Embed Size (px)
Citation preview

J. Pathol. 186: 131–139 (1998)
FREQUENT p53 GENE MUTATIONS IN SERRATEDADENOMAS OF THE COLORECTUM
1,2, 1, 3, 2, 1, 2
1*1First Department of Pathology, Hiroshima University School of Medicine, 1-2-3 Kasumi, Minami-ku, Hiroshima 734, Japan2First Department of Internal Medicine, Hiroshima University School of Medicine, 1-2-3 Kasumi, Minami-ku, Hiroshima 734,
Japan3Department of Anatomical Pathology, Hiroshima University School of Medicine, 1-2-3 Kasumi, Minami-ku, Hiroshima 734, Japan
SUMMARY
Serrated adenoma has been recently proposed as a distinct histological lesion of the colorectum. This study examined p53immunoreactivity, mutations of exons 5–8 of the p53 gene, codon 12 of the Ki-ras gene by PCR–SSCP analyses, and microsatelliteinstability in 19 serrated adenomas, ten adenocarcinomas in/with serrated adenomas, 23 hyperplastic nodules, four hyperplastic polypsand 29 tubular adenomas of the colorectum. Eleven of 11 (100 per cent) serrated adenomas had p53 immunoreactivity and all six (100per cent) adenocacinomas in/with serrated adenomas exhibited moderate to severe p53 immunoreactivity. It was confirmed that 9 of 19(47 per cent) serrated adenomas and 5 of 10 (50 per cent) adenocarcinomas in/with serrated adenomas harboured p53 gene mutations.On the other hand, no p53 gene mutation was detected in the other colorectal lesions. Meanwhile, 11 (58 per cent) serrated adenomasand six (60 per cent) adenocarcinomas in/with serrated adenomas had Ki-ras gene mutations, as also did 9 of 23 (39 per cent)hyperplastic nodules, 3 of 4 (75 per cent) hyperplastic polyps, and 12 of 29 (41 per cent) tubular adenomas. Microsatellite instability wasdetected in one (5 per cent) serrated adenoma and one (10 per cent) adenocarcinoma in a serrated adenoma. The other lesions did notshow microsatellite instability. Serrated adenomas had significantly frequent p53 gene mutations compared with hyperplastic lesions ortubular adenomas (p<0·005). On the other hand, they did not exhibit significant differences in mutations of the Ki-ras gene or inmicrosatellite instability. Genetic changes were then examined in small parts of serrated adenomas, such as the upper or lower parts ofcrypts, to determine the extent of gene mutations by using a microdissection technique. Exon 15 of the APC gene and the DCC gene,in addition to the p53 and Ki-ras genes and microsatellite instability, were analysed. Identical mutations of the p53 gene were found inboth invasive adenocarcinomas and adjacent serrated adenomas by direct sequencing, suggesting single clonal origins for those lesions.Mutations of the APC gene and microsatellite instability were heterogeneous in some lesions. No loss of heterozygosity (LOH) of theDCC gene was found. These findings suggest that mutations of the p53 gene are the most characteristic genetic alterations in serratedadenomas, as a relatively early event in a multistep carcinogenic pathway of this type of colorectal lesion, that might be distinctfrom the ordinary adenoma–carcinoma sequence or from carcinogenesis via mutations of mismatch repair genes. ? 1998 John Wiley& Sons, Ltd.
KEY WORDS—serrated adenoma; p53 gene; Ki-ras gene; microsatellite instability; hyperplastic nodule; hyperplastic polyp; tubularadenoma
*Correspondence to: Professor Eiichi Tahara, First Department ofPathology, Hiroshima University School of Medicine, 1-2-3 Kasumi,Minami-ku, Hiroshima 734, Japan. E-mail: [email protected]
Contract/grant sponsors: Ministry of Health and Welfare of Japan;Ministry of Education, Science, Sports and Culture of Japan.
INTRODUCTION
It is generally supposed that several gene mutationsinvolving the APC, Ki-ras, p53, and DCC genes areresponsible for multistep carcinogenesis of the colorec-tum.1 This concept is based on the scenario called the‘adenoma–carcinoma sequence’. In recent years, how-ever, many epidemiological and histopathologicalstudies have indicated the existence of another pathwaycalled ‘de novo’ colon carcinogenesis.2 In relation to ‘denovo’ colon carcinogenesis, it has been reported thatKi-ras gene mutations are infrequent in flat-type adeno-mas and adenocarcinomas,3 but are frequent in hyper-plastic polyps, which can be precursors of carcinomas.4In addition to mutations of these genes, microsatelliteinstability has been observed in colorectal tumours from
CCC 0022–3417/98/100131–09$17.50? 1998 John Wiley & Sons, Ltd.
individuals with hereditary non-polyposis colorectalcancer (HNPCC) and in some sporadic tumours.5HNPCC can be caused by germline mutations ofmismatch repair genes such as hMSH2, hMLH1,hPMS1, and hPMS2.6 Transforming growth factor-â(TGF-â) type II receptor is one of the target genesfor microsatellite instability-associated mutatormechanisms.7
Serrated adenoma/mixed hyperplastic and adenoma-tous polyp has been recently proposed as a distincthistological lesion.8–10 It is characterized morphologi-cally by a serrated glandular pattern similar to thehyperplastic polyp, the presence of goblet cell imma-turity, upper zone mitoses, prominence of nucleoli, andthe absence of a thickened collagen table. The lesions arevery rare and are often underdiagnosed as hyperplasticpolyps.8 Longacre et al. reported that only 101 serratedadenomas were recognized among more than 18 000polyps reviewed.9 However, they have various degrees ofatypia and are sometimes associated with adenocarci-noma in the deepest portion. Immunohistochemicalstudies have revealed that serrated adenomas have high
Received 23 September 1997Revised 12 December 1997
Accepted 26 May 1998

132 T. HIYAMA ET AL.
cell proliferation rates at the lower part of crypts, whichis different from ordinary tubular adenomas.11 Further-more, it has been reported that serrated adenomas havefrequent and intense p53 immunoreactivity, althoughordinary tubular adenomas do not.12 These reportssuggest that serrated adenomas might be involved in acarcinogenic pathway different from the ‘adenoma–carcinoma sequence’ or carcinogenesis via mutations ofthe mismatch repair genes. However, there are fewstudies concerning genetic alterations in serrated adeno-mas. We examined alterations in the APC, Ki-ras, p53,and DCC genes, as well as microsatellite instability,in serrated adenomas and adenocarcinomas in/withserrated adenomas.
MATERIALS AND METHODS
Specimens
Nineteen serrated adenomas and ten adenocarcino-mas in/with serrated adenomas were obtained fromHiroshima University Hospital and its affiliated hospi-tals between December 1993 and March 1995. Twenty-three hyperplastic nodules, which consisted ofhyperproliferative epithelium without sawtoothed pat-tern, four hyperplastic polyps with sawtoothed hyper-proliferative epithelium, and 29 tubular adenomas, werealso used as controls. Informed consent was obtainedfrom all subjects. Degrees of atypia of serrated aden-omas were determined according to the criteria of theJapanese Research Society for Cancer of the Colon andRectum.13 Three were serrated adenomas with mildatypia, six were with moderate atypia, and ten were withsevere atypia. Five were mucosal carcinomas, four wereadenocarcinomas in serrated adenomas invadingminutely into the submucosa, and one was an adeno-carcinoma in a serrated adenoma invading massively
? 1998 John Wiley & Sons, Ltd.
into the submucosa. These lesions were divided morpho-logically into two groups, the flat (superficial) type andthe polypoid type, according to the criteria proposed byAdachi et al.14 None of the patients had polyposissyndromes or HNPCC.
DNA extraction and amplification
Tissue sections 10 ìm in thickness were stained withhaematoxylin and eosin (H&E), dehydrated in gradedethanol, and then dried without a cover glass. Tissueswere cut with sterile scissors and the DNA was extractedfrom the tissues with 20 ìl of extraction buffer (100 mTris–HCl; 2 m ethylene diamine tetraacetic acid,pH 8·0; 400 ìg/ml proteinase K) at 55)C for 3 h. Thetubes were boiled for 7 min to inactivate proteinase Kand then 1–5 ìl of these extracts was used for eachpolymerase chain reaction (PCR) amplification. In fiveserrated adenomas and three adenocarcinomas in/withserrated adenomas, limited tissues such as upper orlower parts of the crypts or parts invading into thesubmucosa were microdissected from the sections undera stereomicroscope. The DNA of the microdissectedareas was extracted as described.
Table I—Primer sets used in PCR
Priming region Primer sequence
APC exon 15 5*-AACTACCATCCAGCAACAGA-3*(codons 862–1022) 5*-TCTAGTTCTCCATCATTATCAT-3*
APC exon 15 5*-AGACTTATTGTGTAGAAGATAC-3*(codons 1260–1410) 5*-ATGGTTCACTCTGAACGGA-3*
APC exon 15 5*-TCTGTCAGTTCACTTGATAG-3*(codons 1389–1547) 5*-CATTTGATTCTTTAGGCTGC-3*
Ki-ras codon 12 5*-TTGTTGGATCATATTCGTCC-3*5*-GGCCTGCTGAAAATGACTGA-3*
p53 3*-end untranslated region 5*-TTGCCGTCCCAAGCAATGGATGA-3*5*-TCTGGGAAGGGACAGAAGATGAC-3*
p53 exon 4 5*-TTGCCGTCCCAAGCAATGGATGA-3*5*-TCTGGGAAGGGACAGAAGATGAC-3*
p53 exon 5 5*-TTCAACTCTGTCTCCTTCCT-3*5*-CAGCCCTGTCGTCTCTCCAG-3*
p53 exon 6 5*-GCCTCTGATTCCTCACTGAT-3*5*-CCCTTAACCCCTCCTCC-3*
p53 exon 7 5*-GGCGCACTGGCCTCATCTTG-3*5*-GGCTGGGGCACAGCAGG-3*
p53 exon 8 5*-GGTTTTTTAAATGGGACAG-3*5*-TGCTTGCTTACCTCGCTTA-3*
PCR–SSCP analyses and direct sequencing analyses ofthe APC, Ki-ras, and p53 genes
Exon 15 of the APC gene, which included the mu-tation cluster region of colorectal carcinoma cells,15,16
codon 12 of the Ki-ras gene, and exons 5–8 of the p53gene were amplified separately. The sequence of eachprimer used for PCR is shown in Table I. PCR–SSCPanalyses were performed as described by Dix et al.17
Each PCR–SSCP analysis was performed with positiveand negative controls; for example, DNA extracted fromTMK-1, a gastric carcinoma cell line, as a positive
J. Pathol. 186: 131–139 (1998)

133FREQUENT p53 MUTATIONS IN SERRATED ADENOMAS
control and MKN-45 as a negative control for exon 5 ofthe p53 gene.18 Gene mutations detected by PCR–SSCPanalyses were confirmed by direct sequencing of thePCR product, using the Circum Vent Thermal CycleDideoxy DNA Sequencing Kit (New England Labs,Beverly, MA, U.S.A.) except for the Ki-ras gene. TheDNA extraction, PCR, and sequencing reactions wererepeated at least twice to confirm the results.
PCR–RFLP analyses of the p53 gene
PCR–RFLP analyses of 3*-end untranslated regionand exon 4 of the p53 gene were performed using therestriction enzymes Bam HI and Acc II, respectively, todetect loss of heterozygosity (LOH).
Microsatellite assay
A microsatellite marker, D5S505, was used to exam-ine LOH and microsatellite instability at 5q (APC gene)and D18S58 and D18S61 were used to check the 18q(DCC gene) status.19 BATRII, BAT25, and BAT40 werealso used.7,20 The microsatellite assay was performedas described elsewhere.21 Each microsatellite assaywas performed also on colorectal carcinomas with andwithout known microsatellite instability, as positiveand negative controls respectively.
Immunohistochemistry
The avidin–biotin–peroxidase complex method withan antigen retrieval procedure22 was performed. Primaryspecific antibodies against p53 (DO-7) and p21 (sc-187)were purchased from Novocastra Laboratories(Newcastle, U.K.) and Santa Cruz Biotechnology Inc.(Santa Cruz, CA, U.S.A.), respectively. The immuno-reactivity was graded according to the percentage ofpositive tumour cells as follows: + + + (marked;more than 50 per cent of the tumour cells werestained intensely), + + (moderate; 20–50 per cent stainedintensely), + (mild; less than 20 per cent stained,intensely or weakly stained), or " (no staining). Color-ectal carcinomas for which the p53 immunoreactivitystatus was already known were used as positive andnegative controls.
Data analysis
Data for mutation rates were analysed using thechi-square test. Statistical significance was defined asp<0·05.
RESULTS
The overall results of genetic analyses in individualtumours in the present study are summarized in TableII.
p53 immunostaining
Eleven of 11 (100 per cent) serrated adenomas exam-ined had p53 immunoreactivity, of which four (36 per
? 1998 John Wiley & Sons, Ltd.
cent) showed moderate immunoreactivity. All six (100per cent) adenocarcinomas in/with serrated adenomasexhibited moderate to marked p53 immunoreactivity.
Mutational analysis
These data are summarized in Table III. Mutations ofthe p53 gene were found in 9 of 19 (47 per cent) serratedadenomas and in 5 of 10 (50 per cent) adenocarcinomasin/with serrated adenomas (Figs 1 and 2). No p53 genemutation was detected in 23 hyperplastic nodules,four hyperplastic polyps, or 29 tubular adenomas. Inother words, serrated adenomas exhibited significantlyfrequent mutations of the p53 gene, compared withhyperplastic nodules, hyperplastic polyps, and tubularadenomas (p<0·005). Mutations of the Ki-ras gene weredetected in 11 of 19 (58 per cent) serrated adenomas andin 6 of 10 (60 per cent) adenocarcinomas in/with serratedadenomas. Nine of 23 (39 per cent) hyperplastic nodules,3 of 4 (75 per cent) hyperplastic polyps, and 12 of 29 (41per cent) tubular adenomas contained mutations of theKi-ras gene. No significant difference was found betweenthe frequencies of Ki-ras gene mutations of serratedadenomas and those of hyperplastic nodules, hyperplas-tic polyps, or tubular adenomas. According to mor-phology, 3 of 8 (38 per cent) flat-type serrated adenomasand 3 of 4 (75 per cent) flat-type adenocarcinomasin/with serrated adenomas had mutations of the p53gene, as also did 6 of 11 (55 per cent) polypoid-typeserrated adenomas and 2 of 8 (38 per cent) polypoid-type adenocarcinomas in/with serrated adenomas. Fur-thermore, 3 of 8 (38 per cent) flat-type serratedadenomas and 2 of 4 (50 per cent) flat-type adenocarci-nomas in/with serrated adenomas exhibited Ki-ras genemutations, as did 8 of 11 (73 per cent) polypoid-typeserrated adenomas and 4 of 6 (67 per cent) polypoid-type adenocarcinomas in/with serrated adenomas (TableIV). The frequencies of p53 gene mutations were almostthe same between flat-type and polypoid-type (50 percent vs. 48 per cent overall) and those of Ki-ras genemutations tended to be less in flat-type than polypoid-type (42 per cent vs. 71 per cent overall). Microsatelliteinstability was detected in 1 of 19 (5 per cent) serratedadenomas and 1 of 10 (10 per cent) adenocarcinomasin/with serrated adenomas. The other lesions did notshow microsatellite instability.
Microdissection data
Five serrated adenomas and three adenocarcinomasin/with serrated adenomas were chosen for the analysisof the DNA from very limited areas of tissue, such as theupper or lower parts of the crypts, or parts invading intothe submucosa. This was accomplished on paraffin-embedded sections using a microdissection technique.Figure 3 shows a minutely invading adenocarcinoma ina serrated adenoma (case 26) with irregularity of thegland and cytological atypia in the deepest portion.Although little stromal reaction can be seen, the muscu-laris mucosae is completely separated by the invasivegrowth of this tumour and we therefore diagnosed this
J. Pathol. 186: 131–139 (1998)

134 T. HIYAMA ET AL.
Table II—Mutations of the p53 and Ki-ras genes in individual tumours
CaseNo. I.D. Morphology* Histology†
IHC ofp53‡
Mutation ofthe Ki-ras
gene§
Mutation ofthe p53geneQ
Microsatelliteinstability¶
1 443079-1 F SA (mild) + " " "2 441236 P SA (mild) + + + (exon 5) "3 441259 P SA (mild) + + + (exon 7) "4 443079-2 F SA (mod) + + " " "5 443451-1 F SA (mod) + " " "6 443451-2 P SA (mod) + + " "7 95-438 P SA (mod) + + + (exon 7) "8 93-2214 P SA (mod) NE + + (exon 8) "9 93-1794 P SA (mod) NE " " "
10 443105 F SA (sev) + + + + (exon 5) + (BAT25, BAT40)11 443079-3 F SA (sev) + + " + (exon 5) "12 95-859 F SA (sev) + + + " "13 921657 P SA (sev) NE + + (exon 7) "14 921658 P SA (sev) NE " " "15 931471 P SA (sev) NE + " "16 932694 P SA (sev) NE + + (exon 7) "17 95-4628 F SA (sev) NE + " "18 441561 P SA (sev) + " " "19 95-2366 F SA (sev) NE " + (exon 5) "20 931623 P Ca(m) in SA NE + " "21 931204 P Ca(m) in SA NE + + (exon 7) "22 96-2474 P Ca(m) in SA NE " " "23 93-1749 P Ca(m) in SA NE + + (exon 5, 8) "24 396333 P Ca(m) with SA + + + " " "25 95-370 F Ca(sm1) in SA + + " + (exon 5) "26 439118-1 F Ca(sm1) in SA + + " + (exon 8) "27 439118-2 F Ca(sm1) in SA + + + " "28 95–186 P Ca(sm1) in SA + + + " "29 94-1741 F Ca(sm3) with SA + + + + (exon 7) + (BAT25)
*F, flat type; P, polypoid type.†SA (mild), serrated adenoma with mild atypia; SA (mod), serrated adenoma with moderate atypia; SA (sev), serrated adenoma with severe
atypia; Ca(m), mucosal carcinoma; Ca(sm1), adenocarcinoma minutely invading into the submucosa; Ca(sm3), adenocarcinoma massively invadinginto the submucosa.
‡IHC, immunohistochemistry: ", no staining; +, mild staining; + +, moderate staining; + + +, intense staining; NE, not examined.§+, mobility shift is detected by PCR–SSCP analysis; ", no mobility shift is detected by PCR–SSCP analysis.QExon No. which shows a mobility shift is given in parentheses.¶+, microsatellite instability is positive; ", microsatellite instability is negative; positive microsatellite loci which show instability are given in
parentheses.
Table III—Summary of the genetic changes in serrated adenomas, adenocarcinomas in/with serratedadenomas, and other lesions
HistologyMutations ofthe p53 gene*
Mutations ofthe Ki-ras gene*
Microsatelliteinstability†
Serrated adenoma 9/19 (47%)‡ 11/19 (58%) 1/19 (5%)Adenocarcinoma in/with serrated adenoma 5/10 (50%)‡ 6/10 (60%) 1/10 (10%)Hyperplastic nodule 0/23 (0%) 9/23 (39%) 0/23 (0%)Hyperplastic polyp 0/4 (0%) 3/4 (75%) 0/4 (0%)Tubular adenoma 0/29 (0%) 12/29 (41%) 0/29 (0%)
*Mutations detected by PCR–SSCP analysis.†Microsatellite instability at D5S505, D18S58, D18S61, BATRII, BAT25, and BAT40 loci.‡p<0·005 compared with pyperplastic nodules, hyperplastic polyps, and tubular adenomas by the chi-square test.
lesion as a minutely invading adenocarcinoma in aserrated adenoma. The scanty stromal reaction may bedue to the very minute size and early stage of the
? 1998 John Wiley & Sons, Ltd.
invasive tumour. Exon 15 of the APC gene and the DCCgene, in addition to p53, Ki-ras genes, as well as micro-satellite instability, were analysed (Table V). In case 10,
J. Pathol. 186: 131–139 (1998)

135FREQUENT p53 MUTATIONS IN SERRATED ADENOMAS
which was a serrated adenoma with severe atypia,mutated p53 gene was detected only in the lower parts ofthe crypts of the serrated adenoma. What is moreimportant is that the identical mutation of the p53 genewas found in invasive adenocarcinomas and adjacentserrated adenomas of cases 25, 26, and 29, respectively.These data suggest single clonal origins for these lesions.However, no LOH of the p53 gene was detected byPCR–RFLP analyses in these eight samples. Mutationsof the APC gene were observed in two of five serratedadenomas and none of the adenocarcinomas in/withserrated adenomas. Microsatellite instability was seen inone serrated adenoma and one adenocarcinoma in aserrated adenoma. Mutations of the APC gene andmicrosatellite instability were heterogeneous in those
? 1998 John Wiley & Sons, Ltd.
lesions (cases 5 and 11). No LOH was found at theD5S505 locus (APC gene) or at the D18S58 and D18S61loci (DCC gene).
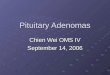
Fig. 1—Polypoid-type serrated adenoma (case 16). (A) Light microscopic view (H&E, #40) showing the serrated, lengthenedglandular architecture. (B) Light microscopic view (H&E, #200) demonstrating high columnar cells and stratified nuclei. (C)Light microscopic view (H&E, #400) indicating relatively hyperchromatic nuclei and a few small nucleoli in a serratedadenoma. (D) Mobility shifts at exon 7 of the p53 gene and codon 12 of the Ki-ras gene detected by PCR–SSCP analyses (seearrow-head). N, normal mucosa; T, serrated adenoma; ex., exon
DISCUSSION
In this study, we demonstrate frequent mutations ofthe p53 gene in serrated adenomas of the colorectum.Colorectal tumourigenesis is one of the best-characterized examples of multistep progression. Acti-vation of an oncogene, Ki-ras gene,23 as well asinactivation of tumour suppressor genes, such asAPC,15,16 p53,17,24 and DCC,25 are consistently involvedin the process. It has been widely accepted that APC
J. Pathol. 186: 131–139 (1998)

136 T. HIYAMA ET AL.
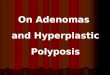
Fig. 2—Flat-type serrated adenoma (case 19). (A) Light microscopic view (H&E, #40) showing the serrated glandulararchitecture. (B) Light microscopic view (H&E, #200) demonstrating high columnar cells and stratified nuclei. (C) Lightmicroscopic view (H&E, #400) indicating relatively hyperchromatic nuclei and a few small nucleoli in a serrated adenoma.(D) Mobility shift at exon 5 of the p53 gene detected by PCR–SSCP analysis (see arrow-head). N, normal mucosa; T, serratedadenoma; ex., exon
Table IV—The frequencies of mutations of Ki-ras and p53 genes in serrated adenomas and adenocarci-nomas in/with serrated adenomas
Morphology HistologyMutations of
the Ki-ras gene*Mutations ofthe p53 gene*
Flat type Serrated adenoma 3/8 (38%) 3/8 (38%)Adenocarcinoma in/with serrated adenoma 2/4 (50%) 3/4 (75%)
Polypoid type Serrated adenoma 8/11 (73%) 6/11 (55%)Adenocarcinoma in/with serrated adenoma 4/6 (67%) 2/6 (33%)
*Mutations detected by PCR–SSCP analysis.
gene mutations are involved in the earliest events andp53 and DCC gene mutations in relatively late events incolorectal tumourigenesis.1,26 It has been reported that50–63 per cent of ordinary colorectal adenomas contain
? 1998 John Wiley & Sons, Ltd.
a mutated APC gene,16 approximately 40 per cent ofthose lesions have a mutated Ki-ras gene,23 and less than10 per cent of those lesions exhibited a mutated p53gene.24
J. Pathol. 186: 131–139 (1998)

Fig. 3—Histological findings of a minutely invading adenocarcinoma in a serrated adenoma (case 26). (A) Light microscopicview (H&E, #20) showing a serrated glandular pattern and minute invasion into the submucosa (see arrow). (B) Lightmicroscopic view (H&E, #100) showing the invasive area. (C) p53 immunohistochemical staining indicating moderateimmunoreactivity (#400). (D) After microdissection (H&E, #20). 1 and 5, lower part of crypts; 2, 4, and 6, upper parts ofcrypts; 3, area of invasive growth into the submucosa. (E) All of the parts exhibited an identical mobility shift at exon 8 of thep53 gene detected by PCR–SSCP analysis (see arrow-head). N, normal mucosa. 1–5, microdissected areas shown in D. (F)Direct sequencing of the sense strand pointing out a missense mutation at codon 278 of the p53 gene

138 T. HIYAMA ET AL.
Table V—Genetic alterations in five serrated adenomas and three adenocarcinomas in/with serrated adenomas using a micro-dissection technique
CaseNo. Histology*
IHC†
Part‡
APC Ki-ras p53 DCCMicrosatelliteinstability**p53 p21 Mutation§ MutationQ Mutation§ LOH¶
1 SA (mild) + + N " " " " "up " " " " "low " " " " "
4 SA (mod) + + + N " " " " "up " " " " "low " " " " "
5 SA (mod) + + N " " " " "up " " " " "low GAA to
GGA(1290)" " " "
10 SA (sev) + + + + + N " " " " "up " + " " + (BAT25, BAT40)low " + ATC to ATG(162) " "
11 SA (sev) + + + N " " " " "up TGT to
TGA(1393)" GTG to ATG(173) " "
low CAG toTAG(1373)
" GTG to ATG(173) " "
25 Ca(sm1) in SA + + + N " " " " "up " " TGG to TCG(146) " "low " " TGG to TCG(146) " "inv " " TGG to TCG(146) " "
26 Ca(sm1) in SA + + " N " " " " "up " " CCT to TCT(278) " "low " " CCT to TCT(278) " "inv " " CCT to TCT(278) " "
29 Ca(sm3) with SA + + " N " " " " "up " + " " + (BAT25)low " + TGC to TGA(242) " "
sup. ca " + TGC to TGA(242) " "deep ca " + TGC to TGA(242) " "
*SA (mild), serrated adenoma with mild atypia; SA (mod), serrated adenoma with moderate atypia; SA (sev), serrated adenoma with severeatypia; Ca(sm1), adenocarcinoma minutely invading into the submucosa in a serrated adenoma; Ca(sm3) with SA, adenocarcinoma massivelyinvading into the submucosa with a serrated adenoma.
†IHC, immunohistochemistry: ", no staining; +, mild staining; + +, moderate staining; + + +, intense staining.‡Part, the part from which DNA was extracted: N, normal mucosa, up, upper part of crypts of serrated adenoma; low, lower part of crypts of
serrated adenoma; inv, part which invaded into the submucosa; Sup. ca, superficial part of adenocarcinoma; deep ca, deep part of adenocarcinoma.§The numbers in parentheses show the codon number which mutated.Q+, mobility shift is detected by PCR–SSCP analysis; ", no mobility shift is detected by PCR–SSCP analysis.¶LOH at D18S58 and D18S61 detected by microsatellite assay.**+, microsatellite instability is positive; ", microsatellite instability is negative; positive microsatellite loci which show instability are given in
parentheses.
In this study, p53 gene mutations were found in 48 percent of serrated adenomas and 50 per cent of adeno-carcinomas in/with serrated adenomas. On the otherhand, no p53 gene mutation was detected in hyperplasticnodules, hyperplastic polyps, or tubular adenomas.These findings imply that serrated adenomas are geneti-cally different from hyperplastic lesions or tubularadenomas. Although no LOH of the p53 gene wasdetected in eight lesions by PCR–RFLP analyses, thelocus that we examined was restricted and some deletionmight exist in another region of the p53 gene. Incontrast, mutations of the Ki-ras gene were found in 58per cent of serrated adenomas and 60 per cent ofadenocarcinomas in/with serrated adenomas. Thirty-nine per cent of hyperplastic nodules, 75 per cent of
? 1998 John Wiley & Sons, Ltd.
hyperplastic polyps, and 41 per cent of tubular adeno-mas contained Ki-ras gene mutations. There were nosignificant differences between the frequences of Ki-rasgene mutations in serrated adenomas, hyperplasticlesions, and tubular adenomas. We divided serratedadenomas and adenocarcinomas in/with serrated adeno-mas into two morphological groups: the flat (superficial)type and the polypoid type. Although there was nosignificant difference between the frequencies of p53 genemutations of flat-type and polypoid-type lesions (50 percent vs. 47 per cent), flat-type lesions had less frequentKi-ras gene mutations than polypoid-type lesions (42per cent vs. 71 per cent). The same tendency for Ki-rasgene mutations was reported in flat- and polypoid-typeadenomas and in flat- and polypoid-type carcinomas.3
J. Pathol. 186: 131–139 (1998)

139FREQUENT p53 MUTATIONS IN SERRATED ADENOMAS
Microsatellite instability is a recently discovered land-mark of some tumours of the colorectum.5,6 Approxi-mately 80–90 per cent of HNPCC tumours and 9–17 percent of sporadic colorectal cancers show microsatelliteinstability. In the present study, only 1 of 19 (5 per cent)serrated adenomas and 1 of 10 (10 per cent) adenocar-cinomas in/with serrated adenomas showed microsatel-lite instability. Microsatellite instability may thereforeplay a limited role in the tumourigenesis of serratedadenomas.
A monoclonal antibody against Ki-67 antigen stainsthe nuclei of proliferating cells in all cycle phases exceptG0 and early G1.27 Immunohistochemical studiesdirected at Ki-67 revealed that serrated adenomas hadhigh cell proliferation rates at the lower parts of thecrypts, which was different from ordinary adenomas.11
All cases in this study had high cell proliferation rates atthe lower part of the crypts, as assessed by Ki-67immunoreactivity (data not shown). In the invasiveadenocarcinoma with a serrated adenoma, the identicalmutation of the p53 gene was found in the invasiveadenocarcinoma and in the lower part of the cryptsof the adjacent serrated adenoma. These results suggestthat the cells of the lower part of the crypts in serratedadenomas are truly neoplastic and progress to adeno-carcinoma.
In conclusion, the data presented here indicate thatserrated adenomas might be involved in a carcinogenicpathway of the colorectum distinct from the ordinaryadenoma–carcinoma sequence and from carcinogenesisvia mutations of the mismatch repair genes. Further-more, some so-called ‘de novo’ cancers might be theresult of carcinogenesis via flat-type serrated adenomas,because serrated adenomas tend to involve thesubmucosa earlier as they become malignant.
ACKNOWLEDGEMENTS
This work was supported in part by a Grant-in-Aidfor the Comprehensive 10-Year Strategy for CancerControl from the Ministry of Health and Welfare ofJapan and a Grant-in-Aid from the Ministry ofEducation, Science, Sports and Culture of Japan. Wethank Drs Y. Kato, A. Yanagisawa, K. Nakano, and T.Hada (Cancer Institute, Tokyo, Japan) for helpful com-ments on this work. We also thank Mr M. Takatani andMr T. Nomi for providing tissue sections.
REFERENCES1. Fearon E, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell
1990; 61: 759–767.
? 1998 John Wiley & Sons, Ltd.
2. Jass JR. Do all colorectal carcinomas arise in preexisting adenoma? WorldJ Surg 1989; 13: 45–51.
3. Minamoto T, Sawaguchi K, et al. Infrequent K-ras activation in superficial-type (flat) colorectal adenomas and adenocarcinomas. Cancer Res 1994; 54:2841–2844.
4. Otori K, Oda Y, Sugiyama K, et al. High frequency of K-ras mutation inhuman colorectal hyperplastic polyps. Gut 1997; 40: 660–663.
5. Aaltonen LA, Peltomäki P, Leach FS, et al. Clues of the pathogenesis offamilial colorectal cancer. Science 1993; 260: 812–816.
6. Liu B, Parsons R, Papadopoulos N, et al. Analysis of mismatch repair genesin hereditary non-polyposis colorectal cancer patients. Nature Med 1996; 2:169–174.
7. Markowitz S, Wang J, Myeroff L, et al. Inactivation of the type II TGF-âreceptor in colon cancer cells with microsatellite instability. Science 1995;268: 1336–1338.
8. Urbanski SJ, Marcon N, Kossakowka AE, Bruce WR. Mixed hyperplasticadenomatous polyps—an underdiagnosed entity. Am J Surg Pathol 1984; 8:551–556.
9. Longacre TA, Fenoglio-Preiser CM. Mixed hyperplastic adenomatouspolyps/serrated adenomas. Am J Surg Pathol 1990; 14: 524–537.
10. Gebbers JO, Laissue JA. Mixed hyperplastic and neoplastic polyp of thecolon. An immunohistological study. Virchows Arch A 1986; 410: 189–194.
11. Rubio CA, Rodensjö M. Flat serrated adenomas and tubular adenomas ofthe colorectal mucosa: differences in the pattern of cell proliferation. Jpn JCancer Res 1995; 86: 756–760.
12. Rubio CA, Rodensjö M. p53 overexpression in flat serrated adenomas andflat tubular adenomas of the colorectal mucosa. J Cancer Res Clin Oncol1995; 121: 571–576.
13. Japanese Research Society for Cancer of the Colon and Rectum. GeneralRules for Clinical and Pathological Studies on Cancer of the Colon, Rectumand Anus. 5th edn. Tokyo: Kanehara, 1994; 49–73.
14. Adachi M, Muto T, Okinaga K, Morioka Y. Clinicopathological features ofthe flat adenoma. Dis Colon Rectum 1992; 35: 543–546.
15. Miyoshi Y, Nagase H, Ando H, et al. Somatic mutations of the APC genein colorectal tumors: mutation cluster region in the APC gene. Hum MolGenet 1992; 1: 229–233.
16. Miyoshi Y, Ando H, Nagase H, et al. Germline mutations of the APC genein 53 familial adenomatous polyposis patients. Proc Natl Acad Sci USA1992; 89: 4452–4456.
17. Dix B, Robbins P, Carrello S, House A, Iacopetta B. Comparison of p53gene mutation and protein overexpression in colorectal carcinomas. Br JCancer 1994; 70: 585–590.
18. Tahara E, Semba S, Tahara H. Molecular biological observations in gastriccancer. Semin Oncol 1996; 23: 307–315.
19. Jen J, Kim H, Piantadosi S, et al. Allelic loss of chromosome 18q andprognosis in colorectal cancer. N Engl J Med 1994; 331: 213–221.
20. Liu B, Farrington SM, Petersen GM, et al. Genetic instability occurs in themajority of young patients with colorectal cancer. Nature Med 1995; 1:348–352.
21. Semba S, Yokozaki H, Yamamoto S, Yasui W, Tahara E. Microsatelliteinstability in precancerous lesions and adenocarcinomas of the stomach.Cancer 1996; 77: 1620–1627.
22. van den Berg FM, Baas IO, Polak MM, Offeraus JA. Detection of p53overexpression in routinely paraffin-embedded tissue of human carcinomasusing a novel target unmasking fluid. Am J Pathol 1993; 142: 381–385.
23. Bos JL, Fearon ER, Hamilton SR, Verlaan-de Vries M, van Boom JH,Vogelstein B. Presence of ras gene mutations in human colorectal cancers.Nature 1987; 327: 293–297.
24. Baker SJ, Fearon ER, Nigro JM, et al. Chromosome 17 deletions and p53gene mutations in colorectal carcinomas. Science 1989; 244: 217–221.
25. Fearon ER, Cho KR, Nigro JM, et al. Identification of a chromosome 18qgene that is altered in colorectal cancers. Science 1990; 247: 49–56.
26. Powell SM, Zilz N, Beazer-Barclay Y, et al. APC mutations occur earlyduring colorectal tumorigenesis. Nature 1992; 359: 235–237.
27. Gerdes J, Lemke H, Baisch H, Wacher HH, Schwab U, Stein H. Cell cycleanalysis of a cell proliferation associated human nuclear antigen defined bythe monoclonal antibody Ki-67. J Immunol 1984; 168: 357–363.
J. Pathol. 186: 131–139 (1998)








![Serrated lesions in colorectal cancer screening: detection ... · SSP are very similar to HPs and very distinct from conventional adenomas[12]. Finally, the ADR has emerged as the](https://img.pdfslide.us/doc/110x75/5ca1e06b88c993ce7d8cfd64/serrated-lesions-in-colorectal-cancer-screening-detection-ssp-are-very.jpg)