Embed Size (px)
Citation preview

Bupa Private and Confidential Date if required
1
Formative Opportunities in Disintegrated CareSchool for Social Care Research Annual Meeting May 2012
Clive Bowman Divisional Medical Director Bupa Care [email protected]

Spain
Sanitas
Sanitas Hospitals
Sanitas Residencial
3800 people in 38 homes,
United Kingdom
Bupa UK Membership
Bupa Health Assurance
Bupa Wellness
UK Care Services 18,700 people in over 300 homesHealthcare at Home
* Cromwell Hospital
Bupa Commissioning
China
Representative Office Beijing
Hong Kong
Bupa Hong Kong
Thailand
Bupa Thailand
Saudi Arabia
Bupa Arabia
Australia
Bupa Australia/ *MBF
Bupa Care Services3,693 residents in 48 homes
New Zealand
Bupa Care Services
2,809 residents
US
* Health Dialog
Bupa International:
Offices in Brighton, England; Copenhagen, Denmark; Miami, US; Dubai, UAE; Cairo, Egypt; and Hong Kong
Insurance businesses
Provision businesses
Integrated health services
India
* Max BupaCare Homes
Bupa 2012

Disease = Health ServiceSqualor = HousingIgnorance = educationIdleness = employmentWant = Social Insurance
Are we stuck in a mindset ?


Moulds can be broken
Bernard Isaacs: 1972 Survival of the unfittest ‐ analysed the various reasons for admission to geriatric wards: therapeutic option (expecting rapid recovery); medical urgency (needing hospital treatment); basic care (unfit to provide food, warmth, cleanliness and safety for themselves); or relief of strain on relatives.
Also the Geriatric Giants ‐ impairment of intellect (cerebral dysfunction), incontinence, immobility & instability (falls).

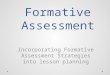
2003* 2006 2009Bupa Bupa United Kingdom Australia New Zealand Spain Full Census
Dementia 36% 38% 44% 53% 50% 46% 46%Heart Disease 10% 10% 21% 39% 47% 28% 27%Stroke 22% 21% 20% 18% 23% 9% 19%Diabetes 8% 9% 14% 18% 20% 20% 16%Arthritis 13% 12% 18% 25% 18% 16% 19%
* The 2003 Census only asked for primary reasons for admission to be counted, and did not count all medical diagnoses
36%38%
44%
53%50%
46% 46%
10% 10%
21%
39%
47%
28% 27%
22% 21% 20%18%
23%
9%
19%
8% 9%
14%
18%20% 20%
16%13% 12%
18%
25%
18%16%
19%
0%
10%
20%
30%
40%
50%
60%
Bupa Bupa United Kingdom Australia New Zealand Spain Full Census
2003* 2006 2009
Dementia Heart Disease Stroke Diabetes Arthritis
Leading diagnoses

Changing care home activity
Health
Dementia
Housing
Time
Activity

Care home trajectories today
Convalescence
Function
Time
Palliative care
Respite
Fluctuating illness
Chronic disease

The challenge in ageing today
Time
Function
To dying from & where’s the finish line
Where’s the transition from living with…..

Medicare analysis of dying
• 20% Short period of evident decline - typical of cancer. Most patients with malignancies maintain comfort and functioning for a substantial period. However, once the illness becomes overwhelming, the patient's status usually declines quite rapidly in the final weeks and days preceding death.
• 20% Long-term limitations with intermittent exacerbations and sudden dying - typical of organ system failure. Patients in this category often live for a relatively long time and may have only minor limitations in everyday life. From time to time, some physiological stress overwhelms the body's reserves and leads to a worsening of serious symptoms. Patients survive a few such episodes but then die from a complication or exacerbation, often rather suddenly. Ongoing disease management, advance-care planning, and mobilizing services to the home are key to optimal care.
• 20% Sudden death or not classifiable
• 40% Prolonged dwindling - typical of dementia, disabling stroke, and frailty. Those who escape cancer and organ system failure are likely to die at older ages of either neurological failure (such as Alzheimer's or other dementia) or generalized frailty of multiple body systems. Supportive services at home, like Meals on Wheels and home health aides, then institutional long-term care facilities are central to good care for this trajectory.
Adapting Health Care to Serious Chronic Illness in Old AgeJoanne Lynn, David M. AdamsonRand Health White Paper WP-137 (2003)

Moulds can be broken
Archie Cochrane’s Effectiveness and Efficiency Rock Carling lectureContributed to foundations to evidence based medicine and the role of theRandomised trial, what is often forgotten is the discussion about the problems of ageing. Cochrane did not foresee the potential of population data sets

Primary preventionPublic healthEducation
HousingDiagnosis and cure
Communities
Care and Support at homeSecondary prevention
Retirement and Pensions
Employmemt
End of Life Care
Management of long term conditionsNew “space” to be developed “Formative Care”

From Compliance
States a minimum performancestandard that everyone must achieve
Uses hierarchy, systems and standardprocedures for co-ordination andcontrol
Threat of penalties/sanctions/shamecreates momentum for delivery
Based on organisational accountability (“if I don't deliver this, I fail to meet my performance objectives”)
To Commitment
States a collective goal that everyonecan aspire to
Based on shared goals, values andsense of purpose for co-ordination andcontrol
Commitment to a common purposecreates energy for delivery
Based on relational commitment (“If Idon’t deliver this, I let the group orcommunity and its purpose down”)
From the old world to the new world
Source: Helen Bevan, NHS Institute of Innovation and Improvement, 2011

Care Home Shopping List
1. Purpose: understand (evolving) role and value in Health and Care, Research needed.
2. Capability: Develop positive attitudes and skills3. Resourcing: Talk to the Treasury on the basis of
evidence