Embed Size (px)
Citation preview

AAGL acknowledges that it has received support in part by educational grants and equipment (in-kind) from the following companies:
3-Dmed, Applied Medical, Boston Scientific, CooperSurgical, Ethicon US, LLC, Marina Medical, Medtronic, Olympus America, Inc.,
Karl Storz Endoscopy-America, Inc., Symmetry Surgical
Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
FULL DAY: How Do You Measure Up? ASSESS Your Skills
PROGRAM CHAIR
Ernest G. Lockrow, DO
Angela Chaudhari, MD Joseph M. Gobern, MD, MBA Malcolm W. Mackenzie, MD
Brent E. Seibel, MD
Grace Chen, MDCandice Jones-Cox, MDDouglas Miyazaki, MD
Sangeeta Senapati, MDSabrina Whitehurst, MD
Susan G. Dunlow, MDLeslie D. Kammire, MD
Jamal Mourad, DOM. Jonathon Solnik, MD

Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 7.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 Laparoscopic Hysterectomy S. Senapati .................................................................................................................................................... 3 Complications of Laparoscopy E.G. Lockrow ............................................................................................................................................... 12 Vaginal Hysterectomy M.J. Solnik .................................................................................................................................................. 21 Retropubic Slings D. Miyazaki ................................................................................................................................................. 28 Cultural and Linguistics Competency ......................................................................................................... 35

SKIL-700
FULL DAY: How Do You Measure Up? ASSESS Your Skills
Presented in affiliation with the American College of Obstetricians and Gynecologists (ACOG)
Ernest G. Lockrow, Chair
Faculty: Angela Chaudhari, Grace Chen, Susan G. Dunlow, Joseph M. Gobern, Candice Jones-Cox, Leslie D. Kammire, Malcolm W. Mackenzie, Douglas Miyazaki,
Jamal Mourad, Brent E. Seibel, Sangeeta Senapati, M. Jonathon Solnik, Sabrina Whitehurst This course was developed in collaboration with the ACOG Simulations Consortium and is specifically designed to assess gynecologic surgeons in all levels of training on various gynecologic surgeries. The modules used from the Advanced Surgical Simulation and Endoscopic Surgical Simulation (ASSESS) Course include: Vaginal Hysterectomy, Laparoscopic Hysterectomy and Retropubic Slings. Whether you are a current expert in the field of gynecologic surgery or have not been able to perform minimally invasive surgical procedures such as vaginal hysterectomy, laparoscopic surgery or retropubic slings, this course will afford you the opportunity to assess your current level of expertise in gynecologic surgery. This is a hands-on course utilizing moderate fidelity simulation models from industry that you will be able to perform an actual vaginal hysterectomy, laparoscopic hysterectomy and retropubic sling. The course is an ABOG Maintenance of Certification (MOC) approved simulation course that will afford the participants credit during their MOC cycle. Learning Objectives: At the conclusion of this course, the clinicians will be able to: 1) Assess their skills in performing laparoscopic hysterectomy; 2) assess their skills in performing vaginal hysterectomy; and 3) assess their skills in performing retropublic slings.
Course Outline 7:00 Welcome, Introductions and Course Overview E.G. Lockrow 7:15 Laparoscopic Hysterectomy S. Senapati 7:45 Complications of Laparoscopy E.G. Lockrow 8:30 Questions & Answers All Faculty 8:45 Break 9:00 LAB I: Using the Limbs and Things Model:
Group A Performs Laparoscopic Hysterectomy, Group B Performs Laparoscopic Suturing Skills
10:50 Questions & Answers 11:00 Adjourn/Lunch 12:30 Vaginal Hysterectomy M.J. Solnik 1:15 Retropubic Slings D. Miyazaki 2:00 Questions & Answers All Faculty 2:15 Break 2:30 LAB II: Using the MIYA Model: Group A Performs Vaginal Hysterectomy, Group B Performs Retropubic Slings 4:15 Wrap-Up 4:30 Adjourn
1

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Amber Bradshaw Speakers Bureau: Myriad Genetics Lab Other: Proctor: Intuitive Surgical Erica Dun* Frank D. Loffer, Medical Director, AAGL* Linda Michels, Executive Director, AAGL* Johnny Yi*
SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: Intuitive Royalty: CooperSurgical Sarah L. Cohen* Jon I. Einarsson* Stuart Hart Consultant: Covidien Speakers Bureau: Boston Scientific, Covidien Kimberly A. Kho Contracted/Research: Applied Medical Other: Pivotal Protocol Advisor: Actamax Matthew T. Siedhoff Other: Payment for Training Sales Representatives: Teleflex M. Jonathon Solnik Consultant: Z Microsystems Other: Faculty for PACE Surgical Courses: Covidien FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Angela Chaudhari* Grace Chen* Susan G. Dunlow* Joseph M. Gobern* Candice Jones-Cox* Leslie D. Kammire* Ernest G. Lockrow* Malcolm W. Mackenzie Consultant: Olympus Douglas Miyazaki* Jamal Mourad* Brent E. Seibel* Sangeeta Senapati Consultant: Emmi M. Jonathon Solnik Consultant: Z Microsystems Other: Faculty for PACE Surgical Courses: Covidien Sabrina Whitehurst*
Asterisk (*) denotes no financial relationships to disclose. 2

Laparoscopic Hysterectomy: A Review of the Basics
Sangeeta Senapati, MD
Northshore University HealthSystem
• Consultant: Emmi
• Explain the rationale for a laparoscopic approach to hysterectomy
• Discuss options for instrumentation and key technical components
• Describe a technique for conventional laparoscopic hysterectomy
• Review variations of laparoscopic hysterectomies
Evolution of Hysterectomy• Approximately 600,000 hysterectomies performed each year in U.S.
• $5 Billion
• By age 60, 1 in 3 women in U.S. will have had a hysterectomy
• 90% performed for elective benign indications
– Fibroids
– Abnormal uterine bleeding
– Endometriosis
– Chronic pelvic pain
Carlson et al N Engl J Med 1993
Epidemiology
• Age range ‐median 44‐45 yrs1
• Ethnicity ‐ 69% Caucasian, 17% African‐American, 10.5% Hispanic2
• LOS ‐median 2‐3 days1
• Complication rates ‐ 1‐3%2
• Transfusion rates ‐ 1‐3%3
1Farquhar CM & Steiner CA Ob Gyn2002; 2Campbell ES et al JRM2003; 4Meikle SF et al Ob Gyn 19973
3

Evolution of Hysterectomy
• Total abdominal & vaginal hysterectomy (TAH, TVH)
• Laparoscopic‐assisted vaginal hysterectomy, introduced by Reich in late 1980s (LAVH)
• Laparoscopic supracervical hysterectomy (LSH)
• Total laparoscopic hysterectomy (TLH)
66% of all hysterectomies performed in the U.S. are abdominal
Wu et al, Ob Gyn 2007
Laparoscopic Hysterectomy Classification
Laparoscopic Hysterectomy Classification
Criteria
• A non‐vaginal hysterectomy candidate who by traditional methods would have undergone hysterectomy abdominally
There are no absolute contraindications, just relative: surgeon experience, anatomical operating field, anesthesia, abdominal entry issues…
Potential Indications
• Difficult vaginal access
• Decreased mobility of the uterus
• Large uterus
• Suspicious adhesions from prior surgeries
• Severe endometriosis
• Presence of an adnexal mass
Benefits of Laparoscopy vs. Laparotomy (Cochrane Review of Hysterectomy)
• Faster return to normal activities
• MD -15.17, 95% CI -17.21 to -13.14
• Fewer febrile episodes
• OR 0.25, 95% CI 0.09 to 0.73
• Fewer wound or abdominal wall infections
• OR 0.29, 95% CI 0.12 to 0.71
4

Benefits in the Obese Patient
• Shorter hospital stay (2.5 vs. 5.6 days)
• Less post operative pain
• Earlier return to normal activity1
• Less post operative ileus (0 vs. 13%)
• Fewer postoperative fevers (5.5 vs. 31.1%)
• Fewer wound infections (9 vs. 22%)2
1Eltabbakh et al. Gynecol Oncol 2000,2Enochsson et al. Surg Endosc 2001
InstrumentsUterine Manipulator
• VCARE
• RUMI + Koh colpotomy rings
• Vaginal balloon pneumo‐occluder
TLH configuration
(Koh colpotomy ring, ZUMI uterine manipulator, vaginal balloon pneumo‐occluder)
Electrosurgical Vessel Sealing Technology
LigaSure
Halo PK
EnSeal
Harmonic Ace
Key Concepts
Advanced bipolar vessel sealing and cutting devices do not work like cold scissors
“TENSION‐FREE SEALING & TRANSECTION”
Surgical technique otherwise modeled after abdominal hysterectomy
Technical Steps
• Survey of operative field: Create a game plan
• Adnexal management
• Round ligament & entry into broad ligament
• Vesico‐uterine reflection
• Skeletonization & ligation of uterine vasculature
Technical Steps
• Management of vaginal cuff
– Colpotomy
– Closure
• Specimen extraction
• Post‐operative care/precautions
5

Patient Positioning
• Dorsal lithotomy
• Arms padded and tucked at sides
• Steep Trendelenburg
• Decompress stomach & bladder
Positioning• Obese patients are at a greater risk of pressure sores and neural injuries!– Ultrafins: Yellowfins for the obese
– Shoulder braces or other antiskid measures
– Vacuum beanbag
– Toboggans or arm supports
– Neck support
Laparoscopic Access
• Direct vs. open (Hasson technique) vs. Veress needle (standard, long)
• Transforniceal
• Left upper quadrant (Palmer’s Point)
Issues with Obesity• Decreased surgical landmarks for placement of the
Veress needle
• Grasp umbilicus with towel hooks
• Assure that you enter the belly perpendicular to the skin
• Use a long Veress 150mm
• Consider a left upper quadrant entry at Palmer’s point
• Consider vaginal placement of
veress in women with no risk
for pelvic adhesive disease
Left Upper Quadrant Entry
• Key Points
– Empty the stomach (OG/NG)
– Placement in the mid clavicular line (or just lateral to this)
– Using a veress needle: 3 “pops” for entry into the peritoneal cavity
– Opening pressure <10mm Hg
– Can insufflate up to 20mm Hg for port placement
Consider in pregnant patients, those with large abdominal masses, large uteri, or those with prior midline surgery
Trocar Placement
A= 5‐10 mm umbilical or supraumbilical for laparoscope
B = 5‐15 mm right & left lower quadrant as well as suprapubic
6

Ports and Port Placement• Long ports (15cm) must be available to use.
• Increase pneumoperitoneum to 20mm Hg to aid with safe placement of the trocars.
• Adjust for the pannus when trying to place your trocars based on the usual anatomic landmarks.
• Think about placing the ports more laterally as this will often give you more exposure and decrease the torque on the ports.
Angled Scope
Retraction Techniques Adnexa
Round Ligament Vesicouterine Peritoneum
7

Uterine Vasculature Blanched Uterus
Morcellation Alternatives to Power Morcellation Techniques
• Vaginal morcellation
• Minilaparotomy morcellation
• Enclosed power morcellation in bag
• Extraction through posterior colpotomy
Vaginal Morcellation
• Bivalving
• Coring
• Wedging
• MyomectomyProtection of the edges of the incision
Self-retaining retractorSpecimen bag
Minilaparotomy
8

Cervical Stump Adhesion Barrier
Colpotomy Cuff Closure
Cystoscopy• Overall urinary tract injury rate 0.73%1
– Risk is greater than with abdominal hysterectomy2
– May have delayed injury from thermal damage
• Procedure: 70 degree or 30 degree scope
– Water, saline, or 10% dextrose as the distention media
– Can use IV indigo carmine, IV methylene blue or preoperative oral phenazo‐pyridine for visualization of ureteral jets of urine
Adelman et al JMIG 20141
Aarts et al Cochrane Database Syst Rev. 20152
Post Op Care
• Hospital discharge either same day or next day
– Expectations (talk about this ahead of time)
• Lifting restrictions (< 10 lbs)
• Pain management: NSAIDS, narcotics
• 2 week recovery time
• Pelvic rest! 6‐8 weeks
9

Vaginal Cuff Dehiscence
• Presentation
– Bleeding, serous discharge, pain
– Cuff separation or bowel evisceration
• Dehiscence Rate (<1‐5%) ‐ > 1.35%
Iaco et al Eur J Obstet Gynecol Reprod Biol. 2006Hur et al Obstet Gynecol 2007, Kim et al Obstet Gynecol Sci 2014
Iaco (%) Hur (%) Kim (%)
TAH 0.25 0.38 1.56*
TVH 0.26 0.11
TLH 0.79 0.75 5.42
* Radical hyst
Challenges of Conventional Laparoscopy
• Limited degree of motion within the body
• Hand movement is counter‐intuitive (fulcrum effect)
• View of operative field is on a 2‐D monitor
• Unsteady image
• Significant learning curve exists for advanced cases
Robotic‐Assisted Laparoscopy: Highlights• Surgeon controls the robotic arms remotely
• 3‐D image through stereoscopic viewer (high definition option)
• No haptic (tactile) feedback
• Seven degrees of movement mimic human wrist movement (eliminate fulcrum effect)
• Tremor filtration & motion scaling
• Enabling technology (shortening learning curves)
Sarle et al. J Endouro 2004
Single Port Surgery
• SPA (single port access) vs. standard multiport technique
– Comparable operative times, blood loss, and length of stay
– No difference in pain or cosmetic outcomes
Kim et al JMIG 2015
Summary
• Laparoscopic hysterectomy is preferred over abdominal hysterectomy where vaginal hysterectomy not appropriate
• Basic technical steps will be the same despite multiple variations on technique
• Know your options regarding instrumentation and suture material
• Pre‐operative counseling is important! Manage expectations
Limbs and Things
10

• Aarts JW, Nieboer TE, Johnson N, Tavender E, Garry R, Mol BW, Kluivers KB. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2015 Aug 12;8:CD003677
• Adelman MR, Bardsley TR, Sharp HT. Urinary tract injuries in laparoscopic hysterectomy: a systematic review. J Minim Invasive Gynecol. 2014 Jul‐Aug;21(4):558‐66
• Campbell ES, Xiao H, Smith MK. Types of hysterectomy. Comparison of characteristics, hospital costs, utilization and outcomes. J Reprod Med. 2003 Dec;48(12):943‐9.
• Carlson KJ, Hichols DH, Schiff I Indications for hysterectomy. N Eng J Med 1993;328:856‐60.
• Eltabbakh GH, Shamonki MI, Moody JM, Garafano LL. Hysterectomy for obese women with endometrial cancer: laparoscopy or laparotomy? Gynecol Oncol. 2000 Sep;78(3 Pt 1):329‐35.
• Enochsson L, Hellberg A, Rudberg C, et al. Laparoscopic vs open appendectomy in overweight patients. Surg Endosc. 2001 Apr;15(4):387‐92
• Farquhar CM, Steiner CA Hysterectomy rates in the United States 1990‐1997. Obstet Gynecol. 2002 Feb;99(2):229‐34.
• Hur HC, Donnellan N, Mansuria S, Barber RE, Guido R, Lee T. Vaginal cuff dehiscence after different modes of hysterectomy. Obstet Gynecol. 2011 Oct;118(4):794‐801.
• Iaco PD, Ceccaroni M, Alboni C, et al. Transvaginal evisceration after hysterectomy: is vaginal cuff closure associated with a reduced risk? Eur J Obstet Gynecol Reprod Biol. 2006;125:134–138
• Kim M, Kim S, Bae H et al. Evaluation of risk factors of vaginal cuff dehiscence after hysterectomy. Vacc Obstet Gynecol Sci2014;57(2):136‐143
• Kim TJ, Shin SJ, Kim TH et al. Multi‐institution, Prospective, Randomized Trial to Compare the Success Rates of Single‐port Versus Multiport Laparoscopic Hysterectomy for the Treatment of Uterine Myoma or Adenomyosis. J Minim Invasive Gynecol. 2015 Jul‐Aug;22(5):785‐91.
• Meikle SF, Nugent EW, Orleans M. Complications and recovery from laparoscopy‐assisted vaginal hysterectomy compared with abdominal and vaginal hysterectomy. Obstet Gynecol. 1997 Feb;89(2):304‐11.
• Olive DL, Parker WH, Cooper JM, Levine RL. The AAGL classification system for laparoscopic hysterectomy. Classification committee of the American Association of Gynecologic Laparoscopists. J Am Assoc Gynecol Laparosc. 2000 Feb;7(1):9‐15
• Sarle R, Tewari A, Shrivastava A, et al. Surgical robotics and laparoscopic training drills. J Endouro 2004; 18:63‐67
• Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007 Nov;110(5):1091‐5.
11

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Laparoscopic Surgery and It’s Complications
Ernest G. Lockrow DOFACOG, FACOOG
Professor and Vice Chair
Department of OBGYN
Uniformed Services University
Director MIGS Fellowship
Walter Reed National Military Medical CenterUNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Disclosures
I have no financial relationships to disclose
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Objectives
Evaluate the risks of laparoscopic surgery Employ risk reducing surgical techniques Evaluate & treat complications of
laparoscopic procedures– Neurologic– Vascular– Bowel– Urological (bladder, ureter)
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Background
Complications range 0.1% to 10%
Approximately 50% entry technique
20% to 25% unrecognized intraoperatively
Meta analysis– 1809 laparoscopy /1802 laparotomy – benign GYN– No difference major or minor
complications
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Contraindications to Laparoscopy
Absolute contraindications include Bowel obstruction Ileus Peritonitis Intraperitoneal hemorrhage Diaphragmatic hernia Severe cardiorespiratory disease
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Risk Factors
Operative 0.1% to 18% vs Diagnostic 0.1% to 7%
Extremes of body weight
Anesthesia risk factors (Class III +)
Distortion of pelvic anatomy
Previous abdominopelvic surgery
Pelvic pathology
12

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Laparoscopic Surgery Risk
Surgeon experience– 3-5 fold increase in complications
Unskilled surgical Assistance– 5-8x more likely to incur a complication
Faulty Instrumentation– Dull trocars– Faulty scope, light cords, electrosurgical
equipmentUNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Anesthesia Risk
Cardiopulmonary function/Position– Monitoring required– Consider central venous monitoring
Fluid Balance– Irrigation/blood loss
Pnuemoperitoneum– GFR, SVR, vagal irritation– Diaphragmatic movement (PIP, MAP increase; FRC
reduced)– Hypercapnea
Subcutaneous Emphysema/ CO2 embolism
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Positioning Risk
Steep Trendelenburg– Increases cardiac pre-load– Increase intrathoracic pressure– Obese patients/impaired cardiopulmonary
function – Aspiration Risk NG/OG
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Technique Prior to the procedure an appropriate
work-up is essential
Indications for the procedure and its appropriateness must be reviewed
Informed consent should be obtained
The consent for operative laparoscopy should always contain permission for possible laparotomy
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Abdominal Entry Blind entry into the abdomen to induce
pneumoperitoneum demands strict attention to detail
The following three principles should be kept in mind: – Elevate the abdominal wall away from the aorta
(if punctured it does not forgive)– Aim at the uterus (if punctured it forgives)– Aim at right angles to the skin close to the umbilicus
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
13

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Abdominal Entry
Correct entry can be judged by the free flow of saline (if using a Veress needle), or an intra-abdominal pressure of 5-12mm Hg for initial flow
There is general agreement that an initial volume of 2L or an intra-abdominal pressure of 15 mm Hg is a satisfactory endpoint prior to trocar entry
In obese patients, it is advisable to distend the abdomen maximally to 20-25mm Hg
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar Entry Large Vessel Injury
3-8 per 10,000 cases
A major complication requiring immediate laparotomy and a call for the vascular surgeon
Only the most skilled laparoscopist, or those comfortable with open laparoscopy, should attempt laparoscopy in a facility where immediate laparotomy is not feasible
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Vascular InjuriesDiagnosis
• Return of blood from Veress needle
• Deterioration of vital signs
• Unexplained volume of blood in peritoneal cavity
• Reappearance of blood after aspiration
Lynn CS J Reprod Med 27:217,1982
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
14

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Vascular Injuries
30-50% of the surgical trauma which occurs during laparoscopy is due to vascular injuries
Veress Needle accounts for 36% of the injuries
Primary and Secondary trocars account for 32%
Yuzpe AA J Reprod Med 35:485,1990
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar Entry
Direct entry techniques should not be used in patients with: previous abdominal surgery morbid obesity
Beware of the thin, athletic, nullipara
Some surgeons advocate only the open laparoscopy or Hasson technique
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar EntryOther trocar site insertions
Know where the superior and inferior epigastric vessels run
Transilluminate the abdominal wall and identify avascular spaces
Insert additional trocars under direct visualization
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar Entry If an epigastric vessel is encountered sometimes
bleeding can be controlled with a thru and thru abdominal figure of eight stitch using an XLH needle
Kleppinger forceps can sometimes cauterize the vessel
Pelvic vessel injuries can be repaired with ligaclips if bleeding is minimal
If the patient is unstable, laparotomy is necessary
15

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar Entry
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar Entry
Port Placement
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Left Upper Quadrant Primary Trocar Insertion
NG tube, flat (no t-bird), 2 fingerbreadths below rib
Mid-clavicular line, cheat lat to avoid sup epigastric
11 blade, towel clips above and below
Resident holds inferior towel clip with left hand, shaft of Verres or optical trocar with right
Staff holds superior towel clip with left hand, manipulates CO2 tubing with right
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar EntryBowel injury
Incidence: 0.03 - 0.39%
Recent systematic review found an overall incidence of bowel injury at 1 in 769
Insertion of the insufflation needle and the initial trocar are the most common cause
Delayed diagnosis mortality rate of 1 in 31 or 3.2%
Bowel Injury in Gynecologic Laparoscopy: A Systematic Review Obstetrics & Gynecology June 2015
16

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar EntryBowel injury
Diagnosis • Stool on needle or trocar tip
• Fecal material in abdominal cavity
• Hematoma on bowel serosa
• Foul smell noted on introducing trocar
• Laparoscope introduced into intestinal lumen
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar EntryBowel injury
Prevention• Use of NG or OG tube
• Lifting the abdominal wall
• Adequate pneumoperitoneum
• Care with use of monopolar electrosurgery
• Make certain bowel is out of field of energy
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of Trocar EntryBowel injury
If immediately recognized, lacerations of the bowel by trocar and needle can be managed by direct suturing
If peritonitis has become established, resection is necessary
Perforations w/Veress needle: Observation and antibiotics
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Electrocoagulation As electrons enter the body they must return to
ground
In unipolar configurations, electrons go through the body to a ground plate
If the ground plate is faulty, electrons seek ground through EKG leads to other smaller points of the patient’s contact with metal on the table causing skin burns
17

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Electrocoagulation In response to unipolar bowel burns,
bipolar forceps were designed; ~ one prong of the forceps is insulated
from the other except at the tip ~ electrons flow between the tips of the
prongs
~ no ground plate is required ~ electrons stay in the fallopian tube ~ the patient is not part of the circuit
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Electrocoagulation
Bowel burn is rare (0.5 per 1000 cases) but a serious complication requiring laparotomy
Bowel perforation should be suspected in all cases of continuing abdominal pain within 24 to 48 hours after laparoscopy
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Capacitive Coupling
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Capacitive Coupling
Omental burn during cholecystectomy
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Electrocoagulation A bipolar bowel burn probably involves no more
than 1 cm of tissue around the edges of the perforation so a simple resection can be performed
With unipolar coagulation, a bowel perforation 1 cm in diameter would involve approximately 6 cm of compromised adjacent bowel– 10 - 12 cm resection and anastomosis would be
required
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Urologic complicationsBladder Injury
Most common reason for injury is lack of catheterization
Diagnosis: recognition of separation of bladder mucosa or urine spillage around trocar sleeve, appearance of gas in the foleybag or hematuria.
18

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Urologic complicationsBladder Injury
Prevention
Visualization of the dome of the bladder when inserting the trocar
Recognize high risk patients
(multiple c-sections etc)
Modify insertion site if needed
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Urologic complicationsBladder Injury
Management• Depending on your laparoscopy skills the injury
can be repaired by direct suturing techniques
• Need to drain the bladder for 7-10 days
• For small injuries (< 5mm) drainage may be sufficient
• Laparotomy may be needed to repair larger injuries
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Urologic complicationsUreteral Injury
Patients usually present 48-72 hours postop with abdominal pain, peritonitis, leukocytosis, and fever
Flank tenderness and hematuria are Rare
Diagnosis is confirmed by IVP or CT w/contrast
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Urologic complicationsUreteral Injury Prevention
Visualization of the ureter in the region of the uterosacrals is difficult, especially in the presence of endometriosis or adhesions
Laparoscopic uterine nerve ablation is associated with an increased risk of injury
Familiarization with the anatomy is key
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Urologic complicationsUreteral Injury Prevention
Use of hydro-dissection
Use of Indigo carmine
Cautious use of electrocautery
Bipolor is preferred over monopolar
Prolonged coagulation can cause damage to vascular supply and subsequent necrosis
19

UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Urologic complicationsUreteral Injury
Management
• Repair should be done in conjunction with the urologic surgeon
• It may be possible to place a stent
• Laparotomy or robotic assistance may be required for : end to end reanastomosis, reimplantation, transureteral ureterostomy
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
Complications of LaparoscopyConclusion
Recognition at the time of injury and immediate repair will prevent morbidity
Delayed diagnosis is the major cause of increased morbidity
Delayed recognition of injury makes laparotomy more likely
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
References
Lynn SC et al, Aortic perforation sustained at laparoscopy, J Reprod Med 1982 Apr;27(4):217-9
Yuzpe AA. Pneumoperitoneum needle and trocar injuries in laparoscopy: a survey on possible contributing factors and prevention. J Reprod Med 1990;35:485–90.
Liarena, NC et al, Bowel Injury in Gynecologic Laparoscopy: A Systematic Review, Obstetrics & Gynecology June 2015 Vol 125 (6), 1407-1417
Xuezhi Jiang et al, The Safety of Direct Trocar Versus Veress Needle for Laparoscopic Entry: A Meta-Analysis of Randomized Clinical Trials, Journal of laparoendoscopic & advanced surgical techniques, 2012 vol22(4) 362-370
Ahmad G, Duffy JM, Phillips K, Watson A. Laparoscopic entry techniques. Cochrane Database Syst Rev 2008;16(2):
UNIFORMED SERVICES UNIVERSITYof the Health SciencesDepartment of Obstetrics and Gynecology
“Life is too short to make all of the mistakes yourself... so learn from the mistakes of others”
author unknown
20

Back to the Basics:Hysteréctomie Vaginale
M. Jonathon Solnik, MD FACOG FACS
Head of Gynaecology & MIS
Mt. Sinai Hospital
Associate Professor
Dept Obstetrics & Gynaecology
Faculty of Medicine ‐ University of Toronto
Disclosures
• Consultant: Z Microsystems
• Other: Faculty for PACE Surgical Courses: Covidien
Objectives
• Demonstrate optimal position for purpose of exposure during vaginal hysterectomy
• Describe technical challenges and means to overcome these barriers
• Review methods for tissue extraction of larger specimen
Why Vaginal Approach ?
• 400,000 inpatient hysterectomies in the US
• 50% performed laparoscopically or vaginally
• Vaginal approach stable ~23%
• Utilization may rise with morcellation debate
• Equates to 200,000 women potentially affected
• Any MIS approach avoids morbidity & mortality of abdominal surgery
Why Vaginal Approach ?
• VH associated with similar outcomes to LH (compared to AH) at a lower cost/time and with fewer urinary tract injuries
• ‘RH and single port hysterectomy should be abandoned or further evaluated…’
When to…, and when NOT too…
Indications
• Benign pathology
• POP
• Pre‐malignant disorders
Contraindications
• Hx pelvic surgery ?
• Only cesarean ?
• Uterus > 12 weeks ?
• Needs BSO ?
• Pelvic arch < 90 degrees ?
• Chronic pelvic pain
• Access to vessels
• Pelvic mass
• Reproductive cancer
21

Keys to Successful Surgery
• Must be able to see what you are doing !
• Positioning
• Lighting
• Retractors (do not over utilize)
• Must know the anatomy (thru a keyhole)
• Peritoneal access
• Must identify & manage complications
• Must know how to extract large tissue volume
Why can this be a challenge ?
• Poor exposure…
• Peritoneal access (anterior/posterior entry)
• Maintain hemostasis
• Avoiding injury to visceral/vascular structures
• Managing the large uterus
• Removing adnexa
#1 ‐ EXPOSUREFeet wrapped or padded
Buttocks slightly off end of bed
Not hyper‐flexed or extended at knee and knee not resting on stirrup
Not hyper‐flexed at hip
#2 ‐ Instruments
#2 ‐ Instruments #2 ‐ Instruments
22

#2: Other instruments
• Briesky‐Navratil retractor
• Right angle retractor
• Lahey clamps
• Double tooth tenaculum
• Towel clips
• Heaney‐Ballentine clamps
• Zeppellin clamps
• Right angle clamps
#3 – Entry (Anterior)
#3 – Entry (Anterior)
As long as bladder is dissected cephalad, it is not necessary to enter anterior peritoneum right away!
Tricks to Anterior Entry
• Finger through posterior colpotomy to anterior cul de sac to delineate peritoneum
• Retrofill bladder
• Curved uterine sound through urethra (especially with procidentia)
• Dissect bladder up (don’t need to enter anteriorly right away – be patient!)
Peritoneal entry Anterior & Posterior Entry
23

Posterior to Anterior Deaver Placement
#4 ‐ Hemostasis
• Proper hand positioning during clamping –cutting – tying• Right angles to vessels
• Vessel sealing devices• Gyrus/Olympus: PK Seal: 7mm• Ligasure Std/Xtd/Max: reusable components• Ligasure Impact: 7mm• Enseal G2 Super Jaw• Altrus: bladeless
Ligasure Max
Enseal #5: The Large Uterus
• Wessels, wessles, wessles…
• Then ‐
• Coring: don’t dig a hole; keep serosa exterior
• Bivalving
• Wedge extraction
• Sequential vaginal myomectomy
24

Bivalve + Myomectomy Bivalving the Uterus
Vaginal Myomectomy Wedge Extraction
The Wedge… Coring
25

Coring #6: The Adnexa
• Don’t use oophorectomy as reason to avoid
• Most ovaries can be removed vaginally
• Endoloop
Traditional (one pedicle) technique
• Mesosalpinx‐mesoovarium in one clamp
• Thick pedicle
• Retraction of vessels
• Incomplete removal
• Ureteral risk
Round Ligament Approach
#7: Complications
• Bleeding• Typically between utero‐ovarian and uterine• Posterior vaginal cuff• Inspect after hysterectomy prior to cuff closure
• Bladder injury• Typically superior to trigone (not near ureter)• Avoid blunt dissection esp with prior cesarean• Always, always CYSTO (sterile water if no indigo)
• Ureteral• Less common than with abdominal approach• Avoid with traction & retraction (lie at 2’ & 10’)
• Bowel injury
VTE Prophylaxis
26

Antimicrobials
• Cephalosporins are the antibiotics of choice
• Timed prior to induction of anesthesia
• Redose if surgery > 3hrs or EBL >1500ml
• Agents of choice in women with hypersensitivity to penicillin or cephalosporins:
• Clindamycin plus gentamycin or quinolone
• Metronidazole plus gentamycin or quinolone
Tricks to Overcome the Tough Case
• Narrow vagina – episiotomy
• Pelvic adhesions – use anatomy; consider lap
• Large uterus – morcellation
• Cervical elongation – delayed peritoneal entry
• Adnexectomy – proper technique
CONSIDER OUTPATIENT HYSTERECTOMY
Episiotomy (yuck…) Conclusions
References
• Aarts JW et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2015
• Geerts WH, et al. Prevention of venous thromboembolism. Chest 2004
• Zakaria MA, et al. Outpatient vaginal hysterectomy. ObstetGynecol 2012
• Surgical curriculum for residents in obstetrics and gynecology. CREOG 2002
Special thanks to:
Erika Banks, MDAndrew Sokol, MDBarbara Levy, MDRosanne Kho, MDMarie Paraiso, MD
27

RETROPUBIC SLINGS
Douglas Miyazaki MD
Womancare, Novant Health Wake Forest University
• I have no financial relationships to disclose
GOALS• Review retropubic anatomy
• Review Indications, Contraindications and Complications of retropubic slings
• Review proper surgical steps for sling placement
• Review steps for cystoscopy
• Understand and use the ACOG Assessment tool
Anterior repairs
Retropubic operationsBurch, MMK
Tension-free synthetic slingse.g. SPARC™, TVT™ 1995
Needle Suspensions Raz, Stamey
Autologous/Graft PV slings
Bone-anchored graft slingse.g. In-Fast Ultra™/InteXēn™
Tension-free biologic slingsBioArc™ SP
Singl Incision slings TO Subfascial HammockMonarcTM, BioArcTM , TOT
SUI Surgery: Historical Perspectives
Retropubic Anatomy Retropubic Anatomy
28

Historical Components of SUI Pathophysiology
• Loss of anatomic urethral support
• Urethral Hypermobility (UH) – Weakness of pelvic structures that support urethral compression during increased abdominal pressure.
• Intrinsic Sphincter Deficiency (ISD)
• Deficiency of urethral intrinsic closing mechanism.
Traditional Concept of SUI• Pathophysiology
SUI
UH ISD
ISD & Loss of Urethral Support A Clinical Continuum
SUI
ISDUH
ISD
Present to some degree in all SUI cases
Loss of Urethral Support with UH
Coexists with ISD in most casesLoss of support with both UH & ISD
Indications
• Symptomatic SUI
• Women who are having prolapse surgery with known or suspected SUI
Contraindications
• Current UTI
• Pregnancy
• Current Anticoagulation
• Structures in the Retropubic space that are a concern for injury
29

Complications
• Bladder injury 3.5‐6% surgeon experience big factor: experienced 1%, inexperienced 15‐34 %
• Voiding dysfunction 19‐47%, retention or incomplete emptying usually PVR>150cc
• Urgency symptoms 5.9‐25%
• Other: mesh exposure, vascular, bowel 0‐2.5%
• UTI fairly common 0‐34%
Assess Course Manuel
• Pre Operative Preparation
• Intra Operative Preparation
• Operative Predissection
Procedural Review• Operative: Dissection
• Retract posterior vaginal wall
• Identify mid‐urethra by placing traction on the Foley catheter
• Place Allis clamps 1 cm on either side of mid urethra
• Incise the epithelium with a 15‐blade with a full thickness vaginal wall – depth 0.3 to 0.7 cm (without hydrodissection)
• Initiate dissection with the blade – 45 – degrees from the midline penetrating 1.5 cm
• Grasp the full thickness dissection with Allis
• Insert Metz scissors and develop tunnel
• Tunnel 4cm at a 45‐degree angle from midline and 45 –degrees from horizontal
Procedural Review
• Operative: Passing Trocars
• Confirm that patient is in Trendelenberg position
• Remove Foley catheter
• Insert 18‐Fr Foley with catheter‐guide
• Assistant deviates the bladder to the patient’s right
• Insert trocar into right tunnel
• Remove all instruments from vagina
• Use the left hand to direct force to penetrate the anterior fibromuscular wall of the bladder. Needle is directed towards the ipsilateral shoulder
Procedural Review
• Operative: passing trocars
• After penetrating this wall, (<5 cm), redirect needle so that it is in‐line with the sagittal plane of the patient
• Advance trocar with the hand in the vagina directly behind the pubic bone until close to the suprapubic exit point.
• Transfer right hand to suprapubic area to assist penetrating skin
• Pull through sheath and disengage the trocar
• Repeat steps 4‐9 to insert trocar into left tunnel
Procedural Review
• Perform cystoscopy
• 70 degree lens
• Wiggle trocars to endure no muscularis injury
30

Procedural Review• Adjust sling tension
• Remove slack from sling so that there is 1‐2mm between sling and urethra
• Have patient cough, anesthesia administer Valsalva or apply suprapubic pressure
• Place Jorgensen scissors (or similar spacer) between the sling and the urethra. Insert until past the bend and to the nut to ensure adequate spacing.
• Slightly tighten sling although consider if patient doesn’t have their levator ani muscle due to anesthesia s to assist in continence
• Remove sheath by breaking the middle attachment of the sheath (for Advantage TF)
• Assistant to apply traction to the suprapubic portion of the sheath
• Confirm that removal sheath did not tighten or distort sling
Procedural Review• Close the vaginal wound
• Cut excess mesh arm below level of skin
• Close skin incisions
Video The ASSESSMENT
• Scoring Instructions: All scores will be in complete integers. No fractions are given. Participant will receive the full credit if the task is performed satisfactorily and 0 if either not performed or performed unsatisfactorily.
• 10 areas of assessment
Pass/Fail
• Assesses tissue and instrument handling
• Ability to function as primary surgeon: use of assistants, flow of operation and forward planning and overall knowledge of procedure
Overall Skill Level
• Rates performance level of surgeon
• Novice through Expert
31

Thank You Dr.s Nihira and Barenberg
• 1. Michael Baggish MK (2006) Atlas of Pelvic Anatomy and Gynecologic Surgery. In., Second edn., pp 315‐332
• 2. Muir TW, Tulikangas PK, Fidela Paraiso M, Walters MD (2003) The relationship of tension‐free vaginal tape insertion and the vascular anatomy. Obstet Gynecol 101 (5 Pt 1):933‐936
• 3. Bent A (2008) TeLinde's Operative Gynecology. In., Tenth edn., pp 942‐958
• 4. MD Walters MK (2007) Urogynecology and Reconstructive Pelvic Surgery. In., Third edn., pp 196‐210
References• 5. Daneshgari F, Kong W, Swartz M (2008) Complications of Mid Urethral
Slings: Important Outcomes for Future Clinical Trials. The Journal of Urology 180 (5):1890‐1897. doi:10.1016/j.juro.2008.07.029
• 6. Ogah J, Cody JD, Rogerson L (2009) Minimally invasive synthetic suburethral sling operations for stress urinary incontinence in women. Cochrane Database Syst Rev 7 (4
• 7. Blaivas JG, Groutz A. In: Retik AB, Vaughan ED Jr, Wein AJ, et al, eds. Urinary Incontinence: Pathophysiology, Evaluation, and Management Overview. Philadelphia, Pa: WB Saunders; 2002:1027–1052.
“Extra slides not part of talk” FDA Public Health NoticeOctober 20, 2008
• Recommendations:
• Specialized Training
Obtain specialized training for each mesh placement technique and be aware of its risks
• Potential Adverse Events from Mesh
Be vigilant for potential adverse events from mesh, especially erosion and infection
• Complications Associated with Mesh Tools
Watch for complications associated with the tools used in transvaginal placement, especially bowel, bladder and blood vessel perforations
FDA Public Health NoticeOctober 20, 2008
– Mesh is Permanent
– Additional Surgery May be Required
– Surgery May / May Not Correct Complication
Inform patients that implantation of surgical mesh is permanent, and that some complications associated with the implanted mesh may require additional surgery that may or may not correct the complication
– Potential for Serious Complications
Inform patients about the potential for serious complications and their effect on quality of life, including dyspareunia, scarring, narrowing of the vaginal wall (in POP repair)
– Provide Written Copy of Labeling
Provide patients with a written copy of the patient labeling from the surgical mesh manufacturer, if available
Second Notification – July 13, 2011
• Purpose of the Document:• Advise the public and medical community of complications related to
transvaginal POP repair with mesh
• Provide recommendations on how to counsel patients
• 13 questions patients should ask their doctor before they agree to have a surgery in which mesh will be used
• “The FDA continues to evaluate the effects of using surgical mesh for the treatment of SUI and will report about that usage at a later date.”
32

FDA September 2011 Recommendations in Part
4
• Reclassification of transvaginal surgical mesh products for POP to Class III (pre‐market approval) and to require manufacturers to conduct additional post‐market surveillance studies.
• Surgical mesh devices for SUI remain in Class II.
• No additional post‐market surveillance studies are necessary for retropubic and transobturator (TOT) slings.
• Pre‐market studies for new devices and additional post‐market surveillance studies for mini‐slings.
As a result of the September 2011 meeting, the panel and FDA found…5
• For surgical mesh slings used for SUI:
• The safety and effectiveness of multi‐incision slings is well‐established in clinical trials that followed patients for up to one‐year. Longer follow‐up data is available in the literature, but there are fewer of these long‐term studies compared to studies with one‐year follow‐up.
• The safety and effectiveness of mini‐slings for female SUI have not been adequately demonstrated. Presently, it is unclear how mini‐slings compare to multi‐incision slings with respect to safety and effectiveness for treating SUI. Additional studies may help the agency to better understand the safety and effectiveness of these devices.
As a result of the September 2011 meeting, the panel and FDA found…5
• Mesh sling surgeries for SUI have been reported to be successful in approximately 70 to 80 percent of women at one year, based on women’s reports and physical exams. Similar effectiveness outcomes are reported following non‐mesh SUI surgeries.
• The use of mesh slings in transvaginal SUI repair introduces a risk not present in traditional non‐mesh surgery for SUI repair,
which is mesh erosion, also known as extrusion.
As a result of the September 2011 meeting, the panel and FDA found…5
• Erosion of mesh slings through the vagina is the most commonly reported mesh‐specific complication from SUI surgeries with mesh. The average reported rate of mesh erosion at one year following SUI surgery with mesh is approximately 2 percent. Mesh erosion is sometimes treated successfully with vaginal cream or an office procedure where the exposed piece of mesh is cut. In some cases of mesh erosion, it may be necessary to return to the operating room to remove part or all of the mesh.
• The long‐term complications of surgical mesh sling repair for SUI that are reported in the literature are consistent with the adverse events reported to the FDA.
• The complications associated with the use of surgical mesh slings currently on the market for SUI repair are not linked to a single brand of mesh.
1. FDA. Public Health Notification: Serious Complications Associated with Transvaginal Placement of Surgical Mesh in Repair of Pelvic Organ Prolapse and Stress Urinary Incontinence CDRH October 2008;http://www.fda.gov/ MedicalDevices/Safety/AlertsandNotices/PublicHealthNotifications/ucm061976.htm.
2. FDA. Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Placement for Pelvic Organ Prolapse CDRH July 2011.
3. FDA. FDA Safety Communication: UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ Prolapse July 13, 2011. http://www.fda.gov/MedicalDevices/Safety/Alerts and Notices/ucm262435.htm.
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/MedicalDevices/MedicalDevicesAdvisoryCommittee/ObstetricsandGynecologyDevices/UCM271769.pdfConsiderations about Surgical Mesh for SUI: http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/UroGynSurgicalMesh/ucm345219.htm#.UWLj7d40J9E.email
33

$$$$$$$
• About Surgical WatchSurgicalWatch.com provides up to date information on lawsuits involving defective medical devices that affect US patients and consumers.
$$$$$$$
• 18,176 Ethicon pelvic mesh cases
• 17,812 AMS mesh lawsuits
• 12,004 Boston Scientific complaints
• 8,555 Bard Avaulta mesh claims
• 1,468 Coloplast mesh lawsuits
• 195 Cook Medical cases
• 52 Neomedic mesh lawsuits
$$$$$$$
• Last March, Bloomberg reported that a $16 million Coloplast mesh settlement was reached between parties in January of 2014 that would effectively resolve an estimated 400 legal complaints. Under the provisions of the agreement, each claimant would secure roughly $40,000 a piece to compensate for injuries and economic losses associated with products such as the Aris‐ Transobtrurator
and Novasilk‐Synthetic mesh systems.
$$$$$$$
• C.R. Bard Inc. agreed to pay more than $200 million to resolve at least 3,000 cases by women injured by the company’s vaginal‐mesh inserts, five people familiar with the accord said.
• The settlement resolves about a fifth of the outstanding suits related to the implants,
• Bard, based in Murray Hill, New Jersey, added $337 million to its $660 million reserve for product‐liability cases while acknowledging it had resolved 2,800 cases over “Women’s Health Products,” according to a July
24 filing with the U.S. Securities and Exchange Commission.
$$$$$$$
• Boston Scientific to pay $119 million to settle some meshclaims
• http://www.modernhealthcare.com/article/20150428/NEWS/150429889
• 4/28/2015 — Boston Scientific Corp. has agreed to pay $119 million to settle nearly 3,000 cases and claims over its transvaginal surgical mesh products, the company disclosed Tuesday in a filing with the Securities and Exchange Commission
$$$$$$$
• On April 30, Endo Health Solutions – parent company of American Medical Systems – agreed to settle approximately 20,000 lawsuits involving vaginal mesh devices sold by their AMS subsidiary. The $830 million vaginal mesh settlementmarked the largest accord achieved thus far in the mesh multidistrict litigation.
34

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
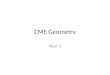
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
35