Embed Size (px)
Citation preview

Four Primary Tumors in One Child
A. D. J. PEARSON, MRCP,',II A. W. CRAFT, MD.'.ll R. H. PERRY, MRCPATH,§'# R. M. KALBAG, FRCS$" AND R. G. 8. EVANS, FRCRt,*
A child is described who, following surgery and irradiation for malignant choroid plexus papilloma at the age of 11 months, developed three further tumors: A benign myxofibroma of the cranium at the age of 3% years, an undifferentiated anaplastic tumor of his clavicle at 7% years, and a chondroblastic osteogenic sarcoma of his pelvis at the age of 12 years. There was no apparent genetic predisposition to malignancy. The latter three neoplasms may have originated either in, or at the edge of, the original radiotherapy field, suggesting that the child has a particular susceptibility to the oncogenic potential of radiotherapy.
Cancer 52:2363-2368, 1983.
HE OCCURRENCE of second malignant neoplasms T (SMN) in survivors of childhood cancer is well es- tablished. ' Some of these occur in individuals with a ge- netic predisposition to malignancy,2 and in others irra- diation and chemotherapy have been implicated as caus- ative factor^.^.^
A child is described who presented with a malignant choroid plexus papilloma and subsequently developed three other neoplasms. The angiographic appearance' and clinical history, along with aspects of the pathology,6 fol- lowing the first two neoplasms have been previously re- ported.
Case Report
The child was the third child of healthy, unrelated parents, and there was no history of malignancy in first or second degree relatives. He had been well until the age of 1 I months when he presented with signs of raised intracranial pressure. Radio- logical investigations showed dilated ventricles with a 6-cm lob- ulated mass within the right lateral ventricle. At operation, in spite of considerable blood loss, the vascular tumor was com-
From the Departments of Child Health* and Radiotherapy,? Royal Victoria Infirmary; the Department of Neurosurgery* and the MRC Neuroendocrinology Unit,§ Newcastle General Hospital, Newcastle upon Tyne.
Supported by the Leukaemia Research Fund. 11 Research Registrar. ll Paediatrician. # Pathologist. ** Neurosurgeon. * Radiotherapist. Address for reprints: A. D. J. Peanon, MRCP, Department of Child
Health, Royal Victoria Infirmary, Newcastle upon Tyne NEI 4LP, United Kingdom.
The authors are grateful to Dr. M. Catto who kindly reviewed the histologic material.
Accepted for publication September 24, 1982.
pletely excised. Histology confirmed a malignant choroid plexus papilloma (Fig. 1).
Postoperatively he received full brain irradiation, but 3 weeks later malignant cells were identified in the cerebrospinal fluid (CSF), and spinal irradiation was added. Radiotherapy details are shown in Table 1. Following this he remained well and no further malignant cells were identified in the CSF.
At the age of 3% years, a right-sided occipital swelling was noticed following a fall. A skull x-ray showed a large defect in the right occipital bone. A ventriculogram revealed a com- municating hydrocephalus and a left-sided ventriculoatrial shunt was inserted. The CSF was normal, as was a right carotid an- giogram. The mass did not regress and was surgically removed 1 month later. It was covered by pericranium and at operation appeared to be arising from the diploe of the skull. It weighed 300 g, was comparately avascular, and the histological appear- ance suggested a benign myxofibroma (Fig. 2).
He was well for a further 3 years when, at the age of 7% years, a hard, well circumscribed mass measuring 4 X 3 cm appeared above the medial end of his left clavicle. An x-ray of the clavicle was normal. The tumor and adjacent clavicle were resected and, macroscopically, the appearances suggested that the tumor was arising from the periosteum. Histologic study revealed a poorly differentiated anaplastic tumor infiltrating muscle and connective tissue. In the majority of areas, the tumor bore no resemblance to either the original choroid plexus tumor or the myxofibroma (Fig. 3A). In occasional areas, the appear-
TABLE 1. Details of Radiotherapy Given for Treatment of Malienant Choroid Plexus Paoilloma
Site Dose Source FractionsJdays
Whole brain 18 Gy 4.2 MV 6/17
Sacrum and lumbar spine
Thoracic and cervical spine
Brain and cervical spine 6 Gy 250 KV 317
(15 X 7 cm) 18 Gy 250 KV 13/23
(15 X 17 cm) 18 Gy 250 KV 12/20
0008-543)</83/ I2 1512363 $ I . 10 0 American Cancer Society
2363

2364 CANCER December 15 1983 Vol. 52
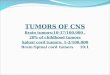
FIG. 1. Malignant choroid plexus tumor. Irregular papillary structures and acini formed by pleomorphic choroid plexus cells. In other areas the neuroglial stroma was infiltrated (H & E, X450).
ance of malignant cellls aligned against stromal tissue resembled histological fields in the original choroid plexus tumor (Fig. 3B). A definite histologic resemblance between these two tumors, however, could not be established. Intensive investigations at this time failed to reveal any further evidence of malignant
disease. He received radiotherapy to the tumor area with a dose of 36 Gy to a 9 X 6 cm field in I8 fractions over 23 days from a Cesium-I37 source.
He remained well, although he was noticed to be slow in- tellectually and his IQ was assessed at 78. A CT scan at the age
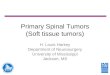
FIG. 2. High-power photomicro- graph of benign myxofibroma. Ir- regular fusiform and spindle cells are set in a myxomatous matrix (H & E, X450).

No. 12 FOUR PRIMARY TUMORS IN ONE CHILD - Peurson et uf. 2365
FIG. 3A. Tumor from the medial clavicular region. Highly cellular, pleomorphic, malignant tumor that showed no differentiation to suggest an origin in connective tissue or muscle, and no features to identify the neoplasm as an Ewing’s tumour, neuroblastoma or lymphoma de- posit. Intracytoplasmic glycogen could not be demonstrated. Several mitoses are present in this field (H & E. X450).
of 9 showed a low density area in the right cerebral cortex compatible with previous infarction.
At the age of I 2 years he developed a limp and a mass was
found in the right iliac region. X-ray confirmed a large soft tissue mass arising from the innominate bone with considerable intratumor calcification. Biopsy showed this to be a chondro-
FIG. 3B. Microscopic field show- ing some resemblance to original choroid plexus neoplasm (see Fig. I ) . A definite connection between the two neoplasms could not be es- tablished (H & E, X450).

2366 CANCER December 15 1983 Vol. 52
FIG. 4A. Bone tumor. The more densely cellular regions of this lob- ulated tumor are composed pre- dominantly of spindle or fusiform cells (arrows), some of which are in- terspersed in areas of chondroid dif- ferentiation (C). In the latter regions areas of ossification have occurred (0). The less differentiated fascicu- lated, malignant cells, favor a di- agnosis of a chondroblastic osteo- sarcoma rather than a chondrosar- coma (H & E, X 150).
blastic osteogenic sarcoma (Figs 4A and 4B). He is currently being treated with intensive chemotherapy, and shows no ev- idence of either growth retardation or endocrine dysfunction.
His serum immunoglobulins and chromosome analysis of pe- ripheral blood lymphocytes were normal. The radiation sen- sitivity of cultured skin fibroblasts also showed no abnormality.
FIG. 4B. High-power view of Fig. 4A (X450).

No. 12 FOUR PRIMARY TUMORS IN ONE CHILD - Peurson er af. 2367
An estimate of the irradiation doses given to the presumed site of origin of the clavicular and pelvic tumors, at the time of the initial radiotherapy, was I .8 Gy to each.
Discussion
Second malignant neoplasms (SMN) in childhood are well documented.' Various factors have been implicated in their pathogenesis: a genetic predisposition to malig- nancy, the therapy for the primary tumor-either irra- diation3 or chemotherapy4-or a combination of these factors. This child has had four separate tumors, three malignant and one benign. There is no evidence that he has a recognized genetic predisposition to malignancy. None of his first- or second-degree relatives have suffered a malignancy, suggesting that he is not a member of a Li-Fraumeni cancer family.7 Similarly, he had no con- genital abnormality or any of the other diseases which are known to predispose to childhood cancer.'
Malignant choroid plexus papilloma is a rare tumor, and in a review of the literature in 19759 only 22 cases were found which satisfied the strict histologic criteria laid down for its diagnosis.".' I Sixteen of these patients were children and all occurred in the lateral ventricle. The survival was poor, but even in those who did survive there have been no reports of second malignant tumors.
The second tumor in the current case, a myxofibroma, is unusual, although such tumors have been described as an abnormal tissue reaction to radiotherapy."
It is difficult to be certain of the exact nature of the third tumor. Circumstantial evidence has been presented to suggest that it may have been an extracranial metastasis from the original malignant choroid plexus papilloma. Extraneural metastases from malignant central nervous system tumors are well recognized, l 3 and their Occurrence increases following surgical in te rvent i~n , '~ but only one case of a metastatic malignant choroid plexus papilloma outside the nervous system has been reported." This oc- curred in a 7-year-old girl who developed multiple pleural lung metastases 1 year following the surgical removal of a malignant choroid plexus papilloma. The histologic characteristics of the metastases in this instance were identical to the primary tumor. The spread of a malignant choroid plexus papilloma into the subarachnoid is, how- ever, well documented.16 The child in this report devel- oped the clavicular lesion after the insertion of a ventric- uloatrial shunt, which potentially would have allowed malignant cells access to the circulation. However, a sol- itary metastasis developing 6 years after the primary in- tracranial tumor was resected would be an unusual oc- currence. The possibility of the clavicular tumor being an additional primary tumor is supported by its disparate
histologic features, its origin within a field of irradiation, and the occurrence of two other tumors within the ir- radiation field.
The fourth tumor, a chondroblastic osteogenic sarcoma, is quite definitely a second malignant neoplasm (SMN). Bone sarcomas are the most common SMN following the treatment of childhood cancer, and in a recent series comprised 40 of 188 such tumors." In 16 of these ir- radiation could be implicated as the causal factor. The importance of irradiation as a cause of SMN is further stressed in a series of 19 tumors in a population of 4 14 survivors of childhood cancer." Seventeen of these had received irradiation for their first tumor.
The radiotherapy following the excision of the malig- nant choroid plexus papilloma involved both megavoltage therapy to the brain and orthovoltage therapy to the spinal cord. The risk of SMN appears to be increased with the use of orthovoltage rather than megavoltage therapy," although SMN has been described following megavoltage therapy.20 SMNs following radiotherapy tend to occur at the periphery of a radiation and in the current case both the clavicular lesion and the chondroblastic osteogenic sarcoma probably arose at the periphery of the original radiotherapy field, these sites receiving rel- atively low doses of radiotherapy. The latent periods be- tween irradiation and the development of the SMN were relatively short, 6 and 1 1 years, respectively. In a review ofbone sarcomas by the Late Effects Study Group,17 eight patients who were irradiated when younger than age 5 years, and who had no known genetic predisposing dis- ease, had a mean latent period of 12 years with a range from 9 to 22 years, compared with a mean of 7 years in those who were both irradiated and had a genetic pre- disposition. The short latent period in the current child might suggest an unusual genetic susceptibility to malig- nancy of a currently unknown nature. We suggest, there- fore, that the latter two tumors in this child were in fact irradiation induced malignancies. Both conform to Ca- han's established criteria for irradiation induced tumors, these being different histologically from the original tu- mor, appearing within a previously irradiated volume of tissue, and occurring after a latent period of a number of years.22
I t is probable that the more widespread use of mega- voltage therapy will lead to a decreased number of SMNs, but this trend may be counterbalanced by the increased survival being achieved for many different types of cancer, particularly those in childhood.
ADDENDUM
The patient has subsequently died of widespread metastatic disease.

2368 CANCER December 15 1983 Vol. 52
REFERENCES
I . Meadows AT, DAngio GJ, MikC V et a/. Patterns of second ma- lignant neoplasms in children. Cancer 1977; 40:1903-191 I .
2. Abramson DH, Ronner HJ, Ellsworth RM. Second tumours in non-irradiated bilateral retinoblastoma. Am J Opthalmol 1979; 87:624- 627.
3. Li FP. Second malignant tumours after cancer in childhood. Cancer
4. Hams CC. A delayed complication of cancer chemotherapy: Can- cer. J Natl Cancer Inst 1979; 63:275-277.
5. Banna M. Angiography of malignant choroid plexus papilloma. Br J Radio1 1971; 44:412-415.
6. Valladores JB, Perry RH, Kalbag RM. Malignant choroid plexus papilloma with extraneural metastasis. J Neurosurg 1980 52:25 1-255.
7. Li FP, Fraumeni JF. Soft tissue sarcomas, breast cancer and other neoplasms: A familial syndrome? Ann Intern Med 1969; 7 1:747-752.
8. Heard G. Malignant disease in von Recklinghausen's neurofibro- matosis. Proc R Soc Med 1963; 50502-503.
9. Dotirmann GJ, Collias JC. Choroid plexus carcinoma. J Neurosurg
10. Ziilch KJ. Brain Tumours: Their Biology and Pathology, ed. 2.
1 I . Russell DS, Rubinstein U. Pathology of Tumours ofthe Nervous
12. Pifer JW, Hempelmann LH, Dodge HJ et af. Neoplasms in the
1977; 4 0 1899-1902.
1975; 43:225-232.
New York: Springer-Verlag, 1965.
System, ed. 2. London: E. Arnold, 1971.
Ann Arbor series of thymus irradiated children: A second survey. Am J Roentgenol 1968; 103:13-18.
13. Duffner PK, Cohen ME. Extraneural metastases in childhood brain tumours. Ann Neurol 1981; 10261-265.
14. Glasauer FE, Yuan RHP. lntracranial tumours with extracranial metastasis: Case report and review of the literature. J Neurosurg 1963;
15. Vraa-Jensen G. Papilloma of the choroid plexus with pulmonary metastases. Acta Psychiatr Neurol 1950; 25:299-306.
16. Lewis P. Carcinoma of the choroid plexus. Brain 1967; 90:177- 186.
17. Meadows AT, Strong LC, Li FP et a/. Bone sarcoma as a second malignant neoplasm in children: Influence of radiation and genetic pre- disposition. Cancer 1980; 46:2603-2606.
18. Li FP, Cassady JR, Jaffe N. Risk of second tumours in the survivors of childhood cancer. Cancer 1975; 35:1230-1235.
19. Tountas AA, Fornasier VL, Hanvood AR, Leung PMK. Post- irradiation sarcoma of bone. Cancer 1979; 43: 182- 187.
20. Haselow RE, Nesbit M, Dehner LP, Khan FM, McHugh R, Levitt SH. Second neoplasms following megavoltage radiation in a pe- diatric population. Cancer 1978; 42:1185-1191.
2 I . Brown JM. The shape of the dose-response curve for radiation carcinogenesis: Extrapolation to low doses. Radial Res 1977; 7 1:34-50.
22. Cahan WG, Woodward HG, Higinbotham NL. Stewart FW, Coley L. Sarcoma arising in irradiated bone: Report of eleven cases. Cancer
20:474-493.
1948: I :3-29.