Embed Size (px)
Citation preview

133 Journal of Managed Care Pharmacy JMCP March 2009 Vol. 15, No. 2 www.amcp.org
ABSTRACT
BACKGROUND: The U.S. Department of Defense (DoD) health care benefit (TRICARE) provides 9.2 million active-duty and retired uniformed services personnel and their family members with access to a comprehensive pharmacy benefit with low out-of-pocket costs. DoD’s Uniform Formulary is available worldwide at DoD’s 3 pharmacy points of service (military phar-macies, contracted mail order, and community [network and non-network] pharmacies). Community pharmacies, military pharmacies, and mail order accounted for 64%, 23%, and 13%, respectively, of DoD’s $6.5 billion total drug expenditures during fiscal year (FY) 2007 (October 1, 2006, through September 30, 2007).
OBJECTIVE: To describe the DoD formulary management process and estimate cost savings associated with implementation of DoD’s 3-tier for-mulary.
SUMMARY: DoD implemented its 3-tier Uniform Formulary in 2005. This implementation required the development of a transparent formulary management process that (a) assesses medications for formulary status based on an evidence-based clinical evaluation and assessment of relative cost-effectiveness using pharmacoeconomic and budget impact modeling, (b) allows open and equitable price competition among pharmaceutical manufacturers based on formulary status, and (c) provides a public forum for beneficiaries and beneficiary organizations to comment on formu-lary changes. Through April 16, 2008, Uniform Formulary decisions had been implemented in 32 drug classes representing 53% of FY 2007 total drug expenditures. The 32 classes containing 343 drugs were reviewed at 12 quarterly meetings of the DoD Pharmacy and Therapeutics (P&T) Committee and the Beneficiary Advisory Panel, resulting in the classifica-tion of 85 drugs (24.8%) in tier 3, 92 drugs (26.8%) in tier 2, and 166 drugs (48.4%) in tier 1. Implementation of the 3-tier formulary was associated with an estimated $926 million in cost avoidance in FY 2007, primarily due to price reductions at military pharmacies and mail order, tier 3 copay-ments at community pharmacies and mail order, and change in product mix and pharmacy type (point of service). An additional $60 million in rebates were obtained in FY 2007 through the Voluntary Agreements for TRICARE Retail Pharmacy Refunds (UF VARR) program for prescriptions filled at community pharmacies; the UF VARR program first became available for drug classes reviewed in August 2006. The total of $986 million in cost avoidance and rebates represents an approximate 13% reduction, com-pared with what DoD otherwise would have paid in FY 2007 ($7.5 billion, compared with actual drug expenditures of $6.5 billion).
CONCLUSION: As in most private-sector health plans, the DoD formu-lary management process (a) includes rigorous decision making that is informed by clinical literature evaluations and pharmacoeconomic analy-ses, (b) results in drug formulary changes that require considerable effort in communication with providers and beneficiaries, and (c) produces drug cost savings derived from increased price competition among drug manu-facturers. Unlike private sector health plans, the DoD uses more disclosure of the results of evaluation of the evidence, solicits provider opinions before P&T committee deliberation, and provides the opportunity for beneficiaries to have input before implementation of formulary changes.
J Manag Care Pharm. 2009;15(2):133-46
Copyright © 2009, Academy of Managed Care Pharmacy. All rights reserved.
Formulary Management in the Department of Defense
Shana Trice, PharmD, BCPS; Joshua Devine, PharmD, PhD;Harsha Mistry, PharmD; Eugene Moore, PharmD, BCPS; and Andrea Linton, MS
• DoD’s TRICARE program is one of the largest health plans intheUnitedStates,providingcarefor9.2millionactive-dutyandretireduniformed servicespersonnel and their families.A totalof121millionoutpatientprescriptionsfor7millionbeneficiarieswerefilledundertheDoDpharmacybenefitinFY2007.
• In the FY 2000National Defense Authorization Act, Congressmandated implementation of an integrated pharmacy benefitprogramforDoDbeneficiariesandalloweddevelopmentofDoD’s3-tierUniformFormulary.
• Although implementation of theUniform Formulary hasmod-ernized formularymanagement inDoD, it also has introducedadditional complexity and creatednewchallenges inmanagingDoD’s$6.5billionpharmacybenefit.Akeyissueiscoordinatingchangesinformularystatusacrossalargesysteminresponsetochangesinclinicalorcost-effectivenesswithindrugclasses.Forexample,whentheprotonpumpinhibitor(PPI)classwasevalu-atedin2005,esomeprazolewasdeterminedtobelesscost-effec-tivethansimilaragentsandwasplacedintier3todiscourageuse.Uponre-evaluationoftheclass in2007,acompetitivebidfromthemanufacturerofesomeprazolecausedacompletereversalinformularyposition:esomeprazolewasnotonlyremovedfromtier3,butalsomadeavailableatthetier1(generic)copayment,withallotherPPIsexceptgenericomeprazoleontier3.
What is already known about this subject
foRMuL ARy MAnAgEMEnT
• The article describes how a large, publicly funded pharmacybenefit program incorporates clinical evaluation and pharma-coeconomicanalysisintoitsformularydecision-makingprocessandusesprice competitionamongpharmaceuticalmanufactur-ers basedon formulary status, includingdirect pricediscountsatmilitarypharmaciesandthemail-orderprogramandrebatesbasedonprescriptionsfilledbyDoDbeneficiariesatcommunitynetworkpharmacies.
• DoD incorporates transparency into its formulary managementprocess that includes publicly available minutes of the P&TCommitteemeetingswithformularyrecommendationsandpro-ceedingsofDoD’sBeneficiaryAdvisoryPanel,whichprovidesanopportunityforbeneficiariesandtheirrepresentativestocommentonthecommittee’srecommendationsbeforefinalapproval.Thisprocesshasnothinderedplacementofdrugsontier3;ofthefirst343drugsreviewed,85(24.8%ofallbrandandgenericdrugsand48.0%ofbranddrugs)wereplacedintier3.
• Continuing challenges that face DoD include the impact ofextendingfederallymandatedgovernmentpricingtomedicationsprovidedthroughDoD’scommunitypharmacynetwork,effectivecommunicationofformularychangestobeneficiariesandprovid-ers,andongoingassessmentoftheclinicaloutcomesofformularychanges, both in terms ofmaintaining or improving outcomeswhile lowering costs and providing data that can be used toimprovepredictivemodeling.
What this study adds

www.amcp.org Vol. 15, No. 2 March 2009 JMCP Journal of Managed Care Pharmacy 134
Formulary Management in the Department of Defense
The pharmacy benefit offered under the Military HealthSystemcomprisesa largecommunitypharmacynetworkandmail-orderplan,inadditiontopharmaciesatmilitary
facilities. It serves a diverse population of 9.2 million eligiblebeneficiaries—active-duty and retired uniformed services per-sonnel and their familymembers. TheDepartment ofDefense(DoD)formularymanagementprocesshasevolvedrapidlysincethe introductionof the3-tierUniformFormulary in2005.Thecurrent process is based on evidence-based clinical evaluationand assessment of relative cost-effectiveness using pharmaco-economic and budget impact modeling; allows for open pricecompetition among pharmaceutical manufacturers based onformulary status; andprovides apublic forum forbeneficiariesto comment on potential formulary changes, consistent withfederalinitiativespromotingquality,efficiency,andtransparencyinhealthcareprograms.1TheprocessalsohasclearconstraintsrelatedtoitsstatusasaU.S.governmentprogramanditsroleinsupporting active-dutymilitarypersonnel.Unlikemost privatesectorprograms,coveragerulesandcopaymentamountsaresetby lawandregulation;changesrequirecongressionalapproval.Theseconstraintsresultedinabroadlyinclusiveformularyandlowcopayments,comparedwithprivatesectorplans.However,inotherrespects,theDoDpharmacybenefitisnotunlikethosefound among commercial health plans, particularly comparedwithotherfederaldrugbenefitprograms.
Background on TRICAREIn fiscal year (FY) 2007, approximately 9.2million Americanswereeligible forhealthcare servicesunder theMilitaryHealthSystem,makingTRICAREoneofthelargesthealthplansintheUnitedStates.Ofthese,7million(76%)usedtheDoDpharmacybenefit in FY 2007, split almost equally between active-dutymembers of the uniformed services and their familymembers(44%)anduniformedserviceretireesandtheirfamilymembers(56%).Atotalof121millionoutpatientprescriptionswerefilledundertheDoDpharmacybenefitinFY2007.
DoD beneficiariesmay access health care throughmilitary-operatedhospitalsandclinicsorthroughaprivate-sectornetworkofhealthcarefacilitiesandproviders.SinceMay2005,DoDhasprovided a prescription drug benefit based on a 3-tier copay-mentstructureforprescriptionsfilledatcommunitypharmaciesandtheTRICAREmail-orderpharmacy(Table1).Beneficiariesmayfillprescriptionsat3pharmacypointsofservice(militarypharmacies, contracted mail order, and approximately 60,000community [network and non-network] pharmacies). Claimsfrom military, mail-order, and community network pharma-cies,includingthoseforwhichTRICAREservesasasecondarypayer,areprocessedonareal-timebasisbythePharmacyDataTransaction Service (PDTS), an online transaction processingsystemthatincludesatleast24monthsofclaimshistoryfortheconduct of concurrent andprospectivedrugutilization review.The PDTS Data Warehouse serves as a comprehensive, single
sourceofpharmacyclaimsdata.CoveragerulesandcopaymentsintheTRICAREhealthplan
areestablishedbylawandfederalregulation.2Withrareexcep-tions(e.g.,smokingcessation,weightreduction,andmedicationsforcosmeticconditions),allU.S.FoodandDrugAdministration(FDA)-approvedlegendmedicationsintendedforuseinanoutpa-tientsettingarecurrentlyavailabletoDoDbeneficiariesthroughcommunitypharmaciesandtheTRICAREmail-orderpharmacy.Table1showsthatcurrentcopaymentsforuptoa30-daysup-ply ofmedication dispensed at community pharmacies are $3forgenericmedications (tier1),$9 forpreferredbrandmedica-tions (tier2), and$22 fornonpreferredbrandmedications (tier3).Thereisnotier4forspecialtymedications(e.g.,oralchemo-therapyagents)orbiotechnologydrugs.Thereisno($0)copay-ment forprescriptionsdispensedbymilitarypharmaciesor foractive-dutymilitarypersonnelatanypointof service.Revisionofthecopaymentstructureandimplementationofatier4havebeenrecommended.3
Unlikeprivatesectorplans,federalregulationsmandatethatbrandmedications,includingthosenewlyapprovedbytheFDA,areautomaticallyavailableatthetier2copaymentuntilreviewedby the DoD Pharmacy and Therapeutics (P&T) Committee.Federalregulationsalsomandatetheexistenceofamechanismallowingbeneficiariestoreceivetier3medicationsat thetier2copaymentifitisdetermined,basedoninformationsuppliedbytheprescriber,thatthebeneficiary’sclinicalneedscannotbemetbymedicationsineithertier1or2.Formsandcriteriatosup-port this exception are provided throughDoD’s contractor formail-orderandcommunitypharmaciesandareavailableontheTRICAREpharmacywebsite.4
TheDoDUniformFormularyhassomewhatdifferentimplica-tionsatmilitarypharmacies,whichsupportmilitaryhealthcare facilities worldwide—ranging from major medical centers to
TABLE 1 DoD Uniform Formulary Copayments by Point of Servicea
Type of Pharmacy
Military Community
Network
Non- Network
Community Mail OrderGeneric(tier1) $0 $3 $3b $3
Preferredbrand(tier2)
$0 $9 $9b $9
Nonpreferred(tier3,“nonformulary”)
- $22 $22b $22
Maximumsupplypercopayment
90days 30days 30days 90days
aActive-duty military personnel pay no ($0) copayment at any point of service.bCost shares vary from 20% to 50% when beneficiaries use non-network commu-nity pharmacies and/or at overseas locations, depending on TRICARE enrollment status.DoD = Department of Defense.

135 Journal of Managed Care Pharmacy JMCP March 2009 Vol. 15, No. 2 www.amcp.org
Formulary Management in the Department of Defense
outpatient clinics. Military pharmacies do not charge copayments. Although medications in all tiers are available atcommunity pharmacies andmail order, medications on tier 3oftheUniformFormularyarenotallowedonformularyatmili-tarypharmaciesandmaybedispensed(a)onlyforprescriptionswrittenbymilitaryprescribers(orcivilianprescriberstowhomthepatientwasreferred),and(b)onlyifthetier3drugisdeter-mined tobemedicallynecessary (i.e., “patienthasexperiencedsignificantadverseeffectswithalloftheformularyalternatives”).1 BecauseDoDbeneficiariesmayfillprescriptionsatanypointofservice, theymay choose to obtain tier 3medications at com-munitypharmaciesormailorderbypayingthe$22copayment.Thisoptionmayleadtosomeshiftingoftier3prescriptionsawayfrommilitaryfacilities.However,militaryfacilitiesareexpectedtofillprescriptionsgeneratedbytheirownprescribers(includingmedicallynecessary tier3prescriptions)unless thebeneficiarychoosestogoelsewhere,apolicycommonlyknownasthe“youwriteit,youfillit”rule.5,6
Inaddition,2coreformularylistsapplyspecificallytomilitarypharmacies.TheprimarycaremedicationslistedonDoD’sBasicCoreFormulary(BCF)mustbestockedandreadilyavailableatallmilitarypharmaciesworldwide.TheExtendedCoreFormulary(ECF)includesmorespecializedmedicationssuchasinjectablesformultiplesclerosisandimmunomodulatorybiologicsforpso-riasisandrheumatoidarthritis;medicationsontheECFmustbeonmilitarypharmacy formularies and readily available if suchcare is provided at aparticular facility.The2 core formularies(BCFandECF)areintendedtoprovideconsistencyacrossfacili-tiesandincreasecontinuityofcareamongDoD’shighlymobilepopulation; they are not complete formularies, and militaryfacilitiesmay(andtypicallydo)addmedicationsavailableattier1andtier2copaymentstotheirlocalformularies,basedontheneedsoftheirpatientpopulations.ThecombinationofUniformFormulary tier 3 and BCF and ECF requirements effectivelycreates both negative and positive formulary requirements formilitaryfacilities(Table2)7,8.Anexceptionappliestoactive-dutymilitarypersonnel,whomayfillprescriptionsat$0copaymentatanyDoDpharmacypointofservice.Tier3medicationsarenotcoveredforactive-dutymilitarypersonnelunlessdeterminedtobemedicallynecessary.
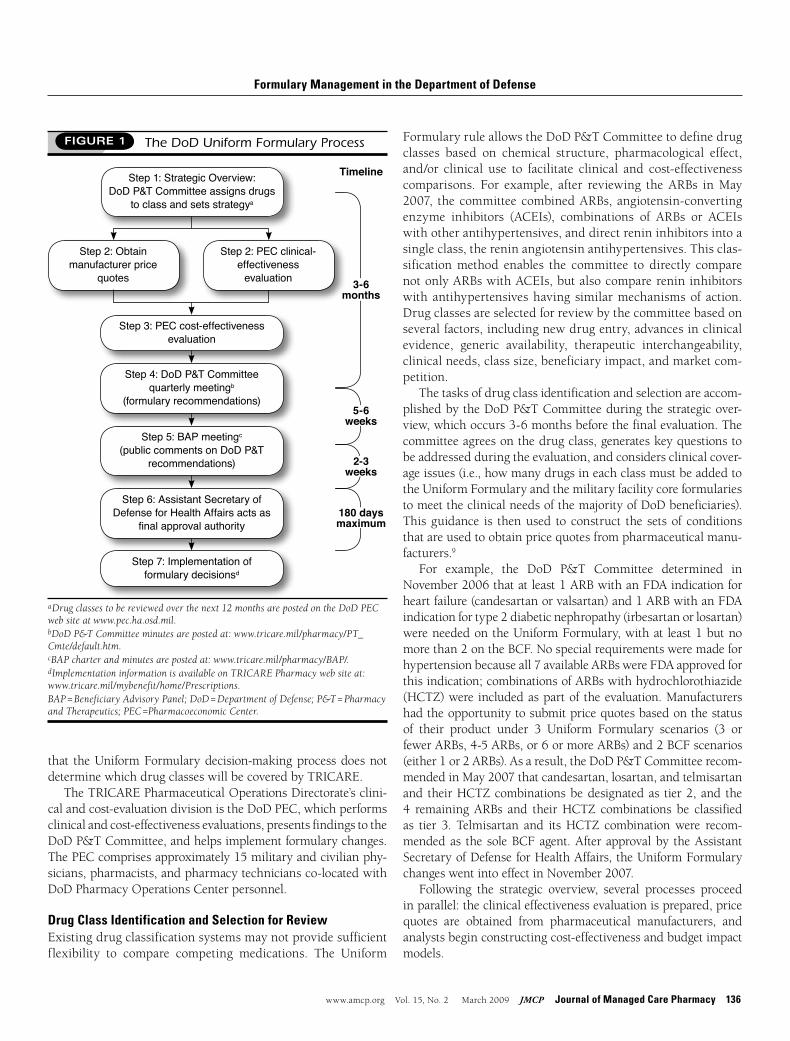
Overview of the Uniform Formulary Decision ProcessThesequenceofeventsandtimelineassociatedwithevaluationofadrugclassaresummarized inFigure1.Thegroupprinci-pallychargedwithimplementingandmaintainingtheUniformFormularyistheDoDP&TCommittee.Thecommittee’s17vot-ingmembersincludeArmy,Navy,andAirForcepharmacistsandphysiciansfrommultiplespecialties;pharmacyleadersfromeachofthemilitaryservices;andDepartmentofVeteransAffairs(VA)and Coast Guard representatives. It is chaired by a physician,with thedirectorof theDoDPharmacoeconomicCenter (PEC)serving as recorder. Although initially chartered in 1998, the
committeedidnottakeitscurrentformuntilimplementationoftheUniformFormularyRulein2005.2
TheUniformFormularyRuleisthebasisforthecommittee’sevaluation process. Under the rule, agents in each therapeuticclassareselectedforinclusionontheUniformFormulary(tier1or2)basedonthe“relativeclinicaleffectivenessandcost-effective-nessoftheagentsinsuchclass.”Asstatedinfederalregulations,thecommitteemayrecommendthatagentsdetermined“not tohaveasignificant,clinicallymeaningfultherapeuticadvantageintermsofsafety,effectiveness,orclinicaloutcomeoverotherphar-maceuticalagentsincludedontheuniformformulary”beclassi-fiedasnonformulary(tier3).Regulationsalsoprovidethat,ifthecommittee’sevaluation“concludesthatapharmaceuticalagentinatherapeuticclassisnotcost-effectiverelativetootherpharma-ceuticalagentsinthattherapeuticclass(consideringcosts,safety,andeffectiveness),thecommitteemayrecommenditbeclassifiedasanonformularyagent”(tier3).2
An important aspect of the implementation of theUniformFormularyisitsincrementalnature.Becausemedicationscannotbeplacedon tier3until after the committeehas reviewed theclass,UniformFormulary changes occur over time.Also, note
TABLE 2 Formulary Requirements at Military Pharmacies
Military Pharmacies Must Have on
Formulary (Readily Available)
Military Pharmacies May Have on Formulary
(Not Required)
Military Pharmacies Must Not Have on
Formulary
• BCFmedications
• ECFmedications,ifrelevanttothe specialtycare providedatfacility
•MedicationsonUniformFormularytier1or2,butnotontheBCForECF
•ECFmedications,ifrelevantspecialtynotprovidedatfacility
•UniformFormularytier3medications
Example: ARBsa
•Telmisartan(±HCTZ) –BCFagent
•Candesartan±HCTZ
•Losartan±HCTZ
•Irbesartan+HCTZ
•Eprosartan+HCTZ
•Olmesartan+HCTZ
•Valsartan+HCTZ
Example: PPIsb
•Genericomeprazole 10mgand20mg only –BCFagent
•Esomeprazole –BCFagent
•Omeprazole40mg(Prilosec)
•Omeprazole-sodiumbicarbonate(Zegerid)
•Rabeprazole
•Pantoprazole
•Lansoprazole
aMTF Formulary Management for ARBs.7 bMTF Formulary Management for PPIs.8
ARB = angiotensin receptor II blocker; BCF = Basic Core Formulary; ECF = Extended Core Formulary; HCTZ = hydrochlorothiazide; MTF = military treatment facility; PPI = proton pump inhibitor.
www.amcp.org Vol. 15, No. 2 March 2009 JMCP Journal of Managed Care Pharmacy 136
Formulary Management in the Department of Defense
that theUniformFormularydecision-makingprocessdoesnotdeterminewhichdrugclasseswillbecoveredbyTRICARE.
TheTRICAREPharmaceuticalOperationsDirectorate’sclini-calandcost-evaluationdivisionistheDoDPEC,whichperformsclinicalandcost-effectivenessevaluations,presentsfindingstotheDoDP&TCommittee,andhelpsimplementformularychanges.ThePECcomprisesapproximately15militaryandcivilianphy-sicians,pharmacists,andpharmacytechniciansco-locatedwithDoDPharmacyOperationsCenterpersonnel.
Drug Class Identification and Selection for ReviewExistingdrugclassificationsystemsmaynotprovidesufficientflexibility to compare competing medications. The Uniform
FormularyruleallowstheDoDP&TCommitteetodefinedrugclasses based on chemical structure, pharmacological effect,and/or clinical use to facilitate clinical and cost-effectivenesscomparisons. For example, after reviewing the ARBs inMay2007, thecommitteecombinedARBs, angiotensin-convertingenzyme inhibitors (ACEIs), combinations of ARBs or ACEIswithotherantihypertensives,anddirectrenininhibitorsintoasingleclass,thereninangiotensinantihypertensives.Thisclas-sificationmethod enables the committee to directly comparenotonlyARBswithACEIs,butalsocomparerenininhibitorswith antihypertensiveshaving similarmechanismsof action.Drugclassesareselectedforreviewbythecommitteebasedonseveralfactors,includingnewdrugentry,advancesinclinicalevidence, generic availability, therapeutic interchangeability,clinicalneeds,classsize,beneficiaryimpact,andmarketcom-petition.
Thetasksofdrugclassidentificationandselectionareaccom-plishedbytheDoDP&TCommitteeduringthestrategicover-view,whichoccurs3-6monthsbeforethefinalevaluation.Thecommitteeagreesonthedrugclass,generateskeyquestionstobeaddressedduringtheevaluation,andconsidersclinicalcover-ageissues(i.e.,howmanydrugsineachclassmustbeaddedtotheUniformFormularyandthemilitaryfacilitycoreformulariestomeettheclinicalneedsofthemajorityofDoDbeneficiaries).Thisguidance is thenused toconstruct the setsof conditionsthatareusedtoobtainpricequotesfrompharmaceuticalmanu-facturers.9
For example, the DoD P&T Committee determined inNovember2006thatatleast1ARBwithanFDAindicationforheartfailure(candesartanorvalsartan)and1ARBwithanFDAindicationfortype2diabeticnephropathy(irbesartanorlosartan)wereneededontheUniformFormulary,withat least1butnomorethan2ontheBCF.Nospecialrequirementsweremadeforhypertensionbecauseall7availableARBswereFDAapprovedforthisindication;combinationsofARBswithhydrochlorothiazide(HCTZ)were includedaspartof theevaluation.Manufacturershadtheopportunitytosubmitpricequotesbasedonthestatusof their product under 3 Uniform Formulary scenarios (3 orfewerARBs,4-5ARBs,or6ormoreARBs)and2BCFscenarios(either1or2ARBs).Asaresult,theDoDP&TCommitteerecom-mendedinMay2007thatcandesartan,losartan,andtelmisartanand theirHCTZcombinationsbedesignatedas tier2, and the4 remainingARBs and theirHCTZ combinations be classifiedas tier 3. Telmisartan and itsHCTZ combinationwere recom-mendedas the soleBCFagent.After approvalby theAssistantSecretaryofDefenseforHealthAffairs,theUniformFormularychangeswentintoeffectinNovember2007.
Following the strategic overview, several processes proceedinparallel:theclinicaleffectivenessevaluationisprepared,pricequotes are obtained from pharmaceutical manufacturers, andanalystsbeginconstructingcost-effectivenessandbudgetimpactmodels.
3-6 months
5-6weeks
2-3weeks
180 daysmaximum
fIguRE 1 The DoD Uniform Formulary Process
aDrug classes to be reviewed over the next 12 months are posted on the DoD PEC web site at www.pec.ha.osd.mil. bDoD P&T Committee minutes are posted at: www.tricare.mil/pharmacy/PT_Cmte/default.htm.cBAP charter and minutes are posted at: www.tricare.mil/pharmacy/BAP/.dImplementation information is available on TRICARE Pharmacy web site at: www.tricare.mil/mybenefit/home/Prescriptions.BAP = Beneficiary Advisory Panel; DoD = Department of Defense; P&T = Pharmacy and Therapeutics; PEC =Pharmacoeconomic Center.
Step 1: Strategic Overview: DoD P&T Committee assigns drugs
to class and sets strategya
Step 2: Obtain manufacturer price
quotes
Step 3: PEC cost-effectiveness evaluation
Step 4: DoD P&T Committee quarterly meetingb
(formulary recommendations)
Step 5: BAP meetingc (public comments on DoD P&T
recommendations)
Step 6: Assistant Secretary of Defense for Health Affairs acts as
final approval authority
Step 7: Implementation of formulary decisionsd
Step 2: PEC clinical-effectiveness
evaluation
Timeline

137 Journal of Managed Care Pharmacy JMCP March 2009 Vol. 15, No. 2 www.amcp.org
Formulary Management in the Department of Defense
Evaluation of Clinical Effectiveness Ateam(consistingofatleast1clinicalpharmacistand1physician)performs the clinical evaluation and summarizes the findingsfor presentation to the DoD P&T Committee. The evaluationincludes both a thorough review and synthesis of the clinicalliteratureandanassessmentofmedicationuseinactualpractice,oftenincludingasurveyofmilitaryhealthcareproviders.
Formulating a Search Strategy and Identifying Available Evidence: KeyquestionsgeneratedbytheDoDP&TCommitteearefirstusedtoformulateasystematicsearchstrategy,takingintoaccounttheamountandqualityofclinicalevidenceavailableinagivendrugclass.Searchesareperformedbytheclinicalevalu-ationteam,usingreferencescitedinPubMed/MEDLINE;sourcesalso are identified by using the reference section of relevantarticlesandmanufacturerinformation.Duetotimeandresourcelimitations,articlesnotavailableinEnglisharerarelyincluded.
ThePECattemptstousethehighestlevelofclinicalevidenceavailable,10 with preference given to published randomizedclinicaltrials(RCTs),followedbypublisheduncontrolledtrialsorobservational studies (includingdatabasestudies).Unpublisheddata,althoughconsideredlessreliableduetolackofpeerreview,maybeincludedif(a)theyprovideadditionalinformation(espe-ciallyconcerningsafety),(b)publisheddataarescarce,or(c)theexistenceofcompletedbutunpublishednegativetrialssuggestspotential publication bias. Indirect comparisons of treatmenteffectbasedonplacebo-oractive-controlled trialsare typicallyused to comparemedications because data from head-to-headRCTsarerare.
Systematic reviews from typically high-quality sources (forexample, the Cochrane Database of Systematic Reviews,11 theDrugEffectivenessReviewProject,12andtechnologyassessmentsfromtheU.S.AgencyforHealthcareResearchandQuality,13theUnitedKingdom’sNationalInstituteforClinicalExcellence,14andthe Canadian Agency for Drugs and Technologies inHealth)15 areincorporatedifavailable.ThePECusuallydoesnotindepen-dentlyassesseveryclinicaltrialincludedintheseoutsidereviewsbutinsteadfocuseson(a)themajortrialsand(b)trialsoutsidethespecificfocusoftherevieworpublishedafterthedatacollec-tionperiodended.Meta-analyticresultsarepresentedalongwithadiscussionofmethodology and trials included;meta-analyticmethodsareavaluabletool fordatasynthesisbuthaveknownlimitations. Although precision of meta-analytic results oftenencouragescertainty,statisticaltechniquescannotimprovepoor-qualitydata in theprimaryRCTsor compensate forpersistentbiasoruncontrolledconfounding.Inaddition,combiningtrialsusing different measures introduces error, and meta-analysisis weakest when trials are heterogeneous and offer conflictingconclusions.16ThePECtypicallyusesthesamemethodologythatwasusedintheoutsidereviewtogradethequalityofmorerecentclinicaltrialresults.Explanationsofthemethodusedforgradingthequalityoftheevidenceandhowitwasappliedareincludedinallclinicalevaluations.
Shortly after the strategic overview, pharmaceutical manu-facturers are asked to submit copies of their product dossiersintheAcademyofManagedCarePharmacy(AMCP)Format for Formulary Submissions.TheAMCPFormat both streamlines theprocess of obtaining clinical information from manufacturersandprovidesguidelinesandavenueformanufacturerstoprovideeconomicevaluationsandpharmacoeconomicmodelstosupportthevalueoftheirproducts.BasedontheformularysubmissiontemplatedevelopedbyRegenceBlueShieldin1998,17theAMCPFormatwas adaptedand released forwidespreaduse in200118 and subsequently refined in Version 2.1 to address feedbackfromusers.19ThedossiersareusedbythePECto(a)evaluatethestrengthofpublishedandunpublishedevidencesupportingvari-ousindications,(b)constructcomparativetables,and(c)identifyclinicalliteraturesources.Mostmanufacturersofbrandmedica-tionsprovidedossiers,althoughqualityandcomprehensivenessvaryamongthedossiersubmissions.
Manufacturers also are typically invited to provide 1-hourclinicalpresentationstotheevaluationteamandotherPECstaff,basedonkeyquestionsidentifiedbytheDoDP&TCommitteeandthePEC.Mostmanufacturersprovidebothdossiersandface-to-facepresentations.Between2and4drugclassesarereviewedeachquarter,withseveralbrand-namedrugsineachclass.Thus,pharmaceuticalmanufacturers typicallymake 50-60 such pre-sentationsperyear.
Surveying Providers: As a part of each clinical evaluation,thePECsurveysasoftenasnecessaryaconveniencesampleofmilitaryphysicians,pharmacists,andotherhealthcareprovidersto obtain information not readily available from clinical trials;generally,2-4suchsurveysareperformedeachcalendarquarter.Questions are developed by the clinical evaluation team andreviewedbyother PEC staff; surveys areperformedby e-mail,phone,orusingawebsurveytool.Dependingonthenatureofthemedicationswithinaclass,surveysmaybetargetedprimarilytospecialistsorprimarycareproviders;awidelytargetedsurveytypically garners responses from several hundred responders.Survey invitations are disseminated through pharmacy andmedical specialty leaders in each of themilitary services.Oneshortcoming of the present system is that little or no input isobtainedfromcivilianproviderscaringforTRICAREbeneficia-ries.SurveyresponsesaresummarizedandpresentedtotheDoDP&TCommitteeduringitsevaluation.
Private-sectorhealthplanswithadequateresourcesmaywishtoconsiderconductingprovidersurveysinconjunctionwithclassevaluations.DoDprovidersurveysyieldusefulinformation,suchas(a)clinicalreasoningbehindthewaymedicationsaretypicallyprescribedandhowprovidersinterprettheclinicalliterature,(b)providerperceptions concerning safety and tolerability (includ-ing theeffectof characteristics suchas taste and tablet sizeonadherence,particularlyinchildren),and(c)pragmaticconcernsamongproviderssuchassuitabilityofproductpackagingforuseinautomateddispensingsystemsandlimitationsonshelfspace,

www.amcp.org Vol. 15, No. 2 March 2009 JMCP Journal of Managed Care Pharmacy 138
especiallyforcontrolledsubstances.Thesurveysalsoalertmili-taryfacilityP&Tcommitteestoupcomingdrugclassevaluationsand allow providers the opportunity to express their opinionsbeforerecommendationsaremadebytheDoDP&TCommittee.
Evaluating the Evidence: For purposes of the evaluation,theterm“clinicaleffectiveness”isbroadlydefinedastheoverallclinical usefulness of medications within a class. Eachmedica-tion is assessed based on its relative efficacy, safety, and toler-ability,comparedwithothermedicationsintheclass.ThePECtypicallyattemptstoconsiderallmajoruses,includingcommonoff-labeluses.Forexample, thePEC’sevaluationofantidepres-sants focused primarily on depression, but also addressed thetreatmentofotherpsychiatricdisorders(e.g.,generalizedanxietydisorderandpost-traumaticstressdisorder),aswellasnonpsy-chiatricconditionssuchasneuropathicpain.
Efficacy is defined as the likelihood that a medication willactuallywork(achieveitsdesiredeffect),withthefocusbeingonhowwellamedicationmaybeexpectedtoworkintheDoDpop-ulation, comparedwithothers in the sameclass.Comparisonsmaybebasedondatafrombothcontrolledclinicaltrials(whichare typically performed in a prescreened patient population,emphasize medication adherence, and thus provide the mostreliable estimate of potential effect when amedication is bothprescribedandtakenasdirected)andstudiesinlesscontrolledsettings thatmaygiveabetterestimateof resultsachievable inactualpractice(adistinctionusuallydenotedas“efficacy”versus“effectiveness”).20 The evaluation often includes multiple mea-sures, includingboth “hard”endpoints (suchas reductions inmortality),aswellasmorecommonlyassessedbiomarkerssuchasbloodpressurereductionorbeneficialeffectson lipid levels,whichareconsideredtobelinkedtoeffectsonmortalityormor-bidity.Wheneverpossible, trialresultsarereportedintermsofreductionsinabsoluterisk(e.g.,differenceinmortalityrates)andnumberneeded to treat (NNT;number of patientswhowouldhavetobetreated,foracertainperiod,toobtainonebeneficialoutcome),which give amore realistic assessment of the actualbenefitprovidedbytreatment,comparedwithestimatesofrela-tiverisk(e.g.,percentreductioninmortalityrates).
Forpurposesoftheclinicaleffectivenessevaluation,safetyisgenerallydefinedasthelikelihoodthatthedrugwillnotcauseharm. Potential safety differences may include the frequencyand severity of adverse events, drug interaction potential, orsafetyinspecialpatientpopulations.Inmostcases,thefocusisonrelativelyrarebutpotentiallyseriousevents,suchasliverorkidneydysfunction.Thenumberneededtoharm(NNH;numberofpatientswhowouldhave tobe treated, foracertainperiod,to result in1adverseevent)maybeused tocomparemultiplesourcesofharm,thepropensityof2ormoremedicationstocauseharm,ortoestimatetheoverallriskversusbenefitofamedica-tionbycomparingNNHwithNNT.ThePECobtainsestimatesofriskfromvarioussources,includingtheclinicalliterature,manu-facturers, and the FDA. In the future, the DoD Patient Safety
Formulary Management in the Department of Defense
Center,whichhasanonvotingrepresentativeontheDoDP&TCommittee,willprovidereportsofadverseeventsandmedica-tionerrorsacross174militaryfacilities.
Theterm“tolerability”isusedwhendifferencesexistbetweenmedicationsthataffectthelikelihoodthatthepatientwillactu-ally take the medication. Potential tolerability differences mayincludecommon,bothersomeadverseevents(suchasnauseaorheadache)ordifferencesindosing,administration,oreaseofusethatmayaffectadherenceorpersistence.Becauseadverseeffectratesandpatient-reportedpreferencesmayvarywidelydepend-ing on methodology and definition, tolerability differencesbetween drugs are often difficult to assess outside of a directcomparativetrial.Forpurposesoftheclinicalevaluation,thePECmayattempttoassesstolerabilitybasedonplacebo-adjusteddis-continuationratesduetoadverseeffectsduringrandomizedtrialsorpostmarketingstudiesofpersistenceoradherence.However,itmaybedifficult todrawmeaningfulconclusions,due todif-ferences in patient population across trials (e.g., age, comorbidillness).
TheclinicaleffectivenessevaluationalsotakesintoaccountthefactthatDoD’spatientpopulationspansallagegroups,frommili-tarydependentstoretirees,whoretaintheDoDpharmacybenefitregardlessofage.Theevaluationtypicallyincludesanextensivelook at utilization. Depending on drug class, this assessmentprocessmayincludeestimatesofuseratesbyagegroup,gender,or disease state treated (e.g., immunomodulatory biologics forrheumatoidarthritis,psoriasis,orCrohn’sdisease).DoD-specificadherencestudiesmayalsobeperformed.Forexample,ananaly-sispresentedaspartofthecommittee’sJune2008evaluationofosteoporosismedicationscomparedmedicationpersistenceratesonweeklyversusmonthlyregimensfor23,044DoDbeneficiariesfilling initialprescriptions fororalbisphosphonates at commu-nitypharmaciesormailorderfromAugust2006throughJanuary2007;resultsoftheanalysissupportedaslightlyhigheroddsofbeingpersistentwith therapyamongmonthlyusers, comparedwithweeklyusers,afteradjustingforage,gender,pointofservice,region,andnumberofconcomitantmaintenancemedications.21
Formulating a Clinical Effectiveness ConclusionAspartofitsevaluation,theclinicalteamprovidestheDoDP&TCommitteewithitsconclusionsabouttherelativeefficacy,safety,and tolerabilityofdrugswithinaclass,alongwithanswers toother key questions. In general, these conclusions address (a)whetherornotthereisevidenceofdifferencebetween2ormoremedications, based on available evidence, (b) the strength oftheevidence(i.e.,thedegreeofuncertainty),(c)themagnitudeofanysuchdifference,and(d)thepotentialimpactonvariouspatientpopulations.Drugswithinaclassarerankedaccordingtovariousattributeswheneverpossible.Theclinicalevaluationteamdoesnotasaruleattempttoassesstherelativeimportance of differences (i.e., whether differences in efficacy, safety, ortolerability aremore important), although theydoprovide the

139 Journal of Managed Care Pharmacy JMCP March 2009 Vol. 15, No. 2 www.amcp.org
communitypharmacypointofservice(Table3).Additional discounts for drugs dispensed by TRICARE
communitynetworkpharmacieshavebecomeavailableinthelast2yearsthroughtheUniformFormularyVoluntaryAgreementforTRICARE Retail Pharmacy Refunds (UF VARR) process. ThisprocessfirstbecameavailableforclassesreviewedattheAugust2006meetingof theDoDP&TCommittee and includesquar-terly rebatespaid to theDoDbydrugmanufacturersbasedonutilization in the communitypharmacynetwork, startingwiththe effectivedateofUniformFormulary status changes (i.e., atthe endof the implementationperiodwhen tier3 copaymentsgointoeffect).Trackingofrebatesandadministrationofthepro-gramareperformedbytheTRICAREPharmaceuticalOperationsDirectorate.
ForboththeUFBPAandUFVARRprograms,utilizationdata,instructionsforsubmittingprices,andconditionsetsarepostedon theTRICAREwebsite for theuseofmanufacturers shortlyafterthecommittee’sstrategicoverviewoftheclass(typically3-6monthsbeforethefinalreview).27Manufacturersarenotrequiredtosubmitpricequotesundereitherprogrambutcommonlydosotoremaincompetitive.
AsshowninTable3, theUFBPAprocessresultedinanesti-mated$926millionincostavoidanceinFY2007,28basedon(a)reductionsinunitpricesatmilitarypharmaciesandmailorder,(b)tier3copaymentsatcommunitypharmaciesandmailorder,(c) migration of patients from higher- to lower-cost points ofservice (i.e., from community pharmacies tomilitary pharma-ciesormailorder),and(d)changeindrugmixfromhigher-tolower-costdrugs(e.g.,fromtier3agentstoatier1or2alterna-tive). TheUFVARRprogram generated $60million in rebatesbasedonbrandnamedrugutilizationbyDoDbeneficiaries atcommunitynetworkpharmaciesinFY2007,thefirstyearoftheprogram,andanestimated$200millioninUFVARRrevenuesareexpectedbyDoDinFY2008asmoreclassesarereviewed.Thetotalof$986millionincostavoidanceandrebatesrepresentsanapproximately13%reduction,comparedwithwhattheDoDwould otherwise have paid in FY 2007, estimated at approxi-mately $7.5 billion rather than the actual drug expenditure of$6.5billion.
Evaluation of Cost-Effectiveness The cost-effectiveness evaluation is typically performed by 1ormore PEC clinical pharmacists with training in pharmaco-economics. Two distinct steps to this process are (a) pharma-coeconomic analysis, which evaluates the outcomes and costsof interventions designed to improve health,29 and (b) budgetimpact analysis, which estimates the likely impact on annualhealthcareuseandcostsoverthefirst,second,andsubsequentyears.30 Sensitivity analysesmay be used at either step to dealwithuncertaintyregardingmodelparameters.Probabilisticsen-sitivityanalysis(PSA)isusedinconjunctionwithbudgetimpactanalysistoevaluatetheuncertaintyaroundpointestimatesofall
committeewithsupportingevidence(e.g.,NNTversusNNH).TheDoD P&TCommittee is responsible for discussing the
conclusionsoftheclinicalteamandcomingtoanoverallclini-cal effectiveness conclusion. In general, the expectation is thatmedications shouldbeefficacious, safe, and tolerable;however,thecommitteeisgenerallymostsensitivetodifferencesinsafety(i.e., lesstolerantofriskandmorewillingtomakedistinctionsbetweendrugsbasedon lesscertainevidence),becauseadrugthatissubstantiallylessefficaciousortolerablethanitscompeti-torsisunlikelytobewidelyused,butthefullimpactofapoten-tially serious adverse eventmaynotbecomeclearuntil a largenumberofpatientshavebeenexposed.
Drug Manufacturer Price Discounts and RebatesBothstatutorydrugpricingandadditionaldiscountsandrebatesofferedbymanufacturersbasedon formularystatusdiffer sub-stantiallyamongDoD’spharmacypointsofservice.Militaryphar-maciesareDoD’sleastcostlypointofservice;theCongressionalBudgetOfficeestimated that, in2003,DoDpaidanaverageof41%ofaveragewholesaleprice(i.e.,a59%discount) forbranddrugsdispensedbymilitarypharmacies,thelowestpricepaidbyallfederalprograms.22Bylaw,atmilitaryfacilitiesandthemail-orderprogram,pricesforbrand-namepharmaceuticalsmustbeatleast24%belowtheaveragemanufacturerpricefornonfederalpurchasers,basedonTitle38oftheU.S.Code,asamendedbyPublicLaw102-585,VeteransHealthCareActof1992.23,24 Thiscalculation establishes the federal ceiling price; prices on theFederalSupplySchedule,whichisadministeredbytheVA,mustbeatorbelowthefederalceilingprice,withsomemanufacturersofferingadditionaldiscounts.25
The process available to manufacturers to offer additional,competitive discounts based on Uniform Formulary or BCF/ECFstatusatmilitarypharmaciesandmailorderistheUniformFormulary Blanket Purchase Agreement (UF BPA). Under theUFBPAprocess, the lowerpricesofferedbymanufacturersaredirectly available tomilitary facilities and themail-orderphar-macythroughpharmaceuticalwholesalerswithoutrequiringspe-cialorderingprocedures.Theadditionaldiscountsgointoeffectgenerallywithin2weeksofapprovalofformularyrecommenda-tionsbytheAssistantSecretaryofDefenseforHealthAffairs.TheUFBPAagreementsareadministeredbyTRICAREManagementActivitycontractingpersonnelinAurora,Colorado.
Historically, TRICARE has incurred much higher costs fordrugsdispensedatcommunitypharmaciesthanatmilitaryphar-maciesormailorder,sincepricesfordrugsdispensedbycom-munitypharmacyarenotgovernedbystatute.AlthoughthepricedifferentialbetweencommunitypharmaciesandDoD’sother2pointsofservice isexpectedtonarrowasrecentlyenactedleg-islationisimplemented(seebelow),26thecommunitypharmacynetworkcontinuestobeDoD’smostcostlypointofservice.InFY2007,about64%ofDoDdrugexpenditures—butonly37%ofallDoD30-dayequivalentprescriptionfills—wereincurredat the
Formulary Management in the Department of Defense

www.amcp.org Vol. 15, No. 2 March 2009 JMCP Journal of Managed Care Pharmacy 140
Formulary Management in the Department of Defense
key assumptions in themodel (e.g., the likelihoodof apatientswitching to a formularymedication).31 The results of the PSAareexpressedasarangeoflikelyoutcomes(lower2.5%toupper97.5%) in total expenditures. Although not a true confidenceintervalinastatisticalsense,theupperandlowerlimitsprovidedecision-makers some insight into the uncertainty associatedwiththecalculatedbudgetimpactofvariousformularyscenarios.One-way sensitivity analysis, which evaluates the uncertaintyaround a single-point estimate, may be used to illustrate theimportance of assumptions around individual parameters thatmighthaveaparticularly substantial effectonanticipatedcost,suchasthefutureavailabilityofgenericmedications.
Cost-effectivenessevaluatorstypicallybeginconstructingtheirmodelswellbeforepricequotesareavailablefrommanufacturers,basedonthefindingsoftheclinicaleffectivenessevaluationandreview of the pharmacoeconomic literature.Manufacturers areaskedtoincluderelevantpharmacoeconomicstudiesandmod-elsaspartoftheirAMCPdossiersubmissions.Ingeneral,fewermanufacturerssubmitpharmacoeconomicinformationthansub-mitclinicalinformation;thePEChasfoundsubstantialvariabilityamongpharmacoeconomicanalysespreparedbymanufacturers,particularlywithregardtotransparencyofmodelsandwilling-nesstoprovide“unlocked”copiesforanalysis.Manufacturersarealsoallowedtopresentpharmacoeconomicmodelsorstudiestothe team, typically during 1-hour face-to-facemeetings (whichoftenfollowclinicalpresentations).Thesemeetingsmayprovideuseful information aboutmethodology and study assumptions;
however,theteamconstructsitsmodelsindependently.Costevaluatorsmayuseanyofthe4basictypesofpharma-
coeconomicanalysis—costminimization,cost-effectiveness,costutility,orcost-benefitanalysis—tocomparemedicationswithinaclass.19
Cost-Minimization Analysis: This analysis is used wheneffectivenessmeasuresforcompetingmedicationsareassumedtobeequal.Thelowest-costmedicationisconsideredtobethemostcost-effective. For example, clinical evaluations of the protonpumpinhibitor(PPI)class,bothin2005andin2007,foundnosignificantdifferenceswithrespecttosafetyandefficacyamongPPIs.32Ananalysisoftheweighted average cost per dayofPPItreat-ment(weightedtonormalizethecostforeachdrugbasedonthepercentmarket share at eachpoint of service across the entiredrug class) was therefore sufficient to rank the PPIs from themostcost-effectivetothe leastcost-effective;normalizingbasedonmarketshareisnecessarytoavoiddisadvantagingmedicationsthatareusedinhigherproportionathigher-costpointsofservice.In2005,esomeprazolewasdetermined tobe lesscost-effectivethansimilaragentsandwasplaced intier3 todiscourageuse.However, because of a competitive bid from themanufacturerof esomeprazole, in 2007 the military treatment facility cost(andweightedsystemcost) forthePPIs, fromlowesttohighestweightedsystemcost,were$0.50($0.70)forgenericomeprazole10mgand20mg,$0.39($1.15)perdayforesomeprazole,$2.84($3.20) for rabeprazole, $2.70 ($3.64) for lansoprazole, $3.44($3.84) for pantoprazole, $3.16 ($4.40) for omeprazole-sodium
TABLE 3 FY 2007 DoD Utilization, Expenditures, and Cost Savings Estimates Attributed to the UF Process, by Pharmacy Type (Point of Service)a
Point of ServiceRxs
(Millions)
30-day Equivalent Rxsb
(Millions)
Drug Expenditures
(Millions)
Estimated Cost Avoidance Due to
UF Changesc,d
(Millions)
UF VARR Rebatese
(Millions)
Estimated Total Cost Without UF Process (Millions)
MilitaryPharmacies 49 80 (48%) $1,470 (23%) $754 (81%) - $2,224
CommunityPharmacies 63 63 (37%) $4,177 (64%) $90 (10%) $60f $4,327
MailOrder 9 25 (15%) $857 (13%) $82 (9%) - $939
Total 121 168 (100%) $6,504 (100%) $926(100%)g $60 $7,490aThe federal fiscal year is from October 1 through September 30.bNormalizes workload between points of service based on 30-day supplies of medications (90 days supply = three 30-day equivalents); calculated as total days supply/(30 × total number of Rxs). cFor classes with at least 6 months of cost avoidance data in FY 2007.dUF cost avoidance was calculated on a month-by-month basis as the difference between the theoretical cost that would have occurred if a UF decision had not been made and the actual cost. The analysis used the days of therapy in a given month, adjusted by baseline market share, cost, and copayments, to estimate what the cost to the DoD would have been in the absence of a UF decision (the theoretical cost). Drug prices used to calculate the theoretical cost were based on Federal Supply Schedule prices at military pharmacies and mail order and current ingredient costs at community pharmacies. The actual cost includes price reductions at military pharmacies and mail order based on accepted bid prices in effect after implementation of UF changes, as well as cost reductions resulting from movement away from tier 3 drugs and toward lower-cost points of service. This methodology takes into account the aggregate effect of price changes, overall drug class growth, and cost and copayment differ-ences due to migration between drugs or points of service, but does not allow isolation of these factors. eUF VARR consists of a quarterly rebate paid to the DoD by drug manufacturers based on utilization in the community pharmacy network. fImplemented in August 2006, estimated at $200 million or more in FY 2008, as more classes are reviewed. gUpdated; the U.S. Government Accountability Office estimated $900 million in an October 2007 report (GAO-08-172R).28 DoD = Department of Defense; FY = fiscal year; Rx = prescription drug claim; UF = Uniform Formulary; VARR = Voluntary Agreement for TRICARE Retail Pharmacy Refunds.

141 Journal of Managed Care Pharmacy JMCP March 2009 Vol. 15, No. 2 www.amcp.org
Formulary Management in the Department of Defense
bicarbonate,and$3.71($4.92)foromeprazole(Prilosec)40mg.8 Thesefindingscausedacompletereversalinformularyposition:esomeprazolewasnotonlyremovedfromtier3,butalsomadeavailableatthetier1(generic)copayment;allotherPPIsexceptgenericomeprazolewereplacedintier3.
Cost-Effectiveness Analysis: When effectiveness measuresforcompetingmedicationsareassumedtobedifferent,asitua-tionthatappliestomanydrugclasses,cost-effectivenessanalysiswill be employed. Often, differences may be seen on severalefficacyorsafetymeasures,andaseriesofmodelsmaybeusedto compare competing products. For example,models used toassessthecost-effectivenessofthelow-densitylipoproteincholes-terol(LDL-C)-loweringmedicationsintheAntilipidemic-1drugclass(medicationsabletoprovideatleasta45%meanreductioninLDL-C:atorvastatin,40mgormoreperday;rosuvastatin,10mgormoreperday;simvastatin,80mgperday;orsimvastatin,20mgincombinationwithezetimibe)includedtheannualcostper1%reductioninLDL-C,aswellastheannualcostforeachpatienttreatedtoLDL-Cgoal.Theexpectationisthatasimilarrankingacrossmultiplemodelsusingdifferentmeasureswouldprovidegreaterconfidenceinthemodelresults.
Cost-Utility Analysis:Thistypeofcost-effectivenessanalysismeasures treatment outcomes in quality-adjusted life years orsomeotheroutcomemeasurebasedonpatientpreferencesamongpossiblehealthstates.Thisapproachisusefulbecauseitcanfacil-itatecomparisonsamongdifferenthealthcareinterventions.20
Cost-utility analysis was used to analyze attention deficithyperactivity disorder medications. Clinical efficacy, based onpercentage of responders, was found to be similar among thedifferentmedications.However, several studies reportedhigherpatientandparentpreferencesforstimulantsthatrequirefewerdailyadministrations(ofparticularimportanceinthistherapeu-ticclasstoavoidtheneedfordosingduringtheschoolday).33,34
Thetypeofmedication(stimulantversusnonstimulant)alsohasbeenshowntoaffectqualityoflife.Inthisinstance,cost-utilityanalysis successfully combined the important outcomes into asinglecompositemeasureandallowed thecommittee toassesstherelativevalueofthemedications.
Cost-Benefit Analysis: This technique allows for differingeffectivenessacrosscompetingmedications,butrequiresboththecostoftreatmentandthemeasureofbenefittobeexpressedinmonetaryunits.Thisrequirementposessomepracticalandethi-calcomplicationsandhasnotbeenusedforanyclassreviewedtodate.
Budget Impact Analysis: Cost-effectiveness analyses aloneare not sufficient to assess the pharmacoeconomic impact offormularydecisions,becauseotherfactorsthatmaychangeasaresultofthedecisionmustbeconsidered.Budgetimpactanalysisis used as part of theUniform Formulary process to comparethefinancialimpactofdifferentformularyscenarios.Thebudgetimpactanalysisaccountsforsuchfactorsascopaymentchanges,potential migration of patients between pharmacy points of
service, anticipated changes in market share for medicationswithinaclass,costassociatedwithmedicalnecessitydetermina-tions, and additional health care service costs associated withmedicationswitches.Itisconductedasthefinalstepinthecost-effectivenessevaluation.
Migrationtopreferredmedicationsoccursovermonthsratherthanminutesafteraformularychangeisimplemented.Forthisreason,Markovmodelsthatincorporatemedicationdiscontinu-ationrates,switchingrates,andtherateofnewpatientstartsateachpointofserviceareusedtoestimatetheimpactofvariousformularyscenariosovera2-to3-yeartimehorizon.
Formulating a Cost-Effectiveness ConclusionUponcompletionofthepharmacoeconomicandbudgetimpactanalyses, the PEC presents a cost-effectiveness conclusion tothe DoD P&TCommittee. This conclusion considers the rela-tivevalueofproductswithina therapeuticclass, theestimatedexpenditures associatedwith various formulary scenarios, andthe impact of uncertainty on the study results. The final cost-effectiveness conclusion incorporates the committee’s judgmentwith respect to the results of pharmacoeconomic and budgetimpact analyses, trade-offs associated with uncertainty aboutfuturedevelopments, and the impactof various formulary sce-nariosonbeneficiaries.
DoD P&T Committee MeetingFindings from the cost-effectiveness evaluation are presentedonlyafterthecommitteehasdiscussedandagreeduponaclini-cal-effectivenessconclusion.Thecommitteethenvotestorecom-mendmedicationstobeincludedontheUniformFormulary(tier1or2)orclassifiedasnonformulary(tier3).Whenmakingtier3 recommendations, the committee also establishes an imple-mentationperiod(nolongerthan180days)andoutlinesmedicalnecessity criteria. The committee then decideswhichUniformFormularymedication(s)shouldbeaddedtotheBCF/ECF.
Whenplacingmedicationsontier3oftheUniformFormulary,the committee must consider the effect on beneficiaries usingcommunity networkpharmacies andmail order (available at ahighercopayment)versusmilitaryfacilities(notavailableunlessmedicallynecessary,andthenonlyifwrittenbyamilitarypro-vider or a civilianprovider towhich thepatientwas referred).Thecommitteemustalsoestablishmedicalnecessitycriteriaforeach tier 3 drug, to be used both bymilitary facilities (whicharerequiredtousemedicalnecessitycriteriaestablishedbytheDoDP&TCommitteefortier3medications)andthecommunitypharmacynetworkandmail-ordercontractor(sincepatientsmayreceivetier3medicationsatthetier2copaymentatcommunitypharmaciesandmailorder,ifdeterminedtobemedicallyneces-sary).
Medicalnecessitycriteriaarebasedonuseofthetier3agentin lieu ofallsimilartier1and2medications.Medicalnecessitycrite-riaarebasedonthe5generalconditionsoutlinedintheUniform

www.amcp.org Vol. 15, No. 2 March 2009 JMCP Journal of Managed Care Pharmacy 142
donot include specific cost comparisons,becausepricequotessubmittedbymanufacturersareproprietaryandconfidential.
TheDoDP&TCommitteetypicallyreviews2-4drugclassesduringeachquarterlymeeting,spending2-4hoursoneachdrugclass,dependingoncomplexity.ThecommitteealsoreviewsnewFDA-approveddrugsandfollow-upreportsonpreviousformu-larydecisions.
Weighing Costs Versus EffectivenessItisoftendifficulttoincorporateallclinicaldifferencesbetweenmedications into pharmacoeconomic models; for example, ifdataareavailableonlyforsomeagentswithinaclass,iftheriskand/orcostsassociatedwithseriousadverseeffectsareunclear,or if time and resource limitations preclude detailed analysisacross all FDA-approved indications. In this case, the DoDP&TCommitteemustweigh thepotentialvalueof suchdiffer-encesalongside results fromthecost-effectivenessanalysis.Forexample, during its review of the targeted immunomodulatorybiologics(i.e.,adalimumab,alefacept,anakinra,efalizumab,andetanercept),thePECperformedcost-effectivenessanalysescom-paringtheseagentsforthetreatmentofrheumatoidarthritisandplaquepsoriasis,whichtogethercompriseabout88%ofallusebyDoDbeneficiaries(basedonmedicalclaimsdata).However,the committee also considered the clinical usefulness of the 2agentswithmultipleindications(adalimumabandetanercept)inotherdiseasestates(e.g.,ankylosingspondylitis,Crohn’sdisease,psoriatic arthritis, juvenile rheumatoid arthritis, and ulcerativecolitis).Twoofthemedicationsinthisclass(etanerceptandanak-inra)weredesignatedastier3,whereastheother3medicationswereretainedintier2.
Inaddition,thecommitteemustmakevaluejudgmentsbasedonrelativecost-effectiveness.Althoughthemostandleastcost-effective agents are readily identified, the committee alsomustmake formulary recommendations for agents that fall betweenthe two extremes. Incremental cost-effectiveness ratios are cal-culated as the ratio of the difference in costs to the differenceinefficacybetweeneachdruginaclassandthenextlesscost-effective.Itisalsohelpfulconceptuallytoshowwhereeachdrugfallswithin1ofthe4quadrantsof thecost-effectivenessplane(lesscostly/moreeffective, lesscostly/lesseffective,morecostly/moreeffective,andmorecostly/lesseffective).20
The committee’s final recommendation is also affected byresultsofthebudgetimpactanalysis,whichevaluatestheoverallimpact(affordability)ofvariousformularyscenarios,typicallyover1-,2-,and3-yeartimehorizons.Asdiscussedearlier,probabilis-ticsensitivityanalysisisusedinconjunctionwithbudgetimpactanalysis to provide the committee with a range (2.5%-97.5%)of projected total expenditures associatedwith each formularyscenario, which enables committee members to evaluate bothbest-caseandworst-casescenariosandthedegreeofuncertaintyassociatedwitheachscenario.
FormularyRule(aslistedbelow),2whichmayormaynotapplyinaspecificdrugclassdependingonthenatureofthedrugclassandthecharacteristicsofthetier3medication.
1.Theuseofformularypharmaceuticalagentsiscontraindi-cated.
2. The patient experiences significant adverse effects fromformularypharmaceuticalagents in the therapeuticclass,or is likely to experience significant adverse effects fromformularypharmaceuticalagentsinthetherapeuticclass.
3. Formulary pharmaceutical agents result in therapeuticfailure,ortheformularypharmaceuticalagentislikelytoresultintherapeuticfailure.
4.Thepatientpreviouslyrespondedtoanonformularyphar-maceuticalagent,andchangingtoaformularypharmaceu-ticalagentwouldincuranunacceptableclinicalrisk.
5.Thereisnoalternativepharmaceuticalagentontheformu-lary.
The committee also identifies specific circumstances underwhich the tier 3 medication would be considered medicallynecessary. For example, medical necessity criteria for tier 3PPIs (lansoprazole,pantoprazole,omeprazole/sodiumbicarbon-ate,andrabeprazole),effectiveOctober24,2007, includeeitherdocumented“significantadverseeffectswithalloftheformularyalternatives: omeprazole (Prilosec; generics) and esomeprazole(Nexium)”or“useofallof the following formularyalternativeshas resulted in therapeutic failure:omeprazole (Prilosec;gener-ics)andesomeprazole(Nexium).”35Themedicalnecessitycriteriafor thePPIs also allowuseof lansoprazole inpatients youngerthan12years,basedonclinical literature supportingpediatricuseandtheavailabilityofliquidandorallydisintegratingtabletformulations.
Thecommitteeisalsoresponsibleforestablishingpriorautho-rization requirements and quantity limits. TRICARE does notcover drugs that require prior authorization (e.g., growth hor-mone)unlesspatientsmeetspecificcriteria(e.g.,growthhormonedeficiency).Quantitylimitsarebasedonunitsper30-or90-daysupply and applyunless a greater amount is determined tobemedicallynecessary(e.g.,higherthanusualamountsofatopicalproductwhen used to treat a condition affecting an unusuallylargepercentageofbodysurfacearea).Thesamegeneralrequire-mentsapplytomilitarypharmacies;however,whilePDTSscansall pharmacy claims includingmilitary pharmacy prescriptionfills when identifying prior use and quantities dispensed, theinterfacebetweenPDTSandthepharmacymanagementsystemcurrently used atmilitary pharmacies does not support PDTSreject messages. Quantity limits and prior authorizations arethereforeadministeredlocallybyeachmilitaryfacility.
Minutesofeachmeetingincludeasummaryofcommitteerec-ommendationsalongwithsupportinginformationfromtheclini-calandcost-effectivenessevaluations.Themeetingminutesalsocontaindescriptionsofthepharmacoeconomicmodelsusedandtherelativecost-effectivenessrankingsbasedonthosemodelsbut
Formulary Management in the Department of Defense

143 Journal of Managed Care Pharmacy JMCP March 2009 Vol. 15, No. 2 www.amcp.org
The Beneficiary Advisory Panel MeetingDoD’sBeneficiaryAdvisoryPanel(BAP)is intendedtoenhancetransparency and provide an opportunity for beneficiaries andtheir representatives to comment on the committee’s recom-mendationsbeforefinalapproval.BAPmembers(nomorethan15 individuals appointed on an annual basis by the SecretaryofDefense to represent the interestsofTRICAREbeneficiaries)meetinapublicforumunderprovisionsoftheFederalAdvisoryCommitteeAct,about6weeksaftereachDoDP&TCommittee.
BAP membership includes representatives from nongovern-ment organizations and associations that represent the viewsandinterestsofalargenumberofeligiblecoveredbeneficiaries,contractors responsible for the community pharmacy networkand mail-order program, and TRICARE network providers.36
Beneficiary organizations currently represented on the BAPare the Fleet Reserve Association, the Military Coalition, theMilitaryFamiliesAssociation, theMilitaryOfficersAssociationofAmerica,theMilitaryAlliance,andtheNationalMilitaryandVeteransAlliance.
MeetingsareannouncedintheFederal Register, withallsup-portingmaterialspostedontheBAPpageontheTRICAREwebsite.37InformationdiscussedattheBAPmeetingdoesnotincludespecific drug pricing or financial information and focuses onUniformFormularydecisionsandpriorauthorizations.TheBAPdoesnotreviewBCF/ECFdecisionsorquantitylimits.PECstaffmembersprovideabriefpresentationexplainingtheclinicalandcost-effectiveness evaluations of each class and are available toanswerquestions;inaddition,1ofthephysicianmembersofthecommitteeispresenttoaddressquestionsaboutthecommittee’srationaleforitsrecommendationsineachclass.
AmajorfocusoftheBAPfromitsinceptionhasbeenontheprocessofimplementationofUniformFormularydecisions,espe-ciallytheprocessofcommunicationwithbeneficiaries.Feedbackfrom the BAPwas instrumental in theDoD’s decision to startsending targeted letters to affectedbeneficiariesduring theup-to-180-day implementation period before drugs are placed ontier3.TheBAPfrequentlycommentsonproposedimplementa-tionperiods,whichhavebeen lengthenedonseveraloccasionsto allowmore time for communication with beneficiaries. Forexample,afteraFebruary2006reviewofmedicationsforoverac-tivebladder,theDoDP&TCommitteerecommendeda60-dayimplementation period for classifying tolterodine immediaterelease, oxybutyninpatch, and trospiumas tier3medications;theBAPrecommended120days;andtheAssistantSecretaryofDefense forHealthAffairs approved an implementation periodof90days.Asinmanycases,thelengthoftheimplementationperiodinthisclasswasdeterminedtoachieveabalancebetweenallowingnecessary time forbeneficiarynotification versus costconsiderations,becauserebatesduetoDoDundertheUFVARRprogramforprescriptionsfilledatcommunitypharmaciesdonotbecomeeffectiveuntiltier3copaymentsgointoeffect.
Formulary Management in the Department of Defense
TABLE 4 Classes Reviewed Under the DoD Uniform Formulary as a Percentage of FY 2007a Expenditures
Rank Class
FY 2007 Drug Spend (Millions)
% of FY 2007 Total
1 Protonpumpinhibitors $530 8.1%
2 Antilipidemicsb $490 7.5%
3 Antidepressantsc $297 4.6%
4 Narcoticanalgesics $172 2.6%
5 Newerantihistamines $171 2.6%
6 Angiotensinreceptorblockers $166 2.5%
7 Thiazolidinediones $134 2.1%
8 Adrenergicbeta-blockingagents $133 2.0%
9 Newersedativehypnotics $125 1.9%
10 Leukotrienemodifiers $124 1.9%
11 Attention-deficit/hyperactivitydisorderandnarcolepsyagents
$108 1.7%
12 Alzheimersagents $97 1.5%
13 Calciumchannelblockers $97 1.5%
14 AntilipidemicsIId $77 1.2%
15 Contraceptives $67 1.0%
16 Overactivebladderagents $67 1.0%
17 Nasalcorticosteroids $63 1.0%
18 Multiplesclerosisagents $59 0.9%
19 Angiotensin-convertingenzymeinhibitors
$57 0.9%
20 GABAanalogse $56 0.9%
21 Ophthalmicglaucomaagents $55 0.8%
22 AlphablockersforBPHf $49 0.7%
23 Miscellaneousantihypertensives $47 0.7%
24 Antiemetics $41 0.6%
25 Phosphodiesterase-5inhibitors $38 0.6%
26 5-αreductaseinhibitors $38 0.6%
27 Macrolides/ketolides $29 0.4%
28 Growth-stimulatingagents $23 0.4%
29 Histamine-2antagonistsand gastrointestinalprotectants
$12 0.2%
30 Topicalantifungals $9 0.1%
31 Oldersedativehypnotics $3 0.0%
32 Monoamineoxidaseinhibitorantidepressants
$0.7 0.0%
$3,434 52.7%
aThe federal fiscal year is from October 1 through September 30.bAntilipidemics I = statins, niacin, and ezetimibe.cAntidepressants I = selective serotonin reuptake inhibitors, duloxetine, venlafaxine, nefazodone, trazodone, bupropion, and mirtazapine.dAntilipidemics II = fibrates, bile acid sequestrants, and omega-3 fatty acids.eGABA analogs = gabapentin, pregabalin, and tiagabine.fBPH = benign prostatic hypertrophy.GABA = gamma-aminobutyric acid.

www.amcp.org Vol. 15, No. 2 March 2009 JMCP Journal of Managed Care Pharmacy 144
Approval of DoD P&T Committee Recommendations AftertheBAPmeeting,DoDP&TCommitteeminutesandBAPcomments are forwarded to theAssistant Secretary ofDefensefor Health Affairs (who is also the director of the TRICAREManagementActivity)forreviewandapproval.Thesigningdatefor themeetingminutesbegins theUniformFormulary imple-mentationperiodforeachclass.DoDP&TCommitteeminutes,BAPcomments,andfinalapprovaldecisionsarepublishedontheTRICAREwebsite.4
Classes ReviewedThrough April 16, 2008, DoD P&T Committee recommenda-tionshavebeenapprovedand implemented in32drugclassesreviewed at 12 quarterlymeetings, representing 53% ofDoD’stotal drug spend (based on total FY 2007 expenditures). Theclass-by-class review process resulted in the classification of343drugs,ofwhich85drugs(24.8%)wereplacedintier3,92(26.8%)intier2,and166(48.4%)intier1.Theclassesaresum-marizedinTable4.
Continuing ChallengesDoDfacesongoingchallengesastheformularydecision-makingprocess continues to evolve, some of which are not found intheprivate sector.For example, theFY2008NationalDefenseAuthorizationAct(NDAA)extendedfederallymandatedgovern-mentpricingtomedicationsprovidedthroughDoD’scommunitynetwork.38 A proposed rule to implement these provisions ofthe 2008 NDAA was published in the Federal Register in July2008 for public comment.26 In brief, the proposed rulewouldrequiremanufacturerstoprovidetheDoDwitharefundbasedonthedifferencebetweentheaveragepricesofferedtononfederalpurchasers and the currently mandated Federal Ceiling Price,the maximum price paid by military facilities and the mail-orderprogramforbranddrugs,althoughmilitaryfacilitiesoftenreceivelowerpricesundertheFederalSupplyScheduleprogram.Although it is clear that implementationof federal pricingwillreducetheDoD’soverallexpendituresatitsmostcostlypointofservice,itisnotyetclearwhattheimpactwillbeattheotherDoDpharmacypointsofservice.
AnotherchallengefacingDoD—aswithprivate-sectorhealthplans—iseffectivecommunicationofformularychangestoben-eficiaries and providers. Many beneficiaries receive their carefromprovidersoutsideofmilitaryfacilities,whoarelikelytobeunfamiliarwiththeformularystatusandout-of-pocketcostsforthemedications that they prescribe.39 DoD has taken steps toimprovecommunicationwithbeneficiariesregardingformularychanges;beginninginOctober2007,patient-specificnotificationlettersaremailedtobeneficiariescurrentlyreceivingmedicationsthatwillbeplacedontier3.Theextenttowhichtheselettersarereadandacteduponisnotknown.DoDalsoistakingstepstoprovide theUniformFormulary and the BCF/ECF inNationalCouncilforPrescriptionDrugProgramsFormularyandBenefit
Formulary Management in the Department of Defense
Standardformat,40bothtofacilitateaccessbycivilianprescribersandtosupportfuturee-prescribinginitiatives.41DoDformularyinformation,includingtheUniformFormularyandtheBCF/ECF,is currently available online in a searchable format for use bybeneficiariesandproviders.42Inaddition,manymilitaryfacilitiesprovideonlineformularylistingsfortheirlocalformularies.
WiththeUniformFormularyinitsthirdyear,DoDalsofacesthe challenge of assessing the clinical outcomes of formularychanges made under the Uniform Formulary. Such analysisserves to (a) ensure that changes actuallymaintainor improveclinical outcomes while lowering DoD pharmacy costs, and(b) provide data that can be used to improve the accuracy ofpharmacoeconomic and budget impactmodels.43,44 The goal istoroutinelyincorporatesuchimprovedmeasuresintotheformu-larymanagementprocess.Asanexampleofthelatter,thePECmadeanefforttovalidateprojectionsfrombudgetimpactmodelsusingactualhealthplandata followinga formularydecisioninthe Antilipidemic I class (statins, niacin, and ezetimibe). Theanalysiscomparedoutcomessuchas thepercentageofpatientswhoswitchedfromnonpreferredtopreferredproductsfollowingcopaymentchangeswithpredictedmodeloutputstotestavarietyofassumptionscommonlyused inbudget impactmodels.Asaresultoftheanalysis,severalchangestocommonmodelparam-etersweremade, including assumptions about generic pricing,marketshareconversion,andgrowthprojectionsconcerningthenumberofuniqueusersinaclass.
■■ ConclusionTheneedforatransparentandcohesiveprocesshasguidedthedevelopmentofaformularymanagementsystemintheDoDthataccomplishes anumberof goals.Likeprivatehealthplans, theDoDformularymanagementsystemisbasedoncriticalevalua-tionoftheevidenceforsafety,efficacy,andtolerabilityofmedica-tionswithindefineddrugclasses,includingpharmacoeconomicanalysis. Unlike private health plans, the DoD requires moretransparentandequitablepricecompetitionamongpharmaceuti-calmanufacturersbasedonformularystatus.Alsounlikeprivatehealthplans,theBAPservesasapublicforumforbeneficiariesandbeneficiaryorganizationstocommentonformularychanges,andtheDoDformularyprocessincludestheconductofsurveysto obtain opinions of providers for consideration by the P&Tcommittee.
TheDoD formularymanagement process and3-tier formu-larywere estimated to avoiddrug costs of $926million inFY2007,plusanadditional$60millioninrebatesobtainedthroughtheUniformFormularyVARRprocessforprescriptionsfilledatcommunitypharmacies.AsofApril2008,UniformFormularydecisionshadbeenimplementedin32drugclasses,representingmorethan53%of totaldrugexpenditures, including85branddrugsplacedintier3,24.8%ofthetotalof343brandandgenericdrugs,or48.0%ofthe177branddrugsreviewed.

145 Journal of Managed Care Pharmacy JMCP March 2009 Vol. 15, No. 2 www.amcp.org
Formulary Management in the Department of Defense
DISCLOSURES
ThisstudywasfundedsolelybyDoD.AllauthorsareemployedbytheDoDandholdnoaffiliationwithorganizationsthatmayincurafinancialbenefitas a result of thiswork being published. Permission to release thismanu-script for public reviewwas issuedby theDoDDirectorate for FreedomofInformationandSecurityReviewonApril1,2008.
Trice,Mistry,Moore,andLintoncontributedtotheconceptanddesignofthisreport.Allauthorscontributedtowritingthisreport,andrevisionwasperformedprimarilybyTriceandDevine.
ACKNOWLEGEMENTS
The authors gratefully acknowledge the assistance of Rear Adm. ThomasMcGinnis, U.S. Public Health Service, Chief, Pharmaceutical OperationsDirectorate, TRICARE Management Activity; Lt. Col. Thom Bacon, USAF,Director, DoD Utilization Management, Pharmaceutical OperationsDirectorate,TRICAREManagementActivity; Lt.Col. BrettKelly,USA; andMaj.WadeTiller,USAF.
DISCLAIMER
Thethoughtsandopinionsexpressedinthispaperarethoseoftheauthorsand do not necessarily represent the official policy or position of the U.S.DepartmentofDefense.
REFERENCES
1.PromotingQualityandEfficientHealthCareinFederalGovernmentAdministeredorSponsoredHealthCarePrograms.PresidentialExecutiveOrderNo.13410,3C.F.R.Availableat:http://edocket.access.gpo.gov/cfr_2007/janqtr/pdf/3CFR13410.pdf.AccessedSeptember8,2008.
2.U.S.CodeofFederalRegulations.Civilianhealthandmedicalpro-gramoftheUniformedServices:pharmacybenefitsprogram(32C.F.R.Sect.199.21).Availableat:http://edocket.access.gpo.gov/cfr_2007/julqtr/32cfr199.21.htm.AccessedSeptember1,2008.
3.DepartmentofDefenseTaskForceontheFutureofMilitaryHealthCare.Finalreport(December2007).Availableat:www.dodfuturehealthcare.net. AccessedSeptember1,2008.
4.TRICAREManagementActivity.TRICAREPharmacywebsite.Availableat:www.tricare.mil/pharmacy.AccessedJanuary13,2008.
5.HealthAffairsPolicy04-032.TRICAREPharmacyBenefitProgramFormularyManagement(December22,2004).Availableat:www.ha.osd.mil/policies/2004/04-032.pdf.AccessedSeptember1,2008.
6.ClarificationtoHealthAffairsPolicy04-032.TRICAREPharmacyBenefitProgramFormularyManagement(March22,2005).Availableat:www.ha.osd.mil/policies/2004/04-032_clarification.pdf.AccessedSeptember1,2008.
7.MTFFormularyManagementforAngiotensinReceptorBlockers(ARBs).Availableat:www.pec.ha.osd.mil/MTF/ARB_MTF_Formulary_Management_Aug07.pdf.AccessedDecember10,2008.
8.MTFFormularyManagementforProtonPumpInhibitors(PPIs).Availableat:www.pec.ha.osd.mil/MTF/PPI_MTF_Formulary_Management_Jul07.pdf. AccessedDecember10,2008.
9.DoDPharmacoeconomicCenter.FuturemeetingsoftheDoDP&TCommittee.Availableat:www.pec.ha.osd.mil/PT_Committee.htm.AccessedSeptember1,2008.
10.OxfordCentreforEvidence-basedMedicine.Levelsofevidence(May2001).Availableat:www.cebm.net.(EBMTools).AccessedJanuary12,2008.
11.TheCochraneCollaboration.Homepage.Availableatwww.cochrane.org.AccessedSeptember1,2008.
12.DrugEffectivenessReviewProject.Homepage.Availableat:www.ohsu.edu/ohsuedu/research/policycenter/DERP/index.cfm.AccessedSeptember1,2008.
13.AgencyforHealthcareResearchandQuality.TechnologyAssessments.Availableat:www.ahrq.gov/clinic/techix.htm.AccessedSeptember1,2008.
14.NationalInstituteforClinicalExcellence.PublishedAppraisals.Availableat:www.nice.org.uk/Guidance/TA/Published.AccessedSeptember1,2008.
15.CanadianAgencyforDrugsandTechnologyinHealth.HealthTechnologyAssessment.Availableat:www.cadth.ca/index.php/en/hta. AccessedSeptember1,2008.
16.PettitiDB.Meta-analysis, decision analysis, and cost-effectiveness analysis. Oxford:OxfordUniversityPress;2000:264-71.
17.FullertonDS,AtherlyDS.FormularydevelopmentatRegenceBlueShield—aformulaforsuccess.Value Health. 2002;5(4):297-300.
18.SullivanSD,LylesA,LuceB,GrigarJ.AMCPguidanceforsubmis-sionofclinicaleconomicevaluationtosupportformularylistinginU.S.healthplansandpharmacybenefitsmanagementorganizations.J Manag Care Pharm.2001;7(4):272-82.Availableat:www.amcp.org/data/jmcp/Research-272-282.pdf.
19.FoundationforManagedCarePharmacy.The AMCP format for formulary submissions. Version 2.1: a format for the submission of clinical and economic eval-uation data in support of formulary consideration by managed health care systems in the United States.Alexandria,VA:AcademyofManagedCarePharmacy;2005.
20.DrummondMF,SculpherMJ,TorranceGW,O’BrianBJ,StoddartGL.Methods for the economic evaluation of health care programmes.3rdEd.Oxford:OxfordUniversityPress;2005.
21.MinutesandDecisionPaperontheDoDPharmacyandTherapeuticsCommitteeMeeting—13June2008—Signed27August2008.Availableat:www.tricare.mil/pharmacy/PT_Cmte/default.htm.AccessedDecember10,2008.
22.TheCongressoftheUnitedStates.CongressionalBudgetOffice.Pricesforbrand-namedrugsunderselectedfederalprograms(June2005).Availableat:www.cbo.gov/ftpdocs/64xx/doc6481/06-16-PrescriptDrug.pdf. AccessedSeptember1,2008.
SHANA TRICE, PharmD, BCPS, is Clinical Pharmacy Analyst, DoD TRICARE Management Activity, Pharmaceutical Operations Directorate, DoD PEC; JOSHUA DEVINE, PharmD, PhD, is a Major in the U.S. Air Force and the Air Force Pharmacy Consultant to the DoD PEC; HARSHA MISTRY, PharmD, and EUGENE MOORE, PharmD, BCPS, are Clinical Pharmacy Analysts, DoD TRICARE Management Activity, Pharmaceutical Operations Directorate, DoD PEC. ANDREA LINTON, MS, is Senior Research Associate, Office of the Assistant Secretary of Defense, Health Affairs, Health Programs Analysis and Evaluation.
AUTHOR CORRESPONDENCE: Shana Trice, Clinical Pharmacy Analyst, DoD PEC, 2450 Stanley Road, Suite 208, Fort Sam Houston, TX 78234. Tel.: 210.295.1271; Fax: 210.295.2789; E-mail: [email protected]
Authors

www.amcp.org Vol. 15, No. 2 March 2009 JMCP Journal of Managed Care Pharmacy 146
34.SecnikK,MatzaL,CottrellS,EdgellE,TildenD,MannixS.Healthstateutilitiesforchildhoodattention-deficit/hyperactivitydisorderbasedonpar-entpreferencesintheUnitedKingdom.Med Decis Making.2005;25:56-70.
35.TRICAREManagementActivity.TRICAREPharmacy:UniformFormularyMedicalNecessityCriteriaforProtonPumpInhibitors.Availableat:www.tricare.mil/pharmacy/ppi_mn_criteria.cfm.AccessedSeptember1,2008.
36.TRICAREManagementActivity.UniformFormularyBeneficiaryAdvisoryPanelCharter(July27,2006).Availableat:www.tricare.mil/pharmacy/bap/Signed%20Charter%20-%20July%202008.pdf.AccessedDecember12,2008.
37.TRICAREManagementActivity.HomepageoftheUniformFormularyBeneficiaryAdvisoryPanel.Availableat:www.tricare.mil/pharmacy/BAP/.AccessedJanuary13,2008.
38.LibraryofCongressTHOMASdatabase.Summary:nationaldefenseauthorizationactforfiscalyear2008(U.S.PublicLaw110-181),section703.Availableat:http://purl.access.gpo.gov/GPO/LPS96466.AccessedJanuary21, 2009.
39.ShrankWH,YoungHN,EttnerSL,GlassmanP,AschSM,KravitzRL.Dotheincentivesin3-tierpharmacybenefitplansoperateasintended?Resultsfromaphysicianleadershipsurvey. Am J Manag Care.2005;11:16-22.
40.NationalCouncilforPrescriptionDrugPrograms.NCPDPePrescrib-ingFactSheet.Availableat:www.ncpdp.org/eprescribing.asp.AccessedDecember10,2008.
41.DepartmentofDefenseawardsU.S.armedforcesformularymanagementcontracttoZynchros,Inc.Availableat:www.zynchros.com/news-events/news/2007/16oct-dod.asp.AccessedSeptember8,2008.
42.TRICAREManagementActivity.DoDFormularySearchTool.Availableat:www.tricareformularysearch.org/dod/medicationcenter/default.aspx. AccessedDecember10,2008.
43.FairmanKA,MotheralBR.Dodecision-analyticmodelsidentifycost-effectivetreatments?AretrospectivelookatHelicobacter pylori eradication. J Manag Care Pharm.2003;9(5):430-40.Availableat:www.amcp.org/data/jmcp/Formulary%20Management-430-440.pdf.
44.CoxER,MotheralB,MagerD.Verificationofadecisionanalyticmodelassumptionusingreal-worldpracticedata:implicationsforthecost-effectivenessofcyclo-oxygenase2inhibitors(COX-2s).Am J Manag Care. 2003;9(12):785-94.
23.U.S.Code.LimitationonpricesofdrugsprocuredbyDepartmentandcertainotherfederalagencies.Title38U.S.C.(Veteran’sBenefits),PartVI,Chap.81,Subchap.II,Sect8126.Availableat:www.gpoaccess.gov/uscode/index.html(searchfor“38USC8126”).AccessedJanuary13,2008.
24.VeteransHealthCareActof1992,Pub.L.No.102-585,Sect.603.Availableat:www.hrsa.gov/opa/pl102585.htm.AccessedJanuary13,2008.
25.DepartmentofVeteransAffairsNationalAcquisitionCenter.Federalsup-plyscheduleservice—pharmaceuticals.Availableat:www1.va.gov/oamm/oa/nac/fsss/pharmfss.cfm.AccessedJanuary13,2008.
26.FederalRegisterOnline.CivilianhealthandmedicalprogramoftheUniformedServices/InclusionofTRICARERetailPharmacyPrograminFederalProcurementofPharmaceuticals(July25,2008).2008:73(144):43394-97.Availableat:http://edocket.access.gpo.gov/2008/E8-17024.htm.AccessedSeptember1,2008.
27.TRICAREManagementActivity.Programinformationforpharmaceuti-calmanufacturers.Availableat:www.tricare.mil/pharm_mfg/default.cfm. AccessedSeptember12,2008.
28.UnitedStatesGovernmentAccountabilityOffice.DoDpharmacybenefitsprogram:reducedpharmacycostsresultingfromtheUniformFormularyandmanufacturerrebates;October31,2007.Report:GAO-08-172R.Availableat:www.gao.gov/new.items/d08172r.pdf.AccessedFebruary28,2008.
29.RussellLB,SiegelJE,DanielsN,GoldMR,LuceBR,MandelblattJS.Cost-effectivenessanalysisasaguidetoresourceallocationinhealth:rolesandlimitations.In:GoldMR,SiegelJE,RussellLB,WeinsteinMC,editors.Cost-Effectiveness in Health and Medicine.NewYork:OxfordUniversityPress;1996:3-24.
30.MauskopfJ,EarnshawS,MullinsCD.Budgetimpactanalysis:reviewofthestateoftheart.Expert Rev Pharmacoeconomics Outcomes Res. 2005;5(1):65-79.
31.BriggsAH.Handlinguncertaintyincost-effectivenessmodels.Pharmacoeconomics.2000;17(5):479-500.
32.MinutesandDecisionPaperoftheDoDPharmacyandTherapeuticsCommitteeMeeting-15-16May2007-Signed24July2007.Availableat:www.tricare.mil/pharmacy/PT_Cmte/default.htm.AccessedDecember10,2008.
33.MatzaLS,SecnikK,RentzAM,etal.Assessmentofhealthstateutilitiesforattention-deficit/hyperactivitydisorderinchildrenusingparentproxyreport.Qual Life Res. 2005;14:735-47.
Formulary Management in the Department of Defense