Embed Size (px)
Citation preview

430
FREE GRAFT REPAIR IN PILONIDAL SINUSBy D. WYNN WILLIAMS, M.S.(Lond.), F.R.C.S.
Plastic Surgery and J'aw Injuries Centre, Queen Victoria Hospital, East Grinstead, Sussex
The problem of satisfactory treatment of thepilonidal sinus is so well-known as to require nofurther justification for reporting a method ofrepair only briefly mentioned in the literature.The aetiology and pathology of pilonidal sinus-
has been fully discussed in many papers andthough varied theories have been propounded itwill suffice to mention only a few. The mostwidely accepted theory is that of Sir John BlandSutton (I9I7) who suggested that a congenitalfaulty skin coalescence in the middle line of thelower sacral region of the back may lead to theformation of post anal dimples and coccygealsinuses, and these may be termed sequestrationdermoids. Patey and Scarff (I946) suggest thatonly a small proportion of sinuses are develop-mental in origin and that the majority are primarilyof an infective origin. King (1947) believes thatirritation in the intergluteal folds leads to adepression or crypt and this crypt becomes therepository of debris and hairs, ultimately infectionwith sinus formation occurs. Davies and Starr(1945) quote and confirm Kooistra's (1942)findings of multiple midline dimples in the caudalmidline zone of embryos and their persistencethrough adult life, they draw attention to the factthat the skin of the natal cleft is thin and contrastswith the thicker texture of the skin of the buttockproper, and in many individuals the natal cleftmanifests one or more dimples which they believeto be embryonic relics and potential pilonidalsinuses. They give a detailed anatomical descrip-tion of the fascia binding the skin of the natal cleftto the sacrum and coccyx and postulate reasons forthe sinuses being more commonly found extendingupwards and to the left of the midline. Theypoint out that the blood supply to the natal cleftin the midline is by means of small branches fromthe posterior perforating arteries which emergefrom the sacral foramina and a strictly midlineblood supply does not exist.The treatment of the acutely inflamed pilonidal
sinus is well understood but the problem lies in thehandling of the non-inflamed and recurrentsinuses. The sinus must be excised together
with all epithelial lined tracts and it is preferablethat surgery should be undertaken when the sinusis in a quiescent phase, with little discharge andno signs of acute inflammation in the surroundingtissues. The amount of skin excised may bevariable but must include all the sinus openings.The tissues defect will therefore be great in all butthe simplest, non-infected cases, and the problemof repair of this tissue defect is one that has taxedthe ingenuity of many surgeons and is undoubtedlya major cause in the very high ' recurrence' rate.
Primary closure with direct approximation ofthe wound edges is the quickest and most satis-factory treatment.
Davies and Starr state that this method ofrepair is possible if:
i. It is realised that the subcutaneous woundis larger than the skin defect, so that overhangingskin edges are the rule, and the obliteration of thesubcutaneous defect is as important as skinclosure because the nutrition at the wound edgesis impaired when its subcutaneous supports havebeen removed.
2. It is recognized that the blood supply of themidline natal cleft is poor when compared to thatof the buttock.
3. The rigidity of the buttock is appreciated.The dense fascia of the buttock and its fixation bythe natal cleft fascia militate against the use ofbuttock fat to close the subcutaneous dead space.
4. It is appreciated that tension of a degreewhich would be permissible in wounds in othersites is excessive in the natal cleft.
5. A haematoma developing under the sutureline can be disastrous.
Unfortunately in many patients direct closure isunsuccessful and for this reason a large number ofalternative surgical procedures have beendescribed; they include:
i. Excision and healing by granulation; thisis time-consuming and in many instancespainful procedure.
2. Sliding flaps of gluteus maximus as describedby Pope and Hudson (1946).
3. Estlander flaps, which are designed to rotate
copyright. on M
ay 10, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.346.430 on 1 A
ugust 1954. Dow
nloaded from

August 1954 WYNN WILLIAMS: Free Graft Repair in Pilonidat Sinus 43I
..... ......................
R
.: :.:.
.............':
~.:.::.:.
~ ~ ~ ~..... '. ::..
........*., ': ........... .... ..
B?INN'':::i:'':
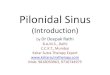
FIG. i.-Case i. Natal cleft with scarring and openingof sinus.
into the defect as described by Davies and Starr.These are satisfactory in most cases, but it involvesa lengthly operation and in some cases a marginalskin loss occurs. The healing time is thenprotracted; haematoma formation beneath suchflaps is utterly disastrous.
4. Dissection of the sinus from under a fullthickness flap of the local skin which is thenresutured over the defect, Brezin (I943).
5. The simpler procedure and far less timeconsuming method described by Boger andPinkham (I9i) of using a split skin graft to coverthe defect.The following two cases of recurrent pilonidal
sinuses are described in detail:
Case IJ.C.S.-male aged 30 years. Occupation:
Seaman in the Royal Navy. In February 195I,while serving at sea, he developed a pilonidalabscess, which was treated by local applicationsand allowed to discharge spontaneously, and thepurulent discharge persisted for four weeks.
Six months later he was admitted to a hospitalwhere complete excision of the sinus, and epitheliallined tract was carried out. The wound was leftopen and packed, and healing by granulation took
........... .ma's
.... .......
........
.....
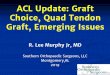
FIG. 2.-Case i. Rotation flaps in position.
place. Subsequently, two further operationsusing the same technique were performed. Hewas transferred to this Unit in July, 1952.
Examination. Normal heavily built man.C.V.S. C.N.S. R.S.-normal. B.P. 120/80.Urine-normal.
Perineum. A large sinus was situated in thenatal cleft, I in. in length and 2 in. in depth,and the tract was lined with unhealthy granulationtissue. The surrounding skin was heavily scarred.(Fig. i).
Proctoscopy. The anal canal was normal.Operation. The sinus, surrounding scarred
skin, the tract and all palpable scar tissue wasexcised. Double rotation flaps were then cutfrom the buttocks and sutured together in themidline to close the defect (Fig. 2).
Superficial loss of the edges of the rotationalflaps occurred (Fig. 3) but the suture lines healedin four weeks. The patient remained free fromrecurrence for three months, but was readmittedat the end of that time because he had a dischargefrom the lower end of the central scar in the natalcleft. Exploration of the sinus showed a largeabscess cavity situated beneath the right rotationflap. The abscess was evacuated and the pyogenic
copyright. on M
ay 10, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.346.430 on 1 A
ugust 1954. Dow
nloaded from

432 POSTGRADUATE MEDICAL JOURNAL August I954
..*. R: :.;;. ::: ..::.
FIG. 3.-Case I. Superficial breakdown of suture linesof rotation flaps.
membrane removed, and the flaps were resutured.Subsequently, the patient complained of an
intermittent purulent discharge from the midlinescar. Six months later a further exploration ofthe sinus was carried out and the pyogenicmembrane was stripped from a further abscesscavity. A stent mould was made of the defect andpainted with mastasol, and a free graft cut fromthe thigh was wrapped on the mould raw surfaceoutwards, and placed into the defect. The mouldwas secured in position and left undisturbed forsix days. During the first four post-operativedays the bowels were constipated by oral tinct.opii. Healing was complete in ten days, and atthe end of six months there was no sign ofrecurrence (Fig. 4).
Case 2G.H.M.-male, aged 35 years. Occupation:
Officer in the Royal Navy. At the age of 33 yearshe developed an abscess in a pilonidal sinus.Immediate excision of the sinus and surroundingskin was carried out and direct primary suture ofthe subcutaneous fat and skin edges was performed.One month later a recurrence of the discharge wasnoticed. The sinus was re-excised, saucerized
;; :.. .. :........ .. . . :
V4
-Hi
. : .,.0
FIG. 4.-Case i. Natal cleft after free grafting.
and the wound was packed and allowed to granu-late. Four months later complete epithelializationhad not occurred and he was referred to this Unit.
Examination. Normal healthy man. C.V.S.C.N.S. R.S.-normal. B.P. 125/80. Urine-normal.
Perineum. There was a large unhealed areapresent in the natal cleft measuring 2 in. by 2 in.(Fig. 5).
Operation. Complete excision of the unhealedarea and surrounding skin edges was carried out,and mobilization and advancement of the gluteusmaximus on both sides of the cleft allowed directsuture of the muscle in the midline. The sub-cutaneous tissue and skin were then sutured under'moderate' tension with nylon mattress sutures.A small area of breakdown of the skin edges
occurred in the middle of the suture line, andalthough epithelialization occurred the suture lineremained unstable. Four months later the patientwas readmitted with a recurrence of the dischargeand a sinus.
Excision of the sinus and surrounding skintogether with all palpable scar tissue in the sub-cutaneous fat was performed. A Thiersch graftwas cut from the thigh, and was sutured into the
copyright. on M
ay 10, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.346.430 on 1 A
ugust 1954. Dow
nloaded from

August I9-54 WYNN WILLIAMS: Free Graft Repair in Pilonidal Sinius 433
.. .. ... .... .... ..... .. ... . : :.'! g
:............
FIG. 5.-Case 2. Natal cleft showing unhealed area.
defect. The cavity was then carefully packed withflavine wool, even pressure being obtained by blacksilk oversutures. The graft took well and thecavity was healed in ten days. Eight months laterthere was no evidence of recurrence (Fig. 6).
DiscussionIn considering the aetiology and pathology
little can be added, except to draw attention to thepossibility that those patients who present withmultiple recurrences, and 'have multiple sinusesopening in the natal fold close to the anus, presenta similar clinical picture to suppurativehidradenitis, in this condition no surgery fallingshort of excision ' en bloc' of all involved areasand subsequent skin graft, can be successful.
In assessing the value of split skin grafting of thedefect after excision of a pilonidal sinus nosuggestion is made that all cases should be treatedin this way. In the small non-infected cystswhere minimum excision is adequate, directclosure is the method of choice.
It is in those cases which have undergonerepeated inflammatory attacks of the cyst anddeveloped multiple sinus openings, or recurrencehas occurred after excision and direct closure, that
n:ii 1iin~
J.....
FIG. 6.-Case 2. Natal cleft after free grafting.
repair by a split skin graft is recommended. Itallows a wide and adequate excision down topresacral fascia and provides a simple method ofhealing the tissue defect with the result that thetime spent in hospital is lessened-a factor not tobe forgotten in the age group in which this condi-tion occurs. With adequate control of the bowelscontamination of the graft is eliminated. Chemo-therapy may be a useful adjunct, though in the twocases discussed, it was not given.A further factor of note is that after one primary
excision skin shortage plays a part in the recurrenceand by a free graft this defect can be corrected.Tenting of the skin over a subcutaneous cavity iseliminated and the possibility of haematomaformation, almost certainly a factor in recurrenceof this condition, is reduced.
Finally, the grafted skin rapidly settles in thenatal fold and becomes adherent to the presacralfascial thereby approximating to the normal natalfold skin.
I am most grateful to Mr. F. T. Moore for hisconstant help aand advice, and to Mr. G. Clemetsonfor the photographs.
Bibliography continued on next page
copyright. on M
ay 10, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.346.430 on 1 A
ugust 1954. Dow
nloaded from

434
/ at gclWt etsli
A new Operation Table forms part of the exhibitof Allen & Hanburys Ltd., at the Medical Exhibi-tion held in conjunction with the Annual Con-ference of the British Medical Association inGlasgow from July 5 to 9, 1954.
Since the latter half of the last century, Allen &Hanburys Ltd. have been producing OperationTables and it is interesting to study the changes indesign they have made to keep pace with modernsurgical practice.
M.
alw
--. .
---
The Model' J' Operation Table is a completelynew and advanced design in which all majoradjustments- are controlled from the head-end ofthe Table. This enables any adjustment ofposition of the Table to be made without inter-ruption of the surgical team. The adoption ofhead-end control has been achieved without anysacrifice of rigidity, the Table being completelyrigid in any of its extremely versatile range ofpositions and ensures ideal operation conditions.The following are details of its range of movement:Minimum height, 29 in.Maximum height, 43 in.Maximum Trendelenburg, 450*Reverse Trendelenburg, 300.Lateral Tilt, Left and Right, 200.
The table top is cast in corrosion-resistantaluminium alloy with a satin finish. The headflap is extendable and allows for fine angularadjustments and instant removal from the Table.The leg flap also is fully adjustable and can be
removed instantly from the Table in any position.A carefully proportioned perineal recess allowsmaximal exposure of the perineum for all diagnosticand surgical procedures with the patient in thelithotomy position. A built-in back elevator iscontrolled from the head-end of the Table.
All main gear mechanisms are enclosed andparticular attention has been given to the overalldesign so as to make routine cleaning and main-tenance simple in the extreme.
For many years past, Allen & Hanburys Ltd.,have achieved a large measure of export businessin Operation Tables and it is considered that thisTable, which combines unrivalled engineeringcraftsmanship with undisputed leadership indesign, will maintain their leading position in theexport field.
Menley & James, Limited, PharmaceuticalManufacturers, Coldharbour Lane, London, S.E.s,announce a new addition to their ' Eskacillin 'range of palatable liquid oral penicillins-' Eska-cillin' 200. This new high strength presents200,000 I.U. procaine penicillin per standardmedical teaspoonful (i fl. drachm: 3.5 ml.).' Eskacillin' 200 is indicated for the treatment ofpenicillin-sensitive infections. The dosage forchildren up to eight years is one teaspoonful threeor four times a day, and for older children andadults two to three teaspoonfuls three or fourtimes a day. ' Eskacillin ' 200 is available, on pre-scription only, in 2 fl. oz. (56 ml.) bottles.
Continuedfrom previous page-D. WYNN WILLIAMS, M.S.(LOND.), F.R.C.S.
BIBLIOGRAPHYBLAND-SUTTON, SIR JOHN (1917), 'Tumours Innocent and
Malignant,' 6tk edition, p. 526, Cassell and Co.PATEY, D. H., and SCARFF, R. W. (I946), Lancet, ii, 484.KING, E. S. J. (1947), Austr. & N. Zeal. J3. of Surgery, I6, I82.DAVIES, L. S.,and STARR, K, W. (I14$), S.G. & O., gI, 309,
KOOISTRA, H. P. (I942), Am.9. Surg., 45, 3.POPE, C. E., and HUDSON, H. W. (I946), Arch. of Surg., 52, 690.BREZIN, C. (I943), Am. J. Surg., 59, i8.BOGER, E. V., and PINKHAM, E. W. (i9$), U.S. Armed Frces
med.,.-, 2, 1733.
copyright. on M
ay 10, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.346.430 on 1 A
ugust 1954. Dow
nloaded from