Embed Size (px)
Citation preview

Images From Headache
Frontal Headache Induced by Osteoma of Frontal Recess
Kyung Soo Kim, MD, PhD
We reported a case of osteoma involving the frontal recess, which presented as frontal headache and reviewed literatures.Also, this case highlights that sinunasal osteomas can cause pain by local mass effects, referred pain, or prostaglandinE2-mediated mechanisms.
Key words: osteoma, frontal headache, pathophysiology
(Headache 2013;53:1152-1154)
A 31-year-old woman presented with a 1-yearhistory of intermittent frontal headache and an unspe-cific compression in the right frontal area.The charac-ter of headache was atypical, dull, and pressure-like.There were no precipitating or aggravating factors.The patient took analgesics (acetaminophen), whichwere partially effective. The patient had no traumahistory or significant past medical history.
The patient had first presented to a neurologist.Physical examinations including neurologic examina-tion and detailed laboratory examinations wereentirely normal. To exclude other symptomatic head-aches, brain computed tomography scan was per-formed, and it showed no intracerebral structurallesions. However, the scan revealed a 1.2 ¥ 0.9 cm,well-defined extremely radiodense lesion in the rightfrontal recess, without invading the neighboringstructures and secondary sinusitis. The patient wasreferred to our department for proper treatment.Sinonasal endoscopic examination revealed a normalnasal septum with an adequate nasal airway bilater-ally. Under general anesthesia, this mass was easilyand completely removed via endoscopic sinus surgery
because the lesion was well demarcated from sur-rounding normal tissues. She reported prompt reliefof her headache. She has done well during a follow-upperiod of 12 months with no signs of recurrence.
COMMENTSAlthough paranasal osteomas are usually asymp-
tomatic, the clinical presentation can vary widely,depending on the location, size, and growth direc-tion.1 Significantly sized osteomas can be associatedwith minor discomfort, while some smaller lesions,located mainly in the frontal recess, can be respon-sible for severe pain and discomfort.2 The mostcommon symptom is pain (including headache) in thefrontal area and facial pain located in the orbitalregion.3
Although it is not enough to know that the pain iscaused by osteoma, there are 3 important points toexplain the pathophysiology of pain.
First, the osteoma pain could be caused by localmass effects. The pressure created by the growth ofthe tumor can result in pain in the head as well as theface.4 Osteomas of the frontal sinus may causechronic headache because continued growth maycause pressure against the anterior or posterior table,resulting in headache.5From the Department of Otorhinolaryngology-Head and Neck
Surgery, Chung-Ang University College of Medicine, Seoul,South Korea. Conflict of Interest: The author reports no conflict of interest.
ISSN 0017-8748doi: 10.1111/head.12029
Published by Wiley Periodicals, Inc.Headache© 2012 American Headache Society
1152

Second, increased prostaglandin E2 (PGE2) syn-thesis suggests an important pathophysiological roleas a mediator of the osteoma pain because osteoma isan osteoblastic benign tumor. Variation in expressionof PGE2 may be related to variations in the states ofproliferation and differentiation of the osteoblastictumor cells in other types of benign bone tumor,such as osteoid osteoma or fibrous dysplasia.6 PGE2probably causes pain by 2 complex mechanisms. Theenhanced blood flow induced by PGE2 may increase
the vascular pressure, stimulating afferent autonomicnerves close to blood vessel. Furthermore, PGE2 maydirectly sensitize unmyelinated nerve fibers, trans-mitters of slow pain.6 A similar mechanism may bethought to exist in osteoma, although the role ofPGE2 has not been investigated in osteoma.7
Third, the osteoma could be a kind of referredneuralgia (trigeminal neuralgia). The ophthalmic andmaxillary divisions of the trigeminal nerve innervatemost of the anterior craniofacial structures including
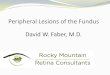
Fig 1.—Computed tomography showed well-defined extremely radiodense lesion in the right frontal recess without invading theneighboring structures and secondary sinusitis. (A) Axial, (B) coronal, and (C) sagittal view.
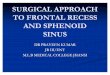
Fig 2.—Correlation between computed tomography (CT) findings and endoscopic findings during endoscopic sinus surgery. (Whiteasterisk: frontal sinus; black circle: osteoma; white heart: ethmoid sinus)
Headache 1153

the nose and paranasal sinuses. Free nerve endingsrespond to any kind of noxious stimulation such aschemical, mechanical, and caloric stimuli to promptthe release of substance P. This produces an ortho-dromic impulse traveling along nociceptive C fibersthat is interpreted centrally as pain, but may not bewell localized by higher cortical centers.8
When a patient complains of headache in thevicinity of an osteoma, and other pathologies leadingto headache have been ruled out, excision is indi-cated.9 Whether intranasal endoscopic or externalapproach, the best decisions must be based on indi-vidual presentation, including the location and extentof the osteomas and the nature of any existing com-plications.1 Recently, resection of small- and medium-sized osteomas of the paranasal sinuses withoutevidence of orbital or intracranial extension can besafely and radically performed using endoscopic tech-niques with very good cosmetic effects.10
STATEMENT OF AUTHORSHIP
Category 1(a) Conception and Design
Kyung Soo Kim
(b) Acquisition of DataKyung Soo Kim
(c) Analysis and Interpretation of DataKyung Soo Kim
Category 2(a) Drafting the Manuscript
Kyung Soo Kim(b) Revising It for Intellectual Content
Kyung Soo Kim
Category 3(a) Final Approval of the Completed Manuscript
Kyung Soo Kim
REFERENCES
1. Lin CJ, Lin YS, Kang BH. Middle turbinate osteomapresenting with ipsilateral facial pain, epiphora, andnasal obstruction. Otolaryngol Head Neck Surg.2003;128:282-283.
2. Bignami M, Dallan I, Terranova P, Battaglia P,Miceli S, Castelnuovo P. Frontal sinus osteomas:The window of endonasal endoscopic approach.Rhinology. 2007;45:315-320.
3. Atallah N, Jay MM. Osteomas of the paranasalsinuses. J Laryngol Otol. 1981;95:291-304.
4. Mansour AM, Salti H, Uwaydat S, Dakroub R,Bashshour Z. Ethmoid sinus osteoma presenting asepiphora and orbital cellulitis: Case report and lit-erature review. Surv Ophthalmol. 1999;43:413-426.
5. Seiden AM, Hefny YIE. Endoscopic trephinationfor the removal of frontal sinus osteoma. Otolaryn-gol Head Neck Surg. 1995;112:607-611.
6. Hasegawa T, Hirose T, Sakamoto R, Seki T, Ikata T,Hizawa K. Mechanism of pain in osteoid osteomas:An immunohistochemical study. Histopathology.1993;22:487-491.
7. Ishimaru T. Superior turbinate osteoma: A casereport. Auris Nasus Larynx. 2005;32:291-293.
8. Stammberger H, Wolf G. Headaches and sinus dis-ease: The endoscopic approach. Ann Otol RhinolLaryngol. 1988;97:3-23.
9. Schick B, Steigerwald C, el Rahman el Tahan A, et al.The role of endonasal surgery in the management offrontoethmoidal osteomas. Rhinology. 2001;39:66-70.
10. Huang HM, Liu CH, Lin KN, Chen HAT. Giantethmoid osteoma with orbital extension, a nasoen-doscopic approach using an intranasal drill. Laryn-goscope. 2001;111:430-432.
Fig 3.—The osteoma, measuring 1.2 ¥ 0.9 cm, was completelyremoved by endoscopic sinus surgery.
1154 July/August 2013