Embed Size (px)
Citation preview

From Myeloma Precursor Disease to Multiple Myeloma: New DiagnosticConcepts and Opportunities for Early Intervention
Ola Landgren1, Robert A. Kyle2, and S. Vincent Rajkumar2
AbstractSince monoclonal gammopathy of undetermined significance (MGUS) was first described more than
30 years ago, the definition of the entity has evolved. Today, 3 distinct clinical MGUS subtypes have been
defined: non–immunoglobulin M (IgM; IgG or IgA) MGUS, IgM MGUS, and light chain MGUS. Each
clinical MGUS subtype is characterized by unique intermediate stages and progression events. Although we
now have strong evidence that multiple myeloma is consistently preceded by a precursor state at the
molecular level, there is urgent need to better understand mechanisms that regulate transformation from
precursor to full-blown multiple myeloma. In the future, if such knowledge was available, it would allow
clinicians to define high-risk and low-risk precursor patients for a more tailored clinical management. Also,
it would provide insights on the individual patient’s disease biology, which, in turn, can be used for
targeted and more individualized treatment strategies. On the basis of current clinical guidelines, patients
diagnosed with MGUS and smoldering myeloma should not be treated outside of clinical trials. In the near
future, it seems reasonable to believe that high-risk precursor patients will likely become candidates for
early treatment strategies. In this review, we discuss novel insights from recent studies and propose future
directions of relevance for clinical management and research studies. Clin Cancer Res; 17(6); 1243–52.
�2011 AACR.
Introduction
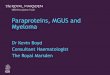
Monoclonal gammopathy of undetermined significance(MGUS) is a premalignant plasma cell disorder present inmore than 3% of the general Caucasian population age 50and older (1, 2). On a clinical note, individuals diagnosedwith MGUS have a 1% annual risk of progression tomultiple myeloma (MM) or related malignancy (3). Typi-cally, MGUS is found incidentally during the work-up of avariety of symptoms and disorders. It is characterized byabnormal immunoglobulins detectable in the patient’speripheral blood and/or urine, as well as clonal plasmacells present in the bone marrow (Fig. 1). Definitions ofdistinct MGUS subtypes are given in Table 1.Furthermore, MGUS has confirmed and reported asso-
ciations with numerous diseases that are commonlyencountered in clinical practice, such as osteoporosisand venous thrombosis (4). Given the fact that MGUS iseasily detected in peripheral blood and it can be monitorednoninvasively, MGUS represents a readily accessible
model to study the conversion of premalignancy tomalignancy (5).
Race and ethnicity play a role in the pathogenesis ofMGUS. African Americans and blacks from Africa have a2- to 3-fold higher prevalence of MGUS compared withwhites (6, 7). In contrast, the risk is lower in Asians fromJapan (8) and in Mexicans (9). Increasing age (1), malegender, family history of MGUS and/or MM (10), immu-nosuppression, and exposure to certain pesticides (11) allincrease the risk of MGUS. Clearly, future studies areneeded to improve our understanding on underlyingmechanisms of these associations.
A more advanced premalignant stage of plasma cellproliferation in non–immunoglobulin M (IgM) MGUS istermed smoldering myeloma and is characterized by amuch higher risk of progression to MM (on average, about10% per year during the first 5 years of follow-up; ref. 12).
During recent years, new concepts and advances haveemerged about the diagnosis, classification, risk stratifica-tion, and management of myeloma precursor disease(MGUS and smoldering myeloma). In this review, wediscuss novel insights from recent studies and proposefuture directions for clinical management and researchstudies (13).
Distinct Clinical Monoclonal Gammopathy ofUndetermined Significance Subtypes
Since MGUS was first described in 1978 (14), the defini-tion of the entity has evolved (15). Today, 3 distinct clinical
Authors' Affiliations: 1Center for Cancer Research, National CancerInstitute (NCI), NIH, Bethesda, Maryland; 2Division of Hematology, MayoClinic, Rochester, Minnesota
Corresponding Author: Ola Landgren, National Cancer Institute, NIH,Center for Cancer Research, Medical Oncology Branch, 9000 RockvillePike, Bldg 10/Room 13N240, Bethesda, MD 20892. Phone: 301-496-0670; Fax: 301-402-0172; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-10-1822
�2011 American Association for Cancer Research.
CCR FOCUS
www.aacrjournals.org 1243
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

MGUS subtypes have been defined: non-IgM (IgG or IgA)MGUS, IgM MGUS, and light chain MGUS (Table 1). Eachclinical MGUS subtype is characterized by unique inter-mediate stages and progression events. For example, asmentioned above, the more advanced premalignant stageof plasma cell proliferation in non-IgM MGUS is smolder-ing myeloma; it has an average 10% annual risk of pro-gression to MM (versus 1% per year collectively for allforms of MGUS; ref. 12). IgM MGUS is associated with apredisposition mainly to Waldenstr€om’s macroglobuline-mia and rarely to IgMMM (16, 17). Recently, a new diseaseentity termed "light chain MGUS" was defined. It repre-sents the premalignant precursor of a subtype of MM called"light chain MM," which accounts for almost 20% of allnew MM cases (18). The equivalent of smoldering mye-loma and smoldering Waldenstr€om’s macroglobulinemiain the spectrum of light chain monoclonal gammopathiesis called idiopathic Bence Jones proteinuria (Table 1; refs.19, 20). At this time, at least 1 large cohort, includingpatients meeting each of the above listed clinical subtypes,has been assembled. These cohorts have allowed cliniciansand researchers to study and define the natural history foreach MGUS subtype (3, 12, 16, 18, 19, 21–23). Conse-quently, we now know how to diagnose each of theseentities accurately, and we also know the outcome ofpatients meeting the specific subtype definition to assist
with management and counseling. In Table 1, we havesummarized the main features and results from the largestepidemiologic and clinical studies focusing on MGUSsubtypes to date (3, 12, 16, 18, 19, 21–23). More specifi-cally, we have listed and commented on prevalence, risk ofprogression, and natural history of non-IgM MGUS, IgMMGUS, and light chain MGUS.
It should be emphasized that, in patients diagnosed withclonal proliferation of plasma cells consistent with a pre-cursor state, the biology and natural history is very differentcompared with patents diagnosed with MM. Importantly,patients with a precursor state should be reassured ratherthan labeled as having a cancer. For example, patients withless than 10% infiltration of the bone marrow by lympho-plasmacytic cells have an overall survival similar to that ofthe general population and should, therefore, not belabeled as having a lymphoma or Waldenstr€om’s macro-globulinemia merely because the bone marrow pathologyshows clonal proliferation of lymphoid cells (22). Further-more, on a clinical note, increasingly better sensitivity fordiagnostic methods will continue to challenge clinicalmanagement, and the line between malignancy and pre-malignancy will most likely continue to blur. As our under-standing of disease progression improves, it will becomemore and more important to recognize that well-designedepidemiologic studies and clinicopathologic disease
© 2011 American Association for Cancer Research
Figure 1. Bone marrow biopsies from a patient with non-IgM MGUS [A, hematoxylin and eosin (H&E) and B, CD138] and from a patient with MM(C, H&E and D, CD138). Magnification 200�.
CCR FOCUS
Clin Cancer Res; 17(6) March 15, 2011 Clinical Cancer Research1244
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

definitions will be required to separate patients who needtreatment, such as chemotherapy or stem cell transplanta-tion for cancer like myeloma (24), from those who call forno therapy and need reassurance (5).
From Precursor to Multiple Myeloma: CurrentClinical Risk Models
It is important to keep in mind that the vast majority ofMGUS patients will never progress toMM. Currently, we donot have access to any reliable markers to predict risk ofMM progression for individual MGUS patients. At thepresent time, the risk of progression of MGUS is assessedby a few selected risk factors. Two major models for riskstratification have been proposed: one model by the MayoClinic and the other by the Spanish study group [Programapara el Estudio de la Terap�eutica en Hemopatı́a Maligna(PETHEMA); Fig. 2].The Mayo Clinic model focuses largely on serum protein
abnormalities. For MGUS patients, the following featuresare considered as adverse risk factors: non-IgG isotype, M-protein concentration � 1.5 g/dL, and an abnormal serumfree light chain (FLC)–ratio (normal reference 0.26 to 1.65;Fig. 2; ref. 25). In the Mayo Clinic model, at 20 years offollow-up, MGUS patients with all 3 risk factors, on aver-age, have an absolute risk of MM progression of 58%;for MGUS patients with 2, 1, and 0 of these risk factors,the corresponding absolute risk is 37%, 21%, and 5%,respectively (25). For smoldering myeloma patients, thefollowing features are considered to be adverse risk factors:�3 g/dLM protein, an FLC ratio outside the reference rangeof 0.125 to 8, and �10% bone marrow plasma cells(BMPC; Fig. 2; refs. 14, 26). In the Mayo Clinic model,at 5 years of follow-up, smoldering myeloma patients withall 3 risk factors, on average, have a cumulative risk of MMprogression of 76% [median time to progression (TTP) was1.9 years]; for patients with 2 or 1 risk factors the corre-sponding risk was 51% (median TTP 5.1 years) and 25%(median TTP 10 years), respectively (12, 26).The Spanish model uses multiparametric flow cytometry
of bone marrow aspirates to differentiate aberrant fromnormal plasma cells (27). Plasma cells characteristicallyexpress CD138 and intense (bright) CD38. The features ofaberrant plasma cells (aPC) included decreased CD38expression, expression of CD56, and the absence ofCD19 and/or CD45. In 93 smoldering myeloma and407MGUS patients, the percentage of phenotypically aPCsof total BMPCs at diagnosis allowed risk stratification ofMGUS and smoldering myeloma patient’s progression toovert MM. In their study, MGUS and smoldering myelomapatients with �95% aPCs/BMPC at diagnosis had a sig-nificantly higher risk of MM progression (27). Further-more, on multivariate analysis, �95% aPCs/BMPC, DNAaneuploidy, and immunoparesis were found to be inde-pendent predictors of MM progression. More specifically,for MGUS patients with 0, 1, or 2 risk factors (�95% aPCs/BMPC and DNA aneuploidy) the risk of progression at5 years was 2%, 10%, and 46%, respectively (Fig. 2). For
smoldering myeloma patients (risk factors: �95% aPCs/BMPC and immunoparesis), the corresponding risks at 5years were 4%, 46%, and 72%, respectively (Fig. 2; ref. 27).
Taken together, these studies emphasize the fact that therisk of MM progression varies greatly among individualsdiagnosed with myeloma precursor disease. As discussed indetail below, we need better markers to define high-risk(versus low-risk) MGUS–smoldering myeloma and to bet-ter predict individual risk of MM progression.
From Precursor to Multiple Myeloma: CurrentKnowledge from the Research Laboratory
Two independent studies have shown that MM is con-sistently preceded by MGUS (28, 29). In the first study, onthe basis of a large cancer-screening trial including 77,469volunteers prospectively followed for up to 10 years in acancer-screening trial, 71 individuals were found todevelop MM. Using stored prediagnostic serum samplesobtained annually from these subjects, evidence of MGUSwas shown prior to MM in all participants (28). In 82% ofMM cases, evidence of MGUS was present in prediagnosticblood collected �8 years prior to MM diagnosis (28). Theother study was based on a large U.S. Army serum repo-sitory. In brief, that study reported that 27 of 30 MM caseswith available prediagnostic serum samples had evidenceof a preceding MGUS diagnosis; the other 3 patients eitherhad IgD MM or lacked samples �8 years prior to MMdiagnosis (29).
Of great relevance from a clinical perspective, in approxi-mately half of the 71 MM patients from the large cancer-screening trial (28), on the basis of the systematicallycollected prediagnostic blood samples, the M-protein con-centration increased annually following initial detection;among the remaining patients, serumM protein was stableuntil MM diagnosis (30). Similar patterns of gradual evolu-tion and sudden increase prior to diagnosis were alsoobserved in the serum FLC ratio (around 85%had a skewedFLC ratio 2 years prior to MM diagnosis; ref. 28). Impor-tantly, these findings emphasize the fact that cliniciansmust be alert in monitoring patients for myeloma-relatedend-organ damage regardless of the stability of serumprotein markers.
At the molecular level, on the basis of our currentknowledge, transformation from precursor to full-blownMM does not seem to be a sudden, discontinuous processwith specific immunophenotypic markers differentiatingplasma cells in patients with MGUS, smoldering myeloma,and MM (31, 32). Instead, several overlapping oncogenicevents within plasma cells and the marrow microenviron-ment accumulate from normal plasma cells through pre-cursor disease to full-blown MM. Indeed, early cytogeneticchanges are seen among almost all patients at the level ofMGUS (31, 32). These potentially overlapping, enduringchanges are seen from MGUS onward and include hyper-diploidy and primary immunoglobulin translocations atthe 14q32 locus (33–35). In both states, cyclin D dysre-gulation is a very common early event (36). Importantly, at
Multiple Myeloma and Its Precursors
www.aacrjournals.org Clin Cancer Res; 17(6) March 15, 2011 1245
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

this time, MGUS from smoldering myeloma cannotbe differentiated using conventional cytogenetics orFISH (37).
Abnormal plasma cells in MGUS, smoldering mye-loma, and MM produce a broad range of immunorecep-tors that are stimulated by both exogenous molecules andmicroenvironmental paracrine signals, such as interleu-kin-6, contributing to the clonal proliferation observed inpatients’ bone marrow biopsies (38). In contrast, manysecondary oncogenic events have been implicated in thetransition from MGUS and/or smoldering myeloma tofull-blown MM and from newly diagnosed MM toadvanced and/or refractory disease. These secondarygenetic events may, in part, be dependent on the primarylesion (39, 40). Furthermore, complex alterations to
microenvironmental interactions occur in the transitionfrom MGUS to MM (41). An apparent manifestation inmyeloma genesis is the interaction between abnormalplasma cells, cells in the bone marrow microenviron-ment, and the bone (41), which ultimately leads tocharacteristic lytic lesions in approximately 80% of MMpatients (42). Although osteoclastic activation and osteo-blastic inactivation leading to lytic lesions is a criterionfor progression from MGUS and/or smoldering myelomato MM, studies using quantitative bone biopsy and levelsof biomarkers for bone turnover [e.g., receptor activatorof NF-kB (RANK) ligand], have revealed excess boneresorption in patients with MGUS (43–45). Future studiesare needed to better define the role of activated osteo-clasts in the pathogenesis of MM.
Table 1. Disease Definitions for the Monoclonal Gammopathies: Monoclonal Gammopathy of Undeter-mined Significance and Related Disorders
Type ofmonoclonalgammopathy
Premalignancy with alow risk of progression(1 to 2% per year)
Premalignancy with a high riskof progression (10% per year)
Malignancy
IgG and IgA(non-IgM)monoclonalgammopathiesa
Non-IgM MGUS Smoldering MM MM
All 3 criteria must be met:* Serum monoclonalprotein < 3 g/dL
* Clonal BMPCs < 10%, and* Absence of end-organdamage such as CRABthat can be attributedto the plasma cellproliferative disorder
Both criteria must be met:* Serum monoclonal protein(IgG or IgA) � 3 g/dL and/orclonal BMPCs � 10%, and
* Absence of end-organ damagesuch as lytic bone lesions,anemia, hypercalcemia, or renalfailure that can be attributedto a plasma cellproliferative disorder
All 3 criteria must be metexcept as noted:* Clonal BMPCs � 10%* Presence of serum and/orurinary monoclonal protein(except in patients with truenonsecretory MM), and
* Evidence of end organdamage that can be attributedto the underlying plasma cellproliferative disorder, specifically* Hypercalcemia: serum
calcium � 11.5 mg/dL or* Renal insufficiency: serum
creatinine > 2 mg/dL orestimatedcreatinine clearance lessthan 40 ml/min
* Anemia: normochromic,normocytic with a hemoglobinvalue of > 2 g/dLbelow the lower limit of normalor a hemoglobin value < 10 g/dL
* Bone lesions: lytic lesions orsevere osteopenia attributed toa plasma cell proliferativedisorder or pathologic fractures
(Continued on the following page)
CCR FOCUS
Clin Cancer Res; 17(6) March 15, 2011 Clinical Cancer Research1246
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Treatment Studies for Smoldering Myeloma:Future Challenges and Opportunities
On the basis of the International Myeloma WorkingGroup 2010 guidelines, patients diagnosed with MGUSand smoldering myeloma should not be treated outside ofclinical trials (2). Overall, treatment trials for MGUSpatients are complicated, as these individuals are relatively
healthy and the majority has a low life-time risk of pro-gression, especially when other causes of death are takeninto account (3). Therefore, it seems reasonable to proposethat an ideal treatment would be effective, nontoxic, anddirected toward patients with a high risk of progression. Atthis time, we do not have access to any such drug.
In contrast to MGUS, early treatment strategies for smol-dering myeloma are particularly attractive, as the rate of
Table 1. Disease Definitions for the Monoclonal Gammopathies: Monoclonal Gammopathy ofUndetermined Significance and Related Disorders (Cont'd )
Type ofmonoclonalgammopathy
Premalignancy with alow risk of progression(1 to 2% per year)
Premalignancy with a high riskof progression (10% per year)
Malignancy
IgM monoclonalgammopathies
IgM MGUSb Smoldering Waldenstr€om'smacroglobulinemia
Waldenstr€om's macroglobulinemia
All 3 criteria must be met:* Serum monoclonalprotein < 3 g/dL
* Clonal bone marrowlymphoplasmacyticcells < 10%, and
* Absence of end-organdamage such as anemia,constitutional symptoms,hyperviscosity,lymphadenopathy, orhepatosplenomegaly thatcan be attributed to theunderlying lymphoproliferativedisorder.
Both criteria must be met:* Serum IgM monoclonalprotein � 3 g/dL and/or bonemarrow lymphoplasmacyticinfiltration � 10%, and
* No evidenceof anemia, constitutionalsymptoms, hyperviscosity,lymphadenopathy,or hepatosplenomegaly that canbe attributed to the underlyinglymphoproliferative disorder.
All criteria must be met:* IgM monoclonal gammopathy(regardless of the size of the Mprotein), and
* � 10% bone marrowlymphoplasmacyticinfiltration (usually intertrabecular)by small lymphocytes that exhibitplasmacytoid or plasma celldifferentiation and a typicalimmunophenotype (e.g.,surface IgMþ, CD5�, CD10�,CD19þ, CD20þ, CD23�) thatsatisfactorily excludes otherlymphoproliferative disordersincluding chronic lymphocyticleukemia and mantle celllymphoma.
* Evidence of anemia, constitutionalsymptoms, hyperviscosity,lymphadenopathy, orhepatosplenomegaly that canbe attributed to the underlyinglymphoproliferative disorder.
IgM myelomaAll criteria must be met:
* Symptomatic monoclonalplasma cell proliferative disordercharacterized by a serum IgMmonoclonal protein regardlessof size
* Presence of 10% plasma cellson bone marrow biopsy
* Presence of lytic bone lesionsrelated to the underlying plasmacell disorder and/ortranslocation t(11;14) on FISH.
(Continued on the following page)
Multiple Myeloma and Its Precursors
www.aacrjournals.org Clin Cancer Res; 17(6) March 15, 2011 1247
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

progression to MM is substantially higher. Prior to theadvent of novel therapies, a randomized-controlled trialof melphalan-prednisone given initially versus at progres-sion to MM found no difference in response rate or overallsurvival (46). Furthermore, a single-arm trial using thali-domide and pamidronate in 76 patients with smolderingmyeloma failed to show a clear benefit for treatment, with aquite unexpected shorter TTP among treatment respondersversus nonresponders (47). In their report, the authorsspeculated that their observation, perhaps, was reflectinggreater drug sensitivity of more aggressive disease (47).Another randomized trial (zoledronic acid versus surveil-lance during 1 year) found reduced skeletal complicationsat progression from smoldering myeloma to MM, butwithout impact on the risk of progression (48). It isunknown whether a more extended bisphosphonate treat-ment influences the risk of progression. The study based onzoledronic acid versus surveillance was prematurely
stopped by the safety committee because of developmentof osteonecrosis of the jaw in a smoldering myelomapatient in the treatment arm (48). Currently, a rando-mized, multicenter phase III trial for patients with high-risk smoldering myeloma is ongoing in Spain (lenalido-mide-dexamethasone versus active surveillance). Aninterim analysis at 19 months of follow-up shows thatabout 50% of patients in the surveillance arm experiencedprogression to MM, whereas only 2 patients in the treat-ment arm had progression (49). A collaborative EasternCooperative Oncology Group (ECOG)–Southwest Oncol-ogy Group (SWOG) study, based on lenalidomide versusactive surveillance, just opened in the United States. Impor-tantly, at the American Society of Hematology (ASH) meet-ing in December of 2010, a few studies reported anincreased occurrence of second malignancies in MM afterextended dosing with lenalidomide, which was given asa maintenance therapy following high-dose melphalan
Table 1. Disease Definitions for the Monoclonal Gammopathies: Monoclonal Gammopathy ofUndetermined Significance and Related Disorders (Cont'd )
Type ofmonoclonalgammopathy
Premalignancy with alow risk of progression(1 to 2% per year)
Premalignancy with a high riskof progression (10% per year)
Malignancy
Light chainmonoclonalgammopathies
Light chain MGUS Idiopathic Bence Jonesproteinuria
Light chain MMb
All criteria must be met:* Abnormal FLC ratio(< 0.26 or > 1.65)
* Increased level of theappropriate involvedlight chain (increasedkappa FLC in patientswith ratio > 1.65 andincreased lambda FLCin patients with ratio < 0.26)
* No immunoglobulin heavychain expression onimmunofixation
* Clonal BMPCs < 10%, and* Absence of end-organdamage such as CRAB thatcan be attributed to theplasma cell proliferativedisorder
All criteria must be met:* Urinary monoclonal protein onurine protein electrophoresis� 500 mg/24 h and/orclonal BMPCs � 10%
* No immunoglobulin heavy chainexpression on immunofixation
* Absence of end-organ damagesuch as CRAB that can beattributed to the plasma cellproliferative disorder
* Same as MM except noevidence of immunoglobulinheavy chain expression
Abbreviation: CRAB, hypercalcemia, renal insufficiency, anemia, and bone lesions.aOccasionally patients with IgD and IgE monoclonal gammopathies have been described and will be considered to be part of thiscategory as well.bNote that, conventionally, IgMMGUS is considered a subtype ofMGUS, and similarly, light chainMM is considered a subtype ofMM.Unless specifically distinguished, when the terms MGUS and MM are used, in general, they include IgM MGUS and light chain MM,respectively.Reproduced with permission from Rajkumar et al. (53).
CCR FOCUS
Clin Cancer Res; 17(6) March 15, 2011 Clinical Cancer Research1248
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

consolidation. These preliminary observations requirecareful investigation with the aim to validate the findings,and, if they are correct, to define underlying causes. Clearly,the outcome of these efforts will have direct implicationsfor the development of "long-term use" treatment strategieswith lenalidomide in MM and SMM. Furthermore, at theNCI in Bethesda, Maryland, novel treatment strategies(designed to facilitate the patient’s own immune system,to achieve antimyeloma effects) are under development,and the first treatment study opened in December 2010. Itis currently unknown whether treating smoldering mye-loma patients improves overall survival and/or quality oflife, as such data are not yet available. As stated above, inaccord with the International Myeloma Working Group2010 guidelines, smoldering myeloma patients should notbe treated outside of clinical trials (2).Although the above discussed trials underscore the
value of ongoing treatment trials for smoldering mye-loma patients, one can envision several scenarios result-ing from treatment of smoldering myeloma. Aimed atpreventing progression, smoldering myeloma could betreated as a chronic disease, with an extended dosingschema used to control the malignant clone (Fig. 3).Alternately, in the future, highly active therapy couldbe used with the goal of cure. However, to responsiblycarry out any such trial, well-designed correlative studies
must be done to assess for the theoretical possibility ofunexpected long-term adverse events or selecting for moreaggressive disease (Fig. 3).
Future Directions
In the context of numerous molecular events and hetero-geneous risk of progression, developing individualized riskprofiles for patients with MGUS and smoldering myelomarepresents an ongoing challenge. Clearly, we need futureprospective studies based on clinical monitoring and exten-sive correlative science. The ultimate goal is to developbetter molecular markers that will allow (i) clinicians todefine high-risk and low-risk precursor patients for a moretailored clinical management, and (ii) to provide insightson the individual patient’s disease biology, which in turncan be used for targeted andmore individualized treatmentstrategies. In the near future, it seems reasonable to believethat high-risk precursor patients will likely become candi-dates for early treatment strategies. As discussed in detail inthis review, future studies need to assess the role of earlytreatment in relation to overall survival and quality oflife (50–52). High response rates among smoldering mye-loma patients receiving treatment may not correlate withsurvival (50, 52). In fact, one may speculate that prolonged"stable disease" may provide key benefit to patients.
5%
Risk factors:
MGUS Smoldering Myeloma
Risk factors:20-year progression
Mayo Clinic
SpanishStudyGroup
Rate of Progression to Multiple Myeloma (%)
5-year progression 5-year progression
5-year progression
58% 76%
72%46%
4%
51%25%
32
01
321
2
01
2
0
0 020 2040 4060 6080 80100
1
37%21%
46%10%
2%
- M-protein ≥1.5 g/dL- Non-lgG MGUS- Free light-chain ratio <0.26 or >1.65
- M-protein ≥3 g/dL- ≥10% clonal bone marrow plasma cells- Free light-chain ratio <0.125 or >8
- ≥95% abnormal plasma cells- Immunoparesis
- ≥95% abnormal plasma cells- DNA aneuploidy
© 2011 American Association for Cancer Research
Figure 2. Risk stratification schemes for MGUS (left) and smoldering myeloma (right). Two major models for risk stratification have been proposed: onemodel by the Mayo Clinic and the other by the Spanish study group (PETHEMA). The Mayo Clinic model focuses largely on serum protein abnormalities.For MGUS patients, the following features are considered as adverse risk factors: non-IgG isotype, M-protein concentration � 1.5 g/dL, and an abnormalserum FLC ratio (normal reference 0.26 to 1.65; ref. 25). For smoldering myeloma patients, the following features are considered to be adverse risk factors:�3g/dL M protein, an FLC ratio outside the reference range of 0.125 to 8, and �10% BMPCs (12, 26). The Spanish model uses multiparametric flowcytometry of bone marrow aspirates to differentiate aberrant from normal plasma cells (27). Plasma cells characteristically express CD138 and intense(bright) CD38. The features of aPCs included decreased CD38 expression, expression of CD56, and the absence of CD19 and/or CD45. In their study,MGUS and smoldering myeloma patients with �95% phenotypically aPC of total BMPC (i.e., �95% aPC/BMPC) at diagnosis had a significantly higher riskof MM progression (27). Furthermore, on multivariate analysis, �95% aPCs/BMPC, DNA aneuploidy, and immunoparesis were found to be independentpredictors of MM progression from MGUS and/or smoldering myeloma. More specifically, for MGUS patients �95% aPCs/BMPC and DNA aneuploidywere found to be risk factors for progression. For smoldering myeloma patients, the risk factors were �95% aPCs/BMPC and immunoparesis (27).
Multiple Myeloma and Its Precursors
www.aacrjournals.org Clin Cancer Res; 17(6) March 15, 2011 1249
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Currently, the answers to these important questions remainunknown.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
We thank Irina Maric, MD, at the NIH, Bethesda, Maryland forproviding the pictures in Figure 1. We also acknowledge Adam J.
Waxman, BA, at the NCI, Bethesda, Maryland for comments and sugges-tions about Figures 2 and 3.
Grant Support
This work was supported by the Intramural Research Program of the NCI ofthe NIH; the grants CA 62242 and CA 107–476-03 from the NCI; and the facilitiesand resources of the Divisions of Hematology, Biostatistics, Clinical Biochem-istry and Immunology, and Epidemiology at the Mayo Clinic, Rochester,Minnesota.
ReceivedOctober 11, 2010; revisedDecember 29, 2010; accepted January21, 2011; published online March 16, 2011.
References1. Kyle RA, Therneau TM, Rajkumar SV, Larson DR, Plevak MF, Offord
JR, et al. Prevalence of monoclonal gammopathy of undeterminedsignificance. N Engl J Med 2006;354:1362–9.
2. Kyle RA, Durie BGM, Rajkumar SV, Landgren O, Blade J, Merlini G,et al. International Myeloma Working Group. Monoclonal gammopa-thy of undetermined significance (MGUS) and smoldering (asympto-matic) multiple myeloma: IMWG consensus perspectives risk factorsfor progression and guidelines for monitoring and management.Leukemia 2010;24:1121–7.
3. Kyle RA, Therneau TM, Rajkumar SV, Offord JR, Larson DR, PlevakMF, et al. A long-term study of prognosis in monoclonal gammopathyof undetermined significance. N Engl J Med 2002;346:564–9.
4. Bida JP, Kyle RA, Therneau TM, Melton LJ 3rd, PlevakMF, Larson DR,et al. Disease associations with monoclonal gammopathy of unde-termined significance: a population-based study of 17,398 patients.Mayo Clin Proc 2009;84:685–93.
5. Rajkumar SV. Prevention of progression in monoclonal gammopathyof undetermined significance. Clin Cancer Res 2009;15:5606–8.
6. Landgren O, Gridley G, Turesson I, Caporaso NE, Goldin LR, Baris D,et al. Risk of monoclonal gammopathy of undetermined significance(MGUS) and subsequent multiple myeloma among African Americanand white veterans in the United States. Blood 2006;107:904–6.
7. Landgren O, Katzmann JA, Hsing AW, Pfeiffer RM, Kyle RA, YeboahED, et al. Prevalence of monoclonal gammopathy of undeterminedsignificance among men in Ghana. Mayo Clin Proc 2007;82:1468–73.
8. Iwanaga M, Tagawa M, Tsukasaki K, Kamihira S, Tomonaga M.Prevalence of monoclonal gammopathy of undetermined signifi-cance: study of 52,802 persons in Nagasaki City, Japan. Mayo ClinProc 2007;82:1474–9.
9. Ruiz-Delgado GJ, Ruiz-Arg€uelles GJ. Genetic predisposition formonoclonal gammopathy of undetermined significance. Mayo ClinProc 2008;83:601–2, author reply 602–3.
10. Vachon CM, Kyle RA, Therneau TM, Foreman BJ, Larson DR, ColbyCL, et al. Increased risk of monoclonal gammopathy in first-degreerelatives of patients with multiple myeloma or monoclonal gammo-pathy of undetermined significance. Blood 2009;114:785–90.
11. Landgren O, Kyle RA, Hoppin JA, Beane Freeman LE, James R,Cerhan JR, et al. Pesticide exposure and risk of monoclonal gammo-pathy of undetermined significance (MGUS) in the Agricultural HealthStudy. Blood 2009;25:6386–91.
12. Kyle RA, Remstein ED, Therneau TM, Dispenzieri A, Kurtin PJ, Hodne-field JM, et al. Clinical course and prognosis of smoldering (asympto-matic) multiple myeloma. N Engl J Med 2007;356:2582–90.
Figure 3. Treatment goals insmoldering myeloma. Underactive surveillance, patients withhigh-risk smoldering MM have a>84% lifetime risk of progressionto full-blown myeloma (52). Onecan envision several scenariosresulting from treatment of SMM.Aimed at preventing progression,SMM could be treated as achronic disease, with relativelybenign maintenance therapy usedto control the malignant clone.Alternately, highly active therapycould be used with the goalof cure, though this may provechallenging in the context ofcurrent treatment options.However, to responsibly do anysuch trial, well-designedcorrelative studies should be doneto assess for the theoreticalpossibility of unexpected long-term adverse events or selectingfor more aggressive disease.
CCR FOCUS
Clin Cancer Res; 17(6) March 15, 2011 Clinical Cancer Research1250
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

13. Lust JA, Lacy MQ, Zeldenrust SR, Dispenzieri A, Gertz MA, Witzig TE,et al. Induction of a chronic disease state in patients with smolderingor indolent multiple myeloma by targeting interleukin 1{beta}-inducedinterleukin 6 production and the myeloma proliferative component.Mayo Clin Proc 2009;84:114–22.
14. Kyle RA. Monoclonal gammopathy of undetermined significance.Natural history in 241 cases. Am J Med 1978;64:814–26.
15. Kyle RA, Rajkumar SV. Criteria for diagnosis, staging, risk stratificationand response assessment of multiple myeloma. Leukemia 2009;23:3–9.
16. Kyle RA, Therneau TM, Rajkumar SV, Remstein ED, Offord JR, LarsonDR, et al. Long-term follow-up of IgM monoclonal gammopathy ofundetermined significance. Blood 2003;102:3759–64.
17. Schuster SR, Rajkumar SV, Dispenzieri A, Morice W, Aspitia AM,Ansell S, et al. IgM multiple myeloma: disease definition, prognosis,and differentiation from Waldenstrom's macroglobulinemia. Am JHematol 2010;85:853–5.
18. Dispenzieri A, Katzmann JA, Kyle RA, Larson DR,Melton LJ 3rd, ColbyCL, et al. Prevalence and risk of progression of light-chain monoclonalgammopathy of undetermined significance: a retrospective popula-tion-based cohort study. Lancet 2010;375:1721–8.
19. Kyle R, Therneau T, Dispenzieri A, Larson D, Plevak M, Melton LJIII, et al. Idiopathic Bence Jones proteinuria: clinical courseand prognosis. Blood (ASH Annual Meeting Abstracts) 2006;108:3493.
20. Kyle RA, Maldonado JE, Bayrd ED. Idiopathic Bence Jones protei-nuria—a distinct entity? Am J Med 1973;55:222–6.
21. Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A, et al.Review of 1027 patients with newly diagnosed multiple myeloma.Mayo Clin Proc 2003;78:21–33.
22. Gobbi PG, Baldini L, Broglia C, GoldanigaM, Comelli M, Morel P, et al.Prognostic validation of the international classification of immuno-globulin M gammopathies: a survival advantage for patients withimmunoglobulin M monoclonal gammopathy of undetermined sig-nificance? Clin Cancer Res 2005;11:1786–90.
23. Baldini L, Goldaniga M, Guffanti A, Broglia C, Cortelazzo S, Rossi A,et al. Immunoglobulin M monoclonal gammopathies of undeterminedsignificance and indolent Waldenstrom's macroglobulinemia recog-nize the same determinants of evolution into symptomatic lymphoiddisorders: proposal for a common prognostic scoring system. J ClinOncol 2005;23:4662–8.
24. Gertz MA, Ansell SM, Dingli D, Dispenzieri A, Buadi FK, Elliott MA,et al. Autologous stem cell transplant in 716 patients with multiplemyeloma: low treatment-related mortality, feasibility of outpatienttransplant, and effect of a multidisciplinary quality initiative. MayoClin Proc 2008;83:1131–8.
25. Rajkumar SV, Kyle RA, Therneau TM, Melton LJ 3rd, Bradwell AR,Clark RJ, et al. Serum free light chain ratio is an independent risk factorfor progression in monoclonal gammopathy of undetermined signifi-cance. Blood 2005;106:812–7.
26. Dispenzieri A, Kyle RA, Katzmann JA, Therneau TM, Larson D, BensonJ, et al. Immunoglobulin free light chain ratio is an independent riskfactor for progression of smoldering (asymptomatic) multiple mye-loma. Blood 2008;111:785–9.
27. P�erez-Persona E, Vidriales MB, Mateo G, Garcı́a-Sanz R, MateosMV, de Coca AG, et al. New criteria to identify risk of progressionin monoclonal gammopathy of uncertain significance and smolder-ing multiple myeloma based on multiparameter flow cyto-metry analysis of bone marrow plasma cells. Blood 2007;110:2586–92.
28. Landgren O, Kyle RA, Pfeiffer RM, Katzmann JA, Caporaso NE, HayesRB, et al. Monoclonal gammopathy of undetermined significance(MGUS) consistently precedes multiple myeloma: a prospectivestudy. Blood 2009;113:5412–7.
29. Weiss BM, Abadie J, Verma P, Howard RS, Kuehl WM. A monoclonalgammopathy precedes multiple myeloma in most patients. Blood2009;113:5418–22.
30. Rosiñol L, Cibeira MT, Montoto S, Rozman M, Esteve J, Filella X, et al.Monoclonal gammopathy of undetermined significance: predictors ofmalignant transformation and recognition of an evolving type
characterized by a progressive increase in M protein size. Mayo ClinProc 2007;82:428–34.
31. Landgren O, Waxman AJ. Multiple myeloma precursor disease. JAMA2010;304:2397–404.
32. Munshi NC, Avet-Loiseau H. Genomics in multiple myeloma. ClinCancer Res 2011;17:1234–42.
33. Fonseca R, Barlogie B, Bataille R, Bastard C, Bergsagel PL, Chesi M,et al. Genetics and cytogenetics of multiple myeloma: a workshopreport. Cancer Res 2004;64:1546–58.
34. Rajkumar SV, Lacy MQ, Kyle RA. Monoclonal gammopathy of unde-termined significance and smoldering multiple myeloma. Blood Rev2007;21:255–65.
35. Chiecchio L, Protheroe RK, Ibrahim AH, Cheung KL, Rudduck C,Dagrada GP, et al. Deletion of chromosome 13 detected by conven-tional cytogenetics is a critical prognostic factor in myeloma. Leuke-mia 2006;20:1610–7.
36. Bergsagel PL, Kuehl WM, Zhan F, Sawyer J, Barlogie B, ShaughnessyJ Jr. Cyclin D dysregulation: an early and unifying pathogenic event inmultiple myeloma. Blood 2005;106:296–303.
37. Fonseca R, Bailey RJ, Ahmann GJ, Rajkumar SV, Hoyer JD, Lust JA,et al. Genomic abnormalities in monoclonal gammopathy of unde-termined significance. Blood 2002;100:1417–24.
38. Mantovani A, Garlanda C. Inflammation and multiple myeloma: theToll connection. Leukemia 2006;20:937–8.
39. Chng WJ, Glebov O, Bergsagel PL, Kuehl WM. Genetic events in thepathogenesis of multiple myeloma. Best Pract Res Clin Haematol2007;20:571–96.
40. Annunziata CM, Davis RE, Demchenko Y, BellamyW, Gabrea A, ZhanF, et al. Frequent engagement of the classical and alternativeNF-kappaB pathways by diverse genetic abnormalities in multiplemyeloma. Cancer Cell 2007;12:115–30.
41. Balakumaran A, Robey PG, Fedarko N, Landgren O. Bone marrowmicroenvironment in myelomagenesis: its potential role in early diag-nosis. Expert Rev Mol Diagn 2010;10:465–80.
42. Melton LJ 3rd, Rajkumar SV, Khosla S, Achenbach SJ, Oberg AL, KyleRA. Fracture risk in monoclonal gammopathy of undetermined sig-nificance. J Bone Miner Res 2004;19:25–30.
43. Bataille R, Chappard D, Basle MF. Quantifiable excess ofbone resorption in monoclonal gammopathy is an early symptomof malignancy: a prospective study of 87 bone biopsies. Blood1996;87:4762–9.
44. Politou M, Terpos E, Anagnostopoulos A, Szydlo R, Laffan M, LaytonM, et al. Role of receptor activator of nuclear factor-kappa B ligand(RANKL), osteoprotegerin and macrophage protein 1-alpha (MIP-1a)in monoclonal gammopathy of undetermined significance (MGUS). BrJ Haematol 2004;126:686–9.
45. Raje N, Roodman GD. Advances in the biology and treatment of bonedisease in multiple myeloma. Clin Cancer Res 2011;17:1278–86.
46. Hjorth M, Hellquist L, Holmberg E, Magnusson B, R€odjer S, WestinJMyeloma Group of Western Sweden. Initial versus deferredmelphalan-prednisone therapy for asymptomatic multiplemyeloma stage I—a randomized study. Eur J Haematol 1993;50:95–102.
47. Barlogie B, van Rhee F, Shaughnessy JD Jr, Epstein J, Yaccoby S,Pineda-Roman M, et al. Seven-year median time to progression withthalidomide for smoldering myeloma: partial response identifies sub-set requiring earlier salvage therapy for symptomatic disease. Blood2008;112:3122–5.
48. Musto P, Petrucci MT, Bringhen S, Guglielmelli T, Caravita T, Bon-garzoni V, et al. GIMEMA (Italian Group for Adult Hematologic Dis-eases)/Multiple Myeloma Working Party and the Italian MyelomaNetwork. Amulticenter, randomized clinical trial comparing zoledronicacid versus observation in patients with asymptomatic myeloma.Cancer 2008;113:1588–95.
49. Mateos MV, Lopez-Corral L, Hernandez MT, de la Rubia J, LahuertaJJ, Giraldo P, et al. Multicenter, randomized, open-label, phase III trialof lenalidomide-dexamethasone (Len/dex) vs therapeutic abstentionin smoldering multiple myeloma at high risk of progression to symp-tomatic MM: results of the first interim analysis. Blood (ASH AnnualMeeting Abstracts)2009;114:614.
Multiple Myeloma and Its Precursors
www.aacrjournals.org Clin Cancer Res; 17(6) March 15, 2011 1251
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

50. Palumbo A, Attal M, Roussel M. Shifts in the therapeutic paradigm forpatients newly diagnosed with multiple myeloma: maintenance ther-apy and overall survival. Clin Cancer Res 2011;17:1253–63.
51. Lonial S, Mitsiades CS, Richardson PG. Treatment options forrelapsed and refractory multiple myeloma. Clin Cancer Res2011;17:1264–77.
52. Waxman AJ, Kuehl WM, Balakumaran A, Weiss B, Landgren O.Smoldering (asymptomatic) multiple myeloma: revisiting the clinical
dilemma and looking into the future. Clin Lymphoma Myeloma Leuk2010;10:248–57.
53. Rajkumar SV, Kyle RA, Buadi FK. Advances in the diagnosis, classi-fication, risk stratification, and management of monoclonal gammo-pathy of undetermined significance: implications for recategorizingdisease entities in the presence of evolving scientific evidence. MayoClin Proc 2010;85:945–8.
CCR FOCUS
Clin Cancer Res; 17(6) March 15, 2011 Clinical Cancer Research1252
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

2011;17:1243-1252. Clin Cancer Res Ola Landgren, Robert A. Kyle and S. Vincent Rajkumar InterventionDiagnostic Concepts and Opportunities for Early From Myeloma Precursor Disease to Multiple Myeloma: New
Updated version
http://clincancerres.aacrjournals.org/content/17/6/1243
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/17/6/1243.full#ref-list-1
This article cites 52 articles, 19 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/17/6/1243.full#related-urls
This article has been cited by 9 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/17/6/1243To request permission to re-use all or part of this article, use this link
Research. on August 1, 2020. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from