Embed Size (px)
Citation preview
CONFIDENTIAL © 2014 PAREXEL INTERNATIONAL CORP.
From theConsultant’s CaseBook:Selected Issues inEarly ClinicalDevelopmentSciLifeLAb Minisymposium: Clinical and Regulatory Perspectives onDrug Development, Uppsala, 12Jun17Anders Neil, PhD, Principal Consultant, PAREXEL
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 2
CONTENTS
ON TODAY’S MENU Introduction
Development cases
•Small moleculesTrue generic - salts
New formulation - excipients
New indication - environment
New active – paediatrics
•Biologics
Biosimilar – assay relevance
•Advanced therapy – odd documentation
Common issues with CTA’s
Why projects fail

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 3
TOKYO, JAPAN
INTRODUCTION
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 4
RULES
“Rule number one in drug making:
No wishful thinking”Sir James Black, Pharmacologist, Nobel laureate
Seminar on drug discovery/development at Pharmacia, Uppsala, c:a 1995.
Nobel prize 1988 for discovery/development of
• Propranolol – first beta-blocker
• Cimetidine – first H2 antagonist
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 5
PHILOSOPHY
• Drug development is about selecting a molecule andadding value to it
• It is a research activity
• Research requires testable hypothesis
=> If you lack clear hypothesis you are lost!

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 6
REGULATORY MADE SIMPLE
• Quality• The technical basis. Useless without.
• Could you reproduce the stuff - every time?
• Efficacy• The reason. From non-clinical studies to controlled clinical trials.
• Could you show intended effect?
• Safety• The denominator. The terminator.
• Is the E/S ratio acceptable – for intended use?
T.I..O...N....S..….
Remember this order!
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 7
TAIPEI, TAIWAN
FROM THECONSULTANTSCASE-BOOKSMALL MOLECULES
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 8
SMALL MOLECULE PROJECTS
• Main product group
• Considerations• CMC: impurities; stability - degradation products; route – formulation & constituents
• Nonclinical: extracellular and intracellular effects; toxicity; metabolism - species selection
• Clinical: indication-dependent
• Many project types• True generics
• New delivery systems
• New indications
• New products
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 9
CASE: GENERIC IN NEW SALT FORM
• Product: true generic – old active; same route and dose form
• Project approach: salt formulation patents => change of salt“The different salts, esters, ethers, isomers, mixtures of isomers, complexes or derivatives ofan active substance shall be considered to be the same active substance, unless they differsignificantly in properties with regard to safety and/or efficacy.” Dir 2001/83/EC Art 10 (2b)
• Project solution: replace HCl with HBr; aim to avoid bioequivalence
• Issue: Regulatory concerns with bromism in renal impairment + forreproduction safety
• Solution: Bibliographic justification of bromide safety at level used•Bromide pharmacology forgotten – retrieved literature back to1921 (British Library...)
=> Salt accepted based on clear scientific data

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 10
CASE: GENERIC WITH NEW EXCIPIENTS
• Product: true generic – old active with low solubility ; same i.v. route
• Project challenge: formulation patents => need change of excipients
• Project solution: new inclusion complex formulation for i.v. use• Since immediate release i.v. no bioequivalence should be needed
• Issue: Regulatory concerns with PK impact of new formulation –potential retention/slow release of active on infusion
• Solution: Mixed justification based on• Animal pharmacology, PK, and toxicology data supporting similar in vivo exposure
• Literature data demonstrating relative affinities favours plasma protein binding with subsequenttissue re-distribution:
=> Issue resolved
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 11
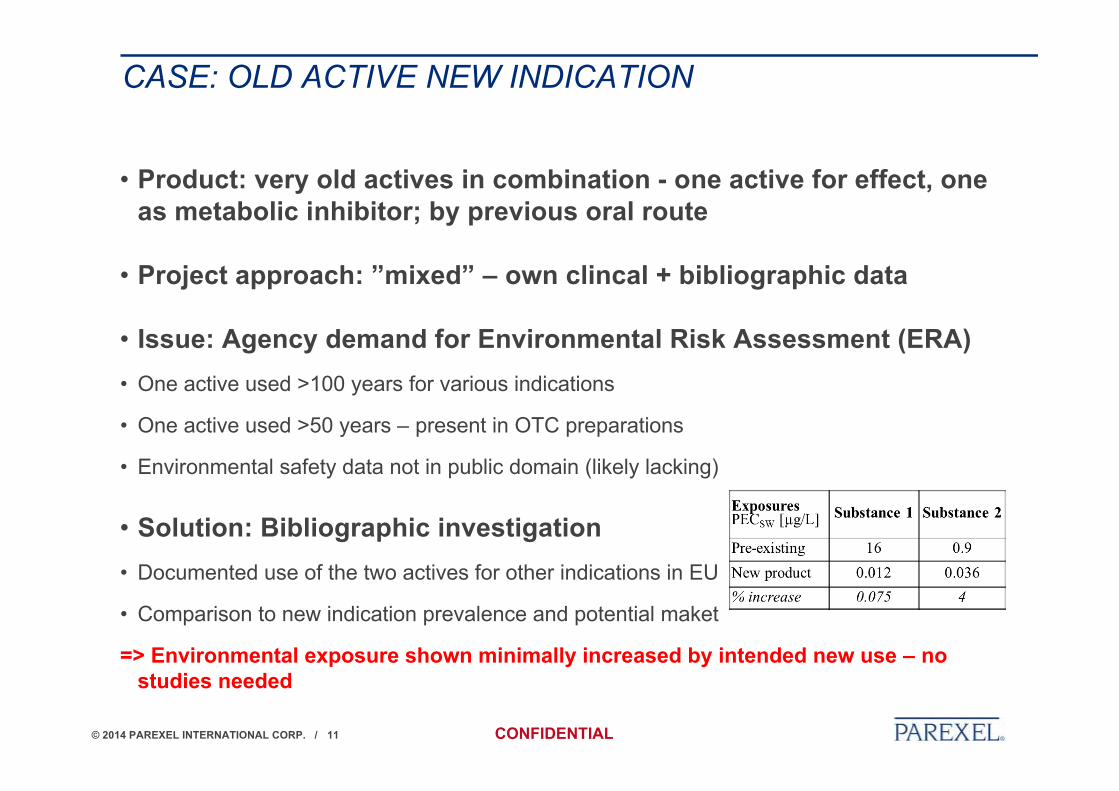
CASE: OLD ACTIVE NEW INDICATION
• Product: very old actives in combination - one active for effect, oneas metabolic inhibitor; by previous oral route
• Project approach: ”mixed” – own clincal + bibliographic data
• Issue: Agency demand for Environmental Risk Assessment (ERA)• One active used >100 years for various indications
• One active used >50 years – present in OTC preparations
• Environmental safety data not in public domain (likely lacking)
• Solution: Bibliographic investigation• Documented use of the two actives for other indications in EU
• Comparison to new indication prevalence and potential maket
=> Environmental exposure shown minimally increased by intended new use – nostudies needed
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 12
CASE: NEW ACTIVE – JUVENILE TOXICITY ISSUE
• Product: Innovative product for an orphan indication
• Project approach: Juvenile development for ages < 6 years
• Project solution: PIP committment on clinical + toxicity studies
• Issue: Specific organ toxicity found in juvenile rodent study
• Solution: Bibliographic investigation assessing• Known drug toxicities in this organ during this early development period
• Known differences from human in this organs development time-line
• Clinical data checked for any similar findings
• => Agency conclusion: ”…this finding is considered to have little relevance to infants andchildren.”
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 13
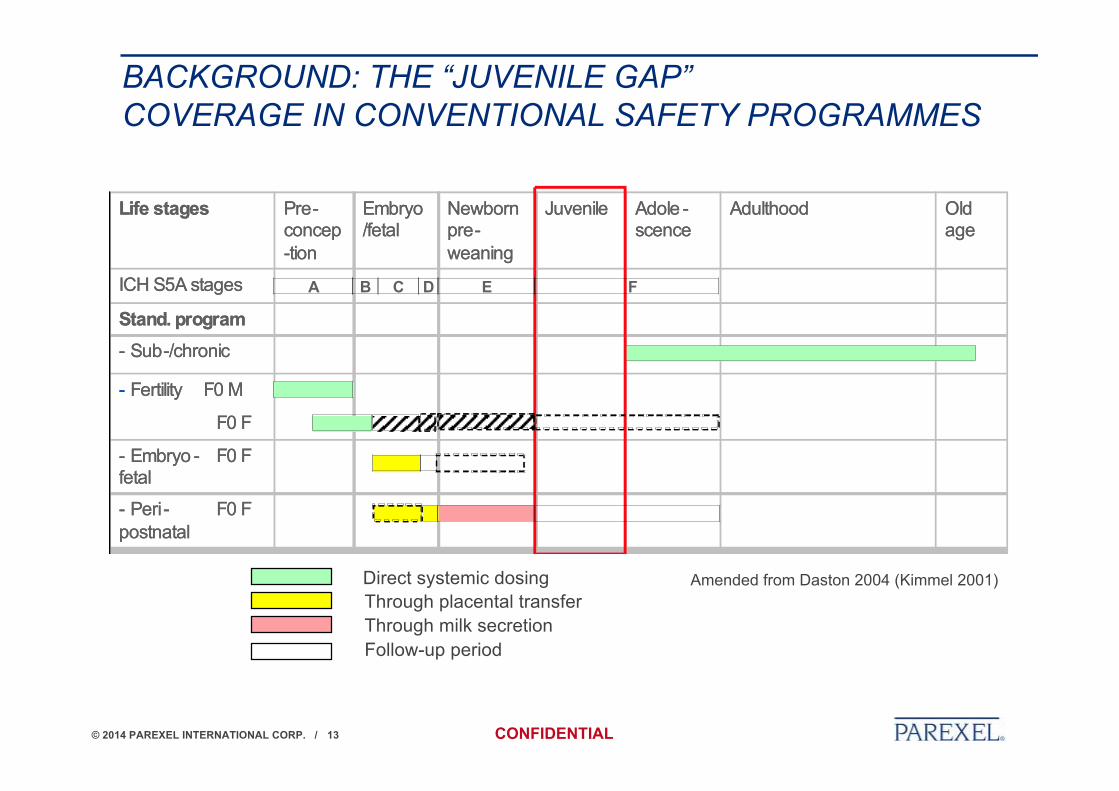
BACKGROUND: THE “JUVENILE GAP”COVERAGE IN CONVENTIONAL SAFETY PROGRAMMES
Amended from Daston 2004 (Kimmel 2001)
- Peri- F0 F postnatal
- Embryo - F0 F fetal
- Fertility F0 M
F0 F
- Sub-/chronic
Stand. program
ICH S5A stages
Life stages Old age
AdulthoodAdole -scence
JuvenileNewborn pre-weaning
Embryo /fetal
Pre-concep-tion
- Peri- F0 F postnatal
- Embryo - F0 F fetal
- Fertility F0 M
F0 F
- Sub-/chronic
Stand. program
ICH S5A stages
Life stages Old age
AdulthoodAdole -scence
JuvenileNewborn pre-weaning
Embryo /fetal
Pre-concep-tion
A B C D E F
Direct systemic dosingThrough placental transferThrough milk secretionFollow-up period
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 14
BERLIN, GERMANY
FROM THECONSULTANTSCASE-BOOKRECOMBINANTPROTEINPRODUCTS ANDADVANCEDTHERAPIES
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 15
BIOTECH (RECOMBINANT PROTEIN) PROJECTS
• Rapidly expanding
• Considerations• CMC: process impurities; viral removal; stability; process consistency
• Nonclinical: exaggerated pharmacological effect; relevant species critical
• Clinical: immunogenicity; indication-dependent
• Few project types• Biosimilars
• New products
• NOTE: The product is the process result - not a single moleculewith defined contaminants. Generics not possible – biosimilar(sufficiently similar) products instead.
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 16
CASE: BIOSIMILAR MONOCLONAL ANTIBODY (1/2)
• Product: Biosimilar mAb for systemic use
• Project challenge: Provide a product not deviating from originator
• Project solution: True copy of amino acid sequence; somedifference in glycosylation pattern
• Issues: Difference found in vitro for assays on Fc binding/functionNOTE: Extensive test battery in EU Guideline (EMA/CHMP/BMWP/403543/2010):
Fab part: Binding to target; Fab-associated function (e.g. neutralization of a soluble ligand,receptor activation or blockade) = at least 1 binding + 1 functional assay
Fc part: Binding to representative isoforms of the relevant three Fc gamma receptors (FcγRI,FcγRII and FcγRIII), FcRn and complement (C1q); Fc-associated functions (e.g. antibody-dependent cell-mediated cytotoxicity, ADCC; complement-dependent cytotoxicity, CDC;complement activation) = at least 8 binding + 2 functional assays
All studies in comparison to EU released reference product (many batches)
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 17
CASE: BIOSIMILAR MONOCLONAL ANTIBODY (2/2)
• Solution:• Extensive investigation of cause for found assay differences (statistical chance excluded)
• Assessment of assay condition impact – ”pure system” found to exaggerate differences(less difference in presence of human serum)
• Additional assays performed using other cells/systems
• Assessment of relevance: differences not related to primary action of this product
• Clinical data (Phase 1 PK; Phase 3 efficacy and safety) did not bear out essentialdifferences in therapeutic effect or safety (including immunogenicity)
=> Biosimilarity accepted

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 18
ADVANCED THERAPY PROJECTS
• Still a small group - few projects• Gene therapy
• Cell therapy
• Tissue engineering
• Considerations• CMC: standardisation of manufacturing; quality control and release of ”live” products (cell
therapy; tissue engineering) – small series, short shelf-life
• Nonclinical: few/no relevant species/models – use MABEL approach
• Clinical: short series; blinding difficult/impossible
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 19
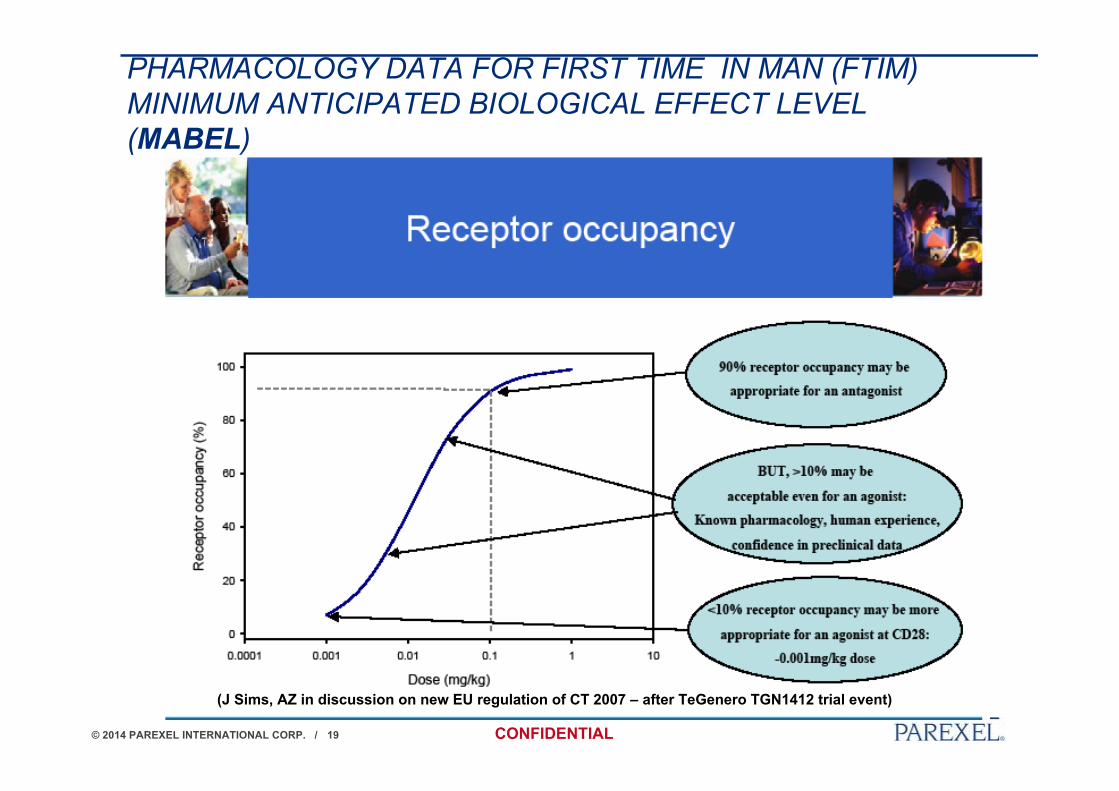
PHARMACOLOGY DATA FOR FIRST TIME IN MAN (FTIM)MINIMUM ANTICIPATED BIOLOGICAL EFFECT LEVEL(MABEL)
(J Sims, AZ in discussion on new EU regulation of CT 2007 – after TeGenero TGN1412 trial event)

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 20
MABEL
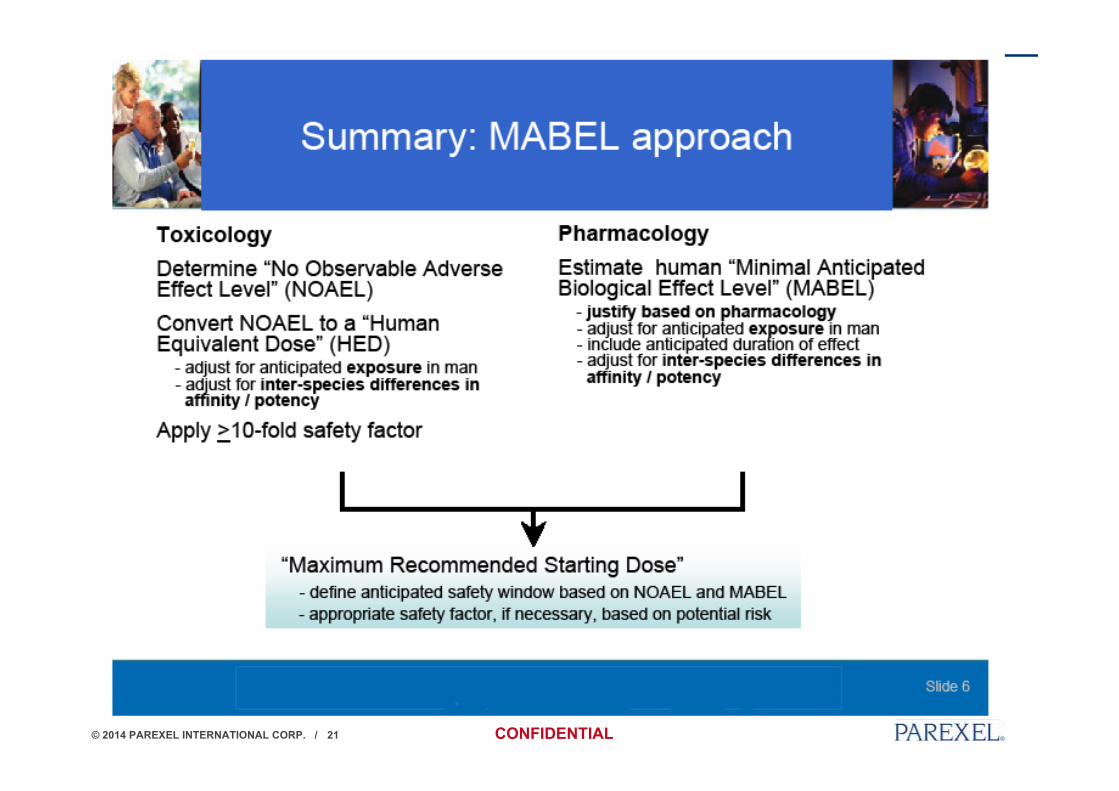
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 21
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 22
CASE: BIOPSIED EXPANDED CELLS (1/2)
• Product: Autologous cell product to increase capacity of an organ(pending graft); Non-EU company developing cell product forglobal studies
• Challenges• General: Research staff never prepared a regulatory submission before
• CMC: No clear definition of drug substance and drug product making product andmanufacturing control strategy non-standard
• Nonclinical: Animal integrated study data to be teased apart for structuredanalysis/presentation in CTD format (pharmacology; pharmacokinetics; toxicology)
• Clinical: FTiM requiring extensive risk assessment
• Regulatory: Important logistic challenges and GMP requirements; needed EUrepresentative for submission and maintenance and advice on ethical approval strategy forEU countries involved in trial; QP requirements

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 23
CASE: BIOPSIED EXPANDED CELLS (2/2)
Project solution:• Instructed researchers on CTD structure, content and regulatory writing
• Reviewed and edited client drafts and finished IMPD
• Support to handle EUDRACT registration and submission
•Issues: Surprisingly few• CMC: One major question raised which had been identified in gap analysis but could not
be addressed in time for submission. Response was accepted.
• Nonclinical: Cleared CTA with minor questions
• Clinical: Questions were raised and responses accepted.
=> Trial approval obtained 7 months from contact

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 24
BOSTON, MASSACHUSETTS
TRIALS APPLICATION ISSUES
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 25
MHRA GUIDANCE: COMMON ISSUES IDENTIFIEDDURING CLINICAL TRIAL APPLICATIONS !!!!
https://www.gov.uk/government/publications/common-issues-identified-during-clinical-trial-applications

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 26
https://www.gov.uk/government/publications/common-issues-identified-during-clinical-trial-applications

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 27
MHRA GUIDANCE: COMMON ISSUES IDENTIFIEDDURING CLINICAL TRIAL APPLICATIONS
https://www.gov.uk/government/publications/common-issues-identified-during-clinical-trial-applications
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 28
MHRA GUIDANCE: COMMON ISSUES IDENTIFIEDDURING CLINICAL TRIAL APPLICATIONS
https://www.gov.uk/government/publications/common-issues-identified-during-clinical-trial-applications
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 29
THE FIRE ENGINEERING APPROACH
Get involved early
•Check design
•Prepare for evacuation
•Minimise loss
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 30
EARLY PROJECT ISSUES HANDLING
Early timing needed
• Design: Verify project regulatory assumptions• Interpretation of ICH guidance may differ considerably among Agencies
• Preparation: Justify positions taken• Cases should be built in advance and may require extensive research
• Damage control: Make contingency plans• Time loss in preparing for new decisions could be minimised by pro-
active planning
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 31
EXAMPLES
• Regulatory assumptions• EU agencies are generally strict on embryo-fetal repro data for inclusion of fertile women
• Exceptions then based on other hard data – e.g. combination w. known teratogens
• Preparation• Do not apply to DE (BfArM) without thorough photo-toxicity evaluation
• Make sure that you have adequate UV/VIS scan data in the IMPD
• Absorption in relevant spectrum need up-front evaluation in terms of skin/eye distributionand exposure data
• ”Plan B”• What inclusion criteria could be modified w/o compromising study objectives?
• To re-instate with new data…

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 32
LONDON, U.K.
WHY PROJECTS FAIL
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 33
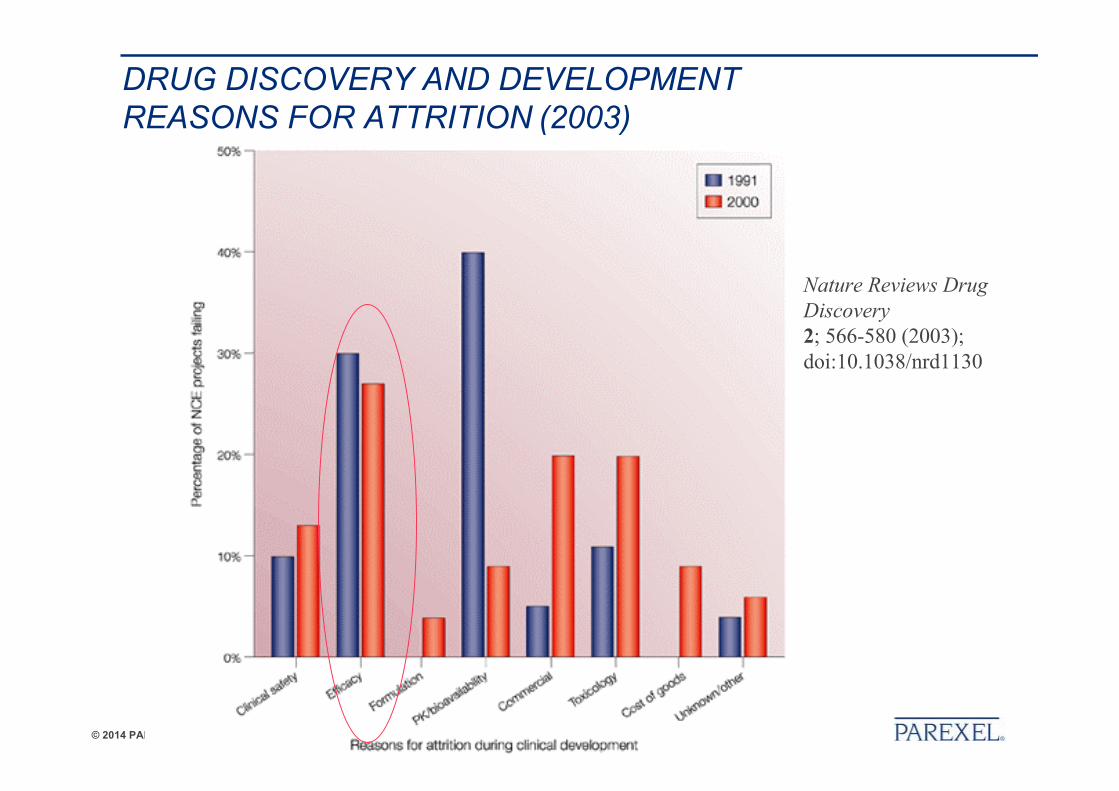
DRUG DISCOVERY AND DEVELOPMENTREASONS FOR ATTRITION (2003)
Nature Reviews DrugDiscovery2; 566-580 (2003);doi:10.1038/nrd1130
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 34
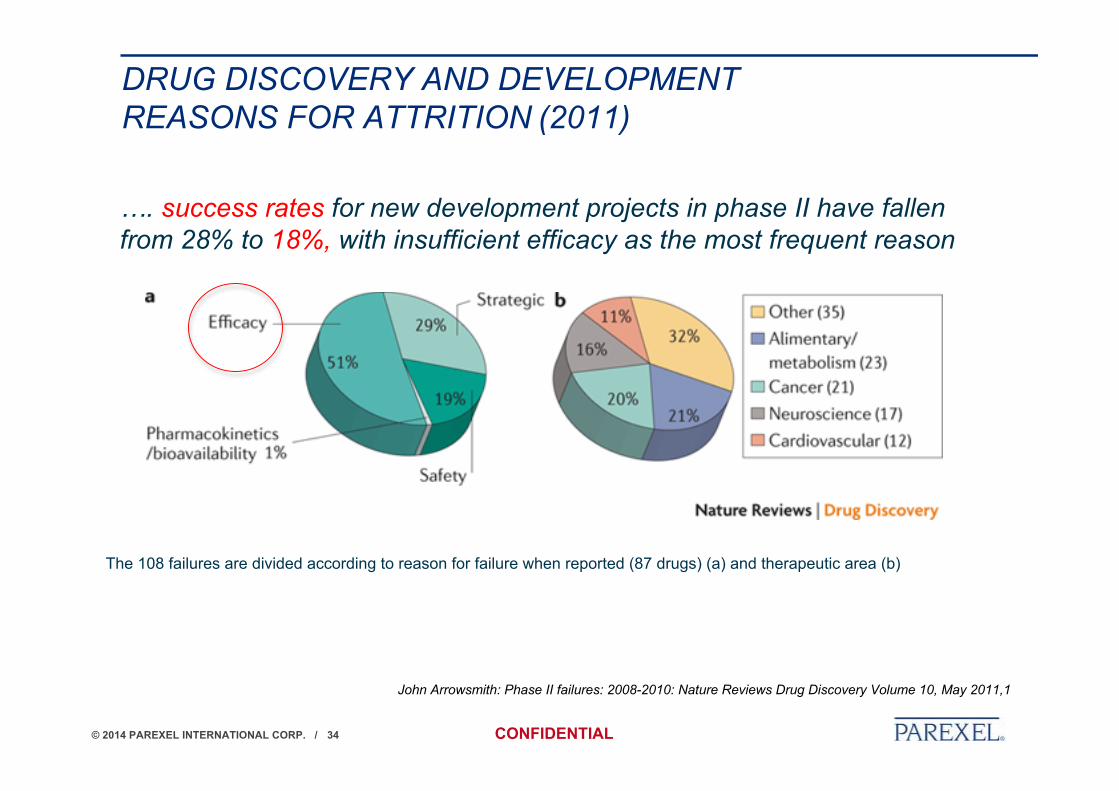
DRUG DISCOVERY AND DEVELOPMENTREASONS FOR ATTRITION (2011)
John Arrowsmith: Phase II failures: 2008-2010: Nature Reviews Drug Discovery Volume 10, May 2011,1
The 108 failures are divided according to reason for failure when reported (87 drugs) (a) and therapeutic area (b)
…. success rates for new development projects in phase II have fallenfrom 28% to 18%, with insufficient efficacy as the most frequent reason

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 35
DUBLIN, IRELAND
CONCLUSIONS?

© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 36
CONSULTANTS PERSPECTIVE
• Question number one: What are you going to do with the data?• Be clear on end use - business (decision; funding), or regulatory – before you do anything
• You need a regulatory strategy from start• Don’t guess - validate your plans early by agency interactions
• US ≠ EU: opinion may differ more between FDA review divisions than among EUagencies
• There is no flawless file• Regulators are your friends
• Don’t try to hide awkward findings – do your homework and discuss
• Keep your documentation safe and in order• Save samples of early substance batches
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 37
THANK YOU
© 2014 PAREXEL INTERNATIONAL CORP. / CONFIDENTIAL 37
ANY QUESTIONS?