Embed Size (px)
Citation preview

Never Events Overview:Fran Watts
Patient Safety Lead –Never Events
NHS Improvement and NHS England
Never Events Overview
• Definitions
• Overview
• Facts and figures- increases during COVID
• Role of Never Events team
• Grading of Never Events and Serious Incidents
• Review of grading wrong site surgery for dermatology
3 |
Never Events are patient safety incidents that are wholly preventable where guidance or safety recommendations* that provide strong systemic protective barriers are available at a national level and have been implemented by healthcare providers.
Current definition of NE ‘barriers’
4 |
CQC report - 2018
Recommendation:
NHS Improvement should work
with professional regulators and
royal colleges to review the
Never Events framework,
focusing on leadership and
safety culture, and exploring the
barriers to preventing errors
such as human behaviours.
5 |
• The Never Events policy framework describes strong systemic protective barriers as:
➢ physical barriers (e.g. equipment that makes it impossible to connect medications via the wrong route); time and place barriers (e.g. withdrawal of concentrated medications from settings to prevent them being accidentally selected) or systems of double or triple checking where these are supported by visual or computerised warnings, standardised procedures or memory/communication aids. As all human action is vulnerable to human error, particularly where there is a risk of staff becoming overloaded, processes that rely solely on one staff member checking the actions of another or referring to written policies are not strong barriers.
Strong systemic safety barriers
Presentation title
6 |
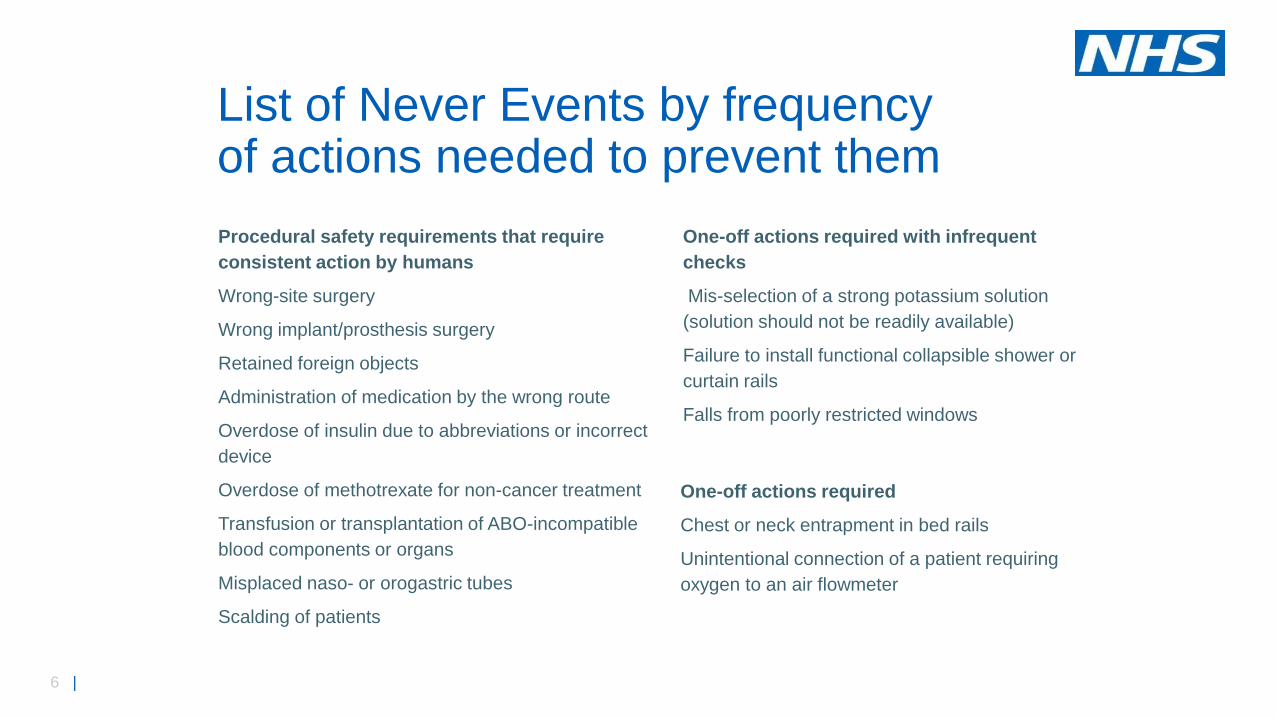
List of Never Events by frequency of actions needed to prevent them
Procedural safety requirements that require
consistent action by humans
Wrong-site surgery
Wrong implant/prosthesis surgery
Retained foreign objects
Administration of medication by the wrong route
Overdose of insulin due to abbreviations or incorrect
device
Overdose of methotrexate for non-cancer treatment
Transfusion or transplantation of ABO-incompatible
blood components or organs
Misplaced naso- or orogastric tubes
Scalding of patients
One-off actions required with infrequent
checks
Mis-selection of a strong potassium solution
(solution should not be readily available)
Failure to install functional collapsible shower or
curtain rails
Falls from poorly restricted windows
One-off actions required
Chest or neck entrapment in bed rails
Unintentional connection of a patient requiring
oxygen to an air flowmeter

7 |
BEFORE AFTER
Some Never Events are about designing out the error (‘act once’)
Human factors engineering – understand what is leading to error/harm and change the equipment, not the human
8 |
• Conducting a review of the Never Events list to explore the strength of the barriers for each Never Event
• Where there are numerous sub types to the Never Event, for example the three surgical Never Events, identifying the top five most frequently occurring:
➢Wrong site surgery – wrong tooth removal, wrong site block, wrong eye injections, wrong side spinal injections and wrong skin lesions
➢Wrong implant/ prosthesis – lens, hip, knee, IUCD and stents
➢Retained foreign objects post procedure -
NHSI response to the CQC recommendation
9 |
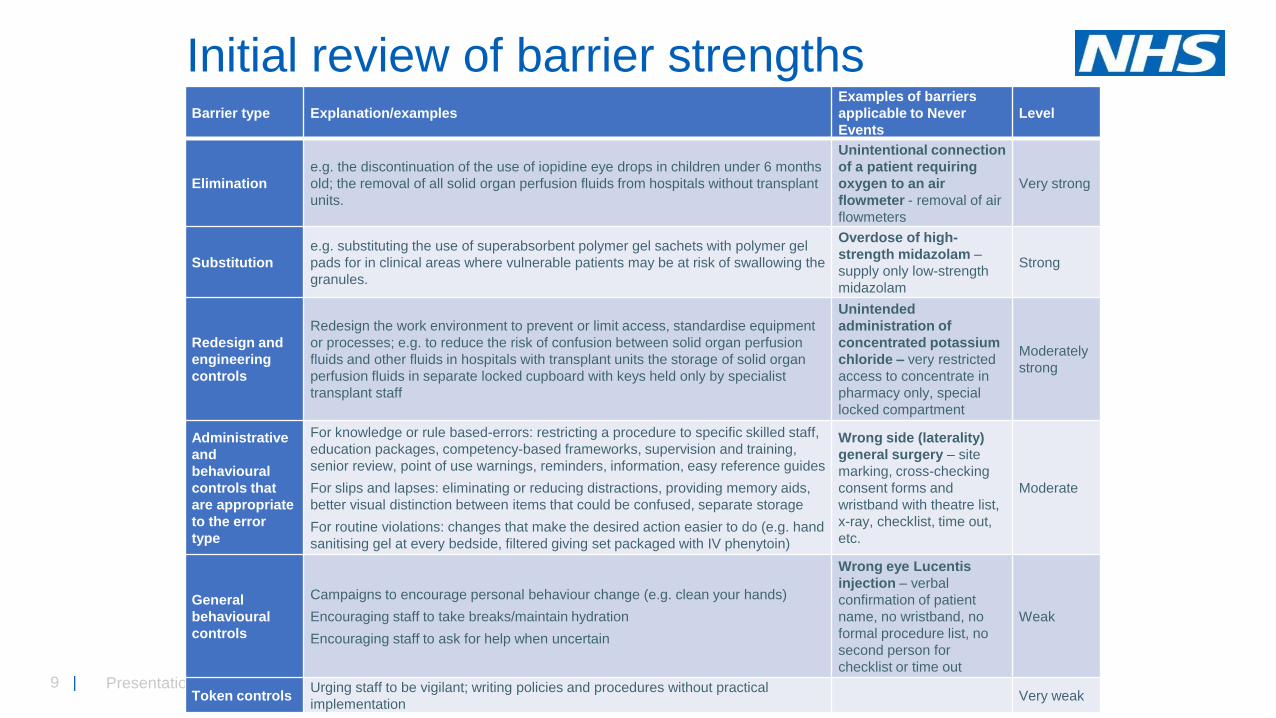
Initial review of barrier strengths
Presentation title
Barrier type Explanation/examples
Examples of barriers
applicable to Never
Events
Level
Elimination
e.g. the discontinuation of the use of iopidine eye drops in children under 6 months
old; the removal of all solid organ perfusion fluids from hospitals without transplant
units.
Unintentional connection
of a patient requiring
oxygen to an air
flowmeter - removal of air
flowmeters
Very strong
Substitution
e.g. substituting the use of superabsorbent polymer gel sachets with polymer gel
pads for in clinical areas where vulnerable patients may be at risk of swallowing the
granules.
Overdose of high-
strength midazolam –
supply only low-strength
midazolam
Strong
Redesign and
engineering
controls
Redesign the work environment to prevent or limit access, standardise equipment
or processes; e.g. to reduce the risk of confusion between solid organ perfusion
fluids and other fluids in hospitals with transplant units the storage of solid organ
perfusion fluids in separate locked cupboard with keys held only by specialist
transplant staff
Unintended
administration of
concentrated potassium
chloride – very restricted
access to concentrate in
pharmacy only, special
locked compartment
Moderately
strong
Administrative
and
behavioural
controls that
are appropriate
to the error
type
For knowledge or rule based-errors: restricting a procedure to specific skilled staff,
education packages, competency-based frameworks, supervision and training,
senior review, point of use warnings, reminders, information, easy reference guides
For slips and lapses: eliminating or reducing distractions, providing memory aids,
better visual distinction between items that could be confused, separate storage
For routine violations: changes that make the desired action easier to do (e.g. hand
sanitising gel at every bedside, filtered giving set packaged with IV phenytoin)
Wrong side (laterality)
general surgery – site
marking, cross-checking
consent forms and
wristband with theatre list,
x-ray, checklist, time out,
etc.
Moderate
General
behavioural
controls
Campaigns to encourage personal behaviour change (e.g. clean your hands)
Encouraging staff to take breaks/maintain hydration
Encouraging staff to ask for help when uncertain
Wrong eye Lucentis
injection – verbal
confirmation of patient
name, no wristband, no
formal procedure list, no
second person for
checklist or time out
Weak
Token controlsUrging staff to be vigilant; writing policies and procedures without practical
implementation Very weak

10 |
Collaboration with experts from the relevant medical royal colleges and other organisations with an interest in Never Events.
Three questions:
➢ Are the barriers for this Never Event strong enough to prevent it?
➢Are there any barriers currently that have not been considered?
➢Can any new barriers be developed to them from happening?
➢
Focus groups
11 |
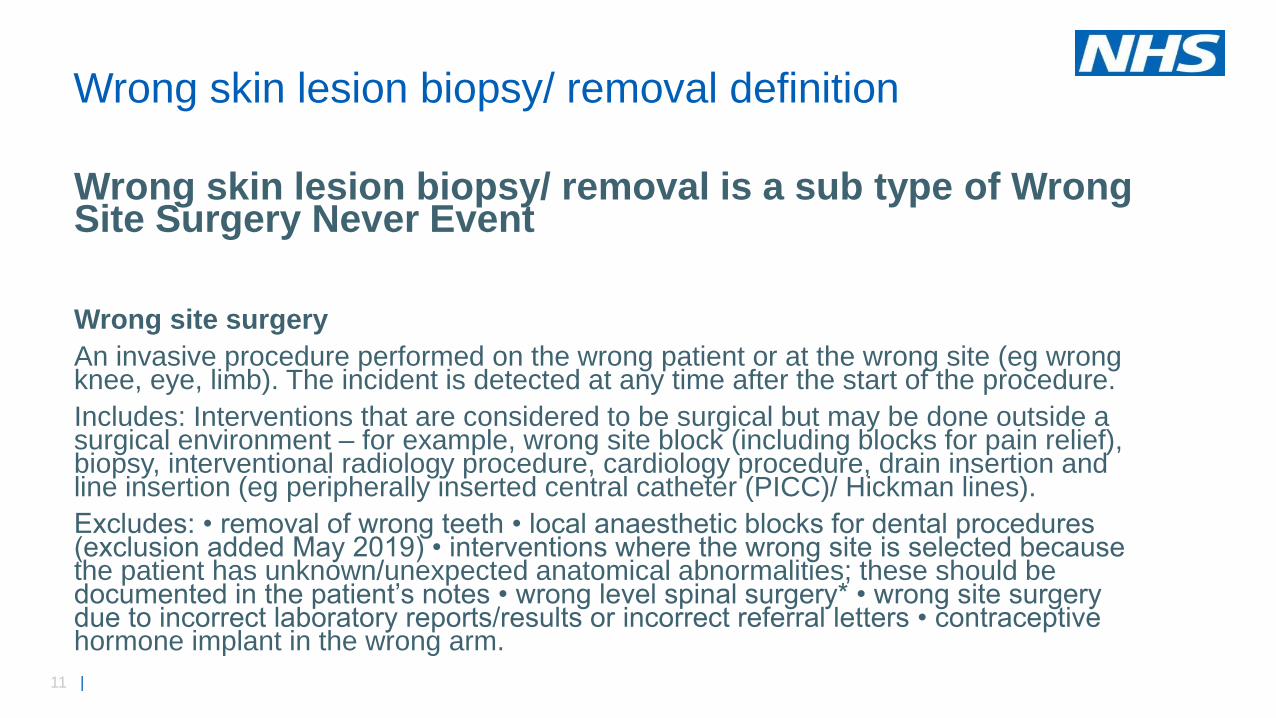
Wrong skin lesion biopsy/ removal is a sub type of Wrong Site Surgery Never Event
Wrong site surgery
An invasive procedure performed on the wrong patient or at the wrong site (eg wrong knee, eye, limb). The incident is detected at any time after the start of the procedure.
Includes: Interventions that are considered to be surgical but may be done outside a surgical environment – for example, wrong site block (including blocks for pain relief), biopsy, interventional radiology procedure, cardiology procedure, drain insertion and line insertion (eg peripherally inserted central catheter (PICC)/ Hickman lines).
Excludes: • removal of wrong teeth • local anaesthetic blocks for dental procedures (exclusion added May 2019) • interventions where the wrong site is selected because the patient has unknown/unexpected anatomical abnormalities; these should be documented in the patient’s notes • wrong level spinal surgery* • wrong site surgery due to incorrect laboratory reports/results or incorrect referral letters • contraceptive hormone implant in the wrong arm.
Wrong skin lesion biopsy/ removal definition
12 |
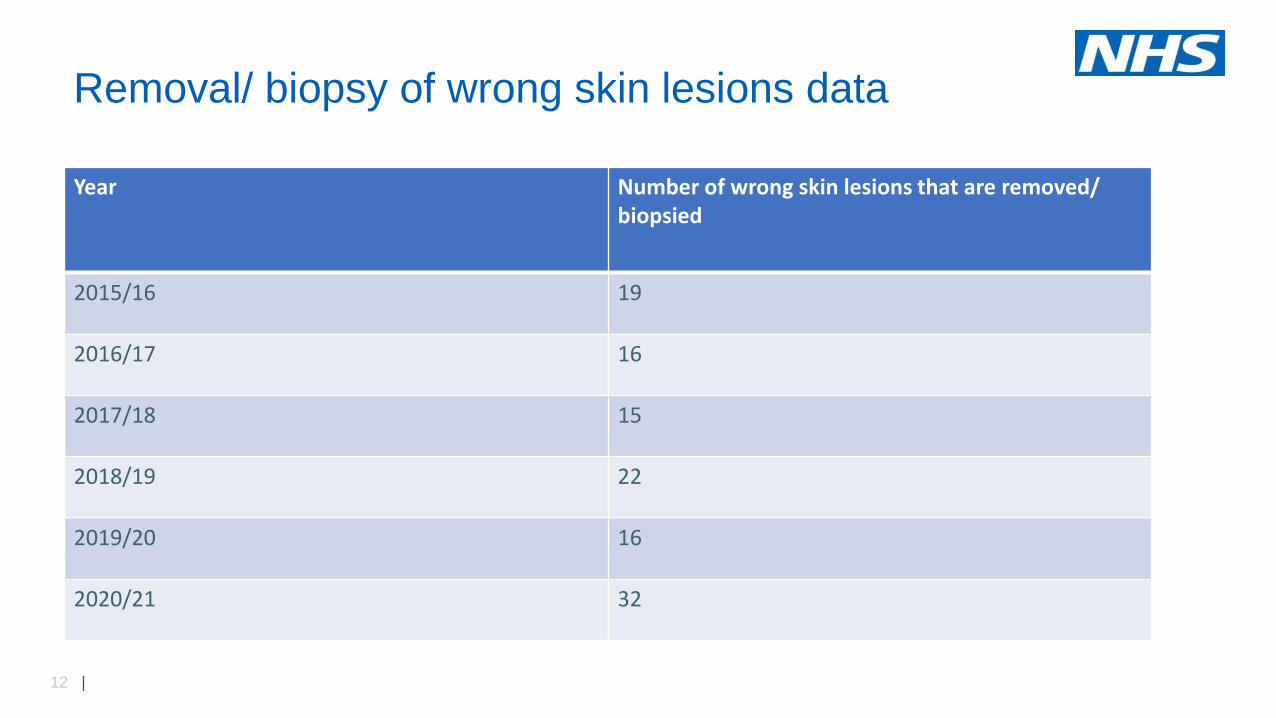
Year Number of wrong skin lesions that are removed/ biopsied
2015/16 19
2016/17 16
2017/18 15
2018/19 22
2019/20 16
2020/21 32
Removal/ biopsy of wrong skin lesions data

13 |
Where the lesions are Number
Back 15
Nose 7
Ear 2
Scalp 2
Thigh 1
Neck 1
Chest 1
Cheek 1
Not known 2
Total 32
Location of skin lesions – 2020/21
14 |
• The patient called to say that they had a minor op procedure to remove a mole from their back and on returning home, their partner informed her that the wrong mole had been removed. She contacted the department and was advised to attend for review
• The patient was scheduled to attend an appointment for excision of a biopsy proven basal cell carcinoma on the right side of the nose. The patient attended their outpatient appointment , however the procedure was carried out on the left side of the nose. Awaiting biopsy results and the Consultant will be reviewing the patient in outpatients.
• A patient with Atypical Mole Syndrome, was seen in the dermatology clinic and 5 moles were identified for removal. The 18 week team (team undertaking the surgery) then saw the patient for removal of 3 moles from her thighs (2 from the right and one from the left). Three moles were removed however when the patient was reviewed prior to having the other 2 moles removed, it was noted that the numbering on the photos did not match the body map/ healthcare records and as a result the moles that were removed were not all the correct ones and wrong site surgery had occurred. The patient has now re-attended for removal of the intended moles.
Examples of incident reports

15 |
Role of the national patient safety team –the challenge of safe care

How we support you to keep your patients safe
17 |
NHS England » Our National Patient Safety Alerts/
NHS England » Patient safety review and response reports
Your incident reports help us and our
partners make a difference….
18 |
We will continue to systematically review the list of Never Events to explore which sub types of Never Events do not meet the definition of a Never Event and could potentially be removed from the list.
Next steps for the Never Events review
19 |
Questions?





























