Embed Size (px)
Citation preview

11/26/11
1
The National Academy of Sports Medicine
From the Table to the Gym
Functional Exercise Progressions for Massage Therapy Clients
Course Objectives
• Learn how to incorporate functional exercises within massage therapy practices.
• Explore simple, evidence-based assessments and CEx strategies.
• Identify neuromyofascial tissues that prevent optimal movement.
• Identify muscles in need of progressive, functional training techniques.

11/26/11
2
Human Movement Refresher
• The Human Movement System is made up of the nervous, muscular and skeletal system.
• Posture is the alignment and function of the human movement system.
Nervous System Muscular System Skeletal System
Importance of Posture
• Proper posture: – Length-tension relationships – Force couples and joint motion
• Neuromuscular Efficiency – Ability of the nervous system to
properly recruit all muscles in all planes of motion.

11/26/11
3
Corrective Exercise Continuum
Inhibit
Lengthen
Activate
Integrate
Plan of Action
Corrective Exercise Continuum
Inhibit Activate Integrate
Inhibitory Techniques
Direct or Self Myofascial Release
Other Soft Tissue Release
Activation Techniques
Positional Isometrics
Isolated Strengthening
Integration Techniques
Integrated Dynamic
Movement
Lengthen
Lengthening Techniques
Static Stretching
Neuromuscular (PNF/Muscle
Energy) Stretching

11/26/11
4
Subjective vs. Objective
MUSCLE IMBALANCE
Can “Feel” Tight Mechanical Tension
Can “Feel” Tight Neural Tension
What muscles often “feel” tight to clients?
Follow the Movement – Don’t Chase the Pain
11/26/11
5
Dysfunction/Impairments
• Hip and Knee Complex – More than 50% of high school and college athletic
injuries involve the knee joint – PFPS and ACL injuries are the 2 most common in
this group – Hyper pronation a precursor for both – Hip abductor weakness and a deficit in hip internal
rotation risk factors as well – An increase in valgus angle may increasing loading
by @ 100% (knee moves in)
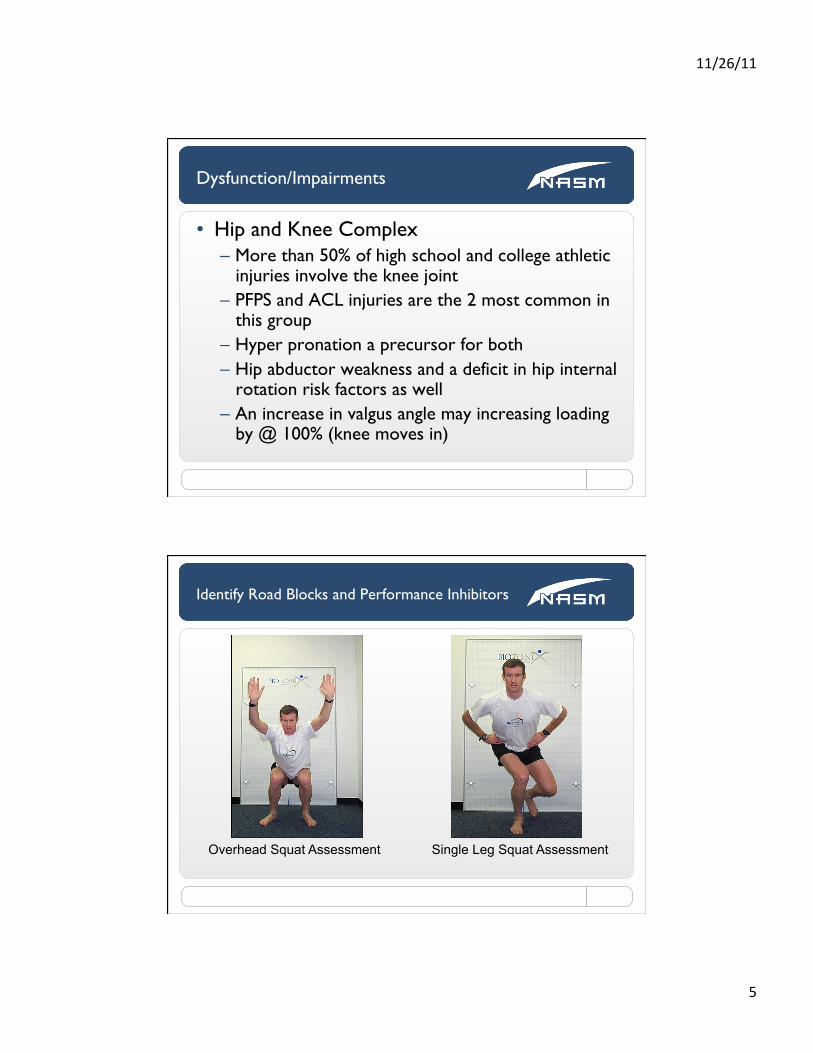
Identify Road Blocks and Performance Inhibitors
Overhead Squat Assessment Single Leg Squat Assessment

11/26/11
6
KNEES: Move Inward
Ideal Compensation
KNEES: Move Inward Overactive Muscles
Biceps Femoris (short head)
Adductor Complex TFL (and IT band)

11/26/11
7
Plan of Action
Corrective Exercise Continuum
Inhibit Activate Integrate
Inhibitory Techniques
Direct or Self Myofascial Release
Other Soft Tissue Release
Activation Techniques
Positional Isometrics
Isolated Strengthening
Integration Techniques
Integrated Dynamic
Movement
Lengthen
Lengthening Techniques
Static Stretching
Neuromuscular (PNF/Muscle
Energy) Stretching
KNEES: Move Inward Underactive Muscles
Gluteus Medius Gluteus Maximus

11/26/11
8
Gluteus Medius
• Origin: – ilium between the PSIS and
iliac crest
• Insertion: – greater trochanter of femur
• Concentric Actions: – Anterior fibers- hip
abduction, flexion, internal rotation
– Posterior fibers- hip abduction, extension, external rotation
Gluteus Maximus
• Origin: – iliac crest, sacrum,
coccyx, and the sacrotuberous and sacroiliac ligaments
• Insertion: – ITB and gluteal
tuberosity of the femur
• Concentric Actions: – hip extension, abduction,
and external rotation

11/26/11
9
Activation : Glute Med Standing Cable Abduction
Start Finish
Activation : Glute Max Floor Bridge
Start Finish

11/26/11
10
Integration: Lower Extremity
Dysfunction/Impairments
• Low Back – Disc pressure increase with APT, PPT and
excessive forward lean – Compression, bending and twisting forces
increases intra-discal pressure – Pelvic asymmetry and asymmetry in hip internal
rotation common in patients with SIJ dysfunction

11/26/11
11
LPHC: Low Back Arches
Ideal Compensation
LPHC: Low Back Arches Overactive Muscles
Hip Flexor Complex Erector Spinae Latissimus Dorsi

11/26/11
12
LPHC: Low Back Arches Overactive Muscle Iliopsoas (Psoas major + Iliacus)
• Origin: – transverse processes and
bodies of L1-L4, ilium
• Insertion: – lesser trochanter of femur
• Concentric Actions: – hip flexion, external
rotation, spinal extension (Bilateral), lateral flexion, flexion and rotation (Unilateral)
Plan of Action
Corrective Exercise Continuum
Inhibit Activate Integrate
Inhibitory Techniques
Direct or Self Myofascial Release
Other Soft Tissue Release
Activation Techniques
Positional Isometrics
Isolated Strengthening
Integration Techniques
Integrated Dynamic
Movement
Lengthen
Lengthening Techniques
Static Stretching
Neuromuscular (PNF/Muscle
Energy) Stretching

11/26/11
13
LPHC: Low Back Arches Underactive Muscles
Abdominal Complex Gluteus Maximus Hamstrings
Transverse Abdominus
• Origin: thoracolumbar fascia, cartilage of the last six ribs and iliac crest
• Insertion: linea alba, pubic crest
• Concentric actions: increases intra-abdominal pressure and supports abdominal viscera

11/26/11
14
Activation: Transverse and Rectus AB Prone Iso Ab - Plank
Activation: Glute Max Floor Bridge
Start Finish

11/26/11
15
Integration : Multiplanar Lunges
Dysfunction/Impairments
• Shoulder – 21% of general population report pain – Impingement most common diagnosis 40-65% – Traumatic dislocations 15-25% prevalence – Forward head posture, rounded shoulders, scapular
dyskinesis precursors to pain – 85% of force to decelerate a throwing/forward arm
motion comes from scapulothoracic stabilizers – Rotator cuff activation can be increased by 23 to 24% just
by stabilizing the scapulae

11/26/11
16
UPPER BODY: Arms Fall Forward
Ideal Compensation
UPPER BODY: Arms Fall Forward Overactive Muscles
Pectoralis Major Pectoralis Minor Latissimus Dorsi

11/26/11
17
Plan of Action
Corrective Exercise Continuum
Inhibit Activate Integrate
Inhibitory Techniques
Direct or Self Myofascial Release
Other Soft Tissue Release
Activation Techniques
Positional Isometrics
Isolated Strengthening
Integration Techniques
Integrated Dynamic
Movement
Lengthen
Lengthening Techniques
Static Stretching
Neuromuscular (PNF/Muscle
Energy) Stretching
UPPER BODY: Arms Fall Forward Underactive Muscles
Middle & Lower Trapezius Rhomboids

11/26/11
18
Activate: Floor Cobra
Integrate: Step Up - Curl – OH Press

11/26/11
19
Confidential and Proprietary • National Academy of Sports Medicine © 2011
Compensation Probable Overactive Muscles Key Exercises
Feet Turn Out Lateral calf complex; biceps femoris (short head)
Single -leg Balance
Knee Moves In Adductor complex, biceps femoris (short head); TFL/IT Band
Bridging, Single-leg Balance, Lateral Tube Walking
Forward Lean Calf complex, hip flexor complex Ball Cobra, Bridges, Ball Wall Squat
Low Back Arches Hip flexor complex, erector spinae, latissimus dorsi
Prone Iso-abs, Quadruped Arm/Leg Raise, Bridges
Arms Fall Forward Latissimus dorsi, pectoral complex, teres major
Ball Cobra, Ball Combo I, Squat-to-Row
Solutions
37
Confidential and Proprietary • National Academy of Sports Medicine © 2011
• Certified Personal Trainer • Corrective Exercise Specialist • Performance Enhancement Specialist • HFPN.com • California University of Pennsylvania
– BS and MS programs 100% web-based
• Con-Ed Requirements/Opportunities • Sharecare.com
Additional Opportunities
38

11/26/11
20
Confidential and Proprietary • National Academy of Sports Medicine © 2011
• Rick Richey, MS, LMT, NASM – CPT, CES, PES, CSCS – [email protected]
• Tony Ambler-Wright, MS, NASM–CPT, CES, PES, CSCS – [email protected]
Contact Information
39
Confidential and Proprietary • National Academy of Sports Medicine © 2011
Thank You! For Your
Commitment to Excellence
40
![INDEX [] · Pocatello High School Gym New Steam Line Table of Contents/1 INDEX ... Pocatello High School Gym New Steam Line Invitation ... The successful bidder](https://img.pdfslide.us/doc/110x75/5b49c98a7f8b9ada3a8ba75f/index-pocatello-high-school-gym-new-steam-line-table-of-contents1-index.jpg)




























