Embed Size (px)
Citation preview

Issue 2, Vol 1, Jan 2017
www.pihpng.com | [email protected] | +675 7998 8000 Ext 247 | ©PIH 2017
T uberculosis is a major public health challenge in PNG. TB, as it is inevita-
bly abbreviated, can present as a disease in any organ, from skin to brain
and is a common cause of ‘Fever of unknown origin( FUO)’.
Pulmonary Tuberculosis is highly infective and today resistance to
primary anti-tubercular drugs is becoming increasingly common. Multidrug
Resistant Tuberculosis( MDR) and Extremely Drug Resistant Tuberculosis( XDR)
have become Public Health nightmares and put patients, families and health
workers at great risk.
Fortunately this young child with Tuberculosis of the brain, who presented to
PIH nine months late, had a quick response and a successful outcome.
Our congratulations to Dr. Baki, Dr Khine, our radiology department and nursing staff who managed the patient’s
evaluation and treatment.
Dr Venkita Suresh
Medical Director
From The Editor’s Desk
A case of TUBERCULOMA of the BRAIN | Dr Baki & Dr Kway Khine
Case scenario A 3-year-old boy was referred from Lihir Medical Centre (ISOS) for further
evaluation and management.
Patient presented with headache, abnormal gait and right upper limb weakness
since March 2016. No other neurological complaint was noted. He could
understand when talked to, but did not speak. There was no history of fever,
cough, night sweats. No history of allergy to medicines.
No significant medical/surgical condition in the past.
He had a normal birth history. He is the only child
to the parents.
Maternal uncle had tuberculosis many years ago and completed anti-TB treatment.
On examination: No distress/lethargy/pallor/cyanosis, Body weight – 13.5 kg
Vital signs: HR – 100/min, RR – 30/min, SPO2 – 100% on room air, Temperature – 36C
Dr Kway with the patient
Dr MJ Baki
Issue 2, Vol 1, Jan 2017 2
www.pihpng.com | [email protected] | +675 7998 8000 Ext 247 | ©PIH 2017
Examination of CNS GCS 15/15, no neck stiffness.
“down and out” left eye. Ptosis, Lt Eye, present on admission
Pupils: 5 mm in left eye, 3 mm in right eye
Fundoscopy: No signs of papilledema
Motor :
Tone – Normal
Power – Right upper limb 2/5, Other limbs – 5/5
Reflexes – Normal
Sensory : intact
Cerebellar signs were difficult to elicit in the child; gait and
coordination difficult to evaluate. No nystagmus
Other systemic examinations were unremarkable.
Provisional Diagnosis Admitted to ward under the care of Dr. Mary Baki (consultant paediatrician) with provisional diagnosis of
space occupying lesion (Tuberculoma/glioma).
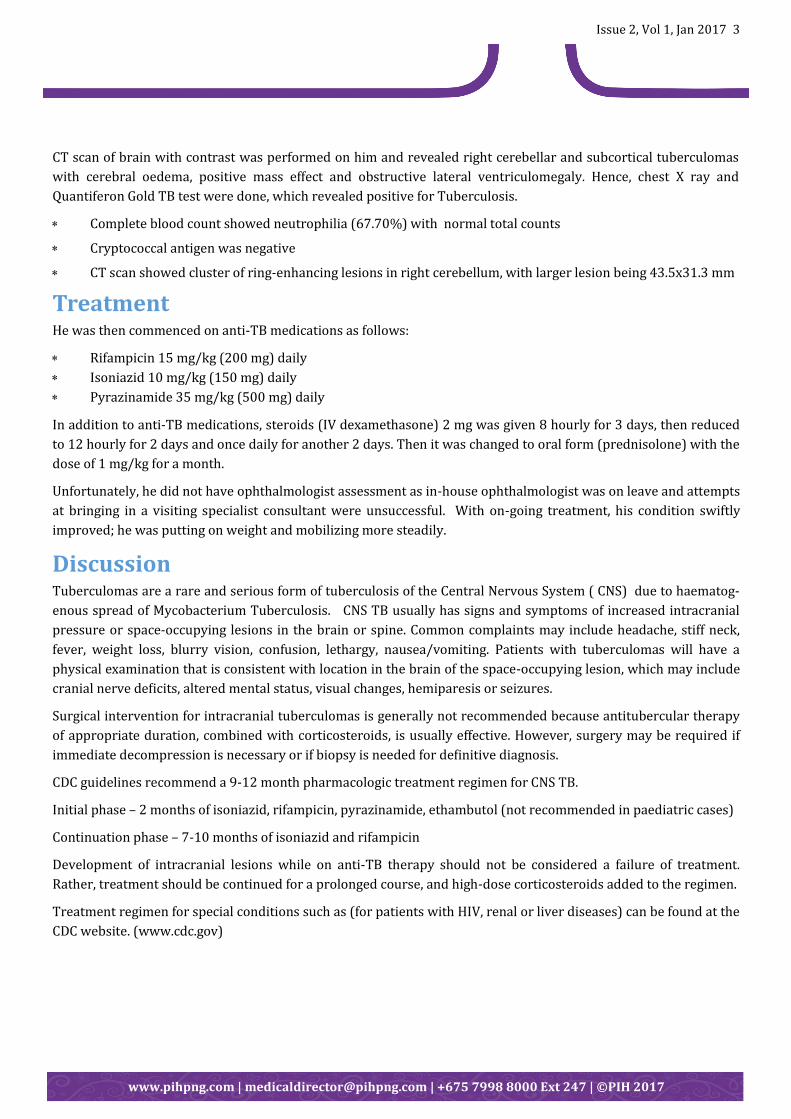
Investigations
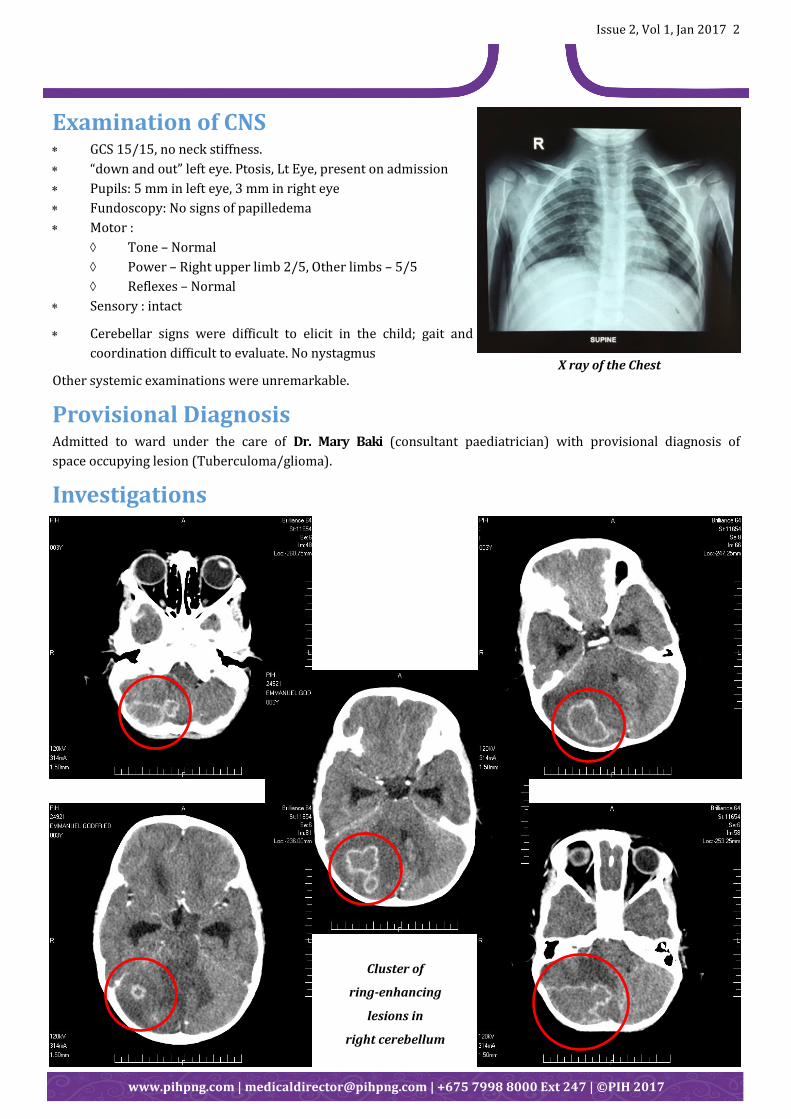
X ray of the Chest
Cluster of
ring-enhancing
lesions in
right cerebellum
Issue 2, Vol 1, Jan 2017 3
www.pihpng.com | [email protected] | +675 7998 8000 Ext 247 | ©PIH 2017
CT scan of brain with contrast was performed on him and revealed right cerebellar and subcortical tuberculomas
with cerebral oedema, positive mass effect and obstructive lateral ventriculomegaly. Hence, chest X ray and
Quantiferon Gold TB test were done, which revealed positive for Tuberculosis.
Complete blood count showed neutrophilia (67.70%) with normal total counts
Cryptococcal antigen was negative
CT scan showed cluster of ring-enhancing lesions in right cerebellum, with larger lesion being 43.5x31.3 mm
Treatment He was then commenced on anti-TB medications as follows:
Rifampicin 15 mg/kg (200 mg) daily
Isoniazid 10 mg/kg (150 mg) daily
Pyrazinamide 35 mg/kg (500 mg) daily
In addition to anti-TB medications, steroids (IV dexamethasone) 2 mg was given 8 hourly for 3 days, then reduced
to 12 hourly for 2 days and once daily for another 2 days. Then it was changed to oral form (prednisolone) with the
dose of 1 mg/kg for a month.
Unfortunately, he did not have ophthalmologist assessment as in-house ophthalmologist was on leave and attempts
at bringing in a visiting specialist consultant were unsuccessful. With on-going treatment, his condition swiftly
improved; he was putting on weight and mobilizing more steadily.
Discussion Tuberculomas are a rare and serious form of tuberculosis of the Central Nervous System ( CNS) due to haematog-
enous spread of Mycobacterium Tuberculosis. CNS TB usually has signs and symptoms of increased intracranial
pressure or space-occupying lesions in the brain or spine. Common complaints may include headache, stiff neck,
fever, weight loss, blurry vision, confusion, lethargy, nausea/vomiting. Patients with tuberculomas will have a
physical examination that is consistent with location in the brain of the space-occupying lesion, which may include
cranial nerve deficits, altered mental status, visual changes, hemiparesis or seizures.
Surgical intervention for intracranial tuberculomas is generally not recommended because antitubercular therapy
of appropriate duration, combined with corticosteroids, is usually effective. However, surgery may be required if
immediate decompression is necessary or if biopsy is needed for definitive diagnosis.
CDC guidelines recommend a 9-12 month pharmacologic treatment regimen for CNS TB.
Initial phase – 2 months of isoniazid, rifampicin, pyrazinamide, ethambutol (not recommended in paediatric cases)
Continuation phase – 7-10 months of isoniazid and rifampicin
Development of intracranial lesions while on anti-TB therapy should not be considered a failure of treatment.
Rather, treatment should be continued for a prolonged course, and high-dose corticosteroids added to the regimen.
Treatment regimen for special conditions such as (for patients with HIV, renal or liver diseases) can be found at the
CDC website. (www.cdc.gov)




























