Embed Size (px)
Citation preview

Population Council, One Dag Hammarskjold Plaza, New York, New York 10017 USA e-mail: [email protected] www.popcouncil.org
over
Nokukhanya is filled with excitement andhope as she discovers she is pregnant forthe first time. Determined to give her babythe best care she can, she visits the localantenatal clinic in KwaZulu-Natal, SouthAfrica. But there she receives the crushingnews: she is HIV-positive and could poten-tially pass the infection to her unborn child.
As the counselor explains steps she can take to pro-tect her baby—things like taking medicine whileshe is pregnant and giving them to her new-
born—Nokukhanya’s head spins and her thoughts race. Allshe can focus on is how much she wants to be around towatch her baby grow, how desperately she wants her babyto be healthy, and how frightened she is of the diagnosis, oftelling her husband, and of her neighbors finding outabout her status.
To help the thousands of mothers like Nokukhanya,the mothers2mothers (m2m) program was created in SouthAfrica in 2001. The idea behind it was simple: to providemuch needed psychosocial support for women who havelearned they are HIV-positive so they can both accept theirHIV status and adhere to medical recommendations forthe prevention of mother-to-child transmission (PMTCT).
In South Africa most PMTCT services are offeredthrough government-supported health facilities that pro-vide rapid HIV testing at the first prenatal care visit andNevirapine for women in labor and for infants after deliv-ery. The facilities are now scaling up to provide dual treat-ment with AZT and Nevirapine for pregnant women andinfant testing for HIV at six weeks of age using HIV DNAPCR tests. However, despite the availability of services, thereality is that for many women, adhering to the recommen-dations is hindered by fear of stigma, lack of information,and little time for overworked health providers to offer
counseling and support services. In addition, there is weakfollow-up in the postpartum period, which means manywomen and children do not get all the services they need.
While anecdotal information suggested that m2m fillsan important gap in service provision, the program had notbeen formally evaluated until now. To determine whether itimproved the psychosocial well-being and behaviors ofwomen living with HIV, and increased the uptake ofPMTCT services, the Horizons Program, in collaborationwith Health Systems Trust, conducted an evaluation of theprogram in 2006.
The mothers2mothers ProgramBased on the concept that peer support is an effectivemodel for education and social empowerment, and thatmothers themselves are the best vehicles to provide supportto other mothers, m2m trains and employs new mothers,who have themselves benefited from PMTCT services.These “mentor mothers” participate in two weeks of train-ing that covers basic medical knowledge about HIV infec-tion and antiretroviral therapy (ART), behaviors that help
FROM MOTHER TO MOTHERA PEER MENTOR PROGRAM TO PREVENT MOTHER-TO-CHILD TRANSMISSION OF HIV IN SOUTH AFRICA OFFERS MUCH NEEDED SUPPORT
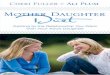
Mentor mothers are HIV-positive women who have gonethrough the PMTCT program and provide peer support.Photo credit: Courtesy of m2m

prevent mother-to-child transmission, safer feedingoptions for infants, strategies for helping women dis-close their status and negotiate safer sexual practices,and nutritional guidelines for women living with HIV.
“The program recognizes that mothers are a com-munity’s single greatest resource,” said Dr. MitchellBesser, founder of m2m. “Mentor mothers, who havegone through PMTCT services themselves, arerecruited locally and paid a stipend for the work theydo, making them professional members of the healthcare team.”
The m2m program exists in partnership withprovincial, district, and municipal initiatives to sup-port the delivery of antenatal care (ANC), HIV test-ing and counseling, and treatment services in order toprevent mother-to-child transmission of HIV.Program activities include health talks conducted inwaiting rooms to introduce new mothers to m2m,individual and group education, and regular supportgroup meetings that include nutritious lunches.Mentor mothers also conduct community outreach toassist women at home with disclosure, supportwomen in their choice of infant feeding method, pro-mote safer sex and family planning, and encouragemothers to return for wellness HIV care or treatmentand to bring their baby back to the clinic for HIVtesting and care.
The EvaluationThe study was conducted in KwaZulu-Natal, SouthAfrica’s most populous province and the one with thehighest HIV prevalence among pregnant women(approximately 39 percent). Prior to the introductionof m2m in three health facilities in the province, theresearch team used a structured survey to collect base-line data from a cross-section of 361 HIV-positivepregnant (6–9 months) and postpartum women (12weeks or less), ages 18–49, accessing services fromSeptember to November 2005. The researchers col-lected data from a second cross-sectional sample of695 HIV-positive pregnant and postpartum womenafter the program had been in place for approximatelyone year (August–October 2006).
To determine the effects of the program, theinvestigators compared data from the baseline and fol-low-up surveys and between participants and non-par-ticipants in the m2m program at follow-up. The out-comes included PMTCT knowledge, disclosure of
HIV status, receipt and ingestion of Nevirapine,infant feeding intentions and practice, family plan-ning intentions and practice, referral and follow-upfor care, and psychosocial well-being.
Exposure to the ProgramThe program achieved substantial coverage at thethree evaluation sites, with high rates of program par-ticipation by both pregnant and postpartum women.Two-thirds of the HIV-positive women interviewed atfollow-up (n = 695) reported that they had heardabout a program called “mothers2mothers.” Amongthe 345 HIV-positive pregnant women who wereinterviewed at follow-up, 6 out of 10 women reportedthat a mentor mother had talked to them. Of the 350HIV-positive postpartum women, over half reportedthat a mentor mother spoke to them during theirmost recent pregnancy, and 39 percent reported thatthis occurred after delivery. Among the postpartumwomen who established contact with a mentor moth-er, the median number of contacts was four duringpregnancy and two after delivery.
For the purpose of this study, respondents wereconsidered program participants if they spoke to amentor mother two or more times. Using that defini-tion, 42 percent of the 345 pregnant women and 49percent of the 350 postpartum women interviewedwere considered program participants at follow-up.For clarity in presenting the study results and forunderstanding the potential impact of the program,data from women who had only one contact (16 per-cent of pregnant women and 9 percent of postpartumwomen) were removed from the analyses.
Are Mentor Mothers Making a Difference?It is an explicit goal of m2m to encourage HIV-positivewomen to disclose to at least one person, as this facili-tates adherence to PMTCT recommendations. For thisreason, the women interviewed were asked whether ornot they had disclosed their status to anyone, as well aswhen and how many people they had told.
The evaluation found that postpartum womenwho had two or more contacts with m2m were sig-nificantly more likely to have disclosed to someonethan non-participants (97 percent vs. 85 percent; p <.01). Among those who disclosed, program partici-pants were more likely to have disclosed prior todelivery than non-participants (91 percent vs. 81 per-

cent; p < .05). Program participants also reported dis-closure to more people than non-participants (medi-an of 3 vs. 2).
The study also found important changes amongpostpartum women in the area of Nevirapine use.Postpartum program participants were significantlymore likely to have received Nevirapine to preventmother-to-child transmission of HIV during theirpregnancy in comparison to non-participants (95 per-cent vs. 86 percent, p < .05). In addition, the womenwho had two or more contacts with mentor motherswere significantly more likely to have ingested thedrug and to have received the infant dose ofNevirapine within three days of delivery.
In accordance with WHO recommendations,m2m does not advocate either breast or formula feed-ing but rather educates women about the importanceof selecting an exclusive feeding method, ideally dur-ing pregnancy, and then supports women’s decisionsand helps them maintain their choice post delivery.The evaluation found that postpartum program partic-ipants were more likely to report practicing an exclu-sive method of feeding (89 percent vs. 76 percent, p <
.01), with most feeding their child infant formulawithout giving breastmilk.
Postpartum program participants were significant-ly more likely to have received Nevirapine during theirpregnancy.
This result of greater adherence to recommendedfeeding practices is supported by postpartum programparticipants being more likely than non-participants tohave decided on a feeding method before delivery (87percent vs. 71 percent, p < .01). Among those whodecided on a feeding method before delivery, 9 out of10 postpartum women (both program participants andnon-participants) indicated that they were feedingtheir infant the method they had previously selected,suggesting that in this study population almost allwomen are able to execute their plans if they made adecision prior to delivery.
CD4 count is a key marker for determining eligi-bility for ARV treatment and having the test done isan important first step in accessing HIV care. Studyresults indicate that significantly more postpartumprogram participants underwent CD4 testing duringtheir last pregnancy than non-participants (79 percent
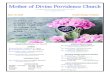
In the words of a mentor mother
“As a mentor mother I encourage women to take care ofthemselves and tell them that when you have this diseaseit’s not the end of the world. I also give them support ondifferent kinds of problems and try and come out withsolutions to the problems that they have.
“When I advise a person who has just tested andfound out that she is positive, the first thing that I tellthat person is that finding out that you are positive doesnot mean that it is written on your body—I am also pos-itive but you cannot tell. What you need to do is cry, andI know that it is difficult in the beginning to deal withfinding out about your status. The only thing that youneed to do is to accept it. I encourage that person tocome to the support group all the times so that she canlearn from other members until she is used to it.
“When I found out I was positive [and there was nom2m program] I thought that it was the end of theworld and I was going to die and leave my child behind.I thought that maybe it had been a long time since I hadthis disease. I blamed my partner for infecting me.
“The program has helped me because I know aboutmy status and about the CD4 count. They also advisedme about the kinds of food that I have to eat. I now visitthe doctor regularly. I am able to help other people and Iam no longer scared. I share the knowledge that I getfrom the mothers2mothers program with my family sothat they know what is happening and how to help mewhen I am sick.
“I am now able to support my child and my familyand I can take care of myself—as you can see I lookbeautiful. By working in the mothers program, I can saythat I have received skills for the food of the soul, to beable to advise people whenever they have a problem.”
—25-year-old mentor mother with one child

vs. 57 percent, p < .01). Logistic regression analysis fur-ther supported this relationship, as postpartum programparticipants were 3.3 times more likely to have under-gone CD4 testing during their last pregnancy comparedto non-participants (adjusted odds ratio: 3.3; 95 percentCI 1.9–5.9; p < .01).
Finally, m2m program participants reported a signif-icantly greater sense of well-being than their counterpartson several measures. More than 9 out of 10 pregnantprogram participants felt that they could do things tohelp themselves, cope with caring for their infants, andlive positively. Fewer postpartum program participantsthan non-participants reported having negative feelingssuch as feeling alone in the world, overwhelmed by prob-lems, and hopeless about the future.
ConclusionsOverall, the evaluation findings indicate that m2m playsa positive role in complementing PMTCT services byproviding psychosocial support and a continuum of carefor HIV-positive women and their infants. The study,which was conducted in a real world setting, providesvaluable quantitative data which suggest that m2m helpswomen utilize PMTCT services and follow PMTCT rec-ommendations. But limitations of the study are its lackof randomized samples and biological markers, such asPCR testing. Thus the findings from this evaluation areproxy measures for reducing vertical transmission andfurther research that directly assesses whether participa-tion in m2m contributes to lower HIV transmission ratesamong infants born to HIV-positive mothers will beimportant.
This evaluation found that postpartum women whoparticipated in the program acted to a greater extent onPMTCT recommendations than pregnant women; thismay be due to the fact that they had more contacts withm2m staff than pregnant women, and also had moretime to come to terms with living with HIV. “The find-ings among postpartum women are encouraging andsuggest that there is a dose effect, and that more contactsand time with the program may lead to greater impactfor more women,” explained Carolyn Baek ofHorizons/Population Council, principal investigator forthe study.
Results from the m2m evaluation are being widelydisseminated in the United States; South Africa; andamong researchers, donors, and stakeholders. A final report is available at www.popcouncil.org/m2mFinalReport. More information about the m2mprogram can be found at www.m2m.org.
This article was written by Hena Khan in conjunction with thestudy team which includes Carolyn Baek of Horizons/PopulationCouncil; Vuyiswa Mathambo, Sibongile Mkhize, and IrwinFriedman of Health Systems Trust; and Louis Apicella and NaomiRutenberg of Horizons/Population Council.
Reprinted from Horizons Report, June 2007www.popcouncil.org/horizons/newsletter/
horizons(14)_2.html
CONTACT [email protected] OR CALL +27 11 438 4400/7200
FOR MORE INFORMATION ABOUT THE POPULATION COUNCIL’S HORIZONS PROGRAM, VISIT WWW.POPCOUNCIL.ORG/HORIZONS
© 2007 The Population Council, Inc. www.popcouncil.org
This work was funded by the President’s Emergency Plan for AIDS Reliefand the generous support of the American people through the United StatesAgency for International Development (USAID). The opinions expressedherein are those of the authors and do not necessarily reflect the views ofUSAID.