Embed Size (px)
Citation preview

Free Radicals and HearingCause, Consequence, and Criteria
PATRICIA EVANSa,c AND BARRY HALLIWELL a,b
aInternational Antioxidant Research Centre, University of London King’s College,London SW3 6LX, UK
bDepartment of Biochemistry, National University of Singapore, Kent Ridge Crescent,Singapore 119260
ABSTRACT: Reactive oxygen and nitrogen species, including free radicals, areproduced in the human body in both health and disease. In health, they mayarise as regulatory mechanisms, intercellular signaling species, or as bacterioci-dal agents. Their production is normally controlled by the antioxidant defensemechanisms that include intracellular enzymes—for example, glutathione per-oxidase and superoxide dismutase—and low molecular-mass compounds suchas vitamin E or ascorbic acid. Although repair mechanisms exist, some steady-state basal oxidative damage occurs in all individuals.
Oxidative stress arises when there is a marked imbalance between the pro-duction and removal of reactive oxygen and nitrogen species. This may originatefrom an overproduction of these substances or from a depletion in the antioxi-dant defenses. Certain drugs may induce oxidative stress by forming drug-de-rived radicals that can not only deplete the antioxidant defenses but can also re-act directly with biomolecules. To be able to assess whether oxidative stress isoccurring in a particular tissue, reliable biomarkers of oxidative damage are re-quired. Since oxidative stress can damage all major biomolecules in vitro andprobably in vivo, biomarkers for DNA, protein, and lipid damage are being de-veloped which, when taken with an assessment of the antioxidant status of theindividual, will allow evaluation of the involvement of oxidative stress in the eti-ology of disease and in the side effects of drugs. There is some evidence to sug-gest that free radical-mediated damage may be involved in the ototoxicity ofaminoglycosides and cisplatin derivatives. Whether this is a cause or conse-quence of the toxic insult to the sensory hair cells of the inner ear remains to bedetermined.
WHAT IS A FREE RADICAL?
A free radical is any atom, molecule, or ion that contains one or more unpairedelectrons. The unpaired electron in a free radical is denoted by a superscript dot afterthe chemical formula or atomic symbol (TABLE 1). Since pairing of electrons in or-bitals represents a lower energy state than the same electrons unpaired, free radicalsare usually more reactive than their parent species. Nevertheless, chemical reactivityof radicals varies enormously.
19
cTo whom correspondence may be addressed. Phone: +44 171 333 4784/4735; fax: +44 171333 4949; e-mail: [email protected]

ANNALS NEW YORK ACADEMY OF SCIENCES20
In healthy cells and tissues, any free radicals generated are likely to encounter andreact with nonradicals since most cellular constituents are nonradicals and thechances of most radicals meeting are low. Such encounters often (depending on thereactivity of the free radical) perpetuate free radicals in reactions of the type:
X· + HY � HX + Y·or,
X· + Y � [X-Y]·
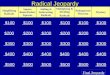
For this reason, free radicals can act as initiators and propagators of chain reactions.One biological example of a free-radical chain reaction is lipid peroxidation, outlinedin FIGURE 1; another is the addition of hydroxyl radical to the DNA base guanine tomake the 8-hydroxyguanine radical.
WHICH RADICALS ARE MADE IN THE HUMAN BODY?
Many free radicals are produced by the body (some examples are shown in TABLE
1). Superoxide (O2· –) is produced by a one-electron addition to molecular oxygen
TABLE 1. Reactive oxygen and nitrogen speciesa produced in the human body
Reactive oxygen speciesb
Radicals Nonradicals
Superoxide, O2· – Hydrogen peroxide, H2O2
Hydroxyl, ·OH Hypochlorous acid, HOClPeroxyl, RO2· Ozone, O3
Alkoxyl, RO· Singlet oxygen, 1�gHydroperoxyl, HO2· Hypobromous acid, HOBr
Reactive nitrogen speciesc
Nitric oxide, NO Nitrous acid, HNO2
Nitrogen dioxide, NO2 Nitrosyl cation, NO+
Nitroxyl anion, NO–
Dinitrogen tetroxide, N2O4
Dinitrogen trioxide, N2O3
Peroxynitrite,d ONOO–
Nitronium cation, NO2+
Nitryl chloride, NO2ClAlkyl peroxynitrates, ROONO–
aThese species have widely varying reactivities: ·OH reacts rapidly with almost everything,whereas H2O2, O2
·–, NO· only react quickly with a few molecules. RO2·, RO·, HOCl, HOBr, NO2Cl,NO2·, ONOO–, and O3 have intermediate reactivities.
bROS is a collective term that includes both oxygen radicals and certain nonradicals that are oxi-dizing agents and/or are easily converted into radicals.
cRNS includes both nitrogen-containing radicals and nonradicals.dPeroxynitrite can be regarded as an ROS or RNS.

and is generated by activated phagocytes such as neutrophils, monocytes,macrophages, and eosinophils as part of the mechanism by which they kill foreigninvaders.1 These cells also generate H2O2 from O2
· – in this process. H2O2 does notcontain unpaired electrons and is therefore not a free radical. However, it is groupedwith free radicals in a collection of substances produced by the body that are looselytermed reactive oxygen species (ROS; TABLE 1). Overproduction of O2
· – and H2O2 inchronic inflammatory conditions such as rheumatoid arthritis2 and inflammatorybowel disease3 causes tissue damage. Furthermore, certain drugs and toxins (e.g.,phenylhydrazine, anthracyclines, and paraquat4) may generate these substances invivo.
Superoxide is also produced during oxidative phosphorylation in aerobic cells,when electrons “leak” from the electron transport chain onto molecular oxygen.5
Other “chemical accidents” also produce superoxide, including auto-oxidation ofsuch biomolecules as catecholamines and hemoglobin. Over 2 kg of superoxide maybe produced per year in the body; athletes and people with chronic infections gener-ate much more.4
NO· is another free radical, with multiple physiological functions.6 It was firstidentified as endothelial-derived relaxing factor,7 but is also produced by many othercell types in the human body. Excess NO· can be harmful; for example, it can com-bine with superoxide to generate peroxynitrite (ONOO–), which forms the toxic per-oxynitrous acid at pH 7.4.8 NO· and ONOO– are examples of reactive nitrogenspecies (RNS); other examples are given in TABLE 1.
Evidence is accumulating that nonphagocytic cell types such as lymphocytes,9 fi-broblasts,10 vascular endothelial cells,11 and cancer cells12 can also produce O2
·–. Anarea currently being explored is the ability of ROS and reactive nitrogen species(RNS) such as O2
· – and NO· to act as intercellular signaling and growth-regulatingagents.13 They have also been implicated in regulation of gene expression.13,14
Superoxide, H2O2 and NO· are not particularly reactive.4,15 They may cause somedamage in vitro; for example, O2
· – inactivates aconitase16 and excess NO· can dam-age iron-sulphur proteins.6 Excess vascular O2
· – production can lead to hypertensionand is implicated in the development of atherosclerosis.17 Peroxynitrite, and productsderived from it, can oxidize protein sulphydryl groups,8,18 nitrate proteins,19 andmodify DNA bases.20 H2O2 is another poorly reactive oxygen species that can oxi-dize sulphydryl groups in some proteins at concentrations >50 �M.21 Many of thesespecies have important functions in the body, but their overproduction can lead to tis-sue damage and cell death.
In 1970, Beauchamp and Fridovich22 proposed that the toxicity of O2· – and H2O2
in vivo might relate to their conversion into the powerfully reactive hydroxyl radical.Transition metal ions such as iron and copper can catalyze this conversion:
Fe2+ + H2O2 � Fe3+ + OH– + ·OH (the Fenton reaction).
O2· – converts Fe3+ into Fe2+, and so recycles the Fe:23
O2· – +Fe3+ � O2 + Fe2+.
It can also contribute to the release of metal ions from such proteins as aconitase16
EVANS & HALLIWELL: FREE RADICALS 21

ANNALS NEW YORK ACADEMY OF SCIENCES22
and ferritin,4 providing the transition metals to act as catalysts in converting poorlyreactive species into more damaging forms. In lipid peroxidation, for example, tran-sition metals catalyze breakdown of lipid peroxides into alkoxyl and peroxyl radi-cals,23 which are excellent propagators of the chain reaction (FIG. 1).
The hydroxyl radical (·OH) is one of the most damaging radicals known and willreact immediately with any substance at or close to its site of generation. If transitionmetal ions are bound to DNA and ·OH is generated from H2O2 as previously, then allfour DNA bases should be modified in a characteristic pattern.24 Indeed, cells treatedwith H2O2 show these base modifications.25,26 If metal ions catalytic for ·OH forma-tion are bound to membranes, then lipid peroxidation will be the resultant damage.The extreme reactivity of ·OH gives rise to these site-specific reactions that will oc-cur wherever there are bound transition metal ions in contact with peroxides such asH2O2.
Some other cellular reactions generate ·OH. Since cells are predominantly com-posed of water, ·OH is produced in cells subjected to ionizing radiation, whichcleaves water:27
H2O � ·OH + H·.
FIGURE 1. An outline of lipid peroxidation.

EVANS & HALLIWELL: FREE RADICALS 23
Peroxynitrite also decomposes to give a species that may be ·OH:28
ONOO– + H+ � ONOOH � NO2. + ·OH
and some ·OH may be produced when hypochlorous acid, produced as part of the“killing” mechanism of activated neutrophils, reacts with29 O2
· –:
O2· – + HOCl � ·OH + O2 + Cl–.
ANTIOXIDANT DEFENSES
To counter the harmful effects of ROS/RNS produced in the body, defense mech-anisms have evolved to detoxify or scavenge radicals and other reactive species.These consist of enzymes, which are mostly intracellular, and low-molecular-massantioxidants, which are located both inside and outside the cell (TABLE 2).
Superoxide dismutase5 (SOD) catalyzes the dismutation of O2· – into H2O2, and is
mainly an intracellular enzyme found in two major forms in animals, one specific tothe cytosol (CuZnSOD) and the other to mitochondria (MnSOD). Some extracellularSOD (EC-SOD), a CuZnSOD, does occur, but may exist largely bound to endothelialcell surfaces in vivo.30 The severe consequences of MnSOD “knockout” in transgenicanimals shows how important MnSOD is in removing O2
· – generated by mitochon-dria in vivo.31 Because SOD enzymes generate H2O2, they work in conjunction withthe H2O2-removing enzymes,32 the most important of which are thought to be the se-
TABLE 2. Antioxidant defenses: A summary
Enzymes (mainly intracellular) removing O2·– and H2O2
Superoxide dismutase: 2O2· – + 2H+ � H2O2 + O2
Glutathione peroxidase:a 2GSH + H2O2 � GSSG + 2H2OGlutathione reductase: GSSG + NAPDH + H+ � 2GSH + NADP+
Catalase (mostly located in peroxisomes): 2H2O2 � 2H2O +O2
Low-molecular-mass antioxidants (intra- and extracellular)
Glutathione: Scavenges ·OH, singlet oxygen, HOCl, ONOO–, RO·, RO2·Ascorbic acid: Reducing agent that reacts with O2
· –, ·OH, HO2·, HOCl, ONOO–, RO·, RO2·,and singlet oxygen. May detoxify other radicals by reducing them
�-Tocopherol: Terminates chain reaction of lipid peroxidation, thought to be recycled byascorbic acid or ubiquinol
Uric acid: Scavenges singlet oxygen, ·OH, HOCl, O3, ONOO–, and peroxyl radicals. Urate radical may be recycled by ascorbate
Protection by sequestration of transition metal ions
Plasma transferrin (Fe3+), ferritin (Fe3+), caeruloplasmin (Cu2+), intracellular metallothioneins (Zn2+, Cu+, Cd2+, Hg2+)
aAlso destroys fatty acid hydroperoxides.

lenoprotein glutathione peroxidases (TABLE 2), although the importance of thiore-doxin-linked peroxide removal systems is now being appreciated.33
LOW-MOLECULAR-MASS ANTIOXIDANTS
These are scavengers of radicals and other reactive species. Glutathione (GSH)can scavenge certain free radicals and other ROS, for example, HOCl and ONOO–,directly,4,36 as well as being a substrate for glutathione peroxidase and several otherenzymes. It is found at millimolar concentrations in all human cells, but only in traceamounts in plasma (1–5 �M) and most other body fluids.34 Fluids of the lower respi-ratory tract are richer in GSH (50–200 �M), where it may help remove inhaled toxins(e.g., oxides of nitrogen and sulphur from vehicle exhaust fumes, tobacco smoke, andROS/RNS, especially ONOO– and HOCl produced by activation of lung phago-cytes).34
Ascorbic acid (vitamin C) is also a good scavenger of some ROS35 and ofONOO–.36 The reducing properties of ascorbate mean that it can reduce Fe3+ ions toprovide Fe2+ for the Fenton reaction described earlier, that is, it could theoreticallyhave a damaging prooxidant rather than an antioxidant role if free transition metalions are present.35 Under normal circumstances, there is very little transition metalion available (see below) and the antioxidant effects of ascorbate are thought to pre-dominate.37,38
�-Tocopherol is located intra- and extracellularly occurring in membranes andlipoproteins. It scavenges peroxyl radical intermediates in lipid peroxidation,39 and isconverted to a less reactive tocopheryl radical that can be recycled back to �-toco-pherol by ascorbate40 and ubiquinol in vivo (TABLE 2).
Uric acid is the end product of purine degradation and is present at about 0.2–0.4mmol/L in human body fluids. It scavenges several ROS/RNS41 to generate variousproducts, including allantoin and parabanic acid, although some of the products ofurate oxidation may themselves be damaging.36 Some dietary antioxidants, for exam-ple, plant flavonoids and polyphenolics, may also have protective qualities in the gas-trointestinal tract, and evidence for their absorption, to a limited extent, is growing.42
A diet rich in fruits, vegetables, nuts, and grains appears protective against severalhuman diseases, probably for multiple reasons,43 one of which is thought to be theantioxidants present.
SEQUESTRATION OF TRANSITION METALS
“Free” transition metal ions would be hazardous in tissues and body fluids due totheir ability to catalyze the conversion of fairly unreactive substances such as H2O2
into highly damaging species such as ·OH. It is only in disease states such as fulmi-nant hepatic failure and hemochromatosis that such metal ions become available inquantities sufficient to cause tissue damage.44,45 Normally these ions are sequesteredin proteins where they are unable to act as catalysts. Iron is stored in the protein fer-ritin and transported bound to plasma transferrin. Copper occurs in plasma on ceru-loplasmin. None of these protein-bound forms of transition metals is able to catalyze
ANNALS NEW YORK ACADEMY OF SCIENCES24

EVANS & HALLIWELL: FREE RADICALS 25
Fenton-type reactions.23,46 A small amount of iron can be mobilized from ferritin byO2
· –, but this probably represents iron in the channels of ferritin through which ironis taken into and released from the protein as part of its physiological function tostore and sequester iron,47 that is, O2
· – apparently cannot release iron safely stored inthe ferritin core. Heme proteins such as hemo- and myoglobin contain iron in a lessprotected form since they react with H2O2 to produce oxidizing species (ferryl-hemo/myoglobin and protein radicals) that can initiate such processes as lipid perox-idation48–50 and interact with some drugs to produce drug-derived radicals.51 WhenH2O2 is in large excess over the protein, both heme and iron are released.52
OXIDATIVE STRESS
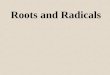
Despite all these lines of defense, some free-radical-related damage still occurs.End products of lipid peroxidation (e.g., lipid hydroperoxides, aldehydes such asmalondialdehyde, hydrocarbon gases, and the F2-isoprostanes53–55) and of free-radi-cal attack on urate41 are present in vivo. Some 8-hydroxydeoxyguanosine derivedfrom oxidation of guanine residues in DNA is always present in cellular DNA, as areseveral other base oxidation products.56 DNA damage is rapidly repaired and some 8-hydroxydeoxyguanosine is excreted in normal human urine.57 TABLE 3 shows a sum-mary of repair mechanisms. Proteins damaged by free-radical attack are usually de-graded more rapidly58 than normal proteins, but nevertheless protein carbonyls fromdamaged amino acid side chains can be detected in vivo.58,59 These and other obser-vations provide evidence for on-going oxidative damage in the human body, even inhealthy individuals (summarized in FIG. 2). Indeed, it has been suggested that the ag-ing process involves the cumulative effects of free-radical damage.60 Why have an-tioxidant defense mechanisms not evolved to an extent that eliminates oxidative dam-age? Presumably deployment of some free radicals such as O2
· – and NO· for usefulpurposes, for example, as protective and regulatory mechanisms, has ensured thattheir removal by the antioxidant defenses is never complete. The body may thereforetolerate a basal level of oxidative damage as payment for its use of radicals, andhence has evolved repair systems, which even then do not instantly remove all thedamaged biomolecules.
A severe disturbance in the balance between production of ROS and the antioxi-dant defenses results in oxidative stress61 (FIG. 3). This can arise through antioxidantdepletion, for example, in severe malnutrition involving inadequate dietary intakes of�-tocopherol, ascorbic acid, amino acids needed to synthesize glutathione, or ri-boflavin required to manufacture the flavin adenine dinucleotide (FAD) cofactor ofglutathione reductase. An overproduction of ROS could also overwhelm the antioxi-dant defenses, even if these are replete, to result in oxidative stress. The latter proba-bly occurs in chronic inflammatory conditions such as inflammatory bowel diseaseand rheumatoid arthritis.2 It may also occur in ischemia-reperfusion injury, whichcontributes to tissue damage in coronary and cerebral thrombosis, rheumatoid arthri-tis, crush injury, organ transplantation, and bypass surgery.4 Hypoxia/ischemia caus-es adenosine triphosphate (ATP) depletion, generating hypoxanthine,62 and activatingCa2+-dependent proteases such as calpain (FIG. 4). These may convert any xanthinedehydrogenase present in the tissue to xanthine oxidase, capable of producing O2
· –

ANNALS NEW YORK ACADEMY OF SCIENCES26
TABLE 3. Repair of oxidative damage
Site of damage Repair system
DNA: All components can beattacked by ·OH, HNO2,ONOO–, HOCl damages bases
Methionine sulphoxide reductaserepairs oxidized methionine residues.Damaged proteins may be recognizedand preferentially degraded by theproteasome complex
A wide range of enzymes removesabnormalities in DNA, by excision,resynthesis, and strand rejoining
Proteins: Many ROS attack -SHgroups, ·OH modifies manyamino acid residues
Lipids: Some ROS and RNS caninitiate lipid peroxidation
Chain-breaking antioxidants removechain-propagating peroxyl radicals.Phospholipid hydroperoxide glutathioneperoxidase/some phospholipases canremove peroxides from membranes.Damaged lipids may be released frommembranes
FIGURE 2. Steady-state oxidative damage.

and H2O2, which can be converted to ·OH if any transition metal ions are present.Such metals may be released from sequestered sites in hypoxic tissue63 as a result ofcell death by necrosis in injured tissue. On reperfusion, the increased flux of oxygengenerates more O2
· – and H2O2, which may result in further tissue damage.62
Another mechanism that may contribute to nervous tissue injury after hypoxia/is-chemia is the generation within the tissue of excitatory neurotransmitters such as glu-tamate or aspartate released due to depolarization following energy loss, and that aretoxic to other neurones. Dykens et al.64 reported that the synthetic excitatory neuro-toxin kainic acid caused the death of cultured mouse cerebellar neurones that couldbe prevented by pretreating the cells with allopurinol (an inhibitor of xanthine oxi-dase) or by adding SOD plus catalase to the culture medium. Excitotoxin-inducedneuronal damage in rodents may involve O2
· – generated by xanthine oxidase as it ox-idizes accumulated hypoxanthine from ATP degradation during repeated “firing” ofneuronal cells.64 Two apparently different mechanisms of injury duringischemia/reperfusion may therefore be linked: free-radical reactions and the genera-tion of excitatory amino acids. Some studies65 also show NO· to be involved.
Certain toxins (e.g., paraquat) and drugs4 are metabolized to ROS, which can alsooverwhelm the antioxidant defenses and some drugs (e.g., paracetamol4) can deplete
EVANS & HALLIWELL: FREE RADICALS 27
FIGURE 3. The balance between ROS/RNS production and the antioxidant defenses.

the antioxidant defenses after activation by the cytochrome P450 system, causing ox-idative stress.
Cells can tolerate mild oxidative stress by upregulating the synthesis of antioxi-dant defense systems,66 but severe oxidative stress produces major disruption of cellmetabolism (FIG. 5), including DNA strand breakage and base modification, rises inintracellular “free” Ca2+ and activation of nucleases and cNOS (Ca2+-calmodulin reg-ulated), damage to membrane ion transporters and receptors, and lipid peroxida-tion.2,67,68 Such cell derangement can lead to release of transition metal ions fromproteins within the cell, such as loss of Fe2+ from mitochondria, which is able to pro-mote ·OH formation. Cell death may occur either as necrosis or apoptosis; the latterprocess can intimately involve ROS,12 although ROS are not essential for apoptosisto occur.69 Necrotic cell death can release prooxidants, for example, iron, which arepotentially able to spread free-radical damage to surrounding cells.70
THE ROLE OF OXIDATIVE STRESS IN HUMAN DISEASE
Most human diseases involve tissue damage that will inevitably be accompaniedby a local oxidative stress, which might exacerbate the damage. The oxidative stresswill be a secondary, but not necessarily unimportant, event. Its importance varies in
ANNALS NEW YORK ACADEMY OF SCIENCES28
FIGURE 4. Ischaemia-reperfusion injury: summary of a proposed mechanism that may oper-ate in tissues containing xanthine dehydrogenase.

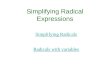
different disease states. Oxidative modification of lipids is a significant factor in thedevelopment of atherosclerosis,71 and there is significant oxidative damage to allclasses of biomolecule in the rheumatoid joint in rheumatoid arthritis.72 Cancer maysometimes originate in oxidative DNA damage.73 Rather than simply demonstratingoxidative stress, it is important to establish whether the oxidative stress that in-evitably accompanies human disease makes a significant contribution to the diseaseactivity. To assess oxidative stress, affected tissues can be screened for the presenceof “biomarkers” of attack of ROS/RNS upon biomolecules (FIG. 6). The developmentof accurate and sensitive assays for these biomarkers is currently one of the mostchallenging areas in the medical free-radical field.74
Reliable markers for DNA damage are the presence and concentration withinDNA of modified bases. All four DNA bases are damaged by ·OH attacks on DNA togive a characteristic spectrum of modified bases that can be detected and determinedby gas chromatography–mass spectrometry.75 Peroxynitrite reaction with DNA leadsto a different pattern of base damage, resulting in conversion of purine bases to hy-poxanthine, xanthine, and 8-nitroguanine.20 Thus the pattern of damage shown cangive an indication of the reactive species causing the damage.
Proteins are modified by ROS/RNS in a number of ways, which include conver-sion of certain amino acid side chains to carbonyl groups76 that can be assayed by de-
EVANS & HALLIWELL: FREE RADICALS 29
FIGURE 5. Damage to major biomolecules as a result of oxidative stress.

FIG
UR
E 6
.B
iom
arke
rs o
f ox
idat
ive
stre
ss a
nd th
eir
met
hods
of
mea
sure
men
t.

EVANS & HALLIWELL: FREE RADICALS 31
rivatizing these groups with dinitrophenylhydrazine to form the yellow chromogendinitrophenylhydrazone, which can be determined colorimetrically and by othermethods. Reactive nitrogen species such as peroxynitrite induce nitration of proteintyrosine groups to give nitrotyrosine residues that can be quantitated by several meth-ods including ELISA techniques77 and Western blotting.78 Products of the oxidationof specific amino acids such as 2-oxohistidine and methionine sulphoxide can be de-tected by high-performance liquid chromatography (HPLC),79 and the amino acidphenylalanine has been used to detect the presence of ·OH in vitro and in vivo, be-cause an attack of ·OH on phenylalanine forms ortho- and meta- isomers of tyrosinethat can be easily separated from the normal para-isomer by HPLC.80
Several methods have been used to estimate the degree of lipid peroxidation in tis-sues and body fluids.23 Measurement of lipid hydroperoxides81 is probably the bestgeneral technique in practice at present, since other methods, such as malondialde-hyde (MDA) measurements, assume malondialdehyde to be a major end product ofperoxidation, which is not always the case.82 Malondialdehyde may also arise as aproduct of free-radical attack on certain carbohydrates such as deoxyribose.23 Sever-al types of end product may result from peroxidation, including hydrocarbon gasesand cytotoxic unsaturated aldehydes such as 4-hydroxynonenal.23,82 Lipid hydroper-oxides represent an early common stage in the peroxidative process (FIG. 1) fromwhich other products, such as MDA and other aldehydes, can arise, and may there-fore be a more reliable index. Recently mass spectrometric assays for isoprostaneshave been developed that look promising for the future.54–56,83 Isoprostanes are endproducts of the nonenzymic peroxidation of lipids such as arachidonic acid. Specificisoprostane end products arise from arachidonic acid, eicosapentaenoic acid, and do-decahexaenoic acid, and hence the type of lipid being attacked can be determined.74
Looking at the effects of oxidative damage is only one aspect of assessment of ox-idative stress. It is now possible to determine the antioxidant status of tissues in termsof their glutathione,84 ascorbate,56 uric acid,41 and �-tocopherol content,85 as well asassaying for the enzymic activities of SOD,5 catalase,85 and glutathione peroxidase.32
Hence an assessment can be made of the state of the antioxidant defenses, and mayreveal valuable information on any specific depletion in antioxidants. It is importantto determine all antioxidants because the relative content of antioxidants varies indifferent tissues and body fluids, and the rate and order of their depletion may alsodiffer in various tissues. Glutathione appears to be depleted early in the substantia ni-gra in Parkinson’s disease,84 but patterns of antioxidant depletion are likely to be tis-sue and disease variable.
Overall consideration of the presence and level of biomarkers and the antioxidantstatus of the tissue will provide important information on the role of free radicals andother reactive species in the disease process. Information of this type has been usedto implicate free radicals in several major human diseases such as atherosclerosis71
and rheumatoid arthritis.2 It is possible in the future that the antioxidant status of anindividual could be part of an overall consideration of the risk factors involved forcontracting diseases involving a high element of oxidative stress. Individuals whoseantioxidant status is deficient through poor diet or cigarette smoking may be moresusceptible to a variety of diseases or may suffer them more severely than individualswho are antioxidant replete. This may also be an important factor to consider in as-sessing the side effects of certain drugs.

It is possible that genetic variations exist in the rates of free-radical production,the antioxidant defenses and repair systems, and the ability to utilize dietary antioxi-dants.86 An extreme example is inborn deficiency in �-tocopherol transfer protein87
and polymorphisms in DNA repair enzymes are well-established. There is a widevariation in steady-state levels of oxidative damage in healthy human subjects withcomparable plasma levels of dietary antioxidants.86
INTERACTION OF DRUGS WITH REACTIVE OXYGEN SPECIES
Drugs, if present to a significant concentration in tissues, may scavenge free radi-cals as a “gratuitous activity.”88 This may improve the overall drug performance byadding an additional protective function to the drug. However, the interaction ofdrugs with free radicals must lead to the formation of drug-derived radicals, anddrugs will only be protective if these radicals are less damaging than the radical withwhich they interacted.88 This may not be the case for some drugs such as phenyl bu-tazone, which reaches relatively high peak plasma concentrations (0.5 mM)89 andmay form a drug-derived radical on reaction with heme protein/H2O2 systems or·OH, which potentiates tissue damage. Such damage may be responsible for the seri-ous side effects associated with use of this drug in rheumatoid arthritis.
A drug may only scavenge free radicals if its concentration is sufficient to allow itto compete with endogenous antioxidants. Some body fluids are richer in antioxidantprotection (e.g., blood plasma) than others (for instance, cerebrospinal fluid).46 Weobtain several compounds (vitamins C and E, possibly carotenoids and related com-pounds, plant flavonoids, and phenolics) from a healthy diet that act (or may act) todiminish oxidative damage in vivo. Suboptimal antioxidant defenses are likely tomake the effects of drug-derived radicals worse, as there will be fewer antioxidantsavailable, which increases the likelihood of radicals reacting with the drug. Ascorbicacid obviates lipid peroxidation induced by phenylbutazone in the presence of hemeproteins and H2O2.51 Rheumatoid arthritis sufferers who have subnormal plasmaascorbate levels90 are particularly prone to side effects with phenylbutazone, whichled to withdrawal of the use of the drug for this disease.
Tetracycline antibiotics and the floxins are sensitizers of singlet-oxygen forma-tion.4 They absorb visible radiation and transfer the energy of this radiation to oxy-gen, converting it to an activated form (singlet oxygen, not a free radical), which cancause damage. Tetracyclines also form chelates with metal ions that can generate·OH from H2O2. They are, however, powerful scavengers of HOCl, an oxidant pro-duced by neutrophil myeloperoxidase, and ONOO–. Effects of these drugs at sites ofinflammation will therefore be complicated4 and also depend on the state of the en-dogenous antioxidant defenses and the products generated when the drug interactswith ROS/RNS. Thus effects of such antibiotics can be exerted by mechanisms otherthan antibacterial activity.
The aminoglycosides are another group of antibiotics that is effective againstmany aerobic gram-negative and some gram-positive bacteria. Members of the groupare closely related in structure, activity, pharmacokinetic characteristics, and toxicity.Aminglycoside side effects include nephro- and ototoxicity. Cochlear tissue containssignificant levels of SOD, catalase, glutathione peroxidase, and glutathione-S-trans-
ANNALS NEW YORK ACADEMY OF SCIENCES32

ferase,91–95 which suggests that this part of the inner ear (like all body tissues) re-quires antioxidant protection. Various reports document the positive and negative ef-fects of free-radical scavengers96,97 and agents thought to decrease intracellular glu-tathione levels in the cochlea98 on gentamycin toxicity. The method of applicationand degree of tissue penetration of such substances will obviously influence the pos-sible outcome. Iron chelators protect against gentamycin-induced hearing loss inguinea pigs,99 which suggests that gentamycin may exert its ototoxic effects throughrecruiting iron into a catalytic iron complex, which has been shown to induce arachi-donic acid peroxidation in vitro.100 Iron-loaded rats have a greater susceptibility togentamycin-induced nephrotoxicity supporting a role for iron in gentamycin-inducedkidney damage.101 Gentamycin is able to enter the vulnerable hair cells of thecochlea, and it is likely that its toxic effects originate from inside the cell rather thanat the cell membrane. Cationic aminoglycosides bind to phospholipids on the cellmembrane and are internalized by endocytosis,102 leading to the formation ofmyeloid bodies. These are lysosomes filled with phospholipid complexes resistant todegradation, as aminoglycoside binding to phospholipid inhibits the action of lysoso-mal phospholipases.102 Aminoglycoside-induced nephrotoxicity is inhibited both invitro and in vivo by polyaspartic acid, which prevents the aminoglycosides from bind-ing to the phospholipids.103,104
An interesting finding is that the severity of ototoxicity is inversely correlatedwith tissue glutathione concentrations in guinea pigs, and dietary glutathione may beprotective.105,106 This may mean that humans with dietary deficiencies in sulphur-containing amino acids, for example, cysteine and methionine, may be more at riskof incurring side effects of these drugs. The increasing use of relatively inexpensiveamino glycosides in poorer countries makes this a cause for concern. Nephrotoxicityis almost completely attenuated by iron chelators such as desferrioxamine,107 whichreduces lipid peroxidation in the kidney, although dietary vitamin E supplementationprior to gentamycin administration does not arrest renal impairment,108 suggestingthat lipid peroxidation is a by-product of another tissue insult (involving iron) bygentamycin in the kidney.
Aminoglycosides also have an excitotoxic effect on the auditory neurones, sincetheir effects can be abrogated by NMDA antagonists.109 Excitotoxins may injure cellsby reducing cellular ATP levels, leading to a scenario similar to that of damage by is-chemia/reperfusion injury (see earlier).4 Noise-induced cochlear damage could in-volve similar mechanisms with episodes of ischemia/reperfusion in the strial vesselssupplying the inner and outer hair cells and neurones.110,111 Iron chelation has beenreported to attenuate neomycin ototoxicity in guinea pigs,112 and iron administrationaggravated gentamycin-induced ototoxicity.113
Other drugs with ototoxic side effects include platinum derivatives such as cis-platin and carboplatin used in certain chemotherapy regimes. The mechanism ofthese drugs is thought to involve intercalation of the drug into the DNA double helixand cross-linkage of bases to irreversibly damage DNA, preventing it from uncoilingfor replication and transcription and thus causing cell death. Because the DNA ismore exposed in tumour cells due to their rate of division and metabolism, tumour-cell DNA is more susceptible to damage, although many different cell types are dam-aged by these cytotoxic drugs. cis-Platin forms aqueous complexes, exchanging itschloride ions for water molecules and thus increasing cellular chloride content. Little
EVANS & HALLIWELL: FREE RADICALS 33

is known about the mechanisms involved in cis-platin ototoxicity, but the primary ef-fect may be depletion of glutathione and binding of the drug to essential proteinsthrough protein sulphydryl groups.114 An effect on lipids is doubtful since cis-platincould not induce lipid peroxidation in rat kidney microsomes containing a nico-tinamide-adenine-dinucleotide-generating system (NADPH).115 Campbell et al.116
have shown that D-methionine may protect against cis-platin induced ototoxicity. L-Methionine is a good scavenger of ROS, such as HOCl and ONOO–,117 but the mech-anism of protection by D-methionine is unclear. Lipoic acid, a powerful scavenger ofROS/RNS118,119 and an agent able to raise GSH levels may be a substance worth fur-ther investigation.120
Cochlear damage following certain acoustic overstimulation and toxin exposurehas many similarities (e.g., pathology, implication of ROS116) that may result fromrelated underlying mechanisms. Finding out why the cochlea, and particularly thehair cells, are so vulnerable would provide valuable insights into possible therapeuticmeasures to prevent cochlear damage.
The beneficial effects of dietary fruits, grains, and vegetables are reflected inprevention or delay in onset of the major diseases—cardiovascular disease and can-cer. Such diets may also protect us at least in part from side effects of drugs andtoxins, with individuals with suboptimal antioxidant levels more at risk of develop-ing side effects. Apart from publicizing the beneficial effects of diets high in natur-al antioxidants to improve overall community health, coadministration of antioxi-dants with drugs known to cause oxidative stress remains a possibility for the fu-ture. For ototoxic side effects of drugs, the site and metabolic nature of the lesionwithin the hair cells of the cochlea or the endolymph surrounding the cells remainto be established.
REFERENCES
1. BABIOR, B. M. & R. C. WOODMAN. 1990. Chronic granulomatous disease. Semin. Hematol.27: 247–259.
2. HALLIWELL, B., J. M. C. GUTTERIDGE & C. E. CROSS. 1992. Free radicals, antioxidants andhuman disease: Where are we now? J. Lab. Clin. Med. 119: 598–620.
3. GRISHAM, M. B. 1993. Role of reactive oxygen metabolites in inflammatory bowel disease.Curr. Opin. Gastroenterol. 9: 971–980.
4. HALLIWELL, B. & J. M. C. GUTTERIDGE. 1999. Free Radicals in Biology and Medicine, 3rded. Oxford Univ. Press. Oxford.
5. FRIDOVICH, I. 1986. Superoxide dismutases. Methods Enzymol. 58: 61–97.6. MONCADA, S. & A. HIGGS. 1993. The L-arginine-nitric oxide pathway. N. Engl. J. Med.
329: 2002–2012.7. PALMER, R. M. J., A. G. FERRIGE & S. MONCADA. 1987. Nitric oxide release accounts for
the biological activity of endothelium-derived relaxing factor. Nature 327: 524–526.8. BECKMAN, J. S., J. CHEN, H. ISCHIROPOULOS & J. P. CROW. 1994. Oxidative chemistry of
peroxynitrite. Methods Enzymol. 233: 229–240.9. MALY, F. E. 1990. The B-lymphocyte: a newly recognised source of reactive oxygen
species with immunoregulatory potential. Free Rad. Res. Commun. 8: 143–148.10. MEIER, B., H. RADEKE, S. SELLE, et al. 1990. Human fibroblasts release reactive oxygen
ANNALS NEW YORK ACADEMY OF SCIENCES34

species in response to treatment with synovial fluids from patients suffering from arthri-tis. Free Rad. Res. Commun. 8: 149–160.
11. BRITIGAN, B. E., T. L. ROEDER & D. M. SHASBY. 1992. Insight into the nature and site ofoxygen-centred free radical generation by endothelial cell monolayers using a novel spin-trapping technique. Blood 79: 699–707.
12. CLEMENT, M. V. & S. PERVAIZ. 1999. Reactive oxygen intermediates regulate cellular re-sponse to apoptotic stimuli: an hypothesis. Free Rad. Res. 30: 247–252.
13. WOLIN, M. S. 1996. Reactive oxygen species and vascular signal transduction mecha-nisms. Microcirculation 3: 1–17.
14. COLLINS, T. 1993. Endothelial nuclear factor-�B and the initiation of the atheroscleroticlesion. Lab. Invest. 68: 499–508.
15. BIELSKI, B. H. J. 1985. Reactivity of HO2/O2·– radicals in aqueous solution. J. Phys.
Chem. Ref. Data 14: 1041–1100.16. FLINT, D. H., J. F. TUMINELLO & M. H. EMPTAGE. 1993. The inactivation of FeS cluster
containing hydro-lyases by superoxide. J. Biol. Chem. 268: 22369–22376.17. MORO, M. A., et al. 1994. Paradoxical fate and biological action of peroxynitrite in hu-
man platelets. Proc. Nat. Acad. Sci. USA 91: 6702–6706.18. RADI, R., R. S. BECKMAN & K. K. M. BUSH. 1990. Peroxynitrite oxidation of sulphydryls.
The cytotoxic potential of superoxide and nitric oxide. J. Biol. Chem. 266: 4244–4250.19. VAN DER VLIET, A., et al. 1996. Nitrotyrosine as biomarker for reactive nitrogen species.
Methods Enzymol. 269: 175–184.20. SPENCER, J. P. E., J. WONG, A. JENNER, O. I. ARUOMA, C. E. CROSS & B. HALLIWELL. 1995.
Base modification and strand breakage in isolated calf thymus DNA and in DNA fromhuman skin epidermal keratinocyes exposed to peroxynitrite or 3-morphosydnonimine.Chem. Res. Toxicol. 9: 1152–1158.
21. COCHRANE, C. G. 1991. Mechanisms of oxidant injury of cells. Mol. Aspects Med. 12:137–147.
22. BEAUCHAMP, C. & I. FRIDOVICH. 1970. A mechanism for the production of ethylene frommethional. The generation of hydroxyl radical by xanthine oxidase. J. Biol. Chem. 243:4641–4646.
23. HALLIWELL, B. & J. M. C. GUTTERIDGE. 1990. Role of free radicals and catalytic metalions in human disease. Methods Enzymol. 186: 1–85.
24. DIZDAROGLU, M. 1993. Chemistry of free radical damage to DNA and nucleoproteins. InDNA and Free Radicals, B. Halliwell and O. I. Aruoma, Eds.: 19–39. Ellis Horwood.Chichester, UK.
25. DIZDAROGLU, M., Z. NACKERDIEN, B. C. CHAO, E. GAJEWSKI & G. RAO. 1991. Chemicalnature of in vivo DNA base damage in hydrogen peroxide-treated mammalian cells.Arch. Biochem. Biophys. 285: 388–390.
26. SPENCER, J. P. E., et al. 1995. DNA strand breakage and base modification induced by hy-drogen peroxide treatment of human respiratory tract epithelial cells. FEBS Lett. 374:233–236.
27. VON SONNTAG, C. 1987. The Chemical Basis of Radiation Biology. Taylor & Francis.London.
28. KAUR, H., M. WHITEMAN & B. HALLIWELL. 1997. Peroxynitrite-dependent aromatic hy-droxylation and nitration of salicylate. Is hydroxyl radical involved? Free Rad. Res. 26:71–82.
29. CANDEIAS, L. P., K. B. PATEL, M. R. L. STRATFORD & P. WARDMAN. 1993. Free hydroxylradicals are formed on reaction between the neutrophil derived species superoxide anionand HOCl. FEBS Lett. 333: 151–153.
30. FOLZ, R. J., J. Z. GUAN, M. F. SELDIN, T. D. OURY, J. J. ENGHIELD & J. D. CRAPO. 1997.Mouse extracellular superoxide dismutase: primary structure, tissue specificity, gene ex-
EVANS & HALLIWELL: FREE RADICALS 35

pression, chromosomal localisation and lung in situ hybridisation. Am. J. Res. Cell Mol.Biol. 17: 393–403.
31. LI, J. B., et al. 1995. Dilated cardiomyopathy and neonatal mortality in mutant mice lack-ing manganese superoxide dismutase. Nature Genet. 11: 376–381.
32. CHANCE, B., H. SIES & A. BOVERIS. 1979. Hydroperoxide metabolism in mammalian or-gans. Physiol. Rev. 59: 527–605.
33. CHAE, H. Z., et al. 1997. Characterisation of the three isoforms of mammalian peroxire-doxin that reduce peroxides in the presence of thioredoxin and their role in signal trans-duction. FASEB J. 11: 981–992.
34. WHITEMAN, M. & B. HALLIWELL. 1996. Protection against peroxynitrite-dependent tyro-sine nitration and �1-antiproteinase inactivation by ascorbic acid: a comparison with oth-er biological antioxidants. Free Rad. Res. 25: 275–283.
35. CROSS, C. E., A. VAN DER VLIET, C. A. O’NEILL, S. LOUIE & B. HALLIWELL. 1994. Oxi-dants, antioxidants and respiratory tract lining fluids. Environ. Health Perspect. 102(Suppl. 10): 185–191.
36. HALLIWELL, B. 1996. Vitamin C: antioxidant or pro-oxidant in vivo? Free Rad. Res. 25:275–283.
37. HALLIWELL, B. 1990. How to characterise a biological antioxidant. Free Rad. Res. Com-mun. 9: 1–32.
38. BERGER, T. M., M. C. POLYDOR, A. DABBAGH, P. J. EVANS, HALLIWELL, J. D. MORROW, L. J.ROBERTS & B. FREI. 1997. Antioxidant activity of vitamin C in iron-overloaded humanplasma. J. Biol. Chem. 272: 15656–15660.
39. MUKAI, K., H. MORIMOTO, Y. OKAIUCHI & S. NAGAOKA. 1993. Kinetic study of reactionsbetween tocopheroxyl radicals and fatty acids. Lipids 28: 753–756.
40. ESTERBAUER, H., G. STRIEGL, H. PUHL & M. ROTHENEDER. 1989. Continuous monitoringof in vitro oxidation of human low density lipoprotein. Free Rad. Res. Commun. 6:67–75.
41. KAUR, H. & B. HALLIWELL. 1990. Action of biologically relevant oxidising species onuric acid: identification of uric acid oxidation products. Biol. Chem. Interact. 73:235–247.
42. PAGANGA, G. & C. RICE-EVANS. 1997. The identification of flavonoids as glycosides inhuman plasma. FEBS Lett. 401: 78–82.
43. HALLIWELL, B. 1996. Oxidative stress, nutrition and health. Experimental strategies foroptimization of nutritional antioxidant intake in humans. Free Rad. Res. 25: 57–74.
44. EVANS, P. J., R. W. EVANS, A. BOMFORD, R. WILLIAMS & B. HALLIWELL. 1994. Metal ionscatalytic for free radical reactions in the plasma of patients with fulminant hepatic fail-ure. Free Rad. Res. Commun. 20: 139–144.
45. GUTTERIDGE, J. M. C., D. A. ROWLEY, E. GRIFFITHS & B. HALLIWELL. 1985. Low molecu-lar weight iron complexes and oxygen radical reactions in idiopathic haemochromatosis.Clin. Sci. 68: 463–467.
46. HALLIWELL, B. & J. M. C. GUTTERIDGE. 1990. The antioxidants of human extracellularfluids. Arch. Biochem. Biophys. 200: 1–8.
47. BOLANN, B. J. & R. J. ULVIK. 1990. On the limited ability of superoxide to release ironfrom ferritin. Eur. J. Biochem. 193: 899–904.
48. KANNER, J., J. B. GERMAN & J. E. KINSELLA. 1987. Initiation of lipid peroxidation in bio-logical systems. CRC Crit. Rev. Food Sci. Nutr. 25: 317–364.
49. PUPPO, A. & B. HALLIWELL. 1988. Formation of hydroxyl radicals from hydrogen perox-ide in the presence of iron. Is haemoglobin a biological Fenton reagent? Biochem. J. 249:185–190.
50. DAVIES, M. J. 1990. Detection of myoglobin-derived radicals on reaction of the myoglobinwith hydrogen peroxide and other peroxidic compounds. Free Rad. Res. Commun. 10:361–370.
ANNALS NEW YORK ACADEMY OF SCIENCES36

EVANS & HALLIWELL: FREE RADICALS 37
51. EVANS, P. J., D. AKANMU & B. HALLIWELL. 1994. Promotion of oxidative damage toarachidonic acid and �1-antiproteinase by anti-inflammatory drugs in the presence of thehaem proteins myoglobin and cytochrome c. Biochem. Pharm. 48: 2173–2179.
52. PUPPO, A. & B. HALLIWELL. 1988. Formation of hydroxyl radicals in biological systems.Does myoglobin stimulate hydroxyl radical formation from hydrogen peroxide? FreeRad. Res. Commun. 4: 415–422.
53. MORROW, J. D. & L. J. ROBERTS. 1994. Mass-spectrometry of prostanoids: F2-isoprostanesproduced by non-cyclooxygenase free radical catalysed reaction. Methods Enzymol.233: 163–174.
54. NOUROOZ-ZADEH, J., et al. 1995. Analysis of F2-isoprostanes as indicators of non-enzy-matic lipid peroxidation in vivo by gas chromatography-mass spectrometry: develop-ment of a solid phase extraction procedure. J. Chromatogr. B667: 199–208.
55. MORROW, J. D., et al. 1995. Increase in circulating products of lipid peroxidation (F2-iso-prostanes) in smokers. N. Engl. J. Med. 332: 1198–1203.
56. REHMAN, A., C. S. COLLIS, M. YANG, M. KELLY, A. T. DIPLOCK, B. HALLIWELL & C. RICE-EVANS. 1998. The effects of iron and vitamin C co-supplementation on oxidative damageto DNA in healthy volunteers. Biochem. Biophys. Res. Commun. 246: 293–298.
57. TEIXEIRA, A. J. R., et al. 1993. Method for the analysis of oxidized nucleosides by gaschromatography-mass spectrometry. Anal. Biochem. 214: 474–483.
58. DEAN, R. T., S. FU, R. STOCKER & M. J. DAVIES. 1997. Biochemistry and pathology of rad-ical-mediated protein oxidation. Biochem. J. 324: 1–18.
59. LYRAS, L., P. J. EVANS, P. J. SHAW, P. G. INCE & B. HALLIWELL. 1996. Oxidative damageand motor neurone disease. Difficulties in the measurement of protein carbonyls in hu-man brain tissues. Free Rad. Res. 24: 397–406.
60. HARMAN, D. 1981. The aging process. Proc. Natl. Acad. Sci. USA 78: 7124–7128.61. SIES, H. 1991. Oxidative stress, oxidants and antioxidants. In Oxidative Stress. Academic
Press. London.62. MCCORD, J. M. 1987. Oxygen-derived radicals: a link between reperfusion injury and in-
flammation. Fed. Proc. 46: 2402–2406.63. EVANS, P. J., J. M. TREDGER, J. B. DUNNE & B. HALLIWELL. 1996. Catalytic metal ions and
the loss of reduced glutathione in organ preservation fluids. Transplantation 62:1046–1049.
64. DYKENS, J. A., A. STERN & E. TRENKNER. 1987. Mechanism of kainate toxicity to cerebel-lar neurones in vitro is analogous to reperfusion tissue injury. J. Neurochem. 49:1222–1228.
65. SANDERS, K. M. & S. M. WARD. 1992. Role of nitric oxide in the brain. Am. J. Physiol.262: G239.
66. HALLIWELL, B. 1994. Free radicals and antioxidants: a personal view. Nutr. Rev. 52:253–265.
67. ORRENIUS, S., D. J. MCCONKEY, G. BELLOMO & P. NICOTERA. 1989. Role of Ca2+ in toxiccell killing. Trends Pharmacol. Sci. 10: 281–285.
68. STADTMAN, E. R. & D. N. OLIVER. 1991. Metal-catalysed oxidation of proteins. Physio-logical consequences. J. Biol. Chem. 266: 2005–2008.
69. VERMES, I. & C. HAANEN. 1994. Apoptosis and programmed cell death in health and dis-ease. Adv. Clin. Chem. 31: 177–246.
70. HALLIWELL, B. 1992. Reactive oxygen species and the central nervous system. J. Neu-rochem. 59: 1609–1623.
71. STEINBERG, D., S. PARATHASARATHY, T. E. CAREW, J. C. KHOO & J. L. WITZTUM. 1989. Be-yond cholesterol. Modifications of low density lipoprotein that increase atherogenicity.N. Engl. J. Med. 320: 915–924.
72. HALLIWELL, B. 1995. Oxygen radicals, nitric oxide and human inflammatory joint dis-ease. Ann. Rheum. Dis. 54: 505–510.

ANNALS NEW YORK ACADEMY OF SCIENCES38
73. AMES, B. N., M. K. SHIGENAGA & T. M. HAGEN. 1993. Oxidants, antioxidants and the neu-rodegenerative diseases of aging. Proc. Natl. Acad. Sci. USA 90: 7915–7922.
74. HALLIWELL, B. 1999. Establishing the significance and optimal intake of dietary antioxi-dants: the biomarker concept. Nutr. Rev. 57: 104–113.
75. JENNER, A., T. C. ENGLAND, O. I. ARUOMA & B. HALLIWELL. 1998. Measurement of oxida-tive DNA damage by GC-MS: ethane thiol prevents artefactual development of oxidisedDNA bases. Biochem. J. 331: 365–367.
76. LEVINE, R. L., J. A. WILLIAMS, E. R. STADTMAN & E. SCHACTER. 1994. Carbonyl assaysfor the determination of oxidatively modified proteins. Methods Enzymol. 233:346–363.
77. KAHN, J., D. M. BRENNAN, N. BRADLEY, B. R. GAO, R. BRUCKDORFER & M. JACOBS. 1998.3-Nitrotyrosine in the proteins of human plasma determined by an Elisa method.Biochem. J. 330: 795–801.
78. EVANS, P. J., H. KAUR, M. J. MITCHINSON & B. HALLIWELL. 1996. Do human atheroscle-rotic lesions contain nitrotyrosine? Biochem. Biophys. Res. Commun. 226: 346–351.
79. FU, S., M. J. DAVIES & R. T. DEAN. 1998. Molecular aspects of free radical damage to pro-teins. In Molecular Biology of Free Radicals in Human Disease. O. I. Aruoma and B.Halliwell, Eds.: 29–56. London and Saint Lucia.
80. KAUR, H. & B. HALLIWELL. 1994. Detection of hydroxyl radicals by aromatic hydroxyla-tion. Methods Enzymol. 233: 67–82.
81. YAMAMOTO, Y. 1994. Chemiluminescence-based high-performance liquid chromatogra-phy assay of lipid hydroperoxides. Methods Enzymol. 233: 319–324.
82. CHIRICO, S. 1994. High performance liquid chromatography-based thiobarbituric acidtests. Methods Enzymol. 233: 314–319.
83. NOUROOZ-ZADEH, J., E. H. C. LIU, E. E. ANGGARD & B. HALLIWELL. 1998. F-4-Iso-prostanes: a novel class of prostanoids found during peroxidation of docosahexanoenoicacid. Biochem. Biophys. Res. Commun. 242: 338–344.
84. SIAN, J., et al. 1994. Alterations in glutathione levels in Parkinson’s disease and other neu-rodegenerative disorders affecting the basal ganglia. Ann. Neurol. 36: 348–361.
85. RICE-EVANS, C., A. T. DIPLOCK & M. C. R. SYMONS. 1991. Assay of antioxidant nutrientsand antioxidant enzymes. In Techniques in Free Radical Research: 185–206. Elsevier.Amsterdam.
86. HALLIWELL, B. 1998. Can oxidative DNA damage be used as a biomarker of cancer riskin humans? Free Rad. Res. 29: 469–486.
87. OUAHCHI, K., M. AVITA, H. KAYDEN, et al. 1995. Ataxia with isolated vitamin E de-ficiency is caused by mutation in the �-tocopherol transfer protein. Nature Genet. 9:141–145.
88. EVANS, P. J. & B. HALLIWELL. 1995. Side-effects of drugs used in the treatment ofrheumatoid arthritis. In Free Radicals and Oxidative Stress: Environment, Drugs andFood Additives, C. Rice-Evans, B. Halliwell, and G. G. Lunt, Eds.: 195–28. Biochem.Soc. Symp. 61. Portland Press. London.
89. BROOKE, P. M., W. F. KEAN & W. W. BUCHANAN. 1986. In the Clinical Pharmacology ofanti-inflammatory agents: 81–82. Taylor & Francis. London.
90. LUNEC, J. & D. R. BLAKE. 1986. The determination of dehydroascorbic acid and ascorbicacid in the serum and synovial fluid of patients with rheumatoid arthritis. Free Rad. Res.Commun. 1: 31–39.
91. PIERSON, M. G. & B. H. GRAY. 1982. Superoxide dismutase activity in cochlea. Hear. Res.6: 141–151.
92. ZELCK, U., R. NOWAK, U. KARNSTEDT, et al. 1993. Specific activities of antioxidative en-zymes in the cochlea of guinea pigs at different stages of development. Eur. Arch. Oto-Rhino-Laryngol. 250: 218–219.

93. EL BARBARY, A., R. ALTSCHULER & J. SCHACHT. 1994. Glutathione-S-transferase enzymesin organ of Corti of the rat-enzymatic activity, subunit composition and immunochemicallocalisation. Hear. Res. 71: 80–90.
94. RUBAK, L. P., R. RAVI & S. M. SOMANI. 1995. Mechanism of protection by diethylcarba-mate against cis-platin ototoxicity: antioxidant system. Fundam. Appl. Toxicol. 26:293–300.
95. RAVI, R., S. M. SOMANI & L. P. RYBAK. 1995. Mechanism of cis-platin cytotoxicity: an-tioxidant system. Pharmacol. Toxicol. 76: 386–394.
96. PEARSON, M. G. & A. R. MOLLER. 1981. Prophylaxis of kanamycin-induced ototoxicityby a radioprotectant. Hear. Res. 4: 79–87.
97. BOCK, G. R., G. K. YAKES, J. J. MILLER & P. MOORJANI. 1983. Effects of N-acetyl cysteineon kanamycin toxicity in the guinea pig. Hear. Res. 9: 255–262.
98. HOFFMAN, D. W., K. L. JONES-KING, C. A. WHITWORK & L. P. RYBAK. 1988. Potentiationof ototoxicity by glutathione depletion. Ann. Otol. Rhinol. Laryngol. 97: 36–42.
99. SONG, B.-B. & J. SCHACHT. 1994. Variable efficacy of radical scavengers and iron chela-tors to attenuate gentamycin ototoxicity in guinea pig in vivo. Hear. Res. 94: 87–93.
100. PRIUSKA, E. M. & J. SCHACHT. 1995. Formation of free radicals by gentamycin and ironand evidence for an iron-gentamycin complex. Biochem. Pharmacol. 50: 1749–1752.
101. KAYS, S. E., W. A. CROWELL & M. A. JOHNSON. 1991. Iron supplementation increases gen-tamycin nephrotoxicity in rats. J. Nutr. 121: 1869–1875.
102. KALOYANIDES, G. J. 1984. Renal pharmacology of aminoglycoside antibiotics. In Contri-butions to Nephrology 42, Drug-Induced Nephrotoxicity, A. Bianchi, A. Bertelli, and C.G. Duarte, Eds.: 148–167. Karger. Basel.
103. KISHORE, B. K., Z. KALLAY & P. LAMBRICHT, et al. 1990. Mechanism of protection afford-ed by polyaspartic acid against gentamycin-induced lipidosis. I. Polyaspartic acid bindsgentamycin and displaces it from negatively charged phospholipid layers in vitro. J. Phar-macol. Exp. Ther. 255: 867–874.
104. KISHORE, B. K., P. LAMBRICHT, G. LAURENT, et al. 1990. Mechanism of protection af-forded by polyaspartic acid against gentamycin-induced lipidosis. II. Comparative in vit-ro and in vivo studies with poly-L-glutamic acids. J. Pharmacol. Exp. Ther. 255: 875–884.
105. GARETZ, S. L., D. J. RHEE & J. SCHACHT. 1994. Sulphydryl compounds and antioxidantsinhibit cytotoxicity to outer hair cells of a gentamycin metabolite in vitro. Hear. Res. 77:75–80.
106. LAUTERMAN, J., J. MCLAREN & J. SCHACHT. 1995. Glutathione protection against gen-tamycin ototoxicity depends on nutritional status. Hear. Res. 86: 15–24.
107. WALKER, P. D. & S. V. SHAH. 1988. Evidence suggesting a role for hydroxyl radical ingentamycin-induced acute renal failure in rats. J. Clin. Invest. 81: 334–341.
108. RAMSAMMY, L. S., C. JOSEPOVITZ, K.-Y. LING, B. P. LANE & G. J. KALOYANIDES. 1987.Failure of inhibition of lipid peroxidation by vitamin E to protect against gentamycinnephrotoxicity in the rat. Biochem. Pharmacol. 36: 2125–2132.
109. BASILE, A. S., J.-M. HUANG, X. CHEN, D. WEBSTER, C. BERLIN & P. SKOLNICK. 1996. N-Methyl-D-aspartate antagonists limit aminoglycoside antibiotic induced hearing loss.Nature Med. 2: 1338–1343.
110. YAMANE, H., Y. NAKAI, et al. 1995. The emergence of free radicals after acoustic stimula-tion and strial blood flow. Acta Otolaryngol. (Stockh.) 519 (Suppl.): 87–92.
111. JACONO, A. A., B. HU, R. D. KOPKE, et al. 1998. Changes in cochlea antioxidant enzymeactivity after sound conditioning and noise exposure in the chinchilla. Hear. Res. 117:31–38.
112. CONLON, B. J., B. P. PERRY & D. W. SMITH. 1998. Attenuation of neomycin ototoxicity byiron chelation. Laryngoscope 108: 284–287.
EVANS & HALLIWELL: FREE RADICALS 39

113. CONLON, B. J. & D. W. SMITH. 1998. Supplemental iron exacerbates aminoglycoside oto-toxicity in vivo. Hear. Res. 115: 1–5.
114. CHU, W. 1994. Cellular responses to cis-platin. The roles of DNA-binding proteins andDNA repair. J. Biol. Chem. 269: 787–790.
115. VERMEULEN, N. P. E. & G. S. BALDEW. 1992. The role of lipid peroxidation in the nephro-toxicity of cis-platin. Biochem. Pharmacol. 44: 1193–1199.
116. CAMPBELL, K. C. M., L. P. RYBAK, K. P. MEECH & L. HUGHES. 1996. D-Methionine pro-vides extra protection from cis-platin ototoxicity in the rat. Hear. Res. 102: 90–98.
117. EVANS, P. J., M. WHITEMAN & B. HALLIWELL. 1997. The antioxidant activity of S-adenosylmethionine: a possible addition to organ storage fluids. Free Radical Biol. Med. 23:1002–1008.
118. PACKER, L. 1998. �-Lipoic acid: a metabolic antioxidant which regulates signal transduc-tion and protects against oxidative injury. Drug Metab. Rev: 30: 245–275.
119. WHITEMAN, M., H. TRITSCHLER & B. HALLIWELL. 1996. Protection against peroxynitrite-dependent tyrosine nitration and �1-antiproteinase inactivation by oxidized and reducedlipoic acid. FEBS Lett. 379: 74–76.
120. CONLON, B. J., J. M. ARAN, J. P. ERRE & D. W. SMITH. 1999. Attenuation of aminoglyco-side-induced cochlear damage with the metabolic antioxidant �-lipoic acid. Hear. Res.128: 40–44.
ANNALS NEW YORK ACADEMY OF SCIENCES40