Embed Size (px)
Citation preview
FORTH VALLEY NHS BOARD A meeting of FORTH VALLEY NHS BOARD will be held on TUESDAY 25 SEPTEMBER 2012 at 9:30AM in the BOARDROOM, FORTH VALLEY NHS BOARD HEADQUARTERS, CARSEVIEW HOUSE, CASTLE BUSINESS PARK, STIRLING,
Please notify apologies for absence to Gail Hayworth, Deputy Head of Corporate Services
email [email protected] or telephone 01786 457248
AGENDA 1/ APOLOGIES FOR ABSENCE 2/ DECLARATIONS OF INTEREST For Noting 3/ MINUTE OF FORTH VALLEY NHS BOARD MEETING HELD ON For Approval
31 JULY 2012
4/ MATTERS ARISING 5/ FINANCIAL & PERFORMANCE ISSUES 5.1 Executive Performance Report to ending August 2012 For Noting (Paper presented by Professor Fiona Mackenzie, Chief Executive) 6/ ASSET BASED APPROACH For Noting
(Presentation by Dr Anne Marie Wallace, Director of Public Health) 7/ REPORTS FROM SUB COMMITTEES
7.1 Minute of Area Clinical Forum meeting held on 19 July 2012 For Noting 7.2 Minute of Performance & Resources Committee meeting held on For Noting 3 August 2012 and 7 September 2012 7.3 Minute of Clinical Governance meeting held on 27 July 2012 For Noting
8/ P atient R ights (S cotland) Ac t 2011 For Noting (Paper presented by Professor Angela Wallace, Director of Nursing) 9/ ACCESS POLICY For Approval (Paper presented by Professor Fiona Mackenzie, Chief Executive) 10/ FORTH VALLEY NHS BOARD MEETING/SEMINAR PROPOSED DATES 2013 For Noting (Paper presented by Professor Fiona Mackenzie, Chief Executive) 11/ ANY OTHER COMPETENT BUSINESS

Forth Valley NHS Board Meeting Tuesday 25 September 2012 Apologies: Ms Fiona Gavine Mr Tom Hart Dr Iain Wallace Present: Mr Alex Linkston (Chairman) Dr Allan Bridges Councillor Margaret Brisley Mr Brendan Clark Dr Stuart Cumming Mr Charles Forbes Mrs Helen Kelly Mr James King Professor Fiona Mackenzie Dr Vicki Nash Mrs Fiona Ramsay Dr Anne Maree Wallace Professor Angela Wallace Councillor Gary Womersley Councillor Linda Gow In Attendance: Ms Elsbeth Campbell, Head of Communications Mr Tom Steele, Director of Projects & Facilities Ms Margaret Duffy, Director of Integration Ms Elaine Vanhegan, Head of Performance Management Mr David Currie, National Finance Trainee Ms Gail Hayworth, Deputy Head of Corporate Services (Minute) Presenters: Ms Aileen Schofield, Health Promotion Officer (Item 6) Ms Roslyn Grant, Service Improvement Manager (Item 9) Mr Andy Rankin, Head of Patient Access (item 9)

1
Forth Valley NHS Board 25 September 2012 This report relates to Item 3 on the Agenda
Minutes of the Forth Valley NHS Board Meeting held on 31 July 2012
For Approval
2
FORTH VALLEY NHS BOARD Minute of the Forth Valley NHS Board meeting held in closed session on Tuesday 31 July 2012 in the Forth Valley NHS Board Headquarters, Carseview House, Castle Business Park, Stirling. Present: Mr Alex Linkston (Chairman) Councillor Margaret Brisley Mr Brendan Clark Mr Charlie Forbes Ms Fiona Gavine Mr James King Mrs Helen Kelly Professor Fiona Mackenzie Dr Vicki Nash Mrs Fiona Ramsay Dr Anne Maree Wallace Professor Angela Wallace Dr Iain Wallace Councillor Gary Womersley In Attendance Ms Margaret Duffy Mr Tom Steele, Director of Projects & Facilities Dr John Schulga. Consultant Paediatrician, Item 6 Ms Sally Boa, Speech & Language Therapist (Specialist Advisor) Item 6 Ms Elsbeth Campbell, Head of Communications Ms Beverley Finch, Head of Corporate Services Ms Marian Smith, Corporate Services Assistant (minute) Mr Linkston extended a warm welcome to Councillor Margaret Brisley and Councillor Gary Womersley to their first NHS Board meeting. 1. APOLOGIES FOR ABSENCE
Apologies for absence were intimated on behalf of Dr Allan Bridges, Dr Stuart Cumming, Councillor Linda Gow and Mr Tom Hart.
2. DECLARATIONS OF INTEREST
There were no declarations of interest.
3. MINUTE OF FORTH VALLEY NHS BOARD MEETING HELD ON 29 MAY 2012
The minute of the Forth Valley NHS Board meeting held on 29 May 2012 was approved as a correct record.
4. MATTERS ARISING
There were no matters arising.
5. FINANCIAL & PERFORMANCE ISSUES
5.1 Executive Performance Report to end June 2012 The NHS Board considered a paper “Executive Performance Report to end June 2012”, presented by Professor Fiona Mackenzie, Chief Executive. Professor Mackenzie advised that the format of the Board Executive Performance Report had been streamlined to ensure the Board is updated on key performance issues whilst

3
acknowledging that the Performance and Resources Committee would consider performance issues in more detail. Professor Mackenzie highlighted the following, as detailed within the report: • First Anniversary of the opening of Forth Valley Royal Hospital • Partnership working with Forestry Commission Scotland and Central Scotland
Lowland Trust • NHS Board Annual Development Day • Waiting Tomes • Annual Review • Lesbian, Gay, Bisexual and Transgender (LGBT) Youth Scotland Charter Mark
‘Essentials’ Award • RoSPA Gold Award to Serco
She further highlighted the ‘talking tablets’ labels pilot currently running in Callander and the new telephone reminder service which has resulted in a decrease in the number of patients failing to attend appointments.
Professor Mackenzie highlighted the Performance Summary within the report, specifically:-
• Heat Key Measure –
o Equitable - Breastfeeding o Efficient - Theatre Management, Attendance Management o Timely - Waiting Times Performance, Stage of treatment targets o Effective - Delayed Discharge o Person Centred - Complaints
• Corporate Risk Summary • Healthcare Associated Infection Reporting Template (HAIRT)
The NHS Board discussed the operational, financial and workforce impact in relation to Access and Capacity issues and Delayed Discharges, the priority areas for focussed discussion at the Performance and Resources Committee meeting and the NHS Board’s Development Session scheduled for October 2012. The need for a consistent approach to performance management reporting within NHS Forth Valley and a whole system approach was also highlighted. The Chairman highlighted the importance of the Board Development Session Scheduled for October to provide an opportunity to reflect on the achievements to date, current actions being taken and to provide an opportunity to re-affirm NHS Forth Valley priorities for the next 12 months.
After detailed discussion, the NHS Board noted:
• the key items of information detailed within the Chief Executive’s Summary • the illustration of EPQ Priorities in Forth Valley within the Strategic Plan 1 • the main areas highlighted in the Balanced Scorecard and Performance Summary –
Appendix 2 • the Corporate Risks Summary the National Healthcare Associated Infection Reporting
Template (HAIRT)

4
5.2 Finance Report for the period ended June 2012
The NHS Board considered a paper “Finance Report for the period ended June 2012” presented by Mrs Fiona Ramsay, Director of Finance and Planning.
Mrs Ramsay advised that the NHS Board was reporting an overspend of £0.463m to the
end of June 2012 with a balanced outturn projected for 2012/2013 and that a detailed report would be submitted to the Performance and Resources Committee on 3 August 2012.
The financial pressures and associated risks with Acute Services and Waiting Times and
the plans in place to ensure the delivery of a balanced position by the 31 March 2013 were highlighted.
Mrs Ramsay reported on the increase in access costs, workforce turnover levels, current
level of spend on bank and agency staff, skill mix changes in the nursing workforce in emergency care, ambulatory care and community hospitals which required action to ensure financial balance. The associated risk to achieve financial balance was projected to be £3.5m.
Mrs Ramsay further reported on a reduction in prescribing unit costs and the additional capital of £125,000 received for work associated with the community hospitals. Mrs Ramsay advised that capital receipts from property sales would be used to reduce NHS Forth Valley’s repayments to the Scottish Government Health Department. She highlighted that property sale proceeds may not achieve their valuation. The NHS Board discussed the extent of the financial challenge over the next five year, links to service redesign, the national work on integration of Adult Health and Social Services, and increasing partnership working locally and regionally whilst ensuring the quality of services and providing best value. In response to a question from Mr James King regarding further detail in relation to bank and agency spend, the Acute position and waiting times, Mrs Ramsay advised that this information would be made available to the Performance and Resources Committee on 3 August 2012. Mrs Ramsay reported that a routine Finance meeting with the Scottish Government Health Department on 6 September 2012.
The NHS Board noted:
• the revenue overspend of £0.463m to 30 June 2012 • that financial balance is projected for March 2014, that that there is some risk
associated with this given the early financial pressures seen across specific areas including medical agency costs and access delivery. This risk is projected to be £3.5m
• the actions required to ensure financial balance by minimising temporary workforce spend (medical in particular), implementation of agreed skill mix changes in nursing workforce, implementation of Access Sustainability Plan and continued focus on prescribing savings
• the balanced capital position projected

5
6. HOME AND AWAY: HIGHLIGHTING THE WORK OF OUR STAFF
Professor Mackenzie introduced Ms Boa and Dr Schulga and provided a brief background to accompany the presentations.
Staff from across NHS Forth Valley are involved in developing and delivering a wide range of health care initiatives across the world which benefit patients and staff oversees, including those in some of the most disadvantaged communities in the world and local staff and patients in Forth Valley. The NHS Board received a presentation “Forth Valley – Chinese Connections”, presented by Ms Sally Boa, Speech & Language Therapist
. Ms Boa highlighted the following as detailed in the presentation:-
• Background • Visit to Shenjing Hospital in Shenyang April 2010 • Purpose of the visit • Challenges • Goal Setting • Listening to the Patient • Outcomes from Initial Visit • Visit to Scotland September 2011 • Future Plans • Second Visit to China – November 2011 • Key Outcomes for Shenjing Hospital • Benefits for NHS Forth Valley
The NHS Board commented on the pace of change, the cultural differences and the comparative financial position. The NHS Board received a presentation “From Forth Valley to Zambezia September 2012/11”, presented by Dr John Schulga. Consultant Paediatrician.
Dr Schulga highlighted the following as detailed in the presentation:-
• Friends of Pebane • Population by Doctor by Province • Population by Nursing Staff by Province • Mozambique Facts • Paediatric Ward Upgrade • Train the Trainers Programme • Cape Wrath to Campbeltown Bike Ride 2012
The NHS Board commented on the management of risk and medical student training opportunities abroad. The NHS Board acknowledged the work that had been undertaken by Ms Boa and Dr Schulga and thanked them both for their detailed and informative presentations.

6
7. REPORTS FROM SUB COMMITTEES 7.1 Minute of Area Clinical Forum meeting held on 17 May 2012 The NHS Board considered the minute of the Area Clinical Forum meeting held on 17
May 2012. Professor Mackenzie highlighted the presentation on CEL 01 (2012), Promoting Health
Services: Action in Hospital Settings.
The NHS Board noted the minute of the Area Clinical Forum meeting held on 17 May 2012.
7.2 Minute of Audit Committee meeting held on 8 June 2012
The NHS Board considered the minute of the Audit Committee meeting held on 8 June 2012, presented by Mr James King
Mr King highlighted the following:-
• Internal Audit Review of Waiting Times Terms of Reference • Internal Audit Reports • External Audit Reports
The NHS Board noted the minute of the Audit Committee meeting held on 8 June 2012.
7.3 Minute of Endowment Committee meeting held on 8 June 2012
The NHS Board considered the minute of the Endowment Committee meeting held on 8 June 2012 presented by Mr James King. Mr King highlighted the following:-
• NHS Forth Valley Endowment Funds Annual Accounts
The NHS Board noted the minute of the Endowment Committee meeting held on 8 June 2012
7.4 Minute of Staff Governance Committee meeting held on 1 June 2012
The NHS Board considered the minute of the Staff Governance Committee meeting held
on 1 June 2012, presented by Mr Brendan Clark. Mr Clark highlighted the following:
• Investigation into Management Culture in NHS Lothian • Health and Safety • Attendance Management • Achievement of the national reduction in Senior Managers
The NHS Board noted the minute of the Staff Governance Committee meeting held on 1
June 2012

7
7.5 Minute of Falkirk Partnership Board meeting held on 6 July 2012
The NHS Board noted the minute of the Falkirk Partnership Board meeting held on 6 July 2012.
7.6 Minute of Performance and Resources Committee meeting held on 6 July 2012 The NHS Board considered the minute of the Performance and Resources Committee meeting held on 6 July 2012, presented by Dr Vicki Nash.
Dr Nash highlighted the following:-
• Management of Significant Adverse Events: NHS Ayrshire and Arran Report • Core Performance Report • Waiting Times update – including Cancer
The NHS Board noted the minute of the Performance and Resources Committee meeting held on 6 July 2012.
8. FIFE AND FORTH VALLEY RESEARCH ETHICS COMMITTEE ANNUAL REPORT The NHS Board considered a paper “Fife and Forth Valley Research Ethics Committee Annual
Report”, presented by Dr Iain Wallace, Medical Director. Dr Wallace reported that the Code of Corporate Governance required the Fife and Forth Valley
Research Ethics Committee to submit an annual report to the NHS Board. The NHS Board noted the Fife and Forth Valley Research Ethics Committee Annual Report. 9. NHS FORTH VALLEY RISK MANAGEMETN ANNUAL REPORT
The NHS Board considered a paper “NHS Forth Valley Risk Management Annual Report”, presented by Professor Fiona Mackenzie, Chief Executive.
Professor Mackenzie reported that the Risk Management Annual Report had been presented to
the NHS Forth Valley Audit Committee, which had the responsibility to evaluate the system of internal control and corporate governance. The report had then been submitted to Governance Committees for information.
She further reported that the Annual Report provided assurance to the NHS Board that there had been adequate management of risk throughout the financial year.
The NHS Board noted the Forth Valley Risk Management Annual Report. 10. FORTH VALLEY NHS BOARD SUB-COMMITTEE ANNUAL REPORTS 10.1 Annual Report of the Acute Services Committee The NHS Board noted the Annual Report of the Acute Services Committee 2011/12.
10.2 Annual Report of the Area Clinical Forum The NHS Board noted the Annual Report of the Area Clinical Forum 2011/12.

8
10.3 Annual Report of the Audit Committee The NHS Board noted the Annual Report of the Audit Committee 2011/12 10.4 Annual Report of the Endowment Committee
The NHS Board noted the Annual Report of the Endowment Committee 2011/12 10.5 Annual Report of the Clinical Governance Committee
The NHS Board noted the Annual Report of the Clinical Governance Committee 2011/12 10.6 Annual Report of the Falkirk Community Health Partnership Board
The NHS Board noted the Annual Report of the Falkirk Community Health Partnership
Board 2011/12 10.7 Annual Report of the Clackmannanshire Community Health Partnership Board
The NHS Board noted the Annual Report of the Clackmannanshire Community Health Partnership Board 2011/12
10.8 Annual Report of the Stirling Community Health Partnership Board The NHS Board noted the Annual Report of the Stirling Community Health Partnership
Board 2011/12
10.9 Annual Report of the Clackmannanshire & Stirling Community Health Partnership Board
The NHS Board noted the Annual Report of the Clackmannanshire & Stirling Community Health Partnership Board 2011/12
10.10 Annual Report of the Staff Governance Committee
The NHS Board noted the Annual Report of the Staff Governance Committee 2011/12
10.11 Annual Report of the Strategic Projects and Property Committee
The NHS Board noted the Annual Report of the Strategic Projects and Property Committee 2011/12.
10.12 Annual Report of the Performance and Resources Committee The NHS Board noted the Annual Report of the Performance and Resources Committee 2011/12
11 Any Other Competent Business There being no other competent business the Chairman closed the meeting at 11.25 am.

1
FORTH VALLEY NHS BOARD 25 September 2012 This report relates to Item 5.1 on the agenda
Executive Performance Report To end of August 2012
(Paper presented by Professor Fiona Mackenzie, Chief Executive)
For Noting

1
NHS Forth Valley
Board Executive Performance Report August 2012 Position

2
Contents Purpose of report
Page
3
Chief Executive’s Summary
3
Recommendations
6
Section 1 - Financial Position
7
Section 2 – Board Executive Performance Summary
Attached
Section 3 - Corporate Risk Summary
Attached
Section 4 - Healthcare Associated Infection Reporting Template (National Template )
Attached
Section 5 – Communications Update
Attached

3
1. PURPOSE OF REPORT The purpose of this Board Executive Performance Report (BEPR) remains to provide assurance to the NHS Board of the overall performance of NHS Forth Valley. Acknowledging more detailed consideration of performance taking place at the Performance and Resources Committee (P&RC), the format of this report continues to be reviewed and streamlined to ensure the Board is succinctly updated on key performance issues. This month the Finance Update has been included in the report. Key areas of performance are highlighted in the performance summary (Section 2) focussed around the Balanced Scorecard (BSC), quality improvement agenda, which includes national Health, Efficiency, Access and Treatment (HEAT) targets from the Local Delivery Plan. This report provides an update to end August 2012. 2. CHIEF EXECUTIVE’S SUMMARY Throughout the summer months NHS Forth Valley has continued to see high levels of emergency activity peaking at certain times which has resulted in ongoing capacity challenges. Work is underway to review the capacity and flow across the system led by Dr Iain Wallace. Staff continue to meet the day to day challenges even when recent surges have stretched the system. Over one weekend the Emergency Department received 10 patients from a major Road Traffic Collision, of which 5 required resuscitation and intensive care. A full emergency trauma team was sent to the scene. The following day saw a further 10 patients with suspected spinal injuries from the Glasgow to Edinburgh cycle and a number with minor injuries. At the same time staff had to manage a potential outbreak of whooping cough within the Emergency Department. Many staff from across the organisation, including staff from Public Health, Occupational Health, IT, Pharmacy and the GP Out-of-Hours service, worked throughout the weekend with colleagues from the Emergency Department to gather information and plan our response. The impact of this outbreak and the additional serious trauma placed great strain on the staffing resources within the Emergency Department. I have extended my thanks to all the staff within the department for providing additional support, assistance and cover during this difficult period. Annual Review The Annual Review took place on the 18th of September. This was a Non Ministerial review which was well attended by members of the public, our patient representatives and our staff. The day started with the Chairman and I meeting with a group of patients to learn from their positive and negative experiences of our services. Lunch was well supported by our partner agencies, members of the Area Clinical Forum and Area Partnership Forum. During lunch people had the opportunity to see over 30 posters celebrating successes and recent awards. The Chairman then led the formal meeting in the afternoon supported by Executive colleagues. He highlighted that this was an opportunity to showcase some of the good work underway in Forth Valley but to also highlight where we have challenges. The agenda was set by the Government and structured around the national outcomes. To ensure as interactive a session as possible there were four presentations threaded through the agenda at relevant points. These considered care in the neonatal unit and early years, patient experience in theatres, the Branching Out work in mental health and efficiencies in prescribing. The audience were encouraged to ask questions at the end of each agendas item which proved very worthwhile. Our success around health

4
improvement, HAI, patient safety and experience were all considered along with the ongoing challenge around waiting times, IVF, the context of our financial position and work to address delayed discharges. The focus around the integration of health and social care and the forthcoming Patient Rights Act were also discussed. Initial feedback from the Government representatives present has been extremely positive. We will receive an Annual Review letter with relevant Action Points as standard. The general view seemed to be that this format worked well. Stirling Care Village I am delighted to update the Board on progress with the care Village proposal. The Stirling Care Village Initial Agreement has been considered by the Health Directorate's Capital Investment Group (CIG). The CIG have recommended approval and Derek Feeley, Director General and NHS Scotland Chief Executive has accepted that recommendation and now requests we submit an Outline Business Case. NHS Forth Valley is expected to fully develop a masterplan for the Stirling Community Hospital site having regard to the wider provision of health and social care services in Stirling and, where appropriate, a wider Forth Valley context. The options appraisal undertaken as part of the OBC will also need to fully explore and confirm the commitment of Stirling Council to planned developments on the site. Given the innovative approach to develop an integrated healthcare model we are expected to work closely with the Scottish Government and Stirling Council to inform future policy development. Finance A financial summary is detailed within Section 1 of this report. NHS Forth Valley is reporting an overspend of £0.741m to the end of August 2012 (£0.543m to the end of July 2012). There has been some overall improvement in expenditure trend for July. As indicated in previous months Acute Services and Waiting Times remain the most significant financial pressures. Work is ongoing to seek a balanced position by the year end. Waiting Times The focus on waiting times continues with the P&RC having a very detailed discussion of the position. A number of challenges persist within inpatients and outpatients with regards to the number of patients waiting for treatment. Focussed work around key specialties continues acknowledging the 12 week Treatment Time Guarantee, which comes into effect in October. Dialogue is ongoing with the Scottish Government to agree additional funding requirements to achieve the target. Cancer waiting times have also been considered with an improving position noted. This remains a standing agenda item on the P&RC. Quality Improvement World Sepsis day The first ever World Sepsis Day took place on 13th September 2012. To coincide with this, NHS Forth Valley reported the considerable success in recognising and treating sepsis. Forth Valley Royal Hospital was one of more than 890 hospitals and organisations supporting World Sepsis Day. Early recognition and treatment of this condition is very important, as sepsis is one of the biggest treatable causes of death. In the UK it is estimated that 37,000 people per year die of sepsis (more than breast cancer, lung cancer or bowel cancer) and in the USA sepsis kills more people each year than heart attacks. As part of the wider Scottish Patient Safety Programme, staff are concentrating on several key areas using six basic interventions which are given to all patients with sepsis within one hour. These include oxygen if needed, starting intravenous antibiotics through a drip, checking two simple blood tests and monitoring the patients urine output. Staff have found

5
that the best way to deliver what is known as the ‘sepsis 6 care bundle' is for a nurse and doctor to work together and use a sticker system in the medical notes. This details the times that the interventions are delivered within the hour after sepsis is identified. Crucial to the success is the contribution of members of the Patient Public Partnership. With the ability to view problems from a patient and relative perspective, they plan to develop information leaflets for patients being discharged on antibiotics and create posters to increase awareness of sepsis amongst patients and visitors. For more information on sepsis day go to www.world-sepsis-day.org Awards / Conferences / Interest President of the Royal College of Surgeons Edinburgh I am pleased to report that Mr Ian Ritchie, Orthopaedic Consultant in Forth Valley, has been elected by the fellows and members of the Royal College of Surgeons Edinburgh as the next the President of the College. He has been the Vice President since 2009 and demits this position to become President on the 16th November. Ian has been a Consultant in Forth Valley for more that 20 years. IHM Conference The Institute of Health Service Management (IHM) Scotland’s Annual Conference is taking place on 2nd & 3rd October 2012 in the Beardmore Hotel, Clydebank, in co-sponsorship with the Scottish NHS Board Chairs Group. This year’s theme is “Improving Leadership – Improving Lives”. The event will focus on integration and innovation and what these will mean for managers, for patients, for clinical leaders and for the wider leadership agenda necessary to deliver the benefits, all of which will be reflected in a range of plenary and workshop sessions. Derek Feeley, Director General and NHS Scotland Chief Executive, and Alasdair McIntosh, Head of Public Bodies and Public Service Reform at the Scottish Government will give a key note address to the Conference. An external keynote speaker and two stroke patients will inspire delegates and address the leadership challenge. The Conference also offers professional learning and development and networking opportunities to be gained. eHealth Awards 2012 The Information Communication and Technology team has been shortlisted for the Best NHS Scotland IT Service Delivery Team at the eHealth Awards 2012. The entry was for the Migration to the New Hospital Project. The awards ceremony takes place on the 20th September. Buggy Groups A scheme in the Falkirk area to encourage new mums to get fit has been so successful that it has just received a Physical Activity and Health Alliance award (PAHA) from NHS Health Scotland. Every year a number of awards are made to recognise outstanding efforts to improve health. Supported by Step Forth and Paths For All, hundreds of mothers have been pushing babies in buggies on organised walks in the company of an NHS Forth Valley Health Visitor. Not only has this given them the time to chat to each other, but it also provides an opportunity to seek health advice. The project began in the Bonnybridge area and was soon extended to other towns and villages. The programme has helped reduce feelings of depression amongst new mums who often feel isolated and overwhelmed by the responsibility and challenges of looking after their new arrival. The success of the scheme has received recognition nationally through professional journals and presentations as an example of good practice in health care.

6
3. RECOMMENDATIONS The Board is asked to note: The key items of information detailed within the Chief Executive’s Summary of this
report Section 1 Financial Summary The main areas highlighted in the Balanced Scorecard and Performance Summary -
Section 2 The Corporate Risks Summary - Section 3 The National Healthcare Associated Infection Reporting Template (HAIRT) -Section 4 Communications Update – Section 5 Author of Paper Name Designation Elaine Vanhegan Head of Performance
Approved By Name Designation Fiona Mackenzie
Chief Executive
September 2012

7
SECTION 1 - FINANCIAL SUMMARY
This report provides a summary of the financial position for NHS Forth Valley as at 31st
August 2012.
There is a statutory requirement for NHS Boards to ensure expenditure is within the Revenue Resource Limit (RRL) and Capital Resource Limit (CRL) set by the Scottish Government Health and Social Care Department (SGHSCD). The Table below provides a summary of the out-turn position:
Annual Actual Actual Budget Overspend / Overspend / Plan (Underspend) (Underspend) to 31/07/2012 to 31/08/2012
£m £m £m Resources Revenue Resource Allocation Core 466.288 0.000 0.000 Revenue Resource Allocation Non Core 0.000 0.000 0.000 Anticipated Resource Allocations 13.806 0.000 0.000 Income - other Scottish Boards 7.166 (0.037) (0.039) Income - Junior Doctors (NES) 6.319 0.000 0.000 Income - Miscellaneous 7.046 0.000 0.000 Total Resources 500.625 (0.037) (0.039) Expenditure Plan Corporate and External Boards 96.629 0.271 0.318 Acute Services 170.839 1.551 2.029 Waiting Times 2.209 0.613 0.769 CHP, Prescribing and Other Areas 221.091 0.151 0.186 Committed Balances / Contingency 9.857 (2.080) (2.600) Total Expenditure 500.625 0.506 0.702 Total Net Revenue Out-turn 0.543 0.741 Net Capital Out-turn 0.000 0.000 NHS Forth Valley is reporting an overspend of £0.741m to the end of August 2012 (£0.543m to the end of July 2012). There has been some overall improvement in expenditure trend for July however the majority of the in-month movement is due to the phased release of the Committed Balances / Contingency budget, which includes savings not yet distributed. As indicated in previous months Acute Services and Waiting Times remain the most significant financial pressures. Work is ongoing to seek a balanced position by the year end. This links to the current work in capacity and flow where costs are not budgeted for are currently being incurred on staffing additional capacity. The main financial risks which could increase overspends remain access costs and workforce turnover to deliver savings. There are specific financial pressures for delivery of Access Targets and Guarantees which are beyond those in spend to date. These are currently being finalised and are subject to discussion with SGHSCD. The current level of spend on bank and agency staff requires to be reduced and skill mix changes in the nursing workforce in emergency care, ambulatory care and Community Hospitals must be actioned in forthcoming months in order to ensure financial balance is achieved.

8
It is also vital that focus continues on the delivery of recurrent savings plans and that detailed action plans are in place to support them. The focus of this work is on prescribing savings and procurement areas with specific work in progress regarding management and administration linked to the ongoing management review. Options for future savings plans beyond 2012/13 are also being progressed for ensuring longer term financial balance, however this remains challenging. A balanced outturn position remains projected for 2012/13 although this is predicated on current cost pressures being brought back into line with budget, and financial support from SGHSCD this year to assist delivery of Access Targets and Guarantees .

1
SECTION 2 - BOARD EXECUTIVE PERFORMANCE SUMMARY – BALANCED SCORECARD Report Format Review of performance management and reporting at the various levels throughout the organisation continues to be a focus. As previously noted the format of this Board Executive Performance Summary has been streamlined to focus on key issues. All aspects within the Balanced Scorecard (BSC) are now considered in detail at the Performance Resources Committee (P&RC). The issues within this report derive from particular areas of note within the BSC and/or major points considered by the P&RC. Balanced Scorecard Work continues to develop the BSC to provide a broader range of measures and build upon the qualitative and quantitative data which will enable and support quality improvement and assurance. The local focus remains across the six dimensions of quality with a balanced approach to measurement. This is reflected in the on-going development of a strategic dashboard and the refocusing of the Board Executive Performance Report.
• The following templates update the position against locally developed quality indicators and HEAT targets
Format
• Progress symbols are noted as:
Improvement in period
Position maintained
Deterioration in period
• Where trajectories have been agreed, this will be reported as red, amber or green
R
A
G On track
Minor deviation from trajectory <5%
Off trajectory >5%
• The narrative will provide contextual information and support

2

3
Performance Summary
NHS Forth Valley continues to deliver strong performance overall. Key highlights are noted below against the balanced scorecard (BSC).
EQUITABLE SAFE Context Most areas under the ‘Equitable’ heading within the BSC are performing well. Recently confirmed Child Healthy Weight intervention figures highlight that NHS Forth Valley is well on track to exceed the Scottish Government target of 883 completions over three years. In 2011/12 programmes were delivered to over 1784 children. Of the participating children, 422 were found to be within the relevant weight range and completed the intervention giving a total of 422 ‘completions’. These successes were highlighted at the Annual Review held on 18th
Context It is positive to note that areas under the ‘Safety’ heading remain at green in the BSC with the exception of SABs. The Amber SABs position causes a degree of challenge with a fluctuating position. Following high level national discussions involving the Director of Public Health the measure will change for this target with a shift from a rate per 1000 acute occupied bed days to a rate per 1000 occupied bed days. This shift should favour NHS Forth Valley.
September.
Child Healthy Weight Staphylococcus Aureus Bacteraemia
Target: 883 Improved position
422 @ March 2012 ↑
Target: 0.26 Position behind target
0.4 @ August 2012 ↓
• HEAT Target to achieve 883 Child Healthy
Weight interventions over the 3 year period ending March 2014
• Interventions are delivered through the two linked mechanisms of Max in the Middle and Max in the Class
• Interventions run from September to December and January to March and are recorded on the Child Health Surveillance System
• To be regarded as a ‘qualifying intervention’ the participant must have been weighed and measured before and after the intervention, be found to be significantly overweight and have completed the full intervention
• Activity to March 2012 highlights that NHS Forth Valley is ahead of trajectory and on track to achieve the target
• The in position for August is 0.4 against a
trajectory of 0.32 • The 12 month rolling position for NHS Forth valley
is 0.42 • The Scotland position for quarter ending March
2012 is 0.31 against a plan of 0.30

4
EFFICIENT
Context There remain a small number of areas under the ‘Efficiency’ heading posing challenge. Some of these relate to overall capacity which is being considered a key focus within the EPQ Prioritisation Plan. Of note below is the red position in respect of theatre ‘under runs’ and the deterioration of the position for ‘late starts’. As noted below this is being reviewed under the capacity and flow heading. Absence management remains at red despite continued and significant effort and activity around the agenda.
Reduction in theatre under runs Theatre late starts Target: 5% or less
Deteriorated position
14.1% @ June 2012 ↓
Target: 3% or less
Deteriorated position
3.7% @ June 2012 ↓
• An under run is when a theatre session is finished
early by 45 minutes or more with the number of theatre list under run hours as a percentage of planned list hours providing the measure
• This target continues to provide challenges with the BSC position remaining red. The overall target of 5% was not met in March with the position for June 14.1%. Work continues to review the situation linking to the wider activity reviewing flow and capacity across the system.
• A late start is recorded when theatre commences
15 minutes or more after the expected start time with the number of hours lost to late starts as a percentage of planned list hours providing the measure.
• The target has moved from a Green to an Amber position in the BSC. The December 2011 target of 3% was met in May however a position of 3.7% was recorded in June 2012.
Attendance Management Target: 4% Deteriorated
position 5.25% @ July 2012 ↓
Sickness Absence(% Hours Lost over total
hours available)
0%
2%
4%
6%
8%
Jul-11 Oct-11 Jan-12 Apr-12 Jul-12
FV TrajectoryScotland
• The March 2009 target of 4% was not achieved • Focus on absence management continues as
challenge remains in achieving this target • The July 2012 position of 5.25% is an increase of
0.34% against the June 2012 position of 4.91% • All services with the exception of Acute (-0.34%)
showed increased absence in the month; CHP's, (0.83%), Corporate (1.12%) and Forth Valley Facilities (1.15%).

5
TIMELY Context Performance under the ‘Timely’ heading is variable. There remain challenges in the area of 18 week RTT and A&E 4 hour waits which were both highlighted at the Annual Review. The cancer position was previously considered with an improving in month position reported below. Publication of quarterly cancer figures April - June 2012 is expected on 25th September 2012
18 Week RTT Performance 4 Hour A&E Wait Target: 90% Deteriorated
position 85.2% @ July 2012 ↓
Target: 98% Deteriorated position
94.5% @ August 2012 ↓
• In July 2012, 85.2% of patients were treated
within 18 weeks. This is a deterioration against the 90% target achievement over previous months
• The Scotland position at July 2012 was 91.7% • Challenges remain within outpatient
ophthalmology, rheumatology and respiratory, along with orthopaedic, general surgery and ophthalmology inpatients and day cases, as targets move to the 12 week Treatment Time Guarantee
• Forth Valley continues dialogue with the Scottish Government to seek additional funding to meet the guarantee
• In August 2012 the position was 94.5% of patients
waited less than 4 hours between arrival at the A&E unit and admission, discharge or transfer.
• There remain fluctuations in activity on a day to day basis and, as previously highlighted to the Board, is a symptom of wider capacity and flow challenges across the system, as noted in the Executive Summary. These issues were highlighted at the Annual Review.
• Focused work continues to address issues in respect of breaches.
• It should be noted that NHS Forth Valley reported no 12 hour breaches.
Cancer Target: 95% Static position
in month 91.2% @ July 2012 ↓
Target: 95%
Improved in month position
95.9% @ July 2012 ↑
• Quarterly statistics at March 2012 highlight that
91.8% of patients were seen within 62 days • This is below the 95% target and the Scotland
position of 94.8% • The monthly position for July 2012 is 91.2% with
the BSC remaining Amber • Supporting action plans are in place to reflect
recent challenges within colorectal and urology cancer services to ensure target delivery
• Quarterly statistics at March 2012 show that 95.6%
of patients were treated within 31 days against a 95% target with a Scotland position at March 2012 of 97.9%
• In July 2012, 95.9% of patients were treated within 31 days with the BSC highlighted as Green.

6
Effective Context The ‘Effective’ heading continues to show a variation in performance. There are an increasing number of delayed discharges over 4 weeks against a reducing trajectory with an increasing number of bed days lost in line with this. This remains a key area of focus for NHS Forth Valley and partner organisations. Use of antibacterials in primary care is highlighted as red in the BSC. It should be noted that this is an annual data collection and work is underway to understand the position.
Delayed Discharge
Target: 0 Deteriorating position
30 @ August 2012 ↓
Target: Reduction
Deteriorating position
1816 @ July 2012 ↓
Delayed Discharge Performance at Census Against 28 Day Target
0
3
6
9
12
15
18
21
24
27
30
Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13
Delay
ed >
28 D
ays
Trajectory Stirling Falkirk Clacks Forth Valley • The total number of delayed discharges over 4
weeks at the April census was zero. This was against a trajectory point of 14
• The BSC position for August is Red with 19 delays over 4 weeks for NHS Forth Valley. This is against a trajectory point of 10. In addition there were 2 patients from Out of Area.
• Breakdown by Local Authority is Clacks – 1, Falkirk – 26, Stirling – 1
• Weekly monitoring is on-going reviewing the over 6 week, over 4 week and over 2 week position
• The BSC position has remained Red with the total
bed days occupied by delayed discharges increasing from 1431 in July to 1816 in August 2012
• Weekly meetings which focus on individual patient needs continues to be critical in ensuring ongoing improvement.
• Due to a number of reasons there are limited vacancies across the care home sector adding to pressure within the system.
• The Falkirk Partnership continues to experience particular challenges, with the Partnership Board considering this issue on the 21st September
Antibacterial use in primary care Target: ≤ 5% Position
deteriorated 10% for 2011/12 ↓
NHS Scotland use of antibacterials in primary care by NHS Board, percentage seasonal quinolones 2011/12 (Winter v Summer) • Within the BSC this annual figure has changed
from Green to Red • NHS Forth Valley previously met this target with
the position in 2009/10 over -5% and 2010/11 -3.9%
• Further work is planned to understand why there has been a deviation this year
*The quinolones are a family of synthetic broad-spectrum antibiotics. The term quinolone(s) refers to potent synthetic chemotherapeutic antibacterials

7
PERSON CENTRED
Context Under the ‘Person centred’ heading the complaints position, although improved, remains at red and is proving challenging. This target is around responses within 20 days and significant activity is underway to address the position. Patient experience survey results were published in August with the overall result an improvement on the previous year. The survey was sent between January and February 2012 to 1,500 people who stayed overnight in an NHS Forth Valley hospital between the beginning of October 2010 and September 2011 with 690 returned. The survey asked questions about people’s experiences of Admission, Hospital Ward and Environment, Care and Treatment, Staff, Leaving hospital care after leaving hospital and Medicines. There are specific areas where NHS Forth Valley fell below the Scottish average and work will be taken forward to address these issues. This was highlighted at the Annual Review. The survey was commissioned by NHS Forth Valley as part of Scotland's Patient Experience Programme “Better Together” Patient Experience Complaints Target: Improvement
Improved position
76.3 @ 2012 ↑
Target: 70% Improved position
55.56% @ June 2012 ↑
2012 2011 2010 Forth Valley 76.3 74.5 74.2 Scotland 81.7 78.1 78.3
• NHS Forth Valley Patient Experience co-ordinator
continues to support individual wards and departments in undertaking patient experience surveys. This is ongoing work, with all acute inpatient areas at Forth Valley Royal Hospital now online
• Work has now been completed in respect of building a generic Patient Experience questionnaire aligned with the Better Together national survey questionnaire into the ‘Transforming and Improving Care’ database. Wards are beginning to receive graphic representation of results for use as feedback at ward level
• Work to address Discharge Arrangements and Care and Treatment issues.
Complaints 20 day response rate
0.00
20.00
40.00
60.00
80.00
100.00
120.00
Apr-11
May-11
Jun-11
Jul-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
Jan-12
Feb-12
Mar-12
Apr-12
May-12
Jun-12
Acute CHP Total Target
• The above graph highlights that NHS Forth Valley’s year to date cumulative position is 55.56% against a 70% target
• CHP position is 50%; Acute position is 56.10% • There are a number of factors being addressed
which are impacting on/causing the dip in response times
• Prison Service complaints are included within the overall CHP figures. These are investigated and responded to by prison staff unless specifically requested otherwise by the complainant
• Focussed work is underway led by the Director of Nursing and General Managers to address the position

1
SECTION 3 - CORPORATE RISKS
Corporate Risks continue to be reviewed on a monthly basis, in addition, and in line with the Risk Register Guidance, a substantial review of the Corporate Risk Register (CRR) is carried out on a quarterly basis by Risk Owners. An extensive review was carried out in August 2012 with appropriate updates and actions taken. The next review is expected in November 2012.
Corporate Risks Summary
Significant risks are detailed below.
Finance Risk and Efficiency Savings Finance risk for 2012/13 remains high. All efforts are focussed on ensuring financial balance with risks updated monthly and reported through all governance processes. Robust monitoring of performance at departmental meetings and areas of overspend in acute reviewed and actions identified. Most significant financial issue is delivery of access guarantee and targets with implications currently being quantified. Inability to meet waiting time targets There are a number of service issues in respect of capacity and workforce causing difficulty in respect of delivery against the access targets. Sustainability plans by specialty prepared and supported by Strategic Management Team. In response to Scottish Government guidance, draft access policy for consideration at August SMT. Planning and scoping work for 12 weeks Treatment Time Guarantee underway including service planning with units. Clinical Risk Provision of healthcare and risk assessment/management for restricted patients who are managed via Health MAPPA (Multi-Agency Public Protection Arrangements) and those for sex offenders in the community managed via non-health MAPPA. Current control measures including access to relevant policies, systems and procedures within mental health services and access to training in MAPPA awareness and risk management are in place however the risk is highlighted in the CRR as a service gap exists to meet full requirements. Safe care risk reviewed to reflect emphasis on transition to community hospital model. Delayed discharges To meet and sustain the delayed discharge zero position in partnership against the current financial pressure and care home capacity continues to pose challenges. A focus on reducing this target from zero delays over 6 to zero delays over 4 weeks, throughout 2012/13 (Local Delivery Plan 2012/13), places additional pressure on this work. A range of actions are in place to reduce delays for patient discharges including Joint Improvement Team working with local authority partners and health.

SECTION 4 – HEALTHCARE ASSOCIATED INFECTION REPORTING TEMPLATE (HAIRT)
Section 1 – Board Wide Issues
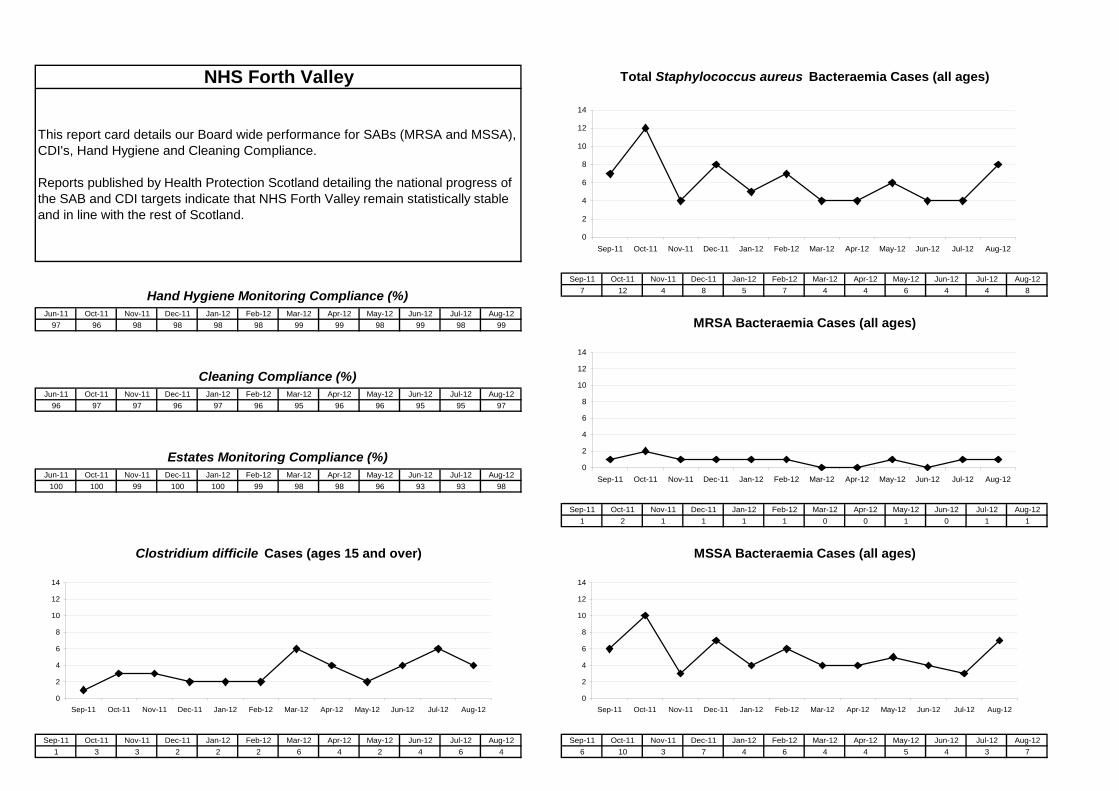
Key Healthcare Associated Infection Headlines for August 2012
• HEAT Targets
o Clostridium difficile infections (CDI) remain stable across NHS Forth Valley and remains one of the lowest rates in Scotland. There was one case this month that was hospital acquired.
o Staphylococcus aureus bacteraemias (SABs) remain statistically stable across NHS Forth Valley. Two cases this month were hospital acquired.
Staphylococcus aureus (including MRSA)
A new HEAT target has been set for 2012/13 that all Health Boards across Scotland achieve a SAB rate of 0.26 per 1000 AOBDs. Our rate between April 2011 and March 2012 was 0.41 per 1000 AOBDs. Following epidemiological analysis of our data, we are now working with various stakeholders to look at areas such as wound management and the appropriate use of invasive devices to help further reduce our numbers. Over the last 12 months, our average number of SAB cases is 6 per month. In August 2012, the number of patients with a SAB infection was 8. Two cases were hospital attributed.
This section of the HAIRT covers Board wide infection prevention and control activity and actions. For reports on individual hospitals, please refer to the ‘Healthcare Associated Infection Report Cards’ in Section 2. A report card summarising Board-wide statistics can be found at the end of section 1
Staphylococcus aureus is an organism which is responsible for a large number of healthcare associated infections, although it can also cause infections in people who have not had any recent contact with the healthcare system. The most common form of this is Meticillin Sensitive Staphylococcus Aureus (MSSA), but the more well known is MRSA (Meticillin Resistant Staphylococcus Aureus), which is a specific type of the organism which is resistant to certain antibiotics and is therefore more difficult to treat. More information on these organisms can be found at:
Staphylococcus aureus : http://www.nhsinform.co.uk/Health-Library/Articles/S/staphylococcal-infections/introduction
MRSA: http://www.nhsinform.co.uk/Health-Library/Articles/M/mrsa/introduction
NHS Boards carry out surveillance of Staphylococcus aureus blood stream infections, known as bacteraemias. These are a serious form of infection and there is a national target to reduce them. The number of patients with MSSA and MRSA bacteraemias for the Board can be found at the end of section 1 and for each hospital in section 2. Information on the national surveillance programme for Staphylococcus aureus bacteraemias can be found at: http://www.hps.scot.nhs.uk/haiic/sshaip/publicationsdetail.aspx?id=30248

Clostridium difficile
A new HEAT target has been set for 2012/13 that all Health Boards across Scotland achieve a CDI rate of 0.39 per 1000 OCBDs. Our rate between April 2011 and March 2012 was 0.12 per 1000 OCBDs. Over the last 12 months, we have managed to reduce the number of CDIs to an average of 3 per month. In August 2012 there were 4 cases of CDI reported. One case was hospital acquired.
Clostridium difficile is an organism which is responsible for a large number of healthcare associated infections, although it can also cause infections in people who have not had any recent contact with the healthcare system. More information can be found at:
http://www.nhsinform.co.uk/Health-Library/Articles/C/clostridium-difficile/introduction
NHS Boards carry out surveillance of Clostridium difficile infections (CDI), and there is a national target to reduce these. The number of patients with CDI for the Board can be found at the end of section 1 and for each hospital in section 2. Information on the national surveillance programme for Clostridium difficile infections can be found at:
http://www.hps.scot.nhs.uk/haiic/sshaip/clostridiumdifficile.aspx?subjectid=79

Hand Hygiene
This month, the HPS national audit report for July gave NHS Forth Valley top marks with 96% compliance with hand hygiene opportunities. Cleaning and the Healthcare Environment
Outbreaks
Good hand hygiene by staff, patients and visitors is a key way to prevent the spread of infections. More information on the importance of good hand hygiene can be found at:
http://www.washyourhandsofthem.com/
NHS Boards monitor hand hygiene and ensure a zero tolerance approach to non compliance. The hand hygiene compliance score for the Board can be found at the end of section 1 and for each hospital in section 2. Information on national hand hygiene monitoring can be found at: http://www.hps.scot.nhs.uk/haiic/ic/nationalhandhygienecampaign.aspx
Keeping the healthcare environment clean is essential to prevent the spread of infections. NHS Boards monitor the cleanliness of hospitals and there is a national target to maintain compliance with standards above 90%. The cleaning compliance score for the Board can be found at the end of section 1 and for each hospital in section 2. Information on national cleanliness compliance monitoring can be found at:
http://www.hfs.scot.nhs.uk/online-services/publications/hai/
Healthcare environment standards are also independently inspected by the Healthcare Environment Inspectorate. More details can be found at: http://www.nhshealthquality.org/nhsqis/6710.140.1366.html
During the months of July and August 2012, there were no outbreaks of norovirus or from any other pathogenic organism reported for this period. A weekly update from Health Protection Scotland can be found at: http:/www.hps.scot.nhs.uk.

Other HAI Related Activity
Scottish Patient Safety Programme A number of areas in the programme focus specifically on reducing healthcare associated infection in theatres, general wards and in critical care units and work is currently underway in pilot areas within Forth Valley Royal Hospital. The work of the SPSP is integrated with all of the other actions described in this report that are being taken forward in NHS Forth Valley to reduce HAI. Three examples of the work to reduce healthcare associated infection are: - preventing ventilator associated pneumonia and catheter related blood stream infections in critical care and increasing hand hygiene in wards. Public and Patient Involvement Forth Valley is fortunate to have a committed patient and public involvement through the Patient Public Forums in the 3 Community Health Partnerships and the Patient Public Panel who are actively engaged in improving healthcare services including preventing HAI and monitoring domestic services. Patient Panel members are working collaboratively with the Infection Control team performing HAI monthly compliance audits across Forth Valley Royal Hospital and the community hospitals. MRSA Screening Since January 2010 NHS Forth Valley has been successfully screening all elective admissions and specific emergency admissions for MRSA. This is a government initiative to help reduce the incidence of MRSA cross infection throughout NHS Scotland. Scottish Government published the Pathfinder Report detailing the findings of the three boards which piloted the MRSA screening programme prior to the rest of NHS Scotland; from this report, amendments to the screening rationale have been changed and patients are now screened following a Clinical Risk Assessment (CRA). Risk Management The risks around managing HAI are considered at every clinical level and included in Risk Registers held in departments. HAI also features in two different sections of the Corporate Risk Register (CRR). The CRR is reviewed every month to make sure all actions to manage any risks are being taken. Primary care Primary care covers a wide area, and includes community hospitals, dental practices and GP practices across NHS Forth Valley. The Infection Control Team provides a full time 5 day service (out of hours covered by the Duty Microbiologist) to Primary care; the service includes advice, support, audit and education and training. This service is crucial; reducing the incidence and number of patients with a HAI in Primary care, can help reduce the HAI incidence in the acute hospitals. For instance strict antimicrobial management in the community can reduce patients developing conditions such as C.difficile Infections (CDI) or even the potential development of multi resistant bacteria which could be subsequently introduced to the hospital environment.
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-127 12 4 8 5 7 4 4 6 4 4 8
Jun-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-1297 96 98 98 98 98 99 99 98 99 98 99
Jun-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-1296 97 97 96 97 96 95 96 96 95 95 97
Jun-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12100 100 99 100 100 99 98 98 96 93 93 98
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-121 2 1 1 1 1 0 0 1 0 1 1
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-121 3 3 2 2 2 6 4 2 4 6 4 6 10 3 7 4 6 4 4 5 4 3 7
NHS Forth Valley
MSSA Bacteraemia Cases (all ages)
Total Staphylococcus aureus Bacteraemia Cases (all ages)
MRSA Bacteraemia Cases (all ages)
Clostridium difficile Cases (ages 15 and over)
Hand Hygiene Monitoring Compliance (%)
Cleaning Compliance (%)
Estates Monitoring Compliance (%)
This report card details our Board wide performance for SABs (MRSA and MSSA), CDI's, Hand Hygiene and Cleaning Compliance.
Reports published by Health Protection Scotland detailing the national progress of the SAB and CDI targets indicate that NHS Forth Valley remain statistically stable and in line with the rest of Scotland.
0
2
4
6
8
10
12
14
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
20
40
60
80
100
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
2
4
6
8
10
12
14
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
2
4
6
8
10
12
14
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
2
4
6
8
10
12
14
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12

0.20 0.17 0.15 0.12 0.120.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39
0.44 0.41 0.45 0.46 0.410.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26Target
Actual PerformanceTarget
Actual Performance
Apr 10 -Mar 11
Jul 10 -Jun 11
Jan 11 -Dec 11
Oct 10 -Sept 11
Jul 10 -Jun 11
Oct 10 -Sept 11
Jan 12 -Dec 12
Oct 11 -Sept 12
Jul 11 -Jun 12
Apr 11 -Mar 12
Jan 12 -Dec 12
Apr 12 -Mar 13
Quarterly rolling year Clostridium difficile Infection Cases per 1000 total occupied bed days for HEAT Target Measurement
Quarterly rolling year Staphylococcus aureus Bacteraemia Rates per 1000 Acute Occupied Bed Days for HEAT Target Measurement
Apr 10 -Mar 11
Jan 11 -Dec 11
Apr 11 -Mar 12
Jul 11 -Jun 12
Oct 11 -Sept 12
Apr 12 -Mar 13
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
0.5
Apr 10 -Mar 11
Jul 10 -Jun 11
Oct 10 -Sept 11
Jan 11 -Dec 11
Apr 11 -Mar 12
Jul 11 -Jun 12
Oct 11 -Sept 12
Jan 12 -Dec 12
Apr 12 -Mar 13
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
Apr 10 -Mar 11
Jul 10 -Jun 11
Oct 10 -Sept 11
Jan 11 -Dec 11
Apr 11 -Mar 12
Jul 11 -Jun 12
Oct 11 -Sept 12
Jan 12 -Dec 12
Apr 12 -Mar 13

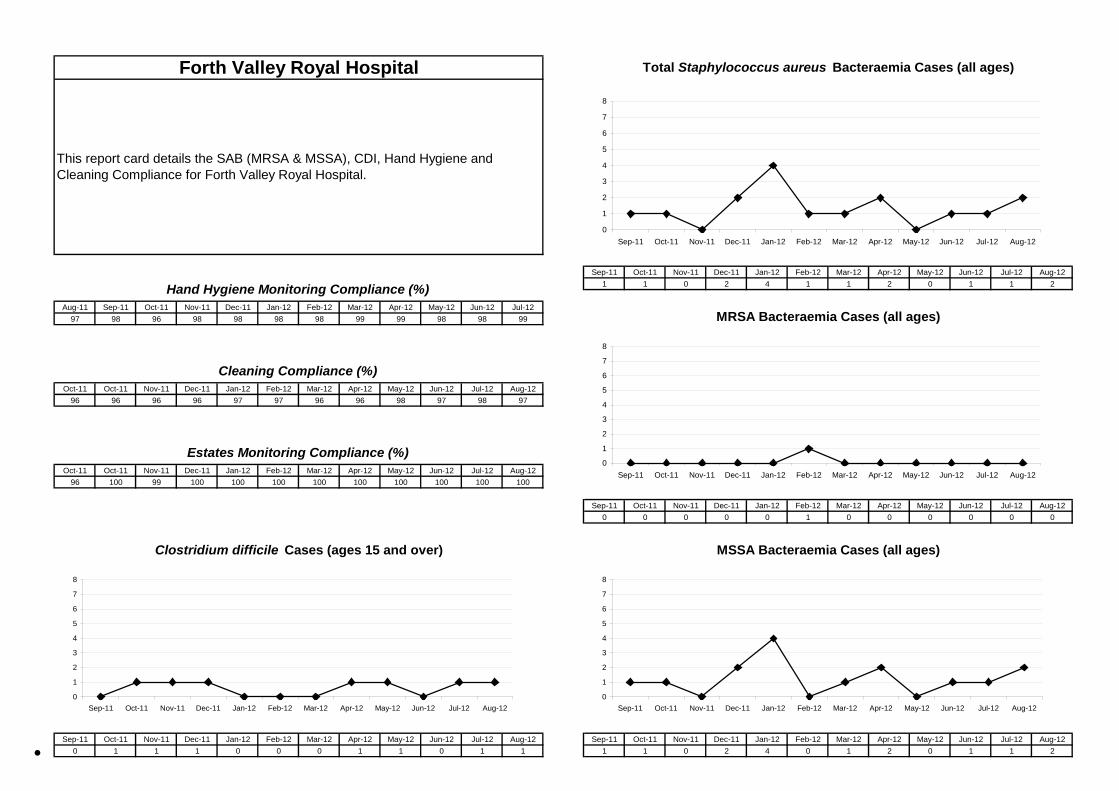
Healthcare Associated Infection Reporting Template (HAIRT) Section 2 – Healthcare Associated Infection Report Cards
The following section is a series of ‘Report Cards’ that provide information, for each acute hospital and key community hospitals in the Board, on the number of cases of Staphylococcus aureus blood stream infections (also broken down into MSSA and MRSA) and Clostridium difficile infections, as well as hand hygiene and cleaning compliance. In addition, there is a single report card which covers all community hospitals which do not have individual cards, and a report which covers infections identified as having been contracted from outwith hospital. The information in the report cards is provisional local data, and may differ from the national surveillance reports carried out by Health Protection Scotland and Health Facilities Scotland. The national reports are official statistics which undergo rigorous validation, which means final national figures may differ from those reported here. However, these reports aim to provide more detailed and up to date information on HAI activities at local level than is possible to provide through the national statistics.
Understanding the Report Cards – Infection Case Numbers
Clostridium difficile infections (CDI) and Staphylococcus aureus bacteraemia (SAB) cases are presented for each hospital, broken down by month. Staphylococcus aureus bacteraemia (SAB) cases are further broken down into Meticillin Sensitive Staphylococcus aureus (MSSA) and Meticillin Resistant Staphylococcus aureus (MRSA). Data are presented as both a graph and a table giving case numbers. More information on these organisms can be found on the NHS24 website:
Clostridium difficile : http://www.nhs24.com/content/default.asp?page=s5_4&articleID=2139§ionID=1
Staphylococcus aureus : http://www.nhs24.com/content/default.asp?page=s5_4&articleID=346
MRSA: http://www.nhs24.com/content/default.asp?page=s5_4&articleID=252§ionID=1
For each hospital the total number of cases for each month are those which have been reported as positive from a laboratory report on samples taken more than 48 hours after admission. For the purposes of these reports, positive samples taken from patients within
Understanding the Report Cards – Hand Hygiene Compliance
48 hours of admission will be considered to be confirmation that the infection was contracted prior to hospital admission and will be shown in the “out of hospital” report card.
Good hand hygiene is crucial for infection prevention and control. More information can be found from the Health Protection Scotland’s national hand hygiene campaign website: http://www.washyourhandsofthem.com/ Hospitals carry out regular audits of how well their staff are complying with hand hygiene. The first page of each hospital report card presents the percentage of hand hygiene compliance for all staff in both graph and table form.
Understanding the Report Cards – Cleaning Compliance
Hospitals strive to keep the care environment as clean as possible. This is monitored through cleaning compliance audits. More information on how hospitals carry out these audits can be found on the Health Facilities Scotland website: http://www.hfs.scot.nhs.uk/online-services/publications/hai/ The first page of each hospital Report Card gives the hospitals cleaning compliance percentage in both graph and table form.
Understanding the Report Cards – ‘Out of Hospital Infections’
Clostridium difficile infections and Staphylococcus aureus (including MRSA) bacteraemia cases are all associated with being treated in hospitals. However, this is not the only place a patient may contract an infection. This total will also include infection from community sources such as GP surgeries and care homes and sources not related to healthcare. The final Report Card report in this section covers ‘Out of Hospital Infections’ and reports on SAB and CDI cases reported to a Health Board which are not attributable to a hospital.
•
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-121 1 0 2 4 1 1 2 0 1 1 2
Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-1297 98 96 98 98 98 98 99 99 98 98 99
Oct-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-1296 96 96 96 97 97 96 96 98 97 98 97
Oct-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-1296 100 99 100 100 100 100 100 100 100 100 100
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120 0 0 0 0 1 0 0 0 0 0 0
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120 1 1 1 0 0 0 1 1 0 1 1 1 1 0 2 4 0 1 2 0 1 1 2
Forth Valley Royal Hospital
MSSA Bacteraemia Cases (all ages)
Total Staphylococcus aureus Bacteraemia Cases (all ages)
MRSA Bacteraemia Cases (all ages)
Clostridium difficile Cases (ages 15 and over)
Hand Hygiene Monitoring Compliance (%)
Cleaning Compliance (%)
Estates Monitoring Compliance (%)
This report card details the SAB (MRSA & MSSA), CDI, Hand Hygiene and Cleaning Compliance for Forth Valley Royal Hospital.
0
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
20
40
60
80
100
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
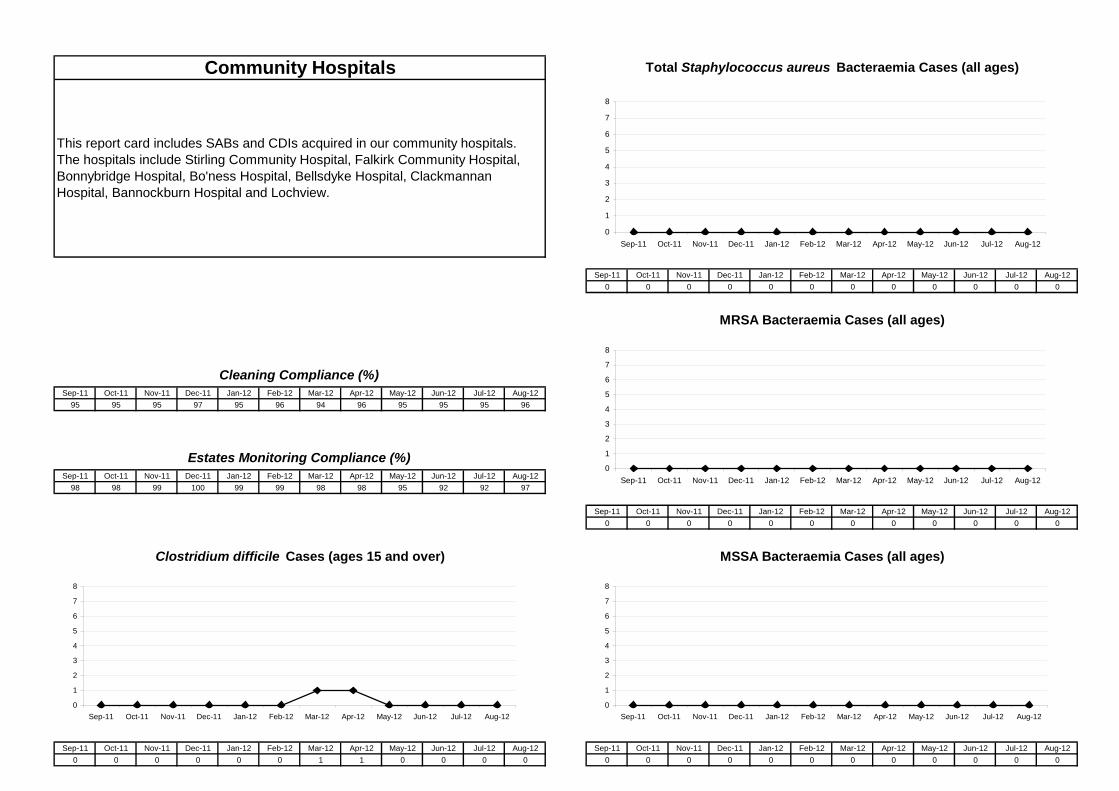
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120 0 0 0 0 0 0 0 0 0 0 0
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-1295 95 95 97 95 96 94 96 95 95 95 96
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-1298 98 99 100 99 99 98 98 95 92 92 97
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120 0 0 0 0 0 0 0 0 0 0 0
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120 0 0 0 0 0 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
MSSA Bacteraemia Cases (all ages)
Total Staphylococcus aureus Bacteraemia Cases (all ages)
MRSA Bacteraemia Cases (all ages)
Clostridium difficile Cases (ages 15 and over)
Cleaning Compliance (%)
Estates Monitoring Compliance (%)
This report card includes SABs and CDIs acquired in our community hospitals. The hospitals include Stirling Community Hospital, Falkirk Community Hospital, Bonnybridge Hospital, Bo'ness Hospital, Bellsdyke Hospital, Clackmannan Hospital, Bannockburn Hospital and Lochview.
Community Hospitals
0
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
20
40
60
80
100
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
1
2
3
4
5
6
7
8
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12

Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120 2 2 0 2 2 5 3 1 3 5 3
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-125 9 3 5 0 6 3 2 5 3 2 5 1 2 1 1 1 0 0 0 1 0 1 1
MSSA Bacteraemia Cases MRSA Bacteraemia Cases
This report card details all SAB and CDIs that were not acquired during their stay at hospital.
Out of Hospital Infections Clostridium difficile Infection Cases
0
2
4
6
8
10
12
14
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
2
4
6
8
10
12
14
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
2
4
6
8
10
12
14
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12

Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-124 4 2 3 0 6 2 1 2 3 2 2 1 1 1 0 1 0 0 0 1 0 1 0
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-121 5 1 2 0 0 0 1 3 0 0 2 0 1 0 1 0 0 0 0 0 0 0 1
Healthcare MRSA Bacteraemia Cases
ANNEX 1. Healthcare & Community acquired Infections
Community MRSA Bacteraemia CasesCommunity MSSA Bacteraemia Cases
Healthcare MSSA Bacteraemia Cases
In this annex, is the breakdown of the 'out of hospital' infections described on the previous page.
Healthcare acquired SABs are infections that can be associated and attributed from previous hospital admissions; this group is an area where the Infection Control team actively investigate and if it is suspected the infection has arisen from a previous hospital admission, it is treated as a hospital acquired SAB; although due to the strict HPS definitions of acquisition type it is classified as out of hospital.
Community acquired SABs are those that have not had any healthcare contact or intervention and as such are outwith our control to reduce these infections.
0
2
4
6
8
10
12
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
20
40
60
80
100
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-120
2
4
6
8
10
12
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
2
4
6
8
10
12
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12
0
2
4
6
8
10
12
Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12

SECTION 5 – COMMUNICATIONS UPDATE MAY – AUGUST 2012 Executive Summary The second quarter of 2012 continued to be a busy period for the Communications Department as the team dealt with a number of high profile issues. They also undertook a wide range of promotional activities to highlight service developments and changes across Forth Valley. The Department continued to proactively promote a wide range of initiatives and service developments at Forth Valley Royal Hospital. These included celebrating the hospital’s first anniversary in July 2012, highlighting the success of a new patient reminder system which is being used in a number of key specialties and the introduction of a new state-of-the-art data system designed to help reduce healthcare associated infections. A new electronic portering system, which is providing a faster and more streamlined service between the wards and departments, was promoted and a new bus service from Kincardine to Forth Valley Royal Hospital was launched in August 2012. Staff and patients took advantage of free haircuts on offer at a pop-up salon which was set up in the hospital for a week. Alba Brass also performed a concert in the atrium in September 2012. These were just two of a number of events which took place at the hospital over the last few months as part of the new NHS Forth Valley art strategy. Plans for the new Forth Valley Maggie’s Centre continued to progress following the announcement that NORD, a Glasgow-based organisation, had been selected as the architects for the new centre. Established in 2002, NORD are known for their unique buildings and for drawing their inspiration from social and cultural issues. Work continued with Forestry Commission Scotland with the launch of a woodland rehabilitation programme for cardiac patients at Forth Valley Royal Hospital. Taking place in the community woodlands immediately opposite the hospital grounds, the pilot programme will run for three hours each week over a six week period to help cardiac patients relax and slowly rebuild their strength in the outdoors. Up to 15 people will attend the programme which includes introductory tai chi, nature photography and willow sculpting, in addition to regular visits to the hospital’s cardiac department. The winning design was also announced for a new permanent loch-side viewing platform which will be built in the woodlands surrounding the hospital. Minister for Public Health, Michael Matheson MSP visited Slamannan Health Centre on 9th
August 2012 to launch NHS Forth Valley’s new Carers Resource Pack. It contains information which will assist GPs to identify carers, and direct them to practical and financial information and support. It also provides details about the importance of referring carers to services such as social services and their local carers centre. During the launch, the Minister met staff and members of the Slamannan Carers Group, who work with the health centre to raise awareness of carers’ issues.
Throughout the summer, NHS Forth Valley organised a wide range of activities and events to help celebrate the Olympics. Local torch bearer Dougie Gillespie from Larbert lit up the children’s faces when he visited the Children’s Ward at Forth Valley Royal Hospital and gave staff and patients the chance to hold the famous torch. A short video clip of the visit was produced which can be seen on the NHS Forth Valley website. The restaurant at Forth Valley Royal Hospital put on an Olympic themed menu and more than 150 members of the Healthy Hearts Club held their own ‘OlymPeak’ event at The Peak sports village in Stirling. During the day-long extravaganza they participated in a wide range of sports including badminton, basketball, cycling, football, table tennis and swimming. Over the last few months, the Communications Team has successfully promoted a wide range of new initiatives and service developments. These included a new scheme to give all pregnant women free vitamins, a new dedicated service to help pregnant women in the Falkirk area give up smoking. A new Therapeutic Day Support Services for residents in Stirling, provided by the Reach team in partnership with Stirling Council, was launched and the use of a pioneering light treatment therapy to help survivors of childhood sexual, physical and emotional abuse from across Scotland to overcome flashbacks and nightmares was also highlighted in local and national media.

A number of national health campaigns were supported throughout the period including the new Detect Breast Cancer Early campaign. A number of awards and achievements were also promoted including our sexual health services which were awarded the LGBT charter mark from LGBT Youth Scotland for providing excellent guidance and advice to young people. The Step Forth Group, which is a partnership between NHS Forth Valley and Falkirk Council, was awarded a coveted Physical Activity and Health Alliance (PAHA) award for the Falkirk buggy scheme which provides health advice and support to new mums during regular buggy walks.
The Summer Issues of Staff News and Community Health News were produced and distributed during this period and online versions were also available for staff and members of the public. During this period, 12 staff briefs were issued to ensure staff were updated on a wide range of local and national issues. During the period, the Communications Department responded to more than 130 media and out-of-hours enquires. We also issued 40 proactive press releases and 47 media statements. A total of 80 % of the coverage was either positive or neutral with only 20% negative. For further information and a detailed analysis of coverage please see appendix FOI Requests The table below details the number of FOI requests received to date and highlights how many met or exceeded the 20 working day deadline. Although performance has improved since the last quarter, work continues with local leads across the organisation to highlight the importance of FOI and identify further areas for improvement.
Month Requests Reviews Met % Met Over 20
days % Over 20 days
May* 41 33 80 7 20 Jun 24 22 88 2 12 Jul 39 34 87 5 13 Aug 32 17 5
* One request was closed without being responded to as the requestor did not provide clarification Forward Look One of the main priorities for the last quarter of 2012 will be winter planning; including the launch of the annual flu and ‘Be Ready for Winter’ campaigns. The Communications Team will continue to work closely with key partners including Serco, Forestry Commission Scotland and Maggie’s Caring Cancer Centers to develop and implement communications plans for a wide range of developments at the new hospital. Work will also continue with communication leads in partner organisations to ensure a consistent and proactive approach to communications on a wide range of joint projects including the ‘Reshaping Care for Older People’ programme.

Coverage by Newspaper STV Online 2.4% The Herald 2.9%Stirling Observer 21% Allanwater Herald 4.3%The Scotsman 2.3% Alloa Advertiser 13.5%Central FM 6.8% Eastside Advertiser 5.6%Sunday Mail 0.5% BBC News 2.4%Daily Record 0.5% Falkirk Herald 26%Eastside Advertiser 5% Bo'ness Journal 5.3%Wee County News 0.5% Holyrood Magazine 0.5%Property Magazine International 0.5% The Courier 0.5%Architects Journal 0.5% Evening Times 0.5%Metro 0.5% Stirling News 0.5%Daily Mail 0.5%
Community Hospitals 2.5% GPs/Health Centres 0.5%Accident & Emergency 2.5% Art 8%Dental 1% Royal Opening 1%School Health 2% Patient Care 9%Transport 4% Services for Older People 2%Announcements/Events 7% Cleanliness 5%Sexual Health 2% Radio Royal 0.5%Charity/Fundraising 11% Awards 5%Acute 2% Technology 2%Care for Abuse Survivors 3% Finance 1.5%Women/Children 6% Public Health 6%Staff 3.5% Parking 2%Bed Moves 2% Environment 2%Appointments 3% Pharmacy/Medicines 3.5%Waiting Times 1.5% Health Education 2%Suicide Bereavement Service 2%
Appendix 1 – Media Monitoring
Media Monitoring and Analysis
TOTAL - 207
Coverage by Subject
Enquiries by NewspaperSTV 1.6% The Herald 2.4%GMTV 0.8% Newsflash 0.8%Central FM 14.2% Scotland on Sunday 2.4%Pulse Magazine 2.4% Falkirk Herald 30%Alloa Advertiser 3.2% Sunday Times 15%Press and Journal 2.4% Sunday Herald 4%Daily Mail 3.2% Wee County News 3.2%BBC News 0.8% Stirling Observer 3.2%Daily Record 0.8% BBC Radio Scotland 1.6%Falkirk Advertiser 0.8% Killin News 3.2%Therapy Weekly 1.6% Pressgang News Agency 0.8%Northscot Agency 0.8% Young Peoples Now Magazine 0.8%
Enquiries by SubjectCharity 0.8% Waiting Times 6.3%Car Parking 0.8% Staff 8%Mental Health 0.8% Nursing Homes 0.8%Taxis 0.8% Sexual Health 0.8%Pharmacy 0.8% Financial 4%Outpatients 2% Ministerial 3%Filming Request 0.8% Community Hospitals 2%GPs/Health Centres 6% Health Policy 6%Women and Children 4% Family Planning 0.8%Alcohol and Drugs Services 6.3% Whistleblowing 0.8%Health Promotion 3% Public Health 17.7%Public Involvement 3% Healthcare Strategy 4%Acute Care 13.5% Dental 0.8%Vaccinations 0.8% A&E 0.8%Diet/Obesity 0.8%
Proactive 64%Reactive 36%
Positive 57%Negative 20.3%Neutral 22.7%

Forth Valley NHS Board 25 September 2012 This report relates to Item 7.1 on the agenda
Minute of Area Clinical Forum Meeting held on
19 July 2012
For Noting

FORTH VALLEY NHS BOARD DRAFT Minute of the Area Clinical Forum meeting held on Thursday 19 July 2012 at 6.15 pm in the Boardroom, NHS Forth Valley, Carseview House, Castle Business Park, Stirling. Present Dr Allan Bridges (Chair) Dr Keith Bowden, Area Psychology Committee Ms Lindsay Cowan, Area Optical Committee Ms Kathleen Cowle, Area Pharmaceutical Committee Dr Stuart Cumming, Stirling CHP Ms Morag Harris, Allied Health Professionals Committee Mr Graeme Inglis, Healthcare Scientists Forum Mr Robert Johnston, Area Dental Committee Dr James King, Clackmannanshire CHP Ms Allison Ramsay, Area Nursing & Midwifery Committee Mr Iain Watt, Area Pharmaceutical Committee In Attendance: Mrs Kathy O’Neill, General Manager, Clackmannanshire and Stirling CHP Ms Debbie Innes, Corporate Services Assistant (minute) 1/ WELCOME AND APOLOGIES FOR ABSENCE
Dr Bridges welcomed everyone to the meeting and apologies for absence were intimated on behalf of, Ms Grace Love, Ms Fiona Mackenzie, Dr Leslie Cruickshank and Ms May Fallon.
2/ MINUTE OF THE AREA CLINICAL FORUM HELD ON 17 MAY 2012 The minute of the Area Clinical Forum was approved as a correct record, subject to the following
amendments:
• Item 4, paragraph 4 – Continued Education and Training (CET) • Item 7 should be item 9 with the addition of Appointment of Area Optometric Advisor • Item 8 should be item 10
3/ MATTERS ARISING There were no matters arising. 4/ INTEGRATED ADULT HEALTH & SOCIAL CARE The Area Clinical Forum received a presentation Integrated Adult Health & Social Care,
presented by Mrs Kathy O’Neill, General Manager, Clackmannanshire & Stirling CHP. Dr Bridges reported that Integrated Adult Health & Social Care is high on the health service
agenda and that all consultation responses are to be returned to Beverley Finch, Head of Corporate Services, prior to being forwarded to the Scottish Government Health Directorate.
Mrs O’Neill reported that Integration of Adult Health & Social Care would be a major
transformation to the NHS Scotland Health Service.

Mrs O’Neill highlighted the following:
• Background o A Joint Future (2003) o Community Health Partnerships o Scottish Governments Views
• Local Examples of Integrated Working • Scottish Government Proposal • Key Elements of Consultation • Health & Social Care Integration: Some Key Issues • Next Steps
Mrs O’Neill highlighted the importance of strong clinical and professional leadership and
addressing the equality agenda on the Integration agenda. The Area Clinical Forum discussed the key issues, wider engagement, the role of current CHP
Sub Committees and Scottish Government legislation. Mrs O’Neill highlighted the importance of receiving feedback from Professional Advisory
Committees on consultation questions. Dr Bridges thanked Mrs O’Neill for an informative presentation. Discussion on the Integrating Adult Health & Social Care will be held at item 4.1.
4.1 Integrating Adult Health & Social Care Consultation The Area Clinical Forum considered a paper Integrating Adult Health & Social Care
Consultation, presented by Dr Allan Bridges, Chair of the Area Clinical Forum. Dr Bridges reported that comments on the consultation would be forwarded to Beverley
Finch, Head of Corporate Services. In response to a question from Ms Allison Ramsay, Area Nursing and Midwifery
Committee regarding the number of potential partnerships, Mrs O’Neill reported that the NHS Board had considered options available and that discussions were ongoing and flexibility at this point was being be sought after.
Ms Ramsay raised concerns about the effect of more than one partnership on smaller
services such as learning disabilities and the impact on North and South sectors. She also raised concerns around the availability of resources, time and commitment to support partnerships.
Mr Iain Watt agreed that from a prescribing point of view the direction of partnerships may
cause issues. Ms Harris commented that area wide services may be an issue as Allied Health
Professional’s had amalgamated recently. Mr Johnston reported that Dental services were also joined, although if outcomes were
agreed then flexibility would ensue. Mr Inglis raised concern about the way services may be viewed and a resource impact on
laboratory services. The Area Clinical Forum discussed current pressures on services, targets and workforce.
Housing, Committee Structures, Lead Accountable Officers, integration of budgets, workforce and planning, long term commitments were also discussed.

Mr King reported on Partnership Board members and expected input from Non Executive
Board members. He also reported on GP locality and the possibility of returning to LHCC arrangements and social levels.
Dr Cumming highlighted the need for:
• Deliverability • Capacity • Targets • local and national strategic focus • outcomes • joint community measures • Older People and complex care • Secondary Care Engagement
Dr Bridges highlighted the following:
• Success of Integrating Adult and Social Care in other NHS Health Boards • Measuring outcomes • Resources, time and commitment • Fragmentation – Primary and Secondary Care • Workforce and professional training
Ms Cowan supported the Integration of Adult Health & Social care however, she raised
concern about the quality of service and cost to the National Health Service. Mrs O’Neill reported on possible levels of disruption to services, timing and a risk that the
Scottish Government’s expectations are unrealistic. Ms Cowle raised concerns about 3rd
Sector partnerships, voluntary sector, care support and change of cultures.
Dr Cumming highlighted the need to be aware of:
• Scheme of Delegation • Fragmentation and division of services • Acute Hospital spend • High Level Strategic Partnerships The Area Clinical Forum agreed that comments should be circulated prior to sending to Ms Finch.
5/ REPORT ON ACF EVENT – 22 MARCH 2012 The Area Clinical Forum considered a paper - Report on the Area Clinical Forum Event – March
2012, presented by Dr Allan Bridges, Chair of the Area Clinical Forum. Dr Bridges reported that he had met with Mrs Morag McLaren, Head of Organisation
Development to discuss the organisation of an Area Clinical Forum Event in November 2012. The next steps, staff engagement and key issues from Forth Valley NHS Board were discussed. Dr Bridges agreed to discuss topics for the next Area Clinical Forum with Professor Fiona
Mackenzie and report back to the Area Clinical Forum at the September 2012 meeting.

Dr Cumming reported that he had met with Mary Cameron, eHealth Manager, Bette Locke and Ann Allison to discuss development of a Forth Valley Strategy for Telehealthcare.
He reported that focus will be on improving independent living through an anticipatory care
planning approach that optimises Long Term Conditions (LTC) management which in turn should help reduce avoidable hospital admissions and enable effective discharges as well as providing better carer and family support.
Dr Cumming highlighted that key workstreams involve:
• DALLAS programme • Telecare • Telehealth • Rehabilitation models • Communication • Telemedicine • Teleconferencing
Dr Cumming suggested using Telehealthcare as focus for a future Area Clinical Forum event. He
also highlighted that the Chairman and Non Executive Board members had expressed an interest in Telehealthcare and had attended a meeting with Mary Cameron.
Dr Bridges highlighted that Telehealthcare connected with the Integration of Health & Social Care
agenda. The Area Clinical Forum discussed the impact of Telehealthcare, integrating with services the
ageing population and smaller workforce, packages of care and communication. The Area Clinical Forum agreed that an event should be arranged for November 2012 and that
Morag McLaren be given assurance that this is what the Forth Valley NHS Board is looking for. 6/ ALLIED HEALTH PROFESSIONALS COMMITTEE – UPDATE The Area Clinical Forum received a presentation – Allied Health Professionals Committee –
Update, presented by Morag Harris, Allied Health Professional Committee Representative. Mrs Harris reported that the Allied Health Professionals meeting held on 16 May 2012 was not
quorate. Mrs Harris highlighted the following:
• Allied Health Professionals Advisory Committee • Allied Health Professionals (AHP’s) - who are we? • New Uniforms • Managed in 5 care groups • Review session • Topics we have discussed • Achievements
Dr Bridges thanked Mrs Harris for her presentation on the Allied Health Professionals Advisory
Committee and invited feedback from the Area Clinical Forum. Mr Johnston highlighted the importance of rebuilding professional’s identities and that
professional advisor remits were still to be agreed. He raised concerns with regard to the consideration of the integration of Health Care Scientists at a national level.
The Area Clinical Forum discussed Allied Health Professional’s influence on waiting times, community and outpatient services and reducing referral waiting times, workforce issues, medical staffing and targets and priorities.

The Area Clinical Forum considered a number of issues and concerns including the Allied Health
Professionals structure, balanced approach to delivery, HEAT targets, In-patient services, the reallocation of resources, medical staffing, workforce plans and integration skills across professionals.
Mrs Ramsay reported that decisions and outcomes from Area Nursing and Midwifery Committee
would be fedback to the Area Clinical Forum. Dr Cumming highlighted the importance of the Area Clinical Forum comments being fedback to
General Managers. Dr Bridges and Dr Cumming agreed to discuss concerns raised by the Area Clinical Forum with
Professor Mackenzie, Chief Executive, Mrs Helen Kelly, Director of Human Resources, Mr Ian Aitken, General Manager for Emergency & Inpatient Based Services, Mrs Kathy O’Neill, CHP General Manager and Mr David McPherson, General Manager for Specialist & Ambulatory Care Services.
Advisory Committee Chairs agreed to discuss with relevant Committees and provide comments
to the Area Clinical Forum at the September 2012 meeting. Dr Bridges thanked Mrs Harris for presenting an update on the Allied Health Professionals
Advisory Committee. 7/ AGENDA ITEMS FOR THE NEXT MEETING The Area Partnership Forum agreed the following items for discussion at the September 2012
meeting: Health Promoting Health Service: Action in Hospital Settings Smoking Cessation Pharmacy 8/ ANY OTHER COMPETENT BUSINESS There being no other competent business the Chair closed the meeting. 9/ DATE OF THE NEXT MEETING Thursday 15 November 2012 at 6.00pm in the Boardroom, NHS Forth Valley, Carseview House,
Castle Business Park, Stirling.

Forth Valley NHS Board 25 September 2012 This report relates to Item 7.2 on the agenda
Minute of Performance & Resources Committee meetings held on 3 August
& 7 September 2012
For Noting

PERFORMANCE AND RESOURCES COMMITTEE
Minute of the Performance and Resources Committee meeting held on Friday 3 August 2012 at 9.30 am in the Boardroom, Forth Valley NHS Board Headquarters, Carseview House, Castle Business Park, Stirling.
Present: Dr Vicki Nash (Chair) Mr Brendan Clark Ms Fiona Gavine Mrs Helen Kelly Mr James King Mr Alex Linkston Professor Fiona Mackenzie Mrs Fiona Ramsay Mr Tom Steele Professor Angela Wallace Dr Iain Wallace In attendance: Mr David McPherson, General Manager (item 6.2) Mr Andy Rankin, Head of Patient Access (item 6.2) Dr Anne Maree Wallace, Director of Public Health (item 7.1) Ms Elaine Vanhegan, Head of Performance Management Ms Marian Smith, Corporate Services Assistant (minute) Dr Nash extended a warm welcome to Mr David McPherson, Mr Andy Rankin and Dr Anne Maree Wallace. 1/ APOLOGIES FOR ABSENCE Apologies for absence were intimated on behalf of Dr Stuart Cumming. 2/ DECLARATIONS OF INTEREST There were no declarations of interest. 3/ MINUTE OF THE PERFORMANCE AND RESOURCES COMMITTTEE MEETING
HELD ON 6 July 2012 The minute of the Performance and Resources Committee meeting held on 6 July
2012 was approved as a correct record subject to the following amendment. Item 7.4 – Proposed Performance Framework 4/ MATTERS ARISING There were no matters arising. 5/ URGENT BUSINESS There was no urgent business to note. 6/ FINANCIAL AND PERFORMANCE ISSUES
6.1. Core Performance Report The Performance and Resources Committee considered a paper “Core Performance Report”, presented by Professor Fiona Mackenzie, Chief Executive.

Professor Mackenzie highlighted that following the Performance and Resources Committee meeting in July, further work had been undertaken to strengthen performance management reporting at various levels within the organisation, the Performance Report presented to the NHS Board had been streamlined to ensure Board Members were updated on key performance issues and the sequencing of meetings would be reviewed following the recent management restructure.
The agenda for the Performance and Resources Committee had been amended to
incorporate comments following the discussion held at the last meeting. It was expected that a rolling programme of specific issues from the Balanced Scorecard, workstreams and priorities would form the agenda.
Professor Mackenzie highlighted the following as detailed in the paper:-
• Cancer Waits • Complaints
The Performance and Resources Committee discussed in detail the challenging targets for Antimicrobial prescribing, the focussed work on increasing performance for responding to complaints, the new telephone reminder service which has resulted in a decrease in the number of patients failing to attend appointments and the reasons behind the cancellation of operations The ongoing work with NHS 24 to assist with ensuring attendance at appointments, links to waiting times, delayed discharges, feedback received from the Scottish Ombudsmen to improve the quality of responses to complaints and a review priority targets for NHS Forth Valley against Government reporting targets for the next 4 – 5 years were also discussed. Dr Nash highlighted that the September Performance and Resources Committee would focus on capacity and flow issues and a prescribing update would be provided at the November meeting. Following discussion the Performance and Resources Committee noted the paper. 62. Waiting Times Update The Performance and Resources Committee received a presentation “Waiting Times Update”, presented by Mr David McPherson, General Manager and Mr Andy Rankin, Head of Access. Mr McPherson highlighted the following as detailed in the presentation:- • Traditional Patient Pathway • 18 Week Referral to Treatment Pathway • Waiting Times Targets • 12 Week Treatment time Guarantee (TTG) • Key issues from TTG • NHS Board Priorities • Challenges • Key Issues
Mr McPherson advised that the new 12 week TTG for inpatient and day case treatment would come into effect from 1 October 2012. This would be a legally

binding maximum wait and Board’s Chief Executive Officers and Chairs were currently in discussion with the Scottish Executive Health Department regarding the implementation as described in the presentation. This guarantee relates to day case or in-patient treatment starting within 12 weeks of the agreement that treatment is necessary. He further advised that the HEAT targets for 2012/13 would ensure that 90% of planned patients would have their total care journey within 18 weeks of initial referral supporting this stage of treatment, referrals stated that no patient should wait longer than 12 weeks for a new outpatient appointment at a consultant-led clinic.
The Performance and Resources Committee discussed the need to manage patients in order to meet the 12 week TTG, the impact on patient choice, increased communications and also noted the complexity associated with this topic. Following discussion the Performance and Resources Committee noted the presentation 6.3 Finance Report to end June 2012 The Performance and Resources Committee considered a paper “Finance Report for the Period Ended 30th
June 2012”, presented by Mrs Fiona Ramsay, Director of Finance and Planning.
Mrs Ramsay reported that the NHS Board was reporting an operational overspend of £0.463m to the end of June 2012 with a balanced outturn projected for 2012/2013
Mrs Ramsay reported on the increase in access costs, workforce turnover levels current level of spend on bank and agency staff, skill mix changes in the nursing workforce in emergency care, ambulatory care and community hospitals which required action to ensure financial balance. The associated risk to achieve financial balance was projected to be £3.5m. Mrs Ramsay highlighted the financial pressures and associated risks with Acute Services and Waiting Times and the plans in place to ensure the delivery of a balanced position by the 31 March 2013. The Performance and Resources Committee noted that future savings plans would require a core strategic approach and collaboration with other agencies. Mrs Ramsay highlighted the continued focus within Acute Services and in particular:- • skill mix issues and contingency nursing costs within Surgical and Cancer
Services, • additional capacity costs of operating CAU overnight and pressure on front door
medical costs for covering vacancies and sickness absence • continued challenges associated with the Paediatric Rota and pressures in
Obstetrics and Gynaecology caused by maternity leave
The Performance and Resources Committee discussed the links to the national work around integration of services, increased partnership working both locally and regionally and sharing financial and savings plans with other NHS Boards. The issues and challenges for the management of non core costs, medical workforce issues, utilisation of national contracts, prioritisation of capacity and access issues. workforce planning, pay and pension issues, low staff turnover rates, ageing

workforce within NHS Forth Valley and integrated workforce plans were also discussed. Following discussion the Performance and Resources Committee noted:- • the revenue overspend of £0.463m to 30 June 2012 • that financial balance is projected for March 2012, but there is some risk
associated with this given the early financial pressures seen across specific areas including medical emergency costs and access delivery. This risk is projected to be £3.5m
• that actions were required to ensure financial balance by minimising temporary workforce spend (medical in particular), implementation of agreed skill mix changes in nursing workforce, implementation of Access Sustainability Plan and continued focus on prescribing savings
• the balanced capital position projected 7/ STRATEGIC PRIORITIES/BALANCED SCORECARD ISSUES 7.1 Breastfeeding Target Position – implications and inequalities
The Performance and Resources Committee received a presentation “Breastfeeding in Forth Valley: The Challenges and Opportunities”, presented by Dr Anne Maree Wallace, Director of Public Health
Dr Wallace highlighted the following as detailed in the presentation:- • Breastfeeding rates • Why breastfeed • Benefits to the baby • Benefits to the mother • Breastfeeding statistics • Factors which affect breastfeeding • Affect of maternal age on breastfeeding • Factors which affect breastfeeding • Actions taken in NHS Forth Valley • Opportunities • Challenges • Proposed way forward • Points for debate
The Performance and Resources committee noted the decrease in breastfeeding rates over the last three years and discussed the support and time commitment required to assist mothers.
The links to inequalities, geographical differences, readily available products, awareness raising of the benefits of breastfeeding, individual choice, the support available from Health visitors, and increased partnership working were also discussed.
Following discussion the Performance and Resources Committee noted the presentation.

8/ STRATEGIC PROJECTS/ISSUES 8.1 Bellsdyke Development Agreement
The Performance and Resources Committee received a verbal update from Mrs Fiona Ramsay, Director of Finance and Planning.
Mrs Ramsay reported that following recent discussions with the consortia all issues except one in relation to incentives had been concluded. It was anticipated that agreement would be reached on the outstanding issue in due course. The Performance and Resources Committee noted the update.
8.2 Sale of Gladstone Place
The Performance and Resources Committee received a verbal update from Mr Tom Steele, Director of Projects and Facilities.
Mr Steele reported that three offers had been received and the Board had been in discussion with the NHS Board’s Property Advisers regarding acceptance.
The Performance and Resources Committee noted the update.
9/ ANY OTHER COMPETENT BUSINESS There being no further competent business the Chair closed the meeting at 12.05 pm. The plans to consider Capacity and Flow at the next meeting were noted.

1
PERFORMANCE AND RESOURCES COMMITTEE
Draft minute of the Performance and Resources Committee meeting held on Friday 7 September 2012 at 9.30 am in the Boardroom, Forth Valley NHS Board Headquarters, Carseview House, Castle Business Park, Stirling.
Present: Dr Vicki Nash (Chair) Dr Stuart Cumming Ms Fiona Gavine Mrs Helen Kelly
Mr Alex Linkston Mrs Fiona Ramsay Mr Tom Steele Dr Iain Wallace In attendance: Mr David McPherson, General Manager (item 6.3) Ms Gail Caldwell, Pharmacy Director (item 7.1) Ms Margaret Duffy (Item 7.2) Ms Elaine Vanhegan, Head of Performance Management Ms Beverley Finch, Head of Corporate Services Ms Elsbeth Campbell, Head of Communications Ms Marian Smith, Corporate Service Assistant (minute) 1/ APOLOGIES FOR ABSENCE
Apologies for absence were intimated on behalf of Mr Brendan Clark, Mr James King, Professor Fiona Mackenzie and Professor Angela Wallace.
2/ DECLARATIONS OF INTEREST There were no declarations of interest. 3/ MINUTE OF THE PERFORMANCE AND RESOURCES COMMITTTEE MEETING
HELD ON 3 AUGUST 2012 The minute of the Performance and Resources Committee meeting held on 3 August
2012 was approved as a correct record. Dr Nash advised that an update on Capacity and Flow would be presented at the
Performance and Resources Committee at the meeting schedule for 5 October 2012. 4/ MATTERS ARISING Bellsdyke Development Agreement Mrs Ramsay reported that discussions had now concluded with agreement reached.
The Board’s Legal Advisers and the Consortium Legal Team were updating contractual information.
Gladstone Place Mr Steele reported that discussions were ongoing with regards to the Sale.

2
5/ URGENT BUSINESS There was no urgent business to note. 6/ FINANCIAL AND PERFORMANCE ISSUES
6.1. Finance Report The Performance and Resources Committee considered a paper “Finance Report to 31 July 2012”, presented by Mrs Fiona Ramsay, Director of Finance. Mrs Ramsay advised the following a meeting with the Scottish Government on 6 September 2012 it had been acknowledged that NHS Forth Valley had made good progress with regards achieving the savings targets. It was noted that NHS Forth Valley was ahead of schedule regarding brokerage repayment with £6.3m of £12.1m remaining based on current projections. The updated brokerage schedule would be included in the next financial report. Sale of Bannockburn Hospital
Mr Steele reported that four offers had been received and were higher than expected. The Board were in discussion with the Board’s Property Advisers regarding acceptance.
Larbert House Mr Steele advised that the appeal to the Scottish Government had been successful.
The Developer had now lodged two further planning applications for the Walled Garden and the Stable block.
Bonnybridge Mr Steele advised that discussions were ongoing with Falkirk Council as part of their
Asset Management Review. Falkirk Council had expressed an interest in acquiring the former Bonnybridge
hospital for Falkirk Community Trust. It had also been proposed that the Joint Loan Equipment Store or a Scottish Ambulance Service base could potentially relocate to the site.
He further advised that a bid had been submitted to hub East Central Territory for
enabling funding Mrs Ramsay reported that NHS Forth Valley Board was reporting an operational overspend of £0.543m to the end of July 2012 with a balanced outturn projected for 2012/2013. This required ongoing scrutiny of and reductions in costs
As previously reported to the Performance and Resources Committee Acute Services and Waiting Times remain the most significant financial pressures. Mrs Ramsay referred to Item 6.3 on the agenda and indicated the costs of Access Target delivery could be covered under this item.

3
Mrs Ramsay highlighted the continued focus on:- • reduction in bank and agency spend • skill mix changes within the nursing workforce in Emergency Care outpatients
departments and Community hospitals • delivery of recurrent savings plans and detailed action plans in place to support
them • the ongoing work regarding management and administration savings which are
linked to the recent management restructure Mrs Ramsay highlighted the planned announcement on 19 September 2012 of the draft Scottish Budget In response to a question from the Chairman on how future savings programmes were proceeding, Mrs Ramsay indicated that work was ongoing and that there had been discussion at the recent Directors of Finance meeting that traditional areas for savings have been exhausted and that there was an increasing challenge in identifying furthersavings without service impact. The Performance and Resources Committee noted:- • the revenue overspend of £0.543m to 31 July 2012 • that financial balance is projected for March 2013, but there is some risk
associated with this given the early financial pressures seen across specific areas including acute costs and access delivery.
• that actions were required to ensure financial balance by minimising temporary workforce spend (medical in particular), implementation of agreed skill mix changes in nursing workforce, implementation of the Access Sustainability Plan and continued focus on prescribing savings and management/administration savings
• the cash savings requirement of £11.244m recurrently required by March 2013 and the further steps required to deliver savings related to organisational structure review.
• the balanced capital position projected 6.2. Core Performance Report The Performance and Resources Committee considered a paper “Core Performance Report”, presented by Mrs Fiona Ramsay, Director of Finance.
Mrs Ramsay highlighted the following as detailed in the paper:-
• Delayed Discharges • Cancer Waits • Complaints • Theatre Under Runs
The Performance and Resources Committee were advised that a Serious Incident Review was underway in relation to a specific cancer wait. Dr Wallace highlighted a recent Freedom of Information Request regarding Critical Incidents subsequent to the Ayrshire and Arran reports. The figures submitted would include this particular review.

4
The Performance and Resources Committee discussed in detail the issues around delayed discharges and particularly challenges in Falkirk. The Performance and Resources Committee were advised that there would be focussed discussion on delayed discharges at the Falkirk Partnership Board meeting scheduled for 21 September 2012 and the November Performance and Resources Committee meeting. It was highlighted that the issue will need to be raised at the Annual Review of NHS Forth Valley’s Performance on 18 September 2012. Ms Duffy highlighted the assistance received from the Joint Improvement Team on delayed discharges and the outcomes that required to be addressed from the action plan. She further highlighted a visit planned by the Government Team on 23 October 2012. In response to a question from Mr Linkston regarding the significance of the visit on 23 October, Ms Duffy advised it was in relation to NHS Forth Valley’s plans to address achieving the delayed discharge target over 6, 4 and 2 weeks. Mrs Ramsay highlighted the ongoing discussions regarding the implementation of the 12 week Treatment Time Guarantee, which would be considered in more detail later in the agenda. The potential for extending the pilot with NHS 24 for contacting patients for outpatient appointments to other areas, e.g. Day Surgery was also discussed, in relation to tackling the issue of theatre under runs when patients fail to attend. The Performance and Resources Committee discussed the format of the Core Performance Report noting that it was easier to read, and that more information had been included in the report highlighting where there had been change in performance. It was noted that once the Covalent system was introduced there would be a further change in format. It was suggested that those areas which required more focus and areas where no change had taken place in month be highlighted. Following discussion the Performance and Resources Committee noted the paper. 6.3. Waiting Times The Performance and Resources Committee received a presentation “Waiting Times” presented by Mrs Fiona Ramsay Director of Finance. Mrs Ramsay highlighted the following as detailed in the presentation:- • Outline • Impact of removal of ‘Award Breach’ on level of breaches • 12 week Treatment Time Guarantee • 18 week Treatment Time Guarantee • Actions
The Performance and Resources Committee discussed in detail the impact of the introduction of the 12 week TTG, the need to ensure that local capacity was maximised, the use of additional capacity within the private sector, associated funding challenges and the need to ensure sustainability from 2013/14 onwards.

5
The potential financial impact of using the private sector, maximising the Golden Jubilee Hospital for specialties other than orthopaedics, communications, the impact of the national detect cancer early campaign and associated risks were also discussed Mrs Ramsay advised that discussions were ongoing with the Scottish Government with regards to additional funding support noting that NHS Forth Valley did not have sufficient funds to deliver the required activity. Following discussion the Performance and Resources Committee noted the presentation.
7/ STRATEGIC PRIORITIES/BALANCED SCORECARD ISSUES 7.1 Prescribing
The Performance and Resources Committee received a presentation “Prescribing Update”, presented by Dr Iain Wallace, Medical Director and Ms Gail Caldwell, Pharmacy Director.
Dr Wallace advised that the introduction of the GP incentive scheme two years ago had assisted towards the NHS Board’s savings targets. The scheme provided the GP Practices with the opportunity to re-invest in their practice.
Ms Caldwell highlighted the following as detailed in the presentation:-
• Introduction • Strategic Priorities/Balanced Scorecard • Efficient Prescribing: Background • Health Board Primary Care Cost Per Patient April 2010 • Why the high cost per patient • 2010/11 and 2011/12 • Health Board Primary Care Cost Per Patient April 2012 • Prescribing strategy • Key activities to date • Ezetimibe Prescribing – Quality Outcomes Framework 11/12 • Whole System Working 11/12: Polypharmacy in frail • GP Prescribing Incentive Scheme • Ways to reduce cost/patient • Practice Visits • 12/13 Plans • Lidocane Medicated Plaster (Versatis) • Risks • Effective: Antimicrobial Prescribing: Background • V1b: % Seasonal variation in prescribing quinolones within primary care(winter v
summer) • Seasonal variation of quinolone use – time period 2011/12 • Quinolone Prescribing – items /1000 patients • Seasonal variation in prescribing quinolones • Conclusions

6
The Performance and Resources Committee discussed using the approach towards Prescribing Savings in other areas, the links between secondary care and primary care prescribing, the effective use of using comparative data to incentivise GPs, the need to have clear criteria and guidance in place. The links to shifting the balance of care, whole system working and the investment in the development of services through the GP incentive scheme were also discussed. Following discussion the Performance and Resources Committee noted the presentation. 7.2 NHS Forth Valley Response to the Integration of Adult Health and Social
Care Consultation The Performance and Resources Committee considered a paper “NHS Forth Valley Response to the Integration of Adult Health and Social Care Consultation”, presented by Ms Margaret Duffy. Ms Duffy advised that each of the statutory organisations in Forth Valley had
responded to the Consultation. Individuals, professional groups and stakeholder organisations also had the opportunity of contributing to the responses from national groups, professions or representative bodies.
She further advised that NHS Forth Valley supported the principles of the integration of health and social care services but recognised the need to ensure local flexibility to enable local agencies to agree an appropriate model to address local issues. Referring to the consultation document the Performance and Resources Committee discussed the following points in detail the:- • need for clarity around budgetary shifts, • role of national agencies, • impact of integration on HR and Information Technology, • importance of information sharing, • data sharing protocols, • different governance arrangements, • role of the Jointly Accountable Officer • communications. The links to the GP contract, the need for clinical involvement in the suggested committee structure and the need for appropriate resources in place to support the integration of services were also discussed. Following discussion the Performance and Resources Committee approved the paper subject to the suggested changes being made.
8/ ANY OTHER COMPETENT BUSINESS Annual Review of NHS Forth Valley’s Performance
Ms Vanhegan advised the Annual Review of NHS Forth Valley Performance had been scheduled for 18 September 2012. It would be non Ministerial visit with a public
engagement session.

7
Ms Vanhegan highlighted the following presentations at the event:-
• Branching Out • Patient Experience • Early years • Prescribing Mr Linkston advised this would be as informal an event as possible which would encourage debate from the public audience and the opportunity for any concerns or issues raised to be addressed.
There being no further competent business the Chair closed the meeting at 11.50 am The plans to consider Capacity and Flow at the next meeting were noted.

1
Forth Valley NHS Board 25 September 2012 This report relates to Item 7.3 on the agenda
Minute of Clinical Governance Committee meeting held on 27 July 2012
For Noting
2
DRAFT Minute of the Forth Valley NHS Board Clinical Governance Committee meeting held on Friday 27 JULY 2012 at 9.30 am in ROOM 1, LEARNING CENTRE, FORTH VALLEY ROYAL HOSPITAL Present: Ms Fiona Gavine, Non Executive Board Member (Chair) Dr A Bridges, Chair of Area Clinical Forum Mrs E Crosbie, NHS Forth Valley Public Partnership Forum Mrs H McGuire, Public Involvement Network Ms V Nash, Non Executive Board Member Mr C Forbes, Non Executive Board Member In Attendance: Dr D Beckett, Clinical Lead for Acute Medicine & Hospital at Night Mrs G Caldwell, Pharmacy Director Mrs I Graham, Personal Assistant (Minute) Mr J Horwood, Infection Control & Public Health Manager Mrs M Inglis, Head of Clinical Governance Mr A Linkston, Chairman, NHS Forth Valley Ms E Vanhegan, Head of Performance Management
Professor A Wallace, Director of Nursing Dr I Wallace, Medical Director 1/ APOLOGIES FOR ABSENCE Apologies for absence were intimated on behalf of Dr S Cumming, Ms M Duffy, Dr AM Wallace, Professor F Mackenzie and Mrs A Richmond-Ferns. 2/ DECLARATIONS OF INTEREST There were no declarations of interest. 3/ QUALITY IMPROVEMENT AND CLINICAL GOVERNANCE IN THE ACUTE
ADMISSIONS UNIT (AAU) The Committee received a presentation from Dr Dan Beckett, Clinical Lead for Acute Medicine and Hospital at Night. Dr Beckett stated that the aim of the project had been to reduce the number of cardiac arrests in the Acute Admissions Unit. A Morbidity and Mortality Group had been established and identified the following issues:

3
• Evidence of failure to identify, and delays in the response to sick patients • Resuscitation attempts on occasions undertaken on patients with terminal illness • Limited learning from adverse outcomes
A Failure Modes Effects Analysis (FMEA) was undertaken with all staff participating. The following were recognised:
• NHS Early Warning Score (NEWS) charts were not being completed correctly • Emergency Department was not utilising the Early Warning Score • There was no structured handover between the Emergency Department and the
Acute Admissions Unit After assessment it was agreed that an aim statement be developed to reduce the cardiac arrest rate in the Acute Admissions Unit. A driver diagram was also produced with actions to recognise and respond to the deteriorating patient, improve learning from adverse events and improve end of life care. Stickers were developed which, when completed by staff, highlighted the recognition/escalation of a patient’s conditon and the response/intervention to be taken should a patient deteriorate rapidly. Safety incident reports were also completed and filed in a red folder which everyone in the department had access to. These were discussed at a weekly multidisiplinary team meeting. A consistent approach was being used in the Emergency Department and a structured handover had been developed when patients moved from the Emergency Department to the Acute Admission Unit. Meetings between the Emergency Department and the Acute Admissions Unit had been established with the first meeting taking place in September. The success of having this ward based team approach had resulted in a significant reduction in the rate of cardiac arrests. The performance of the Acute Admissions Unit together with the numbers of complaints/compliments received were displayed in the Relatives Room. Dr Beckett welcomed any questions from the Committee. In response to a question from Mr Forbes regarding patients who had Do Not Resuscitate in their notes, Dr Beckett stated that staff would always discuss this with the patient on arrival in the Acute Admission Unit. However if the patient was unconscious then staff would make the decision and involve the family if possible. Dr Iain Wallace reported that he had brought together a Reliable Rescue Group who were looking at the spread of this methodology to other areas and a number of wards were already showing an interest in taking this forward. He was also working with Professor Angela Wallace and Mrs Monica Inglis to develop a spreadplan to roll this methodology out. Mrs Gavine thanked Dr Beckett for his informative presentation. 4/ MINUTE OF NHS FORTH VALLEY CLINICAL GOVERNANCE COMMITTEE
MEETING HELD ON 30 MARCH 2012

4
The minute of the Clinical Governance Committee meeting held on 30 March 2012 was approved as a correct record with the addition of apologies being noted from Mrs E Crosbie. 5/ MATTERS ARISING 5.1 Review of Actions The Committee considered the actions from the previous meeting and noted the progress made to date. Item 2 & 4.1 Amendment to the previous minute and draft Clinical Governance Committee
Annual Report had been completed. Item 4.2 Professor Wallace reported that a Patient Panel Information Sub Group had
been formed and would bring feedback from the group to the next meeting. Ms Inglis had not been able to progress work on specific indicators for Primary
and Community Services. Item 5.1 Mrs McGuire confirmed that Patient Panel members had now taken part in
domestic audits at both Falkirk and Stirling Community Hospitals. Mrs Crosbie advised on some environmental issues at Falkirk Community Hospital and Mr Horwood advised that these had been addressed. He agreed to invite Mrs Crosbie to re-visit to see the changes.
Mrs Crosbie advised that 2 out of 4 visits had been cancelled due to staff un-
availability and it was agreed that this was not acceptable and should not happen in the future.
Item 5.3 Mrs Caldwell reported that Janette Fraser, Senior Planning Manager was
involved with taking forward the redesign of the ambulance transport service. Mrs Caldwell agreed to further investigate the point raised by Mrs McGuire regarding rural patient transport.
Mrs Caldwell confirmed that 1st class postage was used for patient and staff
correspondence and all other mail was sent 2nd class. Item 5.4 Mrs Inglis stated that the discrepancy with our figures appeared to be an issue
with the way we counted. The Surgical and Cancer Services Unit was preparing a response to Health Improvement Scotland and this would be brought to the next meeting.
6/ CLINICAL GOVERNANCE: STRATEGY AND OBJECTIVES 6.1 Health Improvement Scotland (HIS) - Ayrshire & Arran The Committee received a paper - Health Improvement Scotland (HIS) - Ayrshire & Arran - presented by Dr Iain Wallace, Medical Director.

5
Dr I Wallace explained that Health Improvement Scotland (HIS) had been asked to undertake a review following the Scottish Information Commissioner’s critical comments regarding a Freedom of Information response by NHS Ayrshire & Arran. Dr I Wallace advised that a short life working group had been established to look at how the recommendations in the subsequent report could be escalated in NHS Forth Valley and a report would be presented to the next meeting of this Committee. Health Improvement Scotland (HIS) advised that they would visit the Boards to review progress from the autumn.
Action: Dr I Wallace The Committee noted the report. 6.2 Joint Clinical Governance Working Group Annual Report The Committee received a paper - Joint Clinical Governance Working Group Annual Report - presented by Ms Monica Inglis, Head of Clinical Governance. Mrs Inglis stated that the report provided a summary of the topics discussed over the year by the Acute Clinical Governance Working Group, Joint Acute/Community Healthcare Partnership Clinical Governance Working Working Group and Community Healthcare Partnership Clinical Governance Working Group. Mr Forbes queried why the admin/reception staff were not included in the membership of the CHP working group and Mrs Inglis agreed to take this back to Kathy O’Neill, Community Healthcare Partnership General Manager for consideration. In response to a question from Mrs McGuire, Dr Wallace described the contractual arrangement in respect of independent practitioners in relation to the quality of Primary Care Services.
Action: Mrs Inglis The Committee approved the report. 6.3 Information Governance Group Annual Report The Committee received a paper - Information Governance Group Annual Report - presented by Dr Iain Wallace, Medical Director. Dr Wallace reported on the volume and breadth of the work undertaken which included the rollout of e-learning, joint working with local authorities, police and procurator fiscals on data protection/confidentiality and the improvement on the response time of Freedom of Information requests. Mr Forbes queried if there could be support for new Board members in relation to Information about the role of Caldicott Guardian and Information Governance and it was agreed to take this forward. The Committee approved the report.

6
6.4 Organ Donation Committee Annual Report The Committee received a paper - Organ Donation Committee Annual Report - presented by Dr Iain Wallace, Medical Director. Dr Wallace reported that there had been an improvement in our organ donation activity figures since last year; however we had not yet been successful in completing a donation after cardiac death. It was recognised that Kate Fawcett, Communications had carried out a huge amount of work to raise public awareness in Forth Valley. The Committee approved the report. 6.5 Risk Management Annual Report The Committee received a paper - Risk Management Annual Report - presented by Mrs Gail Caldwell, Pharmacy Director. Mrs Caldwell gave details on the implementation of the Risk Management Strategy which included:
• Structures • Policies and Procedures • Risk Management Priorities • Clinical Governance • Fire Safety • Violence and Aggression • Civil Contingencies • Reviews and Assessments • Incident Reporting • CNORIS Premiums and Claims • Significant Incidents
Mrs Caldwell gave an update on the current review of Clinical Governance and Risk Management arrangements which would include the recent internal audit report. The Committee discussed the detail of the report and in response to a question from Mrs Crosbie regarding the fire policy at Falkirk Community Hospital; Mrs Caldwell agreed raise this with Peter Mackie, Head of Risk Management
Action: Mrs Caldwell The Committee approved the report.
7/ SAFE CARE 7.1 NHS Forth Valley Healthcare Associated Infection Reporting Template (HAIRT) The Committee received a paper - NHS Forth Valley Healthcare Associated Infection Reporting Template (HAIRT) - presented by Mr Jonathan Horwood, Infection Control & Public Health Manager.

7
Mr Horwood highlighted the Board reporting performance arrangements for Health Associated Infection for June 2012. Mr Horwood reported that there had been 4 cases of Staphylococcus aureus Bacteraemias (SABs) recorded which was within the national norm. There had been 3 cases of Clostridium Difficile (cDif) recorded which again was within the national norm. There had been a decrease in hospital acquired cases, most were in the community. In response to a question from Mrs McGuire on why hand hygiene was not recorded in this report, Mr Horwood explained that hand hygiene figures were captured by the Scottish Patient Safety Programme. The template for the HAIRT was a Scottish Government template and we were unable to alter the format in any way. It was agreed to provide this information in the Safe and Effective person centred indicators report. The Committee noted the report. 7.2 NHS Forth Valley Healthcare Associated Infection (HAI) Annual Report The Committee received a paper - NHS Forth Valley Healthcare Associated Infection (HAI) Quarterly Report - presented by Mr Jonathan Horwood, Infection Control & Public Health Manager. Mr Horwood stated that this was the first report using the new user friendly format. Over the period there had been a decrease of 6% in Staphylococcus aureus Bacteraemias (SABs) this figure being consistent with the previous year - breakdown as follows:
• 24% hospital attributed • 56% healthcare attributed • 1% nursing home attributed • 19% community attributed
There had also been a 38% decrease in Clostridium difficile Infection (CDI) - breakdown as follows:
• 21% hospital attributed • 70% healthcare attributed • 6% nursing home attributed • 3% community attributed
There had been 4 noro virus outbreaks during the period with 1 community hospital closure. Audits on wards were carried out by infection control staff on a monthly basis with Patient Panel members being invited to take part in these audits. Mr Horwood praised the infection control team and laboratory staff for all the good work carried out. Mrs McGuire raised a query in relation to page 4 of the report about which Community Hospital had been included. Mr Horwood agreed to amend the report. The Committee noted the report.

8
7.3 NHS Forth Valley Corporate Risk Register The Committee received a paper - NHS Forth Valley Corporate Risk Register - presented by Mrs Gail Caldwell, Pharmacy Director. The Committee considered the report and following an update from Dr I Wallace agreed that the following would be included in the risk register:
• Modernising Medical Careers and Junior Doctors - the Government were reducing the number of doctors in training to bring them into alignment with consultant posts. This had been recognised as a national problem. It was agreed to add medical work force to a future agenda
Mrs Caldwell stated that as the new committee restructure had now been agreed, a review to align risks with the correct committees would need to be completed. Mrs Inglis agreed to explore sharing risk registers with other Boards. The Committee noted the report. 8/ EFFECTIVE CARE 8.1 NHS Forth Valley Clinical Governance Performance Monitoring Template Summary The Committee received a paper - NHS Forth Valley Clinical Governance Performance Monitoring Template Summary - presented by Mrs Monica Inglis, Head of Clinical Governance. The Committee were asked to note that a review process was being carried out for the following:
• Skin cancer MCN • Hepato-bilary MCN annual report • Urology MCN annual report • Colorectal cancer MCN annual report • MCN for haemato oncology annual report
Mrs Inglis advised that NHS Forth Valley had not yet been notified of a date for the announced visit from Health Improvement Scotland (HIS) in relation to the standard for the care of older people in acute care. The Committee noted the report. 8.2 Safe & Effective Person Centred Indicators The Committee received a paper - Safe & Effective Person Centred Indicators - presented by Mrs Monica Inglis, Head of Clinical Governance. Mrs Inglis stated that this was the second report which utilised data from the Board Executive Performance Report with additional information from the Scottish Patient Safety
9
Programme. Mrs Inglis reported that she was looking at presenting the safe care section in a different way. It was agreed that an educational event would be organised for the Board Non-executives to discuss the data in more depth. It was also agreed to develop the report to make it clear if the data was showing improvement or not. Professor Wallace advised that the information displayed for the public in the wards had been developed from patient/public perspective.
Action: IG to organise The Committee noted the report. 8.3 Health Improvement Scotland (HIS) Medical Profiles The Committee received a presentation - Health Improvement Scotland (HIS) Medical Profiles from Dr Allan Bridges, Chair Area Clinical Forum. Dr Bridges explained the background to medical profiles and stated that they were a suite of clinical indicators regarding the medical care provided by NHS Forth Valley and its hospitals with national comparative data. The indicators comprised of the following topics:
• Acute medicine & emergency medicine • Coronary heart disease • Respiratory medicine • Gastrointestinal medicine • Venous thromboembolism • Palliative care • Renal medicine
The data provided by National Services Scotland gave reassurance of our performance but the problem was that the data was 2 years old and we were also now in a new hospital. There was an issue regarding the accuracy of coding and we were looking at developing local ways of collecting our data. Mrs Gavine thanked Dr Bridges for an interesting presentation. 9/ PERSON CENTRED CARE 9.1 NHS Forth Valley Complaints Performance Report The Committee received a paper - NHS Forth Valley Complaints Performance Report - presented by Professor Angela Wallace, Director of Nursing. Professor Wallace reported that during May there had been a dip in our performance and 34.33% response to complainants within 20 days was achieved. Six complaints had been identified as complex and the performance rate against these complaints was 16.67%.

10
As part of a plan to improve performance the whole organisation would be encouraged to support the Complaints Team with achieving the response timescales. Professor Wallace stated that the Patient Rights Act will also have a work load impact effect on the Patient Relation Team following discussion on the actions taken to prevent issues recurring. It was agreed to review the format of the report. The Committee noted the report. 10/ REPORTS FROM ASSOCIATED CLINICAL GOVERNANCE GROUPS 10.1 Minute of Patient Focus and Public Involvement Steering Group held on 15
March 2012 The Committee noted the minute of the Patient Focus and Public Involvement Steering Group held on 15 March 2012 as presented by Professor Angela Wallace, Director of Nursing. 10.2 Minute of Information Governance Group held on 5 April 2012 and draft minute
held on 25 May 2012 The Committee noted the minute of the Information Governance Group held on 5 April 2012 and draft minute held on 25 May 2012 as presented by Dr Iain Wallace, Medical Director. Mrs McGuire asked if the issues relating to GE health care had been resolved, Dr Wallace advised that this was currently under review. 10.3 Draft Minute of Acute Clinical Governance Working Group held on 24 May 2012 The Committee noted the draft minute of the Acute Clinical Governance Working Group held on 24 May 2012 as presented by Mrs Monica Inglis, Head of Clinical Governance. 10.4 Draft Minute of the Area Prevention and Control of Infection Committee held on
26 April 2012 The Committee noted the draft minute of the Area Prevention and Control of Infection Committee held on 26 April 2012 as presented by Mr Jonathan Horwood, Infection Control and Public Health Manager. 10.5 Draft Minute of the Child Protection Action Group held on 10 May 2012 The Committee noted the draft minute of the Child Protection Action Group held on 10 May 2012 as presented by Professor Angela Wallace, Director of Nursing. 10.6 Child Protection Action Group - Quarterly Report The Committee noted the Child Protection Action Group - Quarterly Report as presented by Professor Angela Wallace, Director of Nursing. It was agreed to add the quarterly report to the agenda in future.
11
10.7 Draft Minute of Area Medical Equipment Committee held on 23 May 2012 The Committee noted the draft minute of the Area Medical Equipment Committee held on 23 May 2012 presented by Dr Iain Wallace, Medical Director. 10.8 Draft Minute of the Joint Clinical Governance Working Group held on 24 May
2012 The Committee noted the draft minute of the Joint Clinical Governance Working Group held on 24 May 2012 as presented by Mrs Monica Inglis, Head of Clinical Governance. 10.9 Minute of Research and Development Committee held on 26 April 2012 The Committee noted the minute of the Research and Development Committee held on 26 April 2012 presented by Dr Iain Wallace, Medical Director. 10.10 Draft Minute of Organ Donation Committee held on 26 March 2012 The Committee noted the draft minute of the Organ Donation Committee held on 26 March 2012 as presented by Dr Iain Wallace. 10.11 Minute of the Civil Contingencies Tactical Group (CCTG) held on 18 August
2011 and draft minute held on 18 April 2012 The Committee noted the minute of the Civil Contingencies Tactical Group (CCTG) held on 18 August 2011 and draft minute held on 18 April 2012 as presented by Mr Jonathan Horwood, Infection Control and Public Health Manager. 10.12 NHS Forth Valley Guidelines and Policies Update The Committee noted the NHS Forth Valley Guidelines and Policies Update for the period March to May 2012 inclusive presented by Dr Iain Wallace, Medical Director.
11/ TO NOTE ANY UNTOWARD INCIDENTS There were no untoward incidents to report. 12/ ANY OTHER COMPETENT BUSINESS There was no other competent business. 13/ DATE AND TIME OF FUTURE MEETINGS The next meeting of the NHS Forth Valley Clinical Governance Committee would be held on Friday 12 October 2012 in the Boardroom, Carseview House, Stirling. There being no further business, the Chair closed the meeting at 1.00pm

Impact of the Patient Rights (Scotland) Act 2011

2
• Supporting patients, carers and the public to give feedback, make comments, raise concerns and complain
Executive Summary The purpose of the paper is to present the duties of the Patient Rights (Scotland) Act 2011 (The Act) places on NHS Boards and Health Service Providers, and to outline the plan for implementation of the supporting guidance on managing feedback, comments concerns and complaints ‘Can I Help You?’ and 12 Week Treatment Time Guarantee. The key priorities are
• Supporting staff to value and respond positively to feedback, comments, concerns and complaints
• Implement systems to capture, record and report feedback, comments, concerns and complaints
• Learn and improve services as a result of feedback, comments, concerns and complaints
• Deliver national waiting times targets which includes the legally binding 12 weeks Treatment Time Guarantee for all Day Cases and Inpatients.
Achieving these priorities will require building on the progress already made in designing a person centred complaints process and achievements through our Patient Experience work and ongoing focus on waiting times. We will also continue to work in partnership with a range of internal and external stakeholders.

3
Introduction The purpose of the paper is to present the duties the Patient Rights (Scotland) Act 2011 (The Act) places on NHS Boards and Health Service Providers, and to outline the plan for implementation of the supporting guidance on managing feedback, comments concerns and complaints ‘Can I Help You?’ and 12 Week Treatment Time Guarantee. Background Through the [then] PFPI Steering Group, NHS Forth Valley played an active role in the development of the Act. Working with patient, public and third sector partners, written evidence was submitted as part of the Patient Rights Bill consultation, followed by oral evidence to the Health and Sport Committee. NHS Forth Valley was represented on the national group which developed ‘Can I Help You?’ the revised guidance for handling and learning from feedback, comments, concerns and complaints about NHS health care services. More recently we have had the opportunity, again with our patient, public partners, to comment on the Patients Charter. Within NHS Forth Valley, the newly established Person Centredness Steering group will direct and monitor the implementation of the Act.

4
• To be treated with dignity and respect
Section 1: The Patient Charter and Health Care Principles The Act 2011 places a duty on ministers to publish a Charter of Patient Rights and Responsibilities by 01 October 2012. This Charter will summarise the rights and responsibilities of patients using the NHS in Scotland and those of people who have an interest in the patient’s welfare. The charter reflects the patient’s rights;
• To have their confidentiality upheld • That NHS services take into account their individual needs, abilities and
circumstances • To information and communication that helps them to make informed choices and
decisions about their health care • The right to give feedback, comments, concerns and complaints.
The Charter also sets out the patient’s responsibility to treat staff with dignity and respect.
Section 2: Feedback Comments Concerns and Complaints The Act and its supporting legislation give patients the right to give feedback, make comments, raise concerns and to make complaints about NHS Services. It also places a duty on NHS Services to encourage, monitor, take action and share learning from views they receive. The secondary legislation regarding feedback, comments, concerns and complaints led to a revision of the Guidance ‘Can I Help you?’ which was issued in April 2012. Work will shortly commence to revise the NHS Forth Valley Policy and Guidance to reflect the Act.
2.1 Supporting Patients and the Public 2.1.1 Access to Independent Advice and Support The Act provides for the establishment of the Patient Advice and Support Service (PASS), which is provided by the Citizens Advice Bureaux, and commenced on 01 April 2012 to provide independent advice and support to patients and the public and raise awareness of their rights and responsibilities. Citizens Advice Scotland is currently working to develop publicity materials for the new PASS service. A local PASS monitoring group is being established to support the development of, and to promote the new service. This will include PASS staff and NHS Forth Valley Complaints Personnel as well as representatives from our third sector and patient public partners. 2.1.2 Making People Aware There is a duty on NHS Bodies and their Healthcare Providers to ensure that procedures on how to give feedback, make comments, raise concerns and to make complaints are well publicised. Health Information Scotland is revising the current information booklets in line with the new guidance and this is available in alternative formats. The Patient Relations Team staff are speaking with the PPFs and local community groups such as Princes Trust Carers, to raise awareness and break down the barriers to people giving feedback, making comments, raising concerns and making complaints.

5
2.2 Supporting Staff The Act makes it a requirement that NHS bodies and Health Service providers ensure feedback, comments and concerns are handled appropriately, monitored and used to identify areas of concern, improve performance and identify and share best practice. Feedback, comments, concerns and complaints may be given to any member of staff or to volunteers and it is important that staff and volunteers are able to differentiate between issues that constitute feedback, comments, concerns and complaints. All staff and volunteers must be trained to welcome and encourage feedback, comments and concerns from patients, carers, families and visitors and should be empowered to respond. Staff also need to know how to report feedback, comments and concerns and systems need to be in place to support this. Where staff are unable to deal with issues, they should be able to give assurance that the person has been listened to and know how to escalate to a more senior person. A national working group with representation from Boards (including NHS Forth Valley), NHS Education and the Scottish Public Services Ombudsman has been set up to develop a learning package for staff. This will support the existing training currently provided in NHS Forth Valley on complaint investigation, patient experience and communication. 2.3 Collecting and reporting data This is a significant undertaking for Boards as previous reporting focused only on the numbers, targets met, and themes from complaints. NHS Bodies and their Health Service Providers are now required to have procedures in place for collecting, recording, and disseminating the information, themes and good practice gained from patient’s views and experiences to improve the quality of service. The legislation places clear responsibility on the relevant NHS bodies and health service providers to record the data they receive in relation to feedback, comments, concerns and complaints: • Relevant NHS bodies will collate and review complaints information quarterly and
feedback, comments and concerns information annually • Quarterly reports will be prepared for complaints only • An annual report will be prepared and published by relevant NHS bodies for feedback,
comments, concerns and complaints. There is a requirement to summarise what action has been or is to be taken to improve services as a result of feedback, comments, concerns and complaints received in the year
• Health service providers will provide their respective relevant NHS body with complaints information as requested on a quarterly basis and feedback, comments and concerns data on an annual basis; and
• NHS bodies will submit complaints data annually to the Information Services Division (ISD), a Division of NHS National Services Scotland, for collation and publication of national complaints statistics.
Work is currently underway with the Information Services Division (ISD), Primary Care Contractors and Safegard ( the risk and complaints management system) to develop systems for capturing and reporting feedback, comments, concerns and complaints. This will now include all independent contractors: General Practitioners, Pharmacists, Optometrists, and Podiatrists. A reporting template will be developed and sent quarterly to the Patient Relations Team where the data will be collated and reported at Board Level and to ISD.

6
Systems will also need to be developed to enable reports on the action taken and learning shared as a result of feedback, comments, concerns and complaints. 2.4 Responding to feedback, comments and concerns It will not always be necessary to respond when feedback, comments and concerns may for example, be given anonymously. Responses are provided in a variety of ways depending on the level and nature of the feedback, comment or concern. ‘Feedback’ would include sources such as the Better Together National Survey and Patient Opinion website. NHS Forth Valley is currently involved in a pilot using the Patient Opinion website for patients to give feedback and comment about their experience. When a patient posts a comment, an alert is sent to staff to enable the board to respond. The pilot has been extended due to the low response rate. ‘Comments’ are captured locally through, for example, the patient experience survey which forms part of the ward Balanced Score Card and through our comments forms ‘What did we do well? What could we do better? Data is currently available on many of the ward and department improvement boards, and work is currently underway to ensure there is consistency across the organisation and make the data more ‘patient friendly’. ‘Concerns’ are generally raised locally with front line staff. Responses to concerns may be given verbally or in writing, and should include an apology where appropriate, and any improvement which may be made. If the person raising the concern is not satisfied with the response, consideration should be given to a meeting with a senior manager or to advice on how to raise a formal concern. A formal system will need to be developed to support staff to record, monitor and share the learning from complaints. Consideration is being given to expansion of the Safeguard complaints management system which is currently used in the organisation to support the management of complaints. 2.5 Encouraging, handling and learning from complaints. The Act aims to support a culture that actively encourages and welcomes views whether these are good or bad. Complaints should be valued alongside all of the other forms of feedback and used to improve the service. The emphasis is on early and local resolution ensuring that learning is shared and improvements made as soon as practicably possible after the complaint is made. 2.5.1 Definition A complaint, which may be made orally or in writing, is defined by the Scottish Public Services Ombudsman as
‘An expression of dissatisfaction about an action or lack of action or standard of care provided’ SPSO 2011 2.5.2 The Complaints Procedure. Complaints still need to be acknowledged within three days, and investigated within 20 days where reasonably practicable. This now applies to all healthcare providers (the previous response time for GPs was 10 days). If we are unable to meet the 20 day target, under the revised guidance, complainants must be advised of the reason for this. A request must made for an extension and revised response date given. If the reason given

7
is not acceptable, complainants can go to the SPSO at this point and ask them to investigate. (Under the previous guidance this was 40 days). Work is currently underway to ‘re-design’ the complaints process in NHS Forth Valley to ensure that we are providing a person centred service to patients, carers (and other third party complainants) and staff. Key areas for improvement from the initial diagnostic work include keeping in touch with the person making the complaint; improving complaint investigation; improving response times and sharing the learning and improvements made. 2.5.3 Complaints that cover more than one service or sector. Where a complaint relates to the action of more that one NHS Body, a nominated person should take the lead, and the complainant informed who the lead will be. Where possible a joint response should be provided. Where the complaint relates to health and social care again a lead should be nominated and where possible a joint response should be provided. It is recognised that different complaint handling processes and timescales currently exist for health and social care service. The complainant must be advised as to how this may impact on the response. NHS Forth Valley Patient Relations Team enjoys good working relationships with our health and social care partners and we will continue to develop this. However, more consideration needs to be given to developing joint responses to complainants. 2.5.4 Alternative Dispute Resolution The Act provides for Alternative Dispute Resolution Services in the form of mediation or conciliation, where both parties feel this would be of benefit. NHS Forth Valley was part of the national pilot for the mediation service. The uptake during the pilot was low and there were no cases identified in NHS Forth Valley during the pilot period. However, following the pilot, the service is now accessible nationally and supporting guidance is now available. 2.5.5 The investigation Implementation of the Act and supporting guidance will have an impact on the way complaints are currently investigated within NHS Forth Valley. The current process involves statements from those involved in the complaint being sent to the Patient Relations Team. The information provided is used to draft a response to the complainant. Difficulties often arise in more complex complaints where there can be nine or ten statements, some of which contain conflicting information, and which contain a large amount of clinical information but miss answering the question being asked. The Act calls for an investigation which should be proportionate to the complaint. Complaints handled by full investigation are typically those that are complex, or require a certain amount of examination to establish the relevant facts before a response can be provided. Complex complaints would include, for example, those where significant harm may have occurred, those concerning end of life care, those with multiple issues which span many departments. The aim of the investigation is to establish all of the facts relevant to the points raised and provide a full, objective and proportionate response that represents the definitive position. This means that we need to be clear about whether or not the complaint is being upheld, and reflect this in our response to the complainant. It is recognised within the guidance that the Patient Relations Team will be the main source of expertise and will oversee the investigation teams, supporting them to plan the investigation. The Patient Relations Team will be the main point of contact for the complainant.
8
In accordance with the complaints Directions, the investigation report issued to the complainant must include the conclusions of the investigation and information as to any remedial action taken or proposed as a result of the complaint. To support this change, in 2010 - 2011 the SPSO worked with the National Complaints Personnel Association Scotland to develop training for senior ‘front line’ staff to undertake complaints investigation. To date over fifty staff across NHS Forth Valley, Band 7 and above, have undertaken the training and work is now underway with the General Managers to implement the role of investigation officer. 2.5.6 Monitoring of Complaints, Learning and Improvement. NHS bodies must ensure that complaints are reviewed by senior management at least twice per year with a view to identifying areas for concern, agreeing remedial action and improving performance. This review must also consider any recommendations made by the SPSO. 2.5.7 Publication In accordance with the complaints Directions, NHS bodies must publish anonymous details annually on patient feedback, comments, concerns and complaints and provide evidence that action is or has been taken, where appropriate, to improve services. These reports should be easily accessible to members of the public and available in alternative formats as requested.

9
Key Areas
Section 3: Key Milestones and Deliverables
Activity Timescale Deliverables Implementation and monitoring of the Act and Supporting Guidance for feedback, comments, concerns and complaints
Establish a working group of key stakeholders including complaints personnel, front line staff, operational and General Managers PASS, independent contractors, patient public partners
October 2012- April 2014
Deliver on all Key Areas within agreed timescales Report to Person Centred Steering Group
Resources Identify resources required to support implementation
Sept 2012 – Dec 2012
All staff and volunteers receive training Systems in place to capture analyse and report data Learning shared across NHS Forth Valley
Supporting Patients and the Public
Establish local NHS Forth Valley PASS implementation and monitoring group as per national agreement.
Sept 2012- April 2013
Publicity materials available and disseminated across NHS Forth Valley Patients and carers and members of the public are aware of how to give feedback, comments raise concerns and make complaints
Supporting staff- Training all staff and volunteers
Representation on National Steering Group Local implementation and delivery plan
August 2012- April 2014 April 2013- March 2014
Development of training resources including eLearning modules based on current SPSO template Link to eKSF Staff in NHS Forth Valley encourage feedback and are empowered to respond and know when and how to escalate.
Feedback Comments and Concerns
Develop and implement systems for
April 2012 –
Demonstrate how feedback, comments

10
Collecting Recording Disseminating
information, themes and good practice across NHS Forth Valley including from independent contractors.
December 2012
and concerns have been used to improve services for patients across NHS Forth Valley Report to Board Quarterly Report to ISD annually
Complaints Review and re-design of NHS Forth Valley Complaints Process Phase 1 Diagnostics Phase 2 Testing Phase 3 Implementation
Apr – July 2012 Oct- Dec 2012 Jan- April 2013
Robust investigation of complaints which result in a clear decision and where appropriate, learning and improvements to service.
Reporting Review of complaints performance report to include themes, learning and action taken as a result of feedback, comments, concerns and complaints from NHS Forth Valley including all independent contractors
Oct 2012- April 2013
Demonstrate how complaints have been used to improve services for patients across NHS Forth Valley Report to Board Quarterly Report complaints to ISD quarterly

11
SECTION 4: Treatment Time Guarantee (TTG) Under the Act, from 01 October 2012, all eligible patients who agree to treatment will start to receive their day case inpatient treatment within 12 weeks of the agreement to treat. The first tranche of patients subject to the Act will be ready for treatment at the end of December 2012. Exceptions to the 12 week TTG include:
• Assisted reproduction • Obstetric Services • Organ, tissue or cell transplantation • Surgical intervention of spinal scoliosis • Spinal injuries
Access Policy The Act requires the NHS Board to have an up to date Access Policy. Work has been undertaken to review and the current Access Policy taking into account the national guidance and requirements. This policy will be considered by the NHS Board under a separate paper. This policy applies to all services including Mental Health Services, Acute Services and any community sites which provide Elective Day case or Inpatient treatment.
• NHS Lothian
Reasonable Offers The NHS Board Access Policy must define what constitutes a reasonable offer and what locations the reasonable offer covers including offers to Golden Jubilee National Hospital and specifically which private sector hospitals are to be used under the term reasonable offer. The sites which are classed as reasonable offer sites are:
• NHS Lanarkshire • NHS Fife • NHS Tayside • NHS Greater Glasgow and Clyde • National Facilities e.g. Golden Jubilee National Hospital Clydebank, Stracathro
Hospital • Private sector - BMI hospitals
In exceptional circumstances e.g. specialist services and for capacity issues it may be that a reasonable offer will be any NHS facility within Scotland. In these circumstances NHS Forth Valley will be responsible for the cost of any transport and accommodation arrangements necessarily and reasonably incurred by the patient and their carer (if necessary). Rights and Responsibilities The NHS Board has a legal obligation to treat inpatients or day cases within 84 days( 12 weeks) of the agreement to treat (usually agreement to treat takes place at the first new outpatient appointment). The Act places Rights and Responsibilities on patients to comply and honour reasonable offers of admission.

12
If patients refuse two reasonable offers i.e. two offers of appointment with at least a minimum of 7 days notice, the clock will be reset to a zero wait. If they then refuse two further reasonable offers they will be referred back to their GP. Patients will only be placed on the waiting list if they are fit for anaesthetic, available, and ready for treatment. If a diagnostic procedure is required or a patient wants time to consider their treatment, they will not be added. There will no longer be the opportunity for patients to wait to be seen by a specific consultant or location without having an impact on their waiting time clock. A period of unavailability will be added. Patients will be given two reasonable offers for an appointment with another Consultant or location. Where patients are ‘indefinitely unavailable’, they will be reviewed in 12 weeks and an alternative appointment offered. If they are unable to accept this appointment, they will be referred back to their GP. This also applies when patients have “patient advised” unavailability for example, because of exam leave, carers leave holidays etc. or when they are unavailable because of medical reasons as decided by a Clinician. If the NHS Board cancels an appointment/admission, the patient will still be entitled to be seen within the 12 weeks TTG. Patients who are willing to wait for what ever reason are no longer able to do so as the treatment time ‘clock’ will continue. Patients can only be made “unavailable” for treatment under specific circumstances and this is set out in the guidance. Communication with the Patient Under the Act patients must be informed in writing regarding any changes to their waiting time clock Patients must be made aware of their responsibilities regarding appointments, impact of non attendance and changing appointments. If a patient breaches the 12 weeks TTG the Health Board must explain in writing why the breach occurred. The patient must be offered the next available date.
• Stricter rules around unavailability with a need to maximise theatre and bed capacity to treat patients.
Other Implications
• The communication requirements of the Act will mean additional administrative time with a patient reminder service to support compliance under consideration.
• The cost of transport out of area is now mandatory if patients accept an offer outwith Forth Valley and are unable to get their own transport.
• There is no precedent detailing the legal implications of breaching the Treatment Time Guarantee. It may be possible that a court could decide punitive actions for non- compliance that has a financial implication for NHS Forth Valley.
• The Patient Administration Systems will require to be upgraded to capture information. • Access Policy compliance will need to be monitored with a review of current roles
underway.

13
Training and Standardisation of Practice All staff and volunteers are required to undertake training in responding positively to feedback comments and concerns, and know how to escalate matters when appropriate. To ensure standard practice of the National Access Policy across all services : NHS Forth Valley has written and is implementing Standard Operating Procedures (SOPs) for all elective IP/Dc service providers. Training of staff on the application of the Access Policy is underway.

Forth Valley NHS Board 25 September 2012 This report relates to Item 8 on the agenda
P atient R ights (S c otland) A c t 2011
(Paper presented by Professor Angela Wallace,
Director of Nursing)
For Noting

SUMMARY 1. IMP AC T OF T HE P AT IE NT R IG HT S (S C OT L AND) AC T 2011 2. PURPOSE OF PAPER
The purpose of the paper is to present the duties the Patient Rights (Scotland) Act 2011 (The Act) places on NHS Boards and Health Service Providers, and to outline the plan for implementation of the supporting guidance on managing feedback, comments concerns and complaints ‘Can I Help You?’ and the 12 Week Treatment Time Guarantee.
3. KEY ISSUES • The implementation of the guidance Can I Help You? will be directed and
supported by a working group made up of key staff, patient, public and third sector stakeholders. This will report to the Person Centredness Steering Group.
• The development and implementation of guidance is supported by national stakeholders including Scottish Public Services Ombudsman, NHS Education Scotland, Health Improvement Scotland, Citizens Advice Scotland, National Complaints Personnel Association Scotland.
• The NHS Board has a legal obligation to treat inpatients or daycases within 12 weeks of the agreement to treat (usually agreement to treat takes place at the first new outpatient appointment).
• The Act places Rights and Responsibilities on patients to comply and honour reasonable offers of admission to treat. This is supported by a revised NHS Board Access Policy which defines a reasonable offer also being considered by the NHS Board.
4. FINANCIAL IMPLICATIONS
Implementation of Can I Help You may impact on a number of areas, these are under review and include:
• Support for the implementation and evaluation of nationally agreed training resources for all staff and volunteers
• Support for the development and implementation of IT systems to facilitate the capture and reporting of data across NHS Forth Valley, including independent contractors.
• Support for the sharing of learning and improvement across NHS Forth Valley
5. WORKFORCE IMPLICATIONS
• All staff and volunteers are required to undertake training in responding positively to feedback comments and concerns, and know how to escalate matters when appropriate. In addition, training will be required for staff in recording details of local resolution and any improvements made as a result of feedback, comments, concerns and complaints.
• The communication requirements of the Act will mean reviewing administrative staff requirements.
6. RISK ASSESSMENT AND IMPLICATIONS:
• Any patient breaching 12 weeks has the right to challenge the NHS Board in court.
7. RELEVANCE TO STRATEGIC PRIORITIES • Implementation of the Act fits with the NHS Forth Valley Integrated Health Care
Strategy 2011-2014 and vision To Improve Health and Healthcare for the people of Forth Valley.
8. RELEVANCE TO DIVERSITY AND / OR EQUALITY ISSUES
• A full impact assessment will be undertaken
9. CONSULTATION PROCESS • There was extensive consultation with NHS Forth Valley Staff, Patient/Public
and Third Sector Partners throughout the development of the Act and supporting guidance.
10. RECOMMENDATION(S) FOR DECISION
Forth Valley NHS Board is asked to: -
• The Board is asked to support the key deliverables within the paper.
11. AUTHOR OF PAPER/REPORT:
Name: Designation: Jacqueline Macrae Andy Rankin
Patient Focus and Relations Manager Head of Patient Access
Approved by: Name: Designation: Angela Wallace Nurse Director

Forth Valley NHS Board 25 September 2012 This report relates to Item 9 on the agenda
Patient Access Policy
(Paper presented by Professor Fiona Mackenzie Chief Executive)
For Approval

SUMMARY 1. AC C E S S P OL IC Y 2. PURPOSE OF PAPER
In preparation for the introduction of the Patients Rights (Scotland) Act 2011 (The Act), NHS Forth Valley has reviewed its Access Policy governing the Rights and Responsibilities of Patients and Services in using and delivering health care. This paper seeks Board approval for the Access Policy.
3. KEY ISSUES • The Act requires the NHS Board to have an Access policy. • The Act requires NHS Forth Valley to describe what constitutes a reasonable offer
of appointment or admission and what locations the reasonable offer covers including the private sector facilities that patients may be offered.
• The Access Policy describes the patient’s rights and responsibilities when entering an agreement to treatment.
• With a stricter application of rules the Access Policy will ensure that patients have an understanding of the consequences of refusing 2 reasonable offers.
• Patients will only be listed who are fit for anaesthetic, available and ready for treatment.
• Offers to the Golden Jubilee National Hospital and private sector hospital are regarded as a “reasonable” offer.
• This policy applies to all services including Mental Health Services, Acute Services and any community sites which provide Day Case or Inpatient treatment.
4. FINANCIAL IMPLICATIONS
• There is no precedent detailing the legal implications of breaching the Treatment Time Guarantee. It may be possible that a court could decide punitive actions for non compliance that has a financial implication for NHS Forth Valley.
• Upgrade of Topas and Helix to record new clock starts and stops. • Administrative costs in support of improved patient information and communication. • Additional transport costs as the provision of transport out of area is now mandatory
if the patient is unable to provide his or her own transport when an offer is accepted outwith Forth Valley.
• Reallocation of resources to support the role of an Access Policy compliance officer. 5. WORKFORCE IMPLICATIONS
• Requirement to provide staff training in respect of the application of the access policy. To ensure standard practice of the National Access Policy across all services NHS Forth Valley has written and is implementing Standard Operating Procedures (SOPs) for all elective IP/Dc service providers.
• Additional administrative requirement in respect of informing patients of changes in their status with regard to adjustments to the waiting time clock.
• Staff require new skills to use system, in particular data extraction skills are required to extract relevant waiting times data from upgraded system
6. RISK ASSESSMENT AND IMPLICATIONS
• Risks in terms of funding required to achieve and maintain the 12 week TTG including staff availability if a gap is identified
• Overall capacity in respect of beds and theatres remains challenging and needs to be managed in a consistent and coordinated way to ensure maximum utilisation and to minimise risk to patient flow.
7. RELEVANCE TO STRATEGIC PRIORITIES
• The legally binding Treatment Time Guarantee (TTG) is an organisational priority and supported by capacity and flow work
• Compliance with Referral to Treatment Target • HEAT Target Compliance
8. RELEVANCE TO DIVERSITY AND / OR EQUALITY ISSUES
• The Diversity and Equality Team have been involved in the production of the access policy.
• Waiting times relates to pathways efficiency and ease of access identifying patients needs at the start of referral so that care can be tailored to need.
9. CONSULTATION PROCESS
A robust communication document is available for scrutiny. Consultation has been undertaken with all key stakeholders such as Patients Panels, CHP groups, Staff with a responsibility for managing waiting times, Clinicians and General Managers. The Communication Team has ensured that NHS Forth Valley staff have been informed through the Staff Brief, Staff Intranet and Staff Newsletter.
10. RECOMMENDATION(S) FOR DECISION
The Forth Valley NHS Board is asked to: - • Approve the Access Policy for implementation across NHS Forth Valley noting
risks and implications. 11. AUTHOR OF PAPER/REPORT:
Name: Designation: Roslyn Grant Service Improvement Manager
Approved by: Name: Designation: Fiona Mackenzie CEO

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
1
NHS Forth Valley Access Policy

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
2
Document Control Sheet Document purpose
Outline the overarching principles of NHS Forth Valley wide access policy following the national Access policy for NHS Scotland.
Title NHS Forth Valley Access Policy
Author Waiting Times Management Review Group
Issue Date Draft June 2012
Consultation Process
• Policy Approval Process Group • Information Governance • General Managers • ISD – Scottish Executive • Scottish Government • Surgical Unit – Service Managers • Health Records/RTT Team • PPP/PPI • CHP core group and sub committee – Stirling and
Falkirk • Chairs of:
Surgical Board Lead Clinicians Group Women and Children’s Unit MECAR GP Committee
Circulation list Senior Staff, Consultants, General Managers, CHPs, staff involved in TTG, Stage of Treatment Standards and 18WRTT NHS Forth Valley Intranet
Description Policy Document
Cross reference NHS Scotland National Access Policy The Patient Right (Scotland) Act 2011 The Patient Rights (Treatment Time Guarantee) (Scotland) Regulations 2012. The Patient Rights (Treatment Time Guarantee) (Scotland) Directions 2012. The Patient Rights (Treatment Time Guarantee)

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
3
(Scotland) Guidance. NHS Scotland Waiting Times Guidance Effective Patient Booking for NHS Scotland (2011) Armed Forces CEL 8 (2008); Armed Forces CEL 3 (2009); Armed Forces CEL 39 (2010) Adult Exceptional Aesthetic Referral Protocol CEL 27 (2011)
Superseded documents
NHS Forth Valley Patient access policy version 1 18 weeks; The referral to Treatment Standard: Principles and Definitions Issue 2..0 (January 2009) New Ways of defining and measuring waiting times: Applying the Scottish Executive Health Department Guidance, Version 3.0 (December 2007)
Change Record Date Author Nature of Change Reference

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
4
Contents 1. Introduction 6 2. Background 7 3. Waiting times standards 7 3.1 Exceptions to Treatment Time Guarantee (TTG) 8 3.2 Patient’s obligations 9 3.3 Patient communication 9 4. Key principles of the NHS Forth Valley access policy 10 5. Responsibilities under the National access policy/NHS FV access policy 12 5.1 To communicate effectively with patients 12 5.2 To manage referrals effectively 14 5.2.1 Referrer 14 5.2.2 Receiving location 15 5.2.3 Receiving clinician 15 5.2.4 Patient Transfer 16 5.3 To manage waiting list effectively 16 5.4 To use information to support implementation in Service
Improvement 18 6. New appointments processes 19 6.1 Patient focused booking (pfb) 19 6.2 Smart booking 19 6.3 Direct booking 19 6.4 Reasonable offer 19 6.4.1Dates of treatment 20 6.5 Waiting for a specific Consultant 21 6.6 Infrequent service 21 6.7 One stop service 21 7. Unavailability 22 7.1 Indefinite unavailability 22 7.2 Medical unavailability 23 7.3 Patient advised 23 7.4 Visiting consultant service 23 8. Managing Appointments of patients who DNA 25 8.1 New OP appointment 25 8.2 Elective admissions 25 8.3 Management of patients who CAN 26 8.4 Short Notice appointments 26 8.5 Cancelled by hospital 27

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
5
8.6 Transfer to different health board 27 9. Adding a patient to elective waiting list 28 9.1 Key principles 28 10. Pre-op assessment 29 11. Admissions 30 11.1 Could Not Attend (CAN) 30 11.2 Did Not Attend (DNA) 31 11.3 Short notice admissions 31 11.4 Cancelled by hospital 31 11.5 Could Not Wait 31 12. Specialist services 33 12.1 National Health cancer access targets 33 12.2. Rapid Access Chest Pain Clinic (RACPC) 34 12.3 Ophthalmology – cataract targets 34 13. Priority treatment for military veterans 35 14. Definitions 37 14.1 waiting time clocks 37 14.2 Treatment waiting times 37 14.3 Stage of treatment waiting times 37 14.4 18 weeks RTT 38 Appendix 1 39 Principles for commissioning additional capacity via waiting lists Appendix 2 41 Exclusions and inclusions 18 weeks RTT standard Appendix 3 42 Waiting list card Appendix 4 43 Direct Booking Letter

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
6
1. Introduction A National Access Policy has been developed to provide a common vision, direction and understanding of how NHS Boards should ensure equitable, safe, clinically effective and efficient access to services for their patients. This policy sets out the principles that will help ensure that systems are in place to optimise the use of facilities and available capacity in order to deliver high quality, safe patient care in a timely manner. NHS Forth Valley using the principles in the National Access policy will ensure that the systems, processes and resources are in place to deliver the responsibilities within the National Access Policy. NHS Forth Valley will also ensure that there are Standard Operating Procedures (SOPs) developed to ensure delivery of the requirements of the National Access Policy. This local access Policy sets out the details of how these principles apply to NHS Forth Valley local services e.g. possible and reasonable service locations to ensure that patients who are waiting for appointments for treatment are managed fairly and consistently across NHS Forth Valley and that NHS Forth Valley has clear and consistent guidance. This policy applies to all services including Mental Health Services, Acute Services and any community sites which provide Day case or Inpatient treatment. The current waiting times standards are:
• Legal 12 weeks Treatment Time Guarantee • 18 weeks Referral to treatment for 90% of patients • 12 weeks for new outpatient appointments • 6 weeks for the eight key diagnostic tests and investigations
The policy has been approved by the Board in an open session and is available on the Intranet.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
7
2. Background NHS Scotland’s Efficiency and Productivity Programme Delivery Framework (June 2009) sets out a commitment to achieve evidence based clinical practice by improving consistency of care, reducing variation and creating the right culture and organisational conditions required to support transformational change. It is essential that NHS Forth Valley uses resources in a cost effective way. It is recognised that a culture of continual service redesign and improvement is necessary to achieve transformational change. The need to improve consistency of care and reduce variation across NHSScotland is part of an explicit ongoing commitment to evidence based clinical practice. NHS Forth Valley’s Access Policy aims to ensure consistency of approach in providing access to services and as such it supports The Patients Rights (Scotland) Act 2011 which includes a guarantee in law that all eligible patients should start to receive their Day Case/in-Patient treatment within 12 weeks of the date of agreement to treat - 12 weeks Treatment Time Guarantee (TTG). The TTG dovetails with existing Stage of Treatment and 18 weeks referral to treatment standards.
The Patient’s Rights (Scotland) Act 2011 establishes a 12 weeks maximum waiting time for eligible patients. Eligible patients should start to receive their treatment within 12 weeks of the treatment being agreed between the patient and NHS Forth Valley. This means once a patient has been diagnosed as requiring inpatient or day case treatment and has agreed to that treatment,
NHS Forth Valley’s Access Policy also firmly supports NHSScotland’s Quality Ambitions, which put quality at the heart of our NHS. The shared ambition is to deliver world-leading person centred, safe and effective healthcare services as well as timely access to care at the point of treatment. As a minimum 90% of patients accessing Acute secondary care services can expect to be treated within 18 weeks from the receipt of their referral to the start of their treatment. 3. Waiting Times Standards NHS Boards are required to ensure that there is equitable and sustainable delivery of waiting time standards, and systems are in place to ensure sufficient capacity is available and there is optimal use of this capacity to deliver waiting times targets. This will involve working collaboratively with other healthcare providers and will ensure patients receive the most appropriate treatment with the shortest wait.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
8
they must start that treatment within 12 weeks of the agreement. This will include Mental Health services. The patients waiting clock will start on the date the patient agreed the treatment and will stop when the patient undergoes an operation or treatment. Diagnostic tests and Outpatient procedures will not fall under the definition of a “treatment” under the Act and so there is no TTG waiting time guarantee attached however the RTT standard still applies 3.1 EXCEPTIONS TO THE TTG
• Assisted reproduction • Obstetric services • Organ, tissue or cell transplantation whether living or deceased donor • Designated national services for surgical intervention of spinal scoliosis • The treatment of injuries, deformities or disease of the spine by an
injection or surgical intervention (until 1 October 2013) Start date The treatment time guarantee will start when the clinician and patient agree to the treatment. For the vast majority of the patients the agreement will be made at an outpatient appointment. If a patient requires to undergo a test before the treatment can be confirmed then the time when the patient is contacted about the test results and subsequent treatment agreed would represent the clock start date for the TTG. A clock will not start if a patient wants to consider whether to go ahead with the treatment. The clock will begin only when the patient agrees to go ahead with the treatment. This date should be noted and this will be the start date for TTG. The patients start date should not be delayed until after pre-operative assessment as this is only checking the patient is fit to come in for their treatment see page 30 for detail regarding pre-op assessment. End date The date the patient undergoes their treatment and must be within 12 weeks from date the patient agreed the treatment. Bilateral treatment For patients waiting for sequential bilateral treatment the waiting time for the second treatment is measured as a separate, second pathway it may be that the agreement for the need for both treatments is made at the same time. However, normally the agreement to commence second treatment is only

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
9
made on or after the post-operative review for the first treatment. The waiting time for the second treatment should not start until the clinician and patient agree to the agreed treatment. The sequential treatment must not be managed as a planed repeat. 3.2 PATIENTS’ OBLIGATIONS The aforementioned document also makes explicit the responsibility of the patient for accepting and honouring a “reasonable offer” of an outpatient appointment or admission date for treatment. Patients who “fail to attend” for an appointment or admission without prior warning will return to the start of the waiting queue, unless there are clinical or other compelling reasons for treating them sooner. Effectively they will have their waiting times “clock” returned to zero. 3.3 PATIENT COMMUNICATION While verbal contact with the patient is the preferred approach when offering appointments or admission dates, where this is not possible, effective processes for delivering and accepting or rejecting offers will be in place. Communications with patients should be in a format appropriate to their needs e.g. large print, community language. There are certain groups of patients who may experience difficulty accessing hospital facilities for specific reasons. GP’s should indicate this on the referral. This will ensure that steps can be taken to facilitate access and no patients are disadvantaged in any way.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
10
4. Key Principles of NHS Forth Valley’s Access Policy There are a number of key principles that underpin the achievement of the aims of the Access Policy and delivery of waiting time standards. • The patients’ interests are paramount. • Patients are offered care according to clinical priority and within agreed
waiting time standards. • Sufficient capacity should be available and optimally utilised to deliver
waiting times. • Referrals are managed effectively through electronic triage. • NHS Forth Valley will provide a common pathway for electronic triage
which includes the option of providing advice to the referrer or an appropriate appointment.
• Variations in referral patterns are identified and reduced. • Waiting lists are managed effectively using electronic systems where
possible. • Patients will be referred to a clinical team and will be seen by an
appropriate member of that team rather than a named consultant. • Patients should not be added to a waiting list if they are not available for
treatment due to medical reasons • Offers should be made as soon as possible after receipt of referral and a
minimum of 7 days notice before the date of the appointment or admission.
• A patient must be offered two reasonable offers for first outpatient and
inpatient admission. • If a patient refuses two reasonable offers, the hospital will refer the patient
back to the referring clinician, normally their GP, unless the consultant requests otherwise on clinical grounds.
• Patient advised unavailability should only be applied by a specific request
from the patient or their carer. This should be clearly documented on the hospital systems.
• The provision of short-stay surgery is maximised.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
11
• Admissions to hospital are actively managed through pre-assessment
services.
• Unnecessary follow up appointments are reduced.
• Information is used to facilitate improvements in service provision.
• There is partnership working with stakeholders in primary, secondary and social care.
• NHS Forth Valley aims to achieve inclusive and equal access for all
service users.
• Leadership and accountability for the improvement of waiting times and achieving waiting times standards are with the Access and Capacity Team and Operational Management Teams.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
12
5. Responsibilities under the National Access Policy/ NHS Forth Valley access policy
The National access policy details the responsibilities that will ensure equity and a consistency in approach to access to services across NHS Scotland as a whole. These same responsibilities have been adopted in NHS Forth Valley’s access policy. The four key responsibilities under the Access Policy are: 1. To communicate effectively with patients. 2. To manage referrals effectively. 3. To manage waiting lists effectively. 4. To use information to support improvements in service provision. 5.1 TO COMMUNICATE EFFECTIVELY WITH PATIENTS There is a need to ensure that patients are appropriately informed at all stages of the patient journey. Communicating effectively with patients or carer if appropriate will help to inform them of when, where and how they are to receive care and their responsibilities in helping to ensure that this happens. It is important that patients are provided with clear, accurate and timely information about how and when they will be admitted to hospital. This information will be included in a patient leaflet given to them by their GP when being referred or when they receive an appointment. The patient will be given clear instructions on how and when to contact the hospital to either accept or decline appointment and admission date, and the timeframe in which to do this. Patients will be given clear information on the consequences of not responding quickly to hospital communications, and the impact this could have on their waiting time. The patients leaflet will help the patient understand their responsibilities. On request the patients leaflet will be in a format appropriate to their additional support needs e.g. large print, community language. NHS Forth Valley has clear processes and procedures in place to ensure that patients can inform NHS Forth Valley of any changes in their details and/or their ability to attend appointment. • GP Practice staff must ensure that patients are aware that the location of
their appointment/treatment will be as described in the local Access Policy. If a patient does not accept a reasonable offer of appointment or

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
13
admission, this may have implications for the time they have to wait and may result in patient being returned to the referrer’s care.
• Where treatment occurs outside the Health Board area, or where clinics
are held infrequently, it will be made clear to patients the reasons at the beginning of the process of organising their appointment or admission.
• The patient leaflet will make patients aware that they must inform the
hospital of any changes to their details, e.g. name, address, postcode, telephone number or GP as soon as possible.
• GPs should ensure that patients are required to attend their agreed
appointment. Where the appointment is not required or they are unable to attend, they should inform the hospital at the earliest available opportunity.
• Patients should be made aware that they need to advise the booking office
when they will not be available to attend any appointment or admission to hospital for any periods of time, e.g. holiday or work commitments. If circumstances change after the referral is made they must inform the hospital at the first opportunity.
• Patients should be made aware that if they no longer wish to have their
outpatient appointment or admission, for whatever reason, they must advise the referrer and / or the hospital.
• Where patients do not attend for appointments and are returned to the
referrer the primary care team should have in place arrangements to follow up with the patient prior to re-referral.
• If NHS Forth Valley breaches the TTG, then the Health Board will provide
the patient or (where appropriate) the patient’s carer an explanation in writing of why the Health Board did not deliver the TTG. This will contain details of the advice and support available and details of how feedback, comments or complaints can be raised.
• Communications about patient clock adjustments are, required by law, to
be in writing unless there has been consent to receive communications via electronic medium.
• Additional needs will be noted in the patient management systems and on
the SCI gateway referral where appropriate.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
14
5.2 TO MANAGE REFERRALS EFFECTIVELY Improvements in waiting times will be delivered through an effective partnership between Primary and Secondary Care, with appropriate protocols and documentation in place. 5.2.1 Referrer • Prior to referral, the clinician will explain to the patient the range of options
to be considered. It will be explained that patients may not need to access specialist or consultant-led services.
• The referring clinician will advise patients of why they are being referred,
the expected waiting time and outline to patients their responsibilities for keeping appointments and the consequences of not attending.
• Where treatment cannot be provided locally and the patient needs to travel
elsewhere, the patient will be made aware of that as early as possible i.e. at the discussion with the patient regarding the agreement to treat.
• When the referrer is aware that the patient will be unavailable for a period
of time, the referrer will either delay sending the referral until they know the patient is available or clearly note the patient’s unavailability period on the referral. The referring clinician will ensure that the patient is available to commence treatment prior to lading to the waiting list.
• Referrals will be made electronically where possible and as per local
protocols. • GPs will make referrals to a clinical service and not a named consultant. • Wherever possible patients should be referred for diagnostic tests prior to
the referral being made for the first outpatient appointment. • Referrers must provide accurate, timely and complete information within
their referral (or they will be returned) including: • CHI identifier (unless they don’t have one) • Full demographic details which include:
o Name o Address o Ethnicity o Postcode o Up to date mobile and home telephone numbers o e-mail address o Preferred method of contacting patient i.e. letter, phone or e-mail o Patient’s unavailability period if applicable o Armed forces/veteran status if applicable o Additional Support Needs

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
15
5.2.2 Receiving location • There is a structured and transparent approach to the management of
referrals, scheduling and booking for all patients. • Referrals are triaged electronically where possible and must be done with
2 working days of receiving the referral. • The date of receipt of all referrals is recorded. • Systems and procedures are in place to triage and prioritise referrals in
accordance with referral category (e.g. Urgent/Routine) • A common pathway that allows advice or an appointment as appropriate is
in place. • Patients referred with suspected cancer must be marked as ‘URGENT-
SUSPICION OF CANCER’ and appropriate SCI referral completed. All suspected cancer patients are required to be seen and treated within the correct cancer waiting time standards see page 34.
• Armed Forces personnel, veterans and their families who move between
areas retain their relative point on the pathway of care within the national waiting time targets. Refer to Access to NHS Care for Armed Forces Personnel CEL 8 (2008) and CEL 3 (2009).
• Special exemptions that exist for Armed Forces veterans enable them to
receive priority treatment for any conditions which are likely to be related to their military service, subject to the clinical needs of all patients. Refer to HDL 2006 16 – Priority Treatment for War Pensioners and to Access to Health Services for Armed Forces Veterans – Extension to Priority Treatment CEL 8 (2008).
• Patients should be booked as close to the date of receipt of referral as
reasonably possible. 5.2.3 Receiving Clinician • It is the receiving clinician’s responsibility to communicate with the referrer
to offer advice on whether a referral is suitable. This will avoid unnecessary outpatient appointments.
• Any referrals received for a service that is not delivered in NHS Forth
Valley area will be returned to the original referrer with advice. Where it is judged that the referral would be more appropriately managed by another service provided by the Health Board, the referral will be passed to that service and the referrer informed by the consultant.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
16
• Receiving clinicians must ensure that waiting lists properly reflect their
clinical priorities and are managed effectively. • No patient will be added to the waiting list other than through the formal
referral process unless they are a transfer from Accident & Emergency or Minor Injuries unit.
5.2.4 Patient Transfer • The transfer of any part of a patient’s health care to other Health Board
areas or to the private sector must always be with the consent of the patient. The consultant will also be notified of this decision.
• Appropriate documentation and information should be provided to the
receiving Health Board or Private Sector provider where appropriate. With an agreed minimum data set between Health Boards.
• If the patient does not wish to be transferred, NHS Forth Valley must
ensure the patient is made a reasonable offer within current national guidance and within the current relevant waiting time standard.
• Private patients opting to transfer to NHS treatment must be referred back
to the GP to discuss their options and if appropriate referred to local NHS provider. The 18 Week RTT will then commence.
5.3 TO MANAGE WAITING LISTS EFFECTIVELY To support delivery of waiting times standards there is a need for NHS Forth Valley to manage their waiting lists effectively. This includes triaging of referrals, management of both new and return patients and accurate recording of clinic outcomes. • Systems, processes and resources are in place to ensure that all staff are
adequately trained to use local systems to help manage access to services using Standard Operating Procedures manual V1 2012.
• All new referrals will be triaged electronically within 2 working days with all
new appointments having a corresponding waiting list entry. • Patients will be seen within maximum standard waiting times and booked
in turn, according to clinical priority. • Details of patients on the waiting list who are admitted as emergency
admissions will be communicated to RTT booking team.
NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
17
• Patients will only be added to a waiting list if they are available to commence treatment.
• Systems and procedures will be in place to ensure that RTT booking team
are aware of any patient cancelled on the day of or after admission. • Systems and procedures will be developed to review and validate waiting
lists to ensure accuracy and that national and local access times are achieved.
• New outpatients will only receive a return appointment if there is a clinical
need. • The amount of return appointments will be monitored and reviewed. • All patients undergoing a procedure must indicate in writing that they
consent to treatment. • There will be a communication process in place to notify the referring
clinician on the decision to treat e.g. treatment to be provided, treatment delayed because medically unavailable.
• There are systems and procedures in place to communicate, manage and
record all outcomes at clinics, additions or alterations to the waiting list electronically.
• Patients who require treatment for different conditions may be on two
separate pathways. NHS Forth Valley has arrangements in place to identify what condition should take precedence.
• NHS Forth Valley regularly review clinic templates to ensure they reflect
changing demands. • Onward referral will be completed to ensure the receiving healthcare
provider has the necessary information to manage the patient treatment pathway. Any transfer of data must comply with NHS standards in relation to data security and confidentiality.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
18
5.4 TO USE INFORMATION TO SUPPORT IMPROVEMENTS IN SERVICE PROVISION
The ability to effectively monitor and manage services requires good quality data. This helps to inform performance and identify areas for future improvement. • The factors which influence waiting times, such as changes in referral
patterns, will be regularly monitored and management action taken in sufficient time to ensure waiting time standards is maintained.
• New to return and DNA ratios will be reviewed regularly and necessary
actions will be taken to address any issues. • There will be effective monitoring of efficiency and productivity and any
necessary change will be supported where required. • Benchmarking information should be used wherever possible in reviewing
clinic templates and efficiency.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
19
6. New Appointments Process NHS Forth Valley has 3 ways of making appointments patient focused booking, direct booking, and smart booking. 6.1 PATIENT FOCUSED BOOKING (PFB) PFB is where an acknowledgement letter is sent to the patients when the referral is received inviting them to make contact to make arrangements for their appointment. 6.2 SMART BOOKING MODEL – TELEPHONE BOOKING This model is where arrangements for the appointment are made by telephoning the patient to make the appointment or by writing to the patient asking them to phone in to make arrangements.
6.3 DIRECT BOOKING This model is where patients’ are sent a letter offering them an appointment date, the patient then calls to accept that date or to advice that they are not available and are then given a second offer. (Copy of letter appendix 4)
6.4 REASONABLE OFFER A “reasonable offer” of appointment is the offer of two or more different date of appointment for each stage of the patient’s treatment pathway, with a minimum of seven days notice from the date of each offer to the date of appointment. NHS Forth Valley offer patients appointments in other areas out with NHS Forth Valley Board area. The sites which are classed as reasonable offer sites are:
• NHS Lothian • NHS Lanarkshire • NHS Fife • NHS Tayside • NHS Greater Glasgow and Clyde • National Facilities e.g. Golden Jubilee National Hospital Clydebank,
Stracathro hospital (NHS Tayside). • Private sector - BMI hospitals
In exceptional circumstances e.g. specialist services and for capacity issues it may be that a reasonable offer will be any NHS facility within Scotland. In these circumstances NHS Forth Valley will be responsible for the cost of any transport and accommodation arrangements necessarily and reasonably incurred by the patient and their carer (if necessary). Other sites are not seen as locations where it is appropriate to adjust the waiting time clock.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
20
The selection criteria NHS Forth Valley has on deciding who to send to these sites are:
• Medically fit to travel • Clinical criteria • Patient choice
If a patient is offered treatment out of area the patient will receive early notice of this (preferably at the time of agreeing the treatment). If NHS Forth Valley offers a patient treatment in the above locations using the selection criteria and the patient subsequently turns down what is deemed a reasonable offer of appointment outwith NHS Forth Valley a period of unavailability will be recorded. Regardless of how an offer is made, all patients will be offered up to two dates for an appointment. Both of these dates should be at minimum of seven days in advance and within the waiting times standards set out in this policy. An offer of treatment for inpatient or day case out with the 12 weeks TTG will be a breach of the TTG and legislation does not allow for any adjustments to the treatment time clock once the patient has breached. Exceptions to these rules are:
• Urgent appointments e.g. suspected cancer – 7 days notice may not be possible
• Infrequent services – occurring every four weeks or less If a patient refuses a reasonable offer NHS Forth Valley will note the patient declined the offer and may either:
• Refer the patient back to their GP or • If it is not reasonable or clinically appropriate to refer them back to their
GP then the treatment time clock will be reset to zero.
6.4.1 Dates of Treatment A reasonable offer should include 2 dates more than seven days in the future. If the first date offered is accepted and no second date proposed, this is also a reasonable offer. Any letter offering an appointment will need to be delivered promptly and received by the patient at least seven days prior to the appointment date to ensure that the minimum standards for reasonable offers are met. It is important that the date on the letter is the date the letter is sent out.
NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
21
6.5 WAITING FOR SPECIFIC CONSULTANT Patients are referred to a clinical team and are seen by the appropriate member of that team rather than to an individual consultant. A reasonable offer off appointment relates to any competent clinician who is part of a consultant led service which NHS Forth Valley provides in that specialty or subspecialty. A named consultant will only be allocated to ensure continuity of care, patient’s safety or for other clinical or exceptional circumstances. It may be that the consultant that the patient sees at outpatient assessment may not be the consultant that carries out the inpatient/day case treatment. If a patient requests a named consultant (this number should be small) it is not a guarantee that the request will be accommodated. Where the patient prefers to wait for an appointment with a named consultant, rather than an appointment with another consultant, the patient’s wait might be longer than necessary. The patient should be made aware of the length of the wait they will experience in writing. It must be clear that this is the patients request and that they are full y aware of the consequences of their decision i.e. impact on waiting time. 6.6 INFREQUENT SERVICES A service which occurs every 4 weeks or less frequently, regardless of demand, should be treated as an Infrequent Service.
• Patients only needed to be offered one• If the patient refuses then the waiting time clock should be reset.
date at least 7 days in advance.
• If demand for a service exceeds capacity then patients should not be suspended and would breach.
6.7 ONE STOP SERVICES For patients seen on an inpatient or day case basis the date the patient agreed treatment and the date of the treatment will be the same, and the patient will have a zero wait recorded against the Treatment Time Guarantee. For the small number of patients where treatment cannot be undertaken on the day, the waiting time clock will continue.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
22
7. Unavailability
Unavailability is the period of time when the patient is considered to be unavailable for treatment. This can be for medical or patient advised
An example of this could be another condition which prevents the patient from undergoing treatment. An example would be at pre-assessment clinic 5 weeks into their treatment time wait the patient has high blood pressure and the clinicians determine this will take around 10 weeks to resolve. The patients waiting time clock will be paused for that 10 week period of time. Once the
reasons. Patients who are unavailable should not be added to the waiting list if there is no known end date to their unavailability. Adding patients to a waiting list could give the patient the impression that they are now in a queue for treatment. It is vital that patients who are on a waiting list but who become unavailable are monitored regularly. Under waiting times guidance, patients who are recorded as unavailable must be reviewed within 13 weeks if no end date to their availability is known. This review must be recorded which will automatically update the guarantee date. It is a legal requirement that the patient and the original referrer sent a letter informing them of any changes to the patient’s waiting list status. The waiting time clock will restart from the date the patient becomes available to accept an appointment or admission date.
7.1 INDEFINITE UNAVAILABILITY This is when the likely period of unavailability cannot be determined. In such cases the patient’s treatment time clock will not start, the patient may be referred back to the referrer or given a date when the service will contact them to discuss the unavailability and a decision made on the next step e.g. further appointment at outpatients or referred back to referrer.. NHS Forth Valley will write to the patient to advise them that they have been deemed indefinitely unavailable. A patient can also become indefinitely unavailable once treatment time clock has started. In this case the treatment time guarantee clock will stop and the treatment time guarantee cease to apply. This will be recorded with the reason for the unavailability i.e. social or medical. The availability of the patient will be reviewed within 12 weeks from the date the patient becomes unavailable for treatment and the outcome of the review will be recorded.
7.2 MEDICAL UNAVAILABILITY This is where a patient is unable to progress along their pathway for reasons that relate to their medical condition.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
23
patients blood pressure has stabilised enough for treatment to go ahead the patients waiting time will restart from week 5 with 7 weeks left to deliver the treatment time guarantee. The start date of the period of unavailability is the date the clinician made the decision that the patient was medically unavailable and is recorded. The end date is when the clinician decides the patient is now fit to undergo their treatment will also be recorded. A letter will also be sent to the patient informing them of the period of unavailability that has been applies to the treatment time guarantee. 7.3 PATIENT ADVISED Patient advised is when a patient is unable to progress along their pathway for reasons that relate to non medical circumstances. Patient advised relates to the patient’s situation and should not be used when staff are unavailable. This is where a patient has personal reasons for not being able to attend hospital such as when they are on holiday, exams, and work commitments or if they have carer responsibilities. The treatment time clock will be paused for the length of the period of unavailability. The start date will be the date when the patient has indicated the period of unavailability will start. The end date will be the date when the patient has indicated the period of availability will stop. In this situation the start date and end date of the unavailability should be recorded. If there is no exact end date available an estimate should be entered where possible. NHS Forth Valley will write to the patient informing them of the period of unavailability that has been applied to their treatment time clock. 7.4. VISITING CONSULTANT SERVICE This is a service where NHS Forth Valley commissions another Health Board to provide a service in the NHS Forth Valley area. If a visiting service cannot be provided due to severe weather that prevents the Consultant from travelling then the patient must be offered an appointment out with the NHS Forth Valley area within the treatment time guarantee. If the patient decides to wait until the next scheduled visiting consultant service, rather than attend an appointment for the agreed treatment outwith NHS Forth Valley, then the period from the date NHS Forth Valley is made aware of the patient’s decision and the date of the next scheduled visiting

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
24
consultant will not count against the treatment time guarantee. The patient will have patient advised unavailability from the period of time that the patient declined treatment elsewhere and the next visiting consultant service. NHS Forth Valley will send a letter to the patient confirming the periods of unavailability.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
25
8. Managing Appointments of Patient Who Did NOT Attend (DNA) 8.1 NEW OUTPATIENT APPOINTMENTS NHS Forth Valley will not routinely offer a further appointment to a patient who does not attend a new accepted outpatient appointment. The clinician will decide whether a further appointment is to be offered. There must be a clear clinical reason for offering a further appointment. • A copy of the standard letter should be sent to the patient and copied to
the referrer, advising them that they have been removed from the waiting list. The letter should also inform the patient that if they contact the service within 14 days, they will be reinstated on the waiting list. After this time, the patient should contact their GP if they still wish to be seen
If the patient is referred back into the service, a new waiting time clock will start from zero. Multiple re-setting of the clock if a patient continually does not attend their appointment is not expected. The patient should be referred back to the referrer. Any child who DNA’s (Did Not Attend) an outpatient appointment/Pre-operative Assessment/Admission without prior warning will be highlighted to the relevant Healthcare Professional as soon as possible. 8.2 ELECTIVE ADMISSIONS NHS Forth Valley will not routinely offer a further admission to a patient who does not attend for an accepted elective admission. The clinician will decide whether further admission date is to be offered. There must be a clear clinical reason for offering a further admission date, and this should be recorded in the patient’s notes. Patients undergoing cancer treatment or active surveillance for cancer should automatically be offered a further admission date. • A copy of the standard letter should be sent to the patient and copied to
the referrer, advising them that they have been removed from the waiting list and that they should contact their GP if they still wish to be seen.
If the patient contacts the RTT booking team and reports that they were not notified of the original admission date, and NHS Forth Valley is unable to demonstrate that the admission date was clearly communicated to the patient, the patient should be reinstated on the waiting list.
NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
26
8.3 MANAGING APPOINTMENTS OF PATIENTS WHO CANNOT ATTEND (CNA) If a patient has accepted a reasonable offer of an appointment or admission and then contacts the department to cancel before the appointment date: • The date of the cancellation and any explanatory text should be recorded. • The waiting time clock will be reset to zero from the date of cancellation
and another appointment should be offered within the pathway stage time limit. Further appointment will be discussed and agreed with the patient at the time of cancellation.
• If a patient requiring urgent treatment cancels their appointment and NHS
Forth Valley consider it reasonable and clinically appropriate to offer another appointment within the treatment time guarantee then they will not reset the clock. This will be the consultant’s decision.
If a patient asks to reschedule a reasonable offer of an appointment or admission for a third time the patient’s notes should be presented to the responsible clinician. The clinician should decide where a further appointment or admission is to be offered. There must be a clear clinical reason for offering a further appointment or admission. If a further appointment or admission is to be offered, the above process should be followed. If no further appointment or admission is to be offered: • The patient will be removed from the waiting list • A copy of the standard letter will be sent to the patient copied to referrer,
advising them that they have been removed from the waiting list and that they should contact their GP if they wish to be re-referred.
8.4 SHORT NOTICE APPOINTMENTS To make best use of resources on occasion a patient will be offered a “short notice” appointment i.e. less than 7 days notice to utilise slots. If a short notice appointment is offered and the patient is happy to accept, it is deemed as a “reasonable offer”. If however, a patient declines a “short notice” appointment, this should not result in any detriment to the patient and the waiting times clock for the patient is not affected in anyway. Short notice appointment may be made due to extra clinics/theatre lists being commissioned. This will only be when the Principles For Commissioning Additional Capacity Via Waiting List Sessions are adhered to (appendix 1)

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
27
8.5 CANCELLED BY HOSPITAL Cancellations resulting from hospital or operational circumstances will not result in any detriment to the patient e.g. cancellation of a clinic at short notice must result in the patient being made a further “reasonable offer” as soon as possible, The patients waiting time clock will not be affected in any way. In accordance with NHS Forth Valley’s leave policy for Medical and Dental staff, 6 weeks notice of planned leave/study leave will be given. Clinics will not be cancelled for any purpose except under exceptional or unavoidable circumstances e.g. sickness absence and sanctioned by the General Managers. 8.6 TRANSFER TO A DIFFERENT HEALTH BOARD This is when a patient’s ordinary residence changes to a different Health Board area and the patient requests to be treated within the different Health Board area (the board of their new residence). In such cases the Board must record the date the responsibility transferred to the different health Board. The treatment time guarantee will cease for the original Board. When the different Health Board receives the transfer request they must record the details of the request including date when the treatment time guarantee started. NHS Forth Valley will then write to the patient and advice them of the consequences of the calculation of the treatment time guarantee; this will be the start of the new treatment time guarantee. It may be in some circumstances the clinician will ask to see the patient before agreeing the treatment.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
28
9. Adding patients to the elective Waiting List 9.1 KEY PRINCIPLES A patient will only be added to an elective waiting list if they are clinically and socially ready for admission on the day the decision to admit is made. Patients will not be added to the waiting list if any of the following apply: • Patient is to lose weight • Patient is pregnant unless in the opinion of clinician the delay with surgery
would be detrimental to patients’ welfare • Patient is to have studies, tests or other investigations before surgery • Patient or Consultant wishes to delay surgery to further in future to see if
there is improvement in health will occur without the need for further intervention
• Patients not ready for surgery at present (including age–related
procedures) as per National Waiting Times Unit Good Practice Guidelines states “A patient is not to be placed on a waiting list as a holding device until the patient’s condition reaches an appropriate stage or the patient reaches a certain age”
When placing a patient on the waiting list the following information must be collected: • Patient demographic details • Patient telephone numbers • GP • Unavailability dates • Suitability for treatment elsewhere • Ability to accept short notice admission • Procedure description • Suitable for pooled list/clinician specifically wishes to do procedure • Clinical urgency or routine (current guidelines) • Intended management i.e. in-patient, day case, 23 hr discharge etc • Pre-operative assessment, requirement for High-Risk assessment etc • Any other information that will aid the smooth admission of the patient, and
any relevant medical history e.g. diabetic, latex allergy • Consultant name and signature • Date of clinic

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
29
10. Pre-operative assessment A patient who accepts a “reasonable offer” and “Did Not Attend” for pre-operative assessment on date given will be removed from Theatre List if arranged. This DNA will be followed up by the pre-operative assessment department to determine the reason and to confirm if the patient still wishes surgery. If the patient still wishes to have surgery: • If patient fails to attend second date for pre-op assessment advice will be
sought from the healthcare professional to whom the referral was made. If there are no clinical reasons for offering a further appointment, remove the patient from the waiting list and refer back to the referrer with copy of letter sent to patient.
If the patient no longer wishes surgery: • Seek advice from healthcare professional to whom the referral was made.
If there are no clinical reasons for offering a further appointment, remove the patient from the waiting list and refer back to the GP with copy of letter sent to patient.
• GP can re-refer the patient if required. If a further referral is received and a
new appointment offered, waiting time starts from zero.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
30
11. Admissions 11.1 COULD NOT ATTEND Patients will be contacted 7 days in advance or earlier (by letter or telephone) with an arranged date for surgery and a date for pre-operative assessment appointment prior to the admission date. It is recognised there are circumstances where the patient has to cancel. Patients will be made aware that under new “rules” the clock is reset to zero from the date of cancellation not date of appointment therefore it is in their own best interests to cancel as soon as possible.
• First CNA A patient accepts a “reasonable offer” of appointment however cannot attend; this is their first CNA. Waiting time is set to zero on the date when the patient makes contact. Details are recorded on the system and the patient should be made another “reasonable offer”.
• Second CNA Having accepted a further appointment, the patient cancels, this is their second CNA. Waiting time is set to zero on the date when the patient makes contact. Details are recorded on the system and the patient should be made another “reasonable offer”. Patients should be given the opportunity to cancel TWICE. If the patient cancels on a THIRD occasion and if clinically appropriate they will be refered back to GP. If instructed to return to GP care:
• GP and patient should be informed by letter that the patient is being
removed from the waiting list. • GP can re-refer the patient if required.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
31
11.2 DID NOT ATTEND If a patient accepts a “reasonable offer” of appointment but does not attend on the agreed date and time the following applies; • Record DNA details on system. • Verify the DNA with the patient by telephone or letter. If verified by
telephone confirm by letter with copy sent to GP. • Seek advice from the healthcare professional to whom the referral was
made. If there are no clinical reasons for offering a further appointment, remove the patient from the waiting list and refer back to the GP with copy of letter sent to patient.
• If the patient is to remain on the waiting list record the reason for DNA and
reset the clock to zero from the date of the original appointment. • Make the patient another reasonable offer of appointment. 11.3 SHORT-NOTICE ADMISSIONS To make best use of resources on occasions a patient will be offered a “short notice” admission i.e. less than 7 days to utilise theatre slots. If a “short notice” admission is offered and patient is happy to accept, it is deemed as a “reasonable offer”. If, however, a patient declines a “short notice” admission the waiting times clock for patient is not affected in any way and they should be made another “reasonable offer”. 11.4 CANCELLED BY HOSPITAL Cancellations resulting from hospital operational circumstances should not result in any detriment to the patient e.g. the cancellation of an admission at short notice must result in the patient being made a further “reasonable offer” as soon as possible. The patient’s waiting clock should not be affected in any way. In line with Good Practice Guidelines a patient cancelled in these circumstances will be given another date for admission as soon as possible. 11.5 COULD NOT WAIT Patients who, having registered their arrival for an elective admission and subsequently leave are deemed to have an outcome of ‘could not wait’ (CNW). There may be occasions where a patient has arrived for an admission as arranged but cannot wait to be seen. What should be recorded will vary dependent on whether it is a patient or service induced situation. Therefore local judgement will be necessary.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
32
• If the delay is caused by the late running of a theatre and that delay is much longer than a patient could reasonably be expected to wait then this should be recorded as ‘Cancelled by Service’ and the patient given another appointment within their original waiting time guarantee.
• If there is a minor delay in the theatre list, providing the patient has been
given guidance on the delay, and the patient is not willing to wait even a short length of time the outcome should be recorded as a ‘Could Not Attend’ (CNA). The patient should be made another reasonable offer but because this is a CNA their waiting time clock will be set to zero.
NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
33
12. Specialist services
12.1 NATIONAL HEALTH CANCER ACCESS TARGETS Better Cancer Care – An Action Plan was launched on 27 October 2008. Central to this was development of a comprehensive programme of work to assure the quality of care delivered. Two key and complimentary strands of this work are assuring compliance with national clinical standards and guidelines through robust clinical governance and delivery of 2 new cancer targets:
Target 1: 62-day target from referral to treatment for all patients referred urgently with a suspicion of cancer and for screened positive patients.
Target 2: 31-day target from decision to treat to first treatment for all patients diagnosed with cancer irrespective of their route of referral. These targets should be in place by quarter 4 (October – December) 2011.
• The Board receiving the referral is responsible for meeting 95%
compliance with the 62-day target. • The Board of first treatment is responsible for meeting 95% compliance
with the 31-day target. • A 5% tolerance level will be applied to the cancer targets to allow for
patients whom it is not appropriate or advisable to expedite through the system for the purpose of achieving target compliance.
• If a NHS Board chooses to outsource part of a patient’s care the
responsibility for delivering the target will remain with the relevant NHS Board.
The 62-day target applies to patients who:
• were referred urgently by a Primary Care clinician or General Dental
Practitioner (GDP) with a suspicion of cancer; • were detected through the National breast, bowel and cervical Screening
Programmes; or • attended A&E or were referred directly to hospital. The 31-day target applies to all patients irrespective of route of referral.
Patients should be included in the relevant waiting times target cohort when they have part of or their entire pathway within NHS Scotland. Patients who choose to have part of their pathway outwith NHS Scotland will be exempt from the relevant target as follows:

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
34
• If the part of their pathway outwith NHS Scotland is pre decision to treat
the patient will not be subject to the 62-day target, irrespective of route of referral.
• The patient will be subject to the 31-day target decision to treat to first treatment.
• If the part of their pathway outwith NHS Scotland is post decision to treat the patient will not be subject to the 62-day target or the 31-day target.
• As the patient is not subject to either of the cancer waiting times targets, data should not be submitted to ISD for these patients.
Exclusion Categories Patients can be excluded from performance calculations under three different exclusion criteria:
• Died before treatment • Refused all treatment • Clinical reasons – where patients breach the target because
medically they require a complex series of investigations (as opposed to the patient having gone through a circuitous pathway)
12.2 RAPID ACCESS CHEST PAIN CLINIC REFERRALS (RACPC) Since December 2007, Cardiac patients should wait no longer than 16 weeks from referral, from any source, through a Rapid Access Chest Pain Clinic (RACPC) to treatment.
From 2011 there is a maximum waiting time of 18 weeks from referral to treatment for all conditions, including cardiac.
12.3 OPHTHALMOLOGY - CATARACT TARGETS Cataract procedures are subject to a whole journey target of 18 weeks. NHS Forth Valley has local stage of treatment targets for the outpatient and inpatient/day case wait for first eye cataract, the total of which is 18 weeks.
For patients waiting for sequential bilateral treatment the waiting time for the second treatment is measured as a separate, 12 week TTG second pathway, it maybe that the agreement for the need for both treatments is made at the same time. The agreement to commence the second treatment is only made on or after the post-operative review for the first treatment. The waiting time for the second treatment should not start until that agreement is reached. The sequential treatment will no be managed as a Planned repeat.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
35
13. Priority Treatment for Military Veterans Under long-standing arrangements since 1953, war pensioners are given priority NHS treatment for the conditions for which they receive a war pension or gratuity, subject to clinical need. General Practitioners and NHS hospitals should give priority to war pensioners, both as out-patients and in-patients, for examination or treatment which relates to the condition or conditions for which they receive a pension or gratuity, unless there is an emergency case or another case demands clinical priority. Veterans should not be given priority treatment for conditions unrelated to service in the armed forces.
• The definition of a veteran is someone who has served at least one day in
the UK armed forces (including those who have served as reservists). • Some service-related health problems do not manifest themselves until
after a person has left the armed forces. Claims may be made for a war pension at any time after service termination.
• Where a person has a health problem as result of service to their country, it is right that they should get priority access to NHS treatment, based on clinical need. They should not need to have first applied, and become eligible for a war pension. Eligibility is related to people’s history in the services and not exclusively to deployment or taking part in conflict.
It is suggested that veterans are most likely to present with service-related conditions requiring: Audiology Services The guidance on priority treatment for war pensioners applies also to service related noise-induced hearing loss, which is accepted as related to service, but for which no award was paid because the level of disablement fell below the threshold for compensation. Lack of clarity about this group’s entitlement to priority treatment in the past may mean that some veterans, who have not previously applied for priority treatment, may come forward now. In addition, there will be future groups of veterans for whom hearing loss may be an issue. Mental Health Services Veterans sometimes do not seek treatment for service-related mental health problems until some years after discharge, including issues related to co-morbidity from substance misuse and alcohol addiction. It can be particularly difficult establishing whether a condition is due to service and its implications in providing treatment. Some community service pilots have been launched in England and there is work currently taking place to establish a pilot in Scotland.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
36
Orthopaedic Services Injuries incurred during a person’s time in the armed forces may, in some cases, present problems some time after discharge and require access to services such as physiotherapy, pain management, and rehabilitation. General Practitioners are asked, when referring a patient that they know to be a veteran to secondary or tertiary care for a condition that, in their clinical opinion, may be related to their armed forces service, to make this clear on referral (as long as the patient is content that the referral mentions their veteran status).

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
37
14. Definitions
14.1 WAITING TIME CLOCK The patient’s waiting time is referred to as a waiting time clock, using the following terms:
• Clock start The date at which the calculation of waiting time starts.
• Clock pause
Any period when the patient is unavailable for treatment (see ‘Unavailability’). These periods are discounted from the calculation of waiting time.
• Clock stop
The date at which the calculation of waiting time stops.
14.2 TREATMENT TIME GUARANTEE WAITING TIME A patient’s Treatment Time Guarantee (TTG) waiting time is a calculation based on the time that has elapsed between the date the patient agrees to proceed with the agreed treatment (agreement is usually at an outpatient clinic), and the date on which the patient starts to receive the agreed treatment on an inpatient or day case basis 14.3 STAGE OF TREATMENT WAITING TIMES Waiting times for separate stages of treatment are calculated based on the following:
• New outpatient appointment The time that has elapsed between the date the referral is received and the date the patient attends the appointment, discounting any periods of patient unavailability.
• Diagnostic test The time that has elapsed between the date the referral is received and the date the verified results of the test or procedure are reported and received by the clinician, discounting any periods of patient unavailability.
• Inpatient/Day case admission
The time that has elapsed between the date the patient agrees to proceed with the agreed treatment and the date on which the patient starts to receive the agreed treatment on an inpatient or day case basis, discounting any periods of patient unavailability.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
38
14.4 18 WEEKS REFERRAL TO TREATMENT WAITING TIME An 18 week patient pathway begins with receipt of the patient’s referral for treatment and ends when the patient’s treatment commences. A patient may be on more than one pathway at the same time for different conditions. There are two types of waiting time patient pathways:
• Non-Admitted Pathway The clock stops when the patient commences definitive treatment, outwith an inpatient or day case setting.
• Admitted Patient Pathway
The clock stops on the date on which the patient starts to receive the agreed treatment.
Appendix 2 highlights exclusions from the 18 weeks RTT.
NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
39
Appendix 1
1. The commissioning process will link in with the capacity plan and only where the proof of additional capacity can be evidenced will additional sessions be authorised. I.e. the capacity plan states the additional capacity requirements to be 6 sessions per month and 12 are requested then only 6 sessions will be granted.
Principles For Commissioning Additional Capacity Via Waiting List Sessions BACKGROUND AND CONTEXT Given the financial environment, the NHS is moving to a more efficiency and value for money based approach to reducing waiting times. The Waiting Times Operational Plan has to reassure the NHS Board that it is purchasing additional capacity and not resourcing activity that is already funded.
PRINCIPLES FOR COMMISSIONING WAITING LIST INITIATIVES Waiting list initiative payments sessions can only be provided on the basis that they purchase additional capacity.
2. Where reductions in waiting times are required i.e. for admitted pathways down from 9 weeks to 7 weeks, then reductions in the numbers waiting over target as detailed in LDP trajectory, must be achieved each month.
3. Waiting list sessions will be agreed with the general manager prior to taking place.
4. Consultant requirements a. Must engage with shared lists b. Fully engage with reducing cancellation rates c. Fully engage with SPSP d. Prepared to offer flexibility to meet service needs e. Must have agreed robust DCC and SPA objectives that are
recognised to meet contractual obligations
5. Payment forms will be signed off by the General Manager and Head of Patient Access.
6. Risks to the delivery of the targets must be highlighted by GMs/Service
leads to the Head of Patient Access as soon as they become aware of them.
7. Planned sessions cannot be cancelled within 6 weeks of taking place
unless authorised by the GM.
8. GMs/Service leads will need to plan and manage service providers’ holidays to avoid excessive reduction in capacity.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
40
9. Where waiting time targets are forecast to be breached, the reasons for the need will be assessed by the GM/Service lead i.e. over allocation of annual leave, sick leave, maternity leave, routine patients managed out of date order and reductions in throughput. These factors will be considered as service generated reductions in capacity and must be redressed within the service by harvesting productive opportunity.
10. Compliance: Each month the Head of Information and Capacity will
provide a detailed utilisation of funded sessions and waiting list sessions.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
41
Appendix 2
Exclusions from 18 Weeks Referral to Treatment Standard Referrals to the following services or some specific procedures are currently excluded and therefore do not trigger clock starts: • Allied Health Professionals (AHPs). Direct referrals to AHP services are
excluded from waiting time standards. However, AHPs may deliver services that are part of the overall waiting time standard e.g. as part of a consultant-led service.
• Assisted conception services. • Dental treatment provided by Undergraduate dental students. • Designated national specialist service for Scoliosis. • Direct access referrals to Diagnostic Services where the referral is not part
of a ‘Straight to Test’ referral pathway as there is no transfer of clinical responsibility to the Consultant-Led team.
• Exceptional Aesthetic Procedures which have been specifically excluded
in the CEL 27 (2011) Adult Exceptional Aesthetic Referral Protocol. • Genitourinary Medicine (GUM). • Homoeopathy. • Obstetrics. • Organ and Tissue transplants. Inclusions in 18 Weeks Referral To Treatment Standard To ensure consistency in reporting for the 18 week referral to treatment pathway across the service, the following also apply: • For reporting purposes, patients on a Cancer pathway should also be
reported through the 18 week referral to treatment pathway. • Where a termination of pregnancy is managed as a planned procedure i.e.
the patient is added to a waiting list, they should be included in 18WRTT. • All Outpatient appointments, New and Return, are required to have a
Clinic Outcome code applied.
NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
42
Appendix 3
Waiting list card
Waiting List Referral Date of Clinic: Date of decision to add: If as above enter
A/A CHI Number: CRN: (or affix Label) Name: Address:
Date of Birth: Patient’s Tel Numbers: Home: Mobile: Work/Other: Patient’s email address: GP Name: GP Address: Specialty: Consultant: Diagnosis: Intended Procedure: Suitable for pooled list: No Yes Is patient aware of being added to
the pooled list: No Yes
Suitable for Private Sector: No Yes
Details for Admission: Suitable For: GJNH (ORTHO ONLY)
DayCase 23 hrs stay Inpatient DOSA DBS May Req HDU Bed May Req ITU Bed GA LA
Jehovah Witness: No Yes
Pre-Op Assessment Required: No Yes
Consultant instructions for WL Dept:
Non Availability for Admission: See reverse for details. (Must be patient advised or authorised by clinician.)
NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
43
f referral if not from clinic: Ward ED MDT Meeting Specify Ward:
Additional Needs: Translator Language:
Impairment Needs Specify:
Other Specify:
Waiting List Pending: Decide to Admit:
Await Diagnostic Await Patient Decision Review Date:
Add to W/L (Date of review) No Yes
Clinicians Signature Date:
UNAVAILABILITY – Only Categories Allowed Waiting Times Unavailability • Medical – Medical Condition • Patient Advised Holiday • Patient Advised Personal Commitment • Patient Advised Carer Commitment • Patient Advised Academic Commitment • Patient Advised Jury Duty • Patient Advised Wishes Named Consultant • Patient Advised Wishes to be Treated Within Local Health Board • Patient Advised ‘Visiting Consultant Service’ – patient wishes to be seen at next scheduled service within Board of Residence Notes & Questions: 1. Other Medical Condition – general feedback on this confirms ICD10 look up is
not feasible without system developments. Therefore where a patient is medically unavailable details of medical reason should be collected locally in your PAS if at all feasible.
2. Patient Advised Personal Commitment – with detail of personal/social engagement collected locally in your PAS if at all feasible.
3. Patient Advised wishes to be treated within local Health Board – suggestion of changing this to “Patient Advised wishes to be treated at specific local Health Board location”?
4. Patient Advised ‘Visiting Consultant Service’ – patient wishes to be seen at next scheduled service within Board of residence. This is intended to be used when the patient advises they are unwilling to travel outwith the commissioning Board.

NHS Forth Valley Access Policy Board Version - September 2012 Review September 2013: R Grant
44
Appendix 4
Direct Booking letter Example

Forth Valley NHS Board 25 September 2012 This report relates to Item 10 of the Agenda
Review of Forth Valley NHS Board, Performance and Resources Committee and Board Seminar
Scheduling
(Paper presented by Professor Fiona Mackenzie, Chief Executive)
For Approval

SUMMARY 1. R E V I E W OF F OR T H V A L L E Y NH S B OA R D, PE R F OR M A NC E A ND R E SOUR C E S
C OM M I T T E E , A ND B OA R D SE M I NA R SC H E DUL I NG 2. PUR POSE OF PA PE R
The purpose of this paper is to seek Board approval to amend the current scheduling arrangements of the Forth Valley NHS Board, the Performance and Resources Committee and Board Seminars.
3. K E Y I SSUE S The role of Performance and Resources Committee (P&RC) was formally extended in June 2012 to strengthen governance and scrutiny arrangements in relation to financial and operational performance management and ensure that corrective actions are taken as required. In May 2012 the P&RC agreed to continue meeting on a monthly basis subject to review over the next 6-9 months. At its August meeting, in order to strengthen timely reporting of information and following the recent management restructuring, it was agreed that the sequencing of meetings and reporting timelines to the NHS Board would be reviewed. At the same time, the frequency of Board Seminars has been reviewed. At the Board Seminar held on 11th
September, a number of options were considered by Board members. The preferred was Option 2 - Alternate bi-monthly Board Meetings and Seminars and monthly P&RC meetings. It was also agreed that a business free month in the summer would be desirable. It is proposed this will be in July and timetables will be altered accordingly
4. F I NA NC I A L I M PL I C A T I ONS There are no specific financial implications.
5. W OR K F OR C E I M PL I C A T I ONS
There are no specific workforce implications.
6. R I SK A SSE SSM E NT A ND I M PL I C A T I ONS There are no specific risks identified to proposals outlined. The Board remains focussed on adopting a risk based approach. Non Executives will continue to hold Executives to account via the Forth alley NHS Board and P&RC.
7. R E L E V A NC E T O ST R A T E G I C PR I OR I T I E S The proposals outlined do not detract from NHS Forth Valley’s ability to manage and deliver against its strategic priorities.
8. R E L E V A NC E T O DI V E R SI T Y A ND / OR E QUA L I T Y I SSUE S There are no specific issues.

9. C ONSUL T A T I ON PR OC E SS The options are for discussion by Board Members at the Board Seminar in September and thereafter any changes and a preferred option will be presented to the NHS Board for approval.
10. R E C OM M E NDA T I ON(S) F OR DI SC USSI ON
The NHS Board members are asked to approve the proposal to: - • alternate Board meetings and Seminars maintaining the monthly Performance and
Resources Committee meetings noting future dates will be confirmed • have no Board or Committee meting in July
11. A UT H OR OF PA PE R /R E POR T :
Name: Designation:
Beverley Finch Head of Corporate Services
Approved by: Name: Designation: Fiona Ramsay Director of Finance

R E V I E W OF F OR T H V A L L E Y NH S B OA R D, PE R F OR M A NC E A ND R E SOUR C E S C OM M I T T E E , A ND B OA R D SE M I NA R SC H E DUL I NG OPTION ONE - COMMITTEE SCHEDULE – Bi-monthly Board meetings, monthly Seminars and P&RC meetings Finance Report Available
Performance & Resources Board Seminar Board Papers Out Meeting Papers Out Meeting Papers Out Meeting
21 Nov ‘12 30 Nov ‘12 7 Dec ’12 Board Development Day
4 Dec ‘12 20 Nov ‘12 27 Nov ‘12
21 Dec ‘12 11 Jan ‘13 18 Jan ‘13 22 Jan ‘13 29 Jan ‘13 24 Jan ‘13 29 Jan ‘13 5 Feb ‘13 5 Feb ‘13 12 Feb ‘13 12 Feb ‘13 19 Feb ‘13 22 Feb ‘13 26 Feb ‘13 5 March ‘13 5 March ‘13 12 March ‘13 22 March ‘13 26 March ‘13 2 April ‘13 2 April ‘13 9 April ‘13 9 April ‘13 16 April ‘13 23 Apr ‘13 30 April ‘13 7 May ‘13 7 May ‘13 14 May ‘13 22 May ‘13 28 May ‘13 4 June ‘13 4 June ‘13 11 June ‘13 11 June ‘13 18 June ‘13 24 June ‘13 25 June ‘13 2 July ‘13 2 July ‘13 9 July ‘13 22 July ‘13 30 July ‘13 6 Aug ‘13 6 Aug ‘13 13 Aug ‘13 13 Aug ‘13 20 Aug ‘13 22 Aug ‘13 27 Aug ‘13 3 Sept ‘13 3 Sept ‘13 10 Sept ‘13 23 Sept ‘13 24 Sept ‘13 1 Oct ‘13 1 Oct ‘13 8 Oct ‘13 8 Oct ‘13 15 Oct ‘13 22 Oct ‘13 29 Oct ‘13 5 Nov ‘13 5 Nov ‘13 12 Nov ‘13 22 Nov ‘13 26 Nov ‘13 3 Dec ‘13 3 Dec ‘13 10 Dec ‘13 10 Dec ‘13 17 Dec ‘13 23 Dec ’13 OPTION TWO - COMMITTEE SCHEDULE Alternate bi-monthly Board Meetings & Seminars and monthly P&RC meetings Finance Report Available
Performance & Resources Board Seminar Board Papers Out Meeting Papers Out Meeting Papers Out Meeting
21 Nov ‘12 30 Nov ‘12 7 Dec ’12 Board Development Day
4 Dec ‘12 20 Nov ‘12 27 Nov ‘12
21 Dec ‘12 11 Jan ‘13 18 Jan ‘13 22 Jan ‘13 29 Jan ‘13 24 Jan ‘13 29 Jan ‘13 5 Feb ‘13 12 Feb ‘13 19 Feb ‘13 22 Feb ‘13 26 Feb ‘13 5 March ‘13 12 March ‘13 19 March ‘13 22 March ‘13 26 March ‘13 2 April ‘13 9 April ‘13 16 April ‘13 23 Apr ‘13 30 April ‘13 7 May ‘13 14 May ‘13 21 May ‘13 22 May ‘13 28 May ‘13 4 June ‘13 11 June ‘13 18 June ‘13 24 June ‘13 25 June ‘13 2 July ‘13 9 July ‘13 16 July ‘13 22 July ‘13 30 July ‘13 6 Aug ‘13 13 Aug ‘13 20 Aug ‘13 22 Aug ‘13 27 Aug ‘13 3 Sept ‘13 10 Sept ‘13 17 Sept ‘13 23 Sept ‘13 24 Sept ‘13 1 Oct ‘13 8 Oct ‘13 15 Oct ‘13 22 Oct ‘13 29 Oct ‘13 5 Nov ‘13 12 Nov ‘13 19 Nov ‘13 22 Nov ‘13 26 Nov ‘13 3 Dec ‘13 10 Dec ‘13 17 Dec ‘13 23 Dec ’13

OPTION THREE - COMMITTEE SCHEDULE Alternate bi-monthly Board Meetings and P&RC meetings and quarterly Seminars Finance Report Available
Performance & Resources Board Board Seminar Papers Out Meeting Papers Out Meeting Papers Out Meeting
21 Nov ‘12 30 Nov ‘12 7 Dec ’12 20 Nov ‘12 27 Nov ‘12 Board Development Day
4 Dec ‘12
21 Dec ‘12 15 Jan ‘13 22 Jan ‘13 22 Jan ‘13 29 Jan ‘13 24 Jan ‘13 29 Jan ‘13 5 Feb ‘13 22 Feb ‘13 26 Feb ‘13 5 March ‘13 22 March ‘13 26 March ‘13 2 April ‘13 16 April ‘13 23 April ‘13 23 Apr ‘13 30 April ‘13 7 May ‘13 22 May ‘13 28 May ‘13 4 June ‘13 24 June ‘13 25 June ‘13 2 July ‘13 16 July ‘13 23 July ‘13 22 July ‘13 30 July ‘13 6 Aug ‘13 22 Aug ‘13 27 Aug ‘13 3 Sept ‘13 23 Sept ‘13 24 Sept ‘13 1 Oct ‘13 15 Oct ‘13 22 Oct ‘13 22 Oct ‘13 29 Oct ‘13 5 Nov ‘13 22 Nov ‘13 26 Nov ‘13 3 Dec ‘13 23 Dec ’13 OPTION FOUR - COMMITTEE SCHEDULE Alternate bi monthly Board meetings and P&RC meetings and monthly Seminars Finance Report Available
Performance & Resources Board Board Seminar Papers Out Meeting Papers Out Meeting Papers Out Meeting
21 Nov ‘12 30 Nov ‘12 7 Dec ’12 20 Nov ‘12 27 Nov ‘12 Board Development Day
4 Dec ‘12
21 Dec ‘12 15 Jan ‘13 22 Jan ‘13 22 Jan ‘13 29 Jan ‘13 24 Jan ‘13 29 Jan ‘13 5 Feb ‘13 12 Feb ‘13 19 Feb ‘13 22 Feb ‘13 26 Feb ‘13 5 March ‘13 12 March ‘13 19 Mar ‘13 22 March ‘13 26 March ‘13 2 April ‘13 9 April ‘13 16 April ‘13 23 Apr ‘13 30 April ‘13 7 May ‘13 14 May ‘13 21 May ‘13 22 May ‘13 28 May ‘13 4 June ‘13 11 June ‘13 18 June ‘13 24 June ‘13 25 June ‘13 2 July ‘13 9 July ‘13 16 July ‘13 22 July ‘13 30 July ‘13 6 Aug ‘13 13 Aug ‘13 20 Aug ‘13 22 Aug ‘13 27 Aug ‘13 3 Sept ‘13 10 Sept ‘13 17 Sept ‘13 23 Sept ‘13 24 Sept ‘13 1 Oct ‘13 8 Oct ‘13 15 Oct ‘13 22 Oct ‘13 29 Oct ‘13 5 Nov ‘13 12 Nov ‘13 19 Nov ‘13 22 Nov ‘13 26 Nov ‘13 3 Dec ‘13 10 Dec ‘13 17 Dec ‘13 23 Dec ’13

OPTION FIVE - COMMITTEE SCHEDULE Alternate bi-monthly Board Meetings and P&RC meetings and bi-monthly Seminars Finance Report Available
Performance & Resources Board Board Seminar Papers Out Meeting Papers Out Meeting Papers Out Meeting
21 Nov ‘12 30 Nov ‘12 7 Dec ’12 20 Nov ‘12 27 Nov ‘12 Board Development Day
4 Dec ‘12
21 Dec ‘12 15 Jan ‘13 22 Jan ‘13 24 Jan ‘13 29 Jan ‘13 5 Feb ‘13 12 Feb ‘13 19 Feb ‘13 22 Feb ‘13 26 Feb ‘13 5 March ‘13 22 March ‘13 26 March ‘13 2 April ‘13 9 April ‘13 16 April ‘13 23 Apr ‘13 30 April ‘13 7 May ‘13 22 May ‘13 28 May ‘13 4 June ‘13 11 June ‘13 18 June ‘13 24 June ‘13 25 June ‘13 2 July ‘13 22 July ‘13 30 July ‘13 6 Aug ‘13 13 Aug ‘13 20 Aug ‘13 22 Aug ‘13 27 Aug ‘13 3 Sept ‘13 23 Sept ‘13 24 Sept ‘13 1 Oct ‘13 8 Oct ‘13 15 Oct ‘13 22 Oct ‘13 29 Oct ‘13 5 Nov ‘13 22 Nov ‘13 26 Nov ‘13 3 Dec ‘13 10 Dec ‘13 17 Dec ‘13 23 Dec ’13 Note – Meetings of the P&RC for 2013 will be held on a Tuesday, except the January meeting which is a Friday. Board Meetings and Board Seminar dates are all Tuesdays





























