Embed Size (px)
Citation preview

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
June 12–14, 2013
Fourth Annual National ACO Summit
Follow us on Twitter at @ACO_LN
and use #ACOsummit.

Track Five: Optimizing Care Teams
SPECIALISTS IN ACCOUNTABLE CARE
Barbara L. Mcaneny, MD, Chief Executive Officer, New Mexico Cancer Center, New Mexico
Oncology Hematology Consultants, Ltd. Allan Field, Executive Consultant, Clinical Integration, Glenridge HealthCare
SolutionsGeraldine McGinty, MD, MBA, Partner, NRAD Medical Associates PC; Chair, Commission on
Economics, American College of Radiology; Former Medical Director, Outpatient Imaging,
Montefiore Medical CenterFrank Opelka, MD, FACS, Vice President, Health Affairs and Medical Education, Louisiana
State University System; Former Vice Chancellor for Clinical Affairs, LSU Health Sciences
Center; Former Associate Medical Director, American College of SurgeonsDavid Scamurra, MD, President, Eastern Great Lakes Pathology; Member, College of
American Pathologists

Barbara McAneny MD CEO, CEO New Mexico Cancer Center
CEO, Innovative Oncology Business SolutionsAMA Board of Trustees

The project described is supported by Funding Opportunity Number CMS-ICI-12-0001 from Centers for Medicare and Medicaid Services, Center for Medicare and Medicaid InnovationThe content of the presentation and the projects are solely the responsibility of the authors and do not necessarily represent the official views of HHS or of any of its agencies.



Chart #12





Medicare payment vs. practice cost inflation

62.1% of Bankruptcies are from Medical bills : 48% of the bills are from Hospitals, 18% drugs, 15% physiciansAnnual Health Care Costs $16,771

When patients visit a physician office that is part of a hospital’s outpatient department, Medicare pays a facility fee to the hospital and a reduced fee for the physician’s services. The combined fees paid for visits to hospital‐based practices are often more than 50 percent greater than rates paid to freestanding practices.


Physician fee schedule payments: $47,500Hospital Outpatient Prospective Payment System: $54,000
Milliman Client Report Oct 19, 2011 by Fitch and Pyenson

A detailed analysis of the demonstration is currently available only for the first two years. That analysis showed that, for patients in the 10 group practices during the second year, average Medicare spending excluding the bonuses paid to physician groups was about 1 percent below projections; with bonuses included, average Medicare spending was just 0.1 percent below
projections—about $7 per beneficiary.

Focus on the patients with expensive illnessesWhat factors can doctors control?What data do we need to prevent complications?

19
CMMI1
Support for Oncology Medical Homes
Source: Innovative Oncology Business Solutions, Albuquerque, NM; Oncology Roundtable interviews and analysis.
1)
Center for Medicare and Medicaid Innovation.2)
Community oncology medical home.
Innovative Oncology Business Solutions’
COME HOME2
Project
1 2 3Development of Medical HomeNew Mexico Cancer Center care delivery model matches medical home
Payer Engagement UnsuccessfulOne local and one national payer approached, unwilling to create new payment model
Application for CMS Health Care Innovation AwardCEO of NMCC forms the consulting group Innovative Oncology Business Solutions
4Spreading the Oncology Medical HomeGrant will support care transformation at seven oncology practices, potentially providing a proof of case
net.orange PartnershipHealth care informatics company will create electronic dashboards to monitor pathway adherence, share blinded data with providers, and compile data useful for the creation of bundled payments
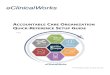
COME HOME Project

Study Patient Types
ED Visits
IP Adm
Group Health Coop of Puget Sound (12 mos) All Pts - 29 % - 11 %
Community Care of North Carolina Asthma - 16 % -
40%
Health Partners Medical Group BestCare Patient Centered Medical Home (PCMH) (5 Yrs)
All Pts - 39 % - 24 %
Genessee Health Plan HealthWorks PCMH (4 yrs) All Pts -
50% - 15 %
Johns Hopkins Guided Care (12 mos) Chronic Disease
- 15 % - 24 %
Geisenger Health System ProvenHealth Navigator Chronic Disease
--- - 14 %
Intermountain Healthcare Medical Group PCMH All Pts --- -
10%

Triage NursesTriage systemSame day appointmentsAbility to function as urgent care (lab, Xray)Extended hours (without the volume to support)Patient educationDoctors on call admitting their own patientsPathway development

Direct admissions (no ED) $196,200Clinic instead of ED visits $1,208,700Hospice instead of Hospital $3,900,000Lower ALOS $2,125,500Avoided Admissions $18,500,040

Innovative Oncology Business Solutions (IOBS) – managing organization formed for the purposes of administering projectSeven community oncology practices◦
New Mexico Cancer Center◦
Center for Cancer & Blood Disorders (Ft. Worth)◦
Dayton Physician Network (OH)◦
Space Coast Oncology◦
Maine Center for Cancer Medicine◦
NW Georgia Oncology Centers◦
Austin Oncology GroupNet.Orange – HIT company creating customized quality & pathway performance dashboards using claims data and integrated EHRsKEW Group – integration of genetic markers into diagnostic and therapeutic pathways UTHSC – evaluation, cost, quality measurement expertise; using claims data for rapid-cycle feedback of cost/utilization performance

Newly diagnosed or relapsed oncology patientsSeven tumor types will be put on Diagnostic/ Therapeutic Pathways:◦
Breast◦
Lung◦
Colorectal◦
Lymphoma◦
Melanoma◦
Pancreas◦
Thyroid
Seeking care @ 1 of 7 participating sites

Enhanced Services (Phase I)◦
Patient education & medication management◦
24/7 practice access: telephone triage, triage pathways, night/weekend clinic hours, on-call physicians
◦
On-site or near-site imaging, lab testing◦
Admitting physicians who shepherd pts through IP encounters, avoiding handoffs & readmits, ensure seamless care
Diagnostic pathways, including genetic markers (Phase II)Therapeutic pathways, including genetic markers (Phase III)

Patient Type Medicare Non-Medicare Total Breast Cancer 1,587 304 1,891Lung Cancer 1,536 294 1,830Colorectal Cancer
888 170 1,058
Lymphoma 538 103 641Melanoma 439 84 523Pancreas 402 77 479Thyroid 147 28 175Other Cancers 2,485 476 2,961Total Cases 8,022 1,536 9,558

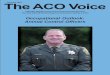
Service
Average Cost Per Unit of Service
Baseline Total Costs Per Patient*
Projected Decrease in Costs
Projected Total Costs Per Patient
ProjectedAverage Savings Per Patient
Hospital $8,225 $17,108 -
21.15 % $13,489 $3,619ED Visits $ 554 $ 1,136 -
52.2 % $543 $ 593Physician $ 228 $ 6,398 + 7.6 % $6,882 -
$ 484Pharmacy $ 90 $13,355 -
3.4 % $12,905 $ 450Other $9,480 $28,573 0.00 % $28,573 $ 0Total $66,569 6.276 % $62,391 $4,178
*Cost Projections based on Medical Expenditure Panel Survey (MEPS) data for Medicare beneficiaries in ‘poor health’, inflated to reflect higher expenditures associated with cancer.

Wish me luck.Any questions?

Track Five: Optimizing Care Teams
SPECIALISTS IN ACCOUNTABLE CARE
Barbara L. Mcaneny, MD, Chief Executive Officer, New Mexico Cancer Center, New Mexico
Oncology Hematology Consultants, Ltd. Allan Field, Executive Consultant, Clinical Integration, Glenridge HealthCare
SolutionsGeraldine McGinty, MD, MBA, Partner, NRAD Medical Associates PC; Chair, Commission on
Economics, American College of Radiology; Former Medical Director, Outpatient Imaging,
Montefiore Medical CenterFrank Opelka, MD, FACS, Vice President, Health Affairs and Medical Education, Louisiana
State University System; Former Vice Chancellor for Clinical Affairs, LSU Health Sciences
Center; Former Associate Medical Director, American College of SurgeonsDavid Scamurra, MD, President, Eastern Great Lakes Pathology; Member, College of
American Pathologists

Track Five: Optimizing Care Teams
ALIGNING ROLES AND RESPONSIBILITIES FOR CARE DELIVERY TEAMS
Terrence O'Malley, MD, Medical Director, Non‐Acute Care Services, Partners; Medical
Director, Spaulding Nursing and Therapy Center, North End; Medical Director, Partners Home
CareDiane Cardwell, MPA, ARNP, PA‐C, Vice President of Healthcare Solutions, TransforMEDJ. Emilio Carillo, MD, MPH, Vice President, Community Health Development, New York
Presbyterian, Former President and Chief Medical Officer, New York‐Presbyterian Community
Health Plan, Former President, New York City Health and Hospitals CorporationPaul Cook, MD, President and Chief Executive Officer, Rocky Mountain Health NetworkTerry McGeeney MD, MBA, Director, BDC Advisors

Aligning Roles and Responsibilities
Maximizing Value

Lewis Carroll on Measuring Value
"Cheshire Puss”, she began, rather timidly, as she did not know at all whether it would like the name: however, it only grinned a little wider. Come,
it's pleased so far, thought Alice, and she went on. “Would you tell me please, which way I ought to go from here?”
“That depends a good deal on where you want to get to”, said the cat.
“I don't much care where”, said Alice.
“Then it doesn't matter which way you go”, said the cat.
“... So long as I get somewhere”, Alice added as an explanation.
“Oh, you’re sure to do that”, said the cat, “if you only walk long enough.“
“Alice in Wonderland” Lewis Carroll

Defining Before Aligning: What’s Value?
• Four questions about Value– How do you define and measure value?– Whose definition of value counts most?– How do you reorganize care to increase
value?– How do you know that what you’ve done has
increased value?

Two Value Definitions
• Value =(Patient Satisfaction + Quality) /Cost
• Value = effective interventions in concordance with the patient’s goals and priorities

What is Value?
• Health care services have value to the patient insofar as they are concordant with the patient’s goals and wishes
• An intervention has value only if the patient– Wants it– Accepts it– Finds it appropriate – Finds it effective– Receives in an acceptable manner

Aligning Roles and Responsibilities
• Goal: Maximize value• Missing pieces: How to bring the patient
into the center of the care plan process– Identify goals of care: who, how, when, where– Create care plans that are consistent with the
patient’s priorities• How to engage the patient in creating the care plan
– Oversee the implementation of this care plan across the entire episode of care
• Who is responsible across sites and teams

What This Means for ACOs
• Critically important to develop process to– Identify the patient’s goals of care– Match proposed interventions with those
goals– Provide care that meets the patient’s needs
• Care that is not concordant with the patient’s goals will add cost without value

The Challenge is Measurement
• Goal: Maximize Concordance • Strategies:
– Address all patient concerns – Provide care that is consistent with the patient’s goals and
wishes– Address all high priority issues
• Tactics:– Identify detailed goals of care (ask the patient)– Record goals of care in a standardized place and format– Make goals of care available to all providers– Assign responsibility to the Care Team to insure that
interventions and patient priorities line up

Measurement
• Chart reviews– Presence of documented goals of care– Presence of explicit connections between
goals, patient priorities and interventions– Targeted review of ED and ICU records
• Patient surveys– Agreement with documented goals of care– Perceived disconnect between interventions
and goals

Aligning Roles and Responsibilities
• Goal: Maximize value• Missing pieces:
– Identify goals of care: who, how, when, where– Create care plans that are consistent with the
patient’s priorities• How to engage the patient in creating the care plan
– Oversee the implementation of this care plan across the entire episode of care
• Who is responsible across sites and teams

Track Five: Optimizing Care Teams
ALIGNING ROLES AND RESPONSIBILITIES FOR CARE DELIVERY TEAMS
Terrence O'Malley, MD, Medical Director, Non‐Acute Care Services, Partners; Medical
Director, Spaulding Nursing and Therapy Center, North End; Medical Director, Partners Home
CareDiane Cardwell, MPA, ARNP, PA‐C, Vice President of Healthcare Solutions, TransforMEDJ. Emilio Carillo, MD, MPH, Vice President, Community Health Development, New York
Presbyterian, Former President and Chief Medical Officer, New York‐Presbyterian Community
Health Plan, Former President, New York City Health and Hospitals CorporationPaul Cook, MD, President and Chief Executive Officer, Rocky Mountain Health NetworkTerry McGeeney
MD, MBA, Director, BDC Advisors

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
June 12–14, 2013
Fourth Annual National ACO Summit
Follow us on Twitter at @ACO_LN
and use #ACOsummit.