Embed Size (px)
Citation preview
FORUM - Vendor Credentialing in Australia Presented by Standards Australia in association with the Medical Technology Association of Australia (MTAA)
Thursday, 7 July 2015 Sydney, Australia
Thursday, 7 July 2015 Sydney, Australia

WELCOME AND OPENING REMARKS
Dr Bronwyn Evans Chief Executive Officer Standards Australia
VENDOR CREDENTIALING IN AUSTRALIA

WHY ARE WE HERE? – FORUM OBJECTIVES
Susi Tegen, Chief Executive Medical Technology Association of Australia (MTAA)
Vendor Credentialing: Why are we here?
7 July 2015

Susi Tegen
Chief Executive, MTAA
Vendor Credentialing • Vendor credentialing within the health sector can
be defined as
“a compliance and risk management system used to manage risk in healthcare facilities (HCFs).” 1
1. Reference: Vendor Credentialing Proposal for Australian Healthcare Facilities on behalf of the Medical Technology Industry 2012, MTAA p: 4
Vendor Credentialing • Vendor Credentialing (VC) is the process of establishing
the qualifications of vendors and assessing their background and legitimacy. 2
2. Reference: White Paper on Vendor Credentialing: A Collaborative Industry Study 2012, HSCN p: 3
Benefits • The greatest benefit of vendor credentialing is patient
safety, with authorised MCRs entering HCFs being more easily identifiable.
• In addition:
• MCRs are better protected from healthcare risks
• HCFs are better able to track inappropriate or non-compliant behaviour
• workplace safety practices are strengthened.
Process • In markets, including Australia:
• credentialing is undertaken by third-party vendor credentialing (TPVC) providers on behalf of an accredited HCF
• an automated integrated database provides badges for accredited MCRs daily on-site at the HCF upon login
• There is no cost to the HCF for this service, only to companies for their staff to be credentialed.
• This process is essentially vendor access management, not vendor credentialing management.
USA experience • Practice is well established in USA and came about as
a result of 911.
1. TPVC conducts checks (e.g. vaccinations, training and police safety checks) of each MCR within a company and current liability insurance of the company on behalf of a hospital.
2. TPVC provides identification badges for those that meet the requirements.
3. TPVC retains data.
USA experience • In September 2007, AdvaMed wrote to The Joint
Commission following a review of existing hospital health care industry representative (HCIR) credentialing requirements.
• AdvaMed proposed nationally recognised credentialing standards that drew on existing standards (e.g. Association of periOperative Registered Nurses (AORN)), which reflected credible, purposeful and practical credentialing requirements for industry.
USA experience • In June 2009, the Independent Medical Distributors
Association (IMDA) released the Updated Joint Best Practices Recommendation for Clinical Health Care Industry Representative Credentialing. 3
• This document enhanced the recommended credentialing criteria put forward to The Joint Commission in 2007 by AdvaMed.
4. Reference: Updated Joint Best Practices Recommendation for Clinical Health Care Industry Representative Credentialing, IMDA (June 2009)

USA: today • While there are a number of relevant Joint Commission
standards including awareness of visitors entering accredited healthcare facilities, maintenance of patient rights and infection control precautions, there are no specific standards that address the credentialing of HCIRs entering healthcare organisations.
USA: today • There is no cost to the HCF for signing up to service,
only to companies requiring service to access a HCF. 3
• Each HCF has its own level of expectation and different credentialing requirements.
• Result is a wide range of disparate systems that don’t necessarily meet the needs of each HCF, which has increased the time and cost burdens on industry.
USA: cost • An HCIR who needs to access multiple HCFs may have
to be credentialed with a number of TPVC providers, increasing the cost burden on companies.
• Its estimated to cost up to $3,000 per rep per year to credential in USA (2010 figures).
• Larger companies have had to employ administration staff to manage VC requirements of HCIR by TPVC providers due to the large administration burden.
Canadian experience • To avoid the multiple vendor credentialing providers that
have sprung into existence in overseas markets, MEDEC has taken an alternative path.
Canadian experience • Working with industry and key stakeholders, a national
vendor credentialing standard was developed by Healthcare Supply Chain Network (HSCN) to: – “minimize the costs to the Canadian healthcare
system, simplify the process, avoid unnecessary duplication and protect the privacy rights of individuals.
– “The Standard makes Vendors responsible to ensure and attest that their employees who call on healthcare facilities meet the Standard.” 5
5. Reference: Information Sheet, HSCN National Standard for Vendor Credentialing (2013). HSCN, Canada.

Canadian experience • “Suppliers who wish to attest to their representatives
meeting the national standard submit their attestation form to be published in the national registry annually at no cost.
• “The National Standard for Vendor Credentialing is an efficient model for transferring accountability to the supplier for potential risks associated with supplier representatives having access to non-public areas of the hospital.” 6
6. Reference: HSCN, Canada website.
Canadian experience • “The goal of the HSCN national standard and centralized
registry is to streamline the credentialing process, so that healthcare providers and their suppliers can address all their credentialing needs in one place and eliminate the need for hospitals and SSO’s to manage the credentialing process individually.” 6
6. Reference: HSCN, Canada website.
Canadian experience • “In January 2013, HSCN unveiled the national standard
and accompanying registry to the healthcare supply chain industry.
• The national standard and registry were developed in response to the request of HSCN members to develop a collaborative approach to vendor credentialing that would avoid the legal risks, inefficiencies and tremendous costs seen the US.” 6
6. Reference: HSCN, Canada website.
Canadian experience • “The development of the national standard was based
on meeting the needs of patients, healthcare providers, but ensuring the process and requirements met legal and ethical standards around human rights, labour rights, and personal privacy laws.
• Under the HSCN model, personally sensitive information is maintained by the representative’s employer and is not transferred to HSCN or stored on 3rd party databases.” 6
6. Reference: HSCN, Canada website.
Vendor credentialing for Australia • Vendor credentialing should balance the need for:
– patient safety – patient and MCR privacy – high quality care – immediate access to medical products – efficient communication of product information and
education provided by the MCR – efficient use of resources by HCFs and vendors.
Australian experience • Vendor credentialing needs to ensure it:
– addresses patient risk concerns of HCFs
– ensures continued effective interactions between clinicians and medical companies for the development and delivery of medical products across Australia
– is standards based
– is comprehensive
– is commercially viable.
INTRODUCTION TO STANDARDS AUSTRALIA
Facilitator: Miss Bronwyn Walker National Sector Manager Standards Australia
HOUSE KEEPING Toilets and venue Emergency procedures Mobiles on silent Return from the break on time
EMERGENCY PROCEDURES

FORUM AGENDA

PROGRAM
10:00 AM - Welcome and opening remarks Bronwyn Evans, CEO, Standards Australia 10:10 AM - Why are we here? Susi Tegen, CE, Medical Technology Association Australia 10:25 AM - Introduction to Standards Australia and the standards development process Bronwyn Walker National Sector Manager, SA 10:40 AM - An industry perspective Pat Callanan, Country Manager, American Medical Systems (AMS) & MTAA Board Director
PROGRAM
11:40 AM - Vendor Credentialing: The Mitcham Private Hospital Experience Samantha Dodd - CEO of Mitcham Private Hospital 12:00 PM - Quality and safe patient care: Important factors to be considered when working in healthcare facilities Dr Patricia Nicholson, Deakin University, President VPNG and ACORN Board Member 12:20 PM - Q and A panel - (Pat Callanan, Samantha Dodd and Dr Patricia Nicholson) 12:50 PM - LUNCH 1:10 PM - Break out groups
PROGRAM
2:50 PM - Afternoon break 3:00 PM - Reporting back - summary and evaluation Fiona Shipman - MTAA/Bronwyn Walker - SA 4:15 PM – Close, Q and A. - Bronwyn Walker, SA

WHY DO WE HAVE STANDARDS?
STANDARDS BENEFIT THE INDUSTRY
Reduce costs
Expand markets
Risk management
tool

ARE STANDARDS LAW?
Standards Australia

STANDARDS DEVELOPMENT – OVERVIEW Our process is built around: • Openness • Transparency • Consensus
PROJECT PROPOSAL PROCESS
For the Standards Resourced Pathway, Project Proposals can be submitted twice a year: Round 10 Monday 2 February – Wednesday 18 March 2015 Round 11 Monday 10 August to Wednesday 23 September 2015
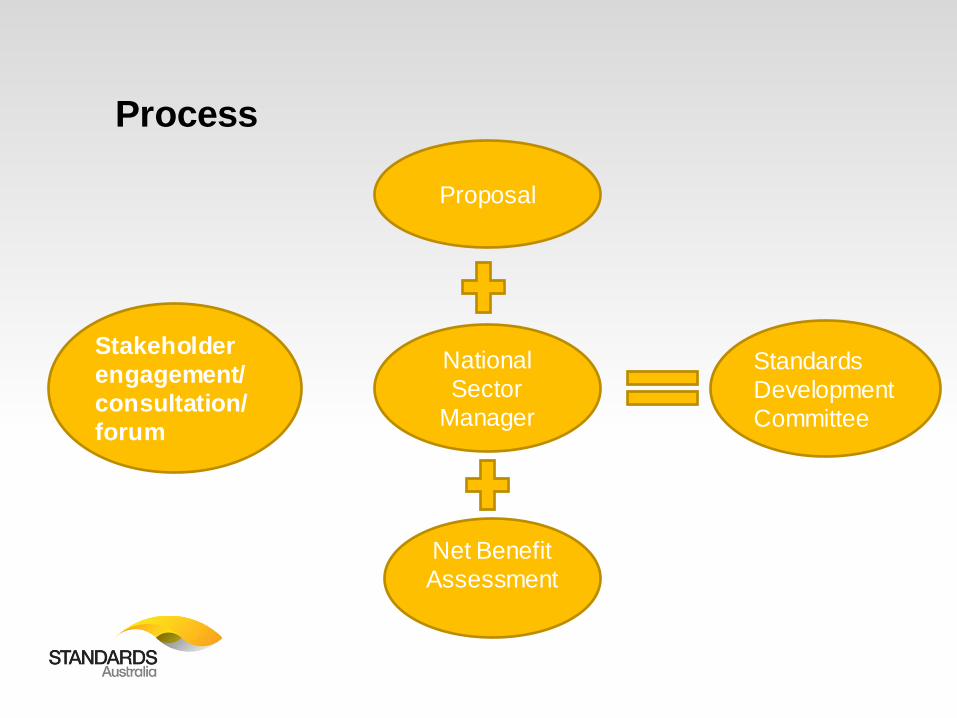
Process
Stakeholder engagement/consultation/ forum
Proposal
National Sector
Manager
Net Benefit Assessment
Standards Development Committee

WE MAKE A DIFFERENCE EVERY DAY
AS 3660 Protection of buildings from subterranean termites
AS 2047-1999 Windows in buildings - Selection and installation
ISO 10993-17:2002 Biological evaluation of medical devices -- Part 17: Establishment of allowable limits for leachable substances
WHAT WE DO MATTERS IN THE DETAIL BUT …..
AS 3660.1-2014 TERMITE MANAGEMENT FOR NEW BUILDING WORK
Standards Australia has recently published a new Australian Standard for Termite Management for New Building Work known as AS 3660.1-2014 AS 3660.1-2014 is primarily concerned with - Providing measures to reduce the risks of undetected subterranean termite attack on
buildings. - The Standard sets out requirements for the design and construction of subterranean termite
management systems for new buildings and new building work. - It includes solutions for both physical and chemical termite management systems. - Options are provided so that various approaches may be used either singly, or in
combination, to provided an integrated termite management system. - Improving design requirements to minimise termite damage is one of several risk reduction
measures available. - The Standard describes measures to deter termite attack arising from concealed entry into a
building. The system options available rely on a combination of: - Partial measures to termite passage - Perimeter inspection zones (so that when termites attack, evidence of their workings is in the open
where it may be detected more readily during regular inspections) NOTE: The measures contained in the Standard cannot guarantee that a building will never be entered by termites nor will ever suffer some form of termite attack.

Simpler | Faster | Better
FURTHER INFORMATION
• Detailed information on our process is available in our
Standardisation Guides available for download on our website.
Standards Development Process
PAT CALLANAN REGIONAL DIRECTOR, AMS, MTAA BOARD DIRECTOR
Vendor Credentialing: An industry perspective
Vendor Credentialing: An industry perspective
7 July 2015
©2012 American Medical Systems, Inc. All rights reserved. 44
©2012 American Medical Systems, Inc. All rights reserved. 45
Pat Callanan
Regional Director, AMS MTAA Board Director
Vendor Credentialing
• Vendor Credentialing (VC) is the process of establishing the qualifications of vendors and assessing their background and legitimacy. 1
1. Reference: White Paper on Vendor Credentialing: A Collaborative Industry Study 2012, HSCN p: 3
The role of industry
– Entry to the hospital environment, particularly the perioperative area, is a privilege and not a right for industry
– Industry representatives play a clear role in the efficient training of hospital staff , with provision of products and services to improve patient outcomes
– Industry provide numerous value added benefits in addition to the products we supply, often at significant cost savings to the institution
©2012 American Medical Systems, Inc. All rights reserved. 47
What does VC mean for industry?
– What problem are we trying to solve? – Multiple providers = multiple costs – Servicing models may be impacted by restricted access – Potential privacy issues with information access – What mechanisms exist to ensure TPVC providers remain
compliant? – The industry is vibrant with over 500 suppliers ranging
from small startups to large multinationals. It is vital that an equitable playing field remains for all, not just those who can pay.
What are the benefits?
– Most perioperative environments already require sign in – MTAA provides MCR accreditation for ACORN standards – The public can access most areas of the hospital without
accreditation, so how does vendor credentialing improve compliance?
– MCR’s provide services free of charge, which would otherwise be borne by the hospitals
– MCR’s are happy to be credentialed providing it is simple and cost effective
What are the costs?
– The financial cost for one MCR to be credentialed to enter one healthcare facility, and then have that process repeated across a number of facilities using a range of TPVC providers could be far reaching.
– Current product pricing restraints means suppliers can not absorb significant credentialing costs without changing servicing models
– Restricted access may result in ‘cost’ transfer to healthcare providers and result in adverse patient outcomes
– Ensuring one entry, many exits of credentialing data is the best way to minimise the cost burden to companies.
Burden on Australian industry
– The three immediate issues for Australian medical companies in relation to vendor credentialing MCRs are: 1. Vendor fees 2. Replication 3. Confidentiality of data
Vendor credentialing
– The aim of vendor credentialing should be to balance the need for: – patient safety – patient and MCR privacy – high quality care – immediate access to medical products – efficient communication of product information and
education provided by the MCR – efficient use of resources by HCFs and vendors.
What is needed?
• It’s essential that the requirements for vendor credentialing be defined to ensure patient safety and the continued effective interactions between clinicians and medical companies for the development and delivery of medical products across Australia.
• A national standard for vendor credentialing, not access control, that is accepted by any Australian healthcare facility is required.
• A single, simple process for credentialing that protects employee privacy,preferably industry developed.
Morning Tea Break – 20 Minutes
ESTABLISHING A UNIFORM POSITION
Samantha Dodd CEO Mitcham Private Hospital
Establishing a uniform position
Samantha Dodd CEO Mitcham Private Hospital
Why trial? Patient factors Theatre is not a selling space Who is there and why? Qualifications Prosthesis management Recall Infection control Governance Standard
How the trial was run 10 weeks 5 theatres App technology Executive buy in Theatre and Dr buy in Rep buy in
The good No reps could enter without a scheduled visit Transparent process Competency had to be completed prior Particular policy sign off good Good compliance with policy Control
The bad Financial stand off with some companies, even though
cost was low (during trial period) Impact on business Other peoples “dirty work” Pass on costs Administration burden Multiple providers therefore multiple costs to
companies
Where to now?? Needs to be regulated Should it be a third party business? How often to register? Who credentials the credentiallers? Impact to companies Minimum standard requirement
Questions

Dr Patricia Nicholson, Deakin University, President VPNG and ACORN Board Member
QUALITY AND SAFE PATIENT CARE: IMPORTANT FACTORS TO BE CONSIDERED WHEN WORKING IN HEALTHCARE FACILITIES

Quality and safe patient
care: Important factors to be considered when working in
healthcare facilities
Dr Pat Nicholson Senior Lecturer, School of Nursing and Midwifery, Deakin University President, Victorian Perioperative Nurses Group

Presentation Overview • Overview of Standards governing Nursing
and Midwifery practice • Visitors in the healthcare facility (HCF) • Patient safety • Visitors to the operating suite • Education and training of visitors • Future of credentialing

Standards in Nursing & Midwifery
• National competency standards for Nurses and Midwives
• Code of Ethics and Professional Conduct (Nursing and Midwifery Board, Australia)
• Australian College of Operating Room Nurses Standards of practice for perioperative nursing (2014 – 2016) & ACORN Competency standards (2006)

Visitors to HCFs
• Orientation to the HCF • WH&S requirements • Professional conduct • Immunization requirements • Infection control

National Safety and Quality Health Service Standards September 2012

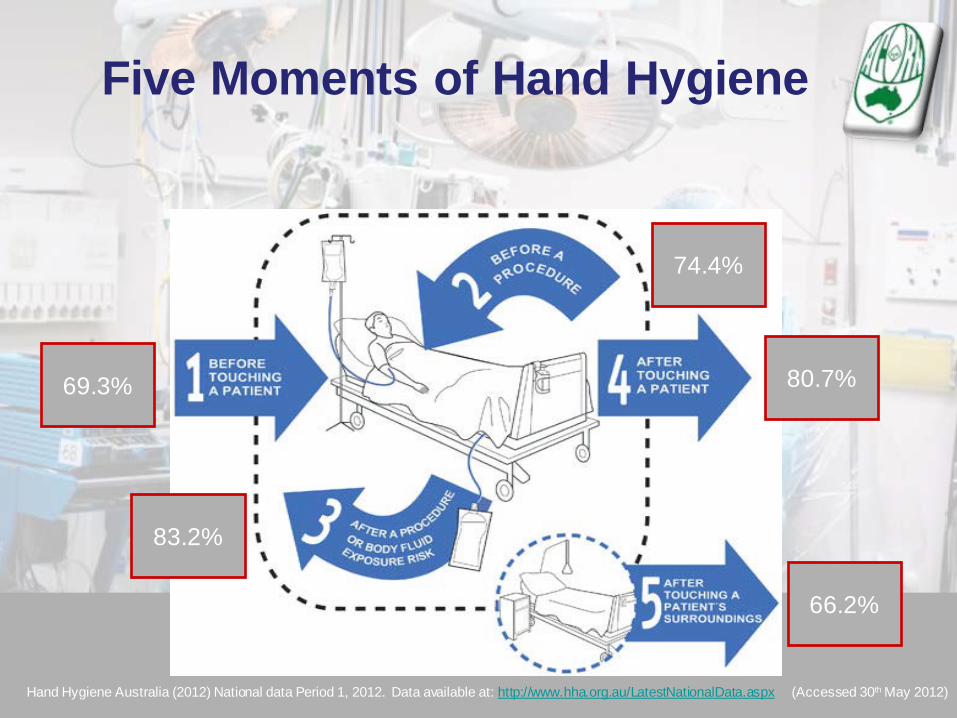
Hand Hygiene Australia (2012) National data Period 1, 2012. Data available at: http://www.hha.org.au/LatestNationalData.aspx (Accessed 30th May 2012)
69.3%
74.4%
80.7%
83.2%
66.2%
Five Moments of Hand Hygiene

Patient healthcare rights
• Safe practice • Respect • Confidentiality • Privacy • Informed consent

76
……..to promote excellence in perioperative nursing care
Australian College of Operating Room Nurses
77
ACORN – The spirit of perioperative nursing Standards utilising evidence based practice Professional growth and development Innovation to achieve best patient care
outcome Representation of all States and Territories Influential in health policy Teamwork development local, nationally &
internationally
ACORN Standards for Perioperative Nursing
Referenced, reflecting evidence-based practice – highest standard of patient care – professional competence
• Provide professional guidelines and specific recommendations
• Valuable resource for perioperative nurses involved with the care of patients in the OR
79




Any visitor in the operating suite not associated in the care that is being provided has been said to be violating the patient's right to privacy and confidentiality. (p. 406)
ACORN 2014-2015
Patient privacy and confidentiality
MCRs shall provide evidence of education and instruction that ensures safe conduct and practice within the perioperative environment. (p: 405)
ACORN 2014-2015
Standard Statement 8

Credentialing is everyone’s
responsibility

OPEN PANEL DISCUSSION: Q&A
Facilitator: Miss Bronwyn Walker National Sector Manager Standards Australia
Lunch – 30 Minutes In the Round Room outside

GROUP DISCUSSION/BREAKOUT GROUPS
Standards Australia

Afternoon Tea Break – 20 Minutes

Standards Australia
Summary and actions
FORUM SUMMARY AND THANKS

Standards Australia
Next steps?

FOLLOW US
www.standards.org.au