Embed Size (px)
Citation preview

ADMINISTRATION OFFICE
MAILING ADDRESS
621 Santa Fe TELEPHONE (559) 499-2450 P.O. BOX 45018
Fresno, CA 93721 FAX (559) 499-2460 FRESNO, CA 93718-5018
Fresno City Employees Health & Welfare Trust
Agenda for the Regular Board Meeting
November 9, 2016
8:00 AM
Location: HealthComp 621 Santa Fe, Fresno CA 93721*
Employer Trustees-City of Fresno Employee Trustees Bruce Rudd, Vice Chairperson Shane Archer, Chairperson FFA Michael Lima, Trustee Jacky Parks, Trustee FPOA Jeffrey Cardell, Trustee Apolonio Munoz, Trustee ATU William Dearsan, Trustee
Martin Hinojosa, Trustee IBEW FCEA
Administrator Robert Mesel, Trustee CFPEA Phil Musson, CEO Shelley Morrison, Trustee CFMEA Michelle Bugg, Plan Manager Mike Alforque, Trustee FFA Marina Magdaleno, Trustee Local 39 Jo Billings, Trustee FPOA Vacant FAPSS
Legal Counsel Consultants
Michael E. Moss, Esq. Jim Rhein Rael & Letson
Roll Call 8:00 A.M.
1) Approval of Agenda**
Approve Agenda for November 9, 2016
Action as required
2) Approval of the Minutes
Approve Minutes of September 14, 2016
Action as required
3) Public Discussion***
4) Correspondence
a) The University of California at Berkeley Wellness Letter
5) Presentation of Administrator’s Report
a) Claim and Benefit Reports
b) Specific Stop-Loss Report
c) Turnaround Time Report
d) Transitional Reinsurance Program Payment
Action as required

Fresno City Employees November 9 ,2016 Health & Welfare Trust Regular Board Meeting Agenda 2
6) Review & Approval of Appeal Interpretations, Report from Appeals Committee
7) Presentation of Reports from Managed Care Vendors
a) Blue Shield of California
i) Quest Diagnostics
Update on Quest Diagnostics
ii) Cologuard
Update on Cologuard
b) Psy-Care
Review of the October 2016 Utilization Reports
c) United Healthcare
d) Optum
i) Executive Summary
Review of the September 2016 Executive Summary
ii) Review and Approve Optum Formulary Tier Change Letter Template
Action as required
iii) Review Prior Authorization Monthly Reporting for September 2016 / Annual Reporting for the 2015-2016 Plan Year
iv) Review and Approve Traditional Comprehensive Prior Authorizations / Quantity Limits / Utilization Management
Action as required
v) Ratification of Urgent Action taken by the Chairperson and Vice Chairperson to Approve EGWP January 1, 2017 Plan Year
Action as required
vi) Account Executive Transition Effective November 14, 2016
e) Delta Dental
Review of the September 2016 Experience Reports
f) ChiroMetrics
Review of the October 2016 Intake Reports
g) PhysMetrics
h) MES Vision
i) Teladoc
Review of the September 2016 Utilization Reports
8) Presentation of Consultant’s Report
a) Ratification of Urgent Action Taken by Chairperson to Approve Flu Shot Agreements
Action as required
b) Fiduciary Liability Insurance Renewal
Review and Approve Fiduciary Liability Insurance Renewal
Action as required

Fresno City Employees November 9 ,2016 Health & Welfare Trust Regular Board Meeting Agenda 3
c) Submission of Vendor Rate Increase Requests for the 2017-2018 Fiscal Year
Vendors requesting a rate increase for the 2017-2018 fiscal year must have the request submitted by December 30, 2016
d) Submission of Proposed Benefit Changes for the 2017-2018 Fiscal Year
Discussion on Requested Benefit Changes for the 2017-2018 Fiscal Year
9) Attorney’s Report
a) Affordable Care Act
Update on the Affordable Care Act
10) Board Meeting Schedule
a) Consider and Approve Modification to Board of Trustee Meeting Schedule
Action as required
11) Executive Session Items
12) Future Agenda Items
13) Adjournment
Action as required *The meeting room is accessible to the physically disabled. If you require a disability related modification or accommodation to participate in the meeting, notify HealthComp Administrators at (559) 499-2450.
** All writings, including Agendas, distributed prior to or during any Regular or Special Meeting are available for public inspection during regular business hours at the offices of HealthComp Administrators located at 621 Santa Fe, Fresno CA.
***Provides an opportunity for members of the public to address the Board of Trustees on items of interest to the public within the Board of Trustees jurisdiction and which are not already on the Agenda. It is the policy of the Board of Trustees not to answer questions impromptu but refer such matters to the Administration Office for placement on the next Agenda. Speakers should limit their comments to no more than three (3) minutes. No more than ten (10) minutes per issue will be allowed. For items which are on the Agenda for this meeting, members of the public will be provided an opportunity to address the Board of Trustees before a vote is taken on each item.
NOTICE APPEALS COMMITTEE
Next Meeting: Monday, December 5, 2016 at 4:00 p.m.
Committee Members to Attend: Bruce Rudd, William Dearsan, Shelly Morrison

~lrt~~ .. lll""111~ rn~~iil":ll~4~~ CITY EMPLOYEES
621 Santa Fe Street Fresno, CA 93721
HEALTH AND WELFARE TRUST
ADMINISTRATION OFFICB:
0 Health Camp Third Party Administration
TELEPHONE (559) 499-2450 FAX (559) 499-2464
MAILING ADDRESS 1'.0. BOX 45018
FR"SNO, CA 93718-5018
FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST MINUTES OF THE REGULAR BOARD MEETING "
September 14, 2016
CALL TO ORDER: The regular monthly meeting of the Board of Trustees for the Fresno City Employees Health & Welfare Trust was called to order by Trustee Mike Alforque at 8:05 A.M., Wednesday, September 14, 2016 in the Conference Room at 621 Santa Fe Street. A quorum was present including the following:
EMPLOYEE TRUSTEES PRESENT: Shelley Morrison Jacky Parks Apolonio Munoz Martin Hinojosa
EMPLOYEE TRUSTEES ABSENT: Shane Archer Marina Magdaleno
EMPLOYER TRUSTEES PRESENT: Jeffrey Cardell
EMPLOYER TRUSTEES ABSENT: Bruce Rudd
OTHERS PRESENT:
HealthComp Phil Musson Michelle Bugg Moss Law Firm Mike Moss
Rael & Letson Jim Rhein
ChiroMetrics/PhysMetrics Jeremy Oswald Stephan Albracht
Blue Shield of CA Linda Patron Joe Safran Optum Kristy Sherman Terry Miller UHC
Psy-Care Sandra Carnahan
Jo Billings Robert Mesel Mike 1\lforque
William Dearsan
Michael Lima
Delta Dental Jerry Sauter Duab Xaochay FORCE Cheri Detweiler
MES Vision Rodney Mattos
Benefit Analyst, COF Dayvonna Youngblood

II
Item 1 Approval of Agenda - A Motion was made by Trustee Robert Mesel and Seconded by Trustee Jeffrey Cardell to approve the Agenda. The Motion was unanimously approved.
Item 2 Approval of Minutes
Approve Minutes of August 10, 2016- A Motion was made by Trustee Michael Lima and Seconded by Trustee Shelley Morrison to approve the Minutes for August 10, 2016. The Motion was unanimously approved.
Item 3 Public Discussion - Ms. Sandra Brock, an employee of the City of Fresno, presented a document referencing the California Government Code commonly referred to as "The Brown Act". Ms. Brock stated "The Brown Act" is not being followed by the Trust.
Ms. Brock also commented that her medical provider informed her that Cologuard testing is approved by every insurance carrier except Blue Shield. Ms. Brock asked whether Blue Shield will approve Cologuard testing. Mr. Mike Moss stated that if Blue Shield wanted to respond they could address this topic under Agenda item ?a.
Ms. Cheri Detweiler, the FORCE representative, informed the Board of Trustees of a workers compensation issue where a provider had incorrectly billed Medicare rather than a Workers Compensation carrier. Ms. Detweiler stated it was corrected but believed the Board of Trustees should be informed.
Item 4 Correspondence
a) The University of California at Berkeley Wellness Letter - Mr. Phil Musson referred the Board of Trustees to the University of California at Berkeley Well ness Newsletter.
b) Jeffrey Cardell's email correspondence dated September 6, 2016 regarding new MOU for FCEA's contribution rate effective October 1, 2016 - Mr. Phil Musson referred the Board of Trustees to the September 6, 2016 email correspondence from Jeffrey Cardell stating the City of Fresno and FCEA has reached an agreement on a new MOU that included a 75/25 contribution for the health insurance premium with future contribution increases to be apportioned 50/50. The MOU will be presented to the City Council for approval on September 22, 2016.
Item 5 Administrator's Report
Mr. Phil Musson reviewed the following reports for the Board of Trustees:
a) Claim and Benefit Reports for two months ending August 31, 2016.
b) Specific Stop-Loss Analysis Report for the period of July 1, 2015 through June 30, 2016 which identified twelve individuals that would have exceeded the specific Stop-Loss deductible of $175,000 if such a policy existed.

III
Fourteen individuals would have been above a 50% specific Stop-Loss claims level.
c) Turnaround Time Report for the month of August 2016.
Item 6 Review & Approval of Appeal Interpretations - Mr. Mike Moss reported the Appeals Committee met on September 6, 2016 to review Appeal 16-00 and Appeal 16-01. Mr. Moss informed the Board of Trustees of the Appeals Committee's unanimous recommendation to approve both appeals. A Motion was made by Trustee Jeffrey Cardell and Seconded by Trustee Robert Mesel to approve both appeals subject to the $50 administrative fee. The Motion was unanimously approved.
Item 7 Reports from Managed Care Vendors
a) Blue Shield of California - Ms. Linda Patron, Account Manager, was present and referred to the following items:
Ms. Patron addressed the Public Discussion topic regarding Cologuard testing and stated she will refer the issue to the medical management department at Blue Shield to determine if there has been a change to the Blue Shield medical policy.
i) Network Contract Representative - Ms. Linda Patron introduced Joe Safron from the Blue Shield Network Contracting Department and Ron Russak the Quest Regional Director for Patient Services. Mr. Russak explained the Quest "Easy Pay" process and informed the Board of Trustees that Quest does not have direct access with payors to identify patient responsibility. Mr. Russak explained Quest's procedure for collecting money in advance of services based on an estimate of the amount that will be owed for plans that have a deductible or coinsurance. Mr. Russak further stated that this option is voluntary unless a member has a past due amount. Trustee Jacky Parks expressed his concerns and belief that Quest is not administering the "Easy Pay" process as presented. After much discussion it was suggested Quest flag Fresno City Employees Health and Welfare Trust members in their system by an identifier such as a Group Number to ensure the member is informed that the "Easy Pay" payment option is voluntary. Trustee Jeffery Cardell requested a writing from Quest confirming that Fresno City Employees Health and Welfare Trust members are identified in Quest's system to ensure the member is informed that the "Easy Pay" payment option is voluntary.
b) Psy-Care - Ms. Sandra Carnahan, a Psy-Care representative, was present and referred the Board of Trustees to the August 2016 Utilization Report.
c) United HealthCare - Mr. Carlos Guzman, Account Executive, was not present.

IV
d) Optum - Catamaran - Ms. Kristy Sherman, Account Executive, was present, introduced colleague Terry Miller and referred to the following items:
i) Executive Summary - Ms. Sherman reviewed the Executive Summary for the period of August 2015 through July 2016.
ii) Review and Approve Amendment 3 to Client Services Agreement -EGWP - Ms. Sherman presented to the Board of Trustees Amendment 3 to the Client Services Agreement-EGWP and Amendment 1 to the Client Services Agreement-Commercial. Mr. Mike Moss stated the Amendments have been reviewed and approved. Ms. Sandra Brock expressed her concern that the Amendments do not address timeframes for pre-certifications and requested Optum streamline physician authorizations. Mr. Moss stated he would review the Client Service Agreements for the timeframes for pre-certification and provide a report at the next meeting. Trustee Robert Mesel requested a copy of the prior authorization questionnaire sent to physicians. Ms. Sherman stated there is not a standard questionnaire but would provide a variety of samples based on the drug. After much discussion a Motion was made by Trustee Jeffery Cardell and Seconded by Trustee Michael Lima to approve Amendment 3 to Client Services Agreement-EGWP and Amendment 1 to Client Services Agreement-Commercial. The Motion was unanimously approved.
iii) Review and Approve Amendment 1 to Client Services Agreement • Commercial- See Agenda item 7.d.iii.
iv) Review and Approve EGWP ID Card Mock-ups and ID Card LetterMs. Sherman referred the Board of Trustees to a draft of the ID card and ID card letter that would be mailed to the EGWP population. Ms. Sherman also informed the Board of Trustees there will be no charge for the ID Cards. A Motion was made by Trustee Jeffrey Cardell and Seconded by Trustee Jacky Parks to approve the ID cards and ID card letter. The Motion was unanimously approved.
v) EGWP January 1, 2017 Plan Year Consideration- A Motion was made by Trustee Jacky Parks and Seconded by Trustee Jeffrey Cardell to table this item until the next Board of Trustees Meeting. The Motion was unanimously approved.
vi) Update regarding EGWP Impact Analysis for Member Copay Issue - Ms. Sherman updated the Board of Trustees on the EGWP member co-pay issue. Ms. Sherman stated 51 members were impacted and refunds were in process.
vii) Review and Approve Traditional Comprehensive Prior Authorizations I Quantity Limits I Utilization Management - Ms. Sherman reviewed the prior authorization timeframe analysis report and referred to the experience map outlining the process. After much

v discussion a Motion was made by Trustee Robert Mesel and Seconded by Trustee Michael Lima to table this item until the next Board of Trustees Meeting. The Motion was unanimously approved.
e) Delta Dental - Mr. Jerry Sauter, Account Manager, was present and introduced Duab Zaochay as the new Account Manager. Mr. Sauter referred the Board of Trustees to the July 2016 Experience report.
f) ChiroMetrics - Dr. Stephan Albracht, was present and referred the Board of Trustees to the August 2016 Intake Report.
g) PhysMetrics - Mr. Jeremy Oswald, Account Manager, was present and had nothing new to report.
h) MES Vision - Rodney Mattos, a MES representative, was present and had nothing new to report.
Item 8 Presentation of Consultation's Report
a) Flu Shot Program - Mr. Jim Rhein referred the Board of Trustees to the Flu Shot notice. A Motion was made by Trustee Jacky Parks and Seconded by Trustee Jeffrey Cardell to approve the notice. The Motion was unanimously approved.
Item 9 International Foundation Employee Benefits Conference - After discussion it was decided that a Trust representative will not attend this conference.
Item 10 Attorney's Report - Mr. Mike Moss updated the Board of Trustees on the Affordable Care Act.
Item 11 Board Meeting Schedule- Discussion on permanently scheduling the Board of Trustee Meetings for every other month. A Motion was made by Trustee Jeffrey Cardell and Seconded by Trustee Jacky Parks to schedule the Board of Trustees Meeting for every other month. The Motion failed with Nay votes from Trustee Robert Mesel, Trustee Michael Lima and Trustee Apolonio Munoz. A Motion was made to table the item to the next Board of Trustees Meeting and to cancel the October 2016 Meeting. The Motion was unanimously approved.
Item 12 Executive Session Items- None
Item 13 Future Agenda Items
a) Optum Prior Authorizations
b) Blue Shield of California- Quest and Sierra Orthopedic
Item 15 Adjournment - A Motion was made by Trustee Jeffrey Cardell and Seconded by Trustee Jo Billings to adjourn the Board of Trustees Meeting at 10:16 A.M. The Motion was unanimously approved.

Shane Archer, Chairperson Fresno City Employees Health & Welfare Trust
Phillip J. Musson, Administrator HealthComp
VI
Date
Date

FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
MONTHLY CLAIMS EXPERIENCE ANALYSIS MEDICAL AND PRESCRIPTION DRUGS
FOUR MONTHS ENDING OCTOBER 31, 2016
ACTIVES COBRA RETIREES
MEDICARE SUPPLEMENT SELF-PAY OVER 65
AVERAGE MONTHLY COST· YTD
PRIOR YEAR AVERAGE MONTHLY COST· YTD FOUR MONTHS ENDING OCTOBER 31, 2015
PRIOR PLAN YEAR AVERAGE MONTHLY COST JULY 2015 ·JUNE 2016
TWELVE MONTH ROLLING AVERAGE November 1, 2015 ·October 31, 2016
$ 10,721,981.78 19,228.88
1 ,298, 758.95
$ 12,039,969.61
$ 579,798.82 62,414.41
$ 12,682,182.84
$ 3,170,545.71
$ 2,833,181.19
$ 3,002,592.34
$ 3,115,047.19
Prepared by HealthComp Inc 1110112016
PER ELIGIBLE
$
$
$
$
$
$
$
$
901.84 2,403.61 1,381.66
937.91
898.91 693.49
934.44
934.44
856.79
901.14
926.89

FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
MONTHLY CLAIMS EXPERIENCE ANALYSIS DENTAL BENEFIT SECTION
FOUR MONTHS ENDING OCTOBER 31, 2016
DELTA DENTAL
ACTIVES RETIREES
TOTAL FOR DELTA DENTAL
AVERAGE MONTHLY COST PUD HMO AVG MONTHLY PREM
TOTAL AVG MONTHLY COST· YTD
PAYMENTS
$ 770,591.55 127,386.05
$ 897,977.60
$ 224,494.40 15,750.90
$ 240,245.30
PRIOR YEAR AVERAGE MONTHLY COST: DELTA DENTAL JULY 2015 ·JUNE 2016
ACTIVES
RETIREES
COMBINED
TWELVE MONTH ROLLING AVERAGE DELTA DENTAL
November 1, 2015. October 31,2016
Prepared by HealthComp 11/01/2016
PER ELIGIBLE
$ $
$
$ $
$
$
$
$
$
73.29 65.93
72.15
72.15 40.70
68.67
74.50
40.70
70.62
73.64

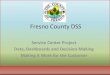
Fresno City Employees H & W Trust
\,l "-, ".-/
/ .,___
\,/ ., : ;/
;I~
1000 950 900 850 800 750
Average Cost Per Participant
Monthly . .3 > ,,, ''U"""'d£"'"-JIS'"'
Fresno City Employees H & W Trust Nov 15- Oct 16
HeallhCompAdministrators
Average Cost Per Participant Year to Date
Fresno City Employees H & W Trust Jul16- Jun 17
-·-- .
/'-
/ +,.L------
---
700 -650 ·-···· 600 r- -----,--------,
J A S 0 N D J F M A M J
HealthCompAdministrators
1

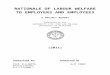
Fresno City Employees H & W Trust
\,/ "> ./
/1 I ~
Average Cost Per Participant 12 Month Rolling Average
Fresno City Employees H & "'Trust Jun 97- Oct 16
1000 ~----
900 +---- • m /'\1 ,,/"\/ 800 +------··· ;, t-·""' 700 +--------- ~ ------600 -1--------------,--~~~!'···lf'i->,.J''-""'::.[! _____ _
~,,~ 500 ----·~~j.•i,.;\,.i#~"•~r,~~"C"'--------
400 71" • .,#' ·····- ------
300 -~""-_,.,.-::,·'--~------------------------
HealthCompAdministrators
2

FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
FINANCIAL ANALYSIS FOR MEDICAL, VISION AND PRESCRIPTION DRUG FOUR MONTHS ENDING OCTOBER 31, 2016
CENSUS CLAIMS FIXED TOTAL NET CATEGORY COUNT COSTS COSTS COSTS RATE INTEREST GAIN(LOSS)
ACTIVES PPO Contributing 2,446 $ 1,010.08 $ 79.00 $ 1,089.08 $ 1,090.00 4.24 5.16 PPO Non-Cont 25 87 $ 813.29 $ 79.00 $ 892.29 $ 854.80 4.24 (33.25) PPO Non-Cont 35 74 $ 168.47 $ 79.00 $ 247.47 $ 737.20 4.24 493.97 PPO Non-Cont 32 366 $ 347.00 $ 79.00 $ 426.00 $ 773.00 4.24 351.24 TOTAL (a) 2973 $ 901.74 $ 79.00 $ 980.74 $ 1,035.31 $ 4.24 $ 58.81
RETIREES PPO Plan 235 $ 1,381.66 $ 79.00 $ 1,460.66 $ 1,090.00 4.24 (366.42) TOTAL 235 1,381.66 79.00 1,460.66 1,090.00 4.24 (366.42)
MEDICARE SUPP PPO Plan 161 $ 898.91 $ 69.64 $ 968.55 $ 607.00 $ 4.24 $ (357.31) TOTAL 161 $ 898.91 $ 69.64 $ 968.55 $ 607.00 $ 4.24 $ (357.31)
SELF-PAY PPO Plan 23 $ 693.49 $ 79.00 $ 772.49 $ 1,315.00 $ 4.24 $ 546.75 TOTAL 23 $ 693.49 $ 79.00 $ 772.49 $ 1,315.00 $ 4.24 $ 546.75
ACA TRP Payment
TOTAL --· -
NOTES: Claims Costs and Census Count represent average per month over the reporting period. Fixed Costs include all plan costs for Blue Shield, Psy-Care, ChiroMetrics, Optum, HealthComp, Rael & Letson, Moss Law Firm, MES, PhysMetrics and BCS Insurance
Interest revenue is based upon $14,400 per month, and has been entirely allocated to the above benefits. Rates are calculated on an average basis over the reporting period. (a) Total Claims Cost and Rate are based upon a weighted average of contributing and non-contributing.
Prepared by HealthComp 11/01/2016
YTD GAIN(LOSS)
50,485.44 (11 ,571.00) 146,215.12 514,215.36
$ 699,337.84
(344,433.35) (344,433.35)
$ (230, 1 07.64) $ (230, 1 07.64)
$ 50,301.00 $ 50,301.00
$ (58,659.70)
$_ 105,505.59

FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
CENSUS CATEGORY COUNT
Delta PPO 3112
PUDHMO 387
TOTAL
NOTES:
FINANCIAL ANALYSIS FOR DENTAL FOUR MONTHS ENDING OCTOBER 31, 2016
CLAIMS FIXED TOTAL COSTS COSTS COSTS RATE INTEREST
$ 72.15 $ 4.96 $ 77.11 $ 86.00
$ - $ 40.70 $ 40.70 $ 86.00
. NET GAIN(LOSS)
$ 8.89
$ 45.30
Claims Costs and Census Count represent average per month over the reporting period. All interest revenue has been allocated to Medical. Rates are calculated on an average basis over the reporting period.
Prepared by HealthComp 11/01/2016
YTD .
GAIN(LOSS)
$ 11 0,662. 72 •
$ 70,124.40
$ 180,787.12

FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
SPECIFIC STOP LOSS THROUGH 9/30/16
INCURRED: 07/0I/I5 THRU: 06/30/I6 PAID· 07/01/15 THRU· 09/30/16
DEDUCTIBLE: $175k, $350k & S500k CARRIER· NONE
~ 1 2
4 15 6 7 8 9 10 11 12 13
50%
1 2 3
5 6 7 8 9 10
! 11 112
13 14 15 i16
PREMIUM
DEDUCTIBLE 175,000 350,000 500,000
FISCAL YEAR
$
NET PAID
2•:4, i.40 5' \3.41 2! .27
'.44 177,293.37 201,750.17
20~~97 514 19 184 .12
NET PAID 1 120,673.01 111. 124.~64
113 155.76 1• 157,227.47 107,803.76 174,791 \1 90,886. 19
11t::o?R" 11 189.18 11 017.36
AMOUNT 84,678.83
34: ·~ 7E 202 )3.36 ,51
i7 ?~
58 2117.44
1.17
~iill $ 1, ,
STILL TO MEET 4
01 50,313.36 65,391.51 4
r72.53
18.5! 8• 13.5' 51 '3.41 6: 0.8: (
a; .335.47
I $ 1 ,940,375.03 $ A~O,A?A 07
PER MEMBER $ 45.17 $ 16.57 $ 9.46
PREMIUM $ 1,703,767.23 $ 625,003.83 $ 356,821.74
SA VINGS/(LOSS) $500 DEDUCTIBLE
CLAIMS OVER DEDUCTIBLE SA VINGS/(LOSS)
$ 1 ,329,385.61 $ 374 381.62 $ 360,734.95 $ 264 268.88 $ 32,231.59 $ 324 590.15

INCURRED: 07/01/16 THRU: 06/30/17 PAID: 07/01/16 THRU: 12/31/17
OVER $500 000 00 '
FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
SPECIFIC STOP LOSS THROUGH 10/31/16
DEDUCTIBLE: $175k, $350k & $500k CARRIER: BCS Insurance Company
MEMBER NET PAID CLAIM AMOUNT
$ - $ -
50% OVER $250,000 00 MEMBER NET PAID STILL TO MEET 1 $ 300,328.32 $ 199,671.68
$ 300,328.32 $ 199,671.68
PREMIUM CLAIMS OVER
DEDUCTIBLE PER MEMBER PREMIUM DEDUCTIBLE SA VINGS/(LOSS) 175,000 $ 45.17 $ 582,512.32 $ - $ 582,512.32 350,000 $ 16.57 $ 213,686.72 $ - $ 213,686.72 500,000 $ 9.69 $ 124,962.24 $ - $ 124,962.24
PRIOR YEAR RESULTS MEMBERS SA VINGS/(LOSS) $500 SA VINGS/(LOSS) SA VINGS/(LOSS) $175
FISCAL YEAR OVER$175K DEDUCTIBLE $300 DEDUCTIBLE DEDUCTIBLE 2008/2009 5 $ 275,694.78 $ 823,731.16 $ 1,333,752.01 2009/2010 11 $ 298,037.47 $ 660,094.16 $ 696,657.85 2010/2011 7 $ 571,249.08 $ 901,645.80 $ 2,451,452.16 2011/2012 12 $ 392,141.96 $ 562,653.55 $ 1,543,342.62 2012/2013 4 $ 690,024.10 $ 1,115,261.30 $ 3,286,763.75 2013/2014 11 $ 892,384.76 $ 1,450,290.57 $ 3,807,297.67 2014/2015 11 $ 546,018.60 $ 941,346.55 $ 3,782,202.62 2015/2016 13 $ 324,590.15 $ 264,268.88 $ 374,381.62
TOTAL 74 $ 3,990,140.90 $ 6,719,291.97 $ 17,275,850.30

PAID CLAIMS LAG TIME ANALYSIS Incurred: 01/01/1990-10/31/2016 I Paid Dates: 10/01/2016-10/31/2016
FRESNO CITY EMP H&W TRUST SUMMARY
RANGE OF INCURRED OATE RECEIVE DATE PROCESS DATE DAYS LAGGED TO RECEIVED DATE TO PROCESS DATE TO PAID DATE
Claims I %Total I %Cum Claims I %Total! %Cum Claims I %Total I %Cum
0-7 1 '112 12.3%
8-14 2,828 31.2%
15-21 1,456 16.1%
22-28 855 9.4%
Over28 2,808 31.0%
TOTAL# OF CLAIMS: 9,059
AVERAGE DAYS FROM INCURRED TO RECEIVED: 52.8
AVERAGE DAYS FROM RECIEVED TO PROCESSED: 2
AVERAGE DAYS FROM PROCESSED TO PAID: 4.5
AVERAGE DAYS FROM RECEIVED TO PAID: 6.6
Underwnter(s) 100 I Group(s) 200 [ Proc!uct(s)· All j Network(s): All
12.3%
43.5%
59.6%
69.0%
100.0%
8,722 96.3% 96.3% 8,863 97.8% 97.8%
156 1.7% 98.0% 120 1.3% 99.2%
19 0.2% 98.2% 75 0.8% 100.0%
15 0.2% 98.4% 0 0.0% 100.0%
147 1.6% 100.0% 1 0.0% 100.0%
RECEIVE DATE TO PAID DATE
Claims] %Total
7,296 80.5%
1,434 15.8%
151 1.7%
21 0.2%
157 1.7%
Report: PdCtmsLag RUN TIME: ~1/1/20162:28:08 PM PAGE 1 OF 1
%Cum
80.5%
96.4%
98.0%
98.3%
100.0%

FRESNO CITY EMPLOYEES HEALTH AND WELFARE TRUST
INSURANCE SERVICES
Fiduciary Liability Insurance Renewall/15/2017
1/15/16-17 1/15/17-18 Current Policy Renewal
Insurer Federal Ins./Chubb Federal Ins./Chubb A.M. Best's Rating 'A++' XV 'A++' XV
Each Loss $1,000,000 $1,000,000 Each Policy 1,000,000 1,000,000 Deductible 5,000 5,000
ERISA Section 502(1) & (i) (20% & 5% Penalties) Included Included
HIPAA Included Included Civil Penalties- Sub limit 1,000,000 1,000,000
EPCRS Sanctions -Sublimit 100,000 100,000 Tmstee Non-Fiduciary- (Settlm)
(civil penalties sublimit) 250,000 250,000 (Defense Only) (Defense On/)')
Spousal Extension-(incl. spouse/domestic partner) Included Included
PPACA Civil Monies Penalties-sublimit 100,000 100,000 Non-Monetary Demands Covered Covered COBRA Extension Included Included
'ANNUAL' PREMIUM $4,525 $4,955 Plus "Waiver of Recourse" Total Waiver Premium- (perfiduciary) 25 25
SS.mpla Dlsdalmer: This document Is for presentation purposes only. The predsa coverage afforded Is subject to the terms, conditions and exclusions of tha policies as Issued. Barney & Barney makes no representations, either expressed or Implied, as to the adequacy of any limits of protection. Determination of the adequacy of the limits of protection Is your responsibility.
CA lnstJranceUc. 0!118131 MARSH&Mttf.NNAN MiFNCY
111212016

BARNEY&BARNEY' Marsh & Mclennan Insurance AgencyllC
MARSH & McLENNAN AGENCY
Lockbox 740663 Los Angeles, CA 90074 Ph: 800.321.4696 Fax: 858.452.7530 CA Insurance LIC: OH18131 www.barneyandbarney.com
---------- I N V 0 I C E ----------
Fresno City Employees H & W Trust; % He Post Office Box 45018 Fresno, CA 93718-5018
Named Insured: Fresno City Employees H & W Trust
Invoice Date Invoice No. Bill-To Code Client Code lnv Order No.
11/02/16 98087 FRESCITY FRESCITY 20*155972
Amount Remitted: $ Please return this portion v.ilh your payment.
Make checks payable to: Marsh & McLennan Agency LLC
Effective Date Policy Period
01/15/17 01/15/17 to
01/15/18
Coverage Description
Federal Insurance Company Policy No. 81708103 Renewal - Fiduciary Liability
Premium Due for Fiduciary Liability Renewal Policy.
Thank you!
Invoice Number: 98087 Amount Due:
Transaction Amount
4,955.00
4,955.00
• *Payments are due upon receipt of the Invoice. Please make check payable to Marsh & Mclennan Agency LLC* *
MOLM Page: 1 ORIGINAL INVOICE

Affordable Care Act-Transitional Reinsurance Program
Another requirement of the Affordable Care Act (ACA) relates to payments by self-insured plans
pursuant to the Transitional Reinsurance Program (TRP). Governmental entities and their subdivisions
are not exempt from the requirement. The purpose of the TRP is to stabilize premiums in the individual
market (Exchanges). For the 2014, 2015 and 2016 benefit (calendar years), the TRP has/will collect
contributions from Contributing Entities to fund reinsurance payments to Exchanges that cover high
cost individuals, the administrative costs of operating the reinsurance program and contribution to the
General Fund of the Treasury. Submission of certain Information and payment of the TRP fee is required
by Contributing Entitles (i.e. Plan Sponsors.)
The TRP fee is based on the Contributing Entity's Gross Annual Enrollment Count. The Gross Annual
Enrollment Count is the total number of Covered Lives enrolled in the Plan. The number must include all
persons enrolled in the Plan including employees and all dependents. However, the number does not
need to include any individuals for whom the Plan is not the primary payor (e.g. the member has
Medicare which is primary or has other group or individual coverage which is primary.) Also, any
individuals listed in the Plan as the dependent of more than one employee (e.g. such as a child whose
parents both work for the same employer) may be counted once. All documentation sufficient to
substantiate the Gross Annual Enrollment Count must be maintained for at least 10 years.
For the calendar year of 2016, the fee is $27.00 per Covered Life. As with the contribution for prior
years, Contributing Entities are given the option of remitting the payment for 2016 by two installments
with the first installment based on $21.60 per Covered Life due on or before January 17,2017 and the
second installment based on $5.40 per Covered Life due on or before November 15, 2017. The
contribution for calendar year 2016 is scheduled to be the final year for the fee.
HealthComp calculated the number of Covered Lives and completed the required submission process for
the Fresno City Employees Health and Welfare Trust for 2016. The total payment due is $147,785.04.
The first installment of $118,228.03 is scheduled for payment on December 30, 2016. The second
installment of $29,557.01 is scheduled for payment on October 31, 2017.

Total
Uoclerwrltcr(s): 100 I Grcup(s): 200 All Oep!S 1 Product: Medica!
Total Dependent
l-l.eal ...... -.11("'- -c::.
Census Summary for Transitional Reinsurance Program FRESNO CITY EMP H&W TRUST
For Underwriter(s): 100 I Group(s): 200 I Product: Medical I Status(es): A C L N M 0 P R S
Exempted Covered
Net Covered
Date
PAGE 1 OF 1
Total Self-Only
OtherThari Self-only coverage
Total Factor
Exempted Covered
Net Covered
1 011312016 8:47:38 AM census\\spRpt_CensusSumm:~ryl'orTRP.rd!

Tom Georgouses I HealthComp
From: Sent: To: Subject:
[email protected] Friday, October 28, 2016 4:19 PM Tom Georgouses I HealthComp Pay.gov Payment Confirmation: ACA TRP BY2016
Your payment has been submitted to Pay.gov and the details are below. To confirm that the payment processed as expected, you may refer to your bank statement on the scheduled payment date. If you have any questions or wish to cancel this payment, you will need to contact the agency you paid at your earliest convenience.
If you chose the option to receive payment reminders in your user profile and this is a deferred or recurring payment, you will receive a reminder email several days before the payment is processed. You may change your payment reminder preferences and email address In your user profile at any time.
If you wish to cancel this transaction, log in to your account at https:Uwww.pay.gov/ and choose the Pending tab of the Payment Activity page.
Application Name: ACA TRP BY2016
Pay.gov Tracking ID: -::::. Agency Tracking ID: 1
Account Holder Name: City of Fresno Transaction Type: ACH Debit Transaction Amount: $118,228.03 Payment Date: 12/30/2016 Account Type: Business Checking
Routing Number: ::=::.1111111111111 Account Number:
Transaction Date: 10/28/2016 07:19:30 PM EDT Total Payments Scheduled: 1 Frequency: OneTime
THIS IS AN AUTOMATED MESSAGE. PLEASE DO NOT REPLY.

Tom Georgouses I HealthComp
From: [email protected] Sent: To:
Friday, October 28, 2016 4:35 PM Tom Georgouses I HealthComp
Subject: Pay.gov Payment Confirmation: ACA TRP BY2016
Your payment has been submitted to Pay.gov and the details are below. To confirm that the payment processed as expected, you may refer to your bank statement on the scheduled payment date. If you have any questions or wish to cancel this payment, you will need to contact the agency you paid at your earliest convenience.
If you chose the option to receive payment reminders in your user profile and this is a deferred or recurring payment, you will receive a reminder email several days before the payment is processed. You may change your payment reminder preferences and email address in your user profile at any time.
If you wish to cancel this transaction, log in to your account at https://www.pay.gov/ and choose the Pending tab of the Payment Activity page.
Application Name: ACA TRP BY2016
Pay.gov Tracking ID:· ~===~ Agency Tracking ID: I
Account Holder Name: City of Fresno Transaction Type: ACH Debit Transaction Amount: $29,557.01 Payment Date: 10/31/2017 Account Type: Business Checking
Routing Number: a:::: ••• Accouni Number:tll
Transaction Date: 10/28/2016 07:35:00 PM EDT Total Payments Scheduled: 1 Frequency: OneTime
THIS IS AN AUTOMATED MESSAGE. PlEASE DO NOT REPLY.
1

Michelle Bugg I HealthComp
From: Sent:
Patron, Linda <[email protected]> Monday, October 17, 2016 2:49 PM
To: Michelle Bugg I HealthComp Cc: Subject:
Tom Georgouses I HealthComp; Jim Rhein; Hammack, Georgia Fresno City Trust -Quest Diagnostics - New Policy
Hello Michelle,
This emails is in follow-up to the discussion during the September board meeting regarding Quest Diagnostic's "Easy Pay'' practice. Blue Shield has been working with Quest to set-up a practice for Fresno City members which will hopefully eliminate the issues they have been experiencing regarding being asked to make some type of payment at the time services are rendered.
Today Quest Diagnostic implemented a new policy as it relates to Fresno City Health and Welfare Trust membersbelow is the new process:
Commitment From Quest Diagnostics: as per our discussion today (October 17, 2016), we received the OK from our billing department to turn off the EasyPay prompt for the Fresco City members temporarily, and monitor the non-payment rates during this time period. If the data indicates that we need to revisit this process, we will certainly reach out to Blue Shield to discuss before making any changes.
Blue Shield will keep you updated regarding the monitoring of this new policy. Please let Georgia and I know if you hear of any issues around this new policy not being their true experience.
Let me know if you have any questions, Linda
Linda Patron Sr. Account Manager! Premier Accounts Blue Shield of California 3021 Reynolds Ranch Parkway, S-2-052 Lodi, CA 95240
p: 209-371-3185 c: 209-329-2865 f: 209-371-5828 linda. [email protected] Lie OD00062
Premier Accounts I blue W of california
This message (including any attachments) contains business proprietary/confidential information intended for a specific individual and purpose and is protected by law. If you are not the intended recipient, you should delete this message and all attachments from your computer or email server. Any disclosure, copying, or distribution of this message, or the taking of any action based on it, without the express permission of the originator, is strictly prohibited.
1

Michelle Bugg I HealthComp
From: Sent: To:
Patron, Linda <[email protected]> Wednesday, September 21, 2016 10:13 AM Michelle Bugg I HealthComp
Cc: Hammack, Georgia Subject: Cologuard Colon Cancer Screening - BSC's Response
Hello Michelle,
Below is Blue Shield's Medical Directors response to the question raised in September's Board meeting regarding "Cologuard". Please feel free to share this response with the Board and the public:
Blue Shield of California (BSC) thanks you for your interest in our policy regarding the colon cancer screening test "Cologuard," or "the multi-target stool DNA (MT-sDNA) Test." BSC has thoroughly investigated the merits and pitfalls of this test, including discussion with representatives of the company making the test (Exact Sciences Corporation) and several national experts on the topic, as well as exhaustive reviews of current medical literature. BSC finds that, even though one Cologuard test may have mildly increased sensitivity to detecting colon cancer than one FIT (fecal immunochemical test) alone, the Cologuard lest does not have a higher cancer detection rate, carriers a higher risk of needing a colonoscopy, and is less cost effective than either FIT test every year or screening colonoscopy every ten years. BSC also notes that major medical societies, including the United States Preventive Services Task Force and the Gastroenterology professional societies, have yet to endorse or require this test as a colon cancer screening method.
BSC remains committed to providing the best screening method to prevent colon cancer for its members, but we are not convinced that MT -sDNA testing is as good as other recommended screening tests. BSC is unaware of a scientific reason this test is reimbursed by another California commercial payer and by Medicare. BSC remains attentive to further research on this innovative means of colon cancer screening, and will consider new evidence supporting its use if and when this evidence becomes available.
REFERENCE: Ladabaum U, Mannalilhara A, Comparative Effectiveness and Cost-Effectiveness of a Multi-target Stool DNA Test to Screen for Colorectal Neoplasia, Gastroenterology (2016), doi: lO.l053/j.gastro.2016.06.003.
Let me know if you have additional questions.
Have a great day, linda Linda Patron Sr. Account Manager! Premier Accounts Blue Shield of California 3021 Reynolds Ranch Parkway, S-2-052 Lodi, CA 95240
p: 209-371-3185 c: 209-329-2865 f: 209-371-5828 [email protected] Lie 0000062
[§] This message (including any attachments) contains business proprietary/confidential information intended for a specific individual and purpose and is protected by law. If you are not the intended recipient, you should delete this message and all attachments from your computer or email server. Any disclosure, copying, or distribution of this message, or the taking of any action based on it, without the express permission of the originator, is strictly prohibited.
1

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
Client: City of Fresno
Measures October 2015 November 2015 December 2015 January 2016 February 2016 March 2016 April 2016 May 2016
Membership
Avg Eligible Members 9,235 9,182 9,243 9,381 9,430 9,359 9,338 9,356
Total Utilizing Members 2,651 2,552 2,647 2,635 2,713 2,731 2,623 2,601
% Utilizing Members 28.7% 27.8% 28.6% 28.1% 28.8% 29.2% 28.1% 27.8%
Avg Member Age 33.24 33.21 33.17 32.97 32.88 32.96 33.01 33.02
Rx and Cost
Total Rxs 6,551 6,117 6,750 6,503 6,687 6,901 6,342 6,399
Total Drug Cost $996,548.00 $989,818.88 $1,066,699.27 $1,042,177.08 $1,091,714.68 $1,188,677.54 $1,126,259.49 $1,240,615.20
Total Plan Paid $890,111.64 $897,694.76 $961,696.30 $935,054.75 $981,251.00 $1,059,538.20 $1,015,806.93 $1,131,313.93
Total Member Paid $106,436.36 $92,124.12 $105,002.97 $107,122.33 $110,463.68 $129,139.34 $110,452.56 $109,301.27
Total Ingredient Cost $987,490.98 $981,385.83 $1,057,378.25 $1,033,111.03 $1,082,443.40 $1,179,181.14 $1,117,448.99 $1,231,718.02
Total Dispensing Fee $9,057.00 $8,433.02 $9,320.95 $9,066.05 $9,271.28 $9,496.40 $8,810.45 $8,897.18
Total Sales Tax $0.02 $0.03 $0.07 $0.00 $0.00 $0.00 $0.05 $0.00
% Plan Paid 89.3% 90.7% 90.2% 89.7% 89.9% 89.1% 90.2% 91.2%
% Member Paid 10.7% 9.3% 9.8% 10.3% 10.1% 10.9% 9.8% 8.8%
Avg Drug Cost / Rx $152.12 $161.81 $158.03 $160.26 $163.26 $172.25 $177.59 $193.88
Avg Plan Paid / Rx $135.87 $146.75 $142.47 $143.79 $146.74 $153.53 $160.17 $176.80
Avg Member Paid / Rx $16.25 $15.06 $15.56 $16.47 $16.52 $18.71 $17.42 $17.08
Per Member Per Month
Avg Rxs PMPM 0.71 0.67 0.73 0.69 0.71 0.74 0.68 0.68
Avg Drug Cost PMPM $107.91 $107.80 $115.41 $111.09 $115.77 $127.01 $120.61 $132.60
1 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the
individual or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

Oct 22, 20166:50:03 AM
Client: City of Fresno
Measures June 2016 July 2016 August 2016 September 2016 Rolling Total
Membership
Avg Eligible Members 9,412 9,442 9,426 9,479 9,357
Total Utilizing Members 2,571 2,474 2,627 2,603 2,619
% Utilizing Members 27.3% 26.2% 27.9% 27.5% 28.0%
Avg Member Age 32.99 32.96 32.95 32.88 33.02
Rx and Cost
Total Rxs 6,328 5,954 6,531 6,245 77,308
Total Drug Cost $1,169,863.28 $1,118,008.11 $1,134,397.34 $1,190,135.30 $13,354,914.17
Total Plan Paid $1,052,487.55 $984,168.43 $1,011,606.40 $1,074,306.04 $11,995,035.93
Total Member Paid $117,375.73 $133,839.68 $122,790.94 $115,829.26 $1,359,878.24
Total Ingredient Cost $1,161,044.43 $1,109,763.22 $1,125,038.87 $1,180,547.71 $13,246,551.87
Total Dispensing Fee $8,818.85 $8,242.51 $9,138.70 $8,680.87 $107,233.26
Total Sales Tax $0.00 $2.38 $6.57 $5.12 $14.24
% Plan Paid 90.0% 88.0% 89.2% 90.3% 89.8%
% Member Paid 10.0% 12.0% 10.8% 9.7% 10.2%
Avg Drug Cost / Rx $184.87 $187.77 $173.69 $190.57 $172.75
Avg Plan Paid / Rx $166.32 $165.30 $154.89 $172.03 $155.16
Avg Member Paid / Rx $18.55 $22.48 $18.80 $18.55 $17.59
Per Member Per Month
Avg Rxs PMPM 0.67 0.63 0.69 0.66 0.69
Avg Drug Cost PMPM $124.29 $118.41 $120.35 $125.55 $118.94
2 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the
individual or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
Client: City of Fresno
Measures October 2015 November 2015 December 2015 January 2016 February 2016 March 2016 April 2016 May 2016
Avg Plan Paid PMPM $96.38 $97.77 $104.05 $99.68 $104.06 $113.21 $108.78 $120.92
Avg Member Paid PMPM $11.53 $10.03 $11.36 $11.42 $11.71 $13.80 $11.83 $11.68
Drug Type
% Single-Source Brand Rxs 19.1% 18.4% 18.7% 17.3% 17.7% 18.8% 18.0% 16.8%
% Multi-Source Brand Rxs 1.6% 1.4% 1.4% 1.3% 1.2% 1.4% 1.5% 1.7%
% Generic Rxs 79.3% 80.2% 79.9% 81.4% 81.0% 79.8% 80.4% 81.5%
% Generic Efficiency 98.0% 98.3% 98.3% 98.4% 98.5% 98.3% 98.1% 97.9%
Drug Channel
% Retail Rxs 79.8% 80.1% 80.3% 81.1% 81.1% 80.5% 80.6% 80.4%
% Retail 90 Rxs 12.4% 11.7% 11.8% 11.9% 11.2% 11.3% 12.0% 12.0%
% Mail Rxs 7.8% 8.2% 7.9% 7.1% 7.7% 8.1% 7.4% 7.6%
Specialty Drugs
Total Specialty Rxs 50 55 57 56 59 62 64 69
Total Specialty Drug Cost $194,533.53 $254,628.79 $225,570.47 $237,628.13 $294,134.43 $280,520.03 $332,272.76 $404,573.67
Total Specialty Plan Paid $189,295.59 $249,541.97 $220,445.84 $232,147.24 $288,388.50 $267,150.46 $322,311.39 $395,540.44
Total Specialty Member Paid $5,237.94 $5,086.82 $5,124.63 $5,480.89 $5,745.93 $13,369.57 $9,961.37 $9,033.23
% Specialty Rxs 0.8% 0.9% 0.8% 0.9% 0.9% 0.9% 1.0% 1.1%
% Specialty of Total Drug Cost 19.5% 25.7% 21.1% 22.8% 26.9% 23.6% 29.5% 32.6%
% Specialty of Total Plan Paid 21.3% 27.8% 22.9% 24.8% 29.4% 25.2% 31.7% 35.0%
% Specialty of Total Member Paid 4.9% 5.5% 4.9% 5.1% 5.2% 10.4% 9.0% 8.3%
Avg Specialty Rxs PMPM 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01
3 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the
individual or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

Oct 22, 20166:50:03 AM
Client: City of Fresno
Measures June 2016 July 2016 August 2016 September 2016 Rolling Total
Avg Plan Paid PMPM $111.82 $104.23 $107.32 $113.34 $106.83
Avg Member Paid PMPM $12.47 $14.17 $13.03 $12.22 $12.11
Drug Type
% Single-Source Brand Rxs 16.4% 16.1% 17.1% 16.4% 17.6%
% Multi-Source Brand Rxs 1.7% 1.7% 1.4% 1.4% 1.5%
% Generic Rxs 82.0% 82.2% 81.5% 82.1% 80.9%
% Generic Efficiency 98.0% 98.0% 98.3% 98.3% 98.2%
Drug Channel
% Retail Rxs 79.8% 79.9% 79.6% 80.3% 80.3%
% Retail 90 Rxs 12.8% 12.7% 12.6% 12.3% 12.0%
% Mail Rxs 7.4% 7.4% 7.8% 7.3% 7.7%
Specialty Drugs
Total Specialty Rxs 57 53 58 73 713
Total Specialty Drug Cost $318,142.38 $292,040.09 $249,576.02 $395,634.60 $3,479,254.90
Total Specialty Plan Paid $311,555.72 $265,142.05 $238,142.34 $384,767.02 $3,364,428.56
Total Specialty Member Paid $6,586.66 $26,898.04 $11,433.68 $10,867.58 $114,826.34
% Specialty Rxs 0.9% 0.9% 0.9% 1.2% 0.9%
% Specialty of Total Drug Cost 27.2% 26.1% 22.0% 33.2% 26.1%
% Specialty of Total Plan Paid 29.6% 26.9% 23.5% 35.8% 28.0%
% Specialty of Total Member Paid 5.6% 20.1% 9.3% 9.4% 8.4%
Avg Specialty Rxs PMPM 0.01 0.01 0.01 0.01 0.01
4 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the
individual or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
Client: City of Fresno
Measures October 2015 November 2015 December 2015 January 2016 February 2016 March 2016 April 2016 May 2016
Avg Specialty Drug Cost PMPM $21.06 $27.73 $24.40 $25.33 $31.19 $29.97 $35.58 $43.24
Avg Specialty Plan Paid PMPM $20.50 $27.18 $23.85 $24.75 $30.58 $28.54 $34.52 $42.28
Avg Specialty Member Paid PMPM $0.57 $0.55 $0.55 $0.58 $0.61 $1.43 $1.07 $0.97
Avg Non-Specialty Rxs PMPM 0.70 0.66 0.72 0.69 0.70 0.73 0.67 0.68
Avg Non-Specialty Drug Cost PMPM $86.85 $80.07 $91.00 $85.76 $84.58 $97.04 $85.03 $89.36
Avg Non-Specialty Plan Paid PMPM $75.89 $70.59 $80.20 $74.93 $73.47 $84.67 $74.27 $78.64
Avg Non-Specialty Member Paid PMPM $10.96 $9.48 $10.81 $10.83 $11.10 $12.37 $10.76 $10.72
5 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the
individual or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

Oct 22, 20166:50:03 AM
Client: City of Fresno
Measures June 2016 July 2016 August 2016 September 2016 Rolling Total
Avg Specialty Drug Cost PMPM $33.80 $30.93 $26.48 $41.74 $30.99
Avg Specialty Plan Paid PMPM $33.10 $28.08 $25.26 $40.59 $29.96
Avg Specialty Member Paid PMPM $0.70 $2.85 $1.21 $1.15 $1.02
Avg Non-Specialty Rxs PMPM 0.67 0.62 0.69 0.65 0.68
Avg Non-Specialty Drug Cost PMPM $90.49 $87.48 $93.87 $83.82 $87.95
Avg Non-Specialty Plan Paid PMPM $78.72 $76.15 $82.06 $72.74 $76.86
Avg Non-Specialty Member Paid PMPM $11.77 $11.33 $11.81 $11.07 $11.09
6 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the
individual or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
Selected FiltersClient(s): City of FresnoCarrier(s): PCN-PHARMACEUTICAL CARE NETWKAccount(s): AllGroup(s): All
Group Report By: Client Member Family ID: All
Care Facility: All Member ID: All
Plan Code: All Member First Name: All
Member Rider: All Member Last Name: All
Member Product: All Member City: All
Date Type: Rolling 12 Months - Closed Months Member State: All
Start Date: October 2015 Member Zip: All
End Date: September 2016 Member Gender: All
Relative Description: Date Submitted Member Age Band: All
Net Paid Claims Only: Yes Pharmacy NCPDP ID: All
Drug Group (GPI 02): All Pharmacy NPI: All
Drug Class (GPI 04): All Pharmacy Name: All
Drug Subclass (GPI 06): All Pharmacy City: All
Drug Basic Name (GPI 08): All Pharmacy State: All
Drug Extended Name (GPI 10): All Pharmacy Zip: All
Drug Dosage Form (GPI 12): All Pharmacy Affiliation: All
Drug Name: All Pharmacy Network: All
Drug Name and Strength: All Mail / Retail: All
7 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the individual
or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
Drug GPI: All Prescriber DEA ID: All
Drug NDC: All Prescriber NPI: All
Drug Manufacturer: All Prescriber First Name: All
Rx / OTC: All Prescriber Last Name: All
Brand / Generic: All Prescriber City: All
Specialty / Non-Specialty: All Prescriber State: All
Drug DEA Code: All Drugs Prescriber Zip: All
Drug Disease: All Prescriber Specialty: All
Drug Therapeutic Group: All Display Report Description: Yes
Pharmacy NCPDP ID Include/Exclude: Include Time Period: Monthly
Pharmacy NPI Include/Exclude: Include Pharmacy NCPDP ID: All
Pharmacy NPI: All
Report Description
Report Overview:
XXXXXXXXXXXXXXXXXXXXXXXX
Detail Line Description:
Column Name Description
Carrier ID RxCLAIM® Carrier ID, alphanumeric. Part of basic four-tiered system (Carrier>Account>Group>Mbr) allowing for flexibility in defining benefit parameters for a group of people. Carriers are the highest level of the hierarchy used in RxCLAIM. A carrier is typically the company or organization who offers benefits to Mbrs.
Account ID Part of a four-tiered system (Carrier>Account>Group>Member) allowing for flexibility in defining benefit parameters for a group of people. Accounts are the second level of the hierarchy used in RxCLAIM. They belong to the Carrier. Accounts can be used by the carrier to categorize their business entities.
Group ID Part of a four-tiered system (Carrier>Account>Group>Member) allowing for flexibility in defining benefit parameters for a group of people. Groups are the third
8 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the individual
or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
level of the hierarchy used in RxCLAIM. They belong to the account. Carriers use groups to further divide accounts, so that specific benefits can be assigned to each group.
Avg Eligible Members The eligible claim count defined in RxTRACK by counting actual days in a month that a member was eligible.
Total Utilizing Members A distinct count of members that have at least one paid claim within the specified time frame.
% Utilizing Members The percentage of the total utilizing members.
Avg Member Age Average member age during the reporting period calculated using a combination of the client's eligibility age bands and member counts.
Total Rxs The total number of rxs.
Total Drug Cost The total drug cost.
Total Plan Paid
"Commercial:The Client Total Amount Due. Typically, amount due is calculated as follows: (Ingredient Cost + Dispensing Fee + Tax) – Patient Pay.Medicare Part D:The Client Total Amount Due. For Medicare Part D claims specifically, amount due is calculated as follows: (Ingredient Cost + Dispensing Fee + Tax + Incentive Fee) – Patient Pay. This calculation does not include LICS amount. However check your benefit setup as there is a flag that controls this value in RxCLAIM."
Total Member Paid"Commercial:The Client Total Patient Pay Amount. The patient pay would include copays and all other charges paid by the member.Medicare Part D:The Client Total Patient Pay Amount. For Medicare Part D claims specifically, the patient pay would include copays and all other charges paid by the member and does also include LICS amount."
Total Ingredient Cost The Client Ingredient Cost.
Total Dispensing Fee The Client Dispensing Fee.
Total Sales Tax The Client Sales Tax.
% Plan Paid The percentage the plan paid of the total drug cost.
% Member Paid The percentage the member paid of the total drug cost.
Avg Drug Cost / Rx The average drug cost per rx.
Avg Plan Paid / Rx The average plan cost per rx.
Avg Member Paid / Rx The average member cost per rx.
Avg Rxs PMPM The average number of rxs per member per month.
Avg Drug Cost PMPM The average drug cost per member per month.
Avg Plan Paid PMPM The average plan cost per member per month.
9 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the individual
or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
Avg Member Paid PMPM The average member cost per member per month.
% Single-Source Brand Rxs The percentage of rxs filled with a single-source brand drug.
% Multi-Source Brand Rxs The percentage of rxs filled with a multi-source brand drug.
% Generic Rxs The percentage of rxs filled with a generic drug.
% Generic Efficiency The percentage of the use of a generic rx where one could potentially be used.
% Retail Rxs The percentage of rxs filled at a retail pharmacy.
% Retail 90 Rxs The percentage of rxs filled at a retail pharmacy where days supply meets "Retail 90" rules.
% Mail Rxs The percentage of rxs filled at a mail order pharmacy.
Total Specialty Rxs The total number of specialty drug rxs.
Total Specialty Drug Cost The total drug cost of specialty drug rxs.
Total Specialty Plan Paid The total plan cost of specialty drug rxs.
Total Specialty Member Paid The total member cost of specialty drug rxs.
% Specialty Rxs The percentage of rxs filled with a specialty drug.
% Specialty of Total Drug Cost The percentage specialty of the total drug cost.
% Specialty of Total Plan Paid The percentage specialty of the total plan paid.
% Specialty of Total Member Paid The percentage specialty of the total member paid.
Avg Specialty Rxs PMPM The average number of specialty rxs per member per month.
Avg Specialty Drug Cost PMPM The average specialty drug cost per member per month.
Avg Specialty Plan Paid PMPM The average specialty plan cost per member per month.
Avg Specialty Member Paid PMPM The average specialty member cost per member per month.
Avg Non-Specialty Rxs PMPM The average number of non-specialty rxs per member per month.
Avg Non-Specialty Drug Cost PMPM The average non-specialty drug cost per member per month.
Avg Non-Specialty Plan Paid PMPM The average non-specialty plan cost per member per month.
10 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the individual
or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

CONFIDENTIALReport View of RXT1020DM - Executive Summary by Time
Period_City of Fresno EmployeesDate Submitted From October 2015 Through September 2016
Oct 22, 20166:50:03 AM
Avg Non-Specialty Member Paid PMPM The average non-specialty member cost per member per month.
11 of 11 Report View of RXT1020DM - Executive
Summary by Time Period_City of Fresno
EmployeesThis document, including any associated documents, may contain information that is confidential and may be privileged and exempt from disclosure under applicable law. It is intended solely for the use of the individual
or entity for which it is created. If you are not the intended recipient of this information, you are hereby notified that any use, disclosure, dissemination, or copying of this document is strictly prohibited. If you have received this document in error, please notify the distributor. Thank you for your cooperation.

Fresno City Employees Health & Welfare Trust
Medicare Prescription Drug Plan (Employer PDP),
administered by OptumRx
Annual Notice of Changes for 2017
You are currently enrolled as a member of Fresno City Employees Health & Welfare Trust.
Next year, there may be some changes to the plan’s costs and benefits. This booklet tells
about any possible changes, which will take effect January 1, 2017.
OptumRx® Member Services: For help or information, please call the OptumRx Member Services or go to our plan website
optumrx.com.
OptumRx Member Services (Calls to these numbers are free):
1-866-443-1095
TTY users call: 711
Hours of Operation:
24 hours a day, 7 days a week
Visit our website at optumrx.com
Optum Insurance of Ohio, Inc. is a Medicare approved Part D sponsor and administers this
plan through its pharmacy benefit manager, OptumRx, on behalf of your employer, union or
trustees of a fund. If you need this information in another language or alternate format
(Braille, large print, audio), please contact OptumRx Member Services at the number located
on the back of your ID card.
S8841_17_MC-DS02_FRS
Fresno City Employees
Health & Welfare Trust

2
Annual Notice of Changes for 2017
Table of Contents
Think about Your Medicare Coverage for Next Year ...............................................................3
Summary of Important Costs for 2017 ........................................................................................4
SECTION 1 Changes to Benefits and Costs for Next Year ....................................................5
Section 1.1 – Changes to the Monthly Premium .......................................................................5
Section 1.2 – Changes to the Pharmacy Network ......................................................................5
Section 1.3 – Changes to Part D Prescription Drug Coverage ..................................................5
SECTION 2 Deciding Which Plan to Choose ..........................................................................8
Section 2.1 – If you want to stay in our plan .............................................................................8
Section 2.2 – If you want to change plans .................................................................................8
SECTION 3 Deadline for Changing Plans ...............................................................................9
SECTION 4 Programs That Help Pay for Prescription Drugs ..............................................9
SECTION 5 Questions?..............................................................................................................9
Section 5.1 – Getting Help from our plan ..................................................................................9
Section 5.2 – Getting Help from Medicare ..............................................................................10

3
Think about Your Medicare Coverage for Next Year
Important things to do:
Check the changes to our benefits and costs to see if they affect you. It is important
to review benefit and cost changes to make sure they will work for you next year. Look
in Section 2 for information about benefit and cost changes for our plan.
Check the changes to our prescription drug coverage to see if they affect you. Will
your drugs be covered? Are they in a different tier? Can you continue to use the same
pharmacies? It is important to review the changes to make sure our drug coverage will
work for you next year.
Think about your overall costs in the plan. How much will you spend out-of-pocket
for the services and prescription drugs you use regularly? How much will you spend on
your premium? How do the total costs compare to other Medicare coverage options?
Think about whether you are happy with our plan.
If you decide to stay with Fresno City Employees Health & Welfare Trust:
If you want to stay with us next year, it’s easy - you don’t need to do anything. You will
remian enrolled in our plan.
If you decide to change plans:
If you decide other coverage will better meet your needs, you can switch plans anytime during
the year. If you enroll in another prescription drug plan other than Fresno City Employees
Health & Welfare Trust, it may impact other benefits, such as medical coverage. Your new
coverage will begin on January 1, 2017.

4
Summary of Important Costs for 2017
The table below compares the 2016 costs and 2017 costs for Fresno City Employees Health
& Welfare Trust in several important areas. Please note this is only a summary of
changes. It is important to read the rest of this Annual Notice of Changes and review the
enclosed Evidence of Coverage to see if other benefit or cost changes affect you.
2016 (this year)
Covered Prescription
Drugs
Retail Pharmacy
(up to a 30-day
supply)
Retail Pharmacy
(up to a 90-day
supply)
Mail Order Pharmacy
(up to a 90-day supply)
Tier 1
(Generic Drugs) 10% 10% $5
Tier 2
(Preferred Brand
Drugs)
20% 20% $20
Tier 3
(Non-Preferred Brand
Drugs)
40% 40% $50
Tier 4
(Specialty Drugs) $100 $100 $100
There is no change for 2017 (next year)

Fresno City Employees Health & Welfare Trust Annual Notice of Changes for 2017 5
SECTION 1 Changes to Benefits and Costs for Next Year
Section 1.1 – Changes to the Monthly Premium
2015 (this year) 2016 (next year)
Monthly premium
(You must continue to pay
your Medicare Part B
premium.)
Please contact Fresno City
Employees Health &
Welfare Trust for more
information regarding any
plan premium you may
have.
Please contact Fresno City
Employees Health &
Welfare Trust for more
information regarding any
plan premium you may
have.
Your monthly plan premium will be more if you are required to pay a late enrollment
penalty.
If you have a higher income, you may have to pay an additional amount each month
directly to the government for your Medicare prescription drug coverage.
Your monthly premium will be less if you are receiving “Extra Help” with your
prescription drug costs.
Section 1.2 – Changes to the Pharmacy Network
Amounts you pay for your prescription drugs may depend on which pharmacy you
use. Medicare drug plans have a network of pharmacies. In most cases, your prescriptions are
covered only if they are filled at one of our network pharmacies.
There are changes to our network of pharmacies for next year.
An up to date Pharmacy Locator tool can be found on our website at optumrx.com. You may
also call OptumRx Member Services for updated pharmacy information.
Section 1.3 – Changes to Part D Prescription Drug Coverage
Changes to Our Drug List
Our list of covered drugs is called a Formulary or “Drug List.” We sent you a copy of our
Abridged Drug List in this envelope.
We made changes to our Drug List, including changes to the drugs we cover and changes to the
restrictions that apply to our coverage for certain drugs. Review the Drug List to make sure
your drugs will be covered next year and to see if there will be any restrictions. The Drug
List we included in this envelope includes many – but not all – of the drugs that we will cover

Fresno City Employees Health & Welfare Trust Annual Notice of Changes for 2017 6
next year. If you don’t see your drug on this list, it might still be covered. You can get the
complete Drug List by calling OptumRx Member Services (see the back cover) or visiting our
website (optumrx.com).
If you are affected by a change in drug coverage you can:
Work with your doctor (or other prescriber) and ask the plan to make an exception to cover the drug. You can ask for an exception before next year and we will give you an
answer before the change takes effect. To learn what you must do to ask for an exception,
see Chapter 7 of your Evidence of Coverage (What to do if you have a problem or
complaint (coverage decisions, appeals, complaints)) or call OptumRx Member Services.
Find a different drug that we cover. You can call OptumRx Member Services to ask for
a list of covered drugs that treat the same medical condition.
In some situations, we will cover a one-time, temporary supply. (To learn more about when you
can get a temporary supply and how to ask for one, see Chapter 5 of the Evidence of Coverage.)
During the time when you are getting a temporary supply of a drug, you should talk with your
doctor to decide what to do when your temporary supply runs out. You can either switch to a
different drug covered by the plan or ask the plan to make an exception for you and cover your
current drug.
If you currently have a formulary exception on file for the 2016 plan year, you may need to
submit a new request for an exception for 2017. The approval letter you received contains a start
and end date for the approval. Please refer to this letter to determine if a request for a new
exception is needed.
Changes to Prescription Drug Costs
There are four drug payment stages. How much you pay for a Part D drug depends on
which drug payment stage you are in.
The information below shows the four drug payment stages. You can also look in your Evidence
of Coverage for more information about the stages.
Note: If you are in a program that helps pay for your drugs (“Extra Help”), the information
about costs for Part D prescription drugs may not apply to you. We will send you a separate
insert, called the “Low Income Subsidy Rider” or the “LIS Rider”), which tells you about your
drug coverage. If you receive this insert, please call OptumRx Member Services at
1-866-443-1095, 24 hours a day, 7 days a week (TTY users call 711).
The information below shows the changes for next year to the first two stages – the Yearly
Deductible Stage and the Initial Coverage Stage. (Most members do not reach the other two
stages – the Coverage Gap Stage or the Catastrophic Coverage Stage. To get information about
your costs in these stages, look at Chapter 4 in the enclosed Evidence of Coverage.

Fresno City Employees Health & Welfare Trust Annual Notice of Changes for 2017 7
Changes to the Deductible Stage - there is no deductible or this plan.
2016 (this year) 2017 (next year)
Stage 1: Yearly Deductible Stage
Because we have no
deductible, this payment
stage does not apply to
you.
Because we have no
deductible, this payment
stage does not apply to
you.
Changes to Your Copayments in the Initial Coverage Stage
2016 (this year) 2017 (next year)
Stage 2: Initial Coverage
Stage
During this stage, the plan
pays its share of the cost of
your drugs and you pay
your share of the cost.
The costs in this row are for
a one-month (34-day) supply
when you fill your
prescription at a network
pharmacy.
Your cost for a one-month
supply filled at a network
pharmacy:
Generic Drugs:
You pay 10% of the total cost
Preferred Brand Drugs:
You pay 20% of the total cost
Non-Preferred Brand Drugs:
You pay 20% of the total cost
Specialty Drugs:
You pay 20% of the total cost
______________
Once your total drugs costs
have reached $4,850, you will
move to the next stage (the
Catastrophic Coverage Stage).
We have added a maximum
out-of-pocket limit of $3,400
for the calendar year. If you
reach this amount, the plan
will pay all of the cost of your
drugs for the rest of the year.
Your cost for a one-month
supply filled at a network
pharmacy:
Generic Drugs:
You pay 10% of the total cost
Preferred Brand Drugs:
You pay 20% of the total cost
Non-Preferred Brand Drugs:
You pay 20% of the total cost
Specialty Drugs:
You pay 20% of the total cost
______________
Once your total drugs costs
have reached $4,950, you will
move to the next stage (the
Catastrophic Coverage Stage).
We have added a maximum
out-of-pocket limit of $3,400
for the calendar year. If you
reach this amount, the plan
will pay all of the cost of your
drugs for the rest of the year.

Fresno City Employees Health & Welfare Trust Annual Notice of Changes for 2017 8
Changes to the Coverage Gap and Catastrophic Coverage Stages
The other two drug coverage stages – the Coverage Gap Stage and the Catastrophic Coverage
Stage – are for people with high drug costs. Most members do not reach the Coverage Gap Stage
or the Catastrophic Coverage Stage. For information about your costs in these stages, look at
Chapter 4 in your Evidence of Coverage.
SECTION 2 Deciding Which Plan to Choose
Section 2.1 – If you want to stay in Fresno City Employees Health & Welfare
Trust
To stay in our plan you don’t need to do anything. If you do not sign up for a different plan,
you will remain enrolled as a member of our plan for 2017.
Section 2.2 – If you want to change plans
We hope to keep you as a member next year but if you want to change for 2017 follow these
steps:
Step 1: Learn about and compare your choices
You can join a different Medicare prescription drug plan,
-- OR-- You can change to a Medicare health plan. Some Medicare health plans also
include Part D prescription drug coverage,
-- OR-- You can keep Original Medicare without a separate Medicare prescription drug
plan.
To learn more about Original Medicare and the different types of Medicare plans, read Medicare
& You 2017, call your State Health Insurance Assistance Program, or call Medicare.
You can also find information about plans in your area by using the Medicare Plan Finder on the
Medicare website. Go to http://www.medicare.gov and click “Find health and drug plans.” Here,
you can find information about costs, coverage, and quality ratings for Medicare plans.
Step 2: Change your coverage To change to a different Medicare prescription drug plan, enroll in the new plan. You
will automatically be disenrolled from Fresno City Employees Health & Welfare Trust.
To change to a Medicare health plan, enroll in the new plan. You will automatically be
disenrolled from Fresno City Employees Health & Welfare Trust.
To change to Original Medicare without a prescription drug plan, you can either:
o Send us a written request to disenroll. Contact OptumRx Member Services if you
need more information on how to do this (phone numbers are located on the front
page of this booklet).
o – or – Contact Medicare, at 1-800-MEDICARE (1-800-633-4227), 24 hours a
day, 7 days a week, and ask to be disenrolled. TTY users should call 1-877-486-
2048.

Fresno City Employees Health & Welfare Trust Annual Notice of Changes for 2017 9
SECTION 3 Deadline for Changing Plans
If you want to change to a different prescription drug plan or to a Medicare health plan for next
year, you can do it anytime of the year. The change will take effect on first day of the following
month.
SECTION 4 Programs That Help Pay for Prescription Drugs
You may qualify for help paying for prescription drugs. There are two basic kinds of help:
“Extra Help” from Medicare. People with limited incomes may qualify for Extra Help
to pay for their prescription drug costs. If you qualify, Medicare could pay up to seventy-
five (75) percent or more of your drug costs including monthly prescription drug
premiums, annual deductibles, and coinsurance. Additionally, those who qualify will not
have a coverage gap or late enrollment penalty. Many people are eligible and don’t even
know it. To see if you qualify, call:
o 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048, 24
hours a day/7 days a week;
o The Social Security Office at 1-800-772-1213 between 7 a.m. and 7 p.m.,
Monday through Friday. TTY users should call, 1-800-325-0778; or
o Your State Medicaid Office.
Help from your state’s pharmaceutical assistance program. There are programs that
help people pay for prescription drugs based on their financial need, age, or medical
condition. To learn more about the program, check with your State Health Insurance
Assistance Program.
Prescription Cost-sharing Assistance for Persons with HIV/AIDS. The AIDS Drug
Assistance Program (ADAP) helps ensure that ADAP-eligible individuals living with
HIV/AIDS have access to life-saving HIV medications. Individuals must meet certain
criteria, including proof of State residence and HIV status, low income as defined by the
State, and uninsured/under-insured status. Medicare Part D prescription drugs that are
also covered by ADAP qualify for prescription cost-sharing assistance. For information
on eligibility criteria, covered drugs, or how to enroll in the program, contact the program
in your local state of residence.
SECTION 5 Questions?
Section 5.1 – Getting Help from Fresno City Employees Health & Welfare Trust
Questions? We’re here to help. Please call OptumRx Member Services at 1-866-443-1095 (TTY
only, call 711). We are available for phone calls 24 hours a day, 7 days a week. Calls to these
numbers are free.

Fresno City Employees Health & Welfare Trust Annual Notice of Changes for 2017 10
Read your 2017 Evidence of Coverage (it has details about next year's
benefits and costs)
This Annual Notice of Changes gives you a summary of changes in your benefits and costs for
2017. For details, look in the 2017 Evidence of Coverage for Fresno City Employees Health &
Welfare Trust. The Evidence of Coverage is the legal, detailed description of your plan benefits.
It explains your rights and the rules you need to follow to get covered services and prescription
drugs. A copy of the Evidence of Coverage was included in this envelope.
Visit our website
You can also visit our website at optum.com. As a reminder, our website has the most up-to-date
information about our pharmacy network and our list of covered drugs (Formulary/Drug List).
Section 5.2 – Getting Help from Medicare
To get information directly from Medicare:
Call 1-800-MEDICARE (1-800-633-4227)
You can call 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY users
should call 1-877-486-2048.
Visit the Medicare website
You can visit the Medicare website (http://www.medicare.gov). It has information about cost,
coverage, and quality ratings to help you compare Medicare prescription drug plans. You can
find information about plans available in your area by using the Medicare Plan Finder on the
Medicare website. (To view the information about plans, go to http://www.medicare.gov and
click on “Compare Drug and Health Plans.”)
Read Medicare & You 2016
You can read Medicare & You 2017 Handbook. Every year in the fall, this booklet is mailed to
people with Medicare. It has a summary of Medicare benefits, rights and protections, and
answers to the most frequently asked questions about Medicare. If you don’t have a copy of this
booklet, you can get it at the Medicare website (http://www.medicare.gov) or by calling
1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY users should call
1-877-486-2048.

1
January 1, 2017 – December 31, 2017
Evidence of Coverage:
Your Medicare Prescription Drug Coverage as a Member of the
Fresno City Employees Health & Welfare Trust Medicare Prescription
Drug Plan (Employer PDP), administered by OptumRx
This booklet gives you the details about your Medicare prescription drug coverage from
January 1, 2017 – December 31, 2017. It explains how to get the prescription drugs you need.
This is an important legal document. Please keep it in a safe place.
OptumRx® Member Services Center:
For help or information, please call the OptumRx Member Services Center or go to our plan
website at optumrx.com.
1-866-443-1095
TTY users call: 711
Calls to these numbers are free.
Hours of Operation:
24 hours a day, 7 days a week
This plan is offered by the Fresno City Employees Health & Welfare Trust, referred throughout
the Evidence of Coverage as “we,” “us,” or “our.” The Fresno City Employees Health & Welfare
Trust Medicare Prescription Drug Plan is referred to as “plan” or “our plan.”
Optum Insurance of Ohio, Inc. is a Medicare approved Part D sponsor and administers this plan
through its pharmacy benefit manager, OptumRx, on behalf of the Fresno City Employees
Health & Welfare Trust.
If you need this information in other formats, such as Braille, large print or audio, please contact
OptumRx Member Services. Benefits, formulary, pharmacy network, premium, deductible,
and/or copayments/coinsurance may change on January 1, 2017.
S8841_17_MC-DS01_FRS
Fresno City Employees
Health & Welfare Trust

2
English: We have free interpreter services to answer any questions you may have about our health
or drug plan. To get an interpreter, just call us at 1-866-443-1095. Someone who speaks
English/Language can help you. This is a free service.
Spanish: Tenemos servicios de intérprete sin costo alguno para responder cualquier pregunta que
pueda tener sobre nuestro plan de salud o medicamentos. Para hablar con un intérprete, por favor
llame al 1-866-443-1095. Alguien que hable español le podrá ayudar. Este es un servicio gratuito.
Chinese Mandarin: 我们提供免费的翻译服务,帮助您解答关于健康或药物保险的任何疑问
。如果您需要此翻译服务,请致电 1-866-443-1095。 我们的中文工作人员很乐意帮助您。 这
是一项免费服务。
Chinese Cantonese: 您對我們的健康或藥物保險可能存有疑問,為此我們提供免費的翻譯服
務。如需翻譯服務,請致電 1-866-443-1095。我們講中文的人員將樂意為您提供幫助。這是
一項免費服務。
Tagalog: Mayroon kaming libreng serbisyo sa pagsasaling-wika upang masagot ang anumang mga
katanungan ninyo hinggil sa aming planong pangkalusugan o panggamot. Upang makakuha ng
tagasaling-wika, tawagan lamang kami sa 1-866-443-1095. Maaari kayong tulungan ng isang
nakakapagsalita ng Tagalog. Ito ay libreng serbisyo.
French: Nous proposons des services gratuits d'interprétation pour répondre à toutes vos questions
relatives à notre régime de santé ou d'assurance-médicaments. Pour accéder au service
d'interprétation, il vous suffit de nous appeler au 1-866-443-1095. Un interlocuteur parlant Français
pourra vous aider. Ce service est gratuit.
Vietnamese: Chúng tôi có dịch vụ thông dịch miễn phí để trả lời các câu hỏi về chương sức khỏe và
chương trình thuốc men. Nếu quí vị cần thông dịch viên xin gọi 1-866-443-1095 sẽ có nhân viên nói
tiếng Việt giúp đỡ quí vị. Đây là dịch vụ miễn phí .
German: Unser kostenloser Dolmetscherservice beantwortet Ihren Fragen zu unserem Gesundheits-
und Arzneimittelplan. Unsere Dolmetscher erreichen Sie unter 1-866-443-1095. Man wird Ihnen dort
auf Deutsch weiterhelfen. Dieser Service ist kostenlos.
Korean: 당사는 의료 보험 또는 약품 보험에 관한 질문에 답해 드리고자 무료 통역
서비스를제공하고 있습니다. 통역 서비스를 이용하려면 전화 1-866-443-1095번으로 문의해
주십시오. 한국어를 하는 담당자가 도와 드릴 것입니다. 이 서비스는 무료로 운영됩니다.
Russian: Если у вас возникнут вопросы относительно страхового или медикаментного
плана, вы можете воспользоваться нашими бесплатными услугами переводчиков. Чтобы
воспользоваться услугами переводчика, позвоните нам по телефону 1-866-443-1095. Вам
окажет помощь сотрудник, который говорит по-pусски. Данная услуга бесплатная.
Arabic: إننا نقدم خدمات المترجم الفوري المجانية للإجابة عن أي أسئلة تتعلق بالصحة أو جدول الأدوية
سيقوم شخص . 1095-443-866-1لدينا. للحصول على مترجم فوري، ليس عليك سوى الاتصال بنا على
.بمساعدتك. هذه خدمة مجانية ما يتحدث العربية
Hindi: हमारे स्वास््य या दवा की योजना के बारे में आपके ककसी भी प्रश्न के जवाब देने के लिए हमारे
पास मुफ्त दभुाषिया सेवाए ँउपिब्ध हैं. एक दभुाषिया प्राप्त करने के लिए, बस हमें 1-866-443-1095 पर
फोन करें. कोई व्यक्तत जो हहन्दी बोिता है आपकी मदद कर सकता है. यह एक मुफ्त सेवा है.

3
Italian: È disponibile un servizio di interpretariato gratuito per rispondere a eventuali domande sul
nostro piano sanitario e farmaceutico. Per un interprete, contattare il numero 1-866-443-1095. Un
nostro incaricato che parla Italianovi fornirà l'assistenza necessaria. È un servizio gratuito.
Portugués: Dispomos de serviços de interpretação gratuitos para responder a qualquer questão que
tenha acerca do nosso plano de saúde ou de medicação. Para obter um intérprete, contacte-nos
através do número 1-866-443-1095. Irá encontrar alguém que fale o idioma Português para o ajudar.
Este serviço é gratuito.
French Creole: Nou genyen sèvis entèprèt gratis pou reponn tout kesyon ou ta genyen konsènan
plan medikal oswa dwòg nou an. Pou jwenn yon entèprèt, jis rele nou nan 1-866-443-1095. Yon
moun ki pale Kreyòl kapab ede w. Sa a se yon sèvis ki gratis.
Polish: Umożliwiamy bezpłatne skorzystanie z usług tłumacza ustnego, który pomoże w uzyskaniu
odpowiedzi na temat planu zdrowotnego lub dawkowania leków. Aby skorzystać z pomocy tłumacza
znającego język polski, należy zadzwonić pod numer 1-866-443-1095. Ta usługa jest bezpłatna.
Japanese: 当社の健康 健康保険と薬品 処方薬プランに関するご質問にお答えするために、
無料の通訳サービスがありますございます。通訳をご用命になるには、1-866-443-1095にお
電話ください。日本語を話す人者 が支援いたします。これは無料のサービスです。

Table of contents
4
Table of Contents
This list of chapters and page numbers is just your starting point. For more help in
finding information you need, go to the first page of a chapter. You will find a
detailed list of topics at the beginning of each chapter.
Chapter 1. Getting started as a participant of the Fresno City Employees Health
& Welfare Trust Medicare Prescription Drug Plan ........................................6
Tells what it means to be in a Medicare prescription drug plan and how to use
this booklet. Tells about materials we will send you, your plan premium, your
plan ID card, and keeping your member (participant) record up to date.
Chapter 2. Important phone numbers and resources........................................................14
Tells you how to get in touch with our plan and with other organizations
including Medicare, the State Health Insurance Assistance Program, the
Quality Improvement Organization, Social Security, Medicaid (the state
health insurance program for people with low incomes), ane programs that
help people pay for their prescription drugs.
Chapter 3. Using the plan’s coverage for your Part D prescription drugs ......................22
Explains rules you need to follow when you get your Part D drugs. Tells how
to use the plan’s List of Covered Drugs (Formulary) to find out which drugs
are covered. Tells which kinds of drugs are not covered. Explains several
kinds of restrictions that apply to your coverage for certain drugs. Explains
where to get your prescriptions filled. Tells about the plan’s programs for
drug safety and managing medications.
Chapter 4. What you pay for your Part D prescription drugs .........................................41
Tells about the four stages of drug coverage (Deductible Stage, Initial
Coverage Stage, Coverage Gap Stage, and Catastrophic Coverage Stage)
and how these stages affect what you pay for your drugs. Explains the four
cost-sharing tiers for your Part D drugs and tells what you must pay for
copayment as your share of the cost for a drug in each cost-sharing tier.
Tells about the late enrollment penalty.
Chapter 5. Asking the plan to pay its share of the costs for covered drugs .....................54
Tells when and how to send a bill to us when you want to ask us to pay you
back for our share of the cost for your drugs.
Chapter 6. Your rights and responsibilities ........................................................................59

Table of contents
5
Explains the rights and responsibilities you have as a participant of our plan.
Tells what you can do if you think your rights are not being respected.
Chapter 7. What to do if you have a problem or complaint (coverage decisions,
appeals, complaints) ..........................................................................................67
Tells you step-by-step what to do if you are having problems or concerns as a
participant of our plan.
Explains how to ask for coverage decisions and make appeals if you are
having trouble getting the prescription drugs you think are covered by our
plan. This includes asking us to make exceptions to the rules and/or extra
restrictions on your coverage.
Explains how to make complaints about quality of care, waiting times,
customer service, and other concerns.
Chapter 8. Ending your coverage in the plan .....................................................................89
Tells when and how you can end your coverage in the plan. Explains
situations in which our plan is required to end your coverage.
Chapter 9. Legal notices .......................................................................................................95
Includes notices about governing law and about nondiscrimination.
Chapter 10. Definitions of important words .........................................................................97
Explains key terms used in this booklet.

Chapter 1: Getting started as a participant in our plan
6
Chapter 1. Getting started as a participant of the your Plan
SECTION 1 Introduction ..........................................................................................................7
Section 1.1 What is the Evidence of Coverage booklet about? ............................................7
Section 1.2 What does this Chapter tell you? .......................................................................7
Section 1.3 What if you are new to our Plan? .......................................................................7
Section 1.4 Legal information about the Evidence of Coverage ..........................................7
SECTION 2 What makes you eligible to be a plan participant? ...........................................8
Section 2.1 Your eligibility requirements .............................................................................8
Section 2.2 What are Medicare Part A and Medicare Part B? ..............................................8
Section 2.3 Here is the plan service area for the your Plan ..................................................8
SECTION 3 What other materials will you get from us? ......................................................9
Section 3.1 Your plan participant ID card – Use it to get all covered prescription drugs ....9
Section 3.2 The Pharmacy Directory: your guide to pharmacies in our network .................9
Section 3.3 The plan’s List of Covered Drugs (Formulary) ...............................................10
Section 3.4 The Explanation of Benefits (the "EOB"): Reports with a summary of
payments made for your prescription drugs...........................................................10
SECTION 4 Your monthly premium for the your Plan ......................................................10
Section 4.1 How much is your plan premium? ...................................................................10
Section 4.2 There are several ways you can pay your plan premium .................................11
Section 4.3 Can we change your monthly plan premium during the year? ........................11
SECTION 5 Please keep your plan participant records up to date ....................................12
Section 5.1 How to help make sure that we have accurate information about you ............12
SECTION 6 We protect the privacy of your personal health information ........................12
Section 6.1 We make sure that your health information is protected .................................12
SECTION 7 How other insurance works with our plan………………………………….12
Section 7.1 Which plan pays first when you have other insurance?...................................12

Chapter 1: Getting started as a participant in our plan
7
SECTION 1 Introduction
Section 1.1 What is the Evidence of Coverage booklet about?
This Evidence of Coverage booklet tells you how to use your Medicare prescription drug
coverage through our plan. This booklet explains your rights and responsibilities, what is
covered, and what you pay as a participant of the plan.
You are covered by Original Medicare for your health care coverage, and you have
chosen to get your Medicare prescription drug coverage through our plan, the Fresno
City Employees Health & Welfare Trust Medicare Prescription Drug Plan.
This plan is offered by the Fresno City Employees Health & Welfare Trust, referred throughout
the Evidence of Coverage as “we,” “us,” or “our.” The Fresno City Employees Health & Welfare
Trust Medicare Prescription Drug Plan is referred to as “plan” or “our plan.”
The word “coverage” and “covered drugs” refers to the prescription drug coverage available
to you as a participant of the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan.
Section 1.2 What does this Chapter tell you?
Look through Chapter 1 of this Evidence of Coverage to learn:
What makes you eligible to be a plan participant?
What materials will you get from us?
What is your plan premium?
What is your plan’s service area?
How do you keep the information in your participant records up to date?
Section 1.3 What if you are new to the Fresno City Employees Health & Welfare
Trust Medicare Prescription Drug Plan?
If you are a new participant, then it’s important for you to learn how the plan operates – what the
rules are and what coverage is available to you. We encourage you to set aside some time to look
through this Evidence of Coverage booklet.
If you are confused or concerned or just have a question, please contact our plan’s Member
Service Center (contact information is on the cover of this booklet).
Section 1.4 Legal information about the Evidence of Coverage
It’s part of our contract with you
This Evidence of Coverage is part of our contract with you about how the Fresno City
Employees Health & Welfare Trust Medicare Prescription Drug Plan covers your care. Other

Chapter 1: Getting started as a participant in our plan
8
parts of this contract include the List of Covered Drugs (Formulary) and any notices you receive
from us about changes or extra conditions that can affect your coverage. These notices are
sometimes called “riders” or “amendments.”
The contract is in effect for the months in which you are enrolled in the Fresno City Employees
Health & Welfare Trust Medicare Prescription Drug Plan between January 1, 2017 to December
31, 2017.
SECTION 2 What makes you eligible to be a plan participant?
Section 2.1 Your eligibility requirements
You are eligible for coverage in our plan as long as:
You live in our geographic service area (section 2.3 below describes our service area)
You are entitled to Medicare Part A and you are enrolled in Medicare Part B (you must
have both Part A and Part B)
You are a United States citizen or are lawfully present in the United States
and – You meet your plans eligibility requirements
Section 2.2 What are Medicare Part A and Medicare Part B?
When you originally signed up for Medicare, you received information about how to get
Medicare Part A and Medicare Part B. Remember:
Medicare Part A generally covers services furnished by providers such as hospitals,
skilled nursing facilities or home health agencies.
Medicare Part B is for most other medical services, such as physician’s services and other
outpatient services.
Note: For Plan members with Diabetes, Medicare Part B supplies that will not be covered
include lancets, test scripts, glucometers, etc. Diabetic supplies that are covered under Medicare
Part D include those items related to the injection of insulin, e.g., insulin syringe, gauze, and
alcohol swabs. Inhalers associated with the inhaled form of insulin are also covered under
Medicare Part D.
Section 2.3 Here is the plan service area for the Fresno City Employees Health &
Welfare Trust Medicare Prescription Drug Plan
Although Medicare is a Federal program, our plan is available only to individuals who live in our
plan service area. Our service area includes all 50 United States, the District of Columbia, Puerto
Rico and Guam.

Chapter 1: Getting started as a participant in our plan
9
If you plan to move out of the service area, please contact OptumRx Member Services (phone
numbers are printed on the front cover of this booklet). When you move, you may have a Special
Enrollment Period that will allow you to enroll in a Medicare health or drug plan that is available
in your new location. You must be a U.S. citizen to be a member of a Medicare plan. If you
become incarcerated, or are no longer lawfully present in the service area, this deems you outside
the service area, which means you are no longer eligible for coverage.
SECTION 3 What other materials will you get from us?
Section 3.1 Your participant identification (ID) card – Use it to get all covered
prescription drugs
While you are a participant of our plan, you must use our ID card for prescription drugs you get
at network pharmacies. If you do not present your card at the pharmacy, you may be responsible
for the full cost of the prescription drug, and may or may not be reimbursed by the Plan. If you
are at the pharmacy and do not have your card, you can show them your Medicare (red, white
and blue) card, or call OptumRx Member Services to verify Coverage.
Please carry your card with you at all times and remember to show your card when you get
covered drugs. If your ID card is damaged, lost, or stolen, call HealthComp at (800) 442-7247
right away and we will send you a new card. You may also print a temporary card from the
member portal site at optumrx.com.
You may need to use your red, white, and blue Medicare card to get covered medical care and
services under Original Medicare.
Section 3.2 The Pharmacy Directory: your guide to pharmacies in our network
What are “network pharmacies”?
Our Pharmacy Directory gives you a list of our network pharmacies – that means the pharmacies
that have agreed to fill covered prescriptions for our plan participants. Visit optumrx.com to
locate a pharmacy.
Why do you need to know about network pharmacies?
You can use the Pharmacy Directory to find the network pharmacy you want to use. This is
important because, with few exceptions, you must get your prescriptions filled at one of our
network pharmacies. You should only use a non-participating pharmacy in emergency situations.
If you use a non-participating pharmacy, you may pay more for your prescriptions.
To locate a pharmacy in your area, our pharmacy locator tool is available for your reference on
our website at optumrx.com. To request an additional copy of this listing be mailed to you,
please contact the OptumRx Member Service center.

Chapter 1: Getting started as a participant in our plan
10
Section 3.3 The plan’s List of Covered Drugs (Formulary)
The plan has a List of Covered Drugs (Formulary). We call it the “Drug List.” It tells which Part
D prescription drugs are covered by the Fresno City Employees Health & Welfare Trust
Medicare Prescription Drug Plan. The drugs on this list are selected with the help of a team of
doctors and pharmacists. The list must meet requirements set by Medicare.
The Abridged Drug List may be included in this packet, and also available for your reference on
our website at optumrx.com. To request a copy be mailed to you, please contact OptumRx
Member Services.
Section 3.4 The Explanation of Benefits (the “EOB”): Reports with a summary of
payments made for your prescription drugs
When you use your prescription drug benefits, we will send you a report to help you understand
and keep track of payments for your prescription drugs. This summary report is called the
Explanation of Benefits.
The Explanation of Benefits tells you the total amount you have spent on your prescription drugs
and the total amount we have paid for each of your prescription drugs during the month. Chapter
4 (What you pay for your Part D prescription drugs) gives more information about the
Explanation of Benefits and how it can help you keep track of your drug coverage.
An Explanation of Benefits summary is also available upon request. To get a copy, please
contact OptumRx Member Services.
SECTION 4 Your monthly premium for the Fresno City Employees
Health & Welfare Trust Medicare Prescription Drug Plan
Section 4.1 How much is your plan premium?
As a member of our plan, you may be required to pay a portion of the monthly plan premium.
The Fresno City Employees Health & Welfare Trust will notify you of the amount, if any, you
need to pay monthly. In addition, you must continue to pay your Medicare Part B premium
(unless your Part B premium is paid for you by Medicaid or another third party). Please contact
your former employer, union or fund, to find out more information about what you may pay for
your monthly plan premium.
In some situations, your plan premium could be less
There are programs to help people with limited resources pay for their drugs. Chapter 2, Section
7 tells more about these programs. If you qualify for one of these programs, enrolling in the
program might reduce your monthly plan premium.
If you are already enrolled and getting help from one of these programs, some of the payment
information in this Evidence of Coverage may not apply to you. You will receive a separate

Chapter 1: Getting started as a participant in our plan
11
notification that tells you about your drug coverage. If you are already enrolled and getting help
from one of these programs and don’t receive this notification, please call OptumRx Member
Services and ask for your “LIS Rider” (the Evidence of Coverage Rider for People Who Get
Extra Help Paying for Prescription Drugs.) Phone numbers for OptumRx Member Services are
on the front cover.
In some situations, your plan premium could be more
Some participants are required to pay a late enrollment penalty because they did not join a
Medicare drug plan when they first became eligible or because they had a continuous period
of 63 days or more when they didn’t keep their creditable coverage. For these participants, the
plan’s monthly premium may be higher. It will be the monthly plan premium plus the amount
of their late enrollment penalty.
If you are required to pay the late enrollment penalty, the amount of your penalty depends on
how long you waited before you enrolled in drug coverage or how many months you were
without drug coverage after you became eligible. Chapter 4 explains the late enrollment
penalty.
Note: If you have a late enrollment penalty, it may be part of your plan premium. If you do not
pay the part of your premium that is the late enrollment penalty, you could be disenrolled for
failure to pay your plan premium.
Section 4.2 There are several ways you can pay your plan premium
As a member of the Fresno City Employees Health & Welfare Trust Medicare Prescription Drug
Plan, you may be required to pay a portion of the premium. The Fresno City Employees Health
& Welfare Trust will notify you of the amount, if any, you need to remit monthly, and how to
pay.
Section 4.3 Can we change your monthly plan premium during the year?
No. We are not allowed to change the amount we charge for the plan’s monthly plan
premium during the year. If the monthly plan premium changes for next year we will tell
you in October and the change will take effect on January 1.
However, in some cases the part of the premium that you have to pay can change during the year.
This happens if you become eligible for Extra Help or if you lose your eligibility for Extra Help
during the year. If a participant qualifies for Extra Help with their prescription drug costs, Extra
Help will pay part of the participant’s monthly plan premium. So a participant who becomes
eligible for Extra Help during the year would begin to pay less toward their monthly premium.
And a participant who loses their eligibility during the year will need to start paying their full
monthly premium. You can find out more about Extra Help in Chapter 2, Section 7.

Chapter 1: Getting started as a participant in our plan
12
SECTION 5 Please keep your participant records up to date
Section 5.1 How to help make sure that we have accurate information about you
The pharmacists in the plan’s network need to have correct information about you. These
network providers use your participant (member) record to know what drugs are covered
for you. Because of this, it is very important that you help us keep your information up to date.
Call HealthComp at 1-800-442-7247 to let them know about these changes:
Changes to your name, your address, or your phone number
Changes in any other medical or drug insurance coverage you have (such as from your
employer, your spouse’s employer, workers’ compensation, or Medicaid)
If you have any liability claims, such as claims from an automobile accident
If you have been admitted to a nursing home
Read over the information we send you about any other insurance coverage you have.
Medicare requires that we collect information from you about any other medical or drug
insurance coverage that you have. That’s because we must coordinate any other coverage you
have with your benefits under our plan.
Once each year, we will send you a letter that lists any other medical or drug insurance coverage
that we know about. Please read over this information carefully. If it is correct, you don’t need to
do anything. If the information is incorrect, or if you have other coverage that is not listed, please
call OptumRx Member Services.
SECTION 6 We protect the privacy of your personal health information
Section 6.1 We make sure that your health information is protected
Federal and state laws protect the privacy of your medical records and personal health
information. We protect your personal health information as required by these laws.
SECTION 7 How other insurance works with our plan
Section 7.1 Which plan pays first when you have other insurance?
When you have other insurance (like employer group health coverage), there are rules set by
Medicare that decide whether our plan or your other insurance pays first. The insurance that pays
first is called the “primary payer” and pays up to the limits of its coverage. The one that pays
second, called the “secondary payer,” only pays if there are costs left uncovered by the primary
coverage. The secondary payer may not pay all of the uncovered costs.

Chapter 1: Getting started as a participant in our plan
13
These rules apply for employer or union group health plan coverage:
If you have retiree coverage, Medicare pays first.
If your group health plan coverage is based on your or a family member’s current
employment, who pays first depends on your age, the number of people employed by
your employer, and whether you have Medicare based on age, disability, or End-stage
Renal Disease (ESRD):
If you’re under 65 and disabled and you or your family member is still working, your
group health plan pays first if the employer has 100 or more employees or at least one
employer in a multiple employer plan that has more than 100 employees.
If you’re over 65 and you or your spouse is still working, your group health plan pays
first if the employer has 20 or more employees or at least one employer in a multiple
employer plan that has more than 20 employees.
If you have Medicare because of ESRD, your group health plan will pay first for the first
30 months after you become eligible for Medicare.
These types of coverage usually pay first for services related to each type:
No-fault insurance (including automobile insurance)
Liability (including automobile insurance)
Black lung benefits
Workers’ compensation
Medicaid and TRICARE never pay first for Medicare-covered services. They only pay after
Medicare, employer group health plans, and/or Medigap have paid.
If you have other insurance, tell your doctor, hospital, and pharmacy. If you have questions about
who pays first, or you need to update your other insurance information, call Member Services
(phone numbers are printed on the back cover of this booklet). You may need to give your plan
member ID number to your other insurers (once you have confirmed their identity) so your bills
are paid correctly and on time.

Chapter 2: Important phone numbers and resources
14
Chapter 2. Important phone numbers and resources
SECTION 1 Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan contacts (how to contact us, including how to
reach OptumRx Member Services at the plan) ....................................................15
SECTION 2 Medicare (how to get help and information directly from the Federal
Medicare program) ..............................................................................................16
SECTION 3 State Health Insurance Assistance Program (free help, information,
and answers to your questions about Medicare) ..................................................17
SECTION 4 Quality Improvement Organization (paid by Medicare to check on the
quality of care for people with Medicare) ...........................................................17
SECTION 5 Social Security ....................................................................................................17
SECTION 6 Medicaid (a joint Federal and state program that helps with medical
costs for some people with limited income and resources) .................................18
SECTION 7 Information about programs to help people pay for their
prescription drugs .............................................................................................19
SECTION 8 Do you have “group insurance” or other health insurance from an
employer? ...........................................................................................................20

Chapter 2: Important phone numbers and resources
15
SECTION 1 Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan contacts
(how to contact us, including how to reach OptumRx Member
Services)
How to contact our plan’s OptumRx Member Services Center and other important
departments.
For assistance with claims, billing or ID card questions, please call the OptumRx Member
Services Center. The OptumRx Member Services Center is available 24 hours a day, 7 days a
week, or please visit our website at optumrx.com. We will be happy to help you.
*This number requires special telephone equipment and is only for people who have difficulties
with hearing or speaking.
Phone TTY* Fax Mailing Address
OptumRx
Member
Services
Center
1-866-443-1095 711 1-808-536-1050 OptumRx
Attn: OptumRx
Member Services
P.O. Box 3410
Lisle, IL 60532
Coverage
Decisions
1-866-443-1095 711 1-866-511-2202 OptumRx
Attn: Prior Auth Part D
Exceptions
P.O. Box 5252
Lisle, IL 60532
Appeals 1-866-443-1095 711 1-866-511-2202 OptumRx
Attn: Part D Appeals
P.O. Box 5252
Lisle, IL 60532
Comments/
Complaints
1-866-443-1095 711 1-866-511-2202 OptumRx
Attn: Part D
Grievances
P.O. Box 3410
Lisle, IL 60532
Payment
Requests
1-866-443-1095 711 1-866-511-2202 OptumRx
Attn: Manual Claims
PO Box 968021
Schaumburg, IL
60196-8021

Chapter 2: Important phone numbers and resources
16
SECTION 2 Medicare (how to get help and information directly from the
Federal Medicare program)
Medicare is the Federal health insurance program for people 65 years of age or older, some
people under age 65 with disabilities, and people with End-Stage Renal Disease (permanent
kidney failure requiring dialysis or a kidney transplant).
The Federal agency in charge of Medicare is the Centers for Medicare & Medicaid Services
(sometimes called “CMS”). This agency contracts with Medicare Prescription Drug Plans,
including us.
Medicare
CALL 1-800-MEDICARE, or 1-800-633-4227
Calls to this number are free.
24 hours a day, 7 days a week.
TTY 1-877-486-2048
This number requires special telephone equipment and is only for
people who have difficulties with hearing or speaking.
Calls to this number are free.
WEBSITE www.medicare.gov
This is the official government website for Medicare. It gives you up-
to-date information about Medicare and current Medicare issues. It
also has information about hospitals, nursing homes, physicians,
home health agencies, and dialysis facilities. It includes booklets you
can print directly from your computer. It has tools to help you
compare Medicare Advantage Plans and Medicare drug plans in your
area. You can also find Medicare contacts in your state by selecting
“Helpful Phone Numbers and Websites.”
If you don’t have a computer, your local library or senior center may
be able to help you visit this website using its computer. Or, you can
call Medicare at the number above and tell them what information
you are looking for. They will find the information on the website,
print it out, and send it to you.

Chapter 2: Important phone numbers and resources
17
SECTION 3 State Health Insurance Assistance Program
(free help, information, and answers to your questions about
Medicare)
The State Health Insurance Assistance Program (SHIP) is a government program with trained
counselors in every state.
State Health Insurance Assistance Program is independent (not connected with any insurance
company or health plan). It is a state program that gets money from the Federal government to
give free local health insurance counseling to people with Medicare. For a listing of all SHIP
programs, please refer to the Appendix at the end of this booklet.
SHIP counselors can help you with your Medicare questions or problems. They can help you
understand your Medicare rights, help you make complaints about your medical care or
treatment, and help you straighten out problems with your Medicare bills. SHIP counselors
can also help you understand your Medicare plan choices and answer questions about
switching plans.
SECTION 4 Quality Improvement Organization
(paid by Medicare to check on the quality of care for people
with Medicare)
There is a Quality Improvement Organization for each state.
Quality Improvement Organizations have a group of doctors and other health care professionals
who are paid by the Federal government. This organization is paid by Medicare to check on and
help improve the quality of care for people with Medicare. Quality Improvement Organizations
are independent organizations. It is not connected with our plan. For a listing of all QIO
programs, please refer to the Appendix at the end of this booklet.
You should contact a QIO if you have a complaint about the quality of care you have received.
For example, you can contact a QIO if you were given the wrong medication or if you were
given medications that interact in a negative way.
SECTION 5 Social Security
Social Security is responsible for determining eligibility and handling enrollment for
Medicare. U.S. citizens who are 65 or older, or who have a disability or End-Stage Renal
Disease and meet certain conditions, are eligible for Medicare. If you are already getting
Social Security checks, enrollment into Medicare is automatic. If you are not getting Social
Security checks, you have to enroll in Medicare. Social Security handles the enrollment
process for Medicare. To apply for Medicare, you can call Social Security or visit your local
Social Security office.

Chapter 2: Important phone numbers and resources
18
Social Security is also responsible for determining who has to pay an extra amount for their
Part D drug coverage because they have a higher income. If you got a letter from Social
Security telling you that you have to pay the extra amount and have questions about the
amount or if your income went down because of a life-changing event, you can call Social
Security to ask for a reconsideration.
Social Security Administration
CALL 1-800-772-1213
Calls to this number are free.
Available 7:00 am to 7:00 pm, Monday through Friday.
You can use our automated telephone services to get recorded
information and conduct some business 24 hours a day.
TTY 1-800-325-0778
This number requires special telephone equipment and is only for
people who have difficulties with hearing or speaking.
Calls to this number are free.
Available 7:00 am ET to 7:00 pm, Monday through Friday.
WEBSITE www.ssa.gov
SECTION 6 Medicaid
(a joint Federal and state program that helps with medical costs
for some people with limited income and resources)
Medicaid is a joint Federal and state government program that helps with medical costs for
certain people with limited incomes and resources. Some people with Medicare are also eligible
for Medicaid. For a listing of all Medicaid programs, please refer to the Appendix at the end of
this booklet.
In addition, there are programs offered through Medicaid that help people with Medicare pay
their Medicare costs, such as their Medicare premiums. These “Medicare Savings Programs”
help people with limited income and resources save money each year:

Chapter 2: Important phone numbers and resources
19
Qualified Medicare Beneficiary (QMB): Helps pay Medicare Part A and Part B
premiums, and other cost sharing (like deductibles, coinsurance, and copayments). (Some
people with QMB are also eligible for full Medicaid benefits (QMB+).)
Specified Low-Income Medicare Beneficiary (SLMB): Helps pay Part B premiums.
(Some people with SLMB are also eligible for full Medicaid benefits (SLMB+).)
Qualified Individual (QI): Helps pay Part B premiums.
Qualified Disabled & Working Individuals (QDWI): Helps pay Part A premiums.
SECTION 7 Information about programs to help people pay for their
prescription drugs
Medicare’s “Extra Help” Program
Medicare provides “Extra Help” to pay prescription drug costs for people who have limited
income and resources. Resources include your savings and stocks, but not your home or car. If
you qualify, you get help paying for any Medicare drug plan’s monthly premium and
prescription copayments. This Extra Help also counts toward your out-of-pocket costs.
People with limited income and resources may qualify for Extra Help. Some people
automatically qualify for Extra Help and don’t need to apply. Medicare mails a letter to people
who automatically qualify for Extra Help.
If you think you may qualify for Extra Help, call Social Security (see Section 5 of this chapter
for contact information) to apply for the program. You may also be able to apply at your State
Medical Assistance or Medicaid Office (see Section 6 of this chapter for contact information).
After you apply, you will get a letter letting you know if you qualify for Extra Help and what you
need to do next.
State Pharmaceutical Assistance Programs
Some states have State Pharmacy Assistance Programs (SPAPs). SPAPs are state-funded
programs that provide financial assistance for prescription drugs to low-income and medically
needy senior citizens and individuals with disabilities. SPAPs may help pay for the premiums
and/or co-payments/co-insurance for those who qualify. In addition, payments made by
Qualified SPAPs on your behalf for co-payments, coinsurance or deductibles. You can contact
1-800-Medicare to find out if there are any Qualified SPAPs in your state.
What if you have coverage from an AIDS Drug Assistance Program (ADAP)?
What is the AIDS Drug Assistance Program (ADAP)?
The AIDS Drug Assistance Program (ADAP) helps ADAP-eligible individuals living with
HIV/AIDS have access to life-saving HIV medications. Medicare Part D prescription drugs that

Chapter 2: Important phone numbers and resources
20
are also covered by ADAP qualify for prescription cost-sharing assistance. Note: To be eligible
for the ADAP operating in your State, individuals must meet certain criteria, including proof of
State residence and HIV status, low income as defined by the State, and uninsured/under-insured
status.
If you are currently enrolled in an ADAP, it can continue to provide you with Medicare Part D
prescription cost-sharing assistance for drugs on the ADAP formulary. In order to be sure you
continue receiving this assistance, please notify your local ADAP enrollment worker of any
changes in your Medicare Part D plan name or policy number.
SECTION 8 Do you have “group insurance” or other health insurance
from an employer?
If you (or your spouse) get prescription drug benefits through an employer/union or retiree group
other than the Fresno City Employees Health & Welfare Trust, call that employer/union
benefits administrator if you have any questions. You can ask about their employer/retiree health
or drug benefits, premiums, or enrollment period.
Important Note: Your (or your spouses’) employer/union benefits may change, or you or your
spouse may lose the benefits, if you or your spouse enrolls in a Medicare Part D program. Call
that employer/union benefits administrator to find out whether the benefits will change or be
terminated if you or your spouse enrolls in a Part D plan.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
22
Chapter 3. Using the plan’s coverage for your
Part D prescription drugs
SECTION 1 Introduction ........................................................................................................24
Section 1.1 This chapter describes your coverage for Part D drugs ...................................24
Section 1.2 Basic rules for the plan’s Part D drug coverage ..............................................24
SECTION 2 Fill your prescription at a network pharmacy or through the plan’s
mail-order service ..............................................................................................24
Section 2.1 To have your prescription covered, use a network pharmacy .........................24
Section 2.2 Finding network pharmacies ............................................................................25
Section 2.3 Using the plan’s mail-order services................................................................26
Section 2.4 How can you get a long-term supply of drugs? ...............................................27
Section 2.5 When can you use a pharmacy that is not in the plan’s network? ...................27
SECTION 3 Your drugs need to be on the plan’s “Drug List” ...........................................28
Section 3.1 The “Drug List” tells which Part D drugs are covered ....................................28
Section 3.2 There are four“cost-sharing tiers” for drugs on the Drug List .........................29
Section 3.3 How can you find out if a specific drug is on the Drug List? ..........................29
SECTION 4 There are restrictions on coverage for some drugs.........................................29
Section 4.1 Why do some drugs have restrictions? ............................................................30
Section 4.2 What kinds of restrictions? ..............................................................................30
Section 4.3 Do any of these restrictions apply to your drugs?............................................30
SECTION 5 What if one of your drugs is not covered in the way you’d like it to be
covered? ..............................................................................................................31
Section 5.1 There are things you can do if your drug is not covered in the way you'd like it
to be covered ..........................................................................................................31
Section 5.2 What can you do if your drug is not on the Drug List or if the drug is restricted
in some way?..........................................................................................................32

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
23
Section 5.3 What can you do if your drug is in a cost-sharing tier you think is too high? .......33
SECTION 6 What if your coverage changes for one of your drugs? ..................................34
Section 6.1 The Drug List can change during the year .......................................................34
Section 6.2 What happens if coverage changes for a drug you are taking? ........................35
SECTION 7 What types of drugs are not covered by the plan? ..........................................35
Section 7.1 Types of drugs we do not cover .......................................................................35
SECTION 8 Show your plan participant ID card when you fill a prescription ................36
Section 8.1 Show your ID card ...........................................................................................36
Section 8.2 What if you don’t have your ID card with you? ..............................................36
SECTION 9 Part D drug coverage in special situations ......................................................37
Section 9.1 What if you’re in a hospital or a skilled nursing facility for a stay that is
covered by the plan? ..............................................................................................37
Section 9.2 What if you’re a resident in a long-term care facility? ....................................37
Section 9.3 What if you are taking drugs covered by Original Medicare? .........................38
Section 9.4 What if you have a Medigap (Medicare Supplement Insurance) policy with
prescription drug coverage? ...................................................................................38
Section 9.5 What if you are in Medicare-certified Hospice? ....................................................38
SECTION 10 Programs on drug safety and managing medications ....................................39
Section 10.1 Programs to help participants use drugs safely ................................................39
Section 10.2 Medication Therapy Management (MTM) Programs............................................39

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
24
SECTION 1 Introduction
Section 1.1 This chapter describes your coverage for Part D drugs
This chapter explains rules for using your coverage for Part D drugs. The next chapter tells what
you pay for Part D drugs (Chapter 4, What you pay for your Part D prescription drugs).
In addition to your coverage for Part D drugs through our plan, Original Medicare (Medicare
Part A and Part B) also covers some drugs:
Medicare Part A covers drugs you are given during Medicare-covered stays in the
hospital or in a skilled nursing facility.
Medicare Part B also provides benefits for some drugs. Part B drugs include certain
chemotherapy drugs, certain drug injections you are given during an office visit, and
drugs you are given at a dialysis facility.
To find out more about this coverage, see your Medicare & You handbook.
Section 1.2 Basic rules for the plan’s Part D drug coverage
The plan will generally cover your drugs as long as you follow these basic rules:
You must use a network pharmacy to fill your prescription. (See Section 2, Fill your
prescriptions at a network pharmacy.)
Your drug must be on the plan’s List of Covered Drugs (Formulary). We call it the
“Drug List”. (See Section 3, Your drugs need to be on the plan’s drug list.)
Your drug must be considered “medically necessary”, meaning reasonable and necessary
for treatment of your illness or injury. It also needs to be an accepted treatment for your
medical condition.
Your prescriber must accept Medicare showing that he or she is qualified to write
prescriptions. You should ask your prescribers the next time you call or visit if they meet
this condition.
SECTION 2 Fill your prescription at a network pharmacy or through
the plan’s mail-order service
Section 2.1 To have your prescription covered, use a network pharmacy
In most cases, your prescriptions are covered only if they are filled at the plan’s network
pharmacies.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
25
A network pharmacy is a pharmacy at which you can get your prescription drug benefits. We call
them “network pharmacies” because they contract with our Plan. In most cases, your
prescriptions are covered only if they are filled at one of our network pharmacies. Once you go
to one, you are not required to continue going to the same pharmacy to fill your prescription; you
can go to any of our network pharmacies. However, if you switch to a different network
pharmacy, you must either have a new prescription written by a physician or have the previous
pharmacy transfer the existing prescription to the new pharmacy if any refills remain.
Section 2.2 Finding network pharmacies
How do you find a network pharmacy in your area?
To find a network pharmacy, visit our website at optumrx.com or call HealthComp to get a
copy of the pharmacy listing. You may also call OptumRx Member Services.
What if the pharmacy you have been using leaves the network?
If the pharmacy you have been using leaves the plan’s network, you will have to find a new
pharmacy that is in the network. To find another network pharmacy in your area, you can get
help from OptumRx Member Services or use the Pharmacy Locator tool available at
optumrx.com.
You may go to any of our network pharmacies. If you switch from one network pharmacy to
another, and you need a refill of a drug you have been taking, you can ask to either have a new
prescription written by a doctor or, if applicable/allowed, to have your prescription transferred to
your new network pharmacy.
What if you need a Specialty network pharmacy?
Sometimes prescriptions must be filled at a Specialty network pharmacy. Specialty network
pharmacies include:
Pharmacies that supply drugs for home infusion therapy.
Pharmacies that supply drugs for residents of a long-term-care facility. Usually, a
long-term care facility (such as a nursing home) has its own pharmacy. Residents may
get prescription drugs through the facility’s pharmacy as long as it is part of our
network. If your long-term care pharmacy is not in our network, please contact
OptumRx Member Services.
Pharmacies that serve the Indian Health Service / Tribal / Urban Indian Health
Program. Except in emergencies, only Native Americans or Alaska Natives have
access to these pharmacies in our network.
Pharmacies that dispense certain drugs that are restricted by the FDA to certain
locations, require extraordinary handling, provider coordination, or education on its
use. (Note: This scenario should happen rarely.)

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
26
To locate a Specialty network pharmacy, call OptumRx Member Services.
Section 2.3 Using the plan’s mail-order services
To get order forms and information about filling your prescriptions by mail, please call OptumRx
Member Services or visit the website at: optumrx.com. If you use a mail-order pharmacy not in
the plan’s network, your prescription will not be covered.
Usually a mail-order pharmacy order will get to you in no more than 7-10 days. OptumRx will
contact you if there will be an extended delay in delivering your medications.
You also have three different options to expedite the delivery of your mail-order prescription to
2nd
day air, or overnight shipping:
Online Refills – visit optumrx.com to submit your order online and choose a shipping
method.
Call OptumRx Member Services - call 1-866-443-1095 to indicate shipping method.
Mail-in the prescription order form – if you mail in a hard copy of your prescription,
you can request your order delivery be expedited by either writing your delivery method
on the prescription itself, on the order form, or on a separate sheet of paper included with
your form.
NOTE: If you need to have your prescription order expedited (not just delivery), you must call
OptumRx Member Services at 1-866-443-1095. We also recommend that you call OptumRx
Member Services to verify your expedited delivery and/or order have been processed properly
when ordering online or sending in a form.
New prescriptions the pharmacy receives directly from your doctor’s office.
The pharmacy will automatically fill and deliver new prescriptions it receives from health care
providers, without checking with you first, if either:
You used mail order services with this plan in the past year, or
You sign up for automatic delivery of all new prescriptions received directly from health
care providers. You may request automatic delivery of all new prescriptions now or at
any time by calling OptumRx Member Services (phone number located on the front of
this booklet).
If you receive a prescription automatically by mail that you do not want, you may be eligible for
a refund.
If you used mail order in the past and do not want the pharmacy to automatically fill and ship
each new prescription, please contact OptumRx Member Services at the number on the front of
this booklet.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
27
If you have never used our mail order delivery and/or decide to stop automatic fills of new
prescriptions, the pharmacy will contact you each time it gets a new prescription from a health
care provider to see if you want the medication filled and shipped immediately. This will give
you an opportunity to make sure that the pharmacy is delivering the correct drug (including
strength, amount, and form) and, if necessary, allow you to cancel or delay the order before you
are billed and it is shipped. It is important that you respond each time you are contacted by the
pharmacy, to let them know what to do with the new prescription and to prevent any delays in
shipping.
To opt out of automatic deliveries of new prescriptions received directly from your health care
provider’s office, please contact OptumRx Member Services at the phone number located on the
front of this booklet.
Refills on mail order prescriptions. For refills, please contact your pharmacy 14 days before
you think the drugs you have on hand will run out to make sure your next order is shipped to you
in time. Refills are not automatically shipped, only new prescriptions.
Section 2.4 How can you get a long-term supply of drugs?
When you get a long-term supply of drugs, your cost sharing may be lower. The plan offers a
way to get a long-term supply of “maintenance” drugs on our plan’s Drug List. (Maintenance
drugs are drugs that you take on a regular basis, for a chronic or long-term medical condition.)
1. Some retail pharmacies in our network allow you to get a long-term supply of
maintenance drugs: Some of these retail pharmacies may agree to accept a lower cost-
sharing amount for a long-term supply of maintenance drugs. Other retail pharmacies
may not agree to accept the lower cost-sharing amounts for a long-term supply of
maintenance drugs. In this case you will be responsible for the difference in price.
The Pharmacy Locator tool online tells you which pharmacies in our network can
give you a long-term supply of maintenance drugs. You can also call OptumRx
Member Services for more information.
2. For certain kinds of drugs, you can use the plan’s network mail-order services. Our
plan’s mail-order service allows you to order a 90-day supply. See Section 2.3 for
more information about using our mail-order services.
Section 2.5 When can you use a pharmacy that is not in the plan’s network?
Your prescription might be covered in certain situations
Generally, we cover drugs filled at an out-of-network pharmacy only when you are not able to
use a network pharmacy. In these situations, please check first with OptumRx Member
Services to see if there is a network pharmacy nearby. Here are the circumstances when we
would cover prescriptions filled at an out-of-network pharmacy:
The prescription is for a medical emergency or urgent care.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
28
You are unable to get a covered drug in a time of need because there are no 24-hour
network pharmacies within a reasonable driving distance.
The prescription is for a drug that is out of stock at an accessible network retail or mail
service pharmacy (including high-cost and unique drugs). If we do pay for the drugs you
get at an out-of-network pharmacy, you may still pay more than you would have paid if
you had gone to an in-network pharmacy. If you do go to an out-of-network pharmacy for
any of the reasons listed above, the Plan will cover up to a one-month supply of drugs.
The prescription is for a drug that is out of stock at an accessible network retail or mail service
pharmacy (including high-cost and unique drugs). If we do pay for the drugs you get at an out-
of-network pharmacy, you may still pay more than you would have paid if you had gone to an
in-network pharmacy. If you do go to an out-of-network pharmacy for any of the reasons listed
above, the Plan will cover up to a one-month supply of drugs.
How do you ask for reimbursement from the plan?
If you must use an out-of-network pharmacy, you may have to pay a higher amount, or the full
cost, (rather than paying your normal share of the cost) when you fill your prescription. You can
ask us to reimburse you for our share of the cost. (Chapter 5 explains how to ask the plan to pay
you back.)
SECTION 3 Your drugs need to be on the plan’s “Drug List”
Section 3.1 The “Drug List” tells which Part D drugs are covered
The plan has a “List of Covered Drugs (Formulary).” In this Evidence of Coverage, we also call
it the “Drug List.”
The drugs on this list are selected with the help of a team of doctors and pharmacists. The list
must meet requirements set by Medicare.
The drugs on the Drug List are only those covered under this Medicare Part D plan (earlier in
this chapter, Section 1.1 explains about Part D drugs).
We will generally cover a drug on the plan’s Drug List as long as you follow the other
coverage rules explained in this chapter and the drug is medically necessary, meaning
reasonable and necessary for treatment of your illness or injury. It also needs to be an
accepted treatment for your medical condition.
The Drug List includes both brand-name and generic drugs
A generic drug is a prescription drug that has the same active ingredients as the brand-name
drug. It works just as well as the brand-name drug, but it costs less. There are generic drug
substitutes available for many brand-name drugs, and generally, the brand-name drug will no
longer be covered.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
29
Section 3.2 There are four “cost-sharing tiers” for drugs on the Drug List
Every drug on the plan’s Drug List is in one of four cost-sharing tiers. In general, the higher the
cost-sharing tier, the higher your cost for the drug:
Cost-Sharing Tier 1 includes Generic drugs. This is the lowest cost-sharing tier.
Cost-Sharing Tier 2 includes Preferred Brand drugs. This is the moderate cost-sharing
tier.
Cost-Sharing Tier 3 includes Non-Preferred Brand drugs. This is the highest cost-sharing
tier.
Cost-Sharing Tier 4 includes High-Cost Drugs. This tier is any drug that costs $600 or
more for up to a 30-day supply.
To find out which cost-sharing tier your drug is in, please reference your plan’s Drug List.
The amount you pay for drugs in each cost-sharing tier is shown in Chapter 4 (What you pay for
your Part D prescription drugs). You can ask us to make an exception (which is a type of
coverage determination) to your drug’s tier placement in certain circumstances. See Chapter 7 to
learn more about how to request a “tiering exception.”
Section 3.3 How can you find out if a specific drug is on the Drug List?
You have three ways to find out:
1. Visit the plan’s website: optumrx.com
2. Call OptumRx Member Services to find out if a particular drug is on the plan’s
Drug List or to ask for a copy of the list.
3. Check the most recent Drug List we sent you in the mail. (Please note: The Drug
List we send includes information for the covered drugs that are most commonly
used by our members. However, we cover additional drugs that are not included
in the printed Drug List. If one of your drugs is not listed in the Drug List, you
should visit our website or contact OptumRx Member Services to find out if we
cover it.)
SECTION 4 There are restrictions on coverage for some drugs
Section 4.1 Why do some drugs have restrictions?
For certain prescription drugs, special rules restrict how and when the plan covers them. A team
of doctors and pharmacists developed these rules to help our participants use drugs in the most
effective ways. These special rules also help control overall drug costs, which keeps your drug
coverage more affordable.
In general, our rules encourage you to get a drug that works for your medical condition and is
safe. Whenever a safe, lower-cost drug will work medically just as well as a higher-cost drug, the

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
30
plan’s rules are designed to encourage you and your doctor or other prescriber to use that lower-
cost option. We also need to comply with Medicare’s rules and regulations for drug coverage and
cost sharing.
Section 4.2 What kinds of restrictions?
Our plan uses different types of restrictions to help our participants use drugs in the most
effective ways. The sections to follow tell you more about the types of restrictions we use for
certain drugs.
Using generic drugs whenever you can
A “generic” drug works the same as a brand-name drug, but usually costs less. When a generic
version of a brand-name drug is available, our network pharmacies may provide you the
generic version. However, if your doctor has told us the medical reason that the generic drug
will not work for you, then we may cover the brand-name drug. (Your share of the cost may be
greater for the brand-name drug than for the generic drug.)
Prior Authorization - Getting plan approval in advance
For certain drugs, you or your doctor need to get approval from the plan before we will agree to
cover the drug for you. This is called “prior authorization.” Sometimes plan approval is required
so we can be sure that your drug is covered by Medicare rules. Sometimes the requirement for
getting approval in advance helps guide appropriate use of certain drugs. If you do not get this
approval, your drug might not be covered by the plan.
Step Therapy - Trying a different drug first
This requirement encourages you to try safer or more effective drugs before the plan covers
another drug. For example, if Drug A and Drug B treat the same medical condition, the plan may
require you to try Drug A first. If Drug A does not work for you, the plan will then cover Drug
B. This requirement to try a different drug first is called “Step Therapy.”
Quantity limits
For certain drugs, we limit the amount of the drug that you can have, or how much of a drug you
can get each time you fill your prescription. For example, if it is normally considered safe to take
only one pill per day for a certain drug, we may limit coverage for your prescription to no more
than one pill per day.
Section 4.3 Do any of these restrictions apply to your drugs?
The plan’s Drug List includes information about the restrictions described above. To find out if
any of these restrictions apply a drug you take or want to take, check the Drug List. For the most
up-to-date information, call OptumRx Member Services or check our website at optumrx.com.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
31
If there is a restriction for your drug, it usually means that you or your provider will have
to take extra steps in order for us to cover the drug. If there is a restriction on the drug you
want to take, you should contact Member Services to learn what you or your provider would
need to do to get coverage for the drug. If you want us to waive the restriction for you, you will
need to use the coverage decision process and ask us to make an exception. We may or may not
agree to waive the restriction for you. (See Chapter 7 for information about asking for
exceptions.)
SECTION 5 What if one of your drugs is not covered in the way you’d
like it to be covered?
Section 5.1 There are things you can do if your drug is not covered in the way
you’d like it to be covered
Suppose there is a prescription drug you are currently taking, or one that you and your doctor
think you should be taking. We hope that your drug coverage will work well for you, but it’s
possible that you might have a problem. For example:
What if the drug you want to take is not covered by the plan? For example, the drug
might not be covered at all. Or maybe a generic version of the drug is covered but the
brand-name version you want to take is not covered.
What if the drug is covered, but there are extra rules or restrictions on coverage for
that drug? As explained in Section 4, some of the drugs covered by the plan have extra
rules to restrict their use. For example, you might be required to try a different drug first,
to see if it will work, before the drug you want to take will be covered for you. Or there
might be limits on what amount of the drug (number of pills, etc.) is covered during a
particular time period.
What if the drug is covered, but it is in a cost-sharing tier that makes your cost
sharing more expensive than you think it should be? The plan puts each covered drug
into one of five different cost-sharing tiers. How much you pay for your prescription
depends in part on which cost-sharing tier your drug is in.
There are things you can do if your drug is not covered in the way that you’d like it to be
covered. Your options depend on what type of problem you have:
If your drug is not on the Drug List or if your drug is restricted, go to Section 5.2 to learn
what you can do.
If your drug is in a cost-sharing tier that makes your cost more expensive than you think
it should be, go to Section 5.3 to learn what you can do.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
32
Section 5.2 What can you do if your drug is not on the Drug List or if the drug is
restricted in some way?
If your drug is not on the Drug List or is restricted, here are things you can do:
You may be able to get a temporary supply of the drug (only participants in certain
situations can get a temporary supply) until you and your doctor decide it is okay to
change to another drug, or while you file an exception.
You can change to another drug.
You can request an exception and ask the plan to cover the drug or remove restrictions
from the drug covered.
You may be able to get a temporary supply
Under certain circumstances, the plan can offer a temporary supply of a drug to you when your
drug is not on the Drug List or when it is restricted in some way. Doing this gives you time to
talk with your doctor about the change in coverage and figure out what to do.
To be eligible for a temporary supply, you must meet the two requirements below:
1. The change to your drug coverage must be one of the following types of changes:
The drug you have been taking is no longer on the plan’s Drug List.
– or –
The drug you have been taking is now restricted in some way (Section 4 in this chapter
tells about restrictions).
2. You must be in one of the situations described below:
For those participants who were in the plan last year:
We will cover a temporary supply of your drug one time only during the first 90 days
of the calendar year. This temporary supply will be for a maximum of a 30-day supply,
or less if your prescription is written for fewer days. The prescription must be filled at a
network pharmacy.
For those participants who are new to the plan and aren’t in a long-term care
facility:
We will cover a temporary supply of your drug one time only during the first 90 days
of your enrollment in the plan. This temporary supply will be for a maximum of a 30-
day supply, or less if your prescription is written for fewer days. The prescription must be
filled at a network pharmacy.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
33
For those who are new participants, and are residents in a long-term care
facility:
We will cover a temporary supply of your drug during the first 90 days of your
enrollment in the plan. The first supply will be for a maximum of a 31 to 34-day supply,
or less if your prescription is written for fewer days. If needed, we will cover additional
refills during your first 90 days in the plan.
For those who have been a participant of the plan for more than 90 days, and are a
resident of a long-term care facility and need a supply right away:
We will cover one 31 to 34-day supply, or less if your prescription is written for fewer
days. This is in addition to the above long-term care transition supply.
To ask for a temporary supply, call OptumRx Member Services (phone numbers are on the front
cover).
During the time when you are getting a temporary supply of a drug, you should talk with your
doctor or other prescriber to decide what to do when your temporary supply runs out. Perhaps
there is a different drug covered by the plan that might work just as well for you. Or you and
your doctor can ask the plan to make an exception for you and cover the drug in the way you
would like it to be covered. The sections below tell you more about these options.
Section 5.3 What can you do if your drug is in a cost-sharing tier you think is too
high?
If your drug is a cost-sharing tier you think is too high, here are things you can do:
You can change to another drug
Start by talking with your doctor or other prescriber. Perhaps there is a different drug in a lower
cost-sharing tier that might work just as well for you. You can call OptumRx Member Services
to ask for a list of covered drugs that treat the same medical condition. This list can help your
doctor or other prescriber to find a covered drug that might work for you.
You can file an exception
You and your doctor or other prescriber can ask the plan to make an exception in the cost-
sharing tier for the drug so that you pay less for the drug. If your doctor or other prescriber says
that you have medical reasons that justify asking us for an exception, your doctor or other
prescriber can help you request an exception to the rule. Please note: not all exceptions may be
approved.
If you and your doctor or other prescriber want to ask for an exception, Chapter 7 tells what to
do. It explains the procedures and deadlines that have been set by Medicare to make sure your
request is handled promptly and fairly.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
34
SECTION 6 What if your coverage changes for one of your drugs?
Section 6.1 The Drug List can change during the year
Most of the changes in drug coverage happen at the beginning of each year (January 1).
However, during the year, there may be changes to the Drug List. For example, the plan might:
Add or remove drugs from the Drug List. New drugs become available,
including new generic drugs. Perhaps the government has given approval to a new
use for an existing drug. Sometimes, a drug gets recalled and we decide not to
cover it. Or we might remove a drug from the list because it has been found to be
ineffective by the FDA.
Move a drug to a lower cost-sharing tier.
Remove a restriction on coverage for a drug (for more information about
restrictions to coverage, see Section 4 in this chapter).
Replace a brand-name drug with a generic drug.
In almost all cases, we must get approval from Medicare for changes we make to the plan’s Drug
List.
Section 6.2 What happens if coverage changes for a drug you are taking?
How will you find out if your drug’s coverage has been changed?
If there is a change to coverage for a drug you are taking, the plan will send you a notice
to tell you. Normally, we will let you know at least 60 days ahead of time.
Once in a while, a drug is suddenly recalled because it’s been found to be unsafe or for
other reasons. If this happens, the plan will immediately remove the drug from the Drug
List. We will let you know of this change right away. Your doctor will also know about
this change, and can work with you to find another drug for your condition.
Do changes to your drug coverage affect you right away?
If any of the following types of changes affect a drug you are taking, the change will not
affect you until January 1 of the next year if you stay in the plan:
If we move your drug into a higher cost-sharing tier.
If we put a new restriction on your use of the drug.
If we remove your drug from the Drug List, but not because of a sudden recall or
because a new generic drug has replaced it.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
35
If any of these changes happens for a drug you are taking, then the change won’t affect
your use or what you pay as your share of the cost until January 1 of the next year. Until
that date, you probably won’t see any increase in your payments or any added restriction
to your use of the drug. However, on January 1 of the next year, the changes will affect
you.
In some cases, you will be affected by the coverage change before January 1:
If a brand-name drug you are taking is replaced by a new generic drug, the
plan must give you at least 60 days’ notice or give you a 60-day refill of your
brand-name drug at a network pharmacy.
o During this 60-day period, you should be working with your doctor to
switch to the generic or to a different drug that we cover.
o Or you and your doctor or other prescriber can ask the plan to make an
exception and continue to cover the brand-name drug for you. For
information on how to ask for an exception, see Chapter 7 (What to do if
you have a problem or complaint).
Again, if a drug is suddenly recalled because it’s been found to be unsafe or for
other reasons, the plan will immediately remove the drug from the Drug List. We
will let you know of this change right away.
o Your doctor or other prescriber will also know about this change, and can
work with you to find another drug for your condition.
SECTION 7 What types of drugs are not covered by the plan?
Section 7.1 Types of drugs we do not cover
This section tells you what kinds of prescription drugs are not covered.
Here are three general rules about drugs that Medicare drug plans will not cover under Part D:
Our plan’s Part D drug coverage cannot cover a drug that would be covered under
Medicare Part A or Part B.
Our plan cannot cover a drug purchased outside the United States and its territories.
“Off-label use” is any use of the drug other than those indicated on a drug’s label as
approved by the Food and Drug Administration.
o Sometimes “off-label use” is allowed. Coverage is allowed only when the use is
supported by certain reference books. These reference books are the American
Hospital Formulary Service Drug Information, the DRUGDEX Information
System, and the USPDI or its successor. If the use is not supported by any of
these reference books, then our plan cannot cover its “off-label use.”
Also, these categories of drugs are not covered by Medicare drug plans:

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
36
Non-prescription drugs (also called over-the-counter drugs)
Drugs when used for the relief of cough or cold symptoms
Drugs when used for cosmetic purposes or to promote hair growth
Prescription vitamins and mineral products, except prenatal vitamins and fluoride
preparations
Drugs when used for the treatment of sexual or erectile dysfunction, such as Viagra,
Cialis, Levitra, and Caverject
Drugs when used for treatment of anorexia, weight loss, or weight gain
Outpatient drugs for which the manufacturer seeks to require that associated tests or
monitoring services be purchased exclusively from the manufacturer as a condition of
sale
In addition, if you are receiving extra help from Medicare to pay for your prescriptions, the
extra help will not pay for the drugs not normally covered. (Please refer to your formulary or call
OptumRx Member Services for more information.) Your state Medicaid program may cover
some prescription drugs not normally covered in a Medicare drug plan. Please contact your state
Medicaid program to determine what drug coverage may be available to you.
SECTION 8 Show your participant identification (ID) card when you fill
a prescription
Section 8.1 Show your ID card
To fill your prescription, show your plan participant ID card at the network pharmacy you
choose. When you show your ID card, the network pharmacy will automatically bill the plan
for our share of your covered prescription drug cost. You will need to pay the pharmacy your
share of the cost when you pick up your prescription.
Section 8.2 What if you don’t have your ID card with you?
If you don’t have your ID card with you when you fill your prescription, ask the pharmacy to call
OptumRx Member Services (phone numbers are on the front cover) to get the necessary
information. If the pharmacy is not able to get the necessary information, you may have to pay
the full cost of the prescription when you pick it up. (You can then ask us to reimburse you for
our share. See Chapter 5 for information about how to ask the plan for reimbursement.)

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
37
SECTION 9 Part D drug coverage in special situations
Section 9.1 What if you’re in a hospital or a skilled nursing facility for a stay that
is covered by the plan?
If you are admitted to a hospital for a stay covered by Original Medicare, Medicare Part A will
generally cover the cost of your prescription drugs during your stay. Once you leave the hospital,
our plan will cover your drugs as long as the drugs meet all of our rules for coverage. See the
previous parts of this chapter that tell about the rules for getting drug coverage.
If you are admitted to a skilled nursing facility for a stay covered by Original Medicare,
Medicare Part A will generally cover your prescription drugs during all or part of your stay. If
you are still in the skilled nursing facility, and Part A is no longer covering your drugs, our plan
will cover your drugs as long as the drugs meet all of our rules for coverage. See the previous
parts of this chapter that tell about the rules for getting drug coverage.
Please Note: When you enter, live in, or leave a skilled nursing facility, you are entitled to a
special enrollment period. During this time period, you can switch plans or change your coverage
at any time. (Chapter 8, Ending your coverage in the plan, tells how you can leave our plan and
join a different Medicare plan.)
Section 9.2 What if you’re a resident in a long-term care facility?
Usually, a long-term care facility (such as a nursing home) has its own pharmacy, or a pharmacy
that supplies drugs for all of its residents. If you are a resident of a long-term care facility, you
may get your prescription drugs through the facility’s pharmacy as long as it is part of our
network.
If you need more information about a particular long-term care facility, please visit
optumrx.com, or contact OptumRx Member Services.
What if you’re a resident in a long-term care facility and become a new participant of the
plan?
If you are a new participant and a resident of a long-term care facility, and you need a drug that
is not on our Drug List or is restricted in some way, the plan will cover a temporary supply of
your drug during the first 90 days of your enrollment. The first supply will be for a maximum of
a 31-day supply, or less if your prescription is written for fewer days. If needed, we will cover
additional refills during your first 90 days in the plan.
If you have been a participant of the plan for more than 90 days and need a drug that is not on
our Drug List or if the plan has any restriction on the drug’s coverage, we will cover one 31-day
supply, or less if your prescription is written for fewer days.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
38
During the time when you are getting a temporary supply of a drug, you should talk with your
doctor or other prescriber to decide what to do when your temporary supply runs out. Perhaps
there is a different drug covered by the plan that might work just as well for you. Or you and
your doctor can ask the plan to make an exception for you and cover the drug in the way you
would like it to be covered. If you and your doctor want to ask for an exception, Chapter 7 tells
what to do.
Section 9.3 What if you are taking drugs covered by Original Medicare?
Your enrollment in the Fresno City Employees Health & Welfare Trust Medicare Prescription
Drug Plan doesn’t affect your coverage for drugs covered under Medicare Part A or Part B. If
you meet Medicare’s coverage requirements, your drug will still be covered under Medicare
Part A or Part B, even though you are enrolled this plan. In addition, if your drug would be
covered by Medicare Part A or Part B, our plan can’t cover it.
If your Plan covers Medicare Part B drugs, some drugs may be covered through the Fresno
City Employees Health & Welfare Trust Medicare Prescription Drug Plan in other situations.
But drugs are never covered by both Part B and our plan at the same time. In general, your
pharmacist or provider will determine whether to bill Medicare Part B or the Fresno City
Employees Health & Welfare Trust Medicare Prescription Drug Plan for the drug.
Section 9.4 What if you have a Medigap (Medicare Supplement Insurance) policy
with prescription drug coverage?
If you currently have a Medigap policy that includes coverage for prescription drugs, you must
contact your Medigap issuer and tell them you have enrolled in our plan. If you decide to keep
your current Medigap policy, your Medigap issuer will remove the prescription drug coverage
portion of your Medigap policy and lower your premium.
Each year your Medigap insurance company should send you a notice by November 15 that tells
if your prescription drug coverage is “creditable,” and the choices you have for drug coverage.
(If the coverage from the Medigap policy is “creditable,” it means that it has drug coverage that
pays, on average, at least as much as Medicare’s standard drug coverage.) The notice will also
explain how much your premium would be lowered if you remove the prescription drug
coverage portion of your Medigap policy. If you didn’t get this notice, of if you can’t find it,
contact your Medicare insurance company and ask for another copy.
In general, if you are currently employed, the prescription drug coverage you get from us will be
secondary to your employer or retiree group coverage. That means your group coverage would
pay first.
Section 9.5 What if you are in Medicare-certified Hospice?
Drugs are never covered by both hospice and our plan at the same time. If you are enrolled in
Medicare hospice and require an anti-nausea, laxative, pain medication, or antianxiety drug that

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
39
is not covered by your hospice because it is unrelated to your terminal illness and related
conditions, our plan must receive notification from either the prescriber or your hospice provider
that the drug is unrelated before our plan can cover the drug. To prevent delays in receiving any
unrelated drugs that should be covered by our plan, you can ask your hospice provider or
prescriber to make sure we have the notification that the drug is unrelated before you ask a
pharmacy to fill your prescription.
In the event you either revoke your hospice election or are discharged from hospice, our plan
should cover all your drugs. To prevent any delays at a pharmacy when your Medicare hospice
benefit ends, you should bring documentation to the pharmacy to verify your revocation or
discharge. See the previous parts of this section that tell about the rules for getting drug coverage
under Part D Chapter 4 (What you pay for your Part D prescription drugs) gives more
information about drug coverage and what you pay.
SECTION 10 Programs on drug safety and managing medications
Section 10.1 Programs to help participants use drugs safely
We conduct drug use reviews for our participants to help make sure that they are getting safe and
appropriate care. These reviews are especially important for participants who have more than one
provider who prescribes their drugs.
We do a review each time you fill a prescription. We also review our records on a regular basis.
During these reviews, we look for potential problems such as:
Possible medication errors.
Drugs that may not be necessary because you are taking another drug to treat the same
medical condition.
Drugs that may not be safe or appropriate because of your age or gender.
Certain combinations of drugs that could harm you if taken at the same time.
Prescriptions written for drugs that have ingredients you are allergic to.
Possible errors in the amount (dosage) of a drug you are taking.
If we see a possible problem in your use of medications, we will work with your doctor to
correct the problem.
Section 10.2 Medication Therapy Management (MTM) Program
Our MTM programs help our participants with special situations. For example, some participants
have several complex medical conditions or they may need to take many drugs at the same time,
or they could have very high drug costs.

Chapter 3: Using the plan’s coverage for your Part D prescription drugs
40
This program is free to participants. A team of pharmacists and doctors developed the programs
for us. The programs can help make sure that our participants are using the drugs that work best
to treat their medical conditions and help us identify possible medication errors.
A pharmacist or other health professional will give you a comprehensive review of all your
medications. You can talk about how best to take your medications, your costs, and any
problems or questions you have about your prescription and over-the-counter medications.
You’ll get a written summary of this discussion. The summary has a medication action plan that
recommends what you can do to make the best use of your medications, with space for you to
take notes or write down any follow-up questions. You’ll also get a personal medication list that
will include all the medications you’re taking and why you take them.
It’s a good idea to have your medication review before your yearly “Wellness” visit, so you can
talk to your doctor about your action plan and medication list. Bring your action plan and
medication list with you to your visit or anytime you talk with your doctors, pharmacists, and
other health care providers. Also, keep your medication list with you (for example, with your ID)
in case you go to the hospital or emergency room.
We will automatically enroll you in the program If you meet the criteria, and send you
information. If you decide not to participate, please notify us and we will withdraw your
participation in the program.

Chapter 4: What you pay for your Part D prescription drugs
41
Chapter 4. What you pay for your Part D prescription drugs
SECTION 1 Introduction ........................................................................................................43
Section 1.1 Use this chapter together with other materials that explain your drug coverage ...43
SECTION 2 What you pay for a drug depends on which “drug payment stage”
you are in when you get the drug .....................................................................43
Section 2.1 What are the four drug payment stages? ..........................................................43
SECTION 3 We send you reports that explain payments for your drugs and
which payment stage you are in .......................................................................44
Section 3.1 We send you a monthly report called the “Explanation of Benefits” ..............44
Section 3.2 Help us keep our information about your drug payments up to date ...............45
SECTION 4 During the Initial Coverage Stage, the plan pays its share of your
drug costs and you pay your share ..................................................................46
Section 4.1 What you pay for a drug depends on the drug and where you fill your
prescription ............................................................................................................46
Section 4.2 A table that shows your costs for a one-month supply of a drug ....................46
Section 4.3 You stay in the Initial Coverage Stage until your out-of-pocket costs for the
year reach $3,400 ...................................................................................................47
Section 4.4 If your doctor prescribes less than a full month's supply, you may not have to
pay the cost of the entire month's supply ...............................................................48
SECTION 5 The Coverage Gap Stage does not apply to members of the Fresno
City Employees Health & Welfare Trust...........................................................45
Section 5.1 You stay in the Initial Stage until your out-of-pocket costs reach $3,400 .......45
Section 5.2 How Medicare calculates your out-of-pocket costs for prescription
drugs………………………………………………………………………...50
SECTION 6 During the Catastrophic Coverage Stage, the plan pays all of the cost
for your drugs ....................................................................................................50

Chapter 4: What you pay for your Part D prescription drugs
42
Section 6.1 Once you are in the Catastrophic Coverage Stage, you will stay in this stage
for the rest of the year ............................................................................................50
SECTION 7 What you pay for vaccinations covered by Part D depends on how
and where you get them ....................................................................................51
Section 7.1 Our plan has separate coverage for the Part D vaccine medication itself and
for the cost of giving you the vaccination shot ......................................................51
Section 7.2 You may want to call us at Member Services before you get a vaccination ...52
SECTION 8 Do you have to pay the Part D “late enrollment penalty”?............................52
Section 8.1 What is the Part D “late enrollment penalty”? .................................................52
Section 8.2 How much is the Part D late enrollment penalty? ...........................................52
Section 8.3 In some situations, you can enroll late and not have to pay the penalty ..........53
Section 8.4 What can you do if you disagree about your late enrollment penalty? ............53

Chapter 4: What you pay for your Part D prescription drugs
43
SECTION 1 Introduction
Section 1.1 Use this chapter together with other materials that explain your drug
coverage
This chapter focuses on what you pay for your Part D prescription drugs. To keep things simple,
we use “drug” in this chapter to mean a Part D prescription drug. As explained in Chapter 3,
some drugs are covered under Original Medicare or are excluded by law.
To understand the payment information we give you in this chapter, you need to know the basics
of what drugs are covered, where to fill your prescriptions, and what rules to follow when you
get your covered drugs. Here are materials that explain these basics:
The plan’s List of Covered Drugs (Formulary). To keep things simple, we call this the
“Drug List.”
o The Drug List tells which drugs are covered for you.
o It also tells which of the five “cost-sharing tiers” the drug is in and whether there
are any restrictions on your coverage for the drug.
o If you need a copy of the Drug List, call OptumRx Member Services. You can also
find the Drug List on our website at optumrx.com.
Chapter 3 of this booklet. Chapter 3 gives the details about your prescription drug
coverage, including rules you need to follow when you get your covered drugs. Chapter 3
also tells which types of prescription drugs are not covered by our plan.
The plan’s Pharmacy Directory. In most situations you must use a network pharmacy
to get your covered drugs (see Chapter 3 for the details). The Pharmacy Locator Tool has
a list of pharmacies in the plan’s network. Visit optumrx.com to find a pharmacy near
you.
SECTION 2 What you pay for a drug depends on which “drug payment
stage” you are in when you get the drug
Section 2.1 What are the two drug payment stages?
As shown in the table below, there are four “drug payment stages” for your prescription drug
coverage. How much you pay for a drug depends on which of these stages you are in at the
time you get a prescription filled or refilled. Keep in mind you are always responsible for the
plan’s monthly premium regardless of the drug payment stage.

Chapter 4: What you pay for your Part D prescription drugs
44
Stage 1
Yearly Deductible
Stage
Stage 2
Initial Coverage Stage
Stage 3
Coverage Gap Stage
Stage 4
Catastrophic Coverage
Stage
Because there is no
deductible for the
plan, this payment
stage does not apply
to you.
You begin in this
payment stage. During
this stage, the plan pays
its share of the cost of
your drugs and you
pay your share of the
cost.
You stay in this stage
until your out-of-
pocket costs have
reached the $3,400
limit for the calendar
year. This amount and
rules for counting costs
toward this amount
have been set by
Medicare.
Because there is
no coverage gap
for the plan, this
payment stage
does not apply to
you.
Once you have paid
enough for your drugs
to move on to this last
payment stage, the plan
will pay all of the cost
of your drugs for the
rest of the year (through
December 31, 2017).
As shown in this summary of the four payment stages, whether you move on to the next payment
stage depends on how much you spend for your drugs.
SECTION 3 We send you reports that explain payments for your drugs
and which payment stage you are in
Section 3.1 We send you a monthly report called the “Explanation of Benefits”
Our plan keeps track of the costs of your prescription drugs and the payments you have made
when you get your prescriptions filled or refilled at the pharmacy. This way, we can tell you
when you have moved from one drug payment stage to the next. In particular, there are two types
of costs we keep track of:
We keep track of how much you have paid. This is called your “out-of-pocket” cost.
We keep track of your “total drug costs.” This is the amount you pay out-of-pocket
or others pay on your behalf plus the amount paid by the plan.
Our plan will send a written report called the Explanation of Benefits (it is sometimes called the
“EOB”) when you have had one or more prescriptions filled. It includes:

Chapter 4: What you pay for your Part D prescription drugs
45
Information for that month. This report gives the payment details about the
prescriptions you have filled during the previous month. It shows the total drugs costs,
what the plan paid, and what you and others on your behalf paid.
Totals for the year since January 1. This is called “year-to-date” information. It shows
you the total drug costs and total payments for your drugs since the year began.
Section 3.2 Help us keep our information about your drug payments up to date
To keep track of your drug costs and the payments you make for drugs, we use records we get
from pharmacies. Here is how you can help us keep your information correct and up to date:
Show your participant ID card when you get a prescription filled. To make sure we
know about the prescriptions you are filling and what you are paying, show your plan ID
card every time you get a prescription filled.
Make sure we have the information we need. There are times you may pay for
prescription drugs when we will not automatically get the information we need. To help
us keep track of your out-of-pocket costs, you may give us copies of receipts for drugs
that you have purchased. (If you are billed for a covered drug, you can ask our plan to
pay our share of the cost. For instructions on how to do this, go to Chapter 5 of this
booklet.) Here are some types of situations when you may want to give us copies of your
drug receipts to be sure we have a complete record of what you have spent for your
drugs:
o When you purchase a covered drug at a network pharmacy at a special price
o When you made a copayment for drugs that are provided under a drug
manufacturer patient assistance program.
o Any time you have purchased covered drugs at out-of-network pharmacies or
other times you have paid the full price for a covered drug under special
circumstances.
Send us information about the payments others have made for you. Payments made
by certain other individuals and organizations also count toward your out-of-pocket costs
and help qualify you for catastrophic coverage. For example, payments made by a State
Pharmaceutical Assistance Program, an AIDS drug assistance program, the Indian Health
Service, and most charities count toward your out-of-pocket costs. You should keep a
record of these payments and send them to us so we can track your costs.
Check the written report we send you. If you receive an Explanation of Benefits in the
mail, please look it over to be sure the information is complete and correct. If you think
something is missing from the report, or you have any questions, please call us at
OptumRx Member Services. Be sure to keep these reports. They are an important record
of your drug expenses.

Chapter 4: What you pay for your Part D prescription drugs
46
SECTION 4 During the Initial Coverage Stage, the plan pays its share of
your drug costs and you pay your share
Section 4.1 What you pay for a drug depends on the drug and where you fill your
prescription
You begin the Initial Coverage Stage when you fill your first prescription of the year. During this
phase, the plan pays its share of the cost of your covered prescription drugs, and you pay your
share. Your share of the cost will vary depending on the drug and where you fill your
prescription.
The plan has four Cost-Sharing Tiers
Every drug on the plan’s Drug List is in one of four cost-sharing tiers. In general, the higher the
cost-sharing tier number, the higher your cost for the drug:
Cost-Sharing Tier 1 includes Generic drugs. This is the lowest cost-sharing tier.
Cost-Sharing Tier 2 includes Preferred Brand drugs. This is the moderate cost-sharing
tier.
Cost-Sharing Tier 3 includes Non-Preferred Brand drugs. This is the highest cost-sharing
tier.
Cost-Sharing Tier 4 includes High-Cost Drugs. This tier is any drug that costs $600 or
more for up to a 30-day supply.
To find out which cost-sharing tier your drug is in, please reference your plan’s Drug List.
Your pharmacy choices
How much you pay for a drug depends on whether you get the drug from:
A network pharmacy that is in our plan’s network
The plan’s mail-order pharmacy
For more information about these pharmacy choices and filling your prescriptions, see Chapter 3
in this booklet and the plan’s Pharmacy Locator tool.
Section 4.2 A table that shows your costs for a 34-day and 90-day supply of a
drug
During the Initial Coverage Stage, your share of the cost of a covered drug will be a
copayment.
“Copayment” means that you pay a fixed amount each time you fill a prescription.
“Coinsurance” means that you pay a percent of the total cost of the drug each time you
fill a prescription.

Chapter 4: What you pay for your Part D prescription drugs
47
As shown in the table below, the amount of the copayment or coinsurance depends on which
tier your drug is in.
Your share of the cost when you get Covered Part D prescription drugs from:
Retail Network
pharmacy –
34-day supply
Retail Network
pharmacy –
90-day supply
The plan’s mail-
order service
Cost-Sharing Tier 1
(Generic drugs) 10%
10%
$5
Cost-Sharing Tier 2
(Preferred Brand drugs)
20% 20% $20
Cost-Sharing Tier 3
(Non-Preferred Brand
drugs)
40% 40% $50
Cost-Sharing Tier 4
(High-Cost drugs)
$100 $100 $100
Note: Amounts in these charts may vary according to your individual out-of-network cost
sharing responsibility.
Section 4.3 You stay in the Initial Coverage Stage until your out-of-pocket costs
have reached the $4,950 limit for the calendar year
You stay in the Initial Coverage Stage until your out-of-pocket costs have reached the Medicare
Part D limit of $4,950 for the calendar year, then you move on to the Catastrophic Coverage
Stage. However, our enhanced plan has a lower out-of-pocket maximum of only $3,400. If you
reach this amount before you reach the $4,950 Part D limit, the plan will pay for all of the cost of
your drugs.
We offer additional coverage on some prescription drugs that are not normally covered in a
Medicare Prescription Drug Plan. Payments made for these drugs will not count towards your
Initial coverage limit or total out-of-pocket costs.
The Explanation of Benefits that we send to you will help you keep track of how much you and
the plan have spent for your drugs during the year. We will let you know if you reach the limit
amount. If you do reach this amount, you will leave the Initial Coverage Stage and move on to
the Catastrophic Coverage Stage.

Chapter 4: What you pay for your Part D prescription drugs
48
Section 4.4 If your doctor prescribes less than a full month’s supply, you may not have to
pay the cost of the entire month’s supply
Typically, you pay a copay to cover a full month’s supply of a covered drug. However your
doctor can prescribe less than a month’s supply of drugs. There may be times when you want to
ask your doctor about prescribing less than a month’s supply of a drug (for example, when you
are trying a medication for the first time that is known to have serious side effects). If you doctor
agrees, you will not have to pay for the full month’s supply for certain drugs.
The amount you pay when you get less than a full month’s supply will depend on whether you
are responsible for paying coinsurance (a percentage of the total cost) or a copayment (a flat
dollar amount).
If you are responsible for coinsurance, you pay a percentage of the total cost of the drug.
You pay the same percentage regardless of whether the prescription is for a full month’s
supply or for fewer days. However, because the entire drug cost will be lower if you get
less than a full month’s supply, the amount you pay will be less.
If you are responsible for a copayment for the drug, your copay will be based on the
number of days of the drug that you receive. We will calculate the amount you pay per
day for your drug (the “daily cost-sharing rate”) and multiply it by the number of days of
the drug you receive.
Daily cost-sharing allows you to make sure a drug works for you before you have to pay for an
entire month’s supply.
SECTION 5 There is no Coverage Gap for Fresno City Employees
Health & Welfare Trust
Section 5.1 You do not have a coverage gap for your Part D drugs
There is no coverage gap for Fresno City Employees Health & Welfare Trust. Once you leave
the Initial Coverage Stage, you move on to the Catastrophic Coverage Stage. See Section 7 for
information about your coverage in the Catastrophic Coverage Stage.
Medicare has rules about what counts and what does not count as your out-of-pocket costs.
When you reach an out-of-pocket limit, you leave the Initial Stage and move on to the
Catastrophic Coverage Stage.

Chapter 4: What you pay for your Part D prescription drugs
49
Section 5.2 How Medicare calculates your out-of-pocket costs for prescription drugs
Medicare has rules about what counts and what does not count as your out-of-pocket costs.
When you reach an out-of-pocket limit of $3,400, you leave the Initial Coverage Stage and move
on to the Catastrophic Coverage Stage.
Here are Medicare’s rules that we must follow when we keep track of your out-of-pocket costs
for your drugs.
These payments are included in your out-of-pocket costs
When you add up your out-of-pocket costs, you can include the payments listed below (as
long as they are for Part D covered drugs and you followed the rules for drug coverage that
are explained in Chapter 3 of this booklet):
o The amount you pay for drugs when you are in any of the following drug payment
stages:
o The Initial Coverage Stage.
o Any payments you made during this calendar year as a member of a different Medicare
prescription drug plan before you joined our plan.
It matters who pays:
o If you make these payments yourself, they are included in your out-of-pocket costs.
o These payments are also included if they are made on your behalf by certain other
individuals or organizations. This includes payments for your drugs made by a friend
or relative, by most charities, by AIDS drug assistance programs, by a State
Pharmaceutical Assistance Program that is qualified by Medicare, or by the Indian
Health Service. Payments made by Medicare’s “Extra Help” Program are also included.
o Some of the payments made by the Medicare Coverage Gap Discount Program are
included. The amount the manufacturer pays for your brand name drugs is included. But
the amount the plan pays for your generic drugs is not included.
Moving on to the Catastrophic Coverage Stage:
When you (or those paying on your behalf) have spent a total of $3,400 in out-of-pocket
costs within the calendar year, you will move from the Initial Coverage Stage to the
Catastrophic Coverage Stage.

Chapter 4: What you pay for your Part D prescription drugs
50
These payments are not included in your out-of-pocket costs
When you add up your out-of-pocket costs, you are not allowed to include any of these
types of payments for prescription drugs:
o The amount you may pay for your monthly premium.
o Drugs you buy outside the United States and its territories.
o Drugs that are not covered by our plan.
o Drugs you get at an out-of-network pharmacy that do not meet the plan’s requirements
for out-of-network coverage.
o Non-Part D drugs, including prescription drugs covered by Part A or Part B and other
drugs excluded from coverage by Medicare.
o Prescription drugs covered by Part A or Part B.
o Payments you make toward drugs covered under our additional coverage but not
normally covered in a Medicare Prescription Drug Plan.
o Payments you make toward prescription drugs not normally covered in a Medicare
Prescription Drug Plan.
o Payments made by the plan for your brand or generic drugs while in the Coverage Gap.
o Payments for your drugs that are made by group health plans including employer health
plans.
o Payments for your drugs that are made by certain insurance plans and government-
funded health programs such as TRICARE and the Veteran’s Administration.
o Payments for your drugs made by a third-party with a legal obligation to pay for
prescription costs (for example, Worker’s Compensation).
Reminder: If any other organization such as the ones listed above pays part or all of your
out-of-pocket costs for drugs, you are required to tell our plan. Call Member Services to let
us know (phone numbers are printed on the front cover of this booklet).
SECTION 6 During the Catastrophic Coverage Stage, the plan pays
most of the cost for your drugs
Section 6.1 Once you are in the Catastrophic Coverage Stage, you will stay in this
stage for the rest of the year
You would qualify for the Catastrophic Coverage Stage when your out-of-pocket costs have
reached the Medicare Part D limit for the calendar year of $4,950. Once you are in the
Catastrophic Coverage Stage, you will stay in this payment stage until the end of the calendar
year. However, since your enhanced plan has a lower out-of-pocket maximum of only $3,400,
you will likely never reach this stage during the year.

Chapter 4: What you pay for your Part D prescription drugs
51
During this stage, the plan will pay most of the cost for your drugs.
Your share of the cost for a covered drug will be either coinsurance or a copayment,
whichever is the larger amount:
o - either – coinsurance of 5% of the cost of the drug
o – or – $3.30 copayment for a generic drug or a drug that is treated like a generic.
Or a $8.25 copayment for all other drugs.
Our plan pays the rest of the cost.
SECTION 7 What you pay for vaccinations depends on how and where
you get them
Section 7.1 Our plan has separate coverage for the vaccine medication itself and
for the cost of giving you the vaccination shot
Our plan provides coverage of a number of vaccines. There are two parts to our coverage of
vaccinations:
The first part of coverage is the cost of the vaccine medication itself. The vaccine is a
prescription medication.
The second part of coverage is for the cost of giving you the vaccination shot. (This is
sometimes called the “administration” of the vaccine.)
What do you pay for a vaccination?
What you pay for a vaccination depends on three things:
1. The type of vaccine (what you are being vaccinated for).
o Some vaccines are considered Part D drugs. You can find these vaccines listed in
the plan’s List of Covered Drugs.
2. Where you get the vaccine medication.
3. Who gives you the vaccination shot.
What you pay at the time you get the vaccination can vary depending on the circumstances. For
example:
Sometimes when you get your vaccination shot, you will have to pay the entire cost for
both the vaccine medication and for getting the vaccination shot. You can ask our plan to
pay you back for our share of the cost.
Other times, when you get the vaccine medication or the vaccination shot, you will pay
only your share of the cost.

Chapter 4: What you pay for your Part D prescription drugs
52
Section 7.2 You may want to call us at OptumRx Member Services before you get
a vaccination
The rules for coverage of vaccinations are complicated. We are here to help. We recommend that
you call us first at OptumRx Member Services whenever you are planning to get a vaccination.
We can tell you about how your vaccination is covered by our plan and explain your
share of the cost.
We can tell you how to keep your own cost down by using providers and pharmacies in
our network.
If you are not able to use a network provider and pharmacy, we can tell you what you
need to do to get payment from us for our share of the cost.
SECTION 8 Do you have to pay the Part D “late enrollment penalty”?
Section 8.1 What is the Part D “late enrollment penalty”?
You may pay a financial penalty if you did not enroll in a plan offering Medicare Part D
drug coverage when you first became eligible for this drug coverage or you experienced a
continuous period of 63 days or more when you didn’t keep your prescription drug
coverage. (“Creditable prescription drug coverage” is coverage that meets Medicare’s
minimum standards.) The amount of the penalty depends on how long you waited before
you enrolled in drug coverage after you became eligible or how many months after 63 days
you went without drug coverage.
The penalty is added to your monthly premium. (Participants who choose to pay their
premium every three months will have the penalty added to their three-month premium.)
When you first enroll in the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan, we let you know the amount of the penalty, if applicable.
Note: If you receive “Extra Help” from Medicare to pay for your prescription drugs, the late
enrollment penalty rules do not apply to you. You will not pay a late enrollment penalty, even if
you go without “creditable” prescription drug coverage.
Section 8.2 How much is the Part D late enrollment penalty?
Medicare determines the amount of the penalty. The penalty is 1% for every month that
you didn’t have creditable coverage. For our example, if you go 14 months without
creditable coverage, your premium will increase by an additional 14% each month.
There are three important things to note about this monthly premium penalty:
First, the penalty may change each year, because the average monthly premium can
change each year. If the national average premium (as determined by Medicare)
increases, your penalty will increase.

Chapter 4: What you pay for your Part D prescription drugs
53
Second, you will continue to pay a penalty every month for as long as you are enrolled
in a plan that has Medicare Part D drug benefits.
Third, if you are under 65 and currently receiving Medicare benefits, the late enrollment
penalty will reset when you turn 65. After age 65, your late enrollment penalty will be
based only on the months that you don’t have coverage after your initial enrollment
period for Medicare.
Section 8.3 In some situations, you can enroll late and not have to pay the penalty
Even if you have delayed enrolling in a plan offering Medicare Part D coverage when you were
first eligible, sometimes you do not have to pay the late enrollment penalty.
You will not have to pay a premium penalty for late enrollment if you are in any of these
situations:
You already have prescription drug coverage at least as good as Medicare’s standard drug
coverage. Medicare calls this “creditable drug coverage.” Creditable coverage could
include drug coverage from a former employer or union, TRICARE, or the Department
of Veterans Affairs. Speak with your insurer or your human resources department to find
out if your current drug coverage is as at least as good as Medicare’s.
If you were without creditable coverage, you can avoid paying the late enrollment penalty
if you were without it for less than 63 days in a row.
You are receiving Extra Help from Medicare.
Section 8.4 What can you do if you disagree about your late enrollment penalty?
If you disagree about your late enrollment penalty, you can ask us to review the decision about
your late enrollment penalty. . Generally, you must request this review within 60 days from the
date on the letter you receive stating you have to pay a late enrollment penalty. Call OptumRx
Member Services at the number on the front of this booklet to find out more about how to do
this.

Chapter 5: Asking the plan to pay its share of the costs for covered drugs
54
Chapter 5. Asking the plan to pay its share of the
costs for covered drugs
SECTION 1 Situations in which you should ask our plan to pay our share of the
cost of your covered drugs ................................................................................55
Section 1.1 If you pay our plan’s share of the cost of your covered drugs, you can ask us
for payment ............................................................................................................55
SECTION 2 How to ask us to pay you back ..........................................................................56
Section 2.1 How and where to send us your request for payment ......................................56
SECTION 3 We will consider your request for payment and say yes or no ......................57
Section 3.1 We check to see whether we should cover the drug and how much we owe ..57
Section 3.2 If we tell you that we will not pay for the drug, you can make an appeal .......57
SECTION 4 Other situations in which you should save your receipts and send
copies to us …………………..………………………………………………..58
Section 4.1 In some cases, you should send copies of your receipts to us to help us track
your out-of-pocket drug costs……………………………………..…………58

Chapter 5: Asking the plan to pay its share of the costs for covered drugs
55
SECTION 1 Situations in which you should ask our plan to pay our
share of the cost of your covered drugs
Section 1.1 If you pay our plan’s share of the cost of your covered drugs, you can
ask us for payment
Sometimes when you get a prescription drug, you may need to pay the full cost right away. Other
times, you may find that you have paid more than you expected under the coverage rules of the
plan. In either case, you can ask our plan to pay you back (paying you back is often called
“reimbursing” you). Asking for reimbursement in the first three examples below are types of
coverage decisions (for more information about coverage decisions, go to Chapter 7 of this
booklet).
Here are examples of situations in which you may need to ask our plan to pay you back:
1. When you use an out-of-network pharmacy to get a prescription filled
If you go to an out-of-network pharmacy and try to use your membership card to fill a
prescription, the pharmacy may not be able to submit the claim directly to us. When that
happens, you will have to pay the full cost of your prescription. (We cover prescriptions
filled at out-of-network pharmacies only in a few special situations. Please call Member
Service for more information).
Save your receipt and send a copy to us when you ask us to pay you back for our share
of the cost.
2. When you pay the full cost for a prescription because you don’t have your ID
card with you
If you do not have your plan ID card with you when you fill a prescription at a network
pharmacy, you may need to pay the full cost of the prescription yourself. The pharmacy can
usually call the plan to get your participant information, but there may be times when you
may need to pay if you do not have your card.
Save your receipt and send a copy to us when you ask us to pay you back for our share
of the cost.
3. When you pay the full cost for a prescription in other situations
You may pay the full cost of the prescription because you find that the drug is not covered
for some reason.
For example, the drug may not be on the plan’s List of Covered Drugs (Formulary); or
it could have a requirement or restriction that you didn’t know about or don’t think
should apply to you. If you decide to get the drug immediately, you may need to pay
the full cost for it.

Chapter 5: Asking the plan to pay its share of the costs for covered drugs
56
Save your receipt and send a copy to us when you ask us to pay you back. In some
situations, we may need to get more information from your doctor in order to pay you
back for our share of the cost.
All of the examples above are types of coverage decisions. This means that if we deny your
request for payment, you can appeal our decision. Chapter 7 of this booklet, What to do if you
have a problem or complaint (coverage decisions, appeals, complaints), has information about
how to make an appeal.
SECTION 2 How to ask us to pay you back
Section 2.1 How and where to send us your request for payment
Send us your request for payment, along with your receipt documenting the payment you have
made. It’s a good idea to make a copy of your receipts for your records.
To make sure you are giving us all the information we need to make a decision, you can fill out
our claim form to make your request for payment.
You don’t have to use the form, but it’s helpful for our plan to process the information
faster.
Either download a copy of the form from our website optumrx.com or call OptumRx
Member Services and ask for the form. The phone numbers for OptumRx Member
Services are on the cover of this booklet.
Mail your request for payment together with any receipts to us at this address:
OptumRx
Attn: Manual Claims
PO Box 968021
Schaumburg, IL 60196-8021
Please be sure to contact OptumRx Member Services if you have any questions. You can also
call if you want to give us more information about a request for payment you have already sent
to us.

Chapter 5: Asking the plan to pay its share of the costs for covered drugs
57
SECTION 3 We will consider your request for payment
Section 3.1 We check to see whether we should cover the drug and how much we
owe
When we receive your request for payment, we will let you know if we need any additional
information from you. Otherwise, we will consider your request and decide whether to pay it and
how much we owe.
If we decide that the drug is covered and you followed all the rules for getting the drug,
we will pay for our share of the cost. We will mail your reimbursement of all but your
share to you within 14 days. (Chapter 3 explains the rules you need to follow for getting
your Part D prescription drugs.)
If we decide that the drug is not covered, or you did not follow all the rules, we will not
pay for our share of the cost. Instead, we will send you a letter that explains the reasons
why we are not sending the payment you have requested and your rights to appeal that
decision.
Section 3.2 If we tell you that we will not pay for the drug, you can make an
appeal
If you think we have made a mistake in turning you down, you can make an appeal. If you make
an appeal, it means you are asking us to change the decision we made when we turned down
your request for payment. The examples of situations in which you may need to ask our plan to
pay you back:
When you use an out-of-network pharmacy to get a prescription filled
When you pay the full cost for a prescription because you don’t have your plan participant
ID card with you
When you pay the full cost for a prescription in other situations
For the details on how to make this appeal, go to Chapter 7 of this booklet, What to do if you
have a problem or complaint (coverage decisions, appeals, complaints). The appeals process is a
legal process with detailed procedures and important deadlines. If making an appeal is new to
you, you will find it helpful to start by reading Section 4 of Chapter 7. Section 4 is an
introductory section that explains the process for coverage decisions and appeals and gives
definitions of terms such as “appeal.” Then after you have read Section 4, you can go to the
Section 5 in Chapter 7 for a step-by-step explanation of how to file an appeal.

Chapter 5: Asking the plan to pay its share of the costs for covered drugs
58
SECTION 4 Other situations in which you should save your receipts and
send copies to us
Section 4.1 In some cases, you should send copies of your receipts to us to help us
track your out-of-pocket drug costs
There are some situations when you should let us know about payments you have made for your
drugs. In these cases, you are not asking us for payment. Instead, you are telling us about your
payments so that we can calculate your out-of-pocket costs correctly. This may help you to
qualify for the Catastrophic Coverage Stage more quickly. Here are two situations when you
should send us copies of receipts to let us know about payments you have made for your drugs:
1. When you buy the drug for a price that is lower than our price
Sometimes when you are in Deductible Stage and Coverage Gap Stage you can buy your
drug at a network pharmacy for a price that is lower than our price.
For example, a pharmacy might offer a special price on the drug. Or you may have a
discount card that is outside our benefit that offers a lower price.
Unless special conditions apply, you must use a network pharmacy in these situations
and your drug must be on our Drug List.
Save your receipt and send a copy to us so that we can have your out-of-pocket
expenses count toward qualifying you for the Catastrophic Coverage Stage.
Please note: If you are in the Deductible Stage and Coverage Gap Stage, we may not
pay for any share of these drug costs. But sending a copy of the receipt allows us to
calculate your out-of-pocket costs correctly and may help you qualify for the
Catastrophic Coverage Stage more quickly.
2. When you get a drug through a patient assistance program offered by a drug
manufacturer
Some members are enrolled in a patient assistance program offered by a drug manufacturer
that is outside the plan benefits. If you get any drugs through a program offered by a drug
manufacturer, you may pay a copayment to the patient assistance program.
Save your receipt and send a copy to us so that we can have your out-of-pocket
expenses count toward qualifying you for the Catastrophic Coverage Stage.
Please note: Because you are getting your drug through the patient assistance
program and not through the plan’s benefits, we will not pay for any share of these
drug costs. But sending a copy of the receipt allows us to calculate your out-of-pocket
costs correctly and may help you qualify for the Catastrophic Coverage Stage more
quickly.
Since you are not asking for payment in the two cases described above, these situations are not
considered coverage decisions. Therefore, you cannot make an appeal if you disagree with our
decision.

Chapter 6: Your rights and responsibilities
59
Chapter 6. Your rights and responsibilities
SECTION 1 Our plan must honor your rights as a participant of the plan ......................60
Section 1.1 We must provide information in a way that works for you (in languages other
than English that are spoken in the plan service area, in Braille, in large print,
or other alternate formats, etc.) ..............................................................................60
Section 1.2 We must treat you with fairness and respect at all times .................................60
Section 1.3 We must ensure that you get timely access to your covered drugs .................60
Section 1.4 We must protect the privacy of your personal health information ..................60
Section 1.5 We must give you information about the plan, its network of pharmacies, and
your covered drugs .................................................................................................61
Section 1.6 We must support your right to make decisions about your care ......................62
Section 1.7 You have the right to make complaints and to ask us to reconsider decisions
we have made .........................................................................................................63
Section 1.8 What can you do if you think you are being treated unfairly or your rights are
not being respected? ...............................................................................................63
Section 1.9 How to get more information about your rights ..............................................64
SECTION 2 You have some responsibilities as a participant of the plan ..........................64
Section 2.1 What are your responsibilities? ........................................................................64

Chapter 6: Your rights and responsibilities
60
SECTION 1 Our plan must honor your rights as a participant of the
plan
Section 1.1 We must provide information in a way that works for you
Our plan has translation services available to answer questions from non-English speaking
participants. Our Member Service Center has special telephone equipment that is used for people
who have difficulties with hearing or speaking. We can also give you information in Braille, in
large print, or other alternate formats if you need it upon request.
Plan information is available for your reference on our website at optumrx.com. To request plan
information be mailed to you, please call HealthComp.
Section 1.2 We must treat you with fairness and respect at all times
Our plan must obey laws that protect you from discrimination or unfair treatment. We do not
discriminate based on a person’s race, disability, religion, sex, health, ethnicity, creed (beliefs),
age, or national origin.
If you want more information or have concerns about discrimination or unfair treatment, please
call the Department of Health and Human Services’ Office for Civil Rights 1-800-368-1019
(TTY 1-800-537-7697) or your local Office for Civil Rights.
If you have a disability and need help with access to care, please call us OptumRx Member
Services. If you have a complaint, such as a problem with wheelchair access, OptumRx Member
Services can help.
Section 1.3 We must ensure that you get timely access to your covered drugs
As a participant of our plan, you also have the right to get your prescriptions filled or refilled at
any of our network pharmacies without long delays. If you think that you are not getting your
Part D drugs within a reasonable amount of time, Chapter 7 of this booklet tells what you can do.
Section 1.4 We must protect the privacy of your personal health information
Federal and state laws protect the privacy of your medical records and personal health
information. We protect your personal health information as required by these laws.
Your “personal health information” includes the personal information you gave us when
you enrolled in this plan as well as your medical records and other medical and health
information.
The laws that protect your privacy give you rights related to getting information and
controlling how your health information is used. The pharmacy provides you a written

Chapter 6: Your rights and responsibilities
61
notice, called a “Notice of Privacy Practice,” that tells about these rights and explains
how we protect the privacy of your health information.
How do we protect the privacy of your health information?
We make sure that unauthorized people don’t see or change your records.
In most situations, if we give your health information to anyone who isn’t providing your
care or paying for your care, we are required to get written permission from you first.
Written permission can be given by you or by someone you have given legal power to
make decisions for you.
There are certain exceptions that do not require us to get your written permission first.
These exceptions are allowed or required by law.
o For example, we are required to release health information to government
agencies that are checking on quality of care.
o Because you are a participant of our plan through Medicare, we are required to
give Medicare your health information including information about your Part D
prescription drugs. If Medicare releases your information for research or other
uses, this will be done according to Federal statutes and regulations.
You can see the information in your records and know how it has
been shared with others
You have the right to look at your records held at the plan, and to get a copy of your records. We
are allowed to charge you a fee for making copies. You also have the right to ask us to make
additions or corrections to your records. If you ask us to do this, we will consider your request
and decide whether the changes should be made.
You have the right to know how your health information has been shared with others for any
purposes that are not routine.
If you have questions or concerns about the privacy of your personal health information, please
call OptumRx Member Services.
Section 1.5 We must give you information about the plan, its network of
pharmacies, and your covered drugs
As a participant of our plan, you have the right to get several kinds of information from us.
If you want any of the following kinds of information, please call OptumRx Member Services:
Information about our plan. To request that a copy of plan information be mailed to
you, please contact OptumRx Member Services.

Chapter 6: Your rights and responsibilities
62
Information about our network pharmacies. You have the right to get information
from us about the pharmacies in our network. For a list of the pharmacies in the plan’s
network, you can call OptumRx Member Services or visit our website at optumrx.com.
Information about your coverage and rules you must follow in using your coverage.
To get the details on your Part D prescription drug coverage, see Chapters 3 and 4 of this
booklet, plus the plan’s List of Covered Drugs (Formulary). These chapters, together with
the List of Covered Drugs, tell you what drugs are covered and explain the rules you
must follow and the restrictions to your coverage for certain drugs. If you have questions
about the rules or restrictions, please call OptumRx Member Services.
Information about why something is not covered and what you can do about it. If a
Part D drug is not covered for you, or if your coverage is restricted in some way, you can
ask us for a written explanation. You have the right to this explanation even if you
received the drug from an out-of-network pharmacy.
If you are not happy or if you disagree with a decision we make about what Part D drug
is covered for you, you have the right to ask us to change the decision. For details on
what to do if something is not covered for you in the way you think it should be covered,
see Chapter 7 of this booklet. It gives you the details about how to ask the plan for a
decision about your coverage and how to make an appeal if you want us to change our
decision. (Chapter 7 also tells about how to make a complaint about quality of care,
waiting times, and other concerns.) If you want to ask our plan to pay our share of the
cost for a Part D prescription drug, see Chapter 5 of this booklet.
Section 1.6 We must support your right to make decisions about your care
You have the right to give instructions about what is to be done if you
are not able to make medical decisions for yourself
Sometimes people become unable to make health care decisions for themselves due to accidents
or serious illness. You have the right to say what you want to happen if you are in this situation.
This means that, if you want to, you can:
Fill out a written form to give someone the legal authority to make medical decisions
for you if you ever become unable to make decisions for yourself.
Give your doctors written instructions about how you want them to handle your
medical care if you become unable to make decisions for yourself.
The legal documents that you can use to give your directions in advance in these situations are
called “advance directives.” There are different types of advance directives and different names
for them. Documents called “living will” and “power of attorney for health care” are examples
of advance directives.
If you want to use an “advance directive” to give your instructions, here is what to do:

Chapter 6: Your rights and responsibilities
63
Get the form. If you want to have an advance directive, you can get a form from your
lawyer, from a social worker, or from some office supply stores. You can sometimes get
advance directive forms from organizations that give people information about Medicare.
Fill it out and sign it. Regardless of where you get this form, keep in mind that it is a
legal document. You should consider having a lawyer help you prepare it.
Give copies to appropriate people. You should give a copy of the form to your doctor
and to the person you name on the form as the one to make decisions for you if you can’t.
You may want to give copies to close friends or family participants as well. Be sure to
keep a copy at home.
If you know ahead of time that you are going to be hospitalized, and you have signed an advance
directive, take a copy with you to the hospital.
If you are admitted to the hospital, they will ask you whether you have signed an advance
directive form and whether you have it with you.
If you have not signed an advance directive form, the hospital has forms available and
will ask if you want to sign one.
Remember, it is your choice whether you want to fill out an advance directive (including
whether you want to sign one if you are in the hospital). According to law, no one can deny you
care or discriminate against you based on whether or not you have signed an advance directive.
What if your instructions are not followed?
If you have signed an advance directive, and you believe that a doctor or hospital hasn’t followed
the instructions in it, you may file a complaint with the State Department of Health.
Section 1.7 You have the right to make complaints and to ask us to reconsider
decisions we have made
If you have any problems or concerns about your covered services or care, Chapter 7 of this
booklet tells what you can do. It gives the details about how to deal with all types of problems
and complaints.
As explained in Chapter 7, what you need to do to follow up on a problem or concern depends on
the situation. You might need to ask our plan to make a coverage decision for you, make an
appeal to us to change a coverage decision, or make a complaint. Whatever you do – ask for a
coverage decision, make an appeal, or make a complaint – we are required to treat you fairly.
Section 1.8 What can you do if you think you are being treated unfairly or your
rights are not being respected?
If it is about discrimination, call the Office for Civil Rights

Chapter 6: Your rights and responsibilities
64
If you think you have been treated unfairly or your rights have not been respected due to your
race, disability, religion, sex, health, ethnicity, creed (beliefs), age, or national origin, you should
call the Department of Health and Human Services’ Office for Civil Rights at 1-800-368-1019
or TTY 1-800-537-7697, or call your local Office for Civil Rights.
Is it about something else?
If you think you have been treated unfairly or your rights have not been respected, and it’s not
about discrimination, you can get help dealing with the problem you are having:
You can call OptumRx Member Services.
You can call the State Health Insurance Assistance Program. For details about this
organization and how to contact it, go to Chapter 2, Section 3.
Section 1.9 How to get more information about your rights
There are several places where you can get more information about your rights:
You can call OptumRx Member Services.
You can call the State Health Insurance Assistance Program. For details about this
organization and how to contact it, go to Chapter 2, Section 3.
You can contact Medicare.
o You can visit the Medicare website (www.medicare.gov) to read or download the
publication “Your Medicare Rights & Protections.”
o Or, you can call 1-800-MEDICARE (1-800-633-4227) 24 hours a day, 7 days a
week. TTY users should call 1-877-486-2048.
SECTION 2 You have some responsibilities as a participant of the plan
Section 2.1 What are your responsibilities?
Things you need to do as a participant of the plan are listed below. If you have any questions,
please call OptumRx Member Services. We’re here to help.
Get familiar with your covered drugs and the rules you must follow to get these
covered drugs. Use this Evidence of Coverage booklet to learn what is covered for you
and the rules you need to follow to get your covered drugs.
o Chapters 3 and 4 give the details about your coverage for Part D prescription
drugs.

Chapter 6: Your rights and responsibilities
65
If you have any other prescription drug coverage besides our plan, you are required to
tell us. Please call 1-855-235-0294 to let us know.
o We are required to follow rules set by Medicare to make sure that you are using
all of your coverage in combination when you get your covered drugs from our
plan. This is called “coordination of benefits” because it involves coordinating
the drug benefits you get from our plan with any other drug benefits available to
you. We’ll help you with it.
Tell your doctor and pharmacist that you are enrolled in our plan. Show your plan ID
card whenever you get your Part D prescription drugs.
Help your doctors and other providers help you by giving them information,
asking questions, and following through on your care.
o To help your doctors and other health providers give you the best care, learn as
much as you are able to about your health problems and give them the
information they need about you and your health. Follow the treatment plans and
instructions that you and your doctors agree upon.
o If you have any questions, be sure to ask. Your doctors and other health care
providers are supposed to explain things in a way you can understand. If you ask
a question and you don’t understand the answer you are given, ask again.
Pay what you owe. As a plan participant, you are responsible for these payments:
o You must pay your plan premiums (if applicable) to continue being a participant
of our plan.
o For some of your drugs covered by the plan, you must pay your share of the cost
when you get the drug. This will be a copayment (a fixed amount) or coinsurance
(a percentage of the total cost) Chapter 4 tells what you must pay for your Part D
prescription drugs.
o If you get any drugs that are not covered by our plan or by other insurance you
may have, you must pay the full cost.
o If you are required to pay a late enrollment penalty, you must pay the penalty to
remain a member of the plan.
Tell us if you move. If you are going to move, contact Fresno City Employees Health &
Welfare Trust immediately to update your records to ensure you receive all necessary
correspondence.
o Call HealthComp if you move so that your participant records are up to date and
we know how to contact you.
Call OptumRx Member Services for help if you have questions or concerns. We also
welcome any suggestions you may have for improving our plan.
o Phone numbers and calling hours for OptumRx Member Services are on the cover
of this booklet.

Chapter 6: Your rights and responsibilities
66
o For more information on how to reach us, including our mailing address, please
see Chapter 2.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
67
Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
BACKGROUND
SECTION 1 Introduction ........................................................................................................69
Section 1.1 What to do if you have a problem or concern ..................................................69
Section 1.2 What about the legal terms? .............................................................................69
SECTION 2 You can get help from government organizations that are not
connected with us ...............................................................................................71
Section 2.1 Where to get more information and personalized assistance ...........................71
SECTION 3 To deal with your problem, which process should you use? ..........................71
Section 3.1 Should you use the process for coverage decisions and appeals? Or should you
use the process for making complaints? ................................................................71
COVERAGE DECISIONS AND APPEALS
SECTION 4 A guide to the basics of coverage decisions and appeals ................................71
Section 4.1 Asking for coverage decisions and making appeals: the big picture ...............71
Section 4.2 How to get help when you are asking for a coverage decision or making an
appeal .....................................................................................................................72
SECTION 5 Your Part D prescription drugs: How to ask for a coverage decision
or make an appeal .............................................................................................73
Section 5.1 This section tells you what to do if you have problems getting a Part D drug or
you want us to pay you back for a Part D drug ......................................................73
Section 5.2 What is an exception? ......................................................................................75
Section 5.3 Important things to know about asking for exceptions ....................................76
Section 5.4 Step-by-step: How to ask for a coverage decision, including an exception ....76

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
68
Section 5.5 Step-by-step: How to make a Level 1 Appeal (how to ask for a review of a
coverage decision made by our plan).....................................................................79
Section 5.6 Step-by-step: How to make a Level 2 Appeal .................................................82
SECTION 6 Taking your appeal to Level 3 and beyond .....................................................84
Section 6.1 Levels of Appeal 3, 4, and 5 for Part D Drug Appeals ....................................84
MAKING COMPLAINTS
SECTION 7 How to make a complaint about quality of care, waiting times,
customer service, or other concerns .................................................................85
Section 7.1 What kinds of problems are handled by the complaint process? .....................85
Section 7.2 The formal name for “making a complaint” is “filing a grievance” ................87
Section 7.3 Step-by-step: Making a complaint ...................................................................87
Section 7.4 You can also make complaints about quality of care to the Quality
Improvement Organization ....................................................................................88

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
69
BACKGROUND
SECTION 1 Introduction
Section 1.1 What to do if you have a problem or concern
Please call us first
Your health and satisfaction are important to us. When you have a problem or concern, we hope
you’ll try an informal approach first: Please call OptumRx Member Services. We will work with
you to try to find a satisfactory solution to your problem.
You have rights as a participant of our plan and as someone who is getting Medicare. We pledge
to honor your rights, to take your problems and concerns seriously, and to treat you with respect.
Two formal processes for dealing with problems
Sometimes you might need a formal process for dealing with a problem you are having as a
participant of our plan.
This chapter explains two types of formal processes for handling problems:
For some types of problems, you need to use the process for coverage decisions and
making appeals.
For other types of problems you need to use the process for making complaints.
Both of these processes have been approved by Medicare. To ensure fairness and prompt
handling of your problems, each process has a set of rules, procedures, and deadlines that must
be followed by us and by you.
Which one do you use? That depends on the type of problem you are having. The guide in
Section 3 will help you identify the right process to use.
Section 1.2 What about the legal terms?
There are technical legal terms for some of the rules, procedures, and types of deadlines
explained in this chapter. Many of these terms are unfamiliar to most people and can be hard to
understand.
To keep things simple, this chapter explains the legal rules and procedures using more common
words in place of certain legal terms. For example, this chapter generally says “making a
complaint” rather than “filing a grievance,” “coverage decision” rather than “coverage

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
70
determination,” and “Independent Review Organization” instead of “Independent Review
Entity.” It also uses abbreviations as little as possible.
However, it can be helpful – and sometimes quite important – for you to know the correct legal
terms for the situation you are in. Knowing which terms to use will help you communicate more
clearly and accurately when you are dealing with your problem and get the right help or
information for your situation. To help you know which terms to use, we include legal terms
when we give the details for handling specific types of situations.
SECTION 2 You can get help from government organizations that are
not connected with us
Section 2.1 Where to get more information and personalized assistance
Sometimes it can be confusing to start or follow through the process for dealing with a problem.
This can be especially true if you do not feel well or have limited energy. Other times, you may
not have the knowledge you need to take the next step. Perhaps both are true for you.
Get help from an independent government organization
We are always available to help you. But in some situations you may also want help or
guidance from someone who is not connected us. You can always contact your State Health
Insurance Assistance Program. This government program has trained counselors in every
state. The program is not connected with our plan or with any insurance company or health
plan. The counselors at this program can help you understand which process you should use to
handle a problem you are having. They can also answer your questions, give you more
information, and offer guidance on what to do.
Their services are free. You will find phone numbers in Chapter 2, Section 3 of this booklet.
You can also get help and information from Medicare
For more information and help in handling a problem, you can also contact Medicare. Here are
two ways to get information directly from Medicare:
You can call 1-800-MEDICARE (1-800-633-4227) 24 hours a day, 7 days a week.
TTY users should call 1-877-486-2048.
You can visit the Medicare website (www.medicare.gov).

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
71
SECTION 3 To deal with your problem, which process should you use?
Section 3.1 Should you use the process for coverage decisions and appeals? Or
should you use the process for making complaints?
If you have a problem or concern and you want to do something about it, you don’t need to read
this whole chapter. You just need to find and read the parts of this chapter that apply to your
situation. The guide that follows will help.
To figure out which part of this chapter will help with your specific problem or concern, START HERE
Is your problem or concern about your benefits or coverage?
(This includes problems about whether particular medical care or prescription drugs are covered or not,
the way in which they are covered, and problems related to payment for medical care or prescription
drugs.)
Yes. My problem is about benefits or coverage.
Go on to the next section of this chapter, Section 4, “A guide to the basics of coverage
decisions and appeals.”
No. My problem is not about benefits or coverage.
Skip ahead to Section 7 at the end of this chapter: “How to make a complaint about
quality of care, waiting times, customer service or other concerns.”
COVERAGE DECISIONS AND APPEALS
SECTION 4 A guide to the basics of coverage decisions and appeals
Section 4.1 Asking for coverage decisions and making appeals: the big picture
The process for coverage decisions and making appeals deals with problems related to your
benefits and coverage for prescription drugs, including problems related to payment. This is the
process you use for issues such as whether a drug is covered or not and the way in which the
drug is covered.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
72
Asking for coverage decisions
A coverage decision is a decision we make about your benefits and coverage, or about the amount we will pay for your prescription drugs. We make a coverage decision for you whenever you fill a prescription at a pharmacy.
We are making a coverage decision for you whenever we decide what is covered for you and how much we pay. Usually, there is no problem. We decide the drug is covered and pay our share of the cost. But in some cases we might decide the drug is not covered or is no longer covered by Medicare for you. If you disagree with this coverage decision, you can make an appeal.
Making an appeal
If we make a coverage decision and you are not satisfied with this decision, you can “appeal” the
decision. An appeal is a formal way of asking us to review and change a coverage decision we
have made.
When you make an appeal we review the coverage decision we have made to check to see if we
were being fair and following all of the rules properly. When we have completed the review we
give you our decision.
If we say no to all or part of your Level 1 Appeal, your case will automatically go on to a Level 2
Appeal. The Level 2 Appeal is conducted by an independent organization that is not connected to
our plan. If you are not satisfied with the decision at the Level 2 Appeal, you may be able to
continue through several more levels of appeal.
Section 4.2 How to get help when you are asking for a coverage decision or
making an appeal
Would you like some help? Here are resources you may wish to use if you decide to ask for any
kind of coverage decision or appeal a decision:
You can call us at OptumRx Member Services.
To get free help from an independent organization that is not connected with our plan,
contact your State Health Insurance Assistance Program (see Section 2 of this chapter).
You should consider getting your doctor or other prescriber involved if possible,
especially if you want a “fast” or “expedited” decision. In most situations involving a
coverage decision or appeal, your doctor or other prescriber must explain the medical
reasons that support your request. Your doctor or other prescriber can’t request every
appeal. He/she can request a coverage decision and a Level 1 Appeal with the plan. To
request any appeal after Level 1, your doctor or other prescriber must be appointed as
your “representative” (see below about “representatives”).
You can ask someone to act on your behalf. If you want to, you can name another
person to act for you as your “representative” to ask for a coverage decision or make an
appeal.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
73
o There may be someone who is already legally authorized to act as your
representative under State law.
o If you want a friend, relative, your doctor or other prescriber, or other person to
be your representative, call OptumRx Member Services and ask for the form to
give that person permission to act on your behalf. The form must be signed by
you and by the person who you would like to act on your behalf. You must give
our plan a copy of the signed form.
You also have the right to hire a lawyer to act for you. You may contact your own
lawyer, or get the name of a lawyer from your local bar association or other referral
service. There are also groups that will give you free legal services if you qualify.
However, you are not required to hire a lawyer to ask for any kind of coverage
decision or appeal a decision.
SECTION 5 Your Part D prescription drugs: How to ask for a coverage
decision or make an appeal
? Have you read Section 4 of this chapter (A guide to “the
basics” of coverage decisions and appeals)? If not, you may
want to read it before you start this section.
Section 5.1 This section tells you what to do if you have problems getting a Part D
drug or you want us to pay you back for a Part D drug
Your benefits as a participant of our plan include coverage for many outpatient prescription
drugs. Medicare calls these outpatient prescription drugs “Part D drugs.” You can get these drugs
as long as they are included in our plan’s List of Covered Drugs (Formulary) and they are
medically necessary for you, as determined by your primary care doctor or other provider.
This section is about your Part D drugs only. To keep things simple, we generally say
“drug” in the rest of this section, instead of repeating “covered outpatient prescription
drug” or “Part D drug” every time.
For details about what we mean by Part D drugs, the List of Covered Drugs, rules and
restrictions on coverage, and cost information, see Chapter 5 (Using our plan’s coverage
for your Part D prescription drugs) and Chapter 6 (What you pay for your Part D
prescription drugs).
Part D coverage decisions and appeals
As discussed in Section 4 of this chapter, a coverage decision is a decision we make about your
benefits and coverage or about the amount we will pay for your drugs.
Legal
Terms
A coverage decision is often called an “initial determination” or “initial
decision.” When the coverage decision is about your Part D drugs, the

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
74
initial determination is called a “coverage determination.”
Here are examples of coverage decisions you ask us to make about your Part D drugs:
You ask us to make an exception, including:
o Asking us to cover a Part D drug that is not on the plan’s List of Covered Drugs
o Asking us to waive a restriction on the plan’s coverage for a drug (such as limits
on the amount of the drug you can get)
o Asking to pay a lower cost-sharing amount for a covered drug on a higher cost-
sharing tier
You ask us whether a drug is covered for you and whether you satisfy any applicable
coverage rules. (For example, when your drug is on the plan’s List of Covered Drugs but we
require you to get approval from us before we will cover it for you.)
You ask us to pay for a prescription drug you already bought. This is a request for a coverage
decision about payment.
If you disagree with a coverage decision we have made, you can appeal our decision.
This section tells you both how to ask for coverage decisions and how to request an appeal. Use
this guide to help you determine which part has information for your situation:
If you are in this situation: This is what you can do:
Do you need a drug that isn’t on our Drug
List or need us to waive a rule or restriction
on a drug we cover?
You can ask us to make an exception. (This is a
type of coverage decision.)
Start with Section 5.2 of this chapter
Do you want us to cover a drug on our Drug
List and you believe you meet any plan
rules or restrictions (such as getting
approval in advance) for the drug you need?
You can ask us for a coverage decision.
Skip ahead to Section 5.4 of this chapter.
Do you want to ask us to pay you back for a
drug you have already received and paid
for?
You can ask us to pay you back. (This is a type
of coverage decision.)
Skip ahead to Section 5.4 of this chapter.
Have we already told you that we will not
cover or pay for a drug in the way that you
want it to be covered or paid for?
You can make an appeal. (This means you are
asking us to reconsider.)
Skip ahead to Section 5.5 of this chapter.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
75
Section 5.2 What is an exception?
If a drug is not covered in the way you would like it to be covered, you can ask the plan to make
an “exception.” An exception is a type of coverage decision. Similar to other types of coverage
decisions, if we turn down your request for an exception, you can appeal our decision.
When you ask for an exception, your doctor or other prescriber will need to explain the medical
reasons why you need the exception approved. We will then consider your request. Here are
three examples of exceptions that you or your doctor or other prescriber can ask us to make:
1. Covering a Part D drug for you that is not on our plan’s List of Covered Drugs
(Formulary). We call it the “Drug List.”
Legal
Terms Asking for coverage of a drug that is not on the Drug List is sometimes
called asking for a “formulary exception.”
If we agree to make an exception and cover a drug that is not on the Drug List, you
will need to pay the cost-sharing amount that applies to the drug. You cannot ask for
an exception to the copayment or co-insurance amount we require you to pay for the
drug.
You cannot ask for coverage of any “excluded drugs” or other non-Part D drugs
which Medicare does not cover. (For more information about excluded drugs, see
Chapter 5.)
2. Removing a restriction on the plan’s coverage for a covered drug. There are extra rules
or restrictions that apply to certain drugs on the plan’s List of Covered Drugs (for more
information, go to Chapter 3).
Legal
Terms Asking for removal of a restriction on coverage for a drug is sometimes
called asking for a “formulary exception.”
The extra rules and restrictions on coverage for certain drugs may include:
o Being required to use the generic version of a drug instead of the brand-name
drug.
o Getting plan approval in advance before we will agree to cover the drug for
you. (This is sometimes called “prior authorization.”)
o Being required to try a different drug first before we will agree to cover the
drug you are asking for. (This is sometimes called “step therapy.”)
o Quantity limits. For some drugs, there are restrictions on the amount of the
drug you can have.
If our plan agrees to make an exception and waive a restriction for you, you can ask
for an exception to the copayment or co-insurance amount we require you to pay for
the drug.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
76
Changing coverage of a drug to a lower cost-sharing tier. Every drug on the plan’s Drug List
is in one of five cost-sharing tiers. In general, the lower the cost-sharing tier number, the less
you will pay as your share of the cost of the drug.
We are not allowed to change the cost-sharing tier for any drug in the high-cost drug tier.
Legal
Terms
Asking to pay a lower preferred price for a covered non-preferred drug is
sometimes called asking for a “tiering exception.”
If your drug is in Tier 3 you can ask us to cover it at the cost-sharing amount that
applies to drugs in Tier 2. This would lower your share of the cost for the drug.
Section 5.3 Important things to know about asking for exceptions
Your doctor must tell us the medical reasons
Your doctor or other prescriber must give us a written statement that explains the medical
reasons for requesting an exception. For a faster decision, include this medical information from
your doctor or other prescriber when you ask for the exception.
Typically, our Drug List includes more than one drug for treating a particular condition. These
different possibilities are called “alternative” drugs. If an alternative drug would be just as
effective as the drug you are requesting and would not cause more side effects or other health
problems, we will generally not approve your request for an exception. If you ask us for a tiering
exception, we will generally not approve your request for an exception unless all alternative
drugs in the low cost-sharing tiers won’t work as well for you.
Our plan can say yes or no to your request
If we approve your request for an exception, our approval usually is valid until the end of
the plan year. This is true as long as your doctor continues to prescribe the drug for you
and that drug continues to be safe and effective for treating your condition.
If we say no to your request for an exception, you can ask for a review of our decision by
making an appeal. Section 5.5 tells you how to make an appeal if we say no.
The next section tells you how to ask for a coverage decision, including an exception.
Section 5.4 Step-by-step: How to ask for a coverage decision, including an
exception
Step 1: You ask our plan to make a coverage decision about the drug(s) or payment you need. If
your health requires a quick response, you must ask us to make a “fast decision.” You cannot ask
for a fast decision if you are asking us to pay you back for a drug you already bought.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
77
What to do:
Request the type of coverage decision you want. Start by calling, writing, or
faxing our plan to make your request. You, your representative, or your doctor (or
other prescriber) can do this. For the details, go to Chapter 2, Section 1 and look
for the section called, How to contact our plan when you are asking for a coverage
decision about your Part D prescription drugs. Or if you are asking us to pay you
back for a drug, go to the section called, Where to send a request that asks us to
pay for our share of the cost for medical care or a drug you have received.
You or your doctor or someone else who is acting on your behalf can ask for a
coverage decision. Section 4 of this chapter tells how you can give written
permission to someone else to act as your representative. You can also have a
lawyer act on your behalf.
If you want to ask our plan to pay you back for a drug, start by reading Chapter
7 of this booklet: Asking the plan to pay its share of a bill you have received for
medical services or drugs. Chapter 7 describes the situations in which you may
need to ask for reimbursement. It also tells how to send us the paperwork that asks
us to pay you back for our share of the cost of a drug you have paid for.
If you are requesting an exception, provide the “doctor’s statement.” Your
doctor or other prescriber must give us the medical reasons for the drug exception
you are requesting. (We call this the “doctor’s statement.”) Your doctor or other
prescriber can fax or mail the statement to our plan. Or your doctor or other
prescriber can tell us on the phone and follow up by faxing or mailing the signed
statement. See Sections 5.2 and 5.3 for more information about exception requests.
If your health requires it, ask us to give you a “fast decision”
Legal
Terms
A “fast decision” is called an “expedited decision.”
When we give you our decision, we will use the “standard” deadlines unless we
have agreed to use the “fast” deadlines. A standard decision means we will give
you an answer within 72 hours after we receive your doctor’s statement. A fast
decision means we will answer within 24 hours.
To get a fast decision, you must meet two requirements:
o You can get a fast decision only if you are asking for a drug you have not yet
received. (You cannot get a fast decision if you are asking us to pay you back
for a drug you are already bought.)
o You can get a fast decision only if using the standard deadlines could cause
serious harm to your health or hurt your ability to function.
If your doctor or other prescriber tells us that your health requires a “fast
decision,” we will automatically agree to give you a fast decision.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
78
If you ask for a fast decision on your own (without your doctor’s or other prescriber’s
support), our plan will decide whether your health requires that we give you a fast
decision.
o If we decide that your medical condition does not meet the requirements for a
fast decision, we will send you a letter that says so (and we will use the
standard deadlines instead).
o This letter will tell you that if your doctor or other prescriber asks for the fast
decision, we will automatically give a fast decision.
o The letter will also tell how you can file a complaint about our decision to give
you a standard decision instead of the fast decision you requested. It tells how
to file a “fast” complaint, which means you would get our answer to your
complaint within 24 hours. (The process for making a complaint is different
from the process for coverage decisions and appeals. For more information
about the process for making complaints, see Section 7 of this chapter.)
Step 2: Our plan considers your request and we give you our answer.
Deadlines for a “fast” coverage decision
If we are using the fast deadlines, we must give you our answer within 24
hours.
o Generally, this means within 24 hours after we receive your request. If you are
requesting an exception, we will give you our answer within 24 hours after we
receive your doctor’s statement supporting your request. We will give you our
answer sooner if your health requires us to.
o If we do not meet this deadline, we are required to send your request on to Level
2 of the appeals process, where it will be reviewed by an independent outside
organization. Later in this section, we tell about this review organization and
explain what happens at Appeal Level 2.
If our answer is yes to part or all of what you requested, we must provide the
coverage we have agreed to provide within 24 hours after we receive your request or
doctor’s statement supporting your request.
If our answer is no to part or all of what you requested, we will send you a written
statement that explains why we said no.
Deadlines for a “standard” coverage decision about a drug you have not yet received
If we are using the standard deadlines, we must give you our answer within 72
hours.
o Generally, this means within 72 hours after we receive your request. If you
are requesting an exception, we will give you our answer within 72 hours after
we receive your doctor’s statement supporting your request. We will give you
our answer sooner if your health requires us to.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
79
o If we do not meet this deadline, we are required to send your request on to
Level 2 of the appeals process, where it will be reviewed by an independent
organization. Later in this section, we tell about this review organization and
explain what happens at Appeal Level 2.
If our answer is yes to part or all of what you requested –
o If we approve your request for coverage, we must provide the coverage we
have agreed to provide within 72 hours after we receive your request or
doctor’s statement supporting your request.
If our answer is no to part or all of what you requested, we will send you a written
statement that explains why we said no.
Deadlines for a “standard” coverage decision about payment for a drug you have already
bought
We must give you our answer within 14 calendar days after we receive your
request.
o If we do not meet this deadline, we are required to send your request on to
Level 2 of the appeals process, where it will be reviewed by an independent
organization. Later in this section, we tell about this review organization and
explain what happens at Appeal Level 2.
If our answer is yes to part or all of what you requested
o If we approve your request for coverage, we are also required to make
payment to you within 14 calendar days after we receive your request.
If our answer is no to part or all of what you requested, we will send you a written
statement that explains why we said no.
Step 3: If we say no to your coverage request, you decide if you want to make an appeal.
If our plan says no, you have the right to request an appeal. Requesting an appeal
means asking us to reconsider – and possibly change – the decision we made.
Section 5.5 Step-by-step: How to make a Level 1 Appeal
(how to ask for a review of a coverage decision made by our plan)
Legal
Terms
When you start the appeals process by making an appeal, it is called the
“first level of appeal” or a “Level 1 Appeal.”
An appeal to the plan about a Part D drug coverage decision is called a plan
“redetermination.”
Step 1: You contact our plan and make your Level 1 Appeal. If your health requires a quick
response, you must ask for a “fast appeal.”

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
80
What to do:
To start your appeal, you (or your representative or your doctor or other
prescriber) must contact our plan.
o For details on how to reach us by phone, fax, mail, or in person for any
purpose related to your appeal, go to Chapter 2, Section 1, and look for the
section called, How to contact our plan when you are making an appeal
about your Part D prescription drugs.
Make your appeal in writing by submitting a signed request.
If you are asking for a standard appeal, make your appeal by submitting a
written request.
If you are asking for a fast appeal, you may make your appeal in writing or
you may call us at OptumRx Member Services.
You must make your appeal request within 60 calendar days from the date on
the written notice we sent to tell you our answer to your request for a coverage
decision. If you miss this deadline and have a good reason for missing it, we may
give you more time to make your appeal.
You can ask for a copy of the information in your appeal and add more
information.
o You have the right to ask us for a copy of the information regarding your
appeal. We are allowed to charge a fee for copying and sending this
information to you.
o If you wish, you and your doctor or other prescriber may give us additional
information to support your appeal.
If your health requires it, ask for a “fast appeal”
Legal
Terms
A “fast appeal” is also called an “expedited appeal.”
If you are appealing a decision our plan made about a drug you have not yet received,
you and your doctor or other prescriber will need to decide if you need a “fast
appeal.”
The requirements for getting a “fast appeal” are the same as those for getting a
“fast decision” in Section 5.4 of this chapter.
Step 2: Our plan considers your appeal and we give you our answer.
When our plan is reviewing your appeal, we take another careful look at all of the
information about your coverage request. We check to see if we were being fair and
following all the rules when we said no to your request. We may contact you or your
doctor or other prescriber to get more information.
Deadlines for a “fast” appeal

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
81
If we are using the fast deadlines, we must give you our answer within 72 hours
after we receive your appeal. We will give you our answer sooner if your health
requires it.
o If we do not give you an answer within 72 hours, we are required to send your
request on to Level 2 of the appeals process, where it will be reviewed by an
Independent Review Organization. (Later in this section, we tell about this
review organization and explain what happens at Level 2 of the appeals
process.)
If our answer is yes to part or all of what you requested, we must provide the
coverage we have agreed to provide within 72 hours.
If our answer is no to part or all of what you requested, we will send you a written
statement that explains why we said no and how to appeal our decision.
Deadlines for a “standard” appeal
If we are using the standard deadlines, we must give you our answer within 7
calendar days after we receive your appeal. We will give you our decision sooner if
you have not received the drug yet and your health condition requires us to do so.
o If we do not give you a decision within 7 calendar days, we are required to send
your request on to Level 2 of the appeals process, where it will be reviewed by
an Independent Review Organization. Later in this section, we tell about this
review organization and explain what happens at Level 2 of the appeals process.
If our answer is yes to part or all of what you requested:
o If we approve a request for coverage, we must provide the coverage we have
agreed to provide as quickly as your health requires, but no later than 7
calendar days after we receive your appeal.
o If we approve a request to pay you back for a drug you already bought, we are
required to send payment to you within 30 calendar days after we receive
your appeal request.
If our answer is no to part or all of what you requested, we will send you a written
statement that explains why we said no and how to appeal our decision.
Step 3: If we say no to your appeal, you decide if you want to continue with the appeals process
and make another appeal.
If our plan says no to your appeal, you then choose whether to accept this decision or
continue by making another appeal.
If you decide to make another appeal, it means your appeal is going on to Level 2 of
the appeals process (see below).

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
82
Section 5.6 Step-by-step: How to make a Level 2 Appeal
If our plan says no to your appeal, you then choose whether to accept this decision or continue
by making another appeal. If you decide to go on to a Level 2 Appeal, the Independent Review
Organization reviews the decision our plan made when we said no to your first appeal. This
organization decides whether the decision we made should be changed.
Legal
Terms
The formal name for the “Independent Review Organization” is the
“Independent Review Entity.” It is sometimes called the “IRE.”
Step 1: To make a Level 2 Appeal, you must contact the Independent Review Organization and
ask for a review of your case.
If our plan says no to your Level 1 Appeal, the written notice we send you will
include instructions on how to make a Level 2 Appeal with the Independent
Review Organization. These instructions will tell who can make this Level 2 Appeal,
what deadlines you must follow, and how to reach the review organization.
When you make an appeal to the Independent Review Organization, we will send the
information we have about your appeal to this organization. This information is called
your “case file.” You have the right to ask us for a copy of your case file. We are
allowed to charge you a fee for copying and sending this information to you.
You have a right to give the Independent Review Organization additional information
to support your appeal.
Step 2: The Independent Review Organization does a review of your appeal and gives you an
answer.
The Independent Review Organization is an outside, independent organization
that is hired by Medicare. This organization is not connected with our plan and it is
not a government agency. This organization is a company chosen by Medicare to
review our decisions about your Part D benefits with our plan.
Reviewers at the Independent Review Organization will take a careful look at all of
the information related to your appeal. The organization will tell you its decision in
writing and explain the reasons for it.
Deadlines for “fast” appeal at Level 2
If your health requires it, ask the Independent Review Organization for a “fast
appeal.”
If the review organization agrees to give you a “fast appeal,” the review organization
must give you an answer to your Level 2 Appeal within 72 hours after it receives
your appeal request.
If the Independent Review Organization says yes to part or all of what you
requested, we must provide the drug coverage that was approved by the review

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
83
organization within 24 hours after we receive the decision from the review
organization.
Deadlines for “standard” appeal at Level 2
If you have a standard appeal at Level 2, the review organization must give you an
answer to your Level 2 Appeal within 7 calendar days after it receives your appeal.
If the Independent Review Organization says yes to part or all of what you
requested
o If the Independent Review Organization approves a request for coverage, we
must provide the drug coverage that was approved by the review organization
within 72 hours after we receive the decision from the review organization.
o If the Independent Review Organization approves a request to pay you back for
a drug you already bought, we are required to send payment to you within 30
calendar days after we receive the decision from the review organization.
What if the review organization says no to your appeal?
If this organization says no to your appeal, it means the organization agrees with
our decision not to approve your request. (This is called “upholding the decision.”
It is also called “turning down your appeal.”)
To continue and make another appeal at Level 3, the dollar value of the drug
coverage you are requesting must meet a minimum amount. If the dollar value of
the coverage you are requesting is too low, you cannot make another appeal and
the decision at Level 2 is final. The notice you get from the Independent Review
Organization will tell you if the dollar value of the coverage you are requesting is
high enough to continue with the appeals process.
Step 3: If the dollar value of the coverage you are requesting meets the requirement, you choose
whether you want to take your appeal further.
There are three additional levels in the appeals process after Level 2 (for a total of
five levels of appeal).
If your Level 2 Appeal is turned down and you meet the requirements to continue
with the appeals process, you must decide whether you want to go on to Level 3 and
make a third appeal. If you decide to make a third appeal, the details on how to do
this are in the written notice you got after your second appeal.
The Level 3 Appeal is handled by an administrative law judge. Section 6 in this
chapter tells more about Levels 3, 4, and 5 of the appeals process.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
84
SECTION 6 Taking your appeal to Level 3 and beyond
Section 6.1 Levels of Appeal 3, 4, and 5 for Part D Drug Appeals
This section may be appropriate for you if you have made a Level 1 Appeal and a Level 2
Appeal, and both of your appeals have been turned down.
If the dollar value of the drug you have appealed meets certain minimum levels, you may be able
to go on to additional levels of appeal. If the dollar value is less than the minimum level, you
cannot appeal any further. If the dollar value is high enough, the written response you receive to
your Level 2 Appeal will explain who to contact and what to do to ask for a Level 3 Appeal.
For most situations that involve appeals, the last three levels of appeal work in much the same
way. Here is who handles the review of your appeal at each of these levels.
Level 3 Appeal A judge who works for the Federal government will review your
appeal and give you an answer. This judge is called an “Administrative
Law Judge.”
If the answer is yes, the appeals process is over. What you asked for in the appeal has
been approved.
If the answer is no, the appeals process may or may not be over.
o If you decide to accept this decision that turns down your appeal, the appeals
process is over.
o If you do not want to accept the decision, you can continue to the next level of the
review process. If the administrative judge says no to your appeal, the notice you
get will tell you what to do next if you choose to continue with you appeal.
Whenever the reviewer says no to your appeal, the notice you get will tell you
whether the rules allow you to go on to another level of appeal. If the rules allow
you to go on, the written notice will also tell you who to contact and what to do next
if you choose to continue with your appeal.
Level 4 Appeal The Medicare Appeals Council will review your appeal and give you
an answer. The Medicare Appeals Council works for the Federal
government.
If the answer is yes, the appeals process is over. What you asked for in the appeal has
been approved.
If the answer is no, the appeals process may or may not be over.
o If you decide to accept this decision that turns down your appeal, the appeals
process is over.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
85
o If you do not want to accept the decision, you might be able to continue to the next
level of the review process. It depends on your situation. If the Medicare Appeals
Council says no to your appeal or denies your request to review the appeal, the
notice you get will tell you whether the rules allow you to go on to a Level 5
Appeal. If the rules allow you to go on, the written notice will also tell you who to
contact and what to do next if you choose to continue with your appeal.
Level 5 Appeal A judge at the Federal District Court will review your appeal.
This is the last stage of the appeals process.
This is the last step of the administrative appeals process.
MAKING COMPLAINTS
SECTION 7 How to make a complaint about quality of care, waiting
times, customer service, or other concerns
? If your problem is about decisions related to benefits, coverage, or payment,
then this section is not for you. Instead, you need to use the process for
coverage decisions and appeals. Go to Section 4 of this chapter.
Section 7.1 What kinds of problems are handled by the complaint process?
This section explains how to use the process for making complaints. The complaint process is
used for certain types of problems only. This includes problems related to quality of care, waiting
times, and the customer service you receive. Here are examples of the kinds of problems handled
by the complaint process.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
86
Complaint Example
Quality of your
medical care
Are you unhappy with the quality of the care you have received?
Respecting your
privacy
Do you believe that someone did not respect your right to privacy or
shared information about you that you feel should be confidential?
Disrespect, poor
customer service,
or other negative
behaviors
Has someone been rude or disrespectful to you?
Are you unhappy with how our Member Services has treated you?
Do you feel you are being encouraged to leave the plan?
Waiting times Have you been kept waiting too long by pharmacists? Or by our Member
Services or other staff at the plan?
Examples include waiting too long on the phone or when getting a
prescription.
Cleanliness Are you unhappy with the cleanliness or condition of a pharmacy?
Information you
get from us
Do you believe we have not given you a notice that we are required to
give?
Do you think written information we have given you is hard to
understand?
Timeliness
(These types of
complaints are all
related to the
timeliness of our
actions related to
coverage decisions
and appeals)
The process of asking for a coverage decision and making appeals is
explained in sections 4-6 of this chapter. If you are asking for a decision
or making an appeal, you use that process, not the complaint process.
However, if you have already asked us for a coverage decision or made
an appeal, and you think that we are not responding quickly enough, you
can also make a complaint about our slowness. Here are examples:
If you have asked us to give you a “fast coverage decision” or a “fast
appeal,” and we have said we will not, you can make a complaint.
If you believe we are not meeting the deadlines for giving you a coverage
decision or an answer to an appeal you have made, you can make a
complaint.
When a coverage decision we made is reviewed and we are told that we
must cover or reimburse you for certain drugs, there are deadlines that
apply. If you think we are not meeting these deadlines, you can make a
complaint.
When we do not give you a decision on time, we are required to forward
your case to the Independent Review Organization. If we do not do that
within the required deadline, you can make a complaint.

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
87
Section 7.2 The formal name for “making a complaint” is “filing a grievance”
Legal
Terms What this section calls a “complaint” is also called a “grievance.”
Another term for “making a complaint” is “filing a grievance.”
Another way to say “using the process for complaints” is “using
the process for filing a grievance.”
Section 7.3 Step-by-step: Making a complaint
Step 1: Contact us promptly – either by phone or in writing.
Usually, calling OptumRx Member Services is the first step. If there is anything else
you need to do, OptumRx Member Services will let you know. Call OptumRx Member
Services at 1-866-443-1095. TTY users call 711. Calls to these numbers are free. The
OptumRx Member Service Center is available 24 hours a day, 7 days a week.
For more information about the Medicare Grievance Process, call OptumRx Member
Services.
If you do not wish to call (or you called and were not satisfied), you can put your
complaint in writing and send it to us. If you do this, it means that we will use our formal
procedure for answering grievances. Here’s how it works:
o Send your compliant in writing and mail it to us at:
OptumRx
Attn: Part D Grievances
PO Box 3410
Lisle, IL 60532-3410
Whether you call or write, you should contact OptumRx Member Services right away.
The complaint must be made within 60 days after you had the problem you want to
complain about.
If you are making a complaint because we denied your request for a “fast response”
to a coverage decision or appeal, we will automatically give you a “fast” complaint. If
you have a “fast” complaint, it means we will give you an answer within 24 hours.
Legal
Terms
What this section calls a “fast complaint” is also called a “fast
grievance.”

Chapter 7: What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
88
Step 2: We look into your complaint and give you our answer.
If possible, we will answer you right away. If you call us with a complaint, we may be
able to give you an answer on the same phone call. If your health condition requires us to
answer quickly, we will do that.
Most complaints are answered in 30 days, but we may take up to 44 days. If we need
more information and the delay is in your best interest or if you ask for more time, we can
take up to 14 more days (44 days total) to answer your complaint.
If we do not agree with some or all of your complaint or don’t take responsibility for the
problem you are complaining about, we will let you know. Our response will include our
reasons for this answer. We must respond whether we agree with the complaint or not.
Section 7.4 You can also make complaints about quality of care to the Quality
Improvement Organization
You can make your complaint about the quality of care you received to our plan by using the
step-by-step process outlined above.
When your complaint is about quality of care, you also have two extra options:
You can make your complaint to the Quality Improvement Organization. If you
prefer, you can make your complaint about the quality of care you received directly to
this organization (without making the complaint to our plan). To find the name,
address, and phone number of the Quality Improvement Organization in your state,
look in Chapter 2, Section 4, of this booklet. If you make a complaint to this
organization, we will work together with them to resolve your complaint.
Or you can make your complaint to both at the same time. If you wish, you can make
your complaint about quality of care to our plan and also to the Quality Improvement
Organization.

Chapter 8: Ending your coverage in the plan
89
Chapter 8. Ending your coverage in the plan
SECTION 1 Introduction ........................................................................................................90
Section 1.1 This chapter focuses on ending your coverage in our plan ..............................90
SECTION 2 When can you end your coverage in our plan? ...............................................90
Section 2.1 Usually, you can end your coverage during the Special Enrollment Period ...90
Section 2.2 Where can you get more information about when you can end your coverage? ...91
SECTION 3 How do you end your coverage in our plan? ...................................................91
Section 3.1 You end your coverage by enrolling in another plan .......................................91
SECTION 4 Until your coverage ends, you must keep getting your drugs through
our plan ...............................................................................................................93
Section 4.1 Until your coverage ends, you are still a participant of our plan .....................93
SECTION 5 The Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan must end your coverage in the plan in
certain situations ................................................................................................93
Section 5.1 When must we end your coverage in the plan? ...............................................93
Section 5.2 We cannot ask you to leave our plan for any reason related to your health ....94
Section 5.3 You have the right to make a complaint if we end your coverage in our plan ......94

Chapter 8: Ending your coverage in the plan
90
SECTION 1 Introduction
Section 1.1 This chapter focuses on ending your coverage in our plan
Ending your coverage in the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan may be voluntary (your own choice) or involuntary (not your own
choice):
You might leave our plan because you have decided that you want to leave.
If you are joining another Prescription Drug Plan, you must contact that Plan to request
enrollment information. Once you are enrolled in your new Plan, your membership in our Plan
will automatically end with no action required on your part. Your new Plan will tell you, in
writing, the date when your prescription drug coverage in that Plan begins. Your prescription
drug coverage with our Plan will end on that same day (this will be your “disenrollment date”).
Remember, you are still a member of our Plan until your disenrollment date, and must continue
to get your prescription drug coverage, as usual, through our Plan until the date your membership
ends.
If you wish to leave our Plan, and you are not enrolling in another Prescription Drug Plan, you
should submit a disenrollment request to HealthComp. Your request should include your name,
Medicare number, date of birth, and plan identification number. Please remember to sign and
date the request and to include a phone number where we can reach you in case we need
additional information. You can also call HealthComp.
There are also limited situations where you do not choose to leave, but we are required to
end your coverage. Section 5 tells you about situations when we must end your coverage.
If you are leaving our plan, you must continue to get your Part D prescription drugs through our
plan until your coverage ends.
SECTION 2 When can you end your coverage in our plan?
Section 2.1 Usually, you can end your coverage during the Annual Enrollment
Period or the Special Enrollment Period
Members of the Fresno City Employees Health & Welfare Trust Medicare Prescription Drug
Plan fall into a Special Enrollment Period because you are part of an Employer Group Waiver
Plan, which means you are allowed to end your membership at any time throughout the year.
What can you do? You can choose to change both your Medicare health coverage
and prescription drug coverage. This means you can choose any of the following
types of plans:
o Another Medicare prescription drug plan.

Chapter 8: Ending your coverage in the plan
91
o Original Medicare without a separate Medicare prescription drug plan.
o – or – A Medicare Advantage plan. A Medicare Advantage plan is a plan
offered by a private company that contracts with Medicare to provide all of
the Medicare Part A (Hospital) and Part B (Medical) benefits. Some Medicare
Advantage plans also include Part D prescription drug coverage.
Note: If you disenroll from a Medicare prescription drug plan and go without
creditable prescription drug coverage, you may need to pay a late enrollment
penalty if you join a Medicare drug plan later. (“Creditable” coverage means
the coverage is at least as good as Medicare’s standard prescription drug
coverage.)
When will your coverage end? Your coverage will usually end on the first day of
the month after we receive your request to change your plan.
Note: Before disenrolling from the Fresno City Employees Health & Welfare
Trust plan, you should first contact the plan you wish to enroll in and confirm that
they will accept your application. If so, and they enroll you, you will
automatically be disenrolled from the Fresno City Employees Health & Welfare
Trust plan.
Section 2.2 Where can you get more information about when you can end your
enrollment?
If you have any questions or would like more information on when you can end your enrollment:
You can call OptumRx Member Services.
You can find the information in the Medicare & You 2017 handbook.
o Everyone with Medicare receives a copy of Medicare & You each fall. Those
new to Medicare receive it within a month after first signing up.
o You can also download a copy from the Medicare website
(www.medicare.gov). Or, you can order a printed copy by calling Medicare at
the number below.
You can contact Medicare at 1-800-MEDICARE (1-800-633-4227) 24 hours a day, 7
days a week. TTY users should call 1-877-486-2048.
SECTION 3 How do you end your coverage in our plan?
Section 3.1 You end your coverage by enrolling in another plan
To end your coverage in our plan, you simply enroll in another Medicare plan. However, there
are a couple of exceptions:

Chapter 8: Ending your coverage in the plan
92
One exception is when you want to switch from our plan to Original Medicare
without a Medicare prescription drug plan. In this situation, you must contact the
Fresno City Employees Health & Welfare Trust and ask to be disenrolled from our
plan.
The table below explains how you should end your coverage in our plan.
If you would like to switch
from our plan to:
This is what you should do:
Another Medicare
prescription drug plan.
Enroll in the new Medicare prescription drug
plan.
You will automatically be disenrolled from the
Fresno City Employees Health & Welfare Trust
Medicare Prescription Drug Plan when your
new plan’s coverage begins.
A Medicare Advantage plan. Enroll in the Medicare Advantage plan.
With most Medicare Advantage plans, you will
automatically be disenrolled from the Fresno
City Employees Health & Welfare Trust
Medicare Prescription Drug Plan when your
new plan’s coverage begins.
Original Medicare without a
separate Medicare
prescription drug plan.
Contact the Fresno City Employees Health
& Welfare Trust and ask to be disenrolled
from the plan.
You can also contact Medicare at 1-800-
MEDICARE (1-800-633-4227) and ask to be
disenrolled. TTY users should call 1-877-486-
2048.

Chapter 8: Ending your coverage in the plan
93
SECTION 4 Until your coverage ends, you must keep getting your drugs
through our plan
Section 4.1 Until your coverage ends, you are still a participant of our plan
If you leave the Fresno City Employees Health & Welfare Trust Medicare Prescription Drug
Plan, it may take time before your coverage ends and your new Medicare coverage goes into
effect. During this time, you must continue to get your prescription drugs through our plan.
You should continue to use our network pharmacies to get your prescriptions filled
until your coverage in our plan ends. Usually, your prescription drugs are only covered
if they are filled at a network pharmacy including through our mail-order pharmacy
services.
SECTION 5 The Fresno City Employees Health & Welfare Trust
Medicare Prescription Drug Plan must end your coverage
in the plan in certain situations
Section 5.1 When must we end your coverage in the plan?
The Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan
must end your coverage in the plan if any of the following happen:
If you do not stay continuously enrolled in Medicare Part A and Part B.
If you move out of the United States, District of Columbia, Puerto Rico or Guam for
more than twelve months.
If you become incarcerated.
If you are no longer a United States citizen or lawfully present within the service area.
If you lie about or withhold information about other insurance you have that provides
prescription drug coverage.
If you intentionally give us incorrect information when you are enrolling in our plan and
that information affects your eligibility for our plan.
If you continuously behave in a way that is disruptive and makes it difficult for us to
provide care for you and other participants of our plan.
o We cannot make you leave our plan for this reason unless we get permission from
Medicare first.
If you let someone else use your participant ID card to get prescription drugs.
o If we end your coverage because of this reason, Medicare may have your case
investigated by the Inspector General.
If you do not pay the plan premiums.
o We must notify you in writing that you have a grace period to pay the plan
premium before we end your coverage.
If you no longer meet the Plan’s eligibility requirements.

Chapter 8: Ending your coverage in the plan
94
Where can you get more information?
You can call OptumRx Member Services if you have questions or would like more information
on when we can end your coverage.
Section 5.2 We cannot ask you to leave our plan for any reason related to your
health
What should you do if this happens?
If you feel that you are being asked to leave our plan because of a health-related reason, you
should call Medicare at 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-
486-2048. You may call 24 hours a day, 7 days a week.
Section 5.3 You have the right to make a complaint if we end your coverage in
our plan
If we end your coverage in our plan, we must tell you our reasons in writing for ending your
coverage. We must also explain how you can make a complaint about our decision to end your
coverage. You can also look in Chapter 7, Section 7 for information about how to make a
complaint.

Chapter 9: Legal notices
95
Chapter 9. Legal notices
SECTION 1 Notice about governing law ...............................................................................96
SECTION 2 Notice about nondiscrimination........................................................................96
SECTION 3 Notice about Medicare Secondary Payer subrogation rights………………96

Chapter 9: Legal notices
96
SECTION 1 Notice about governing law
Many laws apply to this Evidence of Coverage and some additional provisions may apply
because they are required by law. This may affect your rights and responsibilities even if the
laws are not included or explained in this document. The principal law that applies to this
document is Title XVIII of the Social Security Act and the regulations created under the Social
Security Act by the Centers for Medicare & Medicaid Services, or CMS. In addition, other
Federal laws may apply and, under certain circumstances, the laws of the state you live in.
SECTION 2 Notice about non-discrimination
We don’t discriminate based on a person’s race, mental of physical disability, religion, sex,
health status, claims experience, medical history, genetic information, evidence of insurability,
geographic location, ethnicity, creed, age, or national origin. All organizations that provide
Medicare Advantage Plans, like our plan, must obey Federal laws against discrimination,
including Title VI of the Civil Rights Act of 1964, the Rehabilitation Act of 1973, the Age
Discrimination Act of 1975, the Americans with Disabilities Act, Section 1557 of the Affordable
Care Act, and all other laws that apply to organizations that get Federal funding, and any other
laws and rules that apply for any other reason.
SECTION 3 Notice about Medicare Secondary Payer subrogation rights
We have the right and responsibility to collect for covered Medicare prescription drugs for which
Medicare is not the primary payer. According to CMS regulations at 42 CFR sections 422.108
and 423.462, Fresno City Employees Health & Welfare Trust, as a Medicare prescription drug
plan sponsor, will exercise the same rights of recovery that the Secretary exercises under CMS
regulations in subparts B through D of part 411 of 42 CFR and the rules established in this
section supersede any State laws.

Chapter 10: Definitions of important words
97
Chapter 10. Definitions of important words
Appeal – An appeal is something you do if you disagree with a decision to deny a request for health care
services or prescription drugs or payment for services or drugs you already received. You may also make
an appeal if you disagree with a decision to stop services that you are receiving. For example, you may
ask for an appeal if our plan doesn’t pay for a drug, item, or service you think you should be able to
receive. Chapter 7 explains appeals, including the process involved in making an appeal.
Brand Name Drug – A prescription drug that is manufactured and sold by the pharmaceutical company
that originally researched and developed the drug. Brand name drugs have the same active-ingredient
formula as the generic version of the drug. However, generic drugs are manufactured and sold by other
drug manufacturers and are generally not available until after the patent on the brand name drug has
expired.
Catastrophic Coverage Stage – The stage in the Part D Drug Benefit where you pay a low copayment or
coinsurance for your drugs after you or other qualified parties on your behalf have spent $3,400 in
covered drugs during the covered year.
Centers for Medicare & Medicaid Services (CMS) – The Federal agency that runs Medicare. Section 2
explains how to contact CMS.
Coinsurance – An amount you may be required to pay as your share of the cost for prescription drugs
Coinsurance is usually a percentage (for example, 20%).
Cost-Sharing – Cost-sharing refers to amounts that a participant has to pay when drugs are received. It
includes any combination of the following three types of payments: (1) any deductible amount a plan may
impose before drugs are covered; (2) any fixed “copayment” amount that a plan requires when a specific
drug is received; or (3) any “coinsurance” amount, a percentage of the total amount paid for a drug, that a
plan requires when a specific drug is received.
Cost–Sharing Tier – Every drug on the list of covered drugs is in one of four cost-sharing tier. In
general, the higher the cost-sharing tier, the higher your cost for the drug.
Coverage Determination – A decision about whether a drug prescribed for you is covered by the plan
and the amount, if any, you are required to pay for the prescription. In general, if you bring your
prescription to a pharmacy and the pharmacy tells you the prescription isn’t covered under your plan, that
isn’t a coverage determination. You need to call or write to your plan to ask for a formal decision about
the coverage.
Covered Drugs – The term we use to mean all of the prescription drugs covered by our plan.
Creditable Prescription Drug Coverage – Prescription drug coverage (for example, from an employer
or union) that is expected to cover, on average, at least as much as Medicare’s standard prescription drug
coverage. People who have this kind of coverage when they become eligible for Medicare can generally

Chapter 10: Definitions of important words
98
keep that coverage without paying a penalty, if they decide to enroll in Medicare prescription drug
coverage later.
Deductible – The amount you must pay for prescriptions before our plan begins to pay.
Disenroll or Disenrollment – The process of ending your membership in our plan. Disenrollment may be
voluntary (your own choice) or involuntary (not your own choice).
Evidence of Coverage (EOC) and Disclosure Information – This document, along with your
enrollment form and any other attachments, riders, or other optional coverage selected, which explains
your coverage, what we must do, your rights, and what you have to do as a participant of our plan.
Exception – A type of coverage determination that, if approved, allows you to get a drug that is not on
your plan sponsor’s formulary (a formulary exception), or get a non-preferred drug at the preferred cost-
sharing level (a tiering exception). You may also request an exception if your plan sponsor requires you to
try another drug before receiving the drug you are requesting, or the plan limits the quantity or dosage of
the drug you are requesting (a formulary exception).
Employer Group Waiver Plan (EGWP) – Medicare Part D plan that is sponsored by a former employer
union or trustees of a fund.
Extra Help/Low Income Subsidy – A Medicare program to help people with limited income and
resources pay Medicare prescription drug program costs, such as premiums, deductibles, and coinsurance.
Generic Drug – A prescription drug that is approved by the Food and Drug Administration (FDA) as
having the same active ingredient(s) as the brand name drug. Generally, generic drugs cost less than brand
name drugs.
Grievance – A type of complaint you make about us or one of our network pharmacies, including a
complaint concerning the quality of your care. This type of complaint does not involve coverage or
payment disputes.
Initial Coverage Stage – The stage where you pay a copayment or coinsurance for your drugs until your
out-of-pocket costs have reached the $3,400 limit for the calendar year.
Late Enrollment Penalty – An amount added to your monthly premium for Medicare drug coverage if
you go without creditable coverage (coverage that expects to pay, on average, at least as much as standard
Medicare prescription drug coverage) for a continuous period of 63 days or more. You pay this higher
amount as long as you have a Medicare drug plan. There are some exceptions.
List of Covered Drugs (Formulary or “Drug List”) – A list of covered drugs provided by the plan. The
drugs on this list are selected by the plan with the help of doctors and pharmacists. The list includes both
brand name and generic drugs.
Medically Necessary – Drugs that are proper and needed for the diagnosis or treatment of your medical
condition; are used for the diagnosis, direct care, and treatment of your medical condition; meet the

Chapter 10: Definitions of important words
99
standards of good medical practice in the local community; and are not mainly for your convenience or
that of your doctor.
Medicare – The Federal health insurance program for people 65 years of age or older, some people under
age 65 with certain disabilities, and people with End-Stage Renal Disease (generally those with
permanent kidney failure who need dialysis or a kidney transplant).
Medicare Advantage (MA) Plan – Sometimes called Medicare Part C. A plan offered by a private
company that contracts with Medicare to provide you with all your Medicare Part A (Hospital) and Part B
(Medical) benefits. A Medicare Advantage plan can be an HMO, PPO, a Private Fee-for-Service (PFFS)
plan, or a Medicare Medical Savings Account (MSA) plan. In most cases, Medicare Advantage Plans also
offer Medicare Part D (prescription drug coverage). These plans are called Medicare Advantage Plans
with Prescription Drug Coverage. Everyone who has Medicare Part A and Part B is eligible to join any
Medicare Health Plan that is offered in their area, except people with End-Stage Renal Disease (unless
certain exceptions apply).
Medicare Prescription Drug Coverage (Medicare Part D) – Insurance to help pay for outpatient
prescription drugs, vaccines, biologicals, and some supplies not covered by Medicare Part A or Part B.
“Medigap” (Medicare Supplement Insurance) Policy – Medicare supplement insurance sold by private
insurance companies to fill “gaps” in Original Medicare. Medigap policies only work with Original
Medicare. (A Medicare Advantage plan is not a Medigap policy.)
Network Pharmacy – A network pharmacy is a pharmacy where participants of our plan can get their
prescription drug benefits. We call them “network pharmacies” because they contract with our plan. In
most cases, your prescriptions are covered only if they are filled at one of our network pharmacies.
OptumRx Member Services – A department within our Plan responsible for answering your questions
about your enrollment, benefits, grievances, and appeals. See Chapter 2 for information about how to
contact OptumRx Member Services.
Original Medicare (“Traditional Medicare” or “Fee-for-service” Medicare) – Original Medicare is
offered by the government, and not a private health plan like Medicare Advantage plans and prescription
drug plans. Under Original Medicare, Medicare services are covered by paying doctors, hospitals, and
other health care providers payment amounts established by Congress. You can see any doctor, hospital,
or other health care provider that accepts Medicare. You must pay the deductible. Medicare pays its share
of the Medicare-approved amount, and you pay your share. Original Medicare has two parts: Part A
(Hospital Insurance) and Part B (Medical Insurance) and is available everywhere in the United States.
Out-of-Network Pharmacy – A pharmacy that doesn’t have a contract with our plan to coordinate or
provide covered drugs to participants of our plan. As explained in this Evidence of Coverage, most drugs
you get from out-of-network pharmacies are not covered by our plan unless certain conditions apply.
Out-of-Pocket Costs – See the definition for “cost-sharing” above. A participant’s cost-sharing
requirement to pay for a portion of drugs received is also referred to as the participant’s “out-of-pocket”
cost requirement.

Chapter 10: Definitions of important words
100
Part C – see “Medicare Advantage (MA) Plan”.
Part D – The voluntary Medicare Prescription Drug Benefit Program. (For ease of reference, we will
refer to the prescription drug benefit program as Part D.)
Part D Drugs – Drugs that can be covered under Part D. We may or may not offer all Part D drugs. (See
your formulary for a specific list of covered drugs.) Certain categories of drugs were specifically
excluded by Congress from being covered as Part D drugs.
Participant/Member (Participant of our Plan, or “Plan Participant”) – A person with Medicare who
is eligible to get covered services, who has enrolled in our plan and whose enrollment has been confirmed
by the Centers for Medicare & Medicaid Services (CMS).
Preferred Network Pharmacy – A network pharmacy that offers covered drugs to participants of our
plan at lower cost-sharing levels than apply at a non-preferred network pharmacy.
Premium – The periodic payment to Medicare, an insurance company, or a health care plan for health or
prescription drug coverage.
Prior Authorization – Approval in advance to get certain drugs that may or may not be on our
formulary. Some drugs are covered only if your doctor or other network provider gets “prior
authorization” from us. Covered drugs that need prior authorization are marked in the formulary.
Quality Improvement Organization (QIO) – Groups of practicing doctors and other health care experts
that are paid by the Federal government to check and improve the care given to Medicare patients. They
must review your complaints about the quality of care given by Medicare Providers. See Chapter 2,
Section 4 for information about how to contact the QIO in your state and Chapter 7 for information about
making complaints to the QIO.
Quantity Limits – A management tool that is designed to limit the use of selected drugs for quality,
safety, or utilization reasons. Limits may be on the amount of the drug that we cover per prescription or
for a defined period of time.
Service Area – “Service area” is the geographic area approved by the Centers for Medicare & Medicaid
Services (CMS) within which an eligible individual may enroll in a certain plan, and in the case of
network plans, where a network must be available to provide services.
Special Enrollment Period – A set time when members can change their health or drugs plans or return
to Original Medicare. Step Therapy – A utilization tool that requires you to first try another drug to treat
your medical condition before we will cover the drug your physician may have initially prescribed.
Supplemental Security Income (SSI) – A monthly benefit paid by the Social Security Administration to
people with limited income and resources who are disabled, blind, or age 65 and older. SSI benefits are
not the same as Social Security benefits.

Evidence of Coverage Appendix
101
State Pharmaceutical Assistance Program
State Agency Name Street Address City/State Zip Phone number
CO Colorado Bridging the Gap
4300 Cherry Creek
Drive South Denver, CO 80246
(303) 692-2783 or
(303) 692-2716
CT
Connecticut Pharmaceutical
Assistance Contract to the
Elderly and Disabled -
(ConnPACE)
P.O. Box 5011 Hartford, CT 06102 (800) 423-5026 or
(860) 269-2029
DE Delaware Prescription
Assistance Program (DPAP)
P.O. Box 950 New Castle,
DE 19720
(800) 996-9969
ext. 2
DE Delaware Chronic Renal
Disease Program
11-13 Church Ave Milford, DE 19963 (800) 464-4357 or
(302) 424-7180
ID
Idaho AIDS Drug Assistance Program (IDAGAP)
Department of
Health and Welfare
P.O. Box 83720
Boise, ID 83720 (800) 926-5943 or
(208) 334-5943
IN Hoosier Rx
402 W Washington
Street, Room W374,
MS07
Indianapolis,
IN 46206
(317) 234-1381 or
(866) 267-4679
ME Maine Low Cost Drugs for the
Elderly or Disabled Program
Office of MaineCare
Services
242 State Street
Augusta, ME 04333 (866) 796-2463
MD
Maryland Senior Prescription
Drug Assistance Program
(SPDAP)
Maryland SPDAP
c/o Pool
Administrators
628 Hebron Ave,
Suite 212
Glastonbury,
CT 06033 (800) 551-5995
MA Massachusetts Prescription
Advantage P.O. Box 15153
Worcester,
MA 01615
(800) 243-4636
Ext. 2
MO Missouri Rx Plan P.O. Box 6500 Jefferson
City, MO 65102 (800) 375-1406
MT Montana Big Sky Rx Program P.O. Box 202915 Helena, MT 59620 (866) 369-1233 or
(406) 444-1233
NV
Nevada Senior Rx Program & Nevada Disability Rx
Dept of Health and
Human Services
3416 Goni Rd, Suite
D-132
Carson City,
NV 89706
(866) 303-6323 or
(775) 687-4210
NJ
Pharmaceutical Assistance to
the Aged and Disabled
Program (PAAD), Senior Gold
Prescription Discount Program
P.O. Box 715 Trenton, NJ 08625 (800) 792-9745

Evidence of Coverage Appendix
102
State Pharmaceutical Assistance Program
NJ Division of Medical Assistance
and Health Services P.O. Box 712 Trenton, NJ 08625 (800) 356-1561
NY EPIC- Elderly Pharmaceutical
Insurance Coverage
P.O. Box 15018 Albany, NY 12212 (800) 332-3742
NC North Carolina HIV SPAP
1902 Mail Service
Center Raleigh, NC 27699
(877) 466-2232 or
(919) 733-7301
PA
PACE (Pharmaceutical
Assistance Contract for the
Elderly), PACENET
(Pennsylvania PACE Needs
Enhancement Tier)
P.O. Box 8806 Harrisburg,
PA 17105
(800) 225-7223
or
(717) 651-3600
PA
Special Pharmaceutical
Benefits Program for Mental
Health and for HIV/AIDS
P.O. Box 8021 Harrisburg,
PA 17105 (800) 922-9384
RI
Rhode Island Pharmaceutical
Assistance for the Elderly
(RIPAE)
74 West Road,
Hazard Bldg,
Second Floor
Cranston, RI 02920 (401) 462-3000 or
(401) 462-0740
TX Texas HIV State Pharmacy
Assistance Program (SPAP)
Attn: MSJA-MC
1873 P.O. Box
149347
Austin, TX 78714 (800) 255-1090
Ext. 3004
TX Texas Kidney Health Care
Program (KHC)
MC 1938 P.O. Box
149347 Austin, TX 78714
(800) 222-3986 or
(512) 776-7150
VT VPharm
312 Hurricane Lane,
Suite 201
Williston,
VT 05495
(800) 250-8427 or
(802) 879-5900
VA Virginia HIV SPAP P.O. Box 5930 Midlothin,
VA 23112 (800) 366-7741
VI
Senior Citizens Affairs
Pharmaceutical Assistance
Program
1303 Hospital
Ground Knud
Hansen Complex,
Building A
St. Thomas,
VI 00802 (340) 774-0930
WA
Washington State Health
Insurance Pharmacy
Assistance Program
P.O. Box 1090 Great Bend,
KS 67530 (800) 877-5187
WI Wisconsin SeniorCare
Program
P.O. Box 6710 Madison, WI 53716 (800) 657-2038
WI
Chronic Renal Disease, Cystic
Fibrosis Program &
Hemophilia Home Care
P.O. Box 6410 Madison, WI 53716 (800) 947-9627 or
(800) 362-3002

Evidence of Coverage Appendix
103
State Medicaid Offices State Agency Name Street Address City/State Zip Phone Number
AL Medicaid Agency of Alabama
501 Dexter
Avenue, P.O.
Box 5624
Montgomery,
AL 36103 (800) 362-1504
AK Department of Health and Social
Services
3601 C Street
Suite 902
Anchorage,
AK 99503 (907) 465-3030
AR Department of Human Services
Donaghey Plaza South P. O. Box 1437
Slot S401
Little Rock,
AR 72203 (800) 482-5431
AZ AHCCCS (Formerly Arizona
Health Care Cost Containment)
801 E. Jefferson
Street Phoenix, AZ 85034
(800) 523-0231
or
(602) 417-4000
CA Department of Health Services P.O. Box
9972732
Sacramento,
CA 94234 (916) 636-1980
CO Department of Health Care Policy
and Financing
1570 Grant
Street Denver, CO 80203 (800) 221-3943
CT Department of Social Services 25 Sigourney
Street Hartford, CT 06106 (800) 842-1508
DC Department of Health Care
Financing
441 4th
Street,
NW, 900S
Washington,
D.C. 20001 (202) 442-5988
DE Delaware Health and Social
Services
1901 N. DuPont
Highway, Lewis
Bldg.
PO Box 906
New Castle,
DE 19720 (302) 255-9500
FL Agency for Health Care
Administration
2727 Mahan
Drive
Tallahassee,
FL 32308 (888) 419-3456
GA Georgia Department of Community
Health
2 Peachtree
Street NW Atlanta, GA 30303 (404) 656-4507
HI Department of Human Services
(Med-Quest Division) P.O. Box 339 Honolulu, HI 96809 (800) 316-8005
IA Department of Human Services P.O. Box 36510 Des Moines,
IA 50315 (800) 338-8366
ID Department of Health and Welfare P.O. Box 83720 Boise, ID 83720
(208) 334-5795
ext. 4
or
(800) 378-3385
ext. 20
IL Department of Healthcare and
Family Services
201 S Grand
Avenue, East
Springfield,
IL 62763
(800) 843-6154
or
(800) 226-0768

Evidence of Coverage Appendix
104
State Medicaid Offices
IN Family and Social Services
Administration
402 W.
Washington
Street
P.O. Box 7083
Indianapolis,
IN 46207 (800) 403-0864
KS Department of Social and
Rehabilitation Services of Kansas
915 SW
Harrison Street Topeka, KS 66612 (800) 766-9012
KY Department of Medicaid Services P.O. Box 2110 Frankfort, KY 40602 (800) 635-2570
LA Department of Health and
Hospitals P.O. Box 629
Baton Rouge,
LA 70821 (888) 342-6207
MA Office of Health and Human
Services
600 Washington
Street Boston, MA 02111 (800) 841-2900
MD Department of Health and Mental
Hygiene P.O. Box 17259
Baltimore,
MD 21203 (877) 463-3464
ME Department of Health and Human
Services 221 State Street Augusta, ME 04333 (207) 287-3707
MI Department of Community Health
201 Townsend
St, Capitol
View Building
Lansing, MI 48913 (517) 373-3740
MN Department of Human Services 444 Lafayette
Road North St. Paul, MN 55155 (800) 657-3672
MO Department of Social Services
221 West High
Street, P.O. Box
1527
Jefferson
City, MO 65102 (800) 735-2466
MS Division of Medicare
239 N Lamar
Street, Robert E
Lee Bldg, Suite
801
Jackson, MS 39201 (800) 421-2408
MT Department of Public Health and
Human Services
1400 Broadway,
P.O. Box 8005 Helena, MT 59604 (800) 362-8312
NC Department of Health and Human
Services
2501 Mail
Service Center Raleigh, NC 27699 (800) 662-7030
ND Department of Human Services
600 E.
Boulevard
Avenue, Dept
325
Bismarck, ND 58505 (800) 472-2622
NE Department of Health and Human
Services P.O. Box 95026 Lincoln, NE 68509 (402) 471-3121
NH Department of Health and Human
Services 129 Pleasant St Concord, NH 03301 (800) 852-3345
NJ Department of Human Services
Quakerbridge
Plaza, Building
7, P.O. Box 712
Trenton, NJ 08625 (800) 356-1561

Evidence of Coverage Appendix
105
State Medicaid Offices
NM Medical Assistance Division/
Human Services Department P.O. Box 2348 Santa Fe, NM 87504 (888) 997-2583
NV Department of Human Resources,
Aging Division
1100 East
William Street,
Suite 101
Carson City,
NV 89701 (775) 684-0615
NY New York State Department of
Health
800 North Pearl
Street Albany, NY 12204 (518) 473-3782
OH Department of Job and Family
Services
50 West Town
Street, Suite 400
Columbus,
OH 43215 (800) 324-8680
OK Health Care Authority 4545 N Lincoln
Blvd, Suite 124
Oklahoma
City, OK 73105 (800) 522-0310
OR Department of Human Services
500 Summer
Street NE, 3rd
Floor
Salem, OR 97310 (800) 527-5772
PA Department of Public Welfare
P.O. Box 2675,
Health and
Welfare
Building, Room
515
Harrisburg,
PA 17105 (800) 692-7462
RI Department of Human Services
600 New
London
Avenue, Louis
Pasteur
Building
Cranston, RI 02921 (401) 462-5300
SC Department of Health and Human
Services P.O. Box 8206 Columbia, SC 29202 (888) 549-0820
SD Department of Social Services 700 Governors
Drive Pierre, SD 57501 (800) 597-1603
TN Bureau of TennCare 310 Great
Circle Rd. Nashville, TN 37243 (800) 342-3145
TX Health and Human Services
Commission
4900 N. Lamar
Boulevard, 4th
Fl.
Austin, TX 78701 (877) 541-7905
UT Department of Health
288 North 1460
West, P.O. Box
143101
Salt Lake
City, UT 84114 (800) 662-9651
VA Department of Medical Assistance
Services
600 East Broad
Street, Suite
1300
Richmond,
VA 23219 (804) 786-7933
VT Agency of Human Services 103 South Main
Street
Waterbury,
VT 05676 (800) 250-8427
WA Washington State Health Care
Authority P.O. Box 45502 Olympia, WA 98504 (800) 562-3022

Evidence of Coverage Appendix
106
State Medicaid Offices
WI Department of Health Services 1 West Wilson
Street Madison, WI 53703 (800) 362-3002
WV Department of Health and Human
Resources
350 Capitol
Street, Room
251
Charleston,
WV 25301 (304) 558-1700
WY Wyoming Department of Health 401 Hathaway
Building
Cheyenne,
WY 82002 (307) 777-7656
State Medical Assistance Offices
State Agency Name Toll Free Number Local Number Español
Teléfono
AL Medicaid Agency of Alabama (800) 362-1504 (334) 242-5000
AK Alaska Department of Health and Social
Services
(800) 780-9972 (907) 465-3030
AZ AHCCCS (formely Health Care Cost
Containment of Arizona)
(800) 523-0231 (602) 417-4000 (602) 417-7700
AR Department of Human Services of
Arkansas
(800) 482-5431 (501) 682-8233 (800) 482-8988
CA California Department of Health
Services
(916) 636-1980
CO Department of Health Care Policy and
Financing of Colorado
(800) 221-3943 (303) 866-3513
CT Department of Social Services of
Connecticut
(800) 842-1508 (860) 424-4908
DE Delaware Health and Social Services (800) 372-2022 (302) 255-9500
FL Florida Agency for Health Care
Administration
(866) 762-2237 (850) 487-1111
GA Georgia Department of Community
Health
(800) 869-1150 (404) 656-4507
HI Department of Human Services of
Hawaii
(800) 316-8005 (808) 524-3370 (800) 316-8005
ID Idaho Department of Health and
Welfare
(208) 334-6700
IL Illinois Department of Healthcare and
Family Services
(800) 226-0768 (217) 782-4977
IN Family and Social Services
Administration of Indiana
(800) 403-0864 (317) 233-4454
IA Department of Human Services of Iowa (800) 338-8366 (515) 256-4606
KS DCR (formely Department of Social and
Rehabilitation Services of Kansas)
(800) 766-9012 (785) 296-3981

Evidence of Coverage Appendix
107
State Medical Assistance Offices
KY Cabinet for Health Services of Kentucky (800) 635-2570 (502) 564-4321
LA Louisiana Department of Health and
Hospital
(888) 342-6207 (855) 229-6848 (877) 252-2447
ME Maine Department of Health and
Human Services
(800) 977-6740
MD Department of Health and Mental
Hygiene
(800) 456-8900 (410) 767-5800
MA Office of Health and Human Services of
Massachusetts
(800) 841-2900
MI Michigan Department Community
Health
(800) 642-3195 (517) 373-3740
MN Department of Human Services of
Minnesota - MinnesotaCare
(800) 657-3672 (651) 431-2801
MS Office of the Governor of Mississippi (800) 421-2408 (601) 359-6050
MO Department of Social Services of
Missouri - MO HealthNet Division
(800) 392-2161 (573) 751-3425
MT Montana Department of Public Health
& Human Services-Division of Child
and Adult Health Resources
(800) 362-8312
NE Nebraska Department of Health and
Human Services System
(855) 632-7633 (402) 471-3121
NV Nevada Department of Health and
Human Services Division of Welfare
and Supportive Services
(800) 992-0900 (702) 631-7098
NH New Hampshire Department of Health
and Human Services
(800) 852-3345 (603) 271-4344
NJ Department of Human Services of New
Jersey
(800) 356-1561
(800) 356-1561
NM Department of Human Services of New
Mexico
(888) 997-2583 (505) 827-3100 (800) 432-6217
NY Office of Medicaid Inspector General
(formerly New York State Department
of Health
(800) 541-2831 (518) 473-3782
NC North Carolina Department of Health
and Human Services
(800) 662-7030 (919) 855-4100
ND North Dakota Department of Human
Resources
(800) 755-2604 (701) 328-2321
OH Department of Job and Family Services
of Ohio - Ohio Health Plans
(800) 324-8680
OK Health Care Authority of Oklahoma (800) 522-0310 (405) 522-7171
OR Oregon Health Authority (800) 527-5772 (503) 945-5712

Evidence of Coverage Appendix
108
State Medical Assistance Offices
PA Department of Public Welfare of
Pennsylvania
(800) 692-7462
RI Executive Office of Health and Human
Services
(401) 462-5300
SC South Carolina Department of Health
and Human Services
(888) 549-0820 (803) 898-2500
SD Department of Social Services of South
Dakota
(800) 597-1603 (605) 773-3495 (800) 305-9673
TN Bureau of TennCare (800) 342-3145 (866) 311-4290
TX Health and Human Services
Commission of Texas (877) 541-7905 (512) 424-6500
UT Utah Department of Health (800) 662-9651 (801) 538-6155 (800) 662-9651
VT Agency of Human Services of Vermont (800) 250-8427 (802) 871-3009
VA Department of Medical Assistance
Services (804) 786-7933
WA
Health Care Authority (formerly
Department of Social and Health
Services of Washington)
(800) 562-3022
DC
DC Healthy Families and DC
HealthCare Alliance (formerly DC
Healthy Family)
(800) 620-7802 (202) 639-4030
WV West Virginia Department of Health &
Human Resources (800) 642-8589 (304) 558-1700
WI Wisconsin Department of Health
Services (800) 362-3002 (608) 266-1865
WY Wyoming Department of Health (307) 777-7656
State Health Insurance Assistance Program (SHIP)
State Agency Name Street
Address City/State Zip Phone Number
AK
State Health Insurance
Assistance Program (SHIP)
P.O. Box
110601 Juneau, AK 99811 (907) 465-3030
AL
State Health Insurance
Assistance Program (SHIP)
201 Monroe
Street, Suite
350
Montgomery,
AL 36104 (800) 243-5463
AR
Seniors Health Insurance
Information Program (SHIIP)
1200 W. Third
Street
Little Rock,
AR 72201 (800) 224-6330

Evidence of Coverage Appendix
109
State Health Insurance Assistance Program (SHIP)
AZ
Arizona State Health Insurance
Assistance Program (SHIP)
1789 W.
Jefferson,
#950A Phoenix, AZ 85007 (800) 432-4040
CA
Health Insurance Counseling &
Advocacy Program (HICAP)
3950
Industrial
Blvd., Suite
500
Sacramento,
CA 95691 (800) 434-0222
CO
Senior Health Insurance
Assistance Program (SHIP)
1560
Broadway,
Suite 850 Denver, CO 80202 (888) 696-7213
CT
Connecticut Program for Health
Insurance Assistance, Outreach,
Information & Referral
Counseling and Elig. Screening
(CHOICES)
25 Sigourney
Street Hartford, CT 06106 (800) 994-9422
DC Health Insurance Counseling
Project (HICP)
500 K Street,
NE
Washington,
DC 20002 (202) 724-5622
DE
Delaware Medicare Assistance
Bureau (DMAB) (formerly
ELDERinfo )
841 Silver
Lake
Boulevard
Dover, DE 19904 (800) 336-9500
FL SHINE (Serving Health
Insurance Needs of Elders)
4040
Esplanade
Way, Suite
270
Tallahassee,
FL 32399 (800) 963-5337
GA GeorgiaCares
2 Peachtree
St., NW, 33rd
Floor
Atlanta, GA 30303 (800) 669-8387
HI Sage PLUS 250 S. Hotel
St., Suite 406 Honolulu, HI 96813 (888) 875-9229
IA Senior Health Insurance
Information Program (SHIIP) 330 Maple St.
Des Moines,
IA 50319 (800) 351-4664
ID Senior Health Insurance
Benefits Advisors (SHIBA)
P.O. Box
83720 Boise, ID 83720 (800) 247-4422
IL Senior Health Insurance
Program (SHIP)
One Natural
Resources
Way, Suite
100
Springfield,
IL 62702 (800) 548-9034
IN State Health Insurance
Assistance Program (SHIP)
714 W. 53rd
Street Anderson, IN 46013 (800) 452-4800
KS Senior Health Insurance
Counseling for Kansas (SHICK) 503 S. Kansas Topeka, KS 66603 (800) 860-5260
KY State Health Insurance
Assistance Program (SHIP)
275 East Main
Street
Frankfort,
KY 40621 (877) 293-7447

Evidence of Coverage Appendix
110
State Health Insurance Assistance Program (SHIP)
LA Senior Health Insurance
Information Program (SHIIP)
P.O. Box
94214
Baton
Rouge, LA 70804 (800) 259-5300
MA Serving Health Information
Needs of Elders (SHINE)
One
Ashburton
Place, 5th
Floor
Boston, MA 02108 (800) 243-4636
MD Senior Health Insurance
Program
301 West
Preston Street,
Suite 1007
Baltimore,
MD 21201 (800) 243-3425
ME Maine State Health Insurance
Assistance Program
11 State
House Station,
41 Anthony
Ave.
Augusta, ME 04333 (800) 262-2232
MI Medicare/Medicaid Assistance
Program (MMAP)
6105 West St
Joe Hwy,
Suite 204
Lansing, MI 48917 (800) 803-7174
MN
Minnesota State Health
Insurance Assistance
Program/Senior LinkAge Line
540 Cedar
Street St. Paul, MN 55155 (800) 333-2433
MO Community Leaders Assisting
the Insured of MO (CLAIM)
200 N. Keene
Street
Columbia,
MO 65201 (800) 390-3330
MS MS Insurance Counseling and
Assistance Program (MICAP)
750 N. State
Street Jackson, MS 39202 (800) 948-3090
MT Montana State Health Insurance
Assistance Program (SHIP) P.O. Box 4210 Helena, MT 59604 (800) 551-3191
NC Seniors' Health Insurance
Information Program (SHIIP)
11 South
Boylan
Avenue
Raleigh, NC 27603 (800) 443-9354
ND State Health Insurance
Counseling Program (SHIC)
600 E. Blvd.
Ave.
Bismarck,
ND 58505 (888) 575-6611
NE
Nebraska Senior Health
Insurance Information Program
(SHIIP)
941 O Street,
Suite 400 Lincoln, NE 68508 (800) 234-7119
NH NH SHIP - ServiceLink
Resource Center
129 Pleasant
Street, Gallen
State Office
Park
Concord,
NH 03301 (866) 634-9412
NJ State Health Insurance
Assistance Program (SHIP) PO Box 360 Trenton, NJ 08625 (800) 792-8820

Evidence of Coverage Appendix
111
State Health Insurance Assistance Program (SHIP)
NM New Mexico ADRC/ SHIP
Benefits Counseling
2550 Cerrillos
Rd
Santa Fe,
NM 87505 (800) 432-2080
NV State Health Insurance Advisory
Program (SHIP)
1860 E. Sahara
Avenue
Las Vegas,
NV 89104 (800) 307-4444
NY
Health Insurance Information
Counseling and Assistance
Program (HIICAP)
Office for the
Aging, 2
Empire State
Plaza
Albany, NY 12223 (800) 701-0501
OH Ohio Senior Health Insurance
Information Program (OSHIIP)
50 West Town
Street, 3rd
Floor-Suite
300
Columbus,
OH 43215 (800) 686-1578
OK Senior Health Insurance
Counseling Program (SHIP)
5 Corporate
Plaza, 3625
NW 56th
Street, Suite
100
Oklahoma
City, OK 73112 (800) 763-2828
OR Senior Health Insurance Benefits
Assistance (SHIBA)
350 Winter St.
NE Salem, OR 97309 (800) 722-4134
PA APPRISE 555 Walnut
St., 5th Floor
Harrisburg,
PA 17101 (800) 783-7067
RI Senior Health Insurance
Program (SHIP)
74 West Road,
Hazard Bldg,
2nd
Floor
Cranston, RI 02920 (401) 462-0510
SC
Insurance Counseling Assistance
and Referrals for Elders (I-
CARE)
1301 Gervais
Street., Suite
350
Columbia,
SC 29201 (800) 868-9095
SD Senior Health Information and
Insurance Education (SHIINE)
700 Govenors
Drive Pierre, SD 57501 (800) 536-8197
TN TN SHIP
502 Deaderick
Street, 9th
Floor
Nashville,
TN 37243 (877) 801-0044
TX
Health Information, Counseling
and Advocacy Program
(HICAP)
701 W. 51st
Street, MC:
W352
Austin, TX 78751 (800) 252-9240
UT Health Insurance Information
Program (HIIP) 195 N 1950 W
Salt Lake
City, UT 84116 (801) 538-3910
VA Virginia Insurance Counseling
and Assistance Project (VICAP)
1610 Forest
Avenue, Suite
100
Henrico, VA 23229 (800) 552-3402
VT State Health Insurance and
Assistance Program (SHIP)
481 Summer
Street, Suite
101
St.
Johnsbury,
VT
05819 (800) 642-5119

Evidence of Coverage Appendix
112
Quality Improvement Organizations (QIO) State Agency Name Street Address City/State Zip Phone Number
AK Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (877) 588-1123
AL KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills, OH 44131 (844) 430-9504
AR KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills, OH 44131 (844) 430-9504
AZ Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (877) 588-1123
CA Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (877) 588-1123
CO KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills, OH 44131 (844) 430-9504
CT
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
DC KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
DE KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
FL KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
GA KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
State Health Insurance Assistance Program (SHIP)
WA
Statewide Health Insurance
Benefits Advisors (SHIBA)
Helpline
P.O. Box
40256
Olympia,
WA 98504 (800) 562-6900
WI State Health Insurance Program
(SHIP)
1 W. Wilson
St., Rm. 450 Madison, WI 53703 (800) 242-1060
WV
West Virginia State Health
Insurance Assistance Program
(WV SHIP)
1900 Kanawha
Blvd., East
(Mail) Town
Center Mall,
3rd
Level
Charleston,
WV 25305 (877) 987-4463
WY Wyoming State Health Insurance
Information Program (WSHIIP)
106 W. Adams
Avenue
Riverton,
WY 82501 (800) 856-4398

Evidence of Coverage Appendix
113
Quality Improvement Organizations (QIO)
HI Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (877) 588-1123
IA KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
ID Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (877) 588-1123
IL KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
IN KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
KS KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
KY KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills, OH 44131 (844) 430-9504
LA KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills, OH 44131 (844) 430-9504
MA
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
MD KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
ME
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
MI KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
MN KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
MO KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
MS KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills, OH 44131 (844) 430-9504
MT KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills, OH 44131 (844) 430-9504
NC KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708

Evidence of Coverage Appendix
114
Quality Improvement Organizations (QIO)
ND KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504
NE KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
NH
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
NJ
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
NM KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504
NV Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD
20701 (877) 588-1123
NY
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
OH KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
OK KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504
OR Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD
20701 (877) 588-1123
PA
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
RI
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
SC KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
SD KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504
TN KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504
TX KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504

Evidence of Coverage Appendix
115
Quality Improvement Organizations (QIO)
UT KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504
VA KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
VT
Livanta
BFCC_QIO
Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (866) 815-5440
WA Livanta BFCC-
QIO Program
9090 Junction Drive,
Suite 10
Annapolis
Junction, MD 20701 (877) 588-1123
WI KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (855) 408-8557
WV KEPRO 5201 W. Kennedy Blvd,
Suite 900 Tampa, FL 33609 (844) 455-8708
WY KEPRO
Rock Run Center, Suite
100, 5700 Lombardo
Center Dr.
Seven Hills,
OH 44131 (844) 430-9504

Evidence of Coverage Appendix
116

<DATE >
Dear <MEMBER NAME>,
Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan (Employer
PDP) is enrolling you in their retiree Medicare Part D prescription drug plan. Fresno City
Employees Health & Welfare Trust has contracted with OptumRx® to administer this plan to
you. If you do not want to join the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan, you must contact us within 21 days from the date of this letter to inform
us of that. If you do want to be enrolled in this Medicare Prescription Drug Plan, you don’t
have to do anything, unless we contact you for further information.
What do I need to know as a member of the Fresno City Employees Health & Welfare
Trust Medicare Prescription Drug Plan?
This mailing includes important information about the Fresno City Employees Health & Welfare
Trust Medicare Prescription Drug Plan, and you will receive more information about the
coverage it offers. Please review this information carefully. Remember, if you want to be
enrolled in this Medicare Prescription Drug Plan, you don’t have to do anything. You will
be notified when your coverage starts.
As a member of the Fresno City Employees Health & Welfare Trust Medicare Prescription Drug
Plan, you will have the right to appeal plan decisions about payment or services if you disagree.
Soon, you will receive your Evidence of Coverage in the mail, which explains the rules you must
follow to receive coverage with this Medicare Prescription Drug Plan.
The Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan is a
Medicare Part D Prescription Drug Plan and is in addition to your coverage under Medicare Part
A and Part B. Your enrollment in the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan doesn’t affect your coverage under Medicare Part A and Part B. It is
your responsibility to inform the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan of any other prescription drug coverage that you have or may get in the
future.
You can be in only one Medicare Part D Prescription Drug Plan at a time.
If you are currently enrolled in a Medicare Part D Prescription Drug Plan, other than Fresno City
Employees Health & Welfare Trust, your enrollment in the Fresno City Employees Health &
Welfare Trust Medicare Prescription Drug Plan will end that enrollment.
S8841_17_MC-DS07_FRS

If you are a member of a Medicare Advantage Plan (like an HMO or PPO), you may already
have prescription drug coverage from your Medicare Advantage Plan that will meet your needs.
By joining Fresno City Employees Health & Welfare Trust, your membership in your Medicare
Advantage Plan may end. This will affect both your doctor and hospital coverage as well as your
prescription drug coverage. Read the information that your Medicare Advantage Plan sends you
and if you have questions, contact your Medicare Advantage Plan.
If you currently have health coverage from another employer or union, joining Fresno City
Employees Health & Welfare Trust could affect your employer or union health benefits. You
could lose your employer or union health coverage if you join Fresno City Employees Health &
Welfare Trust. Read the communications your employer or union sends you. If you have
questions, visit their website, or contact the office of your benefits administrator listed in their
communications.
By joining the Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan,
you acknowledge that Fresno City Employees Health & Welfare Trust and OptumRx will release
your information to Medicare and other plans as is necessary for treatment, payment and health
care operations. You also acknowledge that Fresno City Employees Health & Welfare Trust and
OptumRx will release your information, including your prescription drug event data, to
Medicare, who may release it for research and other purposes which follow all applicable
Federal statutes and regulations.
What happens if I don’t join the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan?
You are not required to be enrolled in this plan. You can decide to join a different Medicare
drug plan. You can call 1-800-MEDICARE (1-800-633-4227) 24 hours a day, 7 days a week for
help in learning how. TTY users should call 1-877-486-2048.
What should I do if I don’t want to join the Fresno City Employees Health & Welfare
Trust Medicare Prescription Drug Plan?
To request not to be enrolled by this process, please call OptumRx Member Services at the
number below.
What if I want to leave the Fresno City Employees Health & Welfare Trust Medicare
Prescription Drug Plan?
Once you are enrolled, to request to leave or disenroll, call your benefits administrator, or call
OptumRx Member Services at the number below.
Keep in mind that if you leave our plan and don’t have other Medicare prescription drug
coverage or creditable coverage, you may have to pay a late enrollment penalty in addition
to your premium for Medicare prescription drug coverage in the future. If the coverage
from the group plan is “creditable,” it means that it has drug coverage that pays, on
average, at least as much as Medicare’s standard drug coverage.
If you have any questions, please call OptumRx Member Services at 1-866-443-1095. TTY
callers please call 711. OptumRx Member Services is available to assist you 24 hours a day, 7
days a week.

Thank you,
OptumRx
Optum Insurance of Ohio, Inc. is a Medicare approved Part D sponsor and administers this plan
through its pharmacy benefit manager, OptumRx, on behalf of your employer, union or trustees
of a fund. If you need this information in another language or other format (Braille, large print
audio), please contact OptumRx Member Services at the number located on the back of your ID
card.

Fresno City Employees
Health & Welfare Trust
Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan (Employer PDP)
2017 Summary of Benefits January 1, 2017 – December 31, 2017
Thank you for your interest in Fresno City Employees Health & Welfare Trust Medicare Prescription Drug
Plan. Our plan is administered by OptumRx®, on behalf of your employer, union or trustees of a fund. This
Summary of Benefits describes some features of our plan. It doesn’t list every drug we cover, every
limitation or exclusion. To get a complete list of our benefits please contact OptumRx Member Services and
ask for the “Evidence of Coverage”.
Please note: this prescription coverage is offered in conjunction with your medical coverage. If you choose a
different Medicare prescription drug plan other than Fresno City Employees Health & Welfare Trust
Medicare Prescription Drug Plan (Employer PDP), you will need to seek medical coverage at your own
expense.
OptumRx Member Services: Call us toll-free at 1-866-443-1095. TTY user call 711
We are available 24 hours a day, 7 days a week
For more information about Medicare, please call Medicare at 1-800-MEDICARE
(1-800-633-4227). TTY users should call 1-877-486-2048. You can call 24 hours a day, 7 days a week. Or
visit www.medicare.gov on the Web.
Optum Insurance of Ohio, Inc. is a Medicare approved Part D sponsor and administers this plan through its
pharmacy benefit manager, OptumRx, on behalf of your employer, union or trustees of a fund. If you need
this information in another language or alternate format (Braille, large print or audio), please contact
OptumRx Member Services at the number located on the back of your ID card.
S8841_17_MC-DS13

2
Where is the service area for Fresno City Employees Health & Welfare Trust Medicare Prescription
Drug Plan?
The service area for this plan includes all 50 United States, the District of Columbia, Guam and Puerto Rico.
You have choices in your Medicare prescription drug coverage.
As a Medicare beneficiary, you can choose from different Medicare prescription drug coverage options. One
option is to get prescription drug coverage through a Medicare Prescription Drug Plan, like Fresno City
Employees Health & Welfare Trust. Another option is to get your prescription drug coverage through a
Medicare Advantage Plan that offers prescription drug coverage. You make the choice.
How can I compare my options?
The charts in this booklet list some important drug benefits. You can use this Summary of Benefits to
compare the benefits offered by Fresno City Employees Health & Welfare Trust to the benefits offered by
other Medicare Prescription Drug Plans or Medicare Advantage Plans with prescription drug coverage.
Who is eligible to join?
You can join this plan as long as you are entitled to Medicare Part A and enrolled in Medicare Part B, live in
the service area, and meet any additional requirements established by Fresno City Employees Health &
Welfare Trust. If you are enrolled in a Medicare Advantage (MA) coordinated care (HMO or PPO) plan or
an MA Private Fee For Service (PFFS) plan that includes Medicare prescription drugs, you may not enroll in
a PDP unless you disenroll from the HMO, PPO or MA PFFS plan. Enrollees in a PFFS that does not
provide Medicare prescription drug coverage, an MA Medical Savings Account (MSA) plan, or an 1876
Cost Plan may enroll in a PDP.
Where can I get my prescriptions?
Fresno City Employees Health & Welfare Trust has formed a network of pharmacies. You must use a
network pharmacy to receive plan benefits. We will not pay for your prescriptions if you use an out-of-
network pharmacy, except in certain cases. This plan offers national in-network prescription coverage at over
65,000 pharmacies nationwide. This means that you will pay the same cost-sharing amount for your
prescription drugs if you get them at an in-network pharmacy outside of the plan’s service area (for instance
when you travel). However, if you choose to go to a non-participating pharmacy, you must pay for the
prescription in full and file a claim with OptumRx for reimbursement. You will be responsible for the co-
payments outlined in the co-payment table plus a penalty charge that includes the difference in the
participating pharmacy network cost and the amount the pharmacy charged.
The Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan allows you to get your
prescription(s) filled through:
1. Your local retail pharmacy
2. Home delivery
1. Local Retail Pharmacy: The Plan allows you to receive up to a 90-day supply of prescription medication
at an OptumRx participating pharmacy. Simply present your existing Fresno City Employees Health &
Welfare Trust Medicare prescription ID card along with your prescription to a participating pharmacy. If
you go to a participating pharmacy, you will pay only your co-payment/co-insurance amount.
2. Home delivery (Prescription Mail Order Service): The Fresno City Employees Health & Welfare Trust
Medicare Prescription Drug Plan offers participants an option to receive maintenance medications through

3
home delivery. Home delivery offers a convenient and cost effective way to obtain up to a 90-day supply of
maintenance medication through the mail.
Out-of-Network Coverage
You must use the OptumRx network pharmacies to fill your prescriptions. Covered Medicare Part D drugs
are available at out-of-network pharmacies only in special circumstances, such as illness while traveling
outside of the plan’s service area where there is no network pharmacy. You may incur additional costs for
drugs received at an out-of-network pharmacy. Please contact OptumRx Member Services for more
information.
Does my plan cover Medicare Part B or Part D drugs?
The Fresno City Employees Health & Welfare Trust plan does not cover drugs that are covered under
Medicare Part B as prescribed and dispensed. Generally, we only cover drugs, vaccines, biological products
and medical supplies that are covered under the Medicare Prescription Drug Benefit (Part D) and that are on
our drug list.{ }+
What is a Formulary?
Fresno City Employees Health & Welfare Trust uses a formulary. A formulary is a list of drugs covered by
your plan to meet patient needs. We may periodically add, remove, or make changes to coverage limitations
on certain drugs or change how much you pay for a drug. If we make any formulary change that limits our
members’ ability to fill their prescriptions, we will notify the affected enrollees before the change is made.
The plan may require you to first try one drug to treat your condition before it will cover another drug for
that condition. Some drugs have quantity limits. Your provider must get prior authorization from Fresno City
Employees Health & Welfare Trust for certain drugs.
If you are currently taking a drug that is not on our formulary or subject to additional requirements or limits,
you may be able to get a temporary supply of the drug. You can contact us to request an exception or switch
to an alternative drug listed on our formulary with your physician’s help. Call us to see if you can get a
temporary supply of the drug or for more details about our drug transition policy.
What should I do if I have other insurance in addition to Medicare?
If you have a Medigap (Medicare Supplement) policy that includes prescription drug coverage, you must
contact your Medigap Issuer to let them know that you have joined a Medicare Prescription Drug Plan. If
you decide to keep your current Medigap supplement policy, your Medigap Issuer will remove the
prescription drug coverage portion of your policy. Call your Medigap Issuer for details.
How can I get extra help with my prescription drug plan costs or get extra help with other Medicare
costs?
You may be able to get extra help to pay for your prescription drug premiums and costs as well as get help
with other Medicare costs. To see if you qualify for getting extra help, call:
1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048, 24 hours a day, 7
days a week and see www.medicare.gov ‘Programs for People with Limited Income and Resources’
in the publication Medicare & You.
The Social Security Administration at 1-800-772-1213 between 7 a.m. and 7 p.m., Monday through
Friday. TTY users should call 1-800-325-0778.
Your State Medicaid Office.

4
Drug Coverage Determinations
As a member Fresno City Employees Health & Welfare Trust, you have the right to request a coverage
determination, which includes the right to request an exception, the right to file an appeal if we deny
coverage for a prescription drug, and the right to file a grievance. You have the right to request a coverage
determination if you want us to cover a Part D drug that you believe should be covered. An exception is a
type of coverage determination. You may ask us for an exception if you believe you need a drug that is not
on our list of covered drugs or believe you should get a non-preferred drug at a lower out-of-pocket cost.
You can also ask for an exception to cost utilization rules, such as a limit on the quantity of a drug. If you
think you need an exception, you should contact us before you try to fill your prescription at a pharmacy.
Your doctor must provide a statement to support your exception request. If we deny coverage for your
prescription drug(s), you have the right to appeal and ask us to review our decision. Finally, you have the
right to file a grievance if you have any type of problem with us or one of our network pharmacies that does
not involve coverage for a prescription drug. If your problem involves quality of care, you also have the right
to file a grievance with the Quality Improvement Organization (QIO) for your state.
What is a Medication Therapy Management (MTM) Program? A Medication Therapy Management (MTM) Program is a free service we offer. The program can help make
sure that our members are using the drugs that work best to treat their medical conditions and help us identify
possible medication errors. We will automatically enroll you in the program you if you meet the criteria and
send you information. If you decide not to participate, please notify us and we will withdraw your
participation in the program.
Four Stages of Coverage Stage 1:
Yearly Deductible Stage
Because our plan has no deductible, this stage does not apply to you.
Stage 2:
Initial Coverage Stage
In this stage, how much you pay for a drug depends on which “tier” the
drug is in. The table on the next page shows your costs for drugs in each
of the drug tiers.
Stage 3:
Coverage Gap Stage
Because our plan has no Coverage Gap, this stage does not apply to you.
Stage 4:
Catastrophic Coverage Stage
If you have not met your member out-of-pocket maximum of $3,400, but
your yearly out-of-pocket drug costs—including manufacturer
discounts—exceed $4,950 you will pay the greater of 5% coinsurance
or:
a $3.30copayment for covered generic drugs (including brand
drugs treated as generics) with a maximum not to exceed the
standard coinsurance level during the Initial Coverage stage
a $8.25 copayment for all other covered drugs, with a maximum
not to exceed the standard coinsurance level during the Initial
Coverage stage
SUMMARY OF BENEFITS
If you have any questions about this plan’s benefits or costs, please contact OptumRx Member Services for
details.
There is no annual deductible for this plan.

5
The Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan features a four-tier
prescription benefit. Below is a chart showing the copayment amounts that you will be required to pay for
your Medicare prescription drugs.
Copayments and Coinsurance
Covered Prescription Drugs Retail Pharmacy
(up to a 34-day
supply)
Retail Pharmacy
(up to a 90-day
supply)
Mail Order
Pharmacy
(up to a 90-day
supply)
Tier 1
(Preferred Generic Drugs) 10% 10% $5
Tier 2
(Preferred Brand Drugs) 20% 20% $20
Tier 3
(Non-Preferred Brand Drugs) 40% 40% $50
Tier 4
(High-Cost Drugs*) $100 $100 $100
*High-Cost drugs are defined by the Centers for Medicare and Medicaid Services as any medication with a
cost of $600 or more for up to a 30-day supply.
NOTE: We cover some prescription drugs that are not normally covered in a Medicare Prescription Drug
Plan. The amount you pay for these drugs does not count towards your Medicare Part D initial coverage
limit or true out-of-pocket (TrOOP) costs.
Plan Specific
Once your out-of-pocket costs have reached the calendar year maximum of $3,400, the Fresno City
Employees Health & Welfare Trust Medicare Prescription Drug Plan will pay all of the cost of your drugs
until the end of the calendar year. All of the expenses that count toward the out-of-pocket maximum will be
automatically calculated.
However, if you have not met your out-of-pocket maximum of $3,400, but you have met your yearly out-of-
pocket drug costs (including manufacturer discounts) of $4,950, your share of the cost for a covered drug
will be either coinsurance or a copayment, whichever is the larger amount:
either – coinsurance of 5% of the cost of the drug
or – $3.30 copayment for a generic drug or a drug that is treated like a generic. Or a $8.25 copayment
for all other drugs.

6
English: We have free interpreter services to answer any questions you may have about our health or drug plan.
To get an interpreter, just call us at 1-866-443-1095. Someone who speaks English/Language can help you. This
is a free service.
Spanish: Tenemos servicios de intérprete sin costo alguno para responder cualquier pregunta que pueda tener
sobre nuestro plan de salud o medicamentos. Para hablar con un intérprete, por favor llame al 1-866-443-1095.
Alguien que hable español le podrá ayudar. Este es un servicio gratuito.
Chinese Mandarin: 我们提供免费的翻译服务,帮助您解答关于健康或药物保险的任何疑问。如果您需
要此翻译服务,请致电 1-866-443-1095。 我们的中文工作人员很乐意帮助您。 这是一项免费服务。
Chinese Cantonese: 您對我們的健康或藥物保險可能存有疑問,為此我們提供免費的翻譯服務。如需翻
譯服務,請致電 1-866-443-1095。我們講中文的人員將樂意為您提供幫助。這是一項免費服務。
Tagalog: Mayroon kaming libreng serbisyo sa pagsasaling-wika upang masagot ang anumang mga katanungan
ninyo hinggil sa aming planong pangkalusugan o panggamot. Upang makakuha ng tagasaling-wika, tawagan
lamang kami sa 1-866-443-1095. Maaari kayong tulungan ng isang nakakapagsalita ng Tagalog. Ito ay libreng
serbisyo.
French: Nous proposons des services gratuits d'interprétation pour répondre à toutes vos questions relatives à
notre régime de santé ou d'assurance-médicaments. Pour accéder au service d'interprétation, il vous suffit de nous
appeler au 1-866-443-1095. Un interlocuteur parlant Français pourra vous aider. Ce service est gratuit.
Vietnamese: Chúng tôi có dịch vụ thông dịch miễn phí để trả lời các câu hỏi về chương sức khỏe và chương
trình thuốc men. Nếu quí vị cần thông dịch viên xin gọi 1-866-443-1095 sẽ có nhân viên nói tiếng Việt giúp đỡ
quí vị. Đây là dịch vụ miễn phí .
German: Unser kostenloser Dolmetscherservice beantwortet Ihren Fragen zu unserem Gesundheits- und
Arzneimittelplan. Unsere Dolmetscher erreichen Sie unter 1-866-443-1095. Man wird Ihnen dort auf Deutsch
weiterhelfen. Dieser Service ist kostenlos.
Korean: 당사는 의료 보험 또는 약품 보험에 관한 질문에 답해 드리고자 무료 통역 서비스를제공하고
있습니다. 통역 서비스를 이용하려면 전화 1-866-443-1095번으로 문의해 주십시오. 한국어를 하는
담당자가 도와 드릴 것입니다. 이 서비스는 무료로 운영됩니다.
Russian: Если у вас возникнут вопросы относительно страхового или медикаментного плана, вы можете воспользоваться нашими бесплатными услугами
переводчиков. Чтобы воспользоваться услугами переводчика, позвоните нам по телефону [1-866-443-1095]. Вам окажет помощь сотрудник, который говорит по-
pусски. Данная услуга бесплатная.
Arabic: للحصول. لدينا الأدوية جدول أو بالصحة تتعلق أسئلة أي عن للإجابة المجانية الفوري المترجم خدمات نقدم إننا
العربية يتحدث ما شخص سيقوم[. 1095-443-866-1] على بنا الاتصال سوى عليك ليس فوري، مترجم على مجانية خدمة هذه. بمساعدتك .
Hindi: हमारे स्वास््य या दवा की योजना के बारे में आपके ककसी भी प्रश्न के जवाब देने के लिए हमारे पास मुफ्त
दभुाषिया सेवाए ँउपिब्ध हैं. एक दभुाषिया प्राप्त करने के लिए, बस हमें [1-866-443-1095] पर फोन करें. कोई व्यक्तत
जो हहन्दी बोिता है आपकी मदद कर सकता है. यह एक मुफ्त सेवा है.
Italian: È disponibile un servizio di interpretariato gratuito per rispondere a eventuali domande sul nostro piano
sanitario e farmaceutico. Per un interprete, contattare il numero 1-866-443-1095. Un nostro incaricato che parla
Italianovi fornirà l'assistenza necessaria. È un servizio gratuito.
Portugués: Dispomos de serviços de interpretação gratuitos para responder a qualquer questão que tenha acerca
do nosso plano de saúde ou de medicação. Para obter um intérprete, contacte-nos através do número 1-866-443-
1095. Irá encontrar alguém que fale o idioma Português para o ajudar. Este serviço é gratuito.

7
French Creole: Nou genyen sèvis entèprèt gratis pou reponn tout kesyon ou ta genyen konsènan plan medikal
oswa dwòg nou an. Pou jwenn yon entèprèt, jis rele nou nan 1-866-443-1095. Yon moun ki pale Kreyòl kapab
ede w. Sa a se yon sèvis ki gratis.
Polish: Umożliwiamy bezpłatne skorzystanie z usług tłumacza ustnego, który pomoże w uzyskaniu odpowiedzi
na temat planu zdrowotnego lub dawkowania leków. Aby skorzystać z pomocy tłumacza znającego język polski,
należy zadzwonić pod numer 1-866-443-1095. Ta usługa jest bezpłatna.
Japanese: 当社の健康 健康保険と薬品 処方薬プランに関するご質問にお答えするために、無料の通
訳サービスがありますございます。通訳をご用命になるには、1-866-443-1095にお電話ください。日本
語を話す人者 が支援いたします。これは無料のサービスです。

[CLIENT NAME] (EGWPSXXX) [CLIENT ADDRESS LINE 1] [CLIENT ADDRESS LINE 2] [CLIENT CITY] [CLIENT STATE] [CLIENT ZIP] <OptumRx Logo> %(vOD)
Welcome! Medicare has approved your enrollment in the Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan (Employer PDP), administered by OptumRx
®.
Attached is your ID card for the Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan. This card will replace your current card. Please throw your old prescription drug cards away and use the enclosed prescription drug card starting %(v23l). Remember to take this card with you when you go to the pharmacy, so they can update your information in their system. If you lose your card and need a replacement card, please contact OptumRx Member Services at the phone number below.
If you have a spouse or dependent(s) enrolled with Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan, and they are eligible for Medicare Part D, they will receive their own Fresno City Employees Health & Welfare Trust Medicare Prescription Drug Plan ID card when Medicare approves their enrollment. If you have a spouse or dependent(s) enrolled in another Plan through the Fresno City Employees Health & Welfare Trust that is not eligible for Medicare Part D, they will continue to use their existing card.
Soon, you will receive additional plan information about your prescription drug coverage. Please be on the lookout for these materials in your mailbox in the near future.
Once you have received the materials and had a chance to review them, if you have questions or need further information, please note that additional information is also available by visiting our website at optumrx.com. You may also call OptumRx Member Services toll free at 1-866-443-1095, 24 hours a day, 7 days a week. TTY users should call 711.
Thank you, OptumRx
Optum Insurance of Ohio, Inc. is a Medicare approved Part D sponsor and administers this plan through its pharmacy benefit manager, OptumRx, on behalf of your employer, union or trustees of a fund. If you need this information in another language or alternate format (Braille, large print, audio), please contact OptumRx Member Services at the number located on the back of your ID card.
S8841_17_MC-DS04_FRS [PF_EGWPSXXX-DLS1-WELCOME1-000014]

Page 1 o
This abrplan. For a coOptumRPhone: TTY usHour ofWebsite Note to make su This doc2017. Flast upd You mupharmac Optum Ipharmacthis infoMember FormulaVersionS8841_
of 121
FrMed
PL
ridged formu
omplete listinRx® Membe1-866-443-
sers call: 71f operation:e: optumrx.c
existing meure that it sti
cument incluFor a comple
dated the form
ust generallycy network,
Insurance ofcy benefit mormation in ar Services at
ary ID 1702 5 17_MC-DS1
resno Cidicare P
201
LEASE REAABO
ulary was up
ng or other qer Services 1095 1 : 24 hours a com
embers: Thll contains th
udes a partiaete, updated mulary, appe
y use networkpremium an
f Ohio, Inc. imanager, Optanother langt the number
4
10
ty Emplrescriptadmini
17 Ab(List
AD: THIS DUT THE DR
pdated on Jan
questions, pl
day, 7 days
his formularhe drugs you
al list of the dformulary, p
ears on the fr
k pharmaciend/or copaym
is a MedicartumRx, on beguage or other located on
loyees Htion Druistered b
bridgedof Cove
DOCUMENRUGS WE
nuary 1, 201
lease contact
a week
ry has changeu take.
drugs (formuplease contacfront and bac
s to use yourments/coinsu
re approved Pehalf of youer format (Brthe back of y
Health &ug Plan by Optu
d Formered Dru
NT CONTACOVER IN
17 and is not
t:
ed since last
ulary) for ouct us. Our co
ck cover pag
r prescriptiourance may c
Part D sponsr employer, raille, large pyour ID card
& Welfa(Emplo
umRx
mularugs)
AINS INFORN THIS PLA
t a complete
t year. Plea
ur plan whichontact informges.
on drug benechange on Ja
sor and admunion or truprint audio),d.
are Trusoyer PDP
ry
RMATION AN
list of drugs
ase review th
h is current amation, along
efit. Benefitanuary 1, 20
ministers this ustees of a fu, please cont
st P),
s covered by
his document
as of Januaryg with the da
ts, formulary18.
plan throughund. If you ntact OptumR
y our
t to
y 1, ate we
y,
h its need Rx

Page 2 of 121
What is the Abridged Formulary? A formulary is a list of covered drugs selected by Fresno City Employees Health & Welfare Trust in consultation with OptumRx and a team of health care providers, which represents the prescription therapies believed to be a necessary part of a quality treatment program. Fresno City Employees Health & Welfare Trust will generally cover the drugs listed in our formulary as long as the drug is medically necessary, the prescription is filled at an OptumRx network pharmacy, and other plan rules are followed. This document is a partial formulary and includes only some of the drugs covered by Fresno City Employees Health & Welfare Trust. For a complete listing of all prescription drugs covered by Fresno City Employees Health & Welfare Trust, please visit our website or call us. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages. Can the Formulary (drug list) change? Generally, if you are taking a drug on our 2017 formulary that was covered at the beginning of the year, we will not discontinue or reduce coverage of the drug during the 2017 coverage year except when a new, less expensive generic drug becomes available or when new adverse information about the safety or effectiveness of a drug is released. If we remove drugs from our formulary, or add prior authorization, quantity limits and/or step therapy restrictions on a drug or move a drug to a higher cost-sharing tier (as applicable), we must notify affected members of the change at least 60 days before the change becomes effective, or at the time the member requests a refill of the drug, at which time the member will receive a 60-day supply of the drug. If the Food and Drug Administration deems a drug on our formulary to be unsafe or the drug’s manufacturer removes the drug from the market, we will immediately remove the drug from our formulary and provide notice to members who take the drug. The enclosed formulary is current as of January 1, 2017. To get updated information about the drugs covered, please contact OptumRx Member Services. Our contact information appears on the front and back cover pages. If there is a mid-year non-maintenance formulary change (i.e. remove drugs from our formulary, add a prior authorization, quantity limits and/or step therapy restrictions on a drug, or move a drug to a higher cost-sharing tier), we will update our formulary and post it on our Website. The updated formulary may be obtained from our Website at optumrx.com or by calling OptumRx Member Services. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages. We will notify beneficiaries in writing prior to making this type of change. How do I use the Formulary? There are two ways to find your drug within the formulary: Medical Condition
The formulary begins on page 6. The drugs in this formulary are grouped into categories depending on the type of medical conditions that they are used to treat. For example, drugs used to treat a heart condition are listed under the category, “Cardiovascular Agents”. If you know what your drug is used for, look for the category name in the list that begins on page 6. Then look under the category name for your drug.

Page 3 of 121
Alphabetical Listing If you are not sure what category to look under, you should look for your drug in the Index that begins on page 101. The Index provides an alphabetical list of all of the drugs included in this document. Both brand name drugs and generic drugs are listed in the Index. Look in the Index and find your drug. Next to your drug, you will see the page number where you can find coverage information. Turn to the page listed in the Index and find the name of your drug in the first column of the list.
What are generic drugs? Our plan covers both brand name drugs and generic drugs. A generic drug is approved by the FDA as having the same active ingredient as the brand name drug. Generally, generic drugs cost less than brand name drugs.
Are there any restrictions on my coverage? Some covered drugs may have additional requirements or limits on coverage. These requirements and limits may include:
Prior Authorization: A prior authorization requires you or your physician to get prior authorization for certain drugs. This means that you will need to get approval from OptumRx before you fill your prescriptions. If you don’t get approval, the drug may not be covered.
Quantity Limits: For certain drugs, there is a limit on the amount of the drug that will be covered. Step Therapy: In some cases, it will be required that you first try certain drugs to treat your medical
condition before we will cover another drug for that condition. For example, if Drug A and Drug B both treat your medical condition, we may not cover Drug B unless you try Drug A first. If Drug A does not work for you, we will then cover Drug B.
You can find out if your drug has any additional requirements or limits by looking in the formulary that begins on page 6. You can also get more information about the restrictions applied to specific covered drugs by visiting our website. For more information, please call OptumRx Member Services. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages. You can ask OptumRx to make an exception to these restrictions or limits or for a list of other, similar drugs that may treat your health condition. See the section, “How do I request an exception to the formulary?” on page 4 for information about how to request an exception. What if my drug is not on the Formulary? If your drug is not included in this formulary (list of covered drugs), you should first contact Member Services and ask if your drug is covered. This document includes only a partial list of covered drugs, so we may cover your drug. For more information, please call OptumRx Member Services. Our contact information appears on the front and back cover pages. If you learn that your drug is not covered, you have two options:
You can ask Member Services for a list of similar drugs that are covered. When you receive the list, show it to your doctor and ask him or her to prescribe a similar drug that is covered.
You can ask OptumRx to make an exception and cover your drug. See below for information about how to request an exception.

Page 4 of 121
How do I request an exception to the Formulary? You can ask OptumRx to make an exception to our coverage rules. There are several types of exceptions that you can ask us to make.
You can ask us to cover a drug even if it is not on our formulary. If approved, this drug will be covered at a pre-determined cost-sharing level, and you would not be able to ask us to provide the drug at a lower cost-sharing level.
You can ask us to cover a formulary drug at a lower cost-sharing level if this drug is not on the specialty tier. If approved this would lower the amount you must pay for your drug.
You can ask us to waive coverage restrictions or limits on your drug. For example, for certain drugs, we may limit the amount of the drug that we will cover. If your drug has a quantity limit, you can ask us to waive the limit and cover a greater amount.
Generally, we will only approve your request for an exception if the alternative drugs included on the plan’s formulary, or additional utilization restrictions would not be as effective in treating your condition and/or would cause you to have adverse medical effects. You should contact us to ask us for an initial coverage decision for a formulary, tiering or utilization restriction exception. When you request a formulary, tiering or utilization restriction exception you should submit a statement from your prescriber or physician supporting your request. Generally, we must make our decision within 72 hours of getting your prescriber’s supporting statement. You can request an expedited (fast) exception if you or your doctor believe that your health could be seriously harmed by waiting up to 72 hours for a decision. If your request to expedite is granted, we must give you a decision no later than 24 hours after we get a supporting statement from your doctor or other prescriber. What do I do before I can talk to my doctor about changing my drugs or requesting an exception? As a new or continuing member in our plan you may be taking drugs that are not on our formulary. Or, you may be taking a drug that is on our formulary but your ability to get it is limited. For example, you may need a prior authorization from us before you can fill your prescription. You should talk to your doctor to decide if you should switch to an appropriate drug that we cover or request a formulary exception so that we will cover the drug you take. While you talk to your doctor to determine the right course of action for you, we may cover your drug in certain cases during the first 90 days you are a member of our plan. For each of your drugs that is not on our formulary or if your ability to get your drugs is limited, we will cover a temporary 30-day supply (unless you have a prescription written for fewer days) when you go to a network pharmacy. After your first 30-day supply, we will not pay for these drugs, even if you have been a member of the plan less than 90 days. If you are a resident of a long-term care facility, we will allow you to refill your prescription until we have provided you with 31-day transition supply, consistent with dispensing increment, (unless you have a prescription written for fewer days). We will cover more than one refill of these drugs for the first 90 days you are a member of our plan. If you need a drug that is not on our formulary or if your ability to get your drugs is limited, but you are past the first 90 days of membership in our plan, we will cover a 31-day emergency supply of that drug (unless you have a prescription for fewer days) while you pursue a formulary exception. If you are a current enrollee with a level of care change and you need a drug that is not on our formulary or if your ability to get your drugs is limited, we will cover a temporary 31-day transition supply (unless you have a prescription written for fewer days), while you seek to obtain a formulary exception. If you are in the process of seeking an exception, we will consider allowing continued coverage until a decision is made.

Page 5 of 121
For more information For more detailed information about your prescription drug coverage, please review your other plan materials. If you have questions about the Plan, please call OptumRx Member Services. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages. If you have general questions about Medicare prescription drug coverage, please call Medicare at 1-800-MEDICARE (1-800-633-4227) 24 hours a day/7 days a week. TTY users should call 1-877-486-2048. Or, visit www.medicare.gov. Formulary The abridged formulary below provides coverage information about some of the drugs covered. If you have trouble finding your drug in the list, turn to the Index that begins on page 101. Remember: This is only a partial list of drugs covered. If your prescription is not in this partial formulary, please contact us. Our contact information, along with the date we last updated the formulary, appears on the front cover pages. The first column of the chart lists the drug name. Brand name drugs are capitalized (e.g., ZETIA) and generic drugs are listed in lower-case italics (e.g., atenolol). The information in the Requirements/Limits column tells you if there are any special requirements for coverage of your drug.
B/D: This prescription drug has a Part B versus D administrative prior authorization requirement. This drug may be covered under Medicare Part B or D depending upon the circumstances. Information may need to be submitted describing the use and setting of the drug to make the determination.
ED: This prescription drug is not normally covered in a Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count towards your total drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In addition, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for this drug.
GC: Gap Coverage. We provide additional coverage of this prescription drug in the coverage gap. Please refer to our Evidence of Coverage for more information about this coverage.
HI: Home Infusion. This prescription drug may be covered under our medical benefit.
LA: Limited Availability. This prescription may be available only at certain pharmacies.
MO: Mail Order Drug. This prescription drug is available through a mail-order service.
PA: Prior Authorization. Our Plan requires you or your physician to get prior authorization for certain drugs. This means that you will need to get approval from OptumRx before you fill your prescriptions. If you don't get approval, your drug may not be covered.
QL: Quantity Limit. For certain drugs, our Plan limits the amount of the drug that will be covered.
ST: Step Therapy. In some cases, our Plan requires you to first try certain drugs to treat your medical condition before we will cover another drug for that condition. For example, if Drug A and Drug B both treat your medical condition, we may not cover drug B unless you try Drug A first. If Drug A does not work for you, we will then cover Drug B.

Page 6 of 121
Drug Name Drug Tier Requirements/Limits
Analgesics Nonsteroidal Anti-inflammatory Drugs
celecoxib caps 100mg 1 QL (60 EA per 30 days) celecoxib caps 200mg 1 QL (60 EA per 30 days) celecoxib caps 400mg 1 QL (60 EA per 30 days) celecoxib caps 50mg 1 QL (60 EA per 30 days) diclofenac sodium dr tbec 50mg 1 diclofenac sodium dr tbec 75mg 1 diclofenac sodium er tb24 100mg 1 diflunisal tabs 500mg 1 etodolac er tb24 400mg 1 etodolac er tb24 500mg 1 etodolac er tb24 600mg 1 etodolac caps 200mg 1 etodolac caps 300mg 1 etodolac tabs 400mg 1 etodolac tabs 500mg 1 fenoprofen calcium caps 400mg 1 fenoprofen calcium tabs 600mg 1 flurbiprofen tabs 100mg 1 flurbiprofen tabs 50mg 1 ibuprofen susp 100mg/5ml 1 ibuprofen tabs 400mg 1 ibuprofen tabs 600mg 1 ibuprofen tabs 800mg 1 indomethacin er cpcr 75mg 1 PA indomethacin caps 25mg 1 PA indomethacin caps 50mg 1 PA indomethacin inj 1mg 1 PA ketoprofen er cp24 200mg 1 ketoprofen caps 50mg 1 ketoprofen caps 75mg 1 ketorolac tromethamine inj 15mg/ml 1 PA ketorolac tromethamine inj 30mg/ml 1 PA ketorolac tromethamine inj 30mg/ml 1 PA ketorolac tromethamine inj 30mg/ml 1 PA ketorolac tromethamine tabs 10mg 1 QL (20 EA per 30 days) PA meclofenamate sodium caps 100mg 1 meclofenamate sodium caps 50mg 1 mefenamic acid caps 250mg 1 meloxicam susp 7.5mg/5ml 1 meloxicam tabs 15mg 1 meloxicam tabs 7.5mg 1 nabumetone tabs 500mg 1 nabumetone tabs 750mg 1 naproxen dr tbec 375mg 1 naproxen dr tbec 500mg 1 naproxen sodium cr tb24 375mg 1 naproxen sodium er tb24 375mg 1

Page 7 of 121
Drug Name Drug Tier Requirements/Limits
naproxen sodium er tb24 500mg 1 naproxen sodium tabs 275mg 1 naproxen sodium tabs 550mg 1 naproxen sodium tb24 500mg 1 naproxen susp 125mg/5ml 1 naproxen tabs 250mg 1 naproxen tabs 375mg 1 naproxen tabs 500mg 1 oxaprozin tabs 600mg 1 piroxicam caps 10mg 1 piroxicam caps 20mg 1 tolmetin sodium caps 400mg 1 tolmetin sodium tabs 200mg 1 tolmetin sodium tabs 600mg 1
Opioid Analgesics, Long-acting buprenorphine hcl inj 0.3mg/ml 1 buprenorphine hcl inj 0.3mg/ml 1 EMBEDA CPCR 100MG; 4MG 4 EMBEDA CPCR 20MG; 0.8MG 2 EMBEDA CPCR 30MG; 1.2MG 2 EMBEDA CPCR 50MG; 2MG 2 EMBEDA CPCR 60MG; 2.4MG 2 EMBEDA CPCR 80MG; 3.2MG 4 fentanyl pt72 100mcg/hr 1 fentanyl pt72 12mcg/hr 1 fentanyl pt72 25mcg/hr 1 fentanyl pt72 37.5mcg/hr 1 fentanyl pt72 50mcg/hr 1 fentanyl pt72 62.5mcg/hr 1 fentanyl pt72 75mcg/hr 1 fentanyl pt72 87.5mcg/hr 4 hydromorphone hcl er t24a 12mg 1 hydromorphone hcl er t24a 16mg 4 hydromorphone hcl er t24a 32mg 4 hydromorphone hcl er t24a 8mg 1 levorphanol tartrate tabs 2mg 1 methadone hcl intensol conc 10mg/ml 1 methadone hcl conc 10mg/ml 1 methadone hcl soln 10mg/5ml 1 methadone hcl soln 5mg/5ml 1 methadone hcl tabs 10mg 1 methadone hcl tabs 5mg 1 methadose sugar-free conc 10mg/ml 1 methadose conc 10mg/ml 1 morphine sulfate er cp24 100mg 4 morphine sulfate er cp24 10mg 1 morphine sulfate er cp24 120mg 1 morphine sulfate er cp24 20mg 1 morphine sulfate er cp24 30mg 1

Page 8 of 121
Drug Name Drug Tier Requirements/Limits
morphine sulfate er cp24 30mg 1 morphine sulfate er cp24 45mg 1 morphine sulfate er cp24 50mg 1 morphine sulfate er cp24 60mg 1 morphine sulfate er cp24 60mg 1 morphine sulfate er cp24 75mg 1 morphine sulfate er cp24 80mg 1 morphine sulfate er cp24 90mg 1 morphine sulfate er tbcr 100mg 1 morphine sulfate er tbcr 15mg 1 morphine sulfate er tbcr 200mg 1 morphine sulfate er tbcr 30mg 1 morphine sulfate er tbcr 60mg 1 OPANA ER (CRUSH RESISTANT) T12A 10MG 2 OPANA ER (CRUSH RESISTANT) T12A 15MG 2 OPANA ER (CRUSH RESISTANT) T12A 20MG 2 OPANA ER (CRUSH RESISTANT) T12A 30MG 4 OPANA ER (CRUSH RESISTANT) T12A 40MG 4 OPANA ER (CRUSH RESISTANT) T12A 5MG 2 OPANA ER (CRUSH RESISTANT) T12A 7.5MG 2 oxycodone hcl er t12a 10mg 1 oxycodone hcl er t12a 15mg 1 oxycodone hcl er t12a 20mg 1 oxycodone hcl er t12a 30mg 1 oxycodone hcl er t12a 40mg 1 oxycodone hcl er t12a 60mg 1 oxycodone hcl er t12a 80mg 4 oxymorphone hydrochloride er tb12 10mg 1 oxymorphone hydrochloride er tb12 15mg 1 oxymorphone hydrochloride er tb12 20mg 1 oxymorphone hydrochloride er tb12 30mg 1 oxymorphone hydrochloride er tb12 40mg 1 oxymorphone hydrochloride er tb12 5mg 1 oxymorphone hydrochloride er tb12 7.5mg 1 tramadol hcl er tb24 100mg 1 tramadol hcl er tb24 100mg 1 tramadol hcl er tb24 200mg 1 tramadol hcl er tb24 200mg 1 tramadol hcl er tb24 300mg 1 tramadol hcl er tb24 300mg 1
Opioid Analgesics, Short-acting ABSTRAL SUBL 100MCG 4 PA ABSTRAL SUBL 200MCG 4 PA ABSTRAL SUBL 300MCG 4 PA ABSTRAL SUBL 400MCG 4 PA ABSTRAL SUBL 600MCG 4 PA ABSTRAL SUBL 800MCG 4 PA acetaminophen/codeine #3 tabs 300mg; 30mg 1 acetaminophen/codeine soln 120mg/5ml; 12mg/5ml 1

Page 9 of 121
Drug Name Drug Tier Requirements/Limits
acetaminophen/codeine tabs 300mg; 15mg 1 acetaminophen/codeine tabs 300mg; 60mg 1 ACTIQ LPOP 1200MCG 4 PA ACTIQ LPOP 1600MCG 4 PA ACTIQ LPOP 600MCG 4 PA ACTIQ LPOP 800MCG 4 PA ascomp/codeine caps 325mg; 50mg; 40mg; 30mg 1 PA aspirin-caffeine-dihydrocodeine caps 356.4mg; 30mg; 16mg 1 butalbital/aspirin/caffeine/codeine caps 325mg; 50mg; 40mg; 30mg
1 PA
butorphanol tartrate inj 1mg/ml 1 butorphanol tartrate inj 2mg/ml 1 butorphanol tartrate soln 10mg/ml 1 codeine sulfate tabs 15mg 1 codeine sulfate tabs 30mg 1 codeine sulfate tabs 60mg 1 duramorph inj 0.5mg/ml 1 duramorph inj 1mg/ml 1 endocet tabs 325mg; 10mg 1 endocet tabs 325mg; 2.5mg 1 endocet tabs 325mg; 5mg 1 endocet tabs 325mg; 7.5mg 1 fentanyl citrate oral transmucosal lpop 1200mcg 4 PA fentanyl citrate oral transmucosal lpop 1600mcg 4 PA fentanyl citrate oral transmucosal lpop 200mcg 1 PA fentanyl citrate oral transmucosal lpop 400mcg 1 PA fentanyl citrate oral transmucosal lpop 600mcg 4 PA fentanyl citrate oral transmucosal lpop 800mcg 4 PA fentanyl citrate inj 1000mcg/20ml 1 B/D fentanyl citrate inj 100mcg/2ml 1 B/D fentanyl citrate inj 2500mcg/50ml 1 B/D fentanyl citrate inj 250mcg/5ml 1 B/D fentanyl citrate inj 500mcg/10ml 1 B/D FENTORA TABS 100MCG 4 PA FENTORA TABS 200MCG 4 PA FENTORA TABS 400MCG 4 PA FENTORA TABS 600MCG 4 PA FENTORA TABS 800MCG 4 PA hydrocodone bitartrate/acetaminophen soln 325mg/15ml; 7.5mg/15ml
1
hydrocodone bitartrate/acetaminophen tabs 300mg; 10mg 1 hydrocodone bitartrate/acetaminophen tabs 300mg; 5mg 1 hydrocodone bitartrate/acetaminophen tabs 300mg; 7.5mg 1 hydrocodone bitartrate/acetaminophen tabs 325mg; 2.5mg 1 hydrocodone/acetaminophen soln 500mg/15ml; 7.5mg/15ml 1 hydrocodone/acetaminophen tabs 325mg; 10mg 1 hydrocodone/acetaminophen tabs 325mg; 5mg 1 hydrocodone/acetaminophen tabs 325mg; 7.5mg 1 hydrocodone/ibuprofen tabs 10mg; 200mg 1

Page 10 of 121
Drug Name Drug Tier Requirements/Limits
hydrocodone/ibuprofen tabs 2.5mg; 200mg 1 hydrocodone/ibuprofen tabs 5mg; 200mg 1 hydrocodone/ibuprofen tabs 7.5mg; 200mg 1 hydromorphone hcl inj 10mg/ml 1 hydromorphone hcl inj 1mg/ml 1 hydromorphone hcl inj 2mg/ml 1 hydromorphone hcl inj 4mg/ml 1 hydromorphone hcl inj 50mg/5ml 1 hydromorphone hcl liqd 1mg/ml 1 hydromorphone hcl tabs 2mg 1 hydromorphone hcl tabs 4mg 1 hydromorphone hcl tabs 8mg 1 ibudone tabs 5mg; 200mg 1 LAZANDA SOLN 100MCG/ACT 4 PA LAZANDA SOLN 300MCG/ACT 4 PA LAZANDA SOLN 400MCG/ACT 4 PA lorcet plus tabs 325mg; 7.5mg 1 lorcet tabs 325mg; 5mg 1 lortab tabs 325mg; 10mg 1 lortab tabs 325mg; 5mg 1 lortab tabs 325mg; 7.5mg 1 morphine sulfate inj 0.5mg/ml 1 morphine sulfate inj 10mg/ml 1 morphine sulfate inj 150mg/30ml 1 B/D morphine sulfate inj 15mg/ml 1 morphine sulfate inj 1mg/ml 1 morphine sulfate inj 1mg/ml 1 B/D morphine sulfate inj 2mg/ml 1 morphine sulfate inj 4mg/ml 1 morphine sulfate inj 8mg/ml 1 morphine sulfate soln 100mg/5ml 1 morphine sulfate soln 10mg/5ml 1 morphine sulfate soln 20mg/5ml 1 morphine sulfate tabs 15mg 1 morphine sulfate tabs 30mg 1 nalbuphine hcl inj 10mg/ml 1 nalbuphine hcl inj 20mg/ml 1 opium tincture tinc 1% 1 opium tinc 1% 1 oxycodone hcl caps 5mg 1 oxycodone hcl conc 100mg/5ml 1 oxycodone hcl soln 5mg/5ml 1 oxycodone hcl tabs 10mg 1 oxycodone hcl tabs 15mg 1 oxycodone hcl tabs 20mg 1 oxycodone hcl tabs 30mg 1 oxycodone hcl tabs 5mg 1 oxycodone/acetaminophen soln 325mg/5ml; 5mg/5ml 1 oxycodone/acetaminophen tabs 325mg; 10mg 1

Page 11 of 121
Drug Name Drug Tier Requirements/Limits
oxycodone/acetaminophen tabs 325mg; 2.5mg 1 oxycodone/acetaminophen tabs 325mg; 5mg 1 oxycodone/acetaminophen tabs 325mg; 7.5mg 1 oxycodone/aspirin tabs 325mg; 4.835mg 1 oxycodone/ibuprofen tabs 400mg; 5mg 1 oxymorphone hydrochloride tabs 10mg 1 oxymorphone hydrochloride tabs 5mg 1 pentazocine/naloxone hcl tabs 0.5mg; 50mg 1 PA reprexain tabs 10mg; 200mg 1 SUBSYS LIQD 100MCG 4 PA SUBSYS LIQD 1200MCG 4 PA SUBSYS LIQD 1600MCG 4 PA SUBSYS LIQD 200MCG 4 PA SUBSYS LIQD 400MCG 4 PA SUBSYS LIQD 600MCG 4 PA SUBSYS LIQD 800MCG 4 PA tramadol hcl tabs 50mg 1 tramadol hydrochloride/acetaminophen tabs 325mg; 37.5mg 1 vicodin es tabs 300mg; 7.5mg 1 vicodin hp tabs 300mg; 10mg 1 vicodin tabs 300mg; 5mg 1 xylon tabs 10mg; 200mg 1
Anesthetics Local Anesthetics
glydo gel 2% 1 lidocaine hcl jelly gel 2% 1 lidocaine hcl jelly gel 2% 1 lidocaine hcl jelly gel 2% 1 lidocaine hcl/dextrose inj 7.5%; 5% 1 lidocaine hcl gel 2% 1 lidocaine hcl inj 0.5% 1 lidocaine hcl inj 0.5% 1 lidocaine hcl inj 1% 1 lidocaine hcl inj 1% 1 lidocaine hcl inj 1.5% 1 lidocaine hcl inj 2% 1 lidocaine hcl inj 2% 1 lidocaine hcl inj 2% 1 lidocaine hcl inj 4% 1 lidocaine hcl soln 4% 1 lidocaine hcl soln 4% 1 lidocaine viscous soln 2% 1 lidocaine/epinephrine inj 1:100000; 1% 1 lidocaine/epinephrine inj 1:100000; 2% 1 lidocaine/epinephrine inj 1:200000; 0.5% 1 lidocaine/epinephrine inj 1:200000; 1.5% 1 lidocaine/epinephrine inj 1:200000; 2% 1 lidocaine/epinephrine inj 1:50000; 2% 1 lidocaine/prilocaine crea 2.5%; 2.5% 1

Page 12 of 121
Drug Name Drug Tier Requirements/Limits
lidocaine/prilocaine kit 2.5%; 2.5% 1 lidocaine oint 5% 1 lidocaine ptch 5% 1 PA relador pak plus kit 2.5%; 2.5% 1 relador pak kit 2.5%; 2.5% 1 xylocaine dental inj 1:100000; 2% 1 xylocaine dental inj 1:50000; 2% 1
Anti-Addiction/Substance Abuse Treatment Agents Alcohol Deterrents/Anti-craving
acamprosate calcium dr tbec 333mg 1 disulfiram tabs 250mg 1 disulfiram tabs 500mg 1 VIVITROL INJ 380MG 4 PA
Opioid Dependence Treatments buprenorphine hcl/naloxone hcl subl 2mg; 0.5mg 1 QL (360 EA per 30 days) PA buprenorphine hcl/naloxone hcl subl 8mg; 2mg 1 QL (90 EA per 30 days) PA buprenorphine hcl subl 2mg 1 PA buprenorphine hcl subl 8mg 1 PA naltrexone hcl tabs 50mg 1
Opioid Reversal Agents naloxone hcl inj 0.4mg/ml 1 naloxone hcl inj 2mg/2ml 1
Smoking Cessation Agents buproban tb12 150mg 1 QL (60 EA per 30 days) bupropion hcl sr tb12 150mg 1 QL (60 EA per 30 days) NICOTROL NS SOLN 10MG/ML 2 QL (360 ML per 365 days)
Anti-inflammatory Agents Nonsteroidal Anti-inflammatory Drugs
diclofenac sodium gel 3% 4 sulindac tabs 150mg 1 sulindac tabs 200mg 1
Antibacterials Aminoglycosides
amikacin sulfate inj 1gm/4ml 1 amikacin sulfate inj 500mg/2ml 1 gentak oint 0.3% 1 gentamicin sulfate pediatric inj 10mg/ml 1 gentamicin sulfate/0.9% sodium chloride inj 0.8mg/ml; 0.9% 1 gentamicin sulfate/0.9% sodium chloride inj 0.9mg/ml; 0.9% 1 gentamicin sulfate/0.9% sodium chloride inj 1.2mg/ml; 0.9% 1 gentamicin sulfate/0.9% sodium chloride inj 1.4mg/ml; 0.9% 1 gentamicin sulfate/0.9% sodium chloride inj 1.6mg/ml; 0.9% 1 gentamicin sulfate/0.9% sodium chloride inj 1mg/ml; 0.9% 1 gentamicin sulfate/0.9% sodium chloride inj 2mg/ml; 0.9% 1 gentamicin sulfate crea 0.1% 1 gentamicin sulfate inj 10mg/ml 1 gentamicin sulfate inj 40mg/ml 1 gentamicin sulfate oint 0.1% 1 gentamicin sulfate oint 0.3% 1

Page 13 of 121
Drug Name Drug Tier Requirements/Limits
gentamicin sulfate soln 0.3% 1 isotonic gentamicin inj 0.8mg/ml; 0.9% 1 neomycin sulfate tabs 500mg 1 neomycin/polymyxin b sulfates soln 40mg/ml; 200000unit/ml 1 paromomycin sulfate caps 250mg 1 streptomycin sulfate inj 1gm 1 tobramycin sulfate inj 1.2gm 1 tobramycin sulfate inj 10mg/ml 1 tobramycin sulfate inj 40mg/ml 1 tobramycin sulfate inj 80mg/2ml 1 tobramycin sulfate soln 0.3% 1
Antibacterials, Other ALCOHOL PREP PADS PADS 70% 2 baciim inj 50000unit 1 bacitracin inj 50000unit 1 bacitracin oint 500unit/gm 1 chloramphenicol sodium succinate inj 1gm 1 clin single use kit inj 300mg/2ml 1 clindacin etz pledgets swab 1% 1 clindacin etz kit 0; 1%; 0 1 clindacin pac kit 0; 1% 1 clindacin-p swab 1% 1 clindamax gel 1% 1 clindamycin hcl caps 150mg 1 clindamycin hcl caps 300mg 1 clindamycin hcl caps 75mg 1 clindamycin palmitate hcl solr 75mg/5ml 1 clindamycin phosphate add-vantage inj 150mg/ml 1 clindamycin phosphate add-vantage inj 900mg/6ml 1 clindamycin phosphate in d5w inj 300mg/50ml; 5% 1 clindamycin phosphate in d5w inj 600mg/50ml; 5% 1 clindamycin phosphate in d5w inj 900mg/50ml; 5% 1 clindamycin phosphate pharmacy bulk package inj 150mg/ml 1 clindamycin phosphate crea 2% 1 clindamycin phosphate foam 1% 1 clindamycin phosphate gel 1% 1 clindamycin phosphate inj 150mg/ml 1 clindamycin phosphate inj 300mg/2ml 1 clindamycin phosphate inj 600mg/4ml 1 clindamycin phosphate inj 9000mg/60ml 1 clindamycin phosphate inj 900mg/6ml 1 clindamycin phosphate lotn 1% 1 clindamycin phosphate soln 1% 1 clindamycin phosphate swab 1% 1 clindamycin inj 900mg/6ml 1 colistimethate sodium inj 150mg 1 CUBICIN INJ 500MG 4 DALVANCE INJ 500MG 4 lincomycin hcl inj 300mg/ml 1

Page 14 of 121
Drug Name Drug Tier Requirements/Limits
linezolid inj 600mg/300ml 1 linezolid susr 100mg/5ml 4 QL (1800 ML per 30 days) linezolid tabs 600mg 4 QL (28 EA per 30 days) mafenide acetate pack 5% 1 methenamine hippurate tabs 1gm 1 metro iv inj 500mg/100ml; 0.74% 1 metronidazole in nacl 0.79% inj 500mg/100ml; 0.79% 1 metronidazole vaginal gel 0.75% 1 metronidazole caps 375mg 1 metronidazole crea 0.75% 1 metronidazole gel 0.75% 1 metronidazole gel 1% 1 metronidazole lotn 0.75% 1 metronidazole tabs 250mg 1 metronidazole tabs 500mg 1 mupirocin calcium crea 2% 1 mupirocin crea 2% 1 mupirocin oint 2% 1 neo-polycin hc oint 400unit/gm; 1%; 3.5mg/gm; 10000unit/gm1 neomycin/polymyxin/bacitracin/hydrocortisone oint 400unit/gm; 1%; 0.5%; 10000unit/gm
1
neomycin/polymyxin/hydrocortisone susp 1%; 3.5mg/ml; 10000unit/ml
1
nitrofurantoin macrocrystals caps 100mg 1 QL (360 EA per 365 days) nitrofurantoin macrocrystals caps 25mg 1 QL (1440 EA per 365 days) nitrofurantoin macrocrystals caps 50mg 1 QL (720 EA per 365 days) nitrofurantoin monohydrate/macrocrystals caps 100mg 1 QL (180 EA per 365 days) nitrofurantoin monohydrate caps 100mg 1 QL (180 EA per 365 days) nitrofurantoin susp 25mg/5ml 1 QL (7200 ML per 365 days) NORITATE CREA 1% 4 ORBACTIV INJ 400MG 4 polymyxin b sulfate inj 500000unit 1 rosadan kit kit 0.75% 1 rosadan kit kit 0.75% 1 rosadan crea 0.75% 1 rosadan gel 0.75% 1 silver sulfadiazine crea 1% 1 SIVEXTRO INJ 200MG 4 QL (6 EA per 30 days) SIVEXTRO TABS 200MG 4 QL (6 EA per 30 days) ssd crea 1% 1 SYNERCID INJ 350MG; 150MG 4 trimethoprim tabs 100mg 1 TYGACIL INJ 50MG 4 vancomycin hcl in dextrose inj 0; 1gm/200ml 1 vancomycin hcl in dextrose inj 0; 500mg/100ml 1 vancomycin hcl in dextrose inj 0; 750mg/150ml 1 vancomycin hcl caps 125mg 1 vancomycin hcl caps 250mg 1 vancomycin hcl inj 1000mg 1

Page 15 of 121
Drug Name Drug Tier Requirements/Limits
vancomycin hcl inj 10gm 1 vancomycin hcl inj 5000mg 1 vancomycin hcl inj 500mg 1 vancomycin hcl inj 750mg 1 vandazole gel 0.75% 1 XIFAXAN TABS 200MG 4 PA XIFAXAN TABS 550MG 4 PA ZYVOX SUSR 100MG/5ML 4 QL (1800 ML per 30 days) ZYVOX TABS 600MG 4 QL (28 EA per 30 days)
Beta-lactam, Cephalosporins AVYCAZ INJ 0.5GM; 2GM 4 cefadroxil caps 500mg 1 cefadroxil susr 250mg/5ml 1 cefadroxil susr 500mg/5ml 1 cefadroxil tabs 1gm 1 cefazolin sodium/dextrose inj 1gm; 4% 1 cefazolin sodium/dextrose inj 2gm; 3% 1 cefazolin sodium inj 100gm 1 cefazolin sodium inj 10gm 1 cefazolin sodium inj 1gm 1 cefazolin sodium inj 1gm 1 cefazolin sodium inj 1gm; 5% 1 cefazolin sodium inj 20gm 1 cefazolin sodium inj 300gm 1 cefazolin sodium inj 500mg 1 cefazolin inj 2gm/100ml; 4% 1 cefdinir caps 300mg 1 cefdinir susr 125mg/5ml 1 cefdinir susr 250mg/5ml 1 cefepime/dextrose inj 1gm/50ml; 5% 1 cefepime inj 1gm/50ml 1 cefepime inj 1gm 1 cefepime inj 2gm/100ml 1 cefepime inj 2gm/50ml; 5% 1 cefepime inj 2gm 1 cefixime susr 100mg/5ml 1 cefixime susr 200mg/5ml 1 cefotaxime sodium inj 10gm 1 cefotaxime sodium inj 1gm 1 cefotaxime sodium inj 2gm 1 cefotaxime sodium inj 500mg 1 cefotetan/dextrose inj 1gm; 3.58% 1 cefotetan/dextrose inj 2gm; 2.08% 1 cefoxitin sodium inj 10gm 1 cefoxitin sodium inj 1gm 1 cefoxitin sodium inj 1gm; 4% 1 cefoxitin sodium inj 2gm 1 cefoxitin sodium inj 2gm; 2.2% 1 cefpodoxime proxetil susr 100mg/5ml 1

Page 16 of 121
Drug Name Drug Tier Requirements/Limits
cefpodoxime proxetil susr 50mg/5ml 1 cefpodoxime proxetil tabs 100mg 1 cefpodoxime proxetil tabs 200mg 1 cefprozil susr 125mg/5ml 1 cefprozil susr 250mg/5ml 1 cefprozil tabs 250mg 1 cefprozil tabs 500mg 1 ceftazidime/dextrose inj 1gm/50ml; 5% 1 ceftazidime/dextrose inj 2gm/50ml; 5% 1 ceftazidime inj 1gm 1 ceftazidime inj 2gm 1 ceftazidime inj 6gm 1 ceftibuten caps 400mg 1 ceftriaxone in iso-osmotic dextrose inj 20mg/ml; 0 1 ceftriaxone in iso-osmotic dextrose inj 40mg/ml; 0 1 ceftriaxone sodium inj 100gm 1 ceftriaxone sodium inj 10gm 1 ceftriaxone sodium inj 1gm 1 ceftriaxone sodium inj 1gm 1 ceftriaxone sodium inj 250mg 1 ceftriaxone sodium inj 2gm 1 ceftriaxone sodium inj 2gm 1 ceftriaxone sodium inj 500mg 1 ceftriaxone/dextrose inj 1gm; 3.74% 1 ceftriaxone/dextrose inj 2gm; 2.22% 1 cefuroxime axetil tabs 250mg 1 cefuroxime axetil tabs 500mg 1 cefuroxime sodium inj 1.5gm 1 cefuroxime sodium inj 1.5gm 1 cefuroxime sodium inj 225gm 1 cefuroxime sodium inj 7.5gm 1 cefuroxime sodium inj 750mg 1 cefuroxime sodium inj 75gm 1 cephalexin caps 250mg 1 cephalexin caps 500mg 1 cephalexin caps 750mg 1 cephalexin susr 125mg/5ml 1 cephalexin susr 250mg/5ml 1 cephalexin tabs 250mg 1 cephalexin tabs 500mg 1 SUPRAX CAPS 400MG 2 SUPRAX CHEW 100MG 2 SUPRAX CHEW 200MG 2 SUPRAX SUSR 500MG/5ML 2 tazicef inj 1gm 1 tazicef inj 1gm 1 tazicef inj 2gm 1 tazicef inj 2gm 1 tazicef inj 6gm 1

Page 17 of 121
Drug Name Drug Tier Requirements/Limits
TEFLARO INJ 400MG 4 TEFLARO INJ 600MG 4 zinacef inj 1.5gm 1 zinacef inj 1.5gm 1 zinacef inj 1.5gm; 0 1 zinacef inj 750mg 1 zinacef inj 750mg 1
Beta-lactam, Other aztreonam inj 1gm 1 aztreonam inj 2gm 1 cefotetan inj 10gm 1 cefotetan inj 1gm 1 cefotetan inj 2gm 1 imipenem/cilastatin inj 250mg; 250mg 1 imipenem/cilastatin inj 500mg; 500mg 1 meropenem/sodium chloride inj 1gm/50ml; 0.9% 1 meropenem/sodium chloride inj 500mg/50ml; 0.9% 1 meropenem inj 1gm 1 meropenem inj 500mg 1
Beta-lactam, Penicillins amoxicillin/clavulanate potassium er tb12 1000mg; 62.5mg 1 amoxicillin/clavulanate potassium chew 200mg; 28.5mg 1 amoxicillin/clavulanate potassium chew 400mg; 57mg 1 amoxicillin/clavulanate potassium susr 200mg/5ml; 28.5mg/5ml
1
amoxicillin/clavulanate potassium susr 250mg/5ml; 62.5mg/5ml
1
amoxicillin/clavulanate potassium susr 400mg/5ml; 57mg/5ml 1 amoxicillin/clavulanate potassium susr 600mg/5ml; 42.9mg/5ml
1
amoxicillin/clavulanate potassium tabs 250mg; 125mg 1 amoxicillin/clavulanate potassium tabs 500mg; 125mg 1 amoxicillin/clavulanate potassium tabs 875mg; 125mg 1 amoxicillin caps 250mg 1 amoxicillin caps 500mg 1 amoxicillin chew 125mg 1 amoxicillin chew 250mg 1 amoxicillin susr 125mg/5ml 1 amoxicillin susr 200mg/5ml 1 amoxicillin susr 250mg/5ml 1 amoxicillin susr 400mg/5ml 1 amoxicillin tabs 500mg 1 amoxicillin tabs 875mg 1 ampicillin sodium inj 10gm 1 ampicillin sodium inj 10gm 1 ampicillin sodium inj 125mg 1 ampicillin sodium inj 1gm 1 ampicillin sodium inj 1gm 1 ampicillin sodium inj 250mg 1

Page 18 of 121
Drug Name Drug Tier Requirements/Limits
ampicillin sodium inj 2gm 1 ampicillin sodium inj 2gm 1 ampicillin sodium inj 500mg 1 ampicillin-sulbactam inj 10gm; 5gm 1 ampicillin-sulbactam inj 10gm; 5gm 1 ampicillin-sulbactam inj 1gm; 0.5gm 1 ampicillin-sulbactam inj 1gm; 0.5gm 1 ampicillin-sulbactam inj 2gm; 1gm 1 ampicillin caps 250mg 1 ampicillin caps 500mg 1 ampicillin susr 125mg/5ml 1 ampicillin susr 250mg/5ml 1 dicloxacillin sodium caps 250mg 1 dicloxacillin sodium caps 500mg 1 nafcillin sodium inj 10gm 1 nafcillin sodium inj 1gm 1 nafcillin sodium inj 1gm 1 nafcillin sodium inj 2gm 1 nafcillin sodium inj 2gm 1 nafcillin inj 0; 1gm/50ml 1 nafcillin inj 0; 2gm/100ml 1 oxacillin sodium inj 10gm 4 oxacillin sodium inj 1gm 1 oxacillin sodium inj 2gm 1 penicillin g potassium in iso-osmotic dextrose inj 0; 20000unit/ml
1
penicillin g potassium in iso-osmotic dextrose inj 0; 40000unit/ml
1
penicillin g potassium in iso-osmotic dextrose inj 0; 60000unit/ml
1
penicillin g potassium inj 20000000unit 1 penicillin g potassium inj 5000000unit 1 penicillin g sodium inj 5000000unit 1 penicillin v potassium solr 125mg/5ml 1 penicillin v potassium solr 250mg/5ml 1 penicillin v potassium tabs 250mg 1 penicillin v potassium tabs 500mg 1 pfizerpen-g inj 20mu 1 pfizerpen-g inj 5000000unit 1 piperacillin sodium/ tazobactam sodium inj 36gm; 4.5gm 1 piperacillin sodium/tazobactam sodium inj 2gm; 0.25gm 1 piperacillin sodium/tazobactam sodium inj 3gm; 0.375gm 1 piperacillin/tazobactam inj 2gm; 0.25gm 1 piperacillin/tazobactam inj 36gm; 4.5gm 1 piperacillin/tazobactam inj 4gm; 0.5gm 1
Macrolides azithromycin inj 500mg 1 azithromycin pack 1gm 1 azithromycin susr 100mg/5ml 1

Page 19 of 121
Drug Name Drug Tier Requirements/Limits
azithromycin susr 200mg/5ml 1 azithromycin tabs 250mg 1 azithromycin tabs 250mg 1 azithromycin tabs 500mg 1 azithromycin tabs 600mg 1 clarithromycin er tb24 500mg 1 clarithromycin susr 125mg/5ml 1 clarithromycin susr 250mg/5ml 1 clarithromycin tabs 250mg 1 clarithromycin tabs 500mg 1 DIFICID TABS 200MG 4 ERY-TAB TBEC 250MG 2 ERY-TAB TBEC 333MG 2 ERY-TAB TBEC 500MG 2 ery pads 2% 1 erythrocin lactobionate inj 500mg 1 erythromycin base tabs 250mg 1 erythromycin base tabs 500mg 1 erythromycin ethylsuccinate tabs 400mg 1 erythromycin cpep 250mg 1 erythromycin gel 2% 1 erythromycin oint 5mg/gm 1 erythromycin pads 2% 1 erythromycin soln 2% 1 ilotycin oint 5mg/gm 1
Quinolones BESIVANCE SUSP 0.6% 2 ciprofloxacin er tb24 1000mg; 0 1 ciprofloxacin er tb24 500mg; 0 1 ciprofloxacin hcl soln 0.3% 1 ciprofloxacin hcl tabs 100mg 1 ciprofloxacin hcl tabs 250mg 1 ciprofloxacin hcl tabs 500mg 1 ciprofloxacin hcl tabs 750mg 1 ciprofloxacin i.v.-in d5w inj 200mg/100ml; 5% 1 ciprofloxacin i.v.-in d5w inj 400mg/200ml; 5% 1 ciprofloxacin inj 200mg/20ml 1 ciprofloxacin inj 400mg/40ml 1 ciprofloxacin soln 0.2% 1 ciprofloxacin susr 250mg/5ml 1 ciprofloxacin susr 500mg/5ml 1 gatifloxacin soln 0.5% 1 levofloxacin in d5w inj 5%; 250mg/50ml 1 levofloxacin in d5w inj 5%; 500mg/100ml 1 levofloxacin in d5w inj 5%; 750mg/150ml 1 levofloxacin inj 25mg/ml 1 levofloxacin soln 0.5% 1 levofloxacin soln 25mg/ml 1 levofloxacin tabs 250mg 1

Page 20 of 121
Drug Name Drug Tier Requirements/Limits
levofloxacin tabs 500mg 1 levofloxacin tabs 750mg 1 MOXEZA SOLN 0.5% 2 moxifloxacin hcl inj 400mg/250ml 1 moxifloxacin hcl tabs 400mg 1 ofloxacin soln 0.3% 1 ofloxacin soln 0.3% 1 ofloxacin tabs 400mg 1 VIGAMOX SOLN 0.5% 2
Sulfonamides sodium sulfacetamide soln 10% 1 sulfacetamide sodium oint 10% 1 sulfacetamide sodium soln 10% 1 sulfadiazine tabs 500mg 1 sulfamethoxazole/trimethoprim ds tabs 800mg; 160mg 1 sulfamethoxazole/trimethoprim inj 400mg/5ml; 80mg/5ml 1 sulfamethoxazole/trimethoprim susp 200mg/5ml; 40mg/5ml 1 sulfamethoxazole/trimethoprim tabs 400mg; 80mg 1 sulfatrim pediatric susp 200mg/5ml; 40mg/5ml 1
Tetracyclines demeclocycline hcl tabs 150mg 1 demeclocycline hcl tabs 300mg 1 doxy 100 inj 100mg 1 doxycycline hyclate dr tbec 100mg 1 doxycycline hyclate dr tbec 150mg 1 doxycycline hyclate dr tbec 75mg 1 doxycycline hyclate caps 100mg 1 doxycycline hyclate caps 50mg 1 doxycycline hyclate inj 100mg 1 doxycycline hyclate tabs 100mg 1 doxycycline hyclate tabs 20mg 1 doxycycline monohydrate caps 100mg 1 doxycycline monohydrate caps 50mg 1 doxycycline monohydrate tabs 100mg 1 doxycycline monohydrate tabs 150mg 1 doxycycline monohydrate tabs 50mg 1 doxycycline monohydrate tabs 75mg 1 doxycycline caps 150mg 1 doxycycline caps 75mg 1 doxycycline susr 25mg/5ml 1 minocycline hcl er tb24 135mg 1 minocycline hcl er tb24 45mg 1 minocycline hcl er tb24 90mg 1 minocycline hcl caps 100mg 1 minocycline hcl caps 50mg 1 minocycline hcl caps 75mg 1 minocycline hcl tabs 100mg 1 minocycline hcl tabs 50mg 1 minocycline hcl tabs 75mg 1

Page 21 of 121
Drug Name Drug Tier Requirements/Limits
mondoxyne nl caps 100mg 1 mondoxyne nl caps 50mg 1 mondoxyne nl caps 75mg 1 morgidox 1x100mg caps 100mg 1 morgidox 1x100mg kit 0; 100mg; 0 1 morgidox 2x100mg caps 100mg 1 morgidox 2x100mg kit 0; 100mg; 0 1 tetracycline hcl caps 250mg 1 tetracycline hcl caps 500mg 1
Anticonvulsants Anticonvulsants, Other
APTIOM TABS 400MG 4 APTIOM TABS 600MG 4 APTIOM TABS 800MG 4 BRIVIACT SOLN 10MG/ML 4 BRIVIACT TABS 100MG 4 BRIVIACT TABS 10MG 4 BRIVIACT TABS 25MG 4 BRIVIACT TABS 50MG 4 BRIVIACT TABS 75MG 4 levetiracetam er tb24 500mg 1 levetiracetam er tb24 750mg 1 levetiracetam inj 1000mg/100ml; 750mg/100ml 1 levetiracetam inj 1500mg/100ml; 540mg/100ml 1 levetiracetam inj 500mg/100ml; 820mg/100ml 1 levetiracetam inj 500mg/5ml 1 levetiracetam soln 100mg/ml 1 levetiracetam tabs 1000mg 1 levetiracetam tabs 250mg 1 levetiracetam tabs 500mg 1 levetiracetam tabs 750mg 1 magnesium sulfate in d5w inj 5%; 10mg/ml 1 magnesium sulfate in d5w inj 5%; 20mg/ml 1 POTIGA TABS 200MG 4 POTIGA TABS 300MG 4 POTIGA TABS 400MG 4 POTIGA TABS 50MG 4 roweepra tabs 500mg 1
Calcium Channel Modifying Agents ethosuximide caps 250mg 1 ethosuximide soln 250mg/5ml 1 LYRICA CAPS 100MG 2 QL (90 EA per 30 days) LYRICA CAPS 150MG 2 QL (90 EA per 30 days) LYRICA CAPS 200MG 2 QL (90 EA per 30 days) LYRICA CAPS 225MG 2 QL (90 EA per 30 days) LYRICA CAPS 25MG 2 QL (90 EA per 30 days) LYRICA CAPS 300MG 2 QL (60 EA per 30 days) LYRICA CAPS 50MG 2 QL (90 EA per 30 days) LYRICA CAPS 75MG 2 QL (90 EA per 30 days)

Page 22 of 121
Drug Name Drug Tier Requirements/Limits
LYRICA SOLN 20MG/ML 2 QL (900 ML per 30 days) zonisamide caps 100mg 1 zonisamide caps 25mg 1 zonisamide caps 50mg 1
Gamma-aminobutyric Acid (GABA) Augmenting Agents clonazepam odt tbdp 0.125mg 1 QL (90 EA per 30 days) clonazepam odt tbdp 0.25mg 1 QL (90 EA per 30 days) clonazepam odt tbdp 0.5mg 1 QL (90 EA per 30 days) clonazepam odt tbdp 1mg 1 QL (90 EA per 30 days) clonazepam odt tbdp 2mg 1 QL (30 EA per 30 days) clonazepam tabs 0.5mg 1 clonazepam tabs 1mg 1 clonazepam tabs 2mg 1 diazepam gel 10mg 1 diazepam gel 2.5mg 1 diazepam gel 20mg 1 divalproex sodium dr tbec 125mg 1 divalproex sodium dr tbec 250mg 1 divalproex sodium dr tbec 500mg 1 divalproex sodium er tb24 250mg 1 divalproex sodium er tb24 500mg 1 divalproex sodium csdr 125mg 1 gabapentin caps 100mg 1 gabapentin caps 300mg 1 gabapentin caps 400mg 1 gabapentin soln 250mg/5ml 1 gabapentin tabs 600mg 1 gabapentin tabs 800mg 1 ONFI SUSP 2.5MG/ML 4 ONFI TABS 20MG 4 phenobarbital elix 20mg/5ml 1 PA phenobarbital tabs 100mg 1 PA phenobarbital tabs 15mg 1 PA phenobarbital tabs 16.2mg 1 PA phenobarbital tabs 30mg 1 PA phenobarbital tabs 32.4mg 1 PA phenobarbital tabs 60mg 1 PA phenobarbital tabs 64.8mg 1 PA phenobarbital tabs 97.2mg 1 PA primidone tabs 250mg 1 primidone tabs 50mg 1 SABRIL PACK 500MG 4 PA SABRIL TABS 500MG 4 PA tiagabine hydrochloride tabs 2mg 1 tiagabine hydrochloride tabs 4mg 1 valproate sodium inj 500mg/5ml 1 valproic acid caps 250mg 1 valproic acid syrp 250mg/5ml 1
Glutamate Reducing Agents

Page 23 of 121
Drug Name Drug Tier Requirements/Limits
felbamate susp 600mg/5ml 4 felbamate tabs 400mg 1 felbamate tabs 600mg 1 LAMICTAL STARTER/TAKING CARBAMAZEPINE/NOT TAKING VALPROATE KIT 0
4
lamotrigine er tb24 100mg 1 lamotrigine er tb24 200mg 1 lamotrigine er tb24 250mg 1 lamotrigine er tb24 25mg 1 lamotrigine er tb24 300mg 1 lamotrigine er tb24 50mg 1 lamotrigine odt tbdp 100mg 1 lamotrigine odt tbdp 200mg 1 lamotrigine odt tbdp 25mg 1 lamotrigine odt tbdp 50mg 1 lamotrigine titration kit 0 1 lamotrigine titration kit 0 1 lamotrigine titration kit 0 1 lamotrigine chew 25mg 1 lamotrigine chew 5mg 1 lamotrigine tabs 100mg 1 lamotrigine tabs 150mg 1 lamotrigine tabs 200mg 1 lamotrigine tabs 25mg 1 topiramate er cs24 100mg 1 topiramate er cs24 150mg 1 topiramate er cs24 200mg 1 topiramate er cs24 25mg 1 topiramate er cs24 50mg 1 topiramate cpsp 15mg 1 topiramate cpsp 25mg 1 topiramate tabs 100mg 1 topiramate tabs 200mg 1 topiramate tabs 25mg 1 topiramate tabs 50mg 1
Sodium Channel Agents BANZEL SUSP 40MG/ML 4 BANZEL TABS 200MG 4 BANZEL TABS 400MG 4 carbamazepine er cp12 100mg 1 carbamazepine er cp12 200mg 1 carbamazepine er cp12 300mg 1 carbamazepine er tb12 100mg 1 carbamazepine er tb12 200mg 1 carbamazepine er tb12 400mg 1 carbamazepine chew 100mg 1 carbamazepine susp 100mg/5ml 1 carbamazepine tabs 200mg 1 epitol tabs 200mg 1

Page 24 of 121
Drug Name Drug Tier Requirements/Limits
fosphenytoin sodium inj 100mg pe/2ml 1 fosphenytoin sodium inj 500mg pe/10ml 1 oxcarbazepine susp 300mg/5ml 1 oxcarbazepine tabs 150mg 1 oxcarbazepine tabs 300mg 1 oxcarbazepine tabs 600mg 1 phenytoin sodium extended caps 100mg 1 phenytoin sodium extended caps 200mg 1 phenytoin sodium extended caps 300mg 1 phenytoin sodium inj 50mg/ml 1 phenytoin chew 50mg 1 phenytoin susp 125mg/5ml 1
Antidementia Agents Antidementia Agents, Other
ERGOLOID MESYLATES TABS 1MG 2 PA NAMZARIC CP24 10MG; 14MG 2 NAMZARIC CP24 10MG; 28MG 2
Cholinesterase Inhibitors donepezil hcl tabs 10mg 1 donepezil hcl tabs 23mg 1 donepezil hcl tabs 5mg 1 donepezil hcl tbdp 10mg 1 donepezil hcl tbdp 5mg 1 galantamine hydrobromide cp24 16mg 1 galantamine hydrobromide cp24 24mg 1 galantamine hydrobromide cp24 8mg 1 galantamine hydrobromide soln 4mg/ml 1 galantamine hydrobromide tabs 12mg 1 galantamine hydrobromide tabs 4mg 1 galantamine hydrobromide tabs 8mg 1 rivastigmine tartrate caps 1.5mg 1 rivastigmine tartrate caps 3mg 1 rivastigmine tartrate caps 4.5mg 1 rivastigmine tartrate caps 6mg 1 rivastigmine transdermal system pt24 13.3mg/24hr 1 rivastigmine transdermal system pt24 4.6mg/24hr 1 rivastigmine transdermal system pt24 9.5mg/24hr 1
N-methyl-D-aspartate (NMDA) Receptor Antagonist memantine hcl titration pak tabs 0 1 memantine hcl tabs 10mg 1 memantine hcl tabs 5mg 1 memantine hydrochloride soln 2mg/ml 1 NAMENDA XR TITRATION PACK CP24 0 2 QL (56 EA per 365 days) NAMENDA XR CP24 14MG 2 QL (30 EA per 30 days) NAMENDA XR CP24 21MG 2 QL (30 EA per 30 days) NAMENDA XR CP24 28MG 2 QL (30 EA per 30 days) NAMENDA XR CP24 7MG 2 QL (30 EA per 30 days)
Antidepressants Antidepressants, Other

Page 25 of 121
Drug Name Drug Tier Requirements/Limits
APLENZIN TB24 174MG 4 QL (30 EA per 30 days) ST APLENZIN TB24 348MG 4 QL (30 EA per 30 days) ST APLENZIN TB24 522MG 4 QL (30 EA per 30 days) ST bupropion hcl er tb12 100mg 1 QL (90 EA per 30 days) bupropion hcl er tb12 150mg 1 QL (90 EA per 30 days) bupropion hcl er tb12 200mg 1 QL (90 EA per 30 days) bupropion hcl sr tb12 100mg 1 QL (90 EA per 30 days) bupropion hcl sr tb12 150mg 1 QL (90 EA per 30 days) bupropion hcl sr tb12 200mg 1 QL (90 EA per 30 days) bupropion hcl xl tb24 150mg 1 QL (90 EA per 30 days) bupropion hcl xl tb24 300mg 1 QL (30 EA per 30 days) bupropion hcl tabs 100mg 1 bupropion hcl tabs 75mg 1 FORFIVO XL TB24 450MG 2 QL (30 EA per 30 days) maprotiline hcl tabs 25mg 1 maprotiline hcl tabs 50mg 1 maprotiline hcl tabs 75mg 1 mirtazapine odt tbdp 15mg 1 mirtazapine odt tbdp 30mg 1 mirtazapine odt tbdp 45mg 1 mirtazapine tabs 15mg 1 mirtazapine tabs 30mg 1 mirtazapine tabs 45mg 1 mirtazapine tabs 7.5mg 1 trazodone hcl tabs 100mg 1 trazodone hcl tabs 150mg 1 trazodone hcl tabs 300mg 1 trazodone hcl tabs 50mg 1
Monoamine Oxidase Inhibitors EMSAM PT24 12MG/24HR 4 QL (30 EA per 30 days) ST EMSAM PT24 6MG/24HR 4 QL (30 EA per 30 days) ST EMSAM PT24 9MG/24HR 4 QL (30 EA per 30 days) ST phenelzine sulfate tabs 15mg 1 tranylcypromine sulfate tabs 10mg 1
SSRIs/SNRIs (Selective Serotonin Reuptake Inhibitors/Serotonin and Norepinephrine Reuptake Inhibitor
citalopram hydrobromide soln 10mg/5ml 1 citalopram hydrobromide tabs 10mg 1 citalopram hydrobromide tabs 20mg 1 citalopram hydrobromide tabs 40mg 1 duloxetine hcl cpep 20mg 1 QL (60 EA per 30 days) duloxetine hcl cpep 30mg 1 QL (90 EA per 30 days) duloxetine hcl cpep 40mg 1 QL (60 EA per 30 days) duloxetine hcl cpep 60mg 1 QL (60 EA per 30 days) escitalopram oxalate soln 5mg/5ml 1 escitalopram oxalate tabs 10mg 1 escitalopram oxalate tabs 20mg 1 escitalopram oxalate tabs 5mg 1 fluoxetine dr cpdr 90mg 1 QL (4 EA per 28 days)

Page 26 of 121
Drug Name Drug Tier Requirements/Limits
fluoxetine hcl caps 10mg 1 fluoxetine hcl caps 20mg 1 fluoxetine hcl caps 40mg 1 fluoxetine hcl soln 20mg/5ml 1 fluoxetine hcl tabs 10mg 1 fluoxetine hcl tabs 20mg 1 fluoxetine hcl tabs 60mg 1 fluoxetine caps 10mg 1 fluoxetine caps 20mg 1 fluvoxamine maleate er cp24 100mg 1 QL (60 EA per 30 days) fluvoxamine maleate er cp24 150mg 1 QL (60 EA per 30 days) fluvoxamine maleate tabs 100mg 1 fluvoxamine maleate tabs 25mg 1 fluvoxamine maleate tabs 50mg 1 olanzapine/fluoxetine caps 25mg; 12mg 1 QL (30 EA per 30 days) olanzapine/fluoxetine caps 25mg; 3mg 1 QL (90 EA per 30 days) olanzapine/fluoxetine caps 25mg; 6mg 1 QL (90 EA per 30 days) olanzapine/fluoxetine caps 50mg; 12mg 1 QL (30 EA per 30 days) olanzapine/fluoxetine caps 50mg; 6mg 1 QL (30 EA per 30 days) paroxetine hcl er tb24 12.5mg 1 paroxetine hcl er tb24 25mg 1 paroxetine hcl er tb24 37.5mg 1 paroxetine hcl tabs 10mg 1 paroxetine hcl tabs 20mg 1 paroxetine hcl tabs 30mg 1 paroxetine hcl tabs 40mg 1 sertraline hcl conc 20mg/ml 1 sertraline hcl tabs 100mg 1 sertraline hcl tabs 25mg 1 sertraline hcl tabs 50mg 1 venlafaxine hcl er cp24 150mg 1 venlafaxine hcl er cp24 37.5mg 1 venlafaxine hcl er cp24 75mg 1 venlafaxine hcl er tb24 150mg 1 venlafaxine hcl er tb24 225mg 1 venlafaxine hcl er tb24 37.5mg 1 venlafaxine hcl er tb24 75mg 1 venlafaxine hcl tabs 100mg 1 venlafaxine hcl tabs 25mg 1 venlafaxine hcl tabs 37.5mg 1 venlafaxine hcl tabs 50mg 1 venlafaxine hcl tabs 75mg 1
Tricyclics amitriptyline hcl tabs 100mg 1 PA amitriptyline hcl tabs 10mg 1 PA amitriptyline hcl tabs 150mg 1 PA amitriptyline hcl tabs 25mg 1 PA amitriptyline hcl tabs 50mg 1 PA amitriptyline hcl tabs 75mg 1 PA

Page 27 of 121
Drug Name Drug Tier Requirements/Limits
amoxapine tabs 100mg 1 amoxapine tabs 150mg 1 amoxapine tabs 25mg 1 amoxapine tabs 50mg 1 chlordiazepoxide/amitriptyline tabs 12.5mg; 5mg 1 PA chlordiazepoxide/amitriptyline tabs 25mg; 10mg 1 PA clomipramine hcl caps 25mg 1 PA clomipramine hcl caps 50mg 1 PA clomipramine hcl caps 75mg 1 PA desipramine hcl tabs 100mg 1 desipramine hcl tabs 10mg 1 desipramine hcl tabs 150mg 1 desipramine hcl tabs 25mg 1 desipramine hcl tabs 50mg 1 desipramine hcl tabs 75mg 1 doxepin hcl caps 100mg 1 PA doxepin hcl caps 10mg 1 PA doxepin hcl caps 150mg 1 PA doxepin hcl caps 25mg 1 PA doxepin hcl caps 50mg 1 PA doxepin hcl caps 75mg 1 PA doxepin hcl conc 10mg/ml 1 PA imipramine hcl tabs 10mg 1 PA imipramine hcl tabs 25mg 1 PA imipramine hcl tabs 50mg 1 PA imipramine pamoate caps 100mg 1 PA imipramine pamoate caps 125mg 1 PA imipramine pamoate caps 150mg 1 PA imipramine pamoate caps 75mg 1 PA nortriptyline hcl caps 10mg 1 nortriptyline hcl caps 25mg 1 nortriptyline hcl caps 50mg 1 nortriptyline hcl caps 75mg 1 nortriptyline hcl soln 10mg/5ml 1 perphenazine/amitriptyline tabs 10mg; 2mg 1 PA perphenazine/amitriptyline tabs 10mg; 4mg 1 PA perphenazine/amitriptyline tabs 25mg; 2mg 1 PA perphenazine/amitriptyline tabs 25mg; 4mg 1 PA perphenazine/amitriptyline tabs 50mg; 4mg 1 PA protriptyline hcl tabs 10mg 1 protriptyline hcl tabs 5mg 1 trimipramine maleate caps 100mg 1 PA trimipramine maleate caps 25mg 1 PA trimipramine maleate caps 50mg 1 PA
Antiemetics Antiemetics, Other
droperidol inj 2.5mg/ml 1 meclizine hcl tabs 12.5mg 1 meclizine hcl tabs 25mg 1

Page 28 of 121
Drug Name Drug Tier Requirements/Limits
phenadoz supp 12.5mg 1 PA phenadoz supp 25mg 1 PA phenergan supp 12.5mg 1 PA phenergan supp 25mg 1 PA phenergan supp 50mg 1 PA promethazine hcl inj 25mg/ml 1 PA promethazine hcl inj 50mg/ml 1 PA promethazine hcl supp 12.5mg 1 PA promethazine hcl supp 25mg 1 PA promethazine hcl supp 50mg 1 PA promethazine hcl syrp 6.25mg/5ml 1 PA promethazine hcl tabs 12.5mg 1 PA promethazine hcl tabs 25mg 1 PA promethazine hcl tabs 50mg 1 PA promethegan supp 12.5mg 1 PA promethegan supp 25mg 1 PA promethegan supp 50mg 1 PA trimethobenzamide hcl caps 300mg 1 PA
Emetogenic Therapy Adjuncts ANZEMET TABS 100MG 4 QL (5 EA per 30 days) B/D dronabinol caps 10mg 1 QL (60 EA per 30 days) PA dronabinol caps 2.5mg 1 QL (60 EA per 30 days) PA dronabinol caps 5mg 1 QL (60 EA per 30 days) PA granisetron hcl inj 0.1mg/ml 1 granisetron hcl inj 1mg/ml 1 granisetron hcl inj 4mg/4ml 1 granisetron hcl tabs 1mg 1 QL (30 EA per 30 days) B/D ondansetron hcl inj 40mg/20ml 1 QL (120 ML per 30 days) ondansetron hcl inj 4mg/2ml 1 QL (120 ML per 30 days) ondansetron hcl inj 4mg/2ml 1 QL (120 ML per 30 days) ondansetron hcl soln 4mg/5ml 1 QL (450 ML per 30 days) B/D ondansetron hcl tabs 24mg 1 QL (14 EA per 28 days) B/D ondansetron hcl tabs 4mg 1 B/D ondansetron hcl tabs 8mg 1 B/D ondansetron odt tbdp 4mg 1 B/D ondansetron odt tbdp 8mg 1 B/D SANCUSO PTCH 3.1MG/24HR 4 QL (2 EA per 30 days)
Antifungals Antifungals
ABELCET INJ 5MG/ML 4 B/D AMBISOME INJ 50MG 4 B/D amphotericin b inj 50mg 1 B/D CANCIDAS INJ 50MG 4 CANCIDAS INJ 70MG 4 ciclodan cream kit kit 0.77%; 0; 0 1 ciclodan solution kit kit 0; 8%; 0 1 ciclodan crea 0.77% 1 ciclodan soln 8% 1 PA ciclopirox nail lacquer soln 8% 1 PA

Page 29 of 121
Drug Name Drug Tier Requirements/Limits
ciclopirox olamine crea 0.77% 1 ciclopirox gel 0.77% 1 ciclopirox sham 1% 1 ciclopirox susp 0.77% 1 clotrimazole crea 1% 1 clotrimazole soln 1% 1 clotrimazole troc 10mg 1 CRESEMBA CAPS 186MG 4 CRESEMBA INJ 372MG 4 econazole nitrate crea 1% 1 ERAXIS INJ 100MG 4 ERAXIS INJ 50MG 4 fluconazole in dextrose inj 56mg/ml; 200mg/100ml 1 fluconazole in nacl inj 100mg/50ml; 0.9% 1 fluconazole in nacl inj 200mg/100ml; 0.9% 1 fluconazole in nacl inj 400mg/200ml; 0.9% 1 fluconazole susr 10mg/ml 1 fluconazole susr 40mg/ml 1 fluconazole tabs 100mg 1 fluconazole tabs 150mg 1 fluconazole tabs 200mg 1 fluconazole tabs 50mg 1 flucytosine caps 250mg 4 flucytosine caps 500mg 4 griseofulvin microsize susp 125mg/5ml 1 griseofulvin microsize tabs 500mg 1 griseofulvin ultramicrosize tabs 125mg 1 griseofulvin ultramicrosize tabs 250mg 1 itraconazole caps 100mg 1 PA ketoconazole crea 2% 1 ketoconazole foam 2% 1 ketoconazole sham 2% 1 ketoconazole tabs 200mg 1 ketodan kit kit 2%; 0; 0 1 ketodan foam 2% 1 miconazole 3 supp 200mg 1 MYCAMINE INJ 100MG 4 naftifine hcl crea 1% 1 naftifine hydrochloride crea 2% 1 NOXAFIL SUSP 40MG/ML 4 NOXAFIL TBEC 100MG 4 nyamyc powd 100000unit/gm 1 nystatin/triamcinolone crea 100000unit/gm; 0.1% 1 nystatin/triamcinolone oint 100000unit/gm; 0.1% 1 nystatin crea 100000unit/gm 1 nystatin oint 100000unit/gm 1 nystatin powd 100000unit/gm 1 nystatin susp 100000unit/ml 1 nystatin tabs 500000unit 1

Page 30 of 121
Drug Name Drug Tier Requirements/Limits
nystop powd 100000unit/gm 1 ONMEL TABS 200MG 4 PA oxiconazole nitrate crea 1% 1 SPORANOX SOLN 10MG/ML 4 PA terbinafine hcl tabs 250mg 1 QL (84 EA per 180 days) terconazole crea 0.4% 1 terconazole crea 0.8% 1 terconazole supp 80mg 1 voriconazole inj 200mg 1 voriconazole susr 40mg/ml 4 voriconazole tabs 200mg 1 voriconazole tabs 50mg 1 zazole crea 0.8% 1 zazole supp 80mg 1
Antigout Agents Antigout Agents
allopurinol tabs 100mg 1 allopurinol tabs 300mg 1 colchicine tabs 0.6mg 1 probenecid/colchicine tabs 0.5mg; 500mg 1 probenecid tabs 500mg 1 ULORIC TABS 40MG 2 ST ULORIC TABS 80MG 2 ST
Antimigraine Agents Ergot Alkaloids
dihydroergotamine mesylate inj 1mg/ml 4 dihydroergotamine mesylate soln 4mg/ml 4 QL (8 ML per 30 days) ERGOMAR SUBL 2MG 2 MIGRANAL SOLN 4MG/ML 4 QL (8 ML per 30 days)
Serotonin (5-HT) 1b/1d Receptor Agonists almotriptan malate tabs 12.5mg 1 QL (12 EA per 30 days) almotriptan malate tabs 6.25mg 1 QL (12 EA per 30 days) almotriptan tabs 12.5mg 1 QL (12 EA per 30 days) almotriptan tabs 6.25mg 1 QL (12 EA per 30 days) frovatriptan succinate tabs 2.5mg 1 QL (9 EA per 30 days) naratriptan hcl tabs 1mg 1 QL (9 EA per 30 days) naratriptan hcl tabs 2.5mg 1 QL (9 EA per 30 days) rizatriptan benzoate odt tbdp 10mg 1 QL (18 EA per 30 days) rizatriptan benzoate odt tbdp 5mg 1 QL (18 EA per 30 days) rizatriptan benzoate tabs 10mg 1 QL (18 EA per 30 days) rizatriptan benzoate tabs 5mg 1 QL (18 EA per 30 days) sumatriptan succinate refill inj 4mg/0.5ml 1 QL (5 ML per 30 days) sumatriptan succinate refill inj 6mg/0.5ml 1 QL (5 ML per 30 days) sumatriptan succinate inj 4mg/0.5ml 1 QL (5 ML per 30 days) sumatriptan succinate inj 6mg/0.5ml 1 QL (5 ML per 30 days) sumatriptan succinate inj 6mg/0.5ml 1 QL (5 ML per 30 days) sumatriptan succinate inj 6mg/0.5ml 1 QL (5 ML per 30 days) sumatriptan succinate tabs 100mg 1 QL (9 EA per 30 days) sumatriptan succinate tabs 25mg 1 QL (9 EA per 30 days)

Page 31 of 121
Drug Name Drug Tier Requirements/Limits
sumatriptan succinate tabs 50mg 1 QL (9 EA per 30 days) sumatriptan soln 20mg/act 1 QL (12 EA per 30 days) sumatriptan soln 5mg/act 1 QL (12 EA per 30 days) zolmitriptan odt tbdp 2.5mg 1 QL (12 EA per 30 days) zolmitriptan odt tbdp 5mg 1 QL (9 EA per 30 days) zolmitriptan tabs 2.5mg 1 QL (12 EA per 30 days) zolmitriptan tabs 5mg 1 QL (12 EA per 30 days)
Antimyasthenic Agents Parasympathomimetics
MESTINON SYRP 60MG/5ML 4 pyridostigmine bromide er tbcr 180mg 1 pyridostigmine bromide tabs 60mg 1
Antimycobacterials Antimycobacterials, Other
dapsone tabs 100mg 1 dapsone tabs 25mg 1 rifabutin caps 150mg 1
Antituberculars cycloserine caps 250mg 1 ethambutol hcl tabs 100mg 1 ethambutol hcl tabs 400mg 1 isoniazid inj 100mg/ml 1 isoniazid syrp 50mg/5ml 1 isoniazid tabs 100mg 1 isoniazid tabs 300mg 1 pyrazinamide tabs 500mg 1 rifampin caps 150mg 1 rifampin caps 300mg 1 rifampin inj 600mg 1 SIRTURO TABS 100MG 4
Antineoplastics Alkylating Agents
BENDEKA INJ 100MG/4ML 4 BICNU INJ 100MG 4 BUSULFEX INJ 6MG/ML 4 cyclophosphamide caps 25mg 1 B/D cyclophosphamide caps 50mg 1 B/D cyclophosphamide inj 1gm 4 cyclophosphamide inj 2gm 4 cyclophosphamide inj 500mg 4 dacarbazine inj 100mg 1 dacarbazine inj 200mg 1 EVOMELA INJ 50MG 4 HEXALEN CAPS 50MG 4 ifosfamide inj 1gm/20ml 1 ifosfamide inj 1gm 1 ifosfamide inj 3gm/60ml 1 ifosfamide inj 3gm 1 MATULANE CAPS 50MG 4

Page 32 of 121
Drug Name Drug Tier Requirements/Limits
melphalan hydrochloride inj 50mg 4 MUSTARGEN INJ 10MG 4 thiotepa inj 15mg 4 TREANDA INJ 100MG 4 TREANDA INJ 180MG/2ML 4 TREANDA INJ 25MG 4 TREANDA INJ 45MG/0.5ML 4 VALCHLOR GEL 0.016% 4 PA YONDELIS INJ 1MG 4 ZANOSAR INJ 1GM 4
Antiandrogens bicalutamide tabs 50mg 1 flutamide caps 125mg 1 NILANDRON TABS 150MG 4 nilutamide tabs 150mg 4 XTANDI CAPS 40MG 4 PA ZYTIGA TABS 250MG 4 PA
Antiangiogenic Agents POMALYST CAPS 1MG 4 PA POMALYST CAPS 2MG 4 PA POMALYST CAPS 3MG 4 PA POMALYST CAPS 4MG 4 PA REVLIMID CAPS 10MG 4 PA REVLIMID CAPS 15MG 4 PA REVLIMID CAPS 2.5MG 4 PA REVLIMID CAPS 20MG 4 PA REVLIMID CAPS 25MG 4 PA REVLIMID CAPS 5MG 4 PA THALOMID CAPS 100MG 4 PA THALOMID CAPS 150MG 4 PA THALOMID CAPS 200MG 4 PA THALOMID CAPS 50MG 4 PA
Antiestrogens/Modifiers EMCYT CAPS 140MG 4 FARESTON TABS 60MG 4 FASLODEX INJ 250MG/5ML 4 tamoxifen citrate tabs 10mg 1 tamoxifen citrate tabs 20mg 1
Antimetabolites adrucil inj 2.5gm/50ml 1 B/D adrucil inj 500mg/10ml 1 B/D adrucil inj 5gm/100ml 1 B/D ALIMTA INJ 100MG 4 ALIMTA INJ 500MG 4 cladribine inj 10mg/10ml 4 B/D CLOLAR INJ 1MG/ML 4 cytarabine aqueous inj 100mg/ml 1 B/D cytarabine aqueous inj 20mg/ml 1 B/D cytarabine aqueous inj 20mg/ml 1 B/D

Page 33 of 121
Drug Name Drug Tier Requirements/Limits
DEPOCYT INJ 50MG/5ML 4 B/D ELITEK INJ 1.5MG 4 ELITEK INJ 7.5MG 4 floxuridine inj 0.5gm 1 B/D fluorouracil inj 1gm/20ml 1 B/D fluorouracil inj 2.5gm/50ml 1 B/D fluorouracil inj 500mg/10ml 1 B/D fluorouracil inj 5gm/100ml 1 B/D FOLOTYN INJ 20MG/ML 4 PA FOLOTYN INJ 40MG/2ML 4 PA gemcitabine hcl inj 1gm 1 gemcitabine hcl inj 200mg 1 gemcitabine hcl inj 2gm 1 gemcitabine inj 1gm/26.3ml 1 gemcitabine inj 200mg/5.26ml 1 gemcitabine inj 2gm/52.6ml 1 hydroxyurea caps 500mg 1 LONSURF TABS 6.14MG; 15MG 4 QL (100 EA per 28 days) PA LONSURF TABS 8.19MG; 20MG 4 QL (80 EA per 28 days) PA mercaptopurine tabs 50mg 1 NIPENT INJ 10MG 4 PURIXAN SUSP 2000MG/100ML 4
Antineoplastics, Other ABRAXANE INJ 900MG; 100MG 4 amifostine inj 500mg 4 azacitidine inj 100mg 4 BELEODAQ INJ 500MG 4 PA bleomycin sulfate inj 15unit 1 B/D bleomycin sulfate inj 30unit 1 B/D carboplatin inj 150mg/15ml 1 carboplatin inj 450mg/45ml 1 carboplatin inj 50mg/5ml 1 carboplatin inj 600mg/60ml 1 cisplatin inj 100mg/100ml 1 cisplatin inj 200mg/200ml 1 cisplatin inj 50mg/50ml 1 COSMEGEN INJ 0.5MG 4 COTELLIC TABS 20MG 4 QL (90 EA per 30 days) PA daunorubicin hcl inj 5mg/ml 1 decitabine inj 50mg 4 PA dexrazoxane inj 250mg 4 dexrazoxane inj 500mg 4 DOCEFREZ INJ 20MG 4 docetaxel inj 140mg/7ml 4 docetaxel inj 160mg/16ml 4 docetaxel inj 160mg/8ml 4 docetaxel inj 200mg/20ml 4 docetaxel inj 20mg/2ml 4 docetaxel inj 20mg/ml 4

Page 34 of 121
Drug Name Drug Tier Requirements/Limits
docetaxel inj 80mg/4ml 4 docetaxel inj 80mg/8ml 4 doxorubicin hcl liposome inj 2mg/ml 4 B/D doxorubicin hcl inj 10mg 1 B/D doxorubicin hcl inj 2mg/ml 1 B/D doxorubicin hcl inj 50mg 1 B/D epirubicin hcl inj 200mg/100ml 1 epirubicin hcl inj 50mg/25ml 1 ERWINAZE INJ 10000UNIT 4 FARYDAK CAPS 10MG 4 QL (6 EA per 21 days) PA FARYDAK CAPS 15MG 4 QL (6 EA per 21 days) PA FARYDAK CAPS 20MG 4 QL (6 EA per 21 days) PA fludarabine phosphate inj 50mg/2ml 1 fludarabine phosphate inj 50mg 1 FUSILEV INJ 50MG 4 GILOTRIF TABS 20MG 4 QL (30 EA per 30 days) PA GILOTRIF TABS 30MG 4 QL (30 EA per 30 days) PA GILOTRIF TABS 40MG 4 QL (30 EA per 30 days) PA HALAVEN INJ 1MG/2ML 4 PA IBRANCE CAPS 100MG 4 PA IBRANCE CAPS 125MG 4 PA IBRANCE CAPS 75MG 4 PA idarubicin hcl inj 10mg/10ml 4 idarubicin hcl inj 20mg/20ml 4 idarubicin hcl inj 5mg/5ml 4 irinotecan hcl inj 100mg/5ml 1 B/D irinotecan inj 100mg/5ml 1 B/D irinotecan inj 40mg/2ml 1 B/D irinotecan inj 500mg/25ml 1 B/D ISTODAX INJ 10MG 4 PA IXEMPRA KIT INJ 15MG 4 IXEMPRA KIT INJ 45MG 4 JEVTANA INJ 60MG/1.5ML 4 PA leucovorin calcium inj 100mg 1 leucovorin calcium inj 200mg 1 leucovorin calcium inj 350mg 1 leucovorin calcium inj 500mg 1 leucovorin calcium inj 50mg 1 leucovorin calcium tabs 10mg 1 leucovorin calcium tabs 15mg 1 leucovorin calcium tabs 25mg 1 leucovorin calcium tabs 5mg 1 levoleucovorin calcium inj 175mg/17.5ml 4 levoleucovorin inj 175mg/17.5ml 4 levoleucovorin inj 250mg/25ml 4 levoleucovorin inj 50mg 4 lipodox 50 inj 2mg/ml 4 B/D lipodox inj 2mg/ml 4 B/D LYNPARZA CAPS 50MG 4 PA

Page 35 of 121
Drug Name Drug Tier Requirements/Limits
mesna inj 100mg/ml 1 MESNEX TABS 400MG 4 mitomycin inj 20mg 4 mitomycin inj 40mg 4 mitomycin inj 5mg 4 mitoxantrone hcl inj 2mg/ml 1 PA mitoxantrone hcl inj 2mg/ml 1 PA mitoxantrone hcl inj 2mg/ml 1 PA NINLARO CAPS 2.3MG 4 PA NINLARO CAPS 3MG 4 PA NINLARO CAPS 4MG 4 PA ODOMZO CAPS 200MG 4 PA oxaliplatin inj 100mg/20ml 1 B/D oxaliplatin inj 100mg 4 B/D oxaliplatin inj 50mg/10ml 1 B/D oxaliplatin inj 50mg 4 B/D paclitaxel inj 100mg/16.7ml 1 paclitaxel inj 150mg/25ml 1 paclitaxel inj 300mg/50ml 1 paclitaxel inj 30mg/5ml 1 PORTRAZZA INJ 800MG/50ML 4 QL (2 ML per 21 days) PA PROLEUKIN INJ 22000000UNIT 4 SYLATRON INJ 200MCG 4 PA SYLATRON INJ 200MCG 4 PA SYLATRON INJ 300MCG 4 PA SYLATRON INJ 300MCG 4 PA SYLATRON INJ 600MCG 4 PA SYNRIBO INJ 3.5MG 4 PA TAGRISSO TABS 40MG 4 QL (30 EA per 30 days) PA TAGRISSO TABS 80MG 4 QL (30 EA per 30 days) PA THERACYS INJ 81MG/VIAL 4 VALSTAR INJ 40MG/ML 4 VELCADE INJ 3.5MG 4 PA VENCLEXTA STARTING PACK TBPK 0 4 PA VENCLEXTA TABS 100MG 4 PA vinblastine sulfate inj 1mg/ml 1 B/D vincasar pfs inj 1mg/ml 1 B/D vincristine sulfate inj 1mg/ml 1 B/D vinorelbine tartrate inj 10mg/ml 1 vinorelbine tartrate inj 50mg/5ml 1 ZALTRAP INJ 100MG/4ML 4 PA ZALTRAP INJ 200MG/8ML 4 PA ZOLINZA CAPS 100MG 4 PA ZYKADIA CAPS 150MG 4 PA
Aromatase Inhibitors, 3rd Generation anastrozole tabs 1mg 1 exemestane tabs 25mg 1 letrozole tabs 2.5mg 1
Enzyme Inhibitors

Page 36 of 121
Drug Name Drug Tier Requirements/Limits
ETOPOPHOS INJ 100MG 4 etoposide inj 100mg/5ml 1 etoposide inj 100mg/5ml 1 etoposide inj 1gm/50ml 1 etoposide inj 500mg/25ml 1 toposar inj 100mg/5ml 1 toposar inj 1gm/50ml 1 toposar inj 500mg/25ml 1 topotecan hcl inj 4mg/4ml 4 topotecan hcl inj 4mg 4 ZYDELIG TABS 100MG 4 PA ZYDELIG TABS 150MG 4 PA
Molecular Target Inhibitors AFINITOR DISPERZ TBSO 2MG 4 PA AFINITOR DISPERZ TBSO 3MG 4 PA AFINITOR DISPERZ TBSO 5MG 4 PA AFINITOR TABS 10MG 4 QL (30 EA per 30 days) PA AFINITOR TABS 2.5MG 4 QL (30 EA per 30 days) PA AFINITOR TABS 5MG 4 QL (30 EA per 30 days) PA AFINITOR TABS 7.5MG 4 QL (30 EA per 30 days) PA ALECENSA CAPS 150MG 4 QL (240 EA per 30 days) PA BOSULIF TABS 100MG 4 PA BOSULIF TABS 500MG 4 PA CABOMETYX TABS 20MG 4 PA CABOMETYX TABS 40MG 4 PA CABOMETYX TABS 60MG 4 PA CAPRELSA TABS 100MG 4 QL (60 EA per 30 days) PA CAPRELSA TABS 300MG 4 PA COMETRIQ KIT 0 4 PA COMETRIQ KIT 0 4 PA COMETRIQ KIT 20MG 4 PA ERIVEDGE CAPS 150MG 4 PA GLEEVEC TABS 100MG 4 PA GLEEVEC TABS 400MG 4 PA ICLUSIG TABS 15MG 4 QL (60 EA per 30 days) PA ICLUSIG TABS 45MG 4 PA imatinib mesylate tabs 100mg 4 PA imatinib mesylate tabs 400mg 4 PA IMBRUVICA CAPS 140MG 4 PA INLYTA TABS 1MG 4 PA INLYTA TABS 5MG 4 PA IRESSA TABS 250MG 4 PA JAKAFI TABS 10MG 4 QL (60 EA per 30 days) PA JAKAFI TABS 15MG 4 QL (60 EA per 30 days) PA JAKAFI TABS 20MG 4 QL (60 EA per 30 days) PA JAKAFI TABS 25MG 4 QL (60 EA per 30 days) PA JAKAFI TABS 5MG 4 QL (60 EA per 30 days) PA LENVIMA 10 MG DAILY DOSE CPPK 10MG 4 PA LENVIMA 14 MG DAILY DOSE CPPK 0 4 PA

Page 37 of 121
Drug Name Drug Tier Requirements/Limits
LENVIMA 18 MG DAILY DOSE CPPK 0 4 PA LENVIMA 20 MG DAILY DOSE CPPK 10MG 4 PA LENVIMA 24 MG DAILY DOSE CPPK 0 4 PA LENVIMA 8 MG DAILY DOSE CPPK 4MG 4 PA MEKINIST TABS 0.5MG 4 PA MEKINIST TABS 2MG 4 PA NEXAVAR TABS 200MG 4 PA SPRYCEL TABS 100MG 4 PA SPRYCEL TABS 140MG 4 PA SPRYCEL TABS 20MG 4 PA SPRYCEL TABS 50MG 4 PA SPRYCEL TABS 70MG 4 PA SPRYCEL TABS 80MG 4 PA STIVARGA TABS 40MG 4 PA SUTENT CAPS 12.5MG 4 PA SUTENT CAPS 25MG 4 PA SUTENT CAPS 37.5MG 4 PA SUTENT CAPS 50MG 4 PA TAFINLAR CAPS 50MG 4 PA TAFINLAR CAPS 75MG 4 PA TARCEVA TABS 100MG 4 QL (30 EA per 30 days) PA TARCEVA TABS 150MG 4 QL (30 EA per 30 days) PA TARCEVA TABS 25MG 4 QL (90 EA per 30 days) PA TASIGNA CAPS 150MG 4 PA TASIGNA CAPS 200MG 4 PA TYKERB TABS 250MG 4 PA VOTRIENT TABS 200MG 4 PA XALKORI CAPS 200MG 4 PA XALKORI CAPS 250MG 4 PA ZELBORAF TABS 240MG 4 PA
Monoclonal Antibodies ARZERRA INJ 1000MG/50ML 4 PA ARZERRA INJ 100MG/5ML 4 PA AVASTIN INJ 100MG/4ML 4 B/D AVASTIN INJ 400MG/16ML 4 B/D BLINCYTO INJ 35MCG 4 PA CYRAMZA INJ 100MG/10ML 4 PA CYRAMZA INJ 500MG/50ML 4 PA DARZALEX INJ 100MG/5ML 4 PA DARZALEX INJ 400MG/20ML 4 PA EMPLICITI INJ 300MG 4 PA EMPLICITI INJ 400MG 4 PA ERBITUX INJ 100MG/50ML 4 PA ERBITUX INJ 200MG/100ML 4 PA GAZYVA INJ 1000MG/40ML 4 PA HERCEPTIN INJ 440MG 4 PA KADCYLA INJ 100MG 4 PA KADCYLA INJ 160MG 4 PA KEYTRUDA INJ 100MG/4ML 4 PA

Page 38 of 121
Drug Name Drug Tier Requirements/Limits
KEYTRUDA INJ 50MG 4 PA OPDIVO INJ 100MG/10ML 4 PA OPDIVO INJ 40MG/4ML 4 PA PERJETA INJ 420MG/14ML 4 PA RITUXAN INJ 100MG/10ML 4 PA RITUXAN INJ 500MG/50ML 4 PA SYLVANT INJ 100MG 4 PA SYLVANT INJ 400MG 4 PA TECENTRIQ INJ 1200MG/20ML 4 PA UNITUXIN INJ 17.5MG/5ML 4 VECTIBIX INJ 100MG/5ML 4 B/D VECTIBIX INJ 400MG/20ML 4 B/D YERVOY INJ 200MG/40ML 4 PA YERVOY INJ 50MG/10ML 4 PA ZEVALIN Y-90 INJ 3.2MG/2ML 4
Retinoids bexarotene caps 75mg 4 PA PANRETIN GEL 0.1% 4 TARGRETIN CAPS 75MG 4 PA TARGRETIN GEL 1% 4 PA tretinoin caps 10mg 4
Antiparasitics Anthelmintics
ALBENZA TABS 200MG 4 BILTRICIDE TABS 600MG 2 ivermectin tabs 3mg 1
Antiprotozoals atovaquone/proguanil hcl tabs 250mg; 100mg 1 atovaquone/proguanil hcl tabs 62.5mg; 25mg 1 atovaquone susp 750mg/5ml 4 chloroquine phosphate tabs 250mg 1 chloroquine phosphate tabs 500mg 1 DARAPRIM TABS 25MG 4 PA hydroxychloroquine sulfate tabs 200mg 1 mefloquine hcl tabs 250mg 1 primaquine phosphate tabs 26.3mg 1 quinine sulfate caps 324mg 1 PA tinidazole tabs 250mg 1 tinidazole tabs 500mg 1
Pediculicides/Scabicides malathion lotn 0.5% 1 permethrin crea 5% 1
Antiparkinson Agents Anticholinergics
benztropine mesylate inj 1mg/ml 1 benztropine mesylate tabs 0.5mg 1 PA benztropine mesylate tabs 1mg 1 PA benztropine mesylate tabs 2mg 1 PA trihexyphenidyl hcl elix 0.4mg/ml 1 PA

Page 39 of 121
Drug Name Drug Tier Requirements/Limits
trihexyphenidyl hcl tabs 2mg 1 PA trihexyphenidyl hcl tabs 5mg 1 PA
Antiparkinson Agents, Other entacapone tabs 200mg 1 tolcapone tabs 100mg 4
Dopamine Agonists APOKYN INJ 10MG/ML 4 QL (60 ML per 30 days) PA pramipexole dihydrochloride er tb24 0.375mg 1 pramipexole dihydrochloride er tb24 0.75mg 1 pramipexole dihydrochloride er tb24 1.5mg 1 pramipexole dihydrochloride er tb24 2.25mg 1 pramipexole dihydrochloride er tb24 3.75mg 1 pramipexole dihydrochloride er tb24 3mg 1 pramipexole dihydrochloride er tb24 4.5mg 1 pramipexole dihydrochloride tabs 0.125mg 1 pramipexole dihydrochloride tabs 0.25mg 1 pramipexole dihydrochloride tabs 0.5mg 1 pramipexole dihydrochloride tabs 0.75mg 1 pramipexole dihydrochloride tabs 1.5mg 1 pramipexole dihydrochloride tabs 1mg 1 ropinirole er tb24 12mg 1 ropinirole er tb24 2mg 1 ropinirole er tb24 4mg 1 ropinirole er tb24 6mg 1 ropinirole er tb24 8mg 1 ropinirole hcl tabs 0.25mg 1 ropinirole hcl tabs 0.5mg 1 ropinirole hcl tabs 1mg 1 ropinirole hcl tabs 2mg 1 ropinirole hcl tabs 3mg 1 ropinirole hcl tabs 4mg 1 ropinirole hcl tabs 5mg 1
Dopamine Precursors/L- Amino Acid Decarboxylase Inhibitors carbidopa/levodopa er tbcr 25mg; 100mg 1 carbidopa/levodopa er tbcr 50mg; 200mg 1 carbidopa/levodopa odt tbdp 10mg; 100mg 1 carbidopa/levodopa odt tbdp 25mg; 100mg 1 carbidopa/levodopa odt tbdp 25mg; 250mg 1 carbidopa/levodopa/entacapone tabs 12.5mg; 200mg; 50mg 1 carbidopa/levodopa/entacapone tabs 18.75mg; 200mg; 75mg 1 carbidopa/levodopa/entacapone tabs 25mg; 200mg; 100mg 1 carbidopa/levodopa/entacapone tabs 31.25mg; 200mg; 125mg1 carbidopa/levodopa/entacapone tabs 37.5mg; 200mg; 150mg 1 carbidopa/levodopa/entacapone tabs 50mg; 200mg; 200mg 1 carbidopa/levodopa tabs 10mg; 100mg 1 carbidopa/levodopa tabs 25mg; 100mg 1 carbidopa/levodopa tabs 25mg; 250mg 1 carbidopa tabs 25mg 4
Monoamine Oxidase B (MAO-B) Inhibitors

Page 40 of 121
Drug Name Drug Tier Requirements/Limits
AZILECT TABS 0.5MG 2 AZILECT TABS 1MG 2 selegiline hcl caps 5mg 1 selegiline hcl tabs 5mg 1 ZELAPAR TBDP 1.25MG 4
Antipsychotics 1st Generation/Typical
chlorpromazine hcl inj 25mg/ml 1 chlorpromazine hcl inj 50mg/2ml 1 chlorpromazine hcl tabs 100mg 1 chlorpromazine hcl tabs 10mg 1 chlorpromazine hcl tabs 200mg 1 chlorpromazine hcl tabs 25mg 1 chlorpromazine hcl tabs 50mg 1 compro supp 25mg 1 fluphenazine decanoate inj 25mg/ml 1 fluphenazine hcl conc 5mg/ml 1 fluphenazine hcl elix 2.5mg/5ml 1 fluphenazine hcl inj 2.5mg/ml 1 fluphenazine hcl tabs 10mg 1 fluphenazine hcl tabs 1mg 1 fluphenazine hcl tabs 2.5mg 1 fluphenazine hcl tabs 5mg 1 haloperidol decanoate inj 100mg/ml 1 haloperidol decanoate inj 50mg/ml 1 haloperidol lactate inj 5mg/ml 1 haloperidol conc 2mg/ml 1 haloperidol tabs 0.5mg 1 haloperidol tabs 10mg 1 haloperidol tabs 1mg 1 haloperidol tabs 20mg 1 haloperidol tabs 2mg 1 haloperidol tabs 5mg 1 loxapine succinate caps 10mg 1 loxapine succinate caps 25mg 1 loxapine succinate caps 50mg 1 loxapine succinate caps 5mg 1 molindone hydrochloride tabs 10mg 1 molindone hydrochloride tabs 25mg 1 molindone hydrochloride tabs 5mg 1 perphenazine tabs 16mg 1 perphenazine tabs 2mg 1 perphenazine tabs 4mg 1 perphenazine tabs 8mg 1 pimozide tabs 1mg 1 pimozide tabs 2mg 1 prochlorperazine edisylate inj 5mg/ml 1 prochlorperazine maleate tabs 10mg 1 prochlorperazine maleate tabs 5mg 1

Page 41 of 121
Drug Name Drug Tier Requirements/Limits
prochlorperazine supp 25mg 1 thioridazine hcl tabs 100mg 1 PA thioridazine hcl tabs 10mg 1 PA thioridazine hcl tabs 25mg 1 PA thioridazine hcl tabs 50mg 1 PA thiothixene caps 10mg 1 thiothixene caps 1mg 1 thiothixene caps 2mg 1 thiothixene caps 5mg 1 trifluoperazine hcl tabs 10mg 1 trifluoperazine hcl tabs 1mg 1 trifluoperazine hcl tabs 2mg 1 trifluoperazine hcl tabs 5mg 1
2nd Generation/Atypical ABILIFY MAINTENA INJ 300MG 4 ABILIFY MAINTENA INJ 300MG 4 ABILIFY MAINTENA INJ 400MG 4 aripiprazole odt tbdp 10mg 4 QL (60 EA per 30 days) aripiprazole odt tbdp 15mg 4 QL (60 EA per 30 days) aripiprazole soln 1mg/ml 1 QL (750 ML per 30 days) aripiprazole tabs 10mg 1 QL (30 EA per 30 days) aripiprazole tabs 15mg 1 QL (30 EA per 30 days) aripiprazole tabs 20mg 1 QL (30 EA per 30 days) aripiprazole tabs 2mg 1 QL (60 EA per 30 days) aripiprazole tabs 30mg 1 QL (30 EA per 30 days) aripiprazole tabs 5mg 1 QL (60 EA per 30 days) ARISTADA INJ 441MG/1.6ML 4 ARISTADA INJ 662MG/2.4ML 4 ARISTADA INJ 882MG/3.2ML 4 FANAPT TABS 10MG 4 QL (60 EA per 30 days) ST FANAPT TABS 12MG 4 QL (60 EA per 30 days) ST FANAPT TABS 6MG 4 QL (60 EA per 30 days) ST FANAPT TABS 8MG 4 QL (60 EA per 30 days) ST INVEGA SUSTENNA INJ 117MG/0.75ML 4 INVEGA SUSTENNA INJ 156MG/ML 4 INVEGA SUSTENNA INJ 234MG/1.5ML 4 INVEGA TRINZA INJ 273MG/0.875ML 4 INVEGA TRINZA INJ 410MG/1.315ML 4 INVEGA TRINZA INJ 546MG/1.75ML 4 INVEGA TRINZA INJ 819MG/2.625ML 4 INVEGA TB24 6MG 4 QL (60 EA per 30 days) INVEGA TB24 9MG 4 QL (30 EA per 30 days) LATUDA TABS 120MG 4 QL (30 EA per 30 days) LATUDA TABS 20MG 4 QL (30 EA per 30 days) LATUDA TABS 40MG 4 QL (30 EA per 30 days) LATUDA TABS 60MG 4 QL (30 EA per 30 days) LATUDA TABS 80MG 4 QL (60 EA per 30 days) olanzapine odt tbdp 10mg 1 QL (30 EA per 30 days) olanzapine odt tbdp 15mg 1 QL (30 EA per 30 days)

Page 42 of 121
Drug Name Drug Tier Requirements/Limits
olanzapine odt tbdp 20mg 1 QL (30 EA per 30 days) olanzapine odt tbdp 5mg 1 QL (30 EA per 30 days) olanzapine inj 10mg 1 olanzapine tabs 10mg 1 QL (30 EA per 30 days) olanzapine tabs 15mg 1 QL (30 EA per 30 days) olanzapine tabs 2.5mg 1 QL (30 EA per 30 days) olanzapine tabs 20mg 1 QL (30 EA per 30 days) olanzapine tabs 5mg 1 QL (30 EA per 30 days) olanzapine tabs 7.5mg 1 QL (30 EA per 30 days) paliperidone er tb24 1.5mg 1 QL (30 EA per 30 days) paliperidone er tb24 3mg 1 QL (30 EA per 30 days) paliperidone er tb24 6mg 4 QL (60 EA per 30 days) paliperidone er tb24 9mg 4 QL (30 EA per 30 days) quetiapine fumarate tabs 100mg 1 QL (90 EA per 30 days) quetiapine fumarate tabs 200mg 1 QL (90 EA per 30 days) quetiapine fumarate tabs 25mg 1 QL (90 EA per 30 days) quetiapine fumarate tabs 300mg 1 QL (60 EA per 30 days) quetiapine fumarate tabs 400mg 1 QL (60 EA per 30 days) quetiapine fumarate tabs 50mg 1 QL (90 EA per 30 days) REXULTI TABS 0.25MG 4 QL (30 EA per 30 days) REXULTI TABS 0.5MG 4 QL (30 EA per 30 days) REXULTI TABS 1MG 4 QL (30 EA per 30 days) REXULTI TABS 2MG 4 QL (30 EA per 30 days) REXULTI TABS 3MG 4 QL (30 EA per 30 days) REXULTI TABS 4MG 4 QL (30 EA per 30 days) RISPERDAL CONSTA INJ 37.5MG 4 RISPERDAL CONSTA INJ 50MG 4 risperidone odt tbdp 0.25mg 1 QL (60 EA per 30 days) risperidone odt tbdp 0.5mg 1 QL (60 EA per 30 days) risperidone odt tbdp 1mg 1 QL (60 EA per 30 days) risperidone odt tbdp 2mg 1 QL (60 EA per 30 days) risperidone odt tbdp 3mg 1 QL (60 EA per 30 days) risperidone odt tbdp 4mg 1 QL (60 EA per 30 days) risperidone soln 1mg/ml 1 QL (240 ML per 30 days) risperidone tabs 0.25mg 1 QL (60 EA per 30 days) risperidone tabs 0.5mg 1 QL (60 EA per 30 days) risperidone tabs 1mg 1 QL (60 EA per 30 days) risperidone tabs 2mg 1 QL (60 EA per 30 days) risperidone tabs 3mg 1 QL (60 EA per 30 days) risperidone tabs 4mg 1 QL (60 EA per 30 days) VRAYLAR CAPS 1.5MG 4 QL (30 EA per 30 days) ST VRAYLAR CAPS 3MG 4 QL (30 EA per 30 days) ST VRAYLAR CAPS 4.5MG 4 QL (30 EA per 30 days) ST VRAYLAR CAPS 6MG 4 QL (30 EA per 30 days) ST ziprasidone hcl caps 20mg 1 QL (60 EA per 30 days) ziprasidone hcl caps 40mg 1 QL (60 EA per 30 days) ziprasidone hcl caps 60mg 1 QL (60 EA per 30 days) ziprasidone hcl caps 80mg 1 QL (60 EA per 30 days) ZYPREXA RELPREVV INJ 300MG 4

Page 43 of 121
Drug Name Drug Tier Requirements/Limits
ZYPREXA RELPREVV INJ 405MG 4 Antipsychotics
NUPLAZID TABS 17MG 4 QL (60 EA per 30 days) PA Treatment-Resistant
clozapine odt tbdp 100mg 1 QL (270 EA per 30 days) clozapine odt tbdp 12.5mg 1 QL (90 EA per 30 days) clozapine odt tbdp 200mg 4 QL (120 EA per 30 days) clozapine odt tbdp 25mg 1 QL (270 EA per 30 days) clozapine tabs 100mg 1 QL (270 EA per 30 days) clozapine tabs 200mg 1 QL (120 EA per 30 days) clozapine tabs 25mg 1 QL (270 EA per 30 days) clozapine tabs 50mg 1 QL (180 EA per 30 days) FAZACLO TBDP 200MG 4 QL (120 EA per 30 days) VERSACLOZ SUSP 50MG/ML 4 QL (540 ML per 30 days)
Antispasticity Agents Antispasticity Agents
baclofen tabs 10mg 1 baclofen tabs 20mg 1 dantrolene sodium caps 100mg 1 dantrolene sodium caps 25mg 1 dantrolene sodium caps 50mg 1 GABLOFEN INJ 40000MCG/20ML 4 B/D LIORESAL INTRATHECAL INJ 10MG/5ML 4 B/D LIORESAL INTRATHECAL INJ 40MG/20ML 4 B/D tizanidine hcl caps 2mg 1 tizanidine hcl caps 4mg 1 tizanidine hcl caps 6mg 1 tizanidine hcl tabs 2mg 1 tizanidine hcl tabs 4mg 1
Antivirals Anti-cytomegalovirus (CMV) Agents
cidofovir inj 75mg/ml 4 ganciclovir inj 500mg 1 B/D VALCYTE SOLR 50MG/ML 4 valganciclovir tabs 450mg 4
Anti-hepatitis B (HBV) Agents adefovir dipivoxil tabs 10mg 4 BARACLUDE TABS 0.5MG 4 QL (30 EA per 30 days) BARACLUDE TABS 1MG 4 QL (30 EA per 30 days) entecavir tabs 0.5mg 4 QL (30 EA per 30 days) entecavir tabs 1mg 4 QL (30 EA per 30 days) INTRON A W/DILUENT INJ 10MU 4 PA INTRON A INJ 10MU/ML 4 PA INTRON A INJ 18MU 4 PA INTRON A INJ 50MU 4 PA INTRON A INJ 6000000UNIT/ML 4 PA lamivudine tabs 100mg 1 TYZEKA TABS 600MG 4
Anti-hepatitis C (HCV) Agents

Page 44 of 121
Drug Name Drug Tier Requirements/Limits
DAKLINZA TABS 30MG 4 QL (504 EA per 365 days) PA DAKLINZA TABS 60MG 4 QL (168 EA per 365 days) PA DAKLINZA TABS 90MG 4 QL (168 EA per 365 days) PA HARVONI TABS 90MG; 400MG 4 QL (168 EA per 365 days) PA MODERIBA MISC 0 4 moderiba tabs 200mg 1 OLYSIO CAPS 150MG 4 QL (168 EA per 365 days) PA PEG-INTRON REDIPEN INJ 120MCG/0.5ML 4 PA PEG-INTRON REDIPEN INJ 150MCG/0.5ML 4 PA PEG-INTRON REDIPEN INJ 50MCG/0.5ML 4 PA PEG-INTRON REDIPEN INJ 80MCG/0.5ML 4 PA PEG-INTRON INJ 120MCG/0.5ML 4 PA PEG-INTRON INJ 150MCG/0.5ML 4 PA PEG-INTRON INJ 80MCG/0.5ML 4 PA PEGASYS PROCLICK INJ 135MCG/0.5ML 4 PA PEGASYS PROCLICK INJ 180MCG/0.5ML 4 PA PEGASYS INJ 180MCG/0.5ML 4 PA PEGASYS INJ 180MCG/ML 4 PA PEGINTRON INJ 120MCG/0.5ML 4 PA PEGINTRON INJ 150MCG/0.5ML 4 PA PEGINTRON INJ 50MCG/0.5ML 4 PA PEGINTRON INJ 80MCG/0.5ML 4 PA RIBASPHERE RIBAPAK TABS 0 4 ribasphere ribapak tabs 600mg 1 ribasphere caps 200mg 1 ribasphere tabs 200mg 1 ribasphere tabs 600mg 1 ribavirin caps 200mg 1 ribavirin tabs 200mg 1 SOVALDI TABS 400MG 4 QL (336 EA per 365 days) PA TECHNIVIE TABS 12.5MG; 75MG; 50MG 4 QL (168 EA per 365 days) PA VIEKIRA PAK TBPK 250MG; 12.5MG; 75MG; 50MG 4 QL (672 EA per 365 days) PA VIEKIRA XR TB24 200MG; 8.33MG; 50MG; 33.33MG 4 QL (504 EA per 365 days) PA ZEPATIER TABS 50MG; 100MG 4 QL (112 EA per 365 days) PA
Anti-HIV Agents, Integrase Inhibitors (INSTI) ATRIPLA TABS 600MG; 200MG; 300MG 4 QL (30 EA per 30 days) GENVOYA TABS 150MG; 150MG; 200MG; 10MG 4 QL (30 EA per 30 days) ISENTRESS CHEW 100MG 4 ISENTRESS CHEW 25MG 2 ISENTRESS PACK 100MG 4 ISENTRESS TABS 400MG 4 TIVICAY TABS 25MG 4 TIVICAY TABS 50MG 4 VITEKTA TABS 150MG 4 VITEKTA TABS 85MG 4
Anti-HIV Agents, Non-nucleoside Reverse Transcriptase Inhibitors (NNRTI)
COMPLERA TABS 200MG; 25MG; 300MG 4 QL (30 EA per 30 days) EDURANT TABS 25MG 4

Page 45 of 121
Drug Name Drug Tier Requirements/Limits
INTELENCE TABS 100MG 4 INTELENCE TABS 200MG 4 nevirapine er tb24 100mg 1 nevirapine er tb24 400mg 1 nevirapine susp 50mg/5ml 1 nevirapine tabs 200mg 1 ODEFSEY TABS 200MG; 25MG; 25MG 4 QL (30 EA per 30 days) STRIBILD TABS 150MG; 150MG; 200MG; 300MG 4 QL (30 EA per 30 days) SUSTIVA CAPS 200MG 4 SUSTIVA TABS 600MG 4 TRUVADA TABS 100MG; 150MG 4 QL (30 EA per 30 days) TRUVADA TABS 133MG; 200MG 4 QL (30 EA per 30 days) TRUVADA TABS 167MG; 250MG 4 QL (30 EA per 30 days) TRUVADA TABS 200MG; 300MG 4 QL (30 EA per 30 days)
Anti-HIV Agents, Nucleoside and Nucleotide Reverse Transcriptase Inhibitors (NRTI)
abacavir sulfate/lamivudine/zidovudine tabs 300mg; 150mg; 300mg
4 QL (60 EA per 30 days)
abacavir tabs 300mg 1 DESCOVY TABS 200MG; 25MG 4 QL (30 EA per 30 days) didanosine cpdr 125mg 1 didanosine cpdr 200mg 1 didanosine cpdr 250mg 1 didanosine cpdr 400mg 1 EPZICOM TABS 600MG; 300MG 4 QL (30 EA per 30 days) lamivudine/zidovudine tabs 150mg; 300mg 1 QL (60 EA per 30 days) lamivudine soln 10mg/ml 1 lamivudine tabs 150mg 1 lamivudine tabs 300mg 1 stavudine caps 15mg 1 stavudine caps 20mg 1 stavudine caps 30mg 1 stavudine caps 40mg 1 stavudine solr 1mg/ml 1 TRIUMEQ TABS 600MG; 50MG; 300MG 4 QL (30 EA per 30 days) TRIZIVIR TABS 300MG; 150MG; 300MG 4 QL (60 EA per 30 days) VIREAD POWD 40MG/GM 4 VIREAD TABS 200MG 4 VIREAD TABS 250MG 4 VIREAD TABS 300MG 4 zidovudine caps 100mg 1 zidovudine syrp 50mg/5ml 1 zidovudine tabs 300mg 1
Anti-HIV Agents, Other FUZEON INJ 90MG 4 QL (60 EA per 30 days) SELZENTRY TABS 150MG 4 SELZENTRY TABS 300MG 4 TYBOST TABS 150MG 2
Anti-HIV Agents, Protease Inhibitors

Page 46 of 121
Drug Name Drug Tier Requirements/Limits
APTIVUS CAPS 250MG 4 APTIVUS SOLN 100MG/ML 4 CRIXIVAN CAPS 200MG 2 CRIXIVAN CAPS 400MG 2 EVOTAZ TABS 300MG; 150MG 4 QL (30 EA per 30 days) INVIRASE CAPS 200MG 4 INVIRASE TABS 500MG 4 KALETRA TABS 200MG; 50MG 4 LEXIVA TABS 700MG 4 PREZCOBIX TABS 150MG; 800MG 4 QL (30 EA per 30 days) PREZISTA SUSP 100MG/ML 4 PREZISTA TABS 600MG 4 PREZISTA TABS 800MG 4 REYATAZ CAPS 150MG 4 REYATAZ CAPS 200MG 4 REYATAZ CAPS 300MG 4 VIRACEPT TABS 250MG 4 VIRACEPT TABS 625MG 4
Anti-influenza Agents amantadine hcl caps 100mg 1 amantadine hcl syrp 50mg/5ml 1 amantadine hcl tabs 100mg 1 rimantadine hcl tabs 100mg 1
Antiherpetic Agents acyclovir sodium inj 500mg 1 B/D acyclovir sodium inj 50mg/ml 1 B/D acyclovir caps 200mg 1 acyclovir oint 5% 1 acyclovir susp 200mg/5ml 1 acyclovir tabs 400mg 1 acyclovir tabs 800mg 1 DENAVIR CREA 1% 4 famciclovir tabs 125mg 1 famciclovir tabs 250mg 1 famciclovir tabs 500mg 1 trifluridine soln 1% 1 valacyclovir hcl tabs 1000mg 1 QL (120 EA per 30 days) valacyclovir hcl tabs 500mg 1 QL (120 EA per 30 days)
Anxiolytics Anxiolytics, Other
buspirone hcl tabs 10mg 1 buspirone hcl tabs 15mg 1 buspirone hcl tabs 30mg 1 buspirone hcl tabs 5mg 1 buspirone hcl tabs 7.5mg 1
Benzodiazepines alprazolam er tb24 1mg 1 QL (30 EA per 30 days) PA alprazolam er tb24 2mg 1 QL (150 EA per 30 days) PA alprazolam er tb24 3mg 1 QL (90 EA per 30 days) PA

Page 47 of 121
Drug Name Drug Tier Requirements/Limits
alprazolam intensol conc 1mg/ml 1 PA alprazolam odt tbdp 0.25mg 1 QL (120 EA per 30 days) PA alprazolam odt tbdp 0.5mg 1 QL (120 EA per 30 days) PA alprazolam odt tbdp 1mg 1 QL (120 EA per 30 days) PA alprazolam odt tbdp 2mg 1 QL (150 EA per 30 days) PA alprazolam xr tb24 0.5mg 1 QL (30 EA per 30 days) PA alprazolam xr tb24 1mg 1 QL (30 EA per 30 days) PA alprazolam xr tb24 2mg 1 QL (150 EA per 30 days) PA alprazolam xr tb24 3mg 1 QL (90 EA per 30 days) PA alprazolam tabs 0.25mg 1 QL (120 EA per 30 days) PA alprazolam tabs 0.5mg 1 QL (120 EA per 30 days) PA alprazolam tabs 1mg 1 QL (120 EA per 30 days) PA alprazolam tabs 2mg 1 QL (150 EA per 30 days) PA chlordiazepoxide hcl caps 10mg 1 QL (900 EA per 30 days) PA chlordiazepoxide hcl caps 25mg 1 QL (360 EA per 30 days) PA chlordiazepoxide hcl caps 5mg 1 QL (120 EA per 30 days) PA clorazepate dipotassium tabs 15mg 1 QL (180 EA per 30 days) clorazepate dipotassium tabs 3.75mg 1 QL (720 EA per 30 days) clorazepate dipotassium tabs 7.5mg 1 QL (360 EA per 30 days) diazepam intensol conc 5mg/ml 1 diazepam inj 5mg/ml 1 diazepam soln 1mg/ml 1 diazepam tabs 10mg 1 diazepam tabs 2mg 1 diazepam tabs 5mg 1 estazolam tabs 1mg 1 QL (30 EA per 30 days) PA estazolam tabs 2mg 1 QL (30 EA per 30 days) PA lorazepam intensol conc 2mg/ml 1 PA lorazepam inj 2mg/ml 1 PA lorazepam inj 4mg/ml 1 PA lorazepam tabs 0.5mg 1 QL (90 EA per 30 days) PA lorazepam tabs 1mg 1 QL (90 EA per 30 days) PA lorazepam tabs 2mg 1 QL (150 EA per 30 days) PA midazolam hcl inj 10mg/10ml 1 midazolam hcl inj 10mg/2ml 1 midazolam hcl inj 25mg/5ml 1 midazolam hcl inj 2mg/2ml 1 midazolam hcl inj 50mg/10ml 1 midazolam hcl inj 5mg/5ml 1 midazolam hcl inj 5mg/ml 1 oxazepam caps 10mg 1 QL (120 EA per 30 days) PA oxazepam caps 15mg 1 QL (120 EA per 30 days) PA oxazepam caps 30mg 1 QL (120 EA per 30 days) PA
Bipolar Agents Mood Stabilizers
lithium carbonate er tbcr 300mg 1 lithium carbonate er tbcr 450mg 1 lithium carbonate caps 150mg 1 lithium carbonate caps 300mg 1

Page 48 of 121
Drug Name Drug Tier Requirements/Limits
lithium carbonate caps 600mg 1 lithium carbonate tabs 300mg 1 lithium soln 8meq/5ml 1
Blood Glucose Regulators Antidiabetic Agents
acarbose tabs 100mg 1 acarbose tabs 25mg 1 acarbose tabs 50mg 1 BYDUREON PEN INJ 2MG 2 QL (4 EA per 28 days) ST BYDUREON INJ 2MG 2 QL (4 EA per 28 days) ST glimepiride tabs 1mg 1 QL (240 EA per 30 days) glimepiride tabs 2mg 1 QL (120 EA per 30 days) glimepiride tabs 4mg 1 QL (60 EA per 30 days) glipizide er tb24 10mg 1 QL (60 EA per 30 days) glipizide er tb24 2.5mg 1 QL (240 EA per 30 days) glipizide er tb24 5mg 1 QL (120 EA per 30 days) glipizide xl tb24 10mg 1 QL (60 EA per 30 days) glipizide xl tb24 2.5mg 1 QL (240 EA per 30 days) glipizide xl tb24 5mg 1 QL (120 EA per 30 days) glipizide/metformin hcl tabs 2.5mg; 250mg 1 QL (240 EA per 30 days) glipizide/metformin hcl tabs 2.5mg; 500mg 1 QL (120 EA per 30 days) glipizide/metformin hcl tabs 5mg; 500mg 1 QL (120 EA per 30 days) glipizide tabs 10mg 1 QL (120 EA per 30 days) glipizide tabs 5mg 1 QL (240 EA per 30 days) glyburide micronized tabs 1.5mg 1 QL (240 EA per 30 days) PA glyburide micronized tabs 3mg 1 QL (120 EA per 30 days) PA glyburide micronized tabs 6mg 1 QL (60 EA per 30 days) PA glyburide/metformin hcl tabs 1.25mg; 250mg 1 QL (240 EA per 30 days) PA glyburide/metformin hcl tabs 2.5mg; 500mg 1 QL (120 EA per 30 days) PA glyburide/metformin hcl tabs 5mg; 500mg 1 QL (120 EA per 30 days) PA glyburide tabs 1.25mg 1 QL (480 EA per 30 days) PA glyburide tabs 2.5mg 1 QL (240 EA per 30 days) PA glyburide tabs 5mg 1 QL (120 EA per 30 days) PA INVOKAMET TABS 150MG; 1000MG 2 QL (60 EA per 30 days) ST INVOKAMET TABS 150MG; 500MG 2 QL (60 EA per 30 days) ST INVOKAMET TABS 50MG; 1000MG 2 QL (60 EA per 30 days) ST INVOKAMET TABS 50MG; 500MG 2 QL (120 EA per 30 days) ST INVOKANA TABS 100MG 2 QL (90 EA per 30 days) ST INVOKANA TABS 300MG 2 QL (30 EA per 30 days) ST JANUMET XR TB24 1000MG; 100MG 2 QL (30 EA per 30 days) ST JANUMET XR TB24 1000MG; 50MG 2 QL (60 EA per 30 days) ST JANUMET XR TB24 500MG; 50MG 2 QL (60 EA per 30 days) ST JANUMET TABS 1000MG; 50MG 2 QL (60 EA per 30 days) ST JANUMET TABS 500MG; 50MG 2 QL (60 EA per 30 days) ST JANUVIA TABS 100MG 2 ST JANUVIA TABS 25MG 2 ST JANUVIA TABS 50MG 2 ST JARDIANCE TABS 10MG 2 QL (60 EA per 30 days) ST JARDIANCE TABS 25MG 2 QL (30 EA per 30 days) ST

Page 49 of 121
Drug Name Drug Tier Requirements/Limits
KOMBIGLYZE XR TB24 1000MG; 2.5MG 2 QL (60 EA per 30 days) ST KOMBIGLYZE XR TB24 1000MG; 5MG 2 QL (30 EA per 30 days) ST KOMBIGLYZE XR TB24 500MG; 5MG 2 QL (30 EA per 30 days) ST metformin hcl er tb24 500mg 1 QL (120 EA per 30 days) metformin hcl er tb24 750mg 1 QL (60 EA per 30 days) metformin hcl tabs 1000mg 1 QL (60 EA per 30 days) metformin hcl tabs 500mg 1 QL (150 EA per 30 days) metformin hcl tabs 850mg 1 QL (90 EA per 30 days) miglitol tabs 100mg 1 miglitol tabs 25mg 1 miglitol tabs 50mg 1 nateglinide tabs 120mg 1 nateglinide tabs 60mg 1 ONGLYZA TABS 2.5MG 2 ST ONGLYZA TABS 5MG 2 ST pioglitazone hcl-glimepiride tabs 2mg; 30mg 1 pioglitazone hcl-glimepiride tabs 4mg; 30mg 1 pioglitazone hcl/metformin hcl tabs 500mg; 15mg 1 QL (90 EA per 30 days) pioglitazone hcl/metformin hcl tabs 850mg; 15mg 1 QL (90 EA per 30 days) pioglitazone hcl tabs 15mg 1 QL (60 EA per 30 days) pioglitazone hcl tabs 30mg 1 QL (45 EA per 30 days) pioglitazone hcl tabs 45mg 1 QL (30 EA per 30 days) repaglinide/metformin hydrochloride tabs 500mg; 1mg 1 QL (150 EA per 30 days) repaglinide/metformin hydrochloride tabs 500mg; 2mg 1 QL (150 EA per 30 days) repaglinide tabs 0.5mg 1 repaglinide tabs 1mg 1 repaglinide tabs 2mg 1 SYMLINPEN 120 INJ 2700MCG/2.7ML 4 PA SYMLINPEN 60 INJ 1500MCG/1.5ML 4 PA SYNJARDY TABS 12.5MG; 1000MG 2 QL (60 EA per 30 days) ST SYNJARDY TABS 12.5MG; 500MG 2 QL (120 EA per 30 days) ST SYNJARDY TABS 5MG; 1000MG 2 QL (60 EA per 30 days) ST SYNJARDY TABS 5MG; 500MG 2 QL (120 EA per 30 days) ST tolazamide tabs 250mg 1 QL (240 EA per 30 days) tolazamide tabs 500mg 1 QL (120 EA per 30 days) tolbutamide tabs 500mg 1 QL (180 EA per 30 days) TRULICITY INJ 0.75MG/0.5ML 2 QL (2 ML per 28 days) ST TRULICITY INJ 1.5MG/0.5ML 2 QL (2 ML per 28 days) ST VICTOZA INJ 18MG/3ML 2 QL (9 ML per 30 days) ST
Glycemic Agents GLUCAGON EMERGENCY KIT INJ 1MG 2 PROGLYCEM SUSP 50MG/ML 4
Insulins HUMALOG KWIKPEN INJ 100UNIT/ML 2 HUMALOG KWIKPEN INJ 200UNIT/ML 2 HUMALOG MIX 50/50 KWIKPEN INJ 50UNIT/ML; 50UNIT/ML
2
HUMALOG MIX 50/50 INJ 50UNIT/ML; 50UNIT/ML 2

Page 50 of 121
Drug Name Drug Tier Requirements/Limits
HUMALOG MIX 75/25 KWIKPEN INJ 25UNIT/ML; 75UNIT/ML
2
HUMALOG MIX 75/25 INJ 25UNIT/ML; 75UNIT/ML 2 HUMALOG INJ 100UNIT/ML 2 HUMALOG INJ 100UNIT/ML 2 HUMULIN 70/30 KWIKPEN INJ 30UNIT/ML; 70UNIT/ML 2 HUMULIN 70/30 INJ 30UNIT/ML; 70UNIT/ML 2 HUMULIN N KWIKPEN INJ 100UNIT/ML 2 HUMULIN N INJ 100UNIT/ML 2 HUMULIN R U-500 (CONCENTRATED) INJ 500UNIT/ML 2 HUMULIN R U-500 KWIKPEN INJ 500UNIT/ML 2 HUMULIN R INJ 100UNIT/ML 2 LANTUS SOLOSTAR INJ 100UNIT/ML 2 LANTUS INJ 100UNIT/ML 2 LEVEMIR FLEXTOUCH INJ 100UNIT/ML 2 LEVEMIR INJ 100UNIT/ML 2 NOVOLIN 70/30 RELION INJ 30UNIT/ML; 70UNIT/ML 2 NOVOLIN 70/30 INJ 30UNIT/ML; 70UNIT/ML 2 NOVOLIN N RELION INJ 100UNIT/ML 2 NOVOLIN N INJ 100UNIT/ML 2 NOVOLIN R RELION INJ 100UNIT/ML 2 NOVOLIN R INJ 100UNIT/ML 2 NOVOLOG FLEXPEN INJ 100UNIT/ML 2 NOVOLOG MIX 70/30 PREFILLED FLEXPEN INJ 30UNIT/ML; 70UNIT/ML
2
NOVOLOG MIX 70/30 INJ 30UNIT/ML; 70UNIT/ML 2 NOVOLOG PENFILL INJ 100UNIT/ML 2 NOVOLOG INJ 100UNIT/ML 2 TOUJEO SOLOSTAR INJ 300UNIT/ML 2
Blood Products/Modifiers/Volume Expanders Anticoagulants
argatroban inj 125mg/125ml; 0.9% 1 argatroban inj 250mg/250ml; 0.9% 1 argatroban inj 50mg/50ml 1 ELIQUIS TABS 2.5MG 2 QL (60 EA per 30 days) ELIQUIS TABS 5MG 2 QL (90 EA per 30 days) enoxaparin sodium inj 100mg/ml 1 QL (35 ML per 90 days) enoxaparin sodium inj 120mg/0.8ml 1 QL (28 ML per 90 days) enoxaparin sodium inj 150mg/ml 4 QL (35 ML per 90 days) enoxaparin sodium inj 300mg/3ml 1 QL (105 ML per 90 days) enoxaparin sodium inj 30mg/0.3ml 1 QL (10.5 ML per 90 days) enoxaparin sodium inj 40mg/0.4ml 1 QL (14 ML per 90 days) enoxaparin sodium inj 60mg/0.6ml 1 QL (21 ML per 90 days) enoxaparin sodium inj 80mg/0.8ml 1 QL (28 ML per 90 days) fondaparinux sodium inj 10mg/0.8ml 4 QL (28 ML per 90 days) fondaparinux sodium inj 2.5mg/0.5ml 1 QL (17.5 ML per 90 days) fondaparinux sodium inj 5mg/0.4ml 4 QL (14 ML per 90 days) fondaparinux sodium inj 7.5mg/0.6ml 4 QL (21 ML per 90 days) FRAGMIN INJ 10000UNIT/ML 4 QL (35 ML per 90 days)

Page 51 of 121
Drug Name Drug Tier Requirements/Limits
FRAGMIN INJ 12500UNIT/0.5ML 4 QL (17.5 ML per 90 days) FRAGMIN INJ 15000UNIT/0.6ML 4 QL (21 ML per 90 days) FRAGMIN INJ 18000UNT/0.72ML 4 QL (25.3 ML per 90 days) FRAGMIN INJ 7500UNIT/0.3ML 4 QL (10.5 ML per 90 days) FRAGMIN INJ 95000UNIT/3.8ML 4 QL (22.8 ML per 90 days) heparin sodium/d5w inj 5%; 100unit/ml 1 heparin sodium/d5w inj 5%; 40unit/ml 1 heparin sodium/d5w inj 5%; 50unit/ml 1 heparin sodium/nacl 0.45% inj 100unit/ml; 0.45% 1 heparin sodium/nacl 0.45% inj 50unit/ml; 0.45% 1 heparin sodium/nacl 0.9% inj 2unit/ml; 0.9% 1 heparin sodium/nacl inj 4000unit/l; 0.9% 1 heparin sodium/sodium chloride 0.9% premix inj 2unit/ml; 0.9%
1
heparin sodium/sodium chloride 0.9% inj 2unit/ml; 0.9% 1 heparin sodium inj 10000unit/ml 1 heparin sodium inj 1000unit/ml 1 heparin sodium inj 20000unit/ml 1 heparin sodium inj 2000unit/ml 1 heparin sodium inj 2500unit/ml 1 heparin sodium inj 5000unit/0.5ml 1 heparin sodium inj 5000unit/ml 1 jantoven tabs 10mg 1 jantoven tabs 1mg 1 jantoven tabs 2.5mg 1 jantoven tabs 2mg 1 jantoven tabs 3mg 1 jantoven tabs 4mg 1 jantoven tabs 5mg 1 jantoven tabs 6mg 1 jantoven tabs 7.5mg 1 warfarin sodium tabs 10mg 1 warfarin sodium tabs 1mg 1 warfarin sodium tabs 2.5mg 1 warfarin sodium tabs 2mg 1 warfarin sodium tabs 3mg 1 warfarin sodium tabs 4mg 1 warfarin sodium tabs 5mg 1 warfarin sodium tabs 6mg 1 warfarin sodium tabs 7.5mg 1 XARELTO STARTER PACK TBPK 0 2 QL (102 EA per 365 days) XARELTO TABS 10MG 2 QL (30 EA per 30 days) XARELTO TABS 15MG 2 QL (60 EA per 30 days) XARELTO TABS 20MG 2 QL (30 EA per 30 days)
Blood Formation Modifiers anagrelide hydrochloride caps 0.5mg 1 anagrelide hydrochloride caps 1mg 1 ARANESP ALBUMIN FREE INJ 100MCG/0.5ML 4 PA ARANESP ALBUMIN FREE INJ 100MCG/ML 4 PA

Page 52 of 121
Drug Name Drug Tier Requirements/Limits
ARANESP ALBUMIN FREE INJ 150MCG/0.3ML 4 PA ARANESP ALBUMIN FREE INJ 200MCG/0.4ML 4 PA ARANESP ALBUMIN FREE INJ 200MCG/ML 4 PA ARANESP ALBUMIN FREE INJ 300MCG/0.6ML 4 PA ARANESP ALBUMIN FREE INJ 300MCG/ML 4 PA ARANESP ALBUMIN FREE INJ 500MCG/ML 4 PA ARANESP ALBUMIN FREE INJ 60MCG/ML 4 PA EPOGEN INJ 20000UNIT/ML 4 PA GRANIX INJ 300MCG/0.5ML 4 PA GRANIX INJ 480MCG/0.8ML 4 PA LEUKINE INJ 250MCG 4 PA MOZOBIL INJ 24MG/1.2ML 4 QL (38.4 ML per 365 days) PA NEULASTA ONPRO KIT INJ 6MG/0.6ML 4 PA NEULASTA INJ 6MG/0.6ML 4 PA NEUMEGA INJ 5MG 4 PA NEUPOGEN INJ 300MCG/0.5ML 4 PA NEUPOGEN INJ 300MCG/ML 4 PA NEUPOGEN INJ 480MCG/0.8ML 4 PA NEUPOGEN INJ 480MCG/1.6ML 4 PA NPLATE INJ 250MCG 4 PA NPLATE INJ 500MCG 4 PA PROCRIT INJ 20000UNIT/ML 4 PA PROCRIT INJ 40000UNIT/ML 4 PA PROMACTA TABS 12.5MG 4 PA PROMACTA TABS 25MG 4 PA PROMACTA TABS 50MG 4 PA PROMACTA TABS 75MG 4 PA ZARXIO INJ 300MCG/0.5ML 4 PA ZARXIO INJ 480MCG/0.8ML 4 PA
Coagulants aminocaproic acid inj 250mg/ml 1 aminocaproic acid syrp 25% 1 aminocaproic acid tabs 1000mg 1 aminocaproic acid tabs 500mg 1 tranexamic acid inj 1000mg/10ml 1 tranexamic acid tabs 650mg 1
Platelet Modifying Agents aspirin/dipyridamole cp12 25mg; 200mg 1 BRILINTA TABS 60MG 2 BRILINTA TABS 90MG 2 cilostazol tabs 100mg 1 cilostazol tabs 50mg 1 clopidogrel tabs 300mg 1 clopidogrel tabs 75mg 1 dipyridamole tabs 25mg 1 PA dipyridamole tabs 50mg 1 PA dipyridamole tabs 75mg 1 PA EFFIENT TABS 10MG 2 EFFIENT TABS 5MG 2

Page 53 of 121
Drug Name Drug Tier Requirements/Limits
ticlopidine hcl tabs 250mg 1 PA Cardiovascular Agents
Alpha-adrenergic Agonists clonidine hcl inj 100mcg/ml 1 clonidine hcl inj 500mcg/ml 1 clonidine hcl ptwk 0.1mg/24hr 1 clonidine hcl ptwk 0.2mg/24hr 1 clonidine hcl ptwk 0.3mg/24hr 1 clonidine hcl tabs 0.1mg 1 clonidine hcl tabs 0.2mg 1 clonidine hcl tabs 0.3mg 1 guanfacine hcl tabs 1mg 1 PA guanfacine hcl tabs 2mg 1 PA methyldopa/hydrochlorothiazide tabs 15mg; 250mg 1 PA methyldopa/hydrochlorothiazide tabs 25mg; 250mg 1 PA methyldopa tabs 250mg 1 PA methyldopa tabs 500mg 1 PA methyldopate hcl inj 250mg/5ml 1 midodrine hcl tabs 10mg 1 midodrine hcl tabs 2.5mg 1 midodrine hcl tabs 5mg 1 phenylephrine hcl inj 10mg/ml 1
Alpha-adrenergic Blocking Agents phenoxybenzamine hydrochloride caps 10mg 4 prazosin hcl caps 1mg 1 prazosin hcl caps 2mg 1 prazosin hcl caps 5mg 1
Angiotensin II Receptor Antagonists BENICAR HCT TABS 12.5MG; 20MG 2 BENICAR HCT TABS 12.5MG; 40MG 2 BENICAR HCT TABS 25MG; 40MG 2 BENICAR TABS 20MG 2 BENICAR TABS 40MG 2 BENICAR TABS 5MG 2 candesartan cilexetil/hydrochlorothiazide tabs 16mg; 12.5mg 1 candesartan cilexetil/hydrochlorothiazide tabs 32mg; 12.5mg 1 candesartan cilexetil/hydrochlorothiazide tabs 32mg; 25mg 1 candesartan cilexetil tabs 16mg 1 candesartan cilexetil tabs 32mg 1 candesartan cilexetil tabs 4mg 1 candesartan cilexetil tabs 8mg 1 eprosartan mesylate tabs 600mg 1 irbesartan/hydrochlorothiazide tabs 12.5mg; 150mg 1 irbesartan/hydrochlorothiazide tabs 12.5mg; 300mg 1 irbesartan tabs 150mg 1 irbesartan tabs 300mg 1 irbesartan tabs 75mg 1 losartan potassium/hydrochlorothiazide tabs 12.5mg; 100mg 1 losartan potassium/hydrochlorothiazide tabs 12.5mg; 50mg 1

Page 54 of 121
Drug Name Drug Tier Requirements/Limits
losartan potassium/hydrochlorothiazide tabs 25mg; 100mg 1 losartan potassium tabs 100mg 1 losartan potassium tabs 25mg 1 losartan potassium tabs 50mg 1 telmisartan/amlodipine tabs 10mg; 40mg 1 telmisartan/amlodipine tabs 10mg; 80mg 1 telmisartan/amlodipine tabs 5mg; 40mg 1 telmisartan/amlodipine tabs 5mg; 80mg 1 telmisartan/hydrochlorothiazide tabs 12.5mg; 40mg 1 telmisartan/hydrochlorothiazide tabs 12.5mg; 80mg 1 telmisartan/hydrochlorothiazide tabs 25mg; 80mg 1 telmisartan tabs 20mg 1 telmisartan tabs 40mg 1 telmisartan tabs 80mg 1 valsartan/hydrochlorothiazide tabs 12.5mg; 160mg 1 valsartan/hydrochlorothiazide tabs 12.5mg; 320mg 1 valsartan/hydrochlorothiazide tabs 12.5mg; 80mg 1 valsartan/hydrochlorothiazide tabs 25mg; 160mg 1 valsartan/hydrochlorothiazide tabs 25mg; 320mg 1 valsartan tabs 160mg 1 valsartan tabs 320mg 1 valsartan tabs 40mg 1 valsartan tabs 80mg 1
Angiotensin-converting Enzyme (ACE) Inhibitors benazepril hcl/hydrochlorothiazide tabs 10mg; 12.5mg 1 benazepril hcl/hydrochlorothiazide tabs 20mg; 12.5mg 1 benazepril hcl/hydrochlorothiazide tabs 20mg; 25mg 1 benazepril hcl/hydrochlorothiazide tabs 5mg; 6.25mg 1 benazepril hcl tabs 10mg 1 benazepril hcl tabs 20mg 1 benazepril hcl tabs 40mg 1 benazepril hcl tabs 5mg 1 captopril/hydrochlorothiazide tabs 25mg; 15mg 1 captopril/hydrochlorothiazide tabs 25mg; 25mg 1 captopril/hydrochlorothiazide tabs 50mg; 15mg 1 captopril/hydrochlorothiazide tabs 50mg; 25mg 1 captopril tabs 100mg 1 captopril tabs 12.5mg 1 captopril tabs 25mg 1 captopril tabs 50mg 1 enalapril maleate/hydrochlorothiazide tabs 10mg; 25mg 1 enalapril maleate/hydrochlorothiazide tabs 5mg; 12.5mg 1 enalapril maleate tabs 10mg 1 enalapril maleate tabs 2.5mg 1 enalapril maleate tabs 20mg 1 enalapril maleate tabs 5mg 1 enalaprilat inj 1.25mg/ml 1 fosinopril sodium/hydrochlorothiazide tabs 10mg; 12.5mg 1 fosinopril sodium/hydrochlorothiazide tabs 20mg; 12.5mg 1

Page 55 of 121
Drug Name Drug Tier Requirements/Limits
fosinopril sodium tabs 10mg 1 fosinopril sodium tabs 20mg 1 fosinopril sodium tabs 40mg 1 lisinopril/hydrochlorothiazide tabs 12.5mg; 10mg 1 lisinopril/hydrochlorothiazide tabs 12.5mg; 20mg 1 lisinopril/hydrochlorothiazide tabs 25mg; 20mg 1 lisinopril tabs 10mg 1 lisinopril tabs 2.5mg 1 lisinopril tabs 20mg 1 lisinopril tabs 30mg 1 lisinopril tabs 40mg 1 lisinopril tabs 5mg 1 moexipril hcl tabs 15mg 1 moexipril hcl tabs 7.5mg 1 moexipril/hydrochlorothiazide tabs 12.5mg; 15mg 1 moexipril/hydrochlorothiazide tabs 12.5mg; 7.5mg 1 moexipril/hydrochlorothiazide tabs 25mg; 15mg 1 perindopril erbumine tabs 2mg 1 perindopril erbumine tabs 4mg 1 perindopril erbumine tabs 8mg 1 quinapril hcl tabs 10mg 1 quinapril hcl tabs 20mg 1 quinapril hcl tabs 40mg 1 quinapril hcl tabs 5mg 1 quinapril/hydrochlorothiazide tabs 12.5mg; 10mg 1 quinapril/hydrochlorothiazide tabs 12.5mg; 20mg 1 quinapril/hydrochlorothiazide tabs 25mg; 20mg 1 ramipril caps 1.25mg 1 ramipril caps 10mg 1 ramipril caps 2.5mg 1 ramipril caps 5mg 1 trandolapril/verapamil hcl er tbcr 1mg; 240mg 1 trandolapril/verapamil hcl er tbcr 2mg; 180mg 1 trandolapril/verapamil hcl er tbcr 2mg; 240mg 1 trandolapril/verapamil hcl er tbcr 4mg; 240mg 1 trandolapril/verapamil hcl tbcr 1mg; 240mg 1 trandolapril/verapamil hcl tbcr 2mg; 180mg 1 trandolapril/verapamil hcl tbcr 2mg; 240mg 1 trandolapril/verapamil hcl tbcr 4mg; 240mg 1 trandolapril tabs 1mg 1 trandolapril tabs 2mg 1 trandolapril tabs 4mg 1
Antiarrhythmics amiodarone hcl inj 50mg/ml 1 amiodarone hcl inj 50mg/ml 1 amiodarone hcl inj 900mg/18ml 1 amiodarone hcl tabs 100mg 1 amiodarone hcl tabs 200mg 1 amiodarone hcl tabs 400mg 1

Page 56 of 121
Drug Name Drug Tier Requirements/Limits
disopyramide phosphate caps 100mg 1 PA disopyramide phosphate caps 150mg 1 PA dofetilide caps 125mcg 1 dofetilide caps 250mcg 1 dofetilide caps 500mcg 1 flecainide acetate tabs 100mg 1 flecainide acetate tabs 150mg 1 flecainide acetate tabs 50mg 1 ibutilide fumarate inj 1mg/10ml 1 lidocaine hcl in d5w inj 5%; 4mg/ml 1 lidocaine hcl in d5w inj 5%; 8mg/ml 1 lidocaine hcl/dextrose inj 5%; 4mg/ml 1 lidocaine hcl/dextrose inj 5%; 8mg/ml 1 lidocaine hcl inj 10mg/ml 1 lidocaine hcl inj 20mg/ml 1 mexiletine hcl caps 150mg 1 mexiletine hcl caps 200mg 1 mexiletine hcl caps 250mg 1 MULTAQ TABS 400MG 2 pacerone tabs 100mg 1 pacerone tabs 200mg 1 pacerone tabs 400mg 1 procainamide hcl inj 100mg/ml 1 procainamide hcl inj 500mg/ml 1 propafenone hcl er cp12 225mg 1 propafenone hcl er cp12 325mg 1 propafenone hcl er cp12 425mg 1 propafenone hcl tabs 150mg 1 propafenone hcl tabs 225mg 1 propafenone hcl tabs 300mg 1 quinidine gluconate cr tbcr 324mg 1 quinidine gluconate er tbcr 324mg 1 quinidine gluconate inj 80mg/ml 1 quinidine sulfate tabs 200mg 1 quinidine sulfate tabs 300mg 1 sorine tabs 120mg 1 sorine tabs 160mg 1 sorine tabs 240mg 1 sorine tabs 80mg 1 sotalol hcl (af) tabs 120mg 1 sotalol hcl (af) tabs 160mg 1 sotalol hcl (af) tabs 80mg 1 sotalol hcl tabs 120mg 1 sotalol hcl tabs 160mg 1 sotalol hcl tabs 240mg 1 sotalol hcl tabs 80mg 1 sotalol hydrochloride inj 150mg/10ml 4
Beta-adrenergic Blocking Agents acebutolol hcl caps 200mg 1

Page 57 of 121
Drug Name Drug Tier Requirements/Limits
acebutolol hcl caps 400mg 1 atenolol/chlorthalidone tabs 100mg; 25mg 1 atenolol/chlorthalidone tabs 50mg; 25mg 1 atenolol tabs 100mg 1 atenolol tabs 25mg 1 atenolol tabs 50mg 1 betaxolol hcl tabs 10mg 1 betaxolol hcl tabs 20mg 1 bisoprolol fumarate/hydrochlorothiazide tabs 10mg; 6.25mg 1 bisoprolol fumarate/hydrochlorothiazide tabs 2.5mg; 6.25mg 1 bisoprolol fumarate/hydrochlorothiazide tabs 5mg; 6.25mg 1 bisoprolol fumarate tabs 10mg 1 bisoprolol fumarate tabs 5mg 1 BYSTOLIC TABS 10MG 2 BYSTOLIC TABS 2.5MG 2 BYSTOLIC TABS 20MG 2 BYSTOLIC TABS 5MG 2 carvedilol tabs 12.5mg 1 carvedilol tabs 25mg 1 carvedilol tabs 3.125mg 1 carvedilol tabs 6.25mg 1 esmolol hcl inj 100mg/10ml 1 labetalol hcl inj 5mg/ml 1 labetalol hcl tabs 100mg 1 labetalol hcl tabs 200mg 1 labetalol hcl tabs 300mg 1 metoprolol succinate er tb24 100mg 1 metoprolol succinate er tb24 200mg 1 metoprolol succinate er tb24 25mg 1 metoprolol succinate er tb24 50mg 1 metoprolol tartrate inj 1mg/ml 1 metoprolol tartrate inj 1mg/ml 1 metoprolol tartrate tabs 100mg 1 metoprolol tartrate tabs 25mg 1 metoprolol tartrate tabs 37.5mg 1 metoprolol tartrate tabs 50mg 1 metoprolol tartrate tabs 75mg 1 metoprolol/hydrochlorothiazide tabs 25mg; 100mg 1 metoprolol/hydrochlorothiazide tabs 25mg; 50mg 1 metoprolol/hydrochlorothiazide tabs 50mg; 100mg 1 nadolol/bendroflumethiazide tabs 5mg; 40mg 1 nadolol/bendroflumethiazide tabs 5mg; 80mg 1 nadolol tabs 20mg 1 nadolol tabs 40mg 1 nadolol tabs 80mg 1 pindolol tabs 10mg 1 pindolol tabs 5mg 1 propranolol hcl er cp24 120mg 1 propranolol hcl er cp24 160mg 1

Page 58 of 121
Drug Name Drug Tier Requirements/Limits
propranolol hcl er cp24 60mg 1 propranolol hcl er cp24 80mg 1 propranolol hcl inj 1mg/ml 1 propranolol hcl soln 20mg/5ml 1 propranolol hcl soln 40mg/5ml 1 propranolol hcl tabs 10mg 1 propranolol hcl tabs 20mg 1 propranolol hcl tabs 40mg 1 propranolol hcl tabs 60mg 1 propranolol hcl tabs 80mg 1 propranolol/hydrochlorothiazide tabs 25mg; 40mg 1 propranolol/hydrochlorothiazide tabs 25mg; 80mg 1 timolol maleate tabs 10mg 1 timolol maleate tabs 20mg 1 timolol maleate tabs 5mg 1
Calcium Channel Blocking Agents afeditab cr tb24 30mg 1 afeditab cr tb24 60mg 1 amlodipine besylate/atorvastatin calcium tabs 10mg; 10mg 1 amlodipine besylate/atorvastatin calcium tabs 10mg; 20mg 1 amlodipine besylate/atorvastatin calcium tabs 10mg; 40mg 1 amlodipine besylate/atorvastatin calcium tabs 10mg; 80mg 1 amlodipine besylate/atorvastatin calcium tabs 2.5mg; 10mg 1 amlodipine besylate/atorvastatin calcium tabs 2.5mg; 20mg 1 amlodipine besylate/atorvastatin calcium tabs 2.5mg; 40mg 1 amlodipine besylate/atorvastatin calcium tabs 5mg; 10mg 1 amlodipine besylate/atorvastatin calcium tabs 5mg; 20mg 1 amlodipine besylate/atorvastatin calcium tabs 5mg; 40mg 1 amlodipine besylate/atorvastatin calcium tabs 5mg; 80mg 1 amlodipine besylate/benazepril hydrochloride caps 10mg; 20mg
1
amlodipine besylate/benazepril hydrochloride caps 10mg; 40mg
1
amlodipine besylate/benazepril hydrochloride caps 2.5mg; 10mg
1
amlodipine besylate/benazepril hydrochloride caps 5mg; 10mg1 amlodipine besylate/benazepril hydrochloride caps 5mg; 20mg1 amlodipine besylate/benazepril hydrochloride caps 5mg; 40mg1 amlodipine besylate/valsartan tabs 10mg; 160mg 1 amlodipine besylate/valsartan tabs 10mg; 320mg 1 amlodipine besylate/valsartan tabs 5mg; 160mg 1 amlodipine besylate/valsartan tabs 5mg; 320mg 1 amlodipine besylate tabs 10mg 1 amlodipine besylate tabs 2.5mg 1 amlodipine besylate tabs 5mg 1 amlodipine/valsartan/hctz tabs 10mg; 12.5mg; 160mg 1 amlodipine/valsartan/hctz tabs 10mg; 25mg; 160mg 1 amlodipine/valsartan/hctz tabs 10mg; 25mg; 320mg 1 amlodipine/valsartan/hctz tabs 5mg; 12.5mg; 160mg 1

Page 59 of 121
Drug Name Drug Tier Requirements/Limits
amlodipine/valsartan/hctz tabs 5mg; 25mg; 160mg 1 cartia xt cp24 120mg 1 cartia xt cp24 180mg 1 cartia xt cp24 240mg 1 cartia xt cp24 300mg 1 dilt-xr cp24 120mg 1 dilt-xr cp24 180mg 1 dilt-xr cp24 240mg 1 diltiazem cd cp24 120mg 1 diltiazem cd cp24 180mg 1 diltiazem cd cp24 240mg 1 diltiazem cd cp24 300mg 1 diltiazem hcl cd cp24 360mg 1 diltiazem hcl er cp12 120mg 1 diltiazem hcl er cp12 60mg 1 diltiazem hcl er cp12 90mg 1 diltiazem hcl er cp24 120mg 1 diltiazem hcl er cp24 120mg 1 diltiazem hcl er cp24 120mg 1 diltiazem hcl er cp24 180mg 1 diltiazem hcl er cp24 180mg 1 diltiazem hcl er cp24 180mg 1 diltiazem hcl er cp24 240mg 1 diltiazem hcl er cp24 240mg 1 diltiazem hcl er cp24 240mg 1 diltiazem hcl er cp24 300mg 1 diltiazem hcl er cp24 300mg 1 diltiazem hcl er cp24 360mg 1 diltiazem hcl er cp24 360mg 1 diltiazem hcl er cp24 420mg 1 diltiazem hcl er tb24 180mg 1 diltiazem hcl er tb24 240mg 1 diltiazem hcl er tb24 300mg 1 diltiazem hcl er tb24 360mg 1 diltiazem hcl er tb24 420mg 1 diltiazem hcl inj 100mg 1 diltiazem hcl inj 125mg/25ml 1 diltiazem hcl inj 25mg/5ml 1 diltiazem hcl inj 50mg/10ml 1 diltiazem hcl tabs 120mg 1 diltiazem hcl tabs 30mg 1 diltiazem hcl tabs 60mg 1 diltiazem hcl tabs 90mg 1 felodipine er tb24 10mg 1 felodipine er tb24 2.5mg 1 felodipine er tb24 5mg 1 matzim la tb24 180mg 1 matzim la tb24 240mg 1 matzim la tb24 300mg 1

Page 60 of 121
Drug Name Drug Tier Requirements/Limits
matzim la tb24 360mg 1 matzim la tb24 420mg 1 nifedical xl tb24 30mg 1 nifedical xl tb24 60mg 1 nifedipine er tb24 30mg 1 nifedipine er tb24 30mg 1 nifedipine er tb24 60mg 1 nifedipine er tb24 60mg 1 nifedipine er tb24 90mg 1 nifedipine er tb24 90mg 1 nimodipine caps 30mg 4 nisoldipine er tb24 25.5mg 1 nisoldipine tb24 17mg 1 nisoldipine tb24 20mg 1 nisoldipine tb24 30mg 1 nisoldipine tb24 34mg 1 nisoldipine tb24 40mg 1 nisoldipine tb24 8.5mg 1 NYMALIZE SOLN 60MG/20ML 4 taztia xt cp24 120mg 1 taztia xt cp24 180mg 1 taztia xt cp24 240mg 1 taztia xt cp24 300mg 1 taztia xt cp24 360mg 1 verapamil hcl er cp24 100mg 1 verapamil hcl er cp24 120mg 1 verapamil hcl er cp24 180mg 1 verapamil hcl er cp24 200mg 1 verapamil hcl er cp24 240mg 1 verapamil hcl er cp24 300mg 1 verapamil hcl er tbcr 120mg 1 verapamil hcl er tbcr 180mg 1 verapamil hcl er tbcr 240mg 1 verapamil hcl sr cp24 120mg 1 verapamil hcl sr cp24 180mg 1 verapamil hcl sr cp24 240mg 1 verapamil hcl sr cp24 360mg 1 verapamil hcl inj 2.5mg/ml 1 verapamil hcl tabs 120mg 1 verapamil hcl tabs 40mg 1 verapamil hcl tabs 80mg 1
Cardiovascular Agents, Other DEMSER CAPS 250MG 4 digitek tabs 0.125mg 1 QL (30 EA per 30 days) digitek tabs 0.25mg 1 PA digoxin inj 0.25mg/ml 1 PA digoxin soln 0.05mg/ml 1 PA digoxin tabs 125mcg 1 QL (30 EA per 30 days) digoxin tabs 250mcg 1 PA

Page 61 of 121
Drug Name Drug Tier Requirements/Limits
digox tabs 125mcg 1 QL (30 EA per 30 days) digox tabs 250mcg 1 PA dobutamine hcl/d5w inj 5%; 1mg/ml 1 B/D dobutamine hcl/d5w inj 5%; 2mg/ml 1 B/D dobutamine hcl/d5w inj 5%; 4mg/ml 1 B/D dobutamine hcl inj 500mg/40ml 1 B/D dobutamine/dextrose 5% inj 5%; 2mg/ml 1 B/D dobutamine/dextrose 5% inj 5%; 4mg/ml 1 B/D dopamine hcl-dextrose 5% inj 5%; 0.8mg/ml 1 B/D dopamine hcl/dextrose 5% inj 5%; 1.6mg/ml 1 B/D dopamine hcl inj 160mg/ml 1 B/D dopamine hcl inj 40mg/ml 1 B/D dopamine hcl inj 80mg/ml 1 B/D dopamine/d5w inj 5%; 0.8mg/ml 1 B/D dopamine/d5w inj 5%; 1.6mg/ml 1 B/D dopamine/d5w inj 5%; 3.2mg/ml 1 B/D mannitol inj 10% 1 mannitol inj 15% 1 mannitol inj 20% 1 mannitol inj 25% 1 mannitol inj 5% 1 milrinone in dextrose inj 5%; 20mg/100ml 1 B/D milrinone in dextrose inj 5%; 40mg/200ml 1 B/D milrinone lactate inj 10mg/10ml 1 B/D milrinone lactate inj 20mg/20ml 1 B/D milrinone lactate inj 50mg/50ml 1 B/D norepinephrine bitartrate inj 1mg/ml 1 NORTHERA CAPS 100MG 4 PA NORTHERA CAPS 200MG 4 PA NORTHERA CAPS 300MG 4 PA osmitrol viaflex inj 10% 1 osmitrol viaflex inj 15% 1 osmitrol viaflex inj 20% 1 osmitrol viaflex inj 5% 1 PRALUENT INJ 150MG/ML 4 QL (2 ML per 28 days) PA PRALUENT INJ 150MG/ML 4 QL (2 ML per 28 days) PA PRALUENT INJ 75MG/ML 4 QL (2 ML per 28 days) PA PRALUENT INJ 75MG/ML 4 QL (2 ML per 28 days) PA RANEXA TB12 1000MG 2 RANEXA TB12 500MG 2 REPATHA PUSHTRONEX SYSTEM INJ 420MG/3.5ML 4 QL (3.5 ML per 28 days) PA REPATHA SURECLICK INJ 140MG/ML 4 QL (3 ML per 28 days) PA REPATHA INJ 140MG/ML 4 QL (3 ML per 28 days) PA
Diuretics, Carbonic Anhydrase Inhibitors acetazolamide sodium inj 500mg 1 acetazolamide tabs 125mg 1 acetazolamide tabs 250mg 1
Diuretics, Loop bumetanide inj 0.25mg/ml 1

Page 62 of 121
Drug Name Drug Tier Requirements/Limits
bumetanide tabs 0.5mg 1 bumetanide tabs 1mg 1 bumetanide tabs 2mg 1 EDECRIN TABS 25MG 4 ethacrynic acid tabs 25mg 1 furosemide inj 10mg/ml 1 furosemide inj 10mg/ml 1 furosemide soln 10mg/ml 1 furosemide soln 8mg/ml 1 furosemide tabs 20mg 1 furosemide tabs 40mg 1 furosemide tabs 80mg 1 torsemide inj 20mg/2ml 1 torsemide inj 50mg/5ml 1 torsemide tabs 100mg 1 torsemide tabs 10mg 1 torsemide tabs 20mg 1 torsemide tabs 5mg 1
Diuretics, Potassium-sparing amiloride hcl tabs 5mg 1 amiloride/hydrochlorothiazide tabs 5mg; 50mg 1 eplerenone tabs 25mg 1 eplerenone tabs 50mg 1 spironolactone/hydrochlorothiazide tabs 25mg; 25mg 1 spironolactone tabs 100mg 1 spironolactone tabs 25mg 1 spironolactone tabs 50mg 1 triamterene/hydrochlorothiazide caps 25mg; 37.5mg 1 triamterene/hydrochlorothiazide caps 25mg; 50mg 1 triamterene/hydrochlorothiazide tabs 25mg; 37.5mg 1 triamterene/hydrochlorothiazide tabs 50mg; 75mg 1
Diuretics, Thiazide chlorothiazide sodium inj 500mg 1 chlorothiazide tabs 250mg 1 chlorothiazide tabs 500mg 1 chlorthalidone tabs 25mg 1 chlorthalidone tabs 50mg 1 hydrochlorothiazide caps 12.5mg 1 hydrochlorothiazide tabs 12.5mg 1 hydrochlorothiazide tabs 25mg 1 hydrochlorothiazide tabs 50mg 1 indapamide tabs 1.25mg 1 indapamide tabs 2.5mg 1 methyclothiazide tabs 5mg 1 metolazone tabs 10mg 1 metolazone tabs 2.5mg 1 metolazone tabs 5mg 1
Dyslipidemics, Fibric Acid Derivatives fenofibrate micronized caps 134mg 1

Page 63 of 121
Drug Name Drug Tier Requirements/Limits
fenofibrate micronized caps 200mg 1 fenofibrate micronized caps 67mg 1 fenofibrate caps 130mg 1 fenofibrate caps 150mg 1 fenofibrate caps 43mg 1 fenofibrate caps 50mg 1 fenofibrate tabs 120mg 1 fenofibrate tabs 145mg 1 fenofibrate tabs 160mg 1 fenofibrate tabs 40mg 1 fenofibrate tabs 48mg 1 fenofibrate tabs 54mg 1 fenofibric acid dr cpdr 135mg 1 fenofibric acid dr cpdr 45mg 1 fenofibric acid tabs 105mg 1 fenofibric acid tabs 35mg 1 gemfibrozil tabs 600mg 1
Dyslipidemics, HMG CoA Reductase Inhibitors atorvastatin calcium tabs 10mg 1 atorvastatin calcium tabs 20mg 1 atorvastatin calcium tabs 40mg 1 atorvastatin calcium tabs 80mg 1 fluvastatin sodium er tb24 80mg 1 fluvastatin caps 20mg 1 fluvastatin caps 40mg 1 lovastatin tabs 10mg 1 lovastatin tabs 20mg 1 lovastatin tabs 40mg 1 pravastatin sodium tabs 10mg 1 pravastatin sodium tabs 20mg 1 pravastatin sodium tabs 40mg 1 pravastatin sodium tabs 80mg 1 rosuvastatin calcium tabs 10mg 1 rosuvastatin calcium tabs 20mg 1 rosuvastatin calcium tabs 40mg 1 rosuvastatin calcium tabs 5mg 1 simvastatin tabs 10mg 1 simvastatin tabs 20mg 1 simvastatin tabs 40mg 1 simvastatin tabs 5mg 1 simvastatin tabs 80mg 1 PA
Dyslipidemics, Other cholestyramine light pack 4gm 1 cholestyramine light powd 4gm/dose 1 colestipol hcl gran 5gm 1 colestipol hcl pack 5gm 1 colestipol hcl tabs 1gm 1 JUXTAPID CAPS 10MG 4 QL (30 EA per 30 days) PA JUXTAPID CAPS 20MG 4 QL (30 EA per 30 days) PA

Page 64 of 121
Drug Name Drug Tier Requirements/Limits
JUXTAPID CAPS 30MG 4 QL (30 EA per 30 days) PA JUXTAPID CAPS 40MG 4 QL (30 EA per 30 days) PA JUXTAPID CAPS 5MG 4 QL (30 EA per 30 days) PA JUXTAPID CAPS 60MG 4 QL (30 EA per 30 days) PA KYNAMRO INJ 200MG/ML 4 QL (4 ML per 28 days) PA niacin er tbcr 1000mg 1 niacin er tbcr 500mg 1 niacin er tbcr 750mg 1 niacor tabs 500mg 1 omega-3-acid ethyl esters caps 375mg; 465mg; 1gm 1 prevalite pack 4gm 1 prevalite powd 4gm/dose 1 WELCHOL PACK 3.75GM 2 WELCHOL TABS 625MG 2 ZETIA TABS 10MG 2
Vasodilators, Direct-acting Arterial/Venous BIDIL TABS 37.5MG; 20MG 2 ISORDIL TITRADOSE TABS 40MG 4 isosorbide dinitrate er tbcr 40mg 1 isosorbide dinitrate tabs 10mg 1 isosorbide dinitrate tabs 20mg 1 isosorbide dinitrate tabs 30mg 1 isosorbide dinitrate tabs 5mg 1 isosorbide mononitrate er tb24 120mg 1 isosorbide mononitrate er tb24 30mg 1 isosorbide mononitrate er tb24 60mg 1 isosorbide mononitrate tabs 10mg 1 isosorbide mononitrate tabs 20mg 1 minitran pt24 0.1mg/hr 1 minitran pt24 0.2mg/hr 1 minitran pt24 0.4mg/hr 1 minitran pt24 0.6mg/hr 1 nitroglycerin in 5% dextrose inj 5%; 200mcg/ml 1 nitroglycerin in 5% dextrose inj 5%; 400mcg/ml 1 nitroglycerin in dextrose 5% inj 5%; 100mcg/ml 1 nitroglycerin in dextrose 5% inj 5%; 200mcg/ml 1 nitroglycerin in dextrose 5% inj 5%; 400mcg/ml 1 nitroglycerin lingual aers 400mcg/spray 1 nitroglycerin lingual soln 0.4mg/spray 1 nitroglycerin transdermal pt24 0.1mg/hr 1 nitroglycerin transdermal pt24 0.2mg/hr 1 nitroglycerin transdermal pt24 0.4mg/hr 1 nitroglycerin transdermal pt24 0.6mg/hr 1 nitroglycerin inj 5mg/ml 1 NITROSTAT SUBL 0.3MG 2 NITROSTAT SUBL 0.4MG 2 NITROSTAT SUBL 0.6MG 2
Vasodilators, Direct-acting Arterial hydralazine hcl inj 20mg/ml 1

Page 65 of 121
Drug Name Drug Tier Requirements/Limits
hydralazine hcl tabs 100mg 1 hydralazine hcl tabs 10mg 1 hydralazine hcl tabs 25mg 1 hydralazine hcl tabs 50mg 1
Central Nervous System Agents Attention Deficit Hyperactivity Disorder Agents, Amphetamines
amphetamine/dextroamphetamine cp24 1.25mg; 1.25mg; 1.25mg; 1.25mg
1 QL (30 EA per 30 days) PA
amphetamine/dextroamphetamine cp24 2.5mg; 2.5mg; 2.5mg; 2.5mg
1 QL (30 EA per 30 days) PA
amphetamine/dextroamphetamine cp24 3.75mg; 3.75mg; 3.75mg; 3.75mg
1 QL (30 EA per 30 days) PA
amphetamine/dextroamphetamine cp24 5mg; 5mg; 5mg; 5mg 1 QL (30 EA per 30 days) PA amphetamine/dextroamphetamine cp24 6.25mg; 6.25mg; 6.25mg; 6.25mg
1 QL (30 EA per 30 days) PA
amphetamine/dextroamphetamine cp24 7.5mg; 7.5mg; 7.5mg; 7.5mg
1 QL (30 EA per 30 days) PA
amphetamine/dextroamphetamine tabs 1.25mg; 1.25mg; 1.25mg; 1.25mg
1 QL (90 EA per 30 days)
amphetamine/dextroamphetamine tabs 1.875mg; 1.875mg; 1.875mg; 1.875mg
1 QL (90 EA per 30 days)
amphetamine/dextroamphetamine tabs 2.5mg; 2.5mg; 2.5mg; 2.5mg
1 QL (90 EA per 30 days)
amphetamine/dextroamphetamine tabs 3.125mg; 3.125mg; 3.125mg; 3.125mg
1 QL (90 EA per 30 days)
amphetamine/dextroamphetamine tabs 3.75mg; 3.75mg; 3.75mg; 3.75mg
1 QL (90 EA per 30 days)
amphetamine/dextroamphetamine tabs 5mg; 5mg; 5mg; 5mg 1 QL (90 EA per 30 days) amphetamine/dextroamphetamine tabs 7.5mg; 7.5mg; 7.5mg; 7.5mg
1 QL (90 EA per 30 days)
dextroamphetamine sulfate er cp24 10mg 1 QL (180 EA per 30 days) PA dextroamphetamine sulfate er cp24 15mg 1 QL (120 EA per 30 days) PA dextroamphetamine sulfate er cp24 5mg 1 QL (60 EA per 30 days) PA dextroamphetamine sulfate soln 5mg/5ml 1 QL (1800 ML per 30 days) PA dextroamphetamine sulfate tabs 10mg 1 QL (180 EA per 30 days) PA dextroamphetamine sulfate tabs 5mg 1 QL (90 EA per 30 days) PA
Attention Deficit Hyperactivity Disorder Agents, Non-amphetamines
clonidine hcl er tb12 0.1mg 1 dexmethylphenidate hcl er cp24 10mg 1 QL (30 EA per 30 days) PA dexmethylphenidate hcl er cp24 15mg 1 QL (30 EA per 30 days) PA dexmethylphenidate hcl er cp24 20mg 1 QL (60 EA per 30 days) PA dexmethylphenidate hcl er cp24 30mg 1 QL (30 EA per 30 days) PA dexmethylphenidate hcl er cp24 40mg 1 QL (30 EA per 30 days) PA dexmethylphenidate hcl er cp24 5mg 1 QL (30 EA per 30 days) PA dexmethylphenidate hcl tabs 10mg 1 QL (60 EA per 30 days) PA dexmethylphenidate hcl tabs 2.5mg 1 QL (60 EA per 30 days) PA dexmethylphenidate hcl tabs 5mg 1 QL (60 EA per 30 days) PA guanfacine er tb24 1mg 1

Page 66 of 121
Drug Name Drug Tier Requirements/Limits
guanfacine er tb24 2mg 1 guanfacine er tb24 3mg 1 guanfacine er tb24 4mg 1 metadate er tbcr 20mg 1 QL (90 EA per 30 days) PA methylphenidate hcl cd cpcr 10mg 1 QL (30 EA per 30 days) PA methylphenidate hcl cd cpcr 20mg 1 QL (30 EA per 30 days) PA methylphenidate hcl cd cpcr 30mg 1 QL (30 EA per 30 days) PA methylphenidate hcl cd cpcr 40mg 1 QL (30 EA per 30 days) PA methylphenidate hcl cd cpcr 50mg 1 QL (30 EA per 30 days) PA methylphenidate hcl cd cpcr 60mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er cp24 20mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er cp24 30mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er cp24 40mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er tb24 18mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er tb24 27mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er tb24 36mg 1 QL (60 EA per 30 days) PA methylphenidate hcl er tb24 54mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er tbcr 10mg 1 QL (180 EA per 30 days) PA methylphenidate hcl er tbcr 18mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er tbcr 20mg 1 QL (90 EA per 30 days) PA methylphenidate hcl er tbcr 27mg 1 QL (30 EA per 30 days) PA methylphenidate hcl er tbcr 36mg 1 QL (60 EA per 30 days) PA methylphenidate hcl er tbcr 54mg 1 QL (30 EA per 30 days) PA methylphenidate hcl sr tbcr 20mg 1 QL (90 EA per 30 days) PA methylphenidate hcl chew 10mg 1 QL (180 EA per 30 days) PA methylphenidate hcl chew 2.5mg 1 QL (90 EA per 30 days) PA methylphenidate hcl chew 5mg 1 QL (90 EA per 30 days) PA methylphenidate hcl tabs 10mg 1 QL (90 EA per 30 days) PA methylphenidate hcl tabs 20mg 1 QL (90 EA per 30 days) PA methylphenidate hcl tabs 5mg 1 QL (90 EA per 30 days) PA methylphenidate hydrochloride soln 10mg/5ml 1 PA methylphenidate hydrochloride soln 5mg/5ml 1 PA
Central Nervous System, Other butalbital/acetaminophen/caffeine/codeine caps 300mg; 50mg; 40mg; 30mg
1 PA
butalbital/acetaminophen/caffeine/codeine caps 325mg; 50mg; 40mg; 30mg
1 PA
butalbital/acetaminophen/caffeine caps 300mg; 50mg; 40mg 1 PA butalbital/acetaminophen/caffeine caps 325mg; 50mg; 40mg 1 PA butalbital/acetaminophen tabs 325mg; 50mg 1 PA butalbital/aspirin/caffeine caps 325mg; 50mg; 40mg 1 PA caffeine citrate inj 60mg/3ml 1 caffeine citrate soln 60mg/3ml 1 capacet caps 325mg; 50mg; 40mg 1 PA esgic caps 325mg; 50mg; 40mg 1 PA HETLIOZ CAPS 20MG 4 QL (30 EA per 30 days) PA margesic caps 325mg; 50mg; 40mg 1 PA marten-tab tabs 325mg; 50mg 1 PA riluzole tabs 50mg 1 PA

Page 67 of 121
Drug Name Drug Tier Requirements/Limits
tencon tabs 325mg; 50mg 1 PA tetrabenazine tabs 12.5mg 4 PA tetrabenazine tabs 25mg 4 PA vanatol lq soln 325mg/15ml; 50mg/15ml; 40mg/15ml 1 PA XENAZINE TABS 12.5MG 4 PA XENAZINE TABS 25MG 4 PA zebutal caps 325mg; 50mg; 40mg 1 PA
Fibromyalgia Agents SAVELLA TITRATION PACK MISC 0 2 QL (110 EA per 365 days) SAVELLA TABS 100MG 2 QL (60 EA per 30 days) SAVELLA TABS 12.5MG 2 QL (60 EA per 30 days) SAVELLA TABS 25MG 2 QL (60 EA per 30 days) SAVELLA TABS 50MG 2 QL (60 EA per 30 days)
Multiple Sclerosis Agents AMPYRA TB12 10MG 4 QL (60 EA per 30 days) PA AUBAGIO TABS 14MG 4 QL (30 EA per 30 days) PA AUBAGIO TABS 7MG 4 QL (30 EA per 30 days) PA AVONEX PEN INJ 30MCG/0.5ML 4 QL (4 EA per 28 days) PA AVONEX INJ 30MCG/0.5ML 4 QL (4 EA per 28 days) PA AVONEX INJ 30MCG/VIAL 4 QL (4 EA per 28 days) PA BETASERON INJ 0.3MG 4 QL (15 EA per 30 days) PA COPAXONE INJ 20MG/ML 4 QL (30 ML per 30 days) PA COPAXONE INJ 40MG/ML 4 QL (12 ML per 28 days) PA EXTAVIA INJ 0.3MG 4 QL (15 EA per 30 days) PA GILENYA CAPS 0.5MG 4 QL (30 EA per 30 days) PA glatopa inj 20mg/ml 4 QL (30 ML per 30 days) PA PLEGRIDY STARTER PACK INJ 0 4 QL (2 ML per 365 days) PA PLEGRIDY STARTER PACK INJ 0 4 QL (2 ML per 365 days) PA PLEGRIDY INJ 125MCG/0.5ML 4 QL (1 ML per 28 days) PA PLEGRIDY INJ 125MCG/0.5ML 4 QL (1 ML per 28 days) PA REBIF REBIDOSE TITRATION PACK INJ 0 4 QL (8.4 ML per 365 days) PA REBIF REBIDOSE INJ 22MCG/0.5ML 4 QL (6 ML per 28 days) PA REBIF REBIDOSE INJ 44MCG/0.5ML 4 QL (6 ML per 28 days) PA REBIF TITRATION PACK INJ 0 4 QL (8.4 ML per 365 days) PA REBIF INJ 22MCG/0.5ML 4 QL (6 ML per 28 days) PA REBIF INJ 44MCG/0.5ML 4 QL (6 ML per 28 days) PA TECFIDERA STARTER PACK MISC 0 4 QL (120 EA per 365 days) PA TECFIDERA CPDR 120MG 4 QL (60 EA per 30 days) PA TECFIDERA CPDR 240MG 4 QL (60 EA per 30 days) PA TYSABRI INJ 300MG/15ML 4 PA ZINBRYTA INJ 150MG/ML 4 QL (1 ML per 28 days) PA
Dental and Oral Agents Dental and Oral Agents
ARESTIN MISC 1MG 4 cevimeline hcl caps 30mg 1 chlorhexidine gluconate oral rinse soln 0.12% 1 KEPIVANCE INJ 6.25MG 4 oralone pste 0.1% 1 paroex soln 0.12% 1

Page 68 of 121
Drug Name Drug Tier Requirements/Limits
periogard soln 0.12% 1 pilocarpine hcl tabs 7.5mg 1 pilocarpine hydrochloride tabs 5mg 1 triamcinolone acetonide pste 0.1% 1 triamcinolone in orabase pste 0.1% 1
Dermatological Agents Dermatological Agents
acitretin caps 10mg 1 acitretin caps 17.5mg 1 acitretin caps 25mg 1 adapalene pump gel 0.3% 1 PA adapalene crea 0.1% 1 PA adapalene gel 0.1% 1 PA adapalene gel 0.3% 1 PA ammonium lactate crea 12% 1 ammonium lactate lotn 12% 1 amnesteem caps 10mg 1 PA amnesteem caps 20mg 1 PA amnesteem caps 40mg 1 PA avita crea 0.025% 1 PA avita gel 0.025% 1 PA calcipotriene/betamethasone dipropionate oint 0.064%; 0.005%
1 QL (400 GM per 28 days)
calcipotriene crea 0.005% 1 calcipotriene oint 0.005% 1 calcipotriene soln 0.005% 1 calcitrene oint 0.005% 1 calcitrene oint 0.005% 1 calcitriol oint 3mcg/gm 1 claravis caps 10mg 1 PA claravis caps 20mg 1 PA claravis caps 30mg 1 PA claravis caps 40mg 1 PA clindamycin phosphate/tretinoin gel 1.2%; 0.025% 1 PA clindamycin/benzoyl peroxide gel 5%; 1% 1 clindamycin/benzoyl peroxide gel 5%; 1.2% 1 clotrimazole/betamethasone dipropionate crea 0.05%; 1% 1 clotrimazole/betamethasone dipropionate lotn 0.05%; 1% 1 COSENTYX SENSOREADY PEN INJ 150MG/ML 4 PA COSENTYX INJ 150MG/ML 4 PA CURITY GAUZE PADS 2"X2" PADS 2 desonate gel 0.05% 1 diclofenac sodium gel 1% 1 QL (1000 GM per 30 days) diclofenac sodium soln 1.5% 1 PA doxepin hydrochloride crea 5% 1 doxycycline cpdr 40mg 1 erythromycin/benzoyl peroxide gel 5%; 3% 1 FINACEA FOAM 15% 2 FINACEA GEL 15% 2

Page 69 of 121
Drug Name Drug Tier Requirements/Limits
fluocinolone acetonide body oil 0.01% 1 fluocinolone acetonide scalp oil 0.01% 1 fluocinolone acetonide soln 0.01% 1 fluorouracil crea 0.5% 4 fluorouracil crea 5% 1 fluorouracil soln 2% 1 fluorouracil soln 5% 1 imiquimod crea 5% 1 methoxsalen caps 10mg 4 myorisan caps 10mg 1 PA myorisan caps 20mg 1 PA myorisan caps 30mg 1 PA myorisan caps 40mg 1 PA neuac gel 5%; 1.2% 1 PICATO GEL 0.015% 4 PICATO GEL 0.05% 4 podofilox soln 0.5% 1 REGRANEX GEL 0.01% 4 PA selenium sulfide lotn 2.5% 1 STELARA INJ 45MG/0.5ML 4 PA STELARA INJ 90MG/ML 4 PA TACLONEX SUSP 0.064%; 0.005% 4 QL (400 GM per 30 days) tacrolimus oint 0.03% 1 tacrolimus oint 0.1% 1 TALTZ INJ 80MG/ML 4 PA TALTZ INJ 80MG/ML 4 PA tretinoin microsphere pump gel 0.04% 1 PA tretinoin microsphere pump gel 0.1% 1 PA tretinoin microsphere gel 0.04% 1 PA tretinoin microsphere gel 0.1% 1 PA tretinoin crea 0.025% 1 PA tretinoin crea 0.05% 1 PA tretinoin crea 0.1% 1 PA tretinoin gel 0.01% 1 PA tretinoin gel 0.025% 1 PA tretinoin gel 0.05% 1 PA VEREGEN OINT 15% 4 zenatane caps 10mg 1 PA zenatane caps 20mg 1 PA zenatane caps 30mg 1 PA zenatane caps 40mg 1 PA ZYCLARA PUMP CREA 2.5% 4 ZYCLARA PUMP CREA 3.75% 4 ZYCLARA CREA 3.75% 4
Enzyme Replacement/Modifiers Enzyme Replacement/Modifiers
ADAGEN INJ 250UNIT/ML 4 PA ALDURAZYME INJ 2.9MG/5ML 4 PA BUPHENYL TABS 500MG 4

Page 70 of 121
Drug Name Drug Tier Requirements/Limits
CERDELGA CAPS 84MG 4 PA CEREZYME INJ 400UNIT 4 PA CREON CPEP 120000UNIT; 24000UNIT; 76000UNIT 2 CREON CPEP 15000UNIT; 3000UNIT; 9500UNIT 2 CREON CPEP 180000UNIT; 36000UNIT; 114000UNIT 2 CREON CPEP 30000UNIT; 6000UNIT; 19000UNIT 2 CREON CPEP 60000UNIT; 12000UNIT; 38000UNIT 2 CYSTADANE POWD 0 4 ELAPRASE INJ 6MG/3ML 4 PA FABRAZYME INJ 35MG 4 PA FABRAZYME INJ 5MG 4 PA KANUMA INJ 20MG/10ML 4 PA KUVAN PACK 100MG 4 PA KUVAN PACK 500MG 4 PA KUVAN TBSO 100MG 4 PA LUMIZYME INJ 50MG 4 PA MYOZYME INJ 50MG 4 PA NAGLAZYME INJ 1MG/ML 4 PA RAVICTI LIQD 1.1GM/ML 4 PA sodium phenylbutyrate powd 3gm/tsp 4 STRENSIQ INJ 18MG/0.45ML 4 PA STRENSIQ INJ 28MG/0.7ML 4 PA STRENSIQ INJ 40MG/ML 4 PA STRENSIQ INJ 80MG/0.8ML 4 PA SUCRAID SOLN 8500UNIT/ML 4 VIMIZIM INJ 5MG/5ML 4 PA VPRIV INJ 400UNIT 4 PA XIAFLEX INJ 0.9MG 4 PA ZAVESCA CAPS 100MG 4 PA ZENPEP CPEP 109000UNIT; 20000UNIT; 68000UNIT 2 ZENPEP CPEP 136000UNIT; 25000UNIT; 85000UNIT 2 ZENPEP CPEP 16000UNIT; 3000UNIT; 10000UNIT 2 ZENPEP CPEP 218000UNIT; 40000UNIT; 136000UNIT 2 ZENPEP CPEP 27000UNIT; 5000UNIT; 17000UNIT 2 ZENPEP CPEP 55000UNIT; 10000UNIT; 34000UNIT 2 ZENPEP CPEP 82000UNIT; 15000UNIT; 51000UNIT 2
Gastrointestinal Agents Antispasmodics, Gastrointestinal
dicyclomine hcl caps 10mg 1 dicyclomine hcl inj 10mg/ml 1 dicyclomine hcl soln 10mg/5ml 1 dicyclomine hcl tabs 20mg 1 ENTYVIO INJ 300MG 4 PA glycopyrrolate inj 0.2mg/ml 1 glycopyrrolate inj 0.4mg/2ml 1 glycopyrrolate inj 1mg/5ml 1 glycopyrrolate inj 4mg/20ml 1 glycopyrrolate tabs 1mg 1 glycopyrrolate tabs 2mg 1

Page 71 of 121
Drug Name Drug Tier Requirements/Limits
Gastrointestinal Agents, Other CHENODAL TABS 250MG 4 CHOLBAM CAPS 250MG 4 PA CHOLBAM CAPS 50MG 4 PA cromolyn sodium conc 100mg/5ml 1 GATTEX INJ 5MG 4 PA gavilyte-h kit 5mg; 210gm; 0.74gm; 2.86gm; 5.6gm 1 lansoprazole/amoxicillin/clarithromycin misc 0; 0; 0 1 loperamide hcl caps 2mg 1 metoclopramide hcl inj 5mg/ml 1 metoclopramide hcl soln 5mg/5ml 1 metoclopramide hcl tabs 10mg 1 metoclopramide hcl tabs 5mg 1 metoclopramide odt tbdp 10mg 1 metoclopramide odt tbdp 5mg 1 RELISTOR INJ 12MG/0.6ML 4 QL (18 ML per 30 days) PA RELISTOR INJ 12MG/0.6ML 4 QL (18 ML per 30 days) PA RELISTOR INJ 8MG/0.4ML 4 QL (12 ML per 30 days) PA ursodiol tabs 250mg 1 ursodiol tabs 500mg 1
Histamine2 (H2) Receptor Antagonists cimetidine hcl soln 300mg/5ml 1 cimetidine tabs 200mg 1 cimetidine tabs 300mg 1 cimetidine tabs 400mg 1 cimetidine tabs 800mg 1 famotidine premixed inj 0.4mg/ml; 0.9% 1 famotidine inj 200mg/20ml 1 famotidine inj 20mg/2ml 1 famotidine inj 40mg/4ml 1 famotidine susr 40mg/5ml 1 famotidine tabs 20mg 1 famotidine tabs 40mg 1 nizatidine caps 150mg 1 nizatidine caps 300mg 1 nizatidine soln 15mg/ml 1 ranitidine hcl caps 150mg 1 ranitidine hcl caps 300mg 1 ranitidine hcl inj 150mg/6ml 1 ranitidine hcl inj 50mg/2ml 1 ranitidine hcl syrp 15mg/ml 1 ranitidine hcl tabs 150mg 1 ranitidine hcl tabs 300mg 1
Irritable Bowel Syndrome Agents alosetron hydrochloride tabs 0.5mg 4 PA alosetron hydrochloride tabs 1mg 4 PA AMITIZA CAPS 24MCG 2 QL (60 EA per 30 days) AMITIZA CAPS 8MCG 2 QL (60 EA per 30 days) LINZESS CAPS 145MCG 2 QL (30 EA per 30 days)

Page 72 of 121
Drug Name Drug Tier Requirements/Limits
LINZESS CAPS 290MCG 2 QL (30 EA per 30 days) Laxatives
constulose soln 10gm/15ml 1 enulose soln 10gm/15ml 1 gavilyte-c solr 240gm; 2.98gm; 6.72gm; 5.84gm; 22.72gm 1 gavilyte-g solr 236gm; 2.97gm; 6.74gm; 5.86gm; 22.74gm 1 gavilyte-n/flavor pack solr 420gm; 1.48gm; 5.72gm; 11.2gm 1 generlac soln 10gm/15ml 1 lactulose soln 10gm/15ml 1 lactulose soln 10gm/15ml 1 MOVIPREP SOLR 4.7GM; 100GM; 1.015GM; 5.9GM; 2.691GM; 7.5GM
2
peg 3350/electrolytes solr 240gm; 2.98gm; 6.72gm; 5.84gm; 22.72gm
1
peg-3350/electrolytes solr 236gm; 2.97gm; 6.74gm; 5.86gm; 22.74gm
1
peg-3350/nacl/na bicarbonate/kcl solr 420gm; 1.48gm; 5.72gm; 11.2gm
1
polyethylene glycol 3350 pack 0 1 polyethylene glycol 3350 powd 0 1 SUPREP BOWEL PREP SOLN 1.6GM/180ML; 3.13GM/180ML; 17.5GM/180ML
2
trilyte solr 420gm; 1.48gm; 5.72gm; 11.2gm 1 Protectants
misoprostol tabs 100mcg 1 misoprostol tabs 200mcg 1 sucralfate tabs 1gm 1
Proton Pump Inhibitors esomeprazole magnesium cpdr 20mg 1 QL (30 EA per 30 days) esomeprazole magnesium cpdr 40mg 1 QL (30 EA per 30 days) esomeprazole sodium inj 20mg 1 esomeprazole sodium inj 40mg 1 lansoprazole cpdr 15mg 1 QL (30 EA per 30 days) lansoprazole cpdr 30mg 1 QL (30 EA per 30 days) NEXIUM PACK 10MG 2 NEXIUM PACK 2.5MG 2 NEXIUM PACK 20MG 2 NEXIUM PACK 40MG 2 NEXIUM PACK 5MG 2 omeprazole/sodium bicarbonate caps 20mg; 1100mg 1 QL (30 EA per 30 days) omeprazole/sodium bicarbonate caps 40mg; 1100mg 1 QL (30 EA per 30 days) omeprazole cpdr 10mg 1 QL (30 EA per 30 days) omeprazole cpdr 20mg 1 QL (30 EA per 30 days) omeprazole cpdr 40mg 1 QL (30 EA per 30 days) pantoprazole sodium inj 40mg 1 pantoprazole sodium tbec 20mg 1 QL (30 EA per 30 days) pantoprazole sodium tbec 40mg 1 QL (30 EA per 30 days) rabeprazole sodium tbec 20mg 1 QL (30 EA per 30 days)
Genitourinary Agents

Page 73 of 121
Drug Name Drug Tier Requirements/Limits
Antispasmodics, Urinary darifenacin hydrobromide er tb24 15mg 1 darifenacin hydrobromide er tb24 7.5mg 1 flavoxate hcl tabs 100mg 1 MYRBETRIQ TB24 25MG 2 MYRBETRIQ TB24 50MG 2 oxybutynin chloride er tb24 10mg 1 oxybutynin chloride er tb24 15mg 1 oxybutynin chloride er tb24 5mg 1 oxybutynin chloride syrp 5mg/5ml 1 oxybutynin chloride tabs 5mg 1 tolterodine tartrate er cp24 2mg 1 tolterodine tartrate er cp24 4mg 1 tolterodine tartrate tabs 1mg 1 tolterodine tartrate tabs 2mg 1 TOVIAZ TB24 4MG 2 TOVIAZ TB24 8MG 2 trospium chloride er cp24 60mg 1 trospium chloride tabs 20mg 1 VESICARE TABS 10MG 2 VESICARE TABS 5MG 2
Benign Prostatic Hypertrophy Agents alfuzosin hcl er tb24 10mg 1 doxazosin mesylate tabs 1mg 1 doxazosin mesylate tabs 2mg 1 doxazosin mesylate tabs 8mg 1 doxazosin tabs 4mg 1 dutasteride/tamsulosin hydrochloride caps 0.5mg; 0.4mg 1 dutasteride caps 0.5mg 1 finasteride tabs 5mg 1 RAPAFLO CAPS 4MG 2 RAPAFLO CAPS 8MG 2 tamsulosin hcl caps 0.4mg 1 terazosin hcl caps 10mg 1 terazosin hcl caps 1mg 1 terazosin hcl caps 2mg 1 terazosin hcl caps 5mg 1
Genitourinary Agents, Other acetic acid 0.25% soln 0.25% 1 bethanechol chloride tabs 10mg 1 bethanechol chloride tabs 25mg 1 bethanechol chloride tabs 50mg 1 bethanechol chloride tabs 5mg 1
Phosphate Binders calcium acetate caps 667mg 1 calcium acetate tabs 667mg 1 eliphos tabs 667mg 1 FOSRENOL CHEW 1000MG 4 FOSRENOL CHEW 500MG 4

Page 74 of 121
Drug Name Drug Tier Requirements/Limits
FOSRENOL CHEW 750MG 4 FOSRENOL PACK 1000MG 4 FOSRENOL PACK 750MG 4 RENAGEL TABS 400MG 2 RENAGEL TABS 800MG 4 RENVELA PACK 0.8GM 4 RENVELA PACK 2.4GM 4 RENVELA TABS 800MG 4 VELPHORO CHEW 500MG 4
Hormonal Agents, Stimulant/Replacement/Modifying (Adrenal) Hormonal Agents, Stimulant/Replacement/Modifying (Adrenal)
alclometasone dipropionate crea 0.05% 1 alclometasone dipropionate oint 0.05% 1 amcinonide crea 0.1% 1 amcinonide lotn 0.1% 1 amcinonide oint 0.1% 1 augmented betamethasone dipropionate crea 0.05% 1 augmented betamethasone dipropionate gel 0.05% 1 augmented betamethasone dipropionate lotn 0.05% 1 augmented betamethasone dipropionate oint 0.05% 1 baycadron elix 0.5mg/5ml 1 betamethasone dipropionate crea 0.05% 1 betamethasone dipropionate lotn 0.05% 1 betamethasone dipropionate oint 0.05% 1 betamethasone sodium phosphate/betamethasone acetate inj 3mg/ml; 3mg/ml
1
betamethasone valerate crea 0.1% 1 betamethasone valerate foam 0.12% 1 betamethasone valerate lotn 0.1% 1 betamethasone valerate oint 0.1% 1 budesonide cpep 3mg 1 clobetasol propionate e crea 0.05% 1 clobetasol propionate emollient foam 0.05% 1 clobetasol propionate foam 0.05% 1 clobetasol propionate foam 0.05% 1 clobetasol propionate gel 0.05% 1 clobetasol propionate liqd 0.05% 1 clobetasol propionate lotn 0.05% 1 clobetasol propionate oint 0.05% 1 clobetasol propionate sham 0.05% 1 clobetasol propionate soln 0.05% 1 clocortolone pivalate pump crea 0.1% 1 clocortolone pivalate crea 0.1% 1 clodan sham 0.05% 1 colocort enem 100mg/60ml 1 cormax scalp application soln 0.05% 1 cortisone acetate tabs 25mg 1 deltasone tabs 20mg 1 desonide crea 0.05% 1

Page 75 of 121
Drug Name Drug Tier Requirements/Limits
desonide lotn 0.05% 1 desonide oint 0.05% 1 desoximetasone crea 0.05% 1 desoximetasone crea 0.25% 1 desoximetasone gel 0.05% 1 desoximetasone oint 0.05% 1 desoximetasone oint 0.25% 1 dexamethasone intensol conc 1mg/ml 1 dexamethasone sodium phosphate inj 100mg/10ml 1 dexamethasone sodium phosphate inj 10mg/ml 1 dexamethasone sodium phosphate inj 10mg/ml 1 dexamethasone sodium phosphate inj 120mg/30ml 1 dexamethasone sodium phosphate inj 20mg/5ml 1 dexamethasone sodium phosphate inj 4mg/ml 1 dexamethasone elix 0.5mg/5ml 1 dexamethasone soln 0.5mg/5ml 1 dexamethasone tabs 0.5mg 1 dexamethasone tabs 0.75mg 1 dexamethasone tabs 1.5mg 1 dexamethasone tabs 1mg 1 dexamethasone tabs 2mg 1 dexamethasone tabs 4mg 1 dexamethasone tabs 6mg 1 diflorasone diacetate crea 0.05% 1 diflorasone diacetate oint 0.05% 1 fludrocortisone acetate tabs 0.1mg 1 fluocinolone acetonide ear drops oil 0.01% 1 fluocinolone acetonide crea 0.01% 1 fluocinolone acetonide crea 0.025% 1 fluocinolone acetonide oil 0.01% 1 fluocinolone acetonide oint 0.025% 1 fluocinonide-e crea 0.05% 1 fluocinonide crea 0.05% 1 fluocinonide crea 0.1% 1 fluocinonide gel 0.05% 1 fluocinonide oint 0.05% 1 fluocinonide soln 0.05% 1 flurandrenolide crea 0.05% 1 fluticasone propionate crea 0.05% 1 fluticasone propionate lotn 0.05% 1 fluticasone propionate oint 0.005% 1 halobetasol propionate crea 0.05% 1 halobetasol propionate oint 0.05% 1 hydrocortisone butyrate (lipophilic) crea 0.1% 1 hydrocortisone butyrate crea 0.1% 1 hydrocortisone butyrate oint 0.1% 1 hydrocortisone butyrate soln 0.1% 1 hydrocortisone valerate crea 0.2% 1 hydrocortisone valerate oint 0.2% 1

Page 76 of 121
Drug Name Drug Tier Requirements/Limits
hydrocortisone crea 2.5% 1 hydrocortisone enem 100mg/60ml 1 hydrocortisone lotn 2.5% 1 hydrocortisone oint 2.5% 1 hydrocortisone tabs 10mg 1 hydrocortisone tabs 20mg 1 hydrocortisone tabs 5mg 1 lokara lotn 0.05% 1 methylprednisolone acetate inj 40mg/ml 1 methylprednisolone acetate inj 80mg/ml 1 methylprednisolone dose pack tbpk 4mg 1 methylprednisolone sodiumsuccinate inj 1000mg 1 methylprednisolone sodiumsuccinate inj 125mg 1 methylprednisolone sodiumsuccinate inj 40mg 1 methylprednisolone tabs 16mg 1 methylprednisolone tabs 32mg 1 methylprednisolone tabs 4mg 1 methylprednisolone tabs 8mg 1 mometasone furoate crea 0.1% 1 mometasone furoate oint 0.1% 1 mometasone furoate soln 0.1% 1 prednicarbate crea 0.1% 1 prednicarbate oint 0.1% 1 prednisolone sodium phosphate soln 15mg/5ml 1 prednisolone sodium phosphate soln 25mg/5ml 1 prednisolone sodium phosphate soln 5mg/5ml 1 prednisolone syrp 15mg/5ml 1 prednisone intensol conc 5mg/ml 1 prednisone soln 5mg/5ml 1 prednisone tabs 10mg 1 prednisone tabs 1mg 1 prednisone tabs 2.5mg 1 prednisone tabs 20mg 1 prednisone tabs 50mg 1 prednisone tabs 5mg 1 prednisone tbpk 10mg 1 procto-med hc crea 2.5% 1 procto-pak crea 1% 1 proctosol hc crea 2.5% 1 proctozone-hc crea 2.5% 1 RAYOS TBEC 1MG 4 RAYOS TBEC 2MG 4 RAYOS TBEC 5MG 4 synalar crea 0.025% 1 synalar oint 0.025% 1 triamcinolone acetonide aers 0.147mg/gm 1 triamcinolone acetonide crea 0.025% 1 triamcinolone acetonide crea 0.1% 1 triamcinolone acetonide crea 0.5% 1

Page 77 of 121
Drug Name Drug Tier Requirements/Limits
triamcinolone acetonide lotn 0.025% 1 triamcinolone acetonide lotn 0.1% 1 triamcinolone acetonide oint 0.025% 1 triamcinolone acetonide oint 0.1% 1 triamcinolone acetonide oint 0.5% 1 triderm crea 0.1% 1 UCERIS TB24 9MG 4
Hormonal Agents, Stimulant/Replacement/Modifying (Pituitary) Hormonal Agents, Stimulant/Replacement/Modifying (Pituitary)
desmopressin acetate inj 4mcg/ml 1 desmopressin acetate soln 0.01% 1 desmopressin acetate soln 0.01% 1 desmopressin acetate tabs 0.1mg 1 desmopressin acetate tabs 0.2mg 1 EGRIFTA INJ 1MG 4 QL (60 EA per 30 days) PA EGRIFTA INJ 2MG 4 QL (30 EA per 30 days) PA GENOTROPIN MINIQUICK INJ 0.4MG 4 PA GENOTROPIN MINIQUICK INJ 0.6MG 4 PA GENOTROPIN MINIQUICK INJ 0.8MG 4 PA GENOTROPIN MINIQUICK INJ 1.2MG 4 PA GENOTROPIN MINIQUICK INJ 1.4MG 4 PA GENOTROPIN MINIQUICK INJ 1.6MG 4 PA GENOTROPIN MINIQUICK INJ 1.8MG 4 PA GENOTROPIN MINIQUICK INJ 1MG 4 PA GENOTROPIN MINIQUICK INJ 2MG 4 PA GENOTROPIN INJ 12MG 4 PA GENOTROPIN INJ 5MG 4 PA H.P. ACTHAR INJ 80UNIT/ML 4 PA HUMATROPE COMBO PACK INJ 5MG 4 PA HUMATROPE INJ 12MG 4 PA HUMATROPE INJ 24MG 4 PA HUMATROPE INJ 6MG 4 PA INCRELEX INJ 40MG/4ML 4 PA NORDITROPIN FLEXPRO INJ 10MG/1.5ML 4 PA NORDITROPIN FLEXPRO INJ 15MG/1.5ML 4 PA NORDITROPIN FLEXPRO INJ 30MG/3ML 4 PA NORDITROPIN FLEXPRO INJ 5MG/1.5ML 4 PA NORDITROPIN NORDIFLEX PEN INJ 30MG/3ML 4 PA NUTROPIN AQ NUSPIN 10 INJ 10MG/2ML 4 PA NUTROPIN AQ NUSPIN 20 INJ 20MG/2ML 4 PA NUTROPIN AQ NUSPIN 5 INJ 5MG/2ML 4 PA NUTROPIN AQ PEN INJ 10MG/2ML 4 PA NUTROPIN AQ PEN INJ 20MG/2ML 4 PA SAIZEN CLICK.EASY INJ 8.8MG 4 PA SAIZEN INJ 5MG 4 PA SAIZEN INJ 8.8MG 4 PA SEROSTIM INJ 4MG 4 PA SEROSTIM INJ 5MG 4 PA SEROSTIM INJ 6MG 4 PA

Page 78 of 121
Drug Name Drug Tier Requirements/Limits
ZORBTIVE INJ 8.8MG 4 PA Hormonal Agents, Stimulant/Replacement/Modifying (Prostaglandins)
Hormonal Agents, Stimulant/Replacement/Modifying (Prostaglandins)
KORLYM TABS 300MG 4 QL (120 EA per 30 days) PA Hormonal Agents, Stimulant/Replacement/Modifying (Sex Hormones/Modifiers)
Anabolic Steroids ANADROL-50 TABS 50MG 2 PA oxandrolone tabs 10mg 1 QL (60 EA per 30 days) PA oxandrolone tabs 2.5mg 1 QL (240 EA per 30 days) PA
Androgens ANDRODERM PT24 2MG/24HR 2 PA ANDRODERM PT24 4MG/24HR 2 PA ANDROGEL PUMP GEL 1.62% 2 PA ANDROGEL GEL 20.25MG/1.25GM 2 PA ANDROGEL GEL 40.5MG/2.5GM 2 PA danazol caps 100mg 1 danazol caps 200mg 1 danazol caps 50mg 1 methyltestosterone caps 10mg 4 PA testosterone cypionate inj 100mg/ml 1 PA testosterone cypionate inj 200mg/ml 1 PA testosterone enanthate inj 200mg/ml 1 PA
Estrogens altavera tabs 0.03mg; 0.15mg 1 alyacen 1/35 tabs 35mcg; 1mg 1 alyacen 7/7/7 tabs 0; 0 1 amethia lo tabs 0; 0 1 QL (91 EA per 91 days) amethia tabs 0; 0 1 QL (91 EA per 91 days) amethyst tabs 20mcg; 90mcg 1 apri tabs 0.15mg; 30mcg 1 aranelle tabs 0; 0 1 ashlyna tabs 0; 0 1 QL (91 EA per 91 days) aubra tabs 20mcg; 0.1mg 1 aviane tabs 20mcg; 0.1mg 1 azurette tabs 0; 0 1 balziva tabs 35mcg; 0.4mg 1 bekyree tabs 0; 0 1 blisovi 24 fe tabs 20mcg; 75mg; 1mg 1 blisovi fe 1.5/30 tabs 30mcg; 75mg; 1.5mg 1 blisovi fe 1/20 tabs 20mcg; 75mg; 1mg 1 briellyn tabs 35mcg; 0.4mg 1 camrese lo tabs 0; 0 1 QL (91 EA per 91 days) camrese tabs 0; 0 1 QL (91 EA per 91 days) caziant tabs 0; 0 1 chateal tabs 0.03mg; 0.15mg 1 cryselle-28 tabs 30mcg; 0.3mg 1

Page 79 of 121
Drug Name Drug Tier Requirements/Limits
cyclafem 1/35 tabs 35mcg; 1mg 1 cyclafem 7/7/7 tabs 0; 0 1 cyred tabs 0.15mg; 30mcg 1 dasetta 1/35 tabs 35mcg; 1mg 1 dasetta 7/7/7 tabs 0; 0 1 daysee tabs 0; 0 1 QL (91 EA per 91 days) delyla tabs 20mcg; 0.1mg 1 desogestrel/ethinyl estradiol tabs 0.15mg; 30mcg 1 desogestrel/ethinyl estradiol tabs 0; 0 1 drospirenone/ethinyl estradiol tabs 3mg; 0.02mg 1 drospirenone/ethinyl estradiol tabs 3mg; 0.03mg 1 elinest tabs 30mcg; 0.3mg 1 emoquette tabs 0.15mg; 30mcg 1 enpresse-28 tabs 0; 0 1 enskyce tabs 0.15mg; 30mcg 1 estarylla tabs 35mcg; 0.25mg 1 estradiol valerate inj 20mg/ml 1 estradiol valerate inj 40mg/ml 1 estradiol/norethindrone acetate tabs 0.5mg; 0.1mg 1 PA estradiol/norethindrone acetate tabs 1mg; 0.5mg 1 PA estradiol pttw 0.025mg/24hr 1 PA estradiol pttw 0.0375mg/24hr 1 PA estradiol pttw 0.05mg/24hr 1 PA estradiol pttw 0.075mg/24hr 1 PA estradiol pttw 0.1mg/24hr 1 PA estradiol ptwk 0.025mg/24hr 1 PA estradiol ptwk 0.05mg/24hr 1 PA estradiol ptwk 0.06mg/24hr 1 PA estradiol ptwk 0.075mg/24hr 1 PA estradiol ptwk 0.1mg/24hr 1 PA estradiol ptwk 37.5mcg/24hr 1 PA estradiol tabs 0.5mg 1 PA estradiol tabs 1mg 1 PA estradiol tabs 2mg 1 PA estropipate tabs 0.75mg 1 PA estropipate tabs 1.5mg 1 PA estropipate tabs 3mg 1 PA falmina tabs 20mcg; 0.1mg 1 fyavolv tabs 2.5mcg; 0.5mg 1 PA fyavolv tabs 5mcg; 1mg 1 PA gianvi tabs 3mg; 0.02mg 1 gildagia tabs 35mcg; 0.4mg 1 gildess 1.5/30 tabs 30mcg; 1.5mg 1 gildess 1/20 tabs 20mcg; 1mg 1 gildess 24 fe tabs 20mcg; 75mg; 1mg 1 gildess fe 1.5/30 tabs 30mcg; 75mg; 1.5mg 1 gildess fe 1/20 tabs 20mcg; 75mg; 1mg 1 introvale tabs 0.03mg; 0.15mg 1 QL (91 EA per 91 days) jevantique lo tabs 2.5mcg; 0.5mg 1 PA

Page 80 of 121
Drug Name Drug Tier Requirements/Limits
jinteli tabs 5mcg; 1mg 1 PA jolessa tabs 0.03mg; 0.15mg 1 QL (91 EA per 91 days) juleber tabs 0.15mg; 30mcg 1 junel 1.5/30 tabs 30mcg; 1.5mg 1 junel 1/20 tabs 20mcg; 1mg 1 junel fe 1.5/30 tabs 30mcg; 75mg; 1.5mg 1 junel fe 1/20 tabs 20mcg; 75mg; 1mg 1 junel fe 24 tabs 20mcg; 75mg; 1mg 1 kaitlib fe chew 25mcg; 75mg; 0.8mg 1 kariva tabs 0; 0 1 kelnor 1/35 tabs 35mcg; 1mg 1 kimidess tabs 0; 0 1 kurvelo tabs 0.03mg; 0.15mg 1 larin 1.5/30 tabs 30mcg; 1.5mg 1 larin 1/20 tabs 20mcg; 1mg 1 larin 24 fe tabs 20mcg; 75mg; 1mg 1 larin fe 1.5/30 tabs 30mcg; 75mg; 1.5mg 1 larin fe 1/20 tabs 20mcg; 75mg; 1mg 1 larissia tabs 20mcg; 0.1mg 1 layolis fe chew 25mcg; 75mg; 0.8mg 1 leena tabs 0; 0 1 lessina tabs 20mcg; 0.1mg 1 levonest tabs 0; 0 1 levonorgestrel and ethinyl estradiol tabs 0; 0 1 QL (91 EA per 91 days) levonorgestrel and ethinyl estradiol tabs 20mcg; 90mcg 1 levonorgestrel/ethinyl estradiol tabs 0.03mg; 0.15mg 1 levonorgestrel/ethinyl estradiol tabs 0.03mg; 0.15mg 1 QL (91 EA per 91 days) levonorgestrel/ethinyl estradiol tabs 0; 0 1 QL (91 EA per 91 days) levonorgestrel/ethinyl estradiol tabs 0; 0 1 levonorgestrel/ethinyl estradiol tabs 20mcg; 0.1mg 1 levora 0.15/30-28 tabs 0.03mg; 0.15mg 1 lomedia 24 fe tabs 20mcg; 75mg; 1mg 1 lopreeza tabs 0.5mg; 0.1mg 1 PA lopreeza tabs 1mg; 0.5mg 1 PA loryna tabs 3mg; 0.02mg 1 low-ogestrel tabs 30mcg; 0.3mg 1 lutera tabs 20mcg; 0.1mg 1 marlissa tabs 0.03mg; 0.15mg 1 microgestin 1.5/30 tabs 30mcg; 1.5mg 1 microgestin 1/20 tabs 20mcg; 1mg 1 microgestin 24 fe tabs 20mcg; 75mg; 1mg 1 microgestin fe 1.5/30 tabs 30mcg; 75mg; 1.5mg 1 microgestin fe tabs 20mcg; 75mg; 1mg 1 mimvey lo tabs 0.5mg; 0.1mg 1 PA mimvey tabs 1mg; 0.5mg 1 PA mono-linyah tabs 35mcg; 0.25mg 1 mononessa tabs 35mcg; 0.25mg 1 myzilra tabs 0; 0 1 necon 0.5/35-28 tabs 35mcg; 0.5mg 1

Page 81 of 121
Drug Name Drug Tier Requirements/Limits
necon 1/35 tabs 35mcg; 1mg 1 necon 1/50-28 tabs 50mcg; 1mg 1 necon 10/11-28 tabs 35mcg; 0 1 necon 7/7/7 tabs 0; 0 1 nikki tabs 3mg; 0.02mg 1 norethindrone & ethinyl estradiol ferrous fumarate chew 25mcg; 75mg; 0.8mg
1
norethindrone acetate/ethinyl estradiol/ferrous fumarate tabs 20mcg; 75mg; 1mg
1
norethindrone acetate/ethinyl estradiol/ferrous fumarate tabs 20mcg; 75mg; 1mg
1
norethindrone acetate/ethinyl estradiol tabs 2.5mcg; 0.5mg 1 PA norethindrone acetate/ethinyl estradiol tabs 20mcg; 1mg 1 norethindrone acetate/ethinyl estradiol tabs 5mcg; 1mg 1 PA norgestimate/ethinyl estradiol tabs 0; 0 1 norgestimate/ethinyl estradiol tabs 0; 0 1 norgestimate/ethinyl estradiol tabs 0; 0 1 norgestimate/ethinyl estradiol tabs 35mcg; 0.25mg 1 nortrel 0.5/35 (28) tabs 35mcg; 0.5mg 1 nortrel 1/35 tabs 35mcg; 1mg 1 nortrel 1/35 tabs 35mcg; 1mg 1 nortrel 7/7/7 tabs 0; 0 1 ocella tabs 3mg; 0.03mg 1 ogestrel tabs 50mcg; 0.5mg 1 orsythia tabs 20mcg; 0.1mg 1 philith tabs 35mcg; 0.4mg 1 pimtrea tabs 0; 0 1 pirmella 1/35 tabs 35mcg; 1mg 1 pirmella 7/7/7 tabs 0; 0 1 portia-28 tabs 0.03mg; 0.15mg 1 PREMARIN CREA 0.625MG/GM 2 previfem tabs 35mcg; 0.25mg 1 quartette tabs 0; 0 1 QL (91 EA per 91 days) quasense tabs 0.03mg; 0.15mg 1 QL (91 EA per 91 days) reclipsen tabs 0.15mg; 30mcg 1 setlakin tabs 0.03mg; 0.15mg 1 QL (91 EA per 91 days) sprintec 28 tabs 35mcg; 0.25mg 1 sronyx tabs 20mcg; 0.1mg 1 syeda tabs 3mg; 0.03mg 1 tarina fe 1/20 tabs 20mcg; 75mg; 1mg 1 tilia fe tabs 0; 75mg; 1mg 1 tri-estarylla tabs 0; 0 1 tri-legest fe tabs 0; 75mg; 1mg 1 tri-linyah tabs 0; 0 1 tri-lo-estarylla tabs 0; 0 1 tri-lo-marzia tabs 0; 0 1 tri-lo-sprintec tabs 0; 0 1 tri-previfem tabs 0; 0 1 tri-sprintec tabs 0; 0 1

Page 82 of 121
Drug Name Drug Tier Requirements/Limits
trinessa lo tabs 0; 0 1 trinessa tabs 0; 0 1 trivora-28 tabs 0; 0 1 velivet tabs 0; 0 1 vestura tabs 3mg; 0.02mg 1 vienva tabs 20mcg; 0.1mg 1 viorele tabs 0; 0 1 vyfemla tabs 35mcg; 0.4mg 1 wera tabs 35mcg; 0.5mg 1 wymzya fe chew 35mcg; 0; 0.4mg 1 xulane ptwk 35mcg/24hr; 150mcg/24hr 1 zarah tabs 3mg; 0.03mg 1 zenchent fe chew 35mcg; 0; 0.4mg 1 zenchent tabs 35mcg; 0.4mg 1 zovia 1/35e tabs 35mcg; 1mg 1 zovia 1/50e tabs 50mcg; 1mg 1
Progesterone Agonists/Antagonists ELLA TABS 30MG 2
Progestins camila tabs 0.35mg 1 deblitane tabs 0.35mg 1 errin tabs 0.35mg 1 heather tabs 0.35mg 1 hydroxyprogesterone caproate inj 1.25gm/5ml 4 PA jencycla tabs 0.35mg 1 jolivette tabs 0.35mg 1 levonorgestrel tabs 0.75mg 1 levonorgestrel tabs 1.5mg 1 lyza tabs 0.35mg 1 MAKENA INJ 250MG/ML 4 PA medroxyprogesterone acetate inj 150mg/ml 1 QL (1 ML per 90 days) medroxyprogesterone acetate tabs 10mg 1 medroxyprogesterone acetate tabs 2.5mg 1 medroxyprogesterone acetate tabs 5mg 1 megestrol acetate susp 40mg/ml 1 PA megestrol acetate susp 625mg/5ml 1 PA megestrol acetate tabs 20mg 1 PA megestrol acetate tabs 40mg 1 PA nora-be tabs 0.35mg 1 norethindrone acetate tabs 5mg 1 norethindrone tabs 0.35mg 1 norlyroc tabs 0.35mg 1 progesterone caps 100mg 1 progesterone caps 200mg 1 progesterone inj 50mg/ml 1 sharobel tabs 0.35mg 1
Selective Estrogen Receptor Modifying Agents raloxifene hydrochloride tabs 60mg 1
Hormonal Agents, Stimulant/Replacement/Modifying (Thyroid)

Page 83 of 121
Drug Name Drug Tier Requirements/Limits
Hormonal Agents, Stimulant/Replacement/Modifying (Thyroid) levothyroxine sodium tabs 100mcg 1 levothyroxine sodium tabs 112mcg 1 levothyroxine sodium tabs 125mcg 1 levothyroxine sodium tabs 137mcg 1 levothyroxine sodium tabs 150mcg 1 levothyroxine sodium tabs 175mcg 1 levothyroxine sodium tabs 200mcg 1 levothyroxine sodium tabs 25mcg 1 levothyroxine sodium tabs 300mcg 1 levothyroxine sodium tabs 50mcg 1 levothyroxine sodium tabs 75mcg 1 levothyroxine sodium tabs 88mcg 1 levoxyl tabs 100mcg 1 levoxyl tabs 112mcg 1 levoxyl tabs 125mcg 1 levoxyl tabs 137mcg 1 levoxyl tabs 150mcg 1 levoxyl tabs 175mcg 1 levoxyl tabs 200mcg 1 levoxyl tabs 25mcg 1 levoxyl tabs 50mcg 1 levoxyl tabs 75mcg 1 levoxyl tabs 88mcg 1 liothyronine sodium inj 10mcg/ml 1 liothyronine sodium tabs 25mcg 1 liothyronine sodium tabs 50mcg 1 liothyronine sodium tabs 5mcg 1 unithroid tabs 100mcg 1 unithroid tabs 112mcg 1 unithroid tabs 125mcg 1 unithroid tabs 137mcg 1 unithroid tabs 150mcg 1 unithroid tabs 175mcg 1 unithroid tabs 200mcg 1 unithroid tabs 25mcg 1 unithroid tabs 300mcg 1 unithroid tabs 50mcg 1 unithroid tabs 75mcg 1 unithroid tabs 88mcg 1
Hormonal Agents, Suppressant (Adrenal) Hormonal Agents, Suppressant (Adrenal)
LYSODREN TABS 500MG 2 Hormonal Agents, Suppressant (Parathyroid)
Hormonal Agents, Suppressant (Parathyroid) SENSIPAR TABS 30MG 2 SENSIPAR TABS 60MG 4 SENSIPAR TABS 90MG 4
Hormonal Agents, Suppressant (Pituitary)

Page 84 of 121
Drug Name Drug Tier Requirements/Limits
Hormonal Agents, Suppressant (Pituitary) cabergoline tabs 0.5mg 1 ELIGARD INJ 45MG 4 QL (1 EA per 168 days) PA FIRMAGON INJ 120MG 4 QL (4 EA per 365 days) PA leuprolide acetate inj 1mg/0.2ml 1 PA LUPANETA PACK KIT 11.25MG; 5MG 4 QL (1 EA per 84 days) PA LUPANETA PACK KIT 3.75MG; 5MG 4 QL (1 EA per 28 days) PA LUPRON DEPOT-PED INJ 11.25MG 4 QL (1 EA per 84 days) PA LUPRON DEPOT-PED INJ 11.25MG 4 QL (1 EA per 28 days) PA LUPRON DEPOT-PED INJ 15MG 4 QL (1 EA per 28 days) PA LUPRON DEPOT-PED INJ 30MG 4 QL (1 EA per 84 days) PA LUPRON DEPOT-PED INJ 7.5MG 4 QL (1 EA per 28 days) PA LUPRON DEPOT INJ 11.25MG 4 QL (1 EA per 84 days) PA LUPRON DEPOT INJ 22.5MG 4 QL (1 EA per 84 days) PA LUPRON DEPOT INJ 3.75MG 4 QL (1 EA per 28 days) PA LUPRON DEPOT INJ 30MG 4 QL (1 EA per 112 days) PA LUPRON DEPOT INJ 45MG 4 QL (1 EA per 168 days) PA LUPRON DEPOT INJ 7.5MG 4 QL (1 EA per 28 days) PA octreotide acetate inj 1000mcg/ml 1 PA octreotide acetate inj 100mcg/ml 1 PA octreotide acetate inj 200mcg/ml 1 PA octreotide acetate inj 500mcg/ml 1 PA octreotide acetate inj 50mcg/ml 1 PA SANDOSTATIN LAR DEPOT INJ 10MG 4 PA SANDOSTATIN LAR DEPOT INJ 20MG 4 PA SANDOSTATIN LAR DEPOT INJ 30MG 4 PA SIGNIFOR LAR INJ 20MG 4 QL (1 EA per 28 days) PA SIGNIFOR LAR INJ 40MG 4 QL (1 EA per 28 days) PA SIGNIFOR LAR INJ 60MG 4 QL (1 EA per 28 days) PA SIGNIFOR INJ 0.3MG/ML 4 QL (60 ML per 30 days) PA SIGNIFOR INJ 0.6MG/ML 4 QL (60 ML per 30 days) PA SIGNIFOR INJ 0.9MG/ML 4 QL (60 ML per 30 days) PA SOMATULINE DEPOT INJ 120MG/0.5ML 4 PA SOMATULINE DEPOT INJ 60MG/0.2ML 4 PA SOMATULINE DEPOT INJ 90MG/0.3ML 4 PA SOMAVERT INJ 10MG 4 PA SOMAVERT INJ 15MG 4 PA SOMAVERT INJ 20MG 4 PA SOMAVERT INJ 25MG 4 PA SOMAVERT INJ 30MG 4 PA SYNAREL SOLN 2MG/ML 4 TRELSTAR MIXJECT INJ 11.25MG 4 QL (1 EA per 84 days) PA TRELSTAR MIXJECT INJ 22.5MG 4 QL (1 EA per 168 days) PA TRELSTAR MIXJECT INJ 3.75MG 4 QL (1 EA per 28 days) PA TRELSTAR INJ 11.25MG 4 QL (1 EA per 84 days) PA TRELSTAR INJ 3.75MG 4 QL (1 EA per 28 days) PA
Hormonal Agents, Suppressant (Thyroid) Antithyroid Agents
methimazole tabs 10mg 1

Page 85 of 121
Drug Name Drug Tier Requirements/Limits
methimazole tabs 5mg 1 propylthiouracil tabs 50mg 1
Immunological Agents Angioedema (HAE) Agents
BERINERT INJ 500UNIT 4 PA CINRYZE INJ 500UNIT 4 PA FIRAZYR INJ 30MG/3ML 4 PA RUCONEST INJ 2100UNIT 4 PA
Immune Suppressants ASTAGRAF XL CP24 5MG 4 B/D azathioprine inj 100mg 1 B/D azathioprine tabs 50mg 1 B/D BENLYSTA INJ 120MG 4 PA BENLYSTA INJ 400MG 4 PA CELLCEPT SUSR 200MG/ML 4 B/D CIMZIA STARTER KIT INJ 200MG/ML 4 PA CIMZIA INJ 200MG/ML 4 PA CIMZIA INJ 200MG 4 PA cyclosporine modified caps 100mg 1 B/D cyclosporine modified caps 25mg 1 B/D cyclosporine modified caps 50mg 1 B/D cyclosporine modified soln 100mg/ml 1 B/D cyclosporine caps 100mg 1 B/D cyclosporine caps 25mg 1 B/D cyclosporine inj 50mg/ml 1 B/D ENBREL SURECLICK INJ 50MG/ML 4 PA ENBREL INJ 25MG/0.5ML 4 PA ENBREL INJ 25MG 4 PA ENBREL INJ 50MG/ML 4 PA gengraf caps 100mg 1 B/D gengraf caps 25mg 1 B/D gengraf caps 50mg 1 B/D gengraf soln 100mg/ml 1 B/D hecoria caps 0.5mg 1 B/D hecoria caps 1mg 1 B/D hecoria caps 5mg 1 B/D HUMIRA PEDIATRIC CROHNS DISEASE STARTER PACK INJ 40MG/0.8ML
4 PA
HUMIRA PEDIATRIC CROHNS DISEASE STARTER PACK INJ 40MG/0.8ML
4 PA
HUMIRA PEN-CROHNS DISEASESTARTER INJ 40MG/0.8ML
4 PA
HUMIRA PEN-PSORIASIS STARTER INJ 40MG/0.8ML 4 PA HUMIRA PEN INJ 40MG/0.8ML 4 PA HUMIRA INJ 10MG/0.2ML 4 PA HUMIRA INJ 20MG/0.4ML 4 PA HUMIRA INJ 40MG/0.8ML 4 PA KINERET INJ 100MG/0.67ML 4 PA methotrexate sodium inj 100mg/4ml 1

Page 86 of 121
Drug Name Drug Tier Requirements/Limits
methotrexate sodium inj 1gm/40ml 1 methotrexate sodium inj 1gm 1 methotrexate sodium inj 200mg/8ml 1 methotrexate sodium inj 250mg/10ml 1 methotrexate sodium inj 250mg/10ml 1 methotrexate sodium inj 50mg/2ml 1 methotrexate sodium inj 50mg/2ml 1 methotrexate tabs 2.5mg 1 mycophenolate mofetil caps 250mg 1 B/D mycophenolate mofetil susr 200mg/ml 4 B/D mycophenolate mofetil tabs 500mg 1 B/D mycophenolic acid dr tbec 180mg 1 B/D mycophenolic acid dr tbec 360mg 1 B/D NULOJIX INJ 250MG 4 PA ORENCIA INJ 125MG/ML 4 PA ORENCIA INJ 250MG 4 PA RAPAMUNE SOLN 1MG/ML 4 B/D RAPAMUNE TABS 2MG 4 B/D REMICADE INJ 100MG 4 PA SIMPONI ARIA INJ 50MG/4ML 4 PA SIMPONI INJ 100MG/ML 4 PA SIMPONI INJ 100MG/ML 4 PA SIMPONI INJ 50MG/0.5ML 4 PA SIMPONI INJ 50MG/0.5ML 4 PA sirolimus tabs 0.5mg 1 B/D sirolimus tabs 1mg 1 B/D sirolimus tabs 2mg 4 B/D tacrolimus caps 0.5mg 1 B/D tacrolimus caps 1mg 1 B/D tacrolimus caps 5mg 1 B/D TORISEL INJ 25MG/ML 4 ZORTRESS TABS 0.5MG 4 PA ZORTRESS TABS 0.75MG 4 PA
Immunizing Agents, Passive ATGAM INJ 50MG/ML 4 B/D BIVIGAM INJ 10GM/100ML 4 PA BIVIGAM INJ 5GM/50ML 4 PA CARIMUNE NANOFILTERED INJ 12GM 4 PA CARIMUNE NANOFILTERED INJ 6GM 4 PA FLEBOGAMMA DIF INJ 0.5GM/10ML 4 PA FLEBOGAMMA DIF INJ 10% 4 PA FLEBOGAMMA DIF INJ 10% 4 PA FLEBOGAMMA DIF INJ 10% 4 PA FLEBOGAMMA DIF INJ 10GM/200ML 4 PA FLEBOGAMMA DIF INJ 2.5GM/50ML 4 PA FLEBOGAMMA DIF INJ 20GM/400ML 4 PA FLEBOGAMMA DIF INJ 5GM/100ML 4 PA GAMASTAN S/D INJ 0 2 PA GAMMAGARD LIQUID INJ 10GM/100ML 4 PA

Page 87 of 121
Drug Name Drug Tier Requirements/Limits
GAMMAGARD LIQUID INJ 1GM/10ML 4 PA GAMMAGARD LIQUID INJ 2.5GM/25ML 4 PA GAMMAGARD LIQUID INJ 20GM/200ML 4 PA GAMMAGARD LIQUID INJ 30GM/300ML 4 PA GAMMAGARD LIQUID INJ 5GM/50ML 4 PA GAMMAGARD S/D IGA LESS THAN 1MCG/ML INJ 10GM
4 PA
GAMMAGARD S/D IGA LESS THAN 1MCG/ML INJ 5GM4 PA GAMMAKED INJ 10GM/100ML 4 PA GAMMAKED INJ 1GM/10ML 4 PA GAMMAKED INJ 2.5GM/25ML 4 PA GAMMAKED INJ 20GM/200ML 4 PA GAMMAKED INJ 5GM/50ML 4 PA GAMMAPLEX INJ 10GM/200ML 4 PA GAMMAPLEX INJ 2.5GM/50ML 4 PA GAMMAPLEX INJ 20GM/400ML 4 PA GAMMAPLEX INJ 5GM/100ML 4 PA GAMUNEX-C INJ 10GM/100ML 4 PA GAMUNEX-C INJ 1GM/10ML 4 PA GAMUNEX-C INJ 2.5GM/25ML 4 PA GAMUNEX-C INJ 20GM/200ML 4 PA GAMUNEX-C INJ 40GM/400ML 4 PA GAMUNEX-C INJ 5GM/50ML 4 PA HEPAGAM B INJ 0 4 B/D HIZENTRA INJ 10GM/50ML 4 PA HIZENTRA INJ 1GM/5ML 4 PA HIZENTRA INJ 2GM/10ML 4 PA HIZENTRA INJ 4GM/20ML 4 PA HYPERHEP B S/D INJ 0 4 B/D HYPERRAB S/D INJ 150UNIT/ML 2 B/D HYPERRAB S/D INJ 150UNIT/ML 2 B/D NABI-HB INJ 0 4 B/D OCTAGAM INJ 10GM/100ML 4 PA OCTAGAM INJ 10GM/200ML 4 PA OCTAGAM INJ 1GM/20ML 4 PA OCTAGAM INJ 2.5GM/50ML 4 PA OCTAGAM INJ 20GM/200ML 4 PA OCTAGAM INJ 25GM/500ML 4 PA OCTAGAM INJ 2GM/20ML 4 PA OCTAGAM INJ 5GM/100ML 4 PA OCTAGAM INJ 5GM/50ML 4 PA PRIVIGEN INJ 10GM/100ML 4 PA PRIVIGEN INJ 20GM/200ML 4 PA PRIVIGEN INJ 40GM/400ML 4 PA PRIVIGEN INJ 5GM/50ML 4 PA THYMOGLOBULIN INJ 25MG 4 B/D
Immunomodulators ACTEMRA INJ 162MG/0.9ML 4 QL (3.6 ML per 28 days) PA ACTEMRA INJ 200MG/10ML 4 PA

Page 88 of 121
Drug Name Drug Tier Requirements/Limits
ACTEMRA INJ 400MG/20ML 4 PA ACTEMRA INJ 80MG/4ML 4 PA ACTIMMUNE INJ 2000000UNIT/0.5ML 4 ARCALYST INJ 220MG 4 PA ILARIS INJ 180MG 4 PA leflunomide tabs 10mg 1 leflunomide tabs 20mg 1 LEMTRADA INJ 12MG/1.2ML 4 PA OTEZLA TABS 30MG 4 PA OTEZLA TBPK 0 4 PA RIDAURA CAPS 3MG 4 SIMULECT INJ 10MG 4 B/D SIMULECT INJ 20MG 4 B/D SYNAGIS INJ 100MG/ML 4 PA SYNAGIS INJ 50MG/0.5ML 4 PA XELJANZ XR TB24 11MG 4 PA XELJANZ TABS 5MG 4 PA
Vaccines ACTHIB INJ 0 2 ADACEL INJ 15.5MCG/0.5ML; 2LF/0.5ML; 5LF/0.5ML 2 BEXSERO INJ 0 2 BOOSTRIX INJ 18.5MCG/0.5ML; 2.5LF/0.5ML; 5LF/0.5ML2 BOOSTRIX INJ 18.5MCG/0.5ML; 2.5LF/0.5ML; 5LF/0.5ML2 CERVARIX INJ 0 2 COMVAX INJ 7.5MCG/0.5ML; 5MCG/0.5ML 2 DAPTACEL INJ 10MCG/0.5ML; 15LF/0.5ML; 5LF/0.5ML 2 diphtheria/tetanus toxoids adsorbed pediatric inj 25lfu/0.5ml; 5lfu/0.5ml
1
ENGERIX-B INJ 10MCG/0.5ML 2 B/D ENGERIX-B INJ 10MCG/0.5ML 2 B/D ENGERIX-B INJ 20MCG/ML 2 B/D GARDASIL 9 INJ 0 2 GARDASIL 9 INJ 0 2 GARDASIL INJ 0 2 GARDASIL INJ 0 2 HAVRIX INJ 1440ELU/ML 2 HAVRIX INJ 720ELU/0.5ML 2 HIBERIX INJ 10MCG 2 HYQVIA INJ 10GM/100ML; 800UNIT/5ML 4 PA HYQVIA INJ 2.5GM/25ML; 200UNT/1.25ML 4 PA HYQVIA INJ 20GM/200ML; 1600UNIT/10ML 4 PA HYQVIA INJ 30GM/300ML; 2400UNIT/15ML 4 PA HYQVIA INJ 5GM/50ML; 400UNIT/2.5ML 4 PA INFANRIX INJ 58MCG/0.5ML; 25LFU/0.5ML; 10LFU/0.5ML
2
IPOL INACTIVATED IPV INJ 0 2 IXIARO INJ 0 2 KINRIX INJ 58MCG/0.5ML; 25LFU/0.5ML; 0; 10LFU/0.5ML
2

Page 89 of 121
Drug Name Drug Tier Requirements/Limits
M-M-R II INJ 0; 0; 0 2 MENACTRA INJ 0 2 MENHIBRIX INJ 2.5MCG; 5MCG; 5MCG 2 MENOMUNE-A/C/Y/W-135 INJ 0 2 MENVEO INJ 0 2 PEDVAX HIB INJ 7.5MCG/0.5ML 2 PROQUAD INJ 0; 0; 0; 0 2 QUADRACEL INJ 48MCG/0.5ML; 15LFU/0.5ML; 0; 5LFU/0.5ML
2
RECOMBIVAX HB INJ 10MCG/ML 2 B/D RECOMBIVAX HB INJ 10MCG/ML 2 B/D RECOMBIVAX HB INJ 40MCG/ML 2 B/D RECOMBIVAX HB INJ 5MCG/0.5ML 2 B/D ROTARIX SUSR 0 2 ROTATEQ SOLN 0 2 TENIVAC INJ 2LFU; 5LFU 2 TETANUS/DIPHTHERIA TOXOIDS-ADSORBED INJ 2LF/0.5ML; 2LF/0.5ML
2
TRUMENBA INJ 0 2 TWINRIX INJ 720ELU/ML; 20MCG/ML 2 B/D TYPHIM VI INJ 25MCG/0.5ML 2 TYPHIM VI INJ 25MCG/0.5ML 2 VAQTA INJ 25UNIT/0.5ML 2 VAQTA INJ 50UNIT/ML 2 VARIVAX INJ 1350PFU/0.5ML 2 VARIZIG INJ 125UNIT/1.2ML 4 PA YF-VAX INJ 0 2 ZOSTAVAX INJ 19400UNT/0.65ML 2
Inflammatory Bowel Disease Agents Aminosalicylates
APRISO CP24 0.375GM 2 balsalazide disodium caps 750mg 1 CANASA SUPP 1000MG 4 DIPENTUM CAPS 250MG 4 LIALDA TBEC 1.2GM 2 mesalamine enem 4gm 1 mesalamine kit 4gm 1
Sulfonamides sulfasalazine tabs 500mg 1 sulfasalazine tbec 500mg 1
Metabolic Bone Disease Agents Metabolic Bone Disease Agents
alendronate sodium soln 70mg/75ml 1 alendronate sodium tabs 10mg 1 alendronate sodium tabs 35mg 1 alendronate sodium tabs 40mg 1 alendronate sodium tabs 5mg 1 alendronate sodium tabs 70mg 1 QL (4 EA per 28 days) calcitonin-salmon soln 200unit/act 1 QL (3.7 ML per 30 days)

Page 90 of 121
Drug Name Drug Tier Requirements/Limits
calcitriol caps 0.25mcg 1 calcitriol caps 0.5mcg 1 calcitriol inj 1mcg/ml 1 calcitriol soln 1mcg/ml 1 doxercalciferol caps 0.5mcg 1 doxercalciferol caps 1mcg 1 doxercalciferol caps 2.5mcg 1 doxercalciferol inj 4mcg/2ml 1 etidronate disodium tabs 200mg 1 etidronate disodium tabs 400mg 1 FORTEO INJ 600MCG/2.4ML 4 PA ibandronate sodium inj 3mg/3ml 1 ibandronate sodium tabs 150mg 1 QL (1 EA per 28 days) MIACALCIN INJ 200UNIT/ML 4 pamidronate disodium inj 30mg/10ml 1 pamidronate disodium inj 30mg 1 pamidronate disodium inj 6mg/ml 1 pamidronate disodium inj 90mg/10ml 1 pamidronate disodium inj 90mg 1 paricalcitol caps 1mcg 1 paricalcitol caps 2mcg 1 paricalcitol caps 4mcg 1 paricalcitol inj 2mcg/ml 1 paricalcitol inj 5mcg/ml 1 risedronate sodium dr tbec 35mg 1 QL (4 EA per 28 days) risedronate sodium tabs 150mg 1 QL (1 EA per 28 days) risedronate sodium tabs 30mg 1 risedronate sodium tabs 35mg 1 QL (4 EA per 28 days) risedronate sodium tabs 35mg 1 QL (4 EA per 28 days) risedronate sodium tabs 35mg 1 QL (4 EA per 28 days) risedronate sodium tabs 5mg 1 XGEVA INJ 120MG/1.7ML 4 PA zoledronic acid inj 4mg/5ml 1 zoledronic acid inj 4mg 1 zoledronic acid inj 5mg/100ml 1
Miscellaneous Therapeutic Agents Miscellaneous Therapeutic Agents
AMMONUL INJ 10%; 10% 4 BD INSULIN SYRINGE SAFETYGLIDE/1ML/29G X 1/2" MISC
2 QL (200 EA per 30 days)
BD INSULIN SYRINGE ULTRAFINE/0.3ML/31G X 5/16" MISC
2 QL (200 EA per 30 days)
BD INSULIN SYRINGE ULTRAFINE/0.5ML/30G X 1/2" MISC
2 QL (200 EA per 30 days)
BD INSULIN SYRINGE ULTRAFINE/1ML/31G X 5/16" MISC
2 QL (200 EA per 30 days)
BD PEN NEEDLE/ULTRAFINE/29G X 12.7MM MISC 2 QL (200 EA per 30 days) deferoxamine mesylate inj 2gm 1 B/D deferoxamine mesylate inj 500mg 1 B/D

Page 91 of 121
Drug Name Drug Tier Requirements/Limits
KALBITOR INJ 10MG/ML 4 PA KEVEYIS TABS 50MG 4 QL (120 EA per 30 days) PA lactated ringers irrigation soln 3meq/l; 109meq/l; 28meq/l; 4meq/l; 130meq/l
1
levocarnitine inj 200mg/ml 1 levocarnitine soln 1gm/10ml 1 levocarnitine tabs 330mg 1 methergine tabs 0.2mg 4 methylergonovine maleate tabs 0.2mg 4 MYALEPT INJ 11.3MG 4 PA NATPARA INJ 100MCG 4 QL (2 EA per 28 days) PA NATPARA INJ 25MCG 4 QL (2 EA per 28 days) PA NATPARA INJ 50MCG 4 QL (2 EA per 28 days) PA NATPARA INJ 75MCG 4 QL (2 EA per 28 days) PA ORFADIN CAPS 10MG 4 ORFADIN CAPS 2MG 4 ORFADIN CAPS 5MG 4 ORFADIN SUSP 4MG/ML 4 ringers irrigation soln 4.5meq/l; 156meq/l; 4meq/l; 147meq/l 1 sodium phenylacetate/sodium benzoate inj 10%; 10% 4 SOLIRIS INJ 10MG/ML 4 PA sterile water irrigation soln 0 1 tis-u-sol soln 4.5meq/l; 156meq/l; 4meq/l; 147meq/l 1 V-GO 20 KIT 2 V-GO 30 KIT 2 V-GO 40 KIT 2
Ophthalmic Agents Ophthalmic Prostaglandin and Prostamide Analogs
bimatoprost soln 0.03% 1 COMBIGAN SOLN 0.2%; 0.5% 2 latanoprost soln 0.005% 1 QL (2.5 ML per 25 days) LUMIGAN SOLN 0.01% 2 QL (2.5 ML per 25 days) TRAVATAN Z SOLN 0.004% 2 QL (2.5 ML per 25 days) travoprost soln 0.004% 1 QL (2.5 ML per 25 days)
Ophthalmic Agents, Other atropine sulfate soln 1% 1 bacitracin/polymyxin b oint 500unit/gm; 10000unit/gm 1 cyclopentolate hcl soln 1% 1 cyclopentolate hcl soln 2% 1 cyclopentolate hydrochloride soln 0.5% 1 CYSTARAN SOLN 0.44% 4 QL (60 ML per 28 days) PA EYLEA INJ 2MG/0.05ML 4 PA naphazoline hcl soln 0.1% 1 neo-polycin oint 400unit/gm; 3.5mg/gm; 10000unit/gm 1 neomycin/bacitracin/polymyxin oint 400unit/gm; 5mg/gm; 10000unit/gm
1
neomycin/polymyxin/gramicidin soln 0.025mg/ml; 1.75mg/ml; 10000unit/ml
1
polycin oint 500unit/gm; 10000unit/gm 1

Page 92 of 121
Drug Name Drug Tier Requirements/Limits
polymyxin b sulfate/trimethoprim sulfate soln 10000unit/ml; 0.1%
1
PROCYSBI CPDR 25MG 4 PA PROCYSBI CPDR 75MG 4 PA proparacaine hcl soln 0.5% 1 RESTASIS EMUL 0.05% 2
Ophthalmic Anti-allergy Agents azelastine hcl soln 0.05% 1 cromolyn sodium soln 4% 1 epinastine hcl soln 0.05% 1 olopatadine hcl soln 0.1% 1 PATADAY SOLN 0.2% 2 PAZEO SOLN 0.7% 2
Ophthalmic Anti-inflammatories ALREX SUSP 0.2% 2 bromfenac soln 0.09% 1 bromfenac soln 0.09% 1 dexamethasone sodium phosphate soln 0.1% 1 diclofenac sodium soln 0.1% 1 DUREZOL EMUL 0.05% 2 FLAREX SUSP 0.1% 2 fluorometholone susp 0.1% 1 flurbiprofen sodium soln 0.03% 1 FML FORTE SUSP 0.25% 2 FML OINT 0.1% 2 ILEVRO SUSP 0.3% 2 QL (6 ML per 30 days) ketorolac tromethamine soln 0.4% 1 ketorolac tromethamine soln 0.5% 1 MAXIDEX SUSP 0.1% 2 neomycin/polymyxin/dexamethasone oint 0.1%; 3.5mg/gm; 10000unit/gm
1
neomycin/polymyxin/dexamethasone susp 0.1%; 3.5mg/ml; 10000unit/ml
1
NEVANAC SUSP 0.1% 2 QL (6 ML per 30 days) PRED MILD SUSP 0.12% 2 prednisolone acetate susp 1% 1 prednisolone sodium phosphate soln 1% 1 sulfacetamide sodium/prednisolone sodium phosphate soln 0.23%; 10%
1
tobramycin/dexamethasone susp 0.1%; 0.3% 1 VEXOL SUSP 1% 2
Ophthalmic Antiglaucoma Agents acetazolamide er cp12 500mg 1 ALPHAGAN P SOLN 0.1% 2 apraclonidine soln 0.5% 1 AZOPT SUSP 1% 2 betaxolol hcl soln 0.5% 1 brimonidine tartrate soln 0.15% 1 brimonidine tartrate soln 0.2% 1

Page 93 of 121
Drug Name Drug Tier Requirements/Limits
carteolol hcl soln 1% 1 dorzolamide hcl/timolol maleate soln 22.3mg/ml; 6.8mg/ml 1 dorzolamide hcl soln 2% 1 levobunolol hcl soln 0.5% 1 methazolamide tabs 25mg 1 methazolamide tabs 50mg 1 metipranolol soln 0.3% 1 pilocarpine hcl soln 1% 1 pilocarpine hcl soln 2% 1 pilocarpine hcl soln 4% 1 timolol maleate ophthalmic gel forming solg 0.25% 1 timolol maleate ophthalmic gel forming solg 0.5% 1 timolol maleate soln 0.25% 1 timolol maleate soln 0.5% 1
Otic Agents Otic Agents
acetasol hc soln 2%; 1% 1 acetic acid/aluminum acetate soln 2%; 0 1 acetic acid soln 2% 1 CIPRODEX SUSP 0.3%; 0.1% 2 hydrocortisone/acetic acid soln 2%; 1% 1 neomycin/polymyxin/hc soln 1%; 3.5mg/ml; 10000unit/ml 1 neomycin/polymyxin/hydrocortisone susp 1%; 3.5mg/ml; 10000unit/ml
1
Respiratory Tract/Pulmonary Agents Anti-inflammatories, Inhaled Corticosteroids
ADVAIR DISKUS AEPB 100MCG/DOSE; 50MCG/DOSE 2 QL (60 EA per 30 days) ADVAIR DISKUS AEPB 250MCG/DOSE; 50MCG/DOSE 2 QL (60 EA per 30 days) ADVAIR DISKUS AEPB 500MCG/DOSE; 50MCG/DOSE 2 QL (60 EA per 30 days) ADVAIR HFA AERO 115MCG/ACT; 21MCG/ACT 2 QL (24 GM per 30 days) ADVAIR HFA AERO 230MCG/ACT; 21MCG/ACT 2 QL (24 GM per 30 days) ADVAIR HFA AERO 45MCG/ACT; 21MCG/ACT 2 QL (24 GM per 30 days) BREO ELLIPTA AEPB 100MCG/INH; 25MCG/INH 2 BREO ELLIPTA AEPB 200MCG/INH; 25MCG/INH 2 budesonide susp 0.25mg/2ml 1 QL (120 ML per 30 days) B/D budesonide susp 0.5mg/2ml 1 QL (120 ML per 30 days) B/D budesonide susp 1mg/2ml 1 QL (120 ML per 30 days) B/D budesonide susp 32mcg/act 1 QL (17.2 GM per 30 days) FLOVENT DISKUS AEPB 100MCG/BLIST 2 QL (60 EA per 30 days) FLOVENT DISKUS AEPB 250MCG/BLIST 2 QL (240 EA per 30 days) FLOVENT DISKUS AEPB 50MCG/BLIST 2 QL (60 EA per 30 days) FLOVENT HFA AERO 110MCG/ACT 2 QL (24 GM per 30 days) FLOVENT HFA AERO 220MCG/ACT 2 QL (24 GM per 30 days) FLOVENT HFA AERO 44MCG/ACT 2 QL (21.2 GM per 30 days) flunisolide soln 0.025% 1 QL (50 ML per 30 days) fluticasone propionate susp 50mcg/act 1 mometasone furoate susp 50mcg/act 1 QL (34 GM per 30 days) QVAR AERS 40MCG/ACT 2 QL (17.4 GM per 30 days) QVAR AERS 80MCG/ACT 2 QL (26.1 GM per 30 days)

Page 94 of 121
Drug Name Drug Tier Requirements/Limits
SYMBICORT AERO 160MCG/ACT; 4.5MCG/ACT 2 QL (12 GM per 30 days) SYMBICORT AERO 80MCG/ACT; 4.5MCG/ACT 2 QL (13.8 GM per 30 days) triamcinolone acetonide aero 55mcg/act 1
Antihistamines azelastine hcl soln 0.1% 1 QL (60 ML per 30 days) azelastine hcl soln 0.15% 1 QL (60 ML per 30 days) cetirizine hcl syrp 1mg/ml 1 cyproheptadine hcl syrp 2mg/5ml 1 PA cyproheptadine hcl tabs 4mg 1 PA desloratadine tabs 5mg 1 dexchlorpheniramine maleate syrp 2mg/5ml 1 PA diphenhydramine hcl inj 50mg/ml 1 DYMISTA SUSP 137MCG/ACT; 50MCG/ACT 2 QL (23 GM per 30 days) hydroxyzine hcl inj 25mg/ml 1 PA hydroxyzine hcl inj 50mg/ml 1 PA hydroxyzine hcl syrp 10mg/5ml 1 PA hydroxyzine hcl tabs 10mg 1 PA hydroxyzine hcl tabs 25mg 1 PA hydroxyzine hcl tabs 50mg 1 PA hydroxyzine pamoate caps 100mg 1 PA hydroxyzine pamoate caps 25mg 1 PA hydroxyzine pamoate caps 50mg 1 PA levocetirizine dihydrochloride soln 2.5mg/5ml 1 levocetirizine dihydrochloride tabs 5mg 1 olopatadine hcl soln 0.6% 1 QL (30.5 GM per 30 days)
Antileukotrienes montelukast sodium chew 4mg 1 montelukast sodium chew 5mg 1 montelukast sodium pack 4mg 1 montelukast sodium tabs 10mg 1 zafirlukast tabs 10mg 1 zafirlukast tabs 20mg 1 ZYFLO CR TB12 600MG 4 ST ZYFLO TABS 600MG 4 ST
Bronchodilators, Anticholinergic COMBIVENT RESPIMAT AERS 100MCG/ACT; 20MCG/ACT
2 QL (8 GM per 30 days)
ipratropium bromide/albuterol sulfate soln 2.5mg/3ml; 0.5mg/3ml
1 QL (540 ML per 30 days) B/D
ipratropium bromide soln 0.02% 1 QL (312.5 ML per 30 days) B/D ipratropium bromide soln 0.03% 1 ipratropium bromide soln 0.06% 1 SPIRIVA HANDIHALER CAPS 18MCG 2 QL (30 EA per 30 days) SPIRIVA RESPIMAT AERS 1.25MCG/ACT 2 QL (4 GM per 30 days) SPIRIVA RESPIMAT AERS 2.5MCG/ACT 2 QL (4 GM per 30 days)
Bronchodilators, Sympathomimetic albuterol sulfate nebu 0.083% 1 QL (525 ML per 30 days) B/D albuterol sulfate nebu 0.5% 1 QL (100 ML per 30 days) B/D albuterol sulfate nebu 0.63mg/3ml 1 QL (375 ML per 30 days) B/D

Page 95 of 121
Drug Name Drug Tier Requirements/Limits
albuterol sulfate nebu 1.25mg/3ml 1 QL (375 ML per 30 days) B/D ANORO ELLIPTA AEPB 62.5MCG/INH; 25MCG/INH 2 QL (60 EA per 30 days) epinephrine inj 0.15mg/0.15ml 1 epinephrine inj 0.3mg/0.3ml 1 EPIPEN 2-PAK INJ 0.3MG/0.3ML 2 EPIPEN-JR 2-PAK INJ 0.15MG/0.3ML 2 levalbuterol hcl nebu 0.31mg/3ml 1 QL (540 ML per 30 days) B/D levalbuterol hcl nebu 0.63mg/3ml 1 QL (540 ML per 30 days) B/D levalbuterol hcl nebu 1.25mg/3ml 1 QL (270 ML per 30 days) B/D levalbuterol nebu 1.25mg/0.5ml 1 QL (90 EA per 30 days) B/D PROAIR HFA AERS 108MCG/ACT 2 QL (17 GM per 30 days) PROAIR RESPICLICK AEPB 108MCG/ACT 2 QL (2 EA per 30 days) SEREVENT DISKUS AEPB 50MCG/DOSE 2 QL (60 EA per 30 days) terbutaline sulfate inj 1mg/ml 4
Cystic Fibrosis Agents BETHKIS NEBU 300MG/4ML 4 B/D CAYSTON SOLR 75MG 4 PA KALYDECO PACK 50MG 4 PA KALYDECO PACK 75MG 4 PA KALYDECO TABS 150MG 4 PA ORKAMBI TABS 125MG; 200MG 4 QL (112 EA per 28 days) PA PULMOZYME SOLN 1MG/ML 4 PA TOBI PODHALER CAPS 28MG 4 QL (224 EA per 56 days) TOBI NEBU 300MG/5ML 4 B/D tobramycin nebu 300mg/5ml 4 B/D
Mast Cell Stabilizers cromolyn sodium nebu 20mg/2ml 1 B/D
Phosphodiesterase Inhibitors, Airways Disease aminophylline inj 25mg/ml 1 theophylline cr tb12 100mg 1 theophylline cr tb12 200mg 1 theophylline er tb12 100mg 1 theophylline er tb12 300mg 1 theophylline er tb12 450mg 1 theophylline er tb24 400mg 1 theophylline er tb24 600mg 1 theophylline/d5w inj 5%; 0.8mg/ml 1 theophylline soln 80mg/15ml 1
Pulmonary Antihypertensives ADCIRCA TABS 20MG 4 QL (60 EA per 30 days) PA ADEMPAS TABS 0.5MG 4 QL (90 EA per 30 days) PA ADEMPAS TABS 1.5MG 4 QL (90 EA per 30 days) PA ADEMPAS TABS 1MG 4 QL (90 EA per 30 days) PA ADEMPAS TABS 2.5MG 4 QL (90 EA per 30 days) PA ADEMPAS TABS 2MG 4 QL (90 EA per 30 days) PA epoprostenol sodium inj 0.5mg 4 PA epoprostenol sodium inj 1.5mg 4 PA LETAIRIS TABS 10MG 4 QL (30 EA per 30 days) PA LETAIRIS TABS 5MG 4 QL (30 EA per 30 days) PA

Page 96 of 121
Drug Name Drug Tier Requirements/Limits
OPSUMIT TABS 10MG 4 QL (30 EA per 30 days) PA ORENITRAM TBCR 0.25MG 4 PA ORENITRAM TBCR 1MG 4 PA ORENITRAM TBCR 2.5MG 4 PA REMODULIN INJ 10MG/ML 4 PA REMODULIN INJ 1MG/ML 4 PA REMODULIN INJ 2.5MG/ML 4 PA REMODULIN INJ 5MG/ML 4 PA REVATIO SUSR 10MG/ML 4 PA sildenafil inj 10mg/12.5ml 4 PA sildenafil tabs 20mg 1 QL (90 EA per 30 days) PA TYVASO REFILL SOLN 0.6MG/ML 4 QL (87 ML per 30 days) PA TYVASO STARTER SOLN 0.6MG/ML 4 QL (87 ML per 30 days) PA TYVASO SOLN 0.6MG/ML 4 QL (87 ML per 30 days) PA UPTRAVI TABS 1000MCG 4 QL (60 EA per 30 days) PA UPTRAVI TABS 1200MCG 4 QL (60 EA per 30 days) PA UPTRAVI TABS 1400MCG 4 QL (60 EA per 30 days) PA UPTRAVI TABS 1600MCG 4 QL (60 EA per 30 days) PA UPTRAVI TABS 200MCG 4 QL (60 EA per 30 days) PA UPTRAVI TABS 400MCG 4 QL (60 EA per 30 days) PA UPTRAVI TABS 600MCG 4 QL (60 EA per 30 days) PA UPTRAVI TABS 800MCG 4 QL (60 EA per 30 days) PA UPTRAVI TBPK 0 4 QL (400 EA per 365 days) PA VELETRI INJ 0.5MG 4 PA VELETRI INJ 1.5MG 4 PA VENTAVIS SOLN 10MCG/ML 4 QL (270 ML per 30 days) PA VENTAVIS SOLN 20MCG/ML 4 QL (270 ML per 30 days) PA
Respiratory Tract Agents, Other acetylcysteine soln 10% 1 B/D acetylcysteine soln 20% 1 B/D ARALAST NP INJ 1000MG 4 PA ARALAST NP INJ 500MG 4 PA ESBRIET CAPS 267MG 4 PA GLASSIA INJ 1000MG/50ML 4 PA OFEV CAPS 100MG 4 PA OFEV CAPS 150MG 4 PA PROLASTIN-C INJ 1000MG 4 PA promethazine vc plain syrp 5mg/5ml; 6.25mg/5ml 1 PA promethazine/phenylephrine syrp 5mg/5ml; 6.25mg/5ml 1 PA STIOLTO RESPIMAT AERS 2.5MCG/ACT; 2.5MCG/ACT 2 QL (4 GM per 30 days) VIRAZOLE SOLR 6GM 4 XOLAIR INJ 150MG 4 PA ZEMAIRA INJ 1000MG 4 PA
Skeletal Muscle Relaxants Skeletal Muscle Relaxants
carisoprodol tabs 250mg 1 PA carisoprodol tabs 350mg 1 PA chlorzoxazone tabs 500mg 1 PA cyclobenzaprine hcl tabs 10mg 1 PA

Page 97 of 121
Drug Name Drug Tier Requirements/Limits
cyclobenzaprine hcl tabs 5mg 1 PA cyclobenzaprine hcl tabs 7.5mg 1 PA methocarbamol tabs 500mg 1 PA methocarbamol tabs 750mg 1 PA orphenadrine citrate er tb12 100mg 1 PA
Sleep Disorder Agents GABA Receptor Modulators
eszopiclone tabs 1mg 1 QL (30 EA per 30 days) PA eszopiclone tabs 2mg 1 QL (30 EA per 30 days) PA eszopiclone tabs 3mg 1 QL (30 EA per 30 days) PA temazepam caps 15mg 1 QL (30 EA per 30 days) PA temazepam caps 22.5mg 1 QL (30 EA per 30 days) PA temazepam caps 30mg 1 QL (30 EA per 30 days) PA temazepam caps 7.5mg 1 QL (30 EA per 30 days) PA zaleplon caps 10mg 1 QL (60 EA per 30 days) PA zaleplon caps 5mg 1 QL (30 EA per 30 days) PA zolpidem tartrate er tbcr 12.5mg 1 QL (30 EA per 30 days) PA zolpidem tartrate er tbcr 6.25mg 1 QL (30 EA per 30 days) PA zolpidem tartrate subl 1.75mg 1 QL (30 EA per 30 days) PA zolpidem tartrate subl 3.5mg 1 QL (30 EA per 30 days) PA zolpidem tartrate tabs 10mg 1 QL (30 EA per 30 days) PA zolpidem tartrate tabs 5mg 1 QL (30 EA per 30 days) PA
Sleep Disorders, Other modafinil tabs 100mg 1 QL (30 EA per 30 days) PA modafinil tabs 200mg 1 QL (30 EA per 30 days) PA phenobarbital sodium inj 130mg/ml 1 PA phenobarbital sodium inj 65mg/ml 1 PA SILENOR TABS 3MG 2 QL (30 EA per 30 days) SILENOR TABS 6MG 2 QL (30 EA per 30 days) XYREM SOLN 500MG/ML 4 QL (540 ML per 30 days) PA
Therapeutic Nutrients/Minerals/Electrolytes Electrolyte/Mineral Modifiers
CARBAGLU TABS 200MG 4 CUPRIMINE CAPS 250MG 4 DEPEN TITRATABS TABS 250MG 4 EXJADE TBSO 125MG 4 PA EXJADE TBSO 250MG 4 PA EXJADE TBSO 500MG 4 PA FERRIPROX SOLN 100MG/ML 4 PA FERRIPROX TABS 500MG 4 PA JADENU TABS 180MG 4 PA JADENU TABS 360MG 4 PA JADENU TABS 90MG 4 PA kionex powd 0 1 kionex susp 15gm/60ml 1 SAMSCA TABS 15MG 4 QL (30 EA per 60 days) SAMSCA TABS 30MG 4 QL (60 EA per 30 days) sodium acetate inj 2meq/ml 1 sodium lactate inj 5meq/ml 1

Page 98 of 121
Drug Name Drug Tier Requirements/Limits
sodium polystyrene sulfonate powd 0 1 sodium polystyrene sulfonate susp 15gm/60ml 1 sodium polystyrene sulfonate susp 30gm/120ml 1 sps susp 15gm/60ml 1 SYPRINE CAPS 250MG 4
Electrolyte/Mineral Replacement aminosyn 8.5%/electrolytes inj 142meq/l; 1100mg/100ml; 850mg/100ml; 98meq/l; 1100mg/100ml; 260mg/100ml; 620mg/100ml; 810mg/100ml; 624mg/100ml; 10meq/l; 340mg/100ml; 380mg/100ml; 30meq/l; 65meq/l; 750mg/100ml; 370mg/100ml; 65meq/l; 460mg/100ml; 150mg/100ml; 44mg/100ml; 680mg/100ml
1 B/D
aminosyn ii 8.5%/electrolytes inj 61meq/l; 844mg/100ml; 865mg/100ml; 595mg/100ml; 86meq/l; 627mg/100ml; 425mg/100ml; 255mg/100ml; 561mg/100ml; 850mg/100ml; 893mg/100ml; 10meq/l; 146mg/100ml; 253mg/100ml; 30mmole/l; 66meq/l; 614mg/100ml; 450mg/100ml; 80meq/l; 340mg/100ml; 170mg/100ml; 230mg/100ml; 425mg/100ml
1 B/D
clinisol sf 15% inj 151meq/l; 2170mg/100ml; 1470mg/100ml; 434mg/100ml; 749mg/100ml; 1040mg/100ml; 894mg/100ml; 749mg/100ml; 1040mg/100ml; 1180mg/100ml; 749mg/100ml; 1040mg/100ml; 894mg/100ml; 592mg/100ml; 749mg/100ml; 250mg/100ml; 39mg/100ml; 960mg/100ml
1 B/D
dextrose 10%/nacl 0.45% inj 10%; 0.45% 1 dextrose 5% /electrolyte #48 viaflex inj 24meq/l; 5%; 23meq/l; 3meq/l; 3meq/l; 20meq/l; 25meq/l
1
dextrose 10%/nacl 0.2% inj 10%; 0.2% 1 dextrose 10% inj 10% 1 dextrose 2.5%/nacl 0.45% inj 2.5%; 0.45% 1 dextrose 20% inj 20% 1 dextrose 25% inj 250mg/ml 1 dextrose 30% inj 30% 1 dextrose 40% inj 40% 1 dextrose 5%/lactated ringers inj 2.7meq/l; 109meq/l; 5%; 28meq/l; 4meq/l; 130meq/l
1
dextrose 5%/nacl 0.2% inj 5%; 0.2% 1 dextrose 5%/nacl 0.225% inj 5%; 0.225% 1 dextrose 5%/nacl 0.3% inj 5%; 0.3% 1 dextrose 5%/nacl 0.33% inj 5%; 0.33% 1 dextrose 5%/nacl 0.45% inj 5%; 0.45% 1 dextrose 5%/nacl 0.9% inj 5%; 0.9% 1 dextrose 5%/potassium chloride 0.15% inj 5%; 20meq/l 1 dextrose 5% inj 5% 1 dextrose 50% inj 50% 1 dextrose 70% inj 70% 1 k-sol soln 10% 1 kcl 0.075%/d5w/nacl 0.45% inj 5%; 10meq/l; 0.45% 1 kcl 0.15%/d5w/ nacl 0.3% inj 5%; 20meq/l; 0.33% 1

Page 99 of 121
Drug Name Drug Tier Requirements/Limits
kcl 0.15%/d5w/lr inj 3meq/l; 149meq/l; 5%; 28meq/l; 24meq/l; 130meq/l
1
kcl 0.15%/d5w/nacl 0.2% inj 5%; 20meq/l; 0.2% 1 kcl 0.15%/d5w/nacl 0.225% inj 5%; 20meq/l; 0.225% 1 kcl 0.15%/d5w/nacl 0.45% inj 5%; 20meq/l; 0.45% 1 kcl 0.15%/d5w/nacl 0.9% inj 5%; 20meq/l; 0.9% 1 kcl 0.3%/d5w/lr iv lac ring inj 3meq/l; 149meq/l; 5%; 28meq/l; 44meq/l; 130meq/l
1
kcl 0.3%/d5w/nacl 0.45% inj 5%; 40meq/l; 0.45% 1 kcl 0.3%/d5w/nacl 0.9% inj 5%; 40meq/l; 0.9% 1 klor-con 10 tbcr 10meq 1 klor-con 8 tbcr 8meq 1 klor-con m10 tbcr 10meq 1 klor-con m15 tbcr 15meq 1 klor-con m20 tbcr 20meq 1 klor-con sprinkle cpcr 10meq 1 klor-con sprinkle cpcr 8meq 1 lactated ringers viaflex inj 3meq/l; 109meq/l; 28meq/l; 4meq/l; 130meq/l
1
magnesium sulfate inj 20gm/500ml 1 magnesium sulfate inj 2gm/50ml 1 magnesium sulfate inj 40gm/1000ml 1 magnesium sulfate inj 4gm/100ml 1 magnesium sulfate inj 4gm/50ml 1 magnesium sulfate inj 50% 1 magnesium sulfate inj 50% 1 normosol-r in d5w inj 27meq/l; 98meq/l; 5%; 23meq/l; 3meq/l; 5meq/l; 140meq/l
1
plenamine inj 151meq/l; 2170mg/100ml; 1470mg/100ml; 434mg/100ml; 749mg/100ml; 1040mg/100ml; 894mg/100ml; 749mg/100ml; 1040mg/100ml; 1180mg/100ml; 749mg/100ml; 1040mg/100ml; 894mg/100ml; 592mg/100ml; 749mg/100ml; 250mg/100ml; 39mg/100ml; 960mg/100ml
1 B/D
potassium acetate inj 2meq/ml 1 potassium chloride 0.15% /nacl 0.45% viaflex inj 20meq/l; 0.45%
1
potassium chloride 0.15% d5w/nacl 0.33% inj 5%; 20meq/l; 0.33%
1
potassium chloride 0.15% d5w/nacl 0.45% inj 5%; 20meq/l; 0.45%
1
potassium chloride 0.15%/nacl 0.9% inj 20meq/l; 0.9% 1 potassium chloride 0.22% d5w/nacl 0.45% inj 5%; 30meq/l; 0.45%
1
potassium chloride 0.224%/d5w/nacl 0.45% inj 5%; 30meq/l; 0.45%
1
potassium chloride 0.3%/ nacl 0.9% inj 40meq/l; 0.9% 1 potassium chloride 0.3%/d5w inj 5%; 40meq/l 1 potassium chloride cr tbcr 10meq 1 potassium chloride cr tbcr 10meq 1

Page 100 of 121
Drug Name Drug Tier Requirements/Limits
potassium chloride er cpcr 10meq 1 potassium chloride er cpcr 8meq 1 potassium chloride er tbcr 10meq 1 potassium chloride er tbcr 10meq 1 potassium chloride er tbcr 20meq 1 potassium chloride er tbcr 20meq 1 potassium chloride er tbcr 8meq 1 potassium chloride sr tbcr 8meq 1 potassium chloride inj 10meq/100ml 1 potassium chloride inj 10meq/50ml 1 potassium chloride inj 20meq/100ml 1 potassium chloride inj 20meq/50ml 1 potassium chloride inj 2meq/ml 1 potassium chloride inj 40meq/100ml 1 potassium chloride pack 20meq 1 potassium chloride soln 10% 1 potassium chloride soln 20% 1 potassium citrate er tbcr 1080mg 1 potassium citrate er tbcr 15meq 1 potassium citrate er tbcr 540mg 1 premasol inj 56meq/l; 320mg/100ml; 730mg/100ml; 190mg/100ml; 3meq/l; 20mg/100ml; 300mg/100ml; 220mg/100ml; 290mg/100ml; 490mg/100ml; 840mg/100ml; 490mg/100ml; 200mg/100ml; 290mg/100ml; 410mg/100ml; 230mg/100ml; 5meq/l; 15mg/100ml; 250mg/100ml; 120mg/100ml; 140mg/100ml; 470mg/100ml
1 B/D
ringers injection inj 4.5meq/l; 156meq/l; 4meq/l; 147meq/l 1 sodium chloride 0.45% inj 0.45% 1 sodium chloride 0.9% soln 0.9% 1 sodium chloride inj 0.9% 1 sodium chloride inj 0.9% 1 sodium chloride inj 2.5meq/ml 1 sodium chloride inj 3% 1 sodium chloride inj 5% 1 sodium fluoride tabs 1mg 1 sodium phosphate inj 3mmole/ml 1 tpn electrolytes inj 29.5meq/20ml; 4.5meq/20ml; 35meq/20ml; 5meq/20ml; 20meq/20ml; 35meq/20ml
1

Page 101 of 121
Index Drug Name Page #
abacavir 45abacavir sulfate/lamivudine/zidovudine 45
ABELCET 28ABILIFY MAINTENA 41
ABRAXANE 33ABSTRAL 8
acamprosate calcium dr 12acarbose 48
acebutolol hcl 56acetaminophen/codeine 8
acetaminophen/codeine #3 8acetasol hc 93
acetazolamide 61acetazolamide er 92
acetazolamide sodium 61acetic acid 93
acetic acid 0.25% 73acetic acid/aluminum acetate 93
acetylcysteine 96acitretin 68
ACTEMRA 87ACTHIB 88
ACTIMMUNE 88ACTIQ 9
acyclovir 46acyclovir sodium 46
ADACEL 88ADAGEN 69adapalene 68
adapalene pump 68ADCIRCA 95
adefovir dipivoxil 43ADEMPAS 95
adrucil 32ADVAIR DISKUS 93
ADVAIR HFA 93afeditab cr 58
AFINITOR 36AFINITOR DISPERZ 36
ALBENZA 38albuterol sulfate 94
alclometasone dipropionate 74ALCOHOL PREP PADS 13
ALDURAZYME 69ALECENSA 36
alendronate sodium 89alfuzosin hcl er 73
Drug Name Page #ALIMTA 32
allopurinol 30almotriptan 30
almotriptan malate 30alosetron hydrochloride 71
ALPHAGAN P 92alprazolam 47
alprazolam er 46alprazolam intensol 47
alprazolam odt 47alprazolam xr 47
ALREX 92altavera 78
alyacen 1/35 78alyacen 7/7/7 78
amantadine hcl 46AMBISOME 28
amcinonide 74amethia 78
amethia lo 78amethyst 78
amifostine 33amikacin sulfate 12
amiloride hcl 62amiloride/hydrochlorothiazide 62
aminocaproic acid 52aminophylline 95
aminosyn 8.5%/electrolytes 98aminosyn ii 8.5%/electrolytes 98
amiodarone hcl 55AMITIZA 71
amitriptyline hcl 26amlodipine besylate 58
amlodipine besylate/atorvastatin calcium 58amlodipine besylate/benazepril
hydrochloride58
amlodipine besylate/valsartan 58amlodipine/valsartan/hctz 58
ammonium lactate 68AMMONUL 90
amnesteem 68amoxapine 27amoxicillin 17
amoxicillin/clavulanate potassium 17amoxicillin/clavulanate potassium er 17
amphetamine/dextroamphetamine 65amphotericin b 28
ampicillin 18ampicillin sodium 17
ampicillin-sulbactam 18

Page 102 of 121
Drug Name Page #AMPYRA 67
ANADROL-50 78anagrelide hydrochloride 51
anastrozole 35ANDRODERM 78
ANDROGEL 78ANDROGEL PUMP 78
ANORO ELLIPTA 95ANZEMET 28APLENZIN 25
APOKYN 39apraclonidine 92
apri 78APRISO 89
APTIOM 21APTIVUS 46
ARALAST NP 96aranelle 78
ARANESP ALBUMIN FREE 51ARCALYST 88
ARESTIN 67argatroban 50
aripiprazole 41aripiprazole odt 41
ARISTADA 41ARZERRA 37
ascomp/codeine 9ashlyna 78
aspirin/dipyridamole 52aspirin-caffeine-dihydrocodeine 9
ASTAGRAF XL 85atenolol 57
atenolol/chlorthalidone 57ATGAM 86
atorvastatin calcium 63atovaquone 38
atovaquone/proguanil hcl 38ATRIPLA 44
atropine sulfate 91AUBAGIO 67
aubra 78augmented betamethasone dipropionate 74
AVASTIN 37aviane 78
avita 68AVONEX 67
AVONEX PEN 67AVYCAZ 15azacitidine 33
azathioprine 85
Drug Name Page #azelastine hcl 92azelastine hcl 94
AZILECT 40azithromycin 18
AZOPT 92aztreonam 17
azurette 78baciim 13
bacitracin 13bacitracin/polymyxin b 91
baclofen 43balsalazide disodium 89
balziva 78BANZEL 23
BARACLUDE 43baycadron 74
BD INSULIN SYRINGE SAFETYGLIDE/1ML/29G X 1/2"
90
BD INSULIN SYRINGE ULTRAFINE/0.3ML/31G X 5/16"
90
BD INSULIN SYRINGE ULTRAFINE/0.5ML/30G X 1/2"
90
BD INSULIN SYRINGE ULTRAFINE/1ML/31G X 5/16"
90
BD PEN NEEDLE/ULTRAFINE/29G X 12.7MM
90
bekyree 78BELEODAQ 33
benazepril hcl 54benazepril hcl/hydrochlorothiazide 54
BENDEKA 31BENICAR 53
BENICAR HCT 53BENLYSTA 85
benztropine mesylate 38BERINERT 85
BESIVANCE 19betamethasone dipropionate 74
betamethasone sodium phosphate/betamethasone acetate
74
betamethasone valerate 74BETASERON 67
betaxolol hcl 57betaxolol hcl 92
bethanechol chloride 73BETHKIS 95bexarotene 38BEXSERO 88
bicalutamide 32BICNU 31

Page 103 of 121
Drug Name Page #BIDIL 64
BILTRICIDE 38bimatoprost 91
bisoprolol fumarate 57bisoprolol fumarate/hydrochlorothiazide 57
BIVIGAM 86bleomycin sulfate 33
BLINCYTO 37blisovi 24 fe 78
blisovi fe 1.5/30 78blisovi fe 1/20 78
BOOSTRIX 88BOSULIF 36
BREO ELLIPTA 93briellyn 78
BRILINTA 52brimonidine tartrate 92
BRIVIACT 21bromfenac 92
budesonide 74budesonide 93bumetanide 61
BUPHENYL 69buprenorphine hcl 7buprenorphine hcl 12
buprenorphine hcl/naloxone hcl 12buproban 12
bupropion hcl 25bupropion hcl er 25bupropion hcl sr 12bupropion hcl sr 25bupropion hcl xl 25
buspirone hcl 46BUSULFEX 31
butalbital/acetaminophen 66butalbital/acetaminophen/caffeine 66
butalbital/acetaminophen/caffeine/codeine 66butalbital/aspirin/caffeine 66
butalbital/aspirin/caffeine/codeine 9butorphanol tartrate 9
BYDUREON 48BYDUREON PEN 48
BYSTOLIC 57cabergoline 84
CABOMETYX 36caffeine citrate 66
calcipotriene 68calcipotriene/betamethasone dipropionate 68
calcitonin-salmon 89calcitrene 68
Drug Name Page #calcitriol 68calcitriol 90
calcium acetate 73camila 82
camrese 78camrese lo 78CANASA 89
CANCIDAS 28candesartan cilexetil 53
candesartan cilexetil/hydrochlorothiazide 53capacet 66
CAPRELSA 36captopril 54
captopril/hydrochlorothiazide 54CARBAGLU 97
carbamazepine 23carbamazepine er 23
carbidopa 39carbidopa/levodopa 39
carbidopa/levodopa er 39carbidopa/levodopa odt 39
carbidopa/levodopa/entacapone 39carboplatin 33
CARIMUNE NANOFILTERED 86carisoprodol 96carteolol hcl 93
cartia xt 59carvedilol 57
CAYSTON 95caziant 78
cefadroxil 15cefazolin 15
cefazolin sodium 15cefazolin sodium/dextrose 15
cefdinir 15cefepime 15
cefepime/dextrose 15cefixime 15
cefotaxime sodium 15cefotetan 17
cefotetan/dextrose 15cefoxitin sodium 15
cefpodoxime proxetil 15cefprozil 16
ceftazidime 16ceftazidime/dextrose 16
ceftibuten 16ceftriaxone in iso-osmotic dextrose 16
ceftriaxone sodium 16ceftriaxone/dextrose 16

Page 104 of 121
Drug Name Page #cefuroxime axetil 16
cefuroxime sodium 16celecoxib 6
CELLCEPT 85cephalexin 16
CERDELGA 70CEREZYME 70CERVARIX 88cetirizine hcl 94
cevimeline hcl 67chateal 78
CHENODAL 71chloramphenicol sodium succinate 13
chlordiazepoxide hcl 47chlordiazepoxide/amitriptyline 27
chlorhexidine gluconate oral rinse 67chloroquine phosphate 38
chlorothiazide 62chlorothiazide sodium 62
chlorpromazine hcl 40chlorthalidone 62chlorzoxazone 96
CHOLBAM 71cholestyramine light 63
ciclodan 28ciclodan cream kit 28
ciclodan solution kit 28ciclopirox 29
ciclopirox nail lacquer 28ciclopirox olamine 29
cidofovir 43cilostazol 52
cimetidine 71cimetidine hcl 71
CIMZIA 85CIMZIA STARTER KIT 85
CINRYZE 85CIPRODEX 93
ciprofloxacin 19ciprofloxacin er 19
ciprofloxacin hcl 19ciprofloxacin i.v.-in d5w 19
cisplatin 33citalopram hydrobromide 25
cladribine 32claravis 68
clarithromycin 19clarithromycin er 19clin single use kit 13
clindacin etz 13
Drug Name Page #clindacin etz pledgets 13
clindacin pac 13clindacin-p 13clindamax 13
clindamycin 13clindamycin hcl 13
clindamycin palmitate hcl 13clindamycin phosphate 13
clindamycin phosphate add-vantage 13clindamycin phosphate in d5w 13
clindamycin phosphate pharmacy bulk package
13
clindamycin phosphate/tretinoin 68clindamycin/benzoyl peroxide 68
clinisol sf 15% 98clobetasol propionate 74
clobetasol propionate e 74clobetasol propionate emollient 74
clocortolone pivalate 74clocortolone pivalate pump 74
clodan 74CLOLAR 32
clomipramine hcl 27clonazepam 22
clonazepam odt 22clonidine hcl 53
clonidine hcl er 65clopidogrel 52
clorazepate dipotassium 47clotrimazole 29
clotrimazole/betamethasone dipropionate 68clozapine 43
clozapine odt 43codeine sulfate 9
colchicine 30colestipol hcl 63
colistimethate sodium 13colocort 74
COMBIGAN 91COMBIVENT RESPIMAT 94
COMETRIQ 36COMPLERA 44
compro 40COMVAX 88constulose 72
COPAXONE 67cormax scalp application 74
cortisone acetate 74COSENTYX 68
COSENTYX SENSOREADY PEN 68

Page 105 of 121
Drug Name Page #COSMEGEN 33
COTELLIC 33CREON 70
CRESEMBA 29CRIXIVAN 46
cromolyn sodium 71cromolyn sodium 92cromolyn sodium 95
cryselle-28 78CUBICIN 13
CUPRIMINE 97CURITY GAUZE PADS 2"X2" 68
cyclafem 1/35 79cyclafem 7/7/7 79
cyclobenzaprine hcl 96cyclopentolate hcl 91
cyclopentolate hydrochloride 91cyclophosphamide 31
cycloserine 31cyclosporine 85
cyclosporine modified 85cyproheptadine hcl 94
CYRAMZA 37cyred 79
CYSTADANE 70CYSTARAN 91
cytarabine aqueous 32dacarbazine 31DAKLINZA 44
DALVANCE 13danazol 78
dantrolene sodium 43dapsone 31
DAPTACEL 88DARAPRIM 38
darifenacin hydrobromide er 73DARZALEX 37dasetta 1/35 79
dasetta 7/7/7 79daunorubicin hcl 33
daysee 79deblitane 82
decitabine 33deferoxamine mesylate 90
deltasone 74delyla 79
demeclocycline hcl 20DEMSER 60
DENAVIR 46DEPEN TITRATABS 97
Drug Name Page #DEPOCYT 33DESCOVY 45
desipramine hcl 27desloratadine 94
desmopressin acetate 77desogestrel/ethinyl estradiol 79
desonate 68desonide 74
desoximetasone 75dexamethasone 75
dexamethasone intensol 75dexamethasone sodium phosphate 75dexamethasone sodium phosphate 92
dexchlorpheniramine maleate 94dexmethylphenidate hcl 65
dexmethylphenidate hcl er 65dexrazoxane 33
dextroamphetamine sulfate 65dextroamphetamine sulfate er 65
dextrose 10%/nacl 0.45% 98dextrose 5% /electrolyte #48 viaflex 98
dextrose 10% 98dextrose 10%/nacl 0.2% 98
dextrose 2.5%/nacl 0.45% 98dextrose 20% 98dextrose 25% 98dextrose 30% 98dextrose 40% 98
dextrose 5% 98dextrose 5%/lactated ringers 98
dextrose 5%/nacl 0.2% 98dextrose 5%/nacl 0.225% 98
dextrose 5%/nacl 0.3% 98dextrose 5%/nacl 0.33% 98dextrose 5%/nacl 0.45% 98dextrose 5%/nacl 0.9% 98
dextrose 5%/potassium chloride 0.15% 98dextrose 50% 98dextrose 70% 98
diazepam 22diazepam 47
diazepam intensol 47diclofenac sodium 12diclofenac sodium 68diclofenac sodium 92
diclofenac sodium dr 6diclofenac sodium er 6dicloxacillin sodium 18
dicyclomine hcl 70didanosine 45

Page 106 of 121
Drug Name Page #DIFICID 19
diflorasone diacetate 75diflunisal 6
digitek 60digox 61
digoxin 60dihydroergotamine mesylate 30
diltiazem cd 59diltiazem hcl 59
diltiazem hcl cd 59diltiazem hcl er 59
dilt-xr 59DIPENTUM 89
diphenhydramine hcl 94diphtheria/tetanus toxoids adsorbed
pediatric 88
dipyridamole 52disopyramide phosphate 56
disulfiram 12divalproex sodium 22
divalproex sodium dr 22divalproex sodium er 22
dobutamine hcl 61dobutamine hcl/d5w 61
dobutamine/dextrose 5% 61DOCEFREZ 33
docetaxel 33dofetilide 56
donepezil hcl 24dopamine hcl 61
dopamine hcl/dextrose 5% 61dopamine hcl-dextrose 5% 61
dopamine/d5w 61dorzolamide hcl 93
dorzolamide hcl/timolol maleate 93doxazosin 73
doxazosin mesylate 73doxepin hcl 27
doxepin hydrochloride 68doxercalciferol 90doxorubicin hcl 34
doxorubicin hcl liposome 34doxy 100 20
doxycycline 20doxycycline 68
doxycycline hyclate 20doxycycline hyclate dr 20
doxycycline monohydrate 20dronabinol 28droperidol 27
Drug Name Page #drospirenone/ethinyl estradiol 79
duloxetine hcl 25duramorph 9DUREZOL 92dutasteride 73
dutasteride/tamsulosin hydrochloride 73DYMISTA 94
econazole nitrate 29EDECRIN 62
EDURANT 44EFFIENT 52EGRIFTA 77
ELAPRASE 70ELIGARD 84
elinest 79eliphos 73
ELIQUIS 50ELITEK 33
ELLA 82EMBEDA 7
EMCYT 32emoquette 79
EMPLICITI 37EMSAM 25
enalapril maleate 54enalapril maleate/hydrochlorothiazide 54
enalaprilat 54ENBREL 85
ENBREL SURECLICK 85endocet 9
ENGERIX-B 88enoxaparin sodium 50
enpresse-28 79enskyce 79
entacapone 39entecavir 43
ENTYVIO 70enulose 72
epinastine hcl 92epinephrine 95
EPIPEN 2-PAK 95EPIPEN-JR 2-PAK 95
epirubicin hcl 34epitol 23
eplerenone 62EPOGEN 52
epoprostenol sodium 95eprosartan mesylate 53
EPZICOM 45ERAXIS 29

Page 107 of 121
Drug Name Page #ERBITUX 37
ERGOLOID MESYLATES 24ERGOMAR 30ERIVEDGE 36
errin 82ERWINAZE 34
ery 19ERY-TAB 19
erythrocin lactobionate 19erythromycin 19
erythromycin base 19erythromycin ethylsuccinate 19
erythromycin/benzoyl peroxide 68ESBRIET 96
escitalopram oxalate 25esgic 66
esmolol hcl 57esomeprazole magnesium 72
esomeprazole sodium 72estarylla 79
estazolam 47estradiol 79
estradiol valerate 79estradiol/norethindrone acetate 79
estropipate 79eszopiclone 97
ethacrynic acid 62ethambutol hcl 31
ethosuximide 21etidronate disodium 90
etodolac 6etodolac er 6
ETOPOPHOS 36etoposide 36
EVOMELA 31EVOTAZ 46
exemestane 35EXJADE 97
EXTAVIA 67EYLEA 91
FABRAZYME 70falmina 79
famciclovir 46famotidine 71
famotidine premixed 71FANAPT 41
FARESTON 32FARYDAK 34
FASLODEX 32FAZACLO 43
Drug Name Page #felbamate 23
felodipine er 59fenofibrate 63
fenofibrate micronized 62fenofibric acid 63
fenofibric acid dr 63fenoprofen calcium 6
fentanyl 7fentanyl citrate 9
fentanyl citrate oral transmucosal 9FENTORA 9
FERRIPROX 97FINACEA 68finasteride 73FIRAZYR 85
FIRMAGON 84FLAREX 92
flavoxate hcl 73FLEBOGAMMA DIF 86
flecainide acetate 56FLOVENT DISKUS 93
FLOVENT HFA 93floxuridine 33fluconazole 29
fluconazole in dextrose 29fluconazole in nacl 29
flucytosine 29fludarabine phosphate 34
fludrocortisone acetate 75flunisolide 93
fluocinolone acetonide 69fluocinolone acetonide 75
fluocinolone acetonide body 69fluocinolone acetonide ear drops 75
fluocinolone acetonide scalp 69fluocinonide 75
fluocinonide-e 75fluorometholone 92
fluorouracil 33fluorouracil 69
fluoxetine 26fluoxetine dr 25
fluoxetine hcl 26fluphenazine decanoate 40
fluphenazine hcl 40flurandrenolide 75
flurbiprofen 6flurbiprofen sodium 92
flutamide 32fluticasone propionate 75

Page 108 of 121
Drug Name Page #fluticasone propionate 93
fluvastatin 63fluvastatin sodium er 63fluvoxamine maleate 26
fluvoxamine maleate er 26FML 92
FML FORTE 92FOLOTYN 33
fondaparinux sodium 50FORFIVO XL 25
FORTEO 90fosinopril sodium 55
fosinopril sodium/hydrochlorothiazide 54fosphenytoin sodium 24
FOSRENOL 73FRAGMIN 50
frovatriptan succinate 30furosemide 62FUSILEV 34FUZEON 45
fyavolv 79gabapentin 22
GABLOFEN 43galantamine hydrobromide 24
GAMASTAN S/D 86GAMMAGARD LIQUID 86
GAMMAGARD S/D IGA LESS THAN 1MCG/ML
87
GAMMAKED 87GAMMAPLEX 87GAMUNEX-C 87
ganciclovir 43GARDASIL 88
GARDASIL 9 88gatifloxacin 19
GATTEX 71gavilyte-c 72gavilyte-g 72gavilyte-h 71
gavilyte-n/flavor pack 72GAZYVA 37
gemcitabine 33gemcitabine hcl 33
gemfibrozil 63generlac 72gengraf 85
GENOTROPIN 77GENOTROPIN MINIQUICK 77
gentak 12gentamicin sulfate 12
Drug Name Page #gentamicin sulfate pediatric 12
gentamicin sulfate/0.9% sodium chloride 12GENVOYA 44
gianvi 79gildagia 79
gildess 1.5/30 79gildess 1/20 79gildess 24 fe 79
gildess fe 1.5/30 79gildess fe 1/20 79
GILENYA 67GILOTRIF 34GLASSIA 96
glatopa 67GLEEVEC 36glimepiride 48
glipizide 48glipizide er 48glipizide xl 48
glipizide/metformin hcl 48GLUCAGON EMERGENCY KIT 49
glyburide 48glyburide micronized 48
glyburide/metformin hcl 48glycopyrrolate 70
glydo 11granisetron hcl 28
GRANIX 52griseofulvin microsize 29
griseofulvin ultramicrosize 29guanfacine er 65
guanfacine hcl 53H.P. ACTHAR 77
HALAVEN 34halobetasol propionate 75
haloperidol 40haloperidol decanoate 40
haloperidol lactate 40HARVONI 44
HAVRIX 88heather 82hecoria 85
HEPAGAM B 87heparin sodium 51
heparin sodium/d5w 51heparin sodium/nacl 51
heparin sodium/nacl 0.45% 51heparin sodium/nacl 0.9% 51
heparin sodium/sodium chloride 0.9% 51

Page 109 of 121
Drug Name Page #heparin sodium/sodium chloride 0.9%
premix 51
HERCEPTIN 37HETLIOZ 66
HEXALEN 31HIBERIX 88
HIZENTRA 87HUMALOG 50
HUMALOG KWIKPEN 49HUMALOG MIX 50/50 49
HUMALOG MIX 50/50 KWIKPEN 49HUMALOG MIX 75/25 50
HUMALOG MIX 75/25 KWIKPEN 50HUMATROPE 77
HUMATROPE COMBO PACK 77HUMIRA 85
HUMIRA PEDIATRIC CROHNS DISEASE STARTER PACK
85
HUMIRA PEN 85HUMIRA PEN-CROHNS
DISEASESTARTER 85
HUMIRA PEN-PSORIASIS STARTER 85HUMULIN 70/30 50
HUMULIN 70/30 KWIKPEN 50HUMULIN N 50
HUMULIN N KWIKPEN 50HUMULIN R 50
HUMULIN R U-500 (CONCENTRATED) 50HUMULIN R U-500 KWIKPEN 50
hydralazine hcl 64hydrochlorothiazide 62
hydrocodone bitartrate/acetaminophen 9hydrocodone/acetaminophen 9
hydrocodone/ibuprofen 9hydrocortisone 76
hydrocortisone butyrate 75hydrocortisone butyrate (lipophilic) 75
hydrocortisone valerate 75hydrocortisone/acetic acid 93
hydromorphone hcl 10hydromorphone hcl er 7
hydroxychloroquine sulfate 38hydroxyprogesterone caproate 82
hydroxyurea 33hydroxyzine hcl 94
hydroxyzine pamoate 94HYPERHEP B S/D 87
HYPERRAB S/D 87HYQVIA 88
ibandronate sodium 90
Drug Name Page #IBRANCE 34
ibudone 10ibuprofen 6
ibutilide fumarate 56ICLUSIG 36
idarubicin hcl 34ifosfamide 31
ILARIS 88ILEVRO 92
ilotycin 19imatinib mesylate 36
IMBRUVICA 36imipenem/cilastatin 17
imipramine hcl 27imipramine pamoate 27
imiquimod 69INCRELEX 77indapamide 62
indomethacin 6indomethacin er 6
INFANRIX 88INLYTA 36
INTELENCE 45INTRON A 43
INTRON A W/DILUENT 43introvale 79INVEGA 41
INVEGA SUSTENNA 41INVEGA TRINZA 41
INVIRASE 46INVOKAMET 48
INVOKANA 48IPOL INACTIVATED IPV 88
ipratropium bromide 94ipratropium bromide/albuterol sulfate 94
irbesartan 53irbesartan/hydrochlorothiazide 53
IRESSA 36irinotecan 34
irinotecan hcl 34ISENTRESS 44
isoniazid 31ISORDIL TITRADOSE 64
isosorbide dinitrate 64isosorbide dinitrate er 64
isosorbide mononitrate 64isosorbide mononitrate er 64
isotonic gentamicin 13ISTODAX 34
itraconazole 29

Page 110 of 121
Drug Name Page #ivermectin 38
IXEMPRA KIT 34IXIARO 88
JADENU 97JAKAFI 36jantoven 51
JANUMET 48JANUMET XR 48
JANUVIA 48JARDIANCE 48
jencycla 82jevantique lo 79
JEVTANA 34jinteli 80
jolessa 80jolivette 82juleber 80
junel 1.5/30 80junel 1/20 80
junel fe 1.5/30 80junel fe 1/20 80
junel fe 24 80JUXTAPID 63KADCYLA 37
kaitlib fe 80KALBITOR 91KALETRA 46
KALYDECO 95KANUMA 70
kariva 80kcl 0.075%/d5w/nacl 0.45% 98
kcl 0.15%/d5w/ nacl 0.3% 98kcl 0.15%/d5w/lr 99
kcl 0.15%/d5w/nacl 0.2% 99kcl 0.15%/d5w/nacl 0.225% 99kcl 0.15%/d5w/nacl 0.45% 99kcl 0.15%/d5w/nacl 0.9% 99
kcl 0.3%/d5w/lr iv lac ring 99kcl 0.3%/d5w/nacl 0.45% 99kcl 0.3%/d5w/nacl 0.9% 99
kelnor 1/35 80KEPIVANCE 67ketoconazole 29
ketodan 29ketodan kit 29ketoprofen 6
ketoprofen er 6ketorolac tromethamine 6ketorolac tromethamine 92
KEVEYIS 91
Drug Name Page #KEYTRUDA 37
kimidess 80KINERET 85
KINRIX 88kionex 97
klor-con 10 99klor-con 8 99
klor-con m10 99klor-con m15 99klor-con m20 99
klor-con sprinkle 99KOMBIGLYZE XR 49
KORLYM 78k-sol 98
kurvelo 80KUVAN 70
KYNAMRO 64labetalol hcl 57
lactated ringers irrigation 91lactated ringers viaflex 99
lactulose 72LAMICTAL STARTER/TAKING
CARBAMAZEPINE/NOT TAKING VALPROATE
23
lamivudine 43lamivudine 45
lamivudine/zidovudine 45lamotrigine 23
lamotrigine er 23lamotrigine odt 23
lamotrigine titration 23lansoprazole 72
lansoprazole/amoxicillin/clarithromycin 71LANTUS 50
LANTUS SOLOSTAR 50larin 1.5/30 80
larin 1/20 80larin 24 fe 80
larin fe 1.5/30 80larin fe 1/20 80
larissia 80latanoprost 91LATUDA 41layolis fe 80
LAZANDA 10leena 80
leflunomide 88LEMTRADA 88
LENVIMA 10 MG DAILY DOSE 36LENVIMA 14 MG DAILY DOSE 36

Page 111 of 121
Drug Name Page #LENVIMA 18 MG DAILY DOSE 37LENVIMA 20 MG DAILY DOSE 37LENVIMA 24 MG DAILY DOSE 37LENVIMA 8 MG DAILY DOSE 37
lessina 80LETAIRIS 95
letrozole 35leucovorin calcium 34
LEUKINE 52leuprolide acetate 84
levalbuterol 95levalbuterol hcl 95
LEVEMIR 50LEVEMIR FLEXTOUCH 50
levetiracetam 21levetiracetam er 21levobunolol hcl 93
levocarnitine 91levocetirizine dihydrochloride 94
levofloxacin 19levofloxacin in d5w 19
levoleucovorin 34levoleucovorin calcium 34
levonest 80levonorgestrel 82
levonorgestrel and ethinyl estradiol 80levonorgestrel/ethinyl estradiol 80
levora 0.15/30-28 80levorphanol tartrate 7
levothyroxine sodium 83levoxyl 83
LEXIVA 46LIALDA 89lidocaine 12
lidocaine hcl 11lidocaine hcl 56
lidocaine hcl in d5w 56lidocaine hcl jelly 11
lidocaine hcl/dextrose 11lidocaine hcl/dextrose 56
lidocaine viscous 11lidocaine/epinephrine 11
lidocaine/prilocaine 11lincomycin hcl 13
linezolid 14LINZESS 71
LIORESAL INTRATHECAL 43liothyronine sodium 83
lipodox 34lipodox 50 34
Drug Name Page #lisinopril 55
lisinopril/hydrochlorothiazide 55lithium 48
lithium carbonate 47lithium carbonate er 47
lokara 76lomedia 24 fe 80
LONSURF 33loperamide hcl 71
lopreeza 80lorazepam 47
lorazepam intensol 47lorcet 10
lorcet plus 10lortab 10loryna 80
losartan potassium 54losartan potassium/hydrochlorothiazide 53
lovastatin 63low-ogestrel 80
loxapine succinate 40LUMIGAN 91
LUMIZYME 70LUPANETA PACK 84
LUPRON DEPOT 84LUPRON DEPOT-PED 84
lutera 80LYNPARZA 34
LYRICA 21LYSODREN 83
lyza 82mafenide acetate 14
magnesium sulfate 99magnesium sulfate in d5w 21
MAKENA 82malathion 38mannitol 61
maprotiline hcl 25margesic 66marlissa 80
marten-tab 66MATULANE 31
matzim la 59MAXIDEX 92
meclizine hcl 27meclofenamate sodium 6
medroxyprogesterone acetate 82mefenamic acid 6mefloquine hcl 38
megestrol acetate 82

Page 112 of 121
Drug Name Page #MEKINIST 37meloxicam 6
melphalan hydrochloride 32memantine hcl 24
memantine hcl titration pak 24memantine hydrochloride 24
MENACTRA 89MENHIBRIX 89
MENOMUNE-A/C/Y/W-135 89MENVEO 89
mercaptopurine 33meropenem 17
meropenem/sodium chloride 17mesalamine 89
mesna 35MESNEX 35
MESTINON 31metadate er 66
metformin hcl 49metformin hcl er 49
methadone hcl 7methadone hcl intensol 7
methadose 7methadose sugar-free 7
methazolamide 93methenamine hippurate 14
methergine 91methimazole 84
methocarbamol 97methotrexate 86
methotrexate sodium 85methoxsalen 69
methyclothiazide 62methyldopa 53
methyldopa/hydrochlorothiazide 53methyldopate hcl 53
methylergonovine maleate 91methylphenidate hcl 66
methylphenidate hcl cd 66methylphenidate hcl er 66methylphenidate hcl sr 66
methylphenidate hydrochloride 66methylprednisolone 76
methylprednisolone acetate 76methylprednisolone dose pack 76
methylprednisolone sodiumsuccinate 76methyltestosterone 78
metipranolol 93metoclopramide hcl 71metoclopramide odt 71
Drug Name Page #metolazone 62
metoprolol succinate er 57metoprolol tartrate 57
metoprolol/hydrochlorothiazide 57metro iv 14
metronidazole 14metronidazole in nacl 0.79% 14
metronidazole vaginal 14mexiletine hcl 56MIACALCIN 90miconazole 3 29
microgestin 1.5/30 80microgestin 1/20 80microgestin 24 fe 80
microgestin fe 80microgestin fe 1.5/30 80
midazolam hcl 47midodrine hcl 53
miglitol 49MIGRANAL 30
milrinone in dextrose 61milrinone lactate 61
mimvey 80mimvey lo 80
minitran 64minocycline hcl 20
minocycline hcl er 20mirtazapine 25
mirtazapine odt 25misoprostol 72
mitomycin 35mitoxantrone hcl 35
M-M-R II 89modafinil 97
MODERIBA 44moexipril hcl 55
moexipril/hydrochlorothiazide 55molindone hydrochloride 40
mometasone furoate 76mometasone furoate 93
mondoxyne nl 21mono-linyah 80
mononessa 80montelukast sodium 94morgidox 1x100mg 21morgidox 2x100mg 21
morphine sulfate 10morphine sulfate er 7
MOVIPREP 72MOXEZA 20

Page 113 of 121
Drug Name Page #moxifloxacin hcl 20
MOZOBIL 52MULTAQ 56mupirocin 14
mupirocin calcium 14MUSTARGEN 32
MYALEPT 91MYCAMINE 29
mycophenolate mofetil 86mycophenolic acid dr 86
myorisan 69MYOZYME 70
MYRBETRIQ 73myzilra 80
NABI-HB 87nabumetone 6
nadolol 57nadolol/bendroflumethiazide 57
nafcillin 18nafcillin sodium 18
naftifine hcl 29naftifine hydrochloride 29
NAGLAZYME 70nalbuphine hcl 10
naloxone hcl 12naltrexone hcl 12
NAMENDA XR 24NAMENDA XR TITRATION PACK 24
NAMZARIC 24naphazoline hcl 91
naproxen 7naproxen dr 6
naproxen sodium 7naproxen sodium cr 6naproxen sodium er 6
naratriptan hcl 30nateglinide 49NATPARA 91
necon 0.5/35-28 80necon 1/35 81
necon 1/50-28 81necon 10/11-28 81
necon 7/7/7 81neomycin sulfate 13
neomycin/bacitracin/polymyxin 91neomycin/polymyxin b sulfates 13
neomycin/polymyxin/bacitracin/hydrocortisone
14
neomycin/polymyxin/dexamethasone 92neomycin/polymyxin/gramicidin 91
Drug Name Page #neomycin/polymyxin/hc 93
neomycin/polymyxin/hydrocortisone 14neomycin/polymyxin/hydrocortisone 93
neo-polycin 91neo-polycin hc 14
neuac 69NEULASTA 52
NEULASTA ONPRO KIT 52NEUMEGA 52
NEUPOGEN 52NEVANAC 92
nevirapine 45nevirapine er 45NEXAVAR 37
NEXIUM 72niacin er 64
niacor 64NICOTROL NS 12
nifedical xl 60nifedipine er 60
nikki 81NILANDRON 32
nilutamide 32nimodipine 60NINLARO 35
NIPENT 33nisoldipine 60
nisoldipine er 60nitrofurantoin 14
nitrofurantoin macrocrystals 14nitrofurantoin monohydrate 14
nitrofurantoin monohydrate/macrocrystals 14nitroglycerin 64
nitroglycerin in 5% dextrose 64nitroglycerin in dextrose 5% 64
nitroglycerin lingual 64nitroglycerin transdermal 64
NITROSTAT 64nizatidine 71
nora-be 82NORDITROPIN FLEXPRO 77
NORDITROPIN NORDIFLEX PEN 77norepinephrine bitartrate 61
norethindrone 82norethindrone & ethinyl estradiol ferrous
fumarate81
norethindrone acetate 82norethindrone acetate/ethinyl estradiol 81
norethindrone acetate/ethinyl estradiol/ferrous fumarate
81

Page 114 of 121
Drug Name Page #norgestimate/ethinyl estradiol 81
NORITATE 14norlyroc 82
normosol-r in d5w 99NORTHERA 61
nortrel 0.5/35 (28) 81nortrel 1/35 81
nortrel 7/7/7 81nortriptyline hcl 27
NOVOLIN 70/30 50NOVOLIN 70/30 RELION 50
NOVOLIN N 50NOVOLIN N RELION 50
NOVOLIN R 50NOVOLIN R RELION 50
NOVOLOG 50NOVOLOG FLEXPEN 50NOVOLOG MIX 70/30 50
NOVOLOG MIX 70/30 PREFILLED FLEXPEN
50
NOVOLOG PENFILL 50NOXAFIL 29
NPLATE 52NULOJIX 86
NUPLAZID 43NUTROPIN AQ NUSPIN 10 77NUTROPIN AQ NUSPIN 20 77NUTROPIN AQ NUSPIN 5 77
NUTROPIN AQ PEN 77nyamyc 29
NYMALIZE 60nystatin 29
nystatin/triamcinolone 29nystop 30ocella 81
OCTAGAM 87octreotide acetate 84
ODEFSEY 45ODOMZO 35
OFEV 96ofloxacin 20ogestrel 81
olanzapine 42olanzapine odt 41
olanzapine/fluoxetine 26olopatadine hcl 92olopatadine hcl 94
OLYSIO 44omega-3-acid ethyl esters 64
omeprazole 72
Drug Name Page #omeprazole/sodium bicarbonate 72
ondansetron hcl 28ondansetron odt 28
ONFI 22ONGLYZA 49
ONMEL 30OPANA ER (CRUSH RESISTANT) 8
OPDIVO 38opium 10
opium tincture 10OPSUMIT 96
oralone 67ORBACTIV 14
ORENCIA 86ORENITRAM 96
ORFADIN 91ORKAMBI 95
orphenadrine citrate er 97orsythia 81
osmitrol viaflex 61OTEZLA 88
oxacillin sodium 18oxaliplatin 35
oxandrolone 78oxaprozin 7oxazepam 47
oxcarbazepine 24oxiconazole nitrate 30
oxybutynin chloride 73oxybutynin chloride er 73
oxycodone hcl 10oxycodone hcl er 8
oxycodone/acetaminophen 10oxycodone/aspirin 11
oxycodone/ibuprofen 11oxymorphone hydrochloride 11
oxymorphone hydrochloride er 8pacerone 56paclitaxel 35
paliperidone er 42pamidronate disodium 90
PANRETIN 38pantoprazole sodium 72
paricalcitol 90paroex 67
paromomycin sulfate 13paroxetine hcl 26
paroxetine hcl er 26PATADAY 92
PAZEO 92

Page 115 of 121
Drug Name Page #PEDVAX HIB 89
peg 3350/electrolytes 72peg-3350/electrolytes 72
peg-3350/nacl/na bicarbonate/kcl 72PEGASYS 44
PEGASYS PROCLICK 44PEGINTRON 44
PEG-INTRON 44PEG-INTRON REDIPEN 44
penicillin g potassium 18penicillin g potassium in iso-osmotic
dextrose 18
penicillin g sodium 18penicillin v potassium 18
pentazocine/naloxone hcl 11perindopril erbumine 55
periogard 68PERJETA 38
permethrin 38perphenazine 40
perphenazine/amitriptyline 27pfizerpen-g 18
phenadoz 28phenelzine sulfate 25
phenergan 28phenobarbital 22
phenobarbital sodium 97phenoxybenzamine hydrochloride 53
phenylephrine hcl 53phenytoin 24
phenytoin sodium 24phenytoin sodium extended 24
philith 81PICATO 69
pilocarpine hcl 68pilocarpine hcl 93
pilocarpine hydrochloride 68pimozide 40pimtrea 81pindolol 57
pioglitazone hcl 49pioglitazone hcl/metformin hcl 49
pioglitazone hcl-glimepiride 49piperacillin sodium/ tazobactam sodium 18piperacillin sodium/tazobactam sodium 18
piperacillin/tazobactam 18pirmella 1/35 81
pirmella 7/7/7 81piroxicam 7
PLEGRIDY 67
Drug Name Page #PLEGRIDY STARTER PACK 67
plenamine 99podofilox 69
polycin 91polyethylene glycol 3350 72
polymyxin b sulfate 14polymyxin b sulfate/trimethoprim sulfate 92
POMALYST 32portia-28 81
PORTRAZZA 35potassium acetate 99
potassium chloride 100potassium chloride 0.15% /nacl 0.45%
viaflex99
potassium chloride 0.15% d5w/nacl 0.33% 99potassium chloride 0.15% d5w/nacl 0.45% 99
potassium chloride 0.15%/nacl 0.9% 99potassium chloride 0.22% d5w/nacl 0.45% 99
potassium chloride 0.224%/d5w/nacl 0.45% 99potassium chloride 0.3%/ nacl 0.9% 99
potassium chloride 0.3%/d5w 99potassium chloride cr 99potassium chloride er 100potassium chloride sr 100
potassium citrate er 100POTIGA 21
PRALUENT 61pramipexole dihydrochloride 39
pramipexole dihydrochloride er 39pravastatin sodium 63
prazosin hcl 53PRED MILD 92
prednicarbate 76prednisolone 76
prednisolone acetate 92prednisolone sodium phosphate 76prednisolone sodium phosphate 92
prednisone 76prednisone intensol 76
PREMARIN 81premasol 100prevalite 64previfem 81
PREZCOBIX 46PREZISTA 46
primaquine phosphate 38primidone 22
PRIVIGEN 87PROAIR HFA 95
PROAIR RESPICLICK 95

Page 116 of 121
Drug Name Page #probenecid 30
probenecid/colchicine 30procainamide hcl 56prochlorperazine 41
prochlorperazine edisylate 40prochlorperazine maleate 40
PROCRIT 52procto-med hc 76
procto-pak 76proctosol hc 76
proctozone-hc 76PROCYSBI 92
progesterone 82PROGLYCEM 49
PROLASTIN-C 96PROLEUKIN 35PROMACTA 52
promethazine hcl 28promethazine vc plain 96
promethazine/phenylephrine 96promethegan 28
propafenone hcl 56propafenone hcl er 56
proparacaine hcl 92propranolol hcl 58
propranolol hcl er 57propranolol/hydrochlorothiazide 58
propylthiouracil 85PROQUAD 89
protriptyline hcl 27PULMOZYME 95
PURIXAN 33pyrazinamide 31
pyridostigmine bromide 31pyridostigmine bromide er 31
QUADRACEL 89quartette 81quasense 81
quetiapine fumarate 42quinapril hcl 55
quinapril/hydrochlorothiazide 55quinidine gluconate 56
quinidine gluconate cr 56quinidine gluconate er 56
quinidine sulfate 56quinine sulfate 38
QVAR 93rabeprazole sodium 72
raloxifene hydrochloride 82ramipril 55
Drug Name Page #RANEXA 61
ranitidine hcl 71RAPAFLO 73
RAPAMUNE 86RAVICTI 70
RAYOS 76REBIF 67
REBIF REBIDOSE 67REBIF REBIDOSE TITRATION PACK 67
REBIF TITRATION PACK 67reclipsen 81
RECOMBIVAX HB 89REGRANEX 69
relador pak 12relador pak plus 12
RELISTOR 71REMICADE 86
REMODULIN 96RENAGEL 74RENVELA 74repaglinide 49
repaglinide/metformin hydrochloride 49REPATHA 61
REPATHA PUSHTRONEX SYSTEM 61REPATHA SURECLICK 61
reprexain 11RESTASIS 92REVATIO 96
REVLIMID 32REXULTI 42
REYATAZ 46ribasphere 44
RIBASPHERE RIBAPAK 44ribavirin 44
RIDAURA 88rifabutin 31rifampin 31riluzole 66
rimantadine hcl 46ringers injection 100
ringers irrigation 91risedronate sodium 90
risedronate sodium dr 90RISPERDAL CONSTA 42
risperidone 42risperidone odt 42
RITUXAN 38rivastigmine tartrate 24
rivastigmine transdermal system 24rizatriptan benzoate 30

Page 117 of 121
Drug Name Page #rizatriptan benzoate odt 30
ropinirole er 39ropinirole hcl 39
rosadan 14rosadan kit 14
rosuvastatin calcium 63ROTARIX 89ROTATEQ 89
roweepra 21RUCONEST 85
SABRIL 22SAIZEN 77
SAIZEN CLICK.EASY 77SAMSCA 97
SANCUSO 28SANDOSTATIN LAR DEPOT 84
SAVELLA 67SAVELLA TITRATION PACK 67
selegiline hcl 40selenium sulfide 69
SELZENTRY 45SENSIPAR 83
SEREVENT DISKUS 95SEROSTIM 77
sertraline hcl 26setlakin 81
sharobel 82SIGNIFOR 84
SIGNIFOR LAR 84sildenafil 96
SILENOR 97silver sulfadiazine 14
SIMPONI 86SIMPONI ARIA 86
SIMULECT 88simvastatin 63
sirolimus 86SIRTURO 31
SIVEXTRO 14sodium acetate 97
sodium chloride 100sodium chloride 0.45% 100sodium chloride 0.9% 100
sodium fluoride 100sodium lactate 97
sodium phenylacetate/sodium benzoate 91sodium phenylbutyrate 70
sodium phosphate 100sodium polystyrene sulfonate 98
sodium sulfacetamide 20
Drug Name Page #SOLIRIS 91
SOMATULINE DEPOT 84SOMAVERT 84
sorine 56sotalol hcl 56
sotalol hcl (af) 56sotalol hydrochloride 56
SOVALDI 44SPIRIVA HANDIHALER 94
SPIRIVA RESPIMAT 94spironolactone 62
spironolactone/hydrochlorothiazide 62SPORANOX 30
sprintec 28 81SPRYCEL 37
sps 98sronyx 81
ssd 14stavudine 45
STELARA 69sterile water irrigation 91STIOLTO RESPIMAT 96
STIVARGA 37STRENSIQ 70
streptomycin sulfate 13STRIBILD 45
SUBSYS 11SUCRAID 70sucralfate 72
sulfacetamide sodium 20sulfacetamide sodium/prednisolone sodium
phosphate92
sulfadiazine 20sulfamethoxazole/trimethoprim 20
sulfamethoxazole/trimethoprim ds 20sulfasalazine 89
sulfatrim pediatric 20sulindac 12
sumatriptan 31sumatriptan succinate 30
sumatriptan succinate refill 30SUPRAX 16
SUPREP BOWEL PREP 72SUSTIVA 45SUTENT 37
syeda 81SYLATRON 35
SYLVANT 38SYMBICORT 94
SYMLINPEN 120 49

Page 118 of 121
Drug Name Page #SYMLINPEN 60 49
SYNAGIS 88synalar 76
SYNAREL 84SYNERCID 14SYNJARDY 49
SYNRIBO 35SYPRINE 98
TACLONEX 69tacrolimus 69tacrolimus 86
TAFINLAR 37TAGRISSO 35
TALTZ 69tamoxifen citrate 32
tamsulosin hcl 73TARCEVA 37
TARGRETIN 38tarina fe 1/20 81
TASIGNA 37tazicef 16
taztia xt 60TECENTRIQ 38TECFIDERA 67
TECFIDERA STARTER PACK 67TECHNIVIE 44
TEFLARO 17telmisartan 54
telmisartan/amlodipine 54telmisartan/hydrochlorothiazide 54
temazepam 97tencon 67
TENIVAC 89terazosin hcl 73
terbinafine hcl 30terbutaline sulfate 95
terconazole 30testosterone cypionate 78testosterone enanthate 78
TETANUS/DIPHTHERIA TOXOIDS-ADSORBED
89
tetrabenazine 67tetracycline hcl 21
THALOMID 32theophylline 95
theophylline cr 95theophylline er 95
theophylline/d5w 95THERACYS 35
thioridazine hcl 41
Drug Name Page #thiotepa 32
thiothixene 41THYMOGLOBULIN 87
tiagabine hydrochloride 22ticlopidine hcl 53
tilia fe 81timolol maleate 58timolol maleate 93
timolol maleate ophthalmic gel forming 93tinidazole 38
tis-u-sol 91TIVICAY 44
tizanidine hcl 43TOBI 95
TOBI PODHALER 95tobramycin 95
tobramycin sulfate 13tobramycin/dexamethasone 92
tolazamide 49tolbutamide 49
tolcapone 39tolmetin sodium 7
tolterodine tartrate 73tolterodine tartrate er 73
topiramate 23topiramate er 23
toposar 36topotecan hcl 36
TORISEL 86torsemide 62
TOUJEO SOLOSTAR 50TOVIAZ 73
tpn electrolytes 100tramadol hcl 11
tramadol hcl er 8tramadol hydrochloride/acetaminophen 11
trandolapril 55trandolapril/verapamil hcl 55
trandolapril/verapamil hcl er 55tranexamic acid 52
tranylcypromine sulfate 25TRAVATAN Z 91
travoprost 91trazodone hcl 25
TREANDA 32TRELSTAR 84
TRELSTAR MIXJECT 84tretinoin 38tretinoin 69
tretinoin microsphere 69

Page 119 of 121
Drug Name Page #tretinoin microsphere pump 69
triamcinolone acetonide 68triamcinolone acetonide 76triamcinolone acetonide 94
triamcinolone in orabase 68triamterene/hydrochlorothiazide 62
triderm 77tri-estarylla 81
trifluoperazine hcl 41trifluridine 46
trihexyphenidyl hcl 38tri-legest fe 81
tri-linyah 81tri-lo-estarylla 81
tri-lo-marzia 81tri-lo-sprintec 81
trilyte 72trimethobenzamide hcl 28
trimethoprim 14trimipramine maleate 27
trinessa 82trinessa lo 82
tri-previfem 81tri-sprintec 81TRIUMEQ 45trivora-28 82TRIZIVIR 45
trospium chloride 73trospium chloride er 73
TRULICITY 49TRUMENBA 89
TRUVADA 45TWINRIX 89TYBOST 45
TYGACIL 14TYKERB 37
TYPHIM VI 89TYSABRI 67TYVASO 96
TYVASO REFILL 96TYVASO STARTER 96
TYZEKA 43UCERIS 77ULORIC 30unithroid 83
UNITUXIN 38UPTRAVI 96
ursodiol 71valacyclovir hcl 46
VALCHLOR 32
Drug Name Page #VALCYTE 43
valganciclovir 43valproate sodium 22
valproic acid 22valsartan 54
valsartan/hydrochlorothiazide 54VALSTAR 35
vanatol lq 67vancomycin hcl 14
vancomycin hcl in dextrose 14vandazole 15
VAQTA 89VARIVAX 89VARIZIG 89
VECTIBIX 38VELCADE 35VELETRI 96
velivet 82VELPHORO 74
VENCLEXTA 35VENCLEXTA STARTING PACK 35
venlafaxine hcl 26venlafaxine hcl er 26
VENTAVIS 96verapamil hcl 60
verapamil hcl er 60verapamil hcl sr 60
VEREGEN 69VERSACLOZ 43
VESICARE 73vestura 82
VEXOL 92V-GO 20 91V-GO 30 91V-GO 40 91
vicodin 11vicodin es 11vicodin hp 11VICTOZA 49
VIEKIRA PAK 44VIEKIRA XR 44
vienva 82VIGAMOX 20
VIMIZIM 70vinblastine sulfate 35
vincasar pfs 35vincristine sulfate 35
vinorelbine tartrate 35viorele 82
VIRACEPT 46

Page 120 of 121
Drug Name Page #VIRAZOLE 96
VIREAD 45VITEKTA 44
VIVITROL 12voriconazole 30VOTRIENT 37
VPRIV 70VRAYLAR 42
vyfemla 82warfarin sodium 51
WELCHOL 64wera 82
wymzya fe 82XALKORI 37XARELTO 51
XARELTO STARTER PACK 51XELJANZ 88
XELJANZ XR 88XENAZINE 67
XGEVA 90XIAFLEX 70XIFAXAN 15
XOLAIR 96XTANDI 32
xulane 82xylocaine dental 12
xylon 11XYREM 97
YERVOY 38YF-VAX 89
YONDELIS 32zafirlukast 94
zaleplon 97ZALTRAP 35ZANOSAR 32
zarah 82ZARXIO 52
ZAVESCA 70zazole 30
zebutal 67ZELAPAR 40
ZELBORAF 37ZEMAIRA 96
zenatane 69zenchent 82
zenchent fe 82ZENPEP 70
ZEPATIER 44ZETIA 64
ZEVALIN Y-90 38
Drug Name Page #zidovudine 45
zinacef 17ZINBRYTA 67
ziprasidone hcl 42zoledronic acid 90
ZOLINZA 35zolmitriptan 31
zolmitriptan odt 31zolpidem tartrate 97
zolpidem tartrate er 97zonisamide 22
ZORBTIVE 78ZORTRESS 86
ZOSTAVAX 89zovia 1/35e 82zovia 1/50e 82ZYCLARA 69
ZYCLARA PUMP 69ZYDELIG 36
ZYFLO 94ZYFLO CR 94ZYKADIA 35
ZYPREXA RELPREVV 42ZYTIGA 32ZYVOX 15

Page 121 of 121
This abridged formulary was updated on January 1, 2017 and is not a complete list of drugs covered by our plan. For a complete listing or other questions, please contact: OptumRx Member Services Phone: 1-866-443-1095 TTY users call: 711 Hour of operation: 24 hours a day, 7 days a week Website: optumrx.com

Carrier Id Changes PA PA, QL QL ST ST, QL
PCN 2017 Changes 28 0 0 0 0 0 28
Notes
Report does not account for termed members
Members who have changed groups/accounts are counted twice
Drug Summaries count distinct users of each drug
Separate letters are being sent for formulary and each UM
Pharmaceutical Care Network - Multiple Clients
Claims Filled 05/01/2016 - 08/31/2016
UM Member DisruptionFormulary
Member
Disruption
Total
Member
Disruption

Carrier Id Disease State Drug Name Formulary
PCN Misc Skin Condition FINACEA Select
PCN Erectile Dysfunction STENDRA Select
PCN Oncology TASIGNA Select
PCN Migraine/Pain Relief ZOMIG NASAL SPRAY Select
PCN Diabetes KOMBIGLYZE Select
PCN Diabetes ONGLYZA Select
PCN Ulcer/Acid Reflux/Gerd CARAFATE Select
PCN Seizure Disorders OXTELLAR XR Select
PCN Hepatitis DAKLINZA Select
PCN Asthma / COPD TUDORZA Select
Pharmaceutical Care Network - Multiple Clients
Claims Filled 05/01/2016 - 08/31/2016

Tier Change
Nbr Form
Utilizers
Nbr Form
Rxs
Tier 3 8 11
Tier 3 5 11
Tier 3 3 8
Tier 3 3 3
Tier 3 3 8
Tier 3 2 7
Tier 3 1 1
Tier 3 1 3
Tier 3 1 2
Tier 3 1 4
Pharmaceutical Care Network - Multiple Clients
Claims Filled 05/01/2016 - 08/31/2016

Members were selected to receive this communication based on pharmacy claims data. Information in this letter is confidential and not shared with any non-medical personnel or personnel not directly managing pharmacy claims. Medications listed in this letter are subject to change. Please visit www.optumrx.com for the most current formulary information.
This document and others if attached contain information from OptumRx that is proprietary, confidential and/or may contain protected health information (PHI). We are required to safeguard PHI by applicable law. The information in this document is for the sole use of the person(s) or company named above. Proper consent to disclose PHI between these parties has been obtained. If you received this document by mistake, please know that sharing, copying, distributing or using information in this document is against the law. If you are not the intended recipient, please notify the sender immediately and return the document(s) by mail to OptumRx Privacy Office, 17900 Von Karman, M/S CA016-0203, Irvine, CA 92614.
All Optum® trademarks and logos are owned by Optum, Inc. All other brand or product names are trademarks or registered marks of their
respective owners.
ORX5621_170901 • page 1 of 1
2300 Main Street
Irvine, CA 92614
<Member URL>
Important pharmacy benefit information
<Member Name> <Member Address> <Member Address 2> <City>, <ST> <Zip>
Month DD, YYYY
Dear <Member Name>,
OptumRx® manages your pharmacy benefits for your plan sponsor.
Beginning January 1, 2017, <Label Name> will be moved to Tier 3 on your prescription drug list. This
will increase the amount you pay for this drug. To help you manage your prescription costs, there
may be lower-cost alternatives available.
Alternatives
<ALTERNATIVES>
You are not required to change from <Label Name> to an alternative medication. However, if you
continue using <Label Name>, you will pay more. If you wish to consider using an alternative
medication, call your doctor or bring this letter to your next doctor visit to discuss other medication
options that may be right for you.
If you have any questions about this letter or your pharmacy benefit plan, we encourage you to call
OptumRx Customer Service at the toll-free member phone number on the back of your ID card. You
may also visit <member URL> for more information about your pharmacy benefits.
Sincerely,
OptumRx

OPTUMRx''
1
2
6
8 2
1
12 1 6
4
4
6
8 3
2 1
54
12 3
145

1 4 1 6 5
148 2 2 2 7 3
21 1 1 4 1 5 1 1 1
15 5
45 2
11 2 1 1 3
43 6 1 3 9
10 8
47 1 3 1 4
so

44 17
1 7
54 11
626
Total Impact: PA w/QL, and QL Traditional Comprehensive Drug List= 771
Population Live Count: 9332/771-0.08%. 0.1% impacted.

OPTUMRx''
Some medications must be authorized for coverage because they're only approved or effective in treating specific illnesses, they cost more or they may be prescribed for conditions for which safety and effectiveness have not been well-established.
Reviewing Medications
Our review committee of independent doctors and pharmacists meets regularly to review medications and consider how they should be covered by pharmacy benefit plans. They also recommend prior authorization guidelines.
Safe and Effective
When making recommendations, the review committee focuses on proven medication safety, effectiveness and cost. The committee considers:
• U.S. Food and Drug Administration (FDA) approved indications
• Manufacturer's package labeling instructions
• Well-accepted and/or published clinical recommendations
Getting a Short-Term Supply
If you must start taking a medication that requires prior authorization right away, two options may be available to you. First, ask your doctor if a sample is available. If not, check with your pharmacy to request a short-term supply of five days or less- keep in mind you will be responsible for the full cost at that time. If the prior authorization request is approved, then your pharmacist can dispense the rest of your prescription.
Requesting a Prior Authorization
You, your pharmacist or your doctor can start the prior authorization review process by contacting our prior authorization department. A pharmacy technician then works with your doctor to get the information needed for the review. Once we receive a completed prior authorization form from your doctor, we conduct a clinical review within two business days. We then send you and your doctor a letter regarding the prior authorization decision.

Select Prior Authorization
Select Non-Specialty Prior Authorization List
Products on these pages may require prior authorization as determined by your specific benefit plan design. For more information, contact customer service at the number on the back of your benefit plan ID card.
Anti-infectives
Antibiotics
Antifungals
Antimalarial
Antiprotozoal
Cardiology
Antilipemic
Heart Failure
Central Nervous System
ADHD Agents (PA age 19+ only)
OplumRx 1 optumrx.com
XIFAXAN (rifaximan)
CICLODAN KIT (ciclopirox)
CICLOPIROX KIT (ciclopirox)
CNL8 NAIL KIT (ciclopirox)
JUBLIA (efinaconazo.ccle:.c) ___________ ·-··--KERYDIN (tavaborole)
ON MEL (itraconazole)
PEDIPIROX-4 NAIL KIT (ciclopirox)
SPORANOX (itraconazole) Soln
SPORANOX (itraconazole)
QUALAQUIN (quinine)
DARAPRIM (pyrimethamine)
VYTORIN 10-80 MG (simvastatin/ezetimibe)
ZOCOR 80 mg (simvastatin)
CORLANOR (ivabradine)
ENTRESTO (sacubitril/valsartan)
ADDERALL (amphetamine/dextroamphetamine)
ADDERALL XR (amphetamine/dextroamphetamine mixed salts)
APTENSIO XR (methylphenidate)
CONCERTA (methylphenidate)
DAYTRANA (methylphenidate transdermal)
DESOXYN (methamphetamine)
DEXEDRINE (dextroamphetamine)
DYANA VEL XR (amphetamine)
EVEKEO (amphetamine)
FOCALIN (dexmethylphenidate)
FOCALIN XR (dexmethylphenidate)
METADATE CD (methylphenidate)

METADATE ER (methylphenidate) 20 mg
METHYLIN (methylphenidate)
METHYLIN CHEW TAB (methylphenidate)
METHYLIN ER (methylphenidate) 20 mg
METHYLPHENIDATE ER (methylphenidate)
PROCENTRA (dextroamphetamine) Sol
QUILLICHEW ER (methylphenidate)
QUILLIVANT XR (methylphenidate)
RITALIN (methylphenidate)
RITALIN LA (methylphenidate)
RITALIN SR (methylphenidate)
VYVANSE (lisdexamfetamine)
ZENZEDI (dextroamphetamine)
Analgesics (non-opioid) PENNSAID (diclofenac)
QUTENZA (capsaicin)
VIMOVO (naproxen/esomeprazole)
Analgesics (opioid) ABSTRAL (fentanyl citrate)
ACTIQ (fentanyl citrate)
BELBUCA (buprenorphine) film
BUNAVAIL (buprenorphrine/naloxone)
BUTRANS (buprenorphine)
CONZIP (tramadol SR)
FENTORA (fentanyl citrate)
LAZANDA (fentanyl citrate)
ONSOLIS (fentanyl citrate)
SUBOXONE (buprenorphrine/naloxone)
SUBSYS (fentanyl)
SUBUTEX (buprenorphrine)
ZUBSOLV (buprenorphine/naloxone)
Anticonvulsants HORIZANT (gabapentin enacarbil)
Antipsychotics ADASUVE (loxapine)
Benzodiazepines FLURAZEPAM (flurazepam)
ONFI (clobazam)
Hypoactive Sexual Desire Disorder ADDYI (flibanserin)
Miscellaneous RILUTEK (riluzole)
Parkinson's DUOPA (carbidopa-levodopa) Susp
Stimulants NUVIGIL (armodafinil)
_____ ------· PROVIGIL (modafinil)
3

Select Prior Authorization
Weight Loss
Dermatology
Acne
Acne (PA age >25 only)
Miscellaneous
Miscellaneous ( PA age >25 only)
Endocrinology & Metabolism
Androgens, Anabolic Steroids
Androgens, Testosterone
OptumRx [ optumrx.com
ADIPEX-P (phentermine)
BELVIQ (lorcaserin)
BONTRIL (phendimetrazine)
CONTRAVE (naltrexone-bupropion)
DID REX (benzphetamine)
QSYMIA (phentermine/topiramate)
SAXENDA (liraglutide)
SUPRENZA (phentermine)
TENUATE (diethylpropion)
XENICAL (orlistat)
ABSORICA (isotretinoin)
AMNESTEEM (isotretinoin)
CLAVARIS (isotretinoin)
MIRVASO (brimonidine tartrate) Gel
MYORISAN (isotretinoin)
ZENATANE (isotretinoin)
ATRALIN (tretinoin)
A VITA (tretinoin)
DIFFERIN (adapalene)
EPIDUO (adapalene/benzoyl peroxide)
EPIDUO FORTE (adapalene/benzoyl peroxide)
RETIN-A (tretinoin)
RETIN-A MICRO (tretinoin)
TRETIN-X (tretinoin)
VELTIN (clindamycin/tretinoin)
ZIANA (clindamycin/tretinoin)
ENSTILAR (calcipotriene-betamethasone dipropionate)
TAZORAC (tazarotene)
FABIOR (tazarotene)
ANADROL-50 (oxymetholone)
OXANDRIN (oxandrolone)
ANDRODERM (testosterone)
AND ROGEL (testosterone)
ANDROID (methyltestoster?_fl~) __________________ _
ANDROXY (fluoxymesterone)
AVE ED (testosterone undecanoate)

Antidiabetic Agents
Antidiabetic Agents (PA age > 65 only)
Gastroenterology
Antiemetics
Irritable Bowel Syndrome
Opioid-induced Constipation
Miscellaneous
Calcium Modifier
Methotrexate Auto-Injectors
Wound Care
Oncology
Miscellaneous
Ophthalmology
Miscellaneous
Respiratory
AXIRON (testosterone)
DELATESTRYL (testosterone enanthate)
DEPO-TESTOSTERONE (testosterone cypionate)
FORTESTA (testosterone)
METHITEST (methyltestosterone)
NATESTO (testosterone nasal)
STRIANT (testosterone)
TESTIM (testosterone)
TESTOPEL (testosterone pellet)
TESTRED (methyltestosterone)
VOGELXO (testosterone)
AFREZZA (insulin regular)
GLUMETZA (metformin)
SYMLIN (pramlintide)
CHLORPROPAMIDE (chlorpropamide)
CESAMET (nabilone)
DICLEGIS (doxylamine-pyridoxine)
MARINOL (dronabinol)
LOTRONEX (alosetron)
VIBERZI (eluxadoline)
RELISTOR (methylnaltrexone)
SENSIPAR (cinacalcet)
OTREXUP (methotrexate)
RASUVO (methotrexate)
REG RAN EX (becaplermin)
PROVENGE (sipuleucei-T)
RESTASIS (cyclosporine)
Asthma/COPD DALIRESP (roflumilast) ---------------------'----'----------------"-
PLEASE NOTE: This drug list is subject to periodic updates and may not be all inclusive. Drugs affected include both brand and generic where applicable and includes all dosage formulations unless otherwise specifically notated. If a new drug is approved and falls into one of the targeted PA categories, the new drug may automatically be added to this list.
5

Select Prior Authorization
Select Specialty Prior Authorization List
Products on these pages may require prior authorization as determined by your specific benefit plan design. For more information, contact customer service at the number on the back of your benefit plan ID card.
Anti-infectives
Antiretrovirals
Cardiology
Antilipemic
Pulmonary Arterial Hypertension
Vasopressors
Central Nervous System
Anticonvulsants
Depressant
Neurotoxins
OptumRx I optumrx.com
SELZENTRY (maraviroc)
JUXTAPID (lomitapide)
KYNAMRO (mipomersen)
PRALUENT (alirocumab)
REPATHA (evolocumab)
ADCIRCA (tadalafil)
ADEM PAS (riociguat)
FLOLAN (epoprostenol)
LETAIRIS (ambrisentan)
OPSUMIT (macitentan)
ORENITRAM (treprostinil diolamine)
REMODULIN (treprostinil)
REVATIO (sildenafil)
TRACLEER (bosentan)
TYVASO (treprostinil)
UPTRAVI (selexipag)
VELETRI (epoprostenol)
VENTAVIS (iloprost)
NORTH ERA (droxidopa)
SABRIL (vigabatrin)
XYREM (sodium oxybate)
BOTOX (onabotulinumtoxinA)
DYSPORT (abobotulinumtoxinA)
MYOBLOC (rimabotulinumtoxinB)
XEOMIN (incobotulinumtoxinA)

Opiate Antagonist
Parkinson's
Sleep Disorder
Dermatology
Alkylating Agents
Electrolyte & Renal Agents
Diuretics
Endocrinology & Metabolism
Gonadotropins
Growth Hormones and Related Therapy
VIVITROL (naltrexone)
APOKYN (apomorphine)
HETLIOZ (tasimelteon)
VALCHLOR (mechlorethamine) Gel
KEVEYIS (dichlorphenamide)
ELIGARD (leuprolide)
FIRMAGON (degarelix)
LUPANETA PACK (leuprolide)
LUPRON (leuprolide)
LUPRON DEPOT (leuprolide)
LUPRON DEPOT-PED (leuprolide)
SUPPRELIN LA (histrelin acetate)
TRELSTAR (triptorelin)
TRELSTAR DEPOT (triptorelin)
TRELSTAR LA (triptorelin)
VANTAS (histrelin)
EGRIFTA (tesamorelin)
GENOTROPIN (somatropin)
HUMATROPE (somatropin)
INCRELEX (mecasermin)
NORDITROPIN (somatropin)
NUTROPIN (somatropin)
NUTROPIN AQ (somatropin)
OMNITROPE (somatropin)
SAIZEN (somatropin)
SEROSTIM (somatropin)
SOMA VERT (pegvisomant)
TEV-TROPIN (somatropin)
ZOMACTON (somatropin)
ZORBTIVE (somatropin)
7

Select Prior Authorization
Hormone Modifiers MYALEPT (metreleptin)
NATPARA (parathyroid hormone)
Miscellaneous H.P. ACTHAR (corticotropin) ·~--------------------
KORLYM (mifepristone)
Osteoporosis FORTEO (teriparatide)
PROLIA (denosumab)
Somatostatins SANDOSTATIN (octreotide)
SANDOSTATIN LAR (octreotide)
SIGNIFOR (pasireotide)
SIGNIFOR LAR (pasireotide)
SOMATULINE DEPOT (lanreotide)
Enzyme-Related
Alpha-1 proteinase inhibitor ARALAST (alpha-1 proteinase inhibitor)
GLASSIA (alpha-1 proteinase inhibitor)
PROLASTIN (alpha-1 proteinase inhibitor)
ZEMAIRA (alpha-1 proteinase inhibitor)
Cystine-depleting Agents CYSTARAN (cysteamine)
PROCYSBI (cysteamine bitartrate)
Enzyme Replacement ALDURAZYME (laronidase)
CERDELGA (eliglustat)
CEREZYME (imiglucerase)
ELAPRASE (idursulfase)
ELELYSO (taliglucerase)
FABRAZYME (agalsidase beta)
KANUMA (sebelipase alfa)
LUMIZYME (alglucosidase alfa)
MYOZYME (a I glucosidase alfa)
NAGLAZYME (galsulfase)
RAVICTI (glycerol phenylbutyrate)
STRENSIQ (asfotase alfa)
VIMIZIM (elosulfase)
OptumRx 1 optumrx.com

Enzyme, Gout
Phenylketonuria Treatment Agents
Gastroenterology
Bile Acid Agents
Short Bowel Syndrome
Immunology
Allergen Extracts
Hematopoietic Agents
Hemostatic Agent
VPRIV (velaglucerase)
XURIDEN (uri dine triacetate)
ZAVESCA (miglustat)
KRYSTEXXA (pegloticase)
KUVAN (sapropterin)
CHOLBAM (cholic acid)
GATIEX (teduglutide)
GRASTEK (timothy grass pollen)
ORALAIR (mixed grass pollens allergen)
RAG WITEK (short ragweed pollen allergen)
ARANESP (darbepoetin alfa)
EPOGEN (epoetin alfa)
GRANIX (tbo-filgrastim)
LEUKINE (sargramostim)
MIRCERA (methoxy polyethylene glycol-epoetin)
MOZOBIL (plerixafor)
NEULASTA (pegfilgrastim)
NEUMEGA (oprelvekin)
NEUPOGEN (filgrastim)
NPLATE (romiplostim)
PROCRIT (epoetin alfa) __ ___:__:_____:___:___ _______________ _ PROMACTA (eltrombopag)
SOURIS (eculizumab)
ZARXIO (filgrastim)
BERINERT (c1 esterase)
CINRYZE (c1 esterase) --------------- ---------FIRAZYR (icatibant)
KALBITOR (ecallantide)
RUCONEST (c1 esterase)
9

Select Prior Authorization
Hepatitis C Agents
Immune Globulins
lmmunomodulators
OptumRx I optumrx.com
DAKLINZA (daclatasvir dihydrochloride)
HARVONI (ledipasvir-sofosbuvir)
OLYSIO (simeprevir)
PEGASYS (peginterferon alfa-2a)
PEG-INTRON (peginterferon alfa-2b)
SOVALDI (sofosbuvir)
TECHNIVIE (ombitasvir-paritaprevir-ritonavir)
VIEKIRA (simeprevir)
ZEPATIER (elbasvir-grazoprevir)
BIVIGAM (immune globulin)
CARIMUNE (immune globulin)
CYTOGAM (cytomegalovirus immune globulin)
FLEBOGAMMA (immune globulin)
FLEBOGAMMA DIF (immune globulin)
GAMASTAN (immune globulin)
GAMMAGARD (immune globulin)
GAMMAKED (immune globulin)
GAMMAPLEX (immune globulin)
GAMUNEX (immune globulin)
GAMUNEX-C (immune globulin)
HIZENTRA (immune globulin)
HYQVIA (hyaluron immune globulin)
OCTAGAM (immune globulin)
PRIVIGEN (immune globulin)
VARIZIG (varicella-zoster immune globulin)
ACTEMRA (tocilizumab)
CIMZIA (certolizumab)
COSENTYX (secukinumab)
ENBREL (etanercept)
ENTYVIO (vedolizumab)
HUMIRA (adalimumab)
KINERET (anakinra)

lnterleukins
Miscellaneous
Multiple Sclerosis
Transplant
Miscellaneous
Collagenase
Diagnostic
Movement Disorder Agents
Toxicology
ORENCIA (abatacept)
OTEZLA (apremilast)
REMICADE (infliximab)
SIMPONI (golimumab)
SIMPONI ARIA (golimumab)
STELARA (ustekinumab)
XEUANZ (tofacitinib)
XEUANZ XR (tofacitinib)
ARCALYST (rilonacept)
ILARIS (canakinumab)
BENLYSTA (belimumab)
AMPYRA (dalfampridine)
AUBAGIO (teriflunomide)
AVON EX (interferon beta-1 a)
BETASERON (interferon beta-1 b)
COPAXONE (glatiramer)
EXT A VIA (interferon beta-1 b)
GILENYA (fingolimod)
GLATOPA (glatiramer) 20 mg/ml
LEMTRADA (alemtuzumab)
NOVANTRONE (mitoxantrone)
PLEGRIDY (peg interferon beta)
REBIF (interferon beta-1 a)
TECFIDERA (dimethyl fumarate)
TYSABRI (natalizumab)
NULOJIX (belatacept)
ZORTRESS (everolimus)
XIAFLEX (collagenase clostridium histolyticum)
THYROGEN (thyrotropin alia)
XENAZINE (tetrabenazine)
CUPRIMINE (penicillamine)
11

Select Prior Authorization
Viscosupplements
Obstetrics & Gynecology
Fertility Agents
Hormone Replacement
Oncology
Alkylating Agents
Antiandrogen
Antifolate
Antimicrotubular
OptumRx I optumrx.com
EXJADE (deferasirox)
FERRIPROX (deferiprone)
JADENU (deferasirox)
SYPRINE (trientine)
EUFLEXXA (sodium hyaluronate)
GEL-ONE (sodium hyaluronate)
HYALGAN (sodium hyaluronate)
MONOVISC (hyaluronan)
ORTHOVISC (sodium hyaluronate)
SUPARTZ (sodium hyaluronate)
SYNVISC (sodium hyaluronate)
SYNVISC-ONE (sodium hyaluronate)
BRAVELLE (urofollitropin)
CETROTIDE (cetrorelix)
Chorionic gonadotropin (chorionic gonadotropin)
FOLLISTIM AQ (follitropin beta)
Ganirelix acetate (ganirelix)
GONAL-F (follitropin alta)
GONAL-F RFF (follitropin alfa)
GONAL-F RFF REDIINJECT (follitropin alta)
MENOPUR (menotropins)
NOVAREL (chorionic gonadotropin)
PREGNYL (chorionic gonadotropin)
REPRONEX (menotropins)
MAKENA (hydroxyprogesterone caproate)
TEMODAR (temozolomide)
XTANDI (enzalutamide )
ZYTIGA (abiraterone)
FOLOTYN (pralatrexate)
HALAVEN (eribulin)

JEVTANA (cabazitaxel)
Interferons INTRON A (interferon alfa-Zb)
SYLATRON (peginterferon alfa-Zb)
Kinase and Molecular Target Inhibitors AFINITOR (everolimus)
AFINITOR DISPERZ (everolimus)
ALECENSA (alectinib)
BOSULIF (bosutinib)
CAPRELSA (vandetanib)
COMETRIQ (carbozantinib)
COTELLIC (cobimetnib)
ERIVEDGE (vismodegib)
FARYDAK (panobinostat)
GILOTRIF (afatinib)
GLEEVEC (imatinib)
IBRANCE (palbociclib)
ICLUSIG (ponatinib)
IMBRUVICA (ibrutinib)
INLYTA (axitinib)
IRESSA (gefitinib)
JAKAFI (ruxolitinib)
KYPROLIS (carfilzomib)
LENVIMA (lenvatinib)
LYNPARZA (olaparib)
MEKINIST (trametinib)
NEXAVAR (sorafenib)
NINLARO (ixazomib)
ODOMZO (sonidegib)
PORTRAZZA (necitumumab) -------------------
SPRYCEL (dasatinib)
STIVARGA (regorafenib)
SUTENT (sunitinib)
13

Select Prior Authorization
Miscellaneous
Monoclonal Antibody
OptumRx I optumrx.com
TAFINLAR (dabrafenib)
TAG RISSO (osimertinib)
TARCEVA (erlotinib)
TASIGNA (nilotinib)
TYKERB (lapatinib)
VELCADE (bortezomib)
VOTRIENT (pazopanib)
XALKORI (crizotinib)
ZALTRAP (ziv-aflibercept)
ZELBORAF (vemurafenib)
ZYDELIG (idelalisib)
ZYKADIA (ceritinib)
BELEODAQ (belinostat)
DACOGEN (decitabine)
ISTODAX (romidepsin)
LONSURF (trifluridine-tipiracil)
SYNRIBO (omacetaxine)
TARGRETIN (bexarotene) caps
TARGRETIN (bexarotene) Gel
XELODA (capecitabine)
ZOLINZA (vorinostat)
ADCETRIS (brentuximab)
ARZERRA (ofatumumab)
BLINCYTO (blinatumomab)
CYRAMZA (ramucirumab)
DARZALEX (daratumumab)
EMPLICITI (elotuzumab)
ERBITUX (cetuximab)
GAZYVA (obinutuzumab)
HERCEPTIN (trastuzumab)
KADCYLA (ado-trastuzumab emtansine)
KEYTRUDA (pembrolizumab)

Thalidomide-related Agents
Respiratory
Asthma/COPD
Cystic Fibrosis
Pulmonary Fibrosis
Respiratory Syncytial Virus Agents
OPDIVO (nivolumab)
PERJETA (pertuzumab)
RITUXAN (rituximab)
SYLVANT (siltuximab)
XGEVA (denosumab)
YERVOY (ipilimumab)
POMALYST (pomalidomide)
REVLIMID (lenalidomide)
THALOMID (thalidomide)
NUCALA (mepolizumab)
XOLAIR (omalizumab)
CAYSTON (aztreonam)
KALYDECO (ivacaftor)
ORKAMBI (lumacaftor-ivacaftor)
PULMOZYME (dornase alfa)
ESBRIET (pirfenidone)
OFEV (nintedanib)
SYNAGIS (palivizumab) ·-------~-~---~------
PLEASE NOTE: This drug list is subject to periodic updates and may not be all inclusive. Drugs affected include both brand and generic where applicable and includes all dosage formulations unless otherwise specifically notated. If a new drug is approved and falls into one of the targeted PA categories, the new drug may automatically be added to this list.
15

OPTUM" optumrx.com
OptumRx specializes in the delivery, clinical management and affordability of prescription medications and consumer health products. We are an Optum® company- a leading provider of integrated health services. learn more at optum.com.
All Optum5 trademarks and logos are owned by Optum, Inc. All other brand or product names are trademarks or registered marks of their respective owners.
©20 16 OptumRx, Inc. ORX0800A_160418 55528-042016

OPTUMRx'
Your pharmacy benefit plan's quantity limits program protects you and can help you get the best results from your medication therilpy. !\long with supportinq safe and appropriate dosin(], quantity limits ccm also keep prescription clrwJ costs lower for you and your benefit plan sponsor.
Determining Quantity Limits
Quantity limits are meant to minimize the risk of over-dosing and unwanted drug interactions. Quantity limit rules are based on:
• Food and Drug Administration (FDA) approved indications
• Manufacturer's package labeling instructions
• Well-accepted or published clinical recommendations
Establishing Guidelines for Use
Our review committee of independent doctors and pharmacists meets regularly to review medications and consider how they should be covered by pharmacy benefit plans. They also recommend quantity limit guidelines.

Select Quantity limits on Medications
Select Non-Specialty Quantity Limit
Antibiotics SIVEXTRO (tedizolid) Solr 6 vials/30 days SIVEXTRO (tedizolid) Tabs 6 tabs/30 days ZYVOX (linezolid) 28 tabs/30 days ZYVOX (linezolid) Suspension 6 bottles (900 mL)/28 days
_:_Ac:.n:::ti"'fu::cn~gc::a Ices _____ _::L::_Ac..:M_:.:_IS=-:1=-L (,terbi nafi n e) 2 50 mg 84 days supply/180 days_ _ ___ __ Antivirals, Herpetic SITAVIG (acyclovir) 50 mg
VALTREX (valacyclovir) 2 tabs/30 days 4 tabs/day
Antivirals, Influenza
Cardiology
Anticoagulants
Heart Failure
Central Nervous System
ADHD Agents
2 OptumRx I optumrx.com
RELENZA (zanamivir) 40 inh/365 days.
TAMIFLU (oseltamivir) 30 mg 40 caps/365 days TAM I FLU (oseltamivir) 45 mg, 75 mg 20 caps/65 days TAMIFLU (oseltamivir) Suspension 360 mU365 days
ELIQUIS (apixiban) 2 tabs/day ELIQUIS (apixiban) 5 mg 3 tabs/day -=:-==c=->::Jc::c:_:=-=-:c2-____ __:::_:=:=.:L__- --- -------------
PRADAXA (dabigatran) 2 caps/day SAVAYSA (edoxaban) 1 tab/day XARELTO (rivaroxaban) 1 tab/day
XARELTO (rivaroxaban) 15 mg 2 tabs/day XARELTO (rivaroxaban) Starter Pack 1 pack/30 days CORLANOR (ivabradine) 2 tabs/day ENTRESTO (sacubitril/valsartan) 2 tabs/day
ADDERALL (amphetamine/ dextroamphetamine) ADDERALL XR (amphetamine/ dextroamphetamine mixed salts) APTENSIO XR (methylphenidate) CONCERT A (methylphenidate) 36 mg CONCERTA (methylphenidate) DAYTRANA (methylphenidate
3 tabs/day
1 cap/day
1 cap/day 2 tabs/day
_ 1 tab/day 1 patch/day
transdermal) -=-=~::c::cc_:_::."-------------------------------
DESOXYN (methamphetamine) 5 tabs/day DEXEDRINE (dextroamphetamine) 5 mg 3 caps/day DEXEDRINE (dextroamphetamine) 15 mg 4 caps/day DEXEDRINE (dextroamphetamine) 10 mg 6 caps/day DYANA VEL XR (amphetamine) 24 mUday

ADHD Agents (cont.) EVEKEO (amphetamine) 6 tabs/day FOCALIN (dexmethylphenidate) 2 tabs/day FOCALIN XR (dexmethylphenidate) 20 mg 2 caps/day FOCALIN XR (dexmethylphenidate) 1 cap/day METADATE CD (methylphenidate) 1 cap/day METADATE ER (methylphenidate) 20 mg 3 tabs/day METHYLIN (methylphenidate) 3 tabs/day METHYLIN CHEW TAB (methylphenidate) 3 tabs/day METHYLIN CHEW TAB 6 tabs/day (methylphenidate) 10 mg METHYLIN ER (methylphenidate) 20 mg 3 tabs/day METHYLPHENIDATE ER 2 tabs/day (methylphenidate) 10 mg PROCENTRA (dextroamphetamine) Sol 60 mUday QUILLICHEW ER (methylphenidate) 2 tabs/day 30 mg QUILLICHEW ER (methylphenidate) 1 tab/day
---··"-·-~··"-·-
QUILLIVANT XR (methylphenidate) 12 mUday
RITALIN (methylphenidate) 3 tabs/day RITALIN LA (methylphenidate) 1 cap/day RITALIN SR (methylphenidate) 20 mg __ 3 tabs/day STRATIERA (atomoxetine) 1 cap/day STRATIERA (atomoxetine) 10 mg, 40 mg 2 caps/day VYVANSE (lisdexamfetamine) 1 cap/day ZENZEDI (dextroamphetamine) 10 mg 6 tabs/day ZENZEDI (dextroamphetamine) 3 tabs/day ZENZEDI (dextroamphetamine) 30 mg 2 tabs/day
Alzheimers Agents NAMENDA XR (memantine hcl) caps 1 cap/day NAMENDA XR TITRATION PACK 1 cap/day (memantine hcl) caps NAMZARIC (memantine hcl) caps 1 cap/ day
Analgesics (non-opioid) CELEBREX (celecoxib) 2 caps/day DUEXIS (naproxen/esomeprazole) 3 tabs/day FLECTOR (diclofenac epolamine) 2 patches/day up to 1 5 days Ketorolac (ketorolac) 20 tabs or 5 days supply/
30 days QUTENZA (capsaicin) 4 patches/3 months
3

Analgesics (non-opioid) SPRIX (ketorolac) 5 bottles or 5 days supply I (cont.) 30 days
VIMOVO (naproxen/esomeprazol~) 2 tabs/day VOLTAREN (diclofenac) Gel 10 tubes/month
Analgesics (opioid) ABSTRAL (fentanyl citrate) 4 tabs/day ACTIO (fentanyl citrate) 4 lozenges/day AVINZA (morphine ext-release) 1 cap/day AVINZA (morphine ext-release) 120 mg 2 caps/day BELBUCA (buprenorphine) film 2 films/day BUNAVAIL (buprenorphrine/naloxone) 6 films/day 2.1-0.3 mg BUNAVAIL (buprenorphrine/naloxone) 2 films/day 6.3-1 mg
BUNAVAIL (buprenorphrine/naloxone) 3 films/day 4.2-0.7 mg BUTRANS (buprenorphine) 4 patches/28 days CONZIP (tramadol SR) 1 cap/day DURAGESIC (fentanyl transdermal) 15 patches/30 days DURAGESIC (fentanyl transdermal) 30 patches/30 days 75 mcg/hr, 100 mcglhr EMBEDA (morphine/naltrexone) 2 caps/day EXALGO (hydromorphone) 2 tabs/day FENTORA (fentanyl citrate) 4 tabs/day HYSINGLA ER (hydrocodone bitartrate) 1 tab/day KADIAN (morphine ext-release) 2 caps/day LAZANDA (fentanyl citrate) 1 bottle/day
MS CONTIN (morphine ext-release) 3 tabs/day NUCYNTA ER (tapentadol) 2 tabs/day ONSOLIS (fentanyl citrate) 4 films/day
-·-···•'""'''""-"''''·"-·
OPANA ER (oxymorphone ext-release) 4 tabs/day OXYCONTIN (oxycodone ext-release) 4 tabs/day SUBOXONE (buprenorphrine/naloxone) 3 tabs or films/day 8-2 mg
SUBOXONE (buprenorphrine/naloxone) 2 films/day 12-3 mg
SUBOXONE (buprenorphrine/naloxone) 6 films/day 4-1 mg SUBOXONE (buprenorphrine/naloxone) 12 tabs or films/day 2-0.5 mg SUBSYS (fentanyl) 16 sprays/day SUBUTEX (buprenorphrine) 8 m£_ . 3 tabs/day
'l OptumRx 1 optumrx.com

Analgesics (opioid) (cont.) SUBUTEX (buprenorphrine) 2 mg 12 tabs/day ULTRAM ER (tramadol ext-release) 1 tab/day ZUBSOLV (buprenorphine/naloxone) SL 3 tabs/day Tab 5.7-1.4 MG ZUBSOLV (buprenorphine/naloxone) SL 2 tabs/day Tab 8.6/2.1 MG ZUBSOLV (buprenorphine/naloxone) SL 1 tab/day Tab 11.4/2.9 MG ZUBSOLV (buprenorphine/naloxone) SL 6 tabs/day Tab 2.9/0.71 MG ZUBSOLV (buprenorphine/naloxone) SL 12 tabs/day Tab 1.4-0.36 MG
Anticonvulsants DIAZEPAM GEL (diazepam) 2 boxes/fill GRALISE (gabapentin) 300 mg 6 tabs/day GRALISE (gabapentin) 600 mg 3 tabs/day GRALISE (gabapentin) Pack 1 kiVfill (78 tabs per fill) HORIZANT (gabapentin enacarbil) 2 tabs/day LYRICA (pregabalin) 300 mg 2 caps/day LYRICA (pregabalin) caps 3 caps/day
Antidepressants APLENZIN (bupropion) 1 tab/day BRINTELLIX (vortioxetine) 1 tab/day CYMBALTA (duloxetine) 2 caps/day CYMBALTA (duloxetine) 30 mg 3 caps/day desvenlafaxine fumarate (desvenlafaxine) 1 tab/day EMSAM (selegiline) 1 patch/day FETZIMA (levomilnacipran) 1 cap/day FETZIMA (levomilnacipran) Pack 1 pack (28 caps)/year
FORFIVO XL (bupropion) 450 mg 1 tab/day IRENKA (duloxetine) 2 caps/day KHEDEZLA (desvenlafaxine ER) 1 tab/day KHEDEZLA (desvenlafaxine ER) 100 mg 4 tabs/day
LUVOX CR (fluvoxamine) 2 caps/day OLEPTRO (trazodone) 1 tab/day PEXEVA (paroxetine) 1 tab/day PEXEVA (paroxetine) 30 mg 2 tabs/day PRISTIQ (desvenlafaxine) 1 tab/day PRISTIQ (desvenlafaxine) 100 mg 4 tabs/day PROZAC WEEKLY (fluoxetine) 4 caps/28 days VIIBRYD (vilazodone) 1 tab/day VIIBRYD (vilazodone) Kit 1 kit (30 tabs)! fill WELLBUTRIN SR (bupropion) 3 tabs/day WELLBUTRIN XL (bupropion) 1 tab/day
5

Antidepressants (cont.) WELLBUTRIN XL (bupropion) 150 mg 3 tabs/day Antipsychotics ABILIFY (aripiprazole) tabs 1 tab/day
ABILIFY DISCMELT (aripiprazole) 2 tabs/day ABILIFY SOLN (aripiprazole) 1 mg/ml 25 mUday CLOZARIL (clozapine) 100 mg 9 tabs/day CLOZARIL (clozapine) 200 mg 4 tabs/day CLOZARIL (clozapine) 25 mg 9 tabs/day CLOZARIL (clozapine) 50 mg 6 tabs/day FANAPT (iloperidone) 2 tabs/day FANAPT PAK (iloperidone) 1 pack/180 days FAZACLO (clozapine) 100 mg 9 tabs/day FAZACLO (clozapine) 12.5 mg 3 tabs/day FAZACLO (clozapine) 150 mg 6 tabs/day FAZACLO (clozapine) 200 mg 4 tabs/day FAZACLO (clozapine) 25 mg 9 tabs/day GEODON (ziprasidone) 2 caps/day
INVEGA (paliperidone) 1 tab/day INVEGA (paliperidone) 6 mg 2 tabs/day
LATUDA (lurasidone) 20 mg, 40 mg, 1 tab/day 60mg, 120 mg LATUDA (lurasidone) 80 mg 2 tabs/day
REXULTI (brexpiprazole) 1 tab/day ····--.. - .. -~
RISPERDAL (risperidone) 2 tabs/day RISPERDAL M (risperidone) 2 tabs/day
RISPERDAL SOLN (risperidone) 8 mUday SAPHRIS (asenapine) 2 tabs/day SEROQUEL (quetiapine) 2 tabs/day SEROQUEL (quetiapine) 25 mg, 50 mg, 3 tabs/day 100 mg, 200 mg SEROQUEL XR (quetiapine) 2 tabs/day
SEROQUEL XR (quetiapine) 200 mg _______ 3 tabs/day -·-·-·····--·"'"
SYMBYAX (olanzapine/fluoxetine) 1 cap/day SYMBYAX (olanzapine/fluoxetine) 3 caps/day 3-25 mg SYMBYAX (olanzapine/fluoxetine) 3 caps/day 6-25 mg VERSACLOZ (clozapine) 18 mUday ZYPREXA (olanzapine) 1 tab/day ZYPREXA ZYDIS (olanzapine) 1 tab/day
Benzodiazepines FLURAZEPAM (flurazepam) 1 cap/day CHLORDIAZEP (chlordiazepoxide) 10 mg 30 caps/day
6 OptumRx 1 optumrx.com

Fibromyalgia
Hypoactive Sexual Desire Disorder Migraine
Migraine (cont.)
CHLORDIAZEP (chlordiazepoxide) 25 mg 12 caps/day
-'C:.cH.c:Lc::OccRc:cDc:_IAZ=E:_P ~(c::_:h:_::lo'-'rd::c:ia=z""ep""o"-x:c::idc::e,_) 5::__:_cm~g._____c4_::c='apc.:s::.-=/d<Jy ~~~-~-~~ _ CLONAZEP ODT (clonazepam) 3 tabs/day CLONAZEP ODT (clonazepam) 2 mg 10 tabs/day CLORAZ DIPOT (clorazepate) 15 mg 6 tabs/day CLORAZ DIPOT (clorazepate) 3.75 mg 24 tabs/day CLORAZ DIPOT (clorazepate) 7.5 mg 12 tabs/day DORAL (quazepam) 1 tab/day ESTAZOLAM (estazolam) 1 tab/day HALCION (triazolam) 2 tabs/day KLONOPIN (clonazepam) 3 tabs/day LORAZEPAM (lorazepam) 3 tabs/day
LORAZEPAM (lorazepam) 2 mg 10 tabs/day OXAZEPAM (oxazepam) 4 caps/day
TEMAZEPAM (temazepam) 1 cap/day XANAX (alprazolam) 4 tabs/day XANAX (alprazolam) 2 mg 5 tabs/day XANAX XR (alprazolam) 1 tab/day XANAX XR (alprazolam) 2 mg 5 tabs/day XANAX XR (alprazolam) 3 mg 3 tabs/day SA VELLA (milnacipran) 2 tabs/day SA VELLA (milnacipran) Pack 1 pack (55 tabs)/year ADDYI (flibanserin) 1 tab/day
ALSUMA (sumatriptan)
AMERGE (naratriptan) AXERT (almotriptan) FROVA (frovatriptan) IMITREX (sumatriptan) IMITREX (sumatriptan) AUTO-INJECTOR 4 mg/0.5 ml & 6 mg/0 IMITREX (sumatriptan) CARTRIDGE 4 mg/0.5 ml & 6 mg/0.5 m IMITREX (sumatriptan) Nasal IMITREX (sumatriptan) SYRINGE 4 mg/0.5 ml & 6 mg/0.5 ml
5 packages (1 0 syringes)/ 30 days 9 tabs/30 days
12 tabs/30 days 9 tabs/30 days 9 tabs/30 days 5 kits ( 1 0 units)/30 days
5 kits (1 0 units)/30 days
12 spray unit devices/30 days 5 kits (1 0 units)/30 days
MAXALT (rizatriptan) 18 tabs/30 days~-----~----MAXALT-MLT (rizatr _ _,_ip_ta_n,_) ______ 18_ta_b_s/_3_0_d~ay,_s_
MIGRANAL (dihydroergotamine) 1 package (8 vials)/30 days
RELPAX (eletriptan) 12 tabs/30 days SUMAVEL DOSEPRO (sumatriptan) 12 prefilled syringes/30 days
7

Miscellaneous
Sedative Hypnotics
Stimulants
Dermatology Miscellaneous
Miscellaneous
TREXIMET (sumatriptan/naproxen) 9 tabs/30 days
ZECUITY (sum:.=at:.:_r:.cip-"ta"-n"-) ______ __:_4 system?Jl_ci)rton2f30 days. ZOMIG (zolmitriptan) 9 tabs/30 days ZOMIG (zolmitriptan) 2.5 mg 12 tabs/30 days ZOMIG (zolmitriptan) Nasal 2 packages (12 spray units)/
30 days ZOMIG ZMT (zolmitriptan) ZOMIG ZMT (zolmitriptan) 2.5 mg
RILUTEK (riluzole)
AM BIEN (zolpidem)
AMBIEN CR (zolpidem)
BELSOMRA (suvorexant)
EDLUAR (zolpidem)
INTERMEZZO (zolpidem)
LUNESTA (eszopiclone)
ROZEREM (ramelteon)
SILENOR (doxepin)
SONATA (zaleplon) 10 mg SONATA (zaleplon) 5 mg ZOLPIMIST (zolpidem) NUVIGIL (armodafinil) NUVIGIL (armodafinil) 50 mg PROVIGIL (modafinil)
ENSTILAR (calcipotriene-betamethasone dipropionate) TACLONEX (calcipotriene/betamethasone) TACLONEX SCALP (calcipotriene/ betamethasone) TAZORAC (tazarotene) FABIOR (tazarotene)
9 tabs/30 days 12 tabs/30 days 2 tabs/day
1 tab/day
1 tab/day
1 tab/day
1 tab/day
1 tab/da=-'y ______ _ 1 tab/day
1 tab/day
1 tab/day
2 cap/day 1 cap/day 1 bottle (7. 7 g)/30 days 1 tab/day
2 tabs/day 1 tab/day
420 g/28 days
400 g/30 days 120 g/30 days
1 00 g/30 days 1 00 g/30 days
Endocrinology & Metabolism Androgens, Anabolic OXANDRIN (oxandrolone) 10 mg 2 tabs/day Steroids OXANDRIN (oxandrolone) 2.5 mg 8 tabs/day
Antidiabetic Agents _.,B__.Y_.-D_.-U,..R_.-EO___,_,N-'( e::.cxo::.en:.:.:a:.:ti:.::d::ce lc__ _____ __:4-'v:.::ia:.::ls/'J:p_.-e:.:n-:.:.:i n~j/_.-2:::8_.-d--,ayc:-s._. __ _ BYETTA (exenatide) soln 10 meg 2 syringes/30 days BYETTA (exenatide) soln 5 meg 2 syringes/30 days TANZEUM (albiglutide) 4 pen-inj/28 days. TRULICITY (dulaglutide) 4 pen-inj/28 days.
Antidiabetic Agents (cont.) VICTOZA (Jiraglutide) 3 pen-inj/ 30 days Osteoporosis ACTONEL (risedronate) 150 mg 1 tab/28 days
8 OpturnRx ] optumrx.com

ACTONEL (risedronate) 35 mg 4 tabs/28 days
ATELVIA (risedronate) 4 tabs/28 days
BINOSTO (alendronate) 4 tabs/28 days
BON IVA (ibandronate) 1 tabs/28 days -""--·-··------~ --~
BON IVA IV (ibandronate) 1 syringe/90 days
FORTICAL (calcitonin) 1 bottle (3. 7 mL)/30 days
FOSAMAX (alendronate) 35 mg & 70 mg 4 tabs/28 days
FOSAMAX PLUS D (alendronate/ 4 tabs/28 days cholecalciferol) MIACALCIN (calcitonin) 1 bottle (3. 7 mL)/30 days
Gastroenterology
Antiemetics AKYNZEO (netupitant-palonosetron) 2 tabs/30 days
ANZEMET (dolasetron) 2 tabs/30 days
CESAMET (nabilone) 20 tabs/fill or 3 max days
DICLEGIS (doxylamine-pyridoxine) 4 tabs/day
EMEND (aprepitant) 125 mg 2 caps/30 days
EMEND (aprepitant) 125 mg/80 mg 2 packs (6 caps)/30 days
EMEND (aprepitant) 40 mg 1 cap/30 d~ys
EMEND (aprepitant) 80 mg 4 caps/30 days
GRANISOL (granisetron) 1 bottle (30 mL)/30 days
KYTRIL (granisetron) 4 tabs/30 days
MARINOL (dronabinol) 2 caps/day
SANCUSO (granisetron) 2 patches/30 days
VARUBI (rolapitant) 4 tabs/30 days
ZOFRAN (ondansetron) 120 mU30 days
ZOFRAN (ondansetron) 24 mg 2 tabs/30 days
ZOFRAN (ondansetron) 4 mg, 8 mg 15 tabs/30 days
ZOFRAN ODT (ondansetron) 4 mg, 8 mg 15 tabs/30 days
ZUPLENZ (ondansetron) 10 films/30 days
Constipation AMITIZA (lubiprostone) 2 caps/day
LINZESS (linaclotide) 1 cap/day
Diarrhea FULYZAQ (crofelemer) 2 tabs/day
Irritable Bowel Syndrome VIBERZI (eluxadoline) 2 tabs/day
Opioid-induced MOVANTIK (naloxegol) 1 tab/day
Constipation RELISTOR (methylnaltrexone) 1 syringe/day
RELISTOR (methylnaltrexone) Kit 1 vial/day
Proton Pump Inhibitors ACIPHEX (rabeprazole) 1 tab/day
ACIPHEX SPRINKLE (rabeprazole) SPR 1 cap/day
Proton Pump Inhibitors _QE_XJL~f'JI(de_xla_f)!;()Pra;c_ole)____ __ _ 1 cap/day ------------ -------------------------------------
9

Miscellaneous Diabetic Supplies
Methotrexate Auto-Injectors
Smoking Cessation
Products
Obstetrics & Gynecology
esomeprazole strontium (esomeprazole strontium) NEXIUM (esomeprazole) Caps
NEXIUM (esomeprazole) Packs
PREVACID (lansoprazole)
PREVACID (lansoprazole) Solutab
PRILOSEC (omeprazole)
PRILOSEC PACKETS (omeprazole)
PROTONIX (pantoprazole) packets
PROTONIX (pantoprazole) tab
ZEGERID (omeprazole) caps
ZEGERID (omeprazole) packets
Glucose Test Strips & Lancets (test strip & lancets) OTREXUP (methotrexate) RASUVO (methotrexate)
CHANTIX (varenicline)
COMMIT (nicotine lozenges)
NICODERM (nicotine transdermal)
NICORETIE (nicotine gum)
NICOTROL Inhaler (nicotine)
NICOTROL NS (nicotine)
ZYBAN (bupropion)
Contraceptives AMETHIA (levonorg-eth est)
AMETHIA LO (levonorg-eth est)
ASHLYNA (levonorg-eth est)
Contraceptives (cont.)
10 OptumRx I optumrx.com
CAMRESE (levonorg-eth est)
CAMRESE LO (levonorg-eth est)
DAYSEE (levonorg-eth est)
DEPO/DEPO-SUBQ PROVERA (medroxyprogesterone)
INTROVALE (levonorg-eth est)
JOLESSA (levonorg-eth est)
LOSEASONIQUE (ethinyl estradiol/ levonorgestrel) QUARTETIE (levonorg-eth est)
QUASENSE (levonorg-eth est)
SEASONIQUE (ethinyl estradiol/ levonorgestrel)
1 cap/day
1 cap/day
1 packet/day
1 cap/day
1 cap/day
1 cap/day
60 packets/30 days
1 packet/day
1 tab/day
2 caps/day
2 packets/day
300/30 days
4 auto-injectors/28 days 4 auto-injectors/28 days
180 days supply/year
180 days supply/year
180 days supply/year
180 days supply/year
180 days supply/year
180 days supply/year
180 days supply/year
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/90 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)
1/91 days (3 copays per fill)

Hormone Replacement
Miscellaneous
Ophthalmology Anti-inflammatory
Prostaglandins
Respiratory
Allergy (intranasal)
Allergy (intranasal) (cont.)
Asthma/COPD (inhaled)
Asthma/COPD (inhaled) (cont.)
FEMRING (estradiol acetate)
BRISDELLE (paroxetine)
BROMDAY (bromfenac)
ILEVRO (nepafenac) 0.3%
LOTEMAX (loteprednol) gel, oint
NEVANAC (nepafenac) 0.1%
PROLENSA (bromfenac sodium)
LUMIGAN (bimatoprost)
RESCULA (unoprostone)
TRAVATAN (travoprost)
TRAVATAN Z (travoprost)
XALATAN (latanoprost)
ZIOPTAN (tafluprost)
ASTELIN (azelastine)
ASTEPRO (azelastine)
BECONASE AQ (beclomethasone)
DYMISTA (fluticasone/azelastine)
FLUNISOLIDE (flunisolide)
NASON EX (mometasone)
OM NARIS (ciclesonide)
PATANASE (olopatadine)
QNASL (beclomethasone)
QNASL CHILDRENS (beclomethasone)
RHINOCORT AQUA (budesonide)
VERAMYST (fluticasone furoate) ZETONNA (ciclesonide nasal)
ADVAIR DISKUS (fluticasone/salmeterol)
ADVAIR HFA (fluticasone/salmeterol)
AEROSPAN (flunisolide)
ALVESCO (ciclesonide)
AN ORO ELLIPTA (umeclidinium-vilanterol)
1 package/90 days
1 package/90 days
1 cap/day
4 bottles/year
2 bottles/month
4 bottles/year
6 mU30 days
4 bottles/year
1 bottle (2.5 ml)/25 days
1 bottle (5 ml)/25 days
1 bottle (2.5 ml)/25 days
1 bottle (2.5 ml)/25 days
1 bottle (2.5 ml)/25 days
1 container/day
2 bottles (60 ml)/30 days
2 bottles (60 ml)/30 days
1 inhaler (25 g)/25 days
1 inhaler (23 g)/30 days
1 bottle (25 ml)/30 days
2 inhalers/30 days 1 inhaler (12.5 g)/30 days
1 bottle (30.5 g)/30 days
1 inhaler (8. 7 g)/30 days
1 inhaler (4.9 g)/30 days
2 bottles/30 days
1 bottle (1 0 g)/30 days
1 inhaler (6.1 g)/30 days
1 diskus (60 doses)/30 days
1 inhaler/30 days
2 inhalers (8.9 g each)/30 days
2 inhalers (6.1 g each)/30 days
1 package (60 blisters)/30 days
ARCAPTA (indacaterol) 4 caps/day
ARNUITY ELLIPTA (fluticasone furoate) ~-!J"l~aler/30 days
_A_S_M_A_N_E_X_H_F_A__:(_m_o_m_e_ta~so_n_e:__) ~~--c--_1_ inhaler/30 days ASMANEX TWISTHALER (mometasone) 1 inhaler/30 days
ATROVENT HFA (ipratropium)
BREO ELLIPTA (fluticasone furoate-vilanterol)
2 inhalers (12.9 g each)/30 days
1 package (60 blisters)/30 days
11

COMBIVENT RESPIMAT (ipratropium/albuterol)
2 inhalers (4 g each)/30 days
DULERA (mometasone/formoterol) 1 inhaler/30 days
FLOVENT (fluticasone) 110 meg, 220 meg 2 inhalers (12 g each)/30 days
FLOVENT (fluticasone) 44 meg 2 inhalers/30 days
FLOVENT DISK US (fluticasone) 250 meg 240 blisters/30 days - - -~~--~~~--~~-------
FLOVENT DISKUS (fluticasone) 60 blisters/30 days 50 meg, 1 00 meg -----""--:-:----"----:c----------------~-----:----:-----:--- . ---FORADIL (formoterol) 1 package (60 doses)/30 days
IN CRUSE ELLIPTA (umeclidnium) 1 inhaler/30 days
MAXAIR AUTOHALER (pirbuterol) 1 inhaler (14 g)/30 days
PROAIR HFA (albuterol) 2 inhalers/30 days
PROAIR RESPICLICK (albuterol) 2 inhalers/30 days
PROVENTIL HFA (albuterol) 2 inhalers/30 days
PULMICORT FLEXHALER (budesonide) 2 packages/30 days
QVAR (beclomethasone) 40 meg 2 inhalers/30 days
QVAR (beclomethasone) 80 meg 3 inhalers/30 days
SEEBRI NEOHALER (glycopyrolate) 2 caps/day
SEREVENT DISKUS (salmeterol) 50 meg 1 package (60 doses)/30 days
SPIRIVA HANDIHALER (tiotropium) 1 package (30 caps)/30 days
SPIRIVA RESPIMAT (tiotropium) 1 inhaler/30 days
STIOLTO RESPIMAT (tiotropium 1 inhaler/30 days br-olodaterol)
STRIVERDI RESPIMAT (olodaterol)
SYMBICORT (budesonide/formoterol)
TUDORZA (aclidinium bromide)
UTIBRON NEOHALER (indacaterol maleate-glycopyrrolate)
VENTOLIN HFA (albuterol)
XOPENEX HFA (levalbuterol)
1 inhaler/30 days
1 inhaler/30 days
1 pouch (60 doses)/30 days
2 caps/day
2 inhalers/30 days
2 inhalers (15 g)/30 days
Asthma/COPD (nebulized) ACCUNEB (albuterol) 5 packages (125 vials or 375 ml)/30 days
Albuterol (albuterol) 2.5 mg/3 ml (0.083%)
180 vials (540 ml)/30 days
Albuterol (albuterol) 5 mg/ml (0.5%) 5 packages (1 00 ml)/30 days
_A_J_R_O_V_EN_T-c('-'ipc-ra_t_ro_._p_iu_m_-':) _____________ 12_5_v_ia_l--'-s (31~:_5_ml)/3~_d<!E BROVANA (arformoterol) 60 vials (120 ml)/30 days ------~----:-----c' ____ :c-__________ __--':_c--· - -------- ------- --
Asthma/COPD (nebulized) DUONEB (ipratropium/albuterol) 180 vials (540 ml)/30 days
12 OptumRx I optumrx.com

(cont.)
Urology
Erectile Dysfunction
Overactive Bladder Antispasmodics
Metaproterenol (inhalation solution)
PERFOROMIST (formoterol)
PROVENTIL (albuterol) 2.5 mg/3ml (0.083%) PULMICORT RESPULES (budesonide)
XOPENEX (levalbuterol)
XOPENEX (levalbuterol) 1.25 mg/0.5 ml
XOPENEX (levalbuterol) 1.25 mg/3 ml
CAVERJECT (alprostadil)
ClAUS (tadalafil) 10 mg
ClAUS (tadalafil) 2.5 mg ClAUS (tadalafil) 20 mg
ClAUS (tadalafil) 5 mg
EDEX (alprostadil)
LEVITRA (vardenafil)
MUSE (alprostadil) STAXYN (vardenafil) STENDRA (avanafil) VIAGRA (sildenafil)
OXYTROL (oxybutynin)
5 packages (125 ampules or 312.5 mL)/30 days 60 vials (120 mL)/30 days
175 vials (525 ml)/30 days
2 packages (120 ml)/30 days
180 vials (540 ml)/30 days
90 vials (45 ml)/30 days
90 vials (270 mL)/30 days
6 units/30 days
6 tabs/30 days
1 tab/day 6 tabs/30 days
1 tab/day
6 units/30 days
6 tabs/30 days 6 units/30 days
6 tabs/30 days 6 tabs/30 days 6 tabs/30 days 8 patches/28 days
Select Specialty Quantity Limit
Anti-lnfectives
Antiretrovirals, Hepatitis B --'B"-A~R::_A:_:Cc::Lc:_U=-DE"--"'(e::..:n.::.:te:.::ca=-vc:.:ir_,_) -:-:-_____ .-:1.-:ta::.:b:::_/d::.:a:LY ______ _ _________ BARACLUDE (entecavir) Soln 630 mU30 days
Antiretrovirals, HIV
Cardiology Anticoagulants, LMWH
Antilipemic
Pulmonary Arterial
Hypertension
Pulmonary Arterial
FUZE ON (enfuvirtide) 60 vials or 1 kit/30 days
ARIXTRA (fondaparinux) 35 days supply/180 days FRAGMIN (dalteparin) 35 days supply/180 days LOVENOX (enoxaparin) 35 days supply/180 days JUXTAPID (lomitapide) 1 tab/day KYNAMRO (mipomersen) 4 syringes/28 days PRALUENT (alirocumab) 2 syringes/28 days REPATHA (evolocumab) 3 syringes/28 days ADCIRCA (tadalafil) 2 tabs/day ADEM PAS (riociguat) 3 tabs/day LETAIRIS (ambrisentan) 1 tab/day
OPSUMIT (m.:.:ca:..:c::..:ite.::.:n.:.::t.::.:an2 ) ____ _ 1 tab~M=aLy ______ __
13

Hypertension (cont.)
Central Nervous System
REVATIO (sildenafil) Tabs TRACLEER (bosentan)
TYVASO (treprostinil) UPTRAVI (selexipag) UPTRAVI (selexipag) Pack VENTAVIS (iloprost)
2 bottles/30 days 3 tabs/day 2 tabs/day 1 ampule/day
2 tabs/day 2 packs/year 9 ampules/day
Depressant XYREM (sodium oxybate) 3 bottles (540 mL)/30 days
-'-P~a'-rk::cinc:csoc_:n_:_'=-s _____ _:_A..c.P-=O-'-K'-'-Y_N_,('-'ap'-o'-m __ o'-rpcch_:_in=-e:..c) _______ 2_0-'ca'-r-'-tr.idges/3_0'-d"'a_Lys=-----Sieep Disorder HETLIOZ (tasimelteon) 1 cap/day Electrolyte & Renal Agents
Diuretics KEVEYIS (dichlor.r:P:.:_he::n:.=a.:.:.m:::id=-=e,_) --------'4-=t=ab::.:s::c/d=a,_y ______ _
Endocrinology & Metabolism -c:---:c-c-:--:cc:-=---:c--~---:--:-c-:---:::-c-:------Gonadotropins ELIGARD (leuprolide) 22.5 mg (3-month) 1 injection/84 days
Growth Hormones and Related Therapy Hormone Modifiers
Miscellaneous
Somatostatins
Vasopressin Antagonist
14 OptumRx 1 optumrx.com
ELIGARD (leuprolide) 30 mg (4-month) 1 injection/112 days
ELIGARD (leuprolide) 45 mg (6-month) 1 injection/168 days ELIGARD (leuprolide) 7.5 mg (1-month) 1 injection/28 days FIRMAGON (degarelix) 120 mg 2 vials/year FIRMAGON (degarelix) 80 mg 1 vial/28 days LUPANETA PACK (leuprolide) 1 pack/84 days 11.25 mg (3 mon) LUPANETA PACK (leuprolide) 3.75 mg (1 mon) SUPPRELIN LA (histrelin acetate) TRELSTAR (triptorelin) 22.5 mg (6-month)
TRELSTAR DEPOT (triptorelin) 3.75 mg (1-month) TRELSTAR LA (triptorelin) 11.25 mg (3-month) VANTAS (histrelin) ZOLADEX (goserelin) 10.8 mg ZOLADEX (goserelin) 3.6 mg
EGRIFTA (tesamorelin) 1 mg EGRIFTA (tesamorelin) 2 mg NATPARA (parathyroid hormone) KORLYM (mifepristone) PROLIA (denosumab)
SIGNIFOR (pasireotide) SIGNIFOR LAR (pasireotide) SAMSCA (tolvaptan)
1 pack/28 days
1 kit/365 days 1 injection/168 days 1 injection/28 days
1 injection/84 days
1 implant/year
1 injection/84 days 1 injection/28 days 2 vials (1 mg each)/day 1 vial (2 mg each)/day 2 cartridges/28 days
4 tabs/day 2 syringes/year 2 ampules/day 1 vial/28 days
3()_ days supply/60 days

Enzyme-Related
Cystine-depleting Agents
Immunology
Allergen Extracts
Hematopoietic Agents Hepatitis C Agents
lnterleukins Multiple Sclerosis
CYSTARAN (cysteamine) XU RIDEN (uridine triacetate)
GRASTEK (timothy grass pollen) ORALAIR (mixed grass pollens allergen) 3001R ORALAIR ADULT SAMPLE KIT (mixed grass pollens allergen) Kit
ORALAIR ADULT STARTER PACK (mixed grass pollens allergen) ORALAIR CHILDREN/ADOLESCENTS (mixed grass pollens allerg ORALAIR CHILDREN/ADOLESCENTS (mixed grass pollens allerg RAGWITEK (short ragweed pollen allergen) MOZOBIL (plerixafor) DAKLINZA (daclatasvir dihydrochloride) 30 mg DAKLINZA (daclatasvir dihydrochloride) 60 mg HARVONI (ledipasvir-sofosbuvir) OLYSIO (simeprevir) SOVALDI (sofosbuvir)
TECHNIVIE (ombitasvir-paritaprevirritonavir) VIEKIRA (simeprevir)
ZEPATIER (elbasvir-grazoprevir) ILARIS (canakinumab) AMPYRA (dalfampridine) AUBAGIO (teriflunomide)
AVON EX (interferon beta-1 a) BETASERON (interferon beta-1b) COPAXONE (glatiramer) SOSY 20 mg/ml COPAXONE (glatiramer) SOSY 40 mg/ml EXT A VIA (interferon beta-1 b) GILENYA (fingolimod)
GLATOPA (glatiramer) SOSY 20 mg/ml PLEGRIDY (peginterferon beta) PLEGRIDY (peginterferon beta) Starter Pack REBIF (interferon beta-1 a)
4 bottles/28 days 4 packets/day
1 tab/day 1 tab/day
1 kit/year
1 pack/year
2 kits/year
2 packs/year
1 tab/day
8 vials (9.6 mL)/transplant
3 tabs/day
1 tab/day
1 tab/day 1 cap/day 1 tab/day 2 tabs/day
4 tabs/day
1 tab/day 2 vials/4 weeks 2 tabs/day
1 tab/day 1 kit (4 syringes)/28 days
1 package/28 days 1 kit/30 days 1 kit/30 days 1 package/28 days
1 cap/day
1 kit/30 days ·-·--2 pens/syringes/28 days 1 starter pack/30 days
12 syringes/28 days
IS

REBIF (interferon beta-1 a) Starter Pack 1 starter pack/year
_T_E_C_FI_D_ER_A~(d_im_e~t~hy~l_fu_m_a~r~at~e~) ____ ~ __ 2_c~ap~s~M~ay,~------------TECFIDERA (dimethyl fumarate) Starter Pack 1 starter pack/year TYSABRI (natalizumab) 1 injection /28 days
Obstetrics & Gynecology
Hormone Replacement CRINONE (progesterone) 8% Oncology
Kinase and Molecular Target Inhibitors
Miscellaneous
Respiratory
Asthma/COPD Cystic Fibrosis
AFINITOR (everolimus) ALEC EN SA (alectinib) CAPRELSA (vandetanib) 100 mg COTELLIC (cobimetnib) FARYDAK (panobinostat) GILOTRIF (afatinib) ICLUSIG (ponatinib) 15 mg JAKAFI (ruxolitinib) 10 mg NINLARO (ixazomib) PORTRAZZA (necitumumab) Soln TAGRISSO (osimertinib) TARCEVA (erlotinib) 100 mg, 150 mg TARCEVA (erlotinib) 25 mg LONSURF (trifluridine-tipiracil) 15-6.14 MG LONSURF (trifluridine-tipiracil) 20-8.19 MG
NUCALA (mepolizumab) ORKAMBI (lumacaftor-ivacaftor) TOBI PODHALER (tobramycin)
Quantity Limits effective as of July 1, 2016.
60 applicators/30 days
1 tab/day 8 caps/day 2 tabs/day 63 tabs/28 days 6 caps/21 days 1 tab/day 2 tabs/day 2 tabs/day 3 caps/28 days 2 vials/21 days 1 tab/day 1 tab/day 3 tabs/day
100 tabs/28 d~ys __ __ 80 tabs/28 days
1 vial/28 days 112 tabs/28 days 1 package (224 tabs)/56 days
PLEASE NOTE: This drug list is subject to periodic updates and may not be all inclusive. Drugs affected included both brand and generic where applicable and includes all strengths unless otherwise specifically noted. If a targeted drug has a new strength, it will automatically be added to the list.
OPTUM' optumrx.com
OptumRx specializes in the delivery, clinical management and affordability of prescription medications and consumer health products. We are an OptumTM company- a leading provider of integrated health services. learn more at optum,com.
All OptumTM trademarks and logos are owned by Optum, Inc. All other brand or product names are trademarks or registered marks of their respective owners.
© 2016 Optum, Inc. All rights reserved. ORX0801E_160418 55530·042016

OPTUMRx"
Fresno City Employees Health & Welfare Trust Date Filled: July 1, 2015- June 30, 2016
Exclusion
Prior AuthoriUltion
Quantity Limit
Prior Authorization
Quantity Umit
1392
342
390
286
333
1105
307
322
222
288
1385
302
86
$382,539
$185,152
Page 1
67
53
49
3.30%
1.60%
53 42 $47,023 0.41% ,.
$36,817
$132,697
$151,271
$3.43
$1.66

Fresno City Employees Health & Welfare Trust Date Filled: July 1, 2015 -June 30, 2016 Standard Utilization Management Outcomes:
3 4
s 6 7
8
Inhaled Bronchodilator Inhaled Steroids Herpes A&ents Anticonvulsants ~2nd Generation
Ora! Anticoagulants Postherpetic Neuralgia {PHN) Agents Opioid Agonists & Combos
Nonsteroid<tl Anti~lnflammatory Agents
106 38 56 7 3 3
12
100 37 56 7
2 3
11
Page2
11 7
11 1
1 2 6
9 (NSA!Ds) 10 10 4 $2,399 10 Restless Leg Syndrome (Rl5) Agents 1 1 1 $1,995 11 Anti~lnflammatory Agents· Topical 11 11 S $1,780 12 Injectable Anticoagulants 3 3 0 $1,393 13 Opioid Partial Agonists 2 2 0 $892 14 Antifungals 18 18 7 $149
i tt!M WfW¥ AA¥4 lf@fii 'Est f iiH!tM
1 Impotence Agents 237 190 57 2 Migraine Products 53 48 10 3 Inhaled Asthm<:~/COPD Combo 12 12 4
4 Ophthalmic Prostaglandins 12 11 0 s Contraceptives 22 20 3 6 Immunosuppressive Agents 7 4 2
Nonsteroidal Anti·lnflamm<Jtory Aeents 7 (NSAIDs) 3 3 1 8 Inhaled Bronchodilator 5 5 0 9 Osteoporosis Agents 9 9 2 10 Opiold Agoni$1:s & Combos 12 12 s 11 lnh<:~led Steroids 3 3 0 12 Needles & Syringes 10 10 2 13 Herpes Agents. 1 1 0 14 Antidepressants 1 1 0 15 Influenza Agents 1 1 0 16 Antlfungals 2 2 0
$120,543 $10,52.6 $4,946 $4,62.9 $3,852 $2,755
$924 $804 $744
$554 $493 $469 $18 $8 $4
1&11111D1iihiiMM$1111-III*-IIiMjtjijjt-ijtn~-~-41:-ik#W

Fresno City Employees Health & Welfare Trust Date Filled: July 1, 2015 -June 30, 2016
2 Multiple Sclerosis
3 Oncology
4 Immune Serums
5 Antifungals- Topical
6 ADHD & Narcolepw Medications
7 Anti-Obesity Agents
8 Growth Hormones
9 Pulmonary ArteriJ:I Hypertension
10 HIV-Multldass Combo
11 Hepatitis B
12 Resplri>tory Syncytial Virus (RSV} Agents
13 Antipsoriatlcs- Topical
14 A01e Products
15 Anabolic Steroids
16 Osteoporosis Agents
17 Antiemetics
18 PCSK91nhibitors
19 Corticosteroids- Topical
2 ADHD & Narcolepsy Medic,:~tions
3 Proton Pump Inhibitors 4 Immunosuppressive Agents- Topical
5 Opioid Partial Agonists
6 Antifungals
7 Respiratory Syncytial Virus (RSV) Agents
8 Opioid Agonists & Combos
9 Fertility Medications
10 Anti-Obesity Agents
11 Atypical Antipsychotics
12 Progestins
13 Prenatal Vitamins
14 Vitamins & Supplements
2
3 2
35
10 164
2
1 1 1
2
10 15 3
3 6
2 1
39 160 29
12 46
2 4
9 31
2 1 1
1
Page3
2 1 0 $29,882 3 2 0 $28,613 1 1 0 $25,974 31 35 13 $19,466 10 6 2 $19,320
121 159 4 $14,368 2 0 0 $10,156 1 0 0 $7,145 1 1 0 $6,631 1 1 0 $5,612
1 2 2 $4,058 9 9 2 $1,653 13 14 1 $1,621 3 3 0 $810 3 0 0 $726 6 5 0 $621 2 1 0 $205 1 1 0 $153
29 30 11 $27,709 160 139 34 $21,616 27 29 2 $8,662 12 7 0 $6,634 43 42 4 $5,044
1 2 2 $4,939 4 3 0 $3,212 7 9 0 $2,327 28 31 0 $849 2 2 0 $703 1 1 0 $66 1 1 0 $2 1 1 0 $2

Page4
lit£]£&££ I H T 7777 rrmrmn 1' eyrgg;mlf%eyJ!i!l'L&~
Fresno City Employees Health & Welfare Trust Date Filled: July 1, 2015- June 30, 2016
2 3 4 5
SGLT-2 Inhibitors & Combos Injectable Diabetic Meds
Inflammatory Bowel Agents Inhaled Steroids
14 6 2 2
14 6 2 2
3 2 0 0
1 0 0 0
$15,423 $9,529
$2,251 $1,065
6 Diabetes Monitoring and Testing Supplies 9 6 8 3 $981 7 Inhaled Asthma/COPD Combo 1 1 0 0 $981 8 Statins & Combos 3 3 0 0 $943
,.fHf'®l EQ@QW@ pew ] 9'1% d'P'"® @itlfuMM\M*#¥¥¥1
2 Tetracyclines 19 18 19 4 $28,418 3 Antidepressants 23 18 ll ll $21,150 4 Leukotrlene Modulators 50 so 2S 16 $16,679 5 Acne Products 41 38 36 0 $9,360 6 Proton Pump Inhibitors 14 14 10 3 $9,288 7 Nasal Steroids 60 60 53 24 $8,2Sl 8 Anti emetics 6 6 4 0 $5,459 9 Corticosteroids- Topical 9 8 8 0 $5,447
Angiotensin II Receptor Antagonists & 10 Combos 14 14 6 3 $4,190 ll Antipsoriatics- Topical ll ll 10 0 $3,977 12 Sedative Hypnotics 4 3 2 2 $1,907 13 Anabolic Steroids 1 1 1 0 $556
'"' j'; ·''
The Comprehensive UM Program consists ofthe following: UM Type Description
WMi!ttill~-Helps ensure safe and appropriate dosing and avoid dangerous drug interactions through established guidelines and coverage levels. @i.J#.ffii.I.M..,!l!.J.lifMW Recommends pre-approval for certain medications before they are covered to promote safe and effective medication use plus keep pharmacy plan costs in check. ~tj.in,j~W!.!Wfd@ I Requires members to try preferred medications as the initial step in treatment before certain non-preferred medications are covered.

Fresno City Employees Health & Welfare Trust PA Detail Report Summary
Time Frame: 09.01.16-09.30.16
Row Labels Count of Case Number
--,.~~---NEVV 15 illliENI~-~ ,.~w;;$~1 ' ,' - - ._,;
APPEAL 1 NEVV 7
Grand Total 23

16272393498 NEW APPROVED PRIOR BELVIQ TAB 10MG I 09/27/16 09/28/16 1 16273101249 NEW APPROVED PRIOR AMPHETAMINE CAP I 09/28/16 09/30/16 2

OPTUMRx''
Fresno City Employees Health & Welfare Trust PA Detail Report Summary
Time Frame: 07.01.15-06.30.16
Row Labels
APPROVED
APPEAL APPEAL- SECOND LEVEL
NEW
APPROVED DENIED
NEW- DENIED
APPEAL- DENIED
Grand Total
Count of Case Number
299 15
2
281 1
82 77
5 381
APPEAL Total
1
1 2 3
4 5 6
13 14 16 17 18 19 21 27
1 4
0 1
2
3
1 1 2 1 1 1 1 1 1 1
1 1 1
1 15
1 1
68 25 24

494- FRESNO CITY EMP. NEW
NEW Total
NEW- DENIED Total
APPROVED Total
2
4
5 6
7
8 9
12 14 15
17
19 20
38
0 1 2
3
4 5
6 7
8
10 11
13
14 15
18
33
39
46
2
6
9
13
0
15 12
7 3
4 1 4 2 2 1
1 1
1 281
12 15
4 6
8 8
5 5
3
1 2
1
2 1
1
1
1
1
77
1 2
1
1
1
1

I I I
I I
OptumRx Prior Authorization Department Phone: 800-626-0072
OPTUMRx'' Fax: 866-511-2202
INFORMATIONONL¥ Prescriber Information Last Name
I I I I I I DEA/ NPI
I I I I I I Phone
I I I - I I I Member Information Last Name
I I I I I I Member iD Number
I I I I I I Med1cat1on Information· Drug Name and Strength:
Diagnosis:
I I I I I I I - I I
I I I I I I
First Name
I I I I I I I I I I Specialty
I I I I I I I I I I Fax
I I I I I I I - I First Name
I I I I I I I I I I DOB
I I I I I I I I I I
Quantity:
Dosing:
Proton Pump Inhibitors Prior Authorization
Initial Therapy
I I I I I I
I I I I
You must answer ALL of the following questions
I I I I I - I
I I I I
1, Has the patient had a trial and failure or intolerance to one of the following preferred generic PPis? A. Lansoprazoie B. Omeprazole C. Omeprazoie/sodium bicarbonate D, Pantoprazole
Dexilant 1, Has the patient had a trial and failure or intolerance to a preferred generic PPI (i.e.,
lansoprazole, omeprazole, omeprazole/sodium bicarbonate, pantoprazole) or Nexium 24HROTC?
Information given on this form Is accurate as of this date.
I I I
I I
Prescriber or Authorized Signature Date
Authorized Medical Staff- Name/Title
I I I I I I I I I
I I I I I I
y
y
Attention Health care Provider: If you would like to discuss this request with a medical professional, please
Page 1 of 2
5/19/2016
I I I I
I I I I
N
N

OPTUMRx"
OptumRx Prior Authorization Department Phone: 800·626·0072 Fax: 866·511·2202
contact the Prior Authorization Department at 800·626·0072.
I understand that the use or disclosure by OptumRx of Individually identifiable health Information, whether furnished by me or obtained by another source such as medical providers, shall be In accordance with federal privacy regulations under HIPAA (Health Insurance Portability and Accountability Act of 1996).
Page 2 of 2
5/19/2016

I
I I
I I
OptumRx Prior Authorization Department
Phone: 800-626-0072
OPTUMRx''' Fax:
INFORMATION ONLY ·!====!J Prescriber Information Last Name First Name
I I I I I I I I I I I I I I I I I I I I I I I I DEA/ NPI Specialty
I I I I I I I I I I I I I I I I I I I I I I I I Phone Fax
I I I c I I I I - I I I I I I I I I - I I I I - I I Member Information Last Name First Name
I I I I I I I I I I I I I I I I I I I I I I I I Member ID Number DOB
I I I I I I I I I I I I I I I I I I I I I I I I Medication Information·
Drug Name and Strength: Quantity:
Diagnosis: Dosing:
Migraine Quantity Limits Prior Authorization Initial Therapy
You must answer ALL of the following questions 1. What is the patient's diagnosis? (Please circle or provide below.)
A. Acute migraines with or without aura B. Cluster headaches C. Other. Please document:
2. Is the medication prescribed by or in consultation with a neurologist or pain management specialist?
3. Is the patient experiencing 2 or more headaches per month? 4. Does the patient experience 15 or more headaches per month? 5. Is the patient currently receiving prophylactic therapy with at least one of the following:
antidepressants, anticonvulsants, or beta-blockers?
6. Is the medication being used in combination with another triptan or ergotamine-containing product?
7. Is the higher dose or quantity supported in the Dosage and Administration section of the manufacturer's prescribing information?
8. Is the higher dose or quantity supported by one of the following compendia: American Hospital Formulary Service Drug Information or Micromedex DRUGDEX System?
Comments: Information given on this form is accurate as of this date.
Page 1 of2
5/9/2016
I I I I I I I I I I I I I
I I I I I I I I I I
y N
y N y N y N
y N
y N
y N

OptumRx Prior Authorization Department Phone: 800-626-0072
OPTUMRx" Fax: 866-511-2202
Prescriber or Authorized Signature Date
Authorized Medical Staff- Name/Title
Attention Healthcare Provider: If you would like to discuss this request with a medical professional, please contact the Prior Authorization Department at 800-626·0072.
I understand that the use or disclosure by OptumRx of Individually Identifiable health information, whether furnished by me or obtained by another source such as medical providers, shall be In accordance with federal privacy regulations under HIPAA (Health Insurance Portability and Accountability Act of 1996).
Page 2 of 2
5/9/2016

DELTA DENTAL OF CALIFORNIA NETWORK UTILIZATION REPORT BY APPROVED AMOUNT (Excluding Orthodontics) FRESNO CITY EES HEALTH & Group Number: 00273
Delta Dental PPO
Delta Dental Premier
Non-Contracted
Total
Delta Dental Premier
Non-Contracted
$3,357,782
$1,073,935
$204,744
$3,015,502
$978,870
$154,639
$89.54
$28.64
$5.46
$123.63
$83.35
$27.06
$4.27
$114.68
23.6%
3.7%
Note: Benchmark based on statewide averages. Results may vary due to benefit design, industry, age and area location.
* Proc/ 1 k I Yr =Procedures Per 1,000 Enrollees Per Year
38,636
8,815
1,050
48,501
35,190
8,739
953
12,363
2,821
336
15,519
11,672
2,899
316
79.7%
18.2%
2.2%
Delta Dental Actuarial
10/07/2016

DELTA DENTAL OF CALIFORNIA NETWORK UTILIZATION REPORT BY PAID AMOUNT (Excluding Orthodontics) FRESNO CITY EES HEALTH & Group Number: 00273
Delta Dental PPO
Delta Dental Premier
Non-Contracted
$1,963,044
$482,386
$54,896
$1,797,077
$482,746
$40,592
$2,320,415
$52.35
$12.86
$1.46
$66.67
$49.67
$13.34
$1.12
$64.14
77.4%
20.8%
1.7%
Delta Dental Actuarial
10/07/2016

DELTA DENTAL OF CAUFORNIA DISTRIBUTION OF SERVICES BY APPROVED AMOUNT AND NUMBER OF PROCEDURES BY NETWORK (Excludlng Orthodontics) FRESNO CITY EES HEAL. TH & Group Numbor. 00273
Restor3tlvc (DZOOO • OZ499) Endodontk:s (00000 • 00999) Poriodontk:s (O«lOO • 04999) Oral SurgCI)' (07000 • 07999) Miscellaneous (09000 • 09999)"
Subtotal
Delta Dental Actuarial
10/07/2016

DELTA DENTAL OF CAUFORNIA DISTRIBUTION OF SERVICES BY APPROVED AMOUNT AND NUMBER OF PROCEDURES BY NETWORK {Excluding Orthodontics) FRESNO CITY EES HEALTH & Group Number: 00273
Restorotlve (02000 • 02499) Endodontics (03000 • 039911) Pcriodoi\~CS (04000 • 04999) Oral Surgery (07000 • 07999) Mlscell~neous (09000 • 09999)"
Subtotal
• lnoludss Anos~o, ONgo ..,d A<IJ~netl~ 0...,...<1 Servlcer>
~ 13o>nohm..-k -"" bool<ofbuol"""""""'"_.._ Reoulta""')'wryd""l~benolll<looiQn, lnduotry, "'l"<W1d "'""k>callon.
Delta Dental Actuarial
10/07/2016

DELTA DENTAL OF CALIFORNIA DISTRIBUTION OF SERVICES BY PAID AMOUNT BY NETWORK FRESNO CITY EES HEALTH & Group Number: 00273
Restora~ve (02000 • 02499) Enclodol'ltlcs (03000. 03999) Periodontics (04000 ~ 04999) Oral Surgery (07000 • 07999) Miscellaneous {09000. 09999)"
Subtotal
Crowns & lnla)ISIOnlays (02500 • 02999) Removable Prosthodol'ltlcs (05000 • 05999) Implant Services (06000 • 06199) Fixed Prosthodontics (06200 - 06999)
Subtotal
RestoraWe {02000 • 02499) Enclodol'ltlcs {03000 • 03999) PeriodontiCS (04000 • 04999) Oral SurgCI)' {07000 • 07999) Miscellaneous {09000 • 09999)"
Subtotal
Crowns & lntays/Onlays {02500 • 02999) Removable Prosthodontics {05000 • 05999) lmplont Services (06000 • 06199) Axed Prosthodontics {06200 • 06999)
Subtotal
I OrthodontiCS
Orthodontics (08000 ~ 08999)
"lndudesAnoSthe&i<l, Drugs >:~rid Adjunctive Generol Services
Delta Dental Actuarial
10/07/2016

DELTA DENTAL OF CALIFORNIA COST SAVINGS REPORT (Excluding Orthodontics) FRESNO CITY EES HEALTH & Group Number: 00273
2) Provider Discounts* $1,621,828
Other Savings*"' $463,386
Total Savings $2,085,215
3) Plan Pays $1,963,044
4) Patient Liability *** $1,113,925
2) Provider Discounts* $1,262,292
Other Savings** $409,073
Total Savings $1,671,366
3) Plan Pays $1,797,077
4) Patient Liability *** $958,272
procedures for
31.4% $145,927
9.0% $154,680
40.4% $300,607
38.0% $482,386
21.6% $492,329
28.5% $121,764
9.2% $79,199
37.8% $200,963
40.6% $482,746
21.6% $441,144
** Other Savings includes services not payable due to duplicate submissions and missing or invalid information.
11.4%
12.1%
23.6%
37.8%
38.6%
10.8%
7.0%
17.9%
42.9%
39.2%
**'* Patient Liability includes non-covered and optional savings, coinsurance, maximums, deductibles and non-contracted provider fees.
$0 0.0%1 $40,720 18.2%
$40,720 18.2%
$54,896 24.5%
$128,484 57.3%1
$0 0.0%1 $40,869 22.9%
$40,869 22.9%1
$40,592 22.8%1
$96,690 54.3%1
$1,767,755 $658,787
$2,426,542
$2,500,326
$1,734,738
$1,384,057
$529,141
$1,913,198
$2,320,415
$1,496,106
26.0%
24.2%
9.2%
33.4%
40.5%
26.
Delta Dental Actuarial
10/07/2016

DELTA DENTAL OF CALIFORNIA DOLLAR-BANDED UTILIZATION REPORT (Excluding Orthodontics) FRESNO CITY EES HEALTH & Group Number: 00273
30,2016
No Utilization 3,398 35.4% <= $399.99 4,361 45.4%
$400 to $799.99 1,024 10.7%
$800 to $1,199.99 372 3.9% $1,200 to $1,599.99 216 2.3% $1,600 to $1,999.99 136 1.4%
September 30, 2015
No Utilization 3,246 35.0% <= $399.99 4,332 46.7%
$400 to $799.99 976 10.5% $800 to $1,199.99 334 3.6%
$1 ,200 to $1 ,599.99 189 2.0% $1,600 to $1,999.99 119 1.3%
79 0.9%
• Total members eligible to receive benefits during the period.
Delta Dental Actuarial
10/07/2016


0 - Fresno City Trust
TELADOC,
Septemberl1016TeladooUtillzatlon Report ~ ~ : ~ ~ , - , ~~" "_
Primaries 3,239 7 8 0.25%
Dependents 6,149 9 14 0.23%
Total Eligible Lives 9,388 16 22 0.23% 7
Percentage 0.17% 0.68%
Eligible lives: All members with access to the service {primaries and dependents)
YTD Primaries 3,174 148 80 2.52%
YTD Dependents 6,062 140 87 1.44%
YTD Total Eligible lives 9,236 288 167 1.81% 8
YTO Percentage 3.12% 5.26%
Annualized Utilization% 7~02% -
Primary Care Physician 49 $129_00
Specialist $193.00
Urgent Care Cl!n!c 97 $161.00
Emergency Room 6 $1,456.00
No treatment 14 $0.00
Total Consultations 167
azithromycln 250 mg oral tablet
Amoxicill!n 400 mg/5 ml oral powder for reconstitution
Augmentln 875 mg~125 mg oral tablet
Bactrlm OS 800 mg-160 mg oral tablet
Rating
#Responses
Poor
1
$6,321.00
$193.00
$15,617.00
$8,736.00
$0.00
$30,867.00
Total# Consults
#Consults with Rx
#Consults with no Rx
% Consults with Rx
Totai#Rx
Avg # Rx Per Consult
Acute maxillary sinusitis, unspecified
Acute slnuslUs, unspecified
Acute pharyngitis, unspecified
Acute cystitis without hematuria
Good
0 Excellent
7
167
136
31
81%
175
1.0
Increase utilization by communicating the Teladoc service to members. Vlsit hllp:l/teladoc.mymarkel!ngbench.com/ to download customized member communlcaUons.
(c) 2016 Te!aooc.~lnc. ~~ ~ ~~ ~-Proprietary and Confidential ~ ~ c ~ - ~ '~~ ~ Page 1 of 1 ~

0 - Fresno City Trust PPO High Option
TELADOC.
Primaries 2,554 6 5 0.20%
Dependents 4,995 8 12 0.24%
Total Eligible lives 7,549 14 17 0.23% 7
Percentage 0.19% 0.67%
Eligible Uves: All members with access to the service (primaries and dependents)
YTD Primaries 2,535 121 66 2.60%
YTD Dependents 4,970 125 81 1.63%
YTD Total Eligible Lives 7,505 246 147 1.96% 8
YTO Percentage 3.28% 5.80%
Annualized Utillzallan% - - 7.73% -- - -
Primary Care Physician 42 $129.00
Specialist $193.00
Urgent Care Clinic 85 $161.00
Emergency Room 6 $1,456.00
No treatment 13 $0.00
Total ConsurtaUons 147
azithromycin 250 mg oral tablet
Augmentln 875 mg-125 mg oral tablet
Macrobld macrocrystals-monohydrate 100 mg oral capsule
Amoxlclll!n 400 mg/5 ml oral powder for reconstitution
Rating
#Responses
Poor
$5,418.00
$193.00
$13,685,00
$8,736.00
$0.00
$28,032.00
Total# Consults
#Consults with Rx
#Consults with no Rx
% Consults with Rx
Total# Rx
I Acute sinusitis, unspecified
Acute maxillary sinusitis, unspecified
Acute pharyngitis, unspecified
Acute cystitls without hematuria
Good
0
Excellent 7
147
122
25
83%
159
1.1
Increase utilization by communicating the Te!adoc service to members. Visit http:l/teladoc.mymarketingbench.com/ to download customized member communications.
(c)2016Ieladoc;lnc. =-~ ~-- -- --· ProprletaryandConf\den\ial : - - :=-..::..._:_ Rage'! of1~ ~

0 - Fresno City Trust PPO Medium Option
TELADOC.
SeptembeL20J 6JTeladoc.Uiilization Report · · .. •• ·. . .~.· · •. ' ·• • · · · · • •. ·.;,
Percentage 0.06% 0.30%
Eligible Uves: All members with access to the service (primaries and dependents)
YTD Primaries 531 25 10 1.88%
YTD Dependents 923 13 4 0.43%
YTD Total Eligible lives 1,454 38 14 0.96% 10
YTD Percentage 2.61% 2.64%
Annualtzed Uhhzation% - _ _ _ - - ~ - -- 3,52%- -- - __ _-_ -
Primary Care Physician 8 $129.00 $774.00 Total# Consults 14
Specialist 0 $193.00 $0.00 # Consults with Rx 9
Urgent Care CHnfc 7 $161.00 $1,127.00 # Consults with no Rx 5
Emergency Room 0 $1.458.00 $0.00 % Consults with Rx 64%
No treatment $0.00 $0.00 Totai#Rx 11
Total Consultations 14 $1,901.00 Avg # Rx Per Consult 0.8
Bactrim OS 800 mg-160 mg oral tablet Acute maxillary sinusitis, unspecified
Amoxlclllfn 400 mg/5 mL oral powder for reconstitution Acute cystitis without hematuria
amoxicillin 500 mg oral capsule Acute follicular conjunctivitis, left eye
Augmentln amoxlcl11Jn-clavulanale 500 mg-125 mg oral tablet Acute gastritis without bleeding
C!lndamyc!n Hydrochloride 150 mg oral capsule Acute nasopharyngitis [common cold]
Increase utilization by communicating the Teladoc service to members. Visit http:lfleladoc.mymarketingbench.com/ to download customized member communications.

0 - Fresno City Trust PPO Low Option
TELADOC.
Dependents 2
Total Eligible lives 60 3 5.00% 4
Percentage 1.67% 16.67%
Eligible lives: All members \'lith access to the service (primaries and dependents)
YTD Primaries 108 2 4 3.70%
YTD Dependents 168 2 2 1.19%
YTD Total Eligible lives 276 4 6 2.17% 7
YTD Percentage 1.45% 5.56%
Arinuahzed Uliltzatton% ~- =- __ : _- -- - _ -_ _ 7.41% - -_ _ __ - :=
Primary Care Physician $129.00 $129.00 Total# Consults 6
Specialist 0 $193.00 $0.00 #Consults with Rx 5
Urgent Care Clinic 5 $161.00 $805,00 #Consults with no Rx
Emergency Room 0 $1,456.00 $0.00 % Consults with Rx 83%
No treatment 0 $0.00 $0.00 Totai#Rx 5
Total Consultations 6 $934.00 Avg # Rx Per Consult 0.8
Bactrim OS 800 mg-160 mg oral tablet Ac suppr otitis media wfo spon rupl ear drum, recur, I ear
Azlthromycln 3 Day Dose Pack 500 mg oral tablet Acute atopic conjuncllvitls, left eye
Benzonatate 200 mg oral capsule Acute bronchitis, unspecified
Zithromax Z-Pak 250 mg oral tablet Acute cystitis without hematuria
Acute maxillary sinusitis, unspecified
Increase utilization by communicating the Te!adoc service to members, Visit http://teladoc.mymarketingbench,com/ to download customized member commun!caUons,

PNEUMOVAX VACCINE ADMINISTRATION PROGRAM AGREEMENT
This agreement ("Agreement") is entered into by and between FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST (TRUST) and Rite Aid Hdqtrs. Corp. (RITE AID), which hereinafter may be referred to individually as "PARTY" or collectively as "the PARTIES", to be effective from August 22,2016.
!.RITE AID RESPONSIBILITIES
A. RITE AID will provide pneumovax with influenza vaccine ("flu shot") to eligible members of the TRUST ("Services"). The Services will be provided by authorized pharmacists who have been certified under the RITE AID Immunization Program, and in accordance with indications and contraindications recommended in current guidelines from the Advisory Committee on Immunization Practices (ACIP) of the U.S. Centers for Disease Control & Prevention (CDC), the FDA, or other competent authorities, as applicable.
B. In providing the Services, RITE AID agrees to comply with all applicable State and Federal law including all applicable Medicare laws, regulations and Center for Medicare and Medicaid Services (CMS) instructions.
II. TRUST RESPONSIBILITIES
A. TRUST agrees to pay RITE AID for the Services that it renders to members in accordance with Section III below.
III.BILLING AND COMPENSATION
A. BUSINESS agrees to pay and RITE AID shall bill [one hundred dollars and zero cents ($100.00)] for each Pneumovax shot provided to an eligible member of the BUSINESS. This billed amount shall include the costs associated with the Pneumovax shot and the administration fee. RITE AID can provide billing to the BUSINESS either by mail or electronically. BUSINESS will be responsible for paying RITE AID for all claims within thirty (30) days of receipt of the claim by the BUSINESS.
IV.TERM AND TERMINATION
This Agreement will terminate on April 30, 20 17. This Agreement may be terminated earlier upon: (i) sixty (60) business days advanced written notice from either PARTY; (ii) thirty (30) business days written notice upon default or breach by either PARTY of any provision of this Agreement which is not cured within the thirty (30) business day time period by the other PARTY; or (iii) insolvency or the filing of any bankruptcy proceedings by or on behalf of either PARTY, or an assignment for the benefit of creditors or the appointment of a receiver.

V.NOTICES
All notices relating to this Agreement shall be in writing; postage prepaid, and shall be sent by Certified Mail return receipt requested, to one of the addresses below.
NOTICE TO RITE AID RITE AID 30 Hunter Lane Camp Hill, PA 17011
VI. GOVERNING LAW
NOTICE TO FUND ADMINISTRATOR: FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
~~~_i~ ~~40~~~~~ ~ ~; 7 ;]_ J
This Agreement shall be construed and enforced in accordance with the laws of the State of Delaware. Any disputes between the parties shall be exclusively venued in the Delaware Court of Common Pleas for Kent County, Delaware.
IN WITNESS WHEREOF, the PARTIES hereto have caused this Agreement to be executed as of the date set forth herein by their duly authorized officers.
August 22.2016 Date
FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
Signature
Nameffitle
August 22. 2016 Date
2

RITE AID
Signature
Michelle Tenerelli Clinical Director
August 22. 20 16 Date
3

INFLUENZA VACCINE ADMINISTRATION PROGRAM AGREEMENT
This agreement ("Agreement") is entered into by and between FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST (TRUST) and Rite Aid Hdqtrs. Corp. (RITE AID), which hereinafter may be referred to individually as "PARTY" or collectively as "the PARTIES", to be effective from August 22, 2016.
I. RITE AID RESPONSIBILITIES
A. RITE AID will provide immunizations with influenza vaccine ("flu shot") to eligible members of the TRUST ("Services"). The Services will be provided by authorized pharmacists who have been certified under the RITE AID Immunization Program, and in accordance with indications and contraindications recommended in current guidelines from the Advisory Committee on Immunization Practices (ACIP) of the U.S. Centers for Disease Control & Prevention (CDC), the FDA, or other competent authorities, as applicable.
B. In providing the Services, RITE AID agrees to comply with all applicable State and Federal law including all applicable Medicare laws, regulations and Center for Medicare and Medicaid Services (CMS) instructions.
II. TRUST RESPONSIBILITIES
A. TRUST agrees to pay RITE AID for the Services that it renders to members in accordance with Section III below.
III. BILLING A NO COMPENSATION
A. TRUST agrees to pay and RITE AID shall bill [twenty dollars and zero cents ($20.00)] for each standard trivalent flu shot provided to an active city employees, retirees and dependents of the TRUST. This billed amount shall include the costs associated with the flu shot and the administration fee. RITE AID can provide billing to the TRUST either by mail or electronically. TRUST will be responsible for paying RITE AID for all claims within thirty (30) days of receipt of the claim by the TRUST.
IV. TERM AND TERMINATION
This Agreement will terminate on April 30, 2017. This Agreement may be terminated earlier upon: (i) sixty (60) business days advanced written notice from either PARTY; (ii) thirty (30) business days written notice upon default or breach by either PARTY of any provision of this Agreement which is not cured within the thirty (30) business day time period by the other PARTY; or (iii) insolvency or the filing of any bankruptcy proceedings by or on behalf of either PARTY, or an assignment for the benefit of creditors or the appointment of a receiver.

V.NOTICES
All notices relating to this Agreement shall be in writing; postage prepaid, and shall be sent by Certified Mail return receipt requested, to one of the addresses below.
NOTICE TO RITE AID RITE AID 30 Hunter Lane Camp Hill, PA 17011
VI. GOVERNING LAW
NOTICE TO FUND ADMINISTRATOR: FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST J+S Vintage Park tP:J.I SI'JN'l:7'! F<! ~oster City, C" 94404 ;::::yt_{.::S./1./.r.! c.-A c; 3 7 2 )
'
This Agreement shall be construed and enforced in accordance with the laws of the State of Delaware. Any disputes between the parties shall be exclusively venued in the Delaware Cou1t of Common Pleas for Kent County, Delaware.
IN WITNESS WHEREOF, the PARTIES hereto have caused this Agreement to be executed as of the date set forth herein by their duly authorized officers.
tff ftdrV /I-Om;/1..-t_sFrrr"?:?H- ~/J/M~y Name/Title
August 22, 2016 Date
FRESNO CITY EMPLOYEES HEALTH & WELFARE TRUST
Signature
Name/Title
August 22,2016 Date
2

RITE AID
Signature
Michelle Tenerelli Clinical Director
August 22. 2016 Date
3

BerkeleyWellness.com $5.00 1 Volume 33 'Issue 3'
News and expert advice from the School of
!11 The flu vaccine helps protect people with diabetes from cardiovascular disease and premature mortality, concludes a new study in the Canadian Medical Association Journal, which analyzed the medical records of nearly 125,000 people with type 2 diabetes in England over a seven-year period. People who were vaccinated were significantly less likely to be admitted to the hospital for strokes, heart failure, pneumonia, or influenza and 24 percent less likely to die from any cause.
ru Relatively few people over 65 use digital technology for health matters, according to a recent research letter in the Journal of the American Medical Association. Using a sampling of 7,600 people (average age 75) from a large ongoing survey of Medicare beneficiaries, re~ searchers found that while three-quarters of them used cell phones and two~thirds used computers as of2014, only 16 percent used dig~ ita! technology to access health Information. Even fewer used digital devices to fill prescrip~ tions, contact health care providers, or handle insurance matters, with only modest increases between 2011 and 2014 (though the numbers have undoubtedly increased since then).
~Free meals given by pharmaceutical companies to physicians influence their prescribing behavior, according to a study in lAMA Internal Medicine. Comparing data from the government's Open Payments Program to Medicare prescribing data for 280,000 physicians, researchers found that those who received even a single inexpensive meal (under $20, on average) were 20 to 120 percent more likely to prescribe the promoted brand-name drug over a cheaper alternative. Prescribing rates increased with the number of meals received and with pricier meals. The findings reflect an association and not necessarily causality. But as the researchers wrote, if such .meals "change physicians' prescribing practices as a result of promotional influence, either by en~ couraging future use or rewarding an ongoing preference for the promoted drug, this would be cause for concern." You can find out about your doctors at CMS.gov/OpenPayments.
Brave new world of telemedidne The doctor will (vlrtu~lly) see you now
How do you fit that long-delayed appointment with
your doctor into your jam-packed schedule? T elemedicine (also called telehealth, e-health, or virtual health care) may be the answer. Spoiler alert: vVe
11!1 Similarly, if you have diabetes, you can monitor your blood sugar levels at home and upload the results to your doctor's computer. If there is a problem, the office would be able to call you in for care.
haven't figured out how to '---------~~ m After surgery, you can
check with your doctor remotely for follow-up care. teleport you into medical offices yet, but
telemedicine technologies can connect you and a health care provider in cyberspace. This rapidly growing adjunct to the practice of medicine-which involves connecting to a ulive11 health care provider via vldeoconference, phone, web chat, or wearable devices-is expanding and may soon redefine modern health care.
An estimated 1.25 million people participated in online medical consultations in the U.S. in 2015, according to the American Telemedicine Association. Here are some ways it is currently being used:
~ If you have a minor condition such as a cold, pinkeye, stomach upset, fever, sinus infection, or twisted ankle, an online doctor can diagnose and treat you. It's not for emergency situations such as trouble breathing, choking, severe pain, or a suspected heart attack or stroke.
lll If you have a rash, you can send a digital image, along with your medical history, to a doctor who will review it, give you a diagnosis, and prescribe medication if needed.
ff! If you have hypertension, you can wear a monitor that tracks your blood pressure and transmits the readings to your electronic medical record, allowing your doctor to track your progress.
!!l If you have a condition that could benefit from the expertise of a specialist, you (or your regular health care provider) can connect in cyberspace to get a second opinion or more advanced care.
Virtual pros and (ons Telemedicine can save time traveling and sitting in a waiting room. You don't have to wait days or weeks to get an appointment. It can be of great service in rural areas where there is a severe shortage of doctors, particularly specialists, as well as for people in the military, in prisons, and in colleges.
What's more, it can save money: Doctors usually charge far less for a telemedicine consultation than for an in-person visit. Still, experts will have to keep an eye on the economics of telemedicine, since it may have unpredicted financial consequences.
Telemedicine is not withoue controversy, however. There's concern about the safety of diagnosing conditions and prescribing drugs without in-person, hands-on examinations. Can a health care provider really evaluate what patients need ovei' a video link? Subtle yet important signs dis-
continued on next page
Sodium targets I Prostate cancer CJ Seaweed :1 Cupping :J Microwave popcorn

continued from previous page played by patients may be difficult to assess remotely. Telemedicine could also depersonalize and further fragment health care, which has traditionally relied on office visits, during which the patient and health care provider get to know each other, develop a trusting relationship, and ensure continuity of care. Then there are technology issues (you need access to computers, for instance, and good connectivity). And, of course> some medical conditions will always require an in-office visit.
What's ahead? The American Telemedicine Association anticipates the rise of virtual medical centers> which would benefit Americans as well as people .in other countries by providing consultations with medical professionals; some offer interactive medical tools and allow people with similar conditions to connect with one another.
As noted in a recent review article in the New England journal of lvfedicine (NE]lvf}, Canada and some other countries ;vith single-payer health systems have been early adopters of telemedicine pro-
In recent years, many studies have compared telemedical interventions to standard care, with inconsistent findings. Two studies earlier this year addressed the quality~of-care issue.
In one study from UC San Francisco and Harvard, published in JAMA Internal Medicine in May, 67 people posed as patients using eight virtual visit websites, presenting with symptoms of common acute conditions, including a sore throat, sinusitis, twisted ankle, low back pain, and urinary tract infection (UTI). The researchers then compared the care the "patientsn received to professional treatment guidelines.
On average, accuracy of internet-based diagnoses ranged from 71 percent for sinusitis to 91 percent for UTls, but with wide variations seen among the companies. Also problematic were the testing and treatment recommendations. The virtual doctors didn't send enough pa,tients for urine cultures for suspected UTis, for example, and many didn't refer patients with ankle pain for X-rays when such Imaging was warranted. The virtual doctors also
grams. So far, in the U.S., 29 states require private insurers to cover telemedicine services just as they cover in-person care. In particular, organizations that integrate the financing and delivery of health care-such as Kaiser Permanente, the Department of Defense, and the VA system-encourage the use of telemedicine as a way to both improve the delivery of health care and reduce costs.
1\tlany insurers are eager to get on board, and the projected numbers of telemedicine users are impressive. United Healthcare, the largest health insurer in the U.S., has established a partnership with telemedicine companies and by the end of this year it expects that millions of its enrollees will be able to use smartphones to consult health care providers. Kaiser Permanente of Northern California predicts that it will have more virtual visits than in-person visits this year. By 2020, the Mayo Clinic plans to serve 200 million patients from around the world, most of them remotely.
Nearly all state Medicaid programs cover at least some telemedicine services. In contrast, Medicare lags behind, generally
prescribed antibiotics for viral sore throats and sinusitis nearly half the time, which goes against treatment guidelines.
Of course, many of the problems notedsuch as the inappropriate prescribing of antibiotics-also happen with face-to-face doctors' visits and at emergency rooms.
Another study, published online in JAMA Dermatology in May, looked into teledermatology, with researchers posing as patients and submitting their cases {with stock photos) of various skin conditions at 16 websites servicing people in California. Many shortcomings were noted, including failure to obtain complete medical histories, missed diagnoses (for such conditions as eczema caused by herpes and polycystic ovarian syndrome with inflammatory acne), inappropriate treatments (including prescribing psoriasis medication for a secondary syphilis rash), lack of disclosure about possible- side effects of prescribed drugs, and lack of follow-up care coordination. In some cases, diagnoses were made without requesting photos. Some websltes used foreign-based doctors who weren't licensed in California.
2 November 2016 University of California, BerkeleyWellness Letter
reimbursing for telemedidne only in areas \vith a shortage of medical professionals. And legal barriers, including state licensing of doctors and liability issues, limit the growth of telemedicine. For instance, most states require doctors to be licensed in the state where patients are located when medical services are provided.
What's more, a few states are regulating telemedicine in ways that create roadblocks for patients. Texas, for example, passed a law that sided with doctors' organizations over a telemedicine company in requiring virtual doctors to first have an initial face-to-face visit with patients. This may sound reasonable, but it will limit access to a convenient and affordable health care option at a time when demand is surging. And Iowa has banned remote prescribing of abortion pills, which has more to do ;vith politics than good patient care.
"Perhaps the biggest limitation of telehealth is social," according to the NE]lvl review article. "The digital divide, the differential access to telecommunications technologies on the basis of geographic and social factors, is a major barrier to the adoption of telehealth."The same groups that have limited access to in-person health care-especially the poor and less educated-are least likely to have Internet access and digital devices. But with the expected narrmving of the digital divide in the future and the ubiquity of ever-smarter digital devices, telemedicine holds the promise of overcoming the ((profound social and geographic inequities" of U.S. health care, with ((profound implications for health care delivery and medicine," the review concluded.
BOTTOM LINE: Get medical care in person whenever possible-and certainly for emergencies. But if you can't be physically present due to distance, work commitments> or other im,Pediments, you might consider a telemedical option. Discuss the options with your primary health care provider, and check with your insurance plan to see if you are covered. If you make a connection, make sure to get a record of the visit and follow up with any recommended testing or other instructions. . Next month we'll discuss another relatively new way to deliver medical care: walkin clinics at major dmgstore chains and retall stores like Walmart. Are they any good?

---------------!~ Cut sodium, save half a million lives? tha~;:~l~i~:h~h~~;downonsaltactually
I nJune, the FDA released draft guidelines that set voluntary targets for food companies and chain restaurants to grad
ually reduce sodium in their products over the next decade. The Dietary Guidelines for Americans, along with most medical and public health organizations, recommend a dally limit of 2,300 milligrams of sodium a day (the amount in a teaspoon of salt). But the average American consumes nearly 50 percent more than that-about 3,400 milligrams a day. Here are some facts:
dation in August. That is, research clearly shows that when people reduce sodium, blood pressure drops, on average-especially in those who aheady have elevated blood pressure or are ''salt-sensitive" (meaning that their blood pressure is more responsive to sodium intake). One in three Americans has high blood pressure, which is a major contributor to heart disease and stroke.
change their taste preference, so consumers will get used to lower sodiwn levels in their favorite foods.
1!1 Different brands of the same food contain very different sodium levels, and the same brand sold in different countries may be formulated with widely varying sodiwn content. So, clearly, it's feasible for companies to reduce sodium. Some major companies have aheady started to use less sodium.
Iii About 75 percent of U.S. sodium intake comes from processed or commercially prepared foods, not the salt shaker, which is why the guidelines are important.
m "There is incontrovertible evidence of a direct, dose-response relationship between sodium and blood pressure," according to Dr. Tom Frieden, director of the CDC, writing in the journal of the American Medical Asso-
Ill Reducing average sodium intake by just 400 milligrams a day could prevent 32,000 heart attacks and 20,000 strokes every year in the U.S., according to estimates cited by Dr. Frieden. Lowering sodium by 1,200 milligrams a day (that is, to just below the recommended maximum) would reduce the number of Americans with hypertension by nearly 11 million. This could prevent as many as half a million premature deaths over a decade and save nearly $100 billion in health care costs, researchers have estimated.
Ill The U.K. shows it can be done. It set voluntary sodium targets in 2003, and by 2011 average intake dropped by 560 milligrams (15 percent),leading to a modest but clinically significant reduction in average blood pressure. At the same time, deaths from heart attacks and strokes fell by 40 percent, and salt reduction is likely to have played a role in this improvement, according to a study in EM] Open in 2014.
For advice about how to kick the salt habit, see tinyurl.com/sodiurn WL.
John Swartzberg, M.D. Chafr, Edftorfaf Board
Prostate cancer scare The debate about PSA screening for prostate cancer re-erupted this past summer. That's when a sketchy study by researchers from Northwestern University in Chicago showed that the Dincidence"' of metastatic prostate cancer rose significantly during the past decade and suggested this was due, at least
in large part, to recommendations against PSA screening by the influential U.S. Preventive Services Task Force in 2012.
The study got widespread news coverage, which often echoed the university's press release (alarmingly headlined "Metastatic Prostate Cancer Cases Skyrocket") and its singling out of "lax screening" as a likely culprit for this delay in diagnosis until cancers had already spread. This was the smoking gun some PSA proponents were undoubtedly looking for-"'proving"' that the Task Force's anti-screening guidance would lead to more advanced cancers and thus more deaths.
If you stopped having routine PSA blood testing after the Task Force advised against it, you may have shuddered when you read this news. But the study did not prove anything. It looked at a cancer data~ base of patients from 1,089 facilities nationwide and, yes, it found that cases of metastatic prostate cancer rose 70 percent between 2004 and 2013 {low-risk cancers declined and intermediate- and high-risk cancers remained fairly stable). Yet these numbers mean little without knowing the size of the overall pool of men each year, which was not provided. "Incidence" is the rate of occurrence per a specific number of people (usually 10,000 or 1 00,000) over a period of time. There's no "per" here.
There are many reasons why these raw numbers may be rising-a growing and aging population, improved ability to diagnose metastatic cancer early on, or even an increase in the aggressiveness of
prostate cancers, for unknown reasons. Other databases have not found an increase in the incidence of metastatic prostate cancer, though we don't yet have published data for the past couple of years. And I've seen no indication that deaths from prostate cancer have been rising, after years of steady declines. That would be an unmistakable warning sign.
In any case, it makes no sense to blame the Task Force for the uptick In advanced prostate cancer suggested by this study. In its 2002 and 2008 guidelines, the Task Force said there was insufficient evidence to recommend for or against routine PSA screening. It wasn't until mid-2012 that it recommended against screening, concluding that the risks of overdetection and overtreatment outweighed the benefits, which were still unclear. That probably led to decreased screening-but years after the increase in advanced cancers reported in the new study. What's more, any uptick will probably take at least five years to become apparent, and even longer for mortality rates to rise, if that happens.
PSA screening remains an open question. It still is not clear how many lives it saves. The Task Force has been attacked for its interpretation of the two major clinical trials upon which it largely based its guidance. It is now re-evaluating the research for its next set of guidelines, expected in 2018. At the same time, experts are trying to find ways to maximize the benefits of screening with PSA and other tools while minimizing its harms by, for instance, not treating "low-risk" cancers and using a "watchful waiting" approach {also ca11ed active surveillance) more often.
Meanwhile, I agree with the American Cancer Society {ACS) that the choice of whether to be screened is up to each individual man, who should discuss the potential benefits, harms, and uncertainties with his doctor. Good places to start are the ACS decision guides {tinyurl.com/prostateACS), as well as our article about the Task Force's recommendations (tinyurl.com/prostateWL).
We'll keep you informed as the PSA picture becomes clearer.
BerkeleyWellness.com November 2016 3

The other seafood
Seaweed is a regular feature in Asian cuisine, where ies wrapped around sushi, added to soup, and eaten
with vinegar as a "salad." Though not a staple of the American diet, it's being hailed as the "new kale''-used as a condiment and sandwich topping, blended into smoothies and salad dressings, and fashioned into noodles and "chips/'
There are thousands of varieties, but only a few dozen are typically consumed, notably the brown seaweeds wakame and kombu (kelp) and the red seaweeds nori and dulse. Here's a look at the merits (and possible demerits) of seaweed, also called sea vegetables and referred to as macroalgae by scientists.
A pool of nutrients Whether "weeds" or "vegetables/' seaweed is a source of vitamins (including B12, C, D, E, K), minerals (calcium, magnesium, potassium, copper, iodine, iron), carotenoids and other antioxidants, and protein (red seaweeds tend to have the most). Many types provide some omega-3 fatslong-chain DHA and EPA (as found in fatty fish) as well as shorter-chain alphalinolenic acid (found in plant foods such as flaxseeds). Seaweed also contains agar, carrageenan, and other polysaccharides that are good sources of soluble fiber.
People in Asia and other countries who
regularly consume seaweed may get significant amounts of nutrients, fiber, and
other potentially beneficial com-pounds from these sea vegeta
bles. Interestingly, a 2010 study in Nature found that
Japanese people harbor bac-teria in their intestines that
specifically break down algal carbo-hydrates. But the nutritional content
of seaweed is irrelevant for most Americans, who usually eat only small portions on occasion and do not seem to have these seaweed-digesting microbes.
A tsunami of medicinal uses The medicinal use of seaweed dates back thousands of years. Traditional Chinese medicine has relied on it as a treatment for everything from goiter to urinary tract infections. And the ancient Egyptian medical text known as the Ebers Papyrus cites it as a remedy for tumors. Today, lab studies have identified antiviral, anti-cancer, antiinflammatory, and other properties of seaweed, while some small studies in people have linked it to reduced triglycerides, higher HDL ("good") cholesterol, and improved blood sugar control. Some preliminary evidence suggests that the relatively high consumption of seaweed by Asian women may help explain their lower rates of breast cancer.
Seaweed has also been proposed as a potential obesity treatment, due to its alginate, a type of fiber that may block absorp-
Junk on the road
You know what causes car crashesdrunk drivers, distracted drivers, icy road conditions, and so on. But
what about debris on the road? More than 200,000 police-reported crashes involving debris on the road occurred in the U.S. between 2011 and 2014, resulting in 39,000 injuries and 500 deaths, according to a new study by the AAA Foundation for Traffic Safety. Such crashes have increased 40 percent since 2001.
Why do these accidents occur? Because many drivers don't secure the loads their cars or trucks are carrying or don't maintain their
vehicles properly, allowing parts (such as exhaust pipes or fenders) to fall off while they are driving. Here are some statistics:
IJ More than one-third of these deaths occur when drivers swerve to avoid hitting the debris on the road. That causes them to lose control of the car or hit another vehicle.
ill More than one-third of debrisrelated crashes happen between 10 a.m. and 4 p.m., when more people are hauling stuff.
["11\llost of these crashes occur on interstate highways, since driving at high speed increases the chance that cargo will fall off vehicles or that parts will become detached,
4 November 2016 University of California, BerkeleyWellness Letter
tion of fat in the digestive tract. Alginate may help heartburn, too-which is why it's in over-the-counter antacids such as Gaviscon.
A sea of caution Seaweed readily absorbs and stores whatever is in the water, just as fish and shellfish do. If the water is polluted with arsenic, mercury, lead, cadmium, or other heavy metals, the seaweed will contain traces of these contaminants. To be on the safe side, don't go overboard, vary the types or brands, and avoid hijiki, which has been shown to have the highest arsenic levels among seaweed. Red seaweeds are safer options. Most U.S.-based companies that harvest seaweed regularly test their seaweed for arsenic and other heavy metals, as well as bacteria, PCBs, pesticides, and radiation. Two such companies are Rising Tide Sea Vegetables and Maine Coast Sea Vegetables.
BOTTOM LINE: Seaweed is an oftenoverlooked but flavorful food that can spruce up soups, salads, stir-fries, fish, rice, vegetables, and even popcorn. To get a significant amount of nutrients or any possible health benefits, however, you would need to eat it regularly. Seaweed is high in vitamin K (involved in blood clotting) and iodine (needed for maldng thyroid hormones), so if you take a blood thinner or have a thyroid condition, talk to your doctor before consuming seaweed products. Be aware also that, depending on the variety, seaweed can be high in sodium (raw wakame has about 90 milligrams per tablespoon).
Three safe moves m Maintain your vehicle. Get it checked
by a trained mechanic. Replace worn tires so they don't blow out and launch pieces at other vehicles and leave debris on the road.
!J When moving furniture or equipment, secure it properly using rope, netting, or straps. Don't overload.
ill Keep an eye on the road as far ahead as possible, and leave enough space between you and the vehicle ahead so you can steer around any debris on the road. As much as possible, make sure there's open space on at least one side of vour car, so you can swerve g
J ~ if necessary. ::

Glucosamine: yes, no, maybe? amine/chondroitin did not appear to reduce symptoms or delay disease progression."
Millions of Americans with osteoarthritis take glucosamine, often with chondroitin sulfate, making
these two of the top-selling dietary supplements. Produced in the human body, these substances are involved in the production and maintenance of the cartilage that cushions joints, and it has been theorized that supplemental doses may slow or prevent the deterioration of cartilage that causes the most common form of arthritis and thus reduce pain and stiffness. The supplement glucosamine is usually made from shrimp or crab shells; chondroitin, usually from cow or pig cartilage.
But do these supplements really work? A decade ago, the findings of a landmark study threw cold water on the claims, but research has continued.
GAIT casts a big shadow In 2006, the Glucosamine/chondroitin Arthritis Intervention Trial (GAIT) was published. This was a large, well-designed, $12-million government-sponsored clinical trial-a rarity in the field of dietary supplements. Nearly 1,600 people with osteoarthritis of the knee were randomly assigned to receive one of five treatments daily for 24 weeks: glucosarnine hydrochloride alone, chondroitin sulfate alone, glucosamine and chondroitin combined, celecoxib (a prescription drug approved for arthritis pain), or a placebo (dummy pill).
Overall, neither glucosamine nor chondroitin, alone or in combination, reduced pain and other symptoms significantly better than the placebo. One surprising finding: The placebo provided relief of symptoms in 60 percent of people-double the expected placebo effect. Celecoxib did only modestly better; helping 70 percent of users.
The one positive result was that in the subset of participants with moderate to severe symptoms, 79 percent who took both supplements (not either one alone) reported significant relief, versus 54 percent who took the placebo. But because this group was small Qust 70 people) and subgroup analyses can be misleading, the researchers said this finding was only "preliminary" and 1'exploratory" and needed to be confirmed by additional studies. Still, the supplement industry often touts this secondary finding, usually without
mentioning the nearly-as-good response among the placebo takers.
What about the claim that these supplements slow or prevent the deterioration of joint-cushioning cartilage that is the hallmark of arthritis? In a 2008 follow-up GAIT study, participants continued treatment for an extra 18 months and had X-ray exams (befure and after) to measure their cartilage. There were no significant differences in cartilage loss between the groups. Interestingly, glucosamine and chondroitin did worse when taken together than each alone, but nothing worked much better than the placebo.
Research machine keeps running Since GAIT, dozens of additional studies of glucosamine, often with chondroitin, have been done. Here's a sampling, focusing on well-designed research:
1!1 In 2008, a Dutch study of222 people with arthritis of the hip found that glucosamine sulfate, another form, did not reduce pain or stiffness better than a placebo, and X -rays revealed no differences.
!lJ Also in 2010, longer-term findings from GAIT confirmed that glucosamine and chondroitin, taken singly or together for two years, were no better than a placebo at reducing pain.
l'il Later in 2010, a European metaanalysis also found that glucosamine and chondroitin, individually or in combination, worked no better than a placebo in reducing joint pain or joint space narrowing (that is, cartilage loss). In light of this and other research, the American College of Rheumatology, in its 2012 guidelines, recommended against glucosamine and chondroitin.
!!1 In 2014, a 24-week study from the University of Arizona found that glucosamine hydrochloride did not reduce knee cartilage damage (as seen in MRis), relieve pain, or improve function better than a placebo in people with osteoarthritis of the knee.
!11 Also in 2014, an Australian study found that glucosarnine sulfate and/or chondroitin sulfate did not reduce arthritic knee pain more than a placebo over a two-year period, but that the combination may reduce joint space narrowing.
!l In 2015, an analysis of data from the long-term Osteoarthritis Initiative found that "three years of treatment with glucos-
Ill In 2016, a large European clinical trial in the Annals of Rheumatic Diseases found that glucosamine hydrochloride combined with chondroitin, taken for sLx months, was as effective as celecoxib in reducing pain, stiffness, fi.mctionallimitation, and joint swelling in people with osteoarthritis of the knee. The treatments were not compared to a placebo, however.
Ill The newest study, a Spanish clinical trial in Arthritis & Rheumatology, found that glucosarnine sulfate plus chondroitin sulfate worked no better than a placebo in reducing pain or improving physical function over six months in people with knee osteoarthritis.
Adverse effects: No serious side effects were reported in these studies. However, a small study reported in]AMA Ophthalmology in 2013 linked glucosamine supplements with increased intraocular pressure in people with glaucoma and suggested that this "deserves further exploration." And people with shellfish allergy may have reactions to glucosamine made from shells.
Words to the wise Americans spend billions of dollars every year on unproven arthritis remedies. Everything seems to work for a while, at least in some people, largely because there's such a strong placebo effect when it comes to pain. lVIoreover, arthritis pain waxes and wanes, and we tend to blame or credit whatever we are trying at the time. Anti-inflammatory pain relievers help many arthritis sufferers but don't affect the underlying loss of cartilage.
We don't recommend glucosamine and chondroitin~unless you're willing to pay $20 to $30 or so a month for what is probably a placebo effect. If you already take these supplements and find they help, continue with them, but consider stopping for a while to see if there's a difference.
Before taking any supplement for joint pain, consult your doctor for a diagnosis. The pain may be caused by rheumatoid arthritis (an autoimmune disorder), gout, or another condition for which there's no reason to think these supplements could help.
If you have osteoarthritis, we can't overemphasize the importance oflosing weight if you are overweight, and exercising to maintain strength and flexibility. Both steps can help relieve pain and restore mobility.
------- ----~,~--
BerkeleyWellness.com November 2016 5

The cupping craze: long in history, short on science If you watched the Summer Olympics in Rio
this past August, you undoubtedly saw quite a few high-profile athletes-most famously Michael
Phelps-sporting large purple circles on their backs, shoulders, and other body parts, the result of"cupping." We have since received letters from readers asking if this treatment really has healing power and improves sports performance. Obviously some Olympians {and many other people) think it does-but the evidence behind it is dubious.
Though there are several ways to do it, cupping involves creating a suction effect on the skin through the use of special cups {usually made of glass but sometimes plastic, rubber, clay, or bamboo) that are placed on the targeted area. This is said to promote circulation and draw out "stagnant" toxIns and other harmful substances, and relieve musculoskeletal pain, among other supposed benefits. One way to create the suction is by lighting a flame {such as of an alcohol-doused piece of cotton) in the cup, and then, as the flame goes out, quickly placing the Inverted cup on the skin. Another method involves vacuuming out the air in the cup with a pump. In wet (blood) cupping, the skin is pricked first. Typically, about 5 to 8 cups (or sometimes m·ore), ranging from 1 to 2 inches in size, are applied and left on the skin for anywhere from 5 to 15 minutes.
A part of traditional Chinese medicine for thousands of years, cupping Is increasingly used by acupuncturists, physical therapists, massage therapists, athletic trainers, and other health care practitioners in the West. it was reportedly done originally to draw out poisons from insect bites and to drain wounds, but now it's touted as a seeming cure-all. For instance, the International Cupping Therapy Association maintains that "a huge number of conditions respond positively to cupping"-from asthma, colds, digestive disorders, and jaw pain (temporomandibular joint disorders) to menopause symptoms, cellulite, and vertigo. Athletes say it enhances muscle endurance and agility, prevents injuries, and speeds recovery from muscle fatigue.
Several study reviews have attempted to evaluate the effects of cupping, particularly for such conditions as low back pain, knee arthritis, headaches, and shingles. Some of the findings seem positive. For instance, a review of 16 trials, published in the Journal of
Traditional Chinese Medical Sciences in 2014, found "at least moderate evidence that cupping is more efficacious than no treatment or other treatments (such as heat therapy, usual care, and conventional medications) in reducing pain over the short term."
But as with acupuncture and many other alternative therapies, the studies overall are of poor quality and have had mixed results. Among the many problems, most studies don't include proper control groups and thus cannot rule out a placebo effect. And when there Is a placebo comparison group, participants and practitioners cannot easily be "blindedn {that is, they may know who is receiving the real treatment, which can bias the
results}. Some studies combine cupping with other treatments, so it's not known what might have been responsible for the effect, if there was one. Most studies are also small and short term. In fact, the authors of all the reviews reporting positive results repeatedly caution about the inethodological problems and call for more rigorous and longer trials.
There's also no plausible mechanism for how cupping might provide benefits. Some practitioners believe it creates inflammation, which triggers an immune response; others use a form of cupping (massage cupping) as a type of myofascial release or trigger point therapy.
Cupping is considered generally safe, though the suctioning action bursts blood vessels under the skin, which creates the marks. Burns and blisters are also possible if a flame is used. More serious, a case report last year described subdural hematomas (bleeding between the brain and skull) that occurred in a young woman two weeks after she had cupping on her scalp to treat her headachesthough there was no definite proof that cupping was the cause.
BOTTOM LINE: The therapeutic effects of cupping remain controversial, and we remain skeptical of its benefits beyond any placebo effect. There is no scientific support for the idea that cupping helps athletes win (sorry Phelps, though you hardly needed a leg up). Still, it most likely won't hurt to try it if you go to a well-trained practitioner-but cupping should not be done on your scalp or if you have fragile skin or a skin condition like eczema. Insurance generally won't cover it, however, and if it doesn't help, you'll have the telltale marks to remind you of that-for about 10 days or so.
Exercise: medicine for the mind exercise is done in a group). Take that away, as in this study, and active people suffer.
uch research has shown that exercise and staying physically active in general can improve
mood and help counter depression. A study in lvfayo Clinic Proceedings in August provided some interesting evidence for this by examining what happens when active people are denied their exercise boost.
Researchers from the University of lVlississippi recruited 39 young adults, ages 18 to 35, all of whom regularly exercised moderately or vigorously for at least 150 minutes a week before the start of the study. Two-thirds of them were told to stop exer~ cising for a week and to limit walking (the
other third, the control group, continued their normal exercise routine). Before and after the intervention, the participants undetwent psychological evaluation. Even after just seven days, the suddenly sedentary group experienced large adverse effects on mood and depression. Then, after they resumed physical activity for a week, they regained their normal emotional state.
Those results are hardly surprising. Exercise can help improve mood of at least maintain psychological equilibrium in many ways-by reducing stress and an.uety, improving sleep, providing a sense of selfefficacy, and enhancing social support (if
6 November 2016 University of California, Berkeley Wellness Letter
One take-home message, according to the researchers, is that athletes and exercisers who sustain an injury that prevents them from working out should be aware of these "maladaptive effects" ofbecoming sedentary and try to counter them by, for instance, finding another form of physical activity.
More broadly, as the accompanying editorial put it, "Physical activity and reduction of sedentary behavior have a synergistic effect on improving both physical and psychosocial health .... If the benefits of exercise could be distilled into one medication and bottled, it likelywould be the best selling and most prescribed medication in history."

Q I heard that it's better to get the flu shot in the morning. Is that true?
A Possibly, at least according to a recent study published in the journal Vaccine, which found that getting the flu vaccine in the morning may rev up the immune system more than getting vaccinated later in the day. The study, from the University of Birmingham in the U.K., involved almost 300 people, ages 65 and older, half of whom were given the flu vaccine between 9 a.m. and 11 a.m., the other half between 3 p.m. and 5 p.m. A month later, the researchers did blood tests to measure the antibodies produced in response to the vaccine. (It typically takes two weeks to a month for antibody levels to peak.) Antibody levels were significantly higher in the morning group.
The flu shot works by stimulating the immune system to produce antibodies that battle the strains of influenza included in that year's vaccine. The effectiveness of the vaccine depends in part on the age and health of the person getting vaccinated. Various aspects of the immune system decline with age, so anything that could boost the efficacy of the vaccine for older people would be a boon.
This new finding goes along with two studies by the same researchers, published in Psychophysiology in 2008, which found that older men who got the flu shot (as well as young men who got the hepatitis A vaccine} had a better antibody response when vaccinated in the morning than in the afternoon. For unknown reasons, morning vaccination did not improve the immune response of female participants in these older studies.
Like many things in human biology, aspects of the immune system fluctuate during the course of the day. But the clinical significance and practical implications of these daily fluctuations for vaccinations remain
largely unclear. For instance, it's not known if people who get the flu vaccine in the morning are actually less likely to develop the flu than those vaccinated In the afternoon.
Until more definitive studies show that getting the flu vaccine in the morning is more protective, we simply encourage you to get vaccinated at whatever time is convenient. But if you have the choice, opt for morning.
Q Is it true that microwave popcorn contains substances that cause cancer?
A No, but at least one ingredient, when inhaled regularly, can cause lung damagewhat has b~en dubbed 11popcorn lung." The suspect chemical, diacetyl (also known as butanedione) is a natural byproduct of fermentation and is found in low levels in foods such as yogurt, wine, beer, butter, and cheese. But the trouble comes from the synthesized diacetyl added to impart an artificial buttery flavor and smell to popcorn. Diacetyl is also used in some flavored e-cigarettes and is found naturally in tobacco.
Popcorn lung is an irreversible, debilitating, and potentially fatal lung disease. The term was coined when workers in factories producing popcorn (or the flavoring ingredients) developed the respiratory condition, medically known as bronchiolitis obliterans. This inflammatory disease obstructs the small airways of the lung, causing chronic cough and severe shortness of breath.
Most people first heard about popcorn lung when a middle-aged popcorn lover came down with this condition and was awarded $7 million in damages in 2012 in a lawsuit against the manufacturer and retailers. The man reportedly inhaled the buttery vapors from two or three bags of butter-flavored microwave popcorn nearly every day for seven years.
When the Center for Science in the Public
Interest (CSPI) recently contacted major microwave popcorn manufacturers, all claimed they had switched from diacetyl to a similar chemical additive, 2,3-pentanedione. This may also be unsafe when inhaled, at least according to animal data. Neither chemical is named on ingredients lists; they are simply included underuartifidal flavorings:
Microwave popcorn bags may be lined with other potentially harmful chemicals, notably PFOS (perfluorooctane sulfonate). This chemical prevents oil from migrating through the bag and is found not just in microwave popcorn bags but also in some fast-food wrappers, pizza boxes and other food wrappings. Because of safety concerns, including Its hormonal effects and a link to thyroid disease and various cancers, the FDA recently banned PFOS in all food packaging.
The biggest concern with chemicals such as diacetyl and PFOS is for occupational exposure. There's no reason to panic if you eat microwave popcorn occasionally. Still, it's always wise to have good ventilation in your kitchen, since smoke and fumes from cooking contain an array of risky chemicals {see tinyuri.com/ventWL). CSPI recommends allowing a bag of microwave popcorn to cool before opening it-or opening it under a ventilation hood or near an exhaust fan.
To avoid all this, you can pop plain kernels with an air popper, on the stovetop, or in the microwave. If you do buy microwave popcorn, compare labels for calories and sodium, and avoid brands that still have partially h.ydrogenated oils, which contain trans fat.
If you hava a question you would like to see answered In tho Wei/ness Letter, email us at Experts®WellnessLetter.com, Or write to UC Berkeley Wellness Letter, Ask the Ex· parts, Berkeley CA 94720·7360, We regret that we are unable to publish answers to all questions or respond to all letters personally,
•
Editorial Board Vnlvmily of Cellfornla, Dorkoloy
CHAIR Stefano Bertoui, /AD~ Ph.D, Dean, Schoo! of Pubfie Health Marlon Maus, M.O~ D~PJI, F.A.C.S~ M;unct ProfessOf, Pubffc Health John Edwald Swartzbery, M.O~ F.A.C.P. Professor Emeritus, Health and Medical Sciences ASSOCIATE CHAIRS
Edvtard R. BII!Jll, Ph.D. Assistant Cfrico! ProfessOf, C!illical Pharmacy, UCSf Guy MiccCI, M.D. Professor Emeritus, UCB{UCSf Joint Medical Program Cindy J. Chang, M.O .. Associate Clinical Professor, Sports Medicine, UCSF James P. Seward, M.D. M.P .P, Clinical Professor, Pubfic Health Uly Chaput, M.D., M.P.H. UC Davis Medical Center Ki1k R. Smith, Ph.O, Professor, Environmental Health
Jn-{l:e C.lashotM.D., Professor Emerita, Public Hea!th Willia~ A. Pereira, M.O~ M.P.H .. Occupational and Environmental Medicine
Teh-wei Hu, Ph.D. Professor Emeritus, Hea!th Econorr.ks laura E. S!achel, M.D. M.PJI. Instructor, UCB/UCSf Joint Medical Program
Customer S~rvice: Wellness letter, P.O. Box433235, Palm Coast, fl32143-l)235. Email:: Wellnessletter@ema~customerservi£e.com
Editorial correspondence, reprint requests,or bulk· subscription inqu!r!as: Write to Wellness letter, Remedy Health Media, 750Third Avenue, 6th floor, NawYorlc, NY 10017. Email; [email protected]
WL In de~: BerkeleyWelfness.coiTVWellnessletterlndex.
POSTMASTER: Send address changes to Wellness letter, P.O. Box 43323S."Palm Coast, Ft 32143·0235.
Steven Jacohsohn, fo\.0.., Cfuical Professor, Gastroentero!Qgy, UCSf S. leonard Syme, Ph.D, Pmfessor Emeritus, Epidemiology Ronald M.Krauss, M.D~AdiunctProfessor, Nutritional Sciences Dale A Ogar, Managing Editor
Subscription plice {161ssues): U.S~ $49. Canada: $59 plus 13% HST {Canadian funds), HST Number 126230994. Other foreign: $69\U.S. funds). • lfyt~u do notwantyt~ur name passed on to companies for carefully screened mailings that maybe of interest to you, please write to Wel!ness letter, ?.0. Box 433235, Palm Coast, fl32143-0135,or emaiiWetJnasstatter® emailcustome1service.com. • Peliodica!s p<~stage paid at New York, NY, and additional mailing offices. international Publications Mail Agreement#40031451. Canadian retum address: UC BerkelayWellness letter, P.O. Box39, Nor.vich, Ontario NOJ !PO.
U11iversityol California, Berkeley Wet/ness letter (ISSN 0748·9234! is published monthly, plus Spring (March), Summer (June), FoU (September), and Winter (December) issues, by Remedy Health Media,llC, 750 Third Avenue, 6th floor, New York, NY 10017.
Remedy Health Media, UC Michael Cunni on, Chief Executive Officer Rebecca Bauer, Executive Vice President, Editorial David lee, Executive Vice President, Pub~shing Peter Giallorenzo, Chief financial Officer
Michael Go/dma11, Editor Alldrea Klausner, M.S., R.DJI., Senior Editor Tim Jeffs, Art Director Barbara Fa/k,A.ssocfate Consumer Marketing Director
©2016 Remedy Health Media, tlC. All rights reserved. Printed in the United States of America
. This newsleuer Is notiotended to provide medical ; i advice on personal health matters, which should be
l -~~~~~-'!!~-~J.r.~c_t~_!~o~-~-~~Y-~~~!~~·- 1
--------~-~~----~~
BerkeleyWellness.com November 2016 7

Li Beware of unp~:e~~ ~r~:~~;. ~~r~~o~~te~~~~t _h_e_Z-ik_a_v_i-ru_s_. T-h-e
Federal Trade Commission (FTC) recently warned at least 10 online marketers selling products that purportedly protect against Zika that their claims must be supported by well-designed human clinical testing-which was not the case. The products include wristbands, bracelets, patches, and stickers that supposedly repel mosquitoes carrying Zika or otherwise protect users from the virus. l\tlost contain ingredients such as oil of geranium, cedar, soy, and citronella, which provide little protection against mosquitoes. Subsequently, New York's Attorney General issued cease-and-desist letters to seven companies marketing products with false or misleading claims about Zika protection. The only ingredients approved by the EPA as long-lasting mosquito repellents are DEET (preferably 20 to 30 percent), oil oflemon eucalyptus, picaridin (preferably 20 percent), and IR3535. You can also spray clothes (not skin) with permethrin, or wear permethrin-treated garments.
Li If you have chronic sinus congestion, talk to your doctor about nasal irrigation. In a recent study from the U.K. of 871 people with chronic or recurrent sinusitis, published in the journal CMA], those instructed to perform daily nasal irrigation using a neti pot for six months (after brief training and viewing of a short video) reported greater symptom relief and reduced use of over-the-counter medications, compared to those following usual care or those who inhaled steam every day. Nasal irrigation involves pouring a saline solution into one nostril and draining it out the other to flush out accumulated mucus and nasal debris. In preparing the saline solution, it's essential that you use sterile, distilled, or boiled water to avoid potential microbial infection.
@Riding a pedelec (a type of electric bicycle) can provide a good workout, according to a study from the University of Colorado, in the European Journal '!f Applied Physiology. These increasingly popular bikes provide an electric assist only when the rider is actively pedaling (unlike other electric bikes that do all the work for you). In this "real-world" study, 20 people commuted to work at least three days a week (for a minimum of 40 minutes each of those days) on a pedelec, at their own pace. After four weeks, improvements were seen in blood sugar control, aerobic endurance, and power output. Pedelec bikes-which make long and hilly commutes easier on the cyclist~umay especially help older individuals remain active,"the researchers wrote. Some localities, however, ban the use of electric bikes, so check your local laws before purchasing one.
[iZ(' Portion-controlled meals can help dieters lose weight, according to a study of 183 overweight or obese people (ages 25 to 65) in the journal Obesity. All participants received nutrition and behavioral counseling to help them meet a weight-loss goal of at least 5 percent of initial weight. Those who consumed packaged, portion-controlled frozen entrees for lunch and dinner (intervention group) lost more weight over 12 weeks than those in the control group, who ate a self-selected reduced-calorie diet; 74 percent of the portion-control group achieved the weight-loss goal, compared to 53 percent of the control group. Using portion-controlled meals may facilitate weight loss by simplifYing the planning and preparation of meals, the authors concluded. It also teaches dieters about appropriate serving sizes.
@All women who may become pregnant should take a dally supplement of 400 to 800 micrograms of folic acid, not just those who are pregnant or planning to become pregnant, according to the latest recommendation from the U.S. Preventive Services Task Force. This reaffirms the influential group's previous guidelines; nearly all other medical groups advise at least 400 micrograms. Folic acid, the form of the B vitamin folate used for supplements and in fortified foods, gready reduces the risk of neural tube birth defects. The critical period for supplementation starts one month before conception and continues through the first trimester. Since half of all pregnancies are unplanned, all women who are capable of becoming pregnant should take folic acid, just in case. It's hard to get this much folate from food; in addition, folic acid is better absorbed by the body than the folate naturally in food. Most multivitamins contain 400 micrograms of folic acid. ItS estimated that fewer than one-third of women of childbearing age are taking folic acid.
November 2016 University of California, Berkeley Well ness Letter
Joy of dishwasher cooking Americans !ike convenience when it comes to cooking. And dishwasher cooking is among the latest trends. You read that right Fans say it produces tastier and more tender food than traditional cooking methods. Others warn of potential dangers.
Actually, the idea is not new. An article in the Los Angeles Times in 1986 reprinted a recipe for Dishwasher Poached Salmon supposedly datIng back to the 1970s.ln more recent years, the chef David Burke made headlines by cooking turkey in the dishwasher forThanksgiving.
The hot water and steam cook the food, similar in ways to poaching and sous vide cooking (see tinyurl.com/sousvideWL). Foods reportedly cooked with success in the dishwasher include fish, vegetables, eggs, potatoes, couscous, pears-and even lasagna and apple pie. If you're tempted to try it, keep these points in mind:
,. The food must be sealed tightly-for obvious reasons. Though some recipes say to wrap the food In tin foil, it's better to use wellsealed, heat-safe plastic bags or mason jars, which ensures that the food won't get wet (or soapy) and that it is heated more evenly.
~ Dishwasher cooking can save energy, but only if you wash your dirty dishes at the same time-which may not be too appealing, even if the food is properly sealed. Otherwise, running a full cycle just to cook is a waste of energy and water.
rillt can be risky. Depending on your dishwasher's temperature and cycle times, foods may not reach sufficient temperature needed to kill all harmful bacteria. For instance, fish and steaks need to be cooked to 145°F, poultry to 165°F, and eggs to 160<)F. Dishwashers typically reach about 130' to 170'F. You can test how hot yours gets by including a waterfilled glass bottle in the cycle to see what temperature the water reaches. Better yet, use a food thermometer to check that the cooked food has reached a safe internal temperature. Or use the dishwasher only for cooking lowrisk foods like vegetables.
Our advice: Dishwasher cooking is a novel way to prepare meals-and can make for good conversation if you're entertaining. But it's hardly the most practical or timesaving way. Of more concern are the potential dangers. Young children, pregnant women, and anyone who is immunocompromised or in frail health should steer clear of chicken, ground meat, or other higher-risk foods that have been cooked in a dishwasher.
IJf1 Please join us on Face book: ~ Facebook.com/BerkeleyWellness
Activity icons on food labels 'J Peripheral neuropathy ~l DASH vs. gout Fl Food quiz