Embed Size (px)
Citation preview

Free Nipple GraftingAn Alternative for Patients Ineligible for Nipple-Sparing Mastectomy?
Erin Louise Doren, MD,* Lauren Van Eldik Kuykendall, MD,* Jonathan Jeremiah Lopez, MD,*Christine Laronga, MD, FACS,Þ and Paul David Smith, MD*Þ
Abstract: Nipple-sparing mastectomy is an option for patients fitting onco-logic criteria and may improve cosmetic outcomes of breast reconstruction.When anatomical limitations exist, we propose the use of free nipple grafting,akin to reduction mammaplasty. This study is a retrospective review of pa-tients having a nipple-sparing mastectomy and immediate reconstruction usingfree nipple grafting (N = 36 breasts). Average graft take was 93.6% with nonipples having complete graft loss. Four nipples (11%) lost all projectionand 4 nipples experienced significant hypopigmentation requiring tattooing(11%). For those ineligible for nipple-sparing mastectomy due to anatomicallimitations, free nipple grafting is an option with acceptable complication ratessimilar to free nipple grafting in reduction mammaplasties and, more impor-tantly, saves women a subsequent operation for nipple reconstruction.
Key Words: breast reconstruction, nipple-sparing mastectomy, free nipplegrafting, nipple reconstruction, breast reduction
(Ann Plast Surg 2014;72: S112YS115)
Over the past several decades, the surgical management of breastcancer has significantly evolved with guidance by principles of
patient safety, oncologic safety, and more recently cosmetic out-come.1,2 The optimal cosmetic outcome following mastectomy andreconstruction involves preservation of the nipple-areolar complex.2
The nipple-areolar complex defines a breast as a breast and similarlydefines a reconstructed breast mound.2 Nipple-sparing mastectomy isemerging as a safe alternative to skin-sparing mastectomy for boththerapeutic and prophylactic indications in properly selected pa-tients.3 Additionally, nipple-sparing mastectomy has been demon-strated repeatedly to have a positive impact on body image andpatient statisfaction.3
Spear et al, amongmany others, have developed widely acceptedpatient selection criteria for nipple-sparing mastectomy based on on-cologic and surgical factors.2,3 The oncologic criteria include a tumorsize less than 3 cm, tumor greater than 2 cm from the nipple-areolarcomplex, clinically negative axillary nodes, and no skin involvementor inf lammatory cancer/Paget disease.2,3 Operative criteria includenegative intraoperative frozen section and negative permanent nipplepathology.2,3 Certain anatomic criteria also exist that can precludepatients from undergoing nipple-sparing mastectomy, which include
large breast size (greater than 500 g), breast ptosis (grade II-III), radi-ation, and prior periareolar incisions.2Y4 Additional patient factors,although not absolute contraindications, can cause an increased riskfor postoperative complications. Factors including BMI greater than25 kg/m2, breast mass greater than 750 g, and sternal notch to nippledistance greater than 26 cm are associated with increased risk off lap necrosis, partial f lap loss, and wound dehiscence.3,4
When these anatomical limitations exist, alternative strategiesfor preserving the nipple include reducing the skin envelope beforemastectomy, grafting the nipple-areolar complex, or performing amastopexy at the same time as the mastectomy.1,2,5 In 1987, Woodsdescribed his approach to nipple-sparing mastectomy with simulta-neous mastopexy and suggested that the nipple could be spared andthe skin envelope reduced at the time of mastectomy to create bettercosmetic outcomes.5,6 However, that option has become less favor-able because of the need to retain larger quantities of breast tissue toensure nipple and f lap viability.5 More recently, Spear et al proposeda staged approach with a pre-mastectomy mastopexy or reduction incarefully selected patient with ptosis or macromastia.5 Although thisstaged approach has comparable complication rates to publishedranges of nipple-sparing mastectomy and skin-sparing mastectomywith immediate reconstruction, the patients are subjected to multipleoperations.5 We propose an alternative, single-stage reconstructionwith the use of free nipple grafting, akin to reduction mammoplasty,with anticipated similar complication rates.
METHODSThis study is a retrospective review of 21 prospectively gath-
ered patients having a nipple-sparing mastectomy with immediatebreast reconstruction using free nipple grafting. Moffitt Cancer Centerhas established our institutional eligibility and exclusion criteria fornipple-sparing mastectomy which encompasses oncologic and technical/cosmetic considerations. Patients, thus, were excluded from standardnipple-sparing mastectomy at our facility based on the following in-stitutional ineligibility criteria: prior periareolar incisions (n = 2),breast size greater than 700 g (n = 3), grade II-III ptosis (n = 1), pre-vious radiation treatment (n = 5), and desire for autologous recon-struction (n = 10).
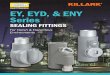
Skin-sparing mastectomies were performed by a single breastsurgeon in a standard fashion via a circumareolar incision. Thenipple-areola complex was then harvested from the mastectomyspecimen as a full-thickness graft with a 10-blade scalpel (Fig. 1).Frozen sections from the base of the nipple were sent to assure therewas no malignancy or atypia in the specimen. The nipples weredefatted in a standard fashion with minimal thinning of the dermis.Breast reconstruction, prosthetic or autologous, was then performed,on occasion requiring a vertical reduction pattern or change of nippleposition. Free nipple grafts were then re-implanted to the de-epithelialized recipient sites and secured with a Xeroform bolster.Bolsters were removed in the clinic on postoperative days 7Y10.Complications and outcome were recorded in the patient’s medicalrecord and subsequently logged in the breast reconstruction database.Photos of all patients were reviewed at the last documented postop-erative visit to assess overall graft take, nipple projection, and areola
CLINICAL PAPERS
S112 www.annalsplasticsurgery.com Annals of Plastic Surgery & Volume 72, Supplement 2, June 2014
ReceivedOctober 21, 2013, and accepted for publication, after revision, October 29, 2013.From the *Division of Plastic Surgery, Department of Surgery, University of South
Florida, Tampa, FL; and †Comprehensive Breast Program, H. Lee MoffittCancer Center, Department of Women’s Oncology, Tampa, FL.
Conflicts of interest and source of funding: none declared.The contents of this paper were reported in poster format at the American As-
sociation of Plastic Surgeons (AAPS), New Orleans, Louisiana, April 2013and at the Southeastern Society of Plastic and Reconstructive Surgeons(SESPRS), Bonita Springs, Florida, June 2013.
Reprints: Erin Louise Doren, MD, Division of Plastic Surgery, Department ofSurgery, University of South Florida, 2 Tampa General Circle, 7th Floor,Tampa, FL 33606. E-mail: [email protected].
Copyright * 2013 by Lippincott Williams & WilkinsISSN: 0148-7043/14/7202-S112DOI: 10.1097/SAP.0000000000000077
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

pigmentation. A chi-square test using exact method with MonteCarlo estimation was used to determine if the type of breast recon-struction affected complication rates. Complications included any-thing that required surgical or procedural intervention.
RESULTSOf 21 patients, 8 women had bilateral prophylactic mastectomy,
6 women had unilateral mastectomies, and 7 women had bilateralmastectomies for unilateral cancer, totaling 36 nipple-areola graftsharvested. The mean patient age at the time of surgery was 48 years(range 21Y66 years) and none of the women had a current or recent(6 months) history of tobacco use. The mean BMI was 24.98 (range20Y33.1). Most of the women had grade 2 ptosis and the meanbreast weight at mastectomy was 481.76 g (range 110.4Y835.8 g).The mean follow-up was 17.28 months (range 0.7Y69 months).Reconstruction was performed as follows: implant sparing withlatissimus dorsi muscle f lap (2/36), transverse rectus abdominusmyocutaneous f lap (TRAM) (18/36), and latissimus dorsi f lapwith tissue expanders (16/36). All nipple base pathology was foundto be benign on frozen and permanent specimens. Upon removalof nipple Xeroform bolsters, many patients had a small amount ofepidermolysis. The average graft take, with full-thickness necrosis be-ing a value of zero and no necrosis 100, was 93.6% (range 60%Y100%).No patients had complete nipple necrosis (0%). Average nipple pro-jection was 59% of original size (n = 34, as 1 patient did not have long-term follow-up photo) (range 0%Y100%). Four (of 36) nipples (11%),in 3 patients, lost all projection and required subsequent nipple recon-struction. Pigmentation of the nipple-areola was rated by the surgicalteam on a scale of 0%Y100%, zero with no pigmentation remaining,100% normal pigmentation, the averagewas 86.5% (n = 34, as 1 patientdid not have long-term follow-up photo) (range 20%Y100%). In addi-tion, four (of 36) nipples (11%), in 2 patients, experienced significant
hypopigmentation requiring subsequent nipple-areola tattooing. Thetype of reconstruction did not impact the rate of complications requiringintervention or return to the operating room (Table 1). No patient hadrecurrence of cancer on final follow-up visit. Examples of preoperativeand postoperative patients can be found in Figures 2 and 3.
DISCUSSIONNipple-sparing mastectomy is increasingly being performed in
appropriately selected patients for both therapeutic and prophylacticindications.1,3,5,7 The benefits of preserving the nipple-areolar com-plex go beyond mere cosmetic results of the breast reconstructionbut also include functional outcomes and patient satisfaction as itcan be difficult to match projection, size, color, shape, texture, po-sition, and sensation with nipple reconstruction.7 Ensuring optimaloutcomes requires appropriate patient selection from an oncologic,surgical, and anatomic perspective. In patients who meet inclusioncriteria from an oncologic standpoint but are limited secondary toanatomic factors such as breast size and degree of breast ptosis, thereconstructive options for preserving the nipple-areolar complexbecome limited and quite challenging. Newer strategies are beingdeveloped to prevent postoperative complications, such as skin f lapand nipple necrosis, which are even more important in this patientpopulation which requires preserving all the native breast skin.5 Forwomen desiring nipple-sparing mastectomy and immediate recon-struction but technically limited by larger breast size or degree ofptosis, we investigated the feasibility of free nipple grafting as asingle-stage approach. Akin to a reduction mammaplasty, we ex-perienced good aesthetic results and a low rate of postoperativecomplications.
In contrast, Spear et al has proposed a pre-mastectomy,mastopexy/reduction, staged approach as an alternative to permitnipple-sparing mastectomy in the large- or ptotic-breasted patient.5
This approach entails that the mastopexy or reduction be performedas a pre-mastectomy procedure with repositioning of the nipple andreducing the skin envelope. After a minimum of 4 weeks, a nipple-sparing mastectomy through the mastopexy incisions is performedwith subsequent final reconstruction.5 Using this staged approach,they report that 17% of the breasts had a complication that requiredreturn to the operating room, and 13% had partial nipple-areolarcomplex necrosis with no total nipple-areolar complex necrosis.5
Patient satisfaction or surgeon satisfaction with final nipple positionwere not discussed. Although the pre-mastectomy staged approach isan acceptable alternative with comparable complication rates, themajor disadvantage is that the patients are subjected to multiple op-erations, which may increase morbidity and cost, and contribute topatient dissatisfaction. Our single-stage approach using immediatereconstruction with free nipple grafting in patients with anatomiclimitations deserves consideration as a viable alternative.
Free nipple-areolar grafting has been described for many de-cades in patients undergoing reduction mammaplasty.8,9 Indicationsfor reduction mammaplasty with free nipple-areolar grafting includepatients with massive breast hypertrophy or gigantomastia, previousbreast surgery that may risk viability of the nipple, overweight ptotic
FIGURE 1. Free nipple grafts harvested.
TABLE 1. Type of Reconstruction Versus Complication Requiring Intervention
Reconstruction Total No Complication Yes Complication P
LD with implant sparing 2 (5.6%) 1 (50%) 1 (50%) 0.3207LD with TE 16 (44.4%) 14 (87.5%) 2 (12.5%)TRAM 18 (50%) 13 (72.2%) 5 (27.8%)Total 36 28 (77.8%) 8 (22.2%)
LD indicates latissimus dorsi; TE, tissue expander.
Annals of Plastic Surgery & Volume 72, Supplement 2, June 2014 Free Nipple Grafting for Nipple-Sparing Mastectomy
* 2013 Lippincott Williams & Wilkins www.annalsplasticsurgery.com S113
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

breast, and poor-risk elderly patients or those with severe systemicdisease where shorter anesthetic time would be an advantage.8Y10
Disadvantages of free nipple grafting include loss of nipple sensation,loss of projection, hypopigmentation, and graft loss requiring furtherreconstruction.8Y10 However, a properly prepared full-thickness nipple-areolar graft can preserve both projection and nipple contour whichleads to improved patient satisfaction and cosmetic outcomes.10 Ad-ditionally, there is some evidence that nipple sensation and eroticfunction can be partially recovered postoperatively with free nipplegrafting.9
Our rates of graft loss, loss of projection, and hypopigmen-tation are comparable to the reported rates in the literature for re-duction mammaplasties with free nipple grafts.8Y11 A review offree nipple grafting and patient satisfaction in breast reduction byMcGregor et al showed complete loss of the nipple-areolar complexin 1 patient and partial loss in 18% of patients requiring minorinterventions.8 Additionally, nipple projection was satisfactory in14 women (55% of nipples) and nipple sensation was present in 30%of nipples.8 Guven et al retrospectively reviewed 24 patients under-going reduction mammaplasty with free nipple grafting over a 4-yearperiod. He reported partial nipple-areolar complex loss in 8% ofpatients, all of which were treated conservatively, and hypopigmen-tation in 20.8% of patients.11
The major advantage of our method is that the reconstructioncan be done in 1 stage, saving the women subsequent operations. Therate of re-operation was low, with no patients requiring nipple re-construction for graft loss and 3 requiring reconstruction for
complete loss of projection. Adequate cosmetic results were obtaineddespite having some loss of nipple projection and hypopigmentationas the presence of a native nipple on a reconstructed breast positivelyinf luences patient satisfaction.12 Previous studies have shown thatpatients express dissatisfaction with various aspects of their recon-structed nipple including poor shape, size, texture, position, color, andprojection.12 Although surgical reconstruction of an absent nipple canprovide acceptable aesthetic results, these results are not ideal.12
In this study, criteria for free nipple grafting with nipple-sparing mastectomy were a prior periareolar incision, breast sizegreater than 700 g, grade II-III ptosis, previous radiation treatment,and desire for autologous reconstruction. When the reason for using afree nipple approach was significant breast ptosis, it raises the issueof how did we change the nipple position. On occasion, we recom-mend performing a small crescent or vertical mastopexy at the timeof mastectomy and reconstruction to change the position for place-ment of the nipple graft. However, we found that this is rarely nec-essary as the act of removing the breast tissue and shaping withimmediate autologous reconstruction allows the nipple position to beadjusted and subsequently the mastectomy skin shrinks to the desiredposition. As a direct result of this study, we have changed our view onthe use of free nipple grafts for the reason of autologous recon-struction alone. Studies have now demonstrated that it is safe to buryf laps, including free f laps, for single-stage breast reconstruction withnipple-sparing mastectomy in the appropriately selected patients.13
Therefore, currently we perform nipple-sparing mastectomy, with-out free nipple grafts, on patients having autologous and free f lap
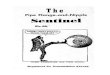
FIGURE 2. A, Preoperative, patient with right breast cancer and prior periareolar incision. B, Postoperative, right breast latissimusimplant reconstruction and free nipple graft, left breast augmentation for symmetry.
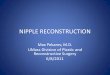
FIGURE 3. A, Preoperative, right breast cancer, desire for autologous reconstruction. B, Postoperative, right mastectomy withTRAM reconstruction and free nipple grafting.
Doren et al Annals of Plastic Surgery & Volume 72, Supplement 2, June 2014
S114 www.annalsplasticsurgery.com * 2013 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

reconstruction, as long as they do not have significant breast ptosis orbreast size, and we are confident that the nipple will end up in thecorrect position.
CONCLUSIONSIncreasingly popular nipple-sparing mastectomy is an option for
women meeting oncologic and anatomic criteria. For those women in-eligible for technical reasons, free nipple grafting is an option withcomplication rates similar to free nipple grafting in reduction mam-maplasties. More importantly, free nipple grafting at mastectomy withimmediate reconstruction saves these women a subsequent operationfor nipple reconstruction.
REFERENCES1. Spear SL, Hannan CM, Wiley SC, et al. Nipple-sparing mastectomy. Plast
Reconstr Surg. 2009;123:1665Y1673.
2. Laronga C, Lewis J, Smith P. The changing face of mastectomy: an oncologicand cosmetic perspective. Cancer Control. 2012;19:286Y294.
3. Spear SL, Willey SC, Feldman ED, et al. Nipple-sparing mastectomy for pro-phylactic and therapeutic indications. Plast Reconstr Surg. 2011;128:1005Y1014.
4. Davies K, Allan L, Roblin P, et al. Factors affecting post-operative complica-tions following skin sparing mastectomy with immediate reconstruction.Breast. 2011;20:21Y25.
5. Spear SL, Rottman SJ, Seiboth LA, et al. Breast reconstruction using a stagednipple-sparing mastectomy following mastopexy or reduction. Plast ReconstrSurg. 2012;129:572Y581.
6. Woods JE. Detailed technique of subcutaneous mastectomy with and withoutmastopexy. Ann Plast Surg. 1987;18:51Y61.
7. Tanna N, Broer PN, Weichman KE, et al. Microsurgical breast reconstructionfor nipple-sparing mastectomy. Plast Reconstr Surg. 2013;131:139eY147e.
8. Mcgregor JC, Hafeez A. Is there still a place for nipple areolar grafting inbreast reduction surgery? A review of cases over a three year period. J PlastReconstr Aesthet Surg. 2006;59:213Y218.
9. Ahmed OA, Kolhe PS. Comparison of nipple and areolar sensation after breastreduction by free nipple graft and inferior pedicle techniques. Br J Plast Surg.2000;53:126Y129.
10. Colen SR. Breast reduction with use of the free nipple graft technique. Aes-thetic Surg J. 2001;21:261Y271.
11. Guven E, Aydin H, Basaran K, et al. Reduction mammaplasty using bipedicleddermoglandular flaps and free-nipple transplantation. Aesth Plast Surg. 2010;34:738Y744.
12. Djohan R, Gage E, Gatherwright J, et al. Patient satisfaction following nipple-sparing mastectomy and immediate breast reconstruction: an 8-year outcomestudy. Plast Reconstr Surg. 2010;125:818Y829.
13. Levine SM, Snider C, Gerald G, et al. Buried flap reconstruction after nipple-sparing mastectomy: advancing toward single-stage breast reconstruction.Plast Reconstr Surg. 2013;132:489eY497e.
Annals of Plastic Surgery & Volume 72, Supplement 2, June 2014 Free Nipple Grafting for Nipple-Sparing Mastectomy
* 2013 Lippincott Williams & Wilkins www.annalsplasticsurgery.com S115
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.