Embed Size (px)
Citation preview

From the Women’s Cancers Program at Dana-Farber Cancer Institute
Turning Point
2009
A new drug offerstargeted therapy forcancer patients
Seeking a second line of defenseagainst HER2-positive breast cancer
Blocking the path
The search for the source of serous ovarian cancers:
A medical detective story
GettingPersonal

LE A D E R S H I P
WOMEN’S CANCERS PROGRAM
J. Dirk Iglehart, MD Director, Women’s Cancers Program, Dana-Farber Cancer Institute Chief, Section on Cancer Biology, Brigham and Women’s Hospital
Eric Winer, MDDirector, Breast Oncology Center, Dana-Farber Cancer Institute
Ross Berkowitz, MD Director, Gynecology and Gynecologic Oncology, Brigham and Women’s Hospital and Dana-Farber Cancer Institute
Ursula Matulonis, MDDirector, Gynecologic Oncology, Dana-Farber Cancer Institute
Jay Harris, MDChair, Radiation Oncology, Dana-Farber Cancer Institute and Brigham and Women’s Hospital
Judy Garber, MD, MPHDirector, Dana-Farber Cancer Risk and Prevention Clinic
Myles Brown, MDChief, Division of Molecular and Cellular Oncology, Department of Medical Oncology, Dana-Farber Cancer Institute
Candace S. Lowe, ScDAdministrative Director, Women’s Cancers Program, Dana-Farber Cancer Institute
Susan F. Smith,* Chair
Jane P. Jamieson,* Co-chair
Carie L. Capossela Adler
Mara G. Aspinall*
Norman J. Cantin
Patrick Carney
Sarit S. Catz
Cecilia Chan
Anne E. Columbia
Julia D. Cox
Randi Gilbert Cutler
Charles A. Dana III*
John A. Duffy, Sr.
Mary Schneider Enriquez
Eileen Epstein
Nina Sing Fialkow
Deborah S. First*
Tracey E. Flaherty
Marian L. Heard*
Brian Hodgett
Matina S. Horner, PhD
William S. Karol*
Melissa Chamberlain Leet
David G. Lubrano*
Stacey J. Lucchino
Melanie D. Mace
Ann Punzak Marcus
Vincent M. O’Reilly*
Vivian W. Pinn, MD
Elizabeth M. Pohl
Amy Zarkin Reiner*
Vicki L. Sato, PhD
Judith P. Schlager*
Laurene Meir Sperling
Scott M. Sperling
Micho F. Spring
Beth F. Terrana*
Karen L. Webster*
Gwill E. York
Mariann A. Youniss
*Trustee, Dana-Farber Cancer Institute
2009Contents 1 Overviews
• Women’s Cancers Program• Breast Cancer Program• Gynecologic Cancers Program• Cancer Risk & Prevention Program• Basic Science
6 Ask the Care TeamThe HPV vaccine, biomarkers, and risk factors for uterine cancer
7 Research RoundupExercise and insulin, vulvar cancer, and blocking DNA repair
9 Blocking the PathA second line of defense againstHER2-positive breast cancer
12 A Medical Detective StoryA surprising discovery may lead researchers to the source of serousovarian cancer.
16 Targeted TherapyA new class of drugs known as PARP inhibitors shows promise for treating some breast and ovarian cancers.
19 Survivor SpotlightMary Kenn battles breast cancer with the steady support of her husband; a doctor faces breast cancer, and her fears.
Turning Point is published for supporters
of Dana-Farber’s Women’s Cancers
Program (WCP). To learn more about
the WCP, call Administrative Director
Candace S. Lowe, ScD, at 617-632-2675.
Comments, suggestions, and requests to be added to or deleted from the mailing list may be sent to:
Turning PointDana-Farber Cancer InstituteDepartment of Communications44 Binney Street, OS300Boston, MA 02115
or call 617-632-4090
or e-mail [email protected]
EDITOR: Michael Buller
SCIENCE ADVISORS: Ian Krop, MD, PhD,
Jennifer Ligibel, MD
ART DIRECTOR: John DiGianni
DESIGN: Lee Whale
CONTRIBUTORS: Christine Cleary, Robert Levy,
Pat McAffrey, Debra Bradley Ruder, Saul Wisnia
PRODUCTION: Jacqueline Czel
PHOTOGRAPHY: Sam Ogden
on the cover:New Hampshire native Fermina Hanson is enrolled in an oral chemotherapy study at Dana-Farber.
9
12
VISIT ING COMMITTEE
Turning Point

Dana-FarberWomen’s Cancers Program
J. Dirk Iglehart, MD Through ongoing exploration into the molec-ular underpinnings of breast cancer and
gynecologic cancers, researchers and clinicians atDana-Farber Cancer Institute’s Women’s CancersProgram (WCP), are working together under thedirection of J. Dirk Iglehart, MD, to shed light onthe differences that define the many sub-types ofthese cancers that we now know exist. At the sametime, researchers are looking to leverage thegenetic similarities among different cancers todevelop novel and increasingly effective therapies.One promising example is the discovery of a closegenetic similarity between triple-negative breastcancer and serous ovarian cancer, a very fast-movingtype of ovarian cancer. (See the article on page 12.)
The WCP’s many clinical trials (about 75 areopen at any given time; see www.dana-farber.org/res/clinical/trials) give patients access to the latesttreatments. For researchers and clinicians, thesestudies provide valuable insight into a treatment’seffectiveness. Many trials evaluate treatments priorto surgery and study the vulnerability of a specificcellular process, allowing oncologists to quicklydetermine the effectiveness of a drug or drugcombination and someday make adjustments, if necessary.
WCP physicians and researchers continue to expand our growing knowledge of women’scancers, through their own research and their closecollaborations with colleagues at Harvard MedicalSchool, and with leading institutions around the world. “The WCP hosts several clinical andresearch meetings each year,” says Dr. Iglehart. For example, Dana-Farber is a founding memberof the Translational Breast Cancer Research Consortium, comprised of scientists from 16 academic medical centers around the country. The consortium started as a WCP-funded meetingof clinical researchers from across the country.
“Our physicians also present at and participatein leading national and international conferencesto further the exchange of discoveries.”
For researchers and
clinicians, these studies
provide valuable insight into
a treatment’s effectiveness.

Research in the Breast Cancer Program is progressing on multiple intersecting tracks.
Studies aim to improve the effectiveness of currenttherapies, develop new agents for drug-resistantcancers, identify additional subtypes of tumorsthat respond to targeted treatments, uncover thebiochemical signs of a tumor’s aggressiveness andvulnerability to therapy, and devise new approachesto cancer prevention and supportive care.
Women’s Cancers Program (WCP) investiga-tors are leading and participating in an array ofclinical trials of drugs for HER2-positive breasttumors that have become resistant to drugs such as trastuzumab (known also by the trade name Herceptin). Laboratory research by Dana-Farberscientists suggests that shutting down a proteincalled PI3 kinase – which may be active intrastuzumab-resistant, HER2-positive tumors –can lead to cancer cell death. Institute investiga-tors are studying the safety and effectiveness ofseveral PI3 kinase blockers in patients.
Many research projects are focused on womenwith metastatic breast cancer. WCP investigatorshave launched studies of drugs that may actagainst breast tumor cells that have spread to thebrain, a site of metastasis that represents a partic-ular challenge.
A variety of investigations center on triple-negative breast cancers, so called because theydon’t respond to hormonal treatment or HER2-directed therapy, such as trastuzumab (Herceptin).An approach to drug resistance is being exploredin clinical trials of agents known as PARP inhibitors,which can block the ability of cancer cells tosustain themselves by repairing their own DNA.
Investigators have also widened their focusfrom a concern with cancer cells themselves to aconsideration of the interactions of tumor cells
with surrounding, healthy tissue. WCP investiga-tors have shown that the ability of tumor cells todisrupt the normal development of milk duct cellsenables the tumor cells to escape the ducts andtravel to other parts of the body.
Critical to the success of this work is access totissue from patients. The Lurie Breast CancerTissue and Translation Initiative has enabledDana-Farber investigators to bank blood samplesfrom thousands of breast cancer patients. Thisresource is complemented by the breast tumortissue bank at Brigham and Women’s Hospital.This bank was begun in 2000 using funds fromthe WCP and now houses breast cancer samplesfrom more than 1,400 patients. Tissue stored inthese facilities is used in studies to uncover cancer-related gene mutations or identify proteins in theblood that signal the presence of early cancer.
In late 2008, investigators launched a newstudy that will follow women with metastaticbreast cancer over several years. Over that time,they will be able to obtain serial blood samplesand tumor specimens that will give researchers thevaluable data and tissue needed to help furtherour understanding of the molecular changes thattake place in metastatic breast cancer. The impor-tant study, which is currently enrolling patients, ismade possible because of a generous gift fromKaren Webster and David Evans.
Physicians within the WCP have uncovered sig-nificant disparities in the extent of breast cancertreatment received by women of different racial andethnic groups. Those findings are a starting pointfor studies of the underlying reasons for the dispari-ties, and for efforts to ensure that all patients receiveequally thorough treatment programs. Other studiesfocus on the physical and psychological effects ofbreast cancer treatment in young women.
Dana-Farber Women’s Cancers Program
Breast Cancer Program
Turning Point 2009 www.dana-farber.org2
Eric Winer, MD

The Women’s Cancers Program at Dana-Farber 3
Research into the basicbiology of gynecologic
cancers – including those of theovary, cervix, uterus, and vulva– is bringing into focus an arrayof new approaches to therapy.
Investigators probingovarian cancer are hoping toidentify precursor (precancerous)cells for this particularly chal-lenging disease, so it can bestopped before it develops.Warning signs like bloating,pelvic/abdominal pain, and
urinary urgency or frequencyusually don’t emerge until cancerous tumors have grownor spread. At this advancedstage, the disease can be verydifficult to treat successfully.
In one project under way at the Dana-Farber/Brighamand Women’s Cancer Center(DF/BWCC), researchers led by Christopher Crum, MD,have shown that some ovariantumors initially arise in the fallopian tubes and secondarilyspread to the ovaries and peri-
toneum. This remarkable resultwas proven by tracking a singlemutation in a gene called p53from the earliest cells in the fallopian tube to advancedcancer in the pelvis. If over -expression of this gene turnsout to be a direct link toovarian cancer, there is a chancethe disease could be detected –and thwarted – much earlieron. (For a detailed story on thep53 mutation, see page 12.)
“We need to find somekind of definite precursor forovarian cancer, like polyps are for colon cancer or DCIS(ductal carcinoma in situ, a pre-cancerous condition in whichabnormal cells grow in the milkducts) has become for breastcancer,” says Ursula Matulonis,MD, director of GynecologicMedical Oncology for Dana-Farber’s Women’s CancersProgram. “If you find and stopthe source, you can better stopthe cancer. I’m confident that’swhere we’re headed.”
In another effort, for whichDana-Farber received a BreastCancer Research Foundationgrant last year, DF/BWCCphysicians including Dr. Matu-lonis, Ross Berkowitz, MD, andCharles Wang, MD, PhD, arecomparing the genetic makeupof triple-negative breast cancer (aparticularly aggressive form) andovarian cancer. Their work is
part of an attempt to understandthe molecular similarities anddissimilarities between these twodiseases, which are both very sen-sitive to platinum-based drugsoften used for cancer treatment.
Beyond ovarianAnother area of increasing
interest is uterine cancer – thefastest-growing gynecologicalcancer in the United States,with about 40,000 new caseseach year. Obesity can drive up estrogen levels in the blood,which in turn can fuel endome-trial growth and raise the risk ofuterine cancer. One promisingstudy is being led by HeidiGreulich, PhD, of Dana-Farberand the Broad Institute ofHarvard and MIT, who isinvestigating the geneticmakeup of endometrial cancer.
On the cervical cancerfront, Dorre Gruenberg, PhD,of Harvard Medical School andthe Broad Institute is leadinginvestigations into the role aparticular kinase (an enzymethat serves as a switch forgenetic activity) may play intumor cell growth. And invulvar cancer, Neil Horowitz,MD, is heading up a promisingclinical trial studying how adeadly abnormal gene known asEGFR (epidermal growth factorreceptor) can be stopped withmolecularly-targeted therapies.
Dana-Farber Women’s Cancers Program
Gynecologic Cancers Program
Ursula Matulonis, MD
If you find and stop the
source, you can better stop the
cancer. I’m confident that’s
where we’re headed.
“
”

Dana-Farber Women’s Cancers Program
Cancer Risk and Prevention Program
Just as the role of genetics in determining cancerrisk has become more widely understood in
recent years, so too has Dana-Farber widened itsknowledge – and its services to help a growingnumber of people assess and manage their risk ofpassing down or developing the disease.
When the Friends of Dana-Farber Cancer Riskand Prevention Clinic (CRPC) first opened itsdoors, there was one medical oncologist and onegenetic counselor on staff. The clinic saw about 400patients and family members that year. Under theleadership of Director Judy Garber, MD, MPH, theCRPC has expanded to include four physicians andseven genetic counselors who last year offered per-sonal risk assessment, genetic counseling, screeningevaluations, and strategies to reduce cancer risk toapproximately 1,500 patients and families.
The clinic now offers a full range of services atboth its main facility in Boston’s Longwood Medical
area as well as at satellite centers at Faulkner Hospitalin Jamaica Plain and at new centers in Milford,Mass., and in Londonderry, N.H.
The CPRC’s impact is also measured in ourgrowing understanding of women’s risk of devel-oping ovarian and breast cancer, and the preven-tion and treatment strategies associated with each.
“It’s one thing to talk with people about theirrisk, and it’s another thing to try to help them dealwith it,” says Dr. Garber. “We don’t just do theassessment. We follow these patients. We managethem. We care for them, and for their families.”
While all women are at risk, women with afamily history of breast cancer in close relatives ofyoung ages have a greater probability of developingone or both diseases over their lifetimes. About 10 percent of breast cancers are hereditary, and, ofthese, mutations in two genes, BRCA1 and BRCA2,are responsible for approximately 40 percent of thediagnoses. Women who have alterations in eitherof these genes have a lifetime risk of developingbreast cancers between 55 percent to 85 percent, anda similar risk of developing a deadly ovariancancer. With this understanding, the Risk andPrevention Clinic can tailor strategies to helpwomen manage that risk.
Multiple studies at the clinic are examiningways to reduce both the threat of breast cancer inhigher-risk women and the complex psychosocialissues related to harboring a susceptibility gene and undergoing genetic testing. One large studyinvolves a drug known as a PARP inhibitor, whichhas been shown to prevent mammary tumors inmice without functional BRCA1 or BRCA2 genes.While it is important that these agents first befully evaluated for safety in breast cancer patients,the findings suggest that PARP inhibitors couldform the basis for effective prevention strategies forwomen with inherited breast cancer risk. Additionalresearch is also studying the potential of PARPinhibitors in treating women with advancedovarian cancer. (See article on page 16.)
Dr. Garber and others at the center are alsoworking with Dana-Farber colleague JenniferLigibel, MD, to examine the effects of exercise onreducing cancer risk. (See article on page 7.)
Looking even further into the future, Dr. Garber can envision a day when a breastcancer gene test will screen for a larger percentageof diseases, help identify at-risk women, and guidecancer prevention strategies. Dr. Garber says,“This is true of heart disease already, and, in manyways, it’s what you hope for in cancer.”
www.dana-farber.orgTurning Point 2009 www.dana-farber.org4
Judy Garber, MD
We don’t just do the assessment. We
follow these patients. We manage them.
We care for them, and for their families.
“”

Vulnerability, or the theory that all cancer cells have at least one weakness, is a concept
embraced by much of the cancer research field.This theory holds that you beat cancer by findingthe molecular Achilles’ heel of particular cancercells and designing drugs that interfere with thisparticularly vulnerable spot. This approach is justone of the ways in which Dana-Farber scientistsare pursuing a multi-front attack on women’scancers. Increasingly, that battle focuses on thecomplex interactions within specific types oftumor cells that allow them to proliferate andsometimes spread to other areas of the body.
The use of the drug trastuzumab (Herceptin)to treat women with HER2-positive breast cancer,for example, has significantly improved the livesof many patients. But in time, the tumors of somepatients become resistant to the drug. Scientistsbelieve that the PI3 kinase plays a critical role inthis process. Like all kinases, the PI3 kinase acts asa switch box in the cell’s communication network.In these trastuzumab-resistant tumors, PI3 kinasemay provide an alternate pathway that allowstumor cells to survive. A Women’s Cancers Program(WCP) clinical trial, headed by Ian Krop, MD,PhD, is studying the effectiveness of a PI3-kinaseinhibitor in shutting down the pathway. (See thearticle on page 16.)
The article on page 12 provides anotherexample of our growing understanding of thegenetic underpinnings of cancer. That story detailsthe findings of Christopher Crum, MD – thatmany serous ovarian cancers may actually begin
in the fallopian tube rather than the ovary – andthe work of other WCP researchers to confirm his findings.
From discoveries of the mechanisms of DNArepair and drug resistance, to the search for bio-markers that aid in early detection of the disease, togene mutations that raise the risk of developingcancer, research from the WCP continues toadvance our understanding of the fundamentalprocesses within tumor cells, and lead us towardmore effective and less toxic treatments for breastand gynecologic cancer patients.
Dana-Farber Women’s Cancers Program
Basic Science
J. Dirk Iglehart, MD
The use of the drug trastuzumab to treat women with HER2-positive breast cancer,
for example, has significantly improved the lives of many patients.
The Women’s Cancers Program at Dana-Farber 5

Ask the Care Team
approved for assessing the response to initial chemotherapyfollowing diagnosis.
CA125, discovered at Dana-Farber/Brigham andWomen’s Cancer Center, is the most studied and widelyused ovarian cancer biomarker. Although it plays a majorrole in monitoring patients, CA125 alone is not good forearly detection because it can be triggered by numerousbenign conditions.
Ongoing studies are trying to address the use of HE4 asa new tool to help doctors determine the most appropriatecourse of care for women with a pelvic mass, and as a bio-marker for early detection of the cancer.
What is uterine cancer and what are the risk
factors for uterine cancer?
Uterine cancer is a malignancy that develops in thelining of the uterus, in the hormone sensitive tissues thatnourish a newly implanted embryo and that slough offmonthly during the menstrual cycle. This tissue is called theendometrium, and the cancer may be called “endometrialcancer.” Uterine cancer typically presents itself as abnormalvaginal bleeding or spotting when it is small, and as anenlargement of the uterus when it is advanced. It is diag-nosed by an endometrial biopsy, done in the office, or by adilation and curretage (“D and C”) in the hospital. It istreated by surgery (hysterectomy), sometimes with radiation,and sometimes with hormones and chemotherapy.
Risk factors for uterine cancer are both genetic (inherited)and non-genetic, and in the categories of lifestyle and envi-ronmental factors. Inherited deficiencies in a class of DNArepair enzymes called “mismatch repair” enzymes can causegastrointestinal cancers (e.g., colon and stomach) and cancerof the uterus. Taking estrogen without taking progesteroneafter menopause is a risk factor for uterine cancer, and thereason why all “hormone replacements” are given as combi-nations of estrogen and progesterone unless a woman haspreviously undergone a hysterectomy. Finally, obesity andlack of exercise seem to put post-menopausal women at riskfor uterine cancer, probably by increasing the exposure toestrogen without the benefit of progesterone.
What is the HPV vaccine? Who should receive it?
And what are the associated side effects?
The vaccine for HPV (or human papilloma virus) ishighly effective in preventing infection in women who havenot previously been infected with two particular viruses –called HPV 16 and 18 – covered by the vaccine. However,there are several other HPV subtypes that are not covered by the current vaccine. It does not prevent the majority ofinfections and abnormal growths caused by these otherviruses, nor does it protect patients who have already beeninfected with HPV 16 or 18. We also don’t know for howlong women who receive the vaccine will be protected.
The main side effect is pain at the injection site andthere have been some news reports about other serious sideeffects. There is a system for reporting adverse events, and to our knowledge those other complications have not beenconfirmed as being caused by the vaccine.
The vaccine does not change the recommendations for having a routine Pap test. The HPV vaccine protectsagainst only two of 13 high-risk viral subtypes, but evenwith those two types, it cannot prevent further conse-quences of pre-existing infections. A Pap test is a screeningtest that looks for cellular changes associated with HPVinfection. Pap testing remains the best method for detectingprecancerous changes. All women should continue followingstandard screening practices. Otherwise, their risk of cer-vical cancer could actually rise. Ultimately, a combinationof an expanded vaccine and more specific viral testing maychange how we screen for cervical cancer, but we’re notthere yet.
What are biomarkers and how are they affecting
diagnosis and treatment of ovarian cancer?
A biomarker is a biochemical feature, usually a protein ina biological fluid (blood, serum, urine, saliva) that can be usedto measure the progress of disease or the effects of treatment.
There are two FDA-approved biomarker tests (bothblood tests) for ovarian cancer: CA125 and HE4. Both are
Turning Point 2009 www.dana-farber.org6

Exercise shown to lower insulin in breast cancer survivors
Through observational studies,doctors and scientists have known thatwomen who engage in even a modestamount of physical activity after breastcancer diagnosis appear to have a lowerrisk of cancer recurrence than inactivepatients. Now, a randomized clinicaltrial led by Jennifer Ligibel, MD, ofDana-Farber’s Breast Oncology Center,suggests that the protective effect ofincreased fitness may result from lowering insulin levels in the body.
A report published in the February2008 issue of the Journal of ClinicalOncology, showed that moderate exercise such as walking, along withsupervised strength training sessions,led to a 30 percent decrease in levels ofinsulin in previously sedentary breastcancer survivors.
“While other types of studies are based on the composition of thetumor, our research is a little differentbecause we focus on the characteristicsof the [patient],” Dr. Ligibel pointsout. “We ask which factors, such asinactivity, set the stage for breast cancerto thrive or come back.”
No one knows if increased fitnesswill prevent breast cancer recurrence,but the women improved their overallhealth. Dr. Ligibel and her colleagueslearned the value of a supervised exer-cise program: “Fitness is all aboutmotivation,” she says. “Women aremore likely to exercise when enrolledin a program with frequent check-ins.”
The study lays the groundwork for further experiments. Dr. Ligibel is leading several other trials at Dana-Farber related to exercise and breastcancer. One trial looks at the potentialbenefits of exercise in women livingwith metastatic breast cancer. Another
trial is evaluating the ability of a telephone-based exercise program toincrease physical activity in survivors ofbreast or colorectal cancer. “Our hopeis that one day, our ongoing researchwill shed more light on the value ofexercise as a standard component inbreast cancer treatment,” she says.
WCP Research Roundup
The Women’s Cancers Program at Dana-Farber 7
At Dana-Farber, there are hundredsof research studies going on as investi-gators attempt to better understand thediseases. You can learn about clinicaltrials through Dana-Farber’s Web siteat www.dana-farber.org/res/clinical, whichlists all open trials by diagnosis, or bycalling 866-790-4500. All Dana-Farbertrials are open to current patients orthose thinking about coming to theInstitute.
Some studies allow individuals whohave not been diagnosed with cancerto participate. Healthy volunteers mayserve as a comparison group in studyinghow chemotherapy and other treatmentsaffect the body.
Finding openclinical trials
Fitness is all about motivation,” says Dr. Ligibel.
“Women are more likely to exercise when enrolled in a
program with frequent check-ins.
“”

Turning Point 2009 www.dana-farber.org8
If Neil Horowitz, MD, wantsextra motivation to continue the work on vulvar cancer that he and his colleagues at Dana-Farber/Brighamand Women’s Cancer Center areundertaking, he need look no furtherthan his e-mail inbox. Every month,Dr. Horowitz gets e-mails from peopleall over the world interested in joiningclinical trials for this relatively raredisease, which is diagnosed in only3,000 patients each year in the U.S.
Cancer of the vulva, the outer partof a woman’s genital organs, typicallypresents with signs like itching, tender-ness, and non-menstrual bleeding. Fortunately, it is often diagnosed whenstill confined to the vulva, in whichcase it carries a five-year survival rate of
90 percent. However, in three out ofevery 10 cases, the cancer can spread tothe lymph nodes. When this happens,survival drops to 50-60 percent. Insuch cases, recurrence rates are highand survival after recurrence is poor.
Clinical trials led by Dr. Horowitzand others are aimed at thwartingvulvar cancer by suppressing the genesand proteins responsible for it. “Ourearly response rate has been veryencouraging,” he says of one studynow underway at Dana-Farber. “Agenetic fingerprint called EGFR [epidermal growth factor receptor] isheightened in many vulvar cancerpatients, and we’re hoping that givingthem a drug called Tarceva, or erlotnib,can block the receptor and its down-
stream growth signals to shrinkexisting tumors. This is especiallyencouraging for patients with recurrentdisease who have few options for treat-ment, or for those in whom radicalsurgery can be disfiguring and nega-tively impact bodily function.”
Dr. Horowitz says two groupsaccount for most vulvar cancer cases:younger women who smoke and havethe human papilloma virus (HPV),and older women who have a longhistory of chronic vulvar irritation.The key will be uncovering whichgroup or subset therein best respondsto Tarceva, and then targeting it tothem. The drug has already proveneffective in treating some advancedsmall-cell lung cancer patients.
Genes may hold vulvar cancer clues
WCP Research Roundup
Along with surgery and chemotherapy, radiation therapyhas been a mainstay of cancer treatment almost since X-rayswere discovered in 1895. High-energy beams of radiationattack rapidly dividing – and therefore vulnerable – cancercells by scrambling their DNA blueprints, halting theirgrowth, and shrinking the tumor.
Technology has continuously improved so that higherdoses of radiation can be delivered more accurately, hittingcancers harder while sparing normal tissues. At the sametime, scientists in Dana-Farber’s Department of RadiationOncology are exploiting defects in cancer cells’ defenses –weakening their ability to repair DNA damage so tumorscan’t rebound after being treated with radiation therapy.
“Tumors become resistant by repairing the DNA damage totheir cells,” explains Dana-Farber’s Alan D’Andrea, MD. Therepair work is done by turning on one or more of six differentmolecular pathways that specialize in repairing damaged DNA.“If you can determine which pathways are active in a patient’stumor, you can predict its sensitivity to particular types of radi-ation or chemotherapy,” Dr. D’Andrea says. Research suggeststhat it may be possible to “throw a wrench” into the repairmechanisms and prevent the tumor from healing itself.
Dr. D’Andrea heads the Division of Genome Stabilityand DNA Repair within the Department of Radiation
Oncology, which is developing various methods to pinpointwhich DNA repair pathways are active in a patient’s tumor.
These “snapshots” of pathway activity help guide therapy.In many cases, cancer cells shut down a major repair pathway sothat they are more prone to mutation and can evolve resistanceto therapies more rapidly. The trade-off is that they becomemore dependent on other pathways. If scientists can knock outone of the remaining dominant repair pathway, radiation orchemotherapy has a greater chance of striking a lethal blow.
Dana-Farber’s Larissa Lee, MD, and collaborators at BethIsrael Deaconess Medical Center are studying a database thatincludes information on the outcomes of treated breast cancerpatients, along with data on molecular studies of their tumortissue. Some of those tissue samples have been “profiled” toidentify the most active DNA repair pathways in the tumor.
“We want to match the profiles with patients who’ve donewell for a long time, and those who have had recurrences, to seeif these biomarkers (indications of repair pathway activity) canpredict who is more likely to have a recurrence,” says Dr. Lee.
Jay Harris, MD, chair of the Dana-Farber Departmentof Radiation Oncology, says, “This research may openopportunities to tweak DNA repair pathways in a way thatenhances the effect of radiation therapy, increasing the kill of tumor cells as well as protecting normal tissues.”
Targeting a tumor’s repair mechanism

The Women’s Cancers Program at Dana-Farber 9
In about 20 percent of breast cancer cases, the tumor cellshave an oversupply of a protein called HER2. For womenwith such “HER2-positive” tumors, trastuzumab can literallybe a lifesaver. By binding to HER2, the drug prevents itfrom transmitting growth signals into the cell, slowing orreversing tumor growth. Combined with chemotherapy, thedrug shrinks or controls tumors in 75-80 percent of womenwith HER2-positive metastatic breast cancer.
Even in these patients, however, the benefits of trastuzumabare far from permanent. Patients with the most advanceddisease generally have a 10- to 14-month period in whichtheir condition improves or stays stable, after which it begins to worsen, although some patients do well for many years.
“It’s as though HER2-positive cancers are speeding downa highway. Trastuzumab cuts them off for a while, but thetumors have a way of finding off-ramps that enable them to get
around the blockade,” says Eric Winer, MD, director of theBreast Oncology Center within Dana-Farber’s Women’s CancersProgram (WCP). “There’s a growing scientific and clinicalconsensus that even when the cancer progresses, Herceptin isstill providing a benefit, so the drug resistance is only partial.
“We’re beginning to understand what’s taking place at amolecular level to enable these tumors to escape the full effectof the drug,” he continues. “What’s exciting is that there area host of drugs in preliminary clinical trials that appear tohave very clear activity against Herceptin-resistant cancers.”(See box on page 11 for a brief description of these studies.)
Molecular maneuversScientists have discovered that when HER2-positive
breast cancer cells become resistant to trastuzumab, proteinscalled PI3 kinases become activated within the cells. The
Able to lock onto a key protein on the surface of some breast cancer cells, the drug
trastuzumab (Herceptin) heralded a new generation of “targeted” therapies when it
received federal approval in 1998. Unfortunately, cancer is often a moving target.
A second line of defense againstHER2-positive breast cancer
Blocking the Path by Robert Levy
Research led by Thomas Roberts,PhD, and Jean Zhao, PhD, suggests that some patients could benefit from drugs thatblock PI3 kinases.

In about 20 percent of breast cancer cases, the tumor cellshave an oversupply of a protein called HER2. For womenwith such “HER2-positive” tumors, trastuzumab can literallybe a lifesaver. By binding to HER2, the drug prevents itfrom transmitting growth signals into the cell, slowing orreversing tumor growth. Combined with chemotherapy, thedrug shrinks or controls tumors in 75-80 percent of womenwith HER2-positive metastatic breast cancer.
Even in these patients, however, the benefits of trastuzumabare far from permanent. Patients with the most advanceddisease generally have a 10- to 14-month period in whichtheir condition improves or stays stable, after which it begins to worsen, although some patients do well for many years.
“It’s as though HER2-positive cancers are speeding downa highway. Trastuzumab cuts them off for a while, but thetumors have a way of finding off-ramps that enable them to getaround the blockade,” says Eric Winer, MD, director of theBreast Oncology Center within Dana-Farber’s Women’s CancersProgram (WCP). “There’s a growing scientific and clinicalconsensus that even when the cancer progresses, Herceptin isstill providing a benefit, so the drug resistance is only partial.
“We’re beginning to understand what’s taking place at amolecular level to enable these tumors to escape the full effectof the drug,” he continues. “What’s exciting is that there area host of drugs in preliminary clinical trials that appear tohave very clear activity against Herceptin-resistant cancers.”(See box on page 11 for a brief description of these studies.)
Molecular maneuversScientists have discovered that when HER2-positive
breast cancer cells become resistant to trastuzumab, proteinscalled PI3 kinases become activated within the cells. Thekinases are a family of enzymes – proteins that spark chemicalreactions – first studied by Thomas Roberts, PhD, co-chairof Dana-Farber’s Department of Cancer Biology, and LewisCantley, PhD, of Beth Israel Deaconess Medical Center anda member of the Dana-Farber/Harvard Cancer Center.
The PI3 kinases usually take their cues from the HER2protein. HER2 is a “receptor” that juts from the cell surfacelike a catcher’s mitt waiting for a growth molecule. The “grow”command is passed along a chain of proteins, including PI3kinases, to the cell’s central command. When HER2 is shutdown by trastuzumab, abnormal PI3 kinases can sometimes
Clinical trials for new HER2-positive
breast cancer therapies
Turning Point 2009 www.dana-farber.org10
The success, and limitations,of trastuzumab for HER2-positive breast cancer haveinspired the creation of a seriesof novel drugs. Investigatorsin the Women’s CancersProgram (WCP) are leading oroffering clinical trials of fiveclasses of these new therapies.They include:
• Agents similar to the drug lapatinib (brand nameTykerb) that latches onto a different portion of theHER2 receptor than does trastuzumab.
• A compound known as TDM1 that hitches achemotherapy agent to a specific antibody. Bygravitating toward HER2-positive breast cancercells, the antibody makes a “special delivery” ofchemotherapy directly to them.
• Agents that block or inhibit a protein known asHSP90. HSP90 is a “chaperone” protein thatenables the HER2 receptor to function better.Inhibiting HSP90 offers a promising, if indirect, way to disable HER2.
• Angiogenesis inhibitors that may block the growthof blood vessels that help feed tumors the nutrientsthey need to grow.
Finally, studies are planned with pertuzimab, a “mono-clonal” antibody (an antibody duplicated millions of timesover) that prevents the HER2 receptor from joining to itssister receptors HER1 and HER3. Without such a connec-tion, HER2 cannot activate cell growth.
“In cases of advanced HER2-positive breast cancer,these potential therapies may provide great hope forwomen whose cancer is resistant to trastuzumab,” says Eric Winer, MD, director of the Breast OncologyCenter within the WCP. “For women with early breasttumors, they may offer an increased number of options ifthe disease progresses.”
Eric Winer, MD

To learn whether breast cancers leave telltale signs of themselves in the bloodstream, researchers need toexamine samples of tumor tissue – several thousand of them, ideally.
Ian Krop, MD, PhD, and Deborah Dillon, MD, of Dana-Farber/Brigham and Women’s Cancer Center are workingto create just such a repository for Women’s CancersProgram scientists. With tumor tissue from current andformer breast cancer patients, the bank will assist thesearch for cancer biomarkers – proteins and other sub-stances in the blood that can reveal whether a tumorhas formed and whether a therapy is effective.
Researchers will be able to divide the samples into
distinct categories to identify biomarkers associated witheach type. “We’d like to study reasonably uniform cohortsof patients who have received similar treatments,” saysDr. Krop. “By examining large numbers of samples, wecan have confidence that our findings will be broadlyapplicable to each group of patients.”
The project involves a sizable commitment of effortand funds. Systems need to be put in place for collectingtumor tissue shortly after surgical removal, preserving it,staining it to show possible biomarkers, and cross-linkingthe data with patients’ medical history. The rewards, bothin terms of improved tumor detection and more rapiddevelopment of treatments, promise to be substantial.
Cancer tissue sampleshelp WCP researchersin their search forbiomarkers.
get activated, transmitting growthsignals on their own. The result, in atumor, is a resurgence of cell division.
Dr. Roberts and his colleague JeanZhao, PhD, have developed colonies ofHER2-positive cells whose growth is hobbled by trastuzumab. When theyinserted a defective, or mutated,version of a PI3 kinase, the cells becametrastuzumab-resistant. “Mutations toPI3 kinases may explain why somepatients with HER2-positive cancersdon’t respond to trastuzumab, and whypatients who initially respond to thedrug eventually relapse,” Dr. Roberts
comments.The discovery suggests that some
patients could benefit from drugs thatblock PI3 kinases. Dana-Farber’s Geof-frey Shapiro, MD, PhD, is leading aclinical trial of such drugs; the secondround of trials will test the drugsspecifically in trastuzumab-resistantbreast cancers.
The insulin issueDeveloping a second line of defense
against HER2-positive tumors isunlikely to be straightforward. The PI3kinases are involved with many cellular
processes, not just HER2. One ofthose is the receptor for insulin, aprotein used by the body to burnsugar. In studies with mice, Dr. Zhaofound that PI3 kinase inhibitors causeinsulin levels in the blood to rise. “It’snot yet clear whether this poses aproblem, but we’ll need to pay atten-tion to it as we go forward,” she says.
Dr. Zhao and her colleagues areexploring whether PI3 kinaseinhibitors can be developed that areeffective against trastuzumab-resistanttumors but don’t drive up insulinamounts so sharply. They’re intrigued
The Women’s Cancers Program at Dana-Farber 11
A project to bank on
pI3K PI3K
Insulin or growth factors
HER2 HER2
trastuzumab(Herceptin)
HER2 amplificationCell membrane
Tumor Cell Growth
PI3K
Tumor Cell Growth
PI3KPI3KInhibitors
umpt
PI3K
minman)
babbb
Blockage of Tumor Cell Growth
Blockage of Tumor Cell Growth
Normal Cell Growth
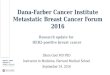
Blocking Trastuzumab-Resistant Tumor Growth
Illus
trat
ion
by J
ohn
DiG
iann
i
In normal breast cells, growthfactors lodge in HER2 receptorson the cell surface. Signalspass from the receptorsthrough a series of proteinsincluding PI3 kinase, whichspurs cell growth and division.
In HER2-positive breastcancers, a surplus ofHER2 receptors pushescell growth into over-drive, leading to tumorformation.
By blocking the HER2receptors, the drugtrastuzumab (Herceptin)can short-circuit tumorgrowth.
If PI3 kinase is overactivat-ed, it can begin sendingtumor growth signals on itsown, without promptingfrom HER2. Such cancersno longer respond well totrastuzumab.
Agents that block defective PI3 kinaseshow promise of halting tumor cell growth intrastuzumab-resistantcancers.

Atop every list of how to deal with cancer is the importance of early detection. Regular
screenings – self exams and those conducted by clinicians – are the surest way of detecting
tumors in their initial stages, when they’re easiest to treat.
For nearly every type of cancer, that advice is perfectlysound. Cancer is like a brush fire, best stamped out or contained when it first forms, before it has a chance to spread.
But there are some cancers that don’t have a knownformative stage, that seem to burst onto the scene in anadvanced, malignant state, having already overrun a wideswath of tissue. Such tumors are notoriously difficult to treat, their sudden emergence a sign of their ferocity.
One of the most common of these tumors is known asserous ovarian cancer. Less than a quarter of the cases aredetected at an early stage, a figure reflected in the survivalrates for the disease.
Serous cancers occur on the surface of the ovaries andsurrounding membranes, often in several places, makingthem impossible to eliminate by surgery alone. The intro-duction of drugs like platinum and taxanes have lengthenedthe survival of many patients, but cure rates have not substan-tially improved.
“When these cancers are diagnosed they seem to beeverywhere at once,” says Ronny Drapkin, MD, PhD, of Dana-Farber’s Women’s Cancers Program (WCP), who isleading some of the research into the tumors’ origins. “Theirdiscovery at an advanced state of development limits ourability to treat them effectively. That’s why it’s so importantto identify ‘precursor’ cells from which the tumors arise.”
Cancer, in a nutshellOver the course of modern cancer research, scientists
have mapped out what might be called “The Genesis of aCancer,” the step-by-step process by which some tumorsform in the lining – or “epithelial” layer – of tissues andorgans. It begins with a completely normal cell, anywhere inthe body, whose DNA is damaged by exposure to a chemical,radiation, or the normal stresses of life. The cell then mayrepair the damage or kill itself to prevent the defect frombeing passed on to its offspring. If the damage is not repairedand occurs in a gene responsible for cell growth and division,the cell may be a cancer precursor, behaving oddly in one ortwo respects, but not immediately dangerous. Only after itacquires additional damage, or genetic mutations, does itacquire the classic characteristics of cancer – proliferation,burrowing into tissue, siphoning blood and nutrients fromother cells, refusing to die on time, and demonstrating anability to spread to other parts of the body.
This process means that scientists should be able to iden-tify a continuum for the development of virtually any tumorthey come across – the normal tissue where it originated, thequirky precursor cells that follow, the invasive and restless cellsthat mark it as cancer. In the case of high-grade serous ovariancancer, however, the trail has been cold: for years, scientistscouldn’t find a trace of the cells that preceded full-blown tumors.
“We had to ask ourselves whether this disease is a
Turning Point 2009 www.dana-farber.org12
The search
for the source
of serous
ovarian cancers:a medical
by Robert Levy

The Women’s Cancers Program at Dana-Farber 13
detective story
Ronny Drapkin, MD, PhD, and his team direct the“living” bank of ovarian tumor tissue at Dana-Farber.

fundamentally different entity from other types of cancer, orwhether we had been looking for precursor cells in the wrongplace all along,” says Christopher Crum, MD, director ofwomen’s and perinatal pathology at Dana-Farber/Brighamand Women’s Cancer Center (DF/BWCC), who sought tounravel the mystery of the condition’s origins.
‘Carpetbagger’ cancersA key clue lay outside the ovaries themselves. The
fallopian tubes, the narrow chutes that carry fertilized eggs to the uterus, also can be the site of origin of serous cancers.Can advanced serous cancers of the ovary actually be decoys– the result of cancer cells that left the fallopian tubes andsettled in the ovary?
The evidence is pointing in that direction. First, theovary and fallopian tubes are next-door neighbors – thebroad end of the fallopian tube cupping the ovary in finger-like strands called fimbria – so cancer cells don’t have totravel far to go from one to the other. Second, ovarian andfallopian tube cancer cells look identical under a pathologist’smicroscope and behave quite similarly.
If high-grade serous ovarian cancers (HGSOCs) are infact masquerading fallopian tube tumors, then women diag-nosed with HGSOC would be likely to have cancerouslesions, or sections of diseased tissue, on their tubes. Tradi-tionally, however, pathologists haven’t examined the entirefallopian tube, concentrating on the more accessible centralsection of the tube.
In 2005, Dr. Crum and his colleagues developed aspecial technique for inspecting the “fimbriated” end of fal-lopian tubes – the portion, adjacent to the ovaries, withslender tendrils like the top of a sea anemone. Using thistechnique, called SEE-FIM (for “Sectioning and ExtensivelyExamining the Fimbriated end”), they conducted a top-to-bottom exam of fallopian tubes that had been removed as apreventive measure from women with an inherited risk forovarian cancer.
In a succession of studies, Dr. Crum’s team found thatsome of the tubes harbored early cancers, almost always inthe fimbriated end, the end closest to the ovary. “This wasstrong evidence that the source of many serous carcinomas in
the pelvic region, including the ovary, is the fimbriated – or‘distal’ – end of the fallopian tube,” Dr. Crum says. “Theseare tumors that seem to grow best outside their birthplace.”
The evidence may have been strong, but it wasn’t yetdefinitive. Then, in 2006, Dana-Farber’s Alexander Miron,PhD, used advanced gene-sequencing technology to showthat the early cancers in the fallopian tube had the samegenetic mutations as the tumors elsewhere in the pelvis.
In search of precursorsHaving found the fallopian tubes to be the “nursery” of
many high-grade serous ovarian cancers, researchers couldfocus on their ultimate quarry, figuring out how and wherenormal cells become precancer and then cancer.
Here, a surprise was in store. Studies had shown thatearly cancers in the lining of the fallopian tube contain highlevels of a protein called p53. The accumulation of the protein,caused by a breakdown in the p53 gene, was dubbed “thep53 signature.” When Dana-Farber and Brigham and Women’s
That was the ‘Wow’ moment,” said Dr. Crum. “We now had a marker for these
types of serous cancers and a pathway by which they develop.
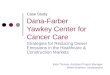
A Model of High-Grade Serous Ovarian Cancer
Evidence assembled by Women’s Cancers Program scientists suggests that many ovarian cancers originate in the finger-likeends of the fallopian tubes.
Illus
trat
ion
by L
ee W
hale
“ ”
Turning Point 2009 www.dana-farber.org14

researchers tested normal-looking fallopian tissues, theyfound that about half the samples also had the p53 signature.
“That was the ‘Wow’ moment,” Dr. Crum says. “Wenow had a marker for these types of serous cancers and apathway by which they develop: normal cells acquire muta-tions in the p53 gene, further mutations produce cancerswithin the fimbrial tissue of the fallopian tube, and thecancers migrate to the ovary.”
The discovery doesn’t imply that every woman whosefallopian tubes carry the p53 signature will develop serouscancers: in fact, only a small percentage of them will. But ithas enabled scientists to construct a narrative about how suchcancers arise and spread, and how they might be stopped.
Every month when women are menstruating, an eggpops out of an ovary in what has been described as a “miniexplosion.” The tear in the ovary is mended by a blend ofhormones and other proteins from the immune system. Onrare occasions, this fix-it crew may inadvertently meddle withthe DNA in nearby cells, such as those in the fimbriatedends of the fallopian tubes. One gene that’s susceptible tosuch changes is p53, whose job is to repair damaged DNA. Amutation can render the p53 protein useless, leaving the cellvulnerable to further mutations that could make it cancerous.The mutation also causes p53 to loiter too long within thecell – hence the p53 signature in precancerous cells.
“The p53 signature is like a sign telling us that the cell’sself-repair system is down,” Dr. Crum says. If this theory iscorrect, then women who have fewer children and have chil-dren at an older age – and thereby have a higher lifetimenumber of menstrual cycles – would be more likely todevelop precancerous cells. Research by Dr. Crum, in associ-ation with Judy Garber, MD, MPH, director of the Friendsof Dana-Farber Cancer Risk and Prevention Clinic, andShelley Tworoger, PhD, an epidemiologist at Brigham andWomen’s Hospital (BWH), found this to be the case.
As for why serous cancers often take root in the ovaryrather than their “native soil” in the fallopian tube, scientistsspeculate that the ovarian terrain is somehow more hospitablefor the fledgling tumor cells.
Future directionsKnowing the ultimate source of many serous ovarian
tumors raises some intriguing possibilities for treatment.Understanding how precancerous cells become cancerous
may suggest ways of disrupting the process before malignan-cies develop. Being able to detect cancers in their earlieststages – or identify tissue where tumors are likely to form –could dramatically raise survival rates for the disease.
WCP researchers have assembled a team with theexpertise to reach those goals. The team includes Dr.Drapkin and his colleagues who are developing modelsystems of fallopian tube cells and their precancerous descen-dents; Dr. Miron, who conducts genetic analyses of cell andtissue samples; Dr. Crum, who heads the pathology efforts;Dr. Garber, who studies cancer risk factors; Tan Ince, MD,PhD, of BWH, who directs a live cell bank; Ross Berkowitz,MD, director of Gynecology and Gynecologic Oncology atBWH and Dana-Farber, Ursula Matulonis, MD, director ofGynecologic Medical Oncology at Dana-Farber, and MichaelMuto, MD, and Colleen Feltmate, MD, of the GynecologicOncology program at DF/BWCC, who treat patients andlead clinical trials of new therapies.
“The pieces are in place, both technological and scientific,to get a handle on the development of serous cancers of theovary, and to use those abilities to design and test more effectivetreatments,” Dr. Drapkin remarks. “We’re in a position to bringtreatment of this disease into the age of targeted therapies.”
A discovery by Christopher Crum, MD, and his colleagues offers insight into how serous cancers arise and spread, and how they might be stopped.
The Women’s Cancers Program at Dana-Farber 15

Turning Point 2009 www.dana-farber.org16
When Fermina Hanson needed to have chemotherapy and radiation for her breast cancer,
one side effect really got her down. It wasn’t the nausea or fatigue, although both were
debilitating. The thing she remembers most was the psychological impact of losing her long,
dark hair. “It was traumatic, and a real struggle,” Hanson recalls.
Fermina Hanson, at homehere in New Hampshire,has been taking a new, targeted therapy to treather breast cancer. Inset isher Dana-Farber oncologist,Harold Burstein, MD, PhD.
takes aim at breast and ovarian cancersby Pat McCaffrey
Targeted therapy

The Women’s Cancers Program at Dana-Farber 17
Back on therapy for a recurrenceof her cancer, the 54-year old Hansonis having a different experience thistime. For the last eight months, she hasbeen taking an experimental drugcalled a PARP inhibitor. [PARP standsfor poly (ADP-ribose) polymerase.]A PARP inhibitor is a new, targetedtherapy for breast and ovarian cancerthat is being tested at Dana-Farber.Her treatment consists of eight pills,twice a day. Her tumor has receded.Her hair looks great.
Targeted therapies, such as PARPinhibitors, are designed to zero in onthe exact genetic changes that makecancer cells so deadly, and leave normalcells alone. That lets the treatmenteffectively kill tumors and sparepatients from the severe side effectsthat often come with chemotherapy.
For Hanson, whose cancer iscaused by a mutation in one of the two most common breast cancer genes(BRCA1 and BRCA2), the PARPinhibitors offer the first potential treat-ment aimed at hereditary breast cancer.That is good news for the approxi-mately five percent of breast andovarian cancer patients with BRCAmutations. For other women, newresearch points to a similar defect evenin tumors without BRCA mutations,and opens the door to the possibilitythat PARP inhibitors could be effectiveagainst a wider range of both ovarianand breast cancers.
Six ways to fix DNA Research into BRCA function over
the past decade, including key work byscientists in Dana-Farber’s Women’sCancers Program, elucidated the roleof BRCA proteins involved in DNA
repair. Researchers have identified sixdifferent repair mechanisms (or path-ways), each made up of dozens of proteins that work together to mendbreaks and correct genetic mistakes.This process is critical to cell life;without it, cells quickly accumulate alethal load of genetic damage.
In breast and ovarian cancers withBRCA mutations, one of the six repairpathways loses function. To survive,the cells compensate by increasing the activity of an alternative repairpathway. The PARP enzyme is a keyprotein in the back-up pathway, andthe tumors soon become dependent on PARP activity for their survival.
Once the biology of PARP inBRCA-deficient cells became clear,clinical translation quickly followed.PARP-inhibiting compounds werealready sitting on the shelf at severalpharmaceutical companies, the productof earlier investigations for otherdisease treatments. So far, the resultsfrom clinical trials in cancer patientshave been encouraging.
In the Gynecologic MedicalOncology Program, Director UrsulaMatulonis, MD, and her team havecompleted a first study of the PARPinhibitor AZD2281. All of the womenwho took part had recurrent ovariancancer and the BRCA1 or BRCA2mutations; they all received the PARPinhibitor, and though the study wassmall, the doctors saw some “remark-able” responses. “PARP inhibitors aredefinitely active drugs in thesepatients,” Dr. Matulonis said.
Doctors are now recruiting for afollow-on study comparing the samePARP inhibitor to a standard treatmentregimen in women with advanced
ovarian cancer whose cancer progressedin spite of prior chemotherapy.
Fermina Hanson had her first boutwith breast cancer in 1997. When thetumor reappeared in 2004, she came to see Harold Burstein, MD, PhD, atDana-Farber’s Breast Oncology Center.She received a standard course of radiation and chemotherapy for herBRCA2-positive tumor. Two years later,after another local recurrence, Dr. Burstein suggested a clinical trial.The first experimental treatment shetried had no effect, but she thenenrolled in a multi-center study ofPARP inhibitors and she’s seen hertumor shrink.
When she was undergoingchemotherapy and radiation, Hansontraveled to Dana-Farber at least weeklyfrom her home in Brookline, NewHampshire, and had to take a leavefrom her job as a medical secretarywhen the side effects became toosevere. With the PARP inhibitor, shetakes her pills in the morning andevening, feels a little tired and some-times nauseous, but she says, “I go to work, I do everything I want to do.To have a drug with so few side effectsand that is effective, is wonderful.”
“This is a very new drug, and I knowthere aren’t that many people on itworldwide. But my background matchedit, and now I’m having positive results,"Hanson said. “A big reason I chose togo to Dana-Farber is because they havethese opportunities for study drugs. Ifeel blessed to have this chance.”
Not for BRCA cells only?Only a fraction of women with
breast and ovarian cancer have BRCAmutations, but many tumors have

defects in DNA repair. In ovarian cancer,up to 70 percent of tumors are defi-cient in some part of the the BRCADNA repair pathway, even though theirBRCA genes may be normal. Theproblem could lie in regulation ofBRCA gene expression or in troublewith other proteins in the samepathway. Whatever the cause, if thecells are relying on the PARP pathwayto take up the slack, the inhibitormight work for these tumors, too.
To test that idea, Dr. Matulonis isplanning a trial to evaluate the com-pound AZD2281 in women withrecurrent ovarian cancer that is stillresponsive to platinum, whether theirtumors have BRCA mutations or not.
In breast cancer, a similar opportu-nity may exist to treat an aggressiveand stubborn class of tumors known astriple negatives. These cancers lackthree clinical cancer markers, estrogenreceptors, progesterone receptors, andthe growth-promoting protein HER2.Because of this, the cells do not respondto anti-estrogen therapy, or to theHER2-targeted therapy trastuzumab.
Dan Silver, MD, PhD, then aresearch fellow with David Livingston,
MD, found that triple negative breastcancers share features of BRCA-mutated tumors, including defects inDNA repair and an accompanying sen-sitivity to the DNA-damaging drugcisplatin. Could this parallel extend tosensitivity to PARP inhibitors?
Dr. Silver, now an assistant professor in the Women’s CancersProgram, believes so. He has foundthat some of the tumors are very sensi-tive to PARP inhibitors when grown inthe lab. This work is being translatedin a clinical trial in collaboration withJudy Garber, MD, MPH, the directorof the Friends of Dana-Farber CancerRisk and Prevention Clinic. Buildingon the program’s recent success usingcisplatin chemotherapy to treat triple-negative breast cancers, the researchersplan to combine a PARP inhibitorwith cisplatin, and treat women withnewly diagnosed triple-negative tumors,with or without BRCA mutations.
Hitting the target Alan D’Andrea, MD, has spent
the last 15 years uncovering the genesand proteins involved in all six DNArepair pathways, and he thinks there
may be more tumors with the rightprofile for PARP inhibitor treatment.
“Any cell that has become depen -dent on the PARP pathway for survivalis fair game,” says Dr. D’Andrea, thechief of the Division of Radiation andCancer Biology.
To sort out the cancers thatqualify, Dr. D’Andrea and colleaguesare working out a series of laboratorytests to determine, in tumor samples,which DNA repair pathways are active.Having that information up front willallow doctors to figure out whichpatients are the best candidates forPARP inhibitor treatment. “This is areally good opportunity for personal-ized medicine,” Dr. D’Andrea says.“Our challenge is to find the perfectpatients for the PARP inhibitors.”
Many questions remain about thenew approach. Which PARP inhibitorsof several in the pipeline will emerge as the best? Should the inhibitors becombined with chemotherapy? Shouldthey be used early in treatment, orlater? Resistance to PARP inhibitorscan emerge when cells find a way toreactivate the BRCA-dependent repairpathway – will that limit their use?
It will take time to get theanswers, but Dr. Matulonis sees PARPinhibitors as just the beginning of awhole new class of therapies. “As timegoes on we are going to see more andmore drugs targeting DNA repair,” shesays. “For women with ovarian cancerwho don’t have the BRCA mutation,this is going to be an area of new drugtherapies and active research. This is anexciting time.”
Women’s Cancers Program physician/ scientists Ursula Matulonis, MD, (left) andDan Silver, MD, PhD, see promise in the use of PARP inhibitors for some breast andovarian cancer patients.
Turning Point 2009 www.dana-farber.org18

There’s a soothing harmony between the Kenns, one inwhich their sentences and stories blend into one voice, evenwhen they’re describing Mary’s three bouts with women’scancers. “I get very involved,” Jim says, using the word “we”when talking about his wife’s treatments.
Mary Kenn became a patient at Dana-Farber/Brigham andWomen’s Cancer Center (DF/BWCC) in spring 2008, whenshe was diagnosed with a rare cancer of the uterus and chose anexperimental treatment. But her saga with women’s cancersgoes back to 1997, when she underwent a lumpectomy forbreast cancer; a year later she learned she had a different type inher other breast. “The second cancer required the whole works– mastectomy, chemotherapy, and radiation,” recalls Kenn, whoreceived her care at a local hospital. “Each time somethingcame up we’d say, ‘we’ll get this fixed,’” adds Jim.
Mary enjoyed good health while taking several medica-tions to help prevent a recurrence. Nearly 10 years later,however, she noticed some mild vaginal bleeding. Her localgynecologist recommended a hysterectomy, and the lab reportafter that procedure showed carcinosarcoma of the uterus, anunusual type of cancer that grows in the muscle and lining ofthe uterus.
A second surgery was scheduled to fully stage the cancer,and although biopsies showed no sign of cancer beyond theuterus, Kenn elected to enroll in a clinical trial to give herselfthe best chances that the cancer would not return. “I thoughtthis would be like an insurance policy,” she explains. “Itwould also help doctors find treatments for other women.”
The trial is testing a combination of radiation therapywith the chemotherapy drugs oxaliplatin and gemcitabine, a
protocol used for other aggressive cancers, says Kenn’s Dana-Farber oncologist Susana Campos, MD, MPH. “We sharedwith the Kenns what we knew, and what we didn’t know aboutthis very rare type of uterine cancer,” explains Dr. Campos.“For example, we do know there is a high risk of spread to theabdomen. But because the cancer is uncommon, there really isno standard of care, so an experimental approach made sense.”
Kenn, 65, finished treatment in December 2008 andreturns for scans and check-ups. She and her husband sing the praises of DF/BWCC and especially their devoted nurse,Christin Whalen, RN. “I was nervous coming into Boston, andChristin put me at ease,” Kenn recalls. “She hugged us whenwe arrived, and often called us at home to see how I was.”
Today, the Kenns relish their roles as “Mima” and“Bampa” for their five grandchildren. Oldest daughter Aliciaand her own daughter, Amanda, 22, live with them, andtheir other two children and families are nearby. A collegestudent studying to be a nurse, Amanda says, “I love myMima and Bampa more than oxygen.”
Thanks to her renewed health, Kenn can continue withone of her favorite hobbies: embroidering blankets and othergifts. After buying a computerized sewing machine sheattended an embroidery class. As usual, her husband, Jim,was at her side.
Survivor Spotlight
By her side: Facing cancer together
In their 44 years of marriage, Mary and Jim Kenn have gonethrough a lot side by side … including Mary’s battles with cancer.
Mary Kenn sits at home in Bridgewater,
Mass., surrounded by familiar comforts.
Framed photos of her three grown children
and their families hang on her wall; the scent
of fresh home-baked blueberry muffins fills
the air; and, most reassuring of all, her
companion of the last 44 years, her husband,
Jim, is at her side.
The Women’s Cancers Program at Dana-Farber 19
by Christine Cleary

Toward the end of her fourth pregnancy, Karen Puopolo, MD, PhD, realized something was
not normal with her left breast. There was a lump, but Puopolo figured it was a blocked duct
or something else related to her pregnancy. Both her breast-feeding consultant and OB/GYN
assured her not to worry, and Puopolo — herself a physician and researcher — opted to “wait
and see.”
But when her daughter ElizabethChloe was about nine months old andPuopolo began to wean her off breastfeeding, the lump became more promi-nent. Puopolo, who specializes in new-born medicine at Brigham and Women’sHospital, booked an evaluation at herhospital’s Comprehensive Breast HealthCenter. The ultrasound, mammogram,and two biopsies that followed revealed
she had stage IIA invasive ductal carci-noma, a cancer that arises from cellslining the milk ducts. The disease hadnot spread to her lymph nodes.
At age 42, with four children anda full-time career, Puopolo was shocked,afraid, and mad. “I thought, ‘Oh, lord,I have an infant.’ I knew I had a smallchance of having breast cancer, but Iwasn’t expecting it,” she recalled recently
in her Longwood Avenue office. “Myhusband told me I had to stay aroundand help him raise our children.”
Puopolo’s experience with adelayed diagnosis is not unique. Breastcancer is the most common cancer inpregnant and postpartum women,affecting roughly one in 3,000 preg-nant women, according to the NationalCancer Institute. The natural breast
A doctor faces breast cancer– and her fears
Physician, researcher, mom … and cancer survivor,Karen Puopolo, MD, PhD.
by Debra Bradley Ruder
Survivor Spotlight
Turning Point 2009 www.dana-farber.org20

The Women’s Cancers Program at Dana-Farber 21
fullness and tenderness during this lifestage can interfere with early detectionand diagnosis of these cancers.
Once her disease was found, Puopolohad four months of chemotherapy atDana-Farber, taking doxorubicin (Adri-amycin), cyclophosphamide (Cytoxan),and paclitaxel (Taxol) every two weeks.A mastectomy and reconstructive surgeryfollowed, along with some additionalanticancer medicines. The chemotherapycaused debilitating fatigue, nausea, andweight loss, but Puopolo’s cancerresponded well to the drugs.
This winter, Puopolo got discour-aging news that she had a new nodulesuspicious for breast cancer in her chestwall. A biopsy and then surgery toremove it revealed invasive ductal carci-noma. Although this cancer had notspread, a genetic test called OncotypeDX suggested that it had a higher-than-normal risk of recurrence. Puopolo’sdoctors recommended radiationtherapy and six more months ofchemotherapy. In addition, she optedfor surgery to remove her ovaries andplans to take an aromatase inhibitor to
help reduce the chance of recurrencethrough estrogen suppression.
She’s also doing her best to stay inshape and remain healthy by routinelyusing the stairs and taking long walksaround her Newton, Mass., neighbor-hood with her husband, Steve Melly.
Those strolls, along with supportfrom her husband and kids — nowages 3 to 16 — have helped her throughthe ordeal, along with several otherfactors. Among them are her caregiversat Dana-Farber/Brigham and Women’sCancer Center. “Dana-Farber is a won-derful place,” Puopolo says. “Everyoneis kind, respectful, and professional.My oncologist Ann Partridge and her nurse practitioner Anne Kelly aregreat, and my oncology nurse DebDiPrete is a godsend. I have the samemedical team as before, and it nowincludes Dr. Jay Harris of RadiationOncology.”
Being a physician and researcher(she runs a small lab that investigatesneonatal infectious diseases) has alsomade it easier to sort through the sci-entific literature and weigh various
options for treatment. “I’m a veryinformed consumer,” Puopolo says. “Iwant to believe everything is going tobe fine, but I can’t fool myself aboutmy medical situation. However, I had a 100-percent risk of death if I didn’tget treated.”
Facing her fears has also helpedPuopolo as a patient, physician, andmom. At a professional conference inWashington, D.C., last summer, shecrossed paths with other women inacademic medicine who were there toreview their skills and career goals.During the three-day event, Puopolorealized that her breast cancer had kepther from crafting a five-year academicplan. She thought to herself, “I’m donebeing afraid. I can’t stand aroundignoring my life.”
Puopolo urges women who arepregnant or breast feeding to payattention to their bodies, despite thehormonal and other changes they’reexperiencing. “If something just doesn’tseem right after a few months,” she advises,“have it checked out.” Good advicefrom a doctor who’s been there.
Dana-Farber is a wonderful place,” Puopolo says. “Everyone is kind, respectful,
and professional. My oncologist Ann Partridge and her nurse practitioner Anne Kelly
are great, and my oncology nurse Deb DiPrete is a godsend.
“”

50%
23%
18%
9% Individuals — $5,443,202
Foundations — $2,529,871
Events — $1,971,559
Corporations — $968,057
Making aDifference
The National Cancer Institute estimates that in 2008more than a quarter million women will have been diagnosedwith breast or gynecological cancers; just shy of 69,000 willlose their lives to these diseases. Thanks to the vision and generosity of donors like you, Dana-Farber continues to offerwomen diagnosed with cancer the best in care while pursuingresearch that will lead to more effective and less toxic treat-ments. Our scientists continue to make progress on manyfronts in their ongoing battle against these complex diseases.There are many ways in which patients, families, and friendscan contribute as well.
Supporting the ResearchDonated blood can help not only existing patients, but
also research efforts at Dana-Farber. For information on howto donate blood, contact Brigham and Women’s Hospital BloodDonor Center at 617-732-6620. To donate platelets, contactthe Kraft Family Blood Donor Center at 617-632-3206.Learn more online at www.dana-farber.org/how/donateblood.
To learn more about becoming a potential stem celldonor, call the National Marrow Donor Program’s DonorRecruitment office at 617-632-2561 or 866-875-3324.
Through the generous support of donors, the Women’sCancers Program has raised more than $62 million over thelast 10 years, and nearly $11 million in fiscal 2008 alone.
To learn more about how you can support the battleagainst women’s cancers, call Ginny Fuller at 617-582-8832.
Donating Funds
Dana-Farber Cancer Institute44 Binney StreetBoston, MA 02115
617-632-4090www.dana-farber.org
A teaching affiliate ofHarvard Medical School
Non-profit Org.U.S. PostageP A I D
Dana-Farber