Embed Size (px)
Citation preview

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
1
Improving Patient Care with Fracture Liaison Service (FLS) Program Implementation
Speakers
Anita J. Meehan, MSN, RN-BC, ONC
Clinical Nurse Specialist, Geriatrics/Med-Surg
NICHE program director
Akron General Medical Center
Disclosures: No competing interests to disclose
Susan Randall, MSN, FNP-BC, RN
Senior Director, Science & Education
National Osteoporosis Foundation
Disclosures: No competing interests to disclose
Objectives
1. Briefly describe the epidemiology of
osteoporosis and related fractures
2. Discuss the role of the NICHE GRN in post-
fracture patient care
3. Define 3 key patient benefits of fracture liaison
service (FLS) program
4. Identify resources for patient counseling and
professional education

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
2
What is Osteoporosis?
“A skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture.”“Bone strength is a
composite of bone density and bone quality”
• Genetics
• Excessive thinness
• Inadequate calcium
intake
• Vitamin D deficiency/
insufficiency
• Smoking
• Co-morbid conditions
Risk Factors for Osteoporosis
• Excessive alcohol
intake
• Lack of physical
activity
• Immobility
• High salt intake
• Treatment for other
health conditions
Osteoporosis is responsible for an estimated 2
million fractures per year, including approximately:
•~297,000 hip fractures
•~547,000 vertebral fractures
•~397,000 wrist fractures
•~135,000 pelvic fractures
•~675,000 fractures at other sites
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and Economic Burden of Osteoporosis-Related Fractures in the United States 2005-2025. JBMR. 2007; 22:465-475.
Incidence of Osteoporotic Fractures

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
3
Significance of Osteoporosis
2,050,6951
0
500,000
1,000,000
1,500,000
2,000,000
Osteoporotic
Fractures
795,0002
Stroke
249,2603
Breast Cancer
547,426vertebral
674,919 other sites
396,961 wrist
296,610 hip
An
nu
al
inci
den
ce o
f co
mm
on
dis
ease
s
750,0002
Heart Attack
134,779 pelvic
1Annual fracture incidence age 50+
2Annual estimate new & recurrent MI ages 35+
2Annual estimate new & recurrent stroke all ages
3 2014 new cases in situ & invasive breast cancer all ages
1 Burge, et al. JBMR. 2007. 465-75.
2 American Heart Association. Heart Disease and Stroke
Statistics – 2016 Update.
3 American Cancer Society. Surveillance Research. 2016.
550,000 new
attacks
200,000 recurrent
attacks
610,000
new
strokes
185,000
recurrent
Overwhelming evidence shows that osteoporosis is a massive public health problem nationwide:
• Nearly 65 percent of people in this country who are 65 years old and older have osteoporosis or low bone mass and are at risk for a fracture, according to data from the Centers for Disease Control.
• Currently only 25 percent of patients who suffer a fracture are treated to reduce the risk of future fractures.
• Hip fracture patients’ use of osteoporosis medications following fracture decreased from 40 percent to 21 percent between 2002 and 2011.
A Public Health Emergency
The Care Gap
• Missed opportunities for osteoporosis assessment & treatment
after fracture, even more so in diverse populations and in men
• Fragmented health care system – Fracture patients get “lost”
from hospital to rehab to nursing home to home to primary care
provider
• FLS programs have been proven to work to reduce this gap –
FLS is a system of patient-centered, coordinated care that
follows the patient throughout the care pathway to ensure
adequate assessment and treatment.
Centers for Disease Control and Prevention, Administration on Aging, Agency for Healthcare Research and Quality, and Centers for
Medicare and Medicaid Services. Enhancing Use of Clinical Preventive Services Among Older Adults. Washington, DC: AARP, 2011.
NCQA. Improving Quality and Patient Experience: The State of Health Care Quality 2013.

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
4
Care of Older Adults with
Fragility Fracture: A Case Study
Evidence based recommendations
NICHE and NOF
Anita Meehan, MSN, RN-BC, ONC, FNGNA
A break in the bone that occurs spontaneously
or following a minor trauma such as coughing,
sneezing or falling from a standing height.
The major cause of fragility fracture is a
decrease in bone mineral density.
Low bone density occurs more often in older
adults
Fragility Fracture Definition
Why is this important?
• 54 million US citizens have osteoporosis or osteopenia (low bone density)
• Osteoporosis contributes to 2 million fractures including approx. 300,000 hip fractures annually
• Medical costs for fractures estimated at $17 billion in 2005
• Results in pain, disfigurement, loss of self esteem, impaired mobility and loss of independence
Wright, N, et al. The Recent Prevalence of Osteoporosis and Low Bone Mass in the United States Based on Bone Mineral Density at the Femoral Neck or Lumbar Spine. JBMR, Vol. 29, No. 11, November 2014, pp 2520–2526

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
5
Morbidity and Mortality
• Fragility Hip fractures have a reported mortality rate of up to 20-24% in the first year after a hip fracture
• The increased risk for dying may persist for at least 5 years after the fracture.
• Loss of function and independence among survivors is significant; 40% unable to walk independently 60% requiring assistance a year later.
• 33% are totally dependent or in a nursing home in the year following fracture.
Downloaded from October 5, 2014. http://www.iofbonehealth.org/facts-statistics
The Aging Imperative
Increasing proportion of elders in global society (2013) (The World Bank Data)
– Australia & US 14% – Canada 15%– Japan 25%– Sweden 19%– UK 17%
– All % predicted to increase– In 2015 the world population of >65 outnumbered <5.
Are We Ready for the Silver
Tsunami??

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
6
Global Implications
8.9 MILLION FRACTURES ANNUALLY A FRAGILITY FRACTURE EVERY 3 SECONDS
Adapted from Cooper C et al, Osteoporosis Int, 1992; 2:285-9
Total number of
hip fractures:
1990 = 1.66 million
2050 = 6.26 million
1990 2050
600
3250
1990 2050
668
400
1990 2050
1990 2050
100
629
378
742
The incidence of spinal & hip fractures in women…
Is greater than the incidence of heart attack, stroke and breast cancer.
COMBINED
The ‘Silent Thief’: No Symptoms then a Fracture
• A prior fracture is associated with an 86% increased risk of a future fracture.
• The majority of those who have had at least one osteoporotic fracture were not evaluated for underlying osteoporosis.

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
7
Risk Factors
Non Modifiable
• Age
• Gender: More common in women. More disability/fatalities with men.
• Ethnicity: Asia, Nordic Europe, Caucasian North & South America, Europe
Potentially Modifiable
• Low BMI
• Inadequate calcium & vitamin D, high intake of acid e.g. cola, caffeine.
• Life Style: Smoking, 3 or more alcoholic drinks/day
Secondary Risk Factors
• Medical conditions/ medications that:
• Impact absorption of calcium and or vitamin D: Chrohn’s, hyperparathyroidism, liver or kidney disease, diabetes
• Limit activity: rheumatoid arthritis or severe pulmonary disease
• Impact sex hormones: early menopause
• Increase body acidity (accelerates osteoclasts)
• Medications: Steroids, Certain chemotherapy agents
Medical conditions and Medications are inter-related
Meet Mrs. Mae Wong
• Frail 82 Year old widow
• Hx of hypertension, arthritis, cataracts, HOH, urge incontinence, mild cognitive impairment
• PSH: Cholecystectomy; hysterectomy, cataract, fx wrist
• Lives in a 1 bedroom apt, 78 year old sister lives in same apt building
• Son and his family live nearby
• Independent in ADL’s family helps with IADLs
• Dentures, cane/glasses/refuses hearing aid
• Difficulty sleeping d/t arthritic pain in her knees

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
8
Case Study
• Awoke during night needing to toilet
• Fell on way to bathroom
• Unable to summon help
• Found by sister next morning
• EMS called
• She arrives at your emergency room
Case Study ~ Cont
• Assessed
• Labs drawn
• IV started
• Pain med admin
• Awaiting arrival of ortho resident
• X-ray
• Fx Prox L Femur
• Admitted for surgical fixation
Time Spent in ED
Varies according to:
• Time of arrival
• Availability of bed
• Availability of staff

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
9
Pre Surgical Care
• OR may be delayed due to an emergency ‘trauma’/full surgery schedule
• Bucks Traction applied to affected leg
• Indwelling urinary catheter
• IV opiates
• NPO after midnight
Post Op Course

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
10
Mrs. Wong’ Care Revisited
• Wrist facture at age 66 was a
‘signal’ fracture
• Dexa Scan ordered
• Osteoporosis/osteopenia Rx
by PCP or FLS
• Possible prevention of future
fracture
Mrs. Wong’s Care Revisited
• Fall occurs
• Transported by EMS
• Care initiated during transport following protocol
• Pain relief provided
• Oxygen & fluids
• Labs Drawn
• EKG
• Information transmitted to ED
Mrs. Wong Revisited
EMS arrives at ER as a priority
Geriatric ER & CNS
PMH obtained from EMR
Transfer immediately to xray
Fracture confirmed
Regional pain block
No skin traction, pillows to off load
heels
Transfer to ortho unit within 2 hours
of arrival

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
11
Potential Complications Identified
• Pain – Acute on Chronic
• Delirium – D/T Cognitive impairment
• Pressure Ulcers
• Rhabdomyolitis?
• DVT
• Infection – Surgical site, PNA, UTI
• Sleep Deprivation
• Constipation
• Functional decline
• Falls
• Depression
Evidence Based Care Strategies
Patient/family is active participant in care
Geriatric Hip Fracture pre and post surgical protocol
Sensory aids in place
Multimodal pain relief initiated
• Regional block: Pre op pain relief
• Scheduled Tylenol for chronic arthritic pain
Screening for cognitive changes
Pressure relieving surfaces, In EMS, ER, OR and Unit
HOB elevated 30%
Surgery within 24-48 hours
Liberalized NPO restrictions
http://www.aaos.org/Research/guidelines/HipFxSummaryofRecommendations.pdf
Which answer best describes fasting pre-op restrictions at your hospital?
A. NPO after midnight
B. Allowed clear liquids 6 hours prior to OR
C. Order for clear high carb drink 2-3 hours prior to OR

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
12
Pre-op Carbohydrate Loading
• 8 oz clear carbohydrate drink 3
hours prior to surgery
• Reduces loss of muscle strength,
post-op N&V, post-op insulin
resistance, LOS, improves patient
satisfaction
Evidence
American College of Surgeons and many Anesthesia Societies have
recommendations to liberalize NPO prior to surgery; allowing clear liquids up
to 2 hours prior to surgery
The European Society of Parenteral and Enteral Nutrition, ESPEN
recommends a carbohydrate rich drink 2 -3 hours before anesthesia
American College of Surgeons Guidelines 2015
Guidelines on Parenteral Nutrition: surgery. Braga M, Ljungqvist O, Soeters P, Fearon K, Weimann
A, Bozzetti F, ESPEN Clin Nutr. 2009 Aug; 28(4):378-86.
Post-op Evidence Based Care Strategies
• Pressure ulcer prevention strategies throughout continuum of
care – ED, OR PACU, Unit
• Early ambulation within 24 hours of surgery ~ starting with
sitting at side of bed DOS
• Nursing mobilizes in conjunction with PT/OT
• High protein oral nutritional supplements in addition to
normal diet
• Encourage/ offer fluids
• Constipation prevention protocol
• Fracture Liaison Nurse Consult prior to discharge

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
13
NICHE “Need to Know”
Post-op Care Information Hip fractures and Repair
Post-op Course
• Family active in care
• Active participant in PT/OT & self care
• Discharge PO day 4
• Rehab for 2 weeks
• Home with family assisting and home
community support services in place
• Secondary fracture prevention
General Recommendations
• Regular weight bearing exercises
• Muscle strengthening exercises
• Avoid Smoking
• Avoid excessive alcohol consumption
• Ensure a diet that includes adequate amounts of
Calcium and Vitamin D for optimal bone health

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
14
National Osteoporosis Foundation Recommendations for Vitamin D
Women and Men
Under age 50 400-800 IU per day**
Age 50 and older 800-1,000 IU per day**
Sources of Vitamin D
Sunlight
Food
Supplements
**Some people may need a Vitamin D supplement depending on diet and where
they live; check with your care provider for recommendations
National Osteoporosis Foundation Recommendations for Calcium
Women Men
Age 50 & Younger 1000 mg* daily Age 70 & younger 1,000 mg/day
Age 51 & Older 1200 mg* daily Age 71 & older 1,200 mg/day
*this amount Includes calcium obtained from food and supplements
Optimal source is dietary, supplement if diet does not meet requirements
Non-Pharmacologic Management
Non-pharmacological management of fragility fractures aims at
preventing a future fracture fracture. This includes 2 main
strategies:
• Fall prevention
• Hip protectors
Fall prevention is the most effective of the two interventions

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
15
Pharmacologic Management
• Non adherence major challenge
• Related to:
– Inadequate patient education
– Lack of understanding of relationship between osteoporosis and
fractures / benefit vs. risk
– Following specific requirement for oral administration
– Adverse effects
– Cost
• No agent or treatment should be taken indefinitely
• Monitoring with Bone Mineral Density (DEXA) testing essential
• Therapy needs to be individualized based on risk/benefits
Bone Mineral Density (BMD)
BMD is one measure of bone strength
Peak BMD occurs at about age 30.
Low BMD occurs when the rate of osteoclasts breaking
down bone exceeds the rate of osteoblast regeneration
of new bone.
Bone Mineral Density Testing
• Women age 65 and older
• Men age 70 and older
• Post menopausal age 50-59 based on risks
• Post menopausal starting at age 50 w/fx history
• BMD 1-2 years after initiating RX
• Q 2 years thereafter

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
16
Standard Measure for BMD:Dual Energy X-ray Absorptiometry (DEXA):
Measures bone mineralization. Detects the amount of X-ray that
passes thru the bone. The lower the bone density, the higher the
amount of ray will pass thru. Measured at the spine, hip and
sometimes wrist. DEXA results reported as a T-Score.
Interpreting DEXA T-Score
T-score compares how far the person’s bone density score
varies from the average population, same gender score at
peak bone health. Low bone density T-score has a minus
sign.
• T-score of -1 to -2.5: Osteopenia
• T-score of -2.5 or lower: Osteoporosis
T-Score
T=0-1-2-2.5
Osteoporosis
Normal distribution of
BMD scoresOsteo-
penia

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
17
When is Pharmacologic Treatment Recommended?
• NOF National Osteoporosis Foundation guidelines recommend
pharmacological treatment based on the following criteria:
• Hip or vertebral fracture
• T-scores of <= -2.5 at femoral neck, total hip or lumbar spine
• Post menopausal women and men age >50 with T-score between -
1.0 and -2.5
• 10-year fracture probability of >3.0% hip fx probability or >20.0%
major osteoporosis-related fracture probability by FRAX
FDA Approved Pharmacologic Management Options
• Anti-resorptive agents
• Selective Estrogen Receptor Modulators (SERMS)
– Raloxifene (Evista)
• Bisphosphonates
– Alendronate, Risedronate, ibandronate (Fosamax, Actonel, Boniva)
• Calcitonin
– Calcitonin (Miacalcin; Fortical)
• Receptor Activator of Nuclear factor Kappa-B ligand (RANKL)
– Denosumab (Prolia)
– Bone Stimulating Agent - Anabolic
• Teriparatide (Forteo)
Individualize Treatment Plan
When developing a treatment plan it is imperative that the
patient be actively involved in the process
• Consider patients’ expectations, concerns and beliefs
• Set realistic and achievable goals
• Communicate information with regard to medical literacy
• For optimal adherence, be willing to negotiate an
acceptable treatment plan
• Active engagement with care provider

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
18
Secondary Fracture Prevention
• Optimize function
• Prevent future fracture
• Fracture Liaison Nurse Role
• Management of Bone Health
• DEXA Scan
• Pharmacological intervention
• Follow up and referral as needed
• Fall Prevention and Balance Enhancement
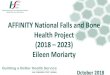
National Committee on Quality Assurance, “The State of Health Care Quality 2014”. 2014.
88%
87%
84%
74%
70%
64%
63%
62%
59%
43%
34%
29%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%100%
RA ANTI-RHEUMATOID THERAPY
CHOLESTEROL MANAGEMENT (CVD …
BETA BLOCKERS (POST-HEART ATTACK)
BREAST CANCER SCREENING
PNEUMOCOCCAL VACCINATIONS (2012)
CONTROLLING HIGH BLOOD PRESSURE
COLORECTAL CANCER SCREENING
FALL RISK INTERVENTION
COMPREHENSIVE DIABETES CARE
COPD SPIROMETRY TESTING
FALL RISK DISCUSSION
TESTING/TREATMENT AFTER A FRACTURE
Osteoporosis Care Lags FAR BEHIND
Other Major Diseases/Conditions
Some Improvement in NCQA
HEDIS Post-Fracture Measure*
* National Committee on Quality Assurance, “The State of Health Care Quality 2014”. 2014: 90-91.
2007-2010: little
change
• HMO +0.3%
• PPO +0.7%
2010-2013:
statistically
significant change
• HMO: +8.5%
• PPO: +3.9%

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
19
The Nurses’ Role in Osteoporosis
Prevention, Diagnosis and Treatment
• Increase patient awareness
• Identify patients at-risk for
osteoporosis and related fractures
• Counsel individuals on risk reduction
strategies with emphasis on promotion of healthy lifestyle choices. These should begin in the childhood years
• Refer to primary healthcare provider to assess need for BMD
• Promote patient adherence with osteoporosis management through support and education
Patient Teaching Points
• Proper way to take prescription medication
• Side effects to watch for (major vs. minor) and what to do about
them
• Counsel calcium & vitamin D (not a substitute for meds)
• Monitor adherence with meds and lifestyle issues
• Refer to tobacco cessation class if indicated
• Counsel re: alcohol moderation
• Counsel re: exercise, safety considerations & fall prevention
measures / Suggest PT referral as needed
• Instruct on the plan for follow up and periodic assessments / bone
density testing
• Support services
Fracture Liaison Service (FLS)
Model of Care
• A coordinated preventive care model
Supervised by bone health specialists and collaborates with
the patient’s primary care physician
Post-fracture care coordinated by an FLS coordinator (RN,
NP, PA or other healthcare professional)
Ensures fracture patients receive appropriate diagnosis,
treatment and support
• Patients tracked via a population registry
• Processes and timelines for patient assessment and follow-up
• Proven success over the last 15 years
• FLS programs have greatly reduced the number of recurrent
fractures by identifying and appropriately treating post-fracture
patients

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
20
Key Facts About Secondary
Fractures
• A prior fracture almost doubles a patient’s future
fracture risk
• Half of patients presenting with hip fractures have
suffered a prior fracture
• Despite the risk of future fractures, the majority of
fragility fracture patients are neither assessed, nor
treated to reduce fracture risk.
• To achieve a significant reduction in future fracture
rates and resulting health care costs, healthcare
systems must target those patients who have already
suffered a fracture, as they are the ones at highest risk
for future fractures.
Hip
fracture
patients
Objective 1: Improve outcomes
and efficiency of care after hip
fractures by delivering
professional standards per
established performance and
quality measures
Non-hip fragility
fracture patients
Objective 2: Respond to the first
fracture to prevent the second
through establishment of Fracture
Liaison Services bridging
hospital and primary care services
for fracture patients
Individuals at high risk of
first fragility fracture or
other injurious falls
Objective 3: Health insurers or
primary care providers to stratify
risk for their patients using
fracture risk assessment tools
combined with bone density
testing
Older peopleObjective 4: Consistent delivery
of public health messages on
preserving physical activity,
healthy lifestyles and reducing
environmental hazards
Maximize cost-
effectiveness
by stepwise
delivery
Why Secondary Fracture Prevention?
(Adapted from Falls and fractures: Effective interventions in health and social care)
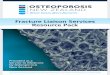
United States FLS Outcomes
1. Kaiser Permanente
• Reduced the hip fracture rate expected by over 40% (since 1998)
• If implemented nationally, a similar effort could reduce the number of hip fractures by over 100,000 (and save over $5 billion/year)
2. Geisinger Health System
• Achieved $7.8 million
in cost savings from 1996-2000
3. American Orthopaedic AssociationOwn the Bone® Program
• Achieved statistically significant changes in health professional behavior/referral (calcium and vitamin D, exercise, fall prevention, etc.)
• Over 190 sites and 20,000+ patients involved from 46 states and the District of Columbia (since mid-2009)
$0
$10,000,000
$20,000,000
$30,000,000
$40,000,000
$50,000,000
$60,000,000
$70,000,000
1996 1997 1998 1999 2000
Cu
mu
lati
ve
co
sts
(m
illio
ns
$)
No interventionActual results
Savings
(millions)
$ 7.8
$ 7.2
$ 3.1
-$ 2.4
Age
group
65-75
75+
All
55-65

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
21
Annual Unadjusted Probability of
Osteoporosis Medication Use Within
12 Months After Discharge
Solomon, et al., “Osteoporosis Medication Use after Hip Fracture in U.S. Patients between 2001 and 2011.” JBMR (September 2014);29(9):
1929-37.
FLS Program Goal
Objective: A post-fracture prevention Fracture Liaison
Service (FLS) program aims to ensure that post-
fracture patients receive appropriate diagnosis,
treatment and follow-up
Expected Outcomes: Improved treatment adherence,
reduction in secondary fractures and cost savings
FLS Care Coordination in Action
FLSCoordinator/
PhysicianChampion
PrimaryCare
MedicalSpecialists
Nursing,physicaltherapy,
nutritionist
Hospital/
Emergency Department
Orthopaedics

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
22
FLS Effectiveness Based on “5 I’s”Identify/Inform/Initiate Treatment/Investigate/Iterate
1. Ganda K et al. Osteoporosis International 2013 Feb; 24(2): 393-406.
2. Osteoporosis Canada. “Make the FIRST break the LAST with Fracture Liaison Services”.
Resources
Fracture Prevention CENTRAL, an Online FLS Resource: this publicly-accessible website
was launched in March 2013 (available at www.FracturePreventionCENTRAL.org) to help
HCPs and administrators implement a coordinator-based, post-fracture FLS model of care to
reduce secondary fractures and the associated costs while increasing patient outcomes:
• NBHA compiled materials from a number of successful domestic and international
post-fracture care programs
• highlights the work of leading FLS programs including the American Orthopaedic
Association Own the Bone program, Kaiser Permanente and Geisinger Health
System
Fracture Prevention CENTRAL enables sites to implement a FLS in support of NBHA’s
20/20 vision to reduce fractures 20% by the year 2020
www.FracturePreventionCENTRAL.org
More than 3,300
individual users
have signed up
to access
these tools
since March
2013

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
23
The Impact of Osteoporosis and Bone Breaks
in the United States
“Cast Mountain” represents
just 1 DAY of fractures caused
by osteoporosis in the U.S.
Online Professional Education
The complete ISO course curriculum,
including the FLS Certificate of Completion
Pathway is available on-
demand
Professional Education

nicheprogram.org • 2016 Annual NICHE Conference • Care Across the Continuum
24
For More Information
NOF: www.NOF.org (Patient education)
www.NOF-ISO.org (FLS Certificate Program)
(202) 223-2223
www.cme.nof.org (Professional Learning Ctr)
NBHA: www.nbha.org/fpc (FLS resources)
http://www.nbha.org/nof-consult-request(FLS 1-on-1 consults)
Ostonics: www.ostonics.com (QCDR registry)
(202) 721-6364
IOF: www.capturethefracture.org (Program recognition)
Questions?
About NOF
Founded in 1984, the National Osteoporosis
Foundation (NOF) is the leading health
organization dedicated to the prevention of
osteoporosis and broken bones; the promotion
of strong bones for life; and the reduction of
human suffering through programs of public and
clinician awareness, education, advocacy, and
research.