Embed Size (px)
Citation preview
703
Introduction
Colon-specific drug delivery by oral route has gained increased importance from the last two decades, to treat local diseases associated with colon and for potential delivery of drugs used to treat colon associated ail-ments (Vincent & Suman, 2002; Maroni et al., 2012). Traditionally, colon targeting is achieved using prodrug approach, pH-sensitive drug delivery, time-dependent delivery systems and microbial degradation meth-ods using tablets, capsules, multiparticulates, micro-spheres and liposomes (Vemula & Veerareddy, 2009). Combination of two approaches has greater flexibility in the design of site specific delivery to colon than single
method. Combining both methods can result in the opti-mum formulation which shows no release during the ini-tial lag period but releases the drug completely and in a sustained fashion within the residence time of the tablet in gastrointestinal tract (Asghar et al., 2009).
Time dependent and pH dependent approaches have been explored with wide variety of polymers of which hydroxypropyl methylcellulose (HPMC) and Eudragits are important. There have also been reports where the investigators have combined both the approaches to achieve desired release profile from the tablets. Diclofenac sodium compression coated tablets (Chickpetty et al., 2010), flurbiprofen microspoges (Orlu et al., 2006),
ReseaRch aRtIcle
Formulation, evaluation and pharmacokinetics of colon targeted pulsatile system of flurbiprofen
Prabhakar Reddy Veerareddy1 and Sateesh Kumar Vemula2
1Department of Pharmaceutics, Chaitanya College of Pharmacy Education and Research, Kishanpura, Hanamkonda, Warangal, Andhra Pradesh, India and 2Department of Pharmaceutics, Jangaon Institute of Pharmaceutical Sciences, Yeshwanthapur, Jangaon, Warangal, Andhra Pradesh, India
abstractObjective: The intent of the present investigation is to develop colon targeted compression coated flurbiprofen pulsatile release tablets that retard the drug release in the upper gastro intestinal system but progressively release in the colon.Materials and methods: Flurbiprofen core tablets were prepared by direct compression method and were compression coated with hydroxypropyl methylcellulose and Eudragit S100. The formulation is optimized based on the in vitro drug release study and further evaluated by X-ray imaging and pharmacokinetic studies in healthy humans for colonic delivery.Results and discussions: The optimized formulation showed negligible drug release (7.26 ± 0.05%) in the initial lag period followed by progressive release (99.27 ± 0.46%) for 24 h. The X-ray imaging study in human volunteers showed that the tablets reached the colon without disintegrating in the upper gastrointestinal tract. The Cmax of colon targeted tablets was 10792.62 ng/mL at Tmax 10 h where as in case of immediate release tablets the Cmax was 15684.79 ng/mL at Tmax 3 h signifies the ability of compression coated tablets to target the colon.Conclusion: Development of pulsatile release compression coated tablets using combination of time dependent and pH sensitive approaches was suitable to target the flurbiprofen to colon.Keywords: Accelerated stability studies, lag period, pH dependent release, pharmacokinetics, time dependent release, X-ray imaging study
Address for Correspondence: Prabhakar Reddy Veerareddy, Department of Pharmaceutics, Chaitanya College of Pharmacy Education and Research, Kishanpura, Hanamkonda, Warangal, Andhra Pradesh, India-506001. E-mail: [email protected]
(Received 27 March 2012; revised 21 June 2012; accepted 27 June 2012)
Journal of Drug Targeting, 2012; 20(8): 703–714© 2012 Informa UK, Ltd.ISSN 1061-186X print/ISSN 1029-2330 onlineDOI: 10.3109/1061186X.2012.712131
Journal of Drug Targeting
20
8
703
714
27March2012
21June2012
27June2012
1061-186X
1029-2330
© 2012 Informa UK, Ltd.
10.3109/1061186X.2012.712131
2012
Colon targeted pulsatile system of flurbiprofen
P. R. Veerareddy and S. K. Vemula
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.

704 P. R. Veerareddy and S. K. Vemula
Journal of Drug Targeting
time dependent insulin delivery system (Maroni, 2009), meloxicam microsponges (Srivastava et al., 2012), pH sensitive nanospheres of budesonide (Makhlof et al., 2009), indomethacin matrix tablets (Asghar et al., 2009) and time dependent 5-fluorouracil tablets (Wu et al., 2007b) are some of the recent colon targeted drug delivery systems.
Colon specific drug delivery can be achieved by the development of coated matrix tablets or coating the directly compressed tablets, either by film coating or compression coating. Among these types of tablets com-pression coated tablets offer coating methodology free of solvents which is safe and inexpensive that doesn’t require special coating equipment and the coating formed through compression offers higher stability as compared to film coating. Compression coating is a sim-ple method as compared to other methods like coating of tablets with different polymers and chemical conjuga-tion of the drug to achieve colon delivery (Hashem et al., 2011). HPMC is a synthetic release retardant that is widely used as an extended release agent in the pharmaceutical industry (Sinha et al., 2007). Eudragit S100 (ED) with a threshold pH 7 was selected as the additional coating material. ED is able to withstand the lower pH values of stomach (1–3.5) and small intestine (5–7), but dissolves at the neutral or slightly alkaline pH of the terminal ileum (7) (Chourasia & Jain, 2003; Shukla & Tiwari, 2012).
Non-steroidal anti-inflammatory agents are one of the choices of drugs for colonic drug delivery through oral route to treat colonic inflammation. Flurbiprofen (FLB) is a non steroidal anti-inflammatory drug (NSAID) used to treat inflammation and pain related to colon (Orlu et al., 2006). The frequent intake of NSAIDs like FLB leads to gastric ulceration, bleeding and other gastric compli-cations (Philip et al., 2008). Hence the development of colonic delivery of FLB is appropriate to reduce its side effects and achieve high local drug concentrations at the afflicted site in the colon, optimal therapeutic effective-ness and good patient compliance (El-Kamel et al., 2008). The purpose of the present study was to develop a novel pulsatile HPMC- ED compression coated tablets for colon delivery of drugs by combining time dependent and pH-sensitive methods, which shows complete and slow release for 24 h and also retards the release of the drug in the upper gastro intestinal tract (GIT). To achieve the desired release profile present study utilizes pH depen-dent release and time dependent release approaches.
Materials and methods
MaterialsFlurbiprofen was a gift sample from FDC Limited, Mumbai, India. HPMC K4M and Eudragit S100 were gift samples from Matrix laboratories, Hyderabad, India. All other chemicals used were of analytical grade.
Analytical method development: HPLC methodThe Chromatographic procedures were carried out on Water’s HPLC equipped with C18 column and UV
detector by modified reported method (Wang et al., 2007). Mobile phase used for the analysis consists of phosphate buffer pH 3.5: acetonitrile aqueous solution in the ratio of 35:65. They were filtered before use through a 0.45 µm membrane filter and pumped through the column Symmetry C18 (X Terra, 4.6 × 150 mm) 5 µm, at a flow rate of 1 mL/min. Stock solution (1 mg/mL) of FLB was prepared using the mobile phase. Working standards of 200, 400, 600, 800 and 1000 µg/mL solutions of FLB were prepared using the mobile phase. Prior to the injec-tion of the drug solution, the column was equilibrated for at least 30 min with the mobile phase flowing through the system. The analysis was performed at ambient tempera-ture and the run time was set to 8 min. The eluents were monitored at 254 nm using UV detector.
Powder characterizationPowder mixtures of different formulations were evalu-ated for angle of repose, bulk density, tapped density and compressibility index. The fixed funnel method was employed to measure the angle of repose (θ) and it was calculated using the following formula:
Tanh
rθ =
(1)
in which, θ is the angle of repose, h is the height of the cone and r is radius of the cone base. To measure the angle of repose, a funnel was fixed to a stand so that the lower tip of funnel was 2.5 cm above the surface. A graph paper was placed on a flat surface. The powder blend was allowed to fall freely on the graph paper through the funnel (6.9 cm diameter), till the tip (8 mm diameter) of heap formed just touches the funnel. The radius of heap was noted and from this angle of repose was determined. Angle of repose less than 30° suggests free flowing prop-erties of the material.
The bulk density of a powder is determined by mea-suring the volume of a known mass of powder sample that may have been passed through a screen, into a 50 mL graduated cylinder. Tapped densities of powder samples were determined by a tap density apparatus (Intelli, Kshitij Innovations, India). The apparatus was set for 500 tappings for 5 min at stroke height 20 mm (100 strokes/min). The compressibility index (Carr’s Index) is a mea-sure of the propensity of a powder to be compressed. It is determined from the bulk and tapped densities and is calculated using the following formulas:
Carr’s Index = [( )/ ] 100ρ ρ ρtap b tap− ×
(2)
in which, ρb is bulk density and ρ
tap is tapped density.
Preparation of core and compression coated tabletsFLB core tablets were prepared by direct compression method. FLB and excipients other than glidant and lubricant were accurately weighed, passed through 60 mesh sieve and mixed in a poly bag for 5–10 min. The obtained blend was lubricated with talc and magnesium
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.
Colon targeted pulsatile system of flurbiprofen 705
© 2012 Informa UK, Ltd.
stearate for another 5 min and the resultant mixture was directly compressed (compression force 5000 kg) into tablets with 7 mm round flat punches using 16 sta-tion rotary tabletting machine (Cmach, Ahmedabad, India, model no M/C CMB16STN, M/C NO 51/50). The amount of FLB was 100 mg and the final weight of the tablet was adjusted to 175 mg (Table 1). Then the core tablets were compression coated with different compo-sitions of coats given in Table 2. Here half the quantity of the coating material was placed in the die cavity, then the core tablet was carefully placed in the centre of the die cavity and finally it was filled with the other half of the coating material. The coating material was compressed using 10 mm round, flat and plain punches to give the compression coated tablets.
Evaluation of physical parametersThe designed formulations were studied for their physical properties like weight variation, hardness and friability. For estimating weight variation, 20 tablets of each formulation were weighed using an electronic weighing balance (AW 120, Shimadzu Corporation, Japan). The hardness of six tablets was measured using Monsanto tablet hardness tester. Friability was deter-mined on ten tablets in a Roche friabilator (Electrolab, Mumbai, India).
Determination of drug contentFor estimation of drug content, ten tablets were crushed, and 100 mg of the powder was accurately weighed and transferred to a 100 mL volumetric flask. Initially about 50 mL of mobile phase was added to the volumetric flask and allowed to stand for 6–8 h with intermittent shak-ing to ensure complete solubility of the drug. Then the
volume was made up to 100 mL with mobile phase fol-lowed by filtration and analysis for FLB content by the developed HPLC method.
In vitro dissolution studyThe release of FLB from compression coated tablets was carried out using USP XXIV Type I dissolution appara-tus (Electro lab, TDT-08L) at a rotation speed of 50 rpm, and a temperature of 37 ± 0.5°C. In order to simulate the gastrointestinal transit conditions, the tablets were sub-jected to different dissolution media. Initially, the drug release was carried out for 2 h in 0.1 N HCl, 2 h in buffer pH 5.5 and finally in phosphate buffer pH 7.4 up to 24 h (Luppi et al., 2008). At specific time intervals, 5 mL of the sample was withdrawn and replaced by an equal volume of fresh pre-warmed dissolution medium. The samples were filtered through 0.45 µm membrane filter (Millipore, USA) and analyzed by HPLC method using UV detector at 254 nm.
In vitro release kineticsThe data obtained from the in vitro dissolution studies was fitted to zero order, first order and Higuchi models to explain the pattern and the release mechanism from the formulations (Wu et al., 2007). Koresmeyer–Peppas model is one of the mathematical expressions, used to understand the mechanism of drug release from these formulations (Ravi et al., 2008). The Koresmeyer–Peppas equation is as follows:
M M Kttn/ α =
(3)
in which, Mt/Mα
is the fractional amount of drug released at time t, K is a kinetic rate constant, and n is the dif-fusional exponent that characterizes the mechanism of drug release (Asghar et al., 2009).
The mean dissolution time (MDT) is defined as the sum of different release fraction periods (release areas) during dissolution studies divided by the initial load-ing dose and is calculated by the following equation (Talukder & Fassihi, 2008):
MDTt M
M
midi
i n
i
i n=×
=
=
=
=
∑∑
∆
∆1
1
(4)
where i is the dissolution sample number, n is the num-ber of dissolution sample time, t
mid is the time at the
Table 1. Composition of FLB core tablets.Ingredients Quantity (mg)Flurbiprofen 100Spry dried lactose 50.5Crosspovidone 17.5Sodium lauryl sulphate 1.75Talc 3.5Magnesium stearate 1.75Core weight (mg) 175Core thickness (mm) 3.01 ± 0.02Core diameter (mm) 7.04 ± 0.01
Table 2. Composition of compression coatings.Formulation Codea
HPMC E50 (mg)
HPMC E100 (mg)
HPMC K4M (mg)
HPMC K15M (mg)
HPMC K100M (mg)
Eudragit S100 (mg)
Coat weight (mg)
Coat thickness (mm)
Coat diameter (mm)
F1 80 – – – – – 200 0.65 ± 0.01 10.01 ± 0.07F2 – 80 – – – – 200 0.64 ± 0.02 10.04 ± 0.02F3 – – 80 – – – 200 0.63 ± 0.01 10.06 ± 0.05F4 – – – 80 – – 200 0.64 ± 0.02 10.11 ± 0.10F5 – – – – 80 – 200 0.62 ± 0.01 10.04 ± 0.06F6 – – 80 – – 40 200 0.65 ± 0.01 10.05 ± 0.03aEach compression coat contains 2% talc, 1% magnesium stearate remaining spray dried lactose to make up the coat weight of 200 mg.
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.

706 P. R. Veerareddy and S. K. Vemula
Journal of Drug Targeting
midpoint between i and i = 1, and ΔM is the amount of drug dissolved between i and i = 1.
Drug–polymer interaction studiesTo study the possible interaction between FLB and polymers, Differential scanning calorimetry (DSC) study was carried out on pure drug and the optimized formulation (F6) and the thermograms were obtained using DSC (Perkin-Elmer, Shelton, U.S). The analy-sis was performed under nitrogen (nitrogen flow rate 50 mL/min) in order to eliminate oxidative and pyrro-lytic effects at a standard heating rate of 15°C/min over a temperature range of 50–350°C. The Fourier trans-form infrared spectra (FTIR) of FLB and optimized formulation (F6) recorded between 400 and 4000 cm−1 on FTIR to detect the drug-excipient interactions. The FTIR spectra for the test samples were obtained using KBr disk method using an FTIR spectrometer (Perkin Elmer FTIR, Perkin Elmer Inst. USA). The resultant spectra were compared for any possible changes in the peaks of the spectra.
Stability studiesTo assess the drug and formulation stability, stabil-ity studies were done according to ICH guidelines. Optimized formulation F6 was sealed in aluminum packaging coated inside with polyethylene, and three replicates were kept in the humidity chamber main-tained at 40 ± 2oC and 75 ± 5% RH for 6 months (ICH Q1A; Chaudhary et al., 2011). Samples were collected after three and 6 months of storage and analyzed for the drug content and in vitro dissolution rate (Mathews, 1999) and they were subjected to statistical analysis using paired t-test to test the significance of difference at 0.05 level of significance (LS).
In vivo X-ray imaging studiesX-ray imaging technique was used to monitor tablets throughout the GI system. The inclusion of radio-opaque material into the solid dosage form enables it to be visualized by the use of X-rays. By incorporating bar-ium sulphate into the pharmaceutical dosage forms, it is possible to follow the movement, location and integ-rity of the dosage form after oral administration by plac-ing the subject under a fluoroscope and taking a series of X-rays at various time points. Three healthy male human volunteers, between 22 and 30 years of age and 50–70 kg body weight, were participated in X-ray imag-ing studies. They were non-alcoholics, non-smokers and have not taken any drugs. The purpose of the study was fully explained to the volunteers and the volunteers had given their written consent. Each subject ingested barium sulphate containing optimized formulation (F6) orally with 200 mL water, after an overnight fast. The tablets were visualized using X-rays. Abdominal radio-graphs were taken after 30 min, 3 h, 6 h, 8 h and 24 h in all the subjects. The volunteers were served with food; 2 h (breakfast) and 4 h (lunch) after the administration
of the tablet (Tugcu-Demiröz et al., 2004). The institu-tional ethical committee (Approval No. 338-04/JIPS/JNG/IHEC/2011) approved the protocol of the X-ray imaging study of colon targeted compression coated tablets of FLB.
Pharmacokinetics in healthy volunteersIn the present study, a crossover study was followed in which twelve human volunteers were participated and divided into two equal groups (group I and group II). All the volunteers were non-alcoholics, non-smokers, in the age group of 20–35 years and body weight ranging from 55 to 65 kg. To ensure that the volunteers were free from both liver and kidney dysfunction the required biochemical tests were carried out and no one was on any drug treatment ten days prior to participation in the study. In the first phase of study group I volunteers (n = 6) received an immediate release tablet (dose 100 mg) whereas group II (n = 6) volunteers received compression coated colon targeted tablet (dose 100 mg). The volunteers received the tablets on an empty stomach with sufficient water, and then a stan-dard breakfast was served after 2 h of the study. At regular time intervals lunch and dinner were served in standard quantity. In the second phase of the study, after ten days washout period, group I volunteers received compression coated colon targeted tablet and group II volunteers received immediate release tablet. Blood samples were collected at 0, 0.5, 1, 2, 3, 4, 5, 6, 8, 10, 12, 18 and 24 h in vials in both the cases. The insti-tutional ethical committee (Approval No. 338-05/JIPS/JNG/IHEC/2011) approved the protocol of the in vivo study of colon targeted compression coated tablets of FLB in human volunteers.
HPLC analysis of FLB in human plasmaThe collected blood samples were centrifuged at 4000 rpm for 15 min and the serum was separated and transferred to 5 mL micro centrifuge tubes. To the 1 mL of above serum 1 mL of acetonitrile was added and centrifuged for 10 min at 3000 rpm and the supernatant liquid was separated and stored at −40°C until the analysis of sample for unchanged drug. Then the quantitative determination of FLB in human plasma was performed using HPLC method by injecting the supernatant liquid into the HPLC column (loop volume 20 µL and flow rate 1 mL/min). The analysis was performed at ambient temperature and the run time was set to 8 min and the eluents were monitored at 254 nm using UV detector. The standard curve was constructed using standard drug solutions ranging from 200–1000 ng/mL by above method and was used to estimate FLB in human plasma. A good linear relationship was observed between the concentration of FLB and the peak areas of FLB with a high correlation coefficient (R2 = 0.9955).
Pharmacokinetic analysisThe required pharmacokinetic parameters were calculated using FLB plasma concentration-time data and by using
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.

Colon targeted pulsatile system of flurbiprofen 707
© 2012 Informa UK, Ltd.
the plot of time versus plasma concentration, the peak plasma concentration (C
max) and the time to reach peak
plasma levels (Tmax
) were obtained. Other pharmacoki-netic parameters were calculated using Kinetica software (Kineitca 20000 version 3.0, InnaPhase Corporation, 2000) based on the following equations (Gibaldi & Perrier, 1990). From linear part in the elimination phase of a semi-log plot of concentration versus time, the elimination rate constant (ke) was calculated and the corresponding biological half life (t
1/2) was calculated using the given equation.
tke1 2
0 693/
.=
(5)
The area under the concentration versus time curve (AUC) from 0 to t h was calculated by applying the trapezoidal rule and then the AUC extended to infinity (0–∞ h) that represents the extent of bioavailability of FLB was calculated using following equations.
AUC C t dtt
t
0 0− = ∫ ( )
(6)
AUCAUC C
ket t
00
−∞−=
+
(7)
where as Ct is the last observed plasma concentration of
FLB at t h.The area under first moment curve (AUMC) was
obtained from the plot of product of plasma drug con-centration and time versus time. The AUMC
0–t was cal-
culated by trapezoidal rule and AUMC0–∞
was calculated using following equation.
AUMC AUMC C t ke C ket t t0 02
−∞ −= + +/ /
(8)
The mean residence time (MRT) is defined as the average amount of time spent by the drug molecules in the body before being eliminated under constant clearance condi-tions and it was calculated using the following equation.
MRTAUMC
AUC=
(9)
Statistical analysisThe calculated pharmacokinetic parameters of both immediate release and colon targeted tablets of FLB were subjected to statistical analysis using analysis of variance (ANOVA) to test the significance of difference. A value of p < 0.05 was considered statistically significant.
In vitro–in vivo correlationThe in vitro–in vivo correlation (IVIVC) of dissolution rate and the absorption rate has been widely used in the quality control and formulation development of oral formulations. IVIVC can also serve as a surrogate for bioequivalence studies of formulations saving time and money in the drug development process. In the pres-ent study the in vitro cumulative percent of FLB release of optimized formulation F6 was compared against the
extent of absorption, i.e. cumulative AUC values of the same formulation.
Results
Powder characterizationThe powder mixtures of different formulations were evaluated for angle of repose, bulk density, tapped den-sity and compressibility index. The values were shown in Table 3. The bulk density and tapped density values ranged from 0.324 to 0.337 and 0.382 to 0.407 respec-tively. The results of angle of repose and % Carr’s index ranged from 26.72 ± 3.15 to 30.96 ± 1.04 and 11.70 to 18.18 respectively.
Evaluation of physical parametersThe physical properties of FLB-HPMC compression coated tablets were given in Table 4. From the weight variation test, it was found that the weight variation of the tablets was in the range of 374.20 ± 3.04 to 374.95 ± 3.30. The pharmaco-poeial limit for weight variation in tablets should not more than 5% of the average weight. The average percentage deviation of all tablet formulations was found to be within the above mentioned limit and hence all formulations passed the uniformity of weight as per official require-ments (Indian Pharmacopoeia, 1996). The hardness of the tablets was found to be in the range of 6.23 ± 0.12 to 6.37 ± 0.25 kg/cm2. Another measure of tablets strength is friability. Conventional compressed tablets that loss less than 1% of their weight are generally considered accept-able. The percentage friability for all formulations was below 1%, i.e. 0.09–0.22%, indicating that the friability is
Table 3. Characterization of powder mixture.
FormulationAngle of
Reposea (°)
Bulk Density (g/cc)
Tapped Density (g/cc)
Carr’s Index (%)
F1 26.90 ± 0.70 0.336 0.392 14.29F2 29.23 ± 2.74 0.324 0.382 15.18F3 26.72 ± 3.15 0.333 0.407 18.18F4 30.96 ± 1.04 0.335 0.393 14.76F5 28.84 ± 3.37 0.337 0.382 11.78F6 28.21 ± 1.28 0.335 0.397 15.62aAll values represent mean ± standard deviation, n = 3.
Table 4. Physical properties of FLB colon specific compression coated tablets.
Formulation
Weight variationa
(mg)Hardnessb (Kg/cm2)
Friability (%)
Drug contentc (%)
F1 374.60 ± 3.49 6.23 ± 0.12 0.18 99.50 ± 1.31F2 374.20 ± 3.04 6.27 ± 0.32 0.22 99.16 ± 0.33F3 374.80 ± 3.41 6.23 ± 0.25 0.09 98.48 ± 0.56F4 374.55 ± 3.43 6.37 ± 0.25 0.13 98.87 ± 1.46F5 374.95 ± 3.30 6.27 ± 0.12 0.09 99.30 ± 2.00F6 374.35 ± 3.10 6.33 ± 0.23 0.13 98.20 ± 1.21aAll values represent mean ± standard deviation, n = 20.bAll values represent mean ± standard deviation, n = 6.cAll values represent mean ± standard deviation, n = 3.
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.
708 P. R. Veerareddy and S. K. Vemula
Journal of Drug Targeting
within the prescribed limits. The tablets were found to con-tain 98.20 ± 1.21% to 99.50 ± 1.31% of the labeled amount indicating uniformity of drug content.
Effect of HPMC amount on compression coat integrityFrom the cumulative mean percent of FLB released from compression coated tablets containing varying amounts of HPMC K4M (20, 40, 60, 80 and 100 mg), incorporation of 80 mg of polymer in the total tablet weight was found to be satisfactory to formulate a tablet with good integrity and satisfactory in vitro release.
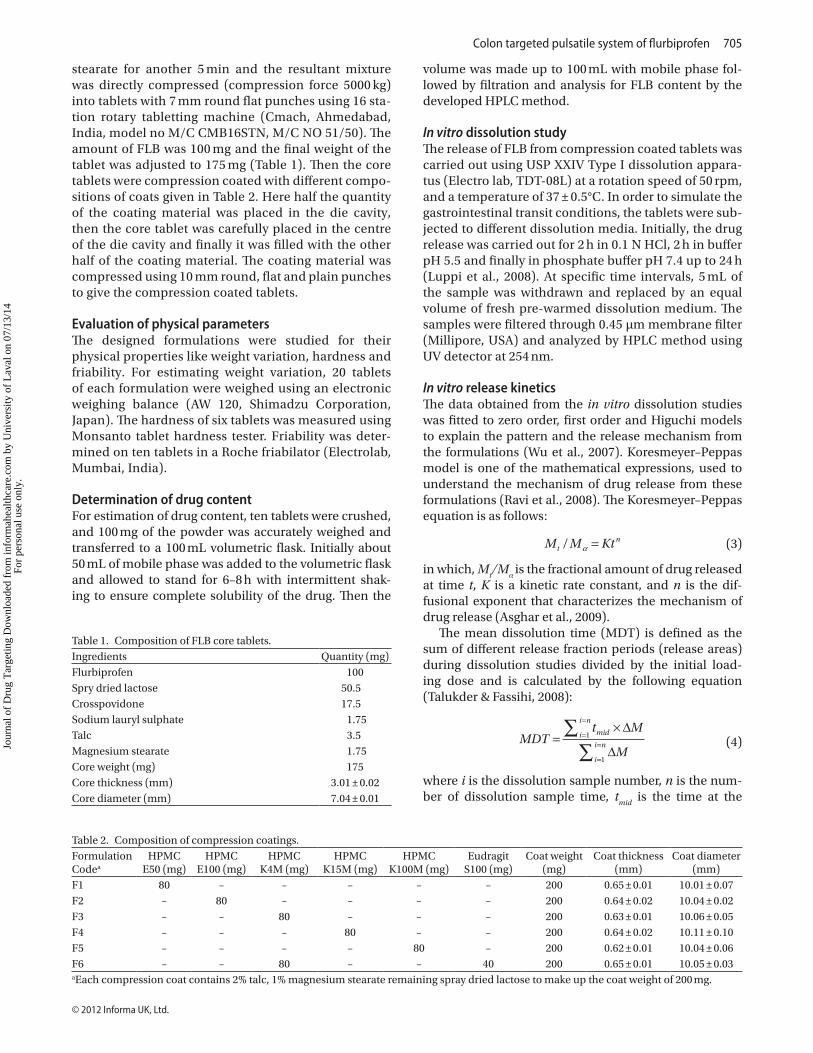
Effect of HPMC viscosity grade on compression coat integrityFigure 1 showed the release profiles of FLB from the HPMC compression coated tablets of different viscosity grades (F1-F5) and it was found to vary from 7.17 ± 0.25 to 98.17 ± 0.29% after 5 h of testing in simulated gastric and intestinal fluids and the percent drug release was increased gradually after 5 h and it was found to be 73.68 ± 2.14 to 39.44 ± 1.06% in 24 h.
Effect of Eudragit S100 incorporation on HPMC compression coatingIn order to evaluate the effect of eudragit S100 incor-poration on HPMC compression coating, 40 mg of Eudragit S100 was incorporated in compression coat
of formulation F6. Figure 1 shows the comparison of release profiles of FLB from the HPMC compression coat with and without eudragit S100. From the in vitro dissolution studies, the formulation F6 containing 20% eudragit S 100 showed 7.26 ± 0.05% drug release in 5 h and it was progressively increased to 99.27 ± 0.46% in 24 h.
In vitro release kineticsThe values of K, and r2 (correlation coefficient of the regression analysis) of zero order, first order and Higuchi models of designed formulations were given in Table 5. The n values calculated for different formulations were found in the range of 1.1591–3.3101. The MDT values were found to be 2.35–11.73. The values of K, n, r2, and MDT from the dissolution data of designed formulations were given in Table 6.
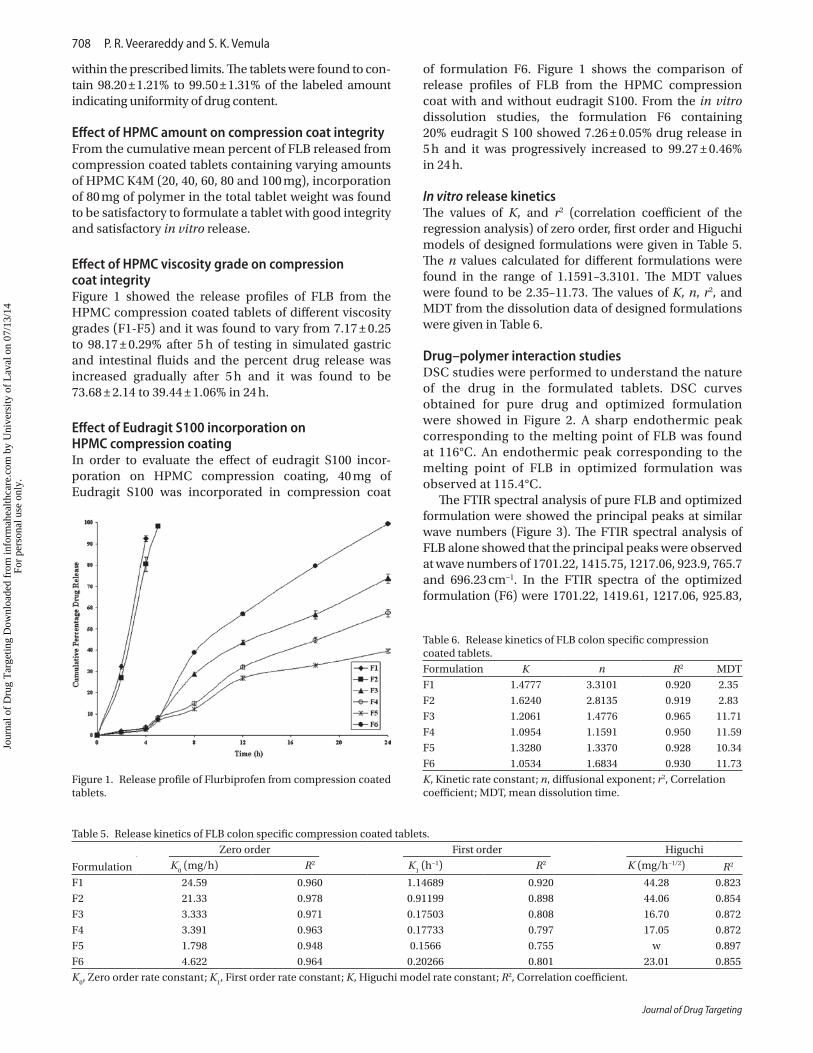
Drug–polymer interaction studiesDSC studies were performed to understand the nature of the drug in the formulated tablets. DSC curves obtained for pure drug and optimized formulation were showed in Figure 2. A sharp endothermic peak corresponding to the melting point of FLB was found at 116°C. An endothermic peak corresponding to the melting point of FLB in optimized formulation was observed at 115.4°C.
The FTIR spectral analysis of pure FLB and optimized formulation were showed the principal peaks at similar wave numbers (Figure 3). The FTIR spectral analysis of FLB alone showed that the principal peaks were observed at wave numbers of 1701.22, 1415.75, 1217.06, 923.9, 765.7 and 696.23 cm−1. In the FTIR spectra of the optimized formulation (F6) were 1701.22, 1419.61, 1217.06, 925.83,
Figure 1. Release profile of Flurbiprofen from compression coated tablets.
Table 6. Release kinetics of FLB colon specific compression coated tablets.Formulation K n R2 MDTF1 1.4777 3.3101 0.920 2.35F2 1.6240 2.8135 0.919 2.83F3 1.2061 1.4776 0.965 11.71F4 1.0954 1.1591 0.950 11.59F5 1.3280 1.3370 0.928 10.34F6 1.0534 1.6834 0.930 11.73K, Kinetic rate constant; n, diffusional exponent; r2, Correlation coefficient; MDT, mean dissolution time.
Table 5. Release kinetics of FLB colon specific compression coated tablets.
Formulation
Zero order First order HiguchiK
0 (mg/h) R2 K
1 (h−1) R2 K (mg/h−1/2) R2
F1 24.59 0.960 1.14689 0.920 44.28 0.823F2 21.33 0.978 0.91199 0.898 44.06 0.854F3 3.333 0.971 0.17503 0.808 16.70 0.872F4 3.391 0.963 0.17733 0.797 17.05 0.872F5 1.798 0.948 0.1566 0.755 w 0.897F6 4.622 0.964 0.20266 0.801 23.01 0.855K
0, Zero order rate constant; K
1, First order rate constant; K, Higuchi model rate constant; R2, Correlation coefficient.
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.
Colon targeted pulsatile system of flurbiprofen 709
© 2012 Informa UK, Ltd.
765.7 and 696.23 cm−1 wave numbers were observed. However, some additional peaks were observed with physical mixtures, which could be due to the presence of polymers.
Stability studiesIn view of the potential utility of the formulation, stabil-ity studies were carried out at 40 ± 2°C and 75 ± 5% RH for 6 months to assess their stability. After storage of 3 and 6 months, the formulation was subjected to a drug assay and in vitro dissolution studies (Table 7) and from the statistical analysis there was no significant difference between before and after storage (p < 0.05).
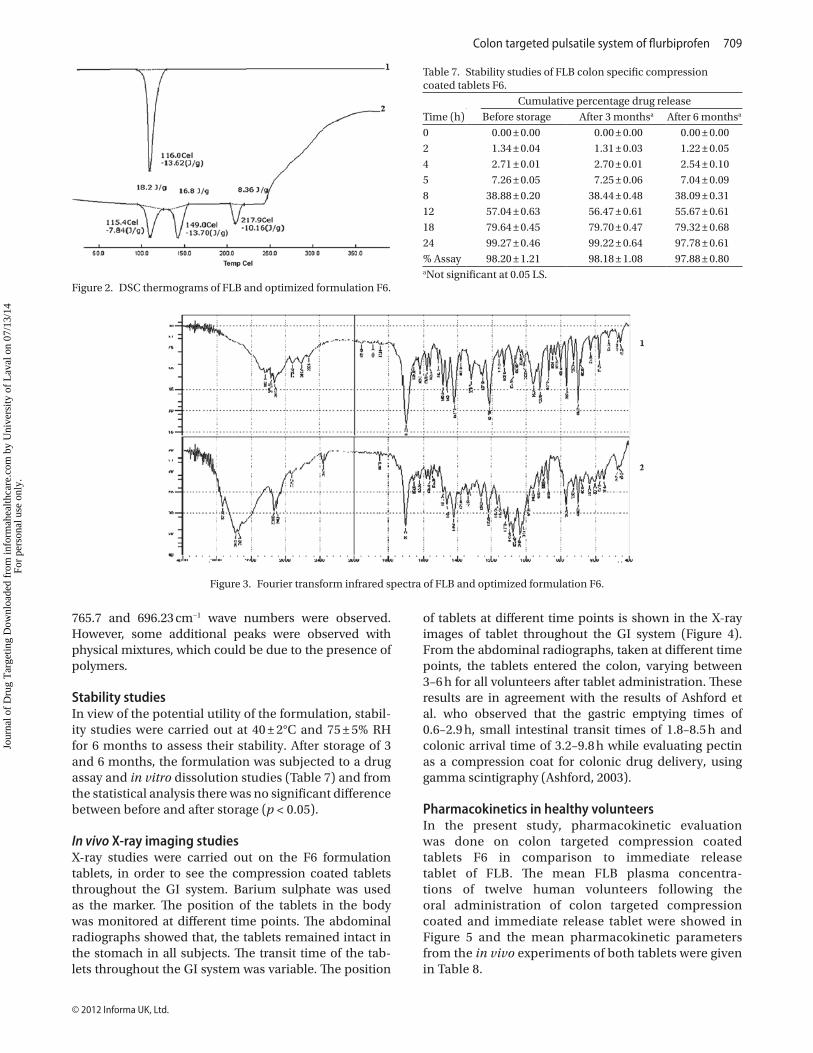
In vivo X-ray imaging studiesX-ray studies were carried out on the F6 formulation tablets, in order to see the compression coated tablets throughout the GI system. Barium sulphate was used as the marker. The position of the tablets in the body was monitored at different time points. The abdominal radiographs showed that, the tablets remained intact in the stomach in all subjects. The transit time of the tab-lets throughout the GI system was variable. The position
of tablets at different time points is shown in the X-ray images of tablet throughout the GI system (Figure 4). From the abdominal radiographs, taken at different time points, the tablets entered the colon, varying between 3–6 h for all volunteers after tablet administration. These results are in agreement with the results of Ashford et al. who observed that the gastric emptying times of 0.6–2.9 h, small intestinal transit times of 1.8–8.5 h and colonic arrival time of 3.2–9.8 h while evaluating pectin as a compression coat for colonic drug delivery, using gamma scintigraphy (Ashford, 2003).
Pharmacokinetics in healthy volunteersIn the present study, pharmacokinetic evaluation was done on colon targeted compression coated tablets F6 in comparison to immediate release tablet of FLB. The mean FLB plasma concentra-tions of twelve human volunteers following the oral administration of colon targeted compression coated and immediate release tablet were showed in Figure 5 and the mean pharmacokinetic parameters from the in vivo experiments of both tablets were given in Table 8.
Figure 2. DSC thermograms of FLB and optimized formulation F6.
Figure 3. Fourier transform infrared spectra of FLB and optimized formulation F6.
Table 7. Stability studies of FLB colon specific compression coated tablets F6.
Time (h)Cumulative percentage drug release
Before storage After 3 monthsa After 6 monthsa
0 0.00 ± 0.00 0.00 ± 0.00 0.00 ± 0.002 1.34 ± 0.04 1.31 ± 0.03 1.22 ± 0.054 2.71 ± 0.01 2.70 ± 0.01 2.54 ± 0.105 7.26 ± 0.05 7.25 ± 0.06 7.04 ± 0.098 38.88 ± 0.20 38.44 ± 0.48 38.09 ± 0.3112 57.04 ± 0.63 56.47 ± 0.61 55.67 ± 0.6118 79.64 ± 0.45 79.70 ± 0.47 79.32 ± 0.6824 99.27 ± 0.46 99.22 ± 0.64 97.78 ± 0.61% Assay 98.20 ± 1.21 98.18 ± 1.08 97.88 ± 0.80aNot significant at 0.05 LS.
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.
710 P. R. Veerareddy and S. K. Vemula
Journal of Drug Targeting
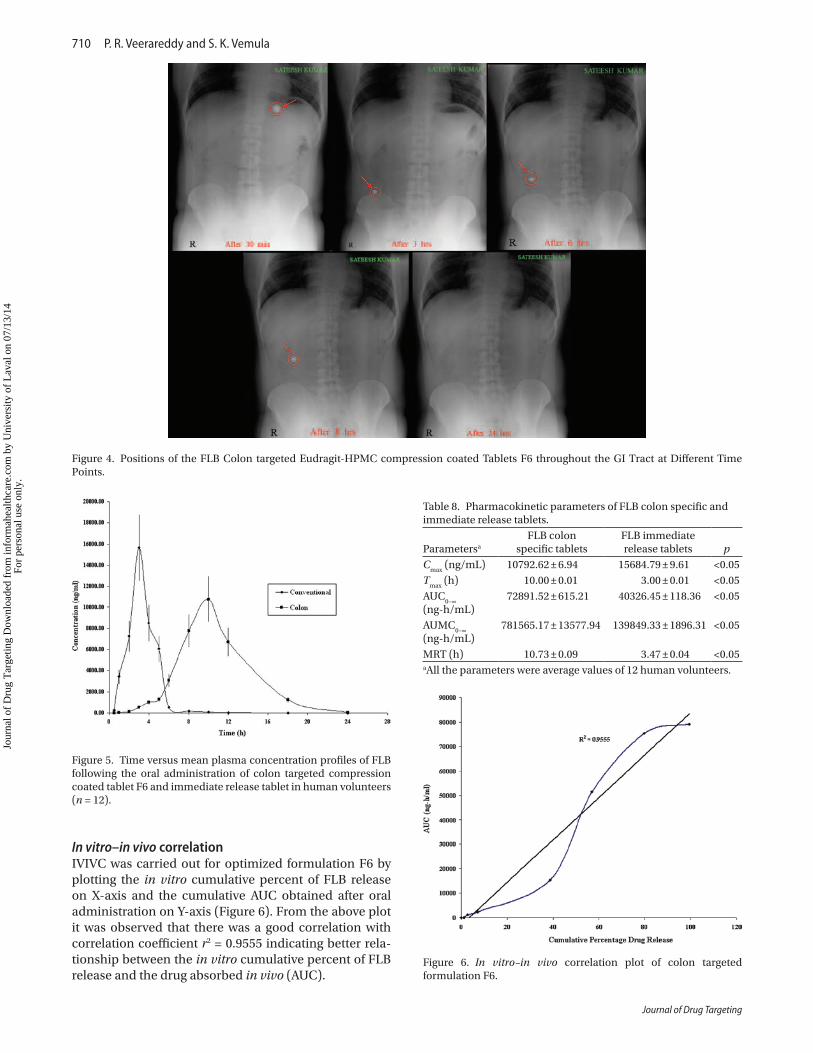
In vitro–in vivo correlationIVIVC was carried out for optimized formulation F6 by plotting the in vitro cumulative percent of FLB release on X-axis and the cumulative AUC obtained after oral administration on Y-axis (Figure 6). From the above plot it was observed that there was a good correlation with correlation coefficient r2 = 0.9555 indicating better rela-tionship between the in vitro cumulative percent of FLB release and the drug absorbed in vivo (AUC).
Figure 4. Positions of the FLB Colon targeted Eudragit-HPMC compression coated Tablets F6 throughout the GI Tract at Different Time Points.
Figure 5. Time versus mean plasma concentration profiles of FLB following the oral administration of colon targeted compression coated tablet F6 and immediate release tablet in human volunteers (n = 12).
Table 8. Pharmacokinetic parameters of FLB colon specific and immediate release tablets.
Parametersa
FLB colon specific tablets
FLB immediate release tablets p
Cmax
(ng/mL) 10792.62 ± 6.94 15684.79 ± 9.61 <0.05T
max (h) 10.00 ± 0.01 3.00 ± 0.01 <0.05
AUC0–∞
(ng-h/mL)
72891.52 ± 615.21 40326.45 ± 118.36 <0.05
AUMC0–∞
(ng-h/mL)
781565.17 ± 13577.94 139849.33 ± 1896.31 <0.05
MRT (h) 10.73 ± 0.09 3.47 ± 0.04 <0.05aAll the parameters were average values of 12 human volunteers.
Figure 6. In vitro–in vivo correlation plot of colon targeted formulation F6.
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.

Colon targeted pulsatile system of flurbiprofen 711
© 2012 Informa UK, Ltd.
Discussion
The angle of repose and Carr’s compressibility index were measured to determine the flow properties of powder mixtures of all formulations and the angle of repose <35 and Carr’s compressibility index <23 indicate fair to pass-able flow properties of the powder mixture (Staniforth & Aulton, 2007). Appreciable flow properties facilitate the flow of powder mixture during the tabletting process.
Weight variation, thickness, hardness and friability of all the tablet formulations were complied with pharmacopoe-ial standards, so all the tablets were with acceptable physical characteristics. In weight variation test, the pharmacopoeial limit for tablets is not more than 5% of the average weight. The average percentage deviation of all tablet formulations was found to be within the specified limit and hence all the formulations passed the uniformity of weight as per the offi-cial requirements of Indian Pharmacopoeia, 1996. From the physical characterization, all the tablet formulations were uniform in hardness, friability and drug content uniformity.
The cumulative mean percent of FLB released from compression coated tablets containing varying amounts of HPMC K4M was estimated to optimize the amount of polymer suitable to produce colon specific drug delivery. The formulation containing 80 mg of HPMC K4M was con-sidered better among other formulations (HPMC K4M 20, 40, 60 and 100 mg) to produce colon targeted drug delivery of FLB with good physical integrity. In a study reported in the literature, 100 mg of HPMC K4M in the coat weight of 200 mg has shown around 4 h lag time in the release of the drug (Wu et al., 2007). In our study, 80 mg of HPMC K4M in the coat weight of 200 mg showed similar lag time. Due to the hydrophobicity of FLB similar lag time has been observed with low amount of HPMC K4M. As the drug’s hydrophobicity increases the time taken for the dissolution of the core tablet increases, resulting in slow release of the drug from the compression coated tablet. The drug delivery systems targeted to the colon should not only protect the drug from being released in the physiological environment of stomach and small intestine, but also release the drug in colon. The optimized compression coat weight for the bet-ter drug release profiles suitable for colon targeted release of FLB was studied by formulating the compression coated tablets with different coat weights. From the dissolution study, it was found that 200 mg is the suitable compression coat weight for colon targeting.
In vitro dissolution study of F1-F5 formulations show the effect of different viscosity grades of HPMC on release profiles of FLB from the HPMC compression coated tab-lets (Figure 1). A minimal amount of the drug (<10%) is released in the physiological environment of stomach and small intestine and progressive drug release was observed in the colonic region with high viscosity grades of HPMC. Low viscosity grades resulted in immediate drug release. Similar observation was reported in a study with 5-fluorouracil where the compression coating with different HPMC grades showed more sustained release with increasing viscosity grades (Wu et al., 2007). From
the above formulations, the formulation F3 showed 8.24% drug release in the initial lag period (5 h) followed by 73.68% drug release for 24 h in a sustained fashion. Formulations with high viscosity HPMC formed swollen gels with substantial integrity resulting in a controlled drug release. Swollen gel offers better control of water and drug diffusion. Tablets coated with low viscosity grades of HPMC, lacked strength and eroded quickly after swelling. In the present investigation, HPMC K4M, HPMC K15M and K100M showed negligible drug release in the initial lag period. Only HPMC K4M showed com-plete release within 24 h where as K15M and K100M did not release the drug completely within 24 h, which is the normal residence time of solid dosage form in the colon (Sarasija & Hota, 2000; Vyas & Roop, 2006).
The effect of ED incorporation in HPMC compres-sion coat (F6) was showed in Figure 1. The presence of ED in hydrophilic compression coat retarded the initial swelling of the coat in acidic to weakly acidic pH, but in alkaline pH enhancement in drug release rate was observed due to the dissolution of ED from the coat with time, resulting in a porous coat structure that resulted in a faster and controlled drug release in the target area (Vyas & Roop, 2006). As the proportion of HPMC is substituted with ED in the coat, the per-centage of drug release is retarded in the upper part of the gastrointestinal tract and the percentage of drug release in the physiological environment of colon was increased. Literature report on compression coated tablets of diclofenac sodium also showed retardation of drug release as the ED percentage is increased in the compression coat (Chickpetty, 2010). This might be due to the fact that on coming in contact with dissolu-tion fluid, in first 5 h of dissolution study ED prevents initial swelling of HPMC present in the coat. After 5 h of dissolution study ED dissolves, HPMC hydrates, swells up and, erodes and drug release increases in the colon target area. From the in vitro dissolution studies, the formulation F6 contains 20% ED showed less than 10% drug release in 5 h and it was progressively increased to 100% in 24 h that indicates only a small amount of drug was released in stomach and small intestine, and a large amount of dose was released in colonic environment. Hence, the formulation F6 containing HPMC K4M-ED compression coat, i.e. combination of time-dependent and pH-sensitive methods was considered as optimized formulation for colon targeted delivery of FLB.
The drug release kinetics revealed high correlation coefficient values for zero order than first order indicat-ing that the drug release from compression coated tablets followed zero order pattern. Zero order release was also observed in a study with 5-fluorouracil using HPMC in the compression coat (Wu et al., 2007). The high regres-sion value of Higuchi model ensured that the release of drug from compression coated tablets followed diffusion mechanism. The n values calculated for different formu-lations indicating a supercase-II transport. The MDT was higher for formulations with high viscosity HPMC grades
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.

712 P. R. Veerareddy and S. K. Vemula
Journal of Drug Targeting
compared to low viscosity grades of HPMC, indicating better controlled release. It is known from the literature that with increasing viscosity grades of the polymer in the compression coat the gel thickness and imperviousness increases in the dissolution medium resulting in a higher MDT (Talukder & Fassihi, 2008).
DSC studies were performed to understand the nature of the drug in the formulated tablets. Thermogram of the optimized formulation did not show any significant shift in the endothermic peak when compared to pure drug, indicating that there was no physical change in drug in the HPMC matrices. From the FTIR spectral analysis all the principal peaks observed in pure drug were present in the FTIR spectra of the optimized formulation (F6) and some additional peaks were observed with physical mixtures, which could be due to the presence of polymers. These results suggest that there is no interaction between the drug and polymers used in the present study.
After storage of 3 and 6 months, the formulation was subjected to a drug assay and in vitro dissolution stud-ies and the data showed that there was no significant change in formulation in the sense of drug content and dissolution behavior. The in vivo X-ray imaging results showed that the tablets (F6) reached the colon without disintegrating in the upper region of the GI system in all subjects. The X-ray images showed that the tablets slowly disintegrated throughout the colon after reaching it. Colon targeted drug delivery systems have been visual-ized widely using gamma scintigraphy in the literature where the tablet integrity is lost in the colon (Ghimire et al., 2011). In the present study, X-ray imaging studies showed gradual reduction in the size of the tablet with time until it disappeared completely (Figure 4).
The in vitro drug release studies of HPMC-ED compres-sion coated colon targeted tablets of FLB (F6) revealed that they provide significant amount of drug release specifically in the physiological environment of colon without loss in the stomach and small intestine. Further the pharmacoki-netic evaluation of these colon targeted tablets in healthy volunteers is needed to prove the ability of site specific release of FLB in the colon. From the evaluation, T
max rep-
resents rate of absorption and AUC is related to extent of absorption while C
max is related to both (Grahnen, 1984).
The extent of absorption is an important factor of a formu-lation hence the AUC is a key parameter for comparative bioavailability study analysis and the others like T
max and
Cmax
are also important features that related to the thera-peutic efficiency of drugs (Krishnaiah et al., 2003a). MRT is also considered in the present pharmacokinetic analy-sis because it gives the tendency of drug to remain in the body. From the pharmacokinetic evaluation, after oral administration of immediate release tablet FLB appeared almost immediately within 30 min while in case of colon targeted compression coated tablets, it took about 5 h for FLB to appear in considerable concentration in plasma. The immediate release (core) tablets disintegrated very fast in GI tract and resulted in quick absorption of the drug
from stomach and small intestine, thereby producing peak plasma concentration C
max of 15684.79 ng/mL at 3 h T
max.
On oral administration of colon targeted tablets (F6), FLB reached peak concentration (C
max = 10792.62 ng/mL) at
10 h Tmax,
which revealed that the colon targeted tablet did not allow the release of FLB in stomach and small intestine. The shift in the T
max to a higher value is typical for the colon
targeted drug delivery systems (Krishnaiah et al., 2003). But after reaching the colonic environment, drug release from the colon targeted tablet by the disintegration of swollen cellulose tablets was progressive. From the above results, achievement of colon specific drug release might be due to fact that on coming in contact with dissolution fluid, in first 5 h of dissolution study ED prevents initial swelling of HPMC present in the coat. After 5 h in contact with disso-lution medium Eudragit dissolves because of the change in pH, HPMC hydrates, swells, erodes and drug release increases in the colon (Vyas & Roop, 2006).
The area under the plasma FLB concentration versus time curves (AUC) for the immediate release and compres-sion coated colon targeted tablets of FLB were 40230.73 and 72668.56 ng-h/mL respectively. These results indi-cated that the colon targeted compression coated tablets did not release the drug appreciably in stomach and small intestine, but in the colon the drug release was in slow manner due to limited absorptive surface area. However, the formulation F6 was absorbed slowly and completely as indicated by increased T
max and AUC. The MRT of immedi-
ate release and compression coated colon targeted tablets of FLB were 3.47 h and 10.73 h respectively indicating long resident time for colon targeted tablet.
The statistical analysis of pharmacokinetic parameters of immediate and colon release tablets was performed by ANOVA test. From the results there was a significant dif-ference in the C
max between immediate release and colon
targeted tablet, indicating that colon targeted tablets did not release the FLB in stomach and small intestine. Similar type of results observed in guar gum based colon targeted tablets of mebendazole (Krishnaiah et al., 2003). The T
max
and MRT of immediate release tablets were significantly different from colon targeted compression coated tablets indicating delayed release of FLB specifically to colon in slow manner. The AUC
0–∞ was significantly different from
each other indicating that the administration of drug as colon targeted tablet affected the extent of absorption (slow and complete).
From the results there was a good correlation between the in vitro drug release pattern and the plasma con-centration of FLB colon-targeted formulation F6 when compared to immediate release tablet during in vitro and in vivo evaluation. In conclusion, the immediate release tablet released its drug content almost immedi-ately within 2 h and available for immediate absorption from the stomach and small intestine thereby resulted in early T
max and higher C
max. But the compression coated
colon targeted tablet did not release its drug content significantly, up to 5 h, yet released majority of its drug content in the physiological environment of colon at
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.

Colon targeted pulsatile system of flurbiprofen 713
© 2012 Informa UK, Ltd.
about 10 h resulting in delayed Tmax
. Thus the results of the in vivo evaluation in healthy human volunteers showed that the colon targeted HPMC-ED compression coated tablets of FLB could specifically release the drug to the human colon.
conclusion
HPMC-ED compression coated tablets are capable of protecting the drug from being released in the upper region of GI system. Based on in vitro drug release stud-ies, F6 formulation showed significant level of drug release in the colon. The drug release from above formu-lation followed zero order profile and the drug release mechanism was supercase II transport. DSC and FTIR spectral studies showed that there is no interaction between the drug and excipients and the accelerated stability studies showed the stability of formulation. The X-ray imaging study in human volunteers showed that the tablets (F6) reached the colon without disintegrat-ing in the upper region of the GI system. The results of the pharmacokinetics in human volunteers showed that the colon targeted tablets did not release the drug in stomach and small intestine, but delivered it to the colon resulting in a slow absorption of the drug and making it available for local action in colon when compared to immediate release tablets. In conclusion, development of pulsatile HPMC-ED compression coated tablets (com-bination of pH sensitive and time dependent methods) is a good approach to target the flurbiprofen in colon.
acknowledgements
The authors acknowledge FDC Limited, Mumbai, India and Matrix laboratories, Hyderabad, India for gift sample of Flurbiprofen, HPMC K4M and Eudragit S100. The authors also thank to Management, Jangaon Institute of Pharmaceutical Sciences for providing facilities.
Declaration of interestThe authors report no conflicts of interest.
ReferencesAsghar LF, Chure CB, Chandran S. (2009). Colon specific delivery of
indomethacin: effect of incorporating pH sensitive polymers in xanthan gum matrix bases. AAPS PharmSciTech, 10, 418–429.
Ashford M, Fell J, Attwood D, Sharma H, Woodhead P. (2003). An evaluation of pectin as a carrier for drug targeting to the colon. J Con Rel, 26, 213–220.
Chaudhary A, Tiwari N, Jain V, Singh R. (2011). Microporous bilayer osmotic tablet for colon-specific delivery. Eur J Pharm Biopharm, 78, 134–140.
Chickpetty SM, Baswaraj R, Nanjwade BK. (2010). Studies on development of novel combined time and pH dependent solventless compression coated delivery systems for colonic delivery of diclofenac sodium. Asian J Pharm Clin Res, 3, 110–113.
Chourasia MK, Jain SK. (2003). Pharmaceutical approaches to colon targeted drug delivery systems. J Pharm Pharm Sci, 6, 33–66.
El-Kamel AH, Abdel-Aziz AA, Fatani AJ, El-Subbagh HI. (2008). Oral colon targeted delivery systems for treatment of inflammatory bowel diseases: synthesis, in vitro and in vivo assessment. Int J Pharm, 358, 248–255.
Ghimire M, Hodges LA, Band J, Lindsay B, O’Mahony B, McInnes FJ, Mullen AB, Stevens HN. (2011). Correlation between in vitro and in vivo erosion behaviour of erodible tablets using gamma scintigraphy. Eur J Pharm Biopharm, 77, 148–157.
Gibaldi M, Perrier D. (1990). Pharmacokinetics. New York: Marcel Dekker.
Grahnen A. (1984). Design of bioavailability studies. Pharm Int, 5, 100–103.
Hashem FM, Shaker DS, Nasr M, Saad IE, Ragaey R. (2011). Guar gum and hydroxy propyl methylcellulose compressed coated tablets for colonic drug delivery: in vitro and in vivo evaluation in healthy human volunteers. Drug Discov Ther, 5, 90–95.
ICH Q1A. Stability testing guidelines: Stability testing of new drug substances and products. CPMP/ICH/380/95, 1–13.
Krishnaiah YS, Satyanarayana V, Dinesh Kumar B, Karthikeyan RS, Bhaskar P. (2003a). In vivo pharmacokinetics in human volunteers: oral administered guar gum-based colon-targeted 5-fluorouracil tablets. Eur J Pharm Sci, 19, 355–362.
Krishnaiah YS, Veer Raju P, Dinesh Kumar B, Satyanarayana V, Karthikeyan RS, Bhaskar P. (2003b). Pharmacokinetic evaluation of guar gum-based colon-targeted drug delivery systems of mebendazole in healthy volunteers. J Control Release, 88, 95–103.
Luppi B, Bigucci F, Cerchiara T, Mandrioli R, Di Pietra AM, Zecchi V. (2008). New environmental sensitive system for colon-specific delivery of peptidic drugs. Int J Pharm, 358, 44–49.
Makhlof A, Tozuka Y, Takeuchi H. (2009). pH-Sensitive nanospheres for colon-specific drug delivery in experimentally induced colitis rat model. Eur J Pharm Biopharm, 72, 1–8.
Maroni A, Curto MDD, Serratoni M, Zema L, Foppoli A, Gazzaniga A, Sangalli ME. (2009). Feasibility, stability and release performance of a time-dependent insulin delivery system intended for oral colon release. Eur J Pharm Biopharm, 72, 246–251.
Maroni A, Zema L, Del Curto MD, Foppoli A, Gazzaniga A. (2012). Oral colon delivery of insulin with the aid of functional adjuvants. Adv Drug Deliv Rev, 64, 540–556.
Mathews BR. (1999). Regulatory aspects of stability testing in Europe. Drug Dev Ind Pharm, 25, 831–856.
Orlu M, Cevher E, Araman A. (2006). Design and evaluation of colon specific drug delivery system containing flurbiprofen microsponges. Int J Pharm, 318, 103–117.
Philip AK, Dubey RK, Pathak K. (2008). Optimizing delivery of flurbiprofen to the colon using a targeted prodrug approach. J Pharm Pharmacol, 60, 607–613.
Ravi V, Siddaramaiah, Pramod Kumar TM. (2008). Influence of natural polymer coating on novel colon targeting drug delivery system. J Mater Sci Mater Med, 19, 2131–2136.
Sarasija S, Hota A. (2000). Colon-specific drug delivery systems. Ind J Pharm Sci, 62, 1–8.
Shukla RK, Tiwari A. (2012). Carbohydrate polymers: Applications and recent advances in delivering drugs to the colon. Carb Polym, 88, 399–316.
Sinha VR, Singh A, Singh S, Bhinge JR. (2007). Compression coated systems for colonic delivery of 5-fluorouracil. J Pharm Pharmacol, 59, 359–365.
Srivastava R, Kumar D, Pathak K. (2012). Colonic luminal surface retention of meloxicam microsponges delivered by erosion based colon-targeted matrix tablet. Int J Pharm, 427, 153–162.
Staniforth JN, Aulton ME. (2007). Powder flow. In: Aulton ME, ed. Aulton’s Pharmaceutics: The Design and Manufacture of Medicines. Vol. 3. Churchill Livingstone: Elsevier, 168–179.
Talukder RM, Fassihi R. (2008). Development and in-vitro evaluation of a colon-specific controlled release drug delivery system. J Pharm Pharmacol, 60, 1297–1303.
Tugcu-Demiröz F, Acartürk F, Takka S, Konus-Boyunaga O. (2004). In-vitro and in-vivo evaluation of mesalazine-guar
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.

714 P. R. Veerareddy and S. K. Vemula
Journal of Drug Targeting
gum matrix tablets for colonic drug delivery. J Drug Target, 12, 105–112.
Vemula SK, Veerareddy PR. (2009). Different approaches to design and evaluation of colon specific drug delivery systems. Int J Pharm Tech, 1, 1–35.
Vincent HL, Suman KM. (2002). Drug delivery-oral colon-specific. In: Swarbick J, Boylan CJ, ed. Encyclopedia of Pharmaceutical Technology. Vol. 1. New York: Marcel Dekker, 871–885.
Vyas SP, Roop KK. (2006). Controlled drug delivery concepts and advances. Delhi: Vallabh Prakashan.
Wang X, Chi Z, Yue L, Li J, Li M, Wu L. (2007). A marine killer yeast against the pathogenic yeast strain in crab (Portunus trituberculatus) and an optimization of the toxin production. Microbiol Res, 162, 77–85.
Wu B, Chen Z, Wei X, Sun N, Lu Y, Wu W. (2007a). Biphasic release of indomethacin from HPMC/pectin/calcium matrix tablet: I. Characterization and mechanistic study. Eur J Pharm Biopharm, 67, 707–714.
Wu B, Shun N, Wei X, Wu W. (2007b). Characterization of 5-fluorouracil release from hydroxypropylmethylcellulose compression-coated tablets. Pharm Dev Technol, 12, 203–210.
Jour
nal o
f D
rug
Tar
getin
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Lav
al o
n 07
/13/
14Fo
r pe
rson
al u
se o
nly.





























