Embed Size (px)
Citation preview

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
Clinical Investigations
From laboratory science to six EMS systems: New understandingof the physiology of cardiopulmonary resuscitation increasessurvival rates after cardiac arrest
Tom P. Aufderheide, MD; Carly Alexander, BS; Charles Lick, MD; Brent Myers, MD; Laurie Romig, MD;Levon Vartanian, MD; Joseph Stothert, MD, PhD; Scott McKnite, BS; Tim Matsuura, BA;Demetris Yannopoulos, MD; Keith Lurie, MD
Objective: The purpose of this study is to 1) describe a newly old device. Humans: Conglomerate quality assurance data werediscovered mechanism of blood flow to the brain during cardio- analyzed from six EMS systems in the United States serving apulmonary resuscitation using the impedance threshold device in population of �3 million people. There were 920 patients treateda piglet model of cardiac arrest, and 2) describe the survival for cardiac arrest after implementation of the 2005 Americanbenefits in humans of applying all of the highly recommended Heart Association Guidelines, including impedance threshold de-changes in the 2005 Guidelines related to increasing circulation vice use, and 1750 patients in the control group during the yearduring cardiopulmonary resuscitation, including use of the imped- before implementation. Demographics were similar between theance threshold device, from six EMS systems in the United States. two groups. Survival to hospital discharge was 9.3% in the control
Design: Animal studies prospective trial with each piglet serv- group versus 13.6% in the intervention group. The odds ratio, 95%ing as its own control. Historical controls were used for the confidence interval, and p values were 1.54 (1.19–1.99) and p =human studies. 0.0008, respectively. This survival advantage was conferred to
Subjects: Piglet and patients with out-of-hospital cardiac arrest. patients with a presenting cardiac arrest rhythm of ventricularInterventions: Piglets (10–12 kg) were treated with an active fibrillation (28.5% vs. 18.0%, p = 0.0008).
(n = 9) or sham (n = 9) impedance threshold device after 6 mins Conclusions: Use of the impedance threshold device in pigletsof ventricular fibrillation. Humans were treated with cardiopul- increased carotid blood flow and coronary and cerebral perfusionmonary resuscitation per the American Heart Association 2005 pressures and reduced intracranial pressure during the decom-Guidelines and the impedance threshold device. pression phase of cardiopulmonary resuscitation at a faster rate
Measurements and Main Results: Animals: The primary end- than controls, resulting in a greater duration of time when intra-point in the piglet study was carotid blood flow which increased cranial pressures are at their nadir. Patients in six EMS systemsfrom 59 mL/min without an impedance threshold device to 91 treated with the impedance threshold device together with themL/min (p = 0.017) with impedance threshold device use. Airway renewed emphasis on more compressions, fewer ventilations, andpressures during the chest recoil phase decreased from -0.46 complete chest wall recoil had a nearly 50% increase in survivalmm Hg to -2.59 mm Hg (p = 0.0006) with the active impedance rates after out-of-hospital cardiac arrest compared with historicalthreshold device. Intracranial pressure decreased more rapidly controls. (Crit Care Med 2008; 36:000–000)and to a greater degree during the decompression phase of KEY WORDS: cardiac arrest; sudden death; impedance thresholdcardiopulmonary resuscitation with the active impedance thresh- device; cerebral perfusion pressure; intracranial pressure; CPR
I t has been nearly a half a decadesince closed chest cardiopulmonaryresuscitation (CPR), also known asstandard CPR, was first described
From the Department of Emergency Medicine (TPA),Medical College of Wisconsin, Milwaukee, WI; Minneap-olis Medical Foundation (CA, SM, KL), Hennepin CountyMedical Center, Minneapolis, MN; Office of the EMSMedical Director (CL), Anoka County, MN; Office of theEMS Medical Director (BM), Wake County, NC; Office ofthe EMS Medical Director (LR), Pinellas County, FL; Officeof the EMS Medical Director (LV), Harris County, TX; Officeof the EMS Medical Director (JS), Omaha, NE; CardiacArrhythmia Center (SM, DY, KL), University of Minnesota,Minneapolis, MN; and Advanced Circulatory Systems, Inc.(KL), Eden Prairie, MN.
This work was supported by the National In-stitute of Health: SBIR Grant Number: 2-R44-
(1). Although this technique has helped tosave hundreds and thousands of peopleworldwide, cardiac output during CPR re-mains less than 20% of baseline (2, 3). Even
HL65851-02 to Advanced Circulatory Syst-ems, Inc.
The authors have not disclosed any potential con-flict of interest.
Dr. Lurie is an inventor of the impedance thresholddevice and founded Advanced Circulating Systems tobring new resuscitation technology into clinical use; heowns a patent and stock.
For information regarding this article, E-mail:[email protected]
Copyright © 2008 by the Society of Critical CareMedicine and Lippincott Williams & Wilkins
DOI: 10.1097/CCM.0b013e31818a7e56
when applied correctly, nine of every tenpatients who suffer a cardiac arrest andreceive standard CPR never survive an out-of-hospital cardiac arrest in most cities (4–6). These dismal survival rates prompted areassessment of the basic physiology ofCPR beginning in the mid-1990s. As aresult, there have been a number of impor-tant breakthroughs in the science of resus-citation (7–22). Many of these break-throughs were incorporated into the Amer-ican Heart Association Guidelines in 2005(23). These advances include a greater em-phasis on continuous chest compressionswithout interruptions (7–9), less frequentventilations (10–13), chest compressionimmediately before and after defibrillation(14–16), complete chest wall recoil (17–
Crit Care Med 2008 Vol. 36, No. 15 1

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
19), and use of a new technology called theimpedance threshold device (ITD) to har-nesses the recoil energy of chest wall de-compression to lower intrathoracic pres-sures, thereby improving the refillingprocess of the cardiac chambers (20–22).Since that time, research has continued onthe mechanism of blood flow during CPRand ways to optimize clinical outcomes(24–26). The purpose of this article was to1) describe a newly discovered mechanismof blood flow to the brain during CPR withthe ITD in a piglet model of cardiac arrest,and 2) describe the survival benefits in hu-mans of applying all of the highly recom-mended changes to increase circulationduring CPR in the 2005 Guidelines, includ-ing use of the ITD, from six EMS systems inthe United States.
MATERIALS AND METHODS
Animal Studies. The study was approved bythe Institutional Animal Care Committee ofthe Minneapolis Medical Research Foundationat Hennepin County Medical Center. Anesthe-sia was used in all surgical interventions toavoid all unnecessary suffering. Experimentswere performed by a qualified, experiencedteam. The study was performed on femalefarm piglets (10–12 kg).
Preparatory Phase. Initial sedation in eachanimal was achieved with 3 mL (100 mg/mL)of intramuscular ketamine HCl (Ketaset®,Fort Dodge Animal Health, Fort Dodge, IA).Propofol anesthesia (PropoFlo®, Abbott Labo-ratories, North Chicago, IL), (2.3 mg/kg), wasalso delivered as an intravenous (iv) bolusthrough the lateral ear vein. While spontane-ously breathing, but sedated, the piglets wereintubated with a 5.0 French endotrachealtube. Additional propofol (1 mg/kg) was thenadministered, followed by a propofol infusionof 160 fg/kg/min. The method of anesthesiaand the general surgical approach for thepreparation was previously described (10, 11).
Although the animals were sedated andmechanically ventilated, under aseptic condi-tions, a hole was drilled through the skull forintracranial pressure recordings. After identi-fying the posterior bony prominence of thepiglet’s cranium, a burr hole was made at themiddle of the distance between the left eye-brow and the posterior bony prominence. A3.5 French continuous recording microma-
®nometer pressure transducer (Mikro-TipTransducer, Millar Instruments, Houston, TX)was inserted 1 cm into the parietal lobe of theanimal and secured in place. The pressuretransducer was connected to a signal amplifier(model No. 13-6615-50, Gould InstrumentSystems, Valley View, OH) and then to a digitalrecording system (SuperScope II) providingreal time intracranial pressure (ICP) tracings.A second hole was drilled in the same way onthe right side for a second ICP transducer
(Camino, Integra Life Sciences) which wasused to calibrate the micromanometer pres-sure transducer.
Animals were then positioned supine andunilateral femoral artery cannulation was per-formed under aseptic conditions. Central aor-tic blood pressures were recorded con-tinuously, with a micromanometer-tippedcatheter (Mikro-Tip® Transducer, Millar In-struments, Houston, TX). A similar centralvenous catheter was placed in the right exter-nal jugular vein. All animals were treated withheparin bolus (100 units/kg, iv), once cathe-ters were in place. The left common carotidartery was then surgically exposed and a Dopp-ler flow probe (Transonic, 420-Series Multi-channel, transonic Systems, Ithaca, NY) wasplaced to quantify common carotid blood flow.Animals were carefully maintained at 37 ±-0.5°C using a warming blanket (Bair Hug-ger, Augustine Medical, Eden Prairie, MN) asneeded.
During the preparatory phase, animalswere ventilated with room air using a volume-control Narkomed 2A ventilator (North Amer-ican Drager, Telford, PA) with the tidal volumeof 10 mL/Kg and rate adjusted to maintain anarterial CO2 at 40 mm Hg and PaO2 of >80mmHg (oxygen saturation >95%), basedupon analysis of arterial blood gases (IL Syn-thesis, Instrumentation Laboratory, Lexing-ton, MA).
Electrocardiographic monitoring was re-corded continuously. Intratracheal pressure(ITP) was measured continuously using a mi-cromanometer-tipped catheter positioned 2cm above the trachea. All data were digitizedby a digital recording system (Superscope IIvl.295, GW Instruments, Somerville, MA)and a Power Macintosh G3® computer (Ap-ple Computer, Cupertino, CA). End tidalCO2 (ETCO2) was measured with a CO2SMOPlus® (Novametrix Medical Systems, Wall-ingford, CT).
All parameters (aortic, right atrial, intra-tracheal, intracranial, coronary perfusion, andcerebral perfusion pressures) were analyzed asfollows: discrete point measurements were ob-tained from the aortic, right atrial, ITP pres-sures measured at the level of the carina as asurrogate for intrathoracic pressure, and ICPrecordings during both compression and de-compression. Each minute of CPR was char-acterized by three sets of four measurementsmade just before a ventilation cycle evenlydistributed throughout the minute (each set20 seconds apart). Coronary perfusion pres-sures were calculated values: coronary perfu-sion pressure was calculated as the differencebetween aortic and right atrial pressures dur-ing decompression. Cerebral perfusion pres-sure was calculated as the difference betweenthe mean values of aortic pressure and ICPusing the mean value of digitalized aortic andICP recordings. ITP was also measured asminute ITP (minute-ITP): electronic data ofITP values over 1 min were transferred toMicrosoft Excel and then averaged, resulting
in the mean ITP value over the whole minuteof intervention. The slope of the ICP waveformwas evaluated by analyzing ICP tracings fromthe same 4 compression or decompression cy-cles selected for calculating the cerebral per-fusion pressure. The slope of the decompres-sion phase was analyzed as follows: the localmaximum value corresponding to compres-sion and the local minimum corresponding todecompression of each cycle were identified.The slope was calculated for the linear portionof the decent of the ICP recording by firstsubtracting 10% of the delta between the localmaximum and minimum values, since thepeak and trough portions of the recordingswere associated with a nonlinear rather thanlinear shape. The slope of the remaining linearportion curves was then calculated. By elimi-nating the upper and lower 10% of the y-component of the ICP waveform, the nonlin-ear portion of the waveform was removedallowing high fidelity between real and calcu-lated slopes.
Experimental Protocol I. Once the surgicalpreparations were completed, oxygen satura-tion was >90% and ETCO2 stable between 35and 42 mm Hg for 5 mins, ventricular fibril-lation (VF) was induced by delivering directelectrical current through a temporary pacingwire (Daig Division, St. Jude Medical,Minnetonka, MN) positioned in the right ven-tricle. At that time, a computer generated ran-domization list was used to determine thesequence of the interventions. Once VF wasinduced, the ventilator was disconnected fromthe ET tube and the dose of propofol wasreduced to 100 mcg/kg/min. After 8 min ofuntreated ventricular fibrillation, closed-cheststandard CPR was performed with a pneumat-ically driven automatic piston device (Pneu-matic Compression Controller, AMBU Inter-national, Glostrup, Denmark) as previouslydescribed (11, 27) for 6 min in all piglets. Thecompression rate was 100/min, uninterrupted,with a 50% duty cycle, and a depth of 25% ofthe anteroposterior diameter of the chest wall.The chest wall was allowed to recoil passivelybut completely with this device as the com-pression piston was actively pulled upward to apoint 0.1 cm off the chest after each compres-sion. Pressure-controlled ventilation was per-formed with a Smart Bag (O2 Systems,Toronto, CA) using 100% oxygen at a constantflow rate (10 L/min). Ventilations were initi-ated synchronously with the decompressionphase of CPR: approximately 10 mL/kg weredelivered with each breath. After 6 mins ofCPR,an active ITD (ResQPOD, Advanced Cir-culatory Systems, resistance of safety checkvalve -10 cm H2O) was added and CPR wasperformed for another 6 mins. After a total of12 mins of CPR, defibrillation was attemptedwith three successive 100-J shocks using adefibrillator (Zoll M Series, Manchester, NH).No additional supportive therapy was pro-vided, but if the pig redeveloped ventricularfibrillation spontaneously after an initiallysuccessful return of spontaneous circulation,
Crit Care Med 2008 Vol. 36, No. 15
AQ:1
2

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
ventilations when the ITD was used, ventilationduration of 1 sec/breath, a compression/ventilation ratio of 30:2 before an advanced air-way, and continuous chest compression withoutinterruption for ventilation (10 breaths/minwith a duration of 1 sec/breath) when an ad-vanced airway was placed. The ITD was deployed
additional defibrillation shocks were used. IfVF persisted after the initial three shocks, thenepinephrine was administered at a dose of 45mcg/kg and then three more shocks (100 J)were delivered. If VF still persisted thereafter,all resuscitation efforts were terminated.When resuscitation was successful, animalswere again ventilated with a Narkomed 2Amachine with a tidal volume of 10 mL/kg. Nofurther interventions were performed afterrestoration of spontaneous circulation. Thirtyminutes after resuscitation, the animals werekilled using an intravenous bolus of propofol60 mg and then 10 M KCl.
Experimental Protocol II. After an analysisof the initial animal study results, a secondseries of piglet studies were performed, butinstead of using an active ITD after 8 mins ofuntreated ventricular fibrillation and 6 minsof CPR, a sham ITD was used instead. Similarto the first series of studies, efforts were madeto defibrillate the piglets after a total of 12mins of CPR.
The analysis of all the parameters duringthe two different intervention protocols wasperformed after averaging data from all ani-mals and calculating the mean. With thisapproach, sequence effects and potentialchanges in key parameters over time wereminimized. CPR was performed continuouslyfor a total of 12 mins. Aortic pressure, rightatrial pressure, ICP, intratracheal pressure,ETCO2, and O2 saturation were measured con-tinuously. Arterial blood gases were sampledbefore ventricular fibrillation was induced andafter 5.5 and 11.5 mins of CPR.
Statistical Analysis. Values are expressedas mean ± SEM. The primary endpoint wascarotid blood flow. Additional measurementsincluded mean arterial pressures, ICP, coro-nary and cerebral perfusion pressures, theslope of the ICP curves, arterial oxygen satu-ration, and arterial partial pressure of oxygen.A paired Student’s t test was used to determinestatistical significance between different inter-ventions. A p value of <0.05 was consideredstatistically significant.
Human Studies. Analysis and publicationof conglomerate, deidentified quality assur-ance data described in this evaluation was ap-proved by Institutional Review Board of theMedical College of Wisconsin. Six EmergencyMedical Services (EMS) systems contributeddata to this study. They were Anoka County,MN; Harris County, TX; Pinellas County, FL;Wake County, NC; and the cities of Milwaukee,WI; and Omaha, NE. The combined sites havea population of approximately 3 million peopleand include urban, suburban, and rural set-tings. Each site deployed the ITD (ResQPOD™Advanced Circulatory Systems, Minneapolis,MN) for a minimum of 3 months durationconcurrently with manual CPR that empha-sized more compressions and fewer ventila-tions, a compression rate of 100/min, completechest wall recoil, minimum interruptions incompressions for pulse checks, a continuouslytight face mask seal during compressions and
Crit Care Med 2008 Vol. 36, No. 15
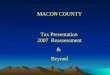
Figure 1. The means ± SEM carotid blood flow increased when the ITD was added to the respiratorycircuit after 8 mins of untreated ventricular fibrillation and 6 mins of CPR without the ITD. Theincrease was rapid and resulted in a 50% increase in carotid blood flow. ITD, impedance thresholddevice; CPR, cardiopulmonary resuscitation.
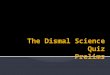
Figure 2. Two groups of piglets were subjected to 8 mins of untreated ventricular fibrillation followedby 6 mins of CPR alone and then CPR with either an active or a sham ITD. Carotid blood flow increasedafter addition of an active ITD in protocol I but did not change after adding a sham ITD in ProtocolII. ITD, impedance threshold device; CPR, cardiopulmonary resuscitation.
3
on both the face mask and an endotracheal tube,or other means to secure the airway including aCombiTube™ or Laryngeal Mask Airway(LMA™). For the purposes of this article, thisphysiologically based approach to optimizingcirculation during CPR will be referred to as“new” CPR. The key aspects of new CPR, includ-

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
ing use of the ITD, are highly recommended(level I or IIa Recommendations) in the 2005American Heart Association Guidelines. TheEMS systems selected for this report had themost extensive clinical experience with the ITDand new CPR at the time the data were pooled.
Patients were included in this analysis ifthey were presented with a cardiac arrest, re-ceived CPR by EMS personnel, and met localcriteria for ITD use. Criteria for ITD use var-ied: it was applied in patients :12 yrs of ageand deployed on a face mask in five of sixsystems. Patients who presented in cardiacarrest secondary to a presumed noncardiacetiology (e.g., blunt or penetrating trauma)were excluded from this analysis. For the pur-pose of this study, patients who presented withburns or electrocution were included in theanalysis.
Historical or concurrent control data wereused for comparison in this evaluation. His-torical controls were derived from patientsusing matching local criteria for ITD use dur-ing a 1 year period before ITD implementationHospital discharge data were available from allsites.
Pooled conglomerate data were analyzedfor statistically significant differences betweenthe historical control and study population.Odds ratios, 95% confidence intervals, and pvalues were calculated.
RESULTS
Animal Studies. To determine the po-tential for the ITD to increase forwardblood flow to the brain and to lower ICPduring the decompression phase of CPR,carotid blood flow and ICP were mea-sured in nine piglets undergoing contin-uous chest compressions in the absenceand then the presence of an ITD with aresistance of -10 cm H2O. Application ofthe ITD resulted in a decrease in airwaypressures (in mm Hg) from -0.71 ± 0.23(SEM) to -2.76 ± 0.45 and in a rapidincrease in carotid blood flow, as shown
F1 in Figure 1, compared with flow duringthe first 6 min epoch without the ITD. Acomparison of the effect of an active ver-sus sham ITD on carotid blood flow com-paring protocols I and II is shown in
F2 Figure 2. There was no change in airwaypressures or carotid flow with the appli-cation of the sham ITD.
To further explore the mechanism ofITD effect on blood flow to the brain, ICPwas measured along with the change inICP during the decompression phase ofCPR. ICP, measured with a pressuretransducer located in the parietal lobe,decreased more rapidly and to a greaterdegree during the decompression phaseof CPR when the ITD was used comparedwith no ITD, as shown in a representative
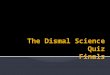
Figure 3. Piglets were subjected to 8 mins of untreated ventricular fibrillation followed by 6 mins ofCPR alone and then CPR with either an active or a sham ITD. The effect of adding an active (a) or asham (b) ITD on changes in airway pressures (ITP), carotid blood flow (flow in pink), aortic pressure(Ao in blue), right atrial pressure (RA in black), and intracranial pressure (ICP in pink) are shown inthese representative figures. The data are shown after 6 min of CPR alone and then at 8 min, 2 minsafter addition of the active ITD (a) or a sham ITD (b). The change in the slope of the ICP curves arehighlighted by the red line and the actual values are shown below each figure. When the active ITDis added to the respiratory circuit, there is a more rapid decrease in the slope of the ICP curve duringthe decompression phase of CPR resulting in less resistance to forward blood flow for a longer periodof time (a). This effect was not observed with the addition of the sham ITD in b. These figures alsohighlight the decreases observed during the chest wall recoil phase of the airway pressure curves withthe addition of the active ITD (labeled ITP for intrathoracic pressure in green) in the top panels. Thiseffect is absent with the sham ITD.
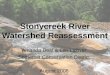
graph in Figure 3. The slope of the ICP Coronary and cerebral perfusion pres- F3
pressure curves during the decompres- sures were calculated to further demon-sion phase of CPR was, on average, 19% strate the ITD effect in the piglets: bothsteeper resulting in a significantly longer were significantly higher with the activeperiod of time that the cerebral perfusion ITD compared with no ITD, as shown inpressures were higher compared with no Figure 4a and b, respectively.ITD. The mean slope values (±SEM) dur- Human Studies. There were 1750 pa-ing the decompression phase of CPR be- tients who had a cardiac arrest in thefore and after addition of the active ITD in control group during the year before im-protocol I was -0.95 ± 0.09 and plementation of new CPR and the ITD.-1.14 ± 0.12, p = 0.001), respectively. During new CPR and the ITD, a total ofBy comparison, the mean slope values 920 patients were evaluated. The ratio ofwere similar before (-0.85 ± 0.08) and male to female patients was similar inafter the sham ITD (0.88 ± 0.08) (p = both groups, 65% of the patients wereNS) was used in protocol II. male. The average age was also similar in
F4
Crit Care Med 2008 Vol. 36, No. 154

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
Figure 4. Piglets were subjected to 8 mins of untreated ventricular fibrillation followed by 6 mins ofCPR alone and then CPR with either an active or a sham ITD and the coronary (a) and cerebral (b)perfusion pressures were compared. Adding an active ITD (a) resulted in a statistically significantincrease in coronary perfusion pressures (calculated by subtracting the right atrial pressure from theaortic pressure during the decompression phase of CPR). By contrast, coronary perfusion pressurestrended lower after adding a sham ITD (a). Similarly, adding an active ITD resulted in a statisticallysignificant increase in cerebral perfusion pressures (b) (difference between mean arterial pressure andintracranial pressure) whereas addition of the sham ITD had no benefit.
both groups at 64 yrs of age. Survival to Survival to hospital discharge was alsohospital discharge was 9.3% in the con- evaluated based on presenting rhythm.trol group versus 13.6% in the interven- For patients with an initial rhythm oftion group. The odds ratio, 95% confi- ventricular fibrillation, survival to hospi-dence interval, and p values were 1.54, tal discharge rates were 18.0% (81/450)1.19–1.99, and p = 0.0008, respectively. in the control group and 28.5% (84/295)
in the new CPR and ITD group (p =0.0008). For patients with an initial rhythmof either asystole or pulseless electrical ac-tivity, hospital discharge rates were 6.2%(81/1300) in the control group and 6.6%(41/635) in the new CPR and ITD group(p = NS).
DISCUSSION
The physiology underlying the benefi-cial effects, as well as the clinical role, ofthe ITD have continued to evolve sincethe concept of lowering intrathoracicpressures during chest wall decompres-sion to augment vital organ perfusionwas first described over a decade ago (28–30). The ITD was initially thought to in-crease circulation to the heart and brainby augmenting venous return to theheart (20, 21). This mechanism was pre-viously supported by a number of animalstudies performed with both standardmanual CPR and active compression de-compression CPR (27, 30).
New data from the current study aswell as data from ongoing animal andclinical studies provide support of an ad-ditional mechanism of action: an activeITD lowers intracranial pressures fasterand to a greater magnitude with eachchest wall recoil when compared withsham controls. More specifically, there isan instantaneous reduction in intracra-nial pressures at a faster rate with theactive ITD than with a sham ITD, therebyallowing for a greater duration of timewhen intracranial pressures are at theirnadir. Because intracranial pressure is amajor determinant of resistance to for-ward flow to the brain, the more rapidreduction in intracranial pressure by theITD further enhances cerebral circula-tion.
The results of these piglet studies sup-port a dual mechanism for the increase incirculation previously reported by usingthe ITD in animals. The first is the aug-mentation in cardiac output by greaterrefilling of the cardiac chambers duringCPR. The second is a reduction in intra-cranial pressure secondary to thoraco-cranial interactions. These data helpexplain the marked improvement inneurologic outcomes previously reportedin pigs treated with an active ITD com-pared with sham-treated controls aftercardiac arrest (30). The mechanism ofpressure transference is most likely viathe spinal column as shown by Guerci etal. (31) in studies on how positive pres-sure ventilation causes an instantaneous
Crit Care Med 2008 Vol. 36, No. 15 5

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
increase in intracranial pressure. The pression/flash) (25). Given the adverse ef- during CPR. Although this is only onecurrent studies are the first demonstra- fects of these common errors in CPR per- step in the overall sequence of care es-tion of how a reduction in intrathoracic formance on the efficacy of the ITD in sential to long-term success, it is thepressure generated with the ITD result in patients undergoing CPR, implementa- most fundamental first step. Treatinga more rapid reduction in intracranial tion of the ITD in the United States was cardiac arrest is like treating other com-pressures. These relationships are funda- performed concurrently with a strong plex and lethal diseases; the treatmentmental for understanding how to opti- emphasis on how to correctly perform requires multiple synergistic therapies.mize blood flow to the brain during CPR CPR. This implementation process incor- For example, optimizing hospital-basedand how to reduce errors that may cause porated re-teaching rescue personnel care of the resuscitated patient is equallyan increase in intrathoracic pressure and how to perform CPR including 1) venti- important, but not yet widely applied.compromise blood flow to the brain (10, lating at the proper compression/ventila- Two of the sites in this clinical evaluation17–19). tion frequency of 30:2 for Basic Life Sup- began to use therapeutic hypothermia
Just as the mechanism of action of the port when using a face mask and the ITD, during the course of implementing newITD has continued to become clearer, so 2) maintaining a continuously tight face- CPR and the ITD, and, as such, one thirdis the role of the ITD as it continues to mask seal during compressions and ven- of the survivors from Anoka County, MNbecome integrated into the care of pa- tilations using a two-handed technique and Wake County, NC received the addedtients in cardiac arrest. An initial, double- throughout the entire BLS phase, 3) al- benefits of therapeutic hypothermia. Theblind, randomized clinical trial demon- lowing for full chest wall recoil by a slight authors believe therapeutic hypothermiastrated that the ITD doubled systolic alteration in the hand position so that the is an additional essential therapy forblood pressure in cardiac arrest patients palm of the hand lifts slightly but com- those patients who remain comatose after(21). That trial was equally significant for pletely off the chest each time the chest a return of spontaneous circulation, andidentifying some of the common and le- recoils, 4) continuous chest compres- represents incompletely utilized potentialthal errors associated with the perfor- sions without interruption for ventilation to even further improve outcome (32, 33).mance of CPR (10, 17). The first error was once an advanced airway was placed, and There are several limitations to thesethat patients are frequently ventilated at 5) CPR for 90 to 180 secs before delivery animal and human investigations. Theexcessive rates, which in turn cause of a shock. Implementing CPR immedi- animal protocols are limited in that nohigher intrathoracic pressures for a ately after a shock was also emphasized. microphere or long-term survival studiesgreater duration of the CPR cycles. The When the ITD was introduced for clinical were performed. As such, the correlationhigher intrathoracic pressures reduce use, these key elements of proper CPR between improved cerebral blood flowcardiac filling, increase intracranial pres- were highlighted during the training ses- with ITD use and survival is lacking.sures, and result in a decrease in coro- sions with first responders and Advanced However, both of these parameters havenary and cerebral perfusion pressures, Life Support personnel. been previously evaluated in 30 kg pigswhich in turn markedly reduce the like- This study, comprising a population (27–30). Those studies showed a doublinglihood of survival (10). The second major base of greater than 3 million people, is of blood flow to the brain with the ITDerror, which has an equally detrimental the first to demonstrate that when CPR is and a dramatic improvement in neuro-effect, is that rescuers often fail to allow performed correctly and the ITD is simul- logically intact survival rates (27–30).the chest to fully recoil after each com- taneously deployed, there is a >50% in- The human studies are limited in thatpression (17). This also results in higher crease in survival to hospital discharge historical controls were used and neuro-intrathoracic pressures during the de- rates when compared with historical con- logic outcome data were not available atcompression phase of CPR which, in trols (13.6% vs. 9.3%, p = 0.0008%) (Ta- the time of this writing for most of theturn, reduces venous blood flow back to ble 1). This survival advantage was con- sites. In addition, the human studies have T1
the heart and increases intracranial pres- ferred to patients with a presenting the inherent limitation that the beneficialsures. As with excessive ventilation rates, cardiac arrest rhythm of ventricular fi- effects of the ITD cannot be attributed toincomplete chest wall recoil reduces vital brillation (28.5% vs. 18.0%, p = 0.0008). any single intervention but only the com-organ blood flow and reduces the likeli- Differences for patients with non-VF bination of interventions. This was inten-hood of survival (17–19). In pigs, the rhythms were not statistically significant tional, and follows advances in othercombination of incomplete chest wall re- (6.6% vs. 6.2%, p = NS). deadly disease states requiring multiplecoil and positive pressure ventilation ef- The findings demonstrate potential for synergistic therapies. This new approachfectively reduces cerebral perfusion pres- increasing survival rates after cardiac ar- is important conceptually, and suggestssure to zero (18). rest by augmenting vital organ blood flow that while different interventions may
The correction of these life-threaten-ing errors has been an important contri-bution to the field of CPR and has helped
Table 1. Hospital discharge rates in control and intervention groups
to reshape to the 2005 American Heart InterventionAssociation Guidelines (23). Further- (“new CPR” + ITD)more, the ITD was redesigned to incor- Parameter Control Group Group p OR (95% CI)porate a timing light that flashes 10times/min at 1 sec/flash to provide rescuepersonnel with a visual cue when to pro-vide a positive pressure ventilation, anappropriate ventilation duration, and
Hospital discharge 9.3% (n = 1750) 13.6% (n = 920) 0.0008 1.541 (1.192–1.990)Hospital discharge (VF) 81/450 (18.0%) 84/295 (28.5%) 0.0008 1.814 (1.259–2.610)Hospital discharge
(non-VF)81/1300 (6.2%) 41/635 (6.6%) 0.7655 1.057 (0.698–1.579)
how often to compress the chest (10 com- VF, ventricular fibrillation; CPR, cardiopulmonary resuscitation; ITD, impedance threshold device.
6 Crit Care Med 2008 Vol. 36, No. 15

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
have benefit in and by themselves, thegreatest clinical benefit will come fromcombining multiple therapies together ina physiologic sound manner. No new cir-culatory technology (including the ITD)will be of maximum benefit unless it isused in a system that optimizes the en-gine (e.g., high quality CPR) that drivescirculation in the first place. Finally, dif-ferences from site to site in both thenumber of patients evaluated and the im-pact of new CPR plus the ITD were par-ticularly notable in patients with non-VFrhythms. In some sites, there was a con-sistent increase in the number of patientswho survived to hospital discharge withan initial non-VF rhythm but this effectwas not observed in the site with thelargest number of patients evaluated.Consequently, there was no increase insurvival to hospital discharge for non-VFpatients when the data were analyzed inaggregate.
The authors believe that as we con-tinue to better understand the physiologyof CPR and how to maximize postresus-citation care, the approaches describedherein have the potential for even greaterimprovements in outcomes. Althoughonly a few patients in the current studywere treated in the postresuscitationphase with therapeutic hypothermia, webelieve this advance will help to reducethe striking mortality rates that occur forpatients after they have been admitted tothe hospital. Thus, the results presentedherein represent an important first stepin overhauling how CPR and postresusci-tation care can and should be providedfor all patients in cardiac arrest. The se-quence of care, including use of new CPRand the ITD represent the best care avail-able today to optimize circulation and thechance for survival. These data providestrong support for physiologic and clini-cal advances of this new approach to thetreatment of patients in cardiac arrest.
CONCLUSIONS
These studies identify a new mecha-nism for improving cerebral perfusionduring CPR. Use of the ITD reduces in-tracranial pressure during the decom-pression phase of CPR at a faster rate,resulting in a greater duration of timewhen intracranial pressures are at theirnadir, thereby enhancing cerebral circu-lation. We also provide the first evidencethat consistently implementing a seriesof interventions (including use of theITD), as recommended by the AHA
Crit Care Med 2008 Vol. 36, No. 15
Guidelines, can result in a nearly 50%increase in survival to hospital dischargerate.
REFERENCES
1. Kouwenhoven WB, Jude JR, KnickerbockerGG: Closed chest cardiac massage. JAMA1960; 173:1064–1067
2. Duggal C, Weil MH, Gazmuri RJ, et al: Re-gional blood flow during closed-chest cardiacresuscitation in rats. J Appl Physiol 1993;74:147–152
3. Andreka P, Frenneaux MP: Haemodynamicsof cardiac arrest and resuscitation. Curr OpinCrit Care 2006; 12:198–203
4. Niemann JT: Cardiopulmonary resuscitation.N Engl J Med 1992; 327:1075–1090
5. Eisenberg MS, Horwood BT, Cummins RO,et al: Cardiac arrest and resuscitation: A taleof 29 cities. Ann Emerg Med 1990; 19:179–186
6. Becker L, Ostrander M, Barrett J, et al: Out-come of cardiopulmonary resuscitation in alarge metropolitan area: Where are the sur-vivors? Ann Emerg Med 1991; 20:355–361
7. Wik L, Kramer-Johansen J, Myklebust H, etal: Quality of cardiopulmonary resuscitationduring out-of-hospital cardiac arrest. JAMA2005; 293:299–304
8. Abella BS, Alvarado JP, Myklebust H, et al:Quality of cardiopulmonary resuscitationduring in-hospital cardiac arrest. JAMA 2005;293:305–310
9. Iwami T, Kawamura T, Hiraide A, et al: Ef-fectiveness of bystander-initiated cardiac-only resuscitation for patients with out-of-hospital cardiac arrest. Circulation 2007;116:2900–2907
10. Aufderheide TP, Sigurdsson G, Pirrallo RG,et al: Hyperventilation-induced hypotensionduring cardiopulmonary resuscitation.Circulation 2004; 109:1960–1965
11. Yannopoulos D, McKnite SH, Tang W, et al:Reducing ventilation frequency during car-diopulmonary resuscitation in a porcinemodel of cardiac arrest. Respir Care 2005;50:628–635
12. Yannopoulos D, Aufderheide TP, Gabrielli A,et al: Clinical and hemodynamic comparisonof 15:2 and 30:2 compression-to-ventilationratios for cardiopulmonary resuscitation.Crit Care Med 2006; 34:1444–1449
13. Yannopoulos D, Sigurdsson G, McKnite S, etal: Reducing ventilation frequency combinedwith an inspiratory impedance device im-proves CPR efficiency in swine model of car-diac arrest. Resuscitation 2004; 61:75–82
14. Cobb LA, Fahrenbruch CE, Walsh TR, et al:Influence of cardiopulmonary resuscitationprior to defibrillation in patients with out-of-hospital ventricular fibrillation. JAMA 1999;281:1182–1188
15. Wik L, Hansen TB, Fylling F, et al: Delayingdefibrillation to give basic cardiopulmonaryresuscitation to patients with out-of-hospitalventricular fibrillation: A randomized trial.JAMA 2003; 289:1389–1395
16. Jacobs IG, Finn JC, Oxer HF, et al: CPRbefore defibrillation in out-of-hospital car-diac arrest: A randomized trial. Emerg MedAustralas 2005; 17:39–45
17. Aufderheide TP, Pirrallo RG, Yannopoulos D,et al: Incomplete chest wall decompression:A clinical evaluation of CPR performance byEMS personnel and assessment of alternativemanual chest compression-decompressiontechniques. Resuscitation 2005; 64:353–362
18. Yannopoulos D, McKnite S, Aufderheide TP,et al: Effects of incomplete chest wall decom-pression during cardiopulmonary resuscita-tion on coronary and cerebral perfusion pres-sures in a porcine model of cardiac arrest.Resuscitation 2005; 64:363–372
19. Aufderheide TP, Pirrallo RG, Yannopoulos D, etal: Incomplete chest wall decompression: Aclinical evaluation of CPR performance bytrained laypersons and assessment of alterna-tive manual chest compression-decompressiontechniques. Resuscitation 2006; 71:341–351
20. Aufderheide TP, Pirrallo RG, Provo TA, et al:Clinical evaluation of an inspiratory imped-ance threshold device during standard car-diopulmonary resuscitation in patients without-of-hospital cardiac arrest. Crit Care Med2005; 33:734–740
21. Pirrallo RG, Aufderheide TP, Provo TA, et al:Effect of an inspiratory impedance thresholddevice on hemodynamics during conven-tional manual cardiopulmonary resuscita-tion. Resuscitation 2005; 66:13–20
22. Thayne RC, Thomas DC, Neville JD, et al: Useof an impedance threshold device improvesshort-term outcomes following out-of-hospital cardiac arrest. Resuscitation 2005;67:103–108
23. 2005 American Heart Association Guidelinesfor Cardiopulmonary Resuscitation andEmergency Cardiovascular Care. Circulation2005; 112 (Suppl I):IV-1–IV-203
24. Aufderheide TP. The problem with and ben-efit of ventilations: Should our approach bethe same in cardiac and respiratory arrest?Curr Opin Crit Care 2006; 12:207–212
25. Aufderheide TP, Frascone RJ, Pirrallo RG.Resuscitation in 2005: New ways to opti-mize manual CPR. EMS Magazine 2005;34:42– 45
26. Yannopoulos D, Nadkarni V, Aufderheide TP,et al: Intrathoracic pressure regulation im-proves vital organ perfusion pressures innormovolemic and hypovolemic pigs. Resus-citation 2006; 70:445–453
27. Lurie KG, Lindner KH: Recent advances incardiopulmonary resuscitation. J CardiovascElectrophysiol 1997; 8:584–600
28. Lurie KG, Mulligan KA, McKnite S, et al:Optimizing standard cardiopulmonary resus-citation with an inspiratory impedancethreshold valve. Chest 1998; 113:1084-1090
29. Lurie KG, Zielinski T, McKnite S, et al: Use ofan inspiratory impedance valve improvesneurologically intact survival in a porcinemodel of ventricular fibrillation. Circulation2002; 105:124–129
7

balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z xppws S=1 9/9/08 13:32 Art: 200718 Input-ma
30. Lurie KG, Coffeen P, Shultz J, et al: Improv- mission of intrathoracic pressure to the thermia, and unanticipated cerebral recov-ing active compression-decompression car- intracranial space during cardiopulmonary ery. Neurologist 2007; 13:369–375diopulmonary resuscitation with an inspira- resuscitation in dogs. Circ Res 1985; 56: 33. Lurie KG, Holbomb J, Idris A. Level I car-tory impedance valve. Circulation 1995; 91: 20 –30 diac arrest centers: Learning from the1629–1632 32. Yannopoulos D, Kotsifas K, Aufderheide TP, trauma surgeons. Acad Emerg Med 2005;
31. Guerci AD, Shi AY, Levin H, et al: Trans- et al: Cardiac arrest, mild therapeutic hypo- 12:80 – 81
Crit Care Med 2008 Vol. 36, No. 158

1
JOBNAME: AUTHOR QUERIES PAGE: 1 SESS: 1 OUTPUT: Tue Sep 9 13:32:34 2008/balt4/zrz-ccm/zrz-ccm/zrz11108/zrz8925-08z
AUTHOR QUERIES
AUTHOR PLEASE ANSWER ALL QUERIES
1—Please note that references have been renumbered to make their text citation in sequentialorder.