Embed Size (px)
Citation preview

MANAGEMENT OF PROXIMAL AND DISTAL HUMERUS FRACTURES 0030-5898/00 $8.00 + .OO
FRACTURES OF THE DISTAL HUMERUS
Role of Elbow Replacement
Bernard F. Morrey, MD
Rigid osteosynthesis and early motion is the well-accepted norm to treat distal humeral fracture~.’~J~,~* In a review of 846 procedures from 13 reports of open reduction and internal fixation of intra-articular fractures of the distal humerus, however, 20% of the patients had an unsatisfactory outcome.z0 Open reduction and internal fixation can be complicated or impos- sible in elderly patients with marked intra- articular comminution. Joint stiffness, loss of reduction, and early posttraumatic osteoar- throsis are common s e q ~ e l a e . ’ ~ ~ ~ ’ ~ ~ ~ As an al- ternative to open reduction and internal fixa- tion, patients older than age 65 years with extensive comminution, replacement with a semiconstrained elbow implant is a reasonable c~nsideration.~ In older patients, because of os- teoporosis and comminution, in some, rigid fixation cannot be attained, and nonunion re- sults. Few options exist to manage this difficult problem reliably once established. Excision of the nonunited segment and replacement with a prosthetic device has proven to be effective and sometimes the only option under these circumstances.30
Posttraumatic osteoarthrosis differs from acute traumatic conditions and nonunion in several aspects and poses more difficulties in the treatment. Elbows with posttraumatic ar- throsis are often characterized by a chronic
painful stiffness, soft tissue contracture, joint and bone deformity, and instability. The typi- cal circumstance of having undergone numer- ous previous procedures results in a poor soft tissue envelope, damaged and hypersensitive nerves, and a predisposition for infect i~n.~~
Few options exist for operative treatment of severe posttraumatic arthrosis. Arthrodesis reliably relieves painz6 and restores a strong extremity. Because it results in great functional
however, arthrodesis of the el- bow rarely is considered a viable 0ption.9,~~ In- terposition arthroplasty may be considered for young patients, particularly those who have stiffness. This procedure has an even higher rate of complications than that associated with semiconstrained total elbow rep1a~ement.l~ For severe posttraumatic osteoarthrosis, total elbow replacement using the semiconstrained Coonrad-Morrey (Zimmer, Warsaw, IN) pros- thesis has proven to be a suitable and reliable option for older patients.
INDICATIONS
Acute Trauma
The indication for semiconstrained total joint replacement for acute fractures of the dis- tal humerus is limited to a restricted group
From the Department of Orthopedic Surgery, Mayo Clinic, Rochester, Minnesota ~ ~~ ~~ ~~
ORTHOPEDIC CLINICS OF NORTH AMERICA
VOLUME 31 *NUMBER 1 *JANUARY 2000 145

146 MORREY
of patients older than 60 to 65 years with an extensively comminuted fracture that is not amenable to an adequate and stable osteo- synthesis. The usual findings are (1) severe comminution with multiple small fragments, (2) severely osteoporotic bone, and (3) preex- isting joint damage in patients with rheuma- toid arthritis or other inflammatory joint dis- eases. The fact that at the Mayo Clinic only 22 acute distal humerus fractures (10 of them having associated rheumatoid arthritis) were treated by total joint replacement during a 10- year period emphasizes the strict selection cri- teria.4
Nonunion
If the nonunited fragment is at or distal to the level of the olecranon fossa, replacement is possible without altering extremity length or muscle tension (Fig. 1). Patients with non- united fragments of the distal humerus who are older than 60 to 65 years old are considered candidates for elbow replacement.
Traumatic Arthrosis
Fracture frequently causes arthrosis re- quiring treatment by replacement. There is lit- tle in the literature about the outcome of total elbow replacement for posttraumatic prob- lems. Advanced destruction of the ulnohu- meral joint with marked narrowing or loss of the joint space in patients who are older than age 60 constitutes the basis for semiconstrained elbow joint replacement. Even in this age group, however, participation in heavy physi- cal work and anticipated noncompliance are considered relative contraind ications for this procedure. For young patients with a severe posttraumatic osteoarthrosis, interposition ar- throplasty may be considered as first choice of treatment rather than total joint replacement. In cases of failed interposition arthroplasty, to- tal joint replacement is the treatment of choice for most patients.
Figure 1. With bone loss at the level of the roof of the olecranon fossa, the axis of rotation remains at the ana- tomic level (A). The flange allows resistance of posterior- directed and rotatory forces (B).
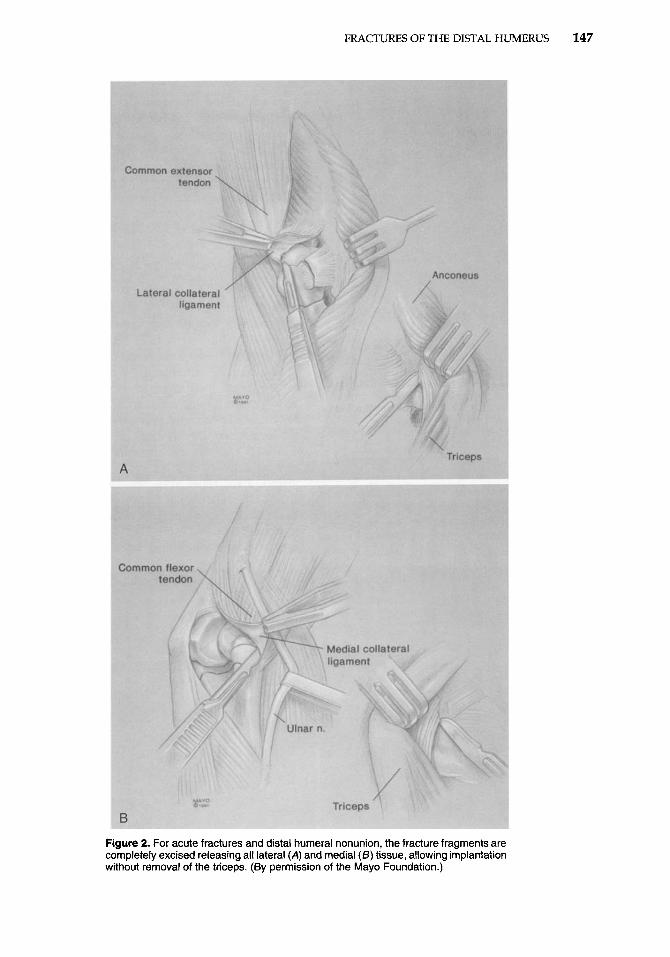
cutaneous pocket if this had not been previ- ously performed. For acute fractures and distal humeral nonunion, preservation of the triceps attachment is possible because in these circum- stances the triceps insertion can be left intact. This is because the fracture is treated by exci- sion allowing articulation with the humeral component fully seated. Otherwise, the triceps reflection technique of Bryan and Morrey3 is performed. To preserve the triceps attachment, all soft tissues are released from the bone frag- ments of the distal humerus, which then are excised (Fig. 2). The distal humerus is then ex- posed from the lateral margin of the triceps. The ulna is exposed from the medial side by rotating the forearm internally. The triceps is partially released to facilitate this maneuver. For conditions with an intact distal humerus, the cutting guide is used to prepare the distal humerus, and the ulna is prepared with serial rasps. An intramedullary injecting system is used for optimal insertion of the cement to which 1 g of vancomycin is added. An impor- tant element is the placement of a bone graft, harvested from a fracture fragment or the re- sected trochlea, between the anterior flange and the distal part of the humerus. After in- growth, this graft is believed to resist posterior displacement and rotational stresses on the humeral comp~nen t .~~ The semiconstrained Coonrad-Moriey device is preferred by the au- thor in all instances (Fig. 3). Significant bone- stock deficiencies with lack of one or both epicondyles do not change or complicate the implantation of the humeral component
TECHNIQUE
A posterior midline incision is used. The ulnar nerve is transposed anteriorly in a sub-
FRACTURES OF THE DISTAL HUMERUS 147
Figure 2. For acute fractures and distal humeral nonunion, the fracture fragments are completely excised releasing all lateral (A) and medial (5) tissue, allowing implantation without removal of the triceps. (By permission of the Mayo Foundation.)
148 MORREY
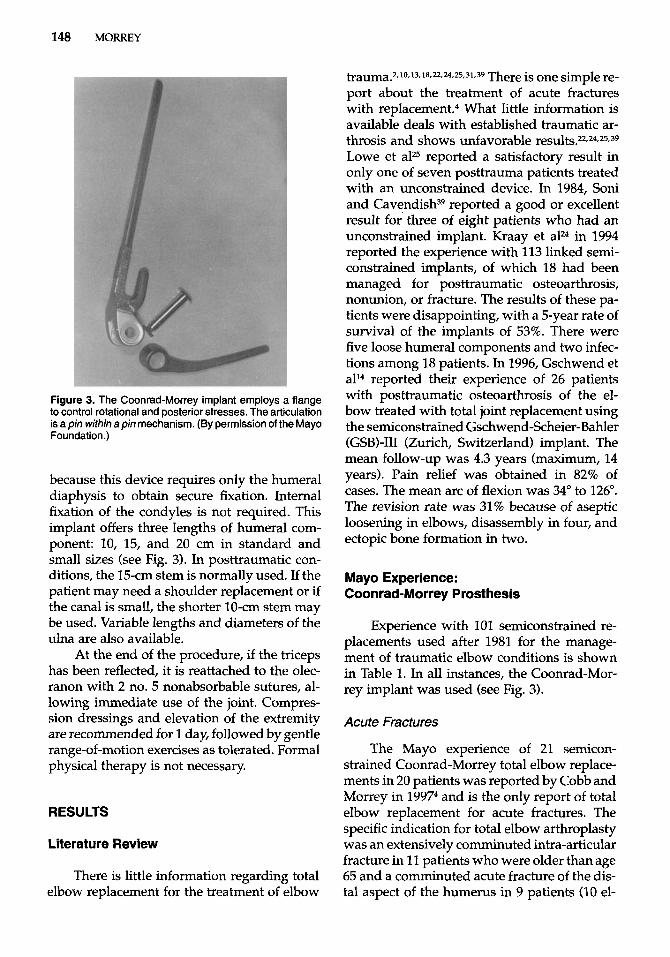
Figure 3. The Coonrad-Morrey implant employs a flange to control rotational and posterior stresses. The articulation is a pin within a pin mechanism. (By permission of the Mayo Foundation.)
because this device requires only the humeral diaphysis to obtain secure fixation. Internal fixation of the condyles is not required. This implant offers three lengths of humeral com- ponent: 10, 15, and 20 cm in standard and small sizes (see Fig. 3). In posttraumatic con- ditions, the 15-cm stem is normally used. If the patient may need a shoulder replacement or if the canal is small, the shorter 10-cm stem may be used. Variable lengths and diameters of the ulna are also available.
At the end of the procedure, if the triceps has been reflected, it is reattached to the olec- ranon with 2 no. 5 nonabsorbable sutures, al- lowing immediate use of the joint. Compres- sion dressings and elevation of the extremity are recommended for 1 day, followed by gentle range-of-motion exercises as tolerated. Formal physical therapy is not necessary.
RESULTS
Literature Review
There is little information regarding total elbow replacement for the treatment of elbow
t r a ~ m a . ~ , ~ ~ , ~ ~ , ~ ~ ~ ~ , ~ ~ , ~ , ~ ~ , ~ ~ There is one simple re- port about the treatment of acute fractures with repla~ement.~ What little information is available deals with established traumatic ar- throsis and shows unfavorable r e s ~ l t s . ~ , ~ ~ , ~ ~ , ~ ~ Lowe et aP5 reported a satisfactory result in only one of seven posttrauma patients treated with an unconstrained device. In 1984, Soni and Cavendi~h~~ reported a good or excellent result for three of eight patients who had an unconstrained implant. Kraay et a P in 1994 reported the experience with 113 linked semi- constrained implants, of which 18 had been managed for posttraumatic osteoarthrosis, nonunion, or fracture. The results of these pa- tients were disappointing, with a 5-year rate of survival of the implants of 53%. There were five loose humeral components and two infec- tions among 18 patients. In 1996, Gschwend et all4 reported their experience of 26 patients with posttraumatic osteoarthrosis of the el- bow treated with total joint replacement using the semiconstrained Gschwend-Scheier-Bahler (GSB)-I11 (Zurich, Switzerland) implant. The mean follow-up was 4.3 years (maximum, 14 years). Pain relief was obtained in 82% of cases. The mean arc of flexion was 34" to 126". The revision rate was 31% because of aseptic loosening in elbows, disassembly in four, and ectopic bone formation in two.
Mayo Experience: Coonrad-Morrey Prosthesis
Experience with 101 semiconstrained re- placements used after 1981 for the manage- ment of traumatic elbow conditions is shown in Table 1. In all instances, the Coonrad-Mor- rey implant was used (see Fig. 3).
Acute Fractures
The Mayo experience of 21 semicon- strained Coonrad-Morrey total elbow replace- ments in 20 patients was reported by Cobb and Morrey in 19974 and is the only report of total elbow replacement for acute fractures. The specific indication for total elbow arthroplasty was an extensively comminuted intra-articular fracture in 11 patients who were older than age 65 and a comminuted acute fracture of the dis- tal aspect of the humerus in 9 patients (10 el-
FRACTURES OF THE DISTAL HUMERUS 149
Table 1. EXPERIENCE WITH COONRAD/MORREY ELBOW REPLACEMENT FOR TRAUMATIC CONDITIONS
Objective Subjective FOIIOW-UP Condition No. Year (satisfaction percentage) (satisfaction percentage) (Y r)
Acute 21 1997 YO 95 4 Arthrosis 41 1997 73 90 6 Nonunion 39 1995 88 92 5 Totul/Meun 101 86 92 5
bows) who also had destruction of the articu- lar surface secondary to rheumatoid arthritis. The mean age of the patients at the time of injury was 72 years (range, 48 to 92 years). Fol- low-up averaged 3.3 years. Subjectively, all 20 patients were satisfied (Fig. 4). On the basis of the Mayo elbow performance score,28 15 el- bows had an excellent result and 5 had a good result. Pain relief was reliably obtained, with 17 patients having no pain and 3 patients having mild pain. The mean arc of flexion- extension was 25" to 130", and the mean arc of pronation-supination was 74" to 73". With a maximum follow-up of 10.5 years, there were no loose implants. Severe osteoporosis was common but did not appear to influence the functional result. One patient fell while sailing and fractured the ulnar component. At 8 years after revision, this retired surgeon is without pain and fully functional. Based on this expe-
rience, it appears that semiconstrained Coon- rad-Morrey total elbow replacement for acute fractures of the distal aspect of the humerus can be a reliable treatment in a specific group of elderly patients, but it is not an alternative procedure to osteosynthesis in younger pa- tients.
Posttraumatic Arthritis
A review of the Mayo experience was pre- sented in 1997 by Schneeberger et aI3* and con- sists of 41 consecutive patients with posttrau- matic osteoarthrosis or dysfunction treated from 1981 to 1993 by semiconstrained Coon- rad-Morrey elbow replacement and followed an average of almost 6 years. The average age of the patients was 57 years (range, 32 to 82 years). The indication for joint replacement was pain for 36 patients; reduced, painful
Figure 4. A, Comminuted distal humeral fracture in a 79-year-old woman. 6, Patient is asymptomatic with essentially normal function 6 years after joint replacement. (By per- mission of the Mayo Foundation.)
150 MORREY
range of motion for 2 patients; and dysfunc- tion with a flail elbow for 3 patients. The av- erage time from the original fracture to the joint replacement was 16 years (range, 3 months to 64 years).
This is a difficult group of patients to manage. All but two patients (95%) had had previous surgery, the average being 2.3 pro- cedures (range, 0 to 7 procedures). Significant bone-stock deficiency with loss of at least one condyle was present in 13 patients, and 14 patients had a significant joint or home de- formity. Ten of 41 elbow joints were pre- operatively subluxed, and 7 were dislocated. Additional complications from prior surgery included mild to moderate ulnar neuropathy in six patients and radial nerve palsy resulting from a complete traumatic laceration in one patient.
At the latest follow-up, objectively, 40% were rated excellent and 43% were considered good for an overall rate of 83% satisfactory ob- jective outcome. Subjectively, 95% of the pa- tients with a functioning implant expressed satisfaction with the operation. Although the incidence of pain relief (76%) was considered to be high, it was not as high as that reported after the treatment of rheumatoid arthritis (93%h30 At follow-up, the mean arc of flexion- extension was 27" to 131", and the mean arc of pronation-supination was 66" to 66" (Fig. 5). An average of 4.8 of 5 activities of daily living could be performed, and strength improve- ment averaged approximately 30%. The radio- logic analysis showed that all grafts behind the flange incorporated. There were no cases of aseptic loosening within the 12 years of
The follow-up of 41 patients to 12 years is the most comprehensive in the literature and shows that severe posttraumatic osteoar- throsis or dysfunction can be reliably and du- rably treated with a noncustomized semicon- strained device. Patient satisfaction was high. All implants were stable, and function was re- liably restored.
follow-up.
Distal Humeral Nonunion
Experience with 39 procedures all em- ploying a triceps attachment-preserving ex-
posure, excision of the fragment, and insertion of a noncustom 15-cm Coonrad-Morrey hu- meral stem was Surveillance av- eraged almost 5 years (range, 2 to 10 years). In this sample, subjective pain relief exceeded 90%, and the mean arc of motion was 25" to 130". Objectively, 88% had satisfactory Mayo Elbow Performance Scores, and 91 % were sub- jectively satisfied with the procedure (Fig. 6).
In this report, no patient had mechanical loosening. Infection occurred in two patients and ulnar nerve irritation in one. The bushing became excessively worn in two patients, and one patient had a major wound dehiscence. Considering the nature of the pathology, the frequency of prior surgery, and previous com- plications, the complication rate of this expe- rience appears understandable. As greater sur- veillance is obtained, it is anticipated that the incidence of wear and lysis will increase as well. Considering that few options exist to manage this difficult problem, it appears that the overall outcome is acceptable with joint re- placement.
Complications
The complications from these three re- ports are shown in Table 2. At least one major postoperative complication occurred in 2 (10%) of 20 patients with an acute fracture and in 13 (27%) of 41 patients in the posttraumatic group. Gschwend et all5 in 1996 described a compli- cation rate of 43% from a meta-analysis of 22 publications of total elbow replacement, and most of these were performed for rheumatoid arthritis, which cases usually are associated with fewer complications compared with cases with posttraumatic osteoarthrosis.
Most complications are of a mechanical nature. In several instances, the C locking ring has become disengaged, but no pin in the au- thor's practice has backed out because of this. Fracture of the ulnar component occurred in one prosthesis in the acute fracture group and in five elbows in the posttraumatic group 2 to 9 years (average, 4.3 years) postoperatively. Before breakage, four patients had an excellent result and two a good result with an asymp- tomatic elbow and essentially normal func- tion. The cause of failure were severe noncom-

FRACTURES OF THE DISTAL HUMERUS 151
Figure 5. A and B, Severe arthrosis with posterior subluxation after open reduction with internal fixation (ORIF) and hardware removal. Cand 0, Excellent result at 3years. (By permission of the Mayo Foundation.)
pliance, such as regular lifting of weights of more than 50 kg in two patients. The fractures occurred through the beaded portion of the implant as a result of the notch effect created by the beads on the titanium implant. Revision required recementation into the same cement mantle. There were no operative or delayed complications from the reoperation.
Because the fractures of the ulnar com- ponent always occurred at the site of sintered beads, in 1991, the beads were replaced by a precoat of methyl methacrylate. No fractures of precoated ulnar components have been ob- served to date. Two patients of the group of posttraumatic osteoarthrosis presented with a particulate synovitis associated with worn
152 MORREY
Figure 6. A and B, Gross deformity after failed open reduction with internal fixation (ORIF). C, Excellent relief of pain and function 76 years after replacement. (By permission of the Mayo Foundation.)
bushings. In one patient, wear of the bushings was attributed to excessive overuse of the el- bows with heavy repetitive work (Fig. 7). Both cases also had a significant preoperative de- formity. Worn bushings cause a black synovitis and over time result in osteolysis. Treatment of worn bushings consists of synovectomy and exchange of the bushings resulting in a satis- factory outcome. One expectation is that wear will become an increasing problem over time.
Despite the use of semiconstrained de- vices, most series of posttraumatic arthrosis are still complicated by 10osening.~~ Other than the author’s experience, only Figgie et allo and Gschwend et all4 reported minimal problems from loosening. No loosening was observed by Figgie et allo in their series of nine semicon- strained triaxial prostheses with custom-de- signed stems for the treatment of posttrau- matic conditions. Gschwend et all4 reported on
FRACTURES OF THE DISTAL HUMERUS 153
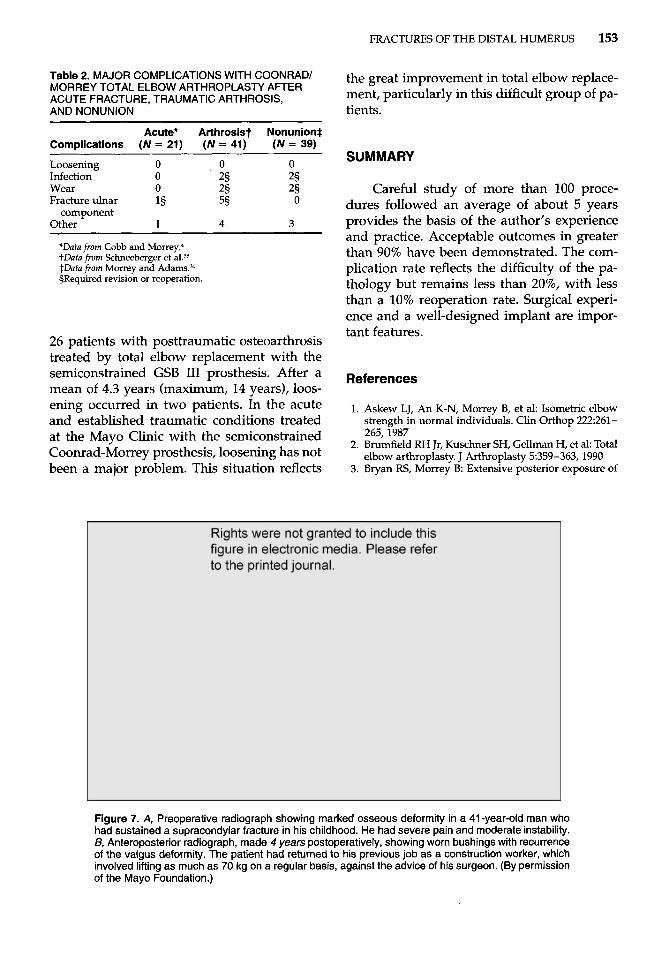
Table 2. MAJOR COMPLICATIONS WITH COONRADI MORREY TOTAL ELBOW ARTHROPLASTY AFTER ACUTE FRACTURE, TRAUMATIC ARTHROSIS, AND NONUNION
Acute* Arthrosist Nonunion* Complications (N = 21) (N = 41) (N = 39)
Loosening 0 0 0 Infection 0 2§ 2§
2§ 0
Wear 0 2§ Fracture ulnar 18 5§
Other 1 4 3 component
*Data from Cobb and M ~ r r e y . ~ tData from Schneeberger et al.38 $Data from Morrey and Adamsm §Required revision or reoperation.
26 patients with posttraumatic osteoarthrosis treated by total elbow replacement with the semiconstrained GSB I11 prosthesis. After a mean of 4.3 years (maximum, 14 years), loos- ening occurred in two patients. In the acute and established traumatic conditions treated at the Mayo Clinic with the semiconstrained Coonrad-Morrey prosthesis, loosening has not been a major problem. This situation reflects
the great improvement in total elbow replace- ment, particularly in this difficult group of pa- tients.
SUMMARY
Careful study dures followed an
of more than 100 proce- average of about 5 years
provides the basis of the author’s experience and practice. Acceptable outcomes in greater than 90% have been demonstrated. The com- plication rate reflects the difficulty of the pa- thology but remains less than 20%, with less than a 10% reoperation rate. Surgical experi- ence and a well-designed implant are impor- tant features.
References
Askew LJ, An K-N, Morrey B, et al: Isometric elbow strength in normal individuals. Clin Orthop 222261- 265,1987 Brumfield RH Jr, Kuschner SH, Gellman H, et al: Total elbow arthroplasty. J Arthroplasty 5359-363,1990 Bryan RS, Morrey B: Extensive posterior exposure of
Figure 7. A, Preoperative radiograph showing marked osseous deformity in a 41 -year-old man who had sustained a supracondylar fracture in his childhood. He had severe pain and moderate instability. B, Anteroposterior radiograph, made 4 years postoperatively, showing worn bushings with recurrence of the valgus deformity. The patient had returned to his previous job as a construction worker, which involved lifting as much as 70 kg on a regular basis, against the advice of his surgeon. (By permission of the Mayo Foundation.)
154 MORREY
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19. .
20.
21.
22.
the elbow: A triceps-sparing approach. Clin Orthop
Cobb T, Morrey B: Total elbow replacement as primary treatment for distal humeral fractures in elderly pa- tients. J Bone Joint Surg Am 79826-832,1997 Davis RF, Weiland AJ, Hungerford DS, et al: Noncon- strained total elbow arthroplasty. Clin Orthop 171:
Dee R Total replacement arthroplasty of the elbow for rheumatoid arthritis. J Bone Joint Surg Br 54:88-95, 1972 Dee R Nonimplantation salvage of failed reconstruc- tive procedures of the elbow. In Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, WB Saun- ders, 1993, pp 690-695 DeLee JC: Fractures and dislocations of the hip. In Rockwood CA Jr, Green DP, Bucholz RW, et a1 (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, Lippincott-Raven, 1996, p 1687 Ewald FC, Jacobs M: Total elbow arthroplasty. Clin Or-
Figgie E 111, Inglis AE, Ranawat CS, et a1 Results of total elbow arthroplasty as a salvage procedure for failed elbow reconstructive operations. Clin Orthop
Froimson AI, Silva JE, Richey M Cutis arthroplasty of the elbow joint. J Bone Joint Surg Am 58:863-865,1976 Garrett JC, Ewald FC, Thomas WH, et al: Loosening associated with GSB hinge total elbow replacement in patients with rheumatoid arthritis. Clin Orthop 127
Gschwend N, Loehr J, Ivosevic-Radovanovic D, et a1 Semiconstrained elbow prosthesis with special refer- ence to the GSB 111 prosthesis. Clin Orthop 232:104-
166~188-192,1982
156-160,1982
thop 182:137-142,1984
219:185-193,1987
170-174,1977
--. .__^ 11 1, I Y W Gschwend N, Scheier H, Bahler A, et al: GSB 111 elbow. In Riither W (ed): The Elbow, Endoprosthetic Replace- ment and Non-endoprosthetic Procedures. Berlin, Springer, 1996, pp 83-98 Gschwend N, Simmen BR, Matejovsky Z Late com- plications in elbow arthroplasty. J Shoulder Elbow Surg 5:86-96,1996 Helfet DL, Schmerling GJ: Bicondylar intra-articular fractures of the distal humerus in adults. Clin Orthop
Hughes RE, Schneeberger AG, An K-N, et al: Reduc- tion of triceps muscle force after shortening of the dis- tal humerus: A computational model. J Shoulder El- bow Surg 6444-448,1997 Inglis AE, Pellicci P: Total elbow replacement. J Bone Joint Surg Am 621252-1258,1980 Iohn H, Rosso R, Neff U, et al: Operative treatment of distal humeral fractures in the elderly. J Bone Joint Surg Br 76793-796,1994 Jupiter J, Morrey B: Fractures of the distal humerus in the adult. In Morrey BF (ed): The Elbow and Its Dis- orders, ed 2. Philadelphia, WB Saunders, 1993, p 351 Jupiter JB, Neff U, Holzach P, et aI: Intercondylar frac- tures of the humerus. J Bone Joint Surg Am 67226, 1985 Kasten MD, Skinner HB Total elbow arthroplasty. Clim Orthop 290:177-188,1993
29226-36'1993
23. Knight RA, Zandt L: Arthroplasty of the elbow. J Bone Joint Surg Am 34:610-618,1952
24. Kraay MJ, Figgie MP, Inglis AE, et al: Primary semi- constrained total elbow arthroplasty. J Bone Joint Surg Br 76636-640,1994
25. Lowe LW, Miller AJ, Allum RL, et a1 The development of an unconstrained elbow arthroplasty. J Bone Joint Surg Br 66:243-247,1984
26. McAuliffe JA, Burkhalter WE, Ouellette EA, et al: Compression plate arthrodesis of the elbow. J Bone Joint Surg Br 74300-304,1992
27. Morrey BF: Post-traumatic contracture of the elbow: Operative treatment including distraction arthro- plasty. J Bone Joint Surg Am 72:601-618,1990
28. Morrey BF, Adams RA: Semi-constrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. J Bone Joint Surg Am 74:479-490,1992
29. Morrey BF, Adams R Semi-constrained elbow replace- ment arthroplasty: Rational, technique, and results. In Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, WB Saunders, 1993, pp 648-644
30. Morrey F, A d a m RA: Semi-constrained elbow re- placement for distal humeral nonunion. J Bone Joint Surg Br 77:67-72,1995
31. Morrey BF, Adams RA, Bryan RS: Total replacement for post-traumatic arthritis of the elbow. J Bone Joint Surg Br 73:607-612,1991
32. Morrey BF, Askew LJ, An K-N: Strength function after elbow arthroplasty. Clin Orthop 234:43-50,1988
33. Morrey BE Askew LJ, An K-N, et al: A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 632372-877,1981
34. Morrey BF, Bryan RS, Dobyns JH, et al: Total elbow arthroplasty: A five-year experience at the Mayo
35.
36.
37.
38.
39.
40.
41.
42.
43.
Clinic.-J Bone Joint Suig Am 631050-1063,1981 O'Driscoll SW, An K-N, Korinek S, et al: Kinematics of semi-constrained total elbow arthroplasty. J Bone Joint Surg Br 74:297-299,1992 ONeill OR, Morrey BF, Tanaka S, et al: Compensatory motion in the upper extremity after elbow arthrodesis.
Pritschard R W Anatomic surface elbow arthroplasty: A preliminary report. Clin Orthop 179:223-230,1979 Schneeberger AG, Adams R, Morrey B: Semicon- strained total elbow replacement for the treatment of post-traumatic osteoarthrosis. J Bone Joint Surg Am
Soni RK, Cavendish ME: A review of the Liverpool elbow prosthesis from 1974 to 1982. J Bone Joint Surg Br 66248-253,1984 Souter WA, Nicol AC, Paul J: Anatomical trochlear stinup arthroplasty of the rheumatoid elbow. J Bone Joint Surg Br 67676,1985 Tsuge K, Murakami T, Yasunaga Y, et al: Arthroplasty of the elbow. J Bone Joint Surg Br 69:116-120,1987 Urbaniak JR, Black KE Jr: Cadaveric elbow allografts: A six year experience. Clin Orthop 197131-140,1985 Zuckerman JD, Lubliner J A Arm, elbow and forearm injuries. In Zuckerman JD (ed): Orthopaedic Injuries in the Elderly. Baltimore, Urban & Schwarzenberg,
Clin Orthop 281239-96,1992
79~1211-1222,1997
1990, pp 345-407
Address reprint requests to
Bernard F. Morrey, MD Department of Orthopedic Surgery
Mayo Clinic 200 First Street SW
Rochester, MN 55905