Embed Size (px)
Citation preview

FSCO 5 Year Review FSCO 5 Year Review Strategies for Strategies for Health care providersHealth care providers
Presentation by Claire WilkinsonRob Deutschmann(July 15, 2009)
Presented by Claire Wilkinson and Rob Deutschmann 2009 1

BackgroundBackground2003 was the last significant change
in auto insurance legislationAutomatic 5 year review inserted in
legislationIntervening years – “tweaking”:
◦Designated Assessment Centres (DACs) to Independent Medical Assessments (IMEs)
◦Treatment provider rates slashed by 1/3◦Lease company and employer liability
limitedPresented by Claire Wilkinson and Rob Deutschmann 2009 2

FSCO ReportFSCO ReportEconomic / Political climateEconomic / Political climate
Loss costs (the costs to provide) for accident benefits saw the largest relative increases during the past five years.
Accident benefits rose by 16.3% since 2003 but since 2004, the increase has been 34.6%.
Presented by Claire Wilkinson and Rob Deutschmann 2009 3

Loss RatioLoss RatioMeasure of performanceMeasure of performanceThe loss ratio is a fraction where
the numerator is the claims paid plus loss reserves and the denominator is the premiums collected.
Two types of loss ratios:◦Accident Benefits; and ◦Bodily Injury claims
Presented by Claire Wilkinson and Rob Deutschmann 2009 4

Loss ratiosLoss ratiosIt’s all about the bottom lineIt’s all about the bottom line
The lower the loss ratio, the better for the insurer ($$$)
For example, if the claims paid plus reserves is $60 in a year and the premiums collected $80, the loss ratio is 60/80, or 75%.
A loss ratio of 75% means an insurer is making a profit. A loss ratio of 90% may represent a loss to the insurer.
Presented by Claire Wilkinson and Rob Deutschmann 2009 5

Accident Benefit loss ratioAccident Benefit loss ratioVaries among insurers - Varies among insurers - 20082008
Co-operators - 72%Pilot Insurance - 180%.
Average for all Canadian P/C insurers – 125%
Bodily injury loss ratio - 69%
Presented by Claire Wilkinson and Rob Deutschmann 2009 6

Statistics according to IBCStatistics according to IBCNo-fault injury claims in Ontario
cost much more than similar claims in other provinces.
Alberta - $3,000 per claimNew Brunswick - $11,700 per claimOntario - $38,000 per claim
Presented by Claire Wilkinson and Rob Deutschmann 2009 7

Statistics according to IBCStatistics according to IBC
in Alberta, 40% of sprain and strain claims are still open after 6 months. In Ontario, that figure doubles to 80%.
This is part of the IBC attack on treatment providers
Presented by Claire Wilkinson and Rob Deutschmann 2009 8

Here’s the scary part Here’s the scary part – according to FSCO– according to FSCO
Rate increases have not kept pace with rising loss costs and the insurance sector reports significant rate inadequacy in the system.
Presented by Claire Wilkinson and Rob Deutschmann 2009 9

FSCO’s “bottom line”FSCO’s “bottom line”Declining profitability, significantly
lower earnings and loss cost increases will accelerate in 2009 in the absence of structural changes to stabilize costs.
Read between the lines – premiums will need to increase if costs are not controlled.
Presented by Claire Wilkinson and Rob Deutschmann 2009 10

Lest we forgetLest we forgetInsurers have done very wellInsurers have done very well2003 to 2007 were record years
for insurersReturn on Equity:2003 – 11.9%2004 – 19.0%2005 – 16.5%2006 – 20.1%2007 – 16.1%2008 – 7.5%
Presented by Claire Wilkinson and Rob Deutschmann 2009 11

Problems with the insurance Problems with the insurance debate in Ontariodebate in Ontario
No one knows what the true numbers are
Numbers are not shared by the IBCHCAI has not been successfulAnecdotal evidence
◦Assessment mills◦Multiple assessments to overwhelm adjuster◦Increasing requests for in-home
assessments
Presented by Claire Wilkinson and Rob Deutschmann 2009 12

Policy vs. PoliticsPolicy vs. PoliticsIt’s all about the politics
Nothing strikes fear in the Ontario provincial government more than the risk of increasing premiums.
Presented by Claire Wilkinson and Rob Deutschmann 2009 13

IBC and Premium IBC and Premium increasesincreasesRecent news stories – IBC has
talked about the need to raise premiums
Cause:◦Investment losses◦Rising costs in Med and Rehab
treatment
Presented by Claire Wilkinson and Rob Deutschmann 2009 14

The IBC plays on The IBC plays on fears of higher premiumsfears of higher premiums
On average, drivers in Ontario pay higher premiums than drivers in all other provinces where auto insurance is sold competitively by private companies – 25% more than in the “private” jurisdiction with the next highest premiums, Alberta. (IBC submission July 2008)
Presented by Claire Wilkinson and Rob Deutschmann 2009 15

FSCO ReportFSCO Report39 RecommendationsThere are a few controversial
recommendationsGeneral theme –
reducing Cost and Complexity
The changes will have the most significant impact on non-CAT seriously injured
Presented by Claire Wilkinson and Rob Deutschmann 2009 16

Health care providersHealth care providersWhat has changed from your
perspective?
What should you be aware of and new strategies to apply?
How do you continue to be an effective advocate on behalf of your patient?
Presented by Claire Wilkinson and Rob Deutschmann 2009 17

Not quite the sameNot quite the sameThe catastrophically injured will
still have access to a higher level of benefits
BUT there will be G A P S in the system
Presented by Claire Wilkinson and Rob Deutschmann 2009 18

Current Catastrophic Current Catastrophic definitionsdefinitionsThere is no change AT THIS TIMEThe “straight forward”
definitions:◦GCS – 9 or less◦Paraplegia or quadriplpegia◦Amputation or impairment causing
total and permanent loss of use of both arms or an arm and a leg
◦Total loss of vision in both eyes.
Presented by Claire Wilkinson and Rob Deutschmann 2009 19

The problem areas:The problem areas:The whole person impairment
rating of 55% or higher
The combining of physical and psychological impairments
Marked impairment
Presented by Claire Wilkinson and Rob Deutschmann 2009 20

Why is it a problem?Why is it a problem?The injured person has to wait for
assessment:
(a)Until health practitioner says persons condition has stabilized; or
(b)Two years elapsed since the accident
To determine whether Catastrophically impaired
Presented by Claire Wilkinson and Rob Deutschmann 2009 21

One big reason it’s a One big reason it’s a problemproblem
The most controversial change recommended by FSCO . . .
Presented by Claire Wilkinson and Rob Deutschmann 2009 22

Recommendation #22Recommendation #22
Reducing the med rehab capReducing the med rehab cap
Reduce the cap for medical and rehabilitation benefits for non-catastrophic claims to $25,000.
Introduce a $100,000 optional medical and rehabilitation benefit along with the existing $1 million optional benefit.
Presented by Claire Wilkinson and Rob Deutschmann 2009 23

Why did FSCO recommend Why did FSCO recommend this?this?FSCO ReportFSCO ReportProvide consumers with more choice
and would allow them to customize coverage according to their needs.
The insurance industry has proposed that a reduced cap of $25,000 would adequately meet the needs of many consumers.
Consumers that feel they need a higher level of coverage could be provided the option of purchasing $100,000
Presented by Claire Wilkinson and Rob Deutschmann 2009 24

““Consumers will appreciate Consumers will appreciate it”it”FSCO ReportFSCO ReportConsidering the rate inadequacy
that currently exists in Ontario, consumers will appreciate opportunities to reduce coverage that they may not need and avoid possible premium increases. ◦As an alternative, the cap could be
reduced to $50,000 but this would reduce the opportunity for consumers to realize savings.
Presented by Claire Wilkinson and Rob Deutschmann 2009 25

Coverage under Tort claimCoverage under Tort claimFSCO ReportFSCO ReportSome auto accident claimants
would be eligible for compensation beyond the $25,000 by suing an at-fault driver.
Those eligible would have to have injuries that exceed the existing “serious and permanent impairment” threshold in the Insurance Act
Presented by Claire Wilkinson and Rob Deutschmann 2009 26

Reducing the med rehab Reducing the med rehab capcapControversial recommendationAlliance of Community Medical &
Rehabilitation Providers have actively lobbied primarily on this recommendation
No one aware until they are a victim – too late
Potential for an increase in cap to $50,000
Presented by Claire Wilkinson and Rob Deutschmann 2009 27

Reducing the med rehab Reducing the med rehab capcapAccident victims suffering from
catastrophic injury will not be affected as long as they are deemed Catastrophically impaired immediately
Will have access to enhanced medical and rehabilitation benefits and attendant care benefits.
Presented by Claire Wilkinson and Rob Deutschmann 2009 28

Future considerations:Future considerations:A third level of coverageA third level of coverage
Some consideration should be given to a more generous level of benefits for group of very seriously injured claimants with serious orthopaedic or brain injury who will not immediately meet the catastrophic test.
Presented by Claire Wilkinson and Rob Deutschmann 2009 29

Even the IBC made a Even the IBC made a recommendationrecommendation (July 2008)(July 2008)
A. For non-Catastrophic (CAT) claimants, establish the maximum limit for payments for medical/rehabilitation and provider-initiated assessments at $25,000, but retain the $100,000 limit for injured persons admitted to a public hospital for at least two consecutive days in the immediate aftermath of the injury;
Presented by Claire Wilkinson and Rob Deutschmann 2009 30

So what does this all So what does this all meanmeanSome seriously injured people will
fall into the $25,000 to $1million GAP
They will use up the AB funds well before 2 year mark
They may include:◦Patient with a GCS of 10 or higher◦Patient with significant orthopaedic
injuries but not complete loss as per CAT defn
Presented by Claire Wilkinson and Rob Deutschmann 2009 31

What do these victims doWhat do these victims doThey are facing the prospect of
trying to get by with $25,000 for 2 years
Future needs will have to be assessed immediately so that strategies can be considered
Contact a personal injury lawyer to develop and implement strategies
Presented by Claire Wilkinson and Rob Deutschmann 2009 32

What should you be What should you be looking for?looking for?Copy of the patient’s insurance
policy, or some confirmation, to determine if optional medical coverage was obtained ($100,000 or more)
Determine what other medical benefit plans are available – employer; dependant◦Some lose employment and medical
benefitsPresented by Claire Wilkinson and Rob Deutschmann 2009 33

Why a personal injury Why a personal injury lawyer?lawyer?Victims, not at fault, can claim in
tort for future medical costs from the at fault party◦Defining regulation makes access
more restricted
Often considered later in the process due to the availability of accident benefits but will become important early in process
Presented by Claire Wilkinson and Rob Deutschmann 2009 34

Strategies for medical Strategies for medical benefitsbenefitsSeek an advance for medical
treatment costs from the at fault insurer
Tort insurer incentive:◦the sooner the victim receives
treatment, ◦the quicker the recovery◦the lower the future damages
Presented by Claire Wilkinson and Rob Deutschmann 2009 35

Strategies for medical Strategies for medical benefitsbenefitsGuarantee payment to third party
provider from tort settlement◦Cash flow problems for treatment
providers
Persuade AB insurers to pay for additional treatment if it can bring injured person back to work sooner ◦Insurer can minimize Income
Replacement Benefits exposurePresented by Claire Wilkinson and Rob Deutschmann 2009 36

Advances spent on other Advances spent on other prioritiesprioritiesThere are some who say we cannot
give the victim these medical fundsMedical funds not applied to future
medical needs but to household debt
Personal injury lawyer could administer the funds
Onus on injured person to use funds for treatment – would reflect poorly at trial
Presented by Claire Wilkinson and Rob Deutschmann 2009 37

Third party lendersThird party lendersFinancial assistance in the form
of “bridge loans” to plaintiffs facing financial pressures in advance of the resolution of their legal claims.
Flexibility regarding termsCarefully review repayment
options, payment priorities and interest rates
Presented by Claire Wilkinson and Rob Deutschmann 2009 38

Other Optional benefits:Other Optional benefits:Housekeeping and CaregiverHousekeeping and CaregiverRecommendation #29Make housekeeping and home
maintenance expenses and caregiver benefits optional. Reimbursement for housekeeping and home maintenance expenses and for replacement caregivers needs to reflect actual economic losses.
Presented by Claire Wilkinson and Rob Deutschmann 2009 39

Optional coverage issuesOptional coverage issuesFSCO view is that as long as the
option is available consumers have access and are protected
Optional coverage will not guarantee all have access if the communication / information process is insufficient
The role of the Insurance Broker becomes more important
Presented by Claire Wilkinson and Rob Deutschmann 2009 40

Housekeeping and Housekeeping and CaregiverCaregiverFSCO relying on information
provided by the IBC◦“increasing at a significant rate …
contributing to rising claim costs”◦Insurer reports high proportion of
payments … although no numbers were provided
◦Anecdotal evidence – receive claims from multiple family members
Presented by Claire Wilkinson and Rob Deutschmann 2009 41

Housekeeping and Housekeeping and CaregiverCaregiverFSCO is “concerned about
growing cost of the benefit”5 other provinces do not provide
caregiver benefitSolution – optional coverage
Presented by Claire Wilkinson and Rob Deutschmann 2009 42

Optional coverageOptional coverageOne approach to address rising
costs and utilization is to provide consumers with more choice by converting a number of mandatory benefits to optional benefits.
Presented by Claire Wilkinson and Rob Deutschmann 2009 43

Optional coverageOptional coverageThis would provide consumers
with the ability to customize coverage according to their needs.
When do we know what we need.
Presented by Claire Wilkinson and Rob Deutschmann 2009 44

Insurance brokers roleInsurance brokers roleInsurance brokers have to step up
and educate their clients/customers on the options
Mandatory disclosure – sign off sheet
Form – outlines the following:◦all optional coverages outlined◦Rationale for purchasing coverage◦Premium associated◦Client to initial off
Presented by Claire Wilkinson and Rob Deutschmann 2009 45

Broker liabilityBroker liabilityWell established in law that the
broker owes a duty to client to advise and review
Presented by Claire Wilkinson and Rob Deutschmann 2009 46

Recommendation #10Recommendation #10
CAT definitionCAT definitionFurther consultation with experts in
the field is needed to amend the definition of “catastrophic impairment.”
FSCO - The goal for this review should be to ensure that the most seriously injured accident victims are treated fairly.
Presented by Claire Wilkinson and Rob Deutschmann 2009 47

FSCO concernsFSCO concernsConfusion based on evolving
decisions on CAT definitionParticularly combining physical
and psychological ◦Despite Desbiens and subsequent
decisions FSCO unsure whether appropriate to combine
Expanded definitions have exposed system to “potential abuse”
Presented by Claire Wilkinson and Rob Deutschmann 2009 48

FSCO concernsFSCO concernsFSCO is searching for a “clear
and fair” definition of catastrophic impairment
Presented by Claire Wilkinson and Rob Deutschmann 2009 49

IBC has already started the IBC has already started the processprocessThe Insurance Bureau of Canada
(IBC) approached the Ontario Neurotrauma Foundation to form an expert panel to review the current science and evidence with which to measure and define brain impairment.
Evidence Based Classification of Brain Impairment: Application to Catastrophic Impairment Classification
Presented by Claire Wilkinson and Rob Deutschmann 2009 50

Attempting to build a better Attempting to build a better predictor “mousetrap”predictor “mousetrap”
Presented by Claire Wilkinson and Rob Deutschmann 2009 51

Attempting to build a better Attempting to build a better predictor “mousetrap”predictor “mousetrap”• Discussion of Evidence Based Framework for Identifying Catastrophic Brain Impairment
• The experts reviewed a large number of assessments that could potentially be used to classify catastrophic brain impairment.
• Measures identified that do have evidence to support their use in classifying catastrophic brain injury.
Presented by Claire Wilkinson and Rob Deutschmann 2009 52

Attempting to build a better Attempting to build a better predictor “mousetrap”predictor “mousetrap” The final set of assessments that were felt to
have sufficient evidence for use were:
1. Glasgow Coma Scale (GCS)
2. Age
3. Computed Tomography (CT) Scan in those with GCS < than 9
4. Somatosensory Evoked Potentials (SEPs)
5. Duration of Post Traumatic Amnesia (possibly measured by the Galveston Orientation and Amnesia Test (GOAT))
6. Disability Rating Scale (DRS)
Presented by Claire Wilkinson and Rob Deutschmann 2009 53

Presented by Claire Wilkinson and Rob Deutschmann 2009 54
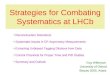
Category Score Timing
Automatically Considered Severe Catastrophic Lowest GCS<5 6- 24 Hours Post Onset
Automatically Catastrophic Lowest GCS <9 and CT scan shows obliteration
of the cerebral ventricles by brain swelling 6- 24 Hours Post Onset
Automatically Catastrophic Lowest GCS <9 and age greater than 60 years of
age 6- 24 Hours Post Onset
Automatically Catastrophic Lowest GCS <9 and SEPS show unilateral or
bilateral absence of potentials First 2 weeks
Provisionally/Probably Catastrophic Lowest GCS =6-9 6- 24 Hours Post Onset
Potentially Catastrophic Lowest GCS 9-14 6- 24 Hours Post Onset
Catastrophic/Severe Impairment GOAT Score<75 At 30 Days and 60 Days
Disability Rating Scale >5 6 Months Up to 2 Years

Which way is FSCO trending Which way is FSCO trending on CAT assessments?on CAT assessments?Could reduce the number of
people deemed catastrophicSome involved with the
Neurotrauma team working on the report argue otherwise◦More people will be covered◦More certainty and fewer disputes
More complication
Presented by Claire Wilkinson and Rob Deutschmann 2009 55

Where should they go with Where should they go with the CAT determination?the CAT determination?If you want to help the most
seriously injured then:Simplify the assessment model –
DON’T make it more complicated◦More CAT variations adds
complicationExpand the number of seriously
injured that qualify as CAT and focus on NEED
Presented by Claire Wilkinson and Rob Deutschmann 2009 56

Recommendation #17Recommendation #17
Catastrophic AssessorsCatastrophic Assessors
Restrict the ability to conduct catastrophic impairment assessments to practitioners with appropriate training and experience.
Presented by Claire Wilkinson and Rob Deutschmann 2009 57

Cost of Catastrophic Cost of Catastrophic assessmentsassessmentsOne insurer provided FSCO with
examples of insurer examinations to determine catastrophic impairment that ranged in cost from $15,000 to $43,000
The Toronto Transit Commission reports assessments often cost between $20,000 and $30,000 and involve a multidisciplinary team of experts
Presented by Claire Wilkinson and Rob Deutschmann 2009 58

Cost of AssessmentsCost of AssessmentsFSCO questions why so much is
being spent on catastrophic impairment assessments
FSCO – “insurers insist on lengthy medical-legal reports in response to requests for catastrophic impairment determinations that have little merit. This type of security comes at a very high price. “
59Presented by Claire Wilkinson and Rob Deutschmann 2009

Cost of AssessmentsCost of AssessmentsFSCO ReportFSCO ReportThe WSIB conducts an analogous
assessment The assessment is also based on
the AMA Guides, but based on the 3rd edition
In the WSIB system, assessors are predominantly physicians who are trained on the use of the Guides.
60Presented by Claire Wilkinson and Rob Deutschmann 2009

The problem with inadequate The problem with inadequate assessmentsassessments
Inaccurate ratings, More FSCO disputes
◦Mediations and arbitrationsAdditional assessments
all adding more costs and uncertainty to the system.
Presented by Claire Wilkinson and Rob Deutschmann 2009 61

Who will do CAT Who will do CAT assessments?assessments?FSCO ReportFSCO ReportWSIB assessors – who are
predominantly specially trained physicians – are paid a substantially lower flat fee which covers time spent with the injured worker, reviewing documentation, and preparing a report.
Presented by Claire Wilkinson and Rob Deutschmann 2009 62

Capping Assessment costsCapping Assessment costsRecommendation #12:The fee for completing forms
including any assessment required to complete the form should be capped at $200. The cost of all other assessments should be capped at $2,000
Presented by Claire Wilkinson and Rob Deutschmann 2009 63

Capping Assessment costsCapping Assessment costsRecommendation #18:The costs of insurer examinations
should be capped at $2,000.00
FSCO - providing “balance” in reducing assessments under s.24 and IMEs under s.42◦Would be interesting to know the
costs attributed under each section
Presented by Claire Wilkinson and Rob Deutschmann 2009 64

FSCO’s view of FSCO’s view of assessmentsassessmentsAssessment costs are getting out of
control and have to be reined in.
FSCO does not want to regulate the provision of third party medical examinations.
FSCO would participate in a process involving health care associations to develop standards
65Presented by Claire Wilkinson and Rob Deutschmann 2009

What is the basis for this What is the basis for this view?view?FSCO does not have it’s own
figuresReliance on IBC informationUse of anecdotal evidence:
◦“Assessment mills”◦Multiple assessment requests to
overwhelm adjusters◦Assessments requested without
consent of insured◦Illegal payments for referrals
Presented by Claire Wilkinson and Rob Deutschmann 2009 66

The cap on assessments and The cap on assessments and IMEsIMEs$2,000 cap on assessments will
not cover the cost◦CAT assessments◦Psychological / neuropsychological
Would the $2,000.00 cap apply per assessment ◦Multi disciplinary assessments
Presented by Claire Wilkinson and Rob Deutschmann 2009 67

Strategy moving forwardStrategy moving forwardIssue - current AB assessors will
reduce or discontinue CAT assessments
A third party source will have to fund assessment costs◦Third party lenders◦Personal injury lawyers
Clarify the per assessment concept Presented by Claire Wilkinson and Rob Deutschmann 2009 68

Recommendation #14Recommendation #14
In-home AssessmentsIn-home AssessmentsAvailability of in-home
assessments should be limited to seriously injured claimants
Evaluate their need for attendant care services and home modifications.
Presented by Claire Wilkinson and Rob Deutschmann 2009 69

In-home AssessmentsIn-home AssessmentsFSCO ReportFSCO ReportExisting industry data does not
separate out assessments conducted in the claimant’s home.
There is sufficient anecdotal information to support the suggestion that they have become a growing source of costs.
Presented by Claire Wilkinson and Rob Deutschmann 2009 70

In-home AssessmentsIn-home AssessmentsFSCO ReportFSCO ReportThe WSIB conducts similar
assessments but they are limited to their most seriously injured clients.
FSCO – “there is nothing unique about auto accident victims when it comes to assessment needs”.
Presented by Claire Wilkinson and Rob Deutschmann 2009 71

In-home AssessmentsIn-home AssessmentsFSCO ReportFSCO ReportExpensive and limited health
care resources are being tied up by health care providers travelling to clients.
Therefore, most assessments should be conducted in a clinical setting.
Presented by Claire Wilkinson and Rob Deutschmann 2009 72

In-home AssessmentsIn-home AssessmentsIssues to considerIssues to considerRecommendation based on IBC
reportsUses WSIB analogyWho is “seriously injured”Not a defined term under the SABsHow do you replicate home setting
in clinical settingWill add uncertainty to the processDelay access to assessment and
treatmentPresented by Claire Wilkinson and Rob Deutschmann 2009 73

Future Concern:Future Concern:FSCO reliance on WSIB FSCO reliance on WSIB modelmodelNumerous references to WSIB
throughout the FSCO report#35 – training adjusters
◦FSCO looked at how WSIB structured claim adjudication
#30 – Harmonizing auto and workplace insurance systems
#26 – Fees◦Reduction in 2003 intended to bring
fees in line with WSIB feesPresented by Claire Wilkinson and Rob Deutschmann 2009 74

Recommendation #25Recommendation #25
Payment for past Attendant Payment for past Attendant Care Care The attendant care benefit
should continue to compensate claimants for incurred expenses.
Looking at payments for past attendant care
Presented by Claire Wilkinson and Rob Deutschmann 2009 75

Past Attendant CarePast Attendant CareMcMichael caseGenerally where 24/7 care requiredInsured did not have to show that
expenses were actually incurred but that they were reasonable and necessary
Insurers could receive windfall by denying and delaying benefit
Presented by Claire Wilkinson and Rob Deutschmann 2009 76

Past Attendant CarePast Attendant CareFSCO trying to balance interests
by recommending payment if insurer is shown to be unreasonably denying
Uncertainty when interpreting “unreasonable” conduct
Insurer’s tinkering to fill a “loophole”
Presented by Claire Wilkinson and Rob Deutschmann 2009 77

Recommendation #33Recommendation #33
Future Care reportsFuture Care reportsThe cost of future care cost
reports should not be an expense recoverable under the SABS
Continuing with the theme of reducing assessment costs
Presented by Claire Wilkinson and Rob Deutschmann 2009 78

Future Care reportsFuture Care reportsInsurers dispute payment of
reports as they do not deal with an “incurred expense”
Insurers would like to see CCAC standards applied to recommendations
FSCO does not consider these reports covered by the SABs
Presented by Claire Wilkinson and Rob Deutschmann 2009 79

Future Care reportsFuture Care reportsOptionsOptionsAccepted that they are necessary
for CAT casesIssue is whether the insured is
seriously injured to require any significant future care needs
Will become a negotiated item with AB adjuster wishing to settle file
Can be covered where insured has a tort claim
Presented by Claire Wilkinson and Rob Deutschmann 2009 80

Role of the family doctorRole of the family doctorRecommendations #15 and #21
have been focused on the role of the family doctor in auto insurance claims
Attempting to control cost of assessments
Attempting to better coordinate rehabilation
Presented by Claire Wilkinson and Rob Deutschmann 2009 81

Recommendation #15Recommendation #15
Assessments Assessments Consider having assessment
requests completed only after a referral is made by the health professional primarily responsible for the claimant’s rehabilitation (in most cases a family physician).
Assessment requests would continue to be submitted by providers following a referral
Presented by Claire Wilkinson and Rob Deutschmann 2009 82

Involvement of family doctorInvolvement of family doctorFSCO ReportFSCO ReportCurrent problem:Any regulated health professional or
social worker is able to submit a request for an assessment and the insurer must respond.
Insurer cannot deny the request until an insurer examination has been conducted.
Insurer must incur costs in response to even the most questionable assessment requests
Presented by Claire Wilkinson and Rob Deutschmann 2009 83

Involvement of family doctorInvolvement of family doctorFSCO ReportFSCO ReportWhy is the Ontario auto insurance
system so different than other systems?
FSCO has concluded that one area where Ontario differs is in how treatment is managed.
The Ontario system appears to lead to multiple and duplicative assessments and fragmented treatment
Presented by Claire Wilkinson and Rob Deutschmann 2009 84

Involvement of family doctorInvolvement of family doctorFSCO reportFSCO reportIn approximately half of
Canadian jurisdictions, physicians direct assessments and treatment. In Saskatchewan claimants are asked to designate a primary practitioner who can be a physician, chiropractor or physiotherapist
Presented by Claire Wilkinson and Rob Deutschmann 2009 85

Involvement of the family Involvement of the family doctordoctorFSCO reportFSCO reportIn Ontario there are 24 professions
that are authorized to conduct an assessment
expansion in the number of regulated health professions may create even more cost pressures on the auto insurance system when implemented such that they begin to conduct assessments
Presented by Claire Wilkinson and Rob Deutschmann 2009 86

Involvement of the family Involvement of the family doctordoctorFSCO conclusionFSCO conclusionA single professional responsible
for rehabilitation can fully and accurately respond to questions from the claimant and adjuster concerning the appropriateness of the proposed assessments and treatment
Presented by Claire Wilkinson and Rob Deutschmann 2009 87

Involvement of the family Involvement of the family doctordoctorFSCO conclusionFSCO conclusionThe increased involvement of
physicians is not expected to impact on the doctor shortage in Ontario.
Claimants with more serious injuries already see their family doctors following an accident.
The proposed changes will not significantly increase the number of doctor visits and will benefit claimants by keeping their family doctors better informed on their progress
Presented by Claire Wilkinson and Rob Deutschmann 2009 88

Recommendation #21Recommendation #21
Access to treatmentAccess to treatmentConsider having treatment plans
completed only after a referral is made by a health professional primarily responsible for the claimant’s rehabilitation (in most cases a family physician)
Treatment plans would continue to be submitted by providers following a referral.
Presented by Claire Wilkinson and Rob Deutschmann 2009 89

Physicians initiate treatment Physicians initiate treatment requestrequestFSCO reportFSCO reportConcern about the expansion of
the definition of regulated health professions
Expanding health practitioner status will increase complexity and diffuse accountability
7 of 10 provinces – physicians only may certify need for treatment
Presented by Claire Wilkinson and Rob Deutschmann 2009 90

Physicians initiate treatment Physicians initiate treatment requestrequestFSCO ReportFSCO ReportNo single health professional
actually overseeing a patient’s rehabilitation◦Left to the AB adjuster.
Directing patient to appropriate treatment providers
The insured would see the health professional before subsequent treatment plans
PAFs would continue Presented by Claire Wilkinson and Rob Deutschmann 2009 91

Physicians initiate treatment Physicians initiate treatment requestrequestFSCO ReportFSCO ReportEliminate the potential for conflict
in existing delivery model - health professional not connected to treatment facility
Family physicians directing their patients to appropriate health care providers and services
Ontarians without family doctors will use walk-in clinics / ambulatory care
Presented by Claire Wilkinson and Rob Deutschmann 2009 92

Potential issues with #15 Potential issues with #15 and #21and #21Delays to see a family doctor
Delay in treatmentShortage of family doctors in Ontario
Increase use of walk in clinics / emergency
Flexibility needed for those without a family doctor
PAF may have to be expandedRecommendation #23
Not supported by the OMA
Presented by Claire Wilkinson and Rob Deutschmann 2009 93

Use of family doctorUse of family doctorThe forms and reporting process will
have to be simplifiedReporting to physicians – inundated
with paperwork and reportsTreatment providers will have to
educate physicians on the SABs process
Treatment providers will have to interact more with family physicians
Presented by Claire Wilkinson and Rob Deutschmann 2009 94

Recommendation #31Recommendation #31
Tort (law suit)changesTort (law suit)changes• Reducing the deductibles (from
$30,000) to $20,000 and (from $15,000) to $10,000• 2003 increase was excessive
• Eliminating the deductibles for fatality claims, • Ex. Grandparent dies leaving a
spouse, 3 children and 10 grandchildren
• Total deductible - $245,000Presented by Claire Wilkinson and Rob Deutschmann 2009 95

Recommendation #31Recommendation #31
Tort (law suit)changesTort (law suit)changes• Revoking the definition of serious
and permanent impairment• Provide clarity
• A closed claim study would assist in determining the impact of further tort changes being considered. • Only jurisdiction with both a
deductible and thresholdPresented by Claire Wilkinson and Rob Deutschmann 2009 96

Recommendation #35Recommendation #35
Better trained adjustersBetter trained adjustersInsurance claims departments
need to better focus on the needs of claimants with serious injuries.
The IBC, Insurance Institute of Ontario and the Ontario Insurance Adjusters Association should work together to train adjusters on the needs of claimants with serious injuries to reduce exposure to potential allegations of unfair and deceptive acts or practices.
Presented by Claire Wilkinson and Rob Deutschmann 2009 97

39 Recommendations39 RecommendationsWhat will happen next?What will happen next?Announcement has been pushed
back to the end of August
Minister not bound by the FSCO recommendations.
Expect most of the package to be adopted with some modifications – focus on the med rehab cap
Presented by Claire Wilkinson and Rob Deutschmann 2009 98

Future ReviewsFuture Reviewss.289, Insurance Acts.289, Insurance ActAt least once every two years, the
Minister shall table a report in respect of the adequacy of statutory accident benefits and setting out changes made to the SABs since the last report and changes that are proposed to the SABs at the time of the report
Last report was end of 2008Presented by Claire Wilkinson and Rob Deutschmann 2009 99

Future reviewFuture reviewThis is in addition to the 5 year
reviewReview the July 2008 IBC submission The IBC will continue to propose
significant cuts to Accident Benefits◦ie. Housekeeping – limiting entitlement to
2 weeks for least serious injuries◦Not payable to family members where no
economic loss incurred
Presented by Claire Wilkinson and Rob Deutschmann 2009 100