-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
1/12
See discussions, stats, and author profiles for this publication
at: http://www.researchgate.net/publication/285728833
Treatment–resistant panic disorder: a systematicreview
ARTICLE in EXPERT OPINION ON PHARMACOTHERAPY ·
DECEMBER 2015
Impact Factor: 3.53 · DOI: 10.1517/14656566.2016.1109628
READS
4
4 AUTHORS, INCLUDING:
Rafael Christophe Freire
Federal University of Rio de Janeiro
70 PUBLICATIONS 582 CITATIONS
SEE PROFILE
Antonio E Nardi
Federal University of Rio de Janeiro
453 PUBLICATIONS 2,883 CITATIONS
SEE PROFILE
Available from: Rafael Christophe Freire
Retrieved on: 08 December 2015
http://www.researchgate.net/?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_1http://www.researchgate.net/profile/Antonio_Nardi?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_7http://www.researchgate.net/institution/Federal_University_of_Rio_de_Janeiro2?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_6http://www.researchgate.net/profile/Antonio_Nardi?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_5http://www.researchgate.net/profile/Antonio_Nardi?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_4http://www.researchgate.net/profile/Rafael_Freire?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_7http://www.researchgate.net/institution/Federal_University_of_Rio_de_Janeiro2?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_6http://www.researchgate.net/profile/Rafael_Freire?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_5http://www.researchgate.net/profile/Rafael_Freire?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_4http://www.researchgate.net/?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_1http://www.researchgate.net/publication/285728833_Treatmentresistant_panic_disorder_a_systematic_review?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_3http://www.researchgate.net/publication/285728833_Treatmentresistant_panic_disorder_a_systematic_review?enrichId=rgreq-82abb6c3-e059-4bbc-801c-75a3b7a36314&enrichSource=Y292ZXJQYWdlOzI4NTcyODgzMztBUzozMDQzODU3ODYwODk0NzJAMTQ0OTU4MjYzNDQwMA%3D%3D&el=1_x_2
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
2/12
Full Terms & Conditions of access and use can be found
athttp://www.tandfonline.com/action/journalInformation?journalCode=ieop20
Download by: [Rafael Freire] Date: 08 December 2015,
At: 05
Expert Opinion on Pharmacotherapy
ISSN: 1465-6566 (Print) 1744-7666 (Online) Journal homepage:
http://www.tandfonline.com/loi/ieop20
Treatment–resistant panic disorder: a systematicreview
Rafael C. Freire, Morena M. Zugliani, Rafael F. Garcia &
Antonio E. Nardi
To cite this article: Rafael C. Freire, Morena M. Zugliani,
Rafael F. Garcia & Antonio E.
Nardi (2015): Treatment–resistant panic disorder: a systematic
review, Expert Opinion onPharmacotherapy, DOI:
10.1517/14656566.2016.1109628
To link to this article:
http://dx.doi.org/10.1517/14656566.2016.1109628
Published online: 04 Dec 2015.
Submit your article to this journal
Article views: 2
View related articles
View Crossmark data
http://crossmark.crossref.org/dialog/?doi=10.1517/14656566.2016.1109628&domain=pdf&date_stamp=2015-12-04http://crossmark.crossref.org/dialog/?doi=10.1517/14656566.2016.1109628&domain=pdf&date_stamp=2015-12-04http://www.tandfonline.com/doi/mlt/10.1517/14656566.2016.1109628http://www.tandfonline.com/doi/mlt/10.1517/14656566.2016.1109628http://www.tandfonline.com/action/authorSubmission?journalCode=ieop20&page=instructionshttp://www.tandfonline.com/action/authorSubmission?journalCode=ieop20&page=instructionshttp://dx.doi.org/10.1517/14656566.2016.1109628http://www.tandfonline.com/action/showCitFormats?doi=10.1517/14656566.2016.1109628http://www.tandfonline.com/loi/ieop20http://www.tandfonline.com/action/journalInformation?journalCode=ieop20
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
3/12
REVIEW
Treatment–resistant panic disorder: a systematic review
Rafael C. Freire , Morena M. Zugliani, Rafael F. Garcia and
Antonio E. Nardi
Laboratory of Panic and Respiration, Institute of Psychiatry,
Federal University of Rio de Janeiro and National Institute for
TranslationalMedicine (INCT-TM), Rio de Janeiro, Brazil
ABSTRACT
Introduction: The prevalence of panic disorder (PD) in the
population is high and these patientshave work impairment, high
unemployment rates, seek medical treatment more frequently andhave
more hospitalizations than people without panic symptoms. Despite
the availability of pharmacological, psychological and
combined treatments, approximately one-third of all PDpatients have
persistent panic attacks and other PD symptoms after treatment.
Areas covered : MEDLINE/Pubmed, CENTRAL, PsycINFO and
Web of Science databases weresearched for clinical trials in
treatment–resistant PD. Only studies published between 1980
and2015, in English, with human subjects, considered
“ journal articles” and clinical trial wereincluded. We
included trials recruiting only adult subjects with
treatment–resistant PD, consistentwith criteria from DSM-III to
DSM5. We included all prospective experimental studies. Case,
caseseries, retrospective studies or studies with
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
4/12
rates were somewhat higher, from 68 to 89%, but from
49 to 64% of the patients did not achieve remission
after 10 – 12 weeks of treatment.[15] In the
general
population, almost one-half of PD patients do not
achieve remission in the first year of treatment andafter 2
years of treatment more than one-third of the
patients still have PD symptoms.[16]
The objective of this systematic review is to summar-
ize and discuss the evidences regarding the treatment
of patients with treatment–resistant PD.
2. Methods
Articles were identified by a search of electronic
records, including the databases from MEDLINE/
Pubmed, the Cochrane Collaboration’s Clinical Trials
Register (CENTRAL), PsycINFO and Thomson Reuters’s
Web of Science. The search terms used were: “Panic
disorder” AND (“ Treatment–resistant” OR
“ Treatment
resistance” OR “Pharmacotherapy-resistant”
OR
“Pharmacotherapy resistance” OR
“Medication-resistant”
OR “Medication resistance” OR
“Drug-resistant” OR
“Drug resistance” OR “Refractory” OR
“Augmentation”).
Only studies published in the years between 1980 and
2015, in English, with human subjects, considered
“ jour-
nal articles” and clinical trial were included. We
included trials recruiting only adult subjects with treat-
ment–resistant PD, consistent with criteria from DSM-III
to DSM5.[17–20] All definitions of treatment–resistance
were accepted. We included all prospective experimen-
tal studies including randomized-controlled trials,
quasi-random trials, crossover designs, and single arm
studies, blinded or open label. Case, case series, retro-
spective studies or studies with
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
5/12
The article from Simon et al . [22]
included three
clinical trials, phases I, II and III. Phase I was not with
treatment–resistant PD and was not included in the
review, phases II and III were treated as independent
trials.
The studied drugs were divalproex sodium, reboxe-
tine, pindolol, aripiprazole, olanzapine, sertraline, esci-
talopram and clonazepam. Among the 12 clinical trials,
the studied treatment was an augmentation of another
treatment in nine of them. The trial duration rangedfrom 4 to 16
weeks. There were no significant differ-
ences between low and high dose of sertraline or esci-
talopram,[22] otherwise all studied treatments were
considered effective.
There were several limitations regarding the ade-
quacy of treatment including doses and duration of
trials. There were trials with no augmentation, augmen-
tation in part of the patients or in all patients.
Frequently the augmentation strategy varied across
subjects, possibly including bias. In few studies the
sample size was too small. The quality evaluation and
list of limitations were summarized in Table 1.
3.1. Randomized controlled double-blind trials
In the study from Hirschmann et al . [23]
pindolol
7.5 mg/day or placebo were added to fluoxetine
20 mg/day in a 4-week clinical trial. Patients on pindololand
fluoxetine had significant improvements in the
Panic Self-questionnaire (PSQ) (Cohen’s d = 2.72) and
Clinical Global Impression – Improvement scale
(CGI-I)
(Cohen’s d = 4.00), compared to patients taking fluox-
etine alone. There were significant improvements in
other panic and anxiety scales, but no difference
regarding depression symptoms. There were already
significant improvements in anxiety symptoms after
2 weeks of treatment.
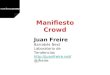
Records identified through database
searching
(n = 306)
S c r e e n i n g
I n c l u d e d
E l i g
i b i l i t y
I d e n t i f i c a t i o n
Additional records identified through
other sources
(n = 0)
Records after duplicates removed(n = 231)
Records screened
(n = 231)
Records excluded
(n = 193)
Full-text articles assessed for
eligibility
(n = 38)
Full-text articles excluded
Not clinical trial 09
Less than 10 PDpatients
07
Not treatment-
resistant patients
07
Retrospective study 02
Full-text not found 01
Not PD patients 01
Total
(n = 27)
Studies included in
qualitative synthesis
(n = 11)
Figure 1. PRISMA diagram of study identification and
selection process.
EXPERT OPINION ON PHARMACOTHERAPY 3
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
6/12
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
7/12
In the study from Simon et al . [22] patients
who
tolerated sertraline 100 mg/day or escitalopram
15 mg/day but did not achieve remission after
6 weeks of treatment with these drugs were included
in next phase of this study. In the second phase of the
same study, patients were randomized in double-blind
fashion either to receive a higher dose of selective
serotonin reuptake inhibitor (SSRI) or to remain in the
same dose. Both groups had a decrease in the Panic
Disorder Severity Scale (PDSS) scores, there were no
differences regarding other anxiety and depression
scales. The high SSRI dose group failed to show differ-
ences compared with the low dose group.Findings from these
studies are summarized in Table 2.
3.2. Open pharmacological trials
Among the five open pharmacological trials, three of
them were augmentation studies and there was con-
current use of antidepressants or benzodiazepines.
[24,25,28] Patients treated with aripiprazole, olanzapine
and divalproex sodium had significant improvements
regarding the PD symptoms. In the study from Baetz
et al . [24] only patients with comorbid mood
disorderand self-reported “mood instability” were
included.
Besides the improvement of anxiety and panic symp-
toms, there was also improvement of depressive and
mood instability symptoms.
Washout of previous medications was performed in
two open studies.[26,27] The noradrenaline reuptake inhi-
bitor (NRI) Reboxetine 2 – 8 mg/day and the
antipsychotic
olanzapine 2.5 – 20 mg/day were effective in
treatment–
resistant PD with no concurrent medications. There was
significant improvement in the panic attacks, anticipatory
anxiety agoraphobia, general anxiety and impairment.
Findings from these studies are summarized in
Table 3.
3.3. Cognitive-behavioral therapy studies
Four CBT trials [29–32] did not include comparisons to
placebo, wait list or other treatments. In one rando-
mized trial,[22] CBT and clonazepam were compared
as augmentation to SSRI and both treatments were
equally effective. All studies had limitations regarding
the treatment–
resistance criteria and concurrent use of multiple
pharmacological agents such as antidepres-
sants, benzodiazepines and lithium. ( Table 1)
All protocols [22,29–32] included 12 sessions of
group therapy. CBT was effective as an augmentation
in all five trials, with improvements in panic attacks,
anticipatory anxiety, agoraphobia, other panic symp-
toms, general anxiety and quality of life. A decrease in
the use of medications was also observed.[31,32] The
improvement of panic symptoms persisted for at least a
couple of months after the end of the CBT.[29] Findings
from these studies are summarized in Table 4.
4. Conclusion
Studies regarding the treatment of treatment–resistant
PD were scant, quality studies regarding this subject
were exiguous. Regarding the pharmacological treat-
ment there was preliminary evidence of efficacy in
treatment–resistant PD for monotherapy with reboxe-
tine and olanzapine. The augmentation of antidepres-
sants, anxiolytics and other drugs with CBT, pindolol,
Table 2. Randomized, controlled and double-blind clinical
trials.
Trial TRPD criteria
Number of patients
(completed) Drug Dose
Trialduration
(in weeks) Outcome Other information
Hirschmann et al . 2000 [23] Previous treatmentwith
at least twoantidepressantsand no responseafter a 8-week trialwith
fluoxetine
20 mg/day
26 (25) Fluoxetine +pindolol orfluoxetine +PBO
Fluoxetine20 mg/day;pindolol7.5 mg/day
4 Superior to PBO;significant differencesin PSQ (ES: 2.72),CGI-I
(ES: 4.00),HAM-A, CAS+PA andNIMH Anxiety Scale *
The clinical changesnoted with pindololwere evident by thesecond
week of thestudy
Simon et al . 2009 – phase II[22]
No response after6-week trial withsertraline (up to100 mg/day)
orescitalopram (upto 15 mg/day)
24 (19) Sertraline orescitalopramhigh dose orPBO (no
doseincrease)
High dose –sertraline 150– 200
mg/day;escitalopram20 – 30 mg/day
6 Not superior to PBO,no significantdifferences in CGI-S(ES:
0.16) and PDSS(ES: 0.01); significantimprovement in PDSSin both
groups **
CAS + PA: Clinical Anxiety Scale with panic attacks; CGI-I:
Clinical Global Impression – Improvement; ES: effect
size compared to placebo, Cohen’s d; HAM-A:Hamilton Rating Scale
for Anxiety; NIMH: National Institute of Mental Health; PBO:
Placebo; PDSS: Panic Disorder Severity Scale; PSQ: Panic
Self-Questionnaire; TRPD: Treatment–resistant panic disorder.
* Response and remission were not defined in this study.**
Remission status was defined as zero panic attacks for at least 1
week and a Clinical Global Impression – Severity score
of 1 or 2.
EXPERT OPINION ON PHARMACOTHERAPY 5
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
8/12
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
9/12
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
10/12
divalproex sodium, aripiprazole and olanzapine demon-
strated some efficacy. Dose escalation after initial
lack
of response produced little improvement or no
improvement at all. More randomized, controlled and
blind clinical trials are needed to ascertain adequate
strategies for treatment–resistant PD.
5. Expert opinion
The lifetime prevalence of PD in the population is
high,
[5,6] among these patients approximately 30% of them
have persistent panic symptoms despite pharmacologi-
cal and psychological treatment.[16,33] Improving the
treatments for PD and finding alternatives for patients
who do not respond to conventional treatments is a
matter of public health with crucial importance.
There is no consensus about the definition of treat-
ment–resistant PD and currently there are no opera-
tional criteria for classifying these patients. We opted
to accept all criteria for treatment–resistance, otherwisevery
few articles would be included in this review. The
authors believe that the best criteria for treatment–
resistant PD were those used by Dannon et al .
[26]
and Hollifield et al . [27]: not responding
to at least
two adequate 8-week treatment trials with drugs recog-
nized as effective for PD in adequate doses or standard
course of CBT. Patients who have poor response to the
first medication trial could respond very well in a sec-
ond trial. In addition, patients who take small doses
of
medication and have poor response after 6 weeks of
treatment could improve if the doses were increased
and the trial was prolonged. These patients cannot be
considered treatment–resistant.
Treatment–resistance in PD may be the consequence
of untreated comorbid disorders and patients could
benefit from treatments directed to the causes.
Patients with comorbid bipolar spectrum disorders
would probably benefit from mood stabilizers and anti-
psychotics. Switching the antidepressant –
including
tricyclic antidepressants (TCA) and monoamine oxidase
inhibitors (MAOI) in the treatment options – or
combin-
ing two antidepressants should be a good strategy for
patients with comorbid major depressive disorder.
Psychotherapy would probably be the best augmenta-
tion strategy for patients with treatment–resistant PD
and comorbid avoidant or dependent personality dis-
orders, agoraphobia or other phobias.
Antidepressants, particularly SSRI and serotonin, and
noradrenaline reuptake inhibitors (SNRI), are highly
recommended by current guidelines [2,11,12] among
the pharmacological agents used in the treatment of PD.
Due to their high efficacy and low risk of adverse reactions
the SSRI escitalopram, citalopram, sertraline, fluoxetine,
paroxetine, fluvoxamine and the SNRI venlafaxine have
the highest recommendation grades. The NRI reboxetine,
the MAOI phenelzine, and the TCA clomipramine, desi-
pramine, imipramine and lofepramine are efficacious, but
they have less favorable side-effects profile. Reboxetine,
moclobemide, duloxetine, milnacipran, nefazodone and
mirtazapine also have some evidence of efficacy in the
treatment of PD.[2,10] There is only one open study
withantidepressants for treatment–resistant PD patients and it
showed that these patients may benefit from augmenta-
tion with reboxetine.[26] Other strategies for treatment–
resistant PD with antidepressants such as switching the
antidepressant to TCA or MAOI, or combining two anti-
depressants are used in clinical practice but have not
been systematically studied. There is preliminary evidence
indicating that escitalopram and venlafaxine are more
effective in the treatment of PD than citalopram and
paroxetine, respectively.[2,13] These evidences make
these antidepressants good candidates as drugs to treat
treatment–resistant PD, but there are still no clinical
trialswith these drugs for treatment–resistant PD.
The benzodiazepines alprazolam, clonazepam, diaze-
pam and lorazepam are efficacious in acute treatment
of
PD, but have lower recommendation grades due to side
effects and risks.[2,11,12] Despite the fact that
benzodiaze-
pines are frequently combined to antidepressants in clin-
ical practice, there are no trials with benzodiazepines as
monotherapy or augmentation for treatment–resistant PD.
Atypical antipsychotics are not recommended by the
current guidelines [2,11,12] as first-line agents for the
treatment of PD, however, aripiprazole, olanzapine, ris-
peridone and sulpiride have demonstrated some efficacy
in this disorder.[10] Quetiapine showed anxiolytic prop-
erties in several studies and is used in mood disorders
with good results,[34,35] for this reason quetiapine is
also a promising agent for the treatment of PD and
treatment–resistant PD. The risks and benefits of atypical
antipsychotics should be weighted in treatment–resis-
tant PD patients because these agents are associated
to increased appetite, weight gain, metabolic abnormal-
ities, amenorrhea/galactorrhea, somnolence, sialorrhea,
sexual dysfunction, somnolence, blurred vision, head-
ache, dizziness, akathisia, insomnia, tremor and other
side effects.[10,36] Increased appetite, weight gain,
metabolic abnormalities and sexual dysfunction are asso-
ciated with both antidepressants and atypical antipsy-
chotics, combining these two compounds could increase
the risk of the mentioned side effects.
According to the guidelines the best treatments for
PD are pharmacological, psychological or a combina-
tion of both.[2] Among psychological treatments for PD
and treatment–resistant PD, CBT has the highest level
of evidence. In most protocols, there are 8 – 12
sessions
8 R. C. FREIRE ET AL.
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
11/12
once in a week, but shorter CBT programs with only five
sessions may also be effective if combined to the CBT
adjuvant D-cycloserine.[10] The CBT adjuvants are also
promising compounds for treatment–resistant PD.
The study of repetitive transcranial magnetic stimu-
lation and transcranial direct current stimulation had
significant developments in the last decade,[37,38]
and in the future, they may become effective treat-ments for PD,
including treatment–resistant PD.
Currently there are very few low quality studies
addressing the treatment–resistant PD, most of them
are open studies with very small samples of PD
patients. Well-designed, double-blind, randomized and
controlled studies with sufficient number of subjects
are needed to shed light on this subject.
Declaration of interest
Funding for this study was provided by the Brazilian Council
for Scientific and Technological Development (CNPq). RCFreire
has received support from the Brazilian Council for
Scientific and Technological Development (CNPq). A Nardi
has received support from the Brazilian Council for
Scientific
and Technological Development (CNPq). The authors have no
other relevant affiliations or financial involvement with
any
other organization or entity with a financial interest in or
financial conflict with the subject matter or materials dis-
cussed in the manuscript apart from those disclosed.
ORCID
Rafael C. Freire http://orcid.org/0000-0003-3875-4601
Bibliography
Papers of special note have been highlighted as either
of
interest (*) or of considerable interest (**) to readers.
1. Andrade LH, Wang YP, Andreoni S, et al. Mental disorders
in megacities: findings from the Sao Paulo megacity
mental health survey, Brazil. PloS One. 2012;7(2):e31879.
2. Baldwin DS, Anderson IM, Nutt DJ, et al. Evidence-based
pharmacological treatment of anxiety disorders, post-trau-
matic stress disorder and obsessive-compulsive disorder: a
revision of the 2005 guidelines from the British
Association for Psychopharmacology. J Psychopharmacol.
2014;28(5):403–439.
3. Andrade LH, Baptista MC, Alonso J, et al. Days
out-of-role
due to common physical and mental health problems:
results from the Sao Paulo Megacity Mental Health
Survey, Brazil. Clinics. 2013;68(11):1392–1399.
4. Lepine JP. Epidemiology, burden, and disability in
depres-
sion and anxiety. J Clin Psychiatry. 2001;62(Suppl 13):4–10.
5. Roy-Byrne PP, Stang P, Wittchen HU, et al. Lifetime
panic-
depression comorbidity in the National Comorbidity
Survey. Association with symptoms, impairment, course
and help-seeking. Br J Psychiatry. 2000;176:229–235.
6. Kessler RC, Chiu WT, Jin R, et al. The epidemiology
of
panic attacks, panic disorder, and agoraphobia in the
National Comorbidity Survey Replication. Arch Gen
Psychiatry. 2006;63(4):415–424.
7. Bystritsky A, Kerwin L, Niv N, et al. Clinical and
subthres-
hold panic disorder. Depress Anxiety. 2010;27(4):381–389.
8. Gorman JM, Kent JM, Sullivan GM, et al. Neuroanatomical
hypothesis of panic disorder, revised. Am J Psychiatry.
2000;157(4):493–505.
9. Nardi AE, Freire RC, Zin WA. Panic disorder and control
of
breathing. Respir Physiol Neurobiol. 2009;167(1):133–143.
10. Freire RC, Machado S, Arias-Carrion O, et al.
Currentpharmacological interventions in panic disorder. CNS
Neurol Disord Drug Targets. 2014;13(6):1057–1065.
11. Bandelow B, Zohar J, Hollander E, et al. World
Federation
of Societies of Biological Psychiatry (WFSBP) guidelines
for the pharmacological treatment of anxiety, obsessive-
compulsive and post-traumatic stress disorders - first
revision. World J Biol Psychiatry. 2008;9(4):248–312.
12. Katzman MA, Bleau P, Blier P, et al. Canadian clinical
practice guidelines for the management of anxiety, post-
traumatic stress and obsessive-compulsive disorders.
BMC Psychiatry. 2014;14(Suppl 1):S1.
13. Freire RC, Hallak JE, Crippa JA, et al. New treatment
options for panic disorder: clinical trials from 2000 to
2010. Expert Opin Pharmacother. 2011;12(9):1419–1428.
14. Bandelow B, Behnke K, Lenoir S, et al. Sertraline versus
paroxetine in the treatment of panic disorder: an acute,
double-blind noninferiority comparison. J Clin Psychiatry.
2004;65(3):405–413.
15. Kjernisted K, McIntosh D. Venlafaxine extended release
(XR) in the treatment of panic disorder. Ther Clin
Risk
Manag. 2007;3(1):59–69.
16. Batelaan NM, De Graaf R, Penninx BW, et al. The 2-year
prognosis of panic episodes in the general population.
Psychol Med. 2010;40(1):147–157.
17. American Psychiatric Association. Diagnostic and
statisti-
cal manual of mental disorders: DSM-III. 3d ed.
Washington (DC): American Psychiatric Association; 1980.18.
American Psychiatric Association. Diagnostic and statisti-
cal manual of mental disorders: DSM-III-R. 3rd ed.
Washington (DC): American Psychiatric Association; 1987.
19. American Psychiatric Association. Diagnostic and
statisti-
cal manual of mental disorders: DSM-IV. 4 ed.
Washington (DC): American Psychiatric Press; 1994.
20. American Psychiatric Association. Diagnostic and
statisti-
cal manual of mental disorders: DSM-5. 5th ed.
Washington (DC): American Psychiatric Association; 2013.
21. Moher D, Liberati A, Tetzlaff J, et al. Preferred
report-
ing items for systematic reviews and meta-analyses:
the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
22. Simon NM, Otto MW, Worthington JJ, et al. Next-step
strategies for panic disorder refractory to initial
pharma-cotherapy: a 3-phase randomized clinical trial. J Clin
Psychiatry. 2009;70(11):1563–1570.
** One of the two randomized controlled double-blind
clinical trials for treatment–resistant panic disorder
(phase II). Also includes the only head-to-head rando-
mized clinical trial for treatment resistant panic dis-
order (phase III).
23. Hirschmann S, Dannon PN, Iancu I, et al. Pindolol
augmen-
tation in patients with treatment-resistant panic disorder:
a double-blind, placebo-controlled trial. J Clin
Psychopharmacol. 2000;20(5):556–559.
EXPERT OPINION ON PHARMACOTHERAPY 9
http://orcid.org/0000-0003-3875-4601http://orcid.org/0000-0003-3875-4601
-
8/20/2019 Freire 2015 - Treatment-resistant PD Review
12/12
* One of the two randomized controlled double-blind
clinical trials for treatment–resistant panic disorder.
24. Baetz M, Bowen RC. Efficacy of divalproex sodium in
patients with panic disorder and mood instability who
have not responded to conventional therapy. Can J
Psychiatry. 1998;43(1):73–77.
25. Hoge EA, Worthington III JJ, Kaufman RE, et al.
Aripiprazole as augmentation treatment of refractory
generalized anxiety disorder and panic disorder. CNS
Spectr. 2008;13(6):522–527.
26. Dannon PN, Iancu I, Grunhaus L. The efficacy of rebox-
etine in the treatment-refractory patients with panic dis-
order: an open-label study. Hum Psychopharmacol.
2002;17(7):329–333.
27. Hollifield M, Thompson PM, Ruiz JE, et al. Potential
effec-
tiveness and safety of olanzapine in refractory panic
disorder. Depress Anxiety. 2005;21:33–40.
28. Sepede G, De Berardis D, Gambi F, et al. Olanzapine
augmentation in treatment-resistant panic disorder: a
12-week, fixed-dose, open-label trial. J Clin
Psychopharmacol. 2006;26(1):45–49.
29. Pollack MH, Otto MW, Kaspi SP, et al. Cognitive behavior
therapy for treatment-refractory panic disorder. J
ClinPsychiatry. 1994;55(5):200–205.
30. Heldt E, Blaya C, Isolan L, et al. Quality of life and
treat-
ment outcome in panic disorder: cognitive behavior
group therapy effects in patients refractory to medication
treatment. Psychother Psychosom. 2006;75(3):183–186.
31. Heldt E, Manfro GG, Kipper L, et al. One-year follow-up
of
pharmacotherapy-resistant patients with panic disorder
treated with cognitive-behavior therapy: outcome and pre-
dictors of remission. Behav Res Ther. 2006;44(5):657–665.
32. Heldt E, Manfro GG, Kipper L, et al. Treating
medication-
resistant panic disorder: predictors and outcome of cog-
nitive-behavior therapy in a Brazilian public hospital.
Psychother Psychosom. 2003;72(1):43–48.
33. Bandelow B, Rüther E. Treatment-resistant panic disor-
der. CNS Spectr. 2004;9(10):725–739.
34. Gao K, Wu R, Kemp DE, et al. Efficacy and safety
of
quetiapine-XR as monotherapy or adjunctive therapy toa mood
stabilizer in acute bipolar depression with gen-
eralized anxiety disorder and other comorbidities: a ran-
domized, placebo-controlled trial. J Clin Psychiatry.
2014;75(10):1062–1068.
35. Chen YC, Chen CK, Wang LJ. Quetiapine fumarate aug-
mentation for patients with a primary anxiety disorder or
a mood disorder: a pilot study. BMC Psychiatry.
2012;12:162.
36. Hershenberg R, Gros DF, Brawman-Mintzer O. Role of
atypical antipsychotics in the treatment of generalized
anxiety disorder. CNS Drugs. 2014;28(6):519–533.
37. George MS, Padberg F, Schlaepfer TE, et al. Controversy:
repetitive transcranial magnetic stimulation or transcra-
nial direct current stimulation shows efficacy in treating
psychiatric diseases (depression, mania, schizophrenia,
obsessive-complusive disorder, panic, posttraumatic
stress disorder). Brain Stimul. 2009;2(1):14–21.
38. Cristancho MA, Cristancho P, O’Reardon JP. Other ther-
apeutic psychiatric uses of superficial brain stimulation.
Handb Clin Neurol. 2013;116:415–422.
10 R. C. FREI RE ET AL.