Embed Size (px)
Citation preview

From Diagnosis to Delivery – Disruptive Innovation
in a Specialty PharmacyPartnering with IDNs: BioPharma Strategy Summit
August 17, 2017
JoAnn Stubbings, BSPharm, MHCAAssistant Director, Specialty Pharmacy Services,
Clinical Associate Professor
University of Illinois at Chicago College of Pharmacy
312.996.3098 [email protected]
OBJECTIVES
• Describe the key characteristics that make an
innovation disruptive and provide examples
• Provide a detailed case study of disruptive
innovation in a specialty pharmacy and tie it
back to the elements of disruption
• Describe opportunities for integration and
strategic partnerships

DISRUPTIVE INNOVATION TRANSFORMS
COMPLICATED, EXPENSIVE PRODUCTS AND
SERVICES INTO SIMPLER, AFFORDABLE ONES
Sources:
Hwang J and Christensen CM. Disruptive innovation in health care delivery: A framework
for business-model innovation. Health Affairs 27(5);2008:1329-1335
• A disruptive business begins with
low quality offerings but eventually
improve quality
• Disruptive businesses in the
initial stages have lower gross
margins, smaller target markets
• Disrupters gain a foothold at the
bottom end of the market that has
been ignored by the incumbent in
favor of more profitable customers

EXAMPLES OF DISRUPTION IN HEALTH CARE
• Minute clinics
• Retail clinics
• Precision medicine/personalized medicine
• Telemedicine/face time
• Changing care of chronic disease: Managing the handoff between diagnosis and adherence
• Passive data collection (wearables and sensors) –change the way healthcare providers interact with patients– Google glass (wearable)
– Digestable sensors
• 3D printers
A MODEL OF DISRUPTION IN SPECIALTY
PHARMACY
• Health system – the original specialty pharmacy
– 1974 – hospital-based investigational drug services documented
– 1978 – first ‘specialty pharmacy’ services for hemophilia patients documented
– 1980s – cyclosporine for kidney transplant, AZT for treatment of AIDS
– 1990s and beyond – hospitals forfeited their ability to become specialty shops to corporate pharmacy organizations

• Specialty pharmacy
management is like navigating
the Chicago ‘el’
• Hub (call center) activity = 1 day
to weeks (insurance
authorization, copayment
assistance)
• Treatment initiation; education
and training; coordination with
clinics; cold chain delivery
• Refill and adherence
management, safety monitoring
and management, clinical
assessments
• Metrics, reporting, outcomes

Normal
56%
At Risk44%
Literacy Risk
CASE STUDY – UNIVERSITY
OF ILLINOIS HOSPITAL AND
HEALTH SCIENCES SYSTEM –
A GRASS ROOTS SPECIALTY
PHARMACY INCUBATOR
• 495 bed academic health center
• DSH; 340B covered entity
• 4,000 employees
• >60 outpatient clinics
• 7 health sciences colleges
• 7 outpatient pharmacies
• 12 Federally Qualified Health
Centers
• 1 million patient encounters
annually
• URAC and ACHC accredited
COMMERCIAL
16% MEDICARE6%
MEDICAID53%
Dual Eligible
24%
SP Payer Mix

SERVICES OFFERED
Specialty Clinics
SPS accepts referrals from clinics via Cerner Specialty Pharmacy Pool. Forward your notes in Cerner to Specialty Pharmacy Services (Pool)
Call CenterInsurance benefit verification
Prior authorization
Medication assistance
SPS program enrollment
Health literacy assessment
Monthly adherence assessments
Escalation to Pharmacist
Documentation in Cerner
Delivery scheduling
Satisfaction surveys
FulfillmentDispensing
Monitor DURs
Multimed management
Safe handling hazardous drugs
Cold chain shipment
Delivery to patient or pickup
Patient Mgt. Program
Specialty Pharmacy Care Plans
Medication and Disease Education
Interventions
Monitoring and Outcomes
Documentation in Cerner
SPECIALTY DISEASE CATEGORIES
Fertility, Growth hormone deficiency, Hepatitis C and Hepatitis B, HIV,
Immune disorders (Crohn’s Disease, IBD, RA, etc.), Lipid disorders,
Multiple sclerosis, Oncology , Orphan disease, Pulmonary arterial
hypertension, Sickle cell disease, Transplant
LOCAL STRATEGY
SERVING THE UI HEALTH
AND UIC COMMUNITY
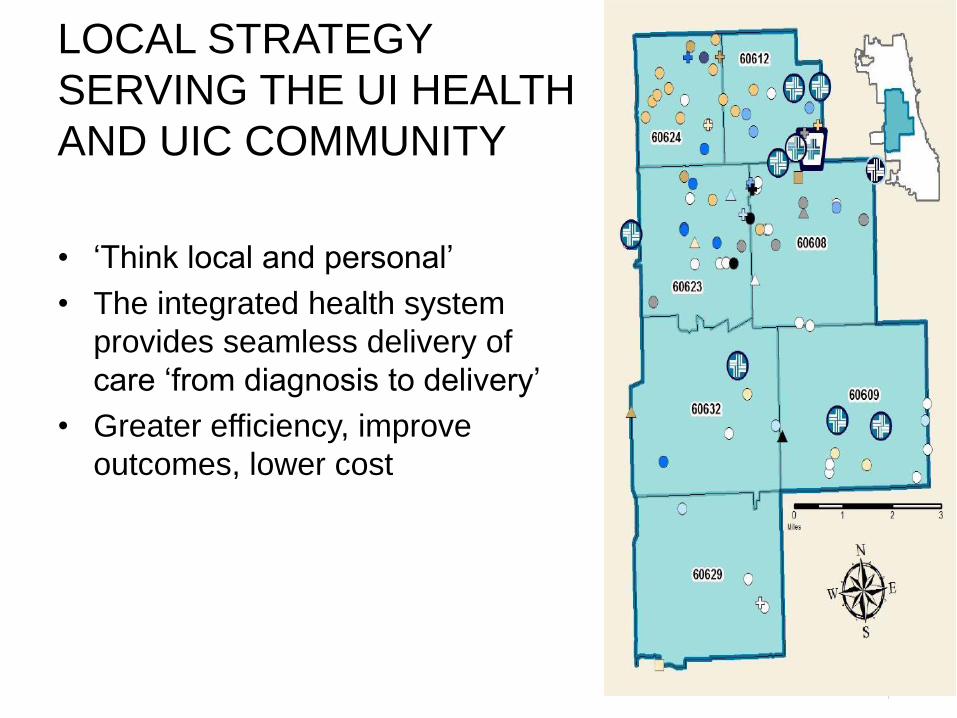
• ‘Think local and personal’
• The integrated health system
provides seamless delivery of
care ‘from diagnosis to delivery’
• Greater efficiency, improve
outcomes, lower cost

CASE: HCV AND HOMELESS
• 49 year old AA man h/o
schizoaffective disorder,
depression, migraines and GT
1a HCV cirrhosis.
• Tx experienced: relapsed after
12 weeks simepravir+sofosbuvir
• Started treatment with Harvoni
2/26/15 x 24 weeks
• Returned to pharmacy same day
to try to return meds - homeless

TWO TYPES OF DISRUPTION – PROCESS AND OUTCOMES
GREATER
EFFICIENCY
IMPROVE
OUTCOMES
LOWER COST
Embedded Clinical Pharmacists X X X
Clinical Intelligence Systems X X X
Seamless Referrals and PA Submissions X X X
Treatment Integration/Waste Management X X X
Lean Staffing and Layered Learning X X
Custom Delivery Solutions X X
Ability to collect and report Outcomes Data X X X
EXAMPLES OF NEW MODELS
Telehealth X X X
Clinical Performance Contracts X X X
Sources:
Toussaint JS and Mannon M. Hosptals are finally starting to put real-time data to use. Harvard Business Review. November 2014.
Available at: https://hbr.org/2014/11/hospitals-are-finally-starting-to-put-real-time-data-to-use.
Honigman B. The 7 biggest innovations in health care technology in 2014. Available at: https://getreferralmd.com/2013/11/health-care-
technology-innovations-2013-infographic/

STEP 1 – LISTEN TO
OUR PATIENTS
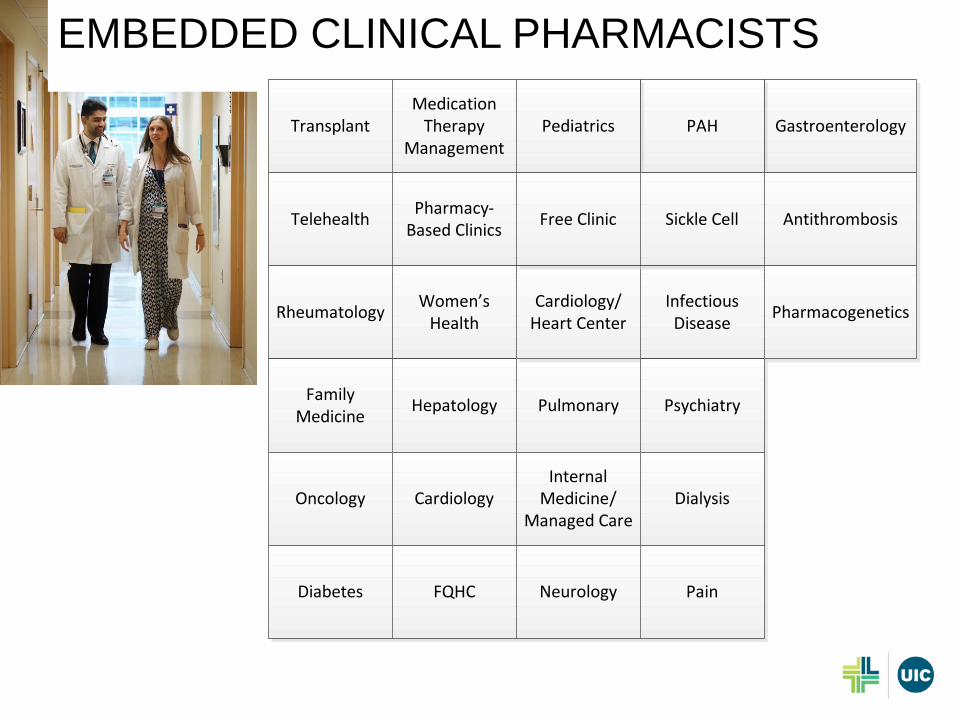
EMBEDDED CLINICAL PHARMACISTS
Transplant
Telehealth
Rheumatology
Medication Therapy
Management
Pharmacy-Based Clinics
Gastroenterology
Women’s Health
Family Medicine
Hepatology
Oncology Cardiology
Pulmonary
PAH
Cardiology/ Heart Center
Internal Medicine/
Managed Care
Infectious Disease
Psychiatry
Dialysis
Diabetes FQHC Neurology Pain
Pediatrics
Free Clinic Sickle Cell Antithrombosis
Pharmacogenetics

CLINICAL INTELLIGENCE SYSTEMS
• Challenge: PCSK9
inhibitors were
approved in 2015
• Anticipated demand
from specialty clinics
and general internal
medicine clinics
• Clinics were not
prepared to manage
challenging PA
process
Sources:
Groo VL, Ardati A, Stubbings JA. Leveraging our strengths: Clinical pharmacist mediated PCSK9 utilization.
American College of Cardiology Annual Scientific Session, Washington DC. March 2017.
Atanda A, Shapiro NL, Stubbings JA, and Groo V. Implementation of a new clinic-based, pharmacist-managed
PCSK9 inhibitor consultation service. To be published in Journal of Managed Care Pharmacy, Best Practices
article, September 2017.
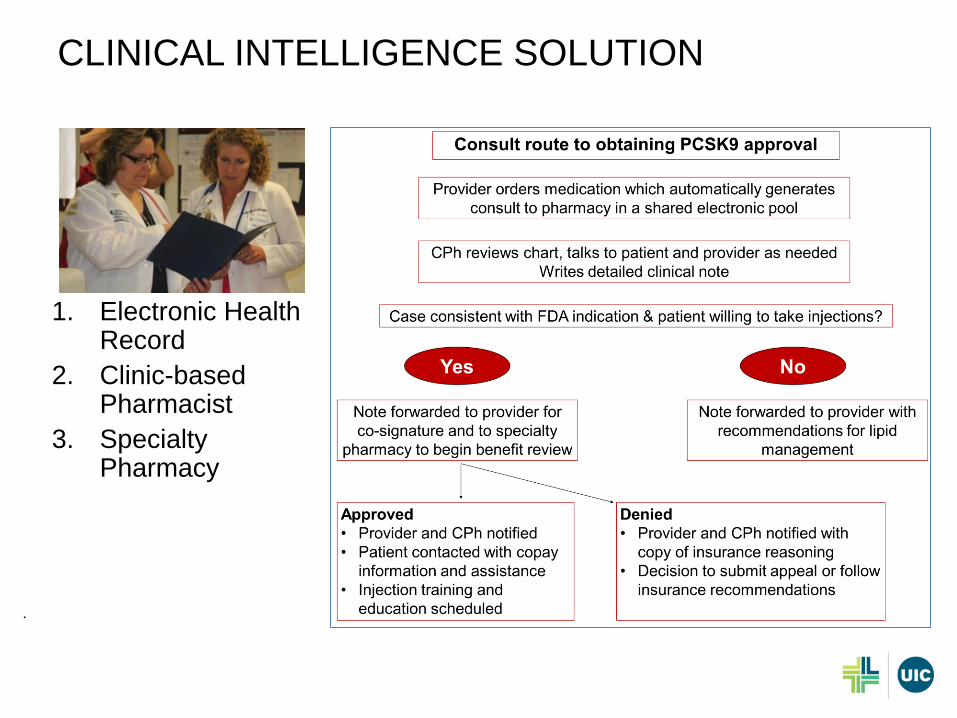
CLINICAL INTELLIGENCE SOLUTION
1. Electronic Health Record
2. Clinic-based Pharmacist
3. Specialty Pharmacy
.

CASE STUDY
• Mr. A is a 52 year old male with history of 3 vessel CABG and AAA
repair at age 50
• Additional history: HTN, sarcoidosis, anxiety, GERD, obesity
• Lipid/statin history:
• PCSK9 ordered – consult generated
TC Trig HDL LDL Drug
Mar 2015 265 70 32 210 Atorvastatin 40mg
Sep 2016 260 39 40 212 Atorvastatin 80mg

PRACTICAL APPLICATIONS OF CLINICAL
INTELLIGENCE SYSTEMS
• The PCSK9 consult service innovation is an example of
an application of a clinical intelligence service and
coordination of care between the provider, a clinic-based
pharmacist, and a specialty pharmacy.
• Benefits of the service:
– Removes the burden from the provider office and
manufacturer/hub
– Increases the success of prior approval
– Improves efficiency, cost effectiveness, and outcomes
• This service could be replicated for other specialty
medications across many clinics

SEAMLESS REFERRALS AND PA SUBMISSIONS
•Range 0-30 days
Benefit Verification to PA Approval* =
3.16 days
Benefit Verification =
<24 hours
Time to Access
Referral from Specialty Clinic via
EHR
Benefit Verfication
Prior Authorization
Start of Therapy

TREATMENT INTEGRATION WITH CLINIC
Treatment Integration with Oncology Clinic
Spec
ialt
y P
har
mac
ySp
ecia
lty
Clin
ic
Diagnosis and Drug Selection
Benefit VerificationPrior Authorization
Approval
Medication Assistance
Start Date
Dispense MedicationWalk to Clinic
Treatment InitiationProgram Enrollment
Monthly Clinical Assessment
Refill MedicationDeliver to Patient at
Homr or in Clinic
Refill AuthorizationLabs and other Diagnositcs
Clinic Appointment
1-2 week Clinical Assessment
• Waste management
• Oral oncology drug will not be
dispensed to patient w/o final approval
from ONC clinic, based on results of
MRI, labs, xrays, and other diagnostic
information.
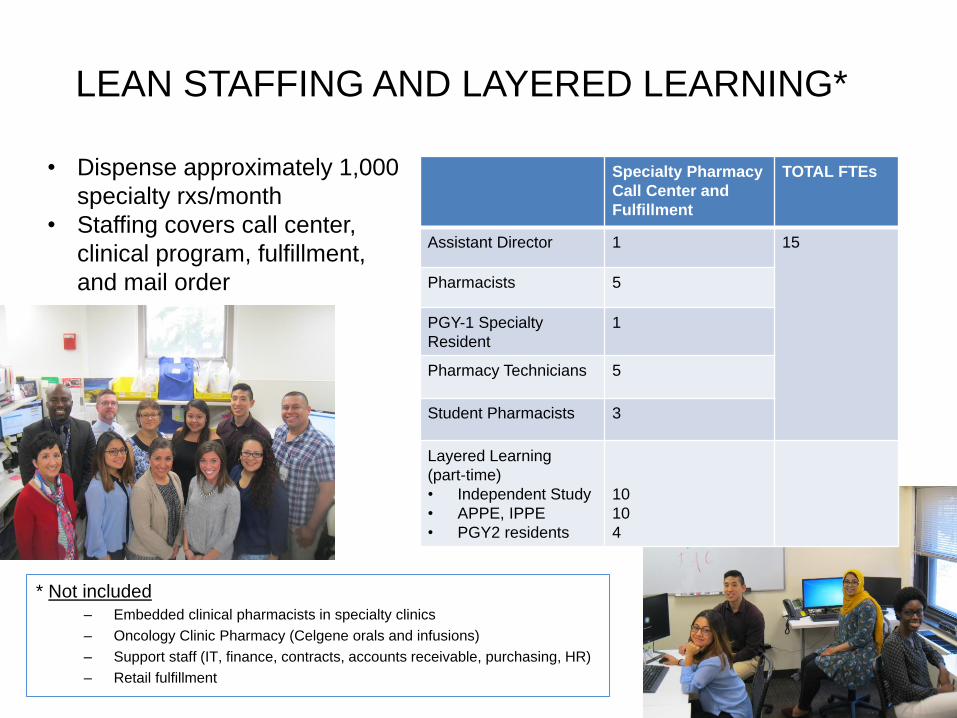
LEAN STAFFING AND LAYERED LEARNING*
Specialty Pharmacy
Call Center and
Fulfillment
TOTAL FTEs
Assistant Director 1 15
Pharmacists 5
PGY-1 Specialty
Resident
1
Pharmacy Technicians 5
Student Pharmacists 3
Layered Learning
(part-time)
• Independent Study
• APPE, IPPE
• PGY2 residents
10
10
4
* Not included
– Embedded clinical pharmacists in specialty clinics
– Oncology Clinic Pharmacy (Celgene orals and infusions)
– Support staff (IT, finance, contracts, accounts receivable, purchasing, HR)
– Retail fulfillment
• Dispense approximately 1,000
specialty rxs/month
• Staffing covers call center,
clinical program, fulfillment,
and mail order
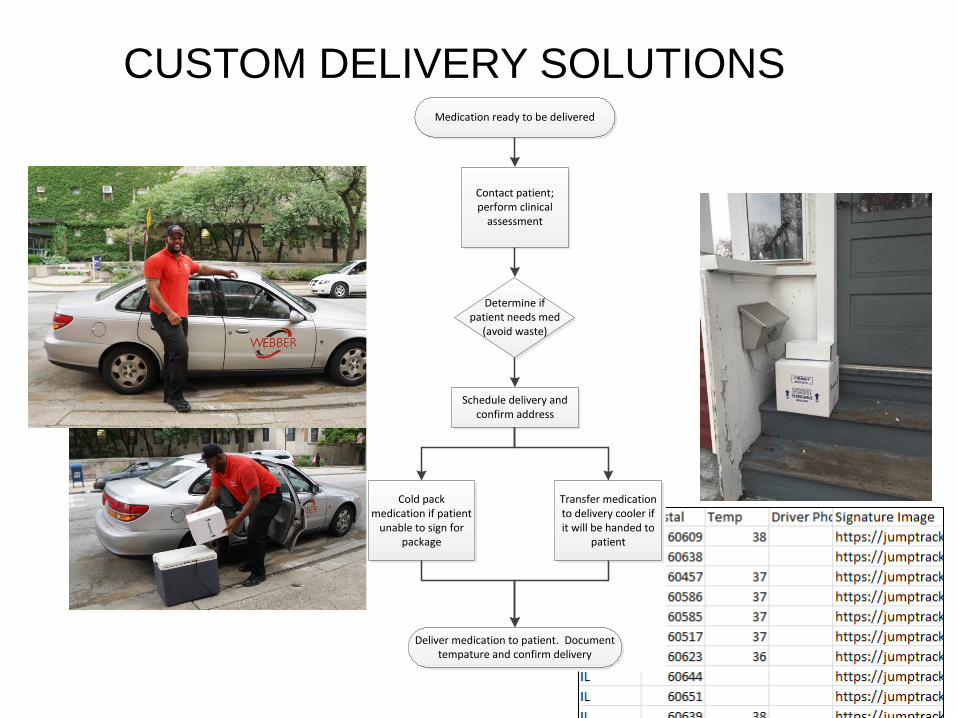
CUSTOM DELIVERY SOLUTIONS
Contact patient; perform clinical
assessment
Medication ready to be delivered
Determine if patient needs med
(avoid waste)
Schedule delivery and confirm address
Cold pack medication if patient
unable to sign for package
Transfer medication to delivery cooler if it will be handed to
patient
Deliver medication to patient. Document tempature and confirm delivery

ABILITY TO COLLECT PRIMARY DATA AND
REPORT CLINICAL, HUMANISTIC, AND
ECONOMIC OUTCOMES
• For all patients: demographics, medications, line of business, clinical interventions, clinical outcomes
• MPR and Primary Medication Nonadherence and reasons form PMN
• Time to access of medication
• Patient and provider satisfaction
• RA patient demographics and disease activity based on PAS-II score
• Hepatitis C: genotype, medication, and SVR
• Multiple sclerosis: medication, hospitalizations, ER visits, relapses/exacerbations, unmanaged symptoms
• Oral oncology: hospitalizations and ER visits related to cancer
• Medication assistance: including copay cards, foundations, and funds from health system
• Hyperlipidemia: medication, HDL and LDL results
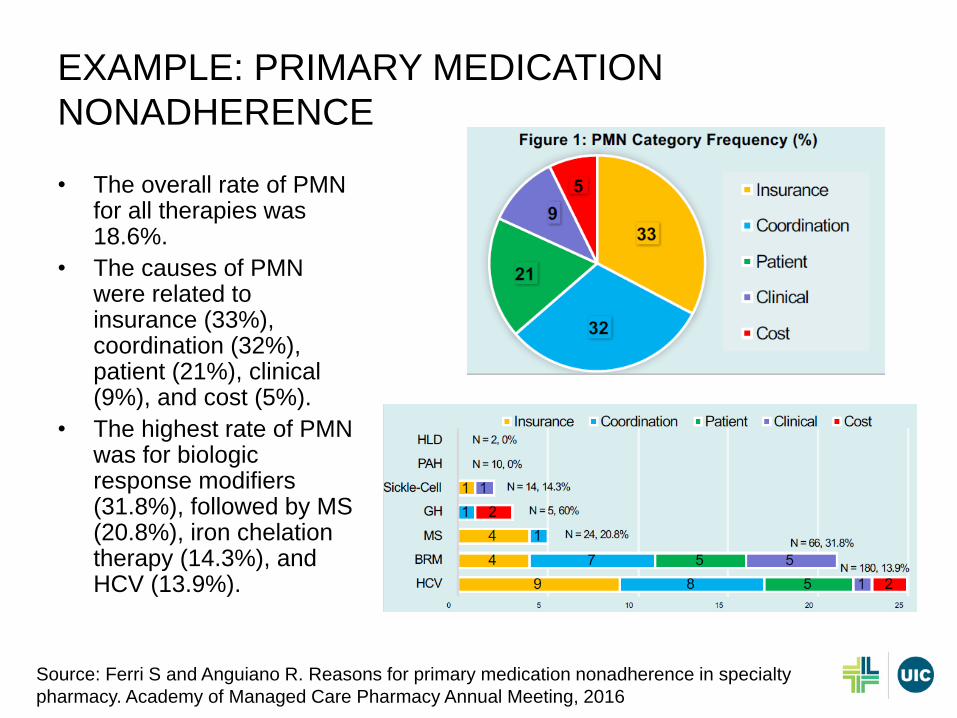
EXAMPLE: PRIMARY MEDICATION
NONADHERENCE
• The overall rate of PMN for all therapies was 18.6%.
• The causes of PMN were related to insurance (33%), coordination (32%), patient (21%), clinical (9%), and cost (5%).
• The highest rate of PMN was for biologic response modifiers (31.8%), followed by MS (20.8%), iron chelation therapy (14.3%), and HCV (13.9%).
Source: Ferri S and Anguiano R. Reasons for primary medication nonadherence in specialty
pharmacy. Academy of Managed Care Pharmacy Annual Meeting, 2016

EXAMPLE: MEDICATION
POSSESSION RATIO
TOTAL
SPS
BRM PAH MS HCV TX HIV ONC
Medicaid 0.91 0.93 0.87 0.92 0.97 0.90 0.84 0.90
Medicare 0.92 0.89 0.89 0.87 0.96 0.92 0.88 0.89
Commercial 0.89 0.89 0.70 0.91 0.93 0.86 0.95 0.90
• Overall MPR is 91%
• No difference by line of business
TOTAL
SPS
BRM PAH MS HCV TX HIV ONC
MPR 0.91 0.91 0.87 0.91 0.96 0.91 0.85 0.90
Min 0.14 0.44 0.47 0.25 0.39 0.14 0.29 0.22
Max 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00
StDev 0.15 0.12 0.15 0.14 0.08 0.17 0.16 0.18
Count 1434 230 23 122 163 655 133 108
% SPS 100.0% 16.0% 1.6% 8.5% 11.4% 45.7% 9.3% 7.5%

OPPORTUNITIES FOR NEW MODELS OF CARE
POINTS OF
COLLABORATION
PARTNERS MODELS
• Prior
authorizations/time to
access
• Clinical services
• Service contracts
• Performance contracts
• Clinical intelligence
systems
• Local access and
personalized care
• Data collection and
reporting
• Manufacturers
• Health plans
• Employers
• Government agencies
• Specialty pharmacies
• Alternative Distribution
Models
• Payment Voucher
• Pay for Performance

• Based on the view that the process for delivery of medical care and services can be continuously improved
• Specific target areas for improvement– Disease state management, preventative care,
patient satisfaction, member outreach
• Incentives– Better clinical care leads to a better clinic
– Monetary
– Favorable public profile
EXAMPLE: CLINICAL PERFORMANCE CONTRACTS
HMO QUALITY IMPROVEMENT (QI) PROGRAM
KEY TAKEAWAYS
• Disrupters gain a foothold at the bottom end of the
market that has been ignored by the incumbent in favor
of more profitable customers
• Health systems can represent grass roots incubators for
specialty pharmacy disruption
• There are opportunities for new models of care and
collaborations





























