Embed Size (px)
Citation preview

FROM GLOBAL TO LOCAL: AN INTRODUCTION TO THE SYMPOSIUMDavid Jernigan, PhDJohns Hopkins Bloomberg School of Public Health

GLOBAL BACKGROUND
Harmful use of alcohol is increasingly recognized as a global public health problem
Alcohol use was responsible for 3.8% of global deaths and 4.6% of global disability in 2004 (Rehm et al., The Lancet, 29 July 2009)
This is nearly equivalent to the harm from tobacco use, even when allowing for potential health benefits of alcohol use
Global strategy on alcohol under development at WHO
Areas of greatest concern: Alcohol and mortality in Russia Alcohol and young people

The U.S.A. in global context
Source: WHO GISAH, as cited in Rehm et al. 2009

Death and Disability Attributable to Alcohol Use Among Youth Ages 15-29, 2000
Source: Rehm et al. 2003
% total Deaths
Afr D 10 5.90% 560 5.30% 2 1.10% 129 1.00%
Afr E 28 7.90% 1,469 8.00% 5 0.90% 257 1.00%
Amr A 9 23.00% 1,388 28.40% 1 9.50% 401 9.80%
Amr B 52 35.50% 3,995 30.80% 4 7.90% 637 7.80%
Amr D 5 17.20% 369 16.80% 1 3.30% 69 3.70%
Emr B 2 4.80% 69 2.40% 0 1.20% 10 0.40%
Emr D 1 1.20% 123 1.60% 0 0.20% 16 0.20%
Eur A 9 25.60% 1,098 24.40% 1 10.20% 237 6.10%
Eur B 9 24.30% 662 16.90% 1 7.20% 103 3.10%
Eur C 42 41.00% 2,293 35.00% 5 19.90% 391 11.20%
Sear B 14 11.70% 839 11.30% 2 2.40% 116 1.80%
Sear D 26 5.70% 1,699 5.30% 6 1.30% 328 0.90%
Wpr A 2 18.40% 214 15.60% 0 7.00% 110 8.70%
Wpr B 39 13.70% 3,665 14.60% 7 4.90% 630 3.10%
WORLD 249 12.90% 18,444 13.10% 36 2.20% 3,434 2.50%
Males 15-29 Females 15-29
REGION Deaths (000s) DALYs (000s) % total DALYs Deaths (000s) % total Deaths DALYs (000s) % total DALYs

Death and Disability Attributable to Alcohol Use Among Youth Ages 15-29, 2000
Source: Rehm et al. 2003
% total Deaths
Afr D 10 5.90% 560 5.30% 2 1.10% 129 1.00%
Afr E 28 7.90% 1,469 8.00% 5 0.90% 257 1.00%
Amr A 9 23.00% 1,388 28.40% 1 9.50% 401 9.80%
Amr B 52 35.50% 3,995 30.80% 4 7.90% 637 7.80%
Amr D 5 17.20% 369 16.80% 1 3.30% 69 3.70%
Emr B 2 4.80% 69 2.40% 0 1.20% 10 0.40%
Emr D 1 1.20% 123 1.60% 0 0.20% 16 0.20%
Eur A 9 25.60% 1,098 24.40% 1 10.20% 237 6.10%
Eur B 9 24.30% 662 16.90% 1 7.20% 103 3.10%
Eur C 42 41.00% 2,293 35.00% 5 19.90% 391 11.20%
Sear B 14 11.70% 839 11.30% 2 2.40% 116 1.80%
Sear D 26 5.70% 1,699 5.30% 6 1.30% 328 0.90%
Wpr A 2 18.40% 214 15.60% 0 7.00% 110 8.70%
Wpr B 39 13.70% 3,665 14.60% 7 4.90% 630 3.10%
WORLD 249 12.90% 18,444 13.10% 36 2.20% 3,434 2.50%
Males 15-29 Females 15-29
REGION Deaths (000s) DALYs (000s) % total DALYs Deaths (000s) % total Deaths DALYs (000s) % total DALYs

Death and Disability Attributable to Alcohol Use Among Youth Ages 15-29, 2000
Source: Rehm et al. 2003
% total Deaths
Afr D 10 5.90% 560 5.30% 2 1.10% 129 1.00%
Afr E 28 7.90% 1,469 8.00% 5 0.90% 257 1.00%
Amr A 9 23.00% 1,388 28.40% 1 9.50% 401 9.80%
Amr B 52 35.50% 3,995 30.80% 4 7.90% 637 7.80%
Amr D 5 17.20% 369 16.80% 1 3.30% 69 3.70%
Emr B 2 4.80% 69 2.40% 0 1.20% 10 0.40%
Emr D 1 1.20% 123 1.60% 0 0.20% 16 0.20%
Eur A 9 25.60% 1,098 24.40% 1 10.20% 237 6.10%
Eur B 9 24.30% 662 16.90% 1 7.20% 103 3.10%
Eur C 42 41.00% 2,293 35.00% 5 19.90% 391 11.20%
Sear B 14 11.70% 839 11.30% 2 2.40% 116 1.80%
Sear D 26 5.70% 1,699 5.30% 6 1.30% 328 0.90%
Wpr A 2 18.40% 214 15.60% 0 7.00% 110 8.70%
Wpr B 39 13.70% 3,665 14.60% 7 4.90% 630 3.10%
WORLD 249 12.90% 18,444 13.10% 36 2.20% 3,434 2.50%
Males 15-29 Females 15-29
REGION Deaths (000s) DALYs (000s) % total DALYs Deaths (000s) % total Deaths DALYs (000s) % total DALYs

Death and Disability Attributable to Alcohol Use Among Youth Ages 15-29, 2000
Source: Rehm et al. 2003
% total Deaths
Afr D 10 5.90% 560 5.30% 2 1.10% 129 1.00%
Afr E 28 7.90% 1,469 8.00% 5 0.90% 257 1.00%
Amr A 9 23.00% 1,388 28.40% 1 9.50% 401 9.80%
Amr B 52 35.50% 3,995 30.80% 4 7.90% 637 7.80%
Amr D 5 17.20% 369 16.80% 1 3.30% 69 3.70%
Emr B 2 4.80% 69 2.40% 0 1.20% 10 0.40%
Emr D 1 1.20% 123 1.60% 0 0.20% 16 0.20%
Eur A 9 25.60% 1,098 24.40% 1 10.20% 237 6.10%
Eur B 9 24.30% 662 16.90% 1 7.20% 103 3.10%
Eur C 42 41.00% 2,293 35.00% 5 19.90% 391 11.20%
Sear B 14 11.70% 839 11.30% 2 2.40% 116 1.80%
Sear D 26 5.70% 1,699 5.30% 6 1.30% 328 0.90%
Wpr A 2 18.40% 214 15.60% 0 7.00% 110 8.70%
Wpr B 39 13.70% 3,665 14.60% 7 4.90% 630 3.10%
WORLD 249 12.90% 18,444 13.10% 36 2.20% 3,434 2.50%
Males 15-29 Females 15-29
REGION Deaths (000s) DALYs (000s) % total DALYs Deaths (000s) % total Deaths DALYs (000s) % total DALYs

Review of public health findings The earlier young people start to drink, the
worse the alcohol-related consequences: Alcohol dependence Traffic crashes Physical violence after drinking Other unintentional injuries after drinking (e.g.
drowning, falls) Potential damage to still-developing adolescent
brain Lower chances of success in school Age of alcohol initiation has long-term influence on
health Bottom line: strong public health interest in
delaying onset of drinking

Minimum drinking age laws
One of many steps taken by societies to limit alcohol-related harm
EVERY society must take on question of how to control intoxicants and their effects
Minimum drinking age laws only one strategy – cannot be expected to do the whole job
International experience reflects U.S. experience: minimum age laws do affect onset of drinking

Age requirement for on- and off-premise purchase of beer and spirits

Countries greater than 18
19 Canada (all but
Alberta, Manitoba and Quebec)
Republic of Korea Nicaragua
20 Iceland Japan Norway Sweden
21 Egypt Indonesia Micronesia Palau USA
Source: WHO GAD 2006

Recent changes
France: Moves to increase minimum purchase for
alcohol and tobacco from 16 to 18 in 2009 New Zealand (AJPH 2006;96:126–131)
Reduced from 20 to 18 in 1999 Comparing four years before and after the
change from 20 to 18, compared to crashes among 20 to 24 year-olds (comparison group), alcohol-involved traffic crashes grew: 14% among 15-17 year-old males 24% among 15-17 year-old females 12% among 18 and 19 year-old males 51% among 18 and 19 year-old females

Drinking Ages in Europe
15 – Slovenia 16 – Italy, Malta, Portugal 17 – Greece 18 – Austria, Belgium, Bulgaria, Croatia,
Czech Republic, Denmark, Estonia, France, Germany, Hungary, Ireland, Latvia, Lithuania, Netherlands, Poland, Romania, Russia, Slovakia, Spain, Switzerland, Ukraine, United Kingdom
20 – Iceland, Norway, Sweden

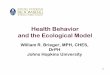
Drinking Among 15-16 year-olds:U.S. and Europe, 2007

Drinking Among 15-16 year-olds:U.S. and Europe, 2007

Drinking Among 15-16 year-olds:U.S. and Europe, 2007

“Extreme drinking worse in U.S.” Actually, looking at indicator “drunk in
past 30 days” 21 countries worse off than U.S., 14 countries better off
Extreme drunkenness worse in U.S.? 15-16 year-olds reporting 10-19 incidents of
drunkenness in past 30 days 1 percent of U.S. 10th graders report this Same percentage as in 14 European countries,
including Austria, Italy and Spain

Background for this syposium “Amethyst Initiative” – signed by 130
college presidents and asking for a re-opening of the debate over the federal law withholding 10% of highway funds if states did not implement age 21 alcohol purchase laws
“Rush to judgment” on 21 largely uninformed by public health research
What light can public health research and experience shed on this debate?

“Eyeball analyses”
Many shortcomings – much more going on in each country than this cursory analysis can capture
More important to review literature in its entirety – never rely on any single study Single studies may mis-specify variables to “wash
out” effects, e.g. Using 15-24 year-olds as focus of analysis Using all traffic crashes instead of alcohol-related
traffic crashes as outcome variable Diluting statistical power by performing state-by-state
analyses which increase range of error, involve fitting linear analysis to trends that are by no means linear

Goals of this symposium
Key questions: What can research tell us about drinking
among college-aged persons? What does the research literature suggest are
the most effective approaches for reducing alcohol-related harm among college students?
What is our specific situation here in Baltimore?
What can we, as campus and community, do in this city to reduce alcohol-related harm among college students?

Structure of the evening
PRESENTATIONS: What is the situation regarding college drinking in the U.S.A.? What has public health research told us to date about what will
be most effective in reducing alcohol-related harm in college campuses and communities?
What can we learn from experience nearby about reducing alcohol-related harm in campus communities?
What special challenges do we face here in Baltimore? DISCUSSION:
How can Baltimore benefit from the findings of research literature and experience?
How do we go forward from here? What partnerships exist and what are needed? What concrete next steps could be proposed?