Embed Size (px)
Citation preview

FRACTIONATED STEREOTACTIC RADIATIONTHERAPY FOR LOCALLY RECURRENT NASOPHARYNXCANCER: REPORT OF THREE CASES
Yong Chan Ahn, MD 1, Dae Yong Kim, MD 1, Seung Jae Huh, MD 1,Chung-Hwan Baek, MD 2, Keunchil Park, MD 3
1 Department of Radiation Oncology, Samsung Medical Center, College of Medicine, Sungkyunkwan University,50 Ilwon-dong, Kangnam-Ku, Seoul, 135-230, Korea. E-mail: [email protected] Department of Otorhinolaryngology-Head & Neck Surgery, Samsung Medical Center, College of Medicine,Sungkyunkwan University, Seoul, Korea3 Department of Hematology/Oncology, Samsung Medical Center, College of Medicine, SungkyunkwanUniversity, Seoul, Korea
Abstract: Background. This article reports on experiencewith fractionated stereotactic radiation therapy (FSRT) for locallyrecurrent nasopharynx cancer.
Methods: Three patients with locally recurrent nasopharynxcancer were given FSRT as reirradiation between September1995 and August 1996. Application of FSRT was the third radia-tion therapy in two patients. Authors used the individually maderelocatable Gill-Thomas-Cosman (GTC) stereotactic frame, andthe radiation dose planning was performed using XKnife-3T. Thetotal doses to the recurrent tumor were 45 Gy/18 fractions in twopatients, who were given concurrent chemotherapy as a radio-sensitizer, and 50 Gy/20 fractions in the other patient. In all threepatients the dose per fraction was 2.5 Gy, and the fraction sched-ule was to give five daily treatments per week.
Results: Authors observed satisfactory symptomatic im-provement and remarkable objective tumor size decreasethrough the magnetic resonance (MR) images taken one monthpost-FSRT in all three patients. No neurological side effect wasobserved. All three patients died with regional and distant seed-
ing outside the FSRT field at seven, nine, and nine months, re-spectively.
Conclusion: FSRT as reirradiation for locally recurrent naso-pharynx cancer seemed to be effective and safe. © 1999 JohnWiley & Sons, Inc. Head Neck 21: 338–345, 1999.
Keywords: fractionation; stereotactic; radiation therapy; recur-rent; nasopharynx cancer
Radiation therapy has played the greatest role inthe management of nonmetastatic nasopharyn-geal cancer. It has been generally accepted thatthere is a positive correlation between tumor bulkand the radiation dose needed for adequate con-trol of the tumor. On the average, about one-third(34%) of nonmetastatic nasopharynx cancer pa-tients experience local tumor recurrences or per-sistence, with a wide range of variations in theincidence (18∼54%) after primary radiationtherapy.1,2 Patients with locally recurrent tumorsgenerally have been offered reirradiation usingvarious techniques, which usually have been as-sociated with the substantial risk of late neuro-logical side effects. The authors employed frac-tionated stereotactic radiation therapy (FSRT) for
Correspondence to: Yong Chan AhnThis work was presented at the 3rd International Stereotactic Radiosur-gery Congress in Madrid, Spain, June 1997.Contract grant sponsor: Korean Atomic Energy Research.
CCC 1043-3074/99/040338-08© 1999 John Wiley & Sons, Inc.
338 FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999

three locally recurrent and symptomatic naso-pharynx cancer patients who were otherwisehopeless and observed remarkable success in lo-cal tumor reduction.
MATERIALS AND METHODS
Three locally recurrent nasopharynx cancer pa-tients were treated with FSRT between Septem-ber 1995 and August 1996 at the Department ofRadiation Oncology at Samsung Medical Center.All three patients were previously given defini-tive high dose radiation therapy after neo-adjuvant systemic chemotherapy; two were man-aged at other hospitals. After the diagnosis oflocal recurrence, two patients with symptomaticskull base invasions were given palliative reirra-diation using external beam with or without in-tracavitary high dose rate brachytherapy to thelocally recurrent tumors before referral to our de-partment. In the third patient, local recurrencewas incidentally diagnosed during the course ofpalliative chemotherapy for the persistent necknode metastases. For the stereotactic three-dimensional coordinate definition, authors usedthe individually made relocatable Gill-Thomas-Cosman (GTC) stereotactic frame. The FSRT doseplanning was done using the XKnife-3t system.The first step of FSRT was to make an individu-alized immobilization assembly device includinga dental bite, an occipital support, and a Y-shapedbelt, all of which were tightly attached to the GTCframe (Figure 1). The contrast enhancing CT scanwas obtained with the GTC frame on, and wastransferred to the XKnife-3t system for the pa-tient’s contour and anatomical information. Themaximum number of CT slices for the image reg-istration was 64. We obtained CT images of 3-mmthickness along the level of the recurrent tumorand 5-mm thickness outside the region of interestto keep the total number of CT slices within thislimit. The radiation therapy dose planning underthe concept of multiple noncoplanar arc rotationswas undertaken after the three-dimensional re-construction of the CT anatomical data. The sizeof the FSRT cone, three-dimensional stereotacticcoordinates of the isocenter, and treatment beamparameters, including couch angles and arcranges, were determined through the dose plan-ning. Before each treatment, the verification ofmechanical accuracy of the linear accelerator andthe laser alignment were performed using the me-chanical isocenter and film testing. The stereotac-tic coordinates of the isocenter were set on therectilinear phantom pointer (RLPP) and the laser
target localization frame (LTLF) by two differenttechnologists, and the coincidence of the isocentersetups were double checked. With the patient ly-ing on the treatment couch with the GTC frameon, the isocenter accuracy was verified using theLTLF on each arc position (Figure 2).
RESULTS
The first patient was a 47-year-old male who vis-ited another hospital with the subjective symp-toms of right neck swelling, right-side hearing dif-ficulty, and nasal obstruction 24 months beforethe current treatment. After the biopsy and stag-ing work-up, the final diagnosis was T4N2bM0undifferentiated carcinoma of the nasopharynx.He was then managed with three cycles of neo-adjuvant chemotherapy (5-FU + cis-platinum),definitive external beam radiation therapy (70.2Gy/eight weeks, 1.8 Gy/fraction, 5 fractions/
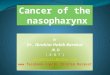
FIGURE 1. A and B. Gill-Thomas-Cosman (GTC) stereotacticframe consists of dental bite, occipital support, and Y-shaped beltfor individualized immobilization.
FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999 339

week), and three cycles of adjuvant chemotherapy(5-FU + cis-platinum), which resulted in completeresponse. Seven months previous to the currentreferral to our department, he received right radi-cal neck dissection because of right upper necknode recurrence. Three months ago this patientdeveloped severe headache and multiple cranialnerve palsies including diplopia, swallowing dif-ficulty, dysarthria, and right facial numbness.The MR scan showed extensive local recurrenceinvolving the right side nasopharynx, which ex-tended into the right cavernous sinus (Figure 3A).A short-course palliative external beam reirradia-tion therapy was undertaken at the other hospi-tal, up to 30.8 Gy over two weeks (1.4 Gy/fraction,2 fractions/day), which resulted in minimal symp-tom relief. When this patient visited our depart-ment, he complained of severe headache that waspoorly controlled by strong narcotic analgesicsand multiple cranial neuropathies (III–VI, IX–XI,and XII). FSRT and intravenous cis-platinumchemotherapy (60 mg/m2) concurrently at thefirst and the last dates of reirradiation were ap-plied as the last resort for this otherwise helplesspatient. We used four arcs with 5.9 cm diametercone to encompass the recurrent mass to givedaily 2.5 Gy at the tumor margin, which is 85% ofthe isocenter dose (Figure 3-B). The total FSRTdose was 45 Gy in 18 treatments over three and ahalf weeks. At weekly interviews the patient firstreported remarkable improvement of headache atthe second week of the FSRT treatment. Towardthe end of FSRT course, he became totally free ofpain without taking any medication; however, therecovery for diplopia was not complete. The fol-low-up MR images taken at one month post-FSRT
showed remarkable reduction of the recurrentmass (Figure 3-C), and the patient was able tolive a symptom-free, active, and useful life forabout four additional months. Unfortunately, thispatient developed extensive recurrences involv-ing the meninges and the paravertebral muscles,and finally succumbed to death at seven monthspost-FSRT.
The second patient was a 47-year-old malewith the initial symptoms of nasal obstructionand bleeding 28 months prior to the current treat-ment. After thorough work-up, he was diagnosedas having T2N0M0 squamous cell carcinoma ofthe nasopharynx and was treated with threecycles of neo-adjuvant chemotherapy (5-FU + cis-platinum) and definitive external beam radiationtherapy (70.2 Gy/eight weeks, 1.8 Gy/fraction, 5fractions/week) at another hospital. The responseafter radiation therapy was scored as completeresponse and this patient refused further adju-vant chemotherapy in fear of toxicity. About 13months prior to the current treatment, he devel-oped local recurrence with nasal bleeding and wasmanaged with laser debulking and reirradiation.The reirradiation technique at the other hospitalincluded low-dose external beam radiationtherapy (20 Gy/2 weeks, 2 Gy/fraction, 5 fractions/week) plus high dose rate intracavitary brachy-therapy (25 Gy/2.5 weeks, 5 Gy/fraction, 2 frac-tions/week). This patient was referred to ourdepartment with severe headache, tinnitus, andnasal bleeding that lasted for two months. TheMR images showed a locally recurrent tumormass involving the posterior and both lateralwalls of the nasopharynx and the clivus (Figure4-A). The patient refused any chemotherapy, and
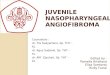
FIGURE 2. (A) Stereotactic coordinates of the isocenter were set on the rectilinear phantom pointer (RLPP) and laser target localizationframe (LTLF) by two technicians for the isocenter setup coincidence. (B) The isocenter accuracy verification was done using LTLF foreach arc with the patient in the treatment position.
340 FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999

it was decided to apply FSRT alone as palliativereirradiation. The total dose by FSRT was 50 Gyto the tumor margin (85% of the isocenter dose)over four weeks (2.5 Gy/ fraction, 5 fractions/week), which was delivered using four arcs with a4.2-cm cone. The follow-up MR scan at one monthpost-FSRT showed marked regression of the re-current tumor mass with partial relief of subjec-tive symptoms (Figure 4-B). However, this pa-tient again complained of recurrent headache at
four months post-FSRT, which was associatedwith the tumor regrowth at the treated skull baseon follow-up MR. Coupled with multiple lung me-tastases, this caused the patient’s death at ninemonths post-FSRT.
The third patient was a 59-year-old male whowas diagnosed as having T2N2cM0 squamous cellcarcinoma of the nasopharynx after the work-upfor asymptomatic neck swelling on both sides 15months prior to the current treatment at our in-
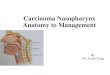
FIGURE 3. (A) Pre-FSRT MR scan of a 47-year-old male withsevere headache and multiple cranial nerve palsies showed ex-tensive local recurrence involving the right side nasopharynx andextending into the right cavernous sinus. (B) Isodose distributionby FSRT shows a good coverage of the recurrent tumor usingfour arcs of 5.9-cm diameter cone. (C) MR scan at one monthpost-FSRT showed remarkable reduction of the recurrent mass.
FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999 341

stitute. He was given three cycles of neo-adjuvantchemotherapy (5-FU + cis-platinum) and radia-tion therapy, which consisted of external beamtherapy (61.2 Gy/6.5 weeks, 1.8 Gy/fraction, 5fractions/week) and high dose rate intracavitarybrachytherapy boost (three weekly fractions of 4Gy at 1 cm distance from the center of the cath-eters). Shortly following three cycles of adjuvantchemotherapy (5-FU + cis-platinum), left modi-fied radical neck dissection had to be performedbecause of the persistent neck node disease on theleft side. As complete removal of all gross tumorswas not possible, this patient was offered severalcourses of palliative chemotherapy of differentregimens, followed by partial tumor removal plusinterstitial brachytherapy. On routine outpatientfollow-up, recurrent tumor at the right side of thenasopharynx was incidentally identified, whichwas confirmed by biopsy, MR (Figure 5-A), andPET scans (Figure 5-B). Since this patient was inrelatively good performance status and generalcondition, it was decided to apply FSRT plus con-current chemotherapy. The total dose of FSRT tothe tumor margin (90% of the isocenter dose) was50 Gy over four weeks (2.5 Gy/fraction, 5 frac-tions/week) using four arcs with a 5.0-cm cone.Concurrent chemotherapy regimen included5-FU (800 mg/m2, continuous infusion from Day 1to Day 5) and hydroxyurea (1.0 g p.o. every 12
hours from Day 1 to Day 5). Two cycles of theabove regimen were given during the FSRTcourse: the first chemotherapy cycle started onthe day of the first FSRT; the second cycle wasrepeated on the third week of FSRT. On physicalexamination, the tumor regressed completely atthe third week of FSRT, and this was confirmedwith the follow-up MR scan at one month (Figure5-C) and the PET scan at two months (Figure5-D). This patient died at nine months post-FSRTwith widespread metastases to the lung and thebones after receiving a few more cycles of pallia-tive systemic chemotherapy for persistent necknode disease.
DISCUSSION
It has been generally accepted that there is a posi-tive dose-response relationship in the local con-trol of nasopharynx cancer with respect to the tu-mor size. The usually recommended radiationdoses to the primary tumor are 60–65 Gy for T1-2lesions and 65–70 Gy for T3-4 lesions, thoughthere may be some variations depending on thehistologic subtypes. Local recurrences, on the av-erage, have been reported in one-third of the totalpatients with the range of 18% to 54%.1,2 Lee etal,1 in their retrospective analyses of more than5000 patients, reported the incidence of the localdisease problems to be 31% (local residual disease
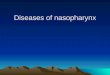
FIGURE 4. (A) Pre-FSRT MR scan of 47-year-old male with severe headache, tinnitus, and nasal bleeding showed locally recurrent tumormass involving the posterior and both lateral walls of the nasopharynx and the clivus. (B) MR at one month post-FSRT showed markedregression of the recurrent tumor mass.
342 FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999

FIGURE 5. Pre-FSRT (A) MR scan and (B) PET scan of 59-year-old male showed recurrent tumor at the right side of the nasopharynx.Post-FSRT (C) MR scan at one month and (D) PET scan at two months showed complete disappearance of the tumor.
FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999 343

13% + local recurrence 18%). Reirradiation for lo-cal recurrences has been accepted as the most op-timal treatment modality, which is without theimmediate life-threatening morbidity or mortal-ity of surgery, and has frequently promisingtreatment results. Summarizing the reports onreirradiation, the local control rates wereachieved in 30% to 60%, and the five-year sur-vival rates were approximately 20%.3,4 Variousreirradiation techniques were tried in an effort tolimit the radiation doses to the surrounding criti-cal normal structures.
Lee et al3 reported the largest series of reirra-diation for 891 recurrent nasopharynx cancer pa-tients. The main treatment modality was 23∼25MeV electron beams, and, for small recurrences,intracavitary or implant brachytherapy tech-niques were also employed. In more than one-halfof those with small local tumors, local control waspossible after the delivery of adequate radiationdoses. The five- and 10-year survivals were 14%and 9%, respectively, and the five-year probabil-ity without neurological complication among sur-vivors was 80%. There have been sporadic reportsof the results of surgical treatment after local re-currences, in which complete removal and long-term survival were possible in well-selected pa-tients with small recurrences. However, thismodality usually had to pay for the price of sub-stantial surgical complication and functional dis-ability.5 It is the authors’ opinion that surgery forlocal recurrences should be carefully limited tothose with small superficial recurrences, and thatsurgery should be performed by highly experi-enced surgeons, where reirradiation is contrain-dicated.
Choy et al6 reported their experiences of per-manent implant brachytherapy using radioactivegold in 43 residual or recurrent tumors. Rela-tively satisfactory results of local tumor controlwere achieved in 60% to 80%, and procedure-related morbidity such as headache, fistula of thesoft palate, and necrosis of the nasopharynx mu-cosa were also reported. Leung7 et al reported ex-periences of high dose rate intracavitary brachy-therapy for 61 patients with local residual andrecurrent diseases. The local control and survivalrates at three years of each group were 82% ver-sus 45% and 82% versus 62%, respectively. Thesereirradiation techniques of brachytherapy may belimited only to those with superficial small recur-rences, where gamma rays from the radioactivesources can be delivered effectively. Brachy-therapy may not be applied to the more extensive
recurrences involving the surrounding deep tis-sues and the skull base, which comprises abouttwo-thirds of the total recurrences.
Feehan et al8 applied heavy charged particleirradiation stereotactically and reported the localcontrol rate of 45%, and three- and five-year sur-vival of 59% and 31%, respectively, in 11 locallyrecurrent cases. These results should be inter-preted cautiously as there were seven occurrencesof complications including brain necrosis. Heavycharged particle beam radiation therapy mayhave some advantages over other more conven-tional external beam radiation therapy with re-spects to radiobiology as well as radiation physics.However, this may not be true in this clinical situ-ation, considering the somewhat guarded treat-ment results. In addition, the very limited num-ber of particle radiotherapy facilities throughoutthe world is another disadvantage of this modal-ity.
In 1991 Kondziolka and Lunsford9 reportedgamma-knife radiosurgery for a locally recurrentnasopharynx cancer patient with resultant sig-nificant tumor reduction. This report might havepractically expanded the clinical indications of ra-diosurgery from within the cranium to the skullbase and outside the cranium, as the tumor tar-geting could be done stereotactically. Buatti etal10 reported their linear accelerator-based ste-reotactic radiosurgery (SRS) experiences for threelocally recurrent nasopharynx cancer patients in1995. One of their patients experienced bilateralcomplete visual loss in six months postradiosur-gery without any clear explanation (possibly fromradiation change or local relapse), and anotherdied of local relapse with cranial nerve dysfunc-tion. As the fractional dose in radiosurgery wasvery high, there certainly existed substantialrisks of serious neurological complications. Theauthors believe that SRS for nasopharynx cancershould be considered with the greatest caution,even if this technique is very accurate in targetlocalization. The nasopharynx cancer recurrencesare rather infiltrative and are surrounded bymany radiation-sensitive critical normal struc-tures such as cranial nerves III-VI, the optic chi-asm, the pituitary fossa, and the temporal lobes.The tumor target is less definable than in intra-cranial candidate lesions of SRS like arteriove-nous malformations or metastases.
The fact that the risk of late neurological dam-age proportionally increases with the incrementof the fractional dose is evident on radiobiologicalas well as on clinical grounds. The idea of com-
344 FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999

bining stereotactic methods and the concept offractionation was inspired by the observation ofneurological complications in the single high doseSRS practices. FSRT is a modification of SRS en-abling conventional fractionation without losingthe advantage of the mechanical accuracy by ste-reotaxy. FSRT may have advantages over SRS ina few respects. First, more radiation damage tothe tumor tissue and less radiation damage to thenormal neural tissue can be expected with FSRT,as this has been the radiobiological principle inusual fractionated radiation therapy. Second, thetumors located close to the critical structures maybe more safely treated by FSRT, as the fractionaldose is the most important factor in late neuro-logical damage. Third, relatively larger targetsmay be treated safely by FSRT than SRS, as thevolume effect is much more problematic in singlehigh dose SRS than FSRT. Indications of FSRTmay also be extended to the benign and malig-nant lesions located not only within the craniumbut also in the skull base and the extracranialstructures including the nasopharynx, the nasalcavity, the orbit, and the paranasal sinuses. How-ever, FSRT may not be recommended ideally forthose lesions that benefit more from the singlehigh dose radiation (ie, arteriovenous malforma-tions, functional SRS).
The authors used the noninvasive, relocatablestereotactic GTC frame and the fractional dose of2.5 Gy to treat the first three locally recurrentnasopharynx cancer patients, who were previ-ously heavily irradiated by the conventional ra-diation techniques. The responses were evaluatedwith fiberoptic nasopharyngoscopic examination(3), MR scan (3), and PET scan (1). Follow-up bi-opsy was not recommended in fear of mucosal ne-crosis, as two of these patients were given radia-tion therapy twice before FSRT. Authors observedradiation mucositis in the posterior soft palateand partial alopecia of mild to moderate degree,which were acute side effects attributable toFSRT. No occurrences of radiation-related neuro-logical complications were observed, which mightbe by the virtue of limited radiation dose to thecritical structures with careful dose planning and/
or short follow-up periods. While local tumor re-sponse was quite satisfactory, all three patientssuccumbed to distant disease progression outsidethe FSRT ranges.
In brief, the authors experienced excellent lo-cal tumor responses after FSRT in all three pa-tients with locally recurrent nasopharynx cancer.Based on the authors’ current experiences, FSRTmay be ideally indicated to treat local recurrencesnot only for symptomatic palliation, if associatedwith metastasis, but also for salvage and cure, iffree of metastasis. The development of a more ef-fective systemic treatment regimen with radio-sensitizing effect and with less side effects wouldbe necessary to improve the treatment outcome.
REFERENCES
1. Lee AWM, Poon YF, Foo W, et al. Retrospective analysisof 5037 patients with nasopharyngeal carcinoma treatedduring 1976–1985: Overall survival and patterns of fail-ure. Int J Radiat Oncol Biol Phys 1992;23:261–270.
2. Yang TS, Ng KT, Wang HM, Wang CH, Liaw CC, Lai GM.Prognostic factors of locoregionally recurrent nasopharyn-geal carcinoma—a retrospective review of 182 cases. Am JClin Oncol 1996;19:337–343.
3. Lee AWM, Law SCK, Foo W, et al. Retrospective analysisof patients with nasopharyngeal carcinoma treated dur-ing 1976-1985: Survival after local recurrence. Int J Ra-diat Oncol Biol Phys 1993;26:773–782.
4. Pryzant RM, Wendt CD, Delclos L, Peters LJ. Re-treatment of nasopharyngeal carcinoma in 53 patients.Int J Radiat Oncol Biol Phys 1992;22:941–947.
5. Morton RP, Liavaag PG, McLean M, Freeman JL. Tran-scervico-mandibulo-palatal approach for surgical salvageof recurrent nasopharyngeal cancer. Head Neck 1996;18:352–358.
6. Choy D, Sham JST, Wei WI, Ho CM, Wu PM. Transpala-tal insertion of radioactive gold grain for the treatment ofpersistent and recurrent nasopharyngeal carcinoma. Int JRadiat Oncol Biol Phys 1993;25:505–512.
7. Leung TW, Tung SY, Wong VYW, et al. High dose rateintracavitary brachytherapy in the management of naso-pharyngeal carcinoma. Acta Oncol 1996;35:43–47.
8. Feehan PE, Castro JR, Phillips TL, et al. Recurrent lo-cally advanced nasopharyngeal carcinoma treated withheavy charged particle irradiation. Int J Radiat OncolBiol Phys 1992;23:881–884.
9. Kondziolka D, Lunsford LD. Stereotactic radiosurgery forsquamous cell carcinoma of the nasopharynx. Laryngo-scope 1991;101:519–522.
10. Buatti JM, Friedman WA, Bova FJ, Mendenhall WM. Li-nac radiosurgery for locally recurrent nasopharyngealcarcinoma: Rationale and technique. Head Neck 1995;17:14–19.
FSRT for Locally Recurrent Nasopharynx Cancer HEAD & NECK July 1999 345