONDENCE: Dr. James K.Min, Dalio Institute of Cardiovascular Imaging, WeillCornell Medical College, 413 East 69th Street, Suite108, New York, New York 10021. E-mail: [email protected].
RE F E RENCE S
1. Marwick TH, Cho I, Ó Hartaigh B, Min JK. Findingthe gatekeeper to the cardiac catheterizationlaboratory: coronary CT angiography or stresstesting? J Am Coll Cardiol 2015;65:2747–56.
2. Sedlis SP, Hartigan PM, Teo KK, et al., for theCOURAGE Trial Investigators. Effect of PCI onlong-term survival in patients with stable ischemicheart disease. N Engl J Med 2015;373:1937–46.
3. Boden WE, O’Rourke RA, Teo KK, et al., for theCOURAGE Trial Research Group. Optimal medicaltherapy with or without PCI for stable coronarydisease. N Engl J Med 2007;356:1503–16.
4. BARI 2D Study Group, Frye RL, August P, et al.A randomized trial of therapies for type 2 diabetes
and coronary artery disease. N Engl J Med 2009;360:2503–15.
5. Douglas PS, Hoffmann U, Patel MR, et al., forthe PROMISE Investigators. Outcomes ofanatomical versus functional testing for coronaryartery disease. N Engl J Med 2015;372:1291–300.
6. SCOT-HEART Investigators. CT coronary angi-ography in patients with suspected angina due tocoronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet2015;385:2383–91.
7. Williams MC, Hunter A, Shah ASV, et al., for theSCOT-HEART Investigators. Use of coronarycomputed tomographic angiography to guide
management of patients with coronary disease.J Am Coll Cardiol 2016;67:1759–68.
8. Koo HJ, Yang DH, Kim YH, et al. CT-basedmyocardial ischemia evaluation: quantitativeangiography, transluminal attenuation gradient,myocardial perfusion, and CT-derived fractionalflow reserve. Int J Cardiovasc Imaging 2016;32Suppl 1:1–19.
9. Danad I, Szymonifka J, Schulman-Marcus J,Min JK. Static and dynamic assessment ofmyocardial perfusion by computed tomography.Eur Heart J Cardiovasc Imaging 2016;17:836–44.
10. Danad I, Ó Hartaigh B, Min JK. Dual-energycomputed tomography for detection of coronary

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Min and JafferJ U L Y 2 0 1 9 : 1 3 2 6 – 9 Editorial Comment
1329
artery disease. Expert Rev Cardiovasc Ther 2015;13:1345–56.
11. Renker M, Schoepf UJ, Becher T, et al.Computed tomography in patients with chronicstable angina: fractional flow reserve measure-ment. Herz 2017;42:51–7.
12. Choi JH, Min JK, Labounty TM, et al. Intra-coronary transluminal attenuation gradient in coro-nary CTangiography fordetermining coronary arterystenosis. J Am Coll Cardiol Img 2011;4:1149–57.
13. Choi JH, Koo BK, Yoon YE, et al. Diagnosticperformance of intracoronary gradient-basedmethods by coronary computed tomographyangiography for the evaluation of physiologicallysignificant coronary artery stenoses: a validation
study with fractional flow reserve. Eur Heart JCardiovasc Imaging 2012;13:1001–7.
14. Celeng C, Leiner T, Maurovich-Horvat P, et al.Anatomical and functional computed tomographyfor diagnosing hemodynamically significant coro-nary artery disease: a meta-analysis. J Am CollCardiol Img 2019;12:1316–25.
15. Coenen A, Kim YH, Kruk M, et al. Diagnosticaccuracy of a machine-learning approach to cor-onary computed tomographic angiography-basedfractional flow reserve: result from the MACHINEConsortium. Circ Cardiovasc Imaging 2018;11:e007217.
16. Itu L, Rapaka S, Passerini T, et al. A machine-learning approach for computation of fractional
flow reserve from coronary computed tomogra-phy. J Appl Physiol (1985) 2016;121:42–52.
17. Dey D, Gaur S, Ovrehus KA, et al. Integratedprediction of lesion-specific ischaemia fromquantitative coronary CT angiography using ma-chine learning: a multicentre study. Eur Radiol2018;28:2655–64.
18. Fryback DG, Thornbury JR. The efficacy ofdiagnostic imaging. Med Decis Making 1991;11:88–94.
KEY WORDS computed tomography, coronaryartery disease, fractional flow reserve, meta-analysis, myocardial perfusion imaging

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
ORIGINAL RESEARCH
10-Year Follow-Up After CoronaryComputed Tomography Angiographyin Patients With SuspectedCoronary Artery Disease
Tom Finck, MD,a Julius Hardenberg, MD,a Albrecht Will, MD,a Eva Hendrich, MD,a Bernhard Haller, PHD,bStefan Martinoff, MD,a Jörg Hausleiter, MD,c Martin Hadamitzky, MDa
ABSTRACT
ISS
Fro
Mü
Te
Ma
Ab
co
Ma
OBJECTIVES The aim of this study was to determine the long-term prognostic power of coronary computed tomog-
raphy angiography (CTA) to predict cardiac death and nonfatal myocardial infarction.
BACKGROUND Prognostic usefulness of coronary CTA has been confirmed for short- and intermediate-term follow-up.
However, long-term data for prognostic usefulness is still lacking, but is paramount because of the slowly progressing
nature of coronary artery disease (CAD).
METHODS A total of 2,011 patients with suspected but not previously diagnosed CAD were examined by coronary CTA.
Mean follow-upwas 10.0 years (interquartile range [IQR]: 8.1 to 11.2 years). Cox proportional hazards analysis was used for
the composite endpoint of cardiac death and nonfatal myocardial infarction. Event-free survival, which was defined as the
years it took to reach a cumulative 1% risk for the composite endpoint and reclassification from clinical risk, was calculated.
RESULTS The study endpoint was reached in 58 patients (42 cardiac deaths, 16 nonfatal myocardial infarctions). Cor-
onary CTA-assessed CAD severity (normal, nonobstructive, or obstructive) showed the best correlation with the
endpoint, with an adjusted c-index of 0.704, compared with a univariate c-index of 0.622 for the clinical risk model
(Morise score) alone. The annual event rate for patients with normal coronary arteries on baseline coronary CTA was
0.04%, which translated to an event-free survival period of 10 years. The highest annual event rate of 1.33% was found
in patients with 3-vessel obstructive CAD. Reclassification from clinical risk (Morise score) was possible in approximately
two-thirds of all patients (68%; p < 0.0001), which led to a substantial reduction of the intermediate-risk group
(reduction from 74% to 15%) in favor of the low-risk group (increase from 20% to 83%).
CONCLUSIONS Patients with normal coronary CTA results benefitted from an event-free survival period of 10 years
against cardiac death and nonfatal myocardial infarction. Risk stratification according to coronary CTA results allowed for
the delineation of clearly diverging prognostic groups and reclassified approximately two-thirds of all patients from
clinical risk groups. (J Am Coll Cardiol Img 2019;12:1330–8) © 2019 by the American College of Cardiology Foundation.
C oronary computed tomography angiography(CTA) is an established noninvasive imagingmodality to assess CAD. The high diagnostic
accuracy of coronary CTA has put it in the spotlight as
N 1936-878X/$36.00
m the aInstitut für Radiologie und Nuklearmedizin, Deutsches Herzzent
nchen, Munich, Germany; bInstitut für Medizinische Informatik, Statist
chnische Universität München, Munich, Germany; and the cMedizinisc
ximilians-Universität München, Munich, Germany. Dr. Hausleiter has rec
bott Vascular and Edwards Lifesciences. All other authors have report
ntents of this paper to disclose.
nuscript received May 8, 2018; revised manuscript received July 10, 2018
a low-risk alternative to invasive angiography in clin-ical workflow (1).
Coronary CTA has the ability to detect both calci-fied and noncalcified plaques as a sign of early CAD,
https://doi.org/10.1016/j.jcmg.2018.07.020
rum München, Klinik an der Technische Universität
ik und Epidemiologie, Klinikum rechts der Isar der
he Klinik und Poliklinik I, Klinikum der Ludwig-
eived speaker honoraria and research support from
ed that they have no relationships relevant to the
, accepted July 23, 2018.

AB BR E V I A T I O N S
AND ACRONYM S
AER = annual event rate
CAD = coronary artery disease
CADRADS = Coronary Artery
Disease Reporting and Data
System
CTA = coronary computed
tomography angiography
SIS = segment involvement
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Finck et al.J U L Y 2 0 1 9 : 1 3 3 0 – 8 Long-Term Prognostic Value of Coronary CT Angiography
1331
and therefore, it can be used as a prognostic tool toassess cardiovascular risk.
The prognostic value of coronary CTA in the short-to-intermediate term has been demonstrated bymultiple single-center and multicenter studies. Todate, the largest follow-up studies have evaluated theprognostic implications of coronary CTA in >25,000patients, with a mean follow-up of 5.6 years, whereasthe longest follow-up was 7.8 years in a cohort of1,469 patients (2–8).
SEE PAGE 1339score
SPECT = single-photon
emission computed
tomography
However, CAD is a slowly developing disease inwhich adverse clinical events often occur with a longlatency to morphological vessel changes. Because themaximum follow-up of previously mentioned studieswas approximately 5 to 6 years, longer observationperiods will be of great importance to establish cor-onary CTA as a useful prognostic tool to assess car-diovascular risk.
We therefore extended our follow-up of previouslypublished studies and adjudicated outcomes to 10years (9). The objective of this study was to validatethe negative predictive value of coronary CTA and toinvestigate the incremental predictive value ofdifferent coronary CTA parameters in risk predictioncompared with standard clinical risk assessment. Weinvestigated if an event-free survival period againstcardiac events could be defined and if risk reclassifi-cation could be achieved based on coronary CTAresults.
METHODS
STUDY POPULATION. All consecutive inpatients andoutpatients with suspected, but not previously diag-nosed, CAD who underwent coronary CTA at ourinstitution from October 10, 2004 to October 31, 2008were eligible for analysis. Patients were excluded ifthey were in an acute life-threatening situation,including patients with acute coronary syndromesand patients who did not have stable sinus rhythmduring the examination. Written informed consentwas obtained before the investigation. Informationabout age, weight, and height of the patient, symp-toms, cardiac history, and current medication wascollected. The following cardiac risk factors wererecorded: 1) presence and degree of hypertension (forbinary analysis, hypertension was defined as a sys-tolic blood pressure of >140 mm Hg or administrationof antihypertensive therapy); 2) diabetes mellitus(defined as fasting blood glucose level >7 mmol/l oruse of oral antidiabetic therapy); 3) smoking (definedas current smoker or previous smoker within the last
year); and 4) positive family history (definedas presence of cardiac death or myocardialinfarction in first-degree relatives youngerthan 55 years in men or younger than 65 yearsin women). In addition, laboratory results fortotal cholesterol, low-density lipoprotein andthe high-density lipoprotein fraction, andtriglycerides were collected. The Morise scorewas calculated from these data. This scoreevaluates both risk factors and clinicalsymptoms, and was best suited to evaluatecardiac risk in our study population (10). Thestudy design was approved by the local ethicscommittee.
CT PROCEDURE. The detailed scan protocol has beendescribed elsewhere (9). Different CT hardware wasused during the study period: a 64-slice, single-source CT scanner was used from October 2004 toSeptember 2006, and a 64-slice, dual-source CTscanner was used from October 2006 to October 2008(both Siemens Healthineers, Erlangen, Germany). Arecently proposed cardiac-specific conversion factorof 0.026 mSv/(mGy � cm) was used to estimate theradiation effective dose (11).
Coronary artery segmentation was performed ac-cording to the simplified American Heart Associationclassification, using the first 15 segments of the orig-inal 18 segments. Vessel segments >1.5 mm diameterwere evaluated by 2 physicians who had read >400cardiac CTs at the time the scan was performed. Dis-agreements were settled by consensus.
Each stenosis was rated visually according to thefollowing groups: no stenosis (0%); minimal stenosis(1% to 24%); and mild (25% to 49%), moderate (50% to69%), and severe ($70%) stenosis. Segments withartifacts were assigned to the most appropriate group.From the primary analysis, the following coronaryCTA scores were calculated, with CAD severityassessed as proposed by Ostrom et al. (12): normal,nonobstructive, and obstructive (which was itselfdivided into 1-, 2-, and 3- vessel obstructive). Thesegment involvement score (SIS) was the number ofsegments with any stenosis $25% or any calcified,mixed, or noncalcified plaque irrespective of thedegree of stenosis. Addition of affected segmentsresulted in a score ranging from 0 to 15.
The CADRADS (Coronary Artery Disease Reportingand Data System) was used as proposed by Cury et al.(13).
FOLLOW-UP. Follow-up information was obtained byclinical visits if available, by detailed questionnairessent by mail, or if the questionnaires were notreturned, by phone contact. All reported events were

TABLE 1 Clinical Characteristics (N ¼ 2,011)
Age (yrs) 59.2 � 11
Male 1,328 (66)
Body mass index (kg/m2) 26.1 � 4.01
Arterial hypertension 1,182 (58.8)
Smoking 402 (20)
Diabetes 146 (7.3)
Hypercholesterolemia 1,040 (51.7)
Family history of CAD 627 (31.2)
Angina
No 1,180 (58.7)
Atypical 733 (36.4)
Typical 98 (4.9)
Dyspnea (NYHA functional class >II) 68 (3.4)
Positive test for ischemia 176 (8.75)
Total cholesterol (mg/dl) 218 � 44.7
LDL (mg/dl) 131 � 37.6
HDL (mg/dl) 58.9 � 19.4
Triglycerides (mg/dl) 151 � 116
Morise risk score
Low 399 (20)
Moderate 1498 (74)
High 114 (6)
Indication for CCTA
CAD risk assessment 576 (28.6)
Dyspnea 120 (6.0)
Ischemia 160 (8.0)
Arrhythmia 405 (20.1)
Other 65 (3.2)
Thoracic pain 685 (34.1)
Values are mean � SD or n (%). Only the leading symptom is counted for eachpatient.
CAD ¼ coronary artery disease; CCTA ¼ coronary computed tomography angi-ography; HDL ¼ high-density lipoprotein; LDL ¼ low-density lipoprotein; NYHA ¼New York Heart Association.
TABLE 2
Morise sco
Low
Interme
High
CI ¼ confide
Finck et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Long-Term Prognostic Value of Coronary CT Angiography J U L Y 2 0 1 9 : 1 3 3 0 – 8
1332
verified by hospital records or phone contact with theattending physician, if possible, and adjudicated by 2physicians in consensus. The primary endpoint of thisstudy was a composite of cardiac death or nonfatalmyocardial infarction.
DEFINITION OF EVENT-FREE SURVIVAL. In an anal-ogy to established practice, low patient risk wasdefined as a cumulative event rate for cardiac deathand nonfatal myocardial infarction as <1% (14). In thesetting of our study, event-free survival was defined
Hazard Ratios and 95% CI for the Clinical Risk Model
No. of Events (%)(n ¼ 1,953)
Events (%)(n ¼ 58)
Hazard Ratio(95% CI) C-Index p Value
re 0.622 <0.001
397 (20) 2 (3) Reference
diate 1,449 (74) 49 (85) 6.4 (2.2–18.1)
107 (6) 7 (12) 11.3 (2.9–45.0)
nce interval.
as the duration that a patient remained in the low-riskcategory, calculated by the number of years it took apatient to cumulatively reach 1% probability of car-diac death or nonfatal myocardial infarction.
STATISTICAL ANALYSIS. Categorical variables wereexpressed as frequencies and percentages; continuousvariables were described as mean � SD or as median(interquartile range [IQR]) for time intervals. All sta-tistical evaluations were based on the event-free sur-vival for the study endpoint using the Kaplan-Meiermethod. Hazard ratios and multivariable analyseswere calculated and performed using the Cox pro-portional hazards method. Concordance c-indexeswere evaluated from time-to-event data as proposedby Harrell et al. (15). In the multivariable model, theincremental c-index for adding the coronary CTAvariable to clinical risk scores was calculated. Non-categorical net reclassification improvement, asproposed by Pencina et al. (16), was calculated.Reclassification was derived from the observed annualevent rate (AER) for the composite endpoint in the 6subgroups defined by the Morise score risk and thepresence of obstructive CAD, with low-risk patientsdefined as having an annual risk of <0.5% and high-risk patients defined as having an annual risk of >1%.All statistical tests were performed 2-sided, and asignificance level of 5% was used. The statisticalpackage R version 2.10.1, including the package rms(R Foundation, Vienna, Austria), was used forstatistical analysis (17,18).
RESULTS
STUDY POPULATION AND PATIENT CHARACTERISTICS.
During the study period, 2,176 patients withsuspected, but not previously diagnosed, CADunderwent coronary CTA. A total of 77 patients wereexcluded; 5 patients with acute aortic dissection whounderwent coronary CTA as a pre-operative assess-ment, 1 patient because of life-threatening conditions,and 71 patients who did not have stable sinus rhythmduring the scan. Of the remaining 2,099 patients, 2011patients were contacted for follow-up at a median of10.0 years (IQR: 8.1 to 11.2 years) and were included inthe study. This translated to a follow-up rate of 96%.
Mean patient age was 59 � 11 years; 1,328 patients(66%) were men. The pre-test risk assessed by theMorise risk score was low in 399 patients (20%),moderate in 1,498 patients (74%), and high in 114patients (6%). Detailed patient baseline characteris-tics are provided in Table 1.
ENDPOINTS AND CLINICAL CORRELATION.
With a total of 42 cardiac deaths and 16 nonfatalmyocardial infarctions, the study endpoint occurred

FIGURE 1 Receiver-Operator Curves for Clinical Risk
1.0
0.8
0.6
0.4Sens
itivi
ty
1 - Specificity
0.2
0.0
0.0 0.2 0.4
C-indexMORISEMORISE + CADMORISE + SISMORISE + CADRADS
0.6220.7280.7120.710
p < 0.001p < 0.001p < 0.001
0.6 0.8 1.0
Receiver-operator curves for clinical risk assessed by Morise score and for a stepwise
predictive model after further addition of coronary artery disease (CAD) severity,
CADRADS (Coronary Artery Disease Reporting and Data System), and segment involve-
ment score (SIS).
TABLE 3 Predictive Values and Hazard Ratios (95% CI) for Patient Subgroups According
to CCTA Parameters
CCTAVariable
No. of Events (%)(n ¼ 19,530)
Events (%)(n ¼ 58)
Multivariate Model(Adjusted for Morise score)
Hazard Ratio(95% CI)
C-Index forImprovement p Value
CAD severity 0.704 <0.001
Normal 568 (29) 2 (3) Reference
Nonobstructive 877 (45) 20 (35) 7.2 (4.3–12.0)
1-Vessel disease 263 (14) 11 (62) 13.0 (6.5–24.8)
2-Vessel disease 160 (8) 14 (24) 24.4 (10.5–56.7)
3-Vessel disease 85 (4) 11 (19) 33.8 (13.4–85.9)
CADRADS 0.673 <0.001
CADRADS 0 568 (29) 2 (3) Reference
CADRADS 1 303 (16) 7 (12) 6.9 (3.9–12.3)
CADRADS 2 574 (29) 13 (22) 7.3 (4.0–13.0)
CADRADS 3 388 (20) 27 (47) 20.1 (8.3–48.7)
CADRADS 4a 80 (4) 7 (12) 25.7 (9.9–67.0)
CADRADS 4b 28 (1) 1 (2) 8.6 (4.6–16.2)
CADRADS 5 12 (1) 1 (2) 26.0 (9.9–67.8)
SIS 0.666 <0.001
SIS 0 568 (29) 2 (3) Reference
SIS 1-5 933 (48) 25 (43) 8.2 (4.2–16.1)
SIS >5 452 (23) 31 (54) 20.4 (7.8–53.9)
CADRADS ¼ Coronary Artery Disease Reporting and Data System; SIS ¼ segment involvement score; otherabbreviations as in Tables 1 and 2.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Finck et al.J U L Y 2 0 1 9 : 1 3 3 0 – 8 Long-Term Prognostic Value of Coronary CT Angiography
1333
in a total of 58 patients (3% of study population).Fifty-three patients died from noncardiac causes,which resulted in a total of 111 deaths.
The Morise score had a decent discriminatoryability for composite endpoints, with a c-index of0.622. Hazard ratios for the clinical risk model areshown in Table 2.
CT RESULTS. The CT scan was performed on a64-slice, single-source scanner in 1,166 patients andon a 64-slice dual-source scanner in 845 patients.Median radiation exposure for coronary CTA was 13.9mSv (IQR: 10.4 to 17.8 mSv).
Analysis for CAD severity showed that 570 patientshad normal coronary arteries, 897 patients had non-obstructive coronary stenosis, and 544 patients hadobstructive CAD. Of these patients, 274 had 1-vesselobstructive CAD, 174 patients had 2-vessel obstruc-tive CAD, and 96 patients had 3-vessel obstructiveCAD.
Investigation for CADRADS resulted in 570 patients(28%) being classified as CADRADS 0, 310 patients(15%) as CADRADS 1, 587 patients (29%) as CADRADS2, 415 patients (21%) as CADRADS 3, 87 patients (5%)as CADRADS 4a, 29 patients (1%) as CADRADS 4b, and13 patients (1%) as CADRADS 5.
The mean SIS was 1.9 � 2.5 segments.
DISCRIMINATORY ABILITY OF CORONARY CTA
PARAMETERS. For primary endpoint analysis, CADseverity and CADRADS classification correlated bestwith outcome. For CAD severity, the c for improve-ment over clinical risk was 0.704 (p < 0.001). Thepredictive power of the CADRADS classificationwas slightly lower, with a c for improvement of 0.673(p < 0.001). SIS had a comparable predictive power,with a c for improvement over clinical risk of 0.666(p < 0.001). Hazard ratio analysis for the differentcoronary CTA parameter groups is shown in Table 3.
Receiver-operator curves for the Morise score as apre-test clinical parameter and a stepwise model afteraddition of coronary CTA parameters (CADRADS, CADseverity, SIS) are given in Figure 1. Kaplan-Meiercurves for patients with normal, nonobstructive,and obstructive coronary segments, CADRADSgroups, and different degrees of SIS are shown inFigure 2. No significant time dependency on survivalanalysis was noted (data not shown).
Annual event rates for endpoints ranged from0.04% (95% confidence intervals: 0.01% to 0.16%) inpatients with normal coronary arteries to 1.33% (95%confidence intervals: 0.74% to 2.41%) for patientswith 3-vessel obstructive CAD.
EVENT-FREE SURVIVAL. Figure 3 shows the averageevent-free survival period of all study participants as

FIGURE 2 Kaplan-Meier Plot for Event-Free Survival
0
1
2
0
1
2
0: Normal / CADRADS 01: Non-obstructive CAD / CADRADS 1-22: Obstructive CAD / CADRADS ≥3
0: SIS 01: SIS 1-52: SIS >5
100%
98%
96%
Surv
ival
Pro
babi
lity
94%
92%
90%
0 2 4 6 8 10Years
100%
98%
96%
Surv
ival
Pro
babi
lity
94%
92%
Patients at risk
90%
0 2 4 6 8 10
570958483
516853424
493825413
458774377
426717347
324455220
Years
Kaplan-Meier plot for event-free survival stratified according to CAD severity, CADRADS
and SIS. Abbreviations as in Figure 1.
Finck et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Long-Term Prognostic Value of Coronary CT Angiography J U L Y 2 0 1 9 : 1 3 3 0 – 8
1334
a function of coronary CTA findings and clinical pa-rameters. Within the complete cohort, but also whenwe analyzed independently of the Morise scores, sex,age, or presence of diabetes, we noticed a strikinglylower AER for patients with normal coronary arterieson baseline coronary CTA in comparison to patientswith obstructive or nonobstructive vessel changes.Event-free survival for all investigated patients agedyounger than 60 years with normal coronary arteriesreached the full observation length of 10 years, in-dependent of clinical risk, age, sex, or presence ofdiabetes. In contrast, the overall event-free survivalfor patients with obstructive or nonobstructive ste-noses fell to 2.2 years, and fell further to 1.4 years inpatients with diabetes.
RECLASSIFICATION FROM CLINICAL RISK. By clin-ical risk assessment (Morise score), 399 (20%) patients
were classified as low risk, 1,498 (74%) as intermedi-ate risk, and 114 (6%) as high risk. Further classifica-tion by CAD severity led to 1,674 (83%) patients beingclassified as low risk, 308 (15%) as intermediate risk,and 29 (2%) as high risk. As such, coronary CTAallowed risk reclassification for approximatelytwo-thirds of all patients for the composite endpoint(Figure 4). Non-categorical net reclassificationimprovement for the composite endpoint was 68%(p < 0.001).
DISCUSSION
For patients with suspected but not previously diag-nosed CAD, we demonstrated that 1) the lack of CADon baseline coronary CTA translated into an excellentlong-term prognosis and conferred an event-freesurvival of 10 years against hard cardiac events; 2)quantitative assessment of both coronary vesselobstruction and the generalized plaque burden, irre-spective of luminal obstruction, identified patients athigher long-term cardiac risk; and 3) approximatelytwo-thirds of all patients were reclassified regardingtheir long-term cardiac risk.
Analysis of 10-year follow-up data within ourpatient cohort revealed AERs of <0.05% for patientswith no CAD on baseline coronary CTA. Althoughsimilar observations were made at 2- and 5- yearfollow-up, long-term prognostic data were para-mount because these data better reflect the slowlyevolving process of CAD (9,19). Similar to our find-ings, Ostrom et al. (12) analyzed electron-beam CTangiography data from 2,538 consecutive patientsover a mean follow-up of 6.5 years and noted a sur-vival rate of 98.3% in patients with normal coronaryarteries. After follow-up of >6 years, Clerc et al. (20)reported comparable results, with 0% incidence ofcardiac death, myocardial infarction, and electiverevascularization in 153 patients with no CAD atbaseline coronary CTA.
Illustrated as event-free survival, all patients(except older adults) with normal coronary arteries onbaseline coronary CTA had a cumulative event rateof <1% during the whole observation length of 10years, irrespective of clinical risk, whereas patientswith obstructive or nonobstructive stenoses had anevent-free survival period of only 2.1 years.
The concept of a “warranty period” for coronaryartery calcium was investigated previously by Valentiet al. (21), who showed an event-free survival of 15years against all-cause mortality in patients with acoronary calcium score of 0 Agatston units.
Normal findings during dobutamine echocardiog-raphy, N13-ammonia positron emission tomography,

FIGURE 3 Event-Free Survival in Years
Negative CCTA (AER 0.04%)
Time in Years0 1 2 3 4 5 6 7 8 9 10
Nega
tive
CCTA
Nega
tive
CCTA
By se
xM
ORI
SEO
vera
ll
Positive CCTA (AER 0.45%)
Posit
ive
CCTA
Posit
ive
CCTA
Nega
tive
CCTA
By a
geDi
abet
es
Posit
ive
CCTA
Nega
tive
CCTA
Posit
ive
CCTA
High risk (AER 0%)
Intermediate risk (AER 0.06%)
Low risk (AER 0%)
High risk (AER 0.78%)
Intermediate risk (AER 0.47%)
Low risk (AER 0.14%)
Male (AER 0.05%)
Female (AER 0.04%)
Male (AER 0.55%)
Female (AER 0.42%)
≤60 y (AER 0%)
≤60 y (AER 0.18%)
>60 y (AER 0.13%)
>60 y (AER 0.64%)
No (AER 0.04%)
Yes (AER 0%)
No (AER 0.43%)
Yes (AER 0.75%)
Event-free survival in years, defined as the observed duration to exceed 1% risk for cardiac death or nonfatal myocardial infarction, for
patients with normal coronary arteries (negative coronary computed tomography angiography [CCTA]) and patients with nonobstructive and/
or obstructive CAD (positive CCTA). For further analysis, the cohort was stratified by the Morise score, sex, age, and presence or lack of
diabetes. AER ¼ annual event rate; other abbreviations as Figure 1.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Finck et al.J U L Y 2 0 1 9 : 1 3 3 0 – 8 Long-Term Prognostic Value of Coronary CT Angiography
1335
and magnetic resonance stress imaging had shorterevent-free survival periods of 1, 3, and 2 years in men(4 years in women), respectively (22–24).
The longest event-free survival for stress�restsingle-photon emission computed tomography(SPECT) was described by Romero-Farina et al. (25)in nearly 3,000 patients with normal stress and restSPECT using a composite endpoint of cardiac deathand nonfatal myocardial infarction. For patientsaged younger than 65 years, they calculated an
event-free survival period of 5 years (25). The shorterevent-free survival periods for functional imagetesting was easily explained by the fact that it reliedon hemodynamically relevant coronary stenosestypical for a more progressive stage of CAD. By notonly assessing obstructive coronary stenosis but alsosubtle coronary changes in earlier stages of CAD,coronary CTA can assess the whole range of coronaryartery changes. This, and the high negative predic-tive value during a 10-year follow-up period as

FIGURE 4 Risk Reclassification for Cardiac Death and Nonfatal
Myocardial Infarction
0.24
1.12
1498
399
1674
308
114
0.060,0
0,5
1,0
1,5
Annu
al E
vent
Rat
e in
%Pr
e-Te
st R
iskPo
st-T
est R
isk
2,0
0
Low
High
0.54
1.24
Intermediate
Intermediate
HighLow
381 18
– +
1275 223 29
– +
85
– +
85
29
1275
Risk reclassification for cardiac death and nonfatal myocardial infarction by
adding CCTA-assessed CAD severity to clinical risk evaluation by the Morise
score. Abbreviations as in Figures 1 and 3.
Finck et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Long-Term Prognostic Value of Coronary CT Angiography J U L Y 2 0 1 9 : 1 3 3 0 – 8
1336
shown in this study, emphasized the particular use-fulness of this modality in the low to intermediatepre-test risk population. This agrees with a recentmeta-analysis of noninvasive cardiac investigations(coronary CTA, cardiovascular magnetic resonance,exercise electrocardiographic testing, positron emis-sion tomography, stress echocardiography, andSPECT). Pooled AERs for >12,000 patients weresignificantly different among modalities, but thelowest event rate of cardiac death or myocardialinfarction occurred in patients with normal findingson coronary CTA (26).
The event-free survival period in our patientcohort was, by method, limited by the follow-upperiod of 10 years. Extrapolating the AER of 0.04%for patients with normal findings on baseline
coronary CTA would logically translate into a sub-stantially longer period of low cardiac risk.
As expected, CAD severity or CADRADS, which areboth parameters that directly quantify the degree ofluminal obstruction, but also the SIS, which takesinto account nonobstructive coronary lesions, all hadcomparable, good predictive power for the compositeendpoint. The levels of CADRADS and/or CADseverity and SIS certainly overlapped to a certaindegree because coronary stenoses are associated witha more advanced stage of CAD. However, the deci-sion for post-coronary CTA revascularization wasmainly based on the presence or lack of obstructiveCAD. Therefore, the similar outcome of patients withobstructive disease and those with a high SIS showedthat even if a coronary stenosis, which is the hall-mark of CAD, can be alleviated by revascularization,the long-term cardiovascular risk in such patientsremains substantially elevated. This can be partlyexplained by previous observations that mostmyocardial infarctions occur after acute rupture ofnonstenotic plaques and should further underlinethe strength of coronary CTA in assessing thegeneralized coronary plaque burden (27). In accor-dance with our observations, Dougoud et al. (28)identified the number of segments with plaques of>25% stenosis, as given by SIS, as an independentpredictor of cardiac death, myocardial infarction, orurgent revascularization on follow-up of <7 years.Min et al. (29) found an absolute difference in all-cause mortality of 5.9% between patients with a SISof >5 and a SIS of #5 after a 15-month follow-up of1,127 patients.
Although prognostic groups could be delineatedduring the entire follow-up period, the survivalcurves of patient subgroups with a high SIS orobstructive stenoses dipped after approximately 5years, whereas the lower risk groups followed a morelinear decrease. This is of interest because it would beexpected that events in high-risk subgroups wouldoccur earlier and underlined the need for longerfollow-up durations after coronary CTA.
A valid diagnostic test should be able to clearlydetect low- and high-risk groups. Assessment ofclinical risk by the Morise score led to most patientsbeing classified as intermediate risk, which might beunsatisfactory when it comes to clinical decisionmaking. After coronary CTA, reclassification could bedone for approximately two-thirds of all patients.Although an additional prognostic benefit in patientswith low clinical risk could not be demonstrated, the85% of intermediate-risk patients without obstructiveCAD had a particularly low event rate and could be

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Coronary CTA is
a reliable tool to assess long-term cardiovascular risk and can
attribute a 10-year event-free survival against hard cardiac
events. A substantial number of patients can be reclassified from
clinical risk after coronary CTA.
TRANSLATIONAL OUTLOOK: The role of future studies will
be to evaluate if primary preventive treatment guidance based
on coronary CTA results will be able to improve patient outcome
or reduce costs.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Finck et al.J U L Y 2 0 1 9 : 1 3 3 0 – 8 Long-Term Prognostic Value of Coronary CT Angiography
1337
reclassified into the low-risk group. Thus, coronaryCTA might be useful for this patient population byguiding further preventive medication, at least incases in which decisions based on clinical risk aloneare difficult.
The results from this study underlined the role ofcoronary CTA as a powerful noninvasive tool toassess cardiovascular risk. The excellent long-termpredictive value of coronary CTA might ultimatelyguide pharmacological or invasive treatment strate-gies for patients with clinically suspected CAD.However, before broad implementation, such stra-tegies will need to be validated in prospectiveoutcome studies.
STUDY LIMITATIONS. This was a single-centerobservational study. Results might be influenced bythe geographical patient characteristics and by thelocal investigation algorithm. Results from the indexcoronary CTA probably guided referring physicianstoward pharmacological treatment, which arguablyled to more patients with preventive cardiovasculartreatment in our study cohort than in the generalpopulation. However, information about patientcompliance with medical treatment was not available.Overall, the study cohort consisted mainly of patientsat low to intermediate risk of obstructive CADbecause patients with an intermediate to high pre-test risk referred to our institution were predomi-nantly investigated by SPECT or invasive coronaryangiography during the study period. Finally, the lownumber of events (n ¼ 58) might have reduced thestatistical power of our analysis. However, we areconvinced that restrictive endpoint analysis for hardcardiac events best reflects the usefulness of coronaryCTA in cardiovascular risk prediction and clinicaldecision-making. The differences of the reportedevent rates (Morise score) are at least partially
explained by the more cardiac-specific endpoints inthe underlying study.
CONCLUSIONS
With a median follow-up of 10 years, this studyprovided the longest prognostic data set of coronaryCTA parameters so far investigated. The absence ofCAD on baseline coronary CTA had an excellentnegative predictive value and allowed for thedefinition of a 10-year event-free survival periodagainst hard cardiac events. Quantification of coro-nary vessel obstruction, but also generalized vesselalterations visualized by coronary CTA improvedrisk prediction over clinical risk scores. Aftercoronary CTA, reclassification from clinical risk canbe done for approximately two-thirds of allpatients.
ADDRESS FOR CORRESPONDENCE: Priv.-Doz. Dr.med. Martin Hadamitzky, Deutsches Herzzentrum,Lazarettstrasse 36, 80636 München, Germany.E-mail: [email protected].
RE F E RENCE S
1. Hoffmann U, Truong QA, Schoenfeld DA, et al.Coronary CT angiography versus standard evalu-ation in acute chest pain. N Engl J Med 2012;367:299–308.
2. Feuchtner G, Kerber J, Burghard P, et al. Thehigh-risk criteria low-attenuation plaque <60HU and the napkin-ring sign are the mostpowerful predictors of MACE: a long-termfollow-up study. Eur Heart J Cardiovasc Imag-ing 2017;18:772–9.
3. Nadjiri J, Hausleiter J, Deseive S, et al. Prog-nostic value of coronary CT angiography in dia-betic patients: a 5-year follow up study. Int JCardiovasc Imaging 2016;32:483–91.
4. Nadjiri J, Hausleiter J, Jahnichen C, et al. In-cremental prognostic value of quantitative plaque
assessment in coronary CT angiography during 5years of follow up. J Cardiovasc Comput Tomogr2016;10:97–104.
5. Blanke P, Naoum C, Ahmadi A, et al. Long-termprognostic utility of coronary CT angiography instable patients with diabetes mellitus. J Am CollCardiol Img 2016;9:1280–8.
6. Cheruvu C, Precious B, Naoum C, et al. Longterm prognostic utility of coronary CT angiographyin patients with no modifiable coronary arterydisease risk factors: results from the 5 year follow-up of the CONFIRM International MulticenterRegistry. J Cardiovasc Comput Tomogr 2016;10:22–7.
7. Deseive S, Shaw LJ, Min JK, et al. Improved5-year prediction of all-cause mortality by
coronary CT angiography applying the CONFIRMscore. Eur Heart J Cardiovasc Imaging 2017;18:286–93.
8. Andreini D, Pontone G, Mushtaq S, et al. Long-term prognostic impact of CT-Leaman score inpatients with non-obstructive CAD: results fromthe COronary CT Angiography EvaluatioN ForClinical Outcomes InteRnational Multicenter(CONFIRM) study. Int J Cardiol 2017;231:18–25.
9. Hadamitzky M, Taubert S, Deseive S, et al.Prognostic value of coronary computed tomogra-phy angiography during 5 years of follow-up inpatients with suspected coronary artery disease.Eur Heart J 2013;34:3277–85.
10. Morise AP, Jalisi F. Evaluation of pretest andexercise test scores to assess all-cause mortality in

Finck et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Long-Term Prognostic Value of Coronary CT Angiography J U L Y 2 0 1 9 : 1 3 3 0 – 8
1338
unselected patients presenting for exercise testingwith symptoms of suspected coronary artery dis-ease. J Am Coll Cardiol 2003;42:842–50.
11. Trattner S, Halliburton S, Thompson CM, et al.Cardiac-specific conversion factors to estimateradiation effective dose from dose-length productin computed tomography. J Am Coll Cardiol Img2018;11:64–74.
12. Ostrom MP, Gopal A, Ahmadi N, et al. Mor-tality incidence and the severity of coronaryatherosclerosis assessed by computed tomogra-phy angiography. J Am Coll Cardiol 2008;52:1335–43.
13. Cury RC, Abbara S, Achenbach S, et al. CAD-RADS Coronary Artery Disease - Reporting andData System. An expert consensus document ofthe Society of Cardiovascular Computed Tomog-raphy (SCCT), the American College of Radiology(ACR) and the North American Society for Car-diovascular Imaging (NASCI). Endorsed by theAmerican College of Cardiology. J CardiovascComput Tomogr 2016;10:269–81.
14. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the managementof patients with chronic stable angina: executivesummary and recommendations. A Report of theAmerican College of Cardiology/American HeartAssociation Task Force on Practice Guidelines(Committee on Management of Patients withChronic Stable Angina). J Am Coll Cardiol 1999;33:2092–197.
15. Harrell FE Jr., Lee KL, Mark DB. Multivariableprognostic models: issues in developing models,evaluating assumptions and adequacy, andmeasuring and reducing errors. Stat Med 1996;15:361–87.
16. Pencina MJ, D’Agostino RB Sr., Steyerberg EW.Extensions of net reclassification improvementcalculations to measure usefulness of new bio-markers. Stat Med 2011;30:11–21.
17. The R Foundation. The R Project for StatisticalComputing. Available at: http://www.R-project.org.Accessed February 15, 2018.
18. Harrell FEJr. rms:RegressionModelingStrategies.R package 3.6-3, 2017. Available at: http://biostat.mc.vanderbilt.edu/wiki/Main/Rrms. Accessed February15, 2018.
19. Hadamitzky M, Distler R, Meyer T, et al.Prognostic value of coronary computed tomo-graphic angiography in comparison with calciumscoring and clinical risk scores. Circ CardiovascImaging 2011;4:16–23.
20. Clerc OF, Kaufmann BP, Possner M, et al.Long-term prognostic performance of low-dosecoronary computed tomography angiographywith prospective electrocardiogram triggering. EurRadiol 2017;27:4650–60.
21. Valenti V, B OH, Heo R, et al. A 15-year warrantyperiod for asymptomatic individuals without coro-nary artery calcium: a prospective follow-up of 9,715individuals. J Am Coll Cardiol Img 2015;8:900–9.
22. Herzog BA, Husmann L, Valenta I, et al. Long-term prognostic value of 13N-ammonia myocardialperfusion positron emission tomography addedvalue of coronary flow reserve. J Am Coll Cardiol2009;54:150–6.
23. Jahnke C, Furundzija V, Gebker R, et al.Gender-based prognostic value of pharmacolog-ical cardiac magnetic resonance stress testing:head-to-head comparison of adenosine perfusion
and dobutamine wall motion imaging. Int J Car-diovasc Imaging 2012;28:1087–98.
24. Marwick TH, Case C, Sawada S, et al. Predic-tion of mortality using dobutamine echocardiog-raphy. J Am Coll Cardiol 2001;37:754–60.
25. Romero-Farina G, Candell-Riera J, Aguade-Bruix S, et al. Warranty periods for normalmyocardial perfusion stress SPECT. J Nuclr Cardiol2015;22:44–54.
26. Smulders MW, Jaarsma C, Nelemans PJ, et al.Comparison of the prognostic value of negativenon-invasive cardiac investigations in patientswith suspected or known coronary artery disease-a meta-analysis. Eur Heart J Cardiovasc Imaging2017;18:980–7.
27. Giroud D, Li JM, Urban P, Meier B,Rutishauer W. Relation of the site of acutemyocardial infarction to the most severe coronaryarterial stenosis at prior angiography. Am J Cardiol1992;69:729–32.
28. Dougoud S, Fuchs TA, Stehli J, et al. Prog-nostic value of coronary CT angiography on long-term follow-up of 6.9 years. Int J CardiovascImaging 2014;30:969–76.
29. Min JK, Shaw LJ, Devereux RB, et al. Prog-nostic value of multidetector coronary computedtomographic angiography for prediction of all-cause mortality. J Am Coll Cardiol 2007;50:1161–70.
KEY WORDS coronary artery disease,coronary computed tomographicangiography, event-free survival, prognosis,reclassification

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E
A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
EDITORIAL COMMENT
Setting the Standard forPrognostic Analysis*
Leslee J. Shaw, PHD, Subhi J. Al’Aref, MDSEE PAGE 1330
A therosclerosis is a progressive disease andonce diagnosed leads to a higher risk of acutecoronary events and end-stage conditions
such as heart failure. This is the rationale for thedemonstration that an imaging modality not onlyrisk stratifies but adds uniquely to the estimation ofatherosclerotic disease events. The disease processimpacts both the peripheral and the coronary circula-tion with imaging findings predicting broadly acrossthe spectrum of cardiovascular disease; although im-aging specific to the heart, such as with coronarycomputed tomographic angiography (CTA), wouldhave the greatest yield in defining cardiac-specificrisk.
Hundreds of publications have reported on theeffectiveness of risk stratification for nuclear andechocardiographic imaging and, more recently, withCTA. Prognostication, when first introduced, wasmeant as a method to overcome many of the limita-tions and bias reported with studies examining diag-nostic accuracy and the selectivity in referral patternsto invasive coronary angiography. The introduction ofimaging for prognosis added a novel dimension toclinical care and provided physicians with a perspec-tive that encompassed more than the episode of carebut glimpse farther into the horizon of a patient’s life.What we have learned from prognostic modeling isthat imaging stratifies best when risk is elevated andwhere events are sufficiently prevalent such that aclear separation among patient subgroups is possible.
Challenges have always existed with risk stratifi-cation of lower risk cohorts such as are being imaged
ISSN 1936-878X/$36.00
*Editorials published in JACC: Cardiovascular Imaging reflect the views of
the authors and do not necessarily represent the views of iJACC or the
American College of Cardiology.
From the Department of Radiology and Medicine, Weill Cornell Medical
College, New York, New York. Both authors have reported that they
have no relationships with industry relevant to the contents of this
paper to disclose.
in today’s cardiovascular laboratories or as havebeen observed in recent randomized trials (1,2). Thisshift from imaging older and higher risk patientsfrom decades past to a younger patient subgroupwith more atypical symptoms is a major hurdle tothe field of risk stratification in today’s clinicalenvironment. The reason is quite simple: if youobserve few events, then stratification into higherrisk subgroups is nearly impossible. The key term is“nearly” and is possible but only if you enroll a verylarge cohort or if you follow patients over a longduration of follow-up.
In this issue of iJACC, Fincka et al. (3) report on theprognostic utility of CTA where patients were fol-lowed for an average of 10 years. Importantly, forclinical purposes, when you observe a patient frommiddle-age to elderly for a decade or longer, thisprovides a closer approximation to their life expec-tancy. Importantly, the research findings reveal agreater number of “hard” coronary events including42 deaths and 16 myocardial infarctions over thislonger duration of follow-up. A review of the survivalcurves makes manifest the progressive nature of thedisease process; with worsening survival notedamong those with evident atherosclerosis. In oneexample, the segment involvement score, whichprovides a numerical value for the extent of athero-sclerotic plaque across the segments of the epicardialcoronary arteries, was associated with a progressiveworsening in coronary artery disease (CAD) event-free survival. Those without any atherosclerotic pla-que were at low risk throughout the decade of follow-up. By comparison, those with a segment involve-ment score of $5 had the lowest event-free survival.These findings correspond to the elevated event riskreported for patients with nonobstructive CAD, with ahazard ratio of 7.2. Previously, any subgroup withoutobstructive CAD was categorized at lower risk. How-ever, more recently, we acknowledge that the
https://doi.org/10.1016/j.jcmg.2018.08.006

Shaw and Al’Aref J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 3 3 9 – 4 0
1340
presence of atherosclerotic disease among patientswith even mild stenosis is associated with an elevatedrisk of major CAD events. Especially noteworthy arethe findings that patients with an acute coronarysyndrome more often have a previously documentednonobstructive stenosis (4).
Moreover, the authors also importantly reportvalidation of their findings across key patient sub-groups such as women and men, younger and olderpatients, and so forth. Validation is a key componentof understanding the generalizability of overall pop-ulation risk findings. Importantly, absent disease isassociated with a very low risk of CAD events over thedecade of follow-up, that is <0.1%. This incrediblefindings has not been observed in other areas ofnoninvasive imaging, for example, a lack of ischemicfindings may still belie underlying atherosclerosisand is associated with an elevated risk of eventscompared to no stenosis or plaque on CTA (5). Onemay speculate based on this report and those from
other CTA registries that anatomic findings moreprofoundly stratify risk groups than functional mea-surements. This does not call into question theprognostic importance of ischemia and other stressimaging markers but does question whether anatomyshould be the core component of all risk assessmentstrategies. Of course, a greater wealth of evidence isnecessary, and the optimal strategy is likely whenboth physiologic and anatomic data are available. Thelingering question is whether anatomy is necessary tooptimally define risk and to clarify prognosis derivedfrom functional imaging or if anatomic findings alonesuffice as the most comprehensive measures of pa-tient risk.
ADDRESS FOR CORRESPONDENCE: Dr. Leslee J.Shaw, Weill Cornell Medical College, 413 East 69thStreet, New York, New York 30342. E-mail: [email protected].
RE F E RENCE S
1. Rozanski A, Gransar H, Hayes SW, et al.Temporal trends in the frequency of induciblemyocardial ischemia during cardiac stresstesting: 1991 to 2009. J Am Coll Cardiol 2013;61:1054–65.
2. Douglas PS, Hoffmann U, Patel MR, et al., forthe Investigators P. Outcomes of anatomicalversus functional testing for coronary artery dis-ease. N Engl J Med 2015;372:1291–300.
3. Finck T, Hardenberg J, Will A, et al. Ten-yearfollow-up after coronary computed tomographyangiography in patients with suspected coronaryarterydisease. J AmColl Cardiol Img2019;12:1330–8.
4. Chang HJ, Lin FY, Lee SE, et al. Coronaryatherosclerotic precursors of acute coronary syn-dromes. J Am Coll Cardiol 2018;71:2511–22.
5. Hoffmann U, Ferencik M, Udelson JE, et al.,for the Investigators P. Prognostic value of
noninvasive cardiovascular testing in patientswith stable chest pain: insights from thePROMISE trial (Prospective Multicenter ImagingStudy for Evaluation of Chest Pain). Circulation2017;135:2320–32.
KEY WORDS coronary CT angiography,coronary artery disease, prognosis

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
ORIGINAL RESEARCH
The Association of Coronary ArteryCalcification With Subsequent Incidence
of Cardiovascular Disease in Type 1 Diabetes The DCCT/EDIC TrialsMatthew Budoff, MD,a Jye-Yu C. Backlund, MPH,b David A. Bluemke, MD, PHD,c Joseph Polak, MD, MPH,d
Ionut Bebu, PHD,b David Schade, MD,e Suzanne Strowig, MSN,f Philip Raskin, MD,f John M. Lachin, SCD,b
for the DCCT/EDIC Research Group*
ABSTRACT
ISS
Fro
Ca
Un
Sh
Ne
Da
pu
gra
En
U0
Ge
pre
OBJECTIVES This study sought to determine the relationship between coronary artery calcium (CAC) scores and
subsequent cardiovascular disease (CVD) events in DCCT (Diabetes Control and Complications Trial)/EDIC (Epidemiology
of Diabetes Interventions and Complications) participants.
BACKGROUND The CAC score has been validated for improved risk stratification in general populations; however, this
association has not been well studied in type 1 diabetes (T1DM).
METHODS Computed tomography (CT) to measure CAC was performed in 1,205 DCCT/EDIC participants at a mean of
42.8 years of age during EDIC years 7 to 9, after the end of DCCT. This study analyzed the association between CAC and
time to the first subsequent CVD event or to the first major adverse cardiac event (MACE), a follow-up of 10 to 13 years.
CAC was categorized as: 0, >0 to 100, >100 to 300, or >300 Agatston units.
RESULTS Of 1,156 participants at risk for subsequent CVD, 105 had an initial CVD event (8.5 per 1,000 patient-years);
and of 1,187 participants at risk for MACE, 51 had an initial MACE event (3.9 per 1,000 patient-years). Event rates among
those with scores of zero (n ¼ 817 [70.7%]) were very low for CVD (5.6 per 1,000 patient years). CAC scores >100 to
300 (hazard ratio [HR]: 4.17, 5.40) and >300 (HR: 6.06, 6.91) were associated with higher risks of CVD and MACE,
respectively, compared to CAC of 0 (p < 0.0001). CAC scores >0 to 100 were nominally associated with CVD (HR: 1.71;
p ¼ 0.0415) but not with MACE (HR: 1.11; p ¼ 0.8134). Similar results were observed when also adjusted for mean HbA1c
and conventional CVD risk factors. The increment in the AUC due to CAC was modest.
CONCLUSIONS CAC scores >100 Agatston units were significantly associated with an increased risk of the subsequent
occurrence of CVD and MACE in DCCT/EDIC cohort. (Diabetes Control and Complications Trial [DCCT]; NCT00360815;
Epidemiology ofDiabetes Interventions andComplications [EDIC]; NCT00360893) (J AmColl Cardiol Img2019;12:1341–9)
© 2019 by the American College of Cardiology Foundation.
N 1936-878X/$36.00 https://doi.org/10.1016/j.jcmg.2019.01.014
m the aLos Angeles Biomedical Research Institute at Harbor-University of California Los Angeles School of Medicine, Torrance,
lifornia; bDepartment of Biostatistics, George Washington University, Rockville, Maryland; cDepartment of Radiology,
iversity of Wisconsin School of Medicine and Public Health, Madison, Wisconsin; dDepartment of Medicine, Lemuel
attuck Hospital and Tufts University School of Medicine, Boston, Massachusetts; eDepartment of Medicine, University of
w Mexico, Albuquerque, New Mexico; and the fDepartment of Medicine, University of Texas Southwestern Medical Center,
llas, Texas. *A complete list of participants in the DCCT/EDIC Research Group is presented in the Supplemental Material
blished online for the article in N Engl J Med 2015;372:1722–33. The DCCT/EDIC studies were supported by cooperative
nts (1982 to 1993, 2012 to 2017, and 2017 to 2022) from and contracts (1982 to 2012) with the Division of Diabetes
docrinology and Metabolic Diseases of the National Institute of Diabetes and Digestive and Kidney Disease (current grants
1 DK094176 and U01 DK094157), and the National Eye Institute, National Institute of Neurologic Disorders and Stroke,
neral Clinical Research Centers Program (1993 to 2007), and Clinical Translational Science Center Program (2006 to the
sent). Contributors included Abbott Diabetes Care, Animas, Bayer Diabetes Care, Becton Dickinson, Eli Lilly, Extend Nutrition,

ABBR EV I A T I ON S
AND ACRONYMS
AER = albumin excretion rate
CAC = coronary artery calcium
CT = computed tomography
CVD = cardiovascular disease
HbA1c = hemoglobin A1c
MACE = major adverse cardiac
event
T1DM = type 1 diabetes
mellitus
T2DM = type 2 diabetes
mellitus
Insulet Cor
Diabetes C
adherence
Health and
from Boeh
relationship
Manuscript
Budoff et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CAC and CVD in DCCT/EDIC J U L Y 2 0 1 9 : 1 3 4 1 – 9
1342
T ype 1 diabetes mellitus (T1DM) isassociated with increased risk ofcardiovascular complications
including myocardial infarction, stroke,congestive heart failure, and unstable angina(1). In addition to glycemia (2), numerousconventional risk factors (age, hypertension,hyperlipidemia, and so forth) and unknownhereditary, genetic, and environmental fac-tors may be involved. Risk factors for cardio-vascular disease (CVD) are well establishedin type 2 diabetes mellitus (T2DM) but areless well established in T1DM, perhaps dueto differences between the duration of dia-
betes, lower body weights, and lower prevalence ofthese conventional risk factors. The coronary arterycalcium (CAC) score provides an assessment of calci-fied coronary artery plaques, a marker of atheroscle-rotic burden (3). An elevated CAC score has beenshown to be predictive of clinical outcomes in severalcohorts that included various proportions of partici-pants with diabetes (4–8). However, the associationwith CAC scores in individuals with T1DM has notbeen well studied (9).
SEE PAGE 1350
The DCCT (Diabetes Control and ComplicationsTrial) (10) enrolled 1,441 T1DM individuals, most ofwhom were enrolled in the follow-up EDIC (Epide-miology of Diabetes Interventions and Complications)study (11). After w7 years of EDIC follow-up, CACscores were measured in 1,205 participants at a meanof 42.8 years of age. Prior intensive treatment duringDCCT was associated with lower CAC scores (12).Herein additional analyses are presented to assess theassociation between CAC scores and the developmentof initial CVD events in DCCT/EDIC participants whowere followed over a subsequent 10 to 13 years.
RESEARCH DESIGN AND METHODS
SUBJECTS. The DCCT, a randomized controlledclinical trial (13), compared the effects of intensive(n ¼ 711) versus conventional (n ¼ 730) diabetestherapy on long-term diabetes complications. From1983 to 1989, 1,441 individuals 13 to 39 years of age
p., Lifescan, Medtronic Diabetes, Nipro Home Diagnostics, Nova
are, and Sanofi-Aventis. Contributors provided free or discoun
to the study but had no role in the DCCT/EDIC study. Dr. Budoff
General Electric. Dr. Raskin is a consultant for Reata Pharmaceuti
ringer-Ingelheim Pharmaceutical and Gan & Lee Pharmaceutical.
s relevant to the contents of this paper to disclose.
received September 14, 2018; revised manuscript received Nove
were enrolled: 726 were randomized to the primaryprevention cohort (diabetes duration 1 to 5 years andno evidence of microvascular complications), and 715into the secondary intervention cohort (diabetesduration 1 to 15 years and minimal retinopathy ornephropathy complications). After the end of theDCCT (1993), participants in the conventional treat-ment group were instructed in intensive therapy andreferred to their personal physicians for continueddiabetes care.
The EDIC study (11) was an observational follow-upof the DCCT cohort, started in 1994. A total of 1,394participants (98.2%) of 1,420 surviving DCCT partici-pants were enrolled. Of these, 1,205 of the 1,296 sur-vivors (93%) consented to undergo CAC computedtomography (CT) 7 to 9 years after completion ofDCCT (EDIC year 7, between 2001 and 2002). Of these,49 participants had a prior CVD event and wereexcluded from these analyses, leaving 1,156 partici-pants with CT data who were at risk of an initial CVDevent. Likewise, 18 participants who had a prior majoradverse cardiac event (MACE) were excluded, leaving1,187 participants at risk for an initial MACE. Figure 1lists the EDIC participants available for subsequentCVD and MACE analyses.
DCCT/EDIC COVARIATES. Covariate values wereobtained concurrently with or at the last visit prior toCT evaluation. Smoking, blood pressure, pulse, andbody mass index were obtained from at annualfollow-up evaluations. The Central BiochemistryLaboratory measured hemoglobin A1c (HbA1c) levelsquarterly during the DCCT study and annually in theEDIC study. The DCCT/EDIC time-weighted meanHbA1c, with weights of 0.25 for DCCT and 1 for EDICvalues, represents the total glycemic exposure duringthe DCCT/EDIC studies. Fasting lipids and albuminexcretion rates (AERs) were measured annuallyduring DCCT and in alternate years during EDIC.Microalbuminuria was defined as the history of AER>30 mg/24 h on at least 2 consecutive annual visits.
CORONARY ARTERY CALCIFICATION ASSESSMENT.
The methods for obtaining CT-derived CAC scoreswere previously described (12). Briefly, CT was per-formed in 19 scanning sites (Supplemental Table 1),using a C-150 cardiac-gated electron beam CT scanner
Diabetes Care, Omron, Perrigo Diabetes Care, Roche
ted supplies or equipment to support participants’
has received support from U.S. National Institutes of
cal; and has received support through his institution
All other authors have reported that they have no
mber 13, 2018, accepted January 3, 2019.

FIGURE 1 Flow Chart of the EDIC Study
DCCT/EDIC patientsN = 1441
CAC & CVD*
N = 1156
Any CVDN = 105 (9.1%)
No CVDN = 1051 (90.9%)
* Patients with prior CVD events during DCCT (N = 49) were eliminated from the analysis.† Patients with prior MACE events during DCCT (N = 18) were eliminated from the analysis.
CAC & MACE†
N = 1187
MACEN = 51 (4.3%)
No MACEN = 1136 (95.7%)
EDIC at Year 8N = 1296
CT conducted andevaluableN = 1205
EDIC participants with available CT evaluations were included. At the time CT was performed (EDIC years 7 to 9), 1,205 patients had obtained
evaluable CT scans. Forty-nine participants were eliminated because of prior CVD events, and 18 were eliminated because of prior MACEs.
CT ¼ computed tomography; CVD ¼ cardiovascular disease; DCCT ¼ Diabetes Control and Complications Trial; EDIC ¼ Epidemiology of
Diabetes Interventions and Complications study; MACE ¼ major adverse cardiac events.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Budoff et al.J U L Y 2 0 1 9 : 1 3 4 1 – 9 CAC and CVD in DCCT/EDIC
1343
(n ¼ 9, Imatron, San Francisco, California), a Light-speed (n ¼ 7, General Electric Medical Systems,Waukesha, Wisconsin), or a Volume Zoom (Siemens,Erlanger, Germany) multidetector CT system, aLightspeed Marconi MX-8000 (General Electric Med-ical Systems), or a Somatom 4þ (Siemens) model(n ¼ 3). All participants were scanned twice overcalibration phantoms of known physical calciumconcentration.
CT scans were read centrally at the Los AngelesBiomedical Research Center Core CT laboratory(University of California, Los Angeles, California) toidentify and quantify CAC, using the method ofAgatston et al. (13). CAC was assessed by measuringall pixels with density >130 Hounsfield units (HU).The area of the calcium was multiplied by the densityfactor, represented by the peak density in eachcalcific lesion, with 1 ¼ 130 to 199 HU; 2 ¼ 200 to 299HU; 3 ¼ 300 to 399 HU; and 4 ¼$400 HU. The calciumscore was obtained by summing all calcific lesions inall 4 major coronary arteries and side branches. Theaverage score from the 2 scans was used in the anal-ysis. Readers were masked to participant identity andprior DCCT treatment assignment. CAC was divided
into 4 categories: 0, >0 to 100, >100 to 300, or >300Agatston units for the current analysis.
Reading center staff evaluated scan quality basedon 7 criteria: motion artifact, streak artifact, phantomplacement, slice registration, lack of noise, axiscoverage, and x-y axis coverage. The 19 scanningcenters were monitored monthly by using thesecriteria. The intrareader and inter-reader precisionwere evaluated by using a set of standard scans thatwere reread by the same reader and another reader atthe reading center. The kappa value of intrareaderagreement beyond chance for the presence or absenceof calcification was 0.81, and the inter-reader kappavalue was 0.86. The coefficient of reliability for thenumerical CAC scores was 0.99 for both inter-readerand intrareader, as reported previously (12).CARDIOVASCULAR OUTCOMES. The primary out-comes included time to CVD, death judged to besecondary to cardiovascular disease; subclinical (“si-lent”) myocardial infarction detected on an annualelectrocardiogram; angina confirmed by ischemicchanges with exercise tolerance testing or by clini-cally significant obstruction on coronary angiog-raphy; congestive heart failure with paroxysmal

TABLE 1 Characteristics Prior to or at CT Scan
All Participants(N ¼ 1,156)
CAC Score Groups
0 (n ¼ 817) >0-100 (n ¼ 221) >100-300 (n ¼ 65) >300 (n ¼ 53)
p Value*
Difference Trend
Females 47.2 54.1 33.5 27.7 22.6 <0.0001 <0.0001
White participants 96.5 96.3 95.9 98.5 100.0 0.3954 0.1792
Intensive group 49.9 50.8 49.8 46.2 41.5 0.5477 0.1704
Primary cohort 50.6 54.4 46.2 36.9 28.3 <0.0001 <0.0001
Age, yrs 42.8 � 6.8 41.4 � 6.7 45.2 � 6.0 47.1 � 5.9 48.9 � 5.1 <0.0001 <0.0001
Duration of T1DM, yrs 21.0 � 4.9 20.6 � 4.7 21.4 � 5.0 23.3 � 5.6 23.0 � 4.5 <0.0001 <0.0001
Current cigarette smokers 14.6 12.0 19.5 23.1 24.5 0.0009 0.0001
Body mass index, kg/m2 27.5 � 4.4 27.4 � 4.5 27.8 � 5.1 27.8 � 3.8 27.6 � 4.0 0.3251 0.7474
Systolic blood pressure, mm Hg 122 � 14 121 � 14 124 � 14 125 � 13 129 � 15 <0.0001 <0.0001
Diastolic blood pressure, mm Hg 76 � 9 77 � 9 76 � 9 76 � 9 78 � 9 0.5037 0.2881
Antihypertensive medication 27.5 22.9 33.9 49.2 45.3 <0.0001 <0.0001
HbA1c 7.9 (1.3) 7.9 (1.3) 8.0 (1.4) 8.0 (1.2) 8.1 (1.4) 0.1960 0.1776
Weighted mean HbA1c 8.1 � 1.1 8.1 �1.1 8.2 � 1.0 8.2 �1.2 8.2 � 1.0 0.1431 0.2727
HDL cholesterol, mg/dl 56 � 15 57 � 15 53 � 14 53 � 12 53 � 15 0.0001 0.0271
Non-HDL cholesterol, mg/dl 130 � 34 128 � 34 133 �36 135 � 28 136 � 33 0.0175 0.1098
LDL cholesterol, mg/dl 112 � 29 111 � 29 114 � 30 116 � 28 115 � 29 0.2448 0.2751
Total cholesterol, mg/dl 186 � 34 186 � 34 187 � 35 188 � 29 188 � 36 0.6624 0.5617
Triglyceride, mg/dl 89 � 61 85 � 53 96 �75 106 � 80 107 � 79 0.0071 0.0059
Lipid-lowering medication 21.0 14.8 31.2 43.1 47.2 <0.0001 <0.0001
Microalbuminuria† 24.6 22.3 24.4 36.9 45.3 0.0002 <0.0001
Values are %, mean � SD, or n (%). *The p values are based on the contingency chi-square test (df ¼ 3) of any differences among CAC score groups and Cochran-Armitage trend test (df ¼ 1) for categoricalvariables; and the Kruskal-Wallis test (df ¼ 3) of any difference and ANOVA linear trend test (df ¼ 1) for continuous variables. †Microalbuminuria was defined as a history of AER $30 mg/24 h on at least 2consecutive visits during the DCCT/EDIC studies.
AER ¼ albumin excretion rate; DCCT/EDIC ¼ Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications studies; T1DM ¼ type 1 diabetes mellitus; HbA1c ¼hemoglobin A1c; HDL ¼ high-density lipoprotein; LDL ¼ low-density lipoprotein.
Budoff et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CAC and CVD in DCCT/EDIC J U L Y 2 0 1 9 : 1 3 4 1 – 9
1344
nocturnal dyspnea, orthopnea, or marked limitationof physical activity caused by heart disease; orrevascularization with angioplasty and/or coronaryartery bypass. Time to the first MACE also was eval-uated, including nonfatal myocardial infarction,nonfatal stroke, or CV death.
Cardiovascular events were captured by partici-pants’ self-reports during the EDIC annual visits,documented by medical records, and centrally adju-dicated by the EDIC Mortality and Morbidity ReviewCommittee, masked to DCCT treatment assignment,HbA1c, and glucose levels. The analyses reported hereincluded only adjudicated qualifying cardiovascularevents that occurred after the CT examination (w2001to 2002) through December 31, 2013, a period of 10 to13 years depending on the time of the CT. This datalocked date period was selected to provide adequatestatistical power for multivariate modeling in thecomplete cohort (2).STATISTICAL ANALYSIS. The contingency chi-square test was used to assess differences in cate-gorical characteristics among the 4 CAC score groups,and the Cochran-Armitage trend test was used toassess a linear trend (increasing or decreasing)in proportions among the ordered groups. The
Kruskal-Wallis test was used to compare quantitativecharacteristics among groups, and the ANOVA lineartrend test was used to assess linear trends in themeans (14).
The Kaplan-Meier estimate of the cumulativeincidence function of a CVD event within the 4 CACscore groups is presented, and the differences amonggroups tested were derived by using the log-ranktest (15). Cox proportional hazards models wereused to assess differences among the CAC scoregroups in the risk of subsequent CVD events,adjusted for known risk factors. Hazard ratios (HRs),95% confidence intervals (CIs), and Wald test pvalues were reported (16). Cox proportional hazardsmodels with CAC score group number as a quanti-tative covariate provided a Wald test of linear trendamong CAC score groups.
Cox model A was minimally adjusted for scanningsite, age, and sex, whereas model B was furtheradjusted for DCCT cohort (primary prevention vs.secondary intervention cohort), mean HbA1c level,systolic blood pressure, antihypertensive medication,low-density lipoprotein cholesterol, high-densitylipoprotein cholesterol, and smoking at the time ofthe CT (EDIC years 7 to 9) and DCCT baseline family

TABLE 2 Incidence of any CVD and of MACE 10 to 13 Years After the CT Examination
All Participants
CT Group
0 >0-100 >100-300 >300 Difference p Value* Trend p Value†
Any CVD event
Participants at risk 1,156 817 221 65 53
First event 105 (9.1) 50 (6.1) 23 (10.4) 15 (23.1) 17 (32.1) <0.0001 <0.0001
Patient-yrs 12,350 8,952 2,334 615 449
Rate per 1,000 patient-yrs 8.5 5.6 9.9 24.4 37.9
95% confidence limits 7.0-10.3 4.2-7.4 6.6-14.8 14.5-41.0 23.2-61.8
MACE event
Participants at risk 1,187 827 226 72 62
First event 51 (4.3) 23 (2.8) 7 (3.1) 10 (13.9) 11 (17.7) <0.0001 <0.0001
Patient-yrs 13,006 9,200 2,479 722 605
Rate per 1,000 patient-yrs 3.9 2.5 2.8 13.9 18.2
95% confidence limits 3.0-5.2 1.7-3.8 1.3-5.9 7.4-26.1 10.1-32.7
Values are n or n (%), unless otherwise indicated. *The difference p values were obtained from a Cox PH model adjusted for the scanning site by using the 4 CAC score groups asa class effect on 3 df. †The trend p values were obtained from a Cox PH model adjusted for the scanning site using the 4 CAC score groups as a quantitative covariate on 1 df.
CAC ¼ coronary artery calcium; CVD ¼ cardiovascular disease; MACE ¼ major adverse cardiac event.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Budoff et al.J U L Y 2 0 1 9 : 1 3 4 1 – 9 CAC and CVD in DCCT/EDIC
1345
history of myocardial infarction (2). The associationbetween CAC and the subsequent risk of any CVD andMACE in these multivariate models was assessed byusing the Wald chi-square test with 3 df. Area underthe receiver-operating curve (AUC) was calculatedusing 4 CAC categories for each Cox model based onthe Gonen-Heller approach (17), and CIs for differencein AUCs were obtained using bootstrapping. The AUCdescribes the predictive accuracy of a model, with anAUC of 0.5 corresponding to random predictions andan AUC of 1 corresponding to perfect predictions. Thepredictive value of a biomarker is represented by theincrease in AUC (if any) when the marker is added tothe model with the other covariates.
Results nominally significant at a 2-sided p valueof <0.05 are cited. All analyses were performed usingSAS version 9.3 software (SAS Institute, Cary, NorthCarolina) and R software (R Foundation for StatisticalComputing, Vienna, Austria).
RESULTS
Of the 1,156 participants at risk for an initial CVDevent, 817 (70.7%) had a CAC score of 0, 221 (19.1%)had a CAC score of >0 to 100, 65 had (5.6%) had aCAC score of >100 to 300, and 53 (4.6%) had a CACscore of >300 Agatston units. Table 1 presentsparticipant characteristics at the time of the CTwithin the 4 CAC score groups. Participants’ meanage was 42.8 years; mean systolic blood pressure was122 mm Hg; 27.5% were taking antihypertensivemedications; and 47.2% were females. Women hadlower CAC scores than men. Based on the trend test,increasing CAC scores were also associated witholder age, longer duration of diabetes, smoking,
higher systolic blood pressure (but not diastolicblood pressure), lower myocardial infarction choles-terol, higher triglycerides, and a history of micro-albuminuria. Also, mean nonmyocardial infarctioncholesterol levels differed significantly among theCAC categories but without a significant linear trend,that is the mean in the CAC score 0 group was lessthan that in the higher CAC score groups afteradjustment for sex. Higher CAC scores were alsoassociated with increasing use of antihypertensiveand lipid-lowering medications. Interestingly, CACscores were not associated with the current HbA1c
level, the DCCT/EDIC time-weighted mean HbA1c
level, the low-density lipoprotein, or the totalcholesterol levels.
During the 10 to 13 years of follow-up after the CTexamination (through December 31, 2013), 105 of the1,156 participants at risk over 12,350 patient-years hadan initial CVD event (8.5 per 1,000 patient years; 95%CI: 7.0 to 10.3), and 51 of 1,187 at risk over 13,006patient-years had an initial MACE (3.9 per 1,000patient years; 95% CI: 3.0 to 5.2).
Table 2 shows that the crude incidence of any CVDamong the 4 CAC score groups increased as the CACscore categories 1 through 4 increased, with values of6.1%, 10.4%, 23.1%, and 32.1%, respectively. Thecorresponding CVD event rates in the 4 CAC cate-gories were 5.6, 9.9, 24.4, and 37.9, respectively, per1,000 patient years. Figure 2 presents the cumulativeincidence of any CVD following the CT examinationwithin the 4 CAC score groups. Increasing calciumscores were strongly associated with higher risks ofCVD events (p < 0.0001).
Using the annual rate per year (Table 2), the ab-solute risks (Figure 2) (cumulative incidence) of any

FIGURE 2 Cardiovascular Events by CAC Score
0 1 2 3 4 5 6 7Years Since Scanning Date
8 9 10
0
>0 – 100
>100 – 300
>300 & upLog–Rank test p < 0.0001Cu
mul
ativ
e In
cide
nce
0.36
0.32
0.28
0.24
0.20
0.16
0.12
0.08
0.04
0.00
No. at Risk7301854732
786206
5440
8172216553
0>0–100>100–300>300
11 12 13
Cumulative incidence of the first cardiovascular event by CAC group scores, where 0 ¼ >0 to 100, >100 to 300, and >300 Agatston units.
The p value from the log-rank test was <0.0001. CAC ¼ coronary artery calcium.
TABLE 3 Association
Among Those Still at
Subclinical CAC Score(Agatston Units)
Model A*
0
>0-100
>100-300
>300
Chi-square test†
Model B‡
0
>0-100
>100-300
>300
Chi-square test†
Values in bold indicate statCT study for each subject dcategories of CAC in the resystolic blood pressure, anbaseline family history of M
MI ¼ myocardial infarcti
Budoff et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CAC and CVD in DCCT/EDIC J U L Y 2 0 1 9 : 1 3 4 1 – 9
1346
CVD over the 5 years following the CAC evaluationof CAC for >0 to 100, >100 to 300, and >300 were2.8%, 4.8%, 11.5%, and 17.3%, respectively. Thus,the 5-year risk of any CVD with a calcium score
Between CAC at EDIC Years 7 to 9 and Subsequent CVD and MACE
Risk During the EDIC Study
CVD (n ¼ 1,156) MACE (n ¼ 1,187)
Hazard Ratio(95% CI) p Value
Hazard Ratio(95% CI) p Value
1.00 (Reference) 1.00 (Reference)
1.71 (1.02-2.88) 0.0415 1.11 (0.46-2.66) 0.8134
4.17 (2.23-7.80) <0.0001 5.40 (2.37-12.27) <0.0001
6.06 (3.22-11.40) <0.0001 6.91 (2.99-15.97) <0.0001
38.68 <0.0001 20.86 <0.0001
1.00 (Reference) 1.00 (Reference)
1.54 (0.91-2.60) �0.1060 0.93 (0.38-2.30) 0.8770
4.05 (2.14-7.64) <0.0001 6.05 (2.56-14.30) <0.0001
4.73 (2.47-9.08) <0.0001 5.57 (2.33-13.35) 0.0001
30.53 <0.0001 27.38 <0.0001
istically significant findings. *Adjusted for scanning site, sex, and age at the time of theuring EDIC years 7 to 9. †3 df Wald chi-square test results of the significance of the 4spective model. ‡Adjusted for scanning site, sex, study cohort, log mean HbA1c, age,tihypertensive medication, LDL, HDL, and smoking at EDIC years 7 to 9, and DCCTI.
on; other abbreviations as in Tables 1 and 2.
>300 was 1.5 times greater than with a calciumscore of >100 to 300, and the latter is 2.4 timesgreater than a calcium score of 0 to 100 Agatstonunits.
The incidence of MACE similarly increased signif-icantly (p < 0.0001) over the 4 CAC score categorieswith respective values of 2.8%, 3.1%, 13.9%, and17.7%, respectively, and corresponding event rates of2.5, 2.8, 13.9, and 18.2 per 1,000 patient years,respectively. The corresponding 5-year absolute risksof MACE for 4 CAC categories of 0, >0 to 100, >100 to300, and >300 were 1.2%, 1.4%, 6.7%, and 8.7%,respectively. Thus, the 5-year risk of subsequentMACE with a calcium score >300 is 1.3 times greaterthan with a calcium score of >100 to 300, and thelatter is 4.8 times greater than with a calcium scoreof >0 to 100 Agatston units.
CAC was highly associated with the subsequentrisk of CVD and MACE in Cox models A (3-df Waldchi-square values of 38.68 and 20.86, respectively;p < 0.0001 for both) and B (3-df Wald chi-squarevalues of 30.53 and 27.38, respectively; p < 0.0001for both).
Table 3 presents HRs for any CVD and for MACEestimated from Cox proportional hazards modelscomparing the upper 3 CAC score groups to the first

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Budoff et al.J U L Y 2 0 1 9 : 1 3 4 1 – 9 CAC and CVD in DCCT/EDIC
1347
category (CAC score of 0), with adjustment for othercovariates. Adjusted only for the scanning site, sex,and age (model A), CAC scores of >100 to 300 (CVDHR: 4.17; 95% CI: (2.23 to 7.80; MACE HR: 5.40; 95%CI: 2.37 to 12.27) and >300 (CVD HR: 6.06; 95% CI:3.22 to 11.40; MACE HR: 6.91; 95% CI: 2.99 to 15.97)had higher risks for both any CVD and MACEcompared with CAC 0 (p < 0.0001), whereas the HRfor a CAC score of>0t o 100was significant for any CVD(HR: 1.71; 95% CI: 1.02 to 2.88; p ¼ 0.0415) but not forMACE (HR: 1.11; 95% CI: 0.46 to 2.66; p ¼ 0.8134). Theincreased risks for CAC scores of >100 to 300 and >300but not >0 to 100 remained significant after furtheradjustment for mean HbA1c level and other conven-tional risk factors (see model B in Supplemental Ta-ble 1). The same findings were observed when themean HbA1c value was substituted for treatment group(data not shown) and when model B was furtheradjusted for use of lipid-lowering medications,angiotensin-converting enzyme inhibitor, or T1DMduration (data not shown). Additionally, the in-teractions between CAC and sex (p ¼ 0.4922), betweenCAC and mean HbA1c level (p ¼ 0.2431), and betweenCAC and intensive versus conventional treatmentgroup (p ¼ 0.3693) were not significant.
In the AUC analysis (Supplemental Table 1), whenCAC score categories were added to the other cova-riates in model A for any CVD, the AUC increased from0.684 without CAC to 0.697 with CAC (95% CI for thedifference: 0.0005 to 0.0292), indicating a significantincrease in the AUC. When added to the covariates inmodel B for any CVD, the AUC increase was not sta-tistically significant. The increase in AUC was notsignificant for MACE.
Statin use (or not) during EDIC was only recordedstarting in EDIC year 11, after CT was conducted. Theproportion of participants known to be using statinsat the time of the CVD event was 44.4% (20 of 45participants) among those with a CAC score 0; 64.7%(11 of 17 participants) among those with a CACscore >0 to 100; 45.5% (5 of 11 participants) with aCAC score >100 to 300; and 60.0% (6 of 10 partici-pants) with a CAC score >300 Agatston units.
DISCUSSION
CAC has been shown in numerous studies to predictCVD events, most strongly in participants with T2DMat intermediate risk (18,19). The present study dem-onstrates similar predictive power for CAC amongpersons with T1DM. The 10- to 13-year CVD incidencewas 23% among subjects with a CAC score >100 to 300and 32% for those with CAC score >300 Agatstonunits.
The largest study prior to the present reportthat evaluated participants with T1DM with CACmeasurements was the CACTI (Coronary ArteryCalcification in Type 1 Diabetes; NCT00005754) study(20). The 656 T1DM participants in the CACTI studyshowed a higher prevalence for and extent of CACthan 764 age- and sex-matched control participantswithout diabetes with no differences between menand women. Prior studies have demonstrated exten-sive calcification even in young adults (17 to 28 yearsof age) with TIDM (21), and calcification has beenassociated with factors including genetic poly-morphism for hepatic lipoxygenase (LIPC-480 T) (22),smoking, and poor glycemic control (22,23). A cross-sectional study correlated CAC with coronary arterydisease in 302 men and women with T1DM in thePittsburgh EDC (Epidemiology of Diabetes Complica-tions) Study cohort (mean age 38.1 � 7.8 years). Thatstudy concluded that CAC had an 84% and 71%sensitivity for CAD in men and women, respectively,and a 100% sensitivity for myocardial infarction andobstructive CAD. The study also reported that a CACcutpoint of 400 was the most efficient coronary cal-cium correlate of CAD (20).
The present study did not find an association be-tween the CAC score and the mean or time-weightedHbA1c measurements. Some studies have demon-strated a relationship between diabetes control andatherosclerosis, and others have not (21–24). A recentreport from the Diabetes Prevention Program (inpersons with T2DM) demonstrated no relationshipbetween CAC or CAC severity and HbA1c levels,similar to findings in the current report (24). CACscore categories did not have a cross-sectional asso-ciation with HbA1c levels in the present study(Table 1). The prior DCCT/EDIC paper showed signif-icant associations among various measurements ofHbA1c over DCCT and EDIC with the prevalence ofCAC >0 and of CAC >200 as well as with the log (CAC).
Results for the present study of T1DM are similar tothose in cohorts that included both asymptomatic (25)and symptomatic persons (26), whereby increasingCAC scores were associated with increasing risk ofMACE, and zero scores were generally associated withlow event rates. The event rates among the cohort forthose with zero scores (n ¼ 817 [70.7% of the cohort])were very low at 5 years (2.8%) and at long-termfollow-up (5.6 per 1,000 patient years) for ASCVD.This represents what has been reported as the “powerof zero” and potentially affords patients and physi-cians the potential to avoid more aggressive riskreduction strategies in this very-low-risk cohort.
The present study showed the lack of interactionbetween sex and CAC, suggesting that T1DM seemed

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE:
TIDM, although less well studied in the context of
the presence and outcomes of atherosclerosis,
demonstrates risk of future CVD with coronary
calcium scores similar to those in persons with T2DM.
It is critical to understand the implications for
clinicians, given the increased risk seen with higher
CAC scores in these asymptomatic patients.
TRANSLATIONAL OUTLOOK: Prospective clinical
trials evaluating CV risk and targeting specific
coronary atherosclerotic treatments in TIDM are
necessary to delineate the impact of disease
modifying therapies on clinical outcomes.
Budoff et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CAC and CVD in DCCT/EDIC J U L Y 2 0 1 9 : 1 3 4 1 – 9
1348
to blunt the age differential for the development ofatherosclerosis in men compared to that in women.The EDIC CVD risk factor analyses (2) also suggestedthat sex was not a significant contributor to the finalmultivariate model when adjusted for other riskfactors.
The ascertainment of statin use started in EDICyear 11, approximately 3 years after the CAC mea-surement. After their year 11 visit, an initial CVDevent subsequently occurred in 55 participants, ofwhom 32 (58%) were taking statins at the last EDICvisit prior to the CVD event. Those studies wereconducted prior to more widespread use of statin andangiotensin-converting enzyme inhibitor therapies.Clearly, a randomized trial of statins in persons withTIDM has not been carried out but would be prudentgiven the increased ASCVD risk associated withhigher CAC scores in the present study.
In the current group of participants with TIDM,higher CAC scores were associated with CV events,suggesting that this is an important assessment toolfor determining CV risk in participants with T1DM.Recommendations by the American College of Cardi-ology/American Heart Association (27) alreadyrecommend testing for CAC: “In asymptomatic adultswith diabetes, 40 years of age and older, measure-ment of CAC is reasonable for cardiovascular riskassessment.” This recommendation was based largelyon data from persons with T2DM in which studiesenrolled T2DM participants >40 years of age; thecurrent study also strongly supports this IIA recom-mendation in T1DM participants. In addition, theAmerican Diabetes Association and American HeartAssociation more recently stated that “it is reasonable
to apply the current guidelines for the use of CACassessment for T1DM as recommended for the generalpopulation.” (28). Coronary artery calcium in personswith T1DM can inform health care providers regardingthe management or risk factors for CV disease in pa-tients at risk.
ACKNOWLEDGEMENT The authors thank WanyuHsu, Biostatistics Center, George Washington Uni-versity, Rockville, Maryland, for technical assistancewith data processing.
ADDRESS FOR CORRESPONDENCE: Dr. MatthewBudoff, Division of Cardiology, Los Angeles BiomedicalResearch Institute, 1124 West Carson Street, Torrance,California 90502. E-mail: [email protected].
RE F E RENCE S
1. Secrest AM, Becker DJ, Kelsey SF, LaPorte RE,Orchard TJ. Cause-specific mortality trends in alarge population-based cohort with long-standingchildhood-onset type 1 diabetes. Diabetes 2010;59:3216–22.
2. Nathan DM, Bebu I, Braffett BH, Orchard TJ,Cowie CC, et al., Diabetes Control and Com-plications Trial (DCCT)-Epidemiology of Dia-betes Interventions and Complications (EDIC)Research Group. Risk factors for cardiovasculardisease in type 1 diabetes. Diabetes 2016;65:1370–9.
3. Hecht HS. Coronary artery calcium scanning:past, present, and future. J Am Coll Cardiol Img2015;8:579–96.
4. Coronary artery calcium score prediction of all-cause mortality and cardiovascular events in peo-ple with type 2 diabetes: systematic review andmeta-analysis. BMJ 2013;346:f1654.
5. McClelland RL, Jorgensen NW, Budoff MJ,Blaha MJ, Post WS, Kronmal RA. 10-Year coronaryheart disease risk prediction using coronary arterycalcium and traditional risk factors derivation inthe MESA (Multi-Ethnic Study of Atherosclerosis)with validation in the HNR (Heinz Nixdorf Recall)study and the DHS (Dallas Heart Study). J Am CollCardiol 2015;66:1643–53.
6. Budoff MJ, Yu D, Nasir K, Mehrotra R,Chen L, Takasu J, et al. Diabetes and progres-sion of coronary calcium under the influenceof statin therapy. Am Heart J 2005;149:695–700.
7. Hecht HS, Narula J. Coronary artery calciumscanning in asymptomatic patients with diabetesmellitus: a paradigm shift. J Diabetes 2012;4:342–50.
8. Budoff MJ, Raggi P, Beller GA, Berman DS,Druz RS, Malik S, et al., for the Imaging Council of
the American College of Cardiology. Noninvasivecardiovascular risk assessment of the asymptom-atic diabetic patient: the Imaging Council of theAmerican College of Cardiology. J Am Coll CardiolImg 2016;9:176–92.
9. Burge MR, Eaton RP, Schade DS. The role of acoronary artery calcium scan in type 1 diabetes.Diabetes Technol Ther 2016;18:594–603.
10. DCCT Research Group. The effect of inten-sive treatment of diabetes on the developmentand progression of long-term complications ininsulin-dependent diabetes mellitus. N Engl JMed 1993;329:977–86.
11. DCCT/EDIC Research Group. Epidemiology ofDiabetes Interventions and Complications (EDIC).Design, implementation, and preliminary resultsof a long-term follow-up of the Diabetes Controland Complications Trial cohort. Diabetes Care1999;22:99–111.

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Budoff et al.J U L Y 2 0 1 9 : 1 3 4 1 – 9 CAC and CVD in DCCT/EDIC
1349
12. Cleary PA, Orchard TJ, Genuth S, Wong ND,Detrano R, Backlund JY, et al. The effect ofintensive glycemic treatment on coronary arterycalcification in type 1 diabetic participants of theDiabetes Control and Complications Trial/Epide-miology of Diabetes Interventions and Compli-cations (DCCT/EDIC) study. Diabetes 2006;55:3556–65.
13. DCCT Research Group. The DiabetesControl and Complications Trial (DCCT). Designand methodologic considerations for the feasi-bility phase. Diabetes 1986;35:530–45.
14. Snedecor GW. Statistical Methods. 7th edition.Ames: Iowa State University Press; 1980.
15. Lachin JL, editor. Biostatistical Methods: theAssessment of Relative Risks. 2nd edition. NewYork, NY: John Wiley and Sons, 2011.
16. Kalbfleisch JDPR, editor. The Statistical Anal-ysis of Failure Time Data. 2nd edition. New York,NY: John Wiley and Sons, 2002.
17. Gonen M, Heller G. Concordance probabilityand discriminatory power in proportional hazardsregression. Biometrika 2005;92:965–70.
18. Malik S, Budoff MJ, Blumenthal RS,Bertoni AG, Nasir K, Szklo M, et al. Impact ofsubclinical atherosclerosis on cardiovasculardisease events in individuals with metabolicsyndrome and diabetes: the multi-ethnic study ofatherosclerosis. Diabetes Care 2011;34:2285–90.
19. Malik S, Zhao Y, Budoff MJ, Nasir K,Blumenthal RS, Bertoni AG, et al. Coronary artery
calcium score for long-term risk classification inindividuals with type 2 and metabolic syndromefrom the multi-ethnic study of atherosclerosis.JAMA Cardiol 2017;2:1332–40.
20. Olson JC, Edmundowicz D, Becker DJ,Kuller LH, Orchard TJ. Coronary calcium in adultswith Type 1 diabetes: A stronger correlate ofclinical coronary artery disease in men than inwomen. Diabetes 2000;49:1571–8.
21. Starkman HS, Cable G, Hala V, Hecht H,Donnelly CM. Delineation of prevalence and riskfactors for early coronary artery disease by elec-tron beam computed tomography in young adultswith type 1 diabetes. Diabetes Care 2003;26:433–6.
22. Hokanson JE, Cheng S, Snell-Bergeon JK,Fijal BA, Grow MA, Hung C, et al. A commonpromoter polymorphism in the hepatic lipase gene(LIPC-480C>T) is associated with an increase incoronary calcification in type 1 diabetes. Diabetes2002;51:1208–13.
23. Snell-Bergeon JK, Hokanson JE, Jensen L,MacKenzie T, Kinney G, Dabelea D, et al. Pro-gression of coronary artery calcification in type 1diabetes: the importance of glycemic control.Diabetes Care 2003;26:2923–8.
24. Goldberg RB, Aroda VR, Bluemke DA, Barrett-Connor E, Budoff MJ, Crandall JP, et al. Diabetesprevention program research group. effect oflong-term metformin and lifestyle in the diabetesprevention program and its outcome study on
coronary artery calcium. Circulation 2017;136:52–64.
25. Joshi PH, Blaha MJ, Budoff MJ, Miedema MD,McClelland RL, Lima JAC, et al. The 10-yearprognostic value of zero and minimal CAC. J AmColl Cardiol Img 2017;10:957–8.
26. Budoff MJ, Mayrhofer T, Ferencik M, Bittner D,Lee KL, Lu MT, et al. The prognostic value ofcoronary artery calcium in the PROMISE study.Circulation 2017;136:1993–2005.
27. Greenland P, Alpert JS, Beller GA, Benjamin EJ,Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHAguideline for assessment of cardiovascular risk inasymptomatic adults: a report of the AmericanCollege of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines.J Am Coll Cardiol 2010;56:50–103.
28. de Ferranti SD, de Boer IH, Fonseca V, Fox CS,Golden SH, Lavie CJ, et al. Type 1 diabetes mellitusand cardiovascular disease: a scientific statementfrom the American Heart Association and Amer-ican Diabetes Association. Diabetes Care 2014;37:2843–63.
KEY WORDS cardiovascular disease,coronary artery calcification, major adversecardiovascular event, type 1 diabetes
APPENDIX For a supplemental table, pleasesee the online version of this paper.

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
EDITORIAL COMMENT
Coronary Calcium in Type 1 Diabetes
To Screen or Not to Screen?*Nathan D. Wong, PHD
B ecause atherosclerotic cardiovascular disease(ASCVD) is the leading cause of death in per-sons with type 1 diabetes mellitus (T1DM)
(1), it is crucial that ways to detect those at highestrisk be identified, ideally years before major adversecardiovascular events (MACE) occur. In this issue ofiJACC, Budoff et al. (2) demonstrate the importantprognostic role for coronary artery calcium (CAC) inpredicting future CVD events in persons with T1DM(2) from the well-characterized EDIC (Epidemiologyof Diabetes Interventions and Complications) cohort,a long-term follow-up of the original DCCT (DiabetesControl and Complications Trial), which tested theimpact of intensive glycemic control on microvas-cular and macrovascular outcomes (3). The EDICstudy was the largest prospective cohort of personswith T1DM, with 10 to 13 years of follow-up fromCAC scanning (done at a mean 43 years of age), thatreported on future ASCVD event risks.
SEE PAGE 1341
ISSN 1936-878X/$36.00
*Editorials published in JACC: Cardiovascular Imaging do not necessarily
represent the views of iJACC or the American College of Cardiology.
From the Division of Cardiology, Heart Disease Prevention Program
University of California, Irvine, Irvine, California. Dr. Wong ha
received research support from Amgen, Boehringer Ingelheim, and
Novo Nordisk; and is a consultant for AstraZeneca.
The authors demonstrated a threshold level of CAC of100 or greater for identifying those at increased riskof a first MACE, although those with lower scores stillshowed an increased relationship to the risk of abroader composite endpoint of future cardiovascularevents. Although MACE event risk was only 3% inthose with scores of 0 or 1 to 100, it was 14% in thosewith scores of 101 to 300 and 18% in those with scoresabove 300, with corresponding total CVD event ratesof 6%, 10%, 23%, and 32%, respectively. Although thenumber of MACE and total CVD events providedrelatively reasonable robust estimates, ideally,
,
s
longer-term follow-up will be needed to furthervalidate the stability of those estimates (2).
Prior investigations have demonstrated the prog-nostic significance of CAC for predicting future CVDevents mainly in those with type 2 diabetes mellitus(T2DM) (4,5), including recently with more than 10years of follow-up (6), and previous American Collegeof Cardiology(ACC)/American Heart Association(AHA) guidelines have recommended screening forCAC for further risk stratification in those with dia-betes 40 years of age and older (7), and more recently,the AHA/American Diabetes Association (ADA) havesuggested recommendations for CAC screening in thegeneral population should also apply to those withT1DM (8). Such information can be useful for theclinician in considering or intensifying preventivetherapies such as statins, particularly in youngerpersons in whom assessment of other risk factors maynot offer a definitive recommendation. Although themost recent 2018 cholesterol management guidelines(9) recommend at least moderate intensity statintherapy for all those with diabetes 40 years of age andolder and for those 20 to 39 years of age if certain riskenhancers are present (i.e., diabetes of long duration,defined as $10 years with T2DM or $20 years withT1DM, microalbuminuria or macroalbuminuria,chronic kidney disease with estimated glomerularfiltration rate of <60 ml/min/1.73 m2, retinopathy,neuropathy, or an ankle-brachial index <0.9),consideration is given for a high-intensity statin ifmultiple risk factors are also present, and ezetimibetherapy in addition to maximally tolerated statin ifthe 10-year ASCVD risk is 20% or greater. It is notclear why increased CAC was not noted as a riskenhancer for those with DM in these guidelines, butboth the current paper (2) and those noted abovefocusing on T2DM support the rationale for the use ofCAC as a risk enhancer for the purposes of initiating orintensifying preventive therapies. Clearly, however,at least with higher levels of CAC (above a score of 100)where increased CVD risk is clear in those with T1DM,
https://doi.org/10.1016/j.jcmg.2019.01.016

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 WongJ U L Y 2 0 1 9 : 1 3 5 0 – 2 Editorial Comment
1351
as the results by Budoff et al. (2) suggest, currentguidelines could extend treatment recommendationsto such persons with T1DM, considering an elevatedCAC score as a risk enhancer for such persons, with aneven stronger recommendation if present in youngerpersons with T2DM (e.g., before the age of 40). As theauthors point out, however, a randomized trial ofstatin therapy to demonstrate improved outcomes hasnot been done in a T1DM population (2).
As Budoff et al. (2) show, in those with T1DM whohave a calcium score of 0, a long-term warrantyagainst MACE with very -low event rates extending to10 to 13 years (5.6 per 1,000 person years) for thosewith T1DM in the EDIC cohort, the question arises asto whether statin therapy could be withheld in suchpersons, perhaps at least until other risk enhancers asnoted earlier are present. Although the recent choles-terol guidelines (9) go further to suggest “de-risking”patients with a 0 calcium score for the purposes ofwithholding statin therapy, they exclude those withdiabetes from this recommendation presumablybecause of the high long-term risk in such persons.
The recent positive cardiovascular outcome trialsof sodium-glucose cotransporter-2 inhibitors andglucagon-like peptide-1 receptor agonists (10) haveraised interest in consideration of appropriate pop-ulations of patients for these agents. Although cur-rent guidelines recommend their use only in thosewith established ASCVD and T2DM (10), given thatthese were the patients shown to benefit from theoutcome trials, one could argue whether suchtherapies could also be recommended for higher riskprimary prevention in patients with diabetes, such asthose with significant subclinical atherosclerosis(e.g., with calcium scores of >100 where increasedASCVD risk is clear). Although there are no studies toshow whether such patients may benefit from thesenewer therapies, and Budoff et al. (2) did not find thecurrent HbA1c to be related to the CAC score, of
interest is an earlier publication from the EDIC studythat showed those subjects who were previouslyrandomized to the intensive glycemic therapy groupin the DCCT study actually had less coronary calciumafter the conclusion of the trial than those originallyassigned to the conventional group, with HbA1c levelsassociated with the extent of CAC before, during, andafter the DCCT study (11). Although this does notprove that intensive glycemic control reducesatherosclerosis, it suggests a possible “legacy effect”of less atherosclerosis, consistent with the long-termfollow-up of the DCCT cohort who did in fact showreduced CVD events from intensive glycemic control(12). The cardiovascular and/or atheroprotective ef-fects seen by SGLT2 inhibitors and GLP-1 receptorantagonists, however, are believed to be independentof their fairly modest glucose-lowering effects (10).
Ultimately, the findings of Budoff et al. (2) provideimportant evidence for the significance of CAC forprediction of CVD events now in persons with T1DM,nicely complementing prior studies in those withT2DM and further emphasizing the role of CACscreening for all persons with diabetes in the ASCVDrisk stratification for initiating or intensifying pre-ventive therapy. The early development of CACscreening in those with T1DM, especially if present ata fairly young age (e.g., <40 years of age) shouldtherefore be considered a risk enhancer, warning ofpotentially significant future ASCVD risk that shouldalert the clinician to earlier and more aggressivemanagement of concomitant risk factors, focusing ontherapies with proven CV risk reduction benefit.
ADDRESS FOR CORRESPONDENCE: Dr. Nathan D.Wong, Heart Disease Prevention Program, Division ofCardiology, C240 Medical Sciences, University ofCalifornia, Irvine, California 92697. E-mail: [email protected].
RE F E RENCE S
1. Secrest AM, Becker DJ, Kelsey SF, et al.Cause-specific mortality trends in a largepopulation-based cohort with long-standingchildhood-onset type 1 diabetes. Diabetes2010;59:3216–22.
2. Budoff M, Backlund J-YC, Bluemke DA, et al.The association of coronary artery calcificationwith subsequent incidence of cardiovascular dis-ease in type 1 diabetes: the DCCT/EDIC trials. J AmColl Cardiol Img 2019;12:1341–9.
3. DCCT Research Group. The effect of intensivetreatment of diabetes on the developmentand progression of long-term complications in
insulin-dependent diabetes mellitus. N Engl J Med1993;329:977–86.
4. Becker A, Leber AW, Becker C, et al. Predictivevalue of coronary calcifications for future cardiacevents in asymptomatic patients with diabetesmellitus: a prospective study in 716 patients over8 years. BMC Cardiovasc Disord 2008;8:27.
5. Malik S, Budoff MJ, Blumenthal RS, Bertoni AG,Nasir K, Szklo M, et al. Impact of subclinicalatherosclerosis on cardiovascular disease events inindividuals with metabolic syndrome and diabetes:the Multi-Ethnic Study of Atherosclerosis. Dia-betes Care 2011;34:2285–90.
6. Malik S, Zhao Y, Budoff MJ, Nasir K,Blumenthal RS, Bertoni AG, et al. Coronary arterycalcium score for long-term risk classification inindividuals with type 2 and metabolic syndromefrom the Multi-Ethnic Study of Atherosclerosis.JAMA Cardiol 2017;2:1332–40.
7. Greenland P, Alpert JS, Beller GA,Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010ACCF/AHA guideline for assessment of cardio-vascular risk in asymptomatic adults: a report ofthe American College of Cardiology Foundation/American Heart Association Task Force on Prac-tice Guidelines. J Am Coll Cardiol 2010;56:50–103.

Wong J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 3 5 0 – 2
1352
8. de Ferranti SD, de Boer IH, Fonseca V, Fox CS,Golden SH, Lavie CJ, et al. Type 1 diabetes mellitusand cardiovascular disease: a scientific statementfrom the American Heart Association and Amer-ican Diabetes Association. Diabetes Care 2014;37:2843–63.
9. Grundy SM, Stone NJ, Bailey AL, Beam C,Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of bloodcholesterol. J Am Coll Cardiol 2018 Nov 10 [E-pubahead of print].
10. Das SR, Everett BM, Birtcher KK, Brown JM,Cefalu WT, Januzzi JL Jr., et al. 2018 ACC expert
consensus decision pathway on novel therapies forcardiovascular risk reduction in patients with type 2diabetes and atherosclerotic cardiovascular dis-ease: a report of the American College ofCardiology Task Force on Expert Consensus Deci-sion Pathways. J Am Coll Cardiol 2018;72:3200–23.
11. Cleary PA, Orchard TJ, Genuth S, Wong ND,Detrano R, Backlund JY, et al. The effect ofintensive glycemic treatment on coronary arterycalcification in type 1 diabetic participants of theDiabetes Control and Complications Trial/Epide-miology of Diabetes Interventions and Complica-tions (DCCT/EDIC) study. Diabetes 2006;55:3556–65.
12. Nathan DM, Cleary PA, Backlund JY,Genuth SM, Lachin JM, Orchard TJ, et al. DiabetesControl and Complications Trial/Epidemiology ofDiabetes Interventions and Complications (DCCT/EDIC) study research group. intensive diabetestreatment and cardiovascular disease in patientswith type 1 diabetes. N Engl J Med 2005;353:2643–53.
KEY WORDS cardiovascular disease, coronaryartery calcium, major adverse cardiovascularevent, type 1 diabetes

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
ORIGINAL RESEARCH
Plaque Morphology as Predictor ofLate Plaque Events in Patients WithAsymptomatic Type 2 Diabetes
A Long-Term Observational StudyDavid A. Halon, MB CHB,a Idit Lavi, MPH,b Ofra Barnett-Griness, PHD,b Ronen Rubinshtein, MD,c Barak Zafrir, MD,d
Mali Azencot, PHD,a Basil S. Lewis, MDa,c
ABSTRACT
ISS
Fro
Me
Te
Ca
Stu
Ma
OBJECTIVES The authors used coronary computed tomography angiography (CTA) to determine plaque characteristics
predicting individual late plaque events precipitating acute coronary syndromes (ACS) in a cohort of asymptomatic
type 2 diabetic patients.
BACKGROUND In patients with coronary artery disease, CTA plaque characteristics may predict mid-term patient
events.
METHODS Asymptomatic patients with diabetes 55 to 74 years of age with no history of coronary artery disease
(N ¼ 630) underwent baseline 64-slice CTA and detailed plaque level analysis. All subsequent clinical events were
recorded and adjudicated. In patients who developed ACS, culprit plaque was identified at invasive angiography and its
precursor located on the baseline CTA. Plaque characteristics predicting an ACS-associated culprit plaque event were
analyzed by time to event accounting for inpatient clustering of plaques and competing events.
RESULTS Among 2,242 plaques in 499 subjects, 24 ACS culprit plaques were identified in 24 subjects during median
follow-up of 9.2 years (interquartile range: 8.4 to 9.8 years). Plaque volume (upper vs. lower quartile hazard ratio [HR]:
6.9; 95% confidence interval [CI]: 1.6 to 30.8; p ¼ 0.011), percentage of low-density plaque content <50 Hounsfield
units (HR: 14.2; 95% CI: 1.9 to 108; p ¼ 0.010), and mild plaque calcification (HR vs. all other plaques 3.3 [95% CI: 1.5 to
7.3]; p ¼ 0.004) predicted plaque events univariately and after adjustment by clinical risk score. A culprit plaque
event occurred in 13 of 376 (3.5%) high-risk plaques (HRP) (plaques with $2 risk predictors) versus 11 of 1,866 (0.6%)
in non-HRPs (p < 0.0001), at 12 of 343 (3.5%) stenotic sites ($50%) versus 12 of 1,899 (0.6%) nonstenotic sites
(p < 0.0001) and in 7 of 131 (5.3%) HRP with stenosis (p < 0.0001 vs. all others). In 130 (20.6%) subjects, no coronary
plaque was present on baseline CTA.
CONCLUSIONS In asymptomatic patients with type 2 diabetes, CTA plaque volume, percent low-density plaque content,
and mild calcification predicted late plaque events. The additional presence of luminal stenosis increased the probability of
an acute event. (J Am Coll Cardiol Img 2019;12:1353–63) © 2019 by the American College of Cardiology Foundation.
D iabetes mellitus (DM) is an independentrisk factor for adverse atheroscleroticevents (1). Several studies have examined
the additional risk in this population afforded by an
N 1936-878X/$36.00
m the aCardiovascular Clinical Research Institute, Lady Davis Carmel Med
dicine and Epidemiology, Lady Davis Carmel Medical Center, Haifa, Isra
chnion-Israel Institute of Technology, Haifa, Israel; and the dPreventive
rmel Medical Center, Haifa, Israel. This study was supported by a rese
dy of Diabetes. The authors have reported that they have no relationship
nuscript received January 25, 2018; accepted February 23, 2018.
elevated coronary artery calcium (CAC) score andthe additional prognostic information obtained bycoronary arterial findings on cardiac computed to-mography angiography (CTA) (2–5). The composition
https://doi.org/10.1016/j.jcmg.2018.02.025
ical Center, Haifa, Israel; bDepartment of Community
el; cRuth and Bruce Rappaport School of Medicine
Cardiology and Rehabilitation Service, Lady Davis
arch grant from the European Foundation for the
s relevant to the contents of this paper to disclose.

ABBR EV I A T I ON S
AND ACRONYMS
ACS = acute coronary
syndrome
CABG = coronary artery bypass
grafting
CAC = coronary artery calcium
CAD = coronary artery disease
CI = confidence interval
CTA = computed tomography
angiography
DM = diabetes mellitus
HR = hazard ratio
HRP = high-risk plaque
HU = Hounsfield units
IQR = interquartile range
LDL-C = low-density
lipoprotein cholesterol
PCI = percutaneous coronary
intervention
Halon et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Coronary Plaque Outcomes in Patients With Diabetes J U L Y 2 0 1 9 : 1 3 5 3 – 6 3
1354
of coronary arterial plaques in patients withdiabetes is different to that of patientswithout diabetes and may be responsible forincreased risk in this population (6).Although plaque characteristics have beenrelated to outcome events in some patientpopulations (7–10), there are few long-termdata relating baseline CTA plaque character-istics and morphology to a late plaque event(causing an acute coronary syndrome) in aninitially asymptomatic diabetic populationwith no clinical history of coronary arterydisease (CAD).
SEE PAGE 1364
METHODS
STUDY POPULATION. The study cohort of630 subjects was derived as detailed inFigure 1. Eligible subjects had type 2 DM, age55 to 74 years of age, no history of CAD, and at
least 1 additional cardiovascular risk factor: DMdiagnosed $5 years previously; systemic hyperten-sion; current smoking; age>60 years; family history ofCAD in a first-degree relative <55 years of age; pe-ripheral, cerebral, or carotid vascular disease; diabeticretinopathy; neuropathy; or albuminuria. Ethicsapproval was obtained from the Ethics Committee ofthe Lady Davis Carmel Medical Center and all patientsprovided written informed consent before study in-clusion. Exclusion criteria were serum creatinine >1.4mg/100 ml, allergy to contrast media, and chronicatrial fibrillation. Baseline clinical risk was assessedusing the UKPDS (United Kingdom Prospective Dia-betes Study) coronary heart disease risk score. Treat-ing physicians and study participants received anassessment of risk (below average, average, or aboveaverage) based on the CAC score. If high-grade stenosisof the left main or very proximal left anteriordescending arteries was diagnosed, the subject wasreferred to an independent cardiologist who assessedthe subjects by standardmeans (generally exercise andor nuclear stress testing) without specific knowledgeof the CTA findings.
CARDIAC SCANNING PARAMETERS. CTA was per-formed between October 2006 and October 2008 witha 64-slice scanner (Brilliance CT, Philips Healthcare,Cleveland, Ohio) using a spiral, retrospective,electrocardiograph-gated protocol. Beta blockers andsublingual nitrates were used routinely. Details of thescanning procedure have previously been described(11). Two slightly different concentrations of intra-venous contrast agent were used (370 mg iodine/ml in
54% subjects; 350 mg iodine/ml in 46% subjects). Thedose-length product was 779 � 201 mGy/cm equiva-lent to 13.2 � 3.4 mSv.
CORONARY ARTERY AND PLAQUE ANALYSIS. Allscans were examined in axial, multiplanar reformatand short-axis cross-sectional views by 1 viewer. Asecond viewer examined a sample of 100 plaques in30 subjects. Window settings were adjusted by theoperator to obtain the best differentiation betweenplaque, surrounding tissue, and vessel lumen and todifferentiate between intraplaque densities. Plaquewas defined as any extraluminal density that could beclearly assigned to the coronary arterial wall. Plaqueposition and length were defined along the arterialcenterline. Dedicated cardiac analysis software with aplaque analysis application (Cardiac Viewer andComprehensive Cardiac Analysis, Extended BrillianceWorkspace V4.0.2, Philips Healthcare) was used forplaque definition and analysis with manual adjust-ment as required. Only studies with good or adequatedelineation of arterial borders were used for analysis.
Plaque and artery volumes were calculated for eachplaque individually. Plaque burden was calculated foreach plaque as the volume of plaque divided by thetotal volume of the same section of coronary arterycontaining the plaque. Area remodeling wasmeasured as maximal cross-sectional artery area atplaque/plaque-free cross-sectional area, sited proxi-mally whenever possible. Bifurcations were assessedby the Medina classification (12). We analyzed bi-furcations in which plaque involved all aspects of thebifurcation in relation to all other plaques. Coronarystenosis was assessed visually on a 5-point scale (0 ¼no plaque, 1 ¼ plaque with <25% narrowing, 2 ¼ 25%to 49%, 3 ¼ 50% to 74%, 4 ¼ 75% to 99%, 5 ¼ 100%).Calcification was assessed visually on a 6-point scale(0 ¼ none, 1 ¼ minimal, 2 ¼ greater than minimalbut <50%, 3 ¼ 50% to 70%, 4 ¼ 71% to 94%, 5 ¼ 95% to100%). A graphic representation of the frequencydistribution of the volume and CT density of eachconstituent plaque was presented by the softwareand stored numerically in a data file. To excludeartifact at arterial borders CT densities below –40Hounsfield units (HU) were considered to be fattytissue outside the arterial wall and were excludedfrom analysis (13). Both intrapericardial fat, possiblyrelated to adipose tissue inflammation, and mechan-ical factors related to endothelial shear stress, whichvaries with changing blood flow and stress patternsrelated to the position of plaque and the bendingpattern of the artery, have been shown to predictoutcome events (14,15). We therefore also examined ifplaques facing the pericardium, which are most likely

FIGURE 1 Derivation of the Study Population
Diabetic population in catchment area of healthinsurance group 55-74 y of age = 20,053
No informed consent = 463
CT scans unavailable for analysis = 29
No coronary plaque present = 130
Excluded due to missing CTA data =
=
15
90Excluded due to insufficient qualityfor plaque analysis
====
31061
Excluded prior to CTA:DiedAcute renal failureACSNew malignancy
Excluded:Missed planned clinic visit Known CADRenal failureAllergy to contrast medium Other life threatening disease Type 1 DMNo study entry criteria
661=======
793221
2042
2515
Potential study subjects = 1,247
Provided informed consent = 784
CTA scan performed = 764
CAC analysis performed = 735
CTA suitable for plaque analysis = 630
Consecutive charts pre-screened in diabeticand family practitioner clinics = 3,024
(15.1% of diabetic population)
499 subjects24 culprit plaques
2,218 non-culprit plaques
Culprit plaquenot identified = 1
No revascularization = 439ACS = 24
24 culprit plaques144 non-culprit plaques
Elective revascularization = 36(14 CABG, 25 PCI)
500 study subjects
Follow-Up 8-10 Years
ACS = 25 No ACS = 475
ACS ¼ acute coronary syndrome; CABG ¼ coronary artery bypass grafting; CAC ¼ coronary artery calcium; CAD ¼ coronary artery disease;
CT ¼ computed tomography; CTA ¼ computed tomography angiography; DM ¼ diabetes mellitus; PCI ¼ percutaneous coronary intervention.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Halon et al.J U L Y 2 0 1 9 : 1 3 5 3 – 6 3 Coronary Plaque Outcomes in Patients With Diabetes
1355

TABLE 1 Individual Patient Data for Patients With ACS During Follow-Up
Patient # ACS TypeTime From
CTA to ACS (yrs)SegmentInvolved
Stenosis Gradeon Baseline CTA*
No. of High-RiskPlaque Features†
1 STEMI 0.6 Proximal RCA 3 2
2 NSTEMI 9.7 Proximal LAD 2 1
3 STEMI 3.8 Proximal LAD 4 1
4 STEMI 8.3 Mid-LAD 4 1
5 STEMI 7.8 First diagonal 3 2
6 STEMI 1.0 Mid-LAD 3 3
7 UAP 0.9 Proximal LAD 1 3
8 UAP 6.1 Mid-LAD 2 1
9 NSTEMI 3.8 Mid-RCA 2 0
10 NSTEMI 4.3 LM 2 2
11 STEMI 1.9 Proximal LAD 2 2
12 UAP 0.5 Proximal RCA 3 3
13 UAP 4.4 Mid-RCA 2 3
14 NSTEMI 2.4 Proximal Cx 1 1
15 NSTEMI 0.6 Mid-LAD 3 2
16 NSTEMI 8.5 Proximal LAD 2 2
17 STEMI 7.5 PDA 3 1
18 STEMI 4.8 Proximal LAD 4 3
19 NSTEMI 7.6 Proximal Cx 1 0
20 NSTEMI 2.5 Mid-Cx 3 2
21 STEMI 4.8 Mid-RCA 2 3
22 NSTEMI 3.7 Mid-LAD 3 1
23 NSTEMI 6.6 Mid-Cx 1 0
24 STEMI 1.8 Mid-LAD 2 0
*Grade 1 ¼ 0%–24% luminal narrowing on visual assessment; grade 2 ¼ 25%-49%; grade 3 ¼ 50%–69%; grade4 ¼70%-99%; grade 5 ¼ 100%. †Features considered: upper quartile for plaque volume or percent low-densityplaque (<50 HU) or presence of mild calcification (<50% calcified).
ACS ¼ acute coronary syndrome; CTA ¼ computed tomography angiography; Cx ¼ left circumflex coronaryartery; LAD ¼ left anterior descending coronary artery; LM ¼ left main coronary artery; PDA ¼ posteriordescending branch of the right coronary artery; RCA ¼ right coronary artery; NSTEMI ¼ non–ST-segmentelevation myocardial infarction; STEMI ¼ ST-segment elevation myocardial infarction; UAP ¼ unstable anginapectoris.
Halon et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Coronary Plaque Outcomes in Patients With Diabetes J U L Y 2 0 1 9 : 1 3 5 3 – 6 3
1356
to be in immediate proximity to overlying fat or pla-ques on the inner or outer curvatures of the artery,were more likely to be related to events. Interobservervariation was examined in 100 individual coronaryplaques in 30 patients following resegmentation, andmoderate correlation was previously reported (11).
FOLLOW-UP. All acute coronary syndrome (ACS)events were identified using an electronic databaseencompassing all national hospitalizations and labo-ratory investigations for the health maintenance or-ganization to which all study subjects belonged. Allevents were adjudicated according to pre-definedcriteria by an independent adjudication committeepresented with all current clinical and laboratory datawhile blinded to baseline CAC and CTA data. Deathswere identified from a national registry of deaths.Patients with ACS underwent invasive angiography atthe presenting hospital; the angiographic film wasobtained by the study center. The culprit plaque wasidentified on the angiographic film with the aid ofclinical data as necessary and on the baseline CTA
with the aid of anatomic landmarks. Plaques under-going elective percutaneous intervention (PCI) and allplaques after coronary artery bypass surgery (CABG)were censored at this time.
STATISTICAL ANALYSIS. Statistical Analysis Soft-ware, version 9.4 (SAS Institute, Cary, North Car-olina), was used for most statistical analyses.Categorical variables are presented as numbers andpercentages and continuous variables as mean � SDor median (interquartile range [IQR]). Time to aculprit plaque event was estimated by the cumulativeincidence function and elective revascularization anddeath before an event were considered as competingevents. Cumulative incidence function curves werecompared by the method of Fine and Gray (16). Theassociation between study variables and time to aculprit plaque event was evaluated with the use ofcause-specific hazard ratios (HR) and 95% confidenceintervals (CI), estimated by the Cox proportionalhazards model with adjusted standard errors to ac-count for correlations induced by clustering of pla-ques within patients (SAS PHREG procedure,sandwich formula). A nested, matched, case-controlsensitivity analysis was conducted in ACS patients(24 culprit, 144 nonculprit plaques) in which eachnonculprit plaque served as a “control” for a culpritplaque. Conditional logistic regression was used toassess association between study variables and culpritplaque events (IBM SPSS, version 24). All p values are2-tailed and level of significance was 0.05.
RESULTS
In 130 of 630 subjects (20.6%), no coronary plaquewas present; these were excluded from the currentanalysis (Figure 1). These subjects suffered no ACSevents throughout the follow-up period. The medianplaque follow-up was 9.2 years (IQR: 8.4 to 9.8 years)and ACS events were identified following eventadjudication in 25 patients. A single culprit plaquewas identified on coronary angiography in 24 pa-tients, whereas in 1 patient with severe multivesseldisease a culprit plaque could not be identified. Inaddition to 24 culprit plaques, these ACS patients had144 nonculprit plaques on the baseline CTA. In thetotal cohort of 499 subjects, 2,242 plaques wereidentified on the baseline CTA. In 36 patients withoutACS, an elective revascularization procedure wasperformed (14 CABG, 25 PCI) at a mean of 4.1 � 2.9years after CTA (Figure 1). The type of ACS event, itstiming in relation to the baseline CTA, stenosis gradeon baseline CTA, and the number of high-risk plaquecharacteristics are tabulated in Table 1. Clinical char-acteristics and laboratory data of subjects at study

TABLE 2 Clinical and Laboratory Characteristics of Patients With and Without
Subsequent ACS
ACS(N ¼ 24)
No ACS(N ¼ 475) p Value
Age, yrs 63.2 � 5.5 64.0 � 5.3 0.45
Male 17 (70.8) 252 (53.3) 0.092
BMI, kg/m2 28.6 � 3.9 29.0 � 4.7 0.66
Duration DM, yrs 12.4 � 9.4 10.4 � 7.6 0.23
Hypertension 16 (66.7) 322 (67.8) 0.91
Smoking, pack-yrs 13.3 � 19.0 15.8 (24.6) 0.63
UKPDS risk score 20.5 � 10.3 19.0 � 11.5 0.54
HbA1c (%) at baseline 8.0 � 1.8 7.4 � 1.5 0.105
HbA1c (%) at ACS or follow-up 7.4 � 1.5 7.5 � 1.4 0.615
Creatinine clearance, ml/min/1.73 m2 85.5 � 19.5 86.9 � 19.0 0.75
Hypoglycemic and lipid-lowering therapy
Insulin treated 6 (25.0) 100 (21.1) 0.65
Insulin treated before ACS 9 (37.5) 902 (40.7) 0.75
Number of hypoglycemic drugsat study entry
0 1 (4.2) 52 (10.9)
1 11 (45.8) 179 (37.7)
2 9 (37.5) 168 (35.4)
3 3 (12.5) 73 (15.4)
4 0 (0) 3 (0.6) 0.951
Metformin at baseline 20 (83.3) 368 (77.4) 0.500
Statin treated at baseline 18 (75) 349 (73.5) 0.816
Statin treated at follow-up 18 (78.3)* 379 (84.2) 0.45
Plasma lipids
Cholesterol at baseline 186.7 � 43.9 178.9 � 36.0 0.307
Cholesterol at ACS or follow-up 154.5 � 46.8 153.7 � 37.9 0.923
HDL-C at baseline 46.6 � 10.9 47.0 � 11 0.843
HDL-C at ACS or follow-up 41.0 � 11.9 46.7 � 17.5 0.107
TG at baseline 192.3 � 189.9 173.0 � 124.7 0.623
TG at ACS or follow-up 181.7 � 193.8 146.7 � 82.1 0.387
LDL-C at baseline† 105.4 � 28.9 97.5 � 28.6 0.207
LDL-C <70 mg/dl at baseline 0 66 (13.9) 0.050
LDL-C at ACS or follow-up 79.8 � 30.6 79.2 � 34.5 0.930
Non–HDL-C at baseline 140 � 40 131 � 36 0.24
Non-HDL at ACS or follow-up 113.5 � 44.0 106.9 � 37.1 0.382
Values are mean � SD or n (%). *Some missing data. †Not calculated in 3 ACS and 71 non-ACS subjects at baselineand in 2 ACS and 30 non-ACS subjects at follow-up or ACS because of TG >400 mg/dl.
ACS ¼ acute coronary syndrome; BMI ¼ body mass index; DM ¼ diabetes mellitus; HbA1c ¼ hemoglobin A1c;HDL-C ¼ high-density lipoprotein cholesterol; LDL-C ¼ low-density lipoprotein cholesterol; TG ¼ triglycerides;UKPDS ¼ United Kingdom Prospective Diabetes Study.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Halon et al.J U L Y 2 0 1 9 : 1 3 5 3 – 6 3 Coronary Plaque Outcomes in Patients With Diabetes
1357
entry and at the time of ACS are listed in Table 2.Findings were mostly similar in the ACS and non-ACScohorts, but no subject in the ACS cohort had abaseline low density lipoprotein cholesterol (LDL-C)level <70 mg/dl in contrast to 66 (13.9%) in the non-ACS cohort (p ¼ 0.050). In contrast to this, we founda clear relationship between a low-density plaquevolume >10% of total plaque (density <50 HU) andplasma lipid levels (LDL-C: 99.7 � 31.1 vs. 96.5 � 27.3,p ¼ 0.012; high-density lipoprotein cholesterol:44.8 � 10.4 vs. 48.1 � 11.1, p < 0.0001; non–high-density lipoprotein cholesterol: 135.1 � 39.0 vs.129.6 � 35.5, p ¼ 0.001).
Plaque variables examined for prediction of ACSculprit plaque are shown in Table 3. Data are providedseparately for the entire plaque and for the maximalplaque cross-section. The most prominent predictorsof ACS culprit plaque were larger plaque volume,percent low density plaque content (Figure 2), andmild calcification on visual assessment (Figure 3).Mild plaque calcification was associated with moreculprit plaques, whereas heavy plaque calcificationwas a stabilizing factor. High-risk plaque (HRP) wasdesignated as plaque with any 2 of the previouslymentioned 3 high-risk characteristics. A culprit pla-que ACS event occurred in 13 of 376 (3.5%) HRPs andin 11 of 1,866 (0.6%) non-HRPs (p < 0.0001). The cu-mulative incidence of events increased with thenumber of high-risk characteristics (Figure 2).Luminal stenosis was also a predictor of a plaqueevent, with the latter occurring in 11 of 341 (3.2%) ofstenoses ($50%) and in 13 of 1,901 (0.7%) withoutstenosis (p < 0.0001). In the presence of HRP andstenosis (N ¼ 131) culprit plaque events occurred in 7(5.3%) (p < 0.0001 vs. all other plaques) (Figure 2). Inaddition, visual assessment demonstrated that pla-ques involving bifurcations, involving that portion ofthe artery facing the pericardium, or causing luminalstenosis were more likely to develop into culprits(Table 3). The prevalence, HRs, and test characteris-tics for combinations of predictors of culprit plaqueare shown in Figure 4. Despite the high HR of variousplaque characteristics for an ACS culprit plaqueevent, the positive predictive value of any individualor combination of characteristics remained lowbecause of the very large number of stable plaquesand small number of culprits.
MAXIMAL PLAQUE CROSS-SECTION. Findings formaximal cross-section of plaque were qualitativelysimilar to those for the total plaque. In addition,circumferential plaque extent and plaque eccentricityat this site predicted culprit plaque outcomes(Table 3). The remodeling index was numerically
higher in culprit than nonculprit plaques but notsignificantly different.
ADJUSTMENT FOR RISK FACTORS. An adjustmentfor patient risk factors was made in a model includingthe UKPDS risk score in addition to plaque volume,percent low density plaque, and mild plaque calcifi-cation. The latter 3 variables were independent pre-dictors of a culprit plaque outcome (plaque volume:p ¼ 0.0007 [HR: 1.03; 95% CI: 1.01 to 1.04)/10 mm3];percent low-density content <50 HU: p ¼ 0.003 [HR:1.4; 95% CI: 1.1 to 1.7)/10%]; mild plaque calcification:p ¼ 0.022 [HR: 2.6; 95% CI: 1.1 to 5.8]).

TABLE 3 Predictors of Culprit Plaque
Culprit(n ¼ 24,
24 Plaques)
Nonculprit(n ¼ 475,
2,218 Plaques)
HR for Plaque Event*
HR* p Value*
Entire plaque
Plaque length, mm 18.1 (9.5–31.2) 8.3 (4.8–15.4) 7.6 (1.7–33.4) 0.007
Plaque volume, mm3 108.5 (42.6–194.2) 44.6 (23.2–94.3) 6.9 (1.6–30.8) 0.011
Plaque burden, %† 57.3 (47.1–64.3) 48.7 (37.2–60.7) 3.4 (0.91–12.4) 0.068
Min lumen area, mm2 1.8 (1.4–3.0) 2.9 (1.5–5.3) 0.24 (0.05–1.2) 0.079
Distance from aorta, mm‡ 23.6 (13.5–46.5) 26.6 (13.3–46.8) 0.27 (0.08–0.95) 0.042
Mean plaque density, HU 184.7 (134.5–313.1) 289 (206–371) 0.31 (0.10–0.94) 0.037
Plaque <30 HU, mm3 11.2 (3.4–23.5) 2.0 (0.66–5.7) 7.3 (1.7–32.3) 0.009
Plaque <30 HU, % 9.0 (4.1–17.5) 4.4 (2.1–8.1) 14.3 (1.9–109) 0.010
Plaque <50 HU, mm3 16.0 (4.8–35.7) 3.2 (1.2–8.9) 7.3 (1.7–32.2) 0.010
Plaque <50 HU, % 13.6 (8.3–25.7) 6.9 (3.7–12.5) 14.2 (1.9–108) 0.010
Low density plaque, #50 HU $10% of total plaque 15 (62.5) 735 (33.1) 3.4 (1.5–7.7) 0.004
Low density plaque, #50 HU $20% of total plaque 8 (33.3) 258 (11.6) 3.9 (1.6–9.0) 0.002
Plaque <150 HU, mm3 47.5 (21.3–102.6) 13.2 (5.7–30.4) 7.9 (1.8–34.8) 0.006
Plaque <150 HU, % 50.4 (29.1–63.3) 28.2 (18.6–43.4) 14.2 (1.9–107) 0.010
Mild plaque calcification <50%§ 12 (50.0) 514 (23.2) 3.3 (1.5–7.2) 0.003
Plaque-artery relations
Stenosis $50%§ 11 (45.8) 330 (14.9) 5.3 (2.4–11.7) <0.0001
Plaque facing myocardiumk 18 (75.0) 930 (41.9) 2.2 (0.89–5.7) .090
Plaque facing pericardiumk 18 (75.0) 1137 (51.3) 2.9 (1.2–7.5) 0.023
Plaque facing myocardium and pericardium 12 (50) 583 (26.3) 3.0 (1.3–6.7) 0.008
Plaque includes inner curve of artery¶ 22 (91.7) 1645 (75.4) 3.5 (0.83–15.1) 0.088
Plaque includes outer curve of artery¶ 14 (58.3) 1197 (54.8) 1.2 (0.55–2.8) 0.606
plaque includes both inner and outer curves¶ 12 (50) 721 (33.0) 2.2 (0.96–4.8) 0.063
True bifurcation (vs. all other plaques)# 12 (50) 473 (21.3) 3.8 (1.7–8.5) 0.001
Maximal plaque X-section
Plaque area, mm2 9.7 (6.2–15.5) 8.1 (5.7–11.8) 1.8 (0.52–6.1) 0.363
Plaque burden, %† 73.4 (60.3–83.0) 65.8 (50.8–79.4) 9.2 (1.2–72.9) 0.035
Lumen area at maximal plaque, mm2 3.0 (2.2–5.2) 3.8 (2.1–6.4) 0.18 (0.02–1.5) 0.113
Distance from aorta, mm 29.8 (25.9–49.6) 32.6 (19.3–51.6) 0.56 (0.07–2.3) 0.401
Mean plaque density, HU 219 (132–387) 330 (213–433) 0.42 (0.15–1.2) 0.098
Plaque <30 HU, mm3** 0.35 (0.07–0.89) 0.13, (0.04–0.32) 3.0 (0.98–9.5) 0.055
Plaque <30 HU, % 10.5 (1.9–19.7) 3.9 (1.4–9.0) 2.2 (0.82–5.7) 0.119
Plaque <50 HU, mm3 0.51 (0.10–1.3) 0.21 (0.08–0.50) 4.1 (1.2–14.4) 0.028
Plaque <50 HU, % 15.4 (3.9–28.7) 6.3 (2.6–13.3) 3.3 (1.1–10.0) 0.038
Plaque <150, mm3 1.4 (0.58–3.3) 0.80 (0.43–1.6) 3.4 (0.94–12.5) 0.062
Plaque <150 HU, % 43.1 (14.8–64.1) 24.2 (14.5–41.0) 2.0 (0.75–5.3) 0.162
Plaque circumferential extent 300 (30–360) 210 (180–300) 8.1 (1.1–61.0) 0.043
Plaque eccentricity†† 0.87 (0.73–0.91) 0.90 (0.86–0.93) 0.26 (0.07–0.93) 0.038
Arterial remodelingkk 1.7 (1.3–2.2) 1.5 (1.2–1.8) 2.6 (0.82–8.5) 0.104
Values are median (IQR) or n (%). *For continuous variables, HRs and p values are for upper versus lower quartiles. †Calculated as percentage plaque volume/total arterialvolume along length of plaque. ‡Measured to proximal border of plaque. §Visual analysis. kAt least part of plaque facing myocardium or pericardium, respectively. ¶Notassessed for 6 nonculprit plaques in straight portion of artery. Percentages are of plaques assessed. #Medina type 3 (plaque proximal, directly opposite, and distal to sidebranch) versus all others. **The cross section has a patient-specific slice thickness providing a volume rather than cross-sectional area of plaque. ††Calculated as 1 – (minimalplaque thickness/maximal plaque thickness). kkCross-sectional area of artery at maximal plaque area/proximal arterial reference area.
HR ¼ hazard ratio; HU ¼ Hounsfield units.
Halon et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Coronary Plaque Outcomes in Patients With Diabetes J U L Y 2 0 1 9 : 1 3 5 3 – 6 3
1358
ADDITIONAL FINDINGS. Two different iodine con-centrations of contrast agents were used for thebaseline CTA (350 and 370 mg iodine/ml). Meanenhancement of the left main and proximal 25 crosssections of the left anterior descending coronaryarteries in subjects without coronary plaque was 359� 62 HU versus 371 � 68 HU, respectively; p ¼ 0.081.
The volume and percentage content of low-densityplaque <30 HU and <50 HU were on average 16%less with the lower iodine concentration (p ¼ 0.002and 0.004, respectively); however, the iodineconcentration of the contrast agent was not apredictor of culprit plaque on univariate analysis(p ¼ 0.33).

FIGURE 2 ACS Culprit Plaque Events
High Risk Features 0 1 2 3
3.0
2.5
2.0
Cum
ulat
ive
Inci
denc
e (%
Pla
ques
)
1.5
1.0
0.5
0.0
0 1
p = 0.017
2 3 4 5Follow-Up (Years)
A
6 7 8 9
Q4
Q2Q3
Q1
10
Q4
Q3
Q2
Q1
3.0
2.5
2.0
Cum
ulat
ive
Inci
denc
e (%
Pla
ques
)
1.5
1.0
0.5
0.0
0 1
p = 0.002
2 3 4 5Follow-Up (Years)
B
6 7 8 9 10
3
2
1
0
7.0
6.0
5.0
Cum
ulat
ive
Inci
denc
e (%
Pla
ques
)
4.0
3.0
2.0
1.0
0.0
0 1
p < 0.001
2 3 4 5Follow-Up (Years)
C
6 7 8 9 10
HRP + Stenosis +
HRP + Stenosis -
HRP - Stenosis +
HRP - Stenosis -
6.0
5.0
2.0
Cum
ulat
ive
Inci
denc
e (%
Pla
ques
)
3.0
2.0
1.0
0.0
0 1
p < 0.001
2 3 4 5Follow-Up (Years)
D
6 7 8 9 10
Cumulative incidence of events in relation to (A) quartiles of plaque volume. (B) Quartiles of percentage low-density plaque content <50 Hounsfield units. (C) Number
of high-risk plaque characteristics present (none, plaque volume, percentage low-density content, mild calcification). (D) Combinations of HRP ($2 HRP character-
istics) and luminal stenosis. ACS ¼ acute coronary syndrome; HRP ¼ high-risk plaque; Q1–Q4 ¼ first to fourth quartiles.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Halon et al.J U L Y 2 0 1 9 : 1 3 5 3 – 6 3 Coronary Plaque Outcomes in Patients With Diabetes
1359
We performed a sensitivity analysis by exclusion ofsmall-volume, heavily calcified plaques. Plaques$70% calcified by visual analysis (grade 3 to 4)(Figure 4) and plaques in the lowest quartile of volumewere both sequentially excluded. Excluding smallvolume plaques, plaque volume (p ¼ 0.001), percentcontent <30 HU (p < 0.0001), and percent content <50HU (p < 0.0001) remained significant predictors ofplaque outcome. Excluding heavily calcified plaques,plaque volume (p < 0.001), percent content <30 HU,
and <50 HU (p ¼ 0.006 for both) remained significantpredictors and excluding both small volume andheavily calcified plaques, plaque volume (p ¼ 0.005),percent content <30 HU (p ¼ 0.006) and percentcontent <50 HU (p ¼ 0.005) remained significant pre-dictors of culprit plaque. In addition, we examinedpredictors of culprit plaque in the 24 ACS patientswith 168 plaques that acted as their own controlsfor patient-related variables and found similarplaque-related outcome predictors (Table 4).

FIGURE 3 Culprit Plaque in Relation to Baseline Calcium Grade
% C
ulpr
it Pl
aque
s
1.5
1.0
0.5
2.5
2.0
3.0
0.00 1 52 3 4
207CAC gradeN plaques 203 393323 516 599
CAC grade 1-2 vsall other grades p = 0.003
The proportion of plaques at each baseline CTA calcium grade that became late culprit
plaques is shown. Plaques with mild calcification were most likely to become culprit
plaques, whereas plaques at high calcium grades were likely to remain stable. Abbrevi-
ation as in Figure 1. For definition of calcium grades, see the Methods section in text.
CAC ¼ coronary artery calcium; CTA ¼ computed tomography angiography.
Halon et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Coronary Plaque Outcomes in Patients With Diabetes J U L Y 2 0 1 9 : 1 3 5 3 – 6 3
1360
DISCUSSION
This study showed that in this initially asymptom-atic diabetic patient cohort, most plaques leading tolate clinical events had at least 1 HRP characteristicon baseline CTA and in 54% of cases 2 HRP char-acteristics were present. Nearly one-half of theculprit plaques were associated with a $50%luminal stenosis on the baseline CTA (Table 2). Thetime to a plaque event was often prolonged (median4.0; range 0.5 to 9.7 years), attesting to the chro-nicity of atherosclerotic CAD with a low individualplaque event rate in this asymptomatic population(Figure 2).
Although multivessel coronary arterial plaquewas common, totally plaque-free arteries werefound on baseline CTA in an important 20% sub-group of patients, attesting to the heterogeneity ofcoronary arterial findings in patients with type 2diabetes. Subjects without coronary plaque wereexcluded from the present analysis. Quantitativeanalysis showed that larger volume plaques,particularly those with a greater low-density con-tent and mild calcification, were the most likely tobecome culprit ACS plaques over the following 8 to10 years; however, the vast majority of coronaryplaques were not involved in an acute clinical eventover the follow-up period. Thus despite a high HRof the designated HRP for plaque events, the
positive predictive value of a specified HRPremained low (around 5% over 8 to 10 years)(Figure 4), highlighting the improbability that indi-vidual plaque interventions based on CTA criteriawould be of prophylactic benefit. Studies in patientswithout diabetes have demonstrated similar plaquecharacteristics acutely and at mid-term outcomes(7–10,17). A recent study examining combined pa-tient outcomes in asymptomatic patients with dia-betes reported two-thirds of patient events amongthose with CTA defined obstructive disease (2).
Clinical data, particularly control of diabetes andplasma lipids, were previously correlated both withplaque characteristics and outcome events (11,18). Inview of the limited number of events in the currentstudy, we could only show a correlation of ACS ofborderline significance with baseline LDL-C levels(Table 2); however, we have reported a clear correla-tion between baseline plasma lipids and extent oflow-density plaque.
In the current study, identification of plaqueevents was based on patient presentation with ACS.Silent plaque events may occur without clinicalconsequences because of dissolution of non-obstructive plaque-associated thrombus or intra-plaque hemorrhage with plaque healing. The lattermay lead to increase in plaque size and additionalluminal stenosis (19). The determinants of progres-sion to a clinically recognizable event may dependnot only on plaque characteristics, but also theextent of the prothrombotic milieu, arterial tone orspasm, plaque and arterial geometry, and flowcharacteristics at the time of a localized plaqueevent as well as the presence of a recruitablecollateral circulation (20,21). We found that plaquefacing the pericardium, and therefore more likely tobe in intimate contact with intrapericardial lipid,was more likely to become an ACS plaque. Therelation of intrapericardial lipid volume andinflammation with outcomes has been reported (14).We found only a tendency to more ACS from pla-ques on the inner surface of arterial bends wherelower endothelial shear stress is expected (15).
Low-density plaque on CTA represents lipid-richplaque (17). We elected to use a primary cutoffvalue <50 HU in our low density definition. Sinceothers have used various values (9,22) we have alsoprovided additional data with a cutoff <30 HU. Thevolume of low-density plaque identified varies withscanning protocols, the cutoff level used to definelow-density plaque and the iodine content of thecontrast medium, but the significance of the find-ings was unchanged whichever cutoff was chosenand for both contrast agent concentrations.

FIGURE 4 Test Characteristics for Combinations of Plaque Event PredictorsCu
lprit
Pla
que
Even
ts (%
Pla
ques
)
3.0
2.0
1.0
5.0
4.0
7.0
6.0
0.01 HRA Q4 Volume +
Low Density2 HRA +Stenosis
All 3 HRA All 3 HRA +Stenosis
2 HRA
4.6 (1.6-13.5) 8.3 (3.7-18.7) 7.7 (3.2-18.6) 8.7 (2.6-29.3)8.1 (3.2-20.5)6.1 (2.7-13.6)52.1 8.6 5.8 2.14.416.883.3 41.7 29.2 12.525.054.248.2 91.7 94.4 98.195.983.61.7 5.2 5.3 6.56.13.5
99.6 99.3 99.3 99.099.299.448.6 91.2 93.7 97.195.183.3
0.005
Hazard ratioPrevalence (%)SensitivitySpecificityPPVNPVPAP-value < 0.0001 < 0.0001 < 0.0005< 0.0001< 0.0001
% Culprit Plaque Events without Risk Attribute% Culprit Plaque Events with Risk Attribute
HRA ¼ high-risk attribute; NPV ¼ negative predictive value; PA ¼ predictive accuracy; PPV ¼ positive predictive value.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Halon et al.J U L Y 2 0 1 9 : 1 3 5 3 – 6 3 Coronary Plaque Outcomes in Patients With Diabetes
1361
Plaques in close approximation to pericardial fatmay be more susceptible to localized pro-inflammatory influences (13), and we found that pla-que on the pericardial side of the artery, in proximityto intrapericardial lipid, was more likely to becomeculprit. Plaques at sites of coronary bifurcations werealso more likely to become culprit lesions. Hemody-namic, geometric, and compositional factors arerelated to the increased plaque prevalence, largervolume, and more rapid progression at these sites(23,24). Whereas a higher Agatston CAC score is apredictor of coronary events, this appears to be basedon the volume component of the score, whereas moredense calcium is a protective factor (25). At the levelof the individual plaque, mild or spotty calcification isa predictor of adverse outcome, whereas heavycalcification is protective (25,26).
We prospectively selected maximal plaque cross-sections for special analysis and found them to beless predictive than data obtained from the plaque asa whole. This is in keeping with recent studies thathave shown that the site of plaque rupture at ACSmost frequently occurred proximal to the minimalluminal area and was related to plaque longitudinal
asymmetry and regional distribution of hemody-namic stress (21). In distinction to other studies (9),we did not find positive remodeling to be a significantoutcome predictor. This may be a real finding in thisdiabetic population several years before the acuteevent or alternatively greater positive remodeling inthe culprit plaques may have been obscured by otherfactors. A proximal reference site only was used in thedata presented, but re-examination of the data usinga mean of proximal and distal references did not alterthe findings (data not shown). Plaque calcification isparticularly prominent in patients with diabetes, andnonculprit lesions were more heavily calcified, whichmay lead to greater blooming of the image at the siteof the plaque in nonculprit lesions, thus tending tomask differences in arterial remodeling between sta-ble and culprit plaque sites.
STUDY LIMITATIONS. The number of plaque eventswithin the context of ACS was small (attesting to thelong-term stability of most plaques with currentmedical therapy). The findings were robust becausethey remained significant for different cutoff defini-tions of low-density plaque, when plaques in the

TABLE 4 Predictors of ACS Culprit Plaque (ACS Patient Cohort)
Culprit(N ¼ 24)
Nonculprit(N ¼ 144)
HR for Plaque Event*
HR* p Value*
Entire plaque
Plaque length, mm 18.1 (9.5–31.2) 9.0 (5.2–16.8) 9.2 (1.4–62.1) 0.022
Plaque volume, mm3 108.5 (42.6–194.2) 51.1 (24.1–109.5) 6.1 (1.2–31.0) 0.027
Plaque burden, %† 57.3 (47.1–64.3) 54.4 (39.7–64.1) 2.4 (0.52–10.9) 0.267
Min lumen area, mm2 1.8 (1.4–3.0) 2.4 (1.1–5.0) 0.43 (0.08–2.4) 0.433
Distance from aorta, mm‡ 23.6 (13.5–46.5) 31.4 (14.2–65.6) 0.12 (0.03–0.50) 0.004
Mean plaque density, HU 184.7 (134.5–313.1) 287.5 (189.7–384.7) 0.22 (0.04–1.0) 0.057
Plaque <30 HU, mm3 11.2 (3.4–23.5) 2.2 (0.85–6.3) 9.3 (1.5–59.4) 0.019
Plaque <30 HU, % 9.0 (4.1–17.5) 5.0 (2.8–8.0) 32.0 (2.3–441) 0.010
Plaque <50 HU, mm3 16.0 (4.8–35.7) 3.6 (1.4–9.4) 9.3 (1.5–58.5) 0.017
Plaque <50 HU, % 13.6 (8.3–25.7) 8.1 (4.6–13.0) 45 (2.2–917) 0.013
Low density plaque, #50 HU $10% of total plaque 15 (62.5) 49 (34.0) 4.8 (1.6–14.3) 0.005
Low density plaque, #50 HU $20% of total plaque 8 (33.3) 17 (11.8) 4.6 (1.5–13.8) 0.007
Plaque volume <150 HU, mm3 47.5 (21.3–102.6) 14.8 (6.1–41.1) 10.8 (1.3–91.7) 0.030
Plaque <150 HU, % 50.4 (29.1–63.3) 30.0 (20.7–46.9) 49.8 (2.8–886) 0.008
Mild plaque calcification (<50%)§ 12 (50.0) 35 (24.3) 3.0 (1.1–8.1) 0.029
Plaque-artery relations
Stenosis $50%§ 11 (45.8) 32 (22.2) 3.8 (1.4–10.4) 0.010
Plaque facing myocardiumk 18 (75.0) 94 (65.3) 1.3 (0.50–3.6) 0.554
Plaque facing pericardiumk 18 (75.0) 69 (47.9) 2.8 (1.1–7.6) 0.038
Plaque facing myocardium and pericardium 12 (50) 41 (28.5) 2.3 (0.88–5.8) 0.090
Plaque includes inner curve of artery¶ 22 (91.7) 106 (76.8) 3.3 (0.73–15.1) 0.121
Plaque includes outer curve of artery¶ 14 (58.3) 78 (56.5) 1.0 (0.41–2.6) 0.947
plaque includes both inner and outer curves¶ 12 (50) 49 (34.0) 2.0 (0.76–5.0) 0.163
True bifurcation, vs. all others# 12 (50) 26 (18.1) 4.2 (1.7–10.6) 0.002
Maximal plaque X-section
Plaque area, mm2 9.7 (6.2–15.5) 8.4 (5.7–13.0) 2.5 (0.58–10.8) 0.216
Plaque burden, %† 73.4 (60.3–83.0) 73.5 (57.9–84.1) 5.1 (0.54–48.7) 0.156
Lumen area at maximal plaque, mm2 3.0 (2.2–5.2) 3.2 (1.6–5.8) 0.42 (0.04–4.1) 0.456
Distance from aorta, mm 29.8 (25.9–49.6) 37.8 (19.4–70.2) 1.3 (0.28–6.2) 0.731
Mean Plaque density, HU 219 (132–387) 332 (195–449) 0.33 (0.08–1.4) 0.138
Plaque <30 HU, mm3** 0.35 (0.07–0.89) 0.16 (0.04–0.36) 4.0 (0.86–18.7) 0.077
Plaque <30 HU, % 10.5 (1.9–19.7) 4.1 (1.5–9.1) 2.4 (0.62–9.4) 0.207
Plaque <50 HU, mm3 0.51 (0.10–1.3) 0.26 (0.08–0.59) 14.6 (1.4–153.8) 0.026
Plaque <50 HU, % 15.4 (3.9–28.7) 6.4 (2.5–13.6) 6.1 (1.1–32.9) 0.036
Plaque <150, mm3 1.4 (0.58–3.3) 0.91 (0.41–1.9) 10.2 (1.0–99.8) 0.046
Plaque <150 HU, % 43.1 (14.8–64.1) 24.2 (15.3–42.5) 2.7 (0.56–13.3) 0.213
Plaque eccentricity†† 0.87 (0.73–0.91) 0.90 (0.86–0.92) 0.35 (0.09–1.4) 0.140
Arterial remodeling area‡‡ 1.7 (1.3–2.2) 1.5 (1.2–1.9) 1.3 (0.38–4.6) 0.670
Values are median (IQR) or n (%). *For continuous variables, hazard ratios and p values are for upper versus lower quartiles unless stated otherwise. †Calculated as percentageplaque volume/total arterial volume along length of plaque. ‡Measured to proximal border of plaque. §Visual analysis. Mild calcification ¼ grades 1–2 of 0–5 grades. kAt leastpart of plaque facing myocardium or pericardium, respectively. ¶Not assessed for 6 nonculprit plaques in straight portion of artery. Percentages are of plaques assessed.#Medina type 3 (plaque proximal, directly opposite and distal to side branch) versus all others. **The cross-section has a patient-specific slice thickness providing a volumerather than cross-sectional area of plaque. ††Calculated as 1 – (minimal plaque thickness/maximal plaque thickness). ‡‡Cross-sectional area of artery at maximal plaque area/proximal arterial reference area.
Abbreviations as in Tables 1 and 3.
Halon et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Coronary Plaque Outcomes in Patients With Diabetes J U L Y 2 0 1 9 : 1 3 5 3 – 6 3
1362
lower quartile for plaque volume and plaques $70%calcified were excluded from the analysis, and also inthe presence of differing concentrations of contrastmedium, the latter suggesting wide applicability ofthe findings under varying scanning conditions.
We necessarily censored plaques after electiverevascularization, which was analyzed as a competingevent. Plaques in electively revascularized patients
may have had a higher rate of events if revasculari-zation had not been performed than in those notundergoing elective revascularization. However,prediction of outcomes should be examined withinthe framework of usual clinical practice as was thecase in this study. Only 36 subjects underwent anelective revascularization procedure, limiting its ef-fect on outcomes.

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: A heterogeneity
of plaque findings exists in patients with type 2 diabetes.
Individual plaque characteristics increase the risk of a plaque-
related ACS but the large majority of plaques remained stable
over 9 years in this asymptomatic diabetic population receiving
guideline-based medical therapy; ACS was uncommon.
TRANSLATIONAL OUTLOOK: It is likely that identification of
asymptomatic diabetic patients who will benefit from individual-
ized preventive therapy will require approaches based on several
different lines of investigation in addition to CTA plaque analysis.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Halon et al.J U L Y 2 0 1 9 : 1 3 5 3 – 6 3 Coronary Plaque Outcomes in Patients With Diabetes
1363
CONCLUSIONS
This plaque level analysis in asymptomatic patientswith type 2 diabetes identified CTA-based plaquecharacteristics that predicted late ACS culprit plaqueseveral years later. Also of note was the low incidenceof clinical events in the current era of intense primaryand secondary prevention despite the high HR forevents in plaques with these features.
ADDRESS FOR CORRESPONDENCE: Prof. David A.Halon, Cardiovascular Clinical Research Institute, LadyDavis Carmel Medical Center, 7 Michal Street, Haifa3436212, Israel. E-mail: [email protected].
RE F E RENCE S
1. Fox CS, Golden SH, Anderson C, et al. Update onprevention of cardiovascular disease in adults withtype 2 diabetes mellitus in light of recent evi-dence: a scientific statement from the AmericanHeart Association and the American Diabetes As-sociation. Circulation 2015;132:691–718.
2. Kang SH, Park G-M, Lee S-W, et al. Long-termprognostic value of coronary CT angiography inasymptomatic type 2 diabetes mellitus. J Am CollCardiol Img 2016;9:1292–300.
3. Raggi P, Cooil B, Ratti C, Callister TQ, Budoff M.Progression of coronary artery calcium andoccurrence of myocardial infarction in patientswith and without diabetes mellitus. Hypertension2005;46:238–43.
4. Anand DV, Lim E, Hopkins D, et al. Risk strati-fication in uncomplicated type 2 diabetes: pro-spective evaluation of the combined use ofcoronary artery calcium imaging and selectivemyocardial perfusion scintigraphy. Eur Heart J2006;27:713–21.
5. Malik S, Zhao Y, Budoff M, et al. Coronary arterycalcium score for long-term risk classification inindividuals with type 2 diabetes and metabolicsyndrome from the Multi-Ethnic Study ofAtherosclerosis. JAMA Cardiol 2017;2:1332–40.
6. Burke AP, Kolodgie FD, Zieske A, et al.Morphologic findings of coronary atheroscleroticplaques in diabetics: a postmortem study. Arte-rioscler Thromb Vasc Biol 2004;24:1266–71.
7. Park HB, Heo R, Ó Hartaigh B, et al. Athero-sclerotic plaque characteristics by CT angiographyidentify coronary lesions that cause ischemia: adirect comparison to fractional flow reserve. J AmColl Cardiol Img 2015;8:1–10.
8. Dey D, Achenbach S, Schuhbaeck A, et al.Comparison of quantitative atherosclerotic plaqueburden from coronary CT angiography in patientswith first acute coronary syndrome and stablecoronary artery disease. J Cardiovasc ComputTomogr 2014;8:368–74.
9. Motoyama S, Ito H, Sarai M, et al. Plaquecharacterization by coronary computed tomogra-phy angiography and the likelihood of acute
coronary events in mid-term follow-up. J Am CollCardiol 2015;66:337–46.
10. Puchner SB, Liu T, Mayrhofer T, et al. High-riskplaque detectedon coronary CT angiography predictsacute coronary syndromes independent of significantstenosis in acute chest pain: results from theROMICAT-II trial. J Am Coll Cardiol 2014;64:684–92.
11. Halon DA, Azencot M, Rubinshtein R, Zafrir B,Flugelman MY, Lewis BS. Coronary computed to-mography (CT) angiography as a predictor of car-diac and noncardiac vascular events inasymptomatic type 2 diabetics: a 7-yearpopulation-based cohort study. J Am Heart Assoc2016;5:e003226.
12. Louvard Y, Thomas M, Dzavik V, et al. Classi-fication of coronary artery bifurcation lesions andtreatments: time for a consensus! Catheter Car-diovasc Interv 2008;71:175–83.
13. Gorter PM, van Lindert ASR, de Vos AM, et al.Quantification of epicardial and peri-coronary fatusing cardiac computed tomography; reproduc-ibility and relation with obesity and metabolicsyndrome in patients suspected of coronary arterydisease. Atherosclerosis 2008;197:896–903.
14. Cheng VY, Dey D, Tamarappoo B, et al. Peri-cardial fat burden on electrocardiogram-gatednoncontrast CT in asymptomatic patients whosubsequently experience adverse cardiovascularevents. J Am Coll Cardiol Img 2010;3:352–60.
15. StonePH, SaitoS, Takahashi S, et al. Predictionofprogression of coronary artery disease and clinicaloutcomes using vascular profiling of endothelialshear stress and arterial plaque characteristics: thePREDICTION study. Circulation 2012;126:172–81.
16. Austin PC, Lee DS, Fine JP. Introduction to theanalysis of survival data in the presence ofcompeting risks. Circulation 2016;133:601–9.
17. Marwan M, Taher MA, El Meniawy K, et al.In vivo CT detection of lipid-rich coronary arteryatherosclerotic plaques using quantitative histo-gram analysis: a head to head comparison withIVUS. Atherosclerosis 2011;215:110–5.
18. Shin S, Park H-B, Chang H-J, et al. Impact ofintensive LDL cholesterol lowering on coronary
artery atherosclerosis progression. J Am Coll Car-diol Img 2017;10:437–46.
19. Burke AP, Kolodgie FD, Farb A, et al. Healedplaque ruptures and sudden coronary death: evi-dence that subclinical rupture has a role in plaqueprogression. Circulation 2001;103:934–40.
20. Choi G, Lee JM, Kim HJ, et al. Coronary arteryaxial plaque stress and its relationship with lesiongeometry. Application of computational fluid dy-namics to coronary CT angiography. J Am CollCardiol Img 2015;8:1156–66.
21. Lee JM, Choi G, Hwang D, et al. Impact oflongitudinal lesion geometry on location of plaquerupture and clinical presentations. J Am Coll Car-diol Img 2017;10:677–88.
22. Feuchtner G, Kerber J, Burghard P, et al. Thehigh-risk criteria low-attenuation plaque <60 HUand the napkin-ring sign are the most powerfulpredictors of MACE: a long-term follow-up study.Eur Heart J Cardiovasc Imaging 2017;18:772–9.
23. García-García H, Gomez-Lara J, Gonzalo N,et al. A comparison of the distribution of necroticcore in bifurcation and non-bifurcation coronarylesions: an in vivo assessment using intravascularultrasound radiofrequency data analysis. Euro-Intervention 2010;6:321–7.
24. Morbiducci U, Kok AM, Kwak BR, Stone PH,Steinman DA, Wentzel JJ. Atherosclerosis atarterial bifurcations: evidence for the role ofhaemodynamics and geometry. Thromb Haemost2016;115:484–92.
25. Criqui MH, Knox JB, Denenberg JO, et al.Coronary artery calcium volume and density: po-tential interactions and overall predictive value:the Multi-Ethnic Study of Atherosclerosis. J AmColl Cardiol Img 2017;10:845–54.
26. Shaw LJ, Narula J, Chandrashekhar Y. Thenever-ending story on coronary calcium: is it pre-dictive, punitive, or protective? J Am Coll Cardiol2015;65:1283–5.
KEY WORDS acute coronary syndrome,coronary plaque, CT angiography, diabetesmellitus, primary prevention

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E A M E R I C A N
C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
EDITORIAL COMMENT
The Search for High-Risk CoronaryPlaque in Patients With Diabetes*
James K. Min, MD, Jessica M. Peña, MD, MPHSEE PAGE 1353
D iabetes is a burgeoning epidemic, with>400 million people living with the diseaseworldwide (1). As a potent cardiovascular
risk factor associated with a 2- to 4-fold increase inthe risk of myocardial infarction (2,3), elucidation ofthe mechanisms by which it contributes to adversecardiovascular outcomes is necessary and timely. Inthis issue of iJACC, Halon et al. (4) report the findingsof a long-term observational study aimed at identi-fying the coronary plaque characteristics associatedwith future acute coronary syndrome (ACS) in pa-tients with diabetes.
The study enrolled 630 asymptomatic men andwomen age 55 to 70 with type 2 diabetes and 1 addi-tional risk factor for cardiovascular disease but noknown history of coronary artery disease (CAD). Pa-tients underwent cardiac computed tomographicangiography (CTA) at baseline; those with CAD (n ¼499) were followed for a median of 9.2 years. Severalatherosclerotic plaque characteristics were harbin-gers of culprit plaques responsible for future ACS.Interestingly, these included markers of both plaquecomposition and anatomy: larger plaque volume,percent low attenuation plaque, mild calcification,stenosis severity, bifurcation lesions, and lesionsfacing the pericardium. In addition, higher baselinelow-density lipoprotein was associated with largeramounts of low-density plaque. In contrast to priorstudies, positive arterial remodeling was not associ-ated with an increased risk of ACS in this study,although the authors speculate that this null finding
ISSN 1936-878X/$36.00
*Editorials published in JACC: Cardiovascular Imaging reflect the views of
the authors and do not necessarily represent the views of iJACC or the
American College of Cardiology.
From the Dalio Institute of Cardiovascular Imaging, Weill Cornell Medical
College and New York-Presbyterian Hospital, New York, New York. Dr.
Min serves on the scientific advisory board of Arineta; has ownership in
MDDX; and has a research agreement with GE Healthcare. Dr. Peña has
reported that she has no relationships relevant to the contents of this
paper to disclose.
may have been a limitation of the methods used inthis study. Although the number of ACS events in thisstudy was small (n ¼ 24), the hazard ratios associatedwith these plaque characteristics ranged from 2.9 to6.9 and remained consistent in a clever sensitivityanalysis comparing culprit lesions with nonculpritlesions where each patient served as his or her owncontrol. An additional noteworthy ancillary finding ofthe study was that 20% of patients who met inclusioncriteria had no evidence of CAD and experienced noACS events over long-term follow-up. These findingsunderscore the prognostic significance of coronaryCTA-derived plaque characteristics in patients withdiabetes and add to the growing body of literaturesupporting plaque features as independent markersof risk of ACS in multiple cohorts.
The study by Halon et al. (4) was well-designedwith notable strengths. These strengths include itsprospective design, nearly 10-year follow-up, andindependent adjudication of ACS. The authors shouldalso be commended for their consideration ofanatomic coronary plaque features such as pericardialversus myocardial facing lesions, location of plaquein relation to the curve of the artery, and bifurcations.These spatial relationships of plaque within an arterymay be related to low endothelial shear stress at thesite of plaque, a proatherogenic stimulus (5).Although the number of plaque variables consideredin the study may raise concern for multiple testing,the analysis highlights the multitude of factors thatlikely interact synergistically in the pathogenesis ofatherosclerosis.
Some limitations bear mention because they pointto both challenges and opportunities in defining therole of coronary CTA for risk stratification. The overallrate of events in this study, w5% during 10 years, wasremarkably low for a diabetic population. This raisesconcern for generalizability of the study findings;however, long-term follow-up of patients with
https://doi.org/10.1016/j.jcmg.2018.04.021

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Min and PeñaJ U L Y 2 0 1 9 : 1 3 6 4 – 6 Editorial Comment
1365
diabetes in a primary prevention trial setting hasshown similar rates of ACS (6). Without clear guide-lines regarding measurement of high-risk plaquefeatures, Halon et al. (4) used various Hounsfield unitcut points for measures of low attenuation plaque andvisually assessed features such as degree of calcifi-cation and location of plaque in relation to the peri-cardium/myocardium, all by a single reader. In a prioranalysis, the authors report moderate correlationwhen a subgroup of these measurements were per-formed by a second reader (7). Advancement of thefield will require adoption of standardized defini-tions, validated across different software platformsand against a reference gold standard. This type ofstandardization would facilitate pooling of data, anecessary endeavor in this era of declining cardio-vascular event rates and aggressive medical therapyfor those at high risk. The Coronary Artery Disease–Reporting and Data System created a coronary CTAreporting nomenclature, moving us in this directionwith the introduction of a modifier for the presence ofhigh-risk or vulnerable plaque. As articulated in thisconsensus document, high-risk plaque is defined asthe presence of 2 or more of the following: “napkinring sign,” spotty or punctate calcification within aplaque, low attenuation plaque (attenuation <30 HU),positive remodeling (ratio >1.1) (8). Recent workdemonstrating only fair inter-reader agreement ofhigh-risk plaque using the Coronary Artery Disease–Reporting and Data System rubric emphasizes theneed for improved standardization and automatedquantitative techniques (9). The small number of ACSevents in this study precluded full multivariateadjustment for potential confounders or the ability todiscern the extent to which patient demographicfactors or use of statins modified the relationshipbetween coronary plaque features and risk of ACS.
This is a foremost question for patients faced with theresults of coronary CTA: will medications make theseplaques go away? Will medications transform theseplaques to a more benign phenotype and, if so, iscoronary CTA an effective way to monitor thesechanges?
The report by Halon et al. (4) is in keeping withprior seminal studies demonstrating an associationbetween high-risk plaque features by coronary CTAand risk of ACS in patients with suspected or knownCAD followed over 2 to 5 years (10,11) or patients withacute chest pain (12) and now extend these priorfindings to a patient population with acceleratedatherosclerosis and a pro-inflammatory milieu. Thefinding that plaques facing the pericardium weremore often implicated in the development of ACS isintriguing, and supported by studies linking epicar-dial fat volume to plaque vulnerability, presumablydriven by inflammatory factors in adipose tissue (13).
To advance the field of atherosclerosis imaging,future studies will need to aggregate and annotatelarge amounts of data and leverage analytic tech-niques such as machine learning to refine imaging-based risk prediction. Beyond prognosis,widespread implementation of detailed plaque char-acterization will depend on our ability to relate thesefindings to therapeutic implications. Last, we mustdistill the multitude of information available to thatwhich is clinically relevant for patients and theirphysicians.
ADDRESS FOR CORRESPONDENCE: Dr. James K.Min, Dalio Institute of Cardiovascular Imaging, NewYork-Presbyterian Hospital, Weill Cornell MedicalCollege, 413 East 69th Street, Suite 108, New York,New York 10021. E-mail: [email protected].
RE F E RENCE S
1. Shaw JE, Sicree RA, Zimmet PZ. Global es-timates of the prevalence of diabetes for2010 and 2030. Diab Res Clin Pract 2010;87:4–14.
2. Kannel WB, McGee DL. Diabetes and cardio-vascular risk factors: the Framingham study. Cir-culation 1979;59:8–13.
3. Yusuf S, Hawken S, Ounpuu S, et al. Effect ofpotentially modifiable risk factors associated withmyocardial infarction in 52 countries (the INTER-HEART study): case-control study. Lancet 2004;364:937–52.
4. Halon DA, Lavi I, Barnett-Griness O, et al.Plaque morphology as predictor of late plaqueevents in patients with asymptomatic type 2diabetes: a long-term observational study. J AmColl Cardiol Img 2019;12:1353–63.
5. Stone PH, Maehara A, Coskun AU, et al. Role oflow endothelial shear stress and plaque charac-teristics in the prediction of nonculprit majoradverse cardiac events: the PROSPECT Study.J Am Coll Cardiol Img 2018;11:462–71.
6. Saito Y, Okada S, Ogawa H, et al. Low-doseaspirin for primary prevention of cardiovascularevents in patients with type 2 diabetes mellitus:10-year follow-up of a randomized controlledtrial. Circulation 2017;135:659–70.
7. Halon DA, Azencot M, Rubinshtein R, Zafrir B,Flugelman MY, Lewis BS. Coronary computed to-mography (CT) angiography as a predictor of car-diac and noncardiac vascular events inasymptomatic type 2 diabetics: a 7-yearpopulation-based cohort study. J Am Heart Assoc2016;5:e003226.
8. Cury RC, Abbara S, Achenbach S, et al. CAD-RADSTM Coronary Artery Disease – Reporting andData System. An expert consensus document ofthe Society of Cardiovascular Computed Tomog-raphy (SCCT), the American College of Radiology(ACR) and the North American Society for Car-diovascular Imaging (NASCI). Endorsed by theAmerican College of Cardiology. J CardiovascComp Tomogr 2016;10:269–81.
9. Maroules CD, Hamilton-Craig C, Branch K, et al.Coronary artery disease reporting and data system(CAD-RADSTM): inter-observer agreement forassessment categories and modifiers. J CardiovascComput Tomogr 2018;12:125–30.
10. Motoyama S, Sarai M, Harigaya H, et al.Computed tomographic angiography characteris-tics of atherosclerotic plaques subsequently

Min and Peña J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 3 6 4 – 6
1366
resulting in acute coronary syndrome. J Am CollCardiol 2009;54:49–57.
11. Motoyama S, Ito H, Sarai M, et al.Plaque characterization by coronarycomputed tomography angiography and thelikelihood of acute coronary events in mid-term follow-up. J Am Coll Cardiol 2015;66:337–46.
12. Puchner SB, Liu T, Mayrhofer T, et al. High-riskplaque detected on coronary CT angiographypredicts acute coronary syndromes independent ofsignificant stenosis in acute chest pain: resultsfrom the ROMICAT-II trial. J Am Coll Cardiol 2014;64:684–92.
13. Ito T, Nasu K, Terashima M, et al. The impactof epicardial fat volume on coronary plaque
vulnerability: insight from optical coherencetomography analysis. Eur Heart J CardiovascImaging 2012;13:408–15.
KEY WORDS acute coronary syndrome,coronary plaque, CT angiography, diabetesmellitus, primary prevention

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
ORIGINAL RESEARCH
Comparative Effectiveness of CT-DerivedAtherosclerotic Plaque Metrics forPredicting Myocardial Ischemia
Hooman Bakhshi, MD,a,* Zahra Meyghani, MD,a,* Satoru Kishi, MD,a,* Tiago A. Magalhães, MD,b,cAndrea Vavere, MPH,d Pieter H. Kitslaar, MSC,e Richard T. George, MD,d Hiroyuki Niinuma, MD, PHD,f
Johan H.C. Reiber, PHD,e Aisha Betoko, PHD,g Matthew Matheson, MS,g Carlos E. Rochitte, MD,c
Marcelo F. Di Carli, MD,h Christopher Cox, PHD,g João A.C. Lima, MD,a Armin Arbab-Zadeh, MD, PHD, MPHa
ABSTRACT
ISS
Fro
Fe
GafDi
Un
*D
stu
de
Dr
Ra
(fo
OBJECTIVES This study sought to investigate the performance of various cardiac computed tomography (CT)–derived
atherosclerotic plaque metrics for predicting provocable myocardial ischemia.
BACKGROUND The association of coronary arterial diameter stenosis with myocardial ischemia is only modest, but
cardiac CT provides several other, readily available atherosclerosis metrics, which may have incremental value.
METHODS The study analyzed 873 nonstented coronary arteries and their myocardial perfusion territories in 356 patients
(mean 62 years of age) enrolled in the CORE320 (Coronary Artery Evaluation using 320-row Multidetector Computed To-
mography Angiography and Myocardial Perfusion) study. Myocardial perfusion defects in static CT perfusion imaging were
graded at rest and after adenosine in 13 myocardial segments using a 4-point scale. The summed difference score was
calculated by subtracting the summed rest score from the summed stress score. Reversible ischemia was defined as summed
difference score$1. In a sensitivity analysis, results were also provided using single-photon emission computed tomography
(SPECT) as the reference standard. Vessel based predictor variables included maximum percent diameter stenosis, lesion
length, coronary calcium score, maximum cross-sectional calcium arc, percent atheroma volume (PAV), low-attenuation
atheroma volume, positive (external) vascular remodeling, and subjective impression of “vulnerable plaque.” The study used
logistic regression models to assess the association of plaque metrics with myocardial ischemia.
RESULTS In univariate analysis, all plaque metrics were associated with reversible ischemia. In the adjusted logistic
model, only maximum percent diameter stenosis (1.26; 95% confidence interval: 1.15 to 1.38) remained an independent
predictor. With SPECT as outcome variable, PAV and “vulnerable” plaque remained predictive after adjustment. In vessels
with intermediate stenosis (40% to 70%), no single metric had clinically meaningful incremental value.
CONCLUSIONS Various plaque metrics obtained by cardiac CT predict provocable myocardial ischemia by CT perfusion
imaging through their association with maximum percent stenosis, while none had significant incremental value.
With SPECT as reference standard, PAV and “vulnerable plaque” remained predictors of ischemia after adjustment
but the predictive value added to stenosis assessment alone was small. (J Am Coll Cardiol Img 2019;12:1367–76)
© 2019 by the American College of Cardiology Foundation.
N 1936-878X/$36.00 https://doi.org/10.1016/j.jcmg.2018.05.019
m the aDepartment of Medicine, Division of Cardiology, Johns Hopkins University, Baltimore, Maryland; bUniversidade
deral do Paraná, Curitiba, Brazil; cHeart Institute (InCor), University of São Paulo, São Paulo, Brazil; dMedImmune,
ithersburg, Maryland; eDepartment of Radiology, Leiden University/Medical Imaging Systems, Leiden, the Netherlands;
vision of Cardiology, St. Luke’s International Hospital, Tokyo, Japan; gDepartment of Epidemiology, Johns Hopkins
iversity, Baltimore, Maryland; and the hDepartment of Radiology, Brigham and Women’s Hospital, Boston, Massachusetts.
rs. Bakhshi, Meyghani, and Kishi contributed equally to this work, and are joint first authors. The sponsor of the CORE320
dy, Canon Medical (formerly Toshiba Medical Systems Corporation), was not involved during any stage of the planning,
sign, data acquisition, data analysis, or manuscript preparation of this study. Ms. Vavere is an employee with MedImmune.
. Kitslaar has a research appointment at the Leiden University Medical Center, Division of Image Processing, Department of
diology; and is an employee of MEDIS (Leiden, the Netherlands). Dr. George has received grant support from Canon
rmerly Toshiba) Medical Systems; has served as a consultant for ICON Medical Imaging; and is an employee of MedImmune.

ABBR EV I A T I ON S
AND ACRONYMS
CAD = coronary artery disease
CTA = computed tomography
angiography
CTP = computed tomography
myocardial perfusion imaging
FFR = fractional flow reserve
%MDS = maximum percent
diameter stenosis
PAV = percent atheroma
volume
SPECT = single-photon
emission computed
tomography
TAV = total atheroma volume
Dr. Reiber i
(formerly T
reported th
Manuscript
Bakhshi et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CT Plaque Metrics for Predicting Myocardial Ischemia J U L Y 2 0 1 9 : 1 3 6 7 – 7 6
1368
C oronary computed tomographyangiography (CTA) is increasinglybeing used for evaluating patients
with suspected coronary artery disease(CAD). Coronary CTA allows for rapid quanti-fication of coronary arterial stenosis withvery good accuracy compared with invasivecoronary angiography (1,2). However, thecorrelation of stenosis assessment by eithercoronary CTA or invasive angiography withcoronary or myocardial blood flow restrictionis only modest, often requiring additionaltesting to determine the hemodynamic sig-nificance of coronary lumen obstruction,particularly in the intermediate stenosisrange (3–7). Fractional flow reserve (FFR)
assessment during cardiac catheterization is thegold standard for detecting hemodynamically signifi-cant CAD, but its invasive nature limits widespreadapplication (8). Recent advancements of CT technol-ogy now facilitate CT myocardial perfusion imaging(CTP) and CT-based FFR assessment for noninva-sively detecting hemodynamically significant CAD(9–14), but these methods require additional imagingor complex, time-consuming analyses. Cardiac CTprovides several readily available atherosclerotic pla-que metrics beyond stenosis evaluation, which haveshown promise for improving prediction of provoca-ble myocardial ischemia (15–19). Total coronaryatherosclerotic disease burden is associated withmyocardial ischemia independent of the degree ofstenosis (20,21). However, few data are available ondirectly comparing various, readily available CT-derived atherosclerotic plaque metrics to standardstenosis assessment for detecting myocardialischemia in the same patients (22). The present studywas undertaken to investigate the hypothesis thatCT-derived atherosclerotic plaque features predictmyocardial ischemia independently from standardcoronary artery stenosis assessment.
SEE PAGE 1377
METHODS
The CORE320 (Coronary Artery Evaluation using 320-row Multidetector Computed Tomography Angiog-raphy and Myocardial Perfusion) study is a
s CEO of MEDIS medical imaging systems (Leiden, the Netherlan
oshiba) Medical Systems. Dr. Arbab-Zadeh has served on the C
at they have no relationships relevant to the contents of this pap
received January 22, 2018; revised manuscript received May 16,
prospective, multicenter study to investigate the ac-curacy of combined coronary CTA and adenosine stressCTP for identifying patients with hemodynamicallysignificant CAD as determined by a combination ofquantitative (invasive) coronary angiography andsingle-photon emission CT (SPECT) myocardialperfusion imaging. The design of the CORE320 studyhas been published in detail (23). Briefly, 436 womenand men, 45 to 85 years of age, with suspected orknown CAD, who were referred for clinically indicatedinvasive coronary angiography, were recruited from 16centers in 8 countries between 2009 and 2011. Exclu-sion criteria for the CORE320 study included knownallergy to iodine contrast material, serum creatinine>1.5 mg/dl or calculated creatinine clearance of <60ml/min, atrial fibrillation, tachyarrhythmia, profoundsinus bradycardia, advanced atrioventricular block,symptomatic heart failure, previous coronary arterybypass or cardiac surgery, coronary interventionwithin the last 6 months, intolerance of beta-blockers,and body mass index >40 kg/m2 (23). The study pro-tocol was approved by central and individual Institu-tional ReviewBoards of participating centers. All studyparticipants provided written informed consent. Allpatients underwent coronary CTA, CTP, and SPECTstudies within 60 days of invasive angiography. In thepresent study, all participants with interpretable cor-onary CTA and CTP images were included for thisanalysis. A total of 153 vessels with stents wereexcluded.
CORONARY CTA AND CTP IMAGE ACQUISITION. Detailsof coronary CTA and static CTP acquisition tech-niques have been described in detail (23,24). Briefly,all images, including coronary calcium scoring,coronary CTA and CTP, were obtained using a320 mm � 0.5 mm detector row CT (Aquilion One,Canon [formerly Toshiba] Medical Systems, Otawara,Japan). Oral or intravenous metoprolol was given tolower heart rates, if applicable. Participants received0.4 mg of sublingual nitroglycerine if systolic bloodpressure was at least 110 mm Hg. After injecting 50 to70 cm3 of iodinated contrast medium (Iopamidol-370)at rates between 4 and 5 ml/s, coronary CTA/restCTP images were obtained using a prospectiveelectrocardiography-triggered protocol. Twenty mi-nutes later, stress CTP images were acquired afteradenosine infusion (0.14 mg/kg/min for 6 min) using
ds). Dr. Lima has received grant support from Canon
ORE320 steering committee. All other authors have
er to disclose.
2018, accepted May 24, 2018.

FIGURE 1 Case Example of Vessel and Lumen Contour Detection
A B
C
An example of lumen and coronary atherosclerotic plaque volume assessment
is provided. (A)Multiplanar reformatted computed tomography image of a
left anterior descending artery with applied lumen and vessel wall contour
tracking using the semiautomated software. (B) Cross-sectional image of the
same artery at the level of the horizontal blue line in A. (C) The same cross-
sectional image as in B after lumen and vessel wall contour tracking. The
plaque area is calculatedby subtracting the lumen area (yellowcircle) fromthe
vessel area (orange circle).
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Bakhshi et al.J U L Y 2 0 1 9 : 1 3 6 7 – 7 6 CT Plaque Metrics for Predicting Myocardial Ischemia
1369
repeat injection of 50 to 70 cm3 of contrastmedium and prospective electrocardiography-triggered protocol.
CORONARY CTA IMAGE ANALYSIS. Coronary CTAand CTP images were reconstructed centrally in a corelaboratory and transferred to 2 independent readingcenters for interpretation. Each reading center wasindependent and blinded to all clinical data. CoronaryCTA images were analyzed by 2 independent readers(A.A.-Z. and Rodrigo J. Cerci) with more than 10 and 5years of reading experience in cardiac CT, respec-tively. CTP images were interpreted by 2 independentreaders (R.T.G and Vishal C. Mehra) with 7 years and 1year of experience in CTP interpretation, respec-tively. Discrepancies were resolved by consensus.
Using multiplanar reformations and the coronaryartery segmentation model described in the CorE-64(Coronary Artery Evaluation Using 64-Row Multi-De-tector Computed Tomography Angiography) study(25), 19 coronary artery segments with $1 mm indiameter were visually evaluated. Segments with atleast 1 stenosis of $30% by visual inspection wereselected for stenosis quantification using a Vitrea FXversion 3.0 workstation (Vital Images, Minnetonka,Minnesota). A separate commercial software with asemiautomated 3-dimensional contour detectionalgorithm (QAngio CT Research Edition version 2.0RC4, MEDIS Medical Imaging Systems, Leiden, theNetherlands) was used to quantify coronary atheromavolume and additional atherosclerotic plaque metrics(Figure 1). Observer variability for atheroma quantifi-cation in our laboratory has been previously reported(18). Segment-based total atheroma volume (TAV) wasdefined as the difference between total vessel volumeand lumen volume in each coronary segments (18).Vessel-based TAV was computed as the sum ofsegment-based TAVs for each coronary artery. Becausethis method does not differentiate between normalwall lumen and atheroma, it likely leads to over-estimation of atherosclerotic disease (18). Accord-ingly, we developed a method to normalize theobserved atheroma volume using normal referencesegments. For each anatomic segment of our seg-mentation model, we selected those that were read asentirely free of atherosclerosis by visual inspectionand fit a linear regression to predict read TAV bysegment volume and length. The coefficients of thismodel were used to calculate TAV in both normal andabnormal segments, estimating the amount of TAVthat was likely to be normal vessel thickness. Thecorrected TAV was calculated as the observed TAVminus the estimated normal vessel thickness; this wasset to zero if the result was negative.
For the purpose of this study, the following plaquemetrics were obtained in each coronary artery.
1. Maximum percent diameter stenosis (%MDS):lesion with the most severe diameter stenosis ineach vessel.
2. Maximum lesion length: length of an arterysegment with continuous atherosclerotic disease ofat least 30% diameter stenosis. In diffusely diseasevessels, the proximal and distal borders of an atleast 30% diameter change was used to demarklesion margins.
3. Coronary artery calcium score: obtained on non-contrast images using the Agatston method foreach coronary artery.

FIGURE 2 Case Example of Cross-Sectional Calcium Arc Assessment
A B
C D
An example of cross-sectional calcium arc evaluation is provided. (A) A curved multiplanar reformatted computed tomography image of a left
anterior descending coronary artery is presented. (B) A cross-sectional image showing the same artery at the level of the horizontal blue line
in A. The cross-sectional calcium arc slightly exceeds 180�. (C) A curved multiplanar reformatted computed tomography image of a left
anterior descending coronary artery from a different patient is shown. (D) A cross-sectional image of the same artery at the level of the
horizontal blue line in C is shown. The cross-sectional calcium arc in this example is clearly <180�.
Bakhshi et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CT Plaque Metrics for Predicting Myocardial Ischemia J U L Y 2 0 1 9 : 1 3 6 7 – 7 6
1370
4. Maximum calcium arc (Figure 2): maximum cross-sectional arc of calcium in each artery categorizedas: 1) cross-sectional calcium arc of #180�; or 2)cross-sectional calcium arc >180� (26).
5. Percent atheroma volume (PAV): calculated as(TAV / total vessel volume) � 100 (18).
6. Low-attenuation (lipid/necrotic core) atheromavolume: lowest mean attenuation value (typicalrange: –30 to 75 HU) for atherosclerotic
plaque among 4 categories (dense calcium,fibrotic, fibrofatty, and necrotic core) usingdynamic threshold determination on semi-automated contour detection as previouslydescribed (27).
7. Positive (external) vascular remodeling: ratio ofvessel area at maximum segment lumen narrowingto a proximal reference point (remodeling index)exceeding 1.1 (28).

TABLE 1 Baseline Characteristics of Study Participants (N ¼ 356)
Age, yrs 62.0 (55.7–68.5)
Male 236 (66.3)
Ethnicity
Hispanic 29 (8.1)
Non-Hispanic 307 (86.2)
Other 20 (5.6)
Race
White 196 (55.1)
Black 39 (11.0)
Asian 116 (32.6)
Other 5 (1.4)
Body mass index, kg/m2 26.6 (24.1–30.2)
Hypertension 275 (77.7)
Medications
ACE inhibitor/ARB 149 (41.9)
Beta-blocker 182 (51.1)
Salicylates 217 (61.0)
Statins 187 (52.5)
Diabetes 120 (33.7)
Dyslipidemia 235 (67.5)
Smoking
Current 61 (18.0)
Past 122 (36.0)
Never 156 (46.0)
Family history of coronary artery disease 147 (43.6)
Values are median (interquartile range) or n (%).
ACE ¼ angiotensin-converting enzyme; ARB ¼ angiotensin receptor blocker.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Bakhshi et al.J U L Y 2 0 1 9 : 1 3 6 7 – 7 6 CT Plaque Metrics for Predicting Myocardial Ischemia
1371
8. “Vulnerable” atherosclerotic plaque: readers’ sub-jective impression of a constellation of athero-sclerotic plaque features in an arterial segmentthat conveyed possible vulnerability for acutecoronary events. Such features included externalvascular remodeling, low-attenuation plaque,suggestion of large lipid core (e.g., napkin-ringsign), and speckled calcification within the pla-que (29,30).
CTP IMAGE ANALYSIS. CTP images were displayed atwindow width of 300 HU and window level of 150HU, rendering coronary arteries uninterpretable forCAD by CTP readers. The severity of perfusion de-fects were graded using a 4-point ordinal scale ineach myocardial segment in a previously described13-segment model (10). Summed stress score for eachcoronary artery was defined as the sum of allmyocardial segmental scores in that artery territorymeasured in stress CTP. Summed rest score wascalculated using the same method using rest CTPimages. To assess reversible ischemia, the summeddifference score for each coronary artery was deter-mined by subtracting summed rest score from sum-med stress score of that artery. Summed difference
score $1 was categorized as reversible ischemia.The detail of adjudication process to align coronaryanatomy and myocardial perfusion territories inthe CORE320 study has been described in detail (31).An adjudication committee reviewed images if therewas a mismatch between coronary CTA and CTP.Final decision regarding realignment was made byconsensus (24).
SENSITIVITY ANALYSIS USING SPECT. To validateour data using CTP, we performed a sensitivity anal-ysis using myocardial ischemia by SPECT as outcomevariable. Details on the SPECT image acquisition inthe CORE320 study have been described in detail (10).Myocardial territories were analyzed by SPECT forseverity of rest and stress myocardial perfusionabnormalities using a 4-point scoring system and a13-territory model. For each artery, a summed dif-ference score of $1 was defined as reversibleischemia.
STATISTICAL ANALYSIS. Clinical and demographiccharacteristics of the study participants were sum-marized using median (interquartile range) forcontinuous variables and number (percentage) forcategorical variables. All predictor and outcome var-iables are vessel based instead of patient based. Weused logistic regression models to assess the effect ofdifferent plaque metrics on the odds of reversiblemyocardial ischemia on provocative testing. Toaccount for the inclusion of multiple vessels perpatient, generalized estimating equations were used.Univariable regression models were used to evaluatethe relation between each plaque metric and theoutcome (model 1). The second model (model 2)included all plaque metrics. We also performed asubgroup analysis for 314 vessels with intermediatecoronary artery stenosis (40% to 70%). Receiver-operating characteristic curve analysis was used todetermine the incremental value of adding all othermetrics to maximum diameter stenosis in predictingreversible ischemia. All statistical analyses were per-formed with SAS version 9.4 (SAS Institute, Cary,North Carolina). All tests were 2 sided and ap value <0.05 was considered statistically significant.
RESULTS
Baseline characteristics and clinical data of all 356participants are summarized in Table 1. Cardiovascu-lar risk factors were highly prevalent among studyparticipants: diabetes 33.7%, dyslipidemia 67.5%,hypertension 77.7%, and current smoker 18%. Amongparticipants with angina at presentation, 96.4%

TABLE 2 Vessel-Based Atherosclerotic Plaque Characteristics According to the Presence of Myocardial Ischemia by CT Perfusion Imaging (N ¼ 873)
Atherosclerotic Plaque Characteristics
LAD LCX RCA
Reversible Ischemia* Reversible Ischemia Reversible Ischemia
No (n ¼ 156) Yes (n ¼ 125) No (n ¼ 178) Yes (n ¼ 121) No (n ¼ 220) Yes (n ¼ 73)
Percent atheroma volume 3.3 (0.8–6.8) 8.5 (4.3–12.3) 2.1 (0.4–6.9) 6.0 (3.0–10.1) 3.4 (0.7–7.4) 7.5 (4.5–10.8)
Total atheroma volume, mm3 55 (13–125) 163 (72–238) 21 (4–76) 80 (26–137) 69 (15–152) 144 (66–236)
Maximum diameter stenosis, % 40.7 (15.0–56.5) 57.1 (45.5–78.6) 33.3 (15.0–51.0) 53.6 (35.0–85.7) 36.2 (15.0–50.8) 60.0 (43.3–82.9)
Maximum lesion length, mm 5.5 (0.0–13.5) 11.5 (7.5–20.4) 0.0 (0.0–7.5) 7.7 (0.0–14.5) 4.8 (0.0–12.5) 10.0 (2.9–20.5)
Maximum calcium arc
Noncalcified or #180� 126 (80.8) 83 (66.4) 162 (91.0) 104 (86.0) 199 (90.5) 53 (72.6)
>180� 30 (19.2) 42 (33.6) 16 (9.0) 17 (14.0) 21 (9.5) 20 (27.4)
Calcium score 9.5 (0.0–129.0) 147 (38.5–306.0) 0.0 (0.0–46.0) 26.0 (0.0–146.0) 3.0 (0.0–75.0) 96.0 (4.0–272.0)
Positive remodeling index 29 (18.6) 33 (26.4) 13 (7.3) 21 (17.4) 26 (11.8) 17 (23.3)
Low-attenuation atheroma volume, mm3 10 (2–23) 22 (12–45) 3 (0–10) 9 (2–19) 13 (2–28) 23 (7–45)
“Vulnerable” plaque 9 (5.8) 22 (17.6) 4 (2.2) 12 (9.9) 6 (2.7) 12 (16.4)
Values are median (interquartile range) or n (%). *Reversible myocardial ischemia was defined as summed difference score $1.
CT ¼ computed tomography; LAD ¼ left anterior descending; LCX ¼ left circumflex artery; RCA ¼ right coronary artery.
TABLE 3 Association
Maximum % stenosis,
Maximum lesion length
Percent atheroma volu
Calcium score, per 10 u
Maximum calcium arc,
Positive remodeling ind
Low-attenuation ather
“Vulnerable” plaque
Model 1 (unadjusted modescore $1.
CI ¼ confidence interval
Bakhshi et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CT Plaque Metrics for Predicting Myocardial Ischemia J U L Y 2 0 1 9 : 1 3 6 7 – 7 6
1372
reported symptoms of stable angina. Most participants(98.0%) were classified as either intermediate or highrisk based on the Diamond-Forrester score (32).Median heart rate during coronary CTA and CTP im-aging was 53 (interquartile range: 49 to 58) beats/minand 68 (interquartile range: 59 to 77) beats/min,respectively. Median coronary calcium scores in theleft anterior descending, left circumflex, and rightcoronary arteries were 55, 5, and 11, respectively.Among 873 analyzed coronary arteries, 319 revealedreversible myocardial ischemia by CTP in theirrespectivemyocardial territories (36.5%). Using SPECTas a reference standard, only 202 of 873 vesselswere associated with myocardial ischemia (23.0%).Table 2 and Supplemental Table 1 present the distri-bution of vessel-based plaque characteristics accord-ing to the presence or absence of reversible ischemiaby CTP and SPECT, respectively.
of CT-Derived Atherosclerotic Plaque Metrics With Myocardial Ischemia
Reversible Ischemia* by CT Perfusion
Model 1 Model 2
OR (95% CI) p Value OR (95% CI)
per 10% 1.34 (1.25–1.44) <0.001 1.26 (1.15–1.38)
, per 10 mm 1.56 (1.31–1.86) <0.001 0.93 (0.76–1.16)
me, per 10% 2.99 (2.07–4.34) <0.001 1.61 (0.89–2.90)
nits 1.02 (1.01–1.03) <0.001 1.01 (1.00–1.02)
>180� vs. #180� 2.39 (1.58–3.61) <0.001 0.85 (0.50–1.44)
ex 2.05 (1.40–3.00) <0.001 0.93 (0.60–1.43)
oma volume, per 10 mm3 1.14 (1.06–1.23) <0.001 0.94 (0.85–1.05)
4.74 (2.68–8.40) <0.001 1.74 (0.91–3.34)
l) involved using each individual plaque metric as the predictor variable. Model 2 includes a
; CT ¼ computed tomography; OR ¼ odds ratio; SPECT ¼ single-photon emission computed
CT PREDICTORS OF MYOCARDIAL ISCHEMIA. Theresults of univariable and multivariable logisticregression models are summarized in Table 3. Inunivariate logistic regression, all plaque metrics wereassociated with reversible ischemia by CTP. Inmultivariable analysis, 10% increase in %MDS wasassociated with 1.26 greater odds of ischemia whereasnone of the other metrics retained a statisticallysignificant relationship with ischemia. Table 3 alsopresents the results of a sensitivity analysis usingSPECT as outcome variable. The magnitude andsignificance of associations remain largely similarto CTP, except for PAV and the impression of“vulnerable plaque,” which remained independentpredictors of reversible ischemia detected by SPECTbut not by CTP.
The results of univariable and multivariablelogistic regression models for 314 vessels with
by CT Perfusion and SPECT
Reversible Ischemia* by SPECT
Model 1 Model 2
p Value OR (95% CI) p Value OR (95% CI) p Value
<0.001 1.25 (1.16–1.35) <0.001 1.15 (1.03–1.27) 0.01
0.53 1.32 (1.10–1.59) 0.003 0.88 (0.71–1.10) 0.27
0.11 2.39 (1.73–3.32) <0.001 1.93 (1.06–3.51) 0.03
0.11 1.01 (1.00–1.02) 0.001 1.01 (1.00–1.01) 0.12
0.55 1.75 (1.15–2.68) 0.001 0.77 (0.45–1.30) 0.33
0.74 1.99 (1.30–3.04) 0.002 1.19 (0.74–1.92) 0.48
0.26 1.09 (1.02–1.16) 0.01 0.91 (0.81–1.02) 0.11
0.10 4.48 (2.67–7.52) <0.001 2.37 (1.30–4.32) 0.005
ll plaque metrics. *Reversible myocardial ischemia was defined as summed difference
tomography.

TABLE 4 Association of CT-Derived Atherosclerotic Plaque Metrics With Myocardial Ischemia by CT Perfusion and SPECT in Vessels With Intermediate-Range
Stenoses (40%–70%)
Reversible Ischemia* by CT Perfusion Reversible Ischemia* by SPECT
Model 1 Model 2 Model 1 Model 2
OR (95% CI) p Value OR (95% CI) p Value OR (95% CI) p Value OR (95% CI) p Value
Maximum % stenosis, per 10% 1.34 (1.02–1.76) 0.03 1.22 (0.88–1.70) 0.24 1.58 (1.12–2.25) 0.01 1.22 (0.81–1.83) 0.34
Maximum lesion length, per 10 mm 1.11 (0.86–1.42) 0.42 0.94 (0.70–1.26) 0.70 1.16 (0.86–1.56) 0.34 0.85 (0.55–1.33) 0.48
Percent atheroma volume, per 10% 1.70 (1.07–2.71) 0.03 1.81 (0.83–3.95) 0.13 2.44 (1.28–4.63) 0.007 3.05 (0.90–10.36) 0.07
Calcium score, per 10 units 1.01 (1.00–1.02) 0.02 1.01 (1.00–1.03) 0.04 1.01 (1.00–1.02) 0.05 1.01 (1.00–1.03) 0.09
Maximum calcium arc, >180� vs. #180� 1.41 (0.83–2.39) 0.21 0.84 (0.42–1.68) 0.62 1.75 (0.92–3.33) 0.09 0.89 (0.36–2.21) 0.80
Positive remodeling index 1.01 (0.60–1.69) 0.97 0.68 (0.36–1.26) 0.22 1.69 (0.95–3.01) 0.08 1.14 (0.55–2.37) 0.72
Low attenuation atheroma volume, per 10 mm3 1.03 (0.94–1.13) 0.46 0.88 (0.75–1.03) 0.12 1.04 (0.93–1.17) 0.46 0.80 (0.62–1.03) 0.08
“Vulnerable” plaque 2.45 (0.60–10.09) 0.21 2.55 (0.53–12.23) 0.24 2.38 (0.60–9.50) 0.22 2.03 (0.47–8.71) 0.34
Model 1 (unadjusted model) involved using each individual plaque metric as the predictor variable. Model 2 includes all plaque metrics. *Reversible myocardial ischemia was defined as summed differencescore $1.
Abbreviations as in Table 3.
FIGURE 3 Receiver-Operating Characteristic Curves for Detecting Provocable
Myocardial Ischemia by Computed Tomography Perfusion
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0.0 0.1 0.2 0.3
Model 1AUC : 0.72 (0.68-0.76)
Model 2AUC : 0.74 (0.70-0.78)
0.4 0.51-Specificity
0.6 0.7 0.8 0.9 1.0
Sens
itivi
ty
Shown are the receiver-operating characteristic curves demonstrating the accuracy of
atherosclerotic plaque metrics to detect reversible myocardial ischemia by computed
tomography perfusion imaging. The pink curve shows results for model 1, which includes
maximum percent diameter stenosis only. The green curve shows results for model 2,
which includes all plaque metrics: maximum percent diameter stenosis, maximum
lesion length, coronary artery calcium score, maximum calcium arc, percent atheroma
volume, low-attenuation atheroma volume, positive remodeling, and “vulnerable”
plaque. AUC ¼ area under the curve.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Bakhshi et al.J U L Y 2 0 1 9 : 1 3 6 7 – 7 6 CT Plaque Metrics for Predicting Myocardial Ischemia
1373
intermediate range stenosis (40% to 70%) are pre-sented in Table 4. In univariate analysis, %MDS, cal-cium score, and PAV were associated with greaterodds of reversible myocardial ischemia by CTP. Noneof the associations remained statistically significantin multivariable analysis using CTP or SPECT asoutcome variable except for calcium score, thoughwith an odds ratio of only 1.01 per 10-U increase.
Results for receiver-operating characteristic curveanalysis are being presented in Figure 3, demon-strating a 0.02 increase of the area under the curve forpredicting reversible ischemia by CTP in the entirecohort when adding plaque metrics to %MDS (0.72[95% confidence interval: 0.68 to 0.76] to 0.74 [95%confidence interval: 0.70 to 0.78]; p ¼ 0.005).
DISCUSSION
We performed a comprehensive analysis on theperformance of many CT-derived atheroscleroticplaque metrics for predicting provocable myocardialischemia detected by CTP or SPECT. Although allmetrics are associated with ischemia by CTP, only %MDS remained an independent predictor afteradjustment, suggesting that their effect is mediatedby their relationship to stenosis severity. In contrast,PAV and subjective presence of “vulnerable plaque”were independent predictors of ischemia by SPECT.In vessels with intermediate stenoses, no plaquemetrics remained a statistically significant orclinically meaningful predictor in multivariableanalysis.
Coronary CTA excludes obstructive CAD insymptomatic patients with high accuracy and hasbecome an effective gatekeeper for invasive

Bakhshi et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CT Plaque Metrics for Predicting Myocardial Ischemia J U L Y 2 0 1 9 : 1 3 6 7 – 7 6
1374
coronary angiography (33). However, coronary CTAonly modestly well predicts provocable myocardialischemia when utilizing standard stenosis assess-ment alone (4,6). Advancements in CT acquisitiontechnique and data reconstruction software nowallow the assessment of various atherosclerotic pla-que characteristics, including lumen area, totalatherosclerotic plaque burden, and lesion length(34). Explorations about the added value ofadvanced atherosclerosis evaluation by coronaryCTA, however, have revealed inconsistent results.Several studies support the role of plaque burden asa predictor of myocardial ischemia (16,18,21). Kishiet al. (18) reported good accuracy of PAV for identi-fying patients with CAD and associated myocardialperfusion defects by SPECT in 374 participants of theCORE320 study. Baskaran et al. (35) found lesionplaque volume and area stenosis to be predictive ofreduced downstream FFR, while there was noassociation between dense calcium volume or non-calcified plaque volume with FFR #0.80. Diaz-Zamudio et al. (21) investigated 56 patients withintermediate stenoses and found total, noncalcified,and low-attenuation plaque burden but not calcifiedplaque burden to be predictive of invasivelymeasured FFR #0.8. More recently, Driessen et al.(28) found noncalcified atheroma volume and posi-tive remodeling to be independently predictive ofabnormal FFR and myocardial perfusion measuredby [15O] H2O positron emission tomography. Ahmadiet al. (36) found low-attenuation plaque volume andseverity of coronary arterial stenoses but not posi-tive remodeling being predictive of invasiveFFR #0.80.
How can we reconcile these inconsistent andsomewhat contradictory results? Some methodolog-ical differences among studies must be considered.Some investigations employed lesion-specificatherosclerotic plaque assessment whereas weanalyzed data on a vessel level. Results also mayvary with the reference standard, as demonstratedby Driessen et al. (28), who found an independentassociation of low-attenuation plaque withabnormal FFR but not with PET in the same studypopulation. We found largely similar results for CTPand SPECT in our study, except for PAV and“vulnerable plaque” remaining statistically signifi-cant predictors of ischemia versus SPECT but notversus CTP after adjustment for other metrics.Given the lower rate of ischemia by SPECT, it isconceivable that the difference compared with CTPis due to chance. CTP has shown to be more
sensitive to detect significant CAD than SPECT,which might have influenced our results (10). Weused CTP as the primary reference standard formyocardial ischemia because of the ease of artery-myocardial territory coregistration. Direct visualiza-tion of the vascular anatomy is likely to decreasethe probability of incorrect territory assignment inthe setting of anatomic variability compared withSPECT, which is blinded to the arterial anatomy(31).
Overall, the degree of lumen obstruction remainsthe most consistent predictor of abnormal coronaryartery blood flow, while the association of othermetrics with provocable ischemia is largely explainedby their correlation with lumen stenosis. The associ-ation of “vulnerable plaque” with downstreammyocardial ischemia is curious and consistent withother studies, suggesting greater probability ofischemia in the setting of noncalcified versus calcifiedplaque (28,36). Although mechanistic factors (e.g.,plaque plasticity) are a possible explanation, it is alsoplausible that later stage (i.e., calcified atheroscle-rotic disease) may be associated with more advancedadaptation (e.g., collateralization), which mayexplain lower rates of associated ischemia.STUDY LIMITATIONS. First, although all data wereprospectively acquired, the CORE320 study was notdesigned to specifically address the current researchquestion and, as such, our statistical power toconclusively detect associations was limited.Because power calculations would not be appro-priate as a post hoc measure, we provide 95%confidence intervals for our analyses. Second, theCORE320 study population contains patients whoare at higher CAD risk than is typically seen withapplication of coronary CTA in clinical practice.Thus, results may not be applicable to low-riskpopulations. Third, atherosclerotic plaque assess-ment was limited to nonstented arterial segments.Fourth, the contour detection algorithm wasupgraded and improved since our analysis and, assuch, its current edition may yield better perfor-mance. Also, the contour detection software is forresearch purposes only at this time and has not yetbeen validated for clinical use. Fifth, we used themost severe atherosclerotic lesion per coronary ar-tery for our data analysis. Therefore, in arterieswith more than 1 lesion, the cumulative effect ofless severe lesions for predicting ischemia was notconsidered. Last, we did not investigate the role ofcollateral circulation for false negative findings ofischemia.

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Among different
CT-derived atherosclerotic plaque metrics, %MDS was the only
independent predictor of vasodilator-provoked myocardial
ischemia detected by CTP, whereas other metrics often associ-
ated with myocardial ischemia (e.g., plaque burden, external
remodeling, low-attenuation plaque) had no independent pre-
dictive value. These data confirm our clinical focus on stenosis
assessment for assessing the hemodynamic significance of cor-
onary heart disease.
TRANSLATIONAL OUTLOOK: The notion that noncalcified
atheroma volume rather than calcified disease burden predicts
myocardial ischemia by provocative testing requires further
investigation. Not only independent mechanisms, but also con-
founding by disease stage and associated adaptation are plau-
sible explanations.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Bakhshi et al.J U L Y 2 0 1 9 : 1 3 6 7 – 7 6 CT Plaque Metrics for Predicting Myocardial Ischemia
1375
CONCLUSIONS
%MDS by coronary CTA is an independent predictorof reversible myocardial ischemia by CTP whereas theassociations of other atherosclerotic plaque metricswith ischemia, such as plaque burden, remodelingindex, “vulnerable plaque,” and lesion calcium arc,are largely explained by their relationship to lumenobstruction. Furthermore, the added predictive valueof plaque metrics to stenosis evaluation is small inthis context.
ACKNOWLEDGMENT The authors thank ChloeStevenson for preparing the images for thismanuscript.
ADDRESS FOR CORRESPONDENCE: Dr. Armin A.Zadeh, Johns Hopkins University School of Medicine,Division of Cardiology, 600 North Wolfe Street, Bla-lock 524, Baltimore, Maryland 21287-8222. E-mail:[email protected].
RE F E RENCE S
1. Miller JM, Rochitte CE, Dewey M, et al. Diag-nostic performance of coronary angiography by64-row CT. N Engl J Med 2008;359:2324–36.
2. Rahsepar AA, Arbab-Zadeh A. Cardiac CT vs.stress testing in patients with suspected coronaryartery disease: review and expert recommenda-tions. Curr Cardiovasc Imaging Rep 2015;8:29.
3. Budoff MJ, Nakazato R, Mancini GB, et al. CTAngiography for the prediction of hemodynamicsignificance in intermediate and severe lesions:head-to-head comparison with quantitative coro-nary angiography using fractional flow reserve asthe reference standard. J Am Coll Cardiol Img2016;9:559–64.
4. Godoy GK, Vavere A, Miller JM, et al. Quanti-tative coronary arterial stenosis assessment bymultidetector CT and invasive coronary angiog-raphy for identifying patients with myocardialperfusion abnormalities. J Nucl Cardiol 2012;19:922–30.
5. Plank F, Burghard P, Friedrich G, et al. Quanti-tative coronary CT angiography: absolute lumensizing rather than %stenosis predicts hemody-namically relevant stenosis. Eur Radiol 2016;26:3781–9.
6. Gould KL. Does coronary flow trump coronaryanatomy? J Am Coll Cardiol Img 2009;2:1009–23.
7. Meijboom WB, Van Mieghem CA, van Pelt N,et al. Comprehensive assessment of coronaryartery stenoses: computed tomography coronaryangiography versus conventional coronary angi-ography and correlation with fractional flowreserve in patients with stable angina. J Am CollCardiol 2008;52:636–43.
8. Corcoran D, Hennigan B, Berry C. Fractionalflow reserve: a clinical perspective. Int J Car-diovasc Imaging 2017;33:961–74.
9. Gonzalez JA, Lipinski MJ, Flors L, Shaw PW,Kramer CM, Salerno M. Meta-analysis of diag-nostic performance of coronary computed to-mography angiography, computed tomographyperfusion, and computed tomography-fractionalflow reserve in functional myocardial ischemiaassessment versus invasive fractional flow reserve.Am J Cardiol 2015;116:1469–78.
10. George RT, Mehra VC, Chen MY, et al.Myocardial CT perfusion imaging and SPECT forthe diagnosis of coronary artery disease: a head-to-head comparison from the CORE320 multi-center diagnostic performance study. Radiology2014;272:407–16.
11. Sorgaard MH, Kofoed KF, Linde JJ, et al.Diagnostic accuracy of static CT perfusion for thedetection of myocardial ischemia. A systematicreview and meta-analysis. J Cardiovasc ComputTomogr 2016;10:450–7.
12. Techasith T, Cury RC. Stress myocardial CTperfusion: an update and future perspective. J AmColl Cardiol Img 2011;4:905–16.
13. Bettencourt N, Chiribiri A, Schuster A, et al.Direct comparison of cardiac magnetic resonanceand multidetector computed tomography stress-rest perfusion imaging for detection of coronaryartery disease. J Am Coll Cardiol 2013;61:1099–107.
14. Tesche C, De Cecco CN, Albrecht MH, et al.Coronary CT Angiography-derived fractional flowreserve. Radiology 2017;285:17–33.
15. Tesche C, De Cecco CN, Caruso D, et al. Coro-nary CT angiography derived morphological andfunctional quantitative plaque markers correlatedwith invasive fractional flow reserve for detectinghemodynamically significant stenosis. J CardiovascComput Tomogr 2016;10:199–206.
16. Bauer RW, Thilo C, Chiaramida SA, Vogl TJ,Costello P, Schoepf UJ. Noncalcified atheroscle-rotic plaque burden at coronary CT angiography: abetter predictor of ischemia at stress myocardialperfusion imaging than calcium score and stenosisseverity. AJR Am J Roentgenol 2009;193:410–8.
17. Wang R, Renker M, Schoepf UJ, et al. Diag-nostic value of quantitative stenosis predictorswith coronary CT angiography compared to inva-sive fractional flow reserve. Eur J Radiol 2015;84:1509–15.
18. Kishi S, Magalhaes TA, Cerci RJ, et al. Totalcoronary atherosclerotic plaque burden assess-ment by CT angiography for detecting obstructivecoronary artery disease associated with myocardialperfusion abnormalities. J Cardiovasc ComputTomogr 2016;10:121–7.
19. Wang R, Baumann S, Schoepf UJ, et al. Com-parison of quantitative stenosis characteristics atroutine coronary computed tomography angiog-raphy with invasive fractional flow reserve forassessing lesion-specific ischemia. J CardiovascComput Tomogr 2015;9:546–52.
20. de Graaf MA, El-Naggar HM, Boogers MJ,et al. Automated quantitative coronary computedtomography correlates of myocardial ischaemia ongated myocardial perfusion SPECT. Eur J Nucl MedMol Imaging 2013;40:1171–80.
21. Diaz-Zamudio M, Dey D, Schuhbaeck A, et al.Automated quantitative plaque burden from cor-onary CT angiography noninvasively predicts he-modynamic significance by using fractional flowreserve in intermediate coronary lesions. Radi-ology 2015;276:408–15.
22. van Rosendael AR, Kroft LJ, Broersen A, et al.Relation between quantitative coronary CTA andmyocardial ischemia by adenosine stress myocar-dial CT perfusion. J Nucl Cardiol 2017;24:1253–62.

Bakhshi et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
CT Plaque Metrics for Predicting Myocardial Ischemia J U L Y 2 0 1 9 : 1 3 6 7 – 7 6
1376
23. Vavere AL, Simon GG, George RT, et al. Diag-nostic performance of combined noninvasive cor-onary angiography and myocardial perfusionimaging using 320 row detector computed to-mography: design and implementation of theCORE320 multicenter, multinational diagnosticstudy. J Cardiovasc Comput Tomogr 2011;5:370–81.
24. George RT, Arbab-Zadeh A, Cerci RJ, et al.Diagnostic performance of combined noninvasivecoronary angiography and myocardial perfusionimaging using 320-MDCT: the CT angiography andperfusion methods of the CORE320 multicentermultinational diagnostic study. AJR Am J Roent-genol 2011;197:829–37.
25. Miller JM, Dewey M, Vavere AL, et al. CoronaryCT angiography using 64 detector rows: methodsand design of the multi-centre trial CORE-64. EurRadiol 2009;19:816–28.
26. Cerci R, Vavere AL, Miller JM, et al. Patterns ofcoronary arterial lesion calcification by a novel,cross-sectional CT angiographic assessment. Int JCardiovasc Imaging 2013;29:1619–27.
27. de Graaf MA, Broersen A, Kitslaar PH, et al.Automatic quantification and characterizationof coronary atherosclerosis with computed
tomography coronary angiography: cross-correlation with intravascular ultrasound virtualhistology. Int J Cardiovasc Imaging 2013;29:1177–90.
28. Driessen RS, Stuijfzand WJ, Raijmakers PG,et al. Effect of plaque burden and morphology onmyocardial blood flow and fractional flow reserve.J Am Coll Cardiol 2018;71:499–509.
29. Maurovich-Horvat P, Hoffmann U,Vorpahl M, Nakano M, Virmani R, Alkadhi H.The napkin-ring sign: CT signature of high-riskcoronary plaques? J Am Coll Cardiol Img2010;3:440–4.
30. Motoyama S, Kondo T, Sarai M, et al. Multi-slice computed tomographic characteristics ofcoronary lesions in acute coronary syndromes.J Am Coll Cardiol 2007;50:319–26.
31. Cerci RJ, Arbab-Zadeh A, George RT, et al.Aligning coronary anatomy and myocardial perfu-sion territories: an algorithm for the CORE320multicenter study. Circ Cardiovasc Imaging 2012;5:587–95.
32. Diamond GA, Forrester JS. Analysis ofprobability as an aid in the clinical diagnosis ofcoronary-artery disease. N Engl J Med 1979;300:1350–8.
33. de Araujo Goncalves P, Campos CA,Serruys PW, Garcia-Garcia HM. Computed tomog-raphy angiography for the interventional cardiol-ogist. Eur Heart J Cardiovasc Imaging 2014;15:842–54.
34. Szilveszter B, Celeng C, Maurovich-Horvat P.Plaque assessment by coronary CT. Int J Car-diovasc Imaging 2016;32:161–72.
35. Baskaran L, B OH, Schulman-Marcus J,Gransar H, Lin F, Min JK. Dense calcium and lesion-specific ischemia: a comparison of CCTA withfractional flow reserve. Atherosclerosis 2017;260:163–8.
36. Ahmadi A, Leipsic J, Ovrehus KA, et al. Lesion-specific and vessel-related determinants of frac-tional flow reserve beyond coronary arterystenosis. J Am Coll Cardiol Img 2018;18:521–30.
KEY WORDS cardiac CT, CT perfusion, CTplaque characterization, diameter stenosis,plaque burden
APPENDIX For a supplemental table, pleasesee the online version of this paper.

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
EDITORIAL COMMENT
2 Steps Forward, 1 Step Back*
Pál Maurovich-Horvat, MD, PHD, MPHSEE PAGE 1367
C oronary computed tomography angiography(CTA) is one of the finest noninvasive imag-ing tools to rule out coronary artery disease.
Guidelines now recommend the use of coronary CTAfor the diagnostic work-up of patients with stable oracute chest pain. However, the high sensitivity andhigh negative predictive value of this noninvasivetest is paired with somewhat limited specificity andpositive predictive value to identify hemodynamical-ly relevant coronary atherosclerotic lesions. Thediscrepancy between anatomy and function, that is,the mismatch between degree of stenosis and the pro-pensity of myocardial ischemia, is well known and itis an inherent limitation of all anatomical imagingstrategies. These test characteristics may result inincreased downstream testing and cost. Therefore,to determine the hemodynamic significance of coro-nary lumen obstruction, both by coronary CTA orinvasive coronary angiography, additional testingis often required, particularly, in the intermediatestenosis range. Recent hardware and software devel-opments of computed tomography (CT) opened newpossibilities in functional coronary artery diseaseassessment. The latest-generation CT scanners arenow capable of acquiring myocardial perfusion scans.Using sophisticated computational hemodynamicsimulations, it is now feasible to derive CT dataset–based fractional flow reserve (FFR-CT) assessments.However, perfusion imaging with CT requiresadditional imaging, whereas FFR-CT is still an expen-sive technique. Importantly, the complex spatialdataset acquired by routine CT imaging containsmuch more information beyond stenosis evaluationor simple qualitative plaque assessment. Numerousatherosclerotic plaque metrics have shown promise
ISSN 1936-878X/$36.00
*Editorials published in JACC: Cardiovascular Imaging reflect the views of
the authors and do not necessarily represent the views of iJACC or the
American College of Cardiology.
From the MTA-SE Cardiovascular Imaging Research Group, Heart and
Vascular Center, Semmelweis University, Budapest, Hungary. Dr.
Maurovich-Horvat has no relationships relevant to the contents of this
paper to disclose.
for improving the prediction of significant myocardialischemia. Recently, it has been shown by severalresearch groups that total coronary atheroscleroticplaque burden, low attenuation plaque volume, andother high-risk plaque features are associated withmyocardial ischemia independent of the degreeof stenosis (1–4).
In this issue of iJACC, Bakhshi et al. (5) report theresults of a substudy of the CORE320 (Combined Non-invasive Coronary Angiography and MyocardialPerfusion Imaging Using 320 Detector Computed To-mography) multicenter trial. In the present analysis,the authors assessed if CT-derived atheroscleroticplaque features predict myocardial ischemia inde-pendently from coronary artery stenosis (5). Allpatients underwent coronary CTA, myocardial CTperfusion imaging, and single-photon emission CT(SPECT) within 60 days of invasive angiography. Theauthors performed meticulous plaque analysis andobtained the following plaque metrics: maximumpercent diameter stenosis, maximum lesion length,coronary artery calcium score, maximum calcium arc,percent atheroma volume, low attenuation atheromavolume, positive remodeling, and subjective“vulnerable” plaque appearance. To assess reversibleischemia, the authors derived a score for each coro-nary artery which was determined by subtracting thesummed rest score from summed stress score of thatartery. In addition, the authors performed a sensi-tivity analysis using myocardial ischemia by SPECT asoutcome variable to validate the myocardium CTperfusion findings. Among 873 analyzed coronaryarteries, 319 revealed reversible myocardial ischemiaby CT perfusion in their respective myocardial terri-tories (36.5%). Using SPECT as a reference standard,only 202 of 873 vessels were associated withmyocardial ischemia (23%). In univariate logisticregression, all plaque metrics were associated withreversible ischemia by myocardial CT perfusion.However, in multivariable analysis, only maximumpercent diameter stenosis was associated withischemia whereas none of the other plaque
https://doi.org/10.1016/j.jcmg.2018.07.031

Maurovich-Horvat J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 3 7 7 – 8
1378
characteristics retained a statistically significantrelationship with ischemia. Using SPECT as outcomevariable, the magnitude and significance of associa-tions remain largely similar to CT perfusion imaging,except for percent atheroma volume and the impres-sion of vulnerable plaque which remained indepen-dent predictors of reversible ischemia detected bySPECT but not by CT perfusion. In vessels with in-termediate stenosis, no plaque metrics remained astatistically significant or clinically meaningful pre-dictor in multivariable analysis using CT perfusion orSPECT.
These results are seemingly contradictory to thelarge number of papers published during the past fewyears, which indicate a strong relationship betweenplaque vulnerability and myocardial ischemia (1–4). Itis conceivable that the various methodologies used inprevious investigations versus the current study mayexplain the different findings. Most of the previousstudies used per plaque analysis, whereas the currentstudy used per vessel analysis. The latter approachcarries the inherent limitation of summing the effectof less severe lesions for predicting ischemia; there-fore, the effects of a few high-risk plaques with lesssevere stenosis were not considered. Furthermore,the precise co-registration of the coronary artery–myocardial territory might be challenging in somecases, especially with SPECT. The authors usedmyocardial CT perfusion as the primary referencestandard for this reason. However, both techniqueshave suboptimal diagnostic performance; therefore,using invasive FFR as the reference standard forischemia would most probably have led to different
conclusions. In addition, the authors used a some-what subjective definition of vulnerable plaque. Incontrast, most previously published papers used the“2-feature positive” rule, which categorizes plaquesas high-risk if at least 2 high-risk features are presentof the 4 traditional characteristics (i.e., positiveremodeling, low attenuation plaque, napkin-ringsign, or spotty calcium).
The strength of the study lies in its large patientpopulation and the detailed plaque analysis. The au-thors have to be complimented for performingquantitative plaque assessment in all patients and forperforming sensitivity analysis using SPECT.Considering the conflicting results of the current pa-per and pervious publications, it is clear that quanti-tative plaque assessment warrants standardizationbefore implementation in clinical practice. The cur-rent study may seem like a small step backward,however, its results convey an important messagethat we need to push our field towards standardiza-tion of methods and nomenclature. Standardizationof quantitative image biomarkers and clinicalreporting are needed to fully use the power of coro-nary CTA imaging. In the era of artificial intelligence,machine learning, and radiomics, this process isinevitable.
ADDRESS FOR CORRESPONDENCE: Dr. Maurovich-Horvat, Heart and Vascular Center, SemmelweisUniversity, MTA-SE Cardiovascular Imaging ResearchGroup, 68 Varosmajor Street, Budapest, Hungary 1122,Hungary. E-mail: [email protected] [email protected].
RE F E RENCE S
1. Driessen RS, Stuijfzand WJ, Raijmakers PG, et al.Effect of plaque burden and morphology onmyocardial blood flow and fractional flow reserve.J Am Coll Cardiol 2018;71:499–509.
2. Ahmadi A, Leipsic J, Ovrehus KA, et al. Lesion-specific and vessel-related determinants of frac-tional flow reserve beyond coronary artery ste-nosis. J Am Coll Cardiol Img 2018;11:521–30.
3. Gaur S, Ovrehus KA, Dey D, et al. Coronaryplaque quantification and fractional flow reserve
by coronary computed tomography angiographyidentify ischaemia-causing lesions. Eur Heart J2016;37:1220–7.
4. Tesche C, De Cecco CN, Caruso D, et al.Coronary CT angiography derived morphologicaland functional quantitative plaque markerscorrelated with invasive fractional flow reservefor detecting hemodynamically significant ste-nosis. J Cardiovasc Comput Tomogr 2016;10:199–206.
5. Bakhshi H, Meyghani Z, Kishi S, et al. Compar-ative effectiveness of CT-derived atheroscleroticplaque metrics for predicting myocardial ischemia.J Am Coll Cardiol Img 2019;12:1367–76.
KEY WORDS atherosclerotic plaquecharacterization, computed tomographic coronaryangiography, computed tomographic perfusion,coronary artery disease, coronary heart disease

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
ORIGINAL RESEARCH
Incremental Prognostic Value ofMyocardial Blood Flow QuantifiedWith Stress Dynamic ComputedTomography Perfusion Imaging
Satoshi Nakamura, MD,a Kakuya Kitagawa, MD,a Yoshitaka Goto, MD,a Taku Omori, MD,b Tairo Kurita, MD,bAkimasa Yamada, MD,a Masafumi Takafuji, MD,a Mio Uno, MD,a Kaoru Dohi, MD,b Hajime Sakuma, MDa
ABSTRACT
ISS
Fro
Ca
res
Sa
an
dis
Ma
OBJECTIVES This study aimed to evaluate whether myocardial blood flow (MBF) quantified with dynamic computed
tomography perfusion imaging (CTP) has an incremental prognostic value over coronary CT angiography (CTA) for
major adverse cardiac events (MACEs) in patients with suspected coronary artery disease (CAD).
BACKGROUND The incremental prognostic value of CTP over CTA is unclear. The quantification of MBF with dynamic
CTP may potentially enhance risk stratification.
METHODS A total of 332 patients (67% men; age: 67 � 10 years) with suspected CAD who underwent CTA and dynamic
CTP was analyzed. A MACE was defined as cardiac death, nonfatal myocardial infarction (MI), unstable angina, or
hospitalization for congestive heart failure. A summed stress score (SSS) was calculated by adding scores of all
myocardial segments according to normalized MBF values. Abnormal perfusion was defined as SSS $4. Obstructive
CAD was defined as $50% stenosis in $1 vessel on CTA.
RESULTS During a median follow-up of 2.5 years, 19 patients had a MACE. Multivariate analysis showed that,
when adjusted for obstructive CAD on CTA, abnormal perfusion was significantly associated with hazards for MACEs
(hazard ratio [HR]: 5.7; 95% confidence interval [CI]: 1.9 to 16.9; p ¼ 0.002), with a significant improvement in the
prognostic value. Abnormal perfusion was an independent predictor even when adjusted for $70% stenosis in $1 vessel
(HR: 5.4; 95% CI: 1.7 to 16.7; p ¼ 0.003) or adjusted for $50% stenosis in $2 vessels (HR: 6.5; 95% CI: 2.2 to 18.9;
p ¼ 0.001). In the setting of obstructive CAD, annualized event rates showed a significant difference between the
patients with and without abnormal perfusion for all events (12.2% vs. 1.5%; p ¼ 0.002) and for cardiac death and
nonfatal MI (4.2% vs. 0%; p ¼ 0.015).
CONCLUSIONS MBF quantified with dynamic CTP has an incremental prognostic value over CTA. The
addition of dynamic CTP to CTA allows improved risk stratification of patients with CTA-detected stenosis.
(J Am Coll Cardiol Img 2019;12:1379–87) © 2019 by the American College of Cardiology Foundation.
C oronary computed tomography angiography(CTA) is a reliable and established noninva-sive imaging tool for the diagnosis of
coronary artery disease (CAD) (1). CTA coronary
N 1936-878X/$36.00
m the aDepartment of Radiology, Mie University Graduate School of M
rdiology and Nephrology, Mie University Graduate School of Medicine, T
earch grants from Siemens Japan. Dr. Dohi has received speaker ho
kuma has received research grants from Daiichi Sankyo Company, Ltd.,
d Eisai Co., Ltd. All other authors have reported that they have no rela
close.
nuscript received March 8, 2018; revised manuscript received May 21, 20
images are useful for evaluating the extent andseverity of anatomical stenosis but are poor predic-tors of hemodynamically significant stenosis (2).Therefore, hemodynamic assessment of coronary
https://doi.org/10.1016/j.jcmg.2018.05.021
edicine, Tsu, Mie, Japan; and the bDepartment of
su, Mie, Japan. This study was partly supported by
noraria from Otsuka Pharmaceutical Co., Ltd. Dr.
Fuji Pharma Co., Ltd., Fujifilm RI Pharma Co., Ltd.,
tionships relevant to the contents of this paper to
18, accepted May 24, 2018.

ABBR EV I A T I ON S
AND ACRONYMS
CAD = coronary artery disease
CAD-RADS = Coronary Artery
Disease-Reporting and Data
System
CI = confidence interval
CTA = computed tomography
angiography
CTP = computed tomography
perfusion
FFR = fractional flow reserve
HR = hazard ratio
ICA = invasive coronary
angiography
MACE = major adverse
cardiac event
MBF = myocardial blood flow
MI = myocardial infarction
MPI = myocardial
perfusion imaging
NRI = net reclassification
improvement
ROC = receiver-operating
curve
Nakamura et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Incremental Prognostic Value of Dynamic CTP J U L Y 2 0 1 9 : 1 3 7 9 – 8 7
1380
lesions is often required to select patientswho would benefit from coronary revascular-ization. Inducible ischemia has been detectedusing several imaging techniques, includingnuclear myocardial perfusion imaging (MPI),magnetic resonance MPI, and stress echocar-diography. Dynamic computed tomography(CT) myocardial perfusion imaging (CTP) isa recently introduced imaging method thatenables the quantification of myocardialblood flow (MBF). Several studies haveshown that dynamic CTP has good diagnosticaccuracy in identifying ischemia determinedby different reference standards (3–6). Thecombination of CTA and dynamic CTP mayprovide a more comprehensive evaluationof patients with suspected CAD than CTAalone.
Previous studies have shown thatanatomical information from CTA imageshave similar prognostic significance to thatobtained using invasive coronary angiog-raphy (ICA) (7). Recently, a multicenter studyby Chen et al. (8) compared a predictive valueof CTA and/or CTP for major adverse cardiac
events (MACEs) with that of ICA and/or nuclear MPI,and revealed a prognostic value of perfusion defectsqualitatively determined by static CTP. However, theincremental prognostic value of CTP over CTAremained unclear. Furthermore, the quantification ofMBF with dynamic CTP may potentially enhance riskstratification. Therefore, the purpose of the presentstudy was to evaluate whether MBF quantified withdynamic CTP has an incremental prognostic valueover CTA for MACEs in patients with suspected CAD.
SEE PAGE 1388
METHODS
STUDY POPULATION. A total of 625 consecutive pa-tients who were referred for CTA and dynamic CTP forevaluation of CAD between March 2012 and February2017 at our hospital were screened for this study. Theinclusion criteria included: 1) age between 45 and 85years; and 2) written informed consent for studyparticipation. The exclusion criteria were as follows:1) impaired renal function (estimated glomerularfiltration rate <30 ml/min per 1.73 m2 body surfacearea); 2) contraindication against an iodinatedcontrast or a stress agent; 3) previous coronaryrevascularization via coronary artery bypass graftingor percutaneous coronary intervention; 4) history ofmyocardial infarction (MI); 5) incomplete tests or
severe artifacts due to motion or breathing; and 6)loss to follow-up. The study was approved by theinstitutional review board, and each patient gavewritten informed consent for participation in thestudy.
IMAGE ACQUISITION. All patients were scanned us-ing a second-generation, dual-source CT scanner (n ¼202; Somatom Definition Flash, Siemens Healthcare,Forchheim, Germany) or a third-generation, dual-source CT scanner (n ¼ 130; Somatom Force; SiemensHealthcare). Patients were instructed to avoidcaffeine drinks for at least 24 h before undergoing astress test.
During the administration of 20 mg of adenosinetriphosphate at 160 mg/kg/min for >3 min (9,10), scanacquisition of dynamic CTP was initiated by injecting40 ml of contrast medium with an iodine concentra-tion of 370 mg/ml at a flow rate of 5 ml/s. Dynamicdata sets were acquired for 30 s via anelectrocardiographically-triggered axial scan mode,repeated at 2 alternating table positions to obtain a Z-axis coverage of 73 or 102 mm (11). Tube voltage wasset at 70 or 80 kV, and tube current was determinedusing an automatic exposure control system with aquality reference of 350 mA per rotation at 120 kV(12,13). After completing data acquisition, adenosinetriphosphate administration was stopped. Electro-cardiography, blood pressure, and arterial oxygensaturation were monitored and recorded throughoutthe procedure.
After dynamic stress CTP, standard prospectiveCTA was performed at rest using the following scanparameters: 2 � 100-kV tube voltage or 80 kV and0.28-s gantry rotation time, with injection of 0.84 ml/kgof contrast medium over 12 s. Tube current wasdetermined using the angular modulation technique.
IMAGE ANALYSIS. The analysis of dynamic CTP im-ages was performed using commercially availableperfusion software (Syngo VPCT body, SiemensHealthcare). MBF was estimated using a dedicatedparametric deconvolution technique, based on a 2-compartment model of the intravascular and extra-vascular spaces (14). The maximum slope of timeattenuation curves fitted for every voxel was used togenerate a MBF map of 3 mm thickness and 1 mmincrements.
Polygonal regions of interest that measured 1 to 2cm2 were placed within each of the 16 myocardialsegments (according to the American Heart Associa-tion), excluding an apical segment, in the short-axisview on the MBF map, at a minimal distance of 1mm from the endocardial and epicardial borders toavoid contamination. A normalized MBF value was

FIGURE 1 A Case in a Patient With Abnormal Perfusion
Absolute MBF (normalized MBF)
0
105(0.73) 101
(0.70) 127(0.88) 88
(0.61) 91
(0.63) 98(0.68)
129(0.90) 125
(0.87)110
(0.76)
144(1.00)
139 (0.97) 124 (0.86)80 (0.56)
111 (0.76) 99 (0.69)99 (0.69)
0
01
00
1
0
01
01
1
3
22
Summed stress score = 12
A B C
D
Images in a 72-year-old man with multiple risk of coronary artery disease (CAD) are shown. Severe stenosis was found in the proximal left anterior descending artery
(LAD) on (A) computed tomography angiography (CTA) and (B) invasive coronary angiography (ICA). No significant stenosis was present in the right coronary artery or
the left circumflex artery. Color-coded myocardial blood flow (MBF) maps in short axis showed reduced perfusion in the left anterior descending vascular territory
(C), and summed stress score (SSS) was calculated to be 12 by adding scores of all segments (D).
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Nakamura et al.J U L Y 2 0 1 9 : 1 3 7 9 – 8 7 Incremental Prognostic Value of Dynamic CTP
1381
calculated as a MBF value in each segment divided bythe highest MBF value within the 16 segments on aMBF map. A summed stress score (SSS) was calculatedby adding scores of all segments using a 5-point scalebased on normalized MBF values: 0 ¼ normal (>0.75),1 ¼ mildly abnormal (#0.75, >0.675), 2 ¼ moderatelyabnormal (#0.675, >0.60), 3 ¼ severely abnormal(#0.60), or 4 ¼ absent. This division was suggested bythe fact that, in patients without $50% stenosis onCTA, the lowest MBF value divided by the highestMBF value within all segments was 0.750 � 0.075.Abnormal perfusion per patient was defined asSSS $4. An example of SSS in a patient with abnormalperfusion is shown in Figure 1. Global MBF wasdefined as a mean value of MBFs in all segments.
CTA images were visually evaluated by at least 2observers, including a radiologist with 10 years ofexperience in CTA, in a joint reading. Coronary seg-ments with a reference diameter $1.5 mm wereassessed for the detection of stenosis. Severity of CADon CTA was ranked by the Coronary Artery Disease-Reporting and Data System (CAD-RADS): 0 (0%), 1(1% to 24%), 2 (25% to 49%), 3 (50% to 69%), 4A (70%to 99% in 1 to 2 vessels), 4B (70% to 99% in 3 vesselsor $50% left main), or 5 (100%). Obstructive CADwas defined as $50% stenosis in $1 vessel(CAD-RADS $3).
FOLLOW-UP. Follow-up information was gatheredthrough a review of hospital records or telephone
interviews. Recorded MACEs consisted of cardiacdeath, nonfatal MI, unstable angina, and hospitali-zation for congestive heart failure. Hard eventsincluded cardiac death and nonfatal MI. Cardiacdeath was defined as death caused by acute MI,ventricular arrhythmias, or congestive heart failure.Nonfatal MI was defined as prolonged anginaaccompanied by new electrocardiographic abnormal-ities and increased cardiac biomarkers. Unstableangina was defined as new-onset, worsening, orangina at rest that required hospital admission.Congestive heart failure was defined as the emer-gence of appropriate symptoms (cough, shortness ofbreath, dyspnea on exertion, paroxysmal nocturnaldyspnea, and reduced exercise tolerance) associatedwith either new radiological findings consistent withcongestive heart failure or the development of phys-ical signs, including pulmonary rales, S3 gallop sound,and weight gain.
STATISTICAL ANALYSIS. Continuous variables arepresented as mean � SD or as the median, and wereassessed using the Student’s t- or Mann-Whitney Utests, as appropriate. Categorical variables areexpressed as frequency (percentage) and werecompared using Fisher’s exact test.
The influence of CTP, CTA, and clinical predictorson MACEs was determined using Cox regressionanalysis, and the results were reported as hazardratios (HRs) with 95% confidence intervals (CIs).

TABLE 1 Baseline Patient Characteristics (N ¼ 332)
Male 221 (67)
Age (yrs) 67 � 10
Coronary risk factors
Hypertension 225 (68)
Dyslipidemia 162 (49)
Diabetes 98 (30)
Current smoker 48 (14)
Family history of CAD 52 (16)
Body mass index >25 112 (34)
Echocardiography
LVEF <50% 20 (6)
Abnormal wall motion 50 (15)
Symptom
Typical 34 (10)
Atypical 76 (23)
Nonanginal 57 (17)
Dyspnea 37 (11)
Values are n (%) or mean � SD.
CAD ¼ coronary artery disease; LVEF ¼ left ventricular ejection fraction.
TABLE 2 Imaging Results (N ¼ 332)
Coronary CT angiography
CAD-RADS 0 87 (26)
CAD-RADS 1–2 127 (38)
CAD-RADS 3 50 (15)
CAD-RADS 4A 48 (14)
CAD-RADS 4B 9 (3)
CAD-RADS 5 11 (3)
Obstructive CAD 118 (36)
1-vessel disease 48 (14)
Multivessel disease 70 (21)
Dynamic CT perfusion
Global MBF value (ml/100 ml/min) 120 � 40
Lowest MBF value (ml/100 ml/min) 102 � 37
SSS $4* 94 (28)
SSS $8 44 (12)
SSS $12 21 (6)
Values are n (%) or mean � SD. *Perfusion abnormality was defined as a summedstress score (SSS) $4 in this study.
CAD-RADS ¼ Coronary Artery Disease–Reporting and Data System; CT ¼ coro-nary tomography; MBF ¼ myocardial blood flow; other abbreviation as in Table 1.
Nakamura et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Incremental Prognostic Value of Dynamic CTP J U L Y 2 0 1 9 : 1 3 7 9 – 8 7
1382
Univariate analysis of baseline clinical characteristics,CTA, and dynamic CTP was performed to identifypotential predictors. To determine independentpredictors of MACEs, multivariate analysis wasperformed using stepwise forward selection for vari-ables, with p < 0.05 in the univariate analysis. Theincremental value of CTP over CTA was assessed bycalculating the global chi-square test. Kaplan-Meiercurves were used to estimate cumulative event ratesfor CTP, CTA, and combined CTA and CTP. Differ-ences between time-to-event curves were comparedusing the log-rank test. Annualized event rates werecalculated by dividing the 4-year Kaplan-Meier eventrates by 4. Patients who underwent early (within60 days after CT) revascularization were censoredfrom follow-up thereafter. Receiver-operatingcharacteristic (ROC) curves were built for CTA, andcombined CTA and dynamic CTP based on a logisticregression model. The Delong test was used tocompare the areas under the curve. Net reclassifica-tion improvement (NRI) was calculated, and cate-gorical and continuous NRI and integrateddiscrimination improvement were estimated. A 2-sided p value of 0.05 was considered statisticallysignificant. All analyses were performed using theSPSS statistical package (version 23.0, IBM, Armonk,New York) and the R statistical package (version3.4.4, R Foundation for Statistical Computing,Vienna, Austria).
RESULTS
PATIENT CHARACTERISTICS, RADIATION DOSE,
AND HEMODYNAMIC RESPONSE DURING ADENOSINE
TRIPHOSPHATE STRESS. A total of 585 patients metthe inclusion criteria. Of these, we excluded 253 pa-tients who had contraindications against iodinatedcontrast agents (n ¼ 2) or a stress agent (n ¼ 2), pre-vious coronary revascularization via coronary arterybypass graft (n ¼ 43) or percutaneous coronaryintervention (n ¼ 143), history of MI (n ¼ 31), incom-plete tests (n ¼ 2), or severe artifacts due to motion orbreathing (n ¼ 10). Incomplete tests were attributableto complications of a contrast agent (n ¼ 1) or a stressagent (n ¼ 1). An additional 20 patients were lost tofollow-up. The study population consisted of theremaining 332 patients with suspected CAD.
Baseline patient characteristics are presented inTable 1. Mean age of the population was 67 � 10 years,and male patients accounted for 67% of the popula-tion. Most patients (61%) presented with chest pain ordyspnea.
The dose�length products for CTA and CTP were185 � 113 mGy$cm and 322 � 117 mGy$cm,
respectively, and the effective dose for the 2 tech-niques was 2.60 � 1.59 mSv and 4.52 � 1.68 mSv,respectively, using a conversion coefficient of 0.014.Heart rate significantly increased from 66 � 25 beats/min at baseline to 78 � 29 beats/min during stress(p < 0.001). Systolic blood pressure significantlydecreased from 136 � 52 mm Hg at baseline to 120 �46 mm Hg during stress (p < 0.001), whereas diastolicblood pressure significantly declined from 71 � 27mm Hg to 59 � 22 mm Hg (p < 0.001).
IMAGING RESULTS. The results of CTA and dynamicCTP are given in Table 2. CAD-RADS scores of 0, 1 to 2,

TABLE 3 Univariate Predictors of MACEs
HR (95% CI) p Value
Male 0.6 (0.3–1.5) 0.313
Age >70 yrs 2.1 (0.8–5.2) 0.113
Coronary risk factors
Hypertension 1.2 (0.4–3.4) 0.681
Dyslipidemia 0.9 (0.4–2.2) 0.800
Diabetes 1.9 (0.8–4.7) 0.178
Current smoker 1.0 (0.3–3.6) 0.951
Family history of CAD 0.2 (0.0–1.8) 0.169
Body mass index >25 kg/m2 0.1 (0.1–1.2) 0.091
Echocardiography
LVEF <50% 3.2 (0.9–11.1) 0.063
Abnormal wall motion 1.7 (0.6–5.0) 0.366
Coronary CT angiography
Obstructive CAD 6.3 (2.3–17.5) <0.001
CAD-RADS $4A 7.2 (2.9–17.9) <0.001
Multivessel disease 5.5 (2.2–13.6) <0.001
Dynamic CT perfusion
SSS $4 8.9 (3.2–24.9) <0.001
SSS $8 6.0 (2.4–14.8) <0.001
CI ¼ confidence interval; HR ¼ hazard ratio; MACE ¼ major adverse cardiac events;other abbreviations as in Tables 1 and 2.
TABLE 4 Multivariate Analysis
Model 1 Model 2 Model 3
HR(95% CI)
pValue
HR(95% CI)
pValue
HR(95% CI)
pValue
Abnormal perfusion 5.7 (1.9–16.9) 0.002 5.4 (1.7–16.7) 0.003 6.5 (2.2–18.9) 0.001
Coronary CT angiography
Obstructive CAD 3.3 (1.1–9.9) 0.030
CAD-RADS $4A 3.4 (1.2–9.2) 0.018
Multivessel disease 3.1 (1.2–8.0) 0.017
Abbreviations as in Table 2 and 3.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Nakamura et al.J U L Y 2 0 1 9 : 1 3 7 9 – 8 7 Incremental Prognostic Value of Dynamic CTP
1383
3, 4A, 4B, or 5 was observed in 87 (26%), 127 (38%),50 (15%), 48 (14%), 9 (3%), or 11 (3%) of 332 patients,respectively. Obstructive CAD was detected in 118(36%) patients. Single-vessel disease ($50% stenosisin 1 vessel) and multivessel disease ($50% stenosisin $2 vessels) were detected in 48 (14%) and 70 (21%)patients, respectively.
The global MBF values and lowest MBF values were120 � 40 ml/100 ml/min and 102 � 37 ml/100 ml/min,respectively. Abnormal perfusion, defined as SSS $4,was observed in 94 (28%) patients. SSS $8 and $12were detected in 44 (12%) and 21 (6%) patients,respectively.
OUTCOMES. The median follow-up was 2.5 years.Twenty-two patients underwent early revasculariza-tion and were censored at the time of revasculariza-tion. Nineteen patients had MACEs: cardiac death(n ¼ 2), nonfatal MI (n ¼ 3), unstable angina (n ¼ 7),and hospitalizations for congestive heart failure (n ¼7). Noncardiac death was observed in 4 patients.
UNIVARIATE AND MULTIVARIATE ANALYSES. Univariatepredictors for MACEs are listed in Table 3. Clinicalpredictors and findings of echocardiography did notreach statistical significance. Obstructive CAD (HR:6.3; 95% CI: 2.3 to 17.5; p < 0.001), CAD-RADSscore $4A (HR: 7.2; 95% CI: 2.9 to 17.9; p < 0.001),and multivessel disease (HR: 5.5; 95% CI: 2.2 to 13.6;p < 0.001) were significant predictors of MACEs.SSS $4 was the strongest predictor of events (HR: 8.9;95% CI: 3.2 to 24.9; p < 0.001). SSS $8 was
significantly associated with risk of events (HR: 6.0;95% CI: 2.4 to 14.8; p < 0.001).
Multivariate models were created to evaluatewhether MBF quantified with dynamic CTP was anindependent predictor (Table 4). When adjusted forobstructive CAD on CTA, abnormal perfusion had asignificant association with hazards for MACEs (HR:5.7; 95% CI: 1.9 to 16.9; p ¼ 0.002). In this model,obstructive CAD was also an independent predictor(HR: 3.3; 95% CI: 1.1 to 9.9; p ¼ 0.030). Even whenadjusted for CAD-RADS $4A, abnormal perfusionremained an independent predictor (HR: 5.4; 95% CI:1.7 to 16.7; p ¼ 0.003). CAD-RADS $4A was also anindependent predictor in this model (HR: 3.4; 95%CI: 1.2 to 9.2; p ¼ 0.018). Furthermore, when adjustedfor multivessel disease, abnormal perfusion remainedan independent predictor (HR: 6.5; 95% CI: 2.2 to 18.9;p ¼ 0.001), and multivessel disease was also an in-dependent predictor (HR: 3.1; 95% CI: 1.2 to 8.0;p ¼ 0.017).
To assess the incremental prognostic value ofdynamic CTP, global chi-square scores were calcu-lated (Figure 2). The addition of abnormal perfusion toobstructive CAD (global chi-square: 16.3) significantlyincreased the global chi-square score (31.9; p ¼ 0.001).Adding abnormal perfusion to the CAD-RADSscore $4A (global chi-square score: 24.6) resulted ina significantly increased global chi-square score (36.3;p ¼ 0.002). When abnormal perfusion was added tomultivessel disease, the global chi-square scoresignificantly increased from 17.5 to 34.9 (p < 0.001).
EVENT RATE. Kaplan-Meier curves by SSS with dy-namic CTP (Figure 3) showed that annualized eventrates for all events were 0.7% for SSS #3, 5.3% for SSS4 to 7, and 10.7% for SSS $8 (p < 0.001) (Figure 3A).Annualized event rates for hard events were 0% forSSS #3, 1.9% for SSS 4 to 7, and 3.3% for SSS $8 (p <
0.001) (Figure 3B). Kaplan-Meier curves by absoluteMBF (lowest MBF) demonstrated that annualizedevent rates were 3.2%, 3.4%, and 0.3% for MBFsof #80, 80 to 120, and >120 for all events, respec-tively (p ¼ 0.059), and 1.0%, 0.7%, and 0% for MBFs

FIGURE
SSPa
SSSS
A
Kaplan-
FIGURE 2 Incremental Prognostic Value of Dynamic CTP Over CTA
16.3
Glob
al c
hi-s
quar
e
31.9
+ Abnormal Perfusion
Obstructive CAD CAD-RADS ≥4A Multi-vessel disease
+ Abnormal Perfusion + Abnormal Perfusion
p = 0.001
24.6
36.3
17.5
34.9
p = 0.002p < 0.001
This illustration shows the incremental prognostic value of dynamic computed tomog-
raphy perfusion (CTP) when added (A) to obstructive coronary artery disease (CAD),
(B) to Coronary Artery Disease–Reporting and Data System (CAD-RADS) $4A, or
(C) to multi-vessel disease.
Nakamura et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Incremental Prognostic Value of Dynamic CTP J U L Y 2 0 1 9 : 1 3 7 9 – 8 7
1384
of #80, 80 to 120, and >120 for hard events, respec-tively (p ¼ 0.294) (Supplemental Figure 1).
Kaplan-Meier curves by CTA (Figure 4) revealedthat the annualized event rates for all events were0.7%, 2.7%, and 10.0% in patients with CAD-RADSscores of #2, 3, and $4A, respectively (p < 0.001)
3 Kaplan-Meier Curves by Dynamic CTP
0
0.0
0.2
0.4
Even
t-Fr
ee S
urvi
val
0.6
0.8
1.0
1 2
log-rank, p < 0.001
Follow-Up Time (Years)
All Events
3 4
238 199 131 87 3450 35 20 11 644
S ≤3tients at risk
S 4-7S ≥8
SSS ≤3
SSS 4-7
SSS ≥8
28 18 10 7
SP
SS
B
Meier curves in patients with SSS # 3, 4-7, or $8 (A) for all events and (B)
(Figure 4A), and annualized event rates for hardevents were 0%, 1.5%, and 2.6% in each patientgroup, respectively (p < 0.001) (Figure 4B).
Figure 5 shows Kaplan-Meier curves in patientswith and without abnormal perfusion among thepatients who had obstructive CAD. In the setting ofobstructive CAD, patients with abnormal perfusionhad significantly higher annualized event rates thanthose without abnormal perfusion for all events(12.2% vs. 1.5%; p ¼ 0.002) (Figure 5A) and for hardevents (4.2% vs. 0%; p ¼ 0.015) (Figure 5B). Annual-ized event rates for MACEs were not significantlydifferent between patients with obstructive CAD butwithout abnormal perfusion and patients withabnormal perfusion but not obstructive CAD (1.5% vs.2.1%; p ¼ 0.596) (Supplemental Figure 2).
ROC CURVE ANALYSIS AND NRI. ROC curve analysisshowed that CAD-RADS plus SSS had better discrim-inative ability for MACEs than CAD-RADS did alone(area under the curve: 0.876 vs. 0.770; p ¼ 0.016)(Supplemental Figure 3). The sensitivity, specificity,positive predictive value, and negative predictivevalue were 74%, 72%, 15%, and 98% for CAD-RADSand 95%, 74%, 19%, and 99% for CAD-RADS plusSSS, respectively.
Adding SSS to CAD-RADS resulted in improvementin risk reclassification for MACEs (SupplementalTable 1). Risk improvement in annual risk categoriesof #1%, 1% to 3%, and >3% was 0.192 for noneventcases and 0.157 for event cases; therefore, categorical
SSS ≤3SSS 4-7SSS ≥8
log-rank, p < 0.001
Hard Events
0
0.0
0.2
0.4
Even
t-Fr
ee S
urvi
val
0.6
0.8
1.0
1 2Follow-Up Time (Years)
3 4
238 202 134 87 3450 36 22 13 744
SS ≤3atients at risk
SS 4-7SS ≥8 28 19 11 9
for hard events are shown. Abbreviations as in Figure 1 and 2.

FIGURE 4 Kaplan-Meier Curves by CTA
0
0.0
0.2
0.4
Even
t-Fr
ee S
urvi
val
0.6
0.8
1.0
1 2
log-rank, p < 0.001
Follow-Up Time (Years)
All Events
3 4
214 181 116 78 3050 42 27 14 1068
CAD-RADS ≤2Patients at risk
CAD-RADS 3CAD-RADS ≥4A
CAD-RADS ≤2CAD-RADS 3
CAD-RADS ≥4A
39 26 16 7
CAD-RADS ≤2CAD-RADS 3CAD-RADS ≥4A
0
0.0
0.2
0.4
Even
t-Fr
ee S
urvi
val
0.6
0.8
1.0
1 2
log-rank, p < 0.001
Follow-Up Time (Years)
Hard Events
3 4
214 184 121 79 3150 43 27 14 1068
CAD-RADS ≤2Patients at risk
CAD-RADS 3CAD-RADS ≥4A 39 27 18 9
A B
Kaplan-Meier curves according to coronary status by CTA based on CAD-RADS (A) for all events and (B) for hard events are shown. Abbreviations as in Figure 1 and 2.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Nakamura et al.J U L Y 2 0 1 9 : 1 3 7 9 – 8 7 Incremental Prognostic Value of Dynamic CTP
1385
NRI was 0.349 (p ¼ 0.003). Continuous NRI and in-tegrated discrimination improvement were 0.514 (p ¼0.028) and 0.196 (p ¼ 0.011), respectively.
DISCUSSION
To our knowledge, this is the first study to evaluatethe incremental prognostic value of MBF quantified
FIGURE 5 Kaplan-Meier Curves for Abnormal Perfusion Among Pati
0
0.0
0.2
0.4
Even
t-Fr
ee S
urvi
val
0.6
0.8
1.0
1 2
log-rank, p = 0.002
Follow-Up Time (Years)
All Events
3 4
55Patients at riskAbnormal perfusion (–)
Abnormal perfusion (+)
Abnormal perfus
Abnormal perfus
43 30 20 11
63 38 23 10 6
A
Kaplan-Meier curves in patients with and without abnormal perfusion in
Abbreviations as in Figure 1.
with dynamic CTP in patients with suspected CAD.The main findings of our study were that dynamic CTPhad an incremental prognostic value over CTA andthat abnormal perfusion was associated with worseprognosis among those who had obstructive CAD.
RISK STRATIFICATION WITH CTA AND STATIC
CTP. A few studies have reported the prognostic
ents With Obstructive CAD
ion (–)
ion (+)
Abnormal perfusion (–)
Abnormal perfusion (+)
0
0.0
0.2
0.4
Even
t-Fr
ee S
urvi
val
0.6
0.8
1.0
1 2
log-rank, p = 0.015
Follow-Up Time (Years)
Hard Events
3 4
55Patients at riskAbnormal perfusion (–)
Abnormal perfusion (+)
44 30 20 11
63 38 24 12 8
B
the setting of obstructive CAD (A) for all events and (B) for hard events are shown.

Nakamura et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Incremental Prognostic Value of Dynamic CTP J U L Y 2 0 1 9 : 1 3 7 9 – 8 7
1386
value of static CTP. Linde et al. (15) showed that in240 patients with acute onset chest pain but who hadnormal electrocardiograms and troponin levels, staticCTP was useful for predicting mid-term (medianfollow-up: 19 months) clinical outcome indepen-dently of the pre-test probability of obstructive CAD.A prospective multicenter international study byChen et al. (8) demonstrated that the combination ofCTA and static CTP yielded a similar prediction of 2-year event-free survival to that obtained by ICA andsingle-photon emission computed tomography MPIamong a cohort of 379 patients with suspected orknown CAD. However, the 2 studies did not investi-gate an independent and incremental prognosticvalue of static CTP over CTA.
RISK STRATIFICATION WITH CTA AND DYNAMIC CTP.
There have been only limited data on the prognosticvalue of dynamic CTP. A retrospective study byMeinel et al. (16) indicated that, during a medianfollow-up of 12 months in 144 patients (including 51patients with known CAD), those who had perfusiondefects assessed visually on CTP images were at anincreased risk of MACEs (HR: 2.50; 95% CI: 1.34 to4.65; p ¼ 0.004). However, visual analysis as used inthat study often requires expertise in the readingof CTP images. Another study by Meinel et al. (17)showed that in the same study population, globalquantification of MBF obtained with dynamic CTPwas an independent predictor of MACEs comparedwith clinical risk factors and assessment of stenosisat CTA. However, in the latter study, when earlyrevascularizations were excluded from MACEs,Kaplan-Meier curves analysis showed no significantdifference in event-free survival between the pa-tients with and without low global MBF. Further-more, these 2 studies by Meinel et al. (17) did notperform additional statistical analysis to investigatean incremental prognostic value of dynamic CTPover CTA.
FRACTIONAL FLOW RESERVED CALCULATED BY
CTA DATA. Noninvasive fractional flow reserve (FFR)calculated using CTA (FFRCT) data is an emergingimaging tool that can be used to determine the he-modynamic significance of stenosis without stressagents (18). Data on the prognostic value of FFRCT arelimited. Douglas et al. (19) revealed that in symp-tomatic patients referred for ICA, care guided byFFRCT was associated with equivalent clinicaloutcomes compared with usual care over a 1-yearfollow-up.
Dynamic CTP has several potential advantagesover FFRCT. The evaluation of ischemia on CTP
images is not influenced by coronary calcification,whereas heavy coronary calcification may affect thehemodynamic assessment of stenosis with FFRCT.Furthermore, FFRCT may be hampered by highertesting costs in the absence of on-site application.
CLINICAL IMPLICATIONS. Our results implied thatMBF quantified with dynamic CTP could stratify pa-tients with suspected CAD for future cardiac events.More importantly, the addition of dynamic CTP toCTA improved risk stratification in patients withCTA-detected stenosis. Abnormal perfusion wasassociated with higher event rates for MACEs in thosewho had obstructive CAD. Consequently, the additionof dynamic CTP to CTA enabled a more appropriateselection of patients with CAD who were at a higherrisk of events.
According to the Kaplan-Meier curve analysis forabsolute MBF, the absence of reduced perfusion wasassociated with good prognosis for MACEs. Moder-ately reduced perfusion was associated with similaradverse outcomes as those of severely reducedperfusion, which suggested that moderately reducedperfusion in absolute MBF was no less important forassessing risk of cardiac events than that of severelyreduced perfusion.
STUDY LIMITATIONS. First, this was a single-centerstudy, and second, this was a retrospective study;clinical decisions and test orders were not managedthrough a standardized protocol. Third, although thetotal radiation dose (7.1 mSv) applied in this studywas relatively small, combining CTP with CTA inev-itably increased the ionizing radiation dose, as wellas the contrast medium volume, compared with CTAalone. Fourth, in the present study, a compositeendpoint that included heart failure was used. Instudies related to the prognostic value of MPI or CTAplus MPI, it is not uncommon to include heart failureas an MACE (8,20,21), because heart failure isfrequently associated with ischemic heart disease.Fifth, all CTA and dynamic CTP images in this studywere obtained using dual-source CT. Furtherresearch is necessary to evaluate whether the sameresults as our study could be obtained using othertypes of CT scanners, such as 320-row detector CT,which has different properties (e.g. temporal reso-lution, Z-axis coverage, and sampling rate) in acqui-sition of dynamic CTP data from dual-source CT.Sixth, our study population was restricted to patientswith suspected CAD because known CAD could havea substantial impact on the occurrence of cardiacevents (8). Furthermore, in a study population with ahigh prevalence of infarction, CTP at rest or with

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Abnormal
perfusion identified with dynamic CTP was strongly associated
with risk of major adverse cardiac events. Dynamic CTP had an
incremental prognostic value over CTA. In the setting of
obstructive CAD, higher event rates were observed in patients
with abnormal perfusion.
TRANSLATIONAL OUTLOOK: Dynamic CTP allows improved
risk stratification of patients with CTA-detected stenosis. In the
workup of patients with suspected CAD, the addition of dynamic
CTP to CTA enables a more appropriate selection of patients with
CAD who are at a higher risk of events.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Nakamura et al.J U L Y 2 0 1 9 : 1 3 7 9 – 8 7 Incremental Prognostic Value of Dynamic CTP
1387
delayed enhancement imaging was desired for eval-uating the influence of infarction on MBF. Furtherstudies are needed to investigate the prognosticusefulness of dynamic CTP in patients with knownCAD (e.g., patients with stents).
CONCLUSIONS
In patients with suspected CAD, MBF quantified withdynamic CTP is an independent predictor of MACEsand has an incremental prognostic value over CTA.Abnormal perfusion was associated with worseprognosis among those who had obstructive CAD.The addition of dynamic CTP to CTA allowsimproved risk stratification of patients with CTA-detected stenosis.
ACKNOWLEDGMENTS The authors thank NaokiNagasawa, RT, Yoshie Kurita, MD, and Tatsuro Ito,MD from Mie University Hospital for their valuablehelp.
ADDRESS FOR CORRESPONDENCE: Dr. Kakuya Kita-gawa, Department of Radiology, Mie University GraduateSchool of Medicine, 2-174 Edobashi, Tsu, Mie 514-8507,Japan. E-mail: [email protected].
RE F E RENCE S
1. Miller JM, Rochitte CE, Dewey M, et al. Diag-nostic performance of coronary angiography by64-row CT. N Engl J Med 2008;359:2324–36.
2. Schuijf JD, Wijns W, Jukema JW, et al. Rela-tionship between noninvasive coronary angiog-raphy with multi-slice computed tomography andmyocardial perfusion imaging. J Am Coll Cardiol2006;48:2508–14.
3. Ho KT, Chua KC, Klotz E, Panknin C. Stress and restdynamic myocardial perfusion imaging by evaluationof complete time-attenuation curves with dual-source CT. J Am Coll Cardiol Img 2010;3:811–20.
4. Bamberg F, Becker A, Schwarz F, et al. Detec-tion of hemodynamically significant coronary ar-tery stenosis: incremental diagnostic value ofdynamic CT-based myocardial perfusion imaging.Radiology 2011;260:689–98.
5. Greif M, von Ziegler F, Bamberg F, et al. CTstress perfusion imaging for detection of haemo-dynamically relevant coronary stenosis as definedby FFR. Heart 2013;99:1004–11.
6. Bamberg F, Marcus RP, Becker A, et al. Dynamicmyocardial CT perfusion imaging for evaluation ofmyocardial ischemia as determined by MR imag-ing. J Am Coll Cardiol Img 2014;7:267–77.
7. Min JK, Shaw LJ, Devereux RB, et al. Prognosticvalue of multidetector coronary computed tomo-graphic angiography for prediction of all-causemortality. J Am Coll Cardiol 2007;50:1161–70.
8. Chen MY, Rochitte CE, Arbab-Zadeh A, et al.Prognostic value of combined CT angiography andmyocardial perfusion imaging versus invasivecoronary angiography and nuclear stress perfusionimaging in the prediction of major adverse car-diovascular events: The CORE320 MulticenterStudy. Radiology 2017:55–65.
9. Chun KA, Lee J, Lee S-W, et al. Direct compar-ison of adenosine and adenosine 50-triphosphateas pharmacologic stress agents in conjunction withTl-201 SPECT: hemodynamic response, myocardialtracer uptake, and size of perfusion defects in thesame subjects. J Nucl Cardiol 2006;13:621–8.
10. Coma-Canella I, Palazuelos J, Bravo N,Velloso MJG. Myocardial perfusion imaging withadenosine triphosphate predicts the rate of car-diovascular events. J Nucl Cardiol 2006;13:316–23.
11. Bamberg F, Klotz E, Flohr T, et al. Dynamicmyocardial stress perfusion imaging using fastdual-source CT with alternating table positions:initial experience. Eur Radiol 2010;20:1168–73.
12. Kim SM, Kim YN, Choe YH. Adenosine-stressdynamic myocardial perfusion imaging using 128-slice dual-source CT: Optimization of the CT pro-tocol to reduce the radiation dose. Int J CardiovascImaging 2013;29:875–84.
13. Fujita M, Kitagawa K, Ito T, et al. Dose reductionin dynamic CT stress myocardial perfusion imaging:comparison of 80-kV/370-mAs and 100-kV/300-mAs protocols. Eur Radiol 2014;24:748–55.
14. Mahnken AH, Klotz E, Pietsch H, et al. Quan-titative whole heart stress perfusion CT imaging asnoninvasive assessment of hemodynamics in cor-onary artery stenosis: preliminary animal experi-ence. Invest Radiol 2010;45:298–305.
15. Linde JJ, Sorgaard M, Kuhl JT, et al. Predictionof clinical outcome by myocardial CT perfusion inpatients with low-risk unstable angina pectoris. IntJ Cardiovasc Imaging 2017;33:261–70.
16. Meinel FG, Pugliese F, Schoepf UJ, et al.Prognostic value of stress dynamic myocardialperfusion CT in a multicenter population with
known or suspected coronary artery disease. AJRAm J Roentgenol 2017;208:761–9.
17. Meinel FG, Wichmann JL, Schoepf UJ, et al.Global quantification of left ventricular myocardialperfusion at dynamic CT imaging: prognostic value.J Cardiovasc Comput Tomogr 2017;11:16–24.
18. Koo B-K, Erglis A, Doh J-H, et al. Diagnosis ofischemia-causing coronary stenoses by noninva-sive fractional flow reserve computed from coro-nary computed tomographic angiograms: resultsfrom the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing StenosesObtained Via Noninvasive Fractional Flow Reserve)study. J Am Coll Cardiol 2011;58:1989–97.
19. Douglas PS, De Bruyne B, Pontone G, et al. 1-Year outcomes of FFR CT-guided care in patientswith suspected coronary disease: the PLATFORMstudy. J Am Coll Cardiol 2016;68:435–45.
20. Ziadi MC, Williams KA, Guo A, et al. Impairedmyocardial flow reserve on rubidium-82 positronemission tomography imaging predicts adverseoutcomes in patients assessed for myocardialischemia. J Am Coll Cardiol 2011;58:740–8.
21. Greenwood JP, Herzog BA, Brown JM, et al.Prognostic value of cardiovascular magnetic reso-nance and single-photon emission computed tomog-raphy in suspected coronary heart disease: long-termfollow-up of a prospective, diagnostic accuracy cohortstudy. Ann Intern Med 2016;165:1–9.
KEY WORDS coronary artery disease,coronary CT angiography, dynamic CTperfusion
APPENDIX For supplemental figures and atable, please see the online version of this paper.

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
EDITORIAL COMMENT
Dynamic Stress Perfusion CT
2 Out of 3 Ain’t Bad?*Andrew M. Crean, BM, Benjamin J.W. Chow, MD
SEE PAGE 1379
I want you, I need youBut there ain’t no way I’m ever gonna love you
Now don’t be sad (don’t be sad)Cause two out of three ain’t bad.
—Meatloaf (1)
Q uantitative assessment of organ blood flowby computed tomography (CT) is not a newgoal. Ironically, it was Leon Axel (2)—later
much better known for his work in the field of cardiacmagnetic resonance (CMR) imaging—who was amongthe first to suggest the theoretical basis for achievingthis in his 1980 paper on quantitating cerebral bloodflow following cerebrovascular events. Subsequently,Ken Miles and Adrian Dixon (3) from Cambridge,United Kingdom, demonstrated the feasibility oftissue-level parametric mapping of blood flow.Initially, the application of this technique to the heartseemed challenging, given the temporal and spatialrequirements for adequate coverage. However, rapidadvances in scanner technology, combined with thecuriosity of the cardiovascular CT community, hasled to growing interest in functional CT imaging ofthe heart. In theory, myocardial CT perfusion (CTP)might be regarded as the perfect partner for CT coro-nary angiography (CTA)—the holy grail of anatomyand perfusion, perfectly coregistered, the ultimatestandard of reference. In practice, CTP has beenlargely overlooked in the headlong rush towardcomputational methods for deriving coronary physi-ology. The reasons are varied but include: 1) a reason-able concern about radiation dose; 2) anunwillingness to prolong examination table time inbusy institutions; 3) a reluctance to employ
ISSN 1936-878X/$36.00
*Editorials published in JACC: Cardiovascular Imaging reflect the views of
the authors and do not necessarily represent the views of iJACC or the
American College of Cardiology.
From the Division of Cardiology, University of Ottawa Heart Institute,
Ottawa, Canada. Dr. Chow has received research and educational
support from TeraRecon; and has investment equity in GE. Dr. Crean
has reported that he has no relationships relevant to the contents of
this paper to disclose.
vasoactive drugs, particularly in some departments;4) a lack of software tools for analyzing CT perfusionimages; and 5) an uncertainty about which of the pub-lished perfusion protocols to employ. This last pointis particularly pertinent because the term perfusionhas been used rather loosely in the cardiac CT pub-lished reports. In essence, perfusion refers to flow ofblood as a function of time. This obviously requiresa dynamic acquisition with the sample volume beingre-imaged at short, evenly spaced intervals followinginjection. However, a number of studies with “perfu-sion” in the title are instead describing imaging ata single fixed time point shortly after contrastinjection—a technique that might be more accuratelydescribed as iodine mapping rather than perfusion.
STUDY POPULATION
In this issue of iJACC, Nakamura et al. (4) employeddual-source technology and rapid shuttle mode to ac-quire genuine time-resolved datasets under vasodi-lator stress, together with a single time pointacquisition at rest for coronary anatomy. The aimof thestudy was to compare CTA alone versus a combinationof CTA and CTP for medium-term outcomes. Consid-ered for inclusion were a retrospective population of625 consecutive patients who were referred for CTA/CTP at a single institution. As in most cardiologystudies, the majority were male (and presumably,though not stated, monoethnic). Regrettably, themean body mass index was not provided; this wouldhave been helpful to assess the generalizability of theCT technique employed (see the following text).
TECHNIQUE
Several points regarding the technique used are dueconsideration. The choice of stress agent, adenosinetriphosphate (ATP) may be unfamiliar to Westernphysicians but is commonly employed in the Far Eastfor nuclear perfusion imaging. As the precursor to
https://doi.org/10.1016/j.jcmg.2018.06.002

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Crean and ChowJ U L Y 2 0 1 9 : 1 3 8 8 – 9 1 Editorial Comment
1389
adenosine, it has very similar vasoactive effects (andside effects) but is usually given at the slightly higherdose of 160 mg/kg/min, with tracer agent (in this caseiodine) given at 3 min but with continued ATP infu-sion post-tracer injection for at least a further 2 min(for single-photon emission computed tomographyimaging) (5). In this study, ATP was discontinuedonce image acquisition was complete, presumably 30to 40 s after contrast injection. It is unclear, therefore,whether maximal coronary dilatation could havebeen achieved in this time period, which likelywas <4 min in total.
Secondly, the authors report the use of 70 or 80 kVfor the CTP portion of the protocol. This results in anacceptable dose but at the risk of introducing unac-ceptable levels of noise, especially in larger patients.Because the body mass index of the subjects is notprovided, it is difficult to assess the applicability ofthe technique to other populations outside of Japan,which has an obesity rate of only 7% compared with27% in the United States (6).
Thirdly, quantitative rather than qualitative (visual)measures of perfusion were employed. Althoughintuitively attractive, one CMR study that addressedthis found no added diagnostic benefit over a purelyqualitative read (7). The authors could not generate ameasurement of perfusion reserve comparing hyper-emic to resting flow—as is conventionally done in CMRand positron emission tomography imaging—becausethey did not acquire time-resolved images in theresting state (presumably to reduced total radiationburden). Instead, they used mathematical modellingto estimate values of absolute myocardial blood flowfrom the stress series alone. They then normalized theblood flow value per segment to the highest flow (i.e.,the most normal segment) anywhere within the 17-segment model. The need for normalization is notspelled out in the paper but presumably reflects a needto average out noise within the data. The presence ofnoise in the system is demonstrated by the fact that inpatients without obstructive disease, the lowest ratioof segmental to global perfusion was not 1.0—as mightbe expected under perfect conditions—but instead was0.75. Scaling to the most normal value in this wayopens the door to the possibility of underestimatingischemia in the presence of triple vessel disease if thereare no segments with normal perfusion. As such, theauthors risk diluting the benefits of using a quantita-tive method in the first place. They then generatedrange categories for normalized stress perfusion andcreated a 17-segment summed stress score based uponthe point value assigned to each of the categories.Withthe exception of the cutoff used to define normal(>0.75), it is unclear how the remaining thresholds
were determined andwhether theywere decided upona priori, a pertinent consideration when reviewing thesubsequent Kaplan-Meier event curves.
RESULTS
After exclusions (due to prior percutaneous coronaryintervention/coronary artery bypass grafting/myocar-dial infarction), 332 patients with suspected coronaryartery disease remained in the study. The fact that only10 patients were excluded due to image artifacts isencouraging, but may reflect the likely low mean bodymass index of their patients by North American andEuropean standards. Mean total dose was a little over 7mSv, which is quite reasonable for this kind of proto-col; whether this could be reproduced with acceptableimage quality in a heavier population is debatable.Only 28% had an abnormal perfusion study (defined asa summed stress score [SSS] >4), and only 6% had aseverely abnormal study (SSS >12). Thus, the overallpresence of obstructive disease, defined by perfusion,was low, which is problematic when looking at rela-tively short-term endpoints (median follow up 2.5years, upper bound around 4 years), borne out by thefact that none of the conventional major coronary riskfactors were associated with a significant hazard formajor adverse cardiac events (MACE), even in univar-iate analysis, due to the short duration of follow-up.Nonetheless, the authors were able to show a signifi-cant difference in combinedMACE between thosewitha SSS >4 (abnormal perfusion) compared with thosewith a SSS <4 (normal perfusion). When consideringonly hard endpoints (death, nonfatal myocardialinfarction), the difference was reduced but remainedstatistically significant, although with a total of only 5hard outcomes, the clinical significance remains opento question. Statistical limitations include the possi-bility of nondifferential loss to follow-up, as well asdeath from competing risks, which if censored, tendsto inflate the cumulative incidence frequency andartificially accentuates differences between groups,therefore requiring a different modelling approach(8,9). Even assuming that competing risk was not anissue, the confidence intervals surrounding the hazardratios for MACE from their Cox proportional hazardsmodelling of abnormal perfusion in varied scenariosare sufficiently wide to suggest they should be inter-preted with appropriate caution.
WHY SHOULD WE STILL STRIVE FOR
CT MEASURES OF ISCHEMIA?
Even the most ardent enthusiast of cardiac CT wouldadmit to its limitations. However, so many advanceshave been made in vendor technology, dose-

Crean and Chow J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 3 8 8 – 9 1
1390
reduction, temporal resolution, reconstruction algo-rithms, and post-processing software that the claimthat cardiac CT is “a step backward” (10) seemsunduly harsh a decade later. Yet, several of Nissen’scriticisms undoubtedly still ring true to our ears (8).Despite excellent negative predictive value, everyreader will have experienced the frustration of tryingto interpret intermediate lesions or deciding whetherthere is simply too much calcium to be able to “readthrough.” The positive predictive value for obstruc-tive disease is variable in trials run by the world’sexperts and may be even lower in real life (11–13).Intravascular ultrasound studies have taught us thatwe routinely underestimate luminal area and thatinterobserver variability for the same lesion is wide(14). Perhaps more importantly, trials such as CECaT(Cost-Effectiveness of Noninvasive Cardiac Testing)(15,16), DEFER (17–19), FAME (Fractional FlowReserve Versus Angiography for Multivessel Evalua-tion) (20,21), and FAME 2 (Fractional Flow Reserve[FFR] Guided Percutaneous Coronary Intervention[PCI] Plus Optimal Medical Treatment [OMT] VersusOMT) (22) have repeatedly demonstrated thatischemia-driven management is as effective as, oroften more effective than, management decisionsbased upon luminography alone (23).
As a result, cardiac CT ischemia research has effec-tively branched in 2 different directions: stress perfu-sion imaging and CT-derived fractional flow reserve(CT-FFR) (24,25). Currently, most research efforts arefocused on the latter (aided by industryfinancing) withseveral encouraging trials having shown improveddiagnostic accuracy compared with CTA alone, even ifthe positive predictive values remain lower thanone might wish (26–29). Furthermore, data from thePLATFORM study (Prospective LongitudinAl Trial ofFFRct: Outcome and Resource IMpacts) suggest that aCT-FFR–guided strategy is associated with equivalentoutcomes and lower costs at 1 year compared with aninvasive angiography strategy (30). However, thetechnique remains limited to some degree by motionand image misregistration, although, counterintui-tively, coronary calcification does not seem to signifi-cantly affect accuracy (31,32). Also unclear is whetherCT-FFR analysis—which is currently provided off-sitecommercially by a single company—will be able toupscale operations quickly enough to cope withthe significant increase in volume expected sinceMedicare approval of the technique at the start of2018 (33). In the longer term, vendor-providedequivalent solutions at point of care will surely berequired.
With so much enthusiasm for deriving physiologyfrom CT, why has CTP failed to make more of an
impact? The reasons are multifactorial. Table time islimited in most hospitals, and fitting in stress studiesmay be difficult without knowing in advance whetherthe coronary anatomy will require this, especiallybecause a wash-out period for contrast is required be-tween the 2 portions of the study. Radiation dose isanother major concern and the dominant reason whysingle time point rather than dynamic CTP acquisitionprotocols have prevailed. Perhaps most importantly,CTP was unlucky to arrive at a time when the zeitgeistfavored computational approaches to identifyingischemia. These factors (together with industry spon-sorship of research in FFR-CT) have left CTP theawkward uncle at the wedding. A recent meta-analysisof published papers on (human) static CTP found fewerthan 1,200 patients, albeit with evidence that CTP im-proves specificity compared with CTA alone (34). Thepublished reports for dynamic CTP are even morelimited and have been dominated by a few centerswithdual-source technology. Mostly these studies havefocused on accuracy, although one multicenter regis-try publication did look at prognostic ability, andshowed, similar to Nakamura et al. (4), that visuallyappreciated perfusion defects provided additionalprognostication even after adjusting for CTA findingsand that the hazard for MACE was strongly related tothe number of abnormal segments (35).
SO, 2 OUT OF 3 AIN’T BAD?
There is a clear argument that CT needs to providephysiological assessment, but there is a dichotomyappearing in the published reports as to how to dothis best and most cost-effectively. Nakamura et al.(4) are to be congratulated for their efforts, and theirwork represents an important contribution to theexisting published experience with dynamic CTP.Whether prognostication is what drives the hand ofthe referring physician when choosing between testsis another matter. For CT perfusion to be acceptedlonger term, there needs to be much more work doneon harmonization of protocols and prospectivemultisite multivendor comparisons of static versusdynamic CTP methods—with a primary focus ondiagnosis and a (still important but) secondary focuson prognosis. We want and need CT perfusion, butwhether ultimately it will prove to be a flirtation or alasting love affair remains to be resolved.
ADDRESS FOR CORRESPONDENCE: Dr. Andrew M.Crean, Division of Cardiology, University of OttawaHeart Institute, 40 Ruskin Street, Ottawa, Ontario K1Y4W7, Canada. E-mail: [email protected].

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Crean and ChowJ U L Y 2 0 1 9 : 1 3 8 8 – 9 1 Editorial Comment
1391
RE F E RENCE S
1. AdayML. TwoOut of Three Ain’t Bad [song]. EpicRecords, 1977. Available at: https://www.azlyrics.com/lyrics/meatloaf/twooutofthreeaintbad.html.Accessed June 12, 2018.
2. Axel L. Cerebral blood flow determination byrapid-sequence computed tomography: theoret-ical analysis. Radiology 1980;137:679–86.
3. Miles KA, Hayball M, Dixon AK. Colour perfusionimaging: a new application of computed tomog-raphy. Lancet 1991;337:643–5.
4. Nakamura S, Kitagawa K, Goto Y, et al. Incre-mental prognostic value of myocardial blood flowquantified with stress dynamic computed tomog-raphy perfusion imaging. J Am Coll Cardiol Img2019;12:1379–87.
5. Saab R, Hage FG. Vasodilator stress agents formyocardial perfusion imaging. J Nucl Cardiol 2017;24:434–8.
6. Ritchie H, Roser M. Obesity. Our World in Datawebsite. 2018. Available at: https://ourworldindata.org/obesity. Accessed April 12, 2018.
7. Foley JRJ, Kidambi A, Biglands JD, et al.A comparison of cardiovascular magnetic reso-nance and single photon emission computedtomography (SPECT) perfusion imaging in leftmain stem or equivalent coronary artery disease: aCE-MARC substudy. J Cardiovasc Magn Reson2017;19:84.
8. Austin PC, Lee DS, Fine JP. Introduction to theanalysis of survival data in the presence ofcompeting risks. Circulation 2016;133:601–9.
9. Wolbers M, Koller MT, Stel VS, et al. Competingrisks analyses: objectives and approaches. EurHeart J 2014;35:2936–41.
10. Nissen SE. Limitations of computed tomogra-phy coronary angiography. J Am Coll Cardiol2008;52:2145–7.
11. Meijboom WB, Meijs MFL, Schuijf JD, et al.Diagnostic accuracy of 64-slice computed to-mography coronary angiography: a prospective,multicenter, multivendor study. J Am Coll Cardiol2008;52:2135–44.
12. Meijboom WB, Van Mieghem CAG, van Pelt N,et al. Comprehensive assessment of coronary ar-tery stenoses: computed tomography coronaryangiography versus conventional coronary angi-ography and correlation with fractional flowreserve in patients with stable angina. J Am CollCardiol 2008;52:636–43.
13. Groothuis JGJ, Beek AM, Meijerink MR, et al.Positive predictive value of computed tomographycoronary angiography in clinical practice. Int JCardiol 2012;156:315–9.
14. Kim C, Hong S-J, Shin D-H, et al. Limitations ofcoronary computed tomographic angiography fordelineating the lumen and vessel contours of
coronary arteries in patients with stable angina.Eur Heart J Cardiovasc Imaging 2015;16:1358–65.
15. Sharples L, Hughes V, Crean A, et al. Cost-effectiveness of functional cardiac testing in thediagnosis and management of coronary arterydisease: a randomised controlled trial. The CECaTtrial. Health Technol Assess 2007;11:iii–iv, ix.
16. Thom H, West NEJ, Hughes V, et al. Cost-effectiveness of initial stress cardiovascular MR,stress SPECT or stress echocardiography as a gate-keeper test, compared with upfront invasivecoronary angiography in the investigation andmanagement of patients with stable chest pain:mid-term outcomes from the CECaT randomisedcontrolled trial. BMJ Open 2014;4:e003419.
17. Zimmermann FM, Ferrara A, Johnson NP, et al.Deferral vs. performance of percutaneous coro-nary intervention of functionally non-significantcoronary stenosis: 15-year follow-up of theDEFER trial. Eur Heart J 2015;36:3182–8.
18. Bech GJ, De Bruyne B, Pijls NH, et al. Frac-tional flow reserve to determine the appropriate-ness of angioplasty in moderate coronary stenosis:a randomized trial. Circulation 2001;103:2928–34.
19. Pijls NHJ, van Schaardenburgh P,Manoharan G, et al. Percutaneous coronary inter-vention of functionally nonsignificant stenosis:5-year follow-up of the DEFER Study. J Am CollCardiol 2007;49:2105–11.
20. Tonino PAL, De Bruyne B, Pijls NHJ, et al.Fractional flow reserve versus angiography forguiding percutaneous coronary intervention.N Engl J Med 2009;360:213–24.
21. van Nunen LX, Zimmermann FM, Tonino PAL,et al. Fractional flow reserve versus angiographyfor guidance of PCI in patients with multivesselcoronary artery disease (FAME): 5-year follow-upof a randomised controlled trial. Lancet 2015;386:1853–60.
22. De Bruyne B, Pijls NHJ, Kalesan B, et al.Fractional flow reserve-guided PCI versus medicaltherapy in stable coronary disease. N Engl J Med2012;367:991–1001.
23. Heyndrickx GR, Tóth GG. The FAME trials:impact on clinical decision making. Interv Cardiol2016;11:116–9.
24. Taylor CA, Fonte TA, Min JK. Computationalfluid dynamics applied to cardiac computed to-mography for noninvasive quantification of frac-tional flow reserve: scientific basis. J Am CollCardiol 2013;61:2233–41.
25. Hulten E, Ahmadi A, Blankstein R. CT assess-ment of myocardial perfusion and fractional flowreserve. Prog Cardiovasc Dis 2015;57:623–31.
26. Koo B-K, Erglis A, Doh J-H, et al. Diagnosisof ischemia-causing coronary stenoses by
noninvasive fractional flow reserve computedfrom coronary computed tomographic angio-grams. Results from the prospective multicenterDISCOVER-FLOW (Diagnosis of Ischemia-CausingStenoses Obtained Via Noninvasive FractionalFlow Reserve) study. J Am Coll Cardiol 2011;58:1989–97.
27. Min JK, Leipsic J, Pencina MJ, et al. Diagnosticaccuracy of fractional flow reserve from anatomicCT angiography. JAMA 2012;308:1237–45.
28. Nørgaard BL, Leipsic J, Gaur S, et al. Diag-nostic performance of noninvasive fractional flowreserve derived from coronary computed tomog-raphy angiography in suspected coronary arterydisease: the NXT trial (Analysis of Coronary BloodFlow Using CT Angiography: Next Steps). J AmColl Cardiol 2014;63:1145–55.
29. Li S, Tang X, Peng L, Luo Y, Dong R, Liu J. Thediagnostic performance of CT-derived fractionalflow reserve for evaluation of myocardialischaemia confirmed by invasive fractional flowreserve: a meta-analysis. Clin Radiol 2015;70:476–86.
30. Douglas PS, De Bruyne B, Pontone G, et al.1-Year outcomes of FFRCT-guided care in pa-tients with suspected coronary disease: thePLATFORM study. J Am Coll Cardiol 2016;68:435–45.
31. Leipsic J, Yang T-H, Thompson A, et al. CTangiography (CTA) and diagnostic performance ofnoninvasive fractional flow reserve: results fromthe Determination of Fractional Flow Reserve byAnatomic CTA (DeFACTO) study. AJR Am JRoentgenol 2014;202:989–94.
32. Nørgaard BL, Gaur S, Leipsic J, et al. Influenceof coronary calcification on the diagnostic per-formance of CT angiography derived FFR in coro-nary artery disease: a substudy of the NXT trial.J Am Coll Cardiol Img 2015;8:1045–55.
33. CMS Will Pay For FFR-CT NoninvasiveCoronary Analysis. DAIC website. November 6,2017. Available at: https://www.dicardiology.com/content/cms-will-pay-ffr-ct-noninvasive-coronary-analysis. Accessed June 10, 2018.
34. Sørgaard MH, Kofoed KF, Linde JJ, et al.Diagnostic accuracy of static CT perfusion for thedetection of myocardial ischemia. A systematicreview and meta-analysis. J Cardiovasc ComputTomogr 2016;10:450–7.
35. Meinel FG, Pugliese F, Schoepf UJ, et al.Prognostic value of stress dynamic myocardialperfusion CT in a multicenter population withknown or suspected coronary artery disease. AJRAm J Roentgenol 2017;208:761–9.
KEY WORDS FFR-CT, CTA, CTP, perfusion

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E
AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
ORIGINAL RESEARCH
A Comparison of the UpdatedDiamond-Forrester, CAD Consortium,and CONFIRM History-Based Risk Scoresfor Predicting Obstructive CoronaryArtery Disease in Patients WithStable Chest Pain
The SCOT-HEART Coronary CTA CohortLohendran Baskaran, MD,a,b Ibrahim Danad, MD,a Heidi Gransar, MS,a Bríain Ó Hartaigh, PHD,a
Joshua Schulman-Marcus, MD,a Fay Y. Lin, MD,a Jessica M. Peña, MD, MPH,a Amanda Hunter, MD,c
David E. Newby, MD,c Philip D. Adamson, MD,c,* James K. Min, MDa,*
ABSTRACT
ISS
FrobN
Kin
by
He
OBJECTIVES This study sought to compare the performance of history-based risk scores in predicting obstructive
coronary artery disease (CAD) among patients with stable chest pain from the SCOT-HEART study.
BACKGROUND Risk scores for estimating pre-test probability of CAD are derived from referral-based populations with
a high prevalence of disease. The generalizability of these scores to lower prevalence populations in the initial patient
encounter for chest pain is uncertain.
METHODS We compared 3 scores among patients with suspected CAD in the coronary computed tomographic angi-
ography (CTA) randomized arm of the SCOT-HEART study for the outcome of obstructive CAD by coronary CTA: the
updated Diamond-Forrester score (UDF), CAD Consortium clinical score (CAD2), and CONFIRM risk score (CRS). We tested
calibration with goodness-of-fit, discrimination with area under the receiver-operating curve (AUC), and reclassification
with net reclassification improvement (NRI) to identify low-risk patients.
RESULTS In 1,738 patients (age 58 � 10 years and 44.0% women), overall calibration was best for UDF, with under-
estimation by CRS and CAD2. Discrimination by AUC was highest for CAD2 at 0.79 (95% confidence interval [CI]: 0.77 to
0.81) than for UDF (0.77 [95% CI: 0.74 to 0.79]) or CRS (0.75 [95% CI: 0.73 to 0.77]) (p < 0.001 for both comparisons).
Reclassification of low-risk patients at the 10% probability threshold was best for CAD2 (NRI 0.31, 95% CI: 0.27 to 0.35)
followed by CRS (NRI 0.21, 95% CI: 0.17 to 0.25) compared with UDF (p < 0.001 for all comparisons), with a consistent
trend at the 15% threshold.
CONCLUSIONS In this multicenter clinic-based cohort of patients with suspected CAD and uniform CAD evaluation by
coronary CTA, CAD2 provided the best discrimination and classification, despite overestimation of obstructive CAD as
evaluated by coronary CTA. CRS exhibited intermediate performance followed by UDF for discrimination and
reclassification. (J Am Coll Cardiol Img 2019;12:1392–400) © 2019 Published by Elsevier on behalf of the
American College of Cardiology Foundation.
N 1936-878X/$36.00 https://doi.org/10.1016/j.jcmg.2018.02.020
m the aDepartment of Radiology, New York–Presbyterian Hospital and the Weill Cornell Medical College, New York, New York;
ational Heart Centre, Singapore; and the cUniversity of Edinburgh/BHF Centre for Cardiovascular Science, Edinburgh, United
gdom. *Drs. Adamson and Min contributed equally to this work and are joint senior authors. This work is supported in part
the Dalio Institute of Cardiovascular Imaging and the Michael Wolk Foundation. Dr. Min has served as a consultant to
artFlow and Abbott Vascular; on the medical advisory boards of GE Healthcare and Arineta; as a consultant for HeartFlow,

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Baskaran et al.J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0 Comparison of History-Based Risk Scores for Pre-Test Probability of CAD
1393
AB BR E V I A T I O N S
AND ACRONYM S
AUC = area under the curve
CAD = coronary artery disease
CAD2 = CAD Consortium
clinical score
CRS = CONFIRM risk score
CTA = computed tomography
angiography
ICA = invasive coronary
angiography
NRI = net reclassification
improvement
PTP = pre-test probability
ROC = receiver-operating
characteristics
UDF = updated Diamond-
Forrester
C oronary artery disease (CAD) is a leadingglobal health burden and a common causeof chest pain. In patients with chest pain,
guidelines recommend initial diagnostic evaluationby assessment of an individual’s pre-test probability(PTP) of CAD to make decisions regarding furtherdiagnostic testing (1–4). Accurate assessment of PTPaffects the accuracy, yield, and cost-effectivenessof downstream diagnostic testing (5). Multiple riskscores have been developed to systematize riskassessment based on clinical history, includingthe updated Diamond-Forrester (UDF), CADConsortium 2 (CAD2), and the CONFIRM registryscores (CRS) (6–8). However, previous evaluationsand comparisons have been performed in referralcohorts for diagnostic testing, with disparate cutoffsfor low-, intermediate-, and high-risk categories,and score performance may deteriorate if applied tomore general chest pain populations (9–11).
We sought to compare the performance of the UDF,CAD2, and CRS scores in predicting the probability ofobstructive CAD in the coronary computed tomogra-phy angiography (CTA)-randomized arm of the Scot-tish COmputed Tomography of the HEART trial(SCOT-HEART) study, a multicenter cohort of pa-tients with chest pain enrolled in the clinic who un-derwent coronary CTA. We also evaluated scoreperformance within important age- and sex-basedsubgroups.
SEE PAGE 1401
METHODS
STUDY POPULATION. Details of the SCOT-HEARTstudy have been described elsewhere (12,13). Briefly,between 2010 and 2014, patients with suspected sta-ble angina were recruited from chest-pain clinics andrandomized to usual care plus coronary CTA versususual care alone. Participants were excluded if theypresented with acute chest pain, renal failure, and/oracute coronary syndrome within 3 months ofrecruitment. Patients gave written informed consent,and the study was approved by the research ethicscommittee. We included only patients in the coronaryCTA randomized arm who had no previous CAD andwho had information on all variables needed for the 3
NeoGraft Technologies, MyoKardia, and CardioDx; and holds ownership in
raria and consultancy from Toshiba Medical Systems; and is also supported
Wellcome Trust Senior Investigator Award (WT103782AIA). All other auth
relevant to the contents of this paper to disclose. Pamela Douglas, MD, serv
Manuscript received January 26, 2018; revised manuscript received Februar
scores, as only the coronary CTA arm under-went uniform evaluation of CAD. Of 2,073patients in the coronary CTA arm of theSCOT-HEART trial, 1,738 patients were ulti-mately included for analysis (Figure 1).
CLINICAL DEFINITIONS. Medical history wasobtained at the time of enrollment. Cardio-vascular risk factors were ascertained by re-view of patients’ medical records (14–16). TheNational Institute for Clinical HealthcareExcellence (NICE) clinical guideline on chestpain was used to categorize chest pain astypical, atypical, or nonanginal (14).
CARDIAC CT SCAN PROTOCOL. All patientsunderwent coronary CTA using a 64-slice(Brilliance 64, Philips Medical Systems, Best,the Netherlands, and Biograph mCT,Siemens, Erlangen, Germany) and a 320-slice
CT scanner (Aquilion ONE, Toshiba Medical Systems,Tokyo, Japan) at 3 imaging sites. The scans weregraded by at least 2 accredited assessors(a cardiologist and radiologist). Obstructive CAD wasdefined as a stenosis causing $50%-diameter stenosison coronary CTA. Intraobserver agreement was 95%,and interobserver agreement was 91% (17).PREDICTION RISK SCORES OF
SIGNIFICANT CAD
Risk scores were calculated for each patient. The UDFrequires only age, sex, and symptom typicality (6).The CAD2 score additionally requires smoking status,diabetes, hypercholesterolemia, hypertension, andbody mass index (BMI) (7), whereas the CRSadditionally requires diabetes, hypertension, familyhistory of CAD, and current smoking status(Supplemental Table 1) (8).
STATISTICAL METHODS
The clinical outcome of interest was obstructive CAD.Continuous variables were described as mean � SD, ormedians with interquartile ranges when appropriate;categorical variables were displayed as frequenciesand percentages. Variables were compared bychi-square statistic for categorical variables and byStudent’s unpaired t test or Mann-Whitney
MDDX and AutoPlaq. Dr. Newby has received hono-
by the British Heart Foundation (CH/09/002) and a
ors have reported that they have no relationships
ed as the Guest Editor for this paper.
y 22, 2018, accepted February 23, 2018.

FIGURE 1 Flow Diagram of Patients From the SCOT-HEART Trial for the Comparison of
CAD Risk Scores
1,083 without obstructiveCAD
35 inadequate informationexcluded
300 with prior CADexcluded
2,073 randomized to non-coronary CTA arm
4,146 patients recruited inSCOT-HEART
2,073 randomized tocoronary CTA arm
1,773 with no prior CAD
1,738 with requiredinformation for all 3 scores
655 with obstructive CAD
Patients in the coronary CTA-randomized arm were included if they had no previous CAD
and had adequate information to calculate all 3 history-based clinical scores: the CAD2
Consortium Score (CAD2), the Updated Diamond-Forrester risk score (UDF), and the
CONFIRM Risk Score (CRS). CAD ¼ coronary artery disease; CTA ¼ computed tomog-
raphy angiography.
TABLE 1
Age, yrs
Female
Typical an
Atypical a
Nonangina
Diabetes m
Dyslipidem
Hypertens
Family his
Smoker
Values are m
CAD ¼ co
Baskaran et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Comparison of History-Based Risk Scores for Pre-Test Probability of CAD J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0
1394
nonparametric test when appropriate for continuousvariables. To assess the calibration of each scoreassigned to the SCOT-HEART population, observedand predicted risk was computed based on categoriesdefined by quintiles of predicted risk. The Hosmer-Lemeshow goodness-of-fit (GOF) chi-square statisticacross each quintile was then calculated to measurethe agreement between observed and predictedevents. The discrimination of each score was thenassessed via the area under the curve (AUC) for the
Baseline Characteristics
Total(N ¼ 1,738)
ObstructiveCAD
(n ¼ 655)
NonobstructiveCAD
(n ¼ 1,083) p Value
57.6 � 9.5 61.4 � 7.9 55.3 � 9.7 <0.001
764 (44.0) 175 (26.7) 589 (54.4) <0.001
gina 643 (37.0) 363 (55.4) 280 (25.9) <0.001
ngina 420 (24.2) 136 (20.8) 284 (26.2) 0.01
l chest pain 675 (38.8) 156 (23.8) 519 (47.9) <0.001
ellitus 190 (10.9) 84 (12.8) 106 (9.8) 0.05
ia 939 (54.0) 473 (72.2) 466 (43.0) <0.001
ion 606 (34.9) 294 (44.9) 312 (28.8) <0.001
tory of CAD 755 (43.4) 267 (40.8) 488 (45.1) 0.08
322 (18.5) 125 (19.1) 197 (18.2) 0.64
ean � SD or n (%).
ronary artery disease.
receiver-operating characteristics (ROC) curve, thencompared using the Hanley and McNeil method forpaired data (18).
To assess the potential difference in decision-making impact of one score over another, reclassifi-cation was evaluated by use of net reclassificationimprovement (NRI), which assesses the improvementof an added model in comparison with a base model(19). For clinical relevance, NRI was assessed in a bi-nary manner to identify low-risk patients, defined asthose not requiring further testing as recommendedby contemporary guidelines. The cutoffs chosen wereat <10% and <15% PTP of disease, per guidelines(1–4). A score is penalized for incorrectly classifiedsubjects (20,21). For this study, the reclassificationperformance of CAD2 and CRS was compared withUDF. Subsequently, CAD2 was used as a base model.Analyses were conducted using Stata version 14(StataCorp LP, College Station, Texas) and SASversion 9.2 (SAS Institute Inc., Cary, North Carolina).Subgroups based on sex and an age cutoff of 65 yearswere evaluated for score calibration and discrimina-tion, but there was insufficient sample size to calcu-late score NRIs based on binary categories. A 2-tailedp value <0.05 was considered statistically significantfor all analyses.
RESULTS
The mean age was 58 � 10 years, 764 (44.0%) werewomen, and 655 (37.7%) had obstructive CAD(Table 1). In addition to being older, patients withobstructive CAD were more likely to be male; havediabetes, hypertension, dyslipidemia; and to exhibittypical angina.
The calibration of the overall cohort demonstrateda good fit for UDF, with no significant deviationbetween observed and expected cases (chi-square4.13; p ¼ 0.53) (Figures 2 and 3). CAD2 underestimatedthe likelihood of obstructive CAD across the riskspectrum (chi-square 35.17; p < 0.001), as did CRS to alesser extent (chi-square 17.22; p ¼ 0.004).
Continuous ROC analysis revealed the AUC for UDFto be 0.767 (95% confidence interval [CI]: 0.744 to0.790), CAD2 to be 0.790 (95% CI: 0.768 to 0.811), andCRS to be 0.749 (95% CI: 0.726 to 0.771) (Figure 4).CAD2 exhibited significantly higher AUC comparedwith UDF and CRS (p < 0.001 for both), with anonsignificant difference between UDF and CRSscores (p ¼ 0.14).
At a probability cutoff of 10% to identify low-riskpatients before further diagnostic testing, CAD2compared with UDF correctly reclassified 45.7% ofpatients with nonobstructive CAD at the cost of

FIGURE 2 Hosmer-Lemeshow Goodness-of-Fit for the Overall Cohort Across the Risk Spectrum
.6
.8
.2
.4
00 .2 .4
UDF
(X2 4.13; p = 0.53)
Predicted (Proportion).6 .8
A
Observed (Proportion) Predicted (Proportion)
CAD2
(X2 35.17; p < 0.001)
.6
.8
.2
.4
0.2 .4
Predicted (Proportion).6 .8
B
CRS
(X2 17.22; p = 0.004)
.6
.8
.2
.4
.2 .4Predicted (Proportion)
.6 .8
C
(A) UDF demonstrates good calibration for diagnosis of obstructive CAD by coronary CTA, whereas (B) CAD2 and (C) CRS exhibit overestimation of risk. Abbreviations as
in Figure 1.
FIGURE 3 Observed and Predicted Frequencies Across Quintiles of Risk for Obstructive CAD
UDF CAD2 CRS
Patie
nts (
%)
100.0
60.070.080.090.0
30.040.050.0
10.020.0
0.01 2 3 4 5 1 2 3 4 5 1 2 3 4 5
AUDF CAD2 CRS
Patie
nts (
%)
100.0
60.070.080.090.0
30.040.050.0
10.020.0
0.01 2 3 4 5 1 2 3 4 5 1 2 3 4 5
B
UDF CAD2 CRS
Patie
nts (
%)
100.0
60.070.080.090.0
30.040.050.0
10.020.0
0.01 2 3 4 5 1 2 3 4 5 1 2 3 4 5
CUDF CAD2 CRS
Patie
nts (
%)
100.0
60.070.080.090.0
30.040.050.0
10.020.0
0.01 2 3 4 5 1 2 3 4 5 1 2 3 4 5
D
Observed Expected
(A) For male patients, UDF fit well (chi-square 6.90; p ¼ 0.23), whereas both CAD2 and CRS underestimated risk (chi-square 20.3 and 27.6, respectively; p < 0.001 for
both). (B) For female patients, both UDF and CRS fit well (chi-square 8.98, p ¼ 0.11 and chi-square 1.30, p ¼ 0.86, respectively), whereas CAD2 underestimated risk
(chi-square 17.07; p ¼ 0.004). (C) For patients age <65 years, there was good calibration for UDF (chi-square 7.62; p ¼ 0.60) and CRS (chi-square 6.90; p ¼ 0.11) and
poor calibration for CAD2 (chi-square 19.43; p ¼ 0.002). (D) For patients $65 years of age, all 3 models had good calibration (p ¼ NS for all). Abbreviations as in
Figure 1.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Baskaran et al.J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0 Comparison of History-Based Risk Scores for Pre-Test Probability of CAD
1395

FIGURE 4 ROC Analysis Across All 3 Scores
Sens
itivi
ty
1.00
0.00
0.25
0.50
0.75
0.00 0.25 0.501-Specificity
0.75 1.00
Sens
itivi
ty
1.00
0.00
0.25
0.50
0.75
0.00 0.25 0.501-Specificity
0.75 1.00
Sens
itivi
ty
1.00
0.00
0.25
0.50
0.75
0.00 0.25 0.501-Specificity
0.75 1.00
Sens
itivi
ty
1.00
0.00
0.25
0.50
0.75
0.00 0.25 0.501-Specificity
0.75 1.00
Sens
itivi
ty
1.00
0.75
0.50
0.25
0.00
0.00 0.25 0.501-Specificity
0.75
0.7488
0.7898
0.7667
p < 0.001
p < 0.001p = 0.14
CRS
CAD2
UDF
CRS
CAD2
UDF
CRS
CAD2
UDF
CRS
CAD2
UDF
CRS
CAD2
UDF
1.00
A
B
0.7374
0.7775
0.7583
p < 0.001
p < 0.001p = 0.19
D
0.7419
0.7857
0.7588
p < 0.001
p < 0.001p = 0.345
C
0.6891
0.7221
0.6863
p = 0.079
p < 0.001p = 1.00
E
0.6877
0.7380
0.7300
p = 0.007
p = 0.722p = 0.07
(A) In the overall group, CAD2 exhibited significantly higher AUC compared with UDF and CRS (p < 0.001 for both), with a nonsignificant difference between UDF and
CRS scores (p ¼ 0.14). Consistent patterns were observed for (B) male patients, (C) female patients, (D) <65 years of age, and (E) $65 years of age. ROC ¼ receiver-
operating characteristic; other abbreviations as in Figure 1.
Baskaran et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Comparison of History-Based Risk Scores for Pre-Test Probability of CAD J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0
1396
incorrectly reclassifying 14.8% of patients withobstructive CAD, resulting in NRI of 0.31 (95% CI: 0.27to 0.35; p < 0.001) (Table 2). CRS improved reclassi-fication compared with UDF with an NRI of 0.21 (95%CI: 0.17 to 0.25; p < 0.001) but incorrectly classified
more patients than CRS with NRI of –0.10 (95% CI:–0.14 to 0.06; p < 0.001). A consistent pattern of su-perior reclassification for CAD2 was observed at aprobability cutoff of 15%, with NRI of 0.23 (95% CI:0.19 to 0.27; p < 0.001) compared with UDF, followed

TABLE 2 Net Reclassification Improvement for the Updated Diamond-Forrester, CAD Consortium Clinical, and CONFIRM Risk Scores
Base Model Comparison Model CAD2 p Value CRS p Value
UDF (10% cutoff) % Obstructive correctly reclassified �14.8 <0.001 �8.2 <0.001
% Nonobstructive correctly reclassified 45.7 <0.001 29.1 <0.001
NRI (95% CI) 0.31 (0.27, 0.35) <0.001 0.21 (0.17, 0.25) <0.001
UDF (15% cutoff) % Obstructive correctly reclassified �17.6 <0.001 �25.6 <0.001
% Nonobstructive correctly reclassified 40.6 <0.001 45.2 <0.001
NRI (95% CI) 0.23 (0.19, 0.27) <0.001 0.20 (0.15, 0.24) <0.001
CAD2 (10% cutoff) % Obstructive correctly reclassified – – 6.6 <0.001
% Nonobstructive correctly reclassified – – �16.6 <0.001
NRI (95% CI) – – –0.10 (–0.14, –0.06) <0.001
CAD2 (15% cutoff) % Obstructive correctly reclassified – – �8.1 <0.001
% Nonobstructive correctly reclassified – – 4.5 <0.001
NRI (95% CI) – – �0.04 (–0.07, 0.00) 0.08
CAD2 ¼ CAD Consortium clinical score; CI ¼ confidence interval; CRS ¼ CONFIRM risk score; NRI ¼ net reclassification improvement; UDF ¼ updated Diamond-Forrester.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Baskaran et al.J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0 Comparison of History-Based Risk Scores for Pre-Test Probability of CAD
1397
by CRS with NRI of 0.20 (95% CI: 0.15 to 0.24; p <
0.001) compared with UDF. Similar to the 10%threshold, CRS compared with CAD2 trended towardworse reclassification, with NRI of –0.04 (95% CI:–0.07 to 0.00; p ¼ 0.08).SEX- AND AGE-BASED SUBGROUPS. For male pa-tients, UDF fit well (chi-square 6.90; p¼0.23), whereasboth CAD2 and CRS underestimated risk (chi-square20.3 and 27.6, respectively; p < 0.001 for both). Therewas no significant difference in AUC between UDF andCRS scores (p for difference¼0.19) for men. For femalepatients, both UDF and CRS fit well (chi-square 8.98,p ¼ 0.11 and chi-square 1.30, p ¼ 0.86, respectively),whereas CAD2 underestimated risk (chi-square 17.07;p ¼ 0.004). For women, UDF had the lowest AUC of0.686 (95% CI: 0.642 to 0.730), CAD2 had the highestAUC of 0.722 (95%CI: 0.680 to 0.763), and CRSAUCwas0.689 (95% CI: 0.646 to 0.732). There was a differencebetween the AUC of UDF and CAD2 (p < 0.001) but nodifference in AUC between CRS and UDF (p ¼ 1.00) orCAD2 (p ¼ 0.08).
A similar pattern was observed for the cohortage <65 years, with good calibration for UDF (chi-square 7.62; p ¼ 0.60) and CRS (chi-square 6.90; p ¼0.11) and poor calibration for CAD2 (chi-square 19.43;p ¼ 0.002). For the cohort age <65 years, CAD2 hadthe highest AUC (0.786, 95% CI: 0.759 to 0.812) (p <
0.001 when compared with UDF or CRS), followed byUDF (0.759, 95% CI: 0.730 to 0.787), then CRS (0.742,95% CI: 0.714 to 0.770). There was no difference inAUC between UDF and CRS (p ¼ 0.345). For age $65years, all 3 models had good calibration (p ¼ NS forall). For the cohort $65 years, the AUC for CAD2(0.738, 95% CI: 0.692 to 0.783) was higher than thatfor CRS (0.688, 95% CI: 0.641 to 0.734) (p ¼ 0.01). AUCfor UDF (0.730, 95% CI: 0.685 to 0.775) was nodifferent from CAD2 or CRS (p ¼ NS for both).
DISCUSSION
In this population of contemporary stableoutpatients with chest pain who underwent uniformstudy-mandated coronary CTA, CAD2 provided thebest discrimination and reclassification for the overallpatient population as well as among women,although it overestimated PTP of obstructive CAD asdetermined by coronary CTA. UDF displayed goodcalibration but lesser discrimination and reclassifica-tion. CRS, which has not been externally validatedexcept in the original manuscript, had equivalentperformance to UDF in some but not all age- and sex-based subgroups for calibration, discrimination, andreclassification.
Candidate scores were chosen to reflect the infor-mation available to clinicians during an initial patientencounter for chest pain and applicability to symp-tomatic patients. UDF, validated against an invasivecoronary angiography (ICA)-based referral cohort,replaces the original ubiquitous Diamond-Forresterscore recommended in American College of Cardiol-ogy/American Heart Association guidelines, relies ononly demographics and chest pain typicality, and iscurrently recommended in European Society of Car-diology guidelines (1,2,4,6,7). CAD2 includes tradi-tional CAD risk factors and basic laboratoryevaluation of lipid profile and has been validatedagainst both ICA-based and coronary CTA-basedreferral cohorts (7,22,23). CRS has been validated ina coronary CTA-based and myocardial perfusionstress-based cohort and requires only patient medicalhistory, which may make it suitable for point-of-caredecisions in an initial patient encounter (8).
In the current study, we sought to examine theperformance of risk scores in a population that uni-formly underwent evaluation for CAD with minimal

Baskaran et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Comparison of History-Based Risk Scores for Pre-Test Probability of CAD J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0
1398
post-test referral bias. This contrasts with previousstudies that have derived and validated scores inpatients who had already been referred for furtherinvestigations (6,7,9–11,18,24). Thus, the populationstudied herein is representative of patients wherepre-test assessment with scores may have optimalutility (2). It also bears mentioning that baselinecharacteristics of the current study sample werebroadly similar to other cohorts enrolled in previouslarge cardiac CT registries (25–28).
A coronary CTA-based definition of obstructiveCAD was chosen rather than an ICA- or ischemia-based definition because there are no large-scaleICA- or ischemia-based cohorts without work-upbias of sufficient size to compare risk scores. SCOT-HEART is one of the very few patient populations,along with other coronary CTA intervention trialssuch as the PROMISE (Prospective Multicenter Imag-ing Study for Evaluation of Chest Pain) trial, in whichrisk scores can be tested uniformly. Because 85% ofthe patients in the overall SCOT-HEART cohort hadexercise treadmill testing (ETT) prior to enrollment,there may have been referral bias that would affectthe performance characteristics for ETT but not forcoronary CTA (13). However, because coronary CTAhas a high negative predictive value for obstructiveCAD by ICA but a lower positive predictive value, it islikely that the prevalence of obstructive CAD isoverestimated in our study. Thus, our study is moreuseful for evaluation of discrimination and reclassi-fication and less useful for evaluation of calibration.
Overall, CAD2 provided the best discrimination.This may be because its derivation included a range ofprevalences, giving it broad applicability (7). The AUCvalue in this study is similar to the value obtained byBittencourt et al. (22). However, in a higher (59%)prevalence group, the AUC obtained was lower.Notably, this study was for patients presenting withtypical angina and not the intended population for adiagnostic risk score (23). A more parsimoniousversion of the CAD2 score has been applied to theSCOT-HEART population, with comparison to thePROMISE minimal-risk tool (29). However, this com-parison was for the identification of low-risk patientswithout CAD. The AUC for UDF obtained in the cur-rent study was 0.767, comparable to its previousvalidation (6), although higher than the value ob-tained by Jensen et al. (9). In the original paper, CRSwas validated in 2 cohorts: 1 undergoing coronaryCTA and the other myocardial perfusion scintigraphy(MPS). AUCs of 0.710 and 0.770 were obtained,respectively (8). The AUC for CRS in the current studywas between both values, suggesting translatabilityacross cohorts.
The binary NRI analysis using guideline-recommended cutoffs was intended to havereal-world applicability by streamlining risk-scoreselection and to help avoid further unnecessarytesting in patients with low PTP. At a threshold of10% and 15%, CAD2 demonstrated consistentlyimproved reclassification of low-risk patients, iden-tifying patients among whom further testing wouldnot be warranted. CRS was slightly inferior at athreshold of 10%, whereas UDF exhibited the worstperformance to identify low-risk patients. This maybe a reflection of the increased accuracy of CAD2 andCRS derived from the greater number of variablesrequired when compared with UDF.
Score calibration is easily affected by the preva-lence of disease in the validation populationcompared with the prevalence in the derivationpopulation. It follows that, as UDF derivation andvalidation cohorts had high prevalences of obstruc-tive CAD, it thus exhibited the best calibration againsta coronary CTA gold standard (6). Conversely, CAD2and CRS, which demonstrated good calibration incoronary CTA studies with a lower prevalence,underestimated the probability of obstructive CAD bycoronary CTA (7,8,23).
On the basis of this study, we find that, in a generalchest-pain population with availability of lipid pro-files, CAD2 has the best discrimination and reclassi-fication across all groups. UDF, althoughparsimonious, has the poorest discriminatory andreclassification performance. CRS may be more usefulin preference to UDF for point-of-care estimation ofCAD probability by medical history at the first clinicvisit, before lipid-profile results become available.STUDY LIMITATIONS. First, the use of coronary CTAas a gold standard for obstructive CAD limits evalu-ation for calibration, as mentioned earlier, but al-lows for a generalizable comparison of these scoresin initial evaluation of chest pain with minimalwork-up bias, which has not been previously per-formed. Second, we evaluated NRI for each score atthresholds that differ from the original manuscriptsbut allow comparison of scores in uniform manner(21). However, to guide clinicians, we chose a priorito compare reclassification qualities of thesedifferent scores in a large, external, generalizablecohort. Third, we chose a limited number of scoresbased on the information that would be availableduring an initial patient encounter. We cannotcomment on the performance of CAD2, UDF, andCRS compared with scores incorporating coronarycalcium, exercise treadmill, or biomarker results,which would only be available at a follow-up patientencounter and thus cannot aid clinicians who need

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: In the SCOT-
HEARTcoronaryCTA-randomizedcohort, thepre-testprobabilityof
obstructive CAD in stable patients with chest pain is best estimated
by the CAD2 score, followed by the CRS, and then the UDF scores,
withconsistencyacross sex-andage-based subgroups, asevaluated
by discrimination and classification. Our results may be useful for
point-of-careestimationofCADprobabilitybymedicalhistoryat the
first clinic visit.
TRANSLATIONAL OUTLOOK: The downstream effect of
different estimates of pretest probability of obstructive CAD by
coronary CTA should be assessed for clinical outcomes including
obstructive CAD by ICA, cath normalcy, and major adverse car-
diac events.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Baskaran et al.J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0 Comparison of History-Based Risk Scores for Pre-Test Probability of CAD
1399
to make immediate decisions about referral to diag-nostic work-up for evaluation of chest pain. Finally,although this comparison of scores assesses re-lationships that may suggest clinical utility, theactual effect of each score in guiding processes ofpatient care is not directly evaluated.
CONCLUSIONS
At the first clinic encounter for patients with chestpain, estimation of the pre-test probability ofobstructive CAD by coronary CTA with history-basedscores may be best performed with CAD2, with thehighest discrimination and accurate reclassificationof low-risk patients with <10% probability ofobstructive CAD. When less information is availableinitially, CRS exhibits intermediate performance fol-lowed by UDF for discrimination and reclassification.This comparison is robust in that CAD evaluation wasuniformly performed in the coronary CTA-randomized arm of the SCOT-HEART study. Howev-er, calibration is generally underestimated usingcoronary CTA as the reference standard. Consistenttrends are observed in sex- and age-based subgroups,most notably in women.
ACKNOWLEDGMENTS Dr. Newby thanks the BritishHeart Foundation (CH/09/002) and the Wellcome
Trust Senior Investigator Award (WT103782AIA)donors for their support.
ADDRESS FOR CORRESPONDENCE: Dr. James K. Min,Dalio Institute of Cardiovascular Imaging, Weill CornellMedical College, 413 East 69th Street, New York, NewYork 10021. E-mail: [email protected].
RE F E RENCE S
1. Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for theDiagnosis and Management of Patients With Sta-ble Ischemic Heart Disease. Executive Summary: AReport of the American College of CardiologyFoundation/American Heart Association TaskForce on Practice Guidelines and the AmericanCollege of Physicians, American Association forThoracic Surgery, Preventive CardiovascularNurses Association, Society for CardiovascularAngiography and Interventions, and Society ofThoracic Surgeons. J Am Coll Cardiol 2012;60:2564–603.
2. Fihn SD, Blankenship JC, Alexander KP, et al.2014 ACC/AHA/AATS/PCNA/SCAI/STS FocusedUpdate of the Guideline for the Diagnosis andManagement of Patients With Stable IschemicHeart Disease: A Report of the American Collegeof Cardiology/American Heart Association TaskForce on Practice Guidelines and the AmericanAssociation for Thoracic Surgery, Preventive Car-diovascular Nurses Association, Society for Car-diovascular Angiography and Interventions, andSociety of Thoracic Surgeons. J Am Coll Cardiol2014;64:1929–49.
3. Skinner JS, Smeeth L, Kendall JM, et al. NICEguidance. Chest pain of recent onset: assessmentand diagnosis of recent onset chest pain ordiscomfort of suspected cardiac origin. Heart2010;96:974–8.
4. Montalescot G, Sechtem U, Achenbach S, et al.2013 ESC guidelines on the management of stablecoronary artery disease: the Task Force on theManagement of Stable Coronary Artery Disease ofthe European Society of Cardiology. Eur Heart J2013;34:2949–3003.
5. Genders TSS, MeijboomWB, Meijs MFL, et al. CTcoronary angiography in patients suspected ofhaving coronary artery disease: decision makingfrom various perspectives in the face of uncer-tainty. Radiology 2009;253:734–44.
6. Genders TSS, Steyerberg EW, Alkadhi H, et al.A clinical prediction rule for the diagnosis of cor-onary artery disease: validation, updating, andextension. Eur Heart J 2011;32:1316–30.
7. Genders TSS, Steyerberg EW, Hunink MGM,et al. Prediction model to estimate presence ofcoronary artery disease: retrospective pooledanalysis of existing cohorts. BMJ 2012;344:e3485.
8. Min JK, Dunning A, Gransar H, et al. Medicalhistory for prognostic risk assessment and diag-nosis of stable patients with suspected coronaryartery disease. Am J Med 2015;128:871–8.
9. Jensen JM, Voss M, Hansen VB, et al. Riskstratification of patients suspected of coronaryartery disease: comparison of five differentmodels. Atherosclerosis 2012;220:557–62.
10. Wasfy MM, Brady TJ, Abbara S, et al.Comparison of the Diamond-Forrester method
and Duke Clinical Score to predict obstructivecoronary artery disease by computed tomo-graphic angiography. Am J Cardiol 2012;109:998–1004.
11. Versteylen MO, Joosen IA, Shaw LJ, et al.Comparison of Framingham, PROCAM, SCORE, andDiamond Forrester to predict coronary athero-sclerosis and cardiovascular events. J Nucl Cardiol2011;18:904–11.
12. Newby DE, Williams MC, Flapan AD, et al. Roleof multidetector computed tomography in thediagnosis and management of patients attendingthe rapid access chest pain clinic, the ScottishComputed Tomography of the Heart (SCOT-HEART) trial: study protocol for randomizedcontrolled trial. Trials 2012;13:184.
13. SCOT-HEART Investigators. CT coronary angi-ography in patients with suspected angina due tocoronary heart disease (SCOT-HEART): anopen-label, parallel-group, multicentre trial. Lan-cet 2015;385:2383–91.
14. Chobanian AV, Bakris GL, Black HR, et al.Seventh Report of the Joint National Committeeon Prevention, Detection, Evaluation, and Treat-ment of High Blood Pressure. Hypertension 2003;42:1206–52.
15. American Diabetes Association. 2: Classifica-tion and diagnosis of diabetes. Diabetes Care2014;38 suppl 1:S8–16.

Baskaran et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Comparison of History-Based Risk Scores for Pre-Test Probability of CAD J U L Y 2 0 1 9 : 1 3 9 2 – 4 0 0
1400
16. Expert Panel on Detection, Evaluation andTreatment of High Blood Cholesterol in Adults.Executive summary of the third report of the Na-tional Cholesterol Education Program (NCEP)Expert Panel on Detection, Evaluation, and Treat-ment of High Blood Cholesterol in Adults (AdultTreatment Panel III). JAMA 2001;285:2486–97.
17. Williams MC, Golay SK, Hunter A, et al.Observer variability in the assessment of CT cor-onary angiography and coronary artery calciumscore: substudy of the Scottish COmputed To-mography of the HEART (SCOT-HEART) trial. OpenHeart 2015;2:e000234.
18. Hanley JA, McNeil BJ. A method of comparingthe areas under receiver operating characteristiccurves derived from the same cases. Radiology1983;148:839–43.
19. Pencina MJ, D’Agostino RB, D’ Agostino RB,et al. Evaluating the added predictive ability of anew marker: from area under the ROC curve toreclassification and beyond. Stat Med 2007;27:157–72.
20. Pencina MJ, D’Agostino RB, Steyerberg EW.Extensions of net reclassification improvementcalculations to measure usefulness of new bio-markers. Stat Med 2010;30:11–21.
21. Leening MJG, Vedder MM, Witteman JCM,et al. Net reclassification improvement: computa-tion, interpretation, and controversies. Ann InternMed 2014;160:122–31.
22. Bittencourt MS, Hulten E, Polonsky TS, et al.European Society of Cardiology-recommendedCoronary Artery Disease Consortium pretestprobability scores more accurately predictobstructive coronary disease and cardiovascularevents than the Diamond and Forrester score:clinical perspective. Circulation 2016;134:201–11.
23. Almeida J, Fonseca P, Dias T, et al. Com-parison of Coronary Artery Disease Consortium1 and 2 Scores and Duke Clinical Score topredict obstructive coronary disease by inva-sive coronary angiography. Clin Cardiol 2016;39:223–8.
24. Morise AP. Comparison of the Diamond-Forrester method and a new score to estimatethe pretest probability of coronary diseasebefore exercise testing. Am Heart J 1999;138:740–5.
25. Hadamitzky M, Achenbach S, Al-Mallah M,et al. Optimized prognostic score for coronarycomputed tomographic angiography. J Am CollCardiol 2013;62:468–76.
26. Cho I, Chang HJ, Ó Hartaigh B, et al. Incre-mental prognostic utility of coronary CT angiog-raphy for asymptomatic patients based uponextent and severity of coronary artery calcium:results from the COronary CT Angiography Eval-uatioN For Clinical Outcomes InteRnationalMulticenter (CONFIRM) Study. Eur Heart J 2014;36:501–8.
27. Yeboah J, Sillau S, Delaney JC, et al.Implications of the new American College ofCardiology/American Heart Associationcholesterol guidelines for primary atheroscle-rotic cardiovascular disease event prevention ina multi ethnic cohort: Multi-Ethnic Study ofAtherosclerosis (MESA). Am Heart J 2015;169:387–95.e383.
28. Douglas PS, Hoffmann U, Patel MR, et al.Outcomes of anatomical versus functional testingfor coronary artery disease. N Engl J Med 2015;372:1291–300.
29. Adamson PD, Fordyce CB, McAllister DA,Udelson JE, Douglas PS, Newby DE. Identifica-tion of patients with stable chest pain derivingminimal value from coronary computed to-mography angiography: an external validationof the PROMISE minimal-risk tool. Int J Cardiol2018;252:31–4.
KEY WORDS angina, calibration, coronaryartery disease, coronary computedtomography angiography, discrimination,pre-test probability, reclassification, riskscore, validation
APPENDIX For a supplemental table, pleasesee the online version of this article.

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E
A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
EDITORIAL COMMENT
Estimating Pre-Test Probabilityof Coronary Artery Disease
Battle of the Scores in an Evolving CAD Landscape*Marcelo F. Di Carli, MD, Ankur Gupta, MD, PHD
SEE PAGE 1392
T he analysis of probability as an aid to diag-nosis of obstructive coronary artery disease(CAD) in stable symptomatic patients has
been standard practice in cardiology since its intro-duction by Diamond and Forrester in 1979 (1). Byintegrating age, sex, and chest pain characteristics,the original score by Diamond and Forrester provideda likelihood of obstructive CAD, which allowed arational approach to referral for diagnostic testing.Since then, a strong evidence base has demonstratedthat noninvasive imaging testing for obstructiveCAD is most cost-effective when applied to patientswith an intermediate likelihood of CAD (2,3). Conse-quently, the analysis of pre-test probability of CADhas served as an effective gatekeeper for noninvasivetesting and has been used to define its appropriate-ness of use in guidelines.
However, over the past 2 decades, the diagnosticyield of visualizing obstructive CAD has fallen forinvasive and noninvasive coronary angiography(4–8), as well as for noninvasive stress testing (9).Multiple recent studies in the contemporary era haveconcluded that the Diamond and Forrester modelleads to a significant overestimation of the pre-testlikelihood of obstructive CAD (10–13), which
ISSN 1936-878X/$36.00
*Editorials published in the JACC: Cardiovascular Imaging reflect the
views of the authors and do not necessarily represent the views of
iJACC or the American College of Cardiology.
From the Cardiovascular Imaging Program, Departments of Medicine and
Radiology; Division of Cardiovascular Medicine, Department of Medicine,
Division of Nuclear Medicine and Molecular Imaging, Department of
Radiology, Brigham and Women’s Hospital, Harvard Medical School,
Boston, Massachusetts. Dr. Di Carli was supported in part by the
National Institutes of Health (grants 5T32HL094301 and R01HL132021);
has received a research grant from SpectrumDynamics; and has
received consulting fees from Sanofi Aventis and General Electric.
Dr. Gupta has reported that he has no relationships relevant to the
contents of this paper to disclose. Pamela Douglas, MD, served as Guest
Editor for this paper.
potentially leads to selection of too many low-riskpatients for noninvasive testing. Recent efforts havefocused on developing newer risk scores for estima-tion of pre-test likelihood of CAD in more contem-porary cohorts. The updated Diamond-Forrester(UDF) model, which uses age, sex, and symptoms, iscalibrated to a more contemporary cohort of patientsand is extended to ages beyond 30 to 69 years (12).The CAD consortium has developed a basic model(based on age, sex, and symptoms), a clinical model(CAD2: basic model þ cardiovascular risk factors thatinclude diabetes, hypertension, smoking, hyperlip-idemia, and body mass index), and an extendedmodel (clinical model þ coronary artery calciumscore) (13). The CONFIRM (Coronary CT AngiographyEvaluation For Clinical Outcomes: An InternationalMulticenter Registry) registry score (CRS) alsouses age, sex, symptoms, and cardiovascular riskfactors (14).
A battle of the scores has since ensued to estimatetheir comparative discriminatory ability for identifi-cation of patients with obstructive CAD. Tradition-ally, these scores have been validated in cohorts ofpatients referred for invasive coronary angiography(ICA) or coronary computed tomography angiography(CCTA). A limitation of using a referral populationto coronary angiography is that it overestimatesthe prevalence of CAD among stable symptomaticpatients, thereby increasing the sensitivity anddecreasing the specificity of CAD likelihood scores. Inthis issue of iJACC, Baskaran et al. (15) sought to avoidthis referral bias by testing these scores in a cohort ofpatients without previous CAD that was randomizedto CCTA in the SCOT-HEART (Scottish ComputedTomography of the Heart Trial) (15). In this multi-center clinic-based cohort of stable symptomaticpatients with uniform evaluation of CAD by
https://doi.org/10.1016/j.jcmg.2018.04.036

FIGURE 1 Studies Comparing Scores for the Estimation of Pre-Test Probability of Obstructive CAD
CRS, 0.76
NMean Age, YearsFemales, %Typical CP, %Obstructive CAD, %
11,225575042 (CP + Dyspnea)18
2,2745643 922
3,46860521323
5,67759422529 (25-60)
1,73858443738
CAD-Clinical, 0.79
CAD-Clinical+CAC, 0.88
CAD-Clinical+CAC, 0.86
CAD-Clinical, 0.79 CAD-Clinical, 0.79
UDF, 0.77
CRS, 0.75
CAD-Basic, 0.77
CAD-Basic, 0.75
UDF, 0.71
0.6CONFIRM PARTNERS PROMISE CAD Consortium SCOT-HEART
0.65
0.7
0.75
0.8
0.85
0.9C-
stat
istic
for O
bstr
uctiv
e CA
D ≥
50%
Referral Only Anatomic Imaging Uniform Anatomic Imaging
CAD-Clinical, 0.72
UDF, 0.69CAD-Basic, 0.69
The population cohort in these studies included stable symptomatic patients without known coronary artery disease (CAD) who underwent
coronary angiography on the basis of clinical referral (referral only anatomic imaging, orange circles) or as part of a randomized trial
(protocol-mandated uniform anatomic imaging, green circles). Obstructive CAD was defined as$50% diameter stenosis in at least 1 epicardial
artery. Studies included are: CONFIRM (14), PARTNERS (10), PROMISE (16), CAD Consortium (13), and SCOT-HEART (15). CAC ¼ coronary
artery calcium; CP ¼ chest pain; CRS ¼ CONFIRM registry score; UDF ¼ updated Diamond-Forrester.
Di Carli and Gupta J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 4 0 1 – 4
1402
CCTA, the clinical CAD consortium model (CAD2)provided the best discrimination for obstructive CAD(c-statistic: 0.79 for CAD2, 0.77 for UDF, and 0.75 forCRS). Compared with the UDF, the CAD2 model alsoprovided better reclassification of low-risk patientsat both 10% and 15% thresholds for pre-test likelihoodof CAD compared with the CONFIRM score. Therelative performance of all these scores was consis-tent in the overall cohort, as well as among age- andsex-based subgroups. They found that overall cali-bration was best for the UDF. However, calibrationresults were of limited validity due to use of CCTAas the reference standard, which had a low positivepredictive value for obstructive CAD on ICA, and thusled to overestimation of obstructive CAD prevalence.
There are multiple other investigations that haveexamined or compared the discriminatory value ofthese scores in various patient cohorts for estimationof pre-test likelihood of obstructive CAD (Figure 1).These studies were typically in middle-aged (meanage w60 years) men and women without known CAD
who presented as outpatients with stable symptomsand who were referred for CCTA or ICA (10,12–14).Overall, the results indicated that among history-based scores, model performance was generallysuperior for the CAD consortium clinical score. Somevariation in discriminatory value of the same scoreacross studies is likely due to different patientcohorts (i.e., referral vs. protocol-mandated coronaryangiography), the underlying prevalence of CAD,and/or use of different modalities as the referencestandard for obstructive CAD (CCTA or ICA). A recentstudy by Genders et al. (16) also evaluated the per-formance of CAD consortium scores in the PROMISE(Prospective Multicenter Imaging Study for Evalua-tion of Chest Pain) trial. Interestingly, the C-statisticof the CAD clinical score was lower in the PROMISEcohort (C-statistic: 0.72) compared with that in theSCOT-HEART trial (C-statistic: 0.79), despite uniformCCTA imaging in both studies (15,16). The differencesmight have been due to differences in the prevalenceof obstructive CAD (23% in PROMISE and 38%

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9 Di Carli and GuptaJ U L Y 2 0 1 9 : 1 4 0 1 – 4 Editorial Comment
1403
SCOT-HEART) and study design (use of ICA inPROMISE and use of CCTA in SCOT-HEART) (15,16).
There are many other potential reasonswhy pre-test likelihood estimates may not work aswell for the task of predicting obstructive CAD inmodern patients. These include changes in patientdemographics; epidemiological shifts in the preva-lence of cardiovascular risk factors in the population,including the growth of obesity, diabetes, and relatedmetabolic disorders; and changing clinical pre-sentations of CAD (17–19). Although angina and dys-pnea remain common presenting symptoms, a highproportion of cardiac patients do not show obstruc-tive lesions in their coronary angiograms (5–7). Forexample, the results of the current study by Baskaranet al. (15) showed consistent superior relative per-formance of the CAD2 score over UDF and CRS in bothmen and women. However, the best absolute perfor-mance in women (CAD2 C-statistic: 0.72) was worsethan the worst performance in men (CRS C-statistic:0.74). This was likely related to the fact that theprevalence of obstructive CAD in women is signifi-cantly lower than that in men (5). This does not meanprognosis in such patients is necessarily benign(5,6,20,21). Consequently, the traditional use ofobstructive stenosis on coronary angiography may nolonger be an adequate definition of CAD. Perhapsfunctional measures, such as coronary flow reserve,that integrate the hemodynamic effects of obstructivestenosis, diffuse atherosclerosis, and microvasculardysfunction and that are more closely related to pa-tient symptoms and risk factors or clinical outcomesmay be a better and more clinically relevant truth
standard against which these scores should becompared.
Despite the efforts and previously described newevidence, the associated overestimation of the pre-test probability of CAD by older risk scores led tothe somewhat surprising and controversial recom-mendation by the recent iteration of the NationalInstitute for Health and Care Excellence guideline inthe United Kingdom to abandon Bayesian probabilityanalysis to guide decisions regarding noninvasivetesting for patients with stable chest pain (22). Thatis, the clinician should no longer consider the pre-testprobability of the patient, whether any imaging isnecessary especially among low-risk patients, and ifso, which test is best. These recommendations are notsupported by high-quality scientific evidence and arebased on the assumption that pre-test likelihoodestimates do not improve the cost-effectiveness ofpatient care. Only time will tell if this “one-size-fitsall approach” is in the best interest of patient care.In the meantime, those of us caring for patients withCAD should try to adhere to sound clinical judgmentthat is supported by guidelines and high-quality evi-dence, which includes the use of pre-test probabilityscores to guide management of CAD as suggested bythe work of Baskaran et al. (15).
ADDRESS FOR CORRESPONDENCE: Dr. Marcelo F.Di Carli, Departments of Medicine and Radiology,Brigham and Women’s Hospital, ASB-L1 037C,75 Francis Street, Boston, Massachusetts 02115.E-mail: [email protected].
RE F E RENCE S
1. Diamond GA, Forrester JS. Analysis of proba-bility as an aid in the clinical diagnosis ofcoronary-artery disease. N Engl J Med 1979;300:1350–8.
2. Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for thediagnosis and management of patients with stableischemic heart disease: a report of the AmericanCollege of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines,and the American College of Physicians, AmericanAssociation for Thoracic Surgery, PreventiveCardiovascular Nurses Association, Society forCardiovascular Angiography and Interventions,and Society of Thoracic Surgeons. J Am CollCardiol 2012;60:e44–164.
3. Task Force M, Montalescot G, Sechtem U, et al.2013 ESC guidelines on the management of stablecoronary artery disease: the Task Force on themanagement of stable coronary artery disease ofthe European Society of Cardiology. Eur Heart J2013;34:2949–3003.
4. Douglas PS, Hoffmann U, Patel MR, et al.Outcomes of anatomical versus functional testingfor coronary artery disease. N Engl J Med 2015;372:1291–300.
5. Jespersen L, Hvelplund A, Abildstrom SZ, et al.Stable angina pectoris with no obstructive coro-nary artery disease is associated with increasedrisks of major adverse cardiovascular events. EurHeart J 2012;33:734–44.
6. Maddox TM, Stanislawski MA, Grunwald GK,et al. Nonobstructive coronary artery disease andrisk of myocardial infarction. JAMA 2014;312:1754–63.
7. Patel MR, Dai D, Hernandez AF, et al. Preva-lence and predictors of nonobstructive coronaryartery disease identified with coronary angiog-raphy in contemporary clinical practice. Am HeartJ 2014;167:846–52.e2.
8. Patel MR, Peterson ED, Dai D, et al. Lowdiagnostic yield of elective coronary angiography.N Engl J Med 2010;362:886–95.
9. Rozanski A, Gransar H, Hayes SW, et al.Temporal trends in the frequency of induciblemyocardial ischemia during cardiac stress testing:1991 to 2009. J Am Coll Cardiol 2013;61:1054–65.
10. Bittencourt MS, Hulten E, Polonsky TS, et al.European Society of Cardiology-recommendedcoronary artery disease consortium pretest prob-ability scores more accurately predict obstructivecoronary disease and cardiovascular events thanthe Diamond and Forrester Score: The PartnersRegistry. Circulation 2016;134:201–11.
11. Cheng VY, Berman DS, Rozanski A, et al.Performance of the traditional age, sex, andangina typicality-based approach for estimatingpretest probability of angiographically significantcoronary artery disease in patients undergoingcoronary computed tomographic angiography:results from the multinational coronary CT angi-ography evaluation for clinical outcomes: aninternational multicenter registry (CONFIRM).Circulation 2011;124:2423–32.

Di Carli and Gupta J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editorial Comment J U L Y 2 0 1 9 : 1 4 0 1 – 4
1404
12. Genders TS, Steyerberg EW, Alkadhi H,et al. A clinical prediction rule for the diagnosisof coronary artery disease: validation, updat-ing, and extension. Eur Heart J 2011;32:1316–30.
13. Genders TS, Steyerberg EW, Hunink MG, et al.Prediction model to estimate presence of coronaryartery disease: retrospective pooled analysis ofexisting cohorts. BMJ 2012;344:e3485.
14. Min JK, Dunning A, Gransar H, et al. Medicalhistory for prognostic risk assessment anddiagnosis of stable patients with suspectedcoronary artery disease. Am J Med 2015;128:871–8.
15. Baskaran L, Danad I, Gransar H, et al.A comparison of the updated Diamond-Forrester,CAD Consortium, and CONFIRM history-basedrisk scores for predicting obstructive coronaryartery disease in patients with stable chest pain:the SCOT-HEART Coronary CTA Cohort. J Am CollCardiol Img 2019;12:1392–400.
16. Genders TSS, Coles A, Hoffmann U, et al. Theexternal validity of prediction models for thediagnosis of obstructive coronary artery disease inpatients with stable chest pain: insights fromthe PROMISE Trial. J Am Coll Cardiol Img 2018;11:437–46.
17. Benjamin EJ, Virani SS, Callaway CW, et al.Heart disease and stroke statistics-2018 update:a report from the American Heart Association.Circulation 2018;137:e67–492.
18. Owan TE, Hodge DO, Herges RM, Jacobsen SJ,Roger VL, Redfield MM. Trends in prevalence andoutcome of heart failure with preserved ejectionfraction. N Engl J Med 2006;355:251–9.
19. Yeh RW, Sidney S, Chandra M, Sorel M,Selby JV, Go AS. Population trends in theincidence and outcomes of acute myocardialinfarction. N Engl J Med 2010;362:2155–65.
20. Gupta A, Taqueti VR, van de Hoef TP, et al.Integrated noninvasive physiological assessment
of coronary circulatory function and impact oncardiovascular mortality in patients with stablecoronary artery disease. Circulation 2017;136:2325–36.
21. Taqueti VR, Shaw LJ, Cook NR, et al. Excesscardiovascular risk in women relative to menreferred for coronary angiography is associatedwith severely impaired coronary flow reserve,not obstructive disease. Circulation 2017;135:566–77.
22. National Institute for Health and Care Excel-lence. Chest pain of recent onset: assessment anddiagnosis of recent onset chest pain or discomfortof suspected cardiac origin (update). Clinicalguideline 95. London: National Institute for Healthand Care Excellence; 2016.
KEY WORDS coronary artery disease,coronary computed tomography angiographyangina, pre-test probability, risk score

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 7 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
EDITOR’S PAGE
ISSN 1936-878X/$36.00
Focused Issue onComputedTomography
Leslee J. Shaw, PHD, Y. Chandrashekhar, MDI n this issue of iJACC, we present a series of arti-cles that explore varied uses of cardiac computedtomography (CT). This relatively new technology
has had tremendous growth in the evidence base, andhigh-quality evidence is now available to supportgreater use of CT in the setting of coronary artery dis-ease. Randomized trials are uncommon in Imagingbut iJACC has tried to showcase some of these fromtime to time (1–4). As part of this ever-expanding,high-quality evidence base, this issue reports on theprimary findings from the CONSERVE (CoronaryComputed Tomographic Angiography for SelectiveCardiac Catheterization) trial (5). Although prior ran-domized trials have focused on comparing the effec-tiveness of a CT-guided strategy with otherfunctional tests, the CONSERVE trial evaluateswhether noninvasive coronary CT angiography isnoninferior to invasive coronary angiography (ICA).Importantly, for readers of this issue, coronary CTangiography was deemed statistically noninferior toICA and reported similar 1-year rates of majorcoronary artery disease (CAD) events (at 4.6%). Thisextends findings from a previous trial that examinedthe primary endpoint of only 48-h follow-up safetybetween coronary CT angiography and ICA (6). Inthe accompanying editorial, Dr. David Newby empha-sizes the importance of safely avoiding unnecessaryICA as a primary take home message from theCONSERVE trial (7). Given the high rate of normal cor-onary angiography following diagnostic stresstesting, the CONSERVE trial supports that coronaryCT angiography is an effective alternative to ICA forpatients with suspected CAD (8).
In this issue of iJACC, there are also several prog-nostic reports that highlight the ability of coronary CT
angiography to risk stratify symptomatic andasymptomatic patient subgroups. There are severalreports that focus on the role of CT in asymptomaticpatients with diabetes. An intriguing secondaryanalysis is reported from the DCCT/EDIC (DiabetesControl and Complications Trial/Epidemiology ofDiabetes Interventions and Complications) observa-tional cohort (9). In this report of asymptomatic pa-tients with type 1 diabetes, long-term follow-up of 10to 13 years was reported according to coronary arterycalcium (CAC) scores. In this high-risk, diabetic sub-group, those patients without CAC (score of 0) had a10-year cumulative incidence of major cardiovascularevents of w5% (or w0.5%/year). This is extraordi-narily low and supports prior evidence that a lack ofdetectable plaque identifies a very low risk cohortwith minimal risk over more than a decade of follow-up. The evidence base with CAC continues to unfoldand strongly supports effective, long-term risk strat-ification across numerous and varied patient sub-groups on the basis of CAC findings.
CTA also has major short- to intermediate-termprognostic value and a paper shows that this extendsto predicting event-free survival over a 10-yearfollow-up and reclassify risk in a large proportion ofpatients from multiple clinical risk groups (10). Thereis also a series of article exploring measures ofischemia using CT technology. A meta-analysis syn-thesized 54 articles reporting on the diagnostic per-formance of fractional flow reserve (FFR-CT), CTperfusion, and transluminal attenuation gradient inestimating functionally significant CAD defined byinvasive FFR (11). This meta-analysis revealed asimilarly high diagnostic accuracy for FFR-CT and CTperfusion, with diagnostic specificity measures of
https://doi.org/10.1016/j.jcmg.2019.06.001

Shaw and Chandrashekhar J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 7 , 2 0 1 9
Editor’s Page J U L Y 2 0 1 9 : 1 4 0 5 – 6
1406
76% and 81% and sensitivity of 81% and 89%,respectively. iJACC has also been on the forefront ofexploring the effect of plaque over and above its roleas a marker of vulnerability alone (12–14). Althoughthese findings are intriguing, another report, from theCORE320 (Coronary Artery Evaluation Using 320-RowMultidetector Computed Tomography Angiographyand Myocardial Perfusion) investigators, examinedCT measurements of atherosclerotic plaque as pre-dictors of regional myocardial perfusion ischemia(15). In this report, only maximum stenosis predictedCT perfusion ischemia, whereas percentage ofatheroma volume and a qualitative variable ofvulnerable plaque were independently predictive ofsingle-photon emission CT myocardial ischemia; thepredictive value over stenosis was modest. Thus, therelationship between CT anatomic features andmeasures of ischemia remains an unfolding area ofresearch. Importantly, most of the prior evidenceexamines the role of CT anatomic features as relatedto vessel-specific ischemia. In this report, theCORE320 investigators extend these prior findings toidentify correlative findings associated with myocar-dial ischemia. Of course, for many, the underlyingplaque features and stenosis severity, as well asrelated specific vessel measurements, such as lumenvolume, may ultimately prove to be optimal markersof vessel and myocardial ischemia. It remains likely
that the underlying plaque and stenosis markers mayprovoke ischemia in the setting of both obstructiveand nonobstructive CAD and shed light onto thehighly variable relationship noted in nuclear perfu-sion imaging between inducible myocardial ischemiaabsence significant CAD (i.e., ischemia and non-obstructive coronary arteries [INOCA]). Finally, pre-dicting pre-test probability with risk scores is still ofmuch interest and some recent data have showndiscordant results (16,17). A study in this issue (18)extends this debate further with additional dataabout how some of these perform when applied to awell-validated dataset.
We believe that this range of reports can furtherprovide readers of our journal with an ever-increasing understanding of the possibilities ofCT-based research to detect unique atheroscleroticplaque and physiological measures as importantguides to improving diagnostic certainty, enhancingrisk stratification, and guiding preventive care forpatients.
ADDRESS FOR CORRESPONDENCE: Dr. Y. Chandra-shekhar, Division of Cardiology, Mail Code: 111c,University of Minnesota/VAMC, 1 Veterans Drive,Minneapolis, Minnesota 55417. E-mail: [email protected].
RE F E RENCE S
1. Sand NPR, Veien KT, Nielsen SS, et al. Pro-spective comparison of FFR derived from coronaryCT angiography with SPECT perfusion imaging instable coronary artery disease. J Am Coll CardiolImg 2018;11:1640–50.
2. Levsky JM, Haramati LB, Spevack DM, et al.Coronary computed tomography angiographyversus stress echocardiography in acute chestpain. J Am Coll Cardiol Img 2018;11:1288297.
3. Sørgaard MH, Linde JJ, Kühl JT, et al. Value ofmyocardial perfusion assessment with coronarycomputed tomography angiography in patientswith recent acute-onset chest pain. J Am CollCardiol Img 2018;11:1611–21.
4. Lubbers M, Coenen A, Kofflard M, et al.Comprehensive cardiac CT with myocardial perfu-sion imaging versus functional testing in sus-pected coronary artery disease. J Am Coll CardiolImg 2018;11:1625–36.
5. Chang H-J, Lin F, Gebow D, et al. Selectivereferral using coronary computed tomographicangiography versus direct referral for individualsreferred to invasive coronary angiography forsuspected coronary artery disease: a randomizedcontrolled open-label trial. J Am Coll Cardiol Img2019;12:1303–12.
6. Dewey M, Rief M, Martus P, et al. Evaluation ofcomputed tomography in patients with atypical
angina or chest pain clinically referred for invasivecoronary angiography: randomised controlledtrial. BMJ 2016;355:i5441.
7. Newby DE. CONSERVE your energy and re-sources. J Am Coll Cardiol Img 2019;12:1313–5.
8. Patel MR, Peterson ED, Dai D, et al. Low diag-nostic yield of elective coronary angiography. NEngl J Med 2010;362:886–95.
9. Budoff M, Backlund J-YC, Bluemke DA, et al.The association of coronary artery calcification(CAC) with subsequent incidence of cardiovasculardisease (CVD) in DCCT/EDIC. J Am Coll Cardiol Img2019;12:1341–9.
10. Finck T, Hardenberg J, Will A, et al. Ten-yearfollow-up after coronary computed tomographyangiography in patients with suspected coronaryartery disease. J Am Coll Cardiol Img 2019;12:1330–8.
11. Celeng C, Leiner T, Maurovich-Horvat P, et al.Anatomical and functional CT for diagnosing he-modynamically significant coronary artery disease:a meta-analysis. J Am Coll Cardiol Img 2019;12:1316–25.
12. Christiansen MK, Jensen JM, Nørgaard BL,et al. Coronary plaque burden and adverse plaquecharacteristics are increased in healthy relatives ofpatients with early onset coronary artery disease. JAm Coll Cardiol Img 2017;10:1128–35.
13. McDermott MM, Kramer CM, Tian L, et al.Plaque composition in the proximal superficialfemoral artery and peripheral artery diseaseevents. J Am Coll Cardiol Img 2017;10:1003–12.
14. Ahmadi A, Leipsic J, Ovrehus A, et al. Lesion-specific and vessel-related determinants offractional flow reserve beyond coronary arterystenosis. J Am Coll Cardiol Img 2018;11:521–30.
15. Bakhshi H, Meyghani Z, Kishi S, et al.Comparative effectiveness of CT derived athero-sclerotic plaque metrics for predicting myocardialischemia. J Am Coll Cardiol Img 2019;12:1367–76.
16. Adamson PD, Newby DE, Hill CL, et al. Com-parison of international guidelines for assessmentof suspected stable angina. J Am Coll Cardiol Img2018;11:1301–10.
17. Genders TS, Coles A, Hoffmann U, et al. Theexternal validity of prediction models for thediagnosis of obstructive coronary artery disease inpatients with stable chest pain. J Am Coll CardiolImg 2018;11:437–46.
18. Baskaran L, Danad I, Gransar H, et al. A com-parison of the updated Diamond-Forrester, CADConsortium and CONFIRM history-based riskscores for predicting obstructive coronary arterydisease in patients with stable chest pain: theSCOT-HEART CCTA cohort. J Am Coll Cardiol Img2019;12:1392–400.









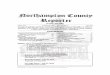

![PROCEEDINGS OF SPIE€¦ · of wave propagation are presented nicely by Achenbach (1973), Auld ( 1973), and Datta (2008) [3~5]. In Achenbach 2003, some interesting re ciprocity concepts](https://img.pdfslide.us/doc/110x75/5eac76d4a43df830eb44c79d/proceedings-of-spie-of-wave-propagation-are-presented-nicely-by-achenbach-1973.jpg)