Embed Size (px)
Citation preview
[National financial regulations]: 'purchase to pay' process /Health Service Executive
Item type Report
Authors Health Service Executive (HSE)
Rights HSE
Downloaded 17-Jul-2018 11:57:40
Link to item http://hdl.handle.net/10147/44495
Find this and similar works at - http://www.lenus.ie/hse
Foreword The new national financial regulations have been prepared, and must be applied, in the context of the primary objective of the Health Service Executive. This primary objective, as set out in the Health Act 2004, is to use the resources available to it in the most beneficial, effective and efficient manner to improve, promote and protect the health and welfare of the public. The public rightly expect high standards of accountability and probity in all that the HSE does and I know that all of our staff are committed to providing excellent services within this context. I hold strongly the view that if we are to move towards a world class health service then every aspect of what we do, our support processes as well as our direct service provision, must meet the highest standards. I see implementation and compliance with these financial regulations as a positive step forward for the HSE. Managers and staff at all levels and across all disciplines within the HSE are responsible and must take responsibility for the successful implementation of these regulations. My thanks goes to all those stakeholders who contributed to the process of compiling these regulations and in particular I would like to congratulate the National Finance Director and his team for their commitment and effort in bringing this important project successfully to this stage.
Professor Brendan Drumm Chief Executive Officer
Health Service Executive National Financial Regulations
Ver 1.3 Page 1 of 176
‘Purchase to Pay’ Process
Contents
MAIN CHAPTERS
Chapter Description Page No.
Introduction to Financial Regulations ................................................9
1. General Provisions regarding Financial Regulations........................10
2. Purchase to Pay (General) ...............................................................19
3. Purchase To Pay – Tendering Process..............................................46
4. Purchase to Pay – Specific Topics .....................................................56
5. Capital Projects and Property Transactions ......................................62 APPENDICES ………………………………………………(Page 68 to 176)
Additional Information Re; Chapter 1, Appendix ……………………………… on page 74
Chapter 2, Purchase to Pay (PTP) ……………… on page 76 Chapter 3 Tendering ……………………………… on page 95 Chapter 4 Non Order Payments ………………… on page 103 to 119 Chapter 5 Capital Projects & Property………… on page 124
INDEX …………………………………………………………………… on page 171 to 175
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 2 of 176
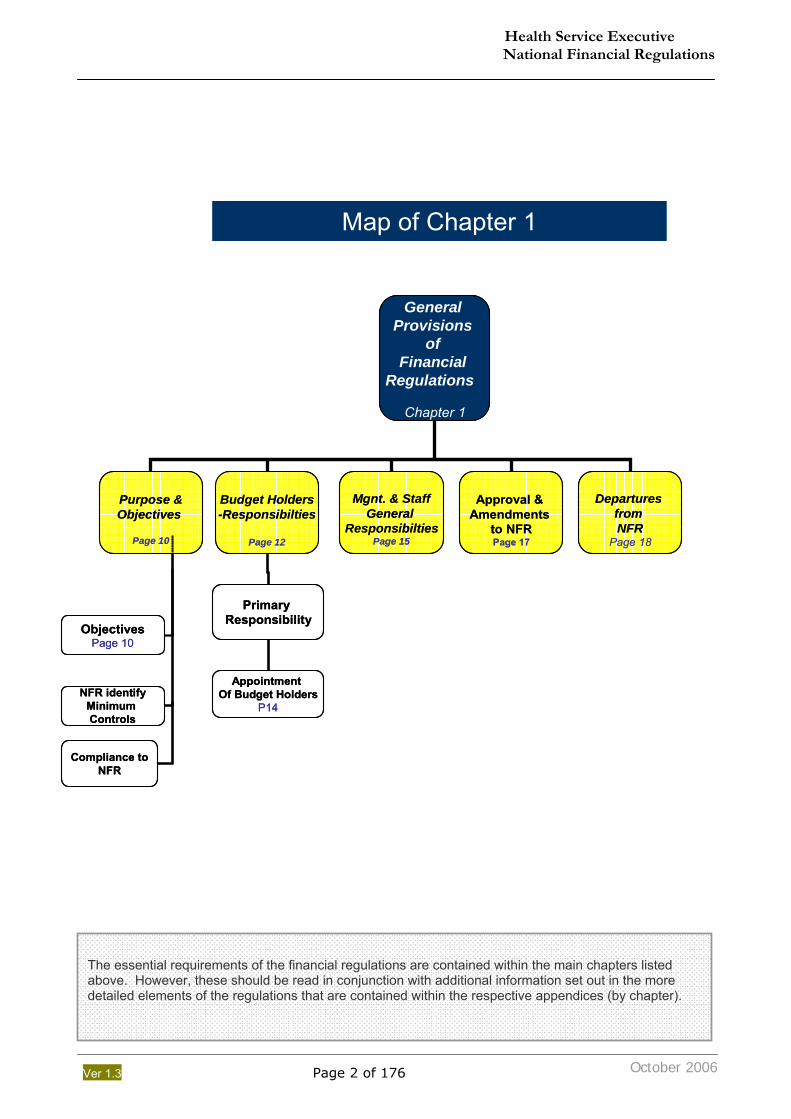
The essential requirements of the financial regulations are contained within the main chapters listed above. However, these should be read in conjunction with additional information set out in the more detailed elements of the regulations that are contained within the respective appendices (by chapter).
General Provisions
of Financial
Regulations
Chapter 1
Purpose &Objectives
Page 10
Budget Holders-Responsibilties
Page 12
Mgnt. & StaffGeneral
ResponsibiltiesPage 15
Approval & Amendments
to NFRPage 17
Departures from NFR
Page 18
Compliance toNFR
ObjectivesPage 10
NFR identifyMinimum Controls
Primary Responsibility
Appointment Of Budget Holders
P14
Map of Chapter 1
General Provisions
of Financial
Regulations
Chapter 1
Purpose &Objectives
Page 10
Budget Holders-Responsibilties
Page 12
Mgnt. & StaffGeneral
ResponsibiltiesPage 15
Approval & Amendments
to NFRPage 17
Departures from NFR
Page 18
Compliance toNFR
ObjectivesPage 10
NFR identifyMinimum Controls
Primary Responsibility
Appointment Of Budget Holders
P14
Map of Chapter 1
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 3 of 176
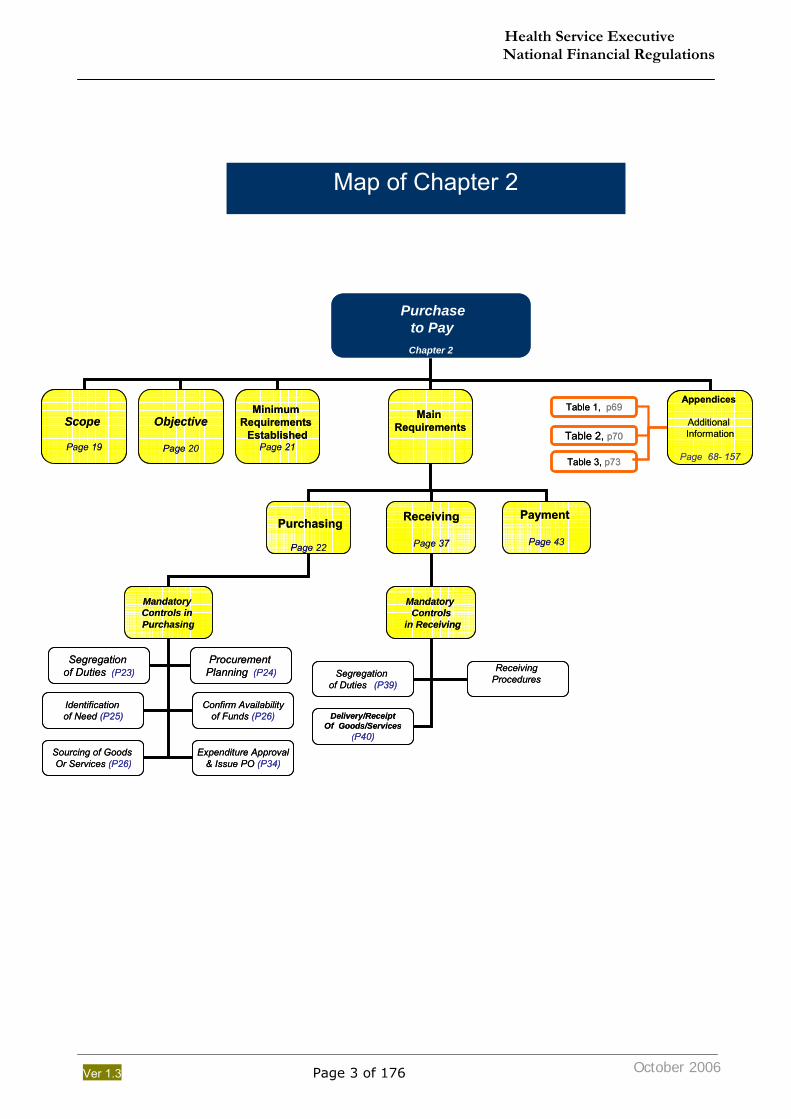
Map of Chapter 2
Purchase to PayChapter 2
Scope
Page 19
Objective
Page 20
Minimum Requirements
EstablishedPage 21
Main Requirements
Appendices
Additional Information
Page 68- 157
Mandatory Controls in Purchasing
Mandatory Controls
in Receiving
Identification of Need (P25)
Confirm Availabilityof Funds (P26)
Sourcing of Goods Or Services (P26)
Expenditure Approval& Issue PO (P34)
Segregation of Duties (P23)
Procurement Planning (P24) Segregation
of Duties (P39)
Delivery/ReceiptOf Goods/Services
(P40)
Receiving Procedures
Purchasing
Page 22
Receiving
Page 37
Payment
Page 43
Table 1, p69
Table 2, p70
Table 3, p73
Purchase to PayChapter 2
Scope
Page 19
Objective
Page 20
Minimum Requirements
EstablishedPage 21
Main Requirements
Appendices
Additional Information
Page 68- 157
Mandatory Controls in Purchasing
Mandatory Controls
in Receiving
Identification of Need (P25)
Confirm Availabilityof Funds (P26)
Sourcing of Goods Or Services (P26)
Expenditure Approval& Issue PO (P34)
Segregation of Duties (P23)
Procurement Planning (P24) Segregation
of Duties (P39)
Delivery/ReceiptOf Goods/Services
(P40)
Receiving Procedures
Purchasing
Page 22
Receiving
Page 37
Payment
Page 43
Table 1, p69
Table 2, p70
Table 3, p73
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 4 of 176
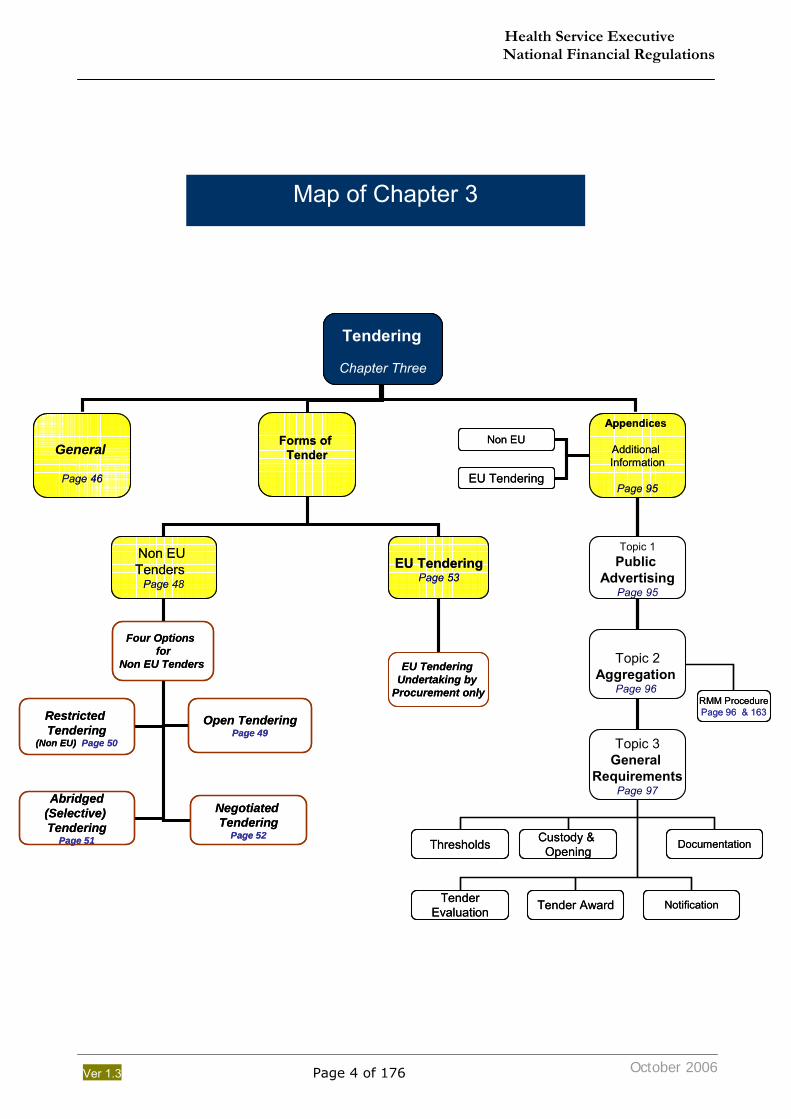
Map of Chapter 3
October 2006
Tendering
Chapter Three
General
Page 46
Forms of Tender
Appendices
Additional Information
Page 95
Four Options for
Non EU Tenders EU Tendering Undertaking by
Procurement only
Restricted Tendering
(Non EU) Page 50
Abridged(Selective) Tendering
Page 51
Negotiated Tendering
Page 52
Open TenderingPage 49
Non EU Tenders
Page 48
EU TenderingPage 53
Topic 3General
RequirementsPage 97
Topic 1Public
AdvertisingPage 95
Non EU
Topic 2Aggregation
Page 96
EU Tendering
Thresholds Custody & Opening
TenderEvaluation Tender Award Notification
Documentation
RMM ProcedurePage 96 & 163
Tendering
Chapter Three
General
Page 46
Forms of Tender
Appendices
Additional Information
Page 95
Four Options for
Non EU Tenders EU Tendering Undertaking by
Procurement only
Restricted Tendering
(Non EU) Page 50
Abridged(Selective) Tendering
Page 51
Negotiated Tendering
Page 52
Open TenderingPage 49
Non EU Tenders
Page 48
EU TenderingPage 53
Topic 3General
RequirementsPage 97
Topic 1Public
AdvertisingPage 95
Non EU
Topic 2Aggregation
Page 96
EU Tendering
Thresholds Custody & Opening
TenderEvaluation Tender Award Notification
Documentation
RMM ProcedurePage 96 & 163
Health Service Executive National Financial Regulations
Ver 1.3 Page 5 of 176
October 2006
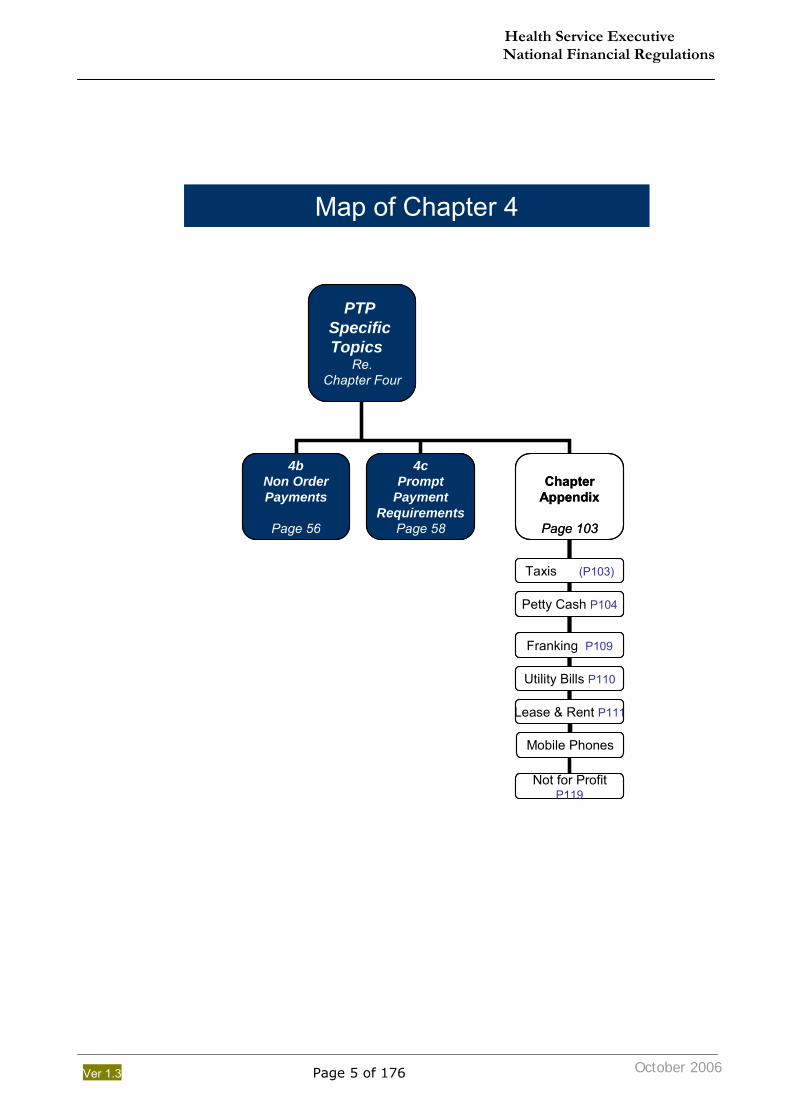
PTP Specific Topics
Re.Chapter Four
4bNon OrderPayments
Page 56
4cPrompt
PaymentRequirements
Page 58
ChapterAppendix
Page 103
Map of Chapter 4
Taxis (P103)
Petty Cash P104
Franking P109
Lease & Rent P111
Utility Bills P110
Mobile Phones
Not for ProfitP119
PTP Specific Topics
Re.Chapter Four
4bNon OrderPayments
Page 56
4cPrompt
PaymentRequirements
Page 58
ChapterAppendix
Page 103
Map of Chapter 4
Taxis (P103)
Petty Cash P104
Franking P109
Lease & Rent P111
Utility Bills P110
Mobile Phones
Not for ProfitP119
Health Service Executive National Financial Regulations
Ver 1.3 Page 6 of 176
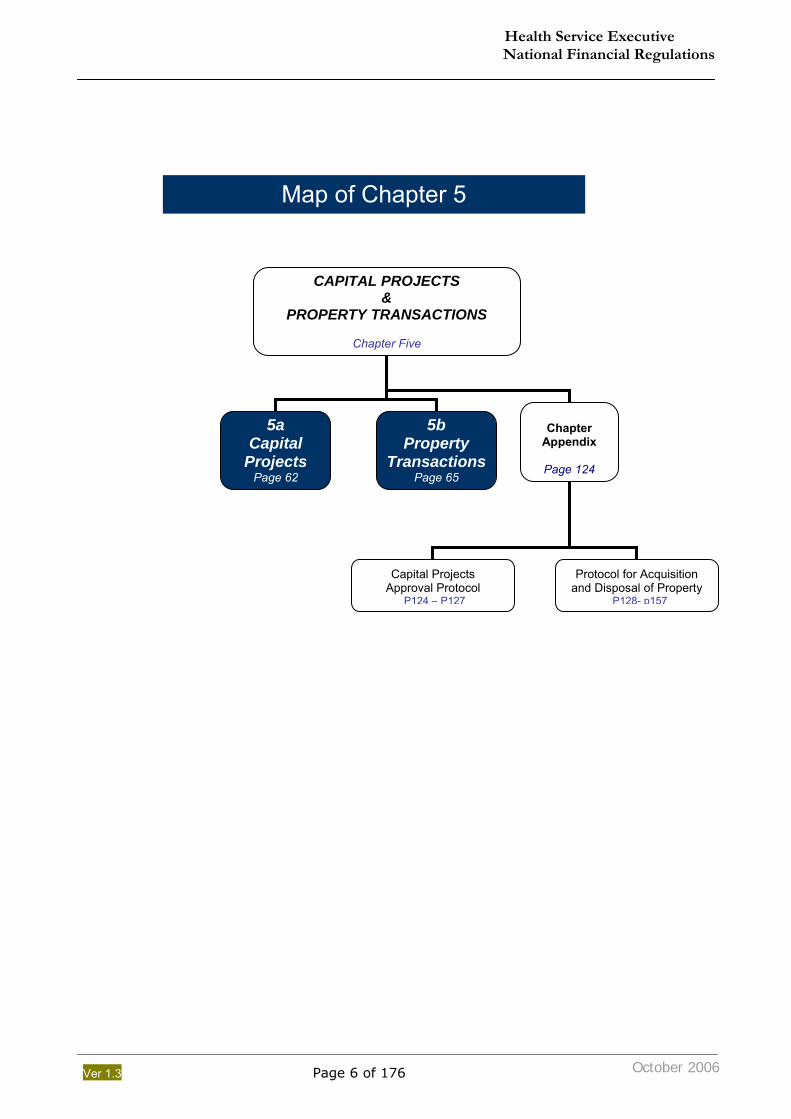
CAPITAL PROJECTS &
PROPERTY TRANSACTIONS
Chapter Five
5a Capital
Projects Page 62
5b Property
TransactionsPage 65
Chapter
Appendix
Page 124
Map of Chapter 5
Capital Projects Approval Protocol
P124 – P127
Protocol for Acquisition and Disposal of Property
P128- p157
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 7 of 176
October 2006
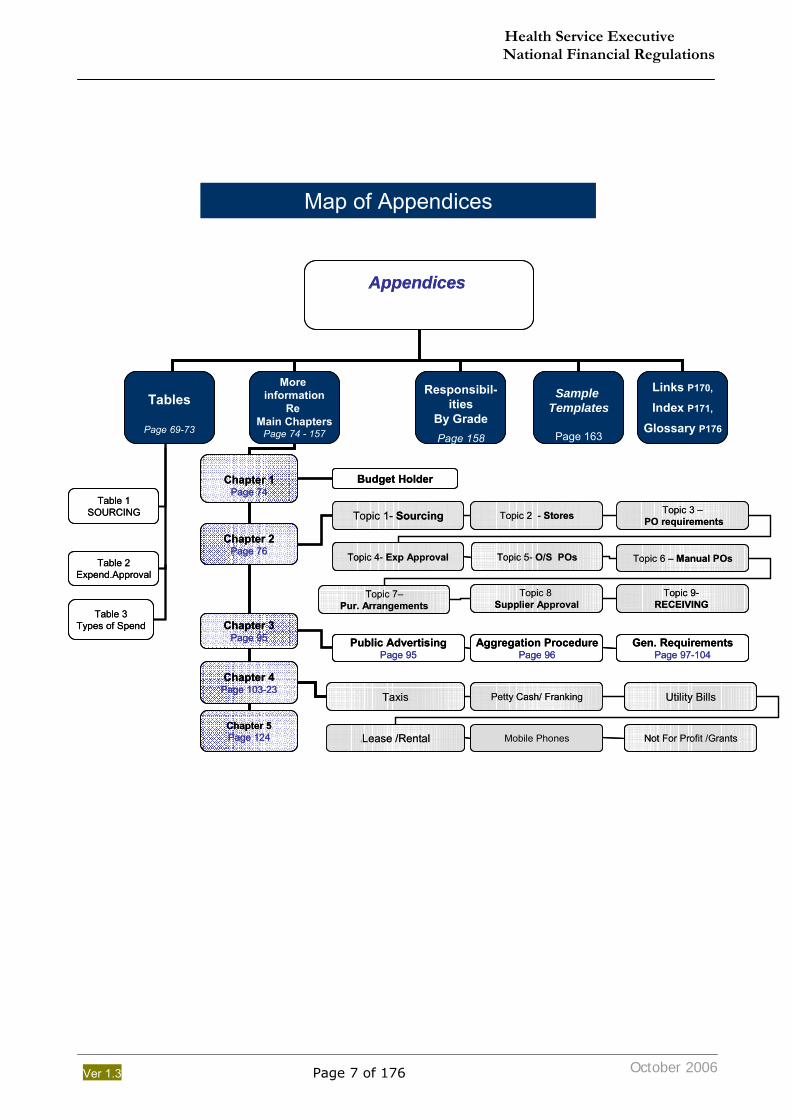
Appendices
Tables
Page 69-73
More information
Re Main Chapters
Page 74 - 157
Responsibil-ities
By GradePage 158
Sample Templates
Page 163
Links P170,
Index P171,
Glossary P176
Table 3Types of Spend
Table 1SOURCING
Table 2Expend.Approval
Chapter 1Page 74
Map of Appendices
Chapter 2Page 76
Chapter 3Page 95
Chapter 4Page 103-23
Budget Holder
Topic 1- Sourcing
Topic 4- Exp Approval
Topic 2 - Stores
Topic 5- O/S POs
Topic 3 –PO requirements
Topic 7–Pur. Arrangements
Topic 6 – Manual POs
Topic 8 Supplier Approval
Topic 9-RECEIVING
Public AdvertisingPage 95
Aggregation ProcedurePage 96
Gen. RequirementsPage 97-104
Taxis Petty Cash/ Franking Utility Bills
LLease /Rental Mobile Phones Not For Profit /GrantsChapter 5Page 124
Appendices
Tables
Page 69-73
More information
Re Main Chapters
Page 74 - 157
Responsibil-ities
By GradePage 158
Sample Templates
Page 163
Links P170,
Index P171,
Glossary P176
Table 3Types of Spend
Table 1SOURCING
Table 2Expend.Approval
Chapter 1Page 74
Map of Appendices
Chapter 2Page 76
Chapter 3Page 95
Chapter 4Page 103-23
Budget Holder
Topic 1- Sourcing
Topic 4- Exp Approval
Topic 2 - Stores
Topic 5- O/S POs
Topic 3 –PO requirements
Topic 7–Pur. Arrangements
Topic 6 – Manual POs
Topic 8 Supplier Approval
Topic 9-RECEIVING
Public AdvertisingPage 95
Aggregation ProcedurePage 96
Gen. RequirementsPage 97-104
Taxis Petty Cash/ Franking Utility Bills
LLease /Rental Mobile Phones Not For Profit /GrantsChapter 5Page 124
Health Service Executive National Financial Regulations
Ver 1.3 Page 8 of 176
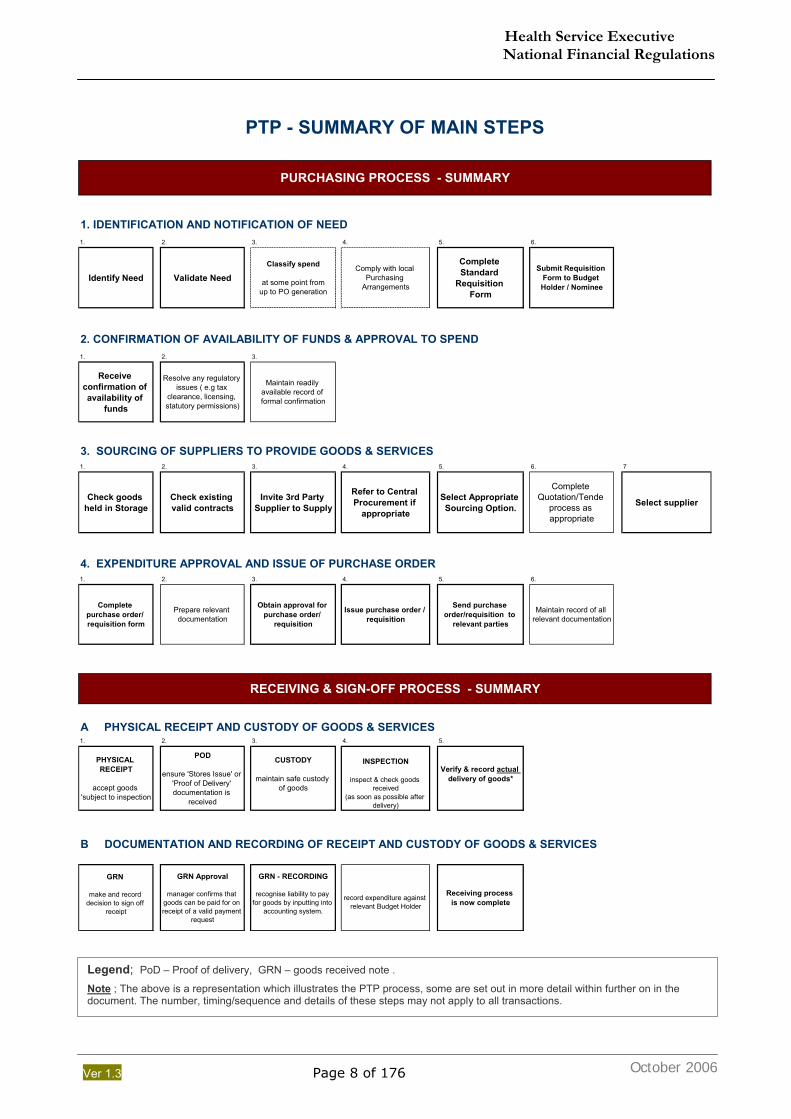
PTP - SUMMARY OF MAIN STEPS
1. 2. 3. 4. 5. 6.
Identify Need Validate NeedClassify spend
at some point fromup to PO generation
Comply with local Purchasing
Arrangements
Complete Standard
Requisition Form
Submit Requisition Form to Budget Holder / Nominee
1. 2. 3.
Receive confirmation of availability of
funds
Resolve any regulatory issues ( e.g tax
clearance, licensing, statutory permissions)
Maintain readily available record of formal confirmation
1. 2. 3. 4. 5. 6. 7
Check goods held in Storage
Check existing valid contracts
Invite 3rd Party Supplier to Supply
Refer to Central Procurement if
appropriate
Select Appropriate Sourcing Option.
Complete Quotation/Tende
process as appropriate
Select supplier
1. 2. 3. 4. 5. 6.
Complete purchase order/ requisition form
Prepare relevant documentation
Obtain approval for purchase order/
requisition
Issue purchase order / requisition
Send purchase order/requisition to
relevant parties
Maintain record of all relevant documentation
1. 2. 3. 4. 5.
PHYSICAL RECEIPT
accept goods 'subject to inspection
POD
ensure 'Stores Issue' or 'Proof of Delivery' documentation is
received
CUSTODY
maintain safe custody of goods
INSPECTION
inspect & check goods received
(as soon as possible after delivery)
Verify & record actual delivery of goods*
GRN
make and record decision to sign off
receipt
GRN Approval
manager confirms that goods can be paid for on receipt of a valid payment
request
GRN - RECORDING
recognise liability to pay for goods by inputting into
accounting system.
record expenditure against relevant Budget Holder
Receiving process is now complete
PURCHASING PROCESS - SUMMARY
3. SOURCING OF SUPPLIERS TO PROVIDE GOODS & SERVICES
2. CONFIRMATION OF AVAILABILITY OF FUNDS & APPROVAL TO SPEND
1. IDENTIFICATION AND NOTIFICATION OF NEED
A PHYSICAL RECEIPT AND CUSTODY OF GOODS & SERVICES
B DOCUMENTATION AND RECORDING OF RECEIPT AND CUSTODY OF GOODS & SERVICES
RECEIVING & SIGN-OFF PROCESS - SUMMARY
4. EXPENDITURE APPROVAL AND ISSUE OF PURCHASE ORDER
Legend; PoD – Proof of delivery, GRN – goods received note .
Note ; The above is a representation which illustrates the PTP process, some are set out in more detail within further on in the document. The number, timing/sequence and details of these steps may not apply to all transactions.
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 9 of 176
0. Introduction to Financial Regulations
0.1. The National Financial Regulations (NFR) contained within this document update and replaces all previous Financial Regulations unless otherwise specified.
0.2. The Financial Regulations form an integral part of the overall system of Financial Corporate
Governance and are intended as the framework underpinning the System of Internal Financial Control.
0.3. The Financial Regulations have been prepared to reflect current best practice generally, as
well as the guiding principles and best practice embedded within the processes under the scope of the Financial Information System Project (FISP).
0.4. Particular attention has been made to ensure that the Financial Regulations, are consistent
with statutory requirements and government guidelines.
0.5. In addition, existing former Health Board and other Financial Regulations already in existence throughout the country and elsewhere have been reviewed, and the best elements have been incorporated as part of the development of these regulations.
0.6. A range of primary reference materials have been used including:
NPPPU Government Procurement Guidelines (2004) Health Service Procurement Policy (updated Jan 2006) Department of Finance Code of Practice for the Governance of State Bodies Prompt payment legislation (1997 Act & SI388 dated 2002) EU tendering legislation FISP design documentation
0.7. The regulations outline responsibilities for all levels of management and staff.
0.8. The importance of managers and staff recognising their personal responsibilities in relation
to the understanding of and compliance with the Financial Regulations is stressed.
0.9. The Financial Regulations and compliance with them will require continuous monitoring by management at all levels to ensure that the level of assurance provided, regarding the effectiveness of our system of internal financial controls, is maximised.
0.10. The initial task for managers in implementing these new Financial Regulations is to identify
any areas where there may be compliance gaps and put in place planned actions to address these gaps.
Nominees of National Management Team Members 0.11. Where these financial regulations reference members of the National Management Team,
such references can be taken to include their formally delegated nominees, unless otherwise expressly provided.
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 10 of 176
1. General Provisions regarding Financial Regulations
Go to next chapter; on page 19 Go to Appendix ; on page 68
1.a Purpose and Objectives of Financial Regulations Ref; Page 10 1.b Appointment & Responsibilities of Budget Holders Ref; Page 12 1.c General Responsibilities of Management and Staff Ref; Page 15 1.d Approval and Amendment to the Financial Regulations Ref; Page 17 1.e Departures from the Financial Regulations ; Ref; Page 18 Approval, Recording, Annual Review and Reapproval The key requirements of the financial regulations are contained within the main chapters. However, this should be read in conjunction with the ‘additional information’ which sets out in the more detailed elements of the regulations that are contained within the respective appendices (by chapter). 1.a Purpose and Objectives of Financial Regulations
1.1. Introduction 1.1.1. The Financial Regulations are intended to outline the high level framework within
which the internal financial control system of the Health Service Executive (HSE) will operate.
1.1.2. These regulations are not intended as a detailed procedural guide for financial
processes or activity within the HSE as the organisation is too diverse to allow that to be achieved in a practical and accessible document.
1.1.3. This document may be of assistance in providing training to managers and staff as to
what their obligations are around compliance with the Financial Regulations, however, it has not been produced as a training document, again for reasons of practicality.
1.1.4. These regulations have been prepared with the intention of ensuring that the financial
controls in operation within the HSE are consistent with: Irish and EU statutory requirements Achievement of Best Value for Money Department of Health and Children and Government policies and guidelines Presently available best practice appropriately interpreted for the Irish Public
Health Service context.
1.2. Compliance with Financial Regulations
1.2.1. No set of Financial Regulations will be effective unless they are specific, understood and monitored for compliance.
1.2.2. It is the responsibility of all Budget Holders, managers and staff to ensure that
the day-to-day operations and procedures of the organisation comply with the Financial Regulations.
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 11 of 176
1.2.3. Budget Holders must ensure that a record is maintained of the training undertaken by
each employee with regard to Financial Regulations. Certification of users of the Financial Regulations where applicable, together with other relevant training records (e.g. Financial Information System/Accounting training) should be maintained as a record of user knowledge, available skill sets, training history etc.
1.2.4. All Budget Holders and other managers and staff have a direct responsibility to be pro-
active in ensuring that they are aware of, understand and comply with these Financial Regulations.
1.2.5. Persistent and negligent failure to comply with the Financial Regulations is a very
serious matter for any HSE employee and may lead to disciplinary proceedings.
1.3. Objectives 1.3.1. The Financial Regulations and the system of internal financial controls that they
underpin are intended to:
i. Support the achievement of the corporate objectives of the HSE
ii. Ensure the HSE operates within the limits of its notified Budget
iii. Facilitate open and transparent accountability for the financial resources
entrusted to the HSE
iv. Support the efficient and effective use of resources assigned to HSE
v. Ensure the safeguarding of the assets of the HSE
vi. Reduce the likelihood of fraud, theft or error in relation to financial matters
and increase the likelihood of its detection
1.4. Context
1.4.1. These Financial Regulations and compliance with them must be viewed in the context of the role of the HSE which is to improve the health and social well being of the population it serves.
1.4.2. Proper financial controls will assist the Health Service Executive in meeting this
primary objective.
1.5. Financial Regulations identify Minimum Controls 1.5.1. These Financial Regulations set out what are, in effect, minimum standards of
financial controls that are acceptable across this very large and diverse organisation.
1.5.2. It is the responsibility of every Budget Holder and his/her staff to put in place and document the detailed arrangements applicable to their own areas of responsibility.
1.5.3. Budget Holders may decide to apply a higher level of control than the minimum set out in the regulations in order to achieve the objectives of the Financial Regulations. For example, expenditure control could be amended for local use so that the value that each grade has approval authority for could be lower than that allowed by these regulations.
Health Service Executive National Financial Regulations
Ver 1.3 Page 12 of 176
Related Appendix ; on page 74
1.b Responsibilities and Appointment of Budget Holders
Budget Holders & Budget Holding More Information regarding Budget Holders responsibilities, see appendix on page 74.
1.6. Minimum Controls required by these Financial Regulations
These regulations require: 1) That there is clarity as to which managers are budget holders and this is known both to
the budget holders and generally, as required.
2) That each budget holder is clear as to what his or her key responsibilities are, and are complying with same to the greatest extent possible.
3) That formal assignment of budget amounts to budget holders must be notified
N1 by the Finance Directorate on foot of decisions of the Chief Executive, each National Directors and their relevant staff.
1.7. These regulations do not require:
1) The delegation of budget holding responsibility N2 to any particular level or grade within the organisation or
2) Complete uniformity across the HSE as to the level at which, or the grades, by which
budgets are held and managed
1.8. Primary responsibilities of Budget Holders
These are:
1) To operate within the limits of the budgets notified to them subject to the overall direction of the budget holder to whom they report
2) To monitor variances from budget limits on an ongoing basis and initiate corrective
measures in order to bring financial performance in on target, at the latest, by the end of each financial year
3) To co-operate fully with the requirements of the budget holder to whom they report so
that higher level budget holder can meet their primary responsibility as outlined above.
4) To comply with the additional responsibilities placed upon them in relation to the general system of internal financial controls as dictated by these financial regulations (see par1.9 below)
1 Notification via the Finance Directorate is a basic control requirement to ensure there is overall corporate clarity in terms of the total financial resource being managed. Responsibility and Authority for budgets, once notified, rest with each of the HSE National Directors, and their staff. 2 It is expected that, over time, HSE will move towards appropriate national standardisation in relation to a range of matters including budget holding and budget management.
Health Service Executive National Financial Regulations
Ver 1.3 Page 13 of 176
Related Appendix; on page 74 Note:
At its most basic and simplified level, the key objective of budget management is to ensure that the HSE meets its statutory requirement not to spend more money, in total, than it has been given by the Oireachtas. In order to meet this objective the HSE needs to assign budgets to individuals so that they can be managed effectively. In essence the Chief Executive assigns budgets to the National Directors who in turn assign them to Assistant National Directors / Hospital Network Managers etc and so on down to whatever level is considered appropriate and feasible by each manager in the chain.
Accountability is exercised in a top down manner. Each budget holder remains fully responsible and accountable for the budget assigned to them regardless of however many levels of staff below them they may have assigned as budget holders. If a budget holder at a particular level achieves breakeven by year end, it is entirely possible that the budget holders they are managing below them may have achieved a variety of results with some over budget and some under budget. This is a matter in the first instance between the higher level budget holder and those managing budgets below him or her. While it would clearly be preferable for all budget holders at all levels to be assigned budgets that they can realistically manage this, for a variety of reasons this may not always be possible. The key requirement is for the higher level manager and those below them to work effectively together so that overall breakeven is achieved. A local budget holder who overspends their budget is unlikely to be considered to be in breach of these financial regulations provided they, at all times;
Act responsibly and pro-actively in managing their budget Keep their manager fully informed of any emerging and continuing material issues affecting
their capacity to achieve financial breakeven Identify any practical options to address these material issues Take corrective action as early as possible Comply fully with any requests or directions of their manager
1.9. Additional responsibilities of Budget Holders in relation to
1.9.1. Financial Controls generally and
1.9.2. The wider aspects of the Financial Regulations
Budget Holders are seen as key managers of resources and as such it is generally appropriate for them to play a role in relation to aspects of financial control that extend beyond the primary requirement for managing budgets within set limits.
These additional responsibilities are set out in more detail in Appendix “Budget Holders – Additional Information” on page 74 and include requirement to ;
1.9.3. To ensure compliance with these Financial Regulations. (A1.2 below).
1.9.4. To put in place Specific Arrangements. (A1.3 below)
1.9.5. To mitigate control deficits with regard to compliance with
the Financial Regulations. (A1.4 below)
1.9.6. To make efficient use of resources. (A1.5 below)
Health Service Executive National Financial Regulations
Ver 1.3 Page 14 of 176
1.10. Appointment of Budget Holders Related Appendix; page 74
1.10.1. All budget holders must be approved and each must be notified of their assignment as budget holders
1.10.2. Only a budget holder can approve the assignment of another person as a budget
holder
1.10.3. Such assignment can only be in relation to an element of the budget held by the budget holder approving the assignment.
1.10.4. Such assignment can only be to a staff member of the budget holder making the
assignment.
1.10.5. The following are deemed, by virtue of the approval of these regulations, to be budget holders in respect of their own areas of responsibility unless otherwise directed by the CEO or their National Director:
National Directors
Assistant National Directors
Hospital Network Managers
Local Health Managers
NHO Hospital Managers
1.10.6. The approval of the assignment of any budget holders below the levels at 1.10.5
above will only take effect once notified to the relevant Assistant National Director of Finance or their nominee(s)
Health Service Executive National Financial Regulations
Ver 1.3 Page 15 of 176
1.c General Responsibilities of Management and Staff
1.11. Managers / Supervisors – General Responsibility
Not withstanding the primary role of the Budget Holder, every manager and supervisor has responsibility in regard to complying with, and assisting with documenting and periodically updating formal arrangements in respect of all the financial processes delegated to him/her including:
a) Responsibility to ensure regulations are complied with by him/her and by any managers and staff that may be involved in the financial processes.
b) Responsibility to ensure awareness, understanding, knowledge, experience, training and
development of any managers and staff he may involve in the processes.
c) Responsibility to minimise staff resource utilised in the financial processes consistent with achieving value for money and complying with the Financial Regulations.
d) Responsibility to mitigate any compliance or capacity deficits regarding any of the managers and staff she/he may involve in the process and notify same to the Budget Holder
1.12. Staff – General Responsibility
1.12.1. Each member of staff has similar responsibilities to the manager / supervisor in respect of themselves with regard to:
Compliance with the regulations. Being personally proactive about his/her own awareness, understanding,
knowledge, training and development in order to ensure this compliance.
1.13. Responsibilities not reduced due to reliance on Health Service Executive Shared Services (HSE-SS)/ Estates / Procurement.
1.13.1. The fact that Budget Holders and their managers may rely upon the Shared Services Organisation or any other party outside their direct control to support them in terms of financial or purchasing activities does not diminish their personal responsibility to ensure compliance with these regulations.
1.13.2. It is a matter for each Budget Holder to effectively manage their relationships with
HSE-SS or any external provider to provide them with the assurances they need around compliance with these regulations.
1.13.3. In practical terms Budget Holders will exercise this responsibility by ensuring that they
fully engage in a proactive manner with the HSE SS in the ongoing monitoring and review of the services provided on their behalf.
Health Service Executive National Financial Regulations
Ver 1.3 Page 16 of 176
1.14. Audit – A Key element of the System of Financial Corporate Governance.
1.14.1. As stated above the Financial Regulations are intended to provide a framework
underpinning the system of Internal Financial Control.
1.14.2. The Financial Regulations will only be effective if they remain robust in nature and if there is a high level of ongoing compliance with their provisions. The responsibilities of Budget Holders, Management and Staff in this regard have been set out on page 12 and 15 and Appendix on page 68 .
1.14.3. Ongoing independent review and compliance monitoring by both internal audit and
external audit (Comptroller and Auditor General) is a key element of the overall assurance required by the Chief Executive Officer and the Board of HSE in respect of the effectiveness of the System of Internal Financial Control.
1.14.4. Further assurance is provided by the existence of a pro-active and empowered Audit
Committee under the guidance of the main board.
1.15. Audit Trail
Throughout these financial regulations there are direct and indirect references that establish the minimum controls that should operate, including supporting documentation, evidence of supply etc. There is an overall requirement irrespective of the level of automation or complexity of the process that sufficient Audit Trail G1 is maintained.
Within the document you will notice that there are; N1 etc - This refers to notes that will appear at the end of the respective page G1 etc. – This refers to Glossary items which provide an explanation of a term used. These will appear at the end of this document but can be accessed by clicking on the item.
Health Service Executive National Financial Regulations
Ver 1.3 Page 17 of 176
1.d Approval of and Amendment to The Financial Regulations
1.16. These regulations take effect when approved by the HSE Chief Executive Officer and the
HSE Board.
1.17. Proposed amendments to the regulations must be recommended by the National Director of Finance and approved by the HSE Chief Executive Officer and the HSE Board.
1.18. Initial approval and any subsequent amendment to the Financial Regulations must be recorded on a formal written decision.
1.19. Clarifications required in respect of these regulations should be addressed to the relevant
Assistant National Director of Finance in the first instance.
Health Service Executive National Financial Regulations
Ver 1.3 Page 18 of 176
1.e Departures from regulations; Approval, Recording, Annual Review and Reapproval
1.20. Unless otherwise provided for in these Financial Regulations, any departures from the regulations must be:
Approved by the relevant National Management Team Member (or Assistant
National Director delegated by the NMTM) and
Co-signed by the relevant Assistant National Director of Finance.
Explained and recorded by way of formal written decision.
Reviewed formally by the relevant MTM or Assistant National Director delegated at
the end of the financial year.
Approved by the relevant MTM and the National Director of Finance where there are
repeated departures from regulations that span more than one financial year.
1.21. The requirement is that a departure from the Financial Regulations must normally represent an interim measure pending the resolution of the issue giving rise to the need for the departure.
1.22. Actions necessary to address issues giving rise to departures from the Financial
Regulations should be identified and implemented as soon as is practicable.
1.23. The relevant National Management Team Member (or Assistant National Director delegated) must identify any additional measures, for example additional supervision or random checking, necessary to mitigate any control risks associated with a departure from the Financial Regulations.
1.24. Such mitigation measures must be complied with fully by the relevant managers and staff.
1.25. The formal written decision approving or renewing a departure from the Financial
Regulations must record:
Description and explanation of the issues giving rise to the need for an approved departure from the Financial Regulations.
Service Area / Location and Budget Holder (s) covered by the departure
Expected duration of the departure and actions proposed to remove the need for the
departure over the short or medium term.
Any expected control risk associated with the departure from the Regulations and the measures being proposed by the National Management Team Member to mitigate that risk.
Health Service Executive National Financial Regulations
Ver 1.3 Page 19 of 176
Go to next chapter; on page 46 Go to last chapter; on page 10
2. Purchase to Pay (General)
The key requirements of the financial regulations are contained within the main chapters. However, this should be read in conjunction with additional information set out in the more detailed elements of the regulations, contained within the respective appendices (by chapter).
2a. Scope 2b. Objective of the Financial Regulations in respect of the ‘Purchase to Pay’ Process. on page 20 2c. Purchase to Pay regulations are Minimum Requirements on page 21 2d. Purchasing Process – Main Requirements on page 22 2e Receiving Process – Main Requirements on page 37 2f Payment Process – Main Requirements on page 43 APPENDIX - More Information re. Chapter 2 Topics on page 76 to 95
2a. Scope
The regulations within this section are intended to set out the Primary Financial Control requirements for all non-pay expenditure (i.e. expenditure not processed through the payroll system).
Summary of Purchase to Pay (PTP) – basic steps / stages
2.1. Section 1.11 above ‘Responsibilities of Management and Staff’ sets out in detail the personal responsibility of Budget Holders, managers and staff in relation to these regulations.
Please ensure that you are familiar with this section before reading this regulation.
Obtaining expenditure approval,
Sourcing of appropriate goods / services from 3rd parties or Stores to meet identified service needs.
Formally requesting the selected 3rd party to provide specified goods or services by issue of PO or contract.
1. PURCHASING
Receipt and checking / inspection of goods and services.
Confirmation that they are fit for purpose, and match what was ordered or contracted for.
Approval that Goods/Service can be paid for upon receipt of an appropriate request for payment
2. RECEIVING ( receipt of goods or services)
● for goods and services – generally on foot of invoices or other payment requests. ● A Key control within this process is the checking and verification of the invoiced price of good or services to the purchase order price.
3. PAYMENT
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 20 of 176
Go to Start of Chapter ;on page 19
2b. Objective of the Financial Regulations in respect of the ‘Purchase to Pay’ process. The objectives set out below are in addition to those relevant to the entirety of the regulations which are listed in section 1.a Purpose and Objectives of Financial Regulations on page 10.
2.2. The objectives of the Financial Regulations in respect of the Purchase to Pay Process are to ensure the HSE, its Budget Holders, Managers and Staff;
Comply with Government and EU Procurement requirements and ensure that the
procurement process is open and competitive. Properly assess the HSE procurement requirements on a periodic basis to enable
proper procurement planning. Demonstrate full accountability and probity as well as the highest ethical standards in
respect of the public funds expended in the purchasing process. Acquire goods and services that are most appropriate and represent best value for
money for the health service in terms of full life-cycle costs.
Make best use of the purchasing power of the HSE by entering into contracts including national contracts, wherever appropriate. Aggregate G2 demand to optimise purchasing power (ref to Page 47)
Obtain formal approval from the appropriate Budget Holder or their nominee before requesting the provision of any goods, services or works.
Do not engage in purchasing above the limits of the budget available.
Operate the 'Purchase To Pay' process in an efficient and effective manner that
facilitates the timely production of accurate and comprehensive Annual Financial Statements (AFS).
Properly manage their contacts with suppliers and provide full clarity to suppliers as
regards what is expected of them in relation to all aspects of the process. Consistently apply high standards with respect to evidencing and recording of
‘Receiving’ of Goods/Services and custody of goods.
Health Service Executive National Financial Regulations
Ver 1.3 Page 21 of 176
Go to start of Chapter; on page 19
2c. Purchase to Pay regulations establish PTP Minimum Requirements
2.3. These regulations set out what are minimum requirements around many aspects of the purchase to pay process including:
1. Number of quotes / tenders required. (details on page 69) 2. Value thresholds for different sourcing options. (details on page 69) 3. Approval levels. (details on page 70) 4. Time periods for receipt of quotes / tenders.
2.4. The requirements set out in this chapter relate to Non Pay expenditure. In addition, there are other requirements that arise due to the specific nature of expenditure and which are governed by separate protocol. These include;
2.4.1. Capital Projects – Project Approval is governed by Capital Projects Approval
Protocol.
2.4.2. Property Transactions - is governed by the Property Transaction Protocol - ‘Protocol for the Acquisition and disposal of Property’.
2.4.3. Funding of Voluntary Organisations (Not for Profit/Grants).
2.5. It is a requirement that managers operating these regulations will apply higher than the
minimum control level (e.g. next level up authorisation) if this is necessary to ensure the objectives set out above at 2.B. are consistently achieved.
Example: A manager may decide that in the case of purchase of routine medical consumables for one of his/ her hospitals he/she needs to get a Grade Vl to approve any purchase between €5,000 and €10,000 (see Table 2 - normally a Grade V can approve expenditure up to €10,000 for routine expenditure) because of any one or a combination of the following: He needs a tighter level of financial control for the remainder of the financial year in order to clear an overspend earlier in the year He does not have a sufficiently experienced Grade V
He decides that the complexity of the equipment or its purchasing process warrants it.
2.6. The actual steps, the number of steps and the sequencing of steps in the process that is being referred to as “Purchase to Pay” will vary depending on a number of factors including:
Type and complexity of goods or service being acquired. For more complex services, works and equipping, third party sign-off shall be required at each stage of the Purchase to Pay process.
Frequency of purchase of specific goods / services
Value
The source of the goods or services
Specific service unit or area acquiring the goods / services etc
The level of computerisation within the process
but the fundamental process and the required financial controls are common.
Health Service Executive National Financial Regulations
Ver 1.3 Page 22 of 176
Go to Start of Chapter ;on page 19 Receiving Process – Main Requirements on page 37 Payment Process – Main Requirements on page 43
2d. PURCHASING/PROCUREMENT; MAIN REQUIREMENTS
2.7. Definition For the purpose of these regulations purchasing includes all activities up to the point where:
A supplier(s) has been selected The supplier(s) has been formally requested to provide goods /services.
2.8. FOUR KEY ELEMENTS for each Purchasing Transaction It is clear that each and every purchasing transaction will have the following elements:
1 Identification and notification of need. Page 25 2 Confirmation of availability of funds and approval to spend. Page 26 3 Sourcing of supplier(s) to provide goods or services. Page 28 4 Formal request issued to supplier to provide goods/services. Page 34
2.9. General Application of Purchasing Regulations
These regulations cover the entire HSE which is a large and very diverse organisation. It is not practical to cover all potential situations or differences that may exist regarding:
2.9.1. Exactly by whom or in what manner a need for goods or services is identified and communicated.
2.9.2. At what precise stage or by whom the approval to spend available funds is decided.
2.9.3. Exactly how the supplier of goods or services is to be sourced in each specific case. Use of HSE standard procedures should be availed of where appropriate.
2.9.4. The precise manner and by whom the formal request to the supplier to provide the goods or services is made.
2.9.5. Budget Holders must ensure that there are documented Purchasing Arrangements in place for Managers and Users for each respective location /main category of spend. (More Information on page 87 )
2.10. Application of Purchasing Regulations to Bodies funded by the HSE
2.10.1. Where works and related service contracts are being awarded by external
organisations and are funded more than 50% the requirements of these regulations as regards sourcing of suppliers are applicable.
2.10.2. Budget Holders must ensure that relevant voluntary, not for profit or other such
organisations are aware of this requirement and it should be included as part of any service agreement or other contract with such organisations.
2.10.3. Refer to Funding Provided to ‘Not for Profit’ organisations, on page 119.
PURCHASE PROCESS
Health Service Executive National Financial Regulations
Ver 1.3 Page 23 of 176
MANDATORY CONTROLS WITHIN PURCHASING.
These regulations prescribe the following mandatory controls within the Purchasing process:
I. Segregation of Duties within Purchasing Ref # below
II. Procurement Planning Ref on page 24 III. Identification and notification of need Ref on page 25 IV. Confirmation of Availability of Funds and Approval to Spend Ref on page 26 V. Sourcing of Suppliers to Provide Goods and Services Ref on page 28 VI. End of Purchasing Stage; Approval & Issue of Purchase Order Ref pages 34 to 37
( I ) Segregation of Duties within Purchasing Next; ‘Identification of Need’ on page 24
2.11. Appropriate segregation of duties is a key element of any financial control framework. In the context of the purchasing process the following requirements are mandatory;
2.11.1. At some point between initial identification of need and the issue of a purchase order
or contract at least one other staff member in addition to the final decision maker must be involved in the process.
This must be evidenced by signatures appearing on purchasing documents e.g. requisition, purchase orders.
2.11.2. No manager (or staff) should have the final decision regarding the issue of a
purchase order or contract for any goods or service that is for their own day to day use.
2.11.3. There must be a clear separation of tasks between the person raising a Purchase
Order and Recording the ‘Receipt’ of the respective goods/Service.
2.11.4. There is a mandatory requirement to obtain appropriate professional procurement input where the value of purchases exceeds €25,000.
2.11.5. Decisions to authorise expenditure (i.e. to issue purchase order or contract) above
€50,000 must be formally written and recorded.
These decisions must be recommended by a manager at least at Grade V who must not be the same person that has 'signed off' the initial decision.
2.11.6. A minimum of 2 staff, one of whom must be Grade VIII or above must be involved in
both the opening and evaluation of all tenders.
2.11.7. Managers responsible for evaluating tenders (i.e. above €50,000) must not have the final decision as regards selection of the successful tenderer and / or approval to issue the purchase order or contract.
Health Service Executive National Financial Regulations
Ver 1.3 Page 24 of 176
2.11.8. Procurement must be notified of and co-ordinate all tenders above the EU threshold
except those tenders relating to Capital Projects which are the responsibility of the Estates Office.
2.11.9. Procurement is responsible for the ‘Commercial Evaluation’ of all EU Tenders
(other than ‘Works’ agreed specialist supplies). The person responsible for procurement shall co-ordinate procurement process and prepare tender analysis report for purchase approver/budget holder’s evaluation.
2.11.10. The Budget holder/Purchase approver makes the ‘decision’ to proceed /’sign-off’ a
tender based on tender report prepared by Commercial Evaluator.
2.11.11. Budget holders must maintain a list of ‘Commercial evaluators’ N3 for the Tender process
2.12. Segregation of duties (SOD) within purchasing should be read in conjunction with
Segregation of duties within receipt/receiving of Goods and Services on page 39.
( II ) Procurement Planning
Next; ‘Identification of Need’ on page 25
2.13. Budget Holders must, within twelve months of the coming into force of these regulations, ensure that they have reviewed and analysed their likely purchasing requirements over the following 3 years.
2.14. They must put in place a procurement plan, in conjunction with procurement/ Materials
Management/ Estates/ICT as appropriate to address:
2.14.1. Appropriate categorisation and rationalisation of suppliers.
2.14.2. Contracts to be renewed or terminated/allowed to lapse and their timeframes
2.14.3. Additional contracts to be put in place
2.14.4. Main service developments (new services, service expansions, service reductions) likely to impact on procurement over the following 12 months.
2.14.5. Any other relevant matters.
2.15. Procurement plans should be updated annually and replaced every three years.
Given the need for obtaining value for money and making best use of scarce staffing resources there is a requirement to co-ordinate and aggregate procurement plans.
N 3 Commercial Evaluators provide support through the procurement process by (a) Co-ordinating the procurement process (b) provide commercial tender analysis (c) ensure purchase systems and procedures are implemented, (d) procure supplies in line with current purchasing policies and procedures.
Health Service Executive National Financial Regulations
Ver 1.3 Page 25 of 176
2.15.1. Specific Assistant National Director(s) delegated by a National Management Team
Member must take the lead in the procurement planning process with appropriate professional procurement input.
2.15.2. It is a mandatory requirement that procurement plans identify any likely purchases
which will require the use of a tendering process or the EU Procurement Procedure, based on the value thresholds.
2.15.3. Account must be taken of the full likely HSE requirement for the goods or service in
deciding which value threshold and related sourcing option is appropriate.
( III ) Identification and Notification of Need Next; ‘Confirm Available Funds’ on page 26
2.16. Managers and staff who identify and communicate needs for goods and services must satisfy themselves and be in a position to demonstrate that the need:
2.16.1. Is genuine and is appropriate to their service.
2.16.2. Takes account of prevailing policies and constraints (including statutory compliance requirements) together with resource constraints under which their service is operating .
2.16.3. Person Approving expenditure must be aware of cost/value of items/service required and knowledge of budget.
2.16.4. Has been identified following a review of existing goods and services that may
already be available to the service
2.17. There is a requirement to obtain appropriate professional procurement input where the value of purchases exceeds €25,000 (see paragraph 2.11.4 above). i.e. for purchases in excess of €25,000 the procurement function should be contacted and guidance sought.
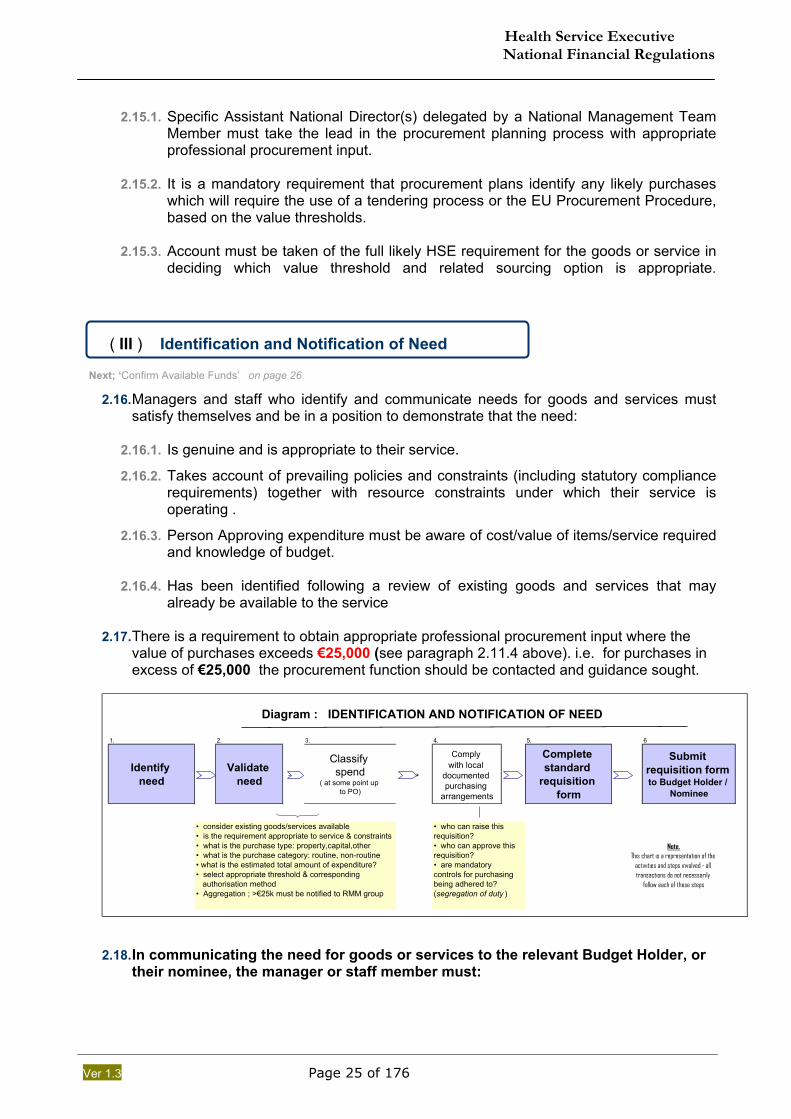
1. 2. 3. 4. 5. 6
Identify need → Validate
need →Classify spend
( at some point up to PO)
→
Comply with local
documented purchasing
arrangements
Complete standard
requisition form
Submit requisition form to Budget Holder /
Nominee
• who can raise this requisition?• who can approve this requisition?• are mandatory controls for purchasing being adhered to? (segregation of duty )
• consider existing goods/services available• is the requirement appropriate to service & constraints• what is the purchase type: property,capital,other• what is the purchase category: routine, non-routine• what is the estimated total amount of expenditure?• select appropriate threshold & corresponding authorisation method• Aggregation ; >€25k must be notified to RMM group
Note.This chart is a representation of the
activities and steps involved - all transactions do not necessarily
follow each of these steps
Diagram : IDENTIFICATION AND NOTIFICATION OF NEED
2.18. In communicating the need for goods or services to the relevant Budget Holder, or
their nominee, the manager or staff member must:
Health Service Executive National Financial Regulations
Ver 1.3 Page 26 of 176
2.18.1. Fully comply with the formal documented purchasing arrangements N4 put in place by or on behalf of the Budget Holder.
2.18.2. Fully comply with any requirement of their own manager 2.18.3. Clearly communicate, in written form, unless otherwise permitted, the following:
Date of Request Specification of goods / services required Name/source of request Purpose for which goods / services required Cost Centre / Internal Order Material Code / GL Preferred delivery address Timescales within which required Likely cost if known & quantity /duration etc
2.18.4. The normal requirement is for requests for the purchase of goods or services to be submitted on a standard pre-formatted sequentially numbered requisition form.
2.18.5. Such standardised requisition forms are particularly important where a purchasing
location receives a high volume of requests from a number of remote locations.
2.18.6. Requisitions must be submitted using the financial information system where required by the relevant Budget Holder.
2.19. Adequately record the request so that it is readily available for future reference or inspection / audit.
( IV ) Confirmation of Availability of Funds and Approval to Spend
Next; ‘Sourcing of Supplier’ on page 28.
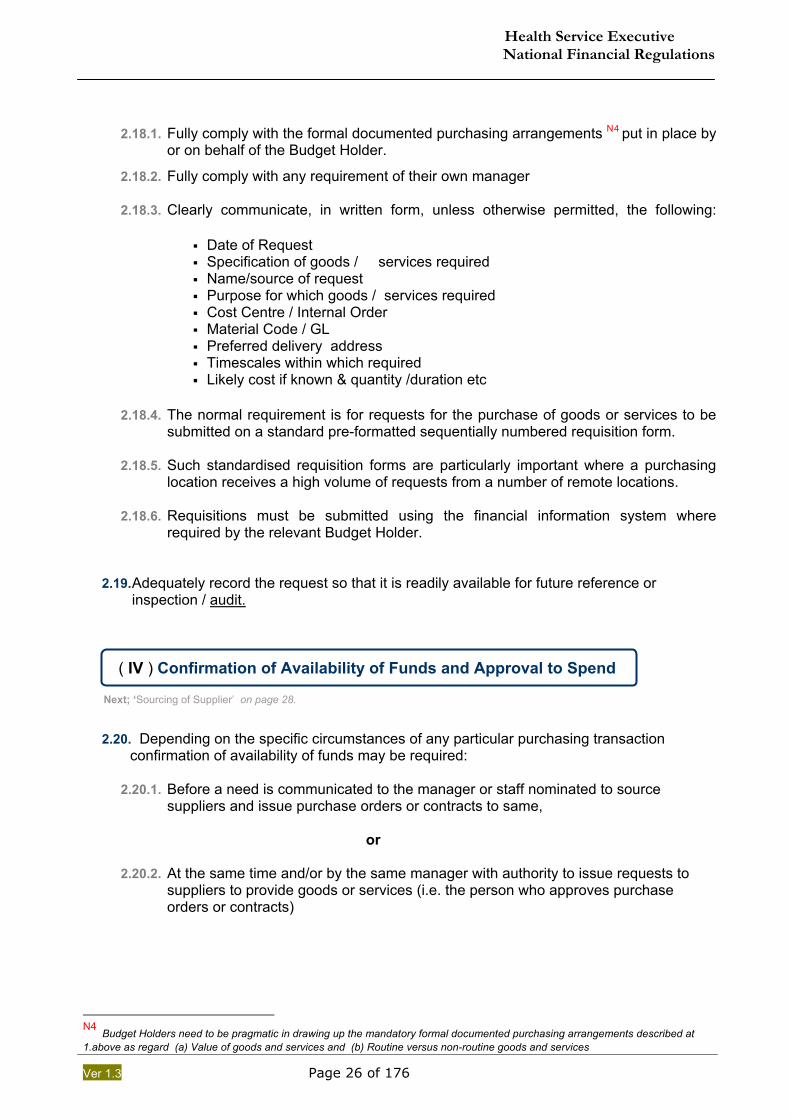
2.20. Depending on the specific circumstances of any particular purchasing transaction confirmation of availability of funds may be required:
2.20.1. Before a need is communicated to the manager or staff nominated to source
suppliers and issue purchase orders or contracts to same, or
2.20.2. At the same time and/or by the same manager with authority to issue requests to
suppliers to provide goods or services (i.e. the person who approves purchase orders or contracts)
N4 Budget Holders need to be pragmatic in drawing up the mandatory formal documented purchasing arrangements described at 1.above as regard (a) Value of goods and services and (b) Routine versus non-routine goods and services
Health Service Executive National Financial Regulations
Ver 1.3 Page 27 of 176
1. 2. 3.
Receive confirmation of
availability of funds
resolve any regulatory issues (
e.g licensing, statutory permissions)
maintain record of
formal confirmation
Diagram: CONFIRMATION OF AVAILABILITY OF FUNDS & APPROVAL TO SPEND
2.21. Expenditure approval thresholds
set out in Table 2; Purchase Order/Contract Approval – Financial Limits by Grade(page 70)
2.22. Mandatory Requirements
It is not intended to prescribe the detail of this element of the purchase process, however the following are mandatory requirements:
2.22.1. Budget Holders must document purchasing arrangements for their area to ensure there is clarity in respect of: 1. The point at which approval to spend is confirmed
2. By whom approval to spend is confirmed
2.22.2. Formal confirmation of available funding and approval to spend must be obtained prior to issuing a purchase order or contract to provide goods or services to a Third party supplier.
2.22.3. Regulatory issues must be resolved prior to the issuing of a purchase order or contract. Such issues may include the following which is not intended to be an exhaustive list:
1. Any licensing issues
2. Other statutory permissions or requirements
3. Tax Clearance Certificates /Tax status issues N5 (see links to forms see page 170)
2.22.4. A record of 2.22.2 above must be readily available whether by reference to the Financial Information System (FIS) G3 record, signature on copy purchase order or other means.
2.22.5. Exceptions to 2.22.2. above are only allowed where they can be clearly demonstrated as necessary to prevent material adverse impacts:
• To clients • To members of the public • To staff • To the service generally • To property or other assets of the Health Service Executive
2.23. All exceptions must be clearly recorded for future audit and must be rectified by obtaining
the necessary approval on the next available working day.
N5ATax Clearance Certificate(TCC) is a written confirmation from Revenue authorities that a person's tax affairs are in order at the date of issue of the certificate. Tax Clearance. Under Section 1095 of the Taxes Consol. Act,1997, it is mandatory that all vendors in receipt of €6,500 or more(inclusive of VAT), within any 12 months period, produce either a valid C2 certificate or a general Tax clearance certificate. Such contracts can involve the purchase, hiring, leasing of goods, services property. The requirement applies even where the provision of goods or services is not the subject of a formal written contract.Ref (http://www.revenue.ie/leaflets/taxclweb.doc)
Health Service Executive National Financial Regulations
Ver 1.3 Page 28 of 176
Additional Material; on page 76
( V ) Sourcing of Suppliers to Provide Goods or Services Next; ‘End of Purchasing Stage’ on page 34
2.24. Budget Holders responsibility in relation to Sourcing Budget holders and their nominees must;
2.24.1. Monitor their purchasing activity on an ongoing basis. They must identify opportunities for appropriate extension of centralised contracting. These opportunities should be pursued with Procurement.
2.24.2. Document their sourcing procedures as part of their formal local purchasing
arrangements and all such sourcing procedures must comply with the National Financial Regulations.
2.24.3. Have regard to the need to avoid ordering excess quantities of goods– it is important
to balance the requirement to ensure goods are available when needed against the issues associated with over ordering including:
1. Lack of appropriate storage
2. Excess goods may not last and have to be scrapped
2.25. These requirements should be addressed in the context of meeting the need for
procurement planning as set out on page 24 above. 1st required preference; Source from Stock or Existing Contract
2.26. It is a specific responsibility of each Budget Holder to ensure that:
to the greatest extent practicable and where consistent with achieving value for money
as many purchases of goods and services are from :
(i) “Stock (Stores)” - Goods held and issued from Stores/ storage location on page 78. (ii) Contracts - Acquired by ordering off a pre-existing and still valid contract, or
2.27. Requirement to Utilise Contracts that are in place and still valid.
2.27.1. “ It is incumbent ………… to establish whether an existing contract is already in
place and, if so, to utilise this contract” (Health Service Procurement Policy)
2.27.2. The terms of any given contract must make clear the extent to which the HSE commits to purchasing from the suppliers who have been awarded the contract.
Health Service Executive National Financial Regulations
Ver 1.3 Page 29 of 176
2.27.3. In the negotiation of any contract care must be taken to very clearly state the terms upon which the HSE agrees to any exclusive use of the supplier and their goods or services.
2.27.4. Particular consideration must be given to HSE locations or services that may have
low volume or low value requirements or may be geographically remote.
2.27.5. The following should be the over riding factor in Putting in Place contracts;
1. the achievement of value for money including the use of scarce staff resources (within procurement and service delivery)
2. At all times, one must fully comply with Public procurement requirements.
2.27.6. The non-use of a relevant existing valid contract, other than as clearly provided for the contract, must be approved by the specifically delegated Assistant National Director (delegated by National Management Team Member) or by the Head of Procurement. The Head of Procurement must be notified in all cases.
2.27.7. Where contracts have already been negotiated this simplifies the purchasing
process. It should enable the relevant staff member to focus on selecting the required goods from the contract list or catalogue.
2nd required preference; Invitation to 3rd Party Supplier to supply General
2.28. If goods or services cannot be sourced from stock or by calling off an existing contract then it will be necessary to source a supplier(s) directly.
2.29. It is a mandatory requirement of these regulations that a competitive process should be
used unless there are justifiably exceptional circumstances (see paragraph A2.1 on page 77 which sets out such circumstances).
2.30. Where HSE funds external organisations;
2.30.1. which are awarding works or related services contracts and
2.30.2. HSE is funding these contracts by 50% or more then
2.30.3. these organisations must comply with the sourcing requirements in these
regulations.
2.31. This provision applies to both commercial and voluntary / not for profit organisations
funded by HSE
2.32. Every manager sourcing a supplier has an obligation to ensure that they are in a position to accurately and clearly specify their requirements to potential suppliers, regardless of value threshold.
Health Service Executive National Financial Regulations
Ver 1.3 Page 30 of 176
2.33. Value Thresholds for Sourcing of Suppliers- General (Ref Table 1, on page 69).
2.33.1. The value of the likely purchase is the major factor in choosing the required method
for sourcing the supplier.
2.33.2. All values should be applied excluding VAT unless otherwise stated.
1. Goods – The threshold should be applied in respect of the need for the same or similar goods for the remainder of the current financial year.
2. Services (including construction related services) - The threshold should be applied in respect of the need for the same or similar services for the remainder of the current financial year.
3. Works – The threshold relates to the specific construction works.
Authorisation of Capital Projects, and the related Expenditure Approval and Sourcing of Supplies and Services must be undertaken and managed by Estates Function.
2.33.3. In applying the value thresholds for sourcing managers must take account
requirements for the same or similar goods or services in as wide an area of the overall HSE service as possible.
2.33.4. In practice, managers must, at a minimum, have regard to the likely needs of their
PCCC area ( HSE South, HSE Dublin North, HSE West, HSE Dublin) or Hospital Network in applying the value thresholds to decide on the appropriate method for sourcing potential suppliers. (refer to Aggregation of Tenders on page 47 below).
2.34. Prohibition on “Splitting of Purchases” to avoid value thresholds
“Splitting of Purchases” occurs where a staff member separates what is in effect one requirement into two or more separate lots for the purpose of applying a lower than appropriate value threshold.
This practice represents a very serious breach of the Financial Regulations and is prohibited. (Refer to paragraph 1.2.5 above)
2.35. Value Thresholds for Sourcing represent the minimum acceptable control levels.
A Budget Holder must, if they believe it appropriate, require the use of the more open methods of sourcing suppliers even where the expected value does not make this mandatory.
Such an approach would be required, for example, if they deem it necessary to:
Ensure proper controls are in place Achieve best value for money
Health Service Executive National Financial Regulations
Ver 1.3 Page 31 of 176
2.36. SOURCING OPTIONS THAT COMPLY WITH THIS FINANCIAL REGULATION
2.36.1. Table 1; A summary of main requirements with regard to Sourcing of Suppliers is set
out in Table 1 on page 69. This includes the Methods of Sourcing, Number and form of quotes/tenders and minimum time for receipt of quotes/tenders allowed by these regulations for different bands of spend.
2.36.2. The following options may be utilised in cases where either acquiring from stock or
from an existing contract are not possible:
1. Direct approach to one or more potential suppliers seeking quotes – see variations below but operates within €1 to €50,000 range, excluding VAT.
2. Public Invitation of Tenders (Non EU) – see variations below but operates between € 50,000 to € 211,000, excluding VAT for goods / services € 5,278,000 for works).
3. EU Public Tender – see variations below but operates for anything over the thresholds listed at 2 above.
2.37. If there is any uncertainty as to which value range the required goods / services fall into
then the next highest range should be assumed and the sourcing options required for that value range are to be utilised.
2.38. Budget Holders and their nominees are required to use the sourcing options required by
the higher value ranges where it is probable that this will yield better value for money. They must satisfy themselves that any additional expense and / or additional time involved can be justified.
2.39. Authorisation to seek quotes / tenders N6
2.39.1. Each Budget Holder or their nominee must set out the appropriate authorisation to
be obtained prior to seeking quotes or tenders. This must be covered in the formal documented purchasing arrangements that is required to put in place.
2.39.2. As a minimum the following must be complied with:
1. Grade VI or higher must approve in advance any proposal to seek tenders (above €50k) up to the EU threshold levels
2. Grade VIII or higher must approve in advance any proposal to seek tenders requiring EU tendering procedures.
2.39.3. The ‘General Requirements’ with regard to Tendering are set out on page 54 and include Tender Receipt, Custody and Opening, Tender Evaluation, Tender Award, Notification of Results and Documentation.
2.40. Please refer to section ‘Professional Input to Tendering’ on page 46 which details the requirements to obtain appropriate professional procurement input where the value of purchases exceeds €25,000.
2.41. Issue of Tender Forms / Documentation
A record must be kept of each request for tender documentation detailing when received, when responded to and documentation issue.
N6 Quotations/Quotes (for the purpose of these regulations) refers to values up to €50,000, the term ‘Tender’ or ‘bid’ refers to a more formal submission by a supplier to supply goods or services greater than €50,000.
Health Service Executive National Financial Regulations
Ver 1.3 Page 32 of 176
2.42. Minimum time to be allowed for receipt of quote/tender.
(Refer to Table 1 on page 69) 2.42.1. The times specified are the minimum allowed. Managers are required to allow
additional time where doing so could be considered reasonably necessary.
2.42.2. Additional time should be allowed if it is considered necessary to secure the minimum number of quotes / tenders or to achieve best value for money.
2.42.3. Real time constraints that may exist around meeting service needs must be taken account of when considering allowing additional time.
2.43. Receipt of less than the required number of quotes
(Refer to Table 1 on page 69) Above the €50,000 threshold the receipt of less than the minimum required number of quotes means that there is a requirement for the next level up of authorisation to approve the resulting purchase order or contract.
For example - ordinarily these regulations provide that a Grade V can approve purchase orders up to €10,000 for routine expenditure but in the event that only 2 quotes are obtained for goods costing €9,000 then the approval of a Grade VI is required.
2.44. The relevant manager is required to consider whether the objective of achieving best
value for money would be better served by restarting the quotation process in an effort to achieve the required minimum number of quotes.
2.45. All potential suppliers must have equal access to information
2.45.1. All potential suppliers must be informed in a consistent way as to any criteria that
may be used to evaluate their quotes or tenders. 2.45.2. HSE staff must not give any real or perceived advantage to any potential supplier.
2.45.3. It is essential that any information or clarification provided to one supplier is
provided in the same format and at the same time to all potential suppliers regardless of whether they have requested it or not.
2.50. Evaluation of Quotes and Tenders
The general principles regarding evaluation of tenders set out on page 54 and 98 must be applied to the quotation process. Evaluation of quotes must involve the use of objective and fair criteria that are consistently applied.
2.50.1. The Most Economically Advantageous Tender (MEAT)G4 or Lowest Price
achieved must be accepted. (see paragraph 3.30 below).
2.50.2. As the value threshold for quotes is lower than for tenders (quotes up to €50k, Tenders thereafter) it is expected that the quotation process will be less formal than the tender process and will require less documentation.
2.50.3. A clear record should be kept of the evaluation of all quotes and tenders - in
particular where the lowest priced quote is not accepted the reasons for this must be recorded for future audit.
Health Service Executive National Financial Regulations
Ver 1.3 Page 33 of 176
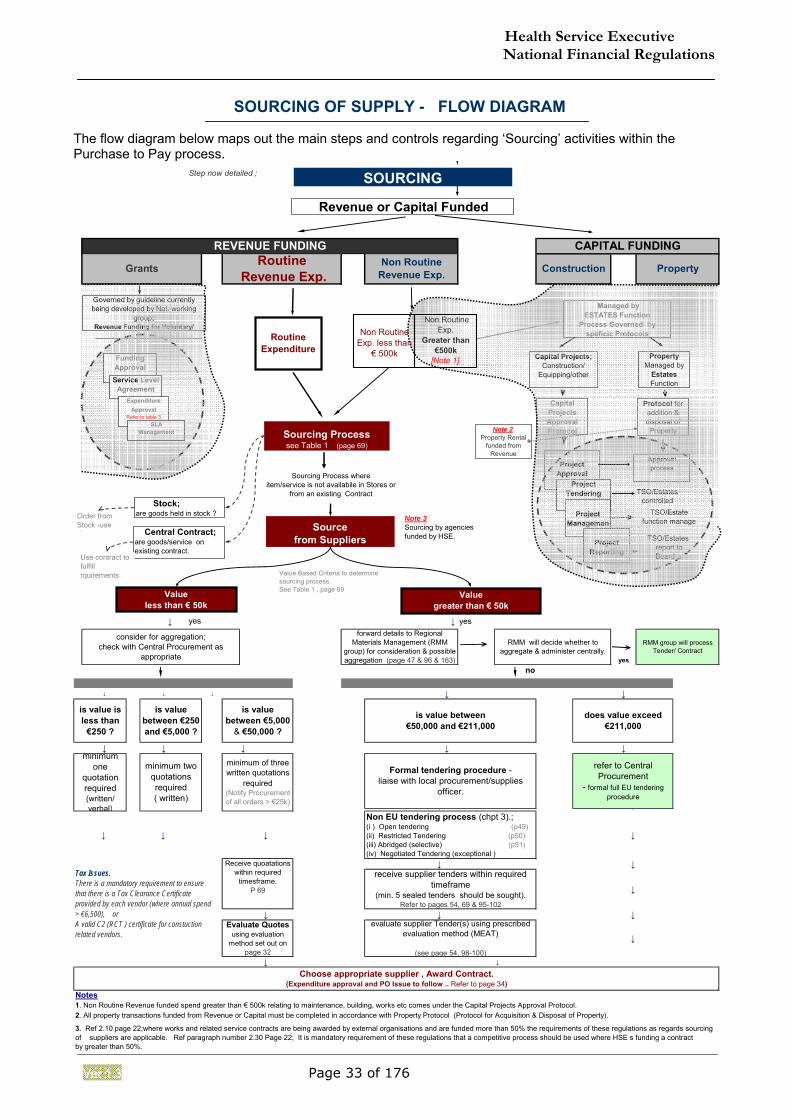
SOURCING OF SUPPLY - FLOW DIAGRAM The flow diagram below maps out the main steps and controls regarding ‘Sourcing’ activities within the Purchase to Pay process. Step now detailed ;
↓ ↓ yes
yesno
↓ ↓ ↓ ↓ ↓
↓ ↓ ↓ ↓ ↓
↓ ↓
↓ ↓ ↓ ↓
↓ ↓
↓
↓ ↓ ↓
↓
↓ ↓
Notes
RMM will decide whether to aggregate & administer centrally.
does value exceed €211,000
refer to Central Procurement
- formal full EU tendering procedure
is value between €50,000 and €211,000
forward details to Regional Materials Management (RMM
group) for consideration & possible aggregation (page 47 & 96 & 163)
RMM group will process Tender/ Contract
Formal tendering procedure - liaise with local procurement/supplies
officer.
1. Non Routine Revenue funded spend greater than € 500k relating to maintenance, building, works etc comes under the Capital Projects Approval Protocol.2. All property transactions funded from Revenue or Capital must be completed in accordance with Property Protocol (Protocol for Acquisition & Disposal of Property).
3. Ref 2.10 page 22;where works and related service contracts are being awarded by external organisations and are funded more than 50% the requirements of these regulations as regards sourcing of suppliers are applicable. Ref paragraph number 2.30 Page 22; It is mandatory requirement of these regulations that a competitive process should be used where HSE s funding a contract by greater than 50%.
Non EU tendering process (chpt 3).;(i ) Open tendering (p49)(ii) Restricted Tendering (p50)(iii) Abridged (selective) (p51)(iv) Negotiated Tendering (exceptional )
receive supplier tenders within required timeframe
(min. 5 sealed tenders should be sought).Refer to pages 54, 69 & 95-102
Choose appropriate supplier , Award Contract. (Expenditure approval and PO Issue to follow .. Refer to page 34)
CAPITAL FUNDINGREVENUE FUNDING
PropertyGrants Non Routine Revenue Exp. ConstructionRoutine
Revenue Exp.
evaluate supplier Tender(s) using prescribed evaluation method (MEAT)
(see page 54, 98-100)
Receive quoatations within required
timesframe.P 69
Evaluate Quotes using evaluation
method set out on page 32
yes
is value is less than
€250 ?
is value between €5,000
& €50,000 ?
is value between €250 and €5,000 ?
minimum of three written quotations
required(Notify Procurement of all orders > €25k)
minimum two quotations required( written)
minimum one
quotation required(written/verbal)
consider for aggregation;check with Central Procurement as
appropriate
Revenue or Capital Funded
Capital ProjectsApproval Protocol
Project Approval
Project Tendering
Property Managed by
Estates Function
Capital Projects;Construction/
Equipping/other
Protocol for addition & disposal of Property
Approval process
TSO/Estates controlled
TSO/Estates report to Board .
Sourcing Processsee Table 1 (page 69)
Sourcing Process whereitem/service is not availabile in Stores or
from an existing Contract Stock;are goods held in stock ?
Central Contract;are goods/service on existing contract.
Source from Suppliers
Value greater than € 50k
Value Based Criteria to determine sourcing process.See Table 1 , page 69
Project Managemen
t
TSO/Estate function manage
Project Reporting
Value less than € 50k
Governed by guideline currently being developed by Nat. working
group; Revenue Funding for Voluntary/
Funding ApprovalService Level
AgreementExpenditure
ApprovalRefer to table 3
SLA Management
Managed by ESTATES Function
Process Governed by speficic Protocols
SOURCING
Order from Stock -use stores
Use contract to fulfill rquirements
Non Routine Exp.
Greater than €500k
[Note 1]
Note 2Property Rental
funded from Revenue
Non Routine Exp. less than
€ 500k
Routine Expenditure
Note 3Sourcing by agencies funded by HSE.
Tax Issues.There is a mandatory requirement to ensure that there is a Tax Clearance Certificate provided by each vendor (where annual spend > €6,500), orA valid C2 (RCT ) certificate for constuction related vendors.
Health Service Executive National Financial Regulations
Ver 1.3 Page 34 of 176
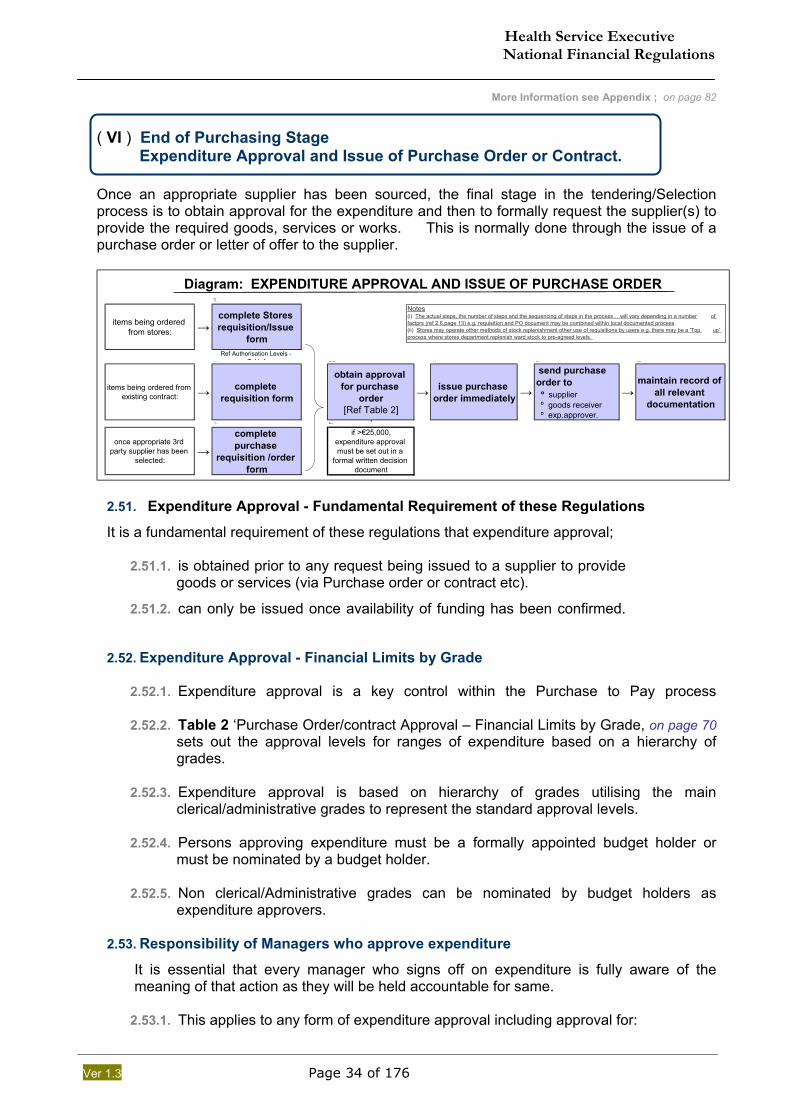
More Information see Appendix ; on page 82
( VI ) End of Purchasing Stage Expenditure Approval and Issue of Purchase Order or Contract. Once an appropriate supplier has been sourced, the final stage in the tendering/Selection process is to obtain approval for the expenditure and then to formally request the supplier(s) to provide the required goods, services or works. This is normally done through the issue of a purchase order or letter of offer to the supplier.
1.
items being ordered from stores: →
complete Stores requisition/Issue
formRef Authorisation Levels -
Table11. 60 4. 5. 6.
items being ordered from existing contract: → complete
requisition form
obtain approval for purchase
order[Ref Table 2]
→ issue purchase order immediately →
send purchase order to º supplier º goods receiver º exp.approver.
→maintain record of
all relevant documentation
↓1. 2.
once appropriate 3rd party supplier has been
selected:→
complete purchase
requisition /order form
if >€25,000,expenditure approval must be set out in a
formal written decision document
Diagram: EXPENDITURE APPROVAL AND ISSUE OF PURCHASE ORDERNotes(i) The actual steps, the number of steps and the sequencing of steps in the process….will vary depending in a number of factprs (ref 2.6,page 13) e.g. requisition and PO document may be combined within local documented process(ii) Stores may operate other methods of stock replenishment other use of requisitions by users e.g. there may be a 'Top up' process where stores department replenish ward stock to pre-agreed levels.
2.51. Expenditure Approval - Fundamental Requirement of these Regulations
It is a fundamental requirement of these regulations that expenditure approval;
2.51.1. is obtained prior to any request being issued to a supplier to provide goods or services (via Purchase order or contract etc).
2.51.2. can only be issued once availability of funding has been confirmed.
2.52. Expenditure Approval - Financial Limits by Grade
2.52.1. Expenditure approval is a key control within the Purchase to Pay process
2.52.2. Table 2 ‘Purchase Order/contract Approval – Financial Limits by Grade, on page 70 sets out the approval levels for ranges of expenditure based on a hierarchy of grades.
2.52.3. Expenditure approval is based on hierarchy of grades utilising the main
clerical/administrative grades to represent the standard approval levels. 2.52.4. Persons approving expenditure must be a formally appointed budget holder or
must be nominated by a budget holder. 2.52.5. Non clerical/Administrative grades can be nominated by budget holders as
expenditure approvers. 2.53. Responsibility of Managers who approve expenditure
It is essential that every manager who signs off on expenditure is fully aware of the meaning of that action as they will be held accountable for same.
2.53.1. This applies to any form of expenditure approval including approval for:
Health Service Executive National Financial Regulations
Ver 1.3 Page 35 of 176
The issue of a purchase order. The issue of a contract. Expenditure by any other means.
2.53.2. In effect the manager is confirming that he has taken all reasonable steps to
assure him/herself that:
1. The expenditure is appropriate to meet the need.
2. Proper procurement has taken place.
3. The expenditure is within the available budget.
4. The Financial Regulations have been complied with.
5. It is in order to request supplier to provide goods/services.
2.53.3. In assessing whether sufficient budget is available to cover any proposed purchase the manager must take account of all expenditure to date including commitments and known additional expenditure to the end of the financial year.
2.54. It is a mandatory requirement that requests to suppliers are in writing in the form of:
System Purchase Orders Manual Purchase Orders Contracts Other written format approved by the relevant Assistant National Director
of Finance
2.55. Purchase orders must actually be sent to suppliers once issued.
Ref to Additional Information regarding PO requirements in the related Appendix on page 84
Where there is a necessity to place orders verbally the appropriate purchase or other written request as approved, must be issued to the supplier on the next available working day and must be clearly marked “confirmation of verbal order dated xx/xx/xx”.
2.56. Information regarding the acceptance of any tender can only be given to unsuccessful
tenderers after the relevant Budget Holder has approved the expenditure and the award of the contract.
2.57. Value thresholds are applied to determine the level of managerial approval required in
respect of any given purchase order / contract or expenditure by any means as set out in Table 2 on page 70.
2.58. Splitting of Expenditure Approvals – Prohibited
Expenditure approvals must not be artificially divided up or “split” so as to avoid the proper application of the expenditure approval limits set out in 111Table 2 on page 70.
2.59. Purchases extending over a number of months
2.59.1. The approval of expenditure for goods or services to be provided over an extended period of time should be treated as one expenditure approval and requires the appropriate grade of manager to approve.
Health Service Executive National Financial Regulations
Ver 1.3 Page 36 of 176
2.59.2. This applies for example to grants to outside agencies (s.65’s etc) – the approval of the annual grant for the year and any subsequent adjustments to that grant are deemed to be expenditure approval decisions.
2.59.3. The processing of the monthly / quarterly grant payments are not expenditure
approval decisions but do require appropriate validation and sign-off in terms of satisfactory receipt of services.
2.60. Departure from the Financial Limits by Grade
2.60.1. This section must be read together with section ‘1.e Departures from Regulations’ on page 18.
2.60.2. Where it can be shown that there is a pressing need individual staff members can
be authorised to hold the expenditure approval limit of the next grade above them.
2.60.3. Contingency arrangements G5 should be prepared to ensure that short term gaps that require temporary departure from financial limits. For example procedures to be put in place to address holiday and sickness cover.
2.60.4. The relevant Assistant National Director/ Hospital Network Manager must approve
such arrangements. These do not take effect until they are notified to the relevant Assistant National Director of Finance.
2.60.5. Departures from limits applies only to Grade IV and above.
2.60.6. Such departures must be treated as exceptional and must be reviewed at least
annually and formally re-approved if they are required to continue.
2.61. Requirement for Written Decisions – General
There is a mandatory requirement to ensure that sufficient documentation is retained to facilitate any necessary future review of the rationale behind any expenditure approval.
2.61.1. For purchases below € 50,000 appropriately filed and accessible copy letters, requests, quotes etc will provide sufficient documentation to meet this requirement.
The approval of the appropriate manager must be clearly noted and dated above their signature on a purchase order or other relevant documentation.
2.61.2. For expenditure above € 50,000 a formal written decision must be retained along
with other written decisions of the relevant manager. Details of requirement for written decision in addition to the requirement to notify the relevant Assistant National Director of Finance are set out on page 83.
2.62. Expenditure Approval on Financial Information System /Accounting System
Ref to Additional Information regarding requirement in related Appendix. on page 82.
Whenever practical the aim should be to facilitate the streamlining of the expenditure approval process without any reduction in financial control. This aim can be achieved by ensuring that managers approving the issue of purchase orders / contracts e.g. do so using accounting system directly. Transitional arrangements will operate for those locations with accounting systems with insufficient functionality to allow on-line approval.
Health Service Executive National Financial Regulations
Ver 1.3 Page 37 of 176
Go to Start of Chapter; on page 19
Procurement Process – Main Requirements on page 22 Payment Process – Main Requirements on page 43
2e. RECEIVING; MAIN REQUIREMENTS Definition The receipt / receiving process for goods or services cover the following activities: 1. Checking and recording that the goods or services received match the specification of what was ordered or contracted by the HSE. 2. Checking and recording that the goods or services that have been received are in good order and are deemed to be fit for the purpose for which they were supplied.
The receipt / receiving process are complete when 1. to 2. are complete.
2.63. The Key control within the Receiving process is to ensure that the quantity and quality
of goods specified have been satisfactorily delivered to meet the customer requirements.
2.64. At this stage it is appropriate to record the accounting entries in the Financial Information System (FIS) to:
i) recognise the liability to pay for the goods, services or works ii) record the expenditure against the relevant Budget Holder
This is achieved by inputting a Goods Received Note (GRN) onto the FIS.
It is important that the receiving process is completed efficiently and without undue delay to ensure that the HSE recognises its liabilities and records expenditure at the earliest appropriate time.
2.65. Receipt / Receipting –Key Control Stage
Receipt / receipting is the second and final key control stage in the purchase to pay process. Once this stage has been appropriately reached what remains are important but lesser control points around invoice checking.
2.65.1. When a manager makes a decision that the receiving process is complete they are in
effect making a decision to pay for the goods and services provided an appropriate payment request (invoice) is subsequently received(refer to paragraphs 2.82 , 2.83 & 2.91 below).
They may never see the invoice unless their personal involvement is required to address any mismatch between the invoice and the goods received.
2.65.2. These regulations support the need to move away from the inefficient process of having invoices circulating around the HSE to be certified.
2.65.3. This is becoming increasingly unnecessary with modern financial systems that can
automate the matching of invoices against purchase orders and delivery documents (Goods Received Notes).
RECEIVING PROCESS
Health Service Executive National Financial Regulations
Ver 1.3 Page 38 of 176
2.46. General Application of Receipt / Receiving regulation
These regulations cover the entire HSE and, given the diversity inherent in the HSE, variations may occur in the detail around:
2.65.4. Exactly by whom or in what manner goods or services are received.
2.65.5. At what precise stage or by whom the checking of what has been received against
the price, quantity and specification of what was ordered or contracted for will be carried out.
2.65.6. The precise manner and by whom it will be decided that it is in order to pay for the
goods or services upon request. 2.65.7. Who exactly performs the related accounting entries involving inputting what FIS
refers to as a Goods Received Note that has the effect of :
Recording a liability in the accounts of the HSE
Recording the expenditure against the budget of the relevant Budget Holder.
It is not intended to prescribe the detail of exactly how the receipt / receiving process will operate in specific locations, however, the following are mandatory requirements:
Mandatory Controls within Receiving. A. Segregation of Duties within Receipt / receiving of goods and services Page 39 B. Procedures for receiving to be put in place by Budget Holders Page 39 C. Delivery of Goods/Services to Nominated Receipting Location Page 40 D. Inspection, Checking and ‘Matching’ of Receipt Page 40 E. Authorisation and Sign-off for Receipt of Goods and Services. Page 41
Health Service Executive National Financial Regulations
Ver 1.3 Page 39 of 176
A. Segregation of Duties within Receipt / receiving of goods and services
2.66. No manager can both make the decision to issue a purchase order or contract and also sign-off on the receipt of the goods or service
2.67. There must a clear separation of duties between the Purchase Ordering and Receiving.
2.68. Required Sign-off on receipt of goods or services :
1. Up to €5,000, receipt must be approved by grade III
2. Up to €25,000, receipt must be approved by grade lV
3. Above €25,000, receiving must involve at least 2 managers one of whom
must be at Grade V or above.
2.69. Example of Receipt of Goods greater than €25,000.
Example A: Staff member A initially receives the goods and physically inspects and signs off that the goods are in order etc and can be paid for when invoiced. A separate staff member must carry out the accounting entries i.e. by recording the receipt on the system.
Example B: Staff member A initially receives the goods and carries out all the inspection checks etc. Staff member B signs off that receipt is complete and it is in order to pay for goods once invoice received. Two people have now been involved in the process so either staff member can complete the accounting entries or a third staff member can do so.
2.70. No manager can have the sole sign-off on receipt of goods or services that are intended primarily for his or her own day to day use.
2.71. Segregation of Duties within Receiving should be read in conjunction with Segregation of
Duties within Purchasing on page 23.
B. Procedures for Receiving to be put in place by Budget Holders
Refer Additional Information on page 89
2.72. Receiving Procedures and Locations
2.72.1. Receiving of good or services may occur at designated receiving points e.g. hospital stores or a health centre within community care. The purchase order should state the designated point of delivery.
2.72.2. Responsibility rests with the relevant Budget Holder to ensure appropriate receiving procedures are in place to enable compliance with these regulations.
2.72.3. Budget Holders must put in place clearly documented procedures for the efficient
operation of the main elements of the receiving process outlined above.
2.72.4. A key control is ensuring that issues with goods or services received are identified as soon as possible after receipt and notified to the supplier.
2.72.5. The receipt / receiving arrangements put in place must be formally reviewed and updated at least annually and the output of these reviews must be held available for future audit.
Health Service Executive National Financial Regulations
Ver 1.3 Page 40 of 176
C. Delivery of Goods/Services to Nominated Receipting Location G6
Refer Additional Information; on page 90
2.73. Initial Receipt of Goods / Services
The person who initially physically receives the goods or services may not be the person who carries out any or all of the checking referred to above.
The mandatory requirement is that all staff who initially receives goods or services on behalf of the HSE is aware that their minimum obligation is to:
i) Accept the goods/services provided that they have not been formally precluded from doing so
ii) Accept the goods or services on a “subject to inspection / confirmation basis only” if they are not in a position to carry out the necessary checking while the deliverer waits.
iii) They must clearly mark this on any documentation they are signing for the deliverer.
iv) Obtain and retain a copy of any delivery documentation including anything signed by them for the deliverer and pass it to the appropriate staff member.
v) Maintain safe custody of the goods until they are brought within whatever local inventory / asset management arrangements are in force for that location.
vi) Immediately, or as soon after as is practical, notify the appropriate staff who is responsible for carrying out the remaining or next step in the process. (This will form part of the ‘Fixed Asset Management and Stock’ section scheduled to be developed and implemented in phase 2 of the NFR)
2.74. Derogation ;
Budget Holders may, with the approval of the Assistant National Director/Hospital Network Manager (or nominee) co-signed by the relevant Assistant National Director of Finance put in place alternative arrangements.
Such arrangements may involve random sample verification or other measures not involving full confirmation of delivery for each specific direct delivery prior to payment. There is a balance to be struck between the value of the goods or services and the cost of verifying their receipt.
D. Inspection, Checking and ‘Matching’ of Receipt
Refer Additional Information on page 91 2.75. Procedure following Initial Physical Receipt
Goods or services must be inspected and checked on a timely basis. This should take place at the time of delivery or if not, then as soon as possible after actual delivery of goods or services. Delivery of goods or services must be inspected and checked in respect of:
i. Match to specification i.e. was it what was ordered in terms of quantity, type etc
ii. Fitness for purpose – i.e. are they fit for the purpose for which they were purchased or are there any obvious defects etc.
iii. Match to price indicated on the purchase order or contract
Health Service Executive National Financial Regulations
Ver 1.3 Page 41 of 176
2.76. Timing of Inspection / Checking of goods or services received
2.76.1. There is a mandatory requirement to inspect goods and services as soon as is practical following delivery.
2.76.2. It is important that Budget Holders ensure that this aspect of the receipting process
is carefully managed to ensure the HSE does not suffer any loss due to late checking of goods or services received.
2.76.3. Suppliers generally have set time periods within which they must be notified of any
problems with goods or services delivered by them. 2.76.4. In respect of services this requirement is particularly important given that services
can generally not be “returned”.
2.77. 1a. Matching to purchase order specification
2.77.1. Discrepancies against the original purchase order or contract must be identified
and a decision made as to what action, if any, is required to resolve the issue.
2.77.2. All material discrepancies and action taken to resolve must be recorded.
2.77.3. Where some of the goods do match what was ordered then a decision must be taken and recorded as to whether these goods will be accepted or whether the entire delivery should be rejected.
2.78. Return of Goods to the Supplier
Refer to Additional information on page 92
2.78.1. Faulty or excess goods or goods that do not match what was ordered should be returned immediately or as soon as possible to the supplier.
2.78.2. The HSE should not suffer the cost of returning goods to any supplier where they are defective or do not match what was ordered.
E. Authorisation and Sign-off for Receipt of Goods and Services.
2.79. Sign-off on Receiving Process
It is a mandatory requirement that at the conclusion of the receiving process a decision is made and appropriately recorded.
2.79.1. Managers must be pragmatic around how this is achieved and in most cases a note on the purchase order or delivery document signed by a manager at the appropriate level will suffice.
2.79.2. The signing off on the satisfactory receipt of a good or service is an
important control. It represents the “point of no return” in respect of most purchases. However, it is a lesser control than that required to authorise expenditure in the first place.
Health Service Executive National Financial Regulations
Ver 1.3 Page 42 of 176
2.80. Professional Input to Receipting Goods/Services over € 50,000
2.80.1. Depending on the nature of the goods or services (remembering that services includes building services) it may be necessary to obtain professional and / or technical advice internally or externally as to the receipt of goods or services.
2.80.2. The provisions outlined on page 25 above within Purchasing as regards obtaining
professional / technical input to expenditure approval above €25,000 also apply to signing off on satisfactory receipt of goods or services above the threshold.
2.81. Written Decisions for Receipts of Goods, Services and Works.
2.81.1. A written decision signing off on the satisfactory receipt of goods or services is required where the value received is in excess of €100,000 for Non Routine expenditure.
2.81.2. This decision must summarise the steps taken to validate that the goods or
services received matched what was ordered/contracted for and were free from obvious defect.
2.82. Responsibility of Managers who sign-off on receipt of Goods/Services
2.82.1. It is essential that every manager who signs off on receipt of goods or services is fully aware of the meaning of that action as they will be held accountable for same.
2.82.2. In effect, once a Goods Receipt Note has been created on the system which matches to a purchase order, the person who has approved the GRN has triggered a decision to pay, subject to receipt of a valid invoice.
2.83. Managers who sign-off on the receipt of the goods or services are confirming the following:
Ref also to paragraph 2.91 on page 44. That all steps in the receiving process up that point whether carried out by them or on
their behalf or otherwise
Are to the best of their knowledge, having taken all reasonable steps to assure themselves of same, fully compliant with these Financial Regulations.
And are fully compliant with any other relevant requirements that are in force at that time.
Health Service Executive National Financial Regulations
Ver 1.3 Page 43 of 176
Go to Start of Chapter; on page 19 Procurement Process – Main Requirements on page 22 Receiving Process – Main Requirements on page 37
2f PAYMENT PROCESS; MAIN REQUIREMENTS
2.84. Definition
The release of payment, following receipt and matching of a payment request (usually an invoice) to what was ordered and satisfactorily received.
2.84.1. Payment is the final stage of the ‘Purchase to Pay’ process.
2.84.2. Payment should only occur after proper sign-off of the satisfactory receipt of goods, services or works.
2.84.3. Authorised Payment requests for specified payments in advance (refer to page 56 onwards).
2.84.4. Payment clears the HSE liability to the supplier.
2.85. Payment - General
The controls around the payment element of the purchase to pay process are essential but not as fundamental as those covering Purchasing and Receipt. The focus of controls currently around invoice certification/approval those within Purchasing and Receiving.
2.85.1. By the time the purchasing and receipt stages have been properly completed the
HSE has:
i. A) Approved expenditure via the issue of a purchase order or contract.
i. B) Signed off that satisfactory receipt has been achieved and payment is in order once a proper payment request is received.
2.85.2. The control issues at payment stage are around confirming that the above have
taken place and that the payment request (usually an invoice) agrees with same, particularly in terms of price.
2.86. These regulations require that the HSE move as quickly as possible to a situation where the bulk of payment requests (invoices) are;
received centrally within the shared services centre or equivalent
automatically matched to the purchase order and GRN
automatically approved for payment once a three way match is achieved
(3 way match = 1. Purchase Order + 2. Goods Receipt Note + 3. Invoice )
routed electronically to the relevant staff member for resolution if auto matching fails
2.87. Information to Appear on Invoices – Minimum requirement
It is the responsibility of each Budget Holder to manage relationships with suppliers, either directly or through the staff operating the procedures to ensure that invoices are received promptly and contain all the necessary prescribed information.
PAYMENT PROCESS.
Health Service Executive National Financial Regulations
Ver 1.3 Page 44 of 176
2.88. An invoice must contain the following information;
Supplier Name and Address
Invoice Number and Invoice Date/ Tax point (date which VAT applies)
Purchase order number or equivalent agreed number.
Delivery details, reference number, delivery date and delivery address
Description of Goods or services being purchased
Supplier VAT and Registration number
Vat Exclusive Amount, Vat amount by Vat Code and total invoice amount
Certification information required e.g. engineering certification of work.
2.89. Tolerance Levels - (When Matching Invoices to PO/GRN)
Refer Additional Information; on page 94
These regulations permit a general price tolerance level of €25 or 2% (whichever is the lower) when matching the total value of an invoice to the relevant amount on the purchase order / GRN.
2.89.1. Quantity differences (Invoice quantity is greater than Ordered) Quantities delivered in excess of the Purchase order quantity should not be accepted and should be taken back by the supplier at no extra cost to the HSE.
2.89.2. Price differences All matching differences above €25 or 2% require the invoice to be referred to the appropriate local staff member for resolution.
2.89.3. Budget Holders must review these reports and report on a quarterly basis to the
relevant Assistant National Director of Finance as regards any trends in the occurrence of matching differences.
2.90. Importance of timely receipting (entry of GRN) on the Fin. Info. System(FIS)
2.90.1. It is essential that goods/services are properly ‘Good Receipted’ on the financial information system (FIS) when actually provided/delivered by the supplier.
2.90.2. This will ensure that any mis-match between the purchase order and goods
received is quickly identified and resolved. This will simplify the process of matching the invoice to the already matched purchase order/Goods Receipt Note.
2.90.3. Prompt entry of the goods receipt notes (GRNs) on the FIS is also essential to
ensure expenditure is recorded at the proper time, i.e. when it is incurred.
2.91. Authorisation Levels for Payment
2.91.1. Provided the purchasing and receipt stages of the process have been carried out in full compliance with these Financial Regulations it is not a requirement to assign any particular authorisation grade level to the payment stage of the process. This is largely due to the fact that this stage is seen as appropriate for automation.
2.91.2. It is crucial therefore that the importance of the purchasing and receipt stages is fully understood by all relevant managers and staff.
Health Service Executive National Financial Regulations
Ver 1.3 Page 45 of 176
2.92. Prompt Payment of Interest Budget Holders must ensure that in designing, implementing and monitoring their purchasing arrangements they are fully aware of and compliant with the requirements of the prompt payment legislation (please read ‘4.c Prompt Payment of Account’ on page 58).
2.92.2. The key prompt payment issue (relating to the purchasing process) is to ensure
that there is clarity as to what payment terms apply in respect of any purchase
order or contract issued to any supplier.
2.92.3. The HSE standard payment terms in respect of normal suppliers or what are
often referred to as “Traders” are within a range of 30 to 45 days from receipt of
invoice or delivery of goods / services whichever is the later.
2.92.4. The payment terms should be quoted on all documentation issued to suppliers
including tender documentation, purchase orders etc.
2.93. There will be cases where payment terms requiring less than 30 days are appropriate
however, these require the specific or general approval of the relevant Assistant National Director of Finance unless encompassed within the following:
2.92.5. Public Utilities (e.g. Eircom, Bord Gais etc.)
2.92.6. Grants to outside agencies – no invoice, paid in accordance with
contract or agreement.
Health Service Executive National Financial Regulations
Ver 1.3 Page 46 of 176
GO TO NEXT CHAPTER on page 56 GO TO LAST CHAPTER ON PAGE 19
3. Purchase To Pay – Tendering
The essential requirements of the financial regulations are contained within the main chapters. However, these should be read in conjunction with additional information contained within the respective appendices (by chapter). More information; on page 95
3.1. TENDERING. .. (A Tendering process is required for all purchases of Supplies or Services above €50,000 unless available from stock or on contract)
3.2. General
3.2.1. The general purchase to pay regulations as set out in pages 19 to 31 must be fully complied with in relation to tenders unless specifically provided for in this section.
3.2.2. This regulation is intended to expand on and clarify the general purchase to pay
regulations in relation to tendering and must always be read in conjunction with those regulations.
3.3. Professional Input to Tendering
3.3.1. Every manager sourcing a supplier has an obligation to ensure that they are in a position to accurately and clearly specify their requirements to potential suppliers, regardless of the value threshold.
3.3.2. Appropriate and necessary procurement input and / or technical / clinical input must
be obtained by the manager sourcing suppliers for values above €25,000.
3.3.3. This input applies to the various stages of the process which can be summarised as:
i) Identification of need and specification of requirements to meet that need
ii) Assessing and evaluating potential suppliers iii) Conduct of tendering process iv) Evaluation and award of tender plus notification to unsuccessful tenderers
v) Supervision of supply of goods, services or works (in some cases project
management)
vi) Sign-off on satisfactory receipt / completion of goods, services or works
3.4. Works - Tenders for Construction Works and Related Services
3.4.1. It is a mandatory requirement that the provisions of the purchase to pay process regulations as specified on page 22 to 43 be fully complied with as regard works and related services unless specifically indicated otherwise in this section.
3.4.2. It is also a mandatory requirement that the provisions of Capital Projects regulations
as specified below on page 62 are fully complied with regard to Works and related services, unless specifically indicated otherwise in this section.
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 47 of 176
3.5. Public Advertisement
More information; on page 95 3.5.1. Compliance with the requirement for public advertisement involves publication on
the government tendering web site www.etenders.gov.ie. or national newspaper.
3.5.2. Only the relevant specially delegated Assistant National Director(s) can approve a departure from the requirement for public advertisement (above €50,000 for goods/services or above €500,000 for works), but only in exceptional circumstances as detailed on page 77.
3.5.3. This approval must be co-signed by the Head of Procurement.
3.6. Aggregation of Tenders/ Tender Coverage (Source ; Regional Material Management’s “Procedure for Tender/Contract Approval”) More information; on page 96 Template form to Complete on page 163
3.6.1. It is the policy of the HSE to move to a situation where the level of aggregation of purchasing is increased consistent with full compliance with EU Procurement requirements and achievement of Value for Money.
3.6.2. These regulations require that pending the completion of the change process
outlined above, the following “Procedure for Tender/Contract Approval (issued in March 2005 by Regional Materials Management Group ) will apply.
3.6.3. This pre-tender procurement Aggregation process (Tender/Contract Approval
procedure) applies to proposed tender process with an estimated contract value in excess of the high values (currently €50k) defined in the procurement policy.
3.7. Dealing with uncertainty around likely tender values
3.7.1. The thresholds for EU Procurement have been set out on on page 69 above. These values are based upon the VAT exclusive value of expected spend.
3.7.2. Reasonable estimates must be used when estimating the likely value of a tender to
determine whether the EU thresholds will be reached.
3.7.3. The estimates must be: i) Properly arrived at ii) Based on appropriate professional / technical input iii) Properly documented and recorded
3.7.4. In the event that an estimate was used to decide that EU Procurement Procedures
were not necessary and this subsequently turns out to be incorrect, the procurement process remains valid provided the original estimate was reasonable in all respects and stands up to scrutiny.
3.7.5. If there is a reasonable expectation that the EU threshold will be reached there is a
requirement to utilise EU procurement procedures.
Health Service Executive National Financial Regulations
Ver 1.3 Page 48 of 176
GO TO TOP OF CHAPTER on page 46 GO TO EU TENDER PROCESS on page 53
3.8. Non-EU Tenders – Forms of Tender Process
Used where values are below the EU Thresholds ( €211,000 Supplies and Services, €5,278,000 Works)
The 4 options for Non EU Tendering Processes are:
Open Tendering (Non EU) (Page 49) Restricted Tendering (Non EU) (Page 50) Abridged (Selective) Tendering (Non EU) (Page 51)
Negotiated Tendering (Non EU) (Page 52)
General
3.8.1. The general requirement is to ensure that any tendering process utilised by the HSE
is conducted fairly, honestly and in a transparent manner.
3.8.2. The objective is to ensure, to the greatest extent practical, that a sufficiently wide field of competition is attracted to the process to provide assurance that best value for money can be achieved.
3.8.3. It is important to stress that any dialogue with tenderers, that could be construed as
“post tender negotiation” on price or which may result in significant changes in the published tender specifications must be avoided.
3.8.4. Such dialogue is only permitted in the limited circumstances in which the Non EU
negotiated procedure is appropriate – see below.
3.9. The public advertisement of the tender notice is for one of the following purposes:
3.9.1. Inviting potential tenderers to submit tenders, or
3.9.2. Inviting potential tenderers to submit details so they can be qualified for inclusion on a specific (restricted tendering) pre-approved tenderer list,
or 3.9.3. Inviting potential tenderers to submit details so they can be qualified for inclusion on
a general (abridged / selective tendering) pre-approved tendering list,
3.9.4. Departure from the public advertisement requirement is only permitted in the case of genuine exceptional circumstances as detailed on page 77.
3.10. The nature of, and steps within, the chosen tendering process must be made clear to all
potential tenderers. This includes clarity on any pre-qualification process.
Health Service Executive National Financial Regulations
Ver 1.3 Page 49 of 176
3.11. Open Tendering (Non EU)
Used for all value thresholds up to EU levels. 3.11.1. All potential interested parties may submit a tender. This method of tendering will be
the quickest to produce completed tender submissions.
3.11.2. Potential suppliers (tenderers) will have become aware of the tender from the public advertisement of the tender notice.
3.11.3. Consideration should be given to whether it may be necessary to short list the
tenderers depending on the volume of tenders received. In such cases only the tenders submitted by those who have been short listed will be fully evaluated.
3.11.4. Short listing can only be used if the publicly advertised tender notice has
made it clear that the HSE reserves the right to do so.
3.11.5. The criteria for short listing must be included in the tender notice and must be limited to any or all of the following:
1. Personal Situation
2. Financial Capacity
3. Technical Capacity
4. Relevant Experience,
5. Expertise and Competency
3.11.6. ‘Open tendering’ should be the norm where the goods, services or works being
tendered for are of lower value and / or are less complex in nature.
3.11.7. In such cases, the combination of the likely number of tenders that will be received and the required effort to properly evaluate them is not expected to place an undue staff or time burden on the HSE.
3.11.8. The general requirement to notify tenderers of the results of the tendering process
applies to advising any tenderers who have been short-listed from the full evaluation process.
Health Service Executive National Financial Regulations
Ver 1.3 Page 50 of 176
3.12. Restricted Tendering (Non EU)
-Can be used for all value thresholds up to EU Level. N 7
3.12.1. With restrictive tendering you prepare a pre-approved list of potential tenderers for each specific tender process.
3.12.2. The tender notice must make clear that HSE is using a restricted tendering process
and must set out the meaning of this.
3.12.3. The list of potential tenderers must be created following public advertisement of the tender notice and the qualification criteria for inclusion on the list the same as that for ‘Open competition’ i.e. (i) Personal situation, (ii) Financial Capacity (iii) Technical Capacity (iv) Relevant Experience, Expertise and Competency.
3.12.4. The initial tender notice in the restricted process is often referred to as a:
o Request for proposals or o Request for expressions of interest
3.12.5. The list of potential tenderers is prepared by applying the qualification criteria to all
valid proposals/ expressions of interest received. Those on this Approved list are then invited to submit their full tenders.
3.12.6. Those not selected for the approved list must be advised of this fact.
3.12.7. Restricted tendering is used where the HSE has decided in advance that there
is a need to have an initial pre-qualification/short listing process in order to limit the number of tenders to be fully evaluated, to a manageable level.
3.12.8. Restricted tendering is suitable where the goods, services or works being tendered
for are of larger value and / or are more complex in nature.
3.13. Invitation to Tender (Under EU Threshold Values only) Direct invitations may be used for values under EU thresholds. It is possible to ‘Invite’ suitable suppliers or service providers to compete for contacts below the EU thresholds.
3.13.1. Invitations to suitably qualified suppliers for a specific project.
3.13.2. Can be used where there is limited number of qualified suppliers.
3.13.3. Invitation from list established on an open and objective basis.
3.13.4. A sufficient number of potential suppliers to ensure adequate competition (minimum five is strongly recommended) should be invited to tender. Suppliers must be selected on an objective and non-discriminatory basis & should be invited to tender.
3.13.5. Approval to proceed with restricted tender process for tenders greater than €50,000
should be obtained in advance from LHO Manager, NHO Hospital Manager (Band 4 &5) or Assistant National Director and co-signed by the relevant Assistant National Director of Finance co-signed or his/her nominee.
3.13.6. Only after notices are published one may approach particular suppliers directly.
N7 Additional Approval is required to proceed with restrictive tenders for contracts greater than €50,000-see para 3.13.5
Health Service Executive National Financial Regulations
Ver 1.3 Page 51 of 176
3.14. Abridged / Selective Tendering (Non EU)
Can be used up to €50,000 for goods / services and up to €500,000 for works.
3.14.1. Abridged tendering involves the creation and maintenance of a pre-approved list of potential tenderers for related goods, services or works which can be used for a number of tenders over the lifetime of the list.
3.14.2. Lists of pre-approved potential tenderers must be prepared following public
advertisement and must be replaced at least every two years. 3.14.3. An extension of one additional year may be obtained upon approval by the relevant
Assistant National Director of Finance. 3.14.4. When selecting potential tenderers for inclusion on a pre-approved list only the
qualification criteria should be the same as that as open competition i.e. (i) Personal situation, (ii) Financial Capacity (iii) Technical Capacity (iv) Relevant Experience, Expertise and Competency.
3.14.5. Where there is a requirement to tender for goods or services then suppliers on the
pre-approved list are:
1. All invited to submit tenders, or
2. Selected at random and invited to submit tenders or
3. Selected by rotation to submit tenders
3.14.6. Care must be taken not to unfairly or inappropriately discriminate against potential tenderers in preparing and maintaining pre-approved lists.
3.15. This form of tender process is acceptable where:
3.15.1. There is a high volume of procurement activity expected in a given area ,
and / or
3.15.2. It is necessary as a means to ensure that scarce procurement expertise is appropriately managed, and / or
3.15.3. There is a need to be ready at short notice to complete a tendering process without disruption to services.
3.15.4. Under no circumstances can the HSE or any of its officers depart from the need
for public advertisement in preparing a list of pre-approved tenderers for use in abridged tendering.
3.15.5. Abridged or selective tendering represents a departure from the normal competitive
tendering process which is why it is limited in terms of value threshold.
3.15.6. It may only be used with the specific written approval of the relevant LHO Manager, NHO Hospital Manager (bands 4 & 5) or Assistant National Director and must be co-signed by the Head of Procurement or his/her nominee. Notification should be sent to the relevant Assistant National Director of Finance.
Health Service Executive National Financial Regulations
Ver 1.3 Page 52 of 176
3.16. Non EU ‘Negotiated’ Procedure Can be used up to EU Threshold Values
3.16.1. This process may only be used in exceptional circumstances and with the approval of the relevant Assistant National Director co-signed by the Head of Procurement, and notified to the relevant Assistant National Director of Finance.
3.16.2. The standard requirement is that dialogue with tenderers that could be construed as
“post tender negotiation” on price, or which may result in significant changes in the published tender specifications must be avoided.
3.17. The negotiated procedure should only be used where:
3.17.1. The Open or Restricted procedure has failed to identify any suitable tenderers or,
3.17.2. Where the nature of the requirement is so complex as to not facilitate overall pricing without negotiation, or,
3.17.3. Where it is not possible to specify requirements with sufficient precision to enable
potential tenderers to respond with priced tenders, or,
3.17.4. Where one or more of the very exceptional circumstances listed on page 77 apply.
3.17.5. Negotiated tendering must only be used following a public advertisement of a tender notice most likely involving a pre-qualification process as for restricted tendering.
3.17.6. Negotiated Tendering must only be used with the specific written approval of the
relevant Assistant National Director or Hospital Network Manager.
The approval must be must be co-signed by the Head of Procurement or his/her nominee. Notification should be sent to the relevant Assistant National Director of Finance.
Health Service Executive National Financial Regulations
Ver 1.3 Page 53 of 176
GO TO TOP OF CHAPTER on page 46 GO TO NON EU TENDER PROCESS on page 48
3.18. Tenders which require use of EU Procurement Procedures
The EU Procurement Directives have the force of law in Ireland and must be fully complied with in all respects.
3.19. The EU Threshold Values that currently apply (from 1-Jan-06 to 31-Dec-07) are;
o Supplies or Service greater than € 211,000
o Works greater than €5.278 million
3.19.1. The Budget Holder or nominee must notify the procurement function of all purchases
that fall within the EU Thresholds.
3.19.2. Procurement will appoint a Commercial Evaluator who ensures that procurement is in line with current policies and procedures and will co ordinate and lead the tendering process.
3.19.3. The importance of the Procurement Planning Process as detailed above (on page 24)
is very clear when it comes to situations where the EU Procurement Procedures must be used.
3.19.4. In a number of cases, the relatively long notice periods required under the EU
procedures can be shortened where a sufficiently detailed and specific Prior Indicative Notice (PIN) has been published in advance.
3.19.5. Procurement planning will facilitate the placing of EU PIN’s as appropriate.
3.19.6. It is neither intended nor practical to seek to set out in these regulations the level of
detail that is required to comply with the EU Procurement Directives.
3.20. In the first instance, HSE staff seeking to ensure compliance should refer to the document:
3.20.1. “Public Procurement Guidelines – Competitive Process” published in 2004 by
the National Public Procurement Policy Unit (NPPPU) of the Department of Finance following consultation with the Government Contracts Committee (GCC).
3.21. Professional procurement must lead the tendering process when engaging in an
EU tendering Process. (refer to Professional input into purchasing on page 46).
Health Service Executive National Financial Regulations
Ver 1.3 Page 54 of 176
Ref Appendix; on page 95.
TENDER PROCESS – GENERAL REQUIREMENTS Details of the requirements of these regulations regarding tender process summarised below are set out in Appendix on page 97 .
3.22. All potential suppliers must have equal access to information [ A3.6 , page 98]
3.23. Tenders Receipt and Handling
Tenders should be sent in sealed envelopes addressed to the nominated manager in accordance with the detail of these regulations in paragraph A3.4, on page 97.
3.24. Tender Deposit
Any tender deposit charged must be limited to the estimated marginal cost associated with reproducing the tender documents and getting them to each extra potential tenderer (i.e. printing/photocopying plus postage/courier etc).
3.25. Receipt of less than the required number of tenders
Above the €50,000 threshold the receipt of less than the required number of tenders means that the approval of the relevant NHO or LHO manager is required.
3.26. Minimum time to be allowed for receipt of quotes / tenders
The provisions set out in Table 1 on page 69 must be complied with as a minimum.
3.27. Tenders received late Late tenders should not be opened and should therefore not be evaluated
3.28. Custody and Opening of Tenders
Above the € 50,000 threshold sealed tenders are required and must be processed in accordance with procedure set out in paragraph A3.5 on page 97.
3.29. Tender Evaluation
The criteria to be used to evaluate any tender must be objective and the evaluation process must be transparent and fair and disclosed to potential tenderers prior to them completing their tender documents.
The relevant Budget Holder must nominate the person(s) to evaluate any tenders that are received. See also; Requirement for Tender Evaluation Report on paragraph 3.31 below.
3.30. Acceptable Basis of Award of Contracts More information [A3.8]
The following are the accepted bases for evaluation for award of tender contracts within the HSE; Most Economically Advantageous Tender (MEAT) N8 or
Lowest Priced Tender
N 8 MEAT; most economically advantageous tender (specifying, in addition to price, various other criteria including running costs, servicing costs, level of after sales service, technical assistance, technical merit, environmental characteristics). It is the recommended as the primary basis of tender evaluation.
Health Service Executive National Financial Regulations
Ver 1.3 Page 55 of 176
3.31. Requirement for Tender Evaluation Report (above € 50,000)
More Information; Tender Evaluation Report A3.9 on page 99.
3.31.1. Tender reports are required in respect of each tender following receipt and evaluation of tenders. They must be retained as part of the documentation supporting the final purchase order / contract. The value and complexity of the specific tender will determine the precise format and amount of detail necessary to accurately report on the tender.
3.31.2. A minimum of 2 staff, one of whom must be at least at Grade VIII must be
involved in the evaluation of all tenders i.e. above €50,000.
3.31.3. The award of the contract is subject to the evaluation and recommendation by the relevant managers.
3.32. Restrictions on Award of Tenders / Contracts More Information; on page 100.
Before the award of any HSE tender/contract the following must be addressed (more details of requirement in appendix reference A3.11) :
Risk Management
Statutory Provisions Conflicts of Interest
Collusive Tendering
Criminal Convictions
The successful tenderer will be obliged to notify the HSE in writing of any change to the status of this compliance statement that may occur during the period of the contract.
3.33. Tender Award More information; [A3.10, page 100] The award of a contract or issue of a purchase order following a tender process is an approval of expenditure and requires a formal written decision (see ‘Written Decision approving expenditure greater than €50,000 on page 83.
3.34. HSE Standard Terms of Contract.
The use of the HSE Standard Terms and Conditions of Contracts is mandatory – a copy of the standard terms and condition of contract is available on the HSE website (www.hse.ie/en /supplyopportunities/termsandconditions ) or the local supplies officer.
The standard Terms and Conditions of Contract should only be varied, in exceptional circumstances ,with the agreement of the HSE Head of Procurement function or of the relevant Assistant National Director of Finance or his/her nominee.
3.35. Notification of Results of Tendering Process More information; Para. [A3.12]
All tenderers, including those who are not successful, should be informed of the result of the tender process without undue delay.
Health Service Executive National Financial Regulations
Ver 1.3 Page 56 of 176
GO TO NEXT CHAPTER ON PAGE 62 GO TO LAST CHAPTER ON PAGE 46
4. Purchase to Pay – Specific Topics
4.a Non Order Payments below 4.b Prompt Payment of Accounts on page 58
4a Non-Order Payments - General
Detailed Policy and Procedures relating to the following areas are documented in the Appendix;
Taxis on page 103 Petty Cash Disbursements on page 104 Franking Machines on page 109 Utility Bills on page 110 Lease and Rental on page 111 Mobile Phones on page 114 Voluntary Organisations/ Not-for Profit on page 119
4.1. The standard means of requesting a supplier to provide goods or services is by issuing
a purchase order to the supplier.
4.1.1. Purchase Orders are the required default means of requesting any supplier to provide goods or services and should be utilised in all situations unless specifically or generally approved by the relevant Assistant National Director of Finance.
4.1.2. The purpose and expected items for inclusion within a purchase order are set out on page 84 below.
4.1.3. Such approval will be granted in cases where it is clear that the use of a
purchase order will add little if any value in terms of the financial controls or the efficient operation of the process.
4.1.4. Control over Non Order Payments will be exercised by a flag on the (Financial
Information/Accounting System) supplier record allowing processing of an invoice without an order. This will be enforced via a ‘validation’ which only allow non order invoices be recorded on a non order vendor.
4.1.5. The relevant Assistant National Director of Finance must, at least annually,
review the list of approved “non order payments” and renew them where he/she deems it appropriate.
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 57 of 176
4.2. Principles for the use of “Non Order Payments”
4.2.1. The relevant Assistant National Director of Finance will give consideration to approving the use of “Non Order Payments” where it can be demonstrated that:
1) A specific contract is in place for the ongoing receipt of a service for
example:
Utility Bills (ESB, Eircom, Water Charges, Mobile phone costs etc) Nursing Home Subvention / Capitation fees Grants to outside organisations Foster Carer payments
And / or 2) They relate to internal payments for example:
Pay over of payroll deductions Payments to staff (including expenses) Petty Cash / Imprest Recoupments Payment for staff seconded to HSE
And / or
3) Payments that do not involve receipt of any goods or services by HSE but relate to operation of a scheme for the benefit of clients including:
Allowances (disability / welfare) PCRS Medical Schemes (formally known as GMS) Dental Treatment Services Scheme Hepatitis C Methadone Treatment Scheme
And / or
4) Where the sole purpose of issuing a purchase order would be to
enable a payment to be made
And / or
5) Where it is not practical, material or useful to issue a purchase order in advance of the service being provided or invoiced for, including:
Taxi Services Courier Services Emergency call outs
4.2.2. In a number of the cases listed above, HSE does not actually receive invoices
requesting payment. The sections that follow detail specific instances where the use of a purchase order is not required, subject to the approval of the relevant Assistant National Director of Finance.
It is stressed that Budget Holders are always free to continue to use purchase orders where they feel it is necessary.
Health Service Executive National Financial Regulations
Ver 1.3 Page 58 of 176
`GO TO TOP OF CHAPTER ON PAGE 56
4.b Prompt Payment of Accounts
4.3. General
4.3.1. In putting in place formal documented arrangements for the operation of the
purchase to pay process in their areas Budget Holders must have specific regard to the need to ensure that these arrangements:
4.3.2. Comply with statutory prompt payment requirements (SI 388 & 1997 act).
4.3.3. Facilitate payment of prompt payment interest where it is due to be paid.
4.3.4. Minimise the occurrence of late payments and therefore of late payment interest
4.3.5. The statutory requirements are set out in the Prompt Payment of Accounts Act
1997 as amended by the S.I. No 388 of 2002 which gives effect to Directive No. 2000/35/EC.
4.3.6. It is important to note that S.I. 388 of 2002 repealed sections 4 to 11 of the
Prompt Payment of Accounts Act 1997 – these sections were the primary detailed sections which previously governed the practical operation of prompt payments.
4.4. Responsibility and Legal Requirement
4.4.1. Budget Holders and relevant managers and staff are obliged to familiarise themselves with the statutory prompt payment requirements.
4.4.2. Compliance with the Purchase to Pay Financial Regulations will largely ensure
that payments are processed promptly and that late payment interest is minimised.
4.4.3. Compliance with the Act / SI 388 requires that the HSE pay the appropriate
interest in relation to late payments as it falls due.
4.4.4. While incurring prompt payment interest is therefore not a breach of the statutory requirement it is a mandatory requirement of these Financial Regulations that Budget Holders ensure that the purchase to pay process is operated efficiently so as to eliminate late payments and interest to the greatest extent possible.
4.4.5. Interest must be paid at the appropriate rate as set out in the statutory
instrument and will be paid without any request from the supplier.
4.4.6. Interest amounts less than €5 do not need to be paid. – (Ref SI 388)
4.4.7. Compensation payments, which are in addition to late payment interest, are to be paid upon receipt of a written request from the supplier for same.
Health Service Executive National Financial Regulations
Ver 1.3 Page 59 of 176
Ref Page 45
4.5. The following are the key elements in reducing / eliminating late payment interest:
Clarity around payment terms
Budget Holders and relevant managers and staff must ensure that they are aware of the payment terms that apply to the various suppliers they utilise.
The HSE ‘Standard Payment Terms’ are the later of: (a) 30 days* from date of receipt of request for payment (usually invoice)
or
(b) 30 days from confirmation of satisfactory receipt of goods or services
*Important note; A number of former Health Boards have in place existing Standard Payment Terms of 45 days from date of receipt of Invoice. Therefore the current standard terms in operation will range between 30 and 45 days. These supplier accounts will continue to operate with their respective terms until such time as there is a specific comprehensive programme to review, revise and consolidate vender terms and details.
4.5.1. The standard terms may only be varied (upwards or downwards) with the
specific or general approval of the relevant Assistant National Director.
4.5.2. Procurement may, as part of a commercial decision, put in place a central
contract with a supplier with payment terms other than the standard terms of 30 days. These must be approved by the relevant Assistant National Director and Head of Procurement and notified to relevant Assistant National Director of Finance.
4.5.3. Other approved ‘Non-Standard Payment terms’ will be in operation. For
example;
Public Utilities (e.g. Telecom/Eircom, Bord Gais etc.)
Grants to outside agencies – no invoice, paid in accordance with contract or agreement.
4.5.4. Payment terms must be quoted on all of the following;
Invitations to quote Tender notices Tender documentation Contracts and or Purchase orders Other relevant documentation
Health Service Executive National Financial Regulations
Ver 1.3 Page 60 of 176
4.6. Managing Supplier Relationships
4.6.1. Responsibility rests with Budget Holders to ensure that suppliers are managed so that any suppliers not complying are dealt with appropriately.
4.6.2. It is essential that Budget Holders ensure that suppliers are clearly advised as
to: Locations where goods or services are to be delivered. HSE requirements around proof of delivery documentation. HSE requirements around information needed on invoices (in particular the
need to quote purchase order number for all amounts invoiced) and where invoices are to be sent to.
4.6.3. Ultimately suppliers that persistently fail to meet the HSE requirements above
should not be utilised.
4.7. Put the effort in before the Invoice arrives The key to prompt payment is to have an efficient purchasing and receipting process so that:
Suppliers know what is required of them and supply it first time and on time Goods and Services are receipted on FIS as soon as possible after delivery Issues with delivery are identified early and resolved early with suppliers Suppliers invoices match what was ordered and receipted and can be
matched for payment with minimal manual intervention
4.8. Proper record keeping and document handling
4.8.1. The HSE is only liable to pay late payment interest where we are responsible for
the delay in making the payment.
4.8.2. The HSE is required to calculate and pay late payment interest for every commercial transactions not paid before the Relevant Payment Date G7.
4.8.3. It is essential that proper records are kept so that it is possible to differentiate
delays in payment caused by HSE from those caused by suppliers or other parties.
4.8.4. In most cases the payment term of 30 days (or other approved period) will begin
to run when the invoice is received. Where the date of receipt of invoice is uncertain or before receipt of goods/services then date of receipt will apply.
4.8.5. Invoices must be date stamped immediately upon receipt. If it transpires that the
invoice was received prior to receipt of the goods then the date received should be amended to the later date.
4.8.6. Queries or issues with invoices need to be:
Identified quickly Notified without delay to the supplier Recorded and followed up effectively to ensure late payment calculations
are correct.
Health Service Executive National Financial Regulations
Ver 1.3 Page 61 of 176
4.9. Disputed invoices with suppliers
4.9.1. A register must be kept of all disputed invoices with sufficient information to facilitate tracking, follow up and closure once the issue that gave rise to the dispute is addressed.
4.9.2. A formal standard notification that the invoice or specified elements of it are in
dispute must be sent immediately to the supplier with a copy of the invoice. 4.9.3. Where a disputed invoice is returned to supplier within 10 working days of
receipt, then the interest penalty will begin to accrue 10 working days after receipt of corrected or replacement invoice from supplier or , if later, the original prescribed payment date.
4.9.4. For practical purposes the 30 days (or other approved period) in which payment
must be made stops running when HSE notifies a supplier of a “dispute” in respect of an invoice.
4.9.5. The payment period starts to run again from the date the supplier provides the
information requested or amends the invoice etc.
4.9.6. Entries to the FIS must ensure that any periods, during which the payment terms period was suspended, while HSE awaited information or clarification from a supplier, are appropriately reflected to avoid an incorrect payment of late interest.
4.10. Pay Promptly anything not in dispute
4.10.1. Any goods or services that have been signed off as having been appropriately received should be paid for within the applicable payment terms.
4.10.2. Where part of an invoice is in order but an element of it is in dispute then only the element in dispute should be withheld from payment and the balance should be paid within the payment term.
4.11. Track and Report on Prompt Payment Interest Incurred Each Budget Holder must monitor and review instances of prompt payment interest for his/her area of responsibility and must:
i. Investigate any interest amount greater than €5.
ii. Investigate any payment that was more than 10 days late
iii. Review and amend arrangements to address any matters uncovered by these investigations
iv. Report monthly to the relevant Assistant National Director / Hospital Network Manager/ LHO or NHO Manager (band 4-5) as appropriate. on (1). to (3) above, copying in the relevant Assistant National Director of Finance.
v. Report on the overall monthly trend by late interest amount and days late for their areas of responsibility in such format as may be specified by the relevant Assistant National Director of Finance.
Health Service Executive National Financial Regulations
Ver 1.3 Page 62 of 176
GO TO NEXT CHAPTER …N/A….. GO TO LAST CHAPTER ON PAGE 56
5. CAPITAL PROJECTS and PROPERTY TRANSACTIONS
5.a Capital Projects below Appendix on page 124
5.b Property Transactions on page 65 Appendix on page 128
5a CAPITAL PROJECTS Capital Projects encompasses all construction, works, refurbishments, building fit-out, equipping etc funded from capital funds. Projects of a capital nature which are funded using non-capital monies (i.e. paid for out of revenue budgets) where the value of the project value is greater than € 500,000 must be treated as capital projects and dealt with in accordance with this financial regulation and the Capital Projects Approval Protocol (CPAP).
The requirements of the regulations are mandatory and must be adhered to in addition to the ‘Protocol for the Acquisition and Disposal of Property, mandatory’.
Capital Projects Approval Protocol Each Capital Project must be approved in accordance with the Capital Projects Approval Protocol (CPAP), with the support of the ‘Estates’/TSO function who also provide project administration, technical expertise and project management.
5.1. Capital Projects Approval Bands
The ‘Capital Projects Approval Protocol’ sets out the specific criteria and requirements with regard to approval and management of capital projects within the specified value bands. Projects are divided into four different Bands which have incremental requirements. The four bands are;
(A) Projects less than €500,000 (B) Projects between €500,000 and €5,000,000 (C) Projects between €5,000,000 and €20,000,000 (D) Projects greater € 20,000,000
Details of these requirements can be obtained from the Capital Projects Approval Protocol The current version of this protocol was included in the Capital Programme/Plan as approved by the Board and is attached at appendices on page 124. The Capital Programme/Plan is currently being reviewed by the HSE following feedback from the DOHC and the Capital Approval Protocol may be amended in that context.
October 2006
Health Service Executive National Financial Regulations
Ver 1.3 Page 63 of 176
5.2. Capital Projects; Financial Regulations
The general principles of the National Financial Regulations (such as balanced budgets, Sourcing options and Expenditure Approval, Receiving, Segregation of Duties) apply to all areas of Non pay spend including Capital Projects. Budget holders are responsible for proposing and selection of Capital Projects. Each Capital Project must be approved in accordance with the Capital Projects Approval Protocol (CPAP), with the support of the ‘Estates’/TSO function who also provide project administration, technical expertise and project management. The ‘Capital Projects Approval Protocol’N9 sets out the specific procedures to be followed in order to obtain approval for a Capital Projects, (refer to page124.), and establishment of related contracts/POs. 5.3. Capital Projects Approval and Contract Approval.
Capital Projects/works expenditure approval and Contract/PO is governed by CPAP approval procedures rather than those for general procurement. However, if there is any uncertainty or where expenditure is made before a project has been approved then the general rules should apply (see Table 2, on page 70). The Estates function is responsible for managing the approval of Capital Projects in accordance with four value thresholds (Bands) set out in the CPAP. They are also responsible for co-ordinating procurement of goods or services and putting in place a contract(s)/POs relating to that project i.e. sourcing, tender process and contract award. Procurement/Tendering and award of Contract or Purchase Order may, depending on the project value occur either as part of the Project authorisation process or after the Project has been autorised, e.g. Band A - minor capital projects are normally approved before expenditure approval/contract is made whereas Band C projects require Tender reports is incorporated into the project approval process.
Example 1. – a Capital Project value € 6m is approved in accordance with CPAP . The approval of the project by HSE corporate requires that the tender is approved by HSE corporate before the project is authorised. A letter of authorisation is then provided.
Example 2. – A Capital Project value €450,000 that had been included in the list of minor projects in the capital plan is submitted by service pillar and is vetted and approved by the local Estates office. A letter of authorisation is issued. The tendering process for this expenditure can then commence and the contract is awarded by the Estates function.
Unless formal notification has been provided then the project should not be considered approved.
Project funding is not available until the project has been approved in accordance with the protocol and that approval is then notified to the relevant project manager and project sponsor. Notification must be provided by the Finance directorate (National Director of Finance or relevant Assistant National Director of Finance).
5.4. Capital Projects; Main Requirements
Project Proposals
1. Each Capital project has to be fully appraised, evaluated, approved and notified.
N 9 This Capital Projects Approval Protocol was prepared by the Estates/TSO Directorate included in the 2006 Capital Plan submission for approval by the HSE board.
Health Service Executive National Financial Regulations
Ver 1.3 Page 64 of 176
2. The inclusion of a Capital Project in an approved Capital Programme/plan does not in itself signify that the project has been authorised.
Project approvals i.e. approvals to progress projects and eventually incur expenditure on same are needed for each individual project or group of projects and this requirement is separate to the capital plan.
3. Only fully costed Capital Project proposals are individually included in the approved budgeted Capital Programme/plan (Minor capital are grouped and totalled).
4. Any preliminary work carried out with regard to project evaluation or appraisal must
be agreed in advance by the budget holder. Project Approval and Authorisation to Commence
5. A Capital Project cannot be considered ‘approved’ and must not commence until formal notification of the project’s approval has been provided by the Finance Directorate.
6. All Capital funded projects and revenue funded capital projects with value greater
than € 0.5m are appraised, evaluated, and approved in accordance with the Capital Projects Approval Protocol. This process is managed under the Estates directorate.
7. The future recurring revenue cost and WTE impact of each Project must be validated
and signed off by the relevant Assistant National Director of Finance or their nominee. Projects must be approved in advance of a contract/order being awarded.
8. Tendering procedures (including EU procedures) must be complied with. 9. Capital Projects with a contract value greater than €10m must be approved by the
HSE board.
Project Management and Report
10. Project Cost ‘Variations’ must be approved in accordance with the ‘Capital Projects Approval Protocol’.
5.5. Controls within Capital Projects;
i) Segregation of Duties
Independent Project evaluation and Appraisal Certification of Work completed for construction contracts Budget holder within service, Project management in Estates directorate.
ii) Capital approval procedure
Specific Capital Projects approval procedures within predefined bands Full costing prepared, including future Revenue and Staffing commitments Cost Variation approval and reporting
iii) Sourcing of Goods/Services for Capital projects
Tendering Process Certification of Work completed for construction contracts
iv) Project Management Project Expenditure – monitoring and review Capital Programme/plan approval by senior management
Health Service Executive National Financial Regulations
Ver 1.3 Page 65 of 176
PROPERTY TRANSACTIONS;
Protocol for Acquisition and Disposal of Property
Property Transactions relate to the acquisition or disposal of Land and/or Buildings by the Health Service Executive. The ‘Protocol for Acquisition and Disposal of Property’
N10 (approved by HSE board March ’06) sets out the specific procedures to be followed in order to obtain approval for a transaction where the HSE acquires or disposes of any property (whether freehold or leasehold) or interest in property. The requirements of these regulations are mandatory and must be adhered to in addition to the ‘Protocol for the Acquisition and Disposal of Property, mandatory’. Property Protocol – Approval Thresholds
The ‘Protocol for Acquisition and Disposal of Property’ sets out the requirements with regard to obtaining approval within the specified value categories. Property transactions are divided into three different categories (based on their value) which have incremental requirements. The categories are;
(1) Property Transactions less than € 1,000,000
(2) Property Transactions between €1,000,000 and € 2,000,000 (3) Property Transactions greater than €2,000,000 The value of a transaction requiring approval is the total cost (for leases, value of lease is the annual rental costs by the number of years of lease) exclusive of Value Added Tax (VAT) and service charges. Authority to approve the acquisition or disposal of property has been delegated by the HSE board for transactions below € 2m. Property related transactions must be approved by the respective National Director of Service and Chief Executive (CEO approval if greater than €1m) or his/her delegated nominee. Formal notification of Approval for the acquisition or disposal of a property must be received before conclusion of negotiations can commence.
5.1. Property Transactions; Main Requirements
Property Transactions Proposals 1. The inclusion of a property related transaction in the approved Capital Programme/plan or
Revenue Budget does not in itself signify that the project has been authorised.
N 10 This protocol was prepared by a Property Operational Sub-Group which included Finance Directorate and Strategic Planning and Development under the lead role provided by the Estates/TSO function.
Health Service Executive National Financial Regulations
Ver 1.3 Page 66 of 176
Specific approval to progress property transactions and eventually incur expenditure are needed for each individual property transaction and this requirement is separate to the Capital plan/ Service plan .
2. Review by ‘Property Committee’ - each Property related project has to be fully appraised
and submitted to ‘The Property Committee’ N 11 for recommendation. Detailed requirement regarding completion of Business Proposal and Business Case, which may include technical and legal advice, are set out in the ‘Protocol for Acquisition and Disposal of Property’.
3. The future recurring revenue cost, confirmation of availability of funds and WTE impact of each property transaction proposed must be validated and signed off by the relevant Assistant National Director of Finance or their nominee.
Property Transaction Approval and Authorisation to Commence 4. A Property transaction cannot be considered ‘approved’ and any commitments must be
clearly flagged as “subject to formal HSE approval” until formal notification of the property transaction approval has been received.
5. Project approval is subject to ;
- Business case approved by Assistant National Director of related service - Review and recommendation of The Property Committee - Approval by National Service Directors,(endorse recommendation if greater than €1m) - Approval by CEO for values between €1m & €2m ( endorsement if greater than € 2m) - Approval by HSE Board for property transaction greater than €2m
6. All Property projects with value greater than € 2m are approved by the HSE Board.
7. Auction and Tendering procedures; refer to schedule IV of protocol. 8. Commitment should not be entered into until notification of approval of a Property
transaction must be received.
5.2. Controls for Property Transactions;
Segregation of Duties
Evaluation and recommendation by ‘Property Committee’ whose members are made up of functional and technical expertise
Expert Legal and technical support if required
Budget holder in function/service, project management in Estates directorate.
Capital approval procedure
Specific Property Transaction procedures within predefined categories based on value
Property Transactions funded from Capital Funds may require to be approved under the Capital Project Approval Protocol.
N 11 The property Committee is an executive group set up by the HSE. Their primary function is to appraise proposals with reference to the corporate, service and capital plans and to make recommendations regarding proposals. The committee is made up of nominee from the NHO (1 no.), PCCC (2no.), Nat Dir of Finance, Estates function (2 no.), in addition to Chairperson (appointed by CEO) and secretary (appointed by Estates Directorate/function).
Health Service Executive National Financial Regulations
Ver 1.3 Page 67 of 176
Management controls
Project Expenditure – monitoring and review
Level at which HSE board must approve is relatively low reflecting nature of projects
Property Transaction Protocol - Contents 1. Procedures for acquisition or disposal of Property or Interests in Property
2. Appendices; Schedule 1 Delegations
Schedule 2 Statutory provisions
Schedule 3. The Property Committee
Schedule 4 Summary of the Provisions of Part 5 of Code of Practice for
the Governance of State Bodies.
Schedule 5 Assessment of the potential or ongoing liabilities
Schedule 6 VAT on property transactions
Schedule 7 Stamp duty on property transactions
Health Service Executive National Financial Regulations
Ver 1.3 Page 68 of 176
APPENDICES
APPROVAL & SOURCING THRESHOLDS – Tables Table 1 Sourcing of Suppliers – Summary of Value Thresholds on page 69
Table 2 Expenditure Authorisation Thresholds on page 70
Table 3 - Types of Spend and Related Regulations/Protocol on page 73
ADDITIONAL INFORMATION
Re Chapter 1 General Provisions re. PTP on page 74 Re Chapter 2 Purchase to Pay (PTP) on page 76 Re Chapter 3 Tendering on page 95 Re Chapter 4 Non Order Payments – more information;
Taxi’s on page 103 Petty Cash Disbursements/Franking Machines on page 104 Utility Bills (Telecom/Eircom, ESB, etc) on page 110 Lease and Rental Requirements on page 111 Mobile Phones on page 114 Funding to ‘Not For Profit’ Organsiations/Grants on page 119
Re Chapter 5 Capital Projects & Property Transactions on page 124
Responsibilities by Grade – Extract Summarised on page 158 Links and References on page 170
Index (quick reference to find a topic) on page 171
Glossary – specific to terms in this document on page 176
The essential requirements of the financial regulations are contained within the main chapters. However, these should be read in conjunction with additional information contained within the respective appendices (listed above).
October 2006
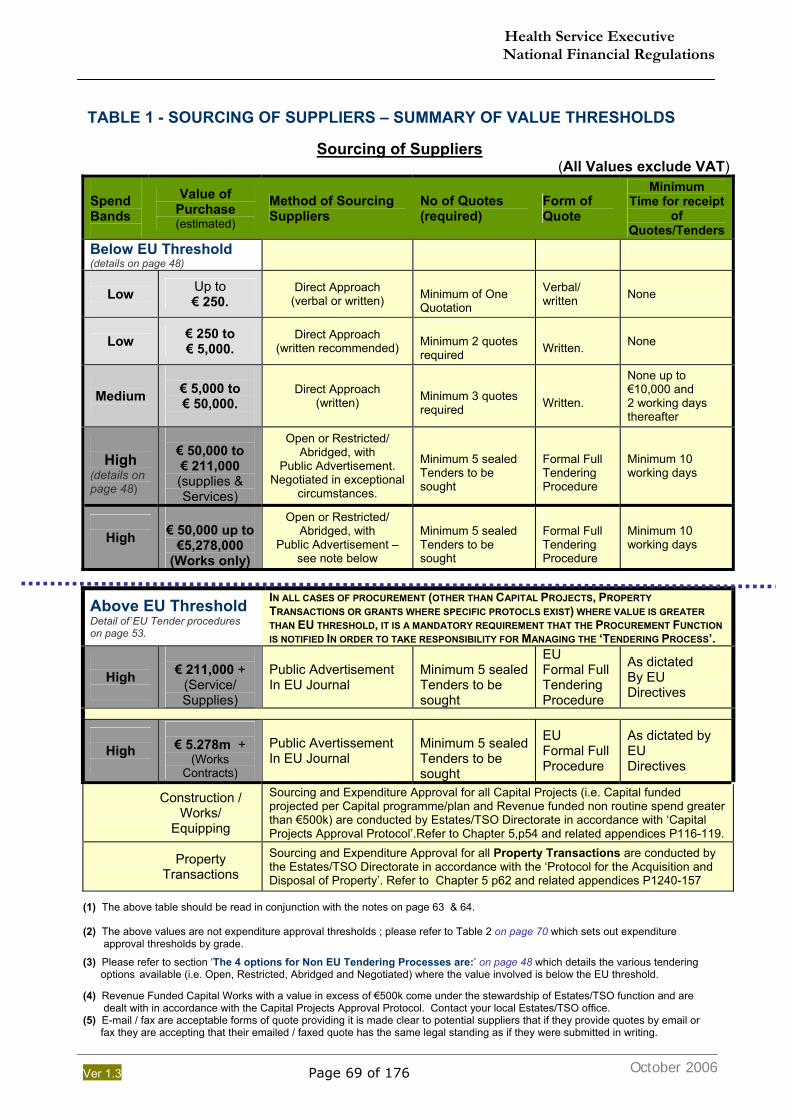
Health Service Executive National Financial Regulations
Ver 1.3 Page 69 of 176
TABLE 1 - SOURCING OF SUPPLIERS – SUMMARY OF VALUE THRESHOLDS
Sourcing of Suppliers (All Values exclude VAT)
Spend Bands
Value of Purchase (estimated)
Method of Sourcing Suppliers
No of Quotes (required)
Form of Quote
Minimum Time for receipt
of Quotes/Tenders
Below EU Threshold (details on page 48)
Low
Up to € 250.
Direct Approach (verbal or written)
Minimum of One Quotation
Verbal/ written None
Low € 250 to € 5,000.
Direct Approach (written recommended)
Minimum 2 quotes required
Written. None
Medium
€ 5,000 to € 50,000.
Direct Approach (written)
Minimum 3 quotes required
Written.
None up to €10,000 and 2 working days thereafter
High
(details on page 48)
€ 50,000 to € 211,000 (supplies & Services)
Open or Restricted/ Abridged, with
Public Advertisement. Negotiated in exceptional
circumstances.
Minimum 5 sealed Tenders to be sought
Formal Full Tendering Procedure
Minimum 10 working days
High
€ 50,000 up to
€5,278,000 (Works only)
Open or Restricted/ Abridged, with
Public Advertisement – see note below
Minimum 5 sealed Tenders to be sought
Formal Full Tendering Procedure
Minimum 10 working days
Above EU Threshold Detail of`EU Tender procedures on page 53.
IN ALL CASES OF PROCUREMENT (OTHER THAN CAPITAL PROJECTS, PROPERTY TRANSACTIONS OR GRANTS WHERE SPECIFIC PROTOCLS EXIST) WHERE VALUE IS GREATER THAN EU THRESHOLD, IT IS A MANDATORY REQUIREMENT THAT THE PROCUREMENT FUNCTION IS NOTIFIED IN ORDER TO TAKE RESPONSIBILITY FOR MANAGING THE ‘TENDERING PROCESS’.
High
€ 211,000 +
(Service/ Supplies)
Public Advertisement In EU Journal
Minimum 5 sealed Tenders to be sought
EU Formal Full Tendering Procedure
As dictated By EU Directives
High
€ 5.278m +
(Works Contracts)
Public Avertissement In EU Journal
Minimum 5 sealed Tenders to be sought
EU Formal Full Procedure
As dictated by EU Directives
Construction / Works/
Equipping
Sourcing and Expenditure Approval for all Capital Projects (i.e. Capital funded projected per Capital programme/plan and Revenue funded non routine spend greater than €500k) are conducted by Estates/TSO Directorate in accordance with ‘Capital Projects Approval Protocol’.Refer to Chapter 5,p54 and related appendices P116-119.
Property Transactions
Sourcing and Expenditure Approval for all Property Transactions are conducted by the Estates/TSO Directorate in accordance with the ‘Protocol for the Acquisition and Disposal of Property’. Refer to Chapter 5 p62 and related appendices P1240-157
(1) The above table should be read in conjunction with the notes on page 63 & 64. (2) The above values are not expenditure approval thresholds ; please refer to Table 2 on page 70 which sets out expenditure approval thresholds by grade.
(3) Please refer to section ‘The 4 options for Non EU Tendering Processes are:’ on page 48 which details the various tendering options available (i.e. Open, Restricted, Abridged and Negotiated) where the value involved is below the EU threshold. (4) Revenue Funded Capital Works with a value in excess of €500k come under the stewardship of Estates/TSO function and are dealt with in accordance with the Capital Projects Approval Protocol. Contact your local Estates/TSO office. (5) E-mail / fax are acceptable forms of quote providing it is made clear to potential suppliers that if they provide quotes by email or fax they are accepting that their emailed / faxed quote has the same legal standing as if they were submitted in writing.
October 2006
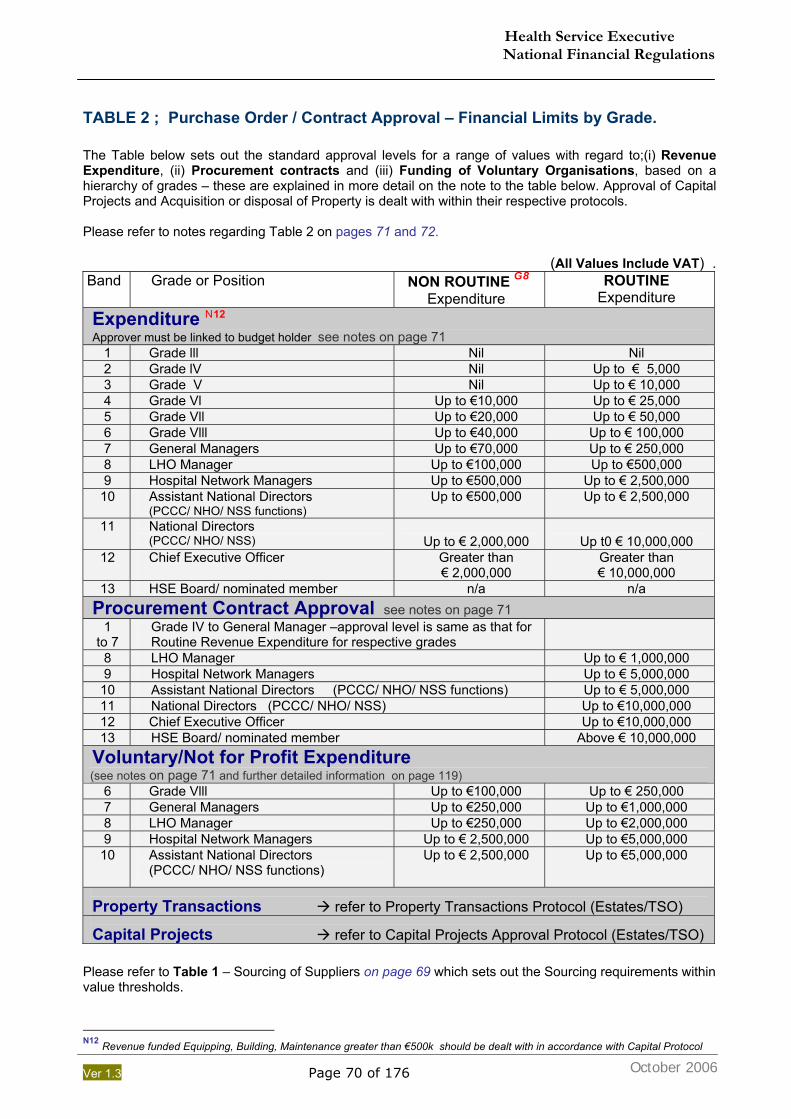
Health Service Executive National Financial Regulations
Ver 1.3 Page 70 of 176
TABLE 2 ; Purchase Order / Contract Approval – Financial Limits by Grade.
The Table below sets out the standard approval levels for a range of values with regard to;(i) Revenue Expenditure, (ii) Procurement contracts and (iii) Funding of Voluntary Organisations, based on a hierarchy of grades – these are explained in more detail on the note to the table below. Approval of Capital Projects and Acquisition or disposal of Property is dealt with within their respective protocols. Please refer to notes regarding Table 2 on pages 71 and 72.
(All Values Include VAT) . Band Grade or Position NON ROUTINE G8
Expenditure. ROUTINE
Expenditure Expenditure N12
Approver must be linked to budget holder see notes on page 71
1 Grade lll Nil Nil 2 Grade lV Nil Up to € 5,000 3 Grade V Nil Up to € 10,000 4 Grade Vl Up to €10,000 Up to € 25,000 5 Grade Vll Up to €20,000 Up to € 50,000 6 Grade Vlll Up to €40,000 Up to € 100,000 7 General Managers Up to €70,000 Up to € 250,000 8 LHO Manager Up to €100,000 Up to €500,000 9 Hospital Network Managers Up to €500,000 Up to € 2,500,000
10 Assistant National Directors (PCCC/ NHO/ NSS functions)
Up to €500,000 Up to € 2,500,000
11 National Directors (PCCC/ NHO/ NSS)
Up to € 2,000,000
Up t0 € 10,000,000
12 Chief Executive Officer
Greater than € 2,000,000
Greater than € 10,000,000
13 HSE Board/ nominated member n/a n/a Procurement Contract Approval see notes on page 71
1 to 7
Grade IV to General Manager –approval level is same as that for Routine Revenue Expenditure for respective grades
8 LHO Manager Up to € 1,000,000 9 Hospital Network Managers Up to € 5,000,000
10 Assistant National Directors (PCCC/ NHO/ NSS functions) Up to € 5,000,000 11 National Directors (PCCC/ NHO/ NSS) Up to €10,000,000 12 Chief Executive Officer Up to €10,000,000 13 HSE Board/ nominated member Above € 10,000,000
Voluntary/Not for Profit Expenditure (see notes on page 71 and further detailed information on page 119)
6 Grade Vlll Up to €100,000 Up to € 250,000 7 General Managers Up to €250,000 Up to €1,000,000 8 LHO Manager Up to €250,000 Up to €2,000,000 9 Hospital Network Managers Up to € 2,500,000 Up to €5,000,000
10 Assistant National Directors (PCCC/ NHO/ NSS functions)
Up to € 2,500,000 Up to €5,000,000
Property Transactions refer to Property Transactions Protocol (Estates/TSO)
Capital Projects refer to Capital Projects Approval Protocol (Estates/TSO)
Please refer to Table 1 – Sourcing of Suppliers on page 69 which sets out the Sourcing requirements within value thresholds.
N12 Revenue funded Equipping, Building, Maintenance greater than €500k should be dealt with in accordance with Capital Protocol
October 2006
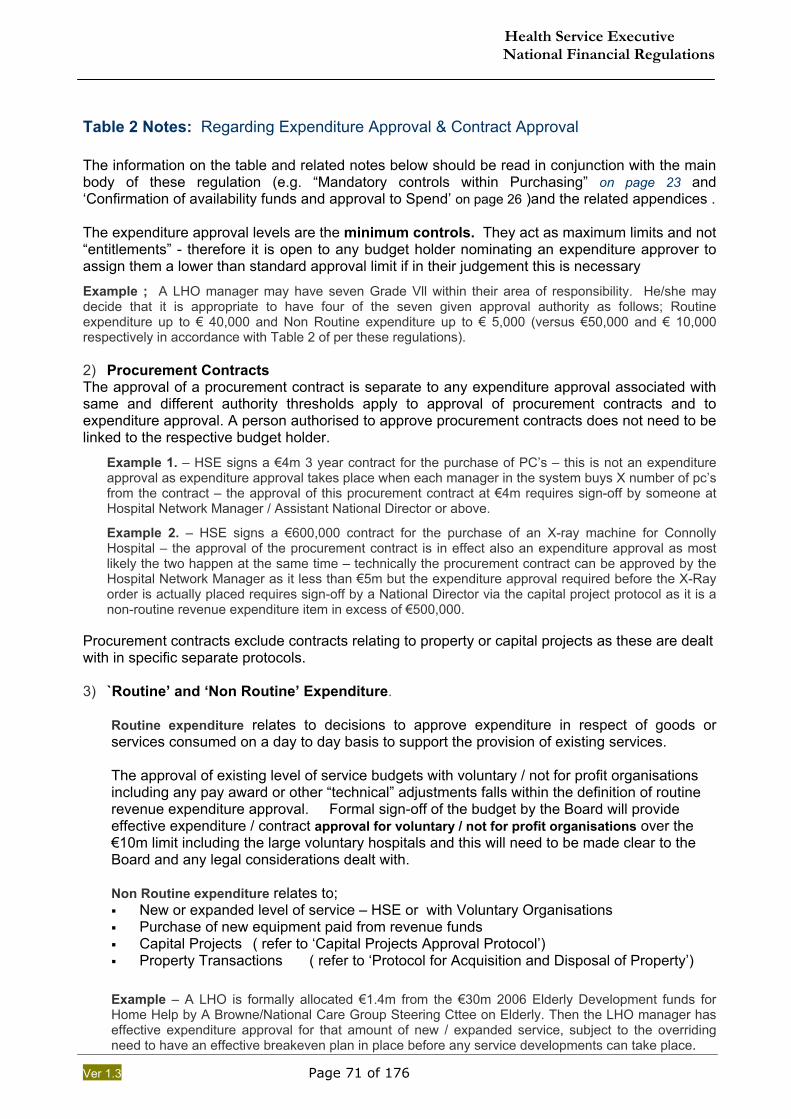
Health Service Executive National Financial Regulations
Ver 1.3 Page 71 of 176
Table 2 Notes: Regarding Expenditure Approval & Contract Approval The information on the table and related notes below should be read in conjunction with the main body of these regulation (e.g. “Mandatory controls within Purchasing” on page 23 and ‘Confirmation of availability funds and approval to Spend’ on page 26 )and the related appendices . The expenditure approval levels are the minimum controls. They act as maximum limits and not “entitlements” - therefore it is open to any budget holder nominating an expenditure approver to assign them a lower than standard approval limit if in their judgement this is necessary
Example ; A LHO manager may have seven Grade Vll within their area of responsibility. He/she may decide that it is appropriate to have four of the seven given approval authority as follows; Routine expenditure up to € 40,000 and Non Routine expenditure up to € 5,000 (versus €50,000 and € 10,000 respectively in accordance with Table 2 of per these regulations). 2) Procurement Contracts The approval of a procurement contract is separate to any expenditure approval associated with same and different authority thresholds apply to approval of procurement contracts and to expenditure approval. A person authorised to approve procurement contracts does not need to be linked to the respective budget holder.
Example 1. – HSE signs a €4m 3 year contract for the purchase of PC’s – this is not an expenditure approval as expenditure approval takes place when each manager in the system buys X number of pc’s from the contract – the approval of this procurement contract at €4m requires sign-off by someone at Hospital Network Manager / Assistant National Director or above.
Example 2. – HSE signs a €600,000 contract for the purchase of an X-ray machine for Connolly Hospital – the approval of the procurement contract is in effect also an expenditure approval as most likely the two happen at the same time – technically the procurement contract can be approved by the Hospital Network Manager as it less than €5m but the expenditure approval required before the X-Ray order is actually placed requires sign-off by a National Director via the capital project protocol as it is a non-routine revenue expenditure item in excess of €500,000.
Procurement contracts exclude contracts relating to property or capital projects as these are dealt with in specific separate protocols. 3) `Routine’ and ‘Non Routine’ Expenditure.
Routine expenditure relates to decisions to approve expenditure in respect of goods or services consumed on a day to day basis to support the provision of existing services. The approval of existing level of service budgets with voluntary / not for profit organisations including any pay award or other “technical” adjustments falls within the definition of routine revenue expenditure approval. Formal sign-off of the budget by the Board will provide effective expenditure / contract approval for voluntary / not for profit organisations over the €10m limit including the large voluntary hospitals and this will need to be made clear to the Board and any legal considerations dealt with. Non Routine expenditure relates to; New or expanded level of service – HSE or with Voluntary Organisations Purchase of new equipment paid from revenue funds Capital Projects ( refer to ‘Capital Projects Approval Protocol’) Property Transactions ( refer to ‘Protocol for Acquisition and Disposal of Property’)
Example – A LHO is formally allocated €1.4m from the €30m 2006 Elderly Development funds for Home Help by A Browne/National Care Group Steering Cttee on Elderly. Then the LHO manager has effective expenditure approval for that amount of new / expanded service, subject to the overriding need to have an effective breakeven plan in place before any service developments can take place.
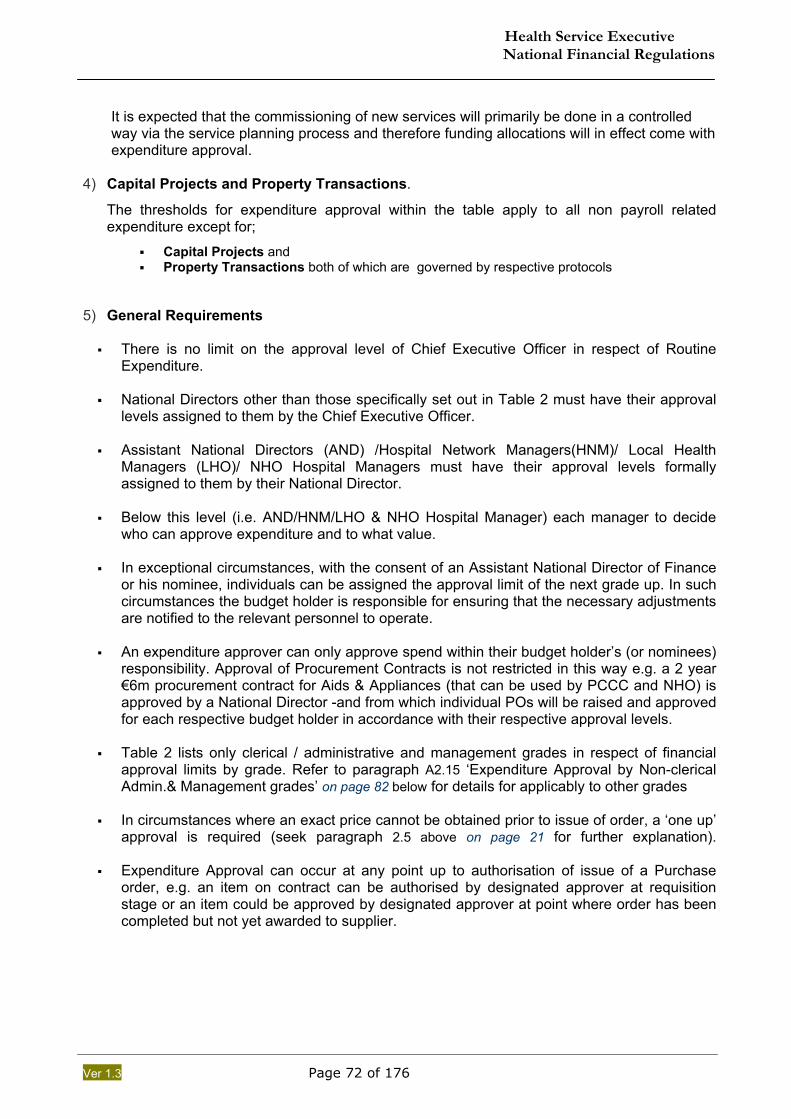
Health Service Executive National Financial Regulations
Ver 1.3 Page 72 of 176
It is expected that the commissioning of new services will primarily be done in a controlled way via the service planning process and therefore funding allocations will in effect come with expenditure approval.
4) Capital Projects and Property Transactions.
The thresholds for expenditure approval within the table apply to all non payroll related expenditure except for;
Capital Projects and Property Transactions both of which are governed by respective protocols
5) General Requirements There is no limit on the approval level of Chief Executive Officer in respect of Routine
Expenditure.
National Directors other than those specifically set out in Table 2 must have their approval levels assigned to them by the Chief Executive Officer.
Assistant National Directors (AND) /Hospital Network Managers(HNM)/ Local Health
Managers (LHO)/ NHO Hospital Managers must have their approval levels formally assigned to them by their National Director.
Below this level (i.e. AND/HNM/LHO & NHO Hospital Manager) each manager to decide
who can approve expenditure and to what value. In exceptional circumstances, with the consent of an Assistant National Director of Finance
or his nominee, individuals can be assigned the approval limit of the next grade up. In such circumstances the budget holder is responsible for ensuring that the necessary adjustments are notified to the relevant personnel to operate.
An expenditure approver can only approve spend within their budget holder’s (or nominees)
responsibility. Approval of Procurement Contracts is not restricted in this way e.g. a 2 year €6m procurement contract for Aids & Appliances (that can be used by PCCC and NHO) is approved by a National Director -and from which individual POs will be raised and approved for each respective budget holder in accordance with their respective approval levels.
Table 2 lists only clerical / administrative and management grades in respect of financial
approval limits by grade. Refer to paragraph A2.15 ‘Expenditure Approval by Non-clerical Admin.& Management grades’ on page 82 below for details for applicably to other grades
In circumstances where an exact price cannot be obtained prior to issue of order, a ‘one up’
approval is required (seek paragraph 2.5 above on page 21 for further explanation).
Expenditure Approval can occur at any point up to authorisation of issue of a Purchase order, e.g. an item on contract can be authorised by designated approver at requisition stage or an item could be approved by designated approver at point where order has been completed but not yet awarded to supplier.
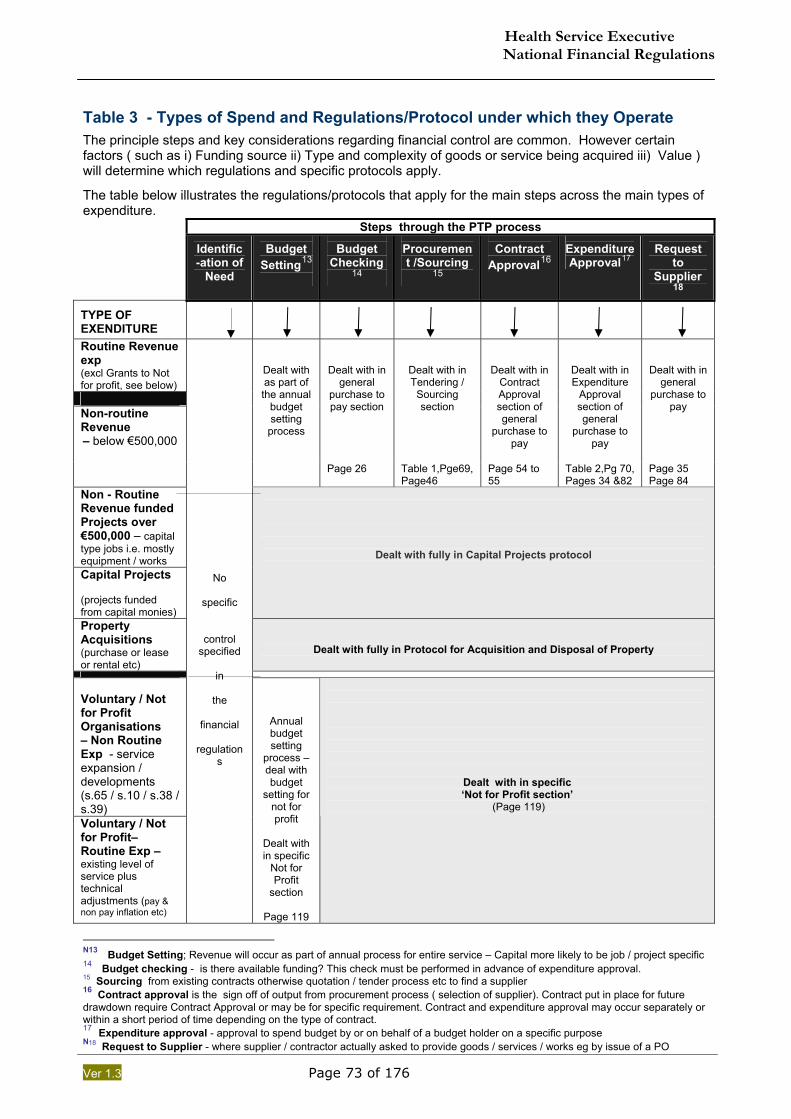
Health Service Executive National Financial Regulations
Ver 1.3 Page 73 of 176
Table 3 - Types of Spend and Regulations/Protocol under which they Operate
The principle steps and key considerations regarding financial control are common. However certain factors ( such as i) Funding source ii) Type and complexity of goods or service being acquired iii) Value ) will determine which regulations and specific protocols apply.
The table below illustrates the regulations/protocols that apply for the main steps across the main types of expenditure. Steps through the PTP process
Identific -ation of
Need
Budget Setting13
Budget Checking
14
Procurement /Sourcing
15
Contract Approval16
Expenditure Approval17
Request to
Supplier18
TYPE OF EXENDITURE
Routine Revenue exp (excl Grants to Not for profit, see below) Non-routine Revenue – below €500,000
Dealt with as part of the annual
budget setting
process
Dealt with in general
purchase to pay section
Dealt with in Tendering / Sourcing section
Dealt with in Contract Approval section of general
purchase to pay
Dealt with in Expenditure
Approval section of general
purchase to pay
Dealt with in general
purchase to pay
Page 26 Table 1,Pge69, Page46
Page 54 to 55
Table 2,Pg 70, Pages 34 &82
Page 35 Page 84
Non - Routine Revenue funded Projects over €500,000 – capital type jobs i.e. mostly equipment / works Capital Projects (projects funded from capital monies)
Dealt with fully in Capital Projects protocol
Property Acquisitions (purchase or lease or rental etc)
Dealt with fully in Protocol for Acquisition and Disposal of Property
Voluntary / Not for Profit Organisations – Non Routine Exp - service expansion / developments (s.65 / s.10 / s.38 / s.39) Voluntary / Not for Profit– Routine Exp – existing level of service plus technical adjustments (pay & non pay inflation etc)
No
specific
control specified
in
the
financial
regulations
Annual budget setting
process – deal with budget
setting for not for profit
Dealt with in specific
Not for Profit
section
Page 119
Dealt with in specific ‘Not for Profit section’
(Page 119)
N13 Budget Setting; Revenue will occur as part of annual process for entire service – Capital more likely to be job / project specific 14 Budget checking - is there available funding? This check must be performed in advance of expenditure approval. 15 Sourcing from existing contracts otherwise quotation / tender process etc to find a supplier 16 Contract approval is the sign off of output from procurement process ( selection of supplier). Contract put in place for future drawdown require Contract Approval or may be for specific requirement. Contract and expenditure approval may occur separately or within a short period of time depending on the type of contract. 17 Expenditure approval - approval to spend budget by or on behalf of a budget holder on a specific purpose N18 Request to Supplier - where supplier / contractor actually asked to provide goods / services / works eg by issue of a PO
Health Service Executive National Financial Regulations
Ver 1.3 Page 74 of 176
Related Chapter ; on page 12
Appendix ToC ; on page 68
Related Chapter; 1. General Provisions Regarding Financial Regulations
TOPIC ; Budget Holders – Additional Information Related section in main chapter on page 12
A1.1. Budget Holders – General Responsibility 1.1.1. The primary role in relation to ensuring compliance with all aspects of these Financial
Regulations rests personally with each and every Budget Holder. 1.1.2. In particular Budget Holders must ensure that they meet their obligation to operate within the
limits of the Budget is notified to them. 1.1.3. Budget Holders may for practical reasons delegate responsibility for aspects of compliance
with the Financial Regulations to other managers and staff who report to them.
1.1.4. Regardless of any such delegation Budget Holders remain personally responsible for ensuring that these regulations are fully complied with.
A1.2. Budget Holders – Responsibility to ensure compliance with these Financial
Regulations
Budget Holders must make formal Procedural Arrangements to ensure that each and every manager and staff member under their control:
Is fully aware of and understands the elements of these Financial Regulations relevant to them.
Is sufficiently knowledgeable and experienced to carry out their tasks in compliance with
the regulations. Receives the appropriate training and development to enable them to carry out their
tasks appropriately. Can comply with the segregation of duties specified by the Budget Holder
Carry out whatever levels of supervisory checks are deemed appropriate.
A1.3. Budget Holders – Responsibility to put in place specific arrangements
1.3.1. Each Budget Holder must document and put in place formal Procedural Arrangements in respect of the following:
Purchase to Pay (PTP) Billing and Income (Implementation in Phase 2) Banking and Cash (Implementation in Phase 2) Asset and Inventory Management (Implementation in Phase 2)
1.3.2. These documents must set out the specifics of how each of the above process areas is operationally managed in compliance with these Financial Regulations in each of the service areas covered by the Budget Holder.
Health Service Executive National Financial Regulations
Ver 1.3 Page 75 of 176
1.3.3. Matters to be covered in these documents include:
I. Details of managers’ sub-delegated authority as Budget Holders. II. Details of managers authorised in respect of:
▪ Purchase Order Authorisation ▪ Receipt of Goods and Services
III. Requisitioning and Purchase Order arrangements IV. Tender Process details; for example information regarding Appointment of ‘User
Groups’/technical evaluators (in conjunction with Procurement) where required as part of the Tender Process.
V. Commercial Evaluators. (requirements on page 24) VI. Initial Receipt and Custody procedures at each location. VII. Tendering Procedures, including co-ordination by the Procurement function. VIII. Income, Banking and Cash Procedures. IX. Debt management and Debt collection arrangements. X. Patients’ Private Property administration. XI. Other topics that require specific mention due to their nature (e.g. mobile phones).
A1.4. Budget Holder’s responsibility to mitigate control deficits in compliance with the
Financial Regulations
1.4.1. Each Budget Holder must put in place additional measures to mitigate any deficits in the ability of their managers and staff to fully comply with these regulations.
1.4.2. Deficits identified and the additional mitigation measures put in place must be notified to the
relevant Assistant National Director and to the relevant Assistant National Director of Finance.
A1.5. Budget Holders responsibility to make efficient use of resources
In recognising our overriding objective of providing health and personal social service to our clients within available resources it is the responsibility of every Budget Holder to ensure that full advantage is taken of all opportunities to;
Share administrative workloads and resources
Streamline processes
Utilise available technology
In order to ensure that the minimum of available staff resource is required to ensure compliance with these Financial Regulations.
A1.6. Written Decision to Record Approval of a Manager as a Budget Holder
1.6.1. The approval of a manager as a Budget Holder represents a formal delegation of responsibility in respect of expenditure and income for a defined service or area.
o The approval of Budget Holders must be recorded by way of formal written
decision.
o Staff members appointed formally to act in place of Budget Holders carry all the responsibility and authority of the post including that of Budget Holder.
o Any exceptions to this general rule i.e. where for some reason a manager is
only being given part of the authority and responsibility for a post he is acting in must be notified to the relevant Assistant National Director of Finance.
A1.7. A list of all approved Budget Holders below those deemed to be budget holders must be
maintained by those nominating and copied to the relevant Assistant National Director of Finance on a quarterly basis.
A1.8. This list must be reviewed and updated at least annually.
These areas will be included in phase ll of the development of the National Financial
Health Service Executive National Financial Regulations
Ver 1.3 Page 76 of 176
Related Chapter; (2) PURCHASE TO PAY (General)
Related Chapter ; Page 19
Appendix ToC ; on page 68
The following is additional information set out by ‘Topic’ heading which relates to Chapter 2. PURCHASING Page TOPIC 1 ; Sourcing of Goods/Services - More information (2d iv) 77 TOPIC 2 - STORES ; Requisitioning of Stock and Receipt from Stores 78
` TOPIC 3: Expenditure Approval - More information (2d VI) ` 82
TOPIC 4: Requirement of Purchase Order - More information (2d VI) 84 TOPIC 5: Outstanding and Incomplete Orders 85 TOPIC 6: Manual Purchase Orders 86
TOPIC 7: Documented Purchasing Arrangements 87
TOPIC 8; Supplier Approval , Categorisation, Performance Management 88 RECEIVING PROCESS TOPIC 9: Receiving Goods or Services - More information 89
PAYMENT PROCESS
TOPIC 10: Supplier Payment Remittance & Supplier Reconciliation 92
TOPIC 11: Invoice Matching Tolerances – More information 94
Health Service Executive National Financial Regulations
Ver 1.3 Page 77 of 176
Related Chapter ; on page 19
TOPIC 1; Sourcing of Goods/Services - More information (2d iv) Related Section ; Page 28
A2.1. Sourcing Options in Exceptional Circumstances
In exceptional circumstances the sourcing options relevant to the value thresholds above may not apply or may not apply fully. These circumstances include:
2.1.1. Extreme Urgency – where necessary to avoid,
(2.1.1). .1. Significant risk to persons (2.1.1). .2. Significant risk to property (2.1.1). .3. Significant financial loss to the HSE.
It is very important to be aware that the circumstances giving rise to the “Urgency” must have been unforeseeable and should not have arisen due to lack of planning or action on the part of the HSE.
2.1.2. Proprietary Materials – the goods or services are available from only one source (to be
periodically market tested, at least annually)
2.1.3. Additional Deliveries – items previously sourced in compliance with the normal requirements if a change of supplier would result in incompatibility or disproportionate technical difficulties.
2.1.4. Bargain Purchases – or purchases under particularly advantageous conditions e.g.
liquidation sale etc.
2.1.5. Confidential Contracts – which required to be placed as such due to particular sensitivity or special strategic importance to the HSE.
2.1.6. Statutory Type Purchases – items of expenditure such as commercial rates, water charges,
Planning permissions etc.
2.1.7. Capital Project approved under the Capital Programme/Plan where an urgent requirement has been identified and justified.
In all cases the Assistant National Director / Hospital Network Manager must approve in writing the application, co-signed by the relevant Assistant National Director of Finance e.g. exceptional circumstances criteria. The Head of Procurement must be notified of such instances.
Health Service Executive National Financial Regulations
Ver 1.3 Page 78 of 176
Related Chapter ; on page 19 GO TO TOP OF APPENDIX - ON PAGE 76
TOPIC 2 - STORES ; Requisitioning of Stock and Receipt from Stores
(Includes Pharmacy Stock and Sterile Supplies)
[ref. on page 28] A2.2. General
The general principles of the ‘Purchase to Pay’ process apply to requisitioning and receipt from stock unless indicated otherwise in this section. This section is intended to address any issues or challenges that may arise in the application of the standard ‘Purchase to Pay’ regulations to this area.
These regulations use the generic term “Stores” to refer to locations where stock is held for issue to services and this term is taken to cover:
o General Stores / warehouses o Maintenance / Engineering Stores o Pharmacy o Sterile Stores (CSSD) o Any other storage location which holds stock
A2.3. “Purchasing from Stock” - Requisitioning of Stock from a Store (Warehouse or
other storage location)
As indicated in Section 2d the generic elements of the purchasing process are as follows: (i.) Identification and notification of need - will still take place albeit in a more routine
process and may be automated by using standard re-order levels etc. (ii.) Confirmation of availability of funds and approval to spend.
Approval to spend for Store items is exercised by the person who approves the requisition (the requisition document in effect replaces the purchase order).
(iii.) Sourcing of supplier(s) to provide goods or services . The sourcing of suppliers
and ordering from them becomes a matter for the stores staff. (iv.) Formal request issued to supplier to provide goods
A2.4. Segregation of Duties
2.4.1. The segregation requirements listed on page 23 above in respect of purchasing apply to the ordering of goods by stores staff and receiving the goods into stock in the store.
2.4.2. Once the goods are in stock and ready to issue, the controls inherent in this segregation have
already been largely complied with.
2.4.3. Accordingly, the segregation of duties required in respect of requisitioning of goods from a stores, is that a person must not approve a requisition that contains goods for his/her own day to day use.
2.4.4. The segregation of duties required in respect of receipt of goods from stores is that the person
who signs off on the requisition should not be responsible for checking and confirming that the goods received match the requisition and are in good order.
A2.5. Requirement for Documented Arrangement for Stores [ref 2.25.5 on page 87 ]
Health Service Executive National Financial Regulations
Ver 1.3 Page 79 of 176
A2.6. Main differences between “Requisitioning from stock” and “normal purchasing”
2.6.1. Stock items refer to goods only and not services or works 2.6.2. In general terms, items held in stock in a store, warehouse or other storage location may be of
a more routine nature than may be the case with purchasing direct from a supplier. 2.6.3. Goods held in stock will generally be in the low to medium value range. 2.6.4. The stores’ staff are responsible for dealing with third party suppliers and will generally place
orders to meet the overall needs of the services/locations which are supplied.
A2.7. Mandatory requirements for ordering / requisitioning from stores.
2.7.1. It is a mandatory requirement that the manager signing off on a must be in accordance with the financial limits set out in Table 2 on page 70.
2.7.2. With regard to approval by other grades of staff outside the clerical administrative /
management stream refer to provisions set out on page 82 2.7.3. It is a matter for Budget Holders to specify which staff /grades may make a requisition from the
stores that supply their area and to set any restrictions that may apply. 2.7.4. Such restrictions may apply to certain goods or categories of goods where, for example, the
store stocks high value items such as surgical implants. 2.7.5. A higher grade of staff may be required to approve such non-routine or higher value goods. 2.7.6. A practical approach will be necessary for Budget Holders when identifying and documenting
what staff or grades of staff may approve requisitions from stores. 2.7.7. The staff member approving the requisition must satisfy themselves that the need is
appropriate and that the budget is available to cover the cost of what is being requisitioned. 2.7.8. Requisition forms should be numbered and in triplicate.
o numbered unique and part of a numbering sequence
o filed for future reference and audit
o circulated as follows:
Original for stores.
1 copy for staff member due to receive the goods.
1 copy to be retained.
2.7.9. Requisitioning from Stores - staff requisitioning from stores should do so using a standard template that clearly records:
o Location / Service requisitioning the goods
o Date of requisition
o Description of goods
o Quantity of goods
o Whether for collection or delivery
o Delivery address, date, preferred time(s) and contact
o Name of person requisition prepared by, date prepared & contact details
o Name of person requisition has been approved by and date
o Key contact for requisition if not one of the above
Health Service Executive National Financial Regulations
Ver 1.3 Page 80 of 176
A2.8. Use of Central Contracts is mandatory where they are in place.
2.8.1. The mandatory requirement to utilise centrally negotiated contracts wherever they are in place applies to stores managers and their staff in terms of the replenishment of their stock by purchasing from suppliers.
2.8.2. In general terms, items are held in stock in a store because there is a readily apparent and continuous need for them.
2.8.3. On that basis there is an expectation that the majority of items held in every stores area will
generally be acquired via centrally negotiated contracts.
A2.9. Splitting of Requisitions is prohibited
Requisitions must not be split for the purposes of avoiding the correct application of approval thresholds in these regulations.
A2.10. Approval of New Items to be held by Stores
2.10.1. Where new products are being added to the list of items held in a store, regard must be had to any financial implications that may arise.
2.10.2. It is the responsibility of the stores manager to notify the relevant Budget Holder(s) or their
nominees, in advance of, or as soon as possible after, the introduction of any products that will have a material impact on costs.
2.10.3. Each Budget Holder should receive a report from the stores in their area (at least every two
months) detailing: a) New products added that month to the list of normal stores items b) Unit costs of new products c) Costs of products they have replaced if relevant d) Expected monthly order quantity and cost of new products
RECEIVING GOODS FROM STORES
General Applicability of Purchase to Pay Receiving regulations
The requirements of the normal receiving process as set on page 39 and on page 89 also 2apply to ‘receiving’ from stores, unless otherwise provided.
A2.11. Main requirements for receiving goods from stores
The mandatory requirements centre around;
2.11.1. Initial receipt and safe custody of deliveries/collections from stores – this is a key priority and must be appropriately planned for and implemented.
2.11.2. Receipt of appropriate stores issue documentation (equivalent of “Proof of Delivery” in
standard Purchase to Pay process) 2.11.3. Checking of goods received for match to stores issue documentation and original requisition 2.11.4. Early notification and resolution of any discrepancies between what was requisitioned and
what was received. 2.11.5. Proper record keeping and follow up on any of the discrepancies referred to at 4. above
Health Service Executive National Financial Regulations
Ver 1.3 Page 81 of 176
A2.12. Importance of Stores Issue Documentation that clearly references the original requisition
2.12.1. Stores Issues - Mandatory requirements;
It is the responsibility of the stores manager to ensure that every collection or delivery is accompanied by the appropriate stores issue documentation that clearly shows:
(i.) What goods are being issued from stores and (ii.) The quantity and value of those goods (iii.) Clearly references each item to the relevant requisition document
2.12.2. The stores manager must ensure that at time of issue or as soon as possible thereafter that
the requisitioner is ;
o Notified of any goods on the requisition not included in the current stores issue,
o Advised as to possible alternatives or date when will be available etc.
A2.13. Checking of expenditure relating to ‘Stores issues’ on Financial Information
System / Accounting System.
2.13.1. Budget Holders and their staff must be in a position to monitor expenditure including expenditure incurred via stores.
2.13.2. It is a mandatory requirement that the level of expenditure recorded as stock issues can be
reconciled by the Budget Holder to his/her records of stock requisitioned and received.
2.13.3. Stores issues recorded on the Financial Information System/ Accounting system against cost centres or Internal Orders (Capital cost centres) must incorporate the requisition number or equivalent.
2.13.4. Appropriate monthly summary and detail reports must be available to and reviewed by Budget
Holders showing stock items issued to them by:
Cost centre / internal order Stock type or category Value Store / storage location
This is to facilitate efficient tracking by Budget Holders of expenditure back to the original requisition.
2.13.5. Stores managers must ensure procedures are in place to facilitate this requirement.
A2.14. Recording and resolving non fulfilled requisitions
2.14.1. The stores manager and the person(s) approving requisitions must ensure that records are kept of outstanding or part outstanding requisitions i.e. where some or all of the goods on a requisition have not yet been issued.
2.14.2. On a monthly basis requisitions outstanding for more than 2 months must be reviewed and closed by both the person approving the requisition and the stores manager.
Co-operation between stores and requisitioning staff is required to enable this process to operate efficiently.
Health Service Executive National Financial Regulations
Ver 1.3 Page 82 of 176
Related Chapter ; on page 19
GO TO TOP OF APPENDIX - ON PAGE 76
TOPIC 3: Expenditure Approval - More information (2d VI)
Related Section; on page 34 Related Table; on page 70
A2.15. Expenditure Approval by Non-Clerical Administrative and Management Grades
Government and Health Service policy promotes the engaging of clinicians more fully in all aspects of the formal management of the health services they deliver. These regulations require:
2.15.1. The formal identification and approval of managers who are being delegated authority as
Budget Holders and also, 2.15.2. The formal documentation by Budget Holders of the key elements of the purchasing
arrangements in force within their areas of responsibility. 2.15.3. In the context of 1. and 2. above there is scope to formally approve non clerical / administrative
or management grades as both Budget Holders and expenditure approvers.
2.15.4. Given the diversity of such grades within the health service it is not proposed to prescribe equivalents to each of the grades listed in the Financial Limits by Grade table above.
2.15.5. Approval of Budget Holders and Expenditure Approval [refer to page 12 & 74 ]
Approval of all Budget Holders by ‘Deemed’ Budget Holders (paragraph 1.10 on page 14) and takes effect when notified to the relevant Assistant National Director of Finance.
2.15.6. There is a need to strike an appropriate balance between:
i. The need to deepen the general management and financial management involvement of
staff in grades outside the clerical / administrative and management stream,
and
ii. the requirement to have appropriately trained and experienced staff with sufficient knowledge and understanding to maintain a high level of internal control.
It remains the responsibility of the Budget Holder member making the delegation to take all steps necessary to oversee that any person they delegate responsibility to as a budget holder complies with requirement of such delegation.
This is particularly important with regards to managing within available budget and full compliance with these regulations.
A2.16. Requirement for Written Decisions for Expenditure Approval – Use of FIS (Expenditure Approval on Financial Information System/Accounting system by Nominees)
2.16.1. Whenever practical the aim should be to facilitate the streamlining of the expenditure approval
process without any reduction in financial control. This aim can be achieved by ensuring that managers approving the issue of purchase orders / contracts e.g. do so using the system directly.
2.16.2. The above assumes that managers, including the most senior managers whose approval is
required in respect of higher value amounts, are in a position to utilise the FIS to approve purchase orders.
Health Service Executive National Financial Regulations
Ver 1.3 Page 83 of 176
2.16.3. In the event that certain managers do not utilise System directly, then they must nominate a manager(s), at Grade VI or above, to implement on the System their decisions to approve expenditure.
2.16.4. The nominated manager will be responsible for approving the necessary purchase orders
within the Financial Information System (FIS)/Accounting System to give effect to the senior manager’s decision.
2.16.5. It is good practice to nominate a substitute to address any absences by the nominated person.
2.16.6. A decision to nominate a manager (applies to NHO/LHO managers or above) and any
substitutes in this context must be given in writing and recorded along with the other written decisions of that senior manager.
2.16.7. The relevant Assistant National Director of Finance must be notified of all managers
nominated in this way and the Budget Holder for the area must ensure that all such nominations are reviewed at least annually.
A2.17. Formal Written decisions approving expenditure greater than €50,000 – minimum requirements.
Each written decision that approves expenditure must: 2.17.1. Be sequentially numbered with a sequence that identifies both the senior manager signing off
on the decision and the year. 2.17.2. Be dated.
2.17.3. Set out a synopsis of, or refer to documents outlining, details of the ‘need’ that is being
addressed.
2.17.4. Set out a synopsis of, or refer to documents (preferably attached) outlining details of the procurement options followed to source the goods / services and the recommended supplier(s).
2.17.5. Identify or refer to documents identifying quantity, specification, price, time period and any
other relevant details.
2.17.6. Specify total expenditure being approved (showing VAT exclusive, VAT and VAT inclusive amounts) and periods over which expenditure will be incurred.
2.17.7. Be specific as to funding source in place to cover the expenditure. 2.17.8. Detail cost centre(s) and cost element(s) that charges are to be made against (or refer to
appropriate documents for same).
2.17.9. Be recommended by a manager of at least grade V level who is not the manager approving the decision.
2.17.10. Be signed by a manager with the authority to expend the amount in question.
2.17.11. Be summarised in an electronic format list as specified by the HSE National Director of
Finance. Updated copies of this list to be forwarded each month before the third working day of the following month to the relevant National Management Team Member and the relevant Assistant National Director of Finance.
Health Service Executive National Financial Regulations
Ver 1.3 Page 84 of 176
GO TO TOP OF APPENDIX - ON PAGE 76 TOPIC 4: Requirement of Purchase Order - More information (2d VI)
Related Section; Page 36 Sample Purchase Ordered Page 164
A2.18. Purpose of a Purchase Order
Ref to main section ‘End of Purchasing Stage’ on page 34 and also ‘Requirement for written Decisions’ on page 82 in this appendix. The purchase order serves a number of purposes including:
2.18.1. Providing a clear request to the supplier with all the necessary details to assist them in
meeting HSE requirements and for future reference.
2.18.2. Forming part of documentation of the legal contract between the HSE as purchaser and the supplier.
2.18.3. Establishing a control whereby purchase orders should not be issued until expenditure is
approved following confirmation of budget availability.
2.18.4. Establishing a reference point for the purpose of accurate accounting where commitments can be recorded and later the expenditure and liability (accrual) when goods are received.
2.18.5. Providing a permanent record for the HSE of what was ordered to facilitate;
Notification of receipting location for delivery Checking or what was delivered against what was ordered Checking of invoice against what was ordered Checking in case of later dispute Checking price agreed at time of order with subsequent invoice
A2.19. Who needs to get copies of Purchase Orders. Once approved, purchase orders must be issued immediately to:
i) The supplier.
ii) The person(s) expected to receive the goods/services.
iii) The person responsible for approving the expenditure i.e. approving the issue of the order or his/her nominee.
It is a mandatory requirement that purchase orders are physically issued to (i). to (iii) above unless approval of the relevant Assistant National Director of Finance (or his/her nominee) has been obtained.
A2.20. Key items for inclusion on purchase orders / contracts Refer to a sample Purchase Order on page 164 . These regulations require that the purchase order or contract must contain, or refer to accompanying documents that contain, sufficient detail to enable the supplier to fully understand and comply with the needs of the HSE.
Each purchase order / contract must include the following:
i) Unique sequential printed order number or equivalent
ii) Name, address and Supplier account Number (Vendor Number) or selected supplier
iii) Description, quantity of Goods or services
Health Service Executive National Financial Regulations
Ver 1.3 Page 85 of 176
iv) Price (showing VAT Exclusive, VAT and VAT Inclusive)
v) Address for delivery of goods or services.
vi) Address for submission of invoice or equivalent.
vii) Address for submission of supplier statements.
viii) Any necessary time constraints around delivery.
ix) Summary of standard HSE payment terms.
x) Date
xi) Material Code / account code
GO TO TOP OF CHAPTER ON PAGE 76 TOPIC 5: Management of Outstanding and Incomplete Orders
A2.21. Monitoring of Purchase Orders not fulfilled
2.21.1. It is a mandatory requirement that officers responsible for approving purchase orders ensure that they monitor purchase orders that have yet to be fulfilled by the supplier i.e. where some or all of the goods or services have yet to be received.
2.21.2. Each month a list of any purchase orders that remains open for more than 3 months must be
prepared.
2.21.3. The purchase orders listed must be investigated and closed by receipting goods against it or cancelled if it will not be fulfilled.
2.21.4. If there is a valid reason to keep open any such purchase order then this reason must be
recorded against it. A summary of the outcome of this monthly review exercise must be sent by each location to the relevant Assistant National Director of Finance or his/her nominee(s).
A2.22. Monitoring of Purchase Orders fulfilled but not invoiced (GRINR)
Goods Received Invoice Not Received (GRINR).
2.22.1. Once a goods receipt note is inputted into the Finanical Information System (FIS) against a purchase order, the expenditure for those goods or services is recorded against the relevant Budget Holders cost centre or internal order.
2.22.2. The Goods received transaction will automatically be accrued to the GRINR account in the
FIS, until such time as the invoice is received and matched against the Purchase order. 2.22.3. It is important to realise that this incurring of expenditure occurs and therefore must be
recorded, in most cases, before the invoice is received. 2.22.4. It is a mandatory requirement that purchase orders for which goods have been receipted but
for which no invoice has yet been received are monitored closely. 2.22.5. A high level of purchase orders that have been goods receipted for a long period i.e. longer
than 3 months without receipt of an invoice may indicate that there are duplicate purchase orders and GRN’s in the system and therefore duplicate expenditure.
2.22.6. Alternatively, it may indicate that there are issues with the invoice receipt and matching
process that could cause prompt payment or cash flow issues when the invoices are eventually matched for payment.
Health Service Executive National Financial Regulations
Ver 1.3 Page 86 of 176
2.22.7. Each month a list of any purchase order that has been goods receipted but not matched to an invoice for more than 3 months must be prepared and compared to the GRINR control account on the Financial Information System.
2.22.8. This list must be investigated and the items on it cleared. 2.22.9. If there is a valid reason to keep open any such item then this reason must be recorded
against it. 2.22.10. A summary of the outcome of this monthly review exercise must be sent by each location to
the relevant Assistant National Director of Finance or his/her nominee (s).
GO TO TOP OF CHAPTER ON PAGE 76 TOPIC 6: Manual Purchase Orders
The issue of a manual purchase order is covered by the same Financial Regulations as set out in sections 2a to 2d on Purchasing (pages 19 to 46 ).
A2.23. The written approval of the relevant Assistant National Director of Finance or nominee is required for
inclusion on the list of service areas/locations eligible for a manual purchase order book.
2.23.1. The list of service areas / locations eligible for inclusion on the list for manual purchase order books must be reviewed at least annually and re-approved if appropriate by the relevant Assistant National Director of Finance.
2.23.2. Within 3 months of the coming into force of these regulations each Budget Holder must
prepare a report detailing each of the locations within his/her area of responsibility that utilise manual purchase orders and must detail:
2.23.3. Number of service areas / locations using manual purchase order books in his/her areas of
responsibility
2.23.4. Approximate number and value of manual purchase orders issued per service area / location.
2.23.5. Reasons for the use of manual purchase orders in each service area / location. A2.24. Manual Purchase Order books should only be supplied in respect of service areas / locations
that; 2.24.1. do not have access to FIS generated purchase orders. 2.24.2. cannot issue FIS purchase orders for certain Goods/services that require a purchase order.
2.24.3. The issue of manual purchase order books must be centrally controlled by or on behalf of
each of the Assistant National Directors of Finance with a permanent record retained of ; (1) Which Budget Holder, service and location are issued Order books (2) Date of issue of manual order book (3) Names and signatures of person issuing and collecting order books. (4) First and last order number in each book issued. (5) Any restrictions on the use of the manual purchase orders
2.24.4. The minimum information to appear on any manual purchase order, including the requirement
for unique sequential numbering, is the same as for a FIS generated purchase order as set out in detail in section 2d on page 22.
2.24.5. Within 12 months of the coming into force of these regulations each Budget Holder must
review and report to the relevant Assistant National Director of Finance as to plans identified to eliminate the use of manual purchase orders.
2.24.6. It is a requirement that the use of manual purchase orders is phased out as soon as practical.
GO TO TOP OF CHAPTER ON PAGE 76
Health Service Executive National Financial Regulations
Ver 1.3 Page 87 of 176
TOPIC 7: Documented Purchasing Arrangements - More information
Related Section; on page 22
A2.25. Formal Documented Purchasing Arrangements for Managers and Users
Budget Holders should set out, for each location/main element of spend, who and how/when points 1 to 4 on page 22 are dealt with.
2.25.1. Identify Need, Who can validly confirm need
Who makes decision on that need
Form of communication, by who and to whom
2.25.2. Confirm Available funds and approval to Spend. Who does what
How is confirmation and approval done
What is process if there is no approval
Who approves spend
2.25.3. Source Supplier Communication of information regarding centralised contracts
What are local arrangements for non contract items and encourage HSE standard procedures, where appropriate
How and who makes contact with suppliers
2.25.4. Issuing of Purchase Orders/ Contracts How are purchase orders generated, approved & sent to vendor
How are contracts are drawn down ,received
Who handles and/or approves invoices
Where Public Capital Funding to ‘Not for Profit’ agencies is provided there is a requirement for the HSE to ensure a lien is made on the asset created (Securing the State’s Interests).
Procedures documented under Capital Section are likely to apply to works, specialist services and equipping.
2.25.5. Stores ; Specific Arrangements for Stores Related Section; on page 78 Within the required formal documented arrangements relating to the operation of the purchase to pay process, each Budget Holder must specifically address the following in relation to requisitioning from stores:
(i.) Which managers (a) may approve stores requisitions, and (b) to what value, setting out any conditions to apply regarding high value goods or non- routine goods etc
(ii.) Process for approval of new products to be held in stores.
(iii.) Monitoring and review arrangements in respect of requisitions from stores.
A2.26. Details of Purchasing arrangements must be reviewed at least quarterly to reflect any changes, and
communicated to all staff involved in the purchase to pay process.
Health Service Executive National Financial Regulations
Ver 1.3 Page 88 of 176
Related Chapter ; on page 19 GO TO TOP OF APPENDIX - ON PAGE 76
TOPIC 8; Supplier Approval , Categorisation, Performance Management (2d iv)
A2.27. Supplier Approval It is a mandatory requirement of these regulations that suppliers are appropriately selected and managed. This is to ensure that HSE utilises, on a continuing basis, only suppliers that provide a consistently high performance in meeting HSE requirements around provision of goods and services.
2.27.1. Performance by suppliers in this area includes facilitating compliance with these regulations by provision of appropriate documentation, responding to queries and related activities.
2.27.2. Any suppliers selected must comply with whatever supplier selection and approval criteria are
in force from time to time within HSE. 2.27.3. Only suppliers (also known as Vendors ) that meet any such criteria should be listed for set up
on the FIS.
A2.28. Supplier Categorisation & Development The scale of the HSE is such that there is a requirement to ensure that a broad base of competitive potential suppliers is available at all times in respect of key purchasing areas.
2.28.1. Budget Holders, and particularly those acting on their behalf in terms of providing procurement
support and advice must ensure that all reasonable steps are taken meet this requirement. 2.28.2. While complying with the above requirement it is important to ensure that HSE contracts with
the appropriate minimum number of suppliers. 2.28.3. It is important that strong mutually beneficial relationships and partnerships are built up with
key suppliers where this assists meeting the best value for money objective. It is important that the purchasing activities of the HSE do not operate to limit choice and competition amongst recently established firms or those seeking to contract with the public sector for the first time.
A2.29. It is a mandatory requirement that any arrangement that might in the long term prevent the
effective operation of competition must be avoided.
A2.30. Supplier Performance Management
Budget Holders must ensure that arrangements are in place to monitor the performance of significant suppliers and that corrective action is taken and followed up where performance is not satisfactory. The Budget holder must link with the designated procurement agent (Material Management, Capital Estates etc) with regard to monitoring and taking action on supplier performance.
Health Service Executive National Financial Regulations
Ver 1.3 Page 89 of 176
GO TO TOP OF CHAPTER ON PAGE 76 TOPIC 9: Receiving Goods or Services - More information
Related Section in chapter 2; on page 37
A2.31. Formal Documented Purchasing Arrangements for Managers and Users
2.31.1. Accounting entries associated with receipt of goods or services In many cases the staff member responsible for creating and inputting what is referred to as “The Goods Receipt Note (GRN)” G9 on the FIS will not be the same person as has checked the goods or services and / or signed off on their satisfactory receipt.
2.31.2. For this reason the creation and inputting (posting) of the GRN within FIS does not require any
specific authorisation level.
2.31.3. The person carrying out this transaction on the system must, however, be able to produce for future audit the appropriate documentation to demonstrate that the receiving process was appropriately signed off before they inputted the GRN into the computer system .
2.31.4. There is a requirement on all Budget Holders to make the purchase to pay process as efficient as possible.
2.31.5. In this context it is clearly necessary to maximise any opportunities that may exist to have sign-off of the receiving process and finalisation of the GRN on the computer system carried out by the same person.
2.31.6. Responsibility for the process of finalising GRN’s on FIS rests with the relevant Budget
Holder and their managers and is important. The act of creating and inputting the GRN in computer system:
Records the liability to the supplier as an accrual Records the expenditure against the budget of the relevant Budget Holder
A2.32. Services provided over a period of months or years
2.32.1. Approval of expenditure for services occurs when the contract:
(i.) Is initially awarded. (ii.) Is amended e.g. increase in cost (iii.) Is renewed
For example: a contract extends over 12 months and payments are made in monthly instalments. In this example each monthly instalment represents a sign-off on satisfactory receipt of the services for that month.
2.32.2. The approval level (i.e. grade) that applies to monthly payments is based on the value
thresholds for the “sign-off on satisfactory receipt”
2.32.3. Each monthly instalment is not a new expenditure approval
2.32.4. This regulation is particularly relevant to grants to voluntary organisations / not for profit organisations.
A2.33. Procedures and Local Receiving Arrangements
2.33.1. It is important that Budget Holders ensure that robust arrangements are in place to identify and
record liabilities on a monthly basis even if supplier does not expect payments each month.
2.33.2. Please refer to the following sections that set responsibilities on page 85.
Health Service Executive National Financial Regulations
Ver 1.3 Page 90 of 176
2.33.3. The recording of liabilities is relatively straightforward where goods are physically received as
this prompts the inputting of a Goods Received Note (GRN) in FIS.
2.33.4. Recording of liabilities is an important element of the ‘Accruals’ G10 process.
2.33.5. In the case of services, including works, procedures must be in place to ensure that each month any material liabilities are estimated and recorded by means of submitting accruals for input into the FIS.
DELIVERY OF GOODS/SERVICES – Additional Information Related Section; on page 40 ,Refer to Sample Template on page 166
A2.34. Proof of Delivery is Mandatory in all situations - including direct delivery to clients or other third parties
In certain cases, HSE purchased goods or services are not physically received by HSE staff but may, for example, be delivered directly to or collected by or on behalf of HSE clients.
This may pose practical issues for Budget Holders in formalising arrangements around the receiving process for their area.
It is stressed that such practical issues do not eliminate the mandatory requirement that each area must obtain reasonable proof of delivery of goods or services before paying for them. There are many options that can be explored in this regard and this is a matter for Budget Holders.
2.34.1. However the requirement is that in respect of each direct delivery;
There is a mechanism for the recipient (i.e. the client) Or someone acting on their behalf Other than the supplier, To confirm receipt of the goods or For a HSE staff member or some one acting on its behalf To verify receipt of the good or service.
A2.35. Minimum Delivery Documentation to facilitate Proof of Delivery
The HSE requires minimum delivery documentation in respect of all goods or services received. Such documentation summarises, from the supplier’s perspective, what he believes he has delivered and must as a minimum enable the HSE to interpret:
When and by whom it was ordered – a Purchase Order Number or agreed alternative must be
quoted on all delivery documentation. What was delivered – quantity, type, description etc in sufficient detail to enable efficient
matching later to the original purchase order/ contract. When and to where it was delivered
2.35.1. It is a matter for Budget Holders to manage their relationships effectively with suppliers to
ensure that they receive the necessary documentation in an appropriate format that assists in implementing the required controls in an efficient manner.
2.35.2. In most cases there will be a need for onward communication of delivery documentation in the form of a “Proof of Delivery Document” (PoD).G11
Health Service Executive National Financial Regulations
Ver 1.3 Page 91 of 176
2.35.3. Actual delivery of any good or service must be verified and recorded.
Wherever practical the delivery documentation provided by the deliverer should be utilised.
2.35.4. This will generally be carried out by a HSE staff member in the form of a legible signature written across the delivery document with whatever notes or qualifications are necessary such as “subject to inspection”.
o In the absence of appropriate delivery documentation being provided by the deliverer
then the appropriate HSE staff involved in the receiving process must themselves prepare a “Proof of Delivery Document”.
o Proof of Delivery documents must be fully legible and contain the basic information listed at A2.36 below.
A2.36. Information to Appear on Suppliers’ ‘Proof of Delivery’
It is the responsibility of each Budget Holder to manage relationships with suppliers to ensure that Delivery Dockets are received promptly and contain necessary prescribed information.
Supplier Name and Address Delivery Address and contact person Purchase order number or equivalent agreed number. Description of Goods/Service to required level of technical detail. Delivery date Details of items not delivered or returned.
INSPECTION, CHECKING AND ‘MATCHING’ OF RECEIPT – Additional Information
Related Section; on page 40
A2.37. 1.b Shortage on Delivery - Follow-up regarding goods ordered and not delivered
2.37.1. Checking of what has been delivered against the purchase order may reveal that less than the quantity ordered has been delivered.
2.37.2. The supplier should be notified of this immediately and requested to deliver the additional
quantity as soon as possible. 2.37.3. Where, for whatever reason, a supplier does not deliver the balance of the goods within a
reasonable time he must be formally notified that the goods are no longer required and the purchase order should be amended accordingly.
2.37.4. It is important to ensure that the appropriate notification of the shortage and delivery is received by the staff member responsible for inputting Goods Receipts Notes into the financial system so that the necessary accounting entries can be dealt with.
A2.38. 2.a Checking if fit for purpose / free from obvious defects
2.38.1. While checking that goods or services are fit for purpose and free from obvious defect
managers and staff should be aware of the warranty position for the goods / services. 2.38.2. The warranty should incorporate the right to rectify any defects that come to light after initial
signing off of receipt for goods or services. 2.38.3. Accordingly the requirement at the goods receipts stage, subject to the above, is a reasonable
but not an exhaustive level of checking to identify any potential defects.
Health Service Executive National Financial Regulations
Ver 1.3 Page 92 of 176
A2.39. 2.b Quality Assurance / Certification
Where certificates of fitness for purpose or any other quality assurance documentation is required in respect of any goods or services (for example R.E.C.I. Certification in relation to electrical wiring) then sign-off on satisfactory receipt cannot take place until the appropriate certificates have been received and are deemed to be in order.
A2.40. Proof of Delivery / Receipt not notified until Invoice receipt
2.40.1. Payment of invoices cannot be made until there is a record of satisfactory receipt of goods or
services.
2.40.2. Delays in recording satisfactory receipt of goods, either due to lack of proper delivery documentation at time of receipt or delays in processing may lead to unnecessary late payments and prompt payment charges being incurred.
2.40.3. It is the responsibility of each individual involved in the delivery/Goods Receipt process to
ensure Goods Receipt Note (GRN) for satisfactorily received goods/services are inputted promptly on the FIS.
2.40.4. Persistent difficulties with obtaining ‘Proof of delivery’ from suppliers must be effectively
followed up and addressed.
A2.41. All returns of Goods must be documented fully, to include: Refer to Sample Template on page 166
i) Purchase order number or Contract reference number ii) Delivery date and location iii) Description of goods returned iv) Quantity of goods returned v) Date and method of return vi) Reason for return vii) Confirmation of acceptance of return by supplier and / or Credit Note reference viii) Supplier name
2.41.1. Where feasible the requirement is to only reject and return those goods that are defective or
do not match what was ordered.
GO TO TOP OF CHAPTER ON PAGE 76 TOPIC 10: Supplier Payment Remittance & Supplier Reconciliation
Related Section in chapter 2;
A2.42. Supplier Statement Reconciliation
Budget Holders must ensure that all supplier statements are reconciled and arrangements made to clear outstanding balances on an ongoing basis. Where a supplier is used by a number of budget holders, each budget holders must ensure that procedures are in place to ensure that each of their transactions relating to that supplier can be fully reconciled and accounted for irrespective as to who actually completes the reconciliation.
The practical operation of this regulation is a matter for each Budget Holder and may require discussion and agreement with shared services or equivalent.
Such practical issues do not affect the requirement to implement this regulation.
Health Service Executive National Financial Regulations
Ver 1.3 Page 93 of 176
A2.43. Supplier Remittances (Payment Remittance Advices)
2.43.1. The ‘Supplier Remittance Advice’ is the document that the supplier receives along with payment to allow the supplier to understand what transactions are being paid.
2.43.2. Budget Holders must ensure that sufficient and accurate details are recorded on the Financial
Information System (FIS) as part of the purchase and receipting stage to enable shared services or the equivalent to efficiently produce remittance advices for suppliers.
A2.44. The minimum requirement for remittance advice is that the following must be provided in respect of each amount appearing on the remittance advice:
i) Invoice number and invoice date
ii) The purchase order number or equivalent.
2.44.1. Sufficient detail to enable the supplier to identify which element of the invoice is being paid if
less than the full amount of an invoice is paid. 2.44.2. Contact details for any queries which where practical should be specific to each remittance
amount 2.44.3. Poor quality information on remittance advices may lead to difficulties in reconciling suppliers’
statements therefore this area requires close attention by Budget Holders and those acting on their behalf.
A2.45. Suppliers Statements and the need to reconcile and address outstanding amounts
2.45.1. There is a mandatory requirement for Budget Holders to ensure that the purchase to pay
process is efficiently organised in their area. 2.45.2. One key performance indicator (KPI) in relation to this is that suppliers are paid on time and
that there are not significant unresolved issues regarding outstanding amounts due to suppliers.
2.45.3. It is essential that any monies recorded by a supplier as due to him/her can be reconciled with
the HSE records of what is deemed to be owed to the supplier.
2.45.4. This is a key control point - recurring and ongoing issues on supplier statement reconciliations often indicate a poorly controlled purchase to pay process.
Health Service Executive National Financial Regulations
Ver 1.3 Page 94 of 176
GO TO TOP OF CHAPTER ON PAGE 76
TOPIC 11: Invoice Matching Tolerances – More information
Related Section; on page 44
A2.46. Tolerance Levels - (When Matching Invoices to PO/GRN)
These regulations permit a general price tolerance level of €25 or 2% (whichever is the lower ) when matching the total value of an invoice to the relevant amount on the purchase order / GRN.
2.46.1. Price differences; All matching differences above €25 or 2% require the invoice to be referred to the appropriate local staff member for resolution. The FIS system will identify where there are price differences (greater than the tolerance level) and change the status of the transaction until the transaction is subsequently released. Resolution may involve engaging with the supplier to have the invoice amended or approval of the additional amount and amendment of the purchase order / goods receipt note as necessary The tolerance level applies to the total value of the invoice compared to the purchase order price/Goods Received Note and not to individual lines on the invoice.
2.46.2. Where an additional amount is being approved the total amount of the relevant invoice must
be looked at in identifying the level of manager required to sign-off on the revised amount.
2.46.3. Delivery charges should not be accepted unless they have been specifically identified and agreed at purchase order stage
2.46.4. All matching differences above €25 or 2% must be listed, summarised appropriately and
reported to the relevant Budget Holder on a monthly basis in the format specified by the Area Director of Finance.
2.46.5. Budget Holders must review these reports and report on a quarterly basis to the Area Director
of Finance as regards any trends in the occurrence of matching differences.
2.46.6. Budget Holders must outline in their quarterly reports the measures being taken to address any inappropriate level of recurring matching differences.
2.46.7. Quantity differences (Invoice quantity is greater than Ordered)
i) Quantities delivered in excess of the Purchase order quantity should not be accepted and should be taken back by the supplier at no extra cost to the HSE.
ii) Where a decision is taken, in exceptional circumstances, to accept additional quantities, this requires the approval of a new purchase order and/or an approved amendment to the original purchase order.
Health Service Executive National Financial Regulations
Ver 1.3 Page 95 of 176
Related Chapter ; on page 46 Appendix ToC ; on page 68
Related Chapter; 3. Tendering
TOPIC 1; Public Advertising Requirements - More information
Related Section; on page 47 A3.1. Public Advertisement
3.1.1. Compliance with the requirement for public advertisement involves publication on the
government tendering web site www.etenders.gov.ie.
3.1.2. Other advertising media such as national newspaper should be utilised in addition to the web site if considered necessary to attract a sufficient number of tenderers.
3.1.3. National and EU advertising information must be consistent – all information regarding a
contract published nationally must be included in EU publications (and visa versa).
EU contract threshold (Supplies / Services over €211,000 and Works over € 5.278m)
3.1.4. The EU thresholds are revised by the EU every two years. The current thresholds are valid from 1-Jan-06 until 31-Dec-07)
3.1.5. Each contract above the EU contract threshold must be published on the Official Journal of the European Union (OJEU) publication accessed via the e-tenders web site or EU website http://simap.eu.int/.
3.1.6. Departure from the requirement for advertisement for contracts above the EU threshold value
is not permitted by these regulations and would be a breach of legal obligation. Non EU Threshold (Supplies / Services less than€211,000 and Works over € 5.278m)
3.1.7. Only the relevant National Management Team Member can approve a departure from the requirement for public advertisement (above €50,000 for goods/services or above €500,000 for works), but only in exceptional circumstances set out on page 77.
3.1.8. This approval must be co-signed by the Area Director of Finance.
A3.2. Prior Indicative Notice (PIN)
3.2.1. It is recommended that Prior indicative Notices G12 (PINs) be for known aggregated
procurement supplies or services requirements in excess of €750,000. 3.2.2. The PIN is normally submitted at the start of the budgetary year and sets out the categories of
products and services likely to be procured during the year
3.2.3. From 1st January ‘07, there will be a mandatory requirement to publish a PIN of all national ‘aggregated’ spend in excess of €750,000 by product area of supply or category of service. It is the responsibility of the Head of Procurement to ensure that PINs are published, setting out categories of products/services for the HSE as a whole.
3.2.4. PINs are intended as an aid to transparency and are for the benefit of suppliers. Insertion of a
PIN does not commit contracting authorities to purchasing or proceeding with a project if circumstances change.
Health Service Executive National Financial Regulations
Ver 1.3 Page 96 of 176
TOPIC 2; Aggregation Procedure - More information Related Section; on page 47 A3.3. Aggregation of Tenders/ Tender Coverage
(Source ; Regional Material Management’s “Procedure for Tender/Contract Approval”) More information; on page 47 Template form to Complete on page 163
3.3.1. It is the policy of the HSE to move to a situation where the level of aggregation of purchasing is increased consistent with full compliance with EU Procurement requirements and achievement of Value for Money.
3.3.2. These regulations require that pending the completion of the change process outlined above
the following “Procedure for Tender/Contract Approval (issued in March 2005) will apply:
3.3.3. This pre tender procurement Aggregation process (Tender/Contract Approval procedure) applies to proposed tender process with an estimated contract value in excess of the high values ( currently €50k) defined in the procurement policy
o Need to Commence tender process Identified
o Refer details of proposed contract to HSE Procurement using template.
Information required;
a) Name of proposed contract
b) Scope of Proposed contract
c) Estimated start date (date of award)
d) Value of proposed contract
e) Contract details
o Following assessment a decision on the appropriate action to be taken will be issued.
o HSE reference number will be assigned to all future tender processes. o Following completion of the tender process a copy of the Contract Approval Request (CAR)
should be forwarded to HSE procurement (see template on page 163). The CAR will be used for formal contract approval and to update the HSE register of contracts.
o This procedure will provide the basis for an efficient streamlining of contracts at sector
level. It will also accelerate compliance with EU procurement Rules on aggregation of expenditure.
Health Service Executive National Financial Regulations
Ver 1.3 Page 97 of 176
TOPIC 3 ; Tendering Process, General Requirements - More information Related Section; on page 54.
A3.4. Tender Addressee - Receipt and Handling of Tenders
3.4.1. A – Below EU Threshold
Tender should be addressed to the relevant HSE National Management Team Member or a nominee, Assistant National Director , LHO Manager, Hospital Manager (NHO bands 4 & 5 only), or otherwise approved by the relevant Assistant National Director of Finance or his/her nominee.
3.4.2. B – Above EU Threshold
Tender should be addressed to the relevant HSE National Management Team Member or nominated Assistant National Director or Hospital Network Manager or as otherwise approved by the relevant Assistant National Director of Finance or his/her nominee.
3.4.3. Minimum time to be allowed for receipt of quotes / tenders
The provisions set out in Table 1 on page 69 must be complied with as a minimum.
3.4.4. Tenders received late
(i.) Late tenders should not be opened and should therefore not be evaluated.
(ii.) Tenderers must be advised as soon as possible that their tender is being considered as
late. Tenders that are received late should be returned, unopened, with a covering letter and with the unopened tender attached, stating that the tender could not be included in the tender process because it was received after the notified time.
(iii.) Tenderers should be advised that they have a defined time period (no less than two
working days) within which to submit evidence that the late delivery was beyond their control.
3.4.5. Tender Deposit
(i.) Any tender deposit charged must be limited to the estimated marginal cost associated
with reproducing the tender documents and getting them to each extra potential tenderer (i.e. printing/photocopying plus postage/courier etc).
(ii.) Tender deposits should be repaid upon receipt of a valid tender by due date.
A3.5. Custody and Opening of Tenders
3.5.1. Above the € 50,000 threshold sealed tenders are required and these must:
(i.) Be numbered sequentially and stamped for date and time upon receipt.
(ii.) Be held securely in a locked container or room and unopened until due for opening after the tender deadline has expired.
(iii.) Be opened at the specified time by a minimum of two staff nominated for that purpose
with the consent of the relevant Assistant National Director of Finance. One of the staff members must be at Grade Vlll or higher.
(iv.) Every tender must be initialled and dated by the staff opening it. Each page of price
sheets should be signed and dated stamped.
Health Service Executive National Financial Regulations
Ver 1.3 Page 98 of 176
(v.) Be recorded in a register kept for that purpose detailing:
Date and time received Date, time and by whom opened Confirmation that tender was not previously opened Name of tenderer Overall price quoted where applicable Specific ‘lots’ tendered for where relevant Date and person handed over to for tender evaluation.
(vi.) Be held safely until handed over for evaluation
3.5.2. Where a tender has been submitted with a covering letter attached the details of the tender must be checked against the letter. Any discrepancies must be notified to the tenderer.
3.5.3. Any additional requirements of EU procedures must be fully complied with.
A3.6. All potential suppliers must have equal access to information
3.6.1. All potential suppliers must be informed in a consistent way as to any criteria that may be used to evaluate their quotes or tenders.
3.6.2. It is essential that any information, or clarification, provided to one supplier, is provided in the
same format and at the same time to all potential suppliers regardless of whether they have requested it or not.
3.6.3. HSE staff must not give any real or perceived advantage to any potential supplier.
3.6.4. Documents to be made available to potential tenderers on request;
(i.) Specification of goods, services or works (ii.) Pre-qualification criteria and forms for completion where appropriate (iii.) Tender document (to be filled in by tenderers) (iv.) HSE Conditions of Contract (to be signed by tenderers to indicate acceptance). (v.) Any other relevant information.
A3.7. Tender Evaluation
More Information; Tender Evaluation Report on page 99. The criteria to be used to evaluate any tender must be objective and the evaluation process must be transparent and fair.
3.7.1. All evaluation criteria must have been disclosed to potential tenderers prior to them completing
their tender documents.
3.7.2. The HSE Procurement Policy establishes different aspects of assessment and evaluation that should be considered for each tender being processed. These include ;
a) Clinical Evaluations b) Technical Evaluation c) Commercial Evaluation
3.7.3. Any criteria not disclosed cannot be used in the evaluation process.
3.7.4. The relevant Budget Holder must nominate the person or persons to evaluate any tenders that
are received.
3.7.5. Cost is a very significant factor in evaluating any quote or tender.
1. When considering costs, managers must consider full cost over likely lifespan of the good or service in so far as is practical.
2. Costs should include any recurring costs during the lifespan of the good or service and any material disposal or decommissioning costs.
Health Service Executive National Financial Regulations
Ver 1.3 Page 99 of 176
A3.8. Acceptable Basis of Award of Contracts
The following are the accepted bases for evaluation for award of tender contracts within the HSE;
Most Economically Advantageous Tender (MEAT)
Or
Lowest Priced Tender
3.8.1. MEAT Basis
Most Economically Advantageous Tender is the recommended as the primary basis of tender evaluation. Other criteria (in addition to price) are considered as part of the evaluation process, e.g. technical assistance and merit, after sales service, environmental concerns.
3.8.2. Examination of Tenders should be carried out by individuals (with the relevant competence and skills. These may include Clinical input or evaluation of tenders in addition to commercial evaluation (as appropriate to specific contract).
3.8.3. All contracts greater than € 25,000 will require input from a Purchasing Professional who should coordinate the procurement process including qualification/assessment, procurement of supplies/service and commercial analysis as well as negotiations.
Application of the M.E.A.T. principle requires criteria to be weighted to indicate the level of importance attached to each of the criteria. A scoring sheet rating each tender/quote against the different elements of the evaluation criteria must be completed for each tender process.
3.8.4. The M.E.A.T. principle enables due regard in the evaluation and award process to be had to
factors such as:
Full cost price over complete life cycle of goods, services or works Match to specification issued with tender documents Capacity (technical and financial) of suppliers to satisfy the full requirement Demonstrated relevant experience and competence Level of after sales service Technical assistance available Technical merit and general suitability of good, service or works Acceptance of HSE Standard Contract Terms
3.8.5. Acceptance of Lowest Price Tender
It is appropriate for a high evaluation weighting to be assigned to cost where goods, services or works are;
relatively standardised and closely comparable in terms of specification and
any after sales support etc
A3.9. Tender Evaluation Report
Related Sections; Paragraph 3.29 on page 54 & paragraph 3.31 on page 55
As a minimum, tender reports must record or refer to readily accessible and preferably attached documents that record:
(i.) Description of goods or services tendered for (ii.) List of tenderers (iii.) All relevant dates in process including for example
Health Service Executive National Financial Regulations
Ver 1.3 Page 100 of 176
Date of advertisement / invitations to tender List of tenders received and dates Deadline for receipt of tenders Date tenders opened Date(s) tenders evaluated and by whom
(iv.) Details of any late tenders (v.) Details of any invalid tenders (vi.) Comparable prices per valid tender following any adjustments necessary to compare
like for like (vii.) Evaluation based on criteria utilised, marked on a score sheet. (viii.) The evaluation score sheet must provide sufficient detail to enable full understanding of
why the lowest tender may not have been accepted. (ix.) Results of the evaluation and a recommendation by the evaluators as to which tender
should be accepted and on what basis. (x.) Signature of persons who carried out the tender evaluation and prepared tender report.
A3.10. Tender Award
3.10.1. The award of a contract or issue of a purchase order following a tender process is an approval
of expenditure and requires a formal written decision (see ‘Written Decision approving expenditure greater than €50,000 on paragraph 2.61 on page 36 and also page 82 ).
3.10.2. The tender evaluation report should be referenced (and preferably attached to) in the written
expenditure approval decision and should include all of the necessary information.
In that context the written decision will, if appropriate: Cover the acceptance of the tender evaluation report Approve the award of the contract or order and Detail any other matters not dealt with in the tender evaluation report which are
required to be included on a written expenditure decision
3.10.3. For administrative efficiency and ease of future reference the tender evaluation report and the expenditure approval decision should be encompassed in the composite document where practical.
A3.11. Restrictions on Award of Tenders / Contracts Related Section; Paragraph & paragraph
Before the award of any HSE tender/contract the following must be addressed:
3.11.1. Risk Management – It is essential that potential risks associated with the supply of any goods
or services are where possible identified and dealt with prior to award of tender / contract. This includes:
Quality/Reliability.
(a) The HSE must have appropriate arrangements/ procedures in place to be able to identify, record and resolve with suppliers, problems identified with goods/services delivered.
(b) Budget Holder/ expenditure approver signing must be able to satisfy themselves that the goods delivered/services provided are of sufficient quality to meet the needs of the service.
Insurance. All suppliers must have adequate Employers and Public Liability or product Insurance as appropriate. Evidence of appropriate insurance must be supplied.
3.11.2. Statutory Provisions – tenders / contracts can only be awarded to organisations that confirm
they are complying with all applicable statutory provisions including those relating to: • Payment of minimum wage
Health Service Executive National Financial Regulations
Ver 1.3 Page 101 of 176
Restrictions on Award of Tenders / Contracts – Statutory provisions …….continued
• Employment Law generally
• Taxation
• Health and Safety Issues
• All other relevant provisions
3.11.3. Conflicts of Interest – anyone involved in
• Tender / contract requirements specification or
• Tender evaluation or
• Expenditure approval / award of tender / contract
must confirm in writing, that the tender has no potential conflicts of interest that might affect in any way their ability to act with impartiality and objectivity in relation to any aspect of the tender process.
3.11.4. They must also undertake to make known to the Budget Holder any potential conflicts that may
subsequently arise.
3.11.5. The Budget Holder must decide whether the potential conflict of interest requires the exclusion of the person from the process
3.11.6. He must inform the relevant Assistant National Director of Finance of his/her decision in writing.
3.11.7. Potential conflicts of interest involving National Management Team Members must be notified
in writing to the HSE Chief Executive Officer.
3.11.8. Potential conflicts of interest involving the HSE Chief Executive Officer must be notified to the Chair of the Board of the HSE.
3.11.9. Collusive Tendering – Staff involved in any tendering process must be vigilant in order to prevent collusion between potential tenderers or any other anti-competitive practices.
3.11.10. Criminal Convictions – public contracts cannot be awarded to persons convicted of: o Organised crime o Fraud o Corruption o Money Laundering
Potential tenders must be made aware of this requirement and of the need to provide written confirmation that demonstrates compliance for proprietors, owners, directors and contract contacts. The successful tenderer will be obliged to notify the HSE in writing of any change to the status of this compliance statement that may occur during the period of the contract.
A3.12. Notification of Results of Tendering Process
All tenderers, including those who are not successful, should be informed of the result of the tender process without undue delay.
3.12.1. No information regarding the final award of any contract or issue of a purchase order following
the tender process can be given to the successful tenderer(s) until the relevant Budget Holder or his/her nominee have approved the expenditure.
3.12.2. It may be necessary to reserve the right to revert to one or more unsuccessful tenderers in the
event that a preferred tenderer does not actually wish to proceed with the provision of the goods, services or works.
Health Service Executive National Financial Regulations
Ver 1.3 Page 102 of 176
3.12.3. Notification of Unsuccessful tenderers;
Unsuccessful tenderers for contracts covered by the EU Directives should be notified promptly of the outcome of a tendering procedure.
A contract is not formally awarded before an interval has elapsed, during which an
unsuccessful tenderer can seek a review of the decision if s/he feels that the process has been unfair or unlawful.
Any notification to the successful tenderer during this interval must be provisional and must
not constitute a contractual arrangement. Tender documentation should include a statement indicating the need for an appropriate
interval after the award decision is notified and before a formal contract is put in place.
A3.13. Documents to be held on every tender file
3.13.1. Documentation relating to a tender file should be retained for the later of ; (i) The end of the contract and (i) The end of the audit period for which the final invoice relating to a contract has been posted.
3.13.2. The following must be retained in respect of each tender process:
i Original requisition or memo etc. setting out need
ii Specifications / description of work
iii Copies of all notices and documents published or issued to potential tenderers.
iv Any correspondence from or to potential tenderers
v Conditions of Tendering
vi Details of marking scheme used as part of MEAT evaluation
vii Terms of Contract
viii Qualifications / short listing report
ix Copies of all tenders received and accompanying documents
x Commercial / Technical / Clinical evaluation reports appropriately signed
xi Minutes of any meetings whether internal or with potential suppliers
xii Details of those involved in the process e.g. tender opening, evaluation, and approval
xiii Copies of any letters to unsuccessful tenderers or debriefing notes
xiv Tender Evaluation Report
xv Expenditure approval decision
xvi Copy of final awarded order or contract and any award notice
Health Service Executive National Financial Regulations
Ver 1.3 Page 103 of 176
Related Chapter; on page 56 Appendix ToC ; on page 68
Related Chapter; (4) NON ORDER PAYMENTS (General)
TAXI’s As with any area of expenditure it is the responsibility of Budget Holders to ensure that taxi costs incurred are necessary for the service, represent value for money, and are appropriately monitored and controlled. Use of Taxi’s presents some practical difficulties in terms of the normal purchase to pay process.
A5.1. Purchasing Taxi Services
5.1.1. A contract or contracts for taxi services should be in place for the HSE and must be renewed at least every 2 years (can be extended to 3 years with approval of the relevant Assistant National Director of Finance.
5.1.2. The taxi contract must provide appreciable benefits to the HSE in terms of cost reductions and
/ or a more efficient billing and activity tracking process. 5.1.3. Wherever practical the contract must be used for all taxi journeys. 5.1.4. It is accepted that in some instances taxi’s will be booked to collect at a certain time and
location whereas in other cases taxi’s may be engaged directly on the street. 5.1.5. It is not required that a purchase order is issued for each individual taxi journey
A5.2. ‘Receiving’ Taxi Services
5.2.1. Each person utilising a taxi which the HSE has to pay for must ensure that:
(a) The taxi meter is correct (should be at zero or appropriate booking/waiting charge) when their journey commences.
(b) They sign for the charge at the end of the journey and get a receipt / docket showing the amount which must match the final charge showing on the meter.
(c) Where they pay the charge themselves they must also obtain a receipt showing the amount which must match the final meter reading.
(d) They forward, without delay, the receipt / docket to the appropriate person responsible for checking taxi invoices and processing them for payment.
(e) This includes where they have paid the taxi themselves and are submitting an expenses claim for re-imbursement.
5.2.2. The receipt / docket referred to. above must also (i) Be dated, (ii) Indicate journey start point
and destination (iii) Show Taxi/hackney registration number.
5.2.3. Budget Holders must have arrangements in place to ensure that taxi invoices / expenses claims are matched against the taxi receipts / dockets and any material discrepancies investigated and dealt with.
A5.3. Monitoring of Taxi Costs
Budget Holders must monitor taxi costs and usage on an ongoing basis to ensure that: Taxi journeys are necessary and appropriate Taxi’s are not being used for personal use Efficient and proper usage is made of taxi’s – for example a protocol around requesting
taxi’s to wait at a destination for a return or onward journey must be in place and enforced.
Health Service Executive National Financial Regulations
Ver 1.3 Page 104 of 176
Related Chapter ;on page 56 Appendix ToC ; on page 68
Petty Cash Disbursements/ Franking Machines General
This regulation deals with the purchase to pay aspects of the use of petty cash. This regulation is framed in the context that there is a clear obligation on all managers to ensure that the use of cash as a payment method is kept to the absolute minimum necessary.
A5.4. Requirements relating to:
5.4.1. Custody and safe keeping of cash including petty cash.
5.4.2. Insurance and security requirements around handling cash including petty cash
5.4.3. Opening and management of bank accounts including bank accounts operated to support
petty cash administration are dealt with in detail within the regulations grouped under Section 7 “Income, Debtors, Banking and Cash”.
5.4.4. This regulation must be read in conjunction with Section 7 referred to above.
A5.5. There are inherent risks and inefficiencies associated with the use of cash as a payment method.
A5.6. Petty Cash Imprest G13
5.6.1. Petty Cash refers to small amounts of cash (or access to cash) authorised to be held by specific locations, used to make payments for incidental expenses where no other method of payment e.g. a cheque, is available or not practical due to the amount.
5.6.2. The availability of petty cash allows local management to obtain low value items without the
requirement for processing them through the normal ordering procedures. 5.6.3. In some instances a petty cash bank account will be operated at a local bank branch to
facilitate secure management of petty cash. 5.6.4. This generally applies where a large number of separate petty cash imprests are administered
by a local service HQ. Prohibition on Splitting of Purchases.
A5.7. Petty Cash accounts must not be used as a means of frustrating or avoiding normal purchasing procedures where the value involved requires the issue of purchase orders etc. Purchases or payments must not be split for the purpose of avoiding the €50 threshold for the maximum petty cash payment.
A5.8. Formal Approval Required for Petty Cash Account
5.8.1. A written decision approved by the Assistant National Director/ Hospital Network Manager/ Local Health Office Manager, NHO Hospital Manager (AND/HNM/LHOM/NHOHM ) and countersigned by the relevant Assistant National Director of Finance is required to:
i) Establish a petty cash account ii) Increase the limit on a petty cash account iii) Increase the cash budget on a petty cash account iv) Approve the write off of any cash loss to the petty cash account v) Record the closure of a petty cash account.
Health Service Executive National Financial Regulations
Ver 1.3 Page 105 of 176
5.8.2. Where a bank account is opened to support the operation of the petty cash account this must be done in accordance with existing financial regulations governing banking arrangements. Updated policy in relation to ‘Opening’ and maintenance of bank account will be included in phase 2 of the NFR project.
5.8.3. Decisions in relation to (i) to (iii) above must as a minimum requirement set out:
i) Name of Petty Cash Account. ii) Description of Service Location petty cash to be utilised by. iii) General purpose / justification for establishment or increase of petty cash
account / cash budget iv) The Imprest amount i.e. the maximum limit or float v) Cash budget amount (see below) vi) Details of the staff member(s) specifically responsible for managing the petty
cash account vii) Details of any bank account associated with the petty cash account viii) Details of arrangements to ensure safe custody of the cash
5.8.4. In the case of the write off of any cash loss the decision must include a copy of the findings of
the investigation into the loss and any relevant recommendations of the budget holder.
A5.9. Petty Cash expenditure
Individual petty cash transactions must not exceed €50. Where there is a justifiable reason to increase the transaction limit above €50 (i.e. raise the limit that would apply to future transactions) a written decision must be approved by the relevant AND/HNM/LHOM/NHOHM N19. This increase will come into effect after notification to relevant Assistant National Director of Finance.
Petty cash transactions may relate to: Reimbursement of cash to an individual staff member who has incurred a cost on behalf of
the HSE utilising their own personal funds. Provision of cash in advance to a staff member to enable them to purchase item(s) required
by the service. The reimbursement option is the preferred model for operation of petty cash.
A5.10. Backup/ Support required for Petty Cash Transactions
Each individual petty cash transaction must be backed up by:
5.10.1. A petty cash approval document which must set out the following,
i) The amount of the transaction ii) A description of the items purchased / to be purchased or other reason for the petty cash
transaction iii) The date of the transaction iv) The name and signature of the staff member claiming petty cash together with date
claimed v) The name and signature of the manager approving the petty cash claim together with the
date approved. vi) Supporting documentation available i.e. receipt, sales slip etc. vii) The cost centre and cost element the expenditure relates to
N 19 AND/HNM/LHOM/NHOHM = Assistant National Director/ Hospital Network Manager/ Local Health Office Manager, NHO Hospital Manager
Health Service Executive National Financial Regulations
Ver 1.3 Page 106 of 176
Petty cash approval documents must be signed off by a Grade IV or higher appointed for that purpose by the relevant budget holder.
Once cash has been issued from the petty cash account the petty cash approval
document must be clearly marked “PAID” to avoid any potential duplicate payments.
5.10.2. Documentary evidence to support the payment / repayment of cash to the staff member should
be attached with the petty cash approval document.
5.10.3. Such evidence may consist of any of the following:
1. Sales receipt 2. Statement indicating amount paid 3. Credit card receipt
5.10.4. Other relevant documentation confirming that a payment has been made on behalf of the HSE
A5.11. The mandatory requirements around documentary evidence are that:
1. It must be available for all transactions above €5.00 2. It must show that the amount that needs to be reimbursed from the petty cash
account has actually been paid out 3. It must be dated
Where petty cash, in exceptional circumstances, is provided in advance to enable a purchase to be made, then the necessary petty cash approval document must be signed before the petty cash is issued. In such cases the relevant documentary evidence (sales receipt etc.) must be attached to same as soon as possible after the purchase is made.
A5.12. Cash Budgets
5.12.1. The Imprest or float amount for each petty cash account is the maximum amount that can be held locally at any given time between cash and vouchers to be submitted to national shared services or equivalent to replenish the petty cash account.
5.12.2. This amount is also the maximum amount that can be issued in any one replenishment cheque
or EFT (Electronic Funds Transfer) payment to the petty cash account. 5.12.3. In addition however there is a requirement to place a limit on the total amount of cash that can
be utilised by any petty cash account in any given financial period. 5.12.4. In the absence of such a cash budget the frequency of petty cash replenishment will dictate
the actual total amount of petty cash used and since petty cash represents actual expenditure there is a need for it to be monitored and controlled as is the case with all other expenditure.
5.12.5. In seeking approval for the establishment or increase in any petty cash account each budget
holder must set out the annual maximum cash that can be expended through the petty cash account.
A5.13. Reporting and Reconciliation Requirements
5.13.1. It is a mandatory requirement that the manager responsible for each petty cash account:
5.13.2. Records each petty cash transaction on a ledger (preferably excel spreadsheet or other electronic format) that captures the information at A5.10, (I – vii) above.
Health Service Executive National Financial Regulations
Ver 1.3 Page 107 of 176
5.13.3. Records the payment from national shared services to replenish each transaction.
5.13.4. Reconciles the petty cash ledger on a daily or weekly basis to ensure that:
i) Cash on hand / in bank + amount to be replenished equals the petty cash account limit or Imprest amount.
ii) The amount to be replenished can only refer to properly completed petty cash approval documents backed up by the necessary documentary evidence (sales receipts etc.)
iii) The cash budget has not been exceeded
A5.14. Requests for payments to replenish petty cash accounts
Requests to national shared services or equivalent to issue a payment to replenish the petty cash account must:
5.14.1. be accompanied by a copy of the reconciliation demonstrating that the payment sought will not cause the petty cash limit to be exceeded
5.14.2. be accompanied by a reconciliation demonstrating that the payment sought will not cause the
petty cash account to exceed its cash budget
5.14.3. be signed by the budget holder or his/her nominee who must confirm that 1. and 2. above have been reviewed and are accurate and who must be a grade appropriate to the amount being approved.
A5.15. Monitoring and Reporting Arrangements
5.15.1. Budget holders must put in place arrangements to ensure that the usage of petty cash is strictly monitored and controlled in full compliance with these regulations.
5.15.2. On a monthly basis reconciliations to petty cash limit and cash budget must be submitted to
the relevant AND/HNM/LHOM/NHOHM N20 and copied the relevant Assistant National Director of Finance or their nominees.
A5.16. Discrepancies in Petty Cash accounts.
5.16.1. Any discrepancies in petty cash must be notified to the relevant budget holder and investigated.
5.16.2. Discrepancies related to loss/theft of petty cash must be notified in writing to the relevant
AND/HNM/LHOM/NHOHM and copied to the relevant Assistant National Director of Finance.
N20 AND/HNM/LHOM/NHOHM = .Assistant National Director/ Hospital Network Manager/ Local Health Office Manager, NHO Hospital Manager
Health Service Executive National Financial Regulations
Ver 1.3 Page 108 of 176
A5.17. Segregation of Duties
5.17.1. No staff member can approve a petty cash transaction in respect of themselves.
5.17.2. The staff member who manages the petty cash locally including handling the cash and completion of the petty cash ledger cannot approve a request to national shared services or equivalent to issue a payment to replenish the petty cash.
A5.18. Locations where use of petty cash is an element of providing services to clients in a
normalised environment.
5.18.1. Units such as residential children’s' homes and mental health community residences may have a requirement, driven by clinical and therapeutic needs, to make purchases without using the normal HSE stock or purchase order processes.
5.18.2. Such units will require approval by the relevant National Management Team Member and
National Director of Finance and their nominees of specific departures from these regulations for practical purposes.
5.18.3. It will be a matter for the relevant budget holders to identify the need for and recommend such
departures.
A5.19. However such departures will be considered during the implementation phase of these regulations in the context of ;
5.19.1. The inherent risks and inefficiency around cash as a payment method
5.19.2. Developments in society generally which have shown a move away from cash as a primary payment method in favour of cheques, credit cards, debit cards etc
5.19.3. Opportunities to introduce card based payments into HSE facilities i.e. purchasing cards etc.
Health Service Executive National Financial Regulations
Ver 1.3 Page 109 of 176
Related Chapter;on page 56 Appendix ToC ; on page 68
FRANKING MACHINES
A5.20. Budget Holders must monitor Franking costs and usage on an ongoing basis to ensure;
5.20.1. that charges incurred reflect the effective and proper use of funds.
5.20.2. usage is necessary and appropriate
5.20.3. Franking is not being used for personal use
A5.21. The manager of a department/location, which has a franking machine on site, shall ensure that the procedures are in operation to ensure proper custody and control of the operation of the Franking machine.
This should include;
5.21.1. Assigning responsibility for the management of the franking machine (Minimum requirement of Grade V).
5.21.2. Security of machine. Franking machine must be lockable with a key where possible
and or stored in a secure location.
5.21.3. Record Keeping - A post book must be kept detailing daily use and periodically checked to machine totals.
i. Staff who use the machine ii. Date and approximate time machine used iii. Number and value of items franked iv. General description of items franked.
5.21.4. Reconciliation – On a daily basis the post book should be reconciled to the machine total and any discrepancies investigated and resolved.
5.21.5. Replenishment of Franking Machines – replenishment of the machine must be
approved by a Grade V or higher.
When approving the replenishment of the franking machine the manager must review and sign off on the post book and reconciliation of the post book to the machine total.
5.21.6. Segregation of Duties – the manager who approves the replenishment of the franking
machine must not be the person with responsibility for day to day security, operation and reconciliation in relation to the franking machine.
Health Service Executive National Financial Regulations
Ver 1.3 Page 110 of 176
Related Chapter;on page 56 Appendix ToC ; on page 68
Utility Bills (Eircom, ESB, etc)
A5.22. The general requirements of the purchase to pay regulations as set out on page 22 above must be complied with in respect of Utilities unless otherwise provided in this section.
A5.23. This Financial Regulation covers:
Telecommunications – land line (Eircom and others) , Electricity Supply – (ESB and others), Gas Supply – Bord Gais and others , Water Charges, Rates Charges, Waste collection services
A5.24. Purchasing – Expenditure Approval
5.24.1. A formal written decision, in effect an Expenditure Approval, is required:
a) To open a new utility account b) To approve a new connection or significantly amended connection c) To approve a move to a new charging or tariff arrangement etc d) To record the discontinuation of a utility contract / connection
5.24.2. An estimate of the likely usage and cost, or additional cost, per annum must be made
and an expenditure approval from the appropriate grade of manager obtained (per Table 2 on page 70 above.
5.24.3. It is not necessary to issue a purchase order in respect of utility costs either in respect
of the initial set up or ongoing periodic bill payments. Deregulation is bringing major change in terms of choice of providers for what was previously a series of monopoly / proprietary sectors.
A5.25. The Procurement and Materials Management Service has responsibility for advising
Budget Holders around requirements that may come into force requiring competitive sourcing to select utility providers.
A5.26. Receiving
5.26.1. The receiving element of the purchase to pay process is typically carried out following receipt of the invoice.
5.26.2. Budget Holders must put in place arrangements to ensure that utility costs are
recorded as expenditure each month by submission of appropriate accruals.
Health Service Executive National Financial Regulations
Ver 1.3 Page 111 of 176
Related Chapter;on page 56 Appendix ToC ; on page 68
Lease and Rental Requirements
A5.27. General
5.27.1. The scope of this regulation does not extend to the rental or leasing of properties. 5.27.2. Leases and hire purchase contracts are means by which companies obtain the right to
use or purchase fixed assets (vehicles, equipment etc). 5.27.3. A Lease / rental agreement is a formal contract undertaken with a supplier or a
leasing company for the usage of fixed assets such as equipment for a defined period of time, referred to as the “term”.
5.27.4. Depending on the nature of the lease contract, ownership of the asset(s) may pass to
the HSE during or at the end of the term or may remain with the leasing company. 5.27.5. There may be 3 parties to the lease / rental i.e.
i. HSE ii. The Supplier iii. A Leasing firm that may act as intermediary / financier
5.27.6. The nature of most leases is such that one is undertaking a commitment that often extends beyond one year.
A5.28. Requirement for Professional Procurement Input
Professional input from the Procurement and Materials Management Service or elsewhere must be sought as part of the procurement process irrespective of the nature or type of lease or rental agreement being considered.
Types of Lease Agreements
There are two main type of lease / rental contracts:
A5.29. Operating Leases
5.29.1. An operating lease is one where the asset is leased by HSE for a relatively short period and in any event the lease term represents a period that is substantially less than the useful economic life of the asset.
5.29.2. The payment made over the term of an operating lease will be substantially less than
the full cost of the asset. 5.29.3. Assets leased under an operating lease remain the property of the leasing company.
A5.30. Finance Leases
5.30.1. A finance lease is one where the HSE leases an asset for most of its useful economic life and over the term of the lease pays a total amount substantially equal to or in excess of the full cost of the asset.
Health Service Executive National Financial Regulations
Ver 1.3 Page 112 of 176
5.30.2. A finance lease may provide for the transfer of ownership of the asset to the HSE
during or at the end of the lease term however this is not a requirement in terms of defining a finance lease.
5.30.3. An interest or ‘finance’ cost is charged by the ‘lessor’ as part of the contract.
5.30.4. In effect a finance lease is a form of ‘loan’ where principle and interest are repaid to
the lessor with each repayment.
A5.31. Restriction on borrowing – Finance Leases
5.31.1. On the basis that Finance leases are a form of borrowing they require the approval of the HSE Board.
5.31.2. No commitments can be entered into in advance of Board approval other than where
they are clearly expressed and accepted as “Subject to HSE Board Approval”. 5.31.3. Recommendations for finance leases must be signed off by the relevant Assistant
National Director/ Hospital Network Manager/ Local Health Office Manager, NHO Hospital Manager and co-signed by the relevant National Director of Finance prior to being considered by the HSE Board.
A5.32. Expenditure approval
5.32.1. A lease represents expenditure equal to the total payments over the full term of the lease contract including any final or “balloon” payments at the end of the term.
5.32.2. The approval of an operating lease requires sign-off by a manager who is authorized
to approve expenditure equal to the total value of all payments under the lease contract over its full term.
5.32.3. Under no circumstance must the value be split to circumvent the approval process. 5.32.4. The approval of any operating lease, regardless of value, requires a written decision
which is to be copied to the relevant National Management Team Member and the relevant Assistant National Director of Finance.
5.32.5. In addition to the normal requirements to be incorporated into a written decision (the
decision must also cover the following;
1. The term of the operating lease 2. The payment schedule setting out the full amount to be paid over the term of
the lease 3. Details of any final or balloon payments 4. Confirmation that the lease is an operating lease and the basis for that
confirmation.
5.32.6. All lease or rental contracts must be reviewed by the legal department before being finalised.
Health Service Executive National Financial Regulations
Ver 1.3 Page 113 of 176
A5.33. Payment Processing
5.33.1. It is not necessary to issue a purchase order in respect of leases.
5.33.2. Payment schedules must be agreed with the supplier / leasing company as part of the rental / lease contract.
5.33.3. A copy of the decision approving the lease must be available to national shared
services, or equivalent, when requesting the issue of a payment for each instalment of the lease.
A5.34. Each lease payment must be approved by a manager of the appropriate grade in
compliance with the regulation on receipting of goods / services as set out in these regulations.
A5.35. Monitoring and Reporting
5.35.1. Budget holders must ensure that the creation and ongoing management of leases is properly managed and controlled within their area.
5.35.2. A list must be kept by each budget holder (in electronic format) of all lease contracts
in his area. 5.35.3. The list must summarise the information included on each lease approval decision. 5.35.4. The list must be reviewed and updated monthly and must be signed off as accurate by
the budget holder and forwarded to the National Director of Estates and copied to the relevant Assistant National Director of Finance.
5.35.5. The purpose of this monthly review is to ensure that payments are only made in
respect of current leases where the asset is still in use by HSE.
Health Service Executive National Financial Regulations
Ver 1.3 Page 114 of 176
Related Chapter;on page 56 Appendix ToC ; Page 68
Declaration Form ; Page 167
Mobile Phones
Scope of this Regulation
This regulation applies to all mobile communication devices including:
o Mobile Phones o Blackberry enabled devices o Lap Top phone cards o Palmtops / handheld PDA’s (Personal Data Assistants o Other similar devices
A5.36. Authority to approve assignment of mobile phones.
5.36.1. The assignment of a mobile phone to an individual represents in effect a decision to
expend on average between €500 and €1,500 per annum in addition to an initial cost of perhaps up to €500.
5.36.2. The relevant AND/HNM/LHOM/NHOHM must approve the assignment of a mobile
phone or may, by formal written decision, nominate a manager(s) who will have authority to approve the assignment of mobile phones.
5.36.3. Nominees in this regard must be at Grade VIII level or higher and a copy of the
decision must be forwarded by the AND/HNM/LHOM/NHOHM to the relevant Management team Member and Assistant National Director of Finance.
A5.37. Criteria for determining requirement for a mobile phone
5.37.1. The decision to approve the issue of a mobile phone to an employee should only be made after careful consideration and examination of that employee’s duties:
5.37.2. Mobile phones must only be issued to staff;
1. Who need to be contactable or able to make contact for business purposes
(including accessing the HSE Network) and 2. Whose duties require those officers to be away from their office on a frequent
basis. or
3. Whose personal security while on duty may be enhanced by having access to a mobile phone.
A5.38. Written Decision ; requirement Decision to obtain a mobile phone
5.38.1. A formal written decision of the AND/HNM/LHOM/NHOHM or their nominee is required to assign a phone to any individual.
5.38.2. A copy of each decision assigning a mobile phone must be forwarded to the relevant
Assistant National Director of Finance or their nominee.
Health Service Executive National Financial Regulations
Ver 1.3 Page 115 of 176
5.38.3. Decisions assigning mobile phones must include the following minimum information:
1. Name, grade, title, service and address of staff member 2. Email address and landline phone number of the staff member 3. Basis for requirement of the mobile phone
5.38.4. The details at 1. and 2. above in respect of the staff member’s manager who will be responsible for reviewing and approving the staff members mobile phone bills.
5.38.5. Any exceptions required to the standard restrictions on mobile phones.
A5.39. Ordering and Management of Mobile Phones
5.39.1. There is a basic control requirement to maintain a central record of all mobile phones in operation in the HSE.
5.39.2. The relevant Assistant National Director of Finance must ensure that there is
centralised visibility of:
1. Assignment of mobile phones 2. Replacement / upgrade of mobile phones 3. Restrictions on usage (see below)
5.39.3. To ensure that this process area operates efficiently the only mandatory requirement
is that the relevant Assistant National Director of Finance must receive copies of properly approved requests in respect of the above.
5.39.4. The relevant Assistant National Director of Finance (or nominee) will then arrange for
the mobile phone provider(s) to be advised that it is in order to proceed and supply whatever has been requested.
5.39.5. Once this has been done it is expected that the local area making the request can
deal directly with the provider to arrange delivery etc.
A5.40. Responsibility
5.40.1. Mobile phones are assigned to staff for business use only. 5.40.2. The person to whom a mobile phone has been authorised and issued has a personal
responsibility to ensure proper custody and access to the phone and that calls are made for business purposes only.
5.40.3. All charges or costs not specifically for business purposes must be identified,
quantified and reimbursed to the HSE. 5.40.4. It is the responsibility of budget holders to ensure that mobile phone costs incurred
are:
1. Necessary for the service 2. Represent value for money and 3. Are appropriately monitored and controlled.
Health Service Executive National Financial Regulations
Ver 1.3 Page 116 of 176
5.40.5. This responsibility will be exercised by making appropriate arrangements to ensure
that manager responsible for reviewing and approving their staff members’ mobile phone bills do so in a consistent and timely manner.
5.40.6. In approving the mobile phone bill of a staff member the relevant manager must take
all reasonable steps to satisfy him/herself as to the appropriateness of any charges on HSE as they will be held accountable for the accuracy.
A5.41. Budget Provision
The manager approving the assignment of any mobile phone must ensure that the necessary budgetary provision has been made for the initial and ongoing costs related to the operation of a mobile phone.
A5.42. Usage Requirements/Restrictions
5.42.1. The standard restrictions incorporated into the usage of mobile phones are as follows:
1. Calling restrictions (Limited to the Republic of Ireland only unless exceptional circumstances exist)
2. Premium rate numbers. All premium numbers are barred (e.g. 1550, 1590) from HSE phones.
3. Internet Access
Not granted or restricted to specific public / health sites etc.
5.42.2. The decision to assign a mobile phone must indicate if any exceptions are required to the above and the justification for same.
5.42.3. Where staff members will have infrequent need to use their mobile phone while on
business outside the Republic of Ireland arrangements can be made in advance of any trip to lift the calling restriction temporarily.
A5.43. Guidelines for Usage of Mobile phone
5.43.1. The manager approving the assignment of a mobile phone must ensure that a copy of this regulation is issued to each member of staff in advance of them receiving their mobile phone.
5.43.2. Each mobile phone user must confirm their consent, in writing, to operate the phone in
accordance with this protocol.
A5.44. Property of Health Service Executive. The phone shall at all times remain the property of the HSE.
A5.45. Use and Abuse of Mobile Phones
5.45.1. A mobile phone is issued to a staff member to assist them to perform the duties assigned to their post.
5.45.2. Unnecessary use of the phone to make private calls must be avoided. Charges relating to Private calls must be reimbursed.
Health Service Executive National Financial Regulations
Ver 1.3 Page 117 of 176
5.45.3. Best practice is to be applied at all times in order to obtain best value for money and
limit costs.
5.45.4. These include;
o Landline phones must be used when available. e.g., do not use a mobile phone while sitting at your desk. o The use of mobile phones to make calls when landline phones are available
incurs unnecessary expense on the HSE.
5.45.5. Economical use of mobile phones should be encouraged at all times. e.g. length of call, time of call, type of phone being called etc
5.45.6. Consideration should be made to location, privacy and disruption to those in the
immediate vicinity while using mobile phone.
A5.46. Monitoring of Mobile Phone expenditure
The Budget Holder must put in place procedures to monitor the usage of phones to eliminate misuse and to ensure HSE is reimbursed by staff members in respect of all costs relating to private usage of mobile phones. (See Standard Declaration Form on page 167)
A5.47. Local Mobile Phone Administrator
5.47.1. The Budget Holder must nominate a member of staff to deal with all local administrative matters relating to the usage of mobile phones in their area of responsibility.
5.47.2. All mobile phone users in the area and the relevant Assistant National Director of
Finance must be informed (in writing) as to the name and contact details of the local administrator.
A5.48. Stolen or Lost Phones
5.48.1. Mobile phones which have been stolen or lost must be reported immediately to the nominated local mobile phone administrator by the staff member.
5.48.2. The local administrator must report the incident immediately to the mobile phone
provider and to the Director of Finance.
A5.49. Processing of Mobile Phone Bills
5.49.1. Individual invoices for each phone will be sent by the local administrator to the staff member.
5.49.2. The staff member must identity and calculate the value of private calls made, sign the invoice and return to the local administrator for payment processing.
5.49.3. If not already approved by the manager responsible for reviewing and approving the
staff members’ mobile phone bill the Local Mobile Phone Administrator will arrange for this to be done.
Health Service Executive National Financial Regulations
Ver 1.3 Page 118 of 176
A5.50. Register of Mobile Phones
Each local mobile phone administrator must prepare and maintain (in electronic format) a list of all mobile phones in their area. This list must include the following information:
1. Staff member name, grade, title, service and contact details 2. Mobile phone number 3. Decision number and date authorising assignment of mobile phone 4. Date of issue of Mobile phone 5. PIN and PUK number 6. Billing address and contact name 7. Delivery Address if different from above 8. Name, grade, title, service and contact details of manager responsible for reviewing
and approving the staff members mobile phone bills 9. Date and details of any upgrades 10. Dates and details of any accessories
This information is required to enable the local administrator to reconcile billing from the respective mobile service providers and to assist in resolving any problems in respect of mobile phones.
A5.51. Staff Member Leaving Health Service Executive.
5.51.1. It is the responsibility of the staff member to return their phone to the local mobile phone administrator before they leave the employment of HSE.
5.51.2. It is the responsibility of the staff member to notify the administrators in the area they
are leaving and the area they are joining when they transfer internally within the HSE. 5.51.3. Local mobile phone administrators must ensure that they have visibility of staff with
mobile phones joining or leaving their areas and that the necessary amendments to their mobile phone records are made and notified to the Director of Finance
5.51.4. In the event of a staff member retiring / resigning, that employee may, by agreement, purchase the phone and any ancillary mobile equipment (e.g. car kits) that may have been provided, from the HSE for their current value.
5.51.5. The current value will be advised by the National Director of Finance.
A5.52. Health and Safety
5.52.1. Mobile phone users are advised and requested not to use a mobile phone while driving but rather to pull in safely to the side of the road to make / receive a call.
5.52.2. Unless a mobile phone user is using an appropriate hands free device, it is illegal to
use a mobile phone while driving a vehicle.
Health Service Executive National Financial Regulations
Ver 1.3 Page 119 of 176
Appendix ; on page 68 Related Chapter ; on page 56
Funding provided to Not-For-Profit Agencies (Also referred to as Grants)
A National working Group under the Chair of Ger Crowley (PCCC Assistant National Director,HSE West) is currently in the process of completing draft guidelines ; “Revenue Funding for Voluntary /Community Bodies”. The requirements of these regulations are the minimum controls that apply to funding of Not for Profit/Voluntary agencies. Additional controls or changes requirements may be put in place after implementation of the above draft guidelines. A5.53. Scope of this Financial Regulation
5.53.1. This regulation is intended to cover arrangements entered into with not-for-profit
organisations. 5.53.2. There are various categories of such organisations and they have often been referred
to generically within the health services as voluntary organisations, community organisations, Section 65’s etc.
5.53.3. A common attribute that distinguishes funding of such organisations and our relation-
ships with them from day to day non-pay expenditure is their not-for-profit status. 5.53.4. There are a wide range of differing organisations funded for a variety and, in some
cases, a combination of reasons including:
(i.) Provision of general advocacy, support, policy influencing and related “services” on behalf of a defined client group
(ii.) Provision of specific services to individual named clients on behalf of the HSE
(iii.) Provision of specific services that clients of HSE may avail of.
(iv.) Other Service Provision
5.53.5. Funding of existing levels of service with Voluntary/Not for Profit organisations is considered as ‘Routine’ expenditure for the purposes of expenditure approval. The approval thresholds and respective approvers are set out in Table 2 on page 70. The value of SLA being approved should include direct support by way of financial grant as well as indirect support for example where the organisation may be provided with goods issued from Stores.
5.53.6. Organisations funded for the first time or new or expanded services are treated as
Non Routine expenditure and require a high level of approval.(refer Table 2 page 70 ).
A5.54. The range of funding mechanisms involved is varied and may include:
5.54.1. General “grant” funding as a full or partial contribution towards the costs of the
services being provided or the running costs of the organisation providing the services.
5.54.2. Funding linked directly to the agreed cost of providing the service on a per client or
per-capita basis.
Health Service Executive National Financial Regulations
Ver 1.3 Page 120 of 176
5.54.3. Funding linked to the total cost of service provision related to specific staff numbers and related non-pay costs of the organisation.
5.54.4. Other funding basis.
A5.55. General Requirement with regard to Not For Profit Organisations When entering into arrangements with any provider of services including not-for-profit organisations the Health Services Executive must ensure that value for money is obtained and that there is full clarity in relation to:
5.55.1. What services are being provided by the organisation.
5.55.2. Any specific or general obligations on the organisation around their provision of services.
5.55.3. The level of funding that the HSE is required to provide to the organisation in return
for its satisfactory provision of services.
5.55.4. Any specific or general obligations on the HSE around the services provided and their funding.
5.55.5. HSE must satisfy itself that funded organisations have adequate governance systems
in place commensurate with the nature and scale of their operations. In summary, every Budget Holder must be in a position to identify clearly what services are being provided in return for the funding which they or their nominees expend including funding given to not-for-profit organisations.
A5.56. Application of Purchasing regulation to funded bodies
Please refer to section 2.10 on page 22 which sets out the purchasing requirements for bodies funded by the HSE.
A5.57. Management of the relationship with Not-for-Profit organisations
5.57.1. This relationship is in effect a contractual relationship and should be subject to the
appropriate levels of ongoing monitoring and management by the relevant Budget Holder or his/her nominee.
5.57.2. Compliance with this regulation requires that, in respect of each funded organisation, there are appropriate levels of:
Direct interaction with the organisation including meetings where necessary to deal with;
a. Agreement of the quantum and specification of services to be provided and related resource input for the year ahead.
b. Ongoing review and management during the year of any service or resource issues that may arise.
c. Monitoring / Evaluation / Inspection of the Service being provided as appropriate.
d. Any other issues
Health Service Executive National Financial Regulations
Ver 1.3 Page 121 of 176
A5.58. Proper documentation systems must be put in place to support the HSE in complying with 1.a to 1.d. above and to provide a record for future audit.
This documentation should include:
o Service Level Agreements or equivalent o Minutes of Meetings o Correspondence o Service activity information or equivalent o Financial Information / reports (see below) o Staffing Information (where relevant) o Other relevant documentation
A5.59. Service Level Agreements (SLA)
In essence a Service Level Agreement (SLA) is an agreement reached between the HSE and the organisation providing the services which is designed to formalise a common shared understanding about service delivery, priorities, responsibilities and issue resolution. In putting in place SLA’s an appropriate balance must be struck between:
a. Respecting the ethos and autonomy of the not-for-profit organisation
and b. Ensuring that HSE can fulfil its obligations around the quality assurance of
services it funds and accountability as well as probity around the utilisation of funds.
A5.60. Service Level Agreements – Mandatory requirements
The following areas must at a minimum be referenced in each SLA with the level of detail and emphasis in each case being commensurate with the nature and the scale of services being provided:
5.60.1. Service Provision - Description of the services to be provided including, as
appropriate:
o Clients / client groups to receive service o Protocols around how clients access services o When services are to be available o Service Volumes / Activity levels o Service limits / protocol around clients exiting the service o Integration with HSE or other services
5.60.2. Service Monitoring / Management Arrangements in relation to:
o Approval of new / expanded services o Reduction / termination of services o Information to be provided to HSE in respect of services and regarding
issues arising in respect of services. o Insurance / indemnity provisions. o Information requirements of the organisation providing services
Health Service Executive National Financial Regulations
Ver 1.3 Page 122 of 176
o Quality assurance / Risk Management encompassing compliance with standards of service provision including statutory requirements, codes of practice etc
o Inspection / Evaluation including external inspection / evaluation of services where appropriate
5.60.3. Resource Inputs including arrangements in relation to:
o Funding to be provided by HSE o Timing of payments by HSE o Other funding sources including internal resources of the organisation o The process for agreeing new funding or funding reductions including the
setting of a budget for the services and ongoing monitoring of performance against that budget
o Agreeing, as appropriate, necessary staff resources to provide and support service provision
o Financial and Staffing information to be provided at agreed frequencies to HSE
o Information required by the organisation from HSE in respect of resources
5.60.4. Other Matters that need to be covered including:
o Corporate Governance arrangements within the organisation providing the service
o Client Confidentiality o Health and Safety o Insurance o General requirement for confirmation of compliance with all statutory
requirements including employment and tax legislation o Freedom of Information / Data protection o Human resource policies and procedures o Key Contacts / responsible persons for different aspects of the SLA o Dispute resolution arrangements o Access by appropriately authorised HSE staff to verify supporting
documentation
A5.61. Formal Visits with SLA recipients - Requirements
5.61.1. A meeting must be held at least once per year with every relevant organisation that receives in excess of €50,000 per annum in HSE funding. This meeting should, as regards resource inputs, address funding utilisation in the previous year and funding requirements for the year ahead.
5.61.2. Organisations that receive funding in excess of €500,000 per annum must be met at
least twice per annum. Where two meetings only are held one of these is intended to allow for a mid-year review and consideration of the resource position to year-end and should be held in the 3rd quarter of the year.
A5.62. New or Expanded Services
5.62.1. SLA’s must make it clear that HSE is under no obligation to provide funding for
new or expanded services that have occurred without its prior agreement to funding.
Health Service Executive National Financial Regulations
Ver 1.3 Page 123 of 176
5.62.2. Clearly the HSE respects the autonomy of not-for-profit organisations to commence
or expand services at their own discretion assuming compliance with statutory requirements.
5.62.3. However organisations must equally respect the HSE position that it can only be
expected to provide funding where it has agreed in advance to do so.
A5.63. HSE must reserve the right to reduce funding where services are reduced or are
not provided in accordance with the SLA.
A5.64. SLA’s must provide that the following mandatory information requirements can be met:
i. Preparation and submission to the HSE of audited accounts for the organisation
ii. Audited accounts should separately identify the actual funding received from HSE
during the financial year in question.
iii. Submission of tax clearance and / or charitable status documentation on initial engagement and at least annually thereafter.
iv. In respect of organisations that receive in excess of €500,000 per annum
submission of reports on financial performance against budget for services funded by the HSE.
These must be received no less than quarterly and must be accompanied by information as to any issues that have or are likely to give rise to a budget overrun and proposals to address same and ensure services are within budget by the year end.
v. Where relevant, information in relation to staffing numbers engaged in respect of
provision of services funded by HSE including information to assist in validating claims for funding of pay awards.
Health Service Executive National Financial Regulations
Ver 1.3 Page 124 of 176
Related Chapter ; en page 62 Appendix ToC ; en page 68
Related Chapter; (5) CAPITAL PROJECTS and PROPERTY TRANSACTIONS
Topic 1; CAPITAL PROJECT APPROVAL PROTOCOL Issued by Estates Directorate 2006
The following protocol should be read in conjunction with the related chapter in the main body of this document (on page 62). I
It is important to reiterate that a project should not considered approved until such time as formal notification has been provided by the Finance Directorate. INTRODUCTION Following the transfer of responsibility and authority for the Health Services Capital Expenditure Programme to the HSE from the Department of Health and Children, it is necessary to put in place protocols to ensure that there is proper governance of capital projects. It is also important to ensure that the protocols will enable the efficient management of capital projects. The HSE is required as part of the service plan to “indicate any capital plans proposed by the HSE” for the approval of the Minister for Health. The HSE also requires the written permission of the Minister to enter into any agreement or arrangements in respect of capital spending or an undertaking if the total amount spent on the undertaking would exceed an amount that may be specified from time to time by the Minister with the consent of the Minister for Finance. The Board of the HSE has delegated to the CEO approval of contracts other than those in excess of €10m. The Estates Directorate will manage the capital programme on behalf of HSE Corporate and regionally. The HSE Capital Planning Group has been established to formulate and coordinate the Capital Plan. The group consists of representatives of the NHO and PCCC service pillars, Estates and Finance Functions. Approval Procedures
The following sets out the approval procedures with which HSE Areas must comply with prior to committing Capital Funding to a project. The guidelines for the Appraisal and Management of Capital Expenditure Proposals in the Public Sector issued by the Department of Finance in January 2005 shall also apply. The projects are divided into different categories depending on the capital cost of the project:
Band Project Cost A less than €500,000 B €500,000 - €5,000,000 C €5,000,000 - €20,000,000 D greater than €20,000,000 The capital cost of a project is the total project cost including VAT. The total project cost includes construction costs, design fees, equipment costs and miscellaneous costs associated with the project. Band A (minor capital and projects less than €0.5m)
Band A projects will include all Minor Capital projects and projects with a total project value of less than €500,000. A list of these projects will be submitted to HSE Corporate for approval within the Capital Plan and once the list of projects is approved no further approval is required.
Health Service Executive National Financial Regulations
Ver 1.3 Page 125 of 176
Topic 1; Capital Projects Approval Protocol … Continued This approval is subject to the following conditions 1 Expenditure on the list of projects cannot exceed the allocation for that year. 2 The maximum carryover of contractual commitments cannot exceed 50% of the current year’s
allocation 3 .Any substitutions on the list must be agreed with the Network Manager (NHO) or LHO manager
(PCCC) and Area Assistant Director of Estates. 4 Any variation on projects must be approved by the Area Assistant Director of Estates. 5 All public procurement directives/guidelines must be complied with. 6 All stages of the projects must be agreed locally and approved by the Area Assistant Director of
Estates. The Assistant Director of Estates shall, at the end of each calendar quarter, submit to the National Director of Estates a report on the list of projects indicating progress and cost performance. Updated cash flow forecast will be part of this report. Band B (€0.5m to €5m) Projects with an estimated total project value exceeding €500,000 but not exceeding €5,000,000 The HSE Area must apply to HSE Corporate for approval for all projects in this category. An individual submission is required for each project. The submission must include the following:
• Project Brief • Option Appraisal study that justified the proposed investment as part of the preferred option for the
required service. • Estimated final project cost for the project (Q Cost). • Year by year cashflow forecast of expenditure. • Project Programme • Revenue costs and WTE associated with the project. HSE Corporate will issue an approval for the project subject to consideration of service priorities and available funding N 21. No further approvals will be required subject to the following conditions. 1 Total expenditure on the project cannot exceed the approved allocation. 2 Yearly expenditure should be within 10% of projected cash flow. 3 Any variation on projects must be approved by the Area Assistant Director of Estates and within the
approved allocation for the project. 4 All public procurement directives/guidelines must be complied with. This includes complying with
EU procurement directives where appropriate. 5 All stages of the project must be agreed with the local service (i.e. Hospital Network or LHO) and
Area Assistant Director of Estates.
The Area Assistant Director of Estates shall, at the end of each calendar quarter, submit to the National Director of Estates a report on the project indicating progress and cost performance. Updated cash flow forecast will be part of this report.
Band C (€5m - €20m) Projects with an estimated total project value exceeding €5m but not exceeding €20m. The HSE Area must apply to HSE Corporate for approval for all projects in this category. An individual submission is required for each project. The submission must include the following:
• Project Brief • Option Appraisal study that justified the proposed investment as part of the preferred option for the
required service.
N21 Notification of project approval (letter of approval) must be provided by the Finance Directorate (National Director of Finance or relevant Assistant National Director of Finance)
Health Service Executive National Financial Regulations
Ver 1.3 Page 126 of 176
Topic 1; Capital Projects Approval Protocol … Continued • Estimated final project cost for the project (Q Cost). • Year by year cash flow forecast of expenditure. • Project Programme • Revenue costs and WTE associated with the project. HSE Corporate will issue written approval to the commencement of the project of the basis of the foregoing data subject to consideration of service priorities and available funding. The commencement covers • Selection of a Design Team and proceeding with design to Stage 2 (Sketch Schemes).
The HSE Area must obtain HSE Corporate approval for the Stage 2 of the project before proceeding with developing the project further. The Stage 2 submission will include equipment schedules which will also be approved at this stage. After receiving approval for the Stage 2 the HSE Area may advance the project up to and including the preparation of the tender documents. All stages of the project must be agreed with the local service (i.e. Hospital Network or LHO) and Area Assistant Director of Estates. The HSE Area must obtain HSE Corporate approval to seek tenders for the project. The submission seeking approval must include the following:
• Reports on the tender process proposed. • If the restricted process is proposed a report on the selection process used to finalise the list of
tenderers. • A cost check based on completed documentation reconciled with the original estimate upon which
the commencement approval was based. • A statement that the tender documents have been examined by the Area Assistant Director of
Estates and that the documentation is considered satisfactory.
After receipt of the tenders for the project, the Area Assistant Director of Estates must submit the tender report to HSE Corporate for approval to accept the tender. Please note that the approval of the Board of the HSE is required to accept tenders in excess of €10m. Approval to accept the tender is subject to the following conditions.
1 Total expenditure on the project cannot exceed the approved allocation. 2 Yearly expenditure should be within 10% of projected cash flow. 3 Any variation on projects must be approved by the Area Assistant Director of Estates and must be
within the approved allocation for the project. 4 All public procurement directives/guidelines must be compiled with. This includes compliance with
EU procurement directives where appropriate. The Area Assistant Director of Estates shall, at the end of each calendar quarter, submit to the National Director of Estates a report on the project indicating progress and cost performance. Updated cash flow forecast will be part of this report. Band D (greater than €20m) Projects with an estimated total project value exceeding €20m. The HSE Areas must apply to HSE Corporate for approval for all projects in this category. An individual submission is required for each project. The submission must include the following: • Project Brief • Option Appraisal study that justified the proposed investment as part of the preferred option for the
required service. • Estimated final project cost for the project (Q Cost). • Year by year cash flow forecast of expenditure. • Project Programme • Revenue costs and WTE associated with the project.
Health Service Executive National Financial Regulations
Ver 1.3 Page 127 of 176
Topic 1; Capital Projects Approval Protocol … Continued
The HSE is obliged to make a submission to the Board of the HSE and to the Minister for Health to obtain approval to proceed with the project. The submission will include
• The reasons why the particular project is considered a priority. • Complies with overall strategy for the provision of a service. • Estimated revenue or operating cost consequences of the proposal. • A statement that the project is affordable within the Capital Plan.
The HSE is also obliged to seek the advice of the National Development Finance Agency on the optimum means of financing the cost of the project. On receipt of written approval from the Department of Finance the HSE National Director of Finance (or nominee) will issue written approval to the commencement of the project of the basis of the foregoing data subject to consideration of service priorities and available funding. The commencement covers
• Selection of a Design Team and proceeding with design to completion of Stage 2.
The HSE Area must make a submission for written approval for each of the following design stages.
• Detailed Sketch design including equipping list (Stage 3) After receiving approval for the Stage 3 the HSE Area may advance the project up to and including the preparation of the tender documents. All stages of the project must be agreed with the local service (i.e. Hospital Network or LHO) and the Area Assistant Director of Estates. The HSE Area must obtain HSE Corporate approval to seek tenders for the project. The submission seeking approval must include the following:
• Reports on the tender process proposed. • If the restricted process is proposed a report on the selection process used to finalise the list of
tenderers. • A cost check based on completed documentation reconciled with the original estimate upon which
the commencement approval was based. • A statement that the tender documents have been examined by the Area Assistant Director of
Estates and that the documentation is considered satisfactory. The HSE is obliged to make a submission to the Department of Finance to obtain approval to proceed to tender. On receipt of approval from DoHC, the National Director of Finance (or nominee) will issue a letter to obtain approval to proceed to tender. After receipt of the tenders for the project, the Area Assistant Director of Estates must submit the tender report to HSE Corporate for approval to accept the tender. Please note that the approval of the Board of the HSE is required to accept tenders in excess of €10m. Approval to accept the tender is subject to the following conditions.
1 Total expenditure on projects cannot exceed the approval allocation. 2 Yearly expenditure should be within 10% of projected cash flow. 3 Any variation on projects must be approved by the Area Assistant Director of Estates and must be
within the approved allocation for the project. 4 All public procurement directives/guidelines must be compiled with. This includes compliance with
EU procurement directives where appropriate. The Area Assistant Director of Estates shall, at the end of each calendar quarter, submit to the National Director of Estates (and copy to the Assistant National Director of Finance, Capital) a report on the projects indicating progress and cost performance. Updated cash flow forecast will be part of this report.
Health Service Executive National Financial Regulations
Ver 1.3 Page 128 of 176
Topic 2; Protocol for Acquisition and Disposal of Property Issued by Property Sub Committee, Approved b y HSE Board- March 2006
HSE, Protocol for the Acquisition and Disposal of Property
26th January 2006 1. Introduction
As of 1st January 2005, all property previously held by any of the health boards became vested in the Health Service Executive (“HSE”).
This protocol sets out the procedure to be followed when the HSE acquires or disposes of any property (whether freehold or leasehold) or interest in property. Terms used in this protocol are defined in Schedule 8, on Page 157
This protocol does not extend to the acquisition of land by compulsory purchase order. The Authority is permitted to compulsorily acquire land pursuant to section 78(1) of the Health Act, 1947 (as amended by Section 75 of the 2004 Act). This protocol does not extend to the provision of affordable housing.
2. Delegations
The CEO is directly responsible to the Board but, subject to any directions the CEO may receive from the Board, he may in writing delegate any of his functions22 to employees of the HSE specified by name, position or otherwise, and authorise the subdelegation of any or all delegated functions to or by other such employees.
Delegations and subdelegations of functions are to be taken to include the delegation or subdelegation of any duty or power incidental to or connected with that function23.
The [draft] delegations from the Board to the CEO and from the CEO to the National Directors in relation to the acquisition and disposal of property are set out in Schedule 1.
3. Relevant Statutory Provisions
The key statutory provisions of the consolidated Health Acts that are or may be relevant to this protocol are set out in Schedule 2.
4. Other Relevant Matters
In addition to the matters discussed in this protocol, in considering the acquisition or disposal of any property or interest in property, the relevant employee of the HSE must consider:
4.1 Whether the contemplated transaction falls within the ambit of any function reserved to the Board of the HSE, the Chief Executive Officer or a National Director.
4.2 How the interests of the HSE in retaining assets funded by the HSE within the healthcare system, and securing a proportionate interest for the HSE in the increased value of any asset upon subsequent realisation are to be protected. This should be considered both in determining the structure of the transaction (e.g. sale and leaseback, purchase and declaration of trust, etc) and the contents of the related documentation (e.g. whether any restrictive covenants, negative pledges, charges, etc are required to protect the HSE’s interests).
N22 The CEO’s functions are set out in Section 18(1) of the 2004 Act: (a) to carry on, manage and control the administration and business of the HSE, (b) any other functions assigned by the Act or delegated by the Board and (c) to supply the Board with information. N23 Section 76 of the 2004 Act.
Health Service Executive National Financial Regulations
Ver 1.3 Page 129 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
For example, tenants of residential premises may avail of a procedure under either the Landlord and Tenant (Ground Rents) Act, 1967 (the “1967 Act”) or the Landlord and Tenant (Ground Rents) No. 2 Act, 1978, and tenants of business premises may avail of a procedure under the 1967 Act to purchase the freehold interest in the relevant property. The HSE is not currently among the bodies excluded from the ambit of this legislation and, accordingly, tenants of the HSE may seek to acquire the freehold interest in property leased by them from the HSE. This would be detrimental to the interests of both the HSE and the State as it can operate to remove important assets from the healthcare system at a significant discount to their market value. Consequently, care should be taken to ensure that any new leases granted by the HSE cannot become qualifying leases for the purposes of this legislation through careful drafting of the relevant lease agreements in each case.
4.3 Any general or specific written directions issued by the Minister which may be relevant to the proposed transaction (Section 10 of the 2004 Act).
4.4 Whether the proposed transaction is consistent with the terms of the HSE’s corporate plan and the service plan (including the capital plan) for the relevant financial year.
4.5 Whether the proposed transaction would involve capital expenditure in excess of the level specified from time to time by the Minister with the consent of the Minister of Finance (Section 34 of the 2004 Act). If so, ministerial consent is required.
4.6 Any regulations made by the Minister for any purposes set out in the 2004 Act. At the time of writing no regulations relevant to property disposals or acquisitions have been made.
4.7 If the transaction would require the HSE Seal to be applied to any document, the Protocol for the Use of the HSE Seal.
4.8 The Code of Practice for the Governance of State Bodies (2001), in particular Section 5 of that Code. Schedule 4 to this protocol includes a detailed summary of the provisions of Section 5. In summary, specific Board approval is required where an asset is disposed of or a grant of access to property for commercial arrangements with third parties is made and the anticipated value of the transaction is at or above EUR70,000, unless the disposal or grant is undertaken by way of auction or competitive tendering process. Disposals of assets to members of the HSE’s Board, or employees of the HSE, or their connected persons may also require Board approval.
4.9 The Guidelines for the Appraisal and Management of Capital Expenditure Proposals in the Public Sector (Department of Finance, 2005).
4.10 Any other codes of conduct or governance adopted by the HSE from time to time.
4.11 The implications of the anticipated transaction in terms of rates (see Schedule 5 for more detail), VAT and stamp duty (see Schedule 6 for more detail) and the implications of the anticipated transaction for the HSE in terms of VAT and stamp duty (see Schedules 6 and 7 for more detail).
5. Procedure for the Acquisition or Disposal of Property or Interests in Property
With respect to any proposed transaction in relation to property or an interest in property, the Manager must first consider whether the transaction would be a:
5.1 Category 1 Transaction (equal to or less than EUR1 million exclusive of VAT and Service charges);
5.2 Category 2 Transaction (in excess of EUR1 million but equal to or less than EUR2 million exclusive of VAT and Service charges ); or
5.3 Category 3 Transaction (in excess of EUR2 million exclusive of VAT and Service charges).
Health Service Executive National Financial Regulations
Ver 1.3 Page 130 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
For these purposes, the value of the lease is deemed to be the annual rental costs payable pursuant to the lease multiplied by the duration in years of the lease.
6. Category 1 Transactions
6.1 The Manager e.g. LHO or other equivalent will submit a Business Proposal to the relevant Assistant National Director e.g. Ass/ PCCC, requesting clearance to develop a Business Case. Each Directorate is responsible for initial assessment of Business Proposals before advancing to Business Case stage.
“Business Proposal” means a written document including the following information:
(a) Care group purpose
(b) Brief outline identifying the needs requirement (including associated risk analysis) linked to corporate and/or strategic plans for service
(c) The revenue funding implications (e.g. existing / new / increase), as appropriate.
(d) WTEs required (e.g. existing / new / increase), as appropriate.
(e) Preliminary Option Appraisal (e.g. replacement / expansion / new)
(f) Linkage requirement to other services / community / special conditions
(g) Funding approval to date / applications made as appropriate
(h) Capital funding implications (e.g. existing / new / increase) as appropriate.
6.2 The Assistant National Director will or will not grant clearance to the Manager to develop a Business Case. The decision shall be notified in writing.
6.3 On grant of clearance from Assistant National Director to the Manager for development of a Business Case, the Manager will do so in accordance with HSE guidance.
“Business Case” means a written document including the following information:
(a) Option Appraisal is essential. Consider options that address service needs and objectives (e.g. demographics/ location/ etc.) and development costs. If the proposed transaction is an acquisition, provide evidence of the requirement for increased/ replacement accommodation. If the proposed transaction is a disposal, evidence of the reduced/ replacement requirement for accommodation, identifying impact on service delivery.
(b) Evidence of alignment of the proposed transaction with the objectives of the HSE’s service plan and capital plan.
(c) Identify property type, location and approximate size (include map).
(d) Technical report, providing support as to the appropriateness of property proposal to be acquired for its intended use, identifying and cost all necessary improvement measures e.g. alterations, fire safety precautions etc.
(a) If it is proposed to acquire or dispose of a freehold or leasehold property, an explanation of why freehold or leasehold acquisition or disposal is appropriate (e.g. if granting a lease to a third party over HSE property, explain proposal option rather than disposing of the property entirely), together with a detailed cost/ revenue projections in relation to such acquisition or disposal.
Health Service Executive National Financial Regulations
Ver 1.3 Page 131 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
(b) If the proposed transaction is the grant of a lease or the acquisition of leasehold property, details of the proposed term and covenants of the lease.
(c) Valuation report from Valuation Office or, where the Valuation Office has confirmed to the Manager in writing that it will not be able to provide a valuation report within the required timeframe, a valuation from an alternative valuer.
(d) If necessary, a legal opinion should be obtained to guide negotiation process and protect interests of HSE for larger/ more complex transactions. Legal advice shall be necessary at conveyance stage.
(e) Source of capital and ongoing revenue funds and impact on revenue budget.
(f) Detail on WTE implication.
(g) Alternative options considered with costs and other advantages/disadvantages associated with such options. Provide VFM report and risk analysis.
(h) A proposed programme for actions and expenditure, stating all assumptions.
In preparing the Business Case, expert advice may be required:
• Technical:
HSE areas, Technical Services/ Capital Project personnel will provide, the in-house engineering technical advice and carry-out a conditional survey, option appraisals in conjunction with service personnel for the properties. The conditional survey will report on: (i) Appropriateness for proposed occupants/ use. (ii) fire safety compliance, (iii) health and safety issues, (iv) essential remedial measures required (with associated costing), (v) compliance with local authority planning and building control, and (vi) any relevant local authority or site specific development plans.
Where external technical expertise (e.g. an architect, engineer or quantity surveyor) is required, the relevant expert shall be selected from the appropriate panel maintained by HSE.
• Auctioneering:
Valuations shall be sought from external valuers only where the Valuation Office has confirmed to the Manager in writing that it will not be able to provide a valuation report within the required timeframe. HSE shall maintain panel of valuers. The expertise of the valuers on the panel may be drawn on to explore options with respect to the acquisition or disposal of the property in question, in accordance with the service specification, available funding, valuation guidance and procurement regulations. Cognisance of local knowledge with ability to verify advice against national norms and provide a competitive pricing proposal for various services shall be among the selection criteria for specific assignments.
• Legal:
Legal opinion should be obtained to guide negotiation process and in the protection of the HSE interest for larger/ more complex transactions. Legal advice shall be necessary at conveyance stage in property transactions. HSE has limited internal legal advice available and shall develop and maintain a panel for legal advice services.
6.4 The completed Business Case for a property transaction shall be submitted by the Property Contact person for the area, on behalf of the relevant manager to the HSE corporate property section, for recommendation by the Property Committee.
Health Service Executive National Financial Regulations
Ver 1.3 Page 132 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
6.5 The Property Committee shall review the Business Case for property transactions. In each
situation the Property Committee shall either,
• Seek further information in writing, for review at subsequent meeting; Or • Recommend the transaction described in the Business Case for approval to the
relevant National Director in writing (draft decision paper attached); Or • Recommend rejection of the Business Case to National Director in writing.
6.6 The relevant National Director will approve or reject the property transaction recommended by the Property Committee The National Director will notify the HSE corporate property section of the decision in writing and attach a copy of signed decision paper if the transaction is approved.
6.7 The HSE corporate property section will advise the responsible manager in writing the decision of the National Director including conditions. In addition the detail of the decision, for the property transaction shall be entered into national property transaction database. Approved transactions shall be notified to the secretary of the HSE Board, as approved Category 1 Transactions, for notification to the Board24.
6.8 On receipt of formal approval for the property transaction, from HSE corporate, the Manager in conjunction with the legal advisors shall conclude negotiations based on submission reviewed by Property Committee and prepare contract documents for the approved Category 1 Transaction. Once these documents are in final form, they will be executed in accordance with the HSE’s Sealing Protocol.
7. Category 2 Transactions
7.1 Paragraphs 6.1 to 0 of the procedure for Category 1 Transactions apply.
7.2 The relevant National Director shall endorse or reject the Property Committee recommendation. The National Director notifies the HSE corporate property section of his/ her endorsement of the recommendation to approve the transaction by the return of the signed draft decision paper or on the decision otherwise in writing.
7.3 For a transaction proposal endorsed by the National Director, the draft decision paper signed by National Director shall be forward to the CEO, by the HSE corporate property section for his approval or rejection. The draft decision paper shall be accompanied by an executive summary of the business case, for briefing purposes.
7.4 Recommendations of the Property Committee that do not have the continued support of the National Director shall be notified to the HSE corporate property section in writing. The corporate section shall advise the Manager of the National Director decision. A copy of the notification shall issue to the CEO for information.
7.5 The CEO will approve or reject the Category 2 Transaction, recommended by the Property Committee and endorsed by the National Director. The CEO’s office shall notify the HSE corporate property section of the decision in writing and attach a copy of signed decision paper if the transaction is approved.
The HSE corporate property section will advise the Manager in writing, copied to the National Director, of the CEO’s decision, including any conditions or restrictions. In addition the detail of the decision of the CEO and the National Director, for the property transaction shall be entered into national property transaction database. Approved transactions shall be notified to the secretary of the HSE board,
N24 Re. The Code of practice for Governance of State Bodies (2001), in particular Section 5 of that Code.
Health Service Executive National Financial Regulations
Ver 1.3 Page 133 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
as approved Category 2 Transactions, for notification to the Board N25.
7.6 On receipt of formal approval for the property transaction, from HSE corporate, the Manager in conjunction with the legal advisors shall conclude negotiations based on submission reviewed by Property Committee and prepare contract documents for the approved Category 2 Transaction. Once these documents are in final form, they will be executed in accordance with the HSE’s Sealing Protocol.
8. Category 3 Transactions
8.1 Paragraphs 7.1 to 7.4 of the procedure for Category 2 Transactions apply.
8.2 The CEO shall endorse or reject the Property Committee recommendation which is initially endorsed by the relevant National Director, prior to submission for approval by the HSE Board. The CEO’s office notifies the HSE corporate property section with the return of the signed draft decision paper or on the decision otherwise, in writing.
8.3 The Manager seeking approval will prepare a briefing note for the Board on the transaction, to be circulated with the board papers in advance of the next meeting of the Board. The briefing note will include as appropriate the following standard information:
(a) Purpose of Category 3 Transaction
(b) Identify service plan and/ or strategic basis for scheme, include service benefits and risk analysis
(c) Identify capital funding source, as appropriate.
(d) Identify revenue cost impact and source, as appropriate.
(e) Identify staffing implications and approval, as appropriate
(f) Verify option appraisal completed
(g) Verify that assessments were completed, as appropriate e.g. legal, technical, financial, VFM
(h) Confirm adherence to public procurement procedures and Guidelines for the Appraisal and Management of Capital Expenditure Proposals in the Public Sector (Department of Finance, 2005)
At the request of a board member (notified to the secretariat in advance of the meeting), the CEO, the relevant National Director or a nominee, will attend the Board meeting or meet with some or all members of the Board by arrangement, to address issues raised by the Board or individual members.
8.4 The Board will approve or reject the Category 3 Transaction, recommended by the CEO. The secretary to the Board shall arrange for notification to the HSE corporate property section, of the decision in writing and attach copy of decision paper signed by 2no. Board members.
N25 Re. The Code of practice for Governance of State Bodies (2001), in particular Section 5 of that Code.
Health Service Executive National Financial Regulations
Ver 1.3 Page 134 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
8.5 The HSE corporate property section will advise the responsible manager in writing, copied to the National Director, of the Boards’ decision including any conditions or restrictions. In addition the detail of the Board, CEO and National Director’s decisions, for the property transaction shall be entered into national property transaction database.
8.6 On receipt of formal approval for the property transaction, from HSE corporate, the Manager in conjunction with the legal advisors shall conclude negotiations based on submission reviewed by Property Committee and prepare contract documents for the approved Category 3 Transaction. Once these documents are in final form, they will be executed in accordance with the HSE’s Sealing Protocol.
Health Service Executive National Financial Regulations
Ver 1.3 Page 135 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
Schedule 1 Delegations
DRAFT FOR SIGNATURE
Delegation by the Board to the Chief Executive Officer
Delegation Order
The Board resolved at its meeting on 1st January 2005 to make the delegation of all functions assigned to the Executive under the Health Act, 2004 and previous Acts as listed in Schedule 1 and 3 of the Health Act, 2004 to the Chief Executive Officer with the exception of functions reserved at the time by the Board including, inter alia, the approval of acquisitions and disposals of land (Section 6(2)).
Pursuant to Section 12 of the Health Act, 2004 the Board resolved at its meeting of 2ndFebruary 2006 to delegate the function listed below to the Chief Executive Officer.
• Approval of acquisitions and disposals of land (Section 6(2)).
Exclusions:
• Approval of acquisitions and disposals of lands wherein the transaction value exceeds €2 Million exclusive of V.A.T. and Service Charges.( ie Category 3 Transactions)
Note: For this purpose, the value of the lease is deemed to be the annual rental costs payable pursuant to the lease multiplied by the duration in years of the lease.
• All reserved functions of the Board.
Subject to:
• The provisions of the HSE, Property Acquisitions and Disposal Protocol. • The general provisions of the approved annual National Service, Capital and
Corporate Plans and the specific resources and targets relevant to the HSE. • The policies, procedures and codes of practice adopted by the HSE. • The Code of Practice for the Governance of State Bodies (2001), in particular
Section 5 of that Code. • The Guidelines for the Appraisal and Management of Capital Expenditure
Proposals in the Public Sector (Department of Finance, 2005).
The Board hereby authorises the sub-delegation of any function delegated to the Chief Executive Officer pursuant to this Delegation Order to or by other employees or the Executive. A person acting in the role of Chief Executive Officer has the same delegated authority and accountability as the substantive post holder for the duration of the acting period. Any dispute as to whether or not a function has been delegated to the Chief Executive Officer will be decided by the Board of the Health Service Executive. Signed: Chairperson – Board of the Health Service Executive Date:
Health Service Executive National Financial Regulations
Ver 1.3 Page 136 of 176
Chapter 5, Topic 2 Protocol for Acquisition and Disposal of Property … Continued
DRAFT FOR CONSIDERATION
Delegation by the Chief Executive Officer to the National Directors Under the Health Act 2004 the Board is the governing body of the Health Services Executive (the “Executive”) with the authority to perform the functions of the Executive. Pursuant to Section 12 of the Health Act 2004 the Board has delegated all functions assigned to the Executive under the Health Act 2004 (with the exception of certain reserved functions) to the Chief Executive Officer.
Section 18(1) of the Health Act 2004 provides that the Chief Executive Officer, shall ‘carry on and manage and control generally the administration and business of the Executive’ and perform other functions assigned under the Health Act 2004 or any other enactment or as may be delegated to him by the Board. The Chief Executive Officer may, subject to any directions issued by the Board, delegate any of his functions to employees of the Executive and authorise the sub-delegation of delegated functions to or by employees of the Executive.
Any function delegated or sub-delegated to an employee is to be performed by the employee under the general direction and control of the Chief Executive Officer, or the employee who sub-delegated the function, and does not preclude the Chief Executive Officer, or the employee who sub-delegated the function, from performing that function.
Delegation Order
Pursuant to Section 19 of the Health Act, 2004, I, [ ], as Chief Executive Officer of the Health Service Executive, hereby delegate the following function to you, as National Director of [ ] (the “Directorate”).
• The approval of acquisitions and disposals of land within your area of responsibility (Section 6(2) of the Health Act, 2004).
Exclusions:
• Approval of acquisitions and disposals of lands wherein the transaction value exceeds €1 Million exclusive of V.A.T. and Service Charges.(i.e. Category 2 or 3 Transactions) Note: For this purpose, the value of the lease is deemed to be the annual rental costs payable pursuant to the lease multiplied by the duration in years of the lease.
• All reserved functions of the Board. Subject to:
• The provisions of the HSE, Property Acquisitions and Disposal Protocol. • The general provisions of the approved annual National Service, Capital and Corporate
Plans and the specific resources and targets relevant to the HSE. • The policies, procedures and codes of practice adopted by the HSE. • The Code of Practice for the Governance of State Bodies (2001), in particular Section 5 of
that Code. • The Guidelines for the Appraisal and Management of Capital Expenditure Proposals in the
Public Sector (Department of Finance, 2005). • The general directions of the Chief Executive Officer.
A person acting in the role of National Director [ ] has the same delegated authority and accountability as the substantive post holder for the duration of the acting period. This Delegation Order should be read in conjunction with all previous delegation orders by the Board of the Executive to the Chief Executive Officer. Any dispute as to whether or not a function has been delegated to a National Director will be decided by the Chief Executive Officer. I hereby revoke all existing Delegation Orders relating to the matters set out above. Signed: Chief Executive Officer – Health Service Executive Date:
Health Service Executive National Financial Regulations
Ver 1.3 Page 137 of 176
Chapter 5, Topic 2, Protocol for Acquisition and Disposal of Property … Continued
Schedule 2 Statutory Provisions
1. Health Act 2004
1.1 Section 6(2)(b)
The HSE may, subject to the Health Acts 1947 to 2001, acquire, hold and dispose of land or an interest in land.
1.2 Section 7(5)(d) and (e)
In performing its functions, the HSE shall have regard to the resources that are available for the purpose of such performance, and the need to secure the most beneficial, effective and efficient use of those resources.
1.3 Section 10
The HSE shall comply with any general or specific written directions issued by the Minister.
1.4 Section 25
In performing the functions of the HSE, employees must maintain proper standards of integrity, conduct and concern for the public interest and shall comply with any relevant code of conduct.
1.5 Section 26
Employees of the HSE must not disclose confidential information (including proposals of a commercial nature or tenders submitted to the HSE) unless authorised by the HSE, or disclosed to the Board of the HSE or the Minister or otherwise in compliance with law.
1.6 Sections 28-30
The HSE must prepare a three (3) year corporate plan, submit it for the Minister’s approval and, following a copy of the approved plan being laid before both Houses of the Oireachtas, publish the approved plan on the internet.
1.7 Section 29(2).
Assistance may be provided by the HSE to any person or body that provides or proposes to provide a service similar or ancillary to a service that the HSE may provide by permitting the use by the person or body of premises maintained by the HSE (and, where requisite, executing alterations and repairs to and supplying furniture and fittings for such premises) or by providing premises (with all requisite furniture and fittings) for use by the person or body.
1.8 Sections 31-33
The HSE must prepare a service plan for each financial year, submit it for the Minister’s approval and, following a copy of the approved plan being laid before both Houses of the Oireachtas, publish the approved plan on the internet. Section 33 provides that the HSE must manage health and personal social services indicated in the approved service plan so as to ensure that the services are delivered in accordance with the plan.
1.9 Section 34
The Executive must not, without the consent of the Minister, enter into any agreement or arrangement or otherwise commit itself to capital spending on a transaction if the total cost
Health Service Executive National Financial Regulations
Ver 1.3 Page 138 of 176
Chapter 5, Topic 2, Protocol for Acquisition and Disposal of Property … Continued
of this would exceed the level specified from time to time by the Minister with the consent of the Minister of Finance N26.
1.10 Section 40
The HSE may accept gifts of land on such trusts or conditions (if any) as may be specified by the donor, unless such trust or condition would be inconsistent with the HSE’s object or functions or with any obligations imposed on the HSE under any enactment.
1.11 Section 62
On 1st January 2005, all land that, immediately before that day, was vested in the predecessors to the HSE (i.e. the health boards or authorities) and all rights, powers and privileges relating to or connected with that land were, without any conveyance or assignment transferred to and vested in the HSE.
1.12 Section 70
The Minister may order the transfer to the HSE of any property, rights and liabilities of any body that is dissolved by the Minister under this Section (being bodies established under the Health (Corporate Bodies) Act, 1961).
2. Health Act, 1970
2.1 Section 38
The HSE may, with the consent of the Minister, provide and maintain any hospital, sanatorium, home, laboratory, clinic, health centre or similar premises required for the provision of services under the Health Acts. The Minister may give to the HSE such direction as he thinks fit in relation to the provision or maintenance of any premises provided and maintained by the HSE and in relation to the arrangements for providing services therein. The HSE must comply with any such instructions.
The HSE may and, if directed by the Minister shall, discontinue the provision and maintenance of any premises provided and maintained by it, but shall not exercise this power in relation to a hospital, sanatorium or home without the consent of the Minister.
2.2 Section 40 (as amended by Section 17 of the Health (Amendment) (No. 3) Act 1996)
Section 40 of the Health Act 1970 provides as follows:
(a) a health board may provide land to a body providing institutional services
(i) on the request of the body;
(ii) subject to any general directions given by the Minister; and
(iii) where the board is satisfied the land is required for the efficient performance of the body’s functions.
(b) where the board decides to provide land to such a body, it may acquire the land
(i) by agreement, subject to any general directions given by the Minister; or
(ii) by compulsory acquisition;
(iii) and may lease the land to or for the benefit of the body. N 26 At the time of writing no level had been specified.
Health Service Executive National Financial Regulations
Ver 1.3 Page 139 of 176
Chapter 5, Topic 2, Protocol for Acquisition and Disposal of Property … Continued
2.3 Section 68
The HSE shall make available a service for the training of disabled persons for employment suitable to their condition of health, and for the making of arrangements with employers for placing disabled persons in suitable employment. For these purposes, the HSE may provide and maintain premises, farms, gardens and similar facilities.
3. Health Act, 1953
3.1 Section 54
A health authority is under a duty to give to every person in its functional area who is eligible for institutional assistance (meaning shelter and maintenance in a county home or similar institution) such institutional assistance as appears to them to be necessary or proper in each particular case.
3.2 Sections 63 and 64
A health authority may, with the consent of the Minister, (and shall if the Minister so directs) provide and maintain a nursing school in connection with a health institution maintained by it.
4. Part IV (Infections Diseases and Infestation) Health Act, 1947
For the purpose of the execution of their powers and duties under this Part of the Act, a health authority may provide and maintain premises, apparatus, material or any other facilities or may make arrangements with any person for the provision of such facilities, for example they may provide temporary accommodation to persons who need it as a result of an infectious disease.
5. Part VIII (Acquisition and Disposal of Land by Health Authorities) Health Act, 1947
5.1 Section 78 (as substituted by Section 75 of the Health Act 2004)
The HSE has the power to acquire land either (a) by agreement, subject to any general directions given by the Minister with the consent of the Minister for Finance or (b) compulsorily under this Part (Part VIII) of this Act or the Acts incorporated within this Act.
5.2 Section 80
An officer or agent of a health authority who is duly authorised by the health authority may enter on any land at reasonable times for the purpose of ascertaining whether the land is or is not suitable for acquisition by the authority. Before the officer enters the land, he must either obtain the consent of the owner or occupier of the land or give the owner or occupier fourteen days’ notice in writing of the intention to make the entry.
5.3 Section 81
A health authority can make an order for compulsory acquisition under this section.
5.4 Section 82
Before a health authority makes an order for compulsory acquisition, it must give notice to the owner or occupier of the land and publish an advertisement in the prescribed form in one or more newspapers circulating in the area.
Health Service Executive National Financial Regulations
Ver 1.3 Page 140 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
5.5 Sections 83, 84 and 85
Section 83 sets out the circumstances in which the Minister can confirm any compulsory acquisition order made by a health authority and Section 84 states that the health authority must also give notice of and advertise the confirmation of the compulsory acquisition order. Section 85 provides for annulment of compulsory acquisitions by the High Court.
5.6 Section 88 (as inserted by Section 18(b) of the Health (Amendment) Act (No.3) 1996)
The consent of the Minister for the purchase, leasing and sale of land by the HSE is no longer required, but any acquisition, disposal, leasing of land must still be carried out in accordance with any “general directions” of the Minister.
The HSE may, subject to the general directions of the Minister, appropriate and use for the purpose of its powers and duties, any land vested for any purpose in it and not required for the purpose for which it was acquired.
5.7 Section 89 (as inserted by Section 18(d) of the Health (Amendment) (No.3) Act 1996)
The HSE may, subject to any general directions given by the Minister with the consent of the Minister of Finance, sell, exchange, let or otherwise dispose of any land vested in it. Any capital proceeds of sale of any land are to be used, subject to the general directions of the Minister, for a purpose to which capital money may properly be applied by the Board.
Where land is exchanged, the land received shall be used for the same purposes as the transferred land.
5.8 Section 105 of the Health Act, 1947
A health authority, may with the approval of the Minister and shall if the Minister so directs, provide and maintain residences for the use of officers appointed or servants employed by them.
Health Service Executive National Financial Regulations
Ver 1.3 Page 141 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
Schedule 3
The Property Committee
The Terms of Reference for the Property Committee
The Property Committee will function as an executive group reporting to the Management Team that will apply their collective experience and knowledge of service requirements and property management, to vet and recommend or reject property transaction proposals. The committee shall operate in a manner that ensures an integrated, consistent and transparent approach in it’s assessment of HSE property transaction proposals and will recommend as appropriate, property proposals to the National Directors, Chief Executive or the HSE Board, in accordance with the current legislation and best practice for property transactions in the public sector. The Property Committee will:
• Appraise property transaction proposals with reference to Corporate Plan, Service Plan, Capital Plan and agreed property protocols that also takes account of legislative requirements and relevant guidance.
• Make recommendations accordingly, to the persons designated in agreed HSE, property
protocols.
• Oversee the work of the corporate property section. The corporate property section shall carryout routine
• preparation in advance of Property Committee meetings and follow-up as necessary to conclude the transaction process at corporate level. The corporate section shall maintain records of submissions to the committee and of the committee’s recommendation, decisions of Board, CEO and National Directors.
• The Committee shall be responsible for co-ordinating an integrated and standardised best
practice approach to corporate property issues and advise the Management Team accordingly.
• Contribute to the development of the HSE’s Strategy for Estate Management.
The Property Committee Composition
The Property Committee is an executive group set up by the HSE, Management Team that comprises of nominees from:
(a) The National Hospitals Office;
(b) The Primary, Community and Continuing Care Office(2no. representatives);
(c) The Directorate of Finance;
(d) The Estates function (3no. representatives). Note: At the time of development of this document Estates function operating under the direction of the National Director of Finance.
(e) Other Directorates – nomination available when items of relevance are before the committee
And
Health Service Executive National Financial Regulations
Ver 1.3 Page 142 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
(f) Chair
(g) Secretary to the committee
The frequency of the Property Committee Meetings will be determined by the Property Committee with reference to the volume of proposals submitted and ongoing workload of the committee. Committee meetings will not take place when a quorum is not available. A quorum requires that five members of the committee are in attendance. The committee will determine the minimum grade, qualifications and experience required for nominees and substitutes that may be required to attend from time to time.
The chairperson of the Committee shall be nominated by the Chief Executive Officer.
The Estates function shall supply the Secretary to the group.
The Secretary’s role shall be to co-ordinate the activities of the Property Committee, to keep records of the Business Cases submitted to the Property Committee and the recommendations made in respect of each, to keep and circulate minutes of meetings of the Property Committee, to draft any correspondence and keep records relating to property transactions, reviewed by the Property Committee, and other ancillary matters.
Health Service Executive National Financial Regulations
Ver 1.3 Page 143 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
Schedule 4 Summary of the Provisions of Part 5 of the Code of Practice for the Governance of State
Bodies (the “Code”)
The Code provides that it should be standard practice that the disposal of assets of State bodies like the HSE, or the granting of access to property for commercial arrangements (e.g. joint ventures with third parties), with an anticipated value at or above a threshold level of EUR70,000 should be by auction or competitive tendering process, other than in exceptional circumstances (such as a sale to a charitable body). The auction or competitive tendering process used should be both transparent and likely to achieve a fair market-related price.
• Determining the anticipated value
The anticipated value may be determined by:
(a) the reserve price recorded in advance in the HSE’s records; or
(b) formal certification by the Director of the HSE with responsibility for financial matters or a Director who is a member of the Audit Committee of the Board of the HSE that, in his or her view, the anticipated value is likely to be less or greater than EUR70,000.
In determining market value, regard should be had to accounting standards best practice in Ireland.
• If an auction or competitive tendering process takes place and the highest bid is not accepted:
Specific Board approval is required before the disposal of the asset or granting of access to property for commercial arrangements with third parties can be completed. This approval and the reason why a lower bid was accepted should be noted in the minutes of the Board.
• If an auction or competitive tendering process does not take place and the agreed price is EUR70,000 or more:
Specific Board approval is required before negotiations start and also before the disposal of the asset or granting of access to property or infrastructure for commercial joint venture arrangements with third parties can be completed.
• No disposal of an asset or grant of access to property or infrastructure for commercial arrangements with third parties should be completed until:
The officer authorising the disposal or grant of access has certified formally that:
(a) Board approval is not necessary, and the reasons why this is the case; or
(b) Board approval has been obtained.
• Disposal of assets to Directors, employees or their families or connected persons
“Families or connected persons” in this context means:
(a) a spouse, parent, brother, sister, child or step-child;
(b) a company with which the person is associated;
(c) a person acting as the trustee of any trust, the beneficiaries of which include the Director/employee or the persons described in (a) above or the company described in (b) above;
Health Service Executive National Financial Regulations
Ver 1.3 Page 144 of 176
(d) a person acting as a partner of the Director/employee or any person or body who, by virtue of (a)-(c) above, is connected with the Director/employee.
These disposals should be at a fair market-related price. A record of all such disposals to such persons (including details of the asset disposed of, price paid and name of the buyer) should be noted in a register kept for this purpose (minor disposals below a threshold approved by the Board may be omitted from the register). This register should be available for inspection, if requested, by the Board or by any member of the Board. The Board may retain a requirement that any disposal above an approved threshold may not be made without having been formally endorsed by the Board. Such endorsement may be subject to any conditions or specific restrictions imposed by the Board.
• Annual Reports to the Board and by the Board to the Minister
Details of all disposals of assets or grants of access to property for commercial arrangements with third parties (save for “Disposals of assets to Directors, employees or their families or connected persons” as discussed above) below the threshold value of EUR70,000 without auction or competitive tendering process should be formally reported, with the paid price and the name of the buyer, to the Board on an annual basis.
Details of and explanations for the disposals of assets or grants of access to property or infrastructure for commercial arrangements with third parties above the threshold of EUR70,000 which have not been subject to auction or competitive tendering process should be included in the Chairperson’s annual report to the relevant Minister.
The Chairperson, in the annual report to the relevant Minister should affirm that the disposal procedures, as outlined in Part 5 of the Code, have been complied with.
Health Service Executive National Financial Regulations
Ver 1.3 Page 145 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
Schedule 5
Assessment of the Potential Future or Ongoing Liabilities of the HSE to pay Outgoings in respect of a Property, in particular Commercial Rates
1. General
On the sale or disposal of any property or property interest by the HSE, the legal procedures and documentation should ensure that all liability on the part of the HSE in respect of the property ceases as at the date of the disposal. The assessment of any potential future ongoing liability for the HSE to pay outgoings in respect of any particular property therefore really only arises on the acquisition of property, both freehold and leasehold. The Manager whose responsibility it is to run the proposed acquisition of the relevant property on behalf of the HSE should always as part of his/her preliminary enquiries in relation to the property ascertain the outgoings (in particular, any unusual outgoings) affecting the property e.g. most commonly the rent payable in respect of a leasehold property. These should be verified and all other outgoings affecting the property established in the course of the due diligence conducted in respect of the acquisition of property e.g., in the case of the property being acquired by means of the grant of a lease, by way of pre-lease enquiries and in the case of the acquisition of a freehold interest and/or the assignment of a leasehold interest, by means of raising appropriate pre-contract enquiries followed by standard Objections and Requisitions on Title.
2. Property acquired by HSE by means of Grant of Lease
While not intended to be an exhaustive list and the appropriateness of the enquiries will depend on the particular property in question, in order to ascertain the outgoings affecting the property going forward generally the pre-lease enquiries raised by the solicitor conducting the legal aspects of the transaction on behalf of the HSE should include the following:
(a) Rates and Charges
(i) What is the rateable valuation of the demised premises.
(ii) Please furnish evidence of payment of rates for the current year.
(iii) Please furnish on completion a letter to the Rating Authority notifying change of occupier.
(iv) If the demised premises is subject to any other periodic or annual charge, give details.
(b) Insurance
(i) If the Landlord is insuring, furnish a certified copy of the Landlord’s insurance policy in receipt for latest premiums.
(ii) What will the tenants insurance payment for the first year of the Lease be?
(c) Service Charges
(i) Please furnish a summary or budget of the service charge for the first year of the term and the anticipated amount of the tenant’s contribution.
(ii) Please confirm the floor areas upon which the tenant’s contribution towards the service charge has been calculated.
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
Health Service Executive National Financial Regulations
Ver 1.3 Page 146 of 176
(iii) Please confirm whether there is a sinking or reserve fund in effect? If so please furnish details.
(iv) Is the Landlord or the service provider aware of any possible claim that will effect the service charge presently payable? Has any work been carried out or expenditure incurred or is there any proposal to carry out any work or incurring expenditure which would substantially affect the charge presently payable.
3. Freehold Property and Leasehold Property Acquired by Assignment of Leasehold Interest
The standard Objections and Requisitions on Title numbers 14, 33 and 37 should be raised prior to entering into any contract in relation to the property to ascertain all encumbrances and outgoings affecting the property.
In addition for leasehold property, where it is clear that a rent review is due under the terms of the Lease, appropriate enquiries should be made as to whether the rent review has taken place. If so, a copy of the related rent review memorandum should be requested and furnished and if not, confirmation should be requested of the vendor that no steps have been taken to initiate the review. In circumstances where a rent review is due and pending and no steps have been taken to initiate a review, the HSE would need to take the advice of a competent valuer as to the estimated or projected rent due on review.
4. Commercial rates – HSE situation under review
Health Service Executive National Financial Regulations
Ver 1.3 Page 147 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
Schedule 6
VAT on Property Transactions
WARNING: THIS NOTE IS INTENDED TO ACT AS A USEFUL SUMMARY GUIDE IN ALERTING USERS TO SITUATIONS WHERE THE VAT STATUS OF A PROPERTY MERITS FURTHER INVESTIGATION. THIS GUIDE SHOULD NOT BE TAKEN AS A DEFINITIVE STATEMENT COVERING ALL CIRCUMSTANCES AND A PROFESSIONAL ADVISER SHOULD AT ALL TIMES BE CONSULTED TO DEAL WITH THE VAT ASPECTS OF ANY DEALINGS WITH PROPERTY.
All references which follow, unless otherwise indicated, are to the Value Added Tax Act, 1972 (“VATA”) (as amended by all subsequent legislation).
6. STEP-BY-STEP APPROACH
In considering the question of Value Added Tax (“VAT”) on a property transaction it is recommended that one should follow a structured approach and the following is suggested:
6.1 Identify the nature of the interest being disposed of – is it a sale of a freehold, creation of a lease, assignment or surrender of an existing lease, creation of a new lease following the surrender of a lease. Different rules apply depending on the nature of the interest being disposed of.
6.2 Consider whether the six conditions mentioned at Paragraph 2 below are met. If any of the six conditions are not satisfied, then the property is not liable to VAT (It should be noted that only the first five conditions are applicable on the sale of a freehold interest);
6.3 If all of the conditions are met then consider how the VAT liability is computed and who is accountable.
7. IS THE PROPERTY SUBJECT TO VAT?
In order for VAT to be chargeable on a disposal, the following conditions must be fulfilled:
7.1 The property must have been developed or redeveloped on or after 1st November 1972. (VAT was introduced in Ireland on that date.) “Development” is defined in Section 1 VATA, as:
“the construction, demolition, extension, alteration or reconstruction of any building on the land”
or
“the carrying out of any engineering or other operation in, on, over, or under the land to adapt it for a materially altered use”
In most cases it will be possible to determine without difficulty whether or not a property has been developed or redeveloped. Where difficulties arise however is in relation to alterations and additions to a building. In this regard, Revenue will ignore relatively small outlay on additions or alterations, notwithstanding that a tax credit may have been claimed in respect of same. In a recent Revenue publication the Revenue has indicated that alterations or additions will only be ignored where (i) the works carried out did not adapt the land for a materially altered use and (ii) it is reasonably clear that the costs incurred did not exceed 10% of the total amount which tax would be chargeable on if the property was treated as developed or €300,000, whichever is the lesser.
Health Service Executive National Financial Regulations
Ver 1.3 Page 148 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
7.2 The person making the disposal must have an interest in the property. An “interest” means a leasehold interest of 10 years or more or a freehold interest. It should be noted that a lease containing an option enabling the tenant to extend the lease to 10 years or beyond is deemed to be a lease of at least 10 years duration. Break clauses in leases are ignored for the purposes of determining whether someone has an interest in a property.
7.3 The person making the disposal must dispose of an “interest” in the property. This could be a disposal of the full interest (e.g. freehold) or of a lesser interest derived from that interest (e.g. the person holding the freehold creates a lease / assigns a lease / surrenders a lease / grants a new lease following a surrender of a lease etc.).
7.4 The person making the disposal must have been entitled to claim a VAT input credit in respect of the acquisition of that “interest” or on the development of the property. Note that the entitlement is sufficient – it would not matter if the VAT was never actually claimed. If a body is VAT exempt (e.g. certain financial institutions, insurance companies etc.) then it would not be entitled to claim VAT input credit.
If the HSE is not entitled to reclaim VAT on costs incurred by it, it is probable that it should not be charging VAT on the disposal of an “interest” in the property, as it is unlikely that the HSE would have been entitled to reclaim VAT on the acquisition/development of its “interest” in the property.
7.5 The disposal must occur in the course or furtherance of business. There is a presumption that the disposal is a business transaction except in the case of the sale of a person’s private residence.
WHERE ANY OF CONDITIONS 7.1 TO 7.5 IS NOT FULFILLED, THE DISPOSAL IS NOT LIABLE TO VAT.
7.6 The introduction of Section 4(3A) VATA (the Economic Value Test, or “EVT”) has meant that a further test must be applied where a new long-lease (i.e. a lease with a term exceeding 10 years) is being created, an existing long-lease is being surrendered/assigned or a new long lease is created following the surrender of an existing long lease. It should be noted that EVT does not apply in the case of a sale of freehold property (or by Revenue concession in the case of leases of 99 years or more duration with a peppercorn rent) such that the five conditions referred to above are the only conditions which need to be satisfied.
The effect of the EVT is that where the capitalised value of a long lease (see paragraph 3.2 below) does not exceed its “economic value” then the disposal of the lease is regarded as being exempt from VAT. In addition if the EVT is failed the VAT reclaimed by the landlord on the purchase/development of the property is disallowed. Therefore it is important that in any property transaction involving a lease (whether acting for the landlord or the tenant) that great care is take to ensure that one does not fail the EVT. In this regard it should be noted that the standard Law Society Contract for Sale provides that in a situation of a surrender/assignment of a lease the Purchaser will be required to indemnify the Vendor against any loss of VAT previously recovered or reclaimed by the Vendor on the property which arises from the Purchaser seeking to attribute an amount less than the EVT to the capitalised value of the “interest” being disposed.
The “economic value” of a property is the amount on which VAT was chargeable on the earlier purchase and development of the property by the person disposing of their “interest”. The economic value also includes all related VATable professional costs incurred e.g. architects fees, solicitors fees on the acquisition or development of the property.
However, the “economic value” of a property can be reduced by up to 25% in the following circumstances:
Health Service Executive National Financial Regulations
Ver 1.3 Page 149 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
(a) the property has not been developed since the Vendors “interest” in the property was acquired;
(b) the disposal is of an “interest” derived (the “lesser interest”) from a greater interest acquired by the lessor (e.g. grant of a lease out of a freehold would be regarded as a lessor interest) and
(c) the lesser interest is not more than 35 years in duration.
If all of the above conditions apply, the “economic value” of the lesser interest should be calculated based on the following formula:
Economic Value x N1 (Number of full years in the lesser interest)
÷
N2 (Number of full years in the greater interest, although if this exceeds 35 years or if the greater interest is a freehold, then N2 shall equal to 35).
Finally, the above relief is limited and the “economic value” of the lesser interest cannot go below 75% of the “economic value” of the greater interest, except where the lesser interest is disposed of by way of surrender/assignment in which case there is no limit on the formula relief (see next paragraph).
In the context of the surrender or assignment of an interest, the “economic value” is calculated based on the remaining term of years in the lease.
8. AMOUNT ON WHICH VAT IS CHARGEABLE
Having established that the disposal is subject to VAT, it is then necessary to decide on what valuation should be levied.
8.1 Sale of Freehold Interest
A supply of a freehold interest in a property is subject to VAT at 13½% on the sale price. Irish VAT legislation states that market value may be imposed where the sale price is less than the market value.
If a freehold interest is sold with the benefit of a taxable “long lease” (i.e. a lease in excess of 10 years) in place the sale will not be subject to VAT where the property has not been developed or redeveloped since the lease was granted. The reason for this is that the taxable interest in the property is treated as having been disposed of by the Vendor when the long lease was granted.
8.2 Creation of a new Lease of 10 years or greater (“long lease”)
On the creation of a long lease VAT at 13½% is chargeable on the capitalised value of the lease provided that the EVT (see paragraph 2(6) above) is passed. The capitalised value is the figure computed under one of the following three valuation methods:
(a) Formula Method: 3/4 of the annual rent X the number of full years in the lease;
(b) Multiplier Method: The annual rent X Revenue multiplier (currently 21.27 N27);
(c) Valuation Method: The valuation arrived at by a competent and qualified valuer.
N27 The value of the multiplier is derived from the return from Government Stocks and is adjusted periodically according to changes in the yield applying to those stocks.
Health Service Executive National Financial Regulations
Ver 1.3 Page 150 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
In practice, the person granting the lease can choose whichever valuation method they wish and therefore if the HSE is a VAT exempt person and thereby not entitled to reclaim VAT care needs to be taken of what method is used i.e. if the highest valuation method is used then the amount of irrecoverable VAT will be higher.
8.3 Reversionary Interest – Leases between 10 – 20 Years
When a landlord creates a lease, the tenant enjoys the right to occupy the property for the duration of the lease. At the end of the lease period, the property reverts to the landlord and this is known as the landlords “reversionary interest”.
If a lease is for a period of 20 years or longer, the value of the reversionary interest is disregarded for VAT purposes. However, if a lease is for a period of between 10 and 20 years, the reversionary interest must be calculated, and the landlord must account at the time of creating the lease for the VAT arising on the reversionary interest. The value of the reversionary interest is the difference between the value of the landlords freehold interest in the property and the capitalised value of the lease (as calculated using the formulas at paragraph 3.2 above).
A landlord will typically want to choose the valuation method which gives the highest capitalised value for the lease so as to minimise the value of the reversionary interest. This is because the landlord will not be able to pass on the VAT cost which arises on the creation of a reversionary interest.
If the tenant is not entitled to reclaim (i.e. it is a partially or wholly exempt person) VAT, the tenant will be anxious that the lowest capitalised value (as calculated using the formulas at Paragraph 3.2 above) is chosen so as to reduce the amount of irrecoverable VAT which the tenant will suffer on the creation of the lease. Therefore care needs to be taken of these considerations if acting for either a landlord or tenant on the creation of a lease of between 10 and 20 years.
In order to avoid the above irrecoverable VAT liability which arise on the granting of 10 to 20 year leases, one possible solution is to agree with the tenant that the lease would be for a minimum of 20 years. This may well be in excess of the tenants requirements, and more than the tenant wishes to commit to. However, the landlord could agree that the lease will contain a break clause at say year 15. As mentioned earlier, the existence of a break clause will be ignored at the date of creation of the lease, and therefore such a lease would be regarded as a lease of 20 years or more with the result that the value of reversionary interest would be disregarded for VAT purposes.
8.4 Assignment And Surrender of Long Lease
A surrender of a lease is the return of the leasehold interest held by the tenant to the landlord. Surrenders include normal surrenders, abandonments, failure by a tenant to exercise an option to extend a lease, ejectment and forfeiture. The VAT liability on a surrender is calculated by reference to the capitalised value of the unexpired term of the leasehold interest being surrendered. The capitalised value is calculated by using the methods outlined in Paragraph 3.2 above. It is important to emphasise that the tenant making the surrender must pass the EVT (see paragraph 2.2 above) given that if the surrender fails the EVT, there is a clawback of the VAT input credit which would have been previously granted to the tenant when they acquired their interest in the property.
An assignment of an interest in a property is a transfer of the interest held by a tenant to a person other than the landlord. An assignment is valued as if it were the creation of an interest in the property for a period equal to the unexpired portion of the lease. Again it is important to emphasise that all assignments must pass the EVT (see paragraph 2.2 above.
Health Service Executive National Financial Regulations
Ver 1.3 Page 151 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
8.5 Supply of Property following the Surrender of a Lease
A complex series of rules apply for determining the VAT treatment which applies to a dealing in property where the property has been the subject of a long lease which has been surrendered. It should be noted that these rules only apply if there was no development of the property since the grant of the long lease which was surrendered (the “Original Lease”) in question. If there has been development of the property since the grant of the Original Lease, the entire property is back within the VAT net again and therefore the rules which follow are not applicable.
The general principle is that one determines the unexpired portion of the Original Lease at the date on which the new dealing (the “New Lease”) is granted. This period is referred to as the “Interval”. The length of the Interval will then determine the VAT treatment which will apply on the grant of the New Lease. New Leases will fall into four categories.
(a) Category 1 New Lease is for a period of less than 10 years
Where the New Lease is for a period of less than ten years the New Lease is exempt from VAT. The landlord will therefore not be entitled to reclaim the VAT arising on the surrender of the Original Lease to them. However, the landlord may waive this exemption and treat the New Lease as taxable and thereby recover the VAT incurred on the surrender of the Original Lease. Unlike the waivers discussed at (Clause 4 – Leases for less than 10 years below), the waiver in this case will only relate to that specific letting (i.e. all other short term rental income remains exempt from VAT). VAT at 21% will therefore be chargeable on the rent from the New Lease as it arises.
(b) Category 2 New Lease is for a period of ten years or greater but the Interval is less than 10 years.
Where the New Lease is for a period of ten years or greater but the Interval is less than 10 years the New Lease is exempt from VAT and therefore the landlord will not be entitled to reclaim VAT on the surrender of the Original Lease. However, the landlord can opt to charge VAT on the New Lease. It should be noted that this option is different to the waiver of exemption mentioned at Category 1 above. If the option is exercised (i.e. the landlord claims an input credit on the VAT arising on the surrender of the Old Lease) VAT will apply a 13½% on the capitalised of the Interval.
(c) Category 3 New Lease is for a period of ten years or greater, the Interval is greater than ten years, and the New Lease is longer than the interval.
Where the New Lease is for a period of ten years or greater, the Interval is greater than ten years, and the New Lease is longer than the Interval, the New Lease is liable to VAT. VAT is charged on the capitalised value (usual valuation methods apply see paragraph 3(b) above) of the Interval.
(d) Category 4 New Lease is for a period of ten years or greater, the Interval is greater than ten years, and the New Lease is shorter that the Interval.
Where the New Lease is for a period of ten years or greater, the Interval is greater than ten years and the New Lease is shorter than the Interval, the New Lease is liable to VAT as per Category 3 above. However, in addition the landlord is liable on the reversionary interest which is created. The reversionary interest in this scenario is the period of time between the end of the New Lease and the end of the Interval. The reversionary interest will be calculated by reference to the capitalised value of the Interval less the capitalised value of the New Lease. If the New Lease is for more than 20 years the reversion is ignored.
Health Service Executive National Financial Regulations
Ver 1.3 Page 152 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
9. LEASES FOR LESS THAN 10 YEARS
A separate VAT treatment applies to the grant of leases with a term which is less than 10 years (“Short Leases”). A Short Lease is considered as a supply of services for VAT purposes and is exempt from VAT.
However if a landlord has recovered VAT on the acquisition or development of a property and subsequently grants a Short Lease the landlord will be regarded as making a self supply for VAT purposes and will therefore suffer a clawback of any VAT which the landlord may have recovered on the acquisition/development of the property. In order to avoid such a VAT cost a landlord can elect to waive the exemption from VAT on Short Leases and thereby charge VAT at 21% on the periodic rents received or invoiced. It should be noted that the waiver extends to all properties let on Short Leases by the landlord. The waiver can be cancelled at any time but doing so may cause a clawback of VAT previously claimed on the property.
10. ACCOUNTABLE PERSON
10.1 Sale of Freehold Interest
In the case of the sale of a freehold interest it is always the Vendor who accounts for VAT on the disposal.
10.2 Grant of Long Lease
On the creation of a Long Lease the lessor is generally the person responsible for accounting and charging for VAT. However in the case of the grant of a Long Lease to a tenant which is Irish VAT registered and entitled to full VAT recoverability in respect of the VAT borne on the lease the landlord can avoid having to charge the VAT if the tenant agrees to self account for the VAT in his VAT return. This procedure is known as the VAT 4A procedure and can only occur after Revenue approval is granted following an application on form VAT 4A. It should be emphasised that the timing of the application for Revenue approval to operate this shift mechanism is important. Application must be made to the Revenue well in advance of the supply of the property in question, and before the earlier of:
(a) The occupation of the property by the tenants; or
(b) The execution of the Long Lease.
Once approval has been obtained from the Revenue the landlord ceases to have any responsibility for VAT on the creation of the Long Lease. The tenant is obliged to account for the VAT in its return, but as it has full deductibility it is also allowed to take a corresponding credit for that VAT with the net result that it does not actually have to pay any VAT over to the Revenue. Obviously the benefit of this procedure from the tenants perspective is that the tenant can avoid the cashflow problems which may be encountered by a tenant in making an upfront payment of VAT.
10.3 Assignment or Surrender of a Long Lease
In the case of an assignment or a surrender of a Long Lease the person to whom the property is assigned/surrendered is generally accountable to the Revenue for VAT on the “reverse charge” basis. Such persons liable to account for VAT on a “reverse charge” basis include:
(a) Taxable persons (i.e. person who is registered for VAT and who make supplies which are subject to VAT);
(b) A Department of Sate and local authorities;
Health Service Executive National Financial Regulations
Ver 1.3 Page 153 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
(c) Some VAT exempt persons including:
(i) Persons supplying exempt property;
(ii) Financial service providers;
(iii) Insurance service providers;
(iv) Passenger transport providers;
(v) Providers of agency services in relation to passenger transport, accommodation, insurance and financial services;
(vi) An Post;
(vii) RTE.
The “reverse charge” basis does not apply to leases assigned/surrendered to:-
• Private individuals;
• Other exempt entities including medical practitioners, educational establishments, the National Lottery and Undertakers.
In these cases it is the person who is assigning his interest/surrendering his interest who is accountable to the Revenue for the VAT liability arising on the surrender/assignment of the lease.
Health Service Executive National Financial Regulations
Ver 1.3 Page 154 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
Schedule 7
Stamp Duty on Property Transactions
WARNING: THIS NOTE IS INTENDED TO ACT AS A USEFUL SUMMARY GUIDE IN ALERTING USERS TO THE RATES OF STAMP DUTY WHICH APPLY ON TRANSFERS OF COMMERCIAL PROPERTY. THIS NOTE SHOULD NOT BE TAKEN AS A DEFINITIVE STATEMENT COVERING ALL CIRCUMSTANCES WHICH MAY ARISE AND A PROFESSIONAL ADVISER SHOULD AT ALL TIMES BE CONSULTED TO DEAL WITH THE STAMP DUTY ASPECTS OF ANY DEALINGS IN PROPERTY.
All references which follow, unless otherwise indicated, are to the Stamp Duties Consolidation Act, 1999 (“SDCA”). 11. GENERAL PRINCIPLES
Stamp duty is a highly technical tax, with great importance attaching to precise interpretation of the various legislative provisions and to the form of documents. With careful planning and structuring it is often possible to structure property transactions so as to reduce/eliminate the charge to stamp duty which would otherwise arise.
Some of the more important general principles of stamp duty law are set out below:
11.1 Stamp duty is a tax on instruments or documents. It is not a tax on transactions or persons but there are “accountable persons” (see Paragraph 6 below).
11.2 The primary charging section is contained in Section 2, SDCA which states:-
“Any instrument which:
(a) is specified in Schedule 1 (i.e. the “heads of charge”); and
(b) is executed in the State or, wherever executed relates to any property situated in the State or any matter or thing done or to be done in the State, shall be chargeable with Stamp Duty”.
11.3 The most common heads of charge are
(a) Conveyance/transfer on sale of property other than stocks or marketable securities;
(b) Conveyance/transfer on sale of stocks or marketable securities;
(c) Lease of immovable property;
(d) Mortgage, Bond, Debenture, Covenant (if a charge on property (e.g. immovable property) situated in Ireland).
11.4 The law in force and the facts in existence at the date of execution of the instrument is the applicable law and the relevant facts for the purposes of assessing stamp duty. This is important not least because numerous changes to the legislation have been made over the years, in particular to the first schedule of the SDCA.
11.5 Stamp duty is payable 30 days after execution of the relevant document. If stamp duty is not paid by the relevant due date interest, penalties and surcharges can accrue and the accountable person becoming liable.
11.6 Stamp duty has since lst November, 1991 been a compulsory tax. It is a debt due to the Minister for Finance by the "accountable person". The “accountable” “person” is:
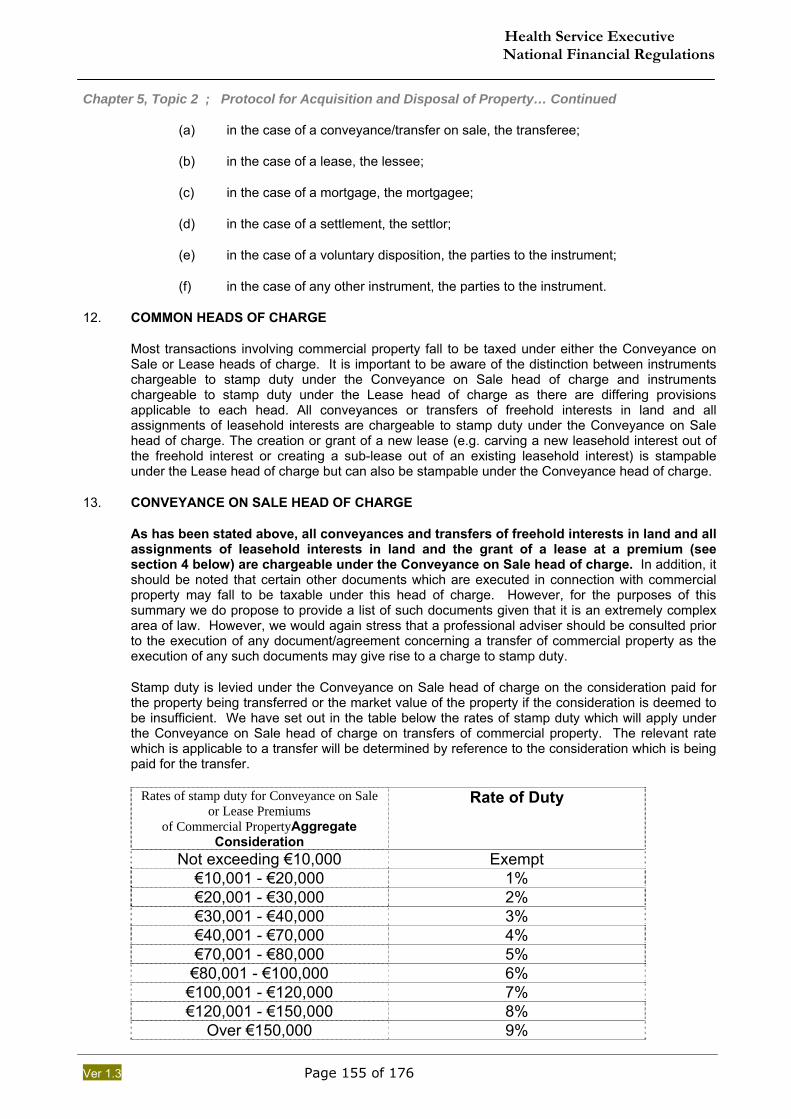
Health Service Executive National Financial Regulations
Ver 1.3 Page 155 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
(a) in the case of a conveyance/transfer on sale, the transferee;
(b) in the case of a lease, the lessee;
(c) in the case of a mortgage, the mortgagee;
(d) in the case of a settlement, the settlor;
(e) in the case of a voluntary disposition, the parties to the instrument;
(f) in the case of any other instrument, the parties to the instrument.
12. COMMON HEADS OF CHARGE
Most transactions involving commercial property fall to be taxed under either the Conveyance on Sale or Lease heads of charge. It is important to be aware of the distinction between instruments chargeable to stamp duty under the Conveyance on Sale head of charge and instruments chargeable to stamp duty under the Lease head of charge as there are differing provisions applicable to each head. All conveyances or transfers of freehold interests in land and all assignments of leasehold interests are chargeable to stamp duty under the Conveyance on Sale head of charge. The creation or grant of a new lease (e.g. carving a new leasehold interest out of the freehold interest or creating a sub-lease out of an existing leasehold interest) is stampable under the Lease head of charge but can also be stampable under the Conveyance head of charge.
13. CONVEYANCE ON SALE HEAD OF CHARGE
As has been stated above, all conveyances and transfers of freehold interests in land and all assignments of leasehold interests in land and the grant of a lease at a premium (see section 4 below) are chargeable under the Conveyance on Sale head of charge. In addition, it should be noted that certain other documents which are executed in connection with commercial property may fall to be taxable under this head of charge. However, for the purposes of this summary we do propose to provide a list of such documents given that it is an extremely complex area of law. However, we would again stress that a professional adviser should be consulted prior to the execution of any document/agreement concerning a transfer of commercial property as the execution of any such documents may give rise to a charge to stamp duty.
Stamp duty is levied under the Conveyance on Sale head of charge on the consideration paid for the property being transferred or the market value of the property if the consideration is deemed to be insufficient. We have set out in the table below the rates of stamp duty which will apply under the Conveyance on Sale head of charge on transfers of commercial property. The relevant rate which is applicable to a transfer will be determined by reference to the consideration which is being paid for the transfer.
Rates of stamp duty for Conveyance on Sale or Lease Premiums
of Commercial PropertyAggregate Consideration
Rate of Duty
Not exceeding €10,000 Exempt €10,001 - €20,000 1% €20,001 - €30,000 2% €30,001 - €40,000 3% €40,001 - €70,000 4% €70,001 - €80,000 5%
€80,001 - €100,000 6% €100,001 - €120,000 7% €120,001 - €150,000 8%
Over €150,000 9%
Health Service Executive National Financial Regulations
Ver 1.3 Page 156 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
14. LEASE HEAD OF CHARGE
As has been stated above, any document evidencing the creation/grant of a new lease is generally stampable under the lease head of charge and certain agreements for Lease. In addition, it should be noted that certain other documents which are executed in connection with commercial property may fall to be taxable under the Lease head of charges. However, for the purposes of this summary we do not propose to provide a detailed list of such documents given that it is an extremely complex area of law. However, we would again stress that a professional advisor should be consulted prior to the execution of any documents concerning the grant of a lease of commercial property.
Stamp duty on the granting of a lease of non-residential property is determined by reference to whether rent is payable under the lease. Where rent is payable under the lease, the stamp duty is calculated as follows (in addition to any stamp duty on the premium):
14.1 If the term of the lease is less than 35 years, stamp duty is calculated at the rate of 1% of the average annual rent;
14.2 If the term of the lease exceeds 35 years but is less than 100 years, stamp duty is calculated at the rate of 6% of the average annual rent;
14.3 If the term of the lease exceeds 100 years, stamp duty is calculated at the rate of 12% of the average annual rent.
If a premium is payable under the lease, either of itself or in addition to a rental payment, the normal rates for conveyances of non-residential property apply in calculating the stamp duty payable on the premium. (see paragraph C above for the relevant rates of stamp duty which apply to premiums).
It should be noted that in general stamp duty on a lease is calculated by reference to the rents/premiums which are provided for in the terms of the lease. However, it should be noted that under Section 54 SDCA, a lease will be deemed to operate as a voluntary disposition inter vivos where it is not executed in good faith or for valuable consideration. Essentially this applies where the consideration is inadequate (or for other circumstances) the lease confers a substantial benefit on the lessee. Where a lease is deemed to operate as a voluntary disposition inter vivos, a capital sum equal to the amount of the benefit conferred on the lessee is imputed to the lease and this capital sum will be stamped in the same way as if it were a premium. This “deemed” premium may be calculated on the basis of the open market rent that the property could achieve, with the premium equating to the amount of rent which the landlord would need to receive in order to compensate him for the reduced rent which has been reserved under the lease.
If the lease contains a break clause which allows the lessee to break the lease before the term reserved thereunder has expired, the lease is stampable upon the maximum duration of the lease without reference to the ability of the lessee to break the lease at an earlier stage. For example, a lease for a term of 40 years which gives the lessee the right to break the lease after a 5 year period will be stampable as a 40 year lease, even if it is likely that the lessee will exercise the break clause.
If the lessee is given the option to renew the lease for a further term, the lease is stampable only in respect of the fixed term and not by reference to the maximum possible term. If the option to renew is exercised, the documentation entered into to effect the exercise of the option will become stampable as a new lease granted on the date of the renewal of the new term.
Licenses over land are essentially authority to do something on that land which would otherwise not be permitted e.g. a concession to sell popcorn at a cinema. Licences relating to land do not represent an interest in land and therefore the creation of a licence relating to land should not in general be stampable under the Lease head (only leases or documents deemed to be
Health Service Executive National Financial Regulations
Ver 1.3 Page 157 of 176
Chapter 5, Topic 2 ; Protocol for Acquisition and Disposal of Property… Continued
leases are stampable on the lease head). However it is important that a licence is correctly documented for this treatment to apply.
15. PURCHASE OF PROPERTY THROUGH PURCHASE OF SHARES
Since the stamp duty rate on the transfer of land is 9% (for land valued in excess of €150,000) it has become increasingly the case that, where properties are held in a company and the shares in the company are sold, resulting in a 1% charge to stamp duty on the transfer of the shares (assuming that the company is an Irish incorporated company). This can result in a significant savings. However, before proceeding with a share acquisition it would be necessary to quantify the latent capital gains which may exist in the company and to obtain cover for historic tax liabilities which may exist in the company. In addition, it should be noted that there will be additional legal costs involved in the acquisition of a company as it would be prudent for a potential purchaser to have a financial and legal due diligence carried out on the company.
16. EXEMPTION FROM STAMP DUTY IF PAYABLE FROM OIREACHTAS FUNDS
There are numerous exemptions/relief available under stamp duty legislation which can utilised to reduce/eliminate the stamp duty charge on a document. Of particular relevance to the Health Services Executive (“HSE”) is Section 111 SDCA which provides that stamp duty shall not be charged upon any instrument if the amount of the stamp duty will be payable solely out of monies provided by the Oireachtas. Therefore if HSE is obliged to pay stamp duty on any document it may be entitled to an exemption from that stamp duty if the duty would have to be paid from funds provided by the Oireachtas.
Schedule 8 Definitions and Interpretation
“2004 Act” means the Health Act, 2004.
“Board” means the board of the HSE.
“Category 1 Transactions” means acquisitions and disposals of property or interests in property valued at an amount equal to or less than one million euro excluding VAT.
“Category 2 Transactions” means acquisitions and disposals of property or interests in property valued at an amount in excess of one million euro but equal to or less than two million euro excluding VAT.
“Category 3 Transactions” means acquisitions and disposals of property or interests in property valued at an amount in excess of two million euro excluding VAT.
“CEO” means the Chief Executive Officer of the HSE.
“HSE” means the Health Service Executive.
“Manager” means any LHO Manager or a HN Manager, as the case may be.
“Minister” means the Minister for Health and Children.
“Property Committee” means the Property Committee described in Schedule 3.
“WTEs” means whole time equivalent staff.
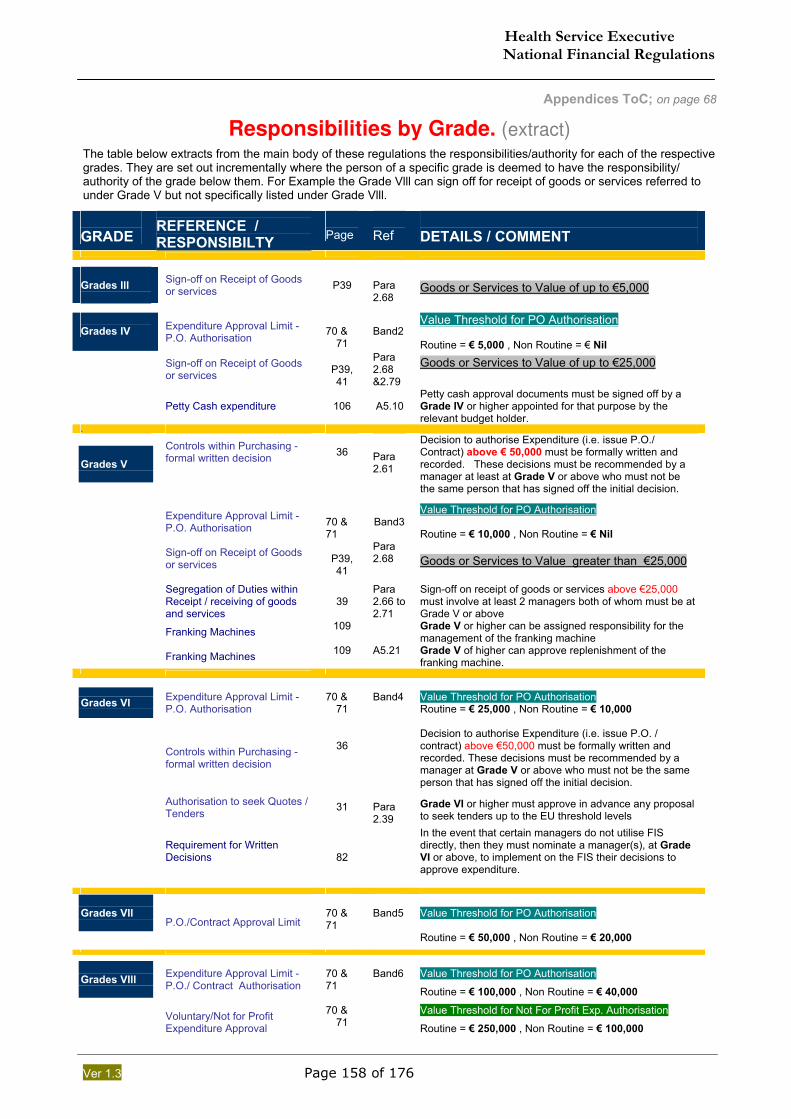
Health Service Executive National Financial Regulations
Ver 1.3 Page 158 of 176
Appendices ToC; on page 68
Responsibilities by Grade. (extract)
The table below extracts from the main body of these regulations the responsibilities/authority for each of the respective grades. They are set out incrementally where the person of a specific grade is deemed to have the responsibility/ authority of the grade below them. For Example the Grade Vlll can sign off for receipt of goods or services referred to under Grade V but not specifically listed under Grade Vlll.
GRADE
REFERENCE / RESPONSIBILTY
Page
Ref
DETAILS / COMMENT
Grades Ill
Sign-off on Receipt of Goods or services
P39
Para 2.68
Goods or Services to Value of up to €5,000
Grades IV Expenditure Approval Limit -
P.O. Authorisation
70 &
71
Band2
Value Threshold for PO Authorisation Routine = € 5,000 , Non Routine = € Nil
Sign-off on Receipt of Goods or services
P39, 41
Para 2.68 &2.79
Goods or Services to Value of up to €25,000
Petty Cash expenditure
106
A5.10
Petty cash approval documents must be signed off by a Grade IV or higher appointed for that purpose by the relevant budget holder.
. Grades V
Controls within Purchasing - formal written decision
36
Para 2.61
Decision to authorise Expenditure (i.e. issue P.O./ Contract) above € 50,000 must be formally written and recorded. These decisions must be recommended by a manager at least at Grade V or above who must not be the same person that has signed off the initial decision.
Expenditure Approval Limit - P.O. Authorisation
70 & 71
Band3
Value Threshold for PO Authorisation Routine = € 10,000 , Non Routine = € Nil
Sign-off on Receipt of Goods or services
P39, 41
Para 2.68
Goods or Services to Value greater than €25,000
Segregation of Duties within Receipt / receiving of goods and services
39
Para 2.66 to 2.71
Sign-off on receipt of goods or services above €25,000 must involve at least 2 managers both of whom must be at Grade V or above
Franking Machines 109 Grade V or higher can be assigned responsibility for the management of the franking machine
Franking Machines 109 A5.21 Grade V of higher can approve replenishment of the franking machine.
Grades VI
Expenditure Approval Limit - P.O. Authorisation
70 &
71
Band4
Value Threshold for PO Authorisation Routine = € 25,000 , Non Routine = € 10,000
Controls within Purchasing - formal written decision
36
Decision to authorise Expenditure (i.e. issue P.O. / contract) above €50,000 must be formally written and recorded. These decisions must be recommended by a manager at Grade V or above who must not be the same person that has signed off the initial decision.
Authorisation to seek Quotes / Tenders
31
Para 2.39
Grade VI or higher must approve in advance any proposal to seek tenders up to the EU threshold levels
Requirement for Written Decisions
82
In the event that certain managers do not utilise FIS directly, then they must nominate a manager(s), at Grade VI or above, to implement on the FIS their decisions to approve expenditure.
Grades VIl
P.O./Contract Approval Limit
70 & 71
Band5
Value Threshold for PO Authorisation Routine = € 50,000 , Non Routine = € 20,000
Grades VIll
Expenditure Approval Limit - P.O./ Contract Authorisation
70 & 71
Band6
Value Threshold for PO Authorisation
Routine = € 100,000 , Non Routine = € 40,000
Voluntary/Not for Profit Expenditure Approval
70 & 71
Value Threshold for Not For Profit Exp. Authorisation
Routine = € 250,000 , Non Routine = € 100,000
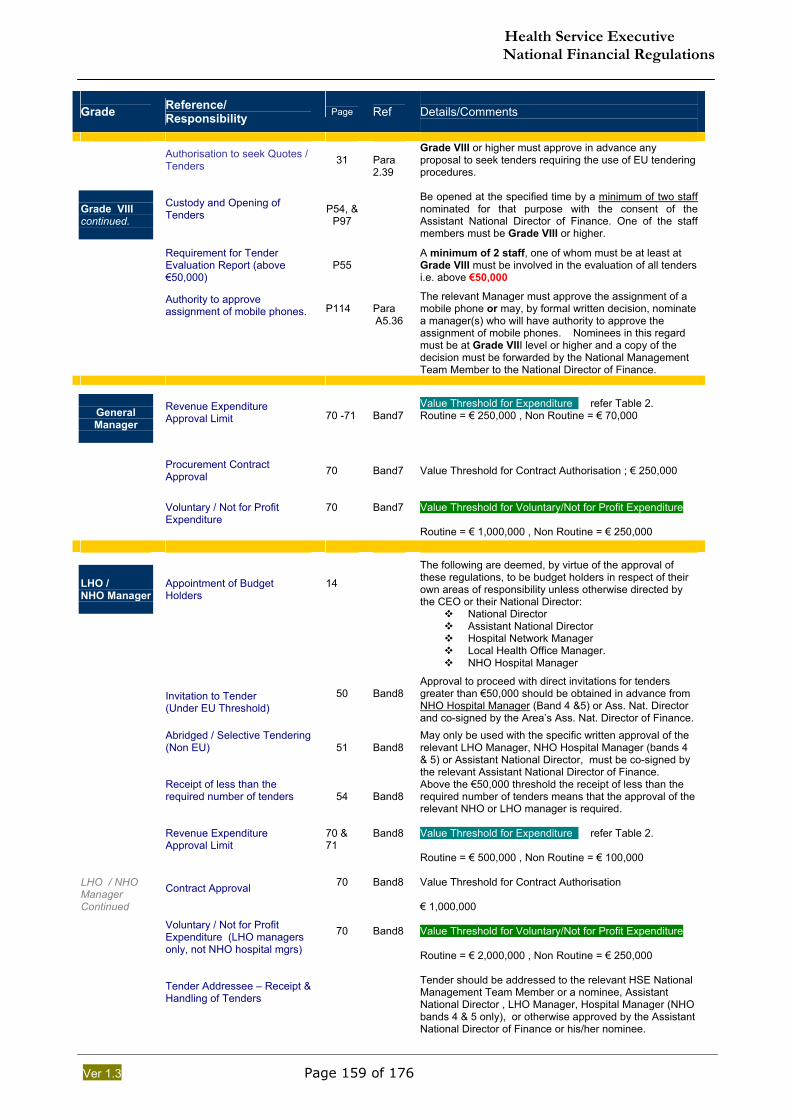
Health Service Executive National Financial Regulations
Ver 1.3 Page 159 of 176
Grade Reference/
Responsibility
Page Ref
Details/Comments
Authorisation to seek Quotes / Tenders
31
Para 2.39
Grade VIII or higher must approve in advance any proposal to seek tenders requiring the use of EU tendering procedures.
Grade VIII continued.
Custody and Opening of Tenders
P54, & P97
Be opened at the specified time by a minimum of two staff nominated for that purpose with the consent of the Assistant National Director of Finance. One of the staff members must be Grade VIII or higher.
Requirement for Tender Evaluation Report (above €50,000)
P55
A minimum of 2 staff, one of whom must be at least at Grade VIlI must be involved in the evaluation of all tenders i.e. above €50,000
Authority to approve assignment of mobile phones.
P114
Para A5.36
The relevant Manager must approve the assignment of a mobile phone or may, by formal written decision, nominate a manager(s) who will have authority to approve the assignment of mobile phones. Nominees in this regard must be at Grade VIII level or higher and a copy of the decision must be forwarded by the National Management Team Member to the National Director of Finance.
General Manager
Revenue Expenditure Approval Limit
70 -71
Band7
Value Threshold for Expenditure refer Table 2. Routine = € 250,000 , Non Routine = € 70,000
Procurement Contract Approval
70
Band7
Value Threshold for Contract Authorisation ; € 250,000
Voluntary / Not for Profit Expenditure
70
Band7
Value Threshold for Voluntary/Not for Profit Expenditure Routine = € 1,000,000 , Non Routine = € 250,000
LHO / NHO Manager
Appointment of Budget Holders
14
The following are deemed, by virtue of the approval of these regulations, to be budget holders in respect of their own areas of responsibility unless otherwise directed by the CEO or their National Director:
National Director Assistant National Director Hospital Network Manager Local Health Office Manager. NHO Hospital Manager
Invitation to Tender (Under EU Threshold)
50
Band8
Approval to proceed with direct invitations for tenders greater than €50,000 should be obtained in advance from NHO Hospital Manager (Band 4 &5) or Ass. Nat. Director and co-signed by the Area’s Ass. Nat. Director of Finance.
Abridged / Selective Tendering (Non EU)
51
Band8
May only be used with the specific written approval of the relevant LHO Manager, NHO Hospital Manager (bands 4 & 5) or Assistant National Director, must be co-signed by the relevant Assistant National Director of Finance.
Receipt of less than the required number of tenders
54
Band8
Above the €50,000 threshold the receipt of less than the required number of tenders means that the approval of the relevant NHO or LHO manager is required.
Revenue Expenditure Approval Limit
70 & 71
Band8
Value Threshold for Expenditure refer Table 2. Routine = € 500,000 , Non Routine = € 100,000
LHO / NHO Manager Continued
Contract Approval
70
Band8
Value Threshold for Contract Authorisation € 1,000,000
Voluntary / Not for Profit Expenditure (LHO managers only, not NHO hospital mgrs)
70
Band8
Value Threshold for Voluntary/Not for Profit Expenditure Routine = € 2,000,000 , Non Routine = € 250,000
Tender Addressee – Receipt & Handling of Tenders
Tender should be addressed to the relevant HSE National Management Team Member or a nominee, Assistant National Director , LHO Manager, Hospital Manager (NHO bands 4 & 5 only), or otherwise approved by the Assistant National Director of Finance or his/her nominee.
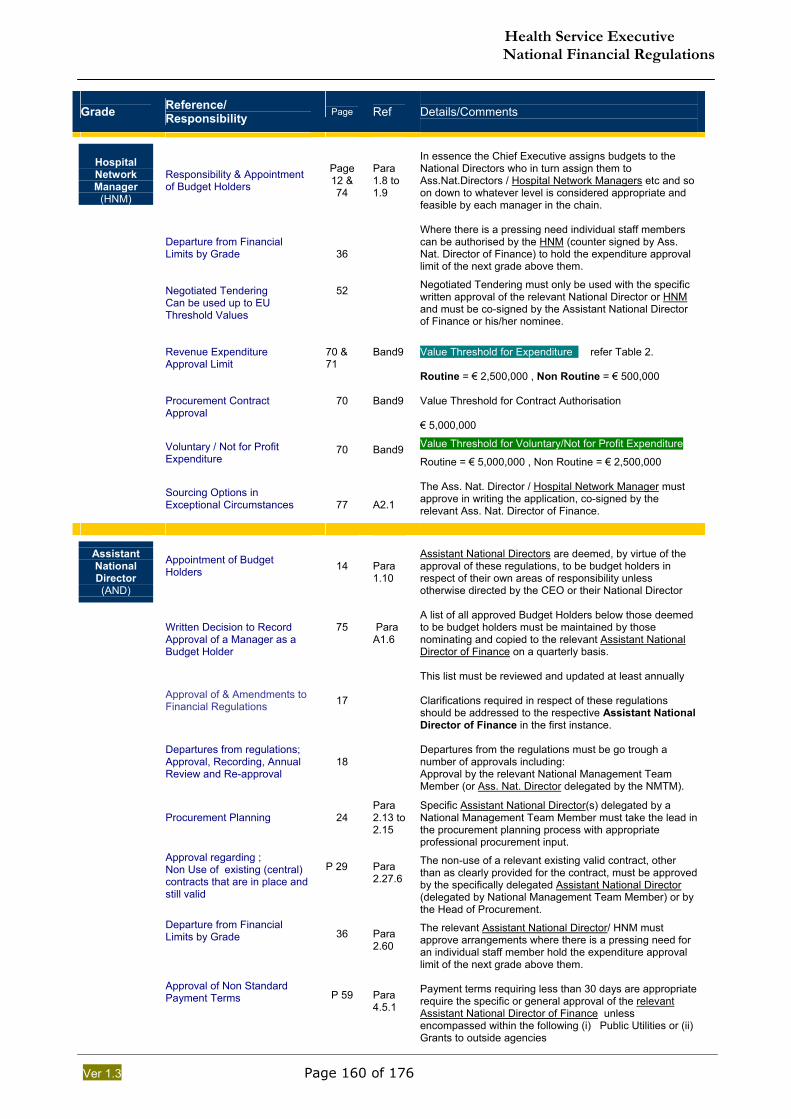
Health Service Executive National Financial Regulations
Ver 1.3 Page 160 of 176
Grade Reference/
Responsibility
Page Ref
Details/Comments
Hospital Network Manager
(HNM)
Responsibility & Appointment of Budget Holders
Page 12 & 74
Para 1.8 to 1.9
In essence the Chief Executive assigns budgets to the National Directors who in turn assign them to Ass.Nat.Directors / Hospital Network Managers etc and so on down to whatever level is considered appropriate and feasible by each manager in the chain.
Departure from Financial Limits by Grade
36
Where there is a pressing need individual staff members can be authorised by the HNM (counter signed by Ass. Nat. Director of Finance) to hold the expenditure approval limit of the next grade above them.
Negotiated Tendering Can be used up to EU Threshold Values
52
Negotiated Tendering must only be used with the specific written approval of the relevant National Director or HNM and must be co-signed by the Assistant National Director of Finance or his/her nominee.
Revenue Expenditure Approval Limit
70 & 71
Band9
Value Threshold for Expenditure refer Table 2. Routine = € 2,500,000 , Non Routine = € 500,000
Procurement Contract Approval
70
Band9
Value Threshold for Contract Authorisation € 5,000,000
Voluntary / Not for Profit Expenditure
70
Band9
Value Threshold for Voluntary/Not for Profit Expenditure
Routine = € 5,000,000 , Non Routine = € 2,500,000
Sourcing Options in Exceptional Circumstances
77
A2.1
The Ass. Nat. Director / Hospital Network Manager must approve in writing the application, co-signed by the relevant Ass. Nat. Director of Finance.
Assistant National Director (AND)
Appointment of Budget Holders
14
Para 1.10
Assistant National Directors are deemed, by virtue of the approval of these regulations, to be budget holders in respect of their own areas of responsibility unless otherwise directed by the CEO or their National Director
Written Decision to Record Approval of a Manager as a Budget Holder
75
Para A1.6
A list of all approved Budget Holders below those deemed to be budget holders must be maintained by those nominating and copied to the relevant Assistant National Director of Finance on a quarterly basis. This list must be reviewed and updated at least annually
Approval of & Amendments to Financial Regulations
17
Clarifications required in respect of these regulations should be addressed to the respective Assistant National Director of Finance in the first instance.
Departures from regulations; Approval, Recording, Annual Review and Re-approval
418
Departures from the regulations must be go trough a number of approvals including: Approval by the relevant National Management Team Member (or Ass. Nat. Director delegated by the NMTM).
Procurement Planning
24
Para 2.13 to 2.15
Specific Assistant National Director(s) delegated by a National Management Team Member must take the lead in the procurement planning process with appropriate professional procurement input.
Approval regarding ; Non Use of existing (central) contracts that are in place and still valid
P 29
Para 2.27.6
The non-use of a relevant existing valid contract, other than as clearly provided for the contract, must be approved by the specifically delegated Assistant National Director (delegated by National Management Team Member) or by the Head of Procurement.
Departure from Financial Limits by Grade
36
Para 2.60
The relevant Assistant National Director/ HNM must approve arrangements where there is a pressing need for an individual staff member hold the expenditure approval limit of the next grade above them.
Approval of Non Standard Payment Terms
P 59
Para 4.5.1
Payment terms requiring less than 30 days are appropriate require the specific or general approval of the relevant Assistant National Director of Finance unless encompassed within the following (i) Public Utilities or (ii) Grants to outside agencies
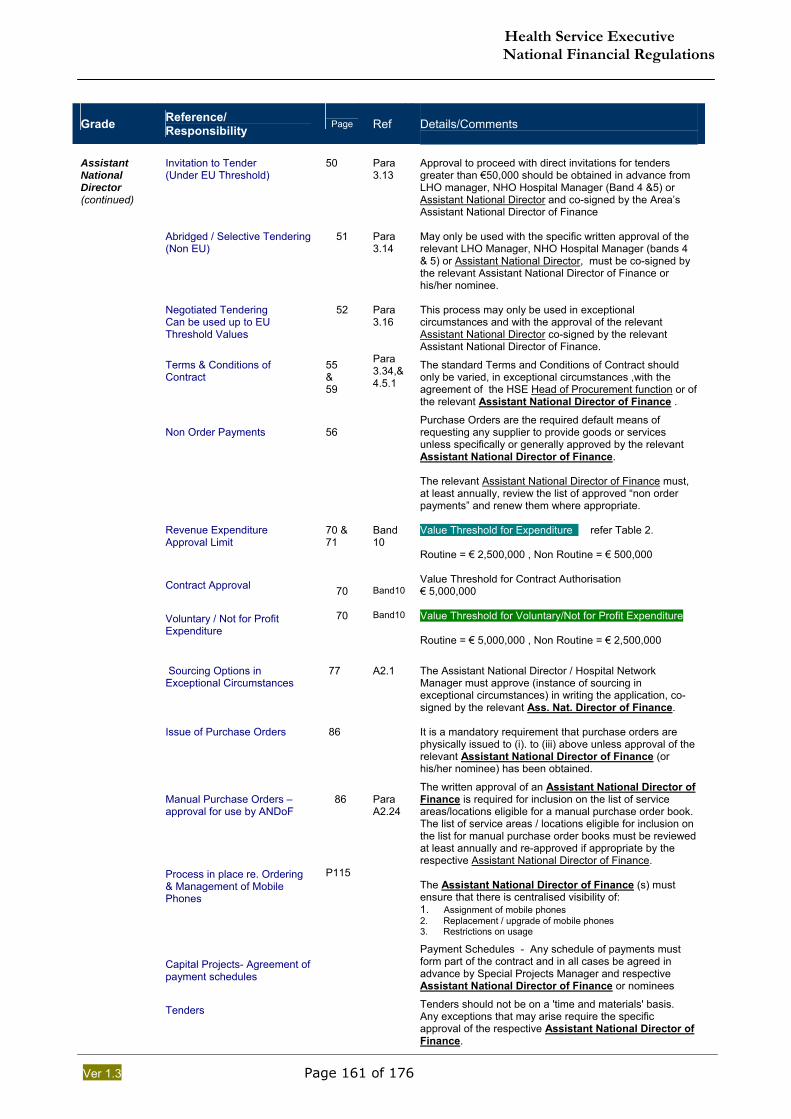
Health Service Executive National Financial Regulations
Ver 1.3 Page 161 of 176
Grade Reference/
Responsibility
Page Ref
Details/Comments
Assistant National Director (continued)
Invitation to Tender (Under EU Threshold)
50
Para 3.13
Approval to proceed with direct invitations for tenders greater than €50,000 should be obtained in advance from LHO manager, NHO Hospital Manager (Band 4 &5) or Assistant National Director and co-signed by the Area’s Assistant National Director of Finance
Abridged / Selective Tendering (Non EU)
51
Para 3.14
May only be used with the specific written approval of the relevant LHO Manager, NHO Hospital Manager (bands 4 & 5) or Assistant National Director, must be co-signed by the relevant Assistant National Director of Finance or his/her nominee.
Negotiated Tendering Can be used up to EU Threshold Values
52
Para 3.16
This process may only be used in exceptional circumstances and with the approval of the relevant Assistant National Director co-signed by the relevant Assistant National Director of Finance.
Terms & Conditions of Contract
55 & 59
Para 3.34,& 4.5.1
The standard Terms and Conditions of Contract should only be varied, in exceptional circumstances ,with the agreement of the HSE Head of Procurement function or of the relevant Assistant National Director of Finance .
Non Order Payments
56
Purchase Orders are the required default means of requesting any supplier to provide goods or services unless specifically or generally approved by the relevant Assistant National Director of Finance. The relevant Assistant National Director of Finance must, at least annually, review the list of approved “non order payments” and renew them where appropriate.
Revenue Expenditure Approval Limit
70 & 71
Band 10
Value Threshold for Expenditure refer Table 2. Routine = € 2,500,000 , Non Routine = € 500,000
Contract Approval 70
Band10
Value Threshold for Contract Authorisation € 5,000,000
Voluntary / Not for Profit Expenditure
70
Band10
Value Threshold for Voluntary/Not for Profit Expenditure Routine = € 5,000,000 , Non Routine = € 2,500,000
Sourcing Options in Exceptional Circumstances
77
A2.1
The Assistant National Director / Hospital Network Manager must approve (instance of sourcing in exceptional circumstances) in writing the application, co-signed by the relevant Ass. Nat. Director of Finance.
Issue of Purchase Orders
86
It is a mandatory requirement that purchase orders are physically issued to (i). to (iii) above unless approval of the relevant Assistant National Director of Finance (or his/her nominee) has been obtained.
Manual Purchase Orders – approval for use by ANDoF
86
Para A2.24
The written approval of an Assistant National Director of Finance is required for inclusion on the list of service areas/locations eligible for a manual purchase order book. The list of service areas / locations eligible for inclusion on the list for manual purchase order books must be reviewed at least annually and re-approved if appropriate by the respective Assistant National Director of Finance.
Process in place re. Ordering & Management of Mobile Phones
P115 The Assistant National Director of Finance (s) must ensure that there is centralised visibility of: 1. Assignment of mobile phones 2. Replacement / upgrade of mobile phones 3. Restrictions on usage
Capital Projects- Agreement of payment schedules
Payment Schedules - Any schedule of payments must form part of the contract and in all cases be agreed in advance by Special Projects Manager and respective Assistant National Director of Finance or nominees
Tenders
Tenders should not be on a 'time and materials' basis. Any exceptions that may arise require the specific approval of the respective Assistant National Director of Finance.
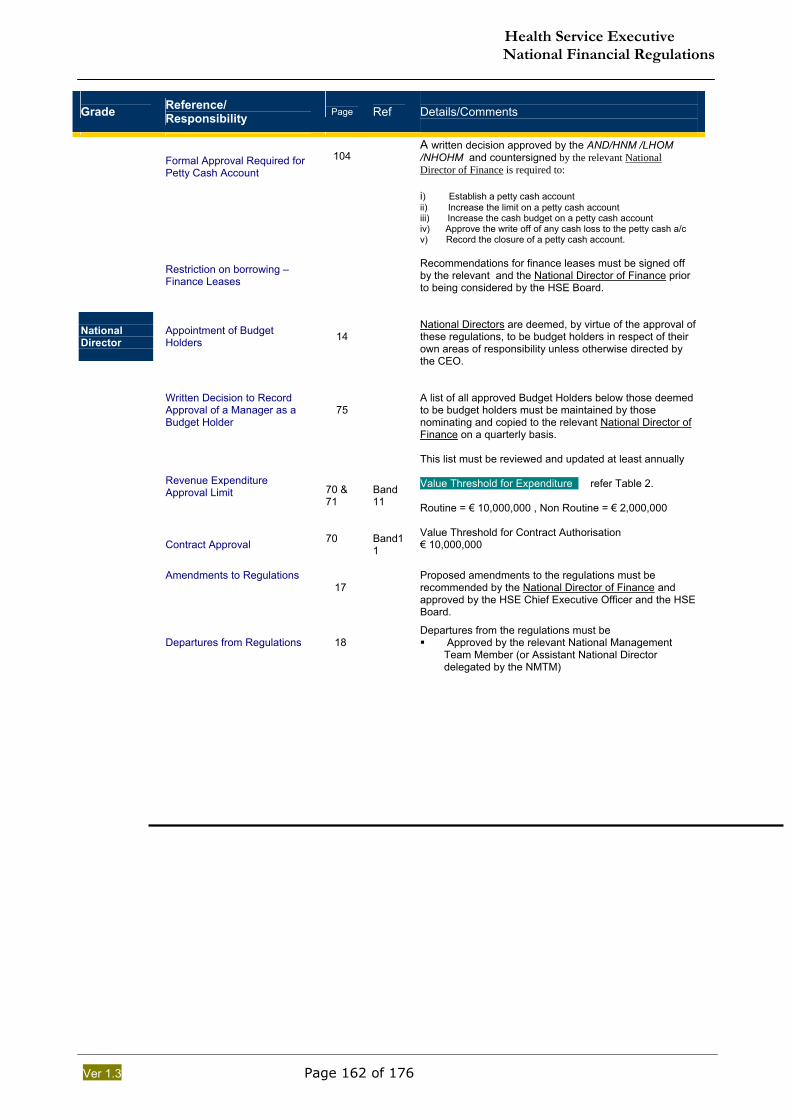
Health Service Executive National Financial Regulations
Ver 1.3 Page 162 of 176
Grade Reference/
Responsibility
Page Ref
Details/Comments
Formal Approval Required for Petty Cash Account
104
A written decision approved by the AND/HNM /LHOM /NHOHM and countersigned by the relevant National Director of Finance is required to: i) Establish a petty cash account ii) Increase the limit on a petty cash account iii) Increase the cash budget on a petty cash account iv) Approve the write off of any cash loss to the petty cash a/c v) Record the closure of a petty cash account.
Restriction on borrowing – Finance Leases
Recommendations for finance leases must be signed off by the relevant and the National Director of Finance prior to being considered by the HSE Board.
National Director
Appointment of Budget Holders
14
National Directors are deemed, by virtue of the approval of these regulations, to be budget holders in respect of their own areas of responsibility unless otherwise directed by the CEO.
Written Decision to Record Approval of a Manager as a Budget Holder
75
A list of all approved Budget Holders below those deemed to be budget holders must be maintained by those nominating and copied to the relevant National Director of Finance on a quarterly basis. This list must be reviewed and updated at least annually
Revenue Expenditure Approval Limit
70 & 71
Band 11
Value Threshold for Expenditure refer Table 2. Routine = € 10,000,000 , Non Routine = € 2,000,000
Contract Approval
70
Band11
Value Threshold for Contract Authorisation € 10,000,000
Amendments to Regulations
17
Proposed amendments to the regulations must be recommended by the National Director of Finance and approved by the HSE Chief Executive Officer and the HSE Board.
Departures from Regulations
18
Departures from the regulations must be Approved by the relevant National Management
Team Member (or Assistant National Director delegated by the NMTM)
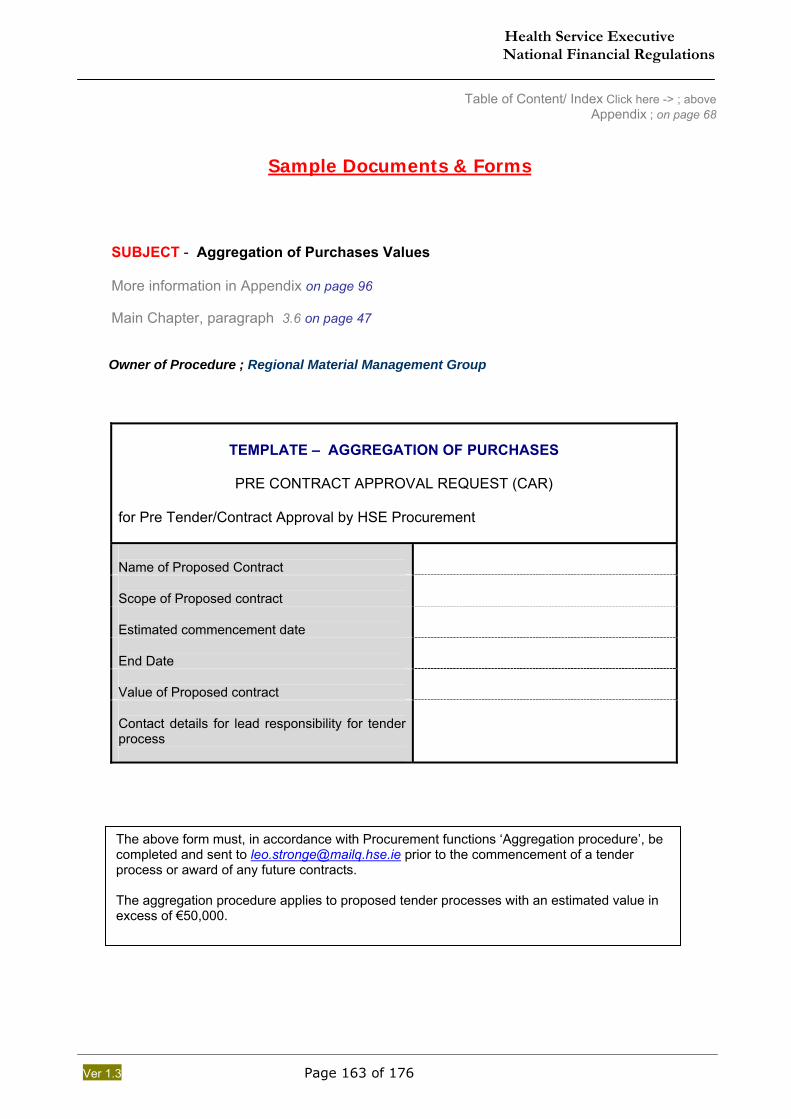
Health Service Executive National Financial Regulations
Ver 1.3 Page 163 of 176
Table of Content/ Index Click here -> ; above Appendix ; on page 68
Sample Documents & Forms
SUBJECT - Aggregation of Purchases Values More information in Appendix on page 96 Main Chapter, paragraph 3.6 on page 47 Owner of Procedure ; Regional Material Management Group
TEMPLATE – AGGREGATION OF PURCHASES
PRE CONTRACT APPROVAL REQUEST (CAR)
for Pre Tender/Contract Approval by HSE Procurement Name of Proposed Contract
Scope of Proposed contract
Estimated commencement date
End Date
Value of Proposed contract
Contact details for lead responsibility for tender process
The above form must, in accordance with Procurement functions ‘Aggregation procedure’, be completed and sent to [email protected] prior to the commencement of a tender process or award of any future contracts. The aggregation procedure applies to proposed tender processes with an estimated value in excess of €50,000.
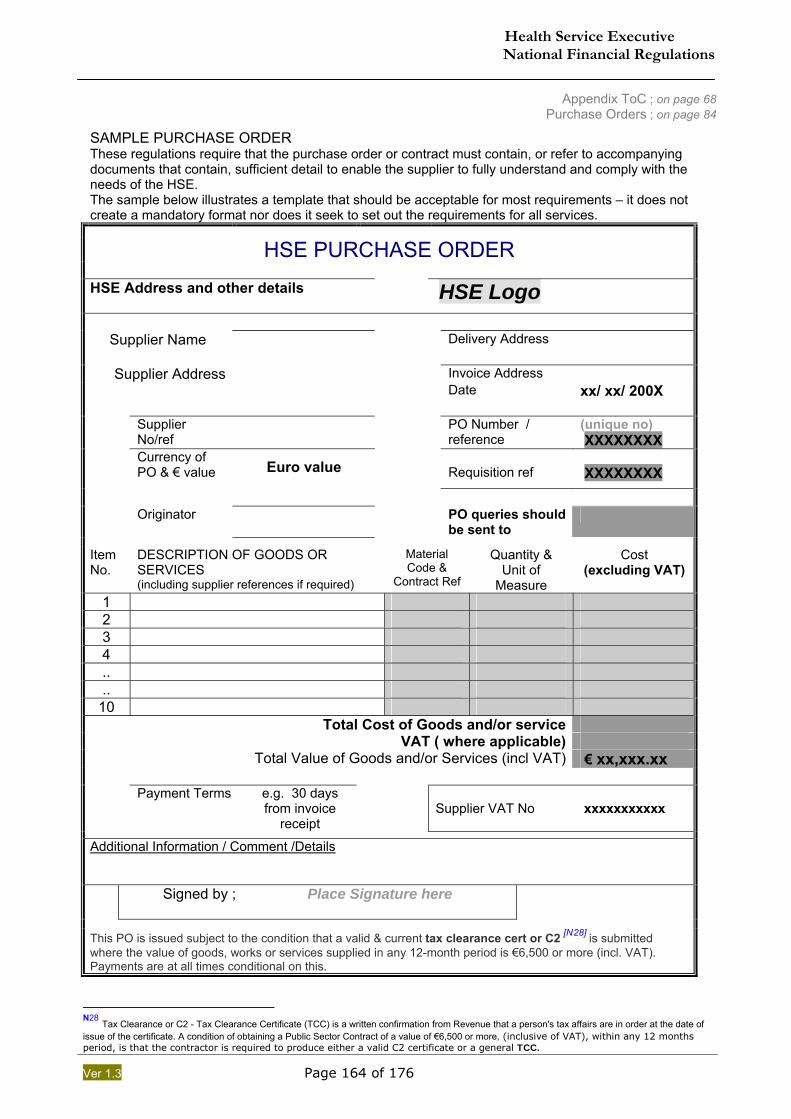
Health Service Executive National Financial Regulations
Ver 1.3 Page 164 of 176
Appendix ToC ; on page 68 Purchase Orders ; on page 84
SAMPLE PURCHASE ORDER These regulations require that the purchase order or contract must contain, or refer to accompanying documents that contain, sufficient detail to enable the supplier to fully understand and comply with the needs of the HSE. The sample below illustrates a template that should be acceptable for most requirements – it does not create a mandatory format nor does it seek to set out the requirements for all services.
HSE PURCHASE ORDER HSE Address and other details
HSE Logo
Supplier Name Delivery Address
Invoice Address Supplier Address Date xx/ xx/ 200X
Supplier
No/ref PO Number /
reference (unique no) XXXXXXXX
Currency of PO & € value
Euro value Requisition ref
XXXXXXXX
Originator PO queries should
be sent to
Item No.
DESCRIPTION OF GOODS OR SERVICES (including supplier references if required)
Material Code &
Contract Ref
Quantity & Unit of
Measure
Cost (excluding VAT)
1 2 3 4 .. ..
10 Total Cost of Goods and/or service VAT ( where applicable) Total Value of Goods and/or Services (incl VAT) € xx,xxx.xx Payment Terms e.g. 30 days
from invoice receipt
Supplier VAT No
xxxxxxxxxxx
Additional Information / Comment /Details Signed by ; Place Signature here
This PO is issued subject to the condition that a valid & current tax clearance cert or C2 [N28] is submitted where the value of goods, works or services supplied in any 12-month period is €6,500 or more (incl. VAT). Payments are at all times conditional on this.
N28 Tax Clearance or C2 - Tax Clearance Certificate (TCC) is a written confirmation from Revenue that a person's tax affairs are in order at the date of issue of the certificate. A condition of obtaining a Public Sector Contract of a value of €6,500 or more, (inclusive of VAT), within any 12 months period, is that the contractor is required to produce either a valid C2 certificate or a general TCC.
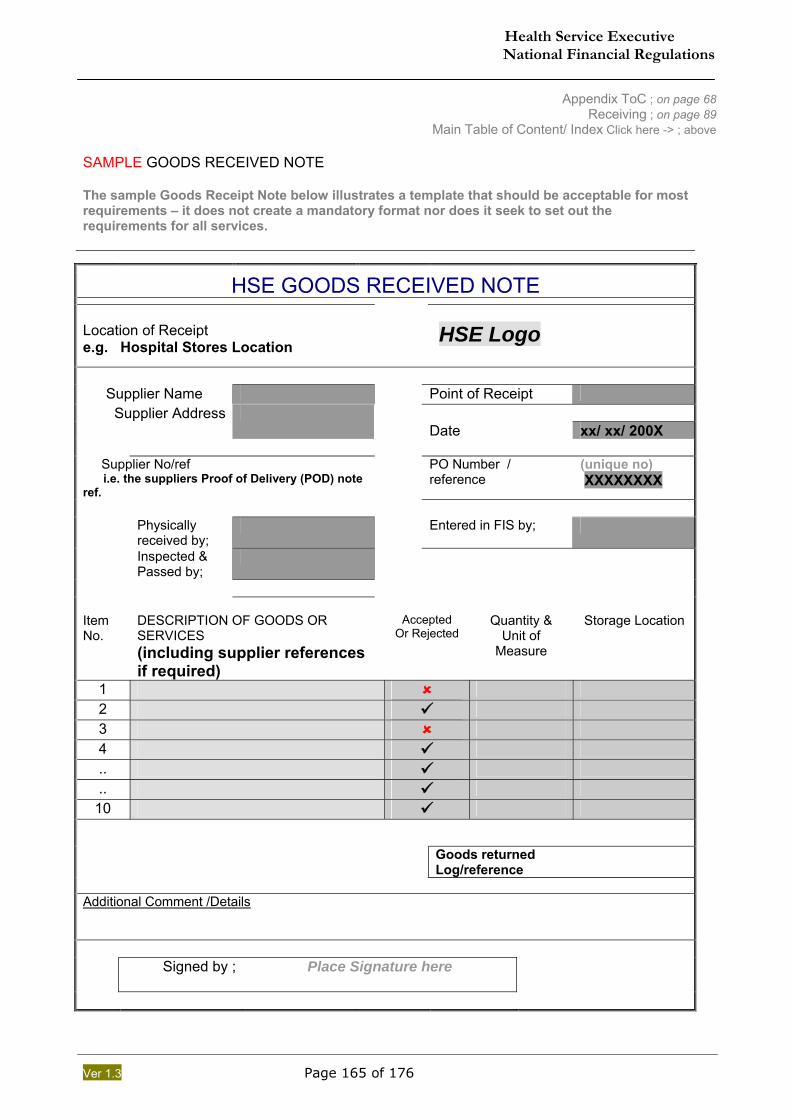
Health Service Executive National Financial Regulations
Ver 1.3 Page 165 of 176
Appendix ToC ; on page 68 Receiving ; on page 89
Main Table of Content/ Index Click here -> ; above SAMPLE GOODS RECEIVED NOTE The sample Goods Receipt Note below illustrates a template that should be acceptable for most requirements – it does not create a mandatory format nor does it seek to set out the requirements for all services.
HSE GOODS RECEIVED NOTE
Location of Receipt e.g. Hospital Stores Location
HSE Logo
Supplier Name Point of Receipt
Supplier Address Date xx/ xx/ 200X
Supplier No/ref i.e. the suppliers Proof of Delivery (POD) note ref.
PO Number / reference
(unique no) XXXXXXXX
Physically
received by; Entered in FIS by;
Inspected & Passed by;
Item No.
DESCRIPTION OF GOODS OR SERVICES (including supplier references if required)
Accepted
Or Rejected
Quantity &
Unit of Measure
Storage Location
1 2 3 4 .. ..
10
Goods returned
Log/reference
Additional Comment /Details Signed by ; Place Signature here
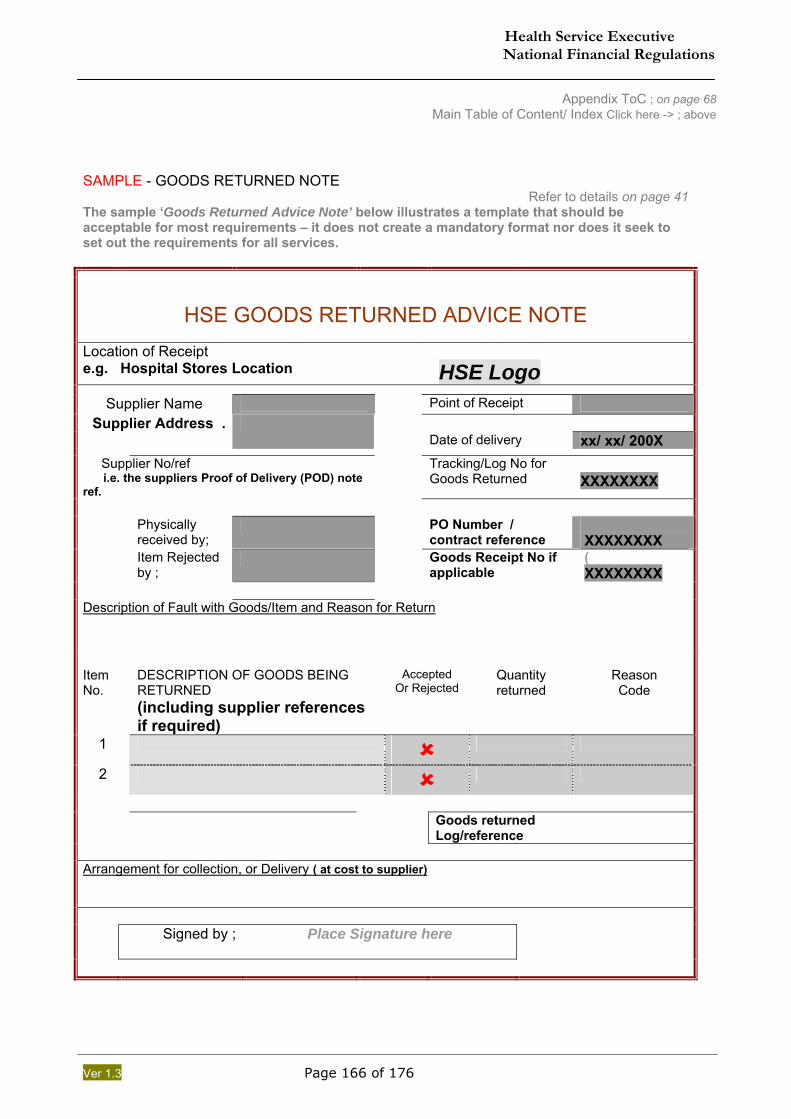
Health Service Executive National Financial Regulations
Ver 1.3 Page 166 of 176
Appendix ToC ; on page 68 Main Table of Content/ Index Click here -> ; above
SAMPLE - GOODS RETURNED NOTE
Refer to details on page 41 The sample ‘Goods Returned Advice Note’ below illustrates a template that should be acceptable for most requirements – it does not create a mandatory format nor does it seek to set out the requirements for all services.
HSE GOODS RETURNED ADVICE NOTE
Location of Receipt e.g. Hospital Stores Location
HSE Logo
Supplier Name Point of Receipt Supplier Address . Date of delivery xx/ xx/ 200X
Supplier No/ref i.e. the suppliers Proof of Delivery (POD) note ref.
Tracking/Log No for Goods Returned
XXXXXXXX
Physically
received by; PO Number /
contract reference (unique no) XXXXXXXX
Item Rejected by ;
Goods Receipt No if applicable
( XXXXXXXX
Description of Fault with Goods/Item and Reason for Return
Item No.
DESCRIPTION OF GOODS BEING RETURNED (including supplier references if required)
Accepted
Or Rejected
Quantity returned
Reason Code
1
2
Goods returned
Log/reference
Arrangement for collection, or Delivery ( at cost to supplier) Signed by ; Place Signature here
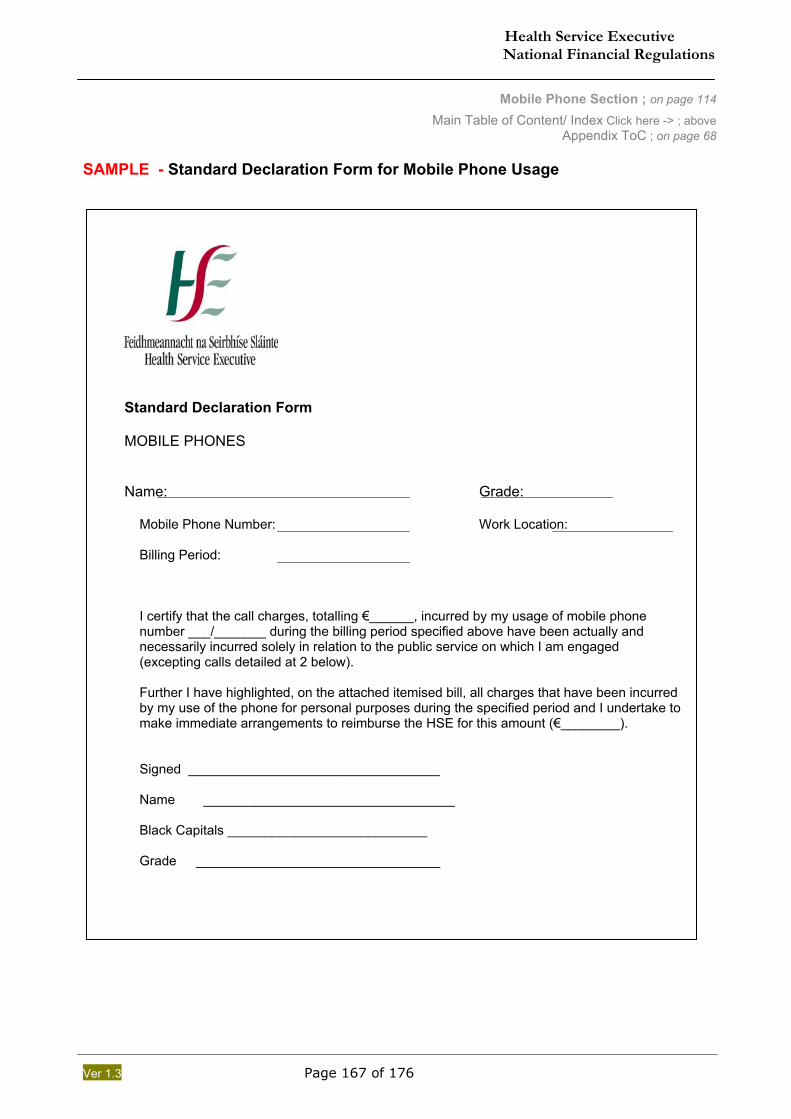
Health Service Executive National Financial Regulations
Ver 1.3 Page 167 of 176
Mobile Phone Section ; on page 114
Main Table of Content/ Index Click here -> ; above Appendix ToC ; on page 68
SAMPLE - Standard Declaration Form for Mobile Phone Usage
Standard Declaration Form MOBILE PHONES Name: Grade:
Mobile Phone Number: Work Location: Billing Period: I certify that the call charges, totalling €______, incurred by my usage of mobile phone number ___/_______ during the billing period specified above have been actually and necessarily incurred solely in relation to the public service on which I am engaged (excepting calls detailed at 2 below). Further I have highlighted, on the attached itemised bill, all charges that have been incurred by my use of the phone for personal purposes during the specified period and I undertake to make immediate arrangements to reimburse the HSE for this amount (€________). Signed __________________________________ Name __________________________________ Black Capitals ___________________________ Grade _________________________________
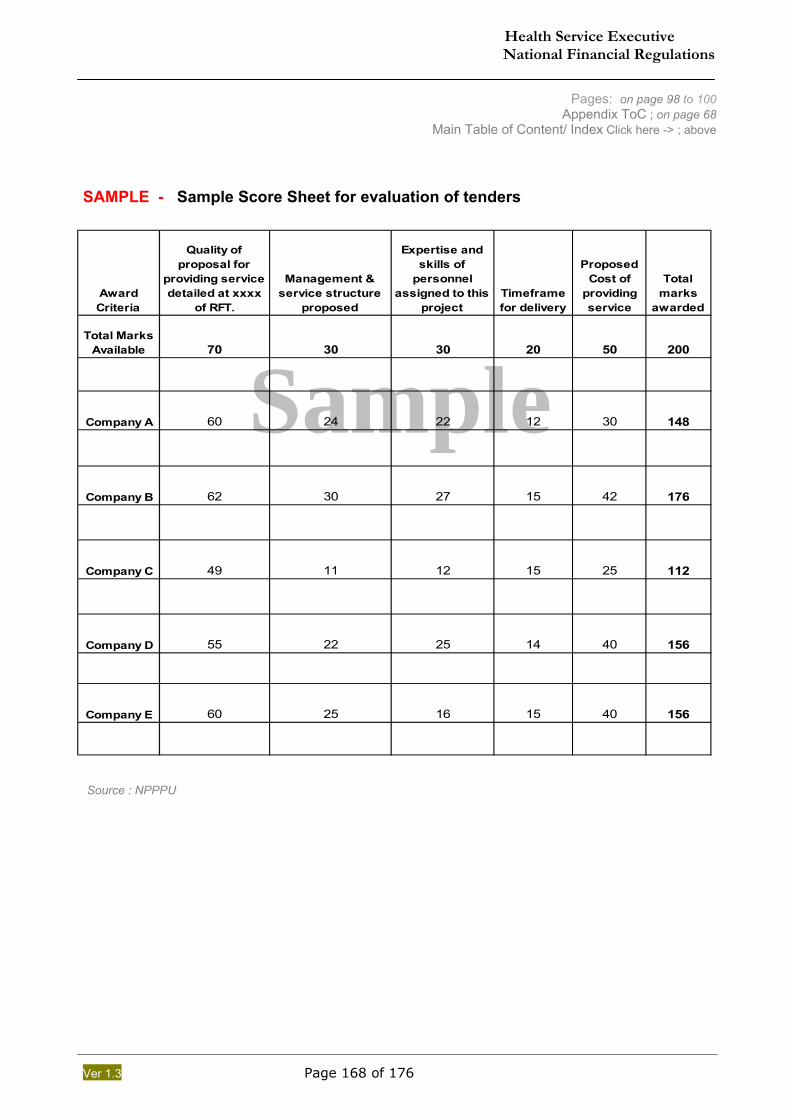
Health Service Executive National Financial Regulations
Ver 1.3 Page 168 of 176
Sample Award Criteria
Quality of proposal for
providing service detailed at xxxx
of RFT.
Management & service structure
proposed
Expertise and skills of
personnel assigned to this
projectTimeframe for delivery
Proposed Cost of
providing service
Total marks
awarded
Total Marks Available 70 30 30 20 50 200
Company A 60 24 22 12 30 148
Company B 62 30 27 15 42 176
Company C 49 11 12 15 25 112
Company D 55 22 25 14 40 156
Company E 60 25 16 15 40 156
Pages: on page 98 to 100 Appendix ToC ; on page 68
Main Table of Content/ Index Click here -> ; above SAMPLE - Sample Score Sheet for evaluation of tenders
Source : NPPPU
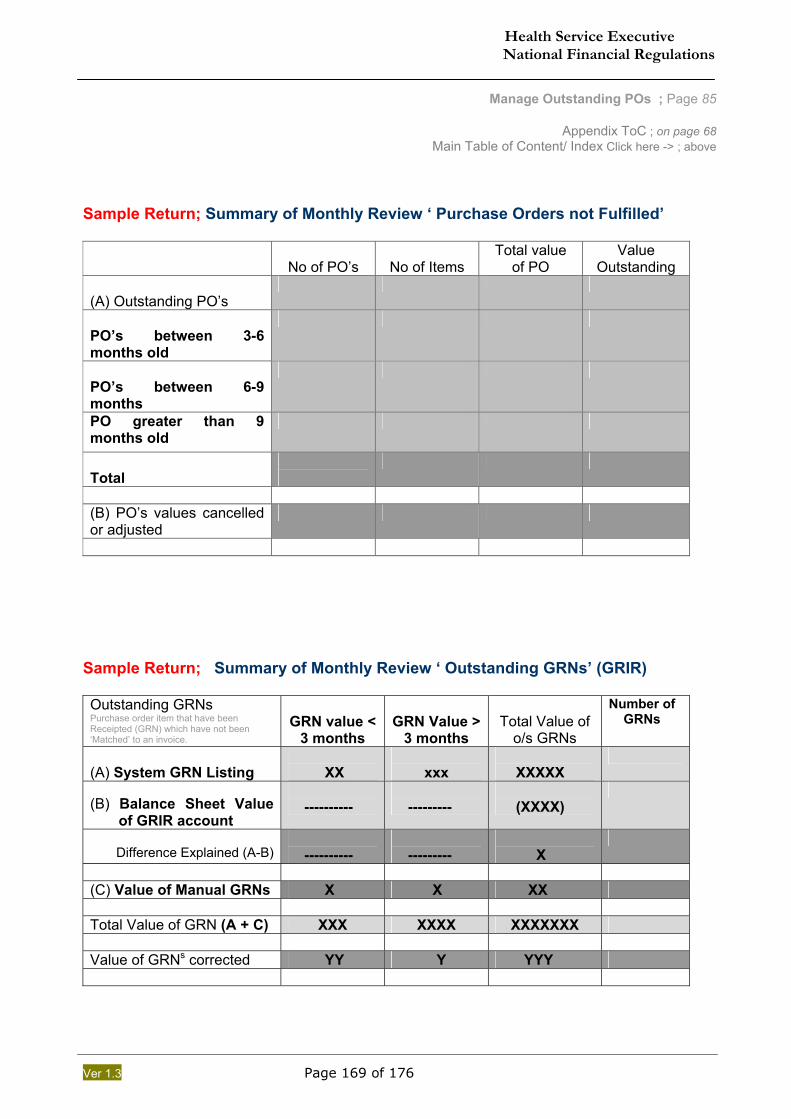
Health Service Executive National Financial Regulations
Ver 1.3 Page 169 of 176
Manage Outstanding POs ; Page 85
Appendix ToC ; on page 68 Main Table of Content/ Index Click here -> ; above
Sample Return; Summary of Monthly Review ‘ Purchase Orders not Fulfilled’
No of PO’s
No of Items Total value
of PO Value
Outstanding (A) Outstanding PO’s
PO’s between 3-6 months old
PO’s between 6-9 months
PO greater than 9 months old
Total
(B) PO’s values cancelled or adjusted
Sample Return; Summary of Monthly Review ‘ Outstanding GRNs’ (GRIR) Outstanding GRNs Purchase order item that have been Receipted (GRN) which have not been ‘Matched’ to an invoice.
GRN value <
3 months
GRN Value >
3 months
Total Value of
o/s GRNs
Number of GRNs
(A) System GRN Listing
XX
xxx
XXXXX
(B) Balance Sheet Value of GRIR account
----------
---------
(XXXX)
Difference Explained (A-B)
----------
---------
X
(C) Value of Manual GRNs X X XX Total Value of GRN (A + C) XXX XXXX XXXXXXX Value of GRNs corrected YY Y YYY
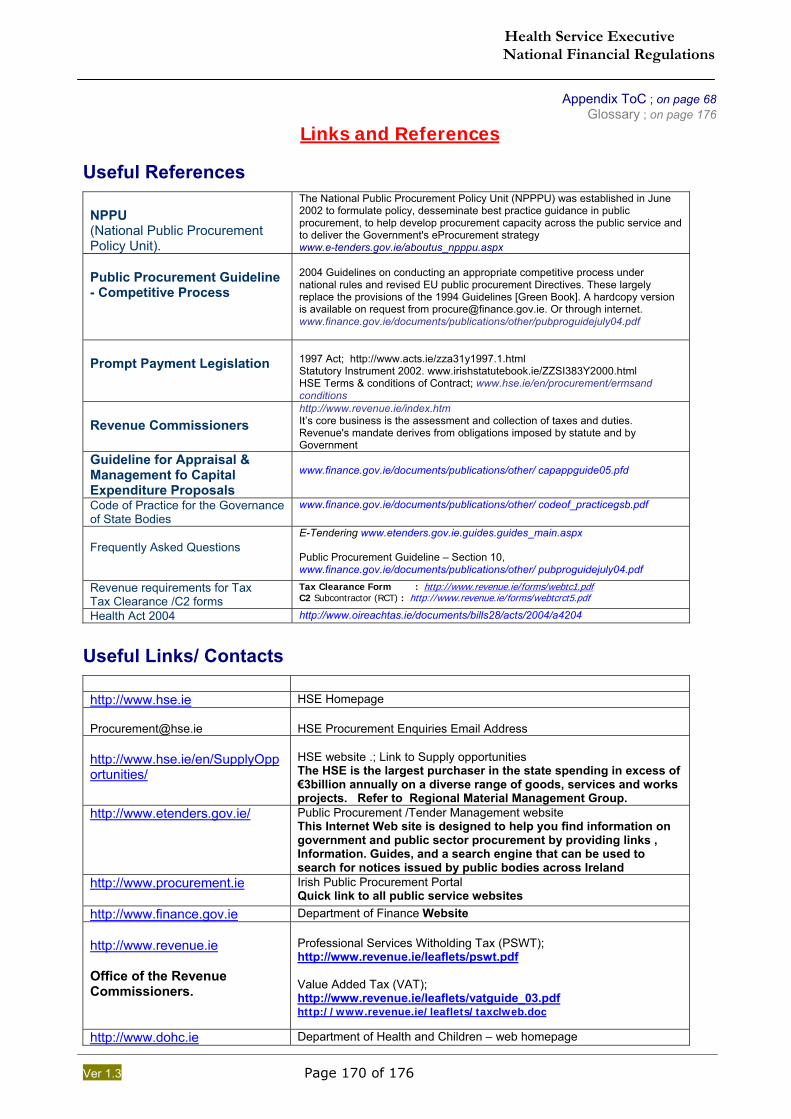
Health Service Executive National Financial Regulations
Ver 1.3 Page 170 of 176
Appendix ToC ; on page 68 Glossary ; on page 176
Links and References Useful References
NPPU (National Public Procurement Policy Unit).
The National Public Procurement Policy Unit (NPPPU) was established in June 2002 to formulate policy, desseminate best practice guidance in public procurement, to help develop procurement capacity across the public service and to deliver the Government's eProcurement strategy www.e-tenders.gov.ie/aboutus_npppu.aspx
Public Procurement Guideline - Competitive Process
2004 Guidelines on conducting an appropriate competitive process under national rules and revised EU public procurement Directives. These largely replace the provisions of the 1994 Guidelines [Green Book]. A hardcopy version is available on request from [email protected]. Or through internet. www.finance.gov.ie/documents/publications/other/pubproguidejuly04.pdf
Prompt Payment Legislation
1997 Act; http://www.acts.ie/zza31y1997.1.html Statutory Instrument 2002. www.irishstatutebook.ie/ZZSI383Y2000.html HSE Terms & conditions of Contract; www.hse.ie/en/procurement/ermsand conditions
Revenue Commissioners
http://www.revenue.ie/index.htm It’s core business is the assessment and collection of taxes and duties. Revenue's mandate derives from obligations imposed by statute and by Government
Guideline for Appraisal & Management fo Capital Expenditure Proposals
www.finance.gov.ie/documents/publications/other/ capappguide05.pfd
Code of Practice for the Governance of State Bodies
www.finance.gov.ie/documents/publications/other/ codeof_practicegsb.pdf
Frequently Asked Questions
E-Tendering www.etenders.gov.ie.guides.guides_main.aspx Public Procurement Guideline – Section 10, www.finance.gov.ie/documents/publications/other/ pubproguidejuly04.pdf
Revenue requirements for Tax Tax Clearance /C2 forms
Tax Clearance Form : http://www.revenue.ie/forms/webtc1.pdf C2 Subcontractor (RCT) : http://www.revenue.ie/forms/webtcrct5.pdf
Health Act 2004 http://www.oireachtas.ie/documents/bills28/acts/2004/a4204
Useful Links/ Contacts
http://www.hse.ie HSE Homepage [email protected]
HSE Procurement Enquiries Email Address
http://www.hse.ie/en/SupplyOpportunities/
HSE website .; Link to Supply opportunities The HSE is the largest purchaser in the state spending in excess of €3billion annually on a diverse range of goods, services and works projects. Refer to Regional Material Management Group.
http://www.etenders.gov.ie/
Public Procurement /Tender Management website This Internet Web site is designed to help you find information on government and public sector procurement by providing links , Information. Guides, and a search engine that can be used to search for notices issued by public bodies across Ireland
http://www.procurement.ie
Irish Public Procurement Portal Quick link to all public service websites
http://www.finance.gov.ie Department of Finance Website http://www.revenue.ie Office of the Revenue Commissioners.
Professional Services Witholding Tax (PSWT); http://www.revenue.ie/leaflets/pswt.pdf Value Added Tax (VAT); http://www.revenue.ie/leaflets/vatguide_03.pdf http://www.revenue.ie/leaflets/taxclweb.doc
http://www.dohc.ie Department of Health and Children – web homepage
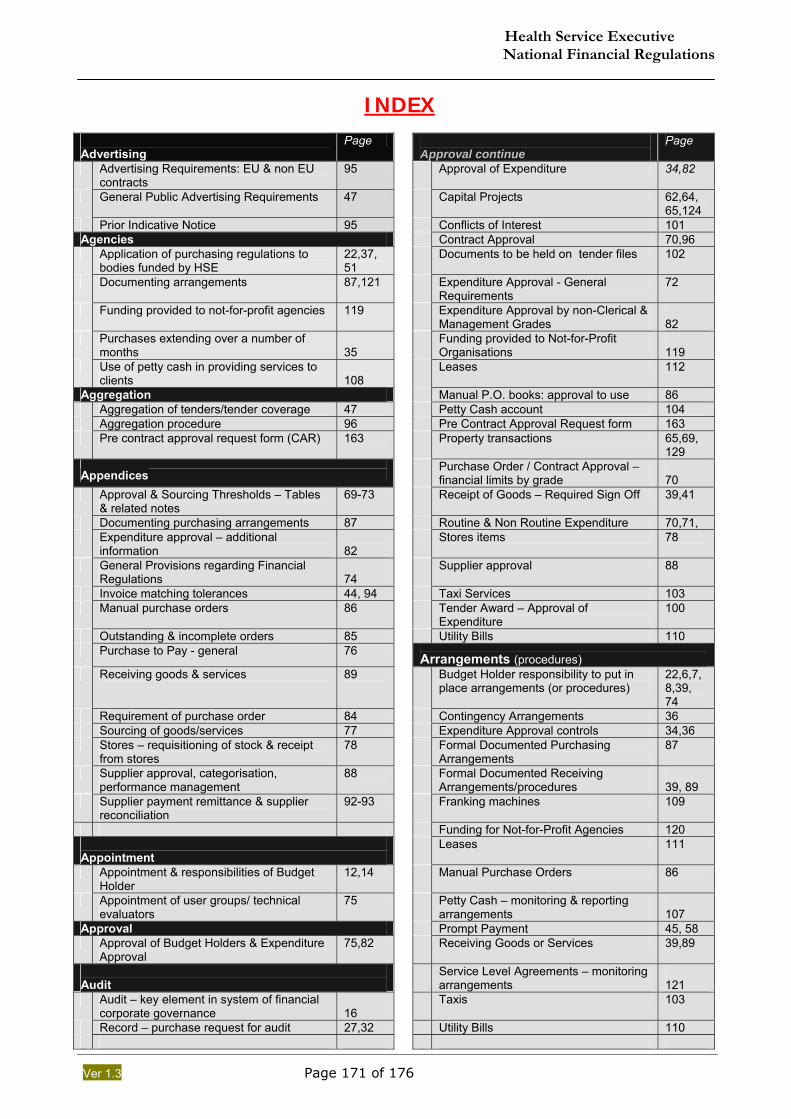
Health Service Executive National Financial Regulations
Ver 1.3 Page 171 of 176
INDEX
Advertising
Page Approval continue
Page
Advertising Requirements: EU & non EU contracts
95 Approval of Expenditure 34,82
General Public Advertising Requirements 47 Capital Projects 62,64, 65,124
Prior Indicative Notice 95 Conflicts of Interest 101 Agencies Contract Approval 70,96 Application of purchasing regulations to
bodies funded by HSE 22,37, 51
Documents to be held on tender files 102
Documenting arrangements 87,121 Expenditure Approval - General Requirements
72
Funding provided to not-for-profit agencies 119 Expenditure Approval by non-Clerical & Management Grades
82
Purchases extending over a number of months
35
Funding provided to Not-for-Profit Organisations
119
Use of petty cash in providing services to clients
108
Leases 112
Aggregation Manual P.O. books: approval to use 86 Aggregation of tenders/tender coverage 47 Petty Cash account 104 Aggregation procedure 96 Pre Contract Approval Request form 163 Pre contract approval request form (CAR) 163 Property transactions 65,69,
129 Appendices
Purchase Order / Contract Approval – financial limits by grade
70
Approval & Sourcing Thresholds – Tables & related notes
69-73 Receipt of Goods – Required Sign Off 39,41
Documenting purchasing arrangements 87 Routine & Non Routine Expenditure 70,71, Expenditure approval – additional
information 82
Stores items 78
General Provisions regarding Financial Regulations
74
Supplier approval 88
Invoice matching tolerances 44, 94 Taxi Services 103 Manual purchase orders 86 Tender Award – Approval of
Expenditure 100
Outstanding & incomplete orders 85 Utility Bills 110 Purchase to Pay - general 76
Arrangements (procedures) Receiving goods & services 89 Budget Holder responsibility to put in
place arrangements (or procedures) 22,6,7,8,39, 74
Requirement of purchase order 84 Contingency Arrangements 36 Sourcing of goods/services 77 Expenditure Approval controls 34,36 Stores – requisitioning of stock & receipt
from stores 78 Formal Documented Purchasing
Arrangements 87
Supplier approval, categorisation, performance management
88 Formal Documented Receiving Arrangements/procedures
39, 89
Supplier payment remittance & supplier reconciliation
92-93 Franking machines 109
Funding for Not-for-Profit Agencies 120 Appointment
Leases 111
Appointment & responsibilities of Budget Holder
12,14 Manual Purchase Orders 86
Appointment of user groups/ technical evaluators
75 Petty Cash – monitoring & reporting arrangements
107
Approval Prompt Payment 45, 58 Approval of Budget Holders & Expenditure
Approval 75,82 Receiving Goods or Services 39,89
Audit
Service Level Agreements – monitoring arrangements
121
Audit – key element in system of financial corporate governance
16
Taxis 103
Record – purchase request for audit 27,32 Utility Bills 110
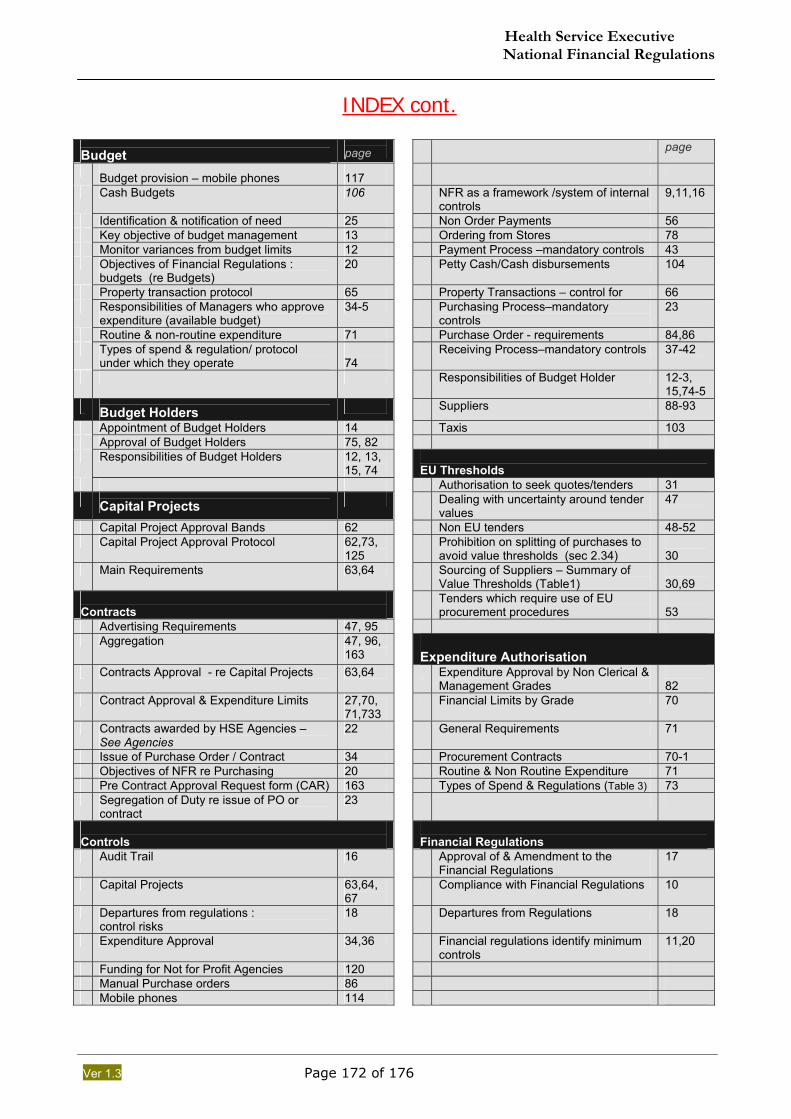
Health Service Executive National Financial Regulations
Ver 1.3 Page 172 of 176
INDEX cont.
Budget
page page
Budget provision – mobile phones
117
Cash Budgets 106 NFR as a framework /system of internal controls
9,11,16
Identification & notification of need 25 Non Order Payments 56 Key objective of budget management 13 Ordering from Stores 78 Monitor variances from budget limits 12 Payment Process –mandatory controls 43 Objectives of Financial Regulations :
budgets (re Budgets) 20 Petty Cash/Cash disbursements 104
Property transaction protocol 65 Property Transactions – control for 66 Responsibilities of Managers who approve
expenditure (available budget) 34-5 Purchasing Process–mandatory
controls 23
Routine & non-routine expenditure 71 Purchase Order - requirements 84,86 Types of spend & regulation/ protocol
under which they operate 74
Receiving Process–mandatory controls 37-42
Responsibilities of Budget Holder 12-3, 15,74-5
Budget Holders Suppliers 88-93
Appointment of Budget Holders 14 Taxis 103 Approval of Budget Holders 75, 82 Responsibilities of Budget Holders 12, 13,
15, 74
EU Thresholds Authorisation to seek quotes/tenders 31
Capital Projects Dealing with uncertainty around tender values
47
Capital Project Approval Bands 62 Non EU tenders 48-52 Capital Project Approval Protocol 62,73,
125 Prohibition on splitting of purchases to
avoid value thresholds (sec 2.34) 30
Main Requirements 63,64 Sourcing of Suppliers – Summary of Value Thresholds (Table1)
30,69
Contracts
Tenders which require use of EU procurement procedures
53
Advertising Requirements 47, 95 Aggregation 47, 96,
163
Expenditure Authorisation Contracts Approval - re Capital Projects 63,64 Expenditure Approval by Non Clerical &
Management Grades 82
Contract Approval & Expenditure Limits 27,70, 71,733
Financial Limits by Grade 70
Contracts awarded by HSE Agencies – See Agencies
22 General Requirements 71
Issue of Purchase Order / Contract 34 Procurement Contracts 70-1 Objectives of NFR re Purchasing 20 Routine & Non Routine Expenditure 71 Pre Contract Approval Request form (CAR) 163 Types of Spend & Regulations (Table 3) 73 Segregation of Duty re issue of PO or
contract 23
Controls
Financial Regulations
Audit Trail 16 Approval of & Amendment to the Financial Regulations
17
Capital Projects 63,64, 67
Compliance with Financial Regulations 10
Departures from regulations : control risks
18 Departures from Regulations 18
Expenditure Approval 34,36 Financial regulations identify minimum controls
11,20
Funding for Not for Profit Agencies 120 Manual Purchase orders 86 Mobile phones 114
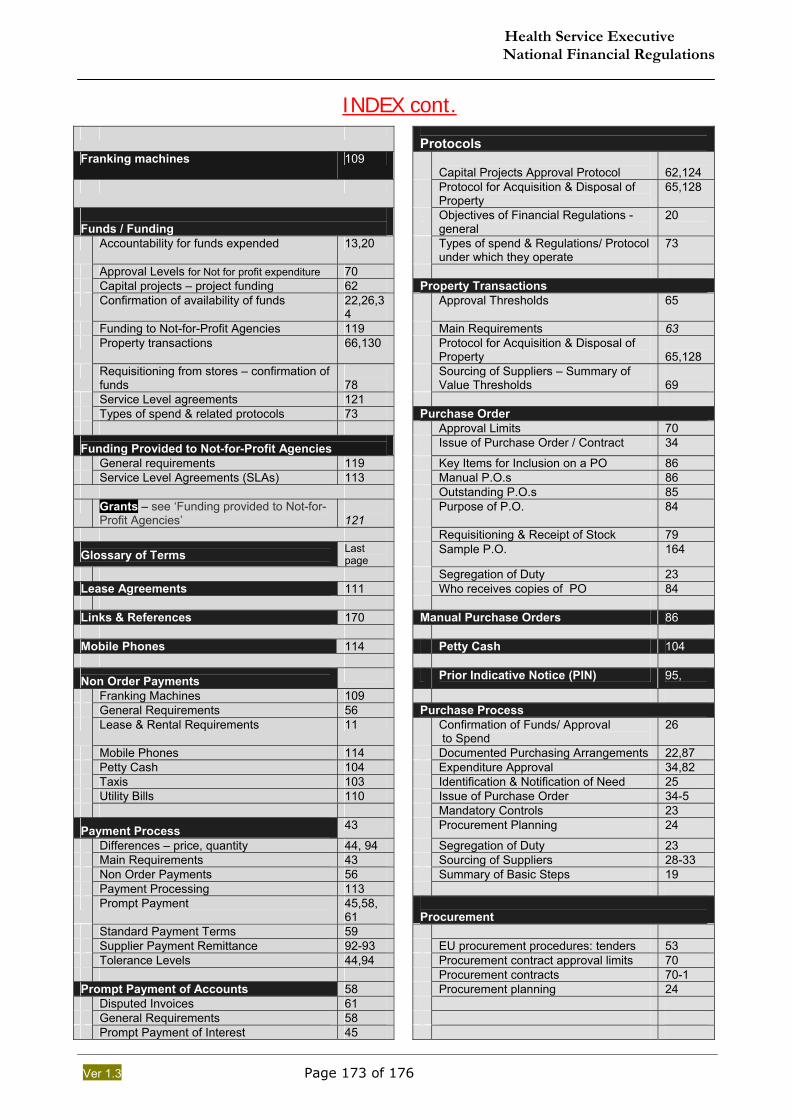
Health Service Executive National Financial Regulations
Ver 1.3 Page 173 of 176
INDEX cont.
Protocols Franking machines 109
Capital Projects Approval Protocol 62,124
Protocol for Acquisition & Disposal of Property
65,128
Funds / Funding
Objectives of Financial Regulations - general
20
Accountability for funds expended 13,20 Types of spend & Regulations/ Protocol under which they operate
73
Approval Levels for Not for profit expenditure 70 Capital projects – project funding 62 Property Transactions Confirmation of availability of funds 22,26,3
4 Approval Thresholds 65
Funding to Not-for-Profit Agencies 119 Main Requirements 63 Property transactions 66,130 Protocol for Acquisition & Disposal of
Property 65,128
Requisitioning from stores – confirmation of funds
78
Sourcing of Suppliers – Summary of Value Thresholds
69
Service Level agreements 121 Types of spend & related protocols 73 Purchase Order Approval Limits 70
Funding Provided to Not-for-Profit Agencies Issue of Purchase Order / Contract 34
General requirements 119 Key Items for Inclusion on a PO 86 Service Level Agreements (SLAs) 113 Manual P.O.s 86 Outstanding P.O.s 85 Grants – see ‘Funding provided to Not-for-
Profit Agencies’ 121
Purpose of P.O. 84
Requisitioning & Receipt of Stock 79
Glossary of Terms Last page
Sample P.O. 164
Segregation of Duty 23 Lease Agreements 111 Who receives copies of PO 84 Links & References 170 Manual Purchase Orders 86 Mobile Phones 114 Petty Cash 104
Non Order Payments Prior Indicative Notice (PIN) 95,
Franking Machines 109 General Requirements 56 Purchase Process Lease & Rental Requirements 11 Confirmation of Funds/ Approval
to Spend 26
Mobile Phones 114 Documented Purchasing Arrangements 22,87 Petty Cash 104 Expenditure Approval 34,82 Taxis 103 Identification & Notification of Need 25 Utility Bills 110 Issue of Purchase Order 34-5 Mandatory Controls 23
Payment Process 43 Procurement Planning 24
Differences – price, quantity 44, 94 Segregation of Duty 23 Main Requirements 43 Sourcing of Suppliers 28-33 Non Order Payments 56 Summary of Basic Steps 19 Payment Processing 113 Prompt Payment 45,58,
61
Procurement Standard Payment Terms 59 Supplier Payment Remittance 92-93 EU procurement procedures: tenders 53 Tolerance Levels 44,94 Procurement contract approval limits 70 Procurement contracts 70-1 Prompt Payment of Accounts 58 Procurement planning 24 Disputed Invoices 61 General Requirements 58 Prompt Payment of Interest 45
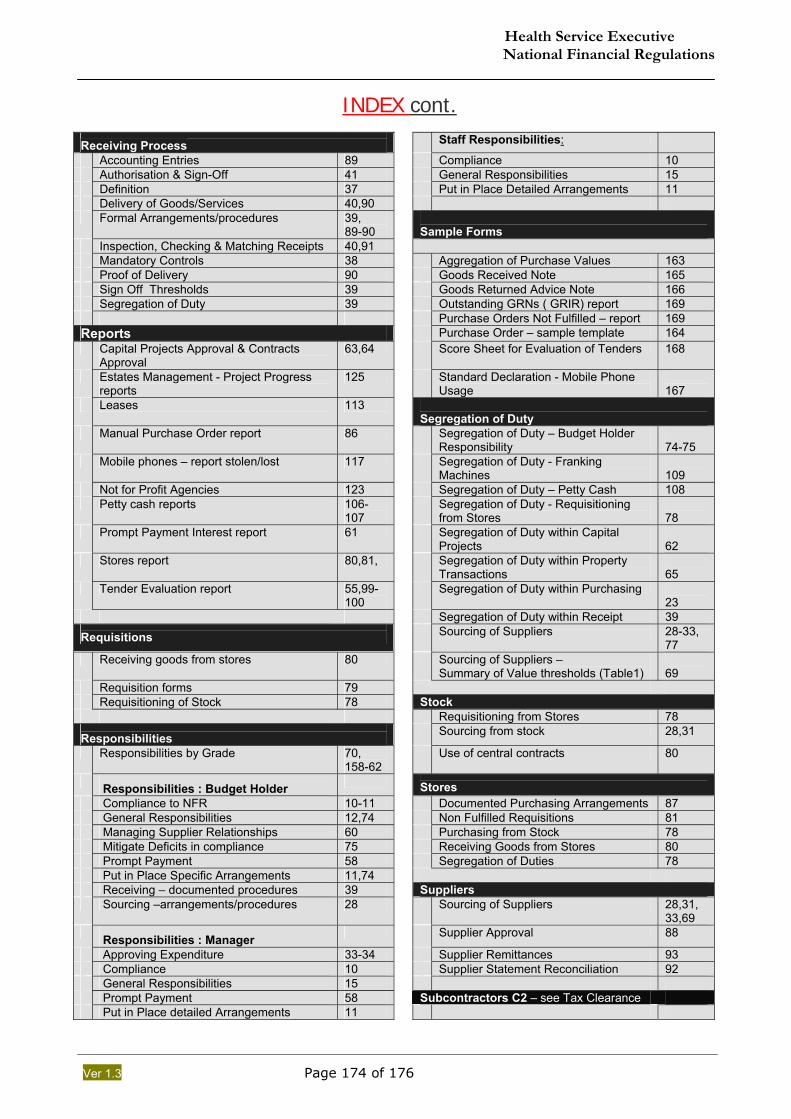
Health Service Executive National Financial Regulations
Ver 1.3 Page 174 of 176
INDEX cont.
Receiving Process Staff Responsibilities:
Accounting Entries 89 Compliance 10 Authorisation & Sign-Off 41 General Responsibilities 15 Definition 37 Put in Place Detailed Arrangements 11 Delivery of Goods/Services 40,90 Formal Arrangements/procedures 39,
89-90
Sample Forms Inspection, Checking & Matching Receipts 40,91 Mandatory Controls 38 Aggregation of Purchase Values 163 Proof of Delivery 90 Goods Received Note 165 Sign Off Thresholds 39 Goods Returned Advice Note 166 Segregation of Duty 39 Outstanding GRNs ( GRIR) report 169 Purchase Orders Not Fulfilled – report 169 Reports Purchase Order – sample template 164 Capital Projects Approval & Contracts
Approval 63,64 Score Sheet for Evaluation of Tenders 168
Estates Management - Project Progress reports
125 Standard Declaration - Mobile Phone Usage
167
Leases 113 Segregation of Duty
Manual Purchase Order report 86 Segregation of Duty – Budget Holder Responsibility
74-75
Mobile phones – report stolen/lost 117 Segregation of Duty - Franking Machines
109
Not for Profit Agencies 123 Segregation of Duty – Petty Cash 108 Petty cash reports 106-
107 Segregation of Duty - Requisitioning
from Stores 78
Prompt Payment Interest report 61 Segregation of Duty within Capital Projects
62
Stores report 80,81, Segregation of Duty within Property Transactions
65
Tender Evaluation report 55,99-100
Segregation of Duty within Purchasing 23
Segregation of Duty within Receipt 39
Requisitions Sourcing of Suppliers 28-33, 77
Receiving goods from stores 80 Sourcing of Suppliers – Summary of Value thresholds (Table1)
69
Requisition forms 79 Requisitioning of Stock 78 Stock Requisitioning from Stores 78
Responsibilities Sourcing from stock 28,31
Responsibilities by Grade 70, 158-62
Use of central contracts 80
Responsibilities : Budget Holder
Stores Compliance to NFR 10-11 Documented Purchasing Arrangements 87 General Responsibilities 12,74 Non Fulfilled Requisitions 81 Managing Supplier Relationships 60 Purchasing from Stock 78 Mitigate Deficits in compliance 75 Receiving Goods from Stores 80 Prompt Payment 58 Segregation of Duties 78 Put in Place Specific Arrangements 11,74 Receiving – documented procedures 39 Suppliers Sourcing –arrangements/procedures 28 Sourcing of Suppliers 28,31,
33,69
Responsibilities : Manager Supplier Approval 88
Approving Expenditure 33-34 Supplier Remittances 93 Compliance 10 Supplier Statement Reconciliation 92 General Responsibilities 15 Prompt Payment 58 Subcontractors C2 – see Tax Clearance Put in Place detailed Arrangements 11
Health Service Executive National Financial Regulations
Ver 1.3 Page 175 of 176
INDEX cont. Tables Voluntary Bodies 1. Sourcing of Suppliers –
summary of value thresholds 69 Funding of Not for Profit Agencies 119
2. Purchase Order/Contract Approval – Financial Limits by Staff Grade
70 Services provided over months / years (paragraph 2.59.2)
36
3. Types of Spend & Regulations / Protocols under which they Operate
73
Voluntary / Not for Profit Expenditure Approval Limits: Table 2
70
Taxis 103 Tax Clearance Certificates (TCC) &C2 Links to application forms
27, 170
Works
Advertisement 47, 95 Tenders Approval Limits by staff grade 74 Advertising Requirements 47, 5 Professional input to tendering 25, 46 Aggregation of Tenders 47,
95 Sourcing of Suppliers – Summary of
Value Thresholds 69
Documentation to be held on file 102 Tenders for Construction Works & Related Services
46
General Requirements – Tenders 54, 97 Types of Spend & Regulations 74 MEAT Basis of Evaluation 99 Value Thresholds for Sourcing 69 Notification of Results of Tenders 101 Works contracts awarded by ext. orgs. 14 Professional Input to Tendering 46 Written decision for receipt of goods,
services & works 42
Purchase Order/Contract Approval Limits by Staff Grade: Table 2
70
Receipt of Tenders 54, 97
Written Decisions
Restricted Tendering 50 Approval of Managers as Budget Holders
75
Tender Award 100 Authorisation to seek quotes 31 Tender Evaluation 98 Decisions – see requirement for Written
Decisions
Types of Tenders - EU 53 Approval of Managers as Budget Holders
75
Types of Tenders – Non EU 48 Authorisation to seek quotes 31 Mobile Phone Approval 114 Utility Bills 110 Operating Lease Approval 112 Value Thresholds
Petty Cash Approval – formal approval 104
Authorisation to seek quotes/tenders 31 Receipt of Goods & Services 37,42 Capital Projects Approval Bands 64 Requirement for Written Decisions-
General 36,
Dealing with uncertainty around likely tender values
47 Requirement for Written Decisions – Expenditure approval (para2.11.5 & A2.16)
23 82
Expend. approval – Limits by grade 70 Petty Cash 104
Requirement for Written Decisions – Receipt of Goods/Services
37, 42
Prohibition on splitting of purchases 30 Tender Award 55, 100 Property Protocol Approval Thresholds 63 Public Advertising Requirements 95 Service Level Agreements 121 Services provided over a period of months
or years 90
Sourcing of Suppliers 30,69 Tenders 53,69 Voluntary Bodies Expenditure Approval Limits 70 Funds provided to Not for Profit orgs 119 Prompt Payment of Interest 45 Securing the State’s interest 88
End of index. Version 1.3 (.3) ,
October 2006

Health Service Executive National Financial Regulations
Ver 1.3 Page 176 of 176
Glossary of Terms G 1 Audit Trail - A visible trail of evidence enabling a person to trace information in the financial statements or other information reported back to the original source document. For example, Purchase of Lab Supplies can reported in the AFS can be tracked back to the respective individual transactions, including supporting authorised Purchase Requisition or Order, Goods Received Note (& Proof of Delivery) , invoice and payment details. G 2 Aggregate Demand (Aggregation) – term used to describe the maximum potential quantity/ value that could be considered when sourcing particular goods or services. Refer to RMM Aggregation procedure on pages 47& 96. G 3 Financial Information System (FIS) ; the computerised accounting system used for recording financial transactions and balances. A number of different systems are used by the HSE include Aran and SAP. G 4 Most Economically Advantageous Tender (MEAT) Please refer to Tender Evaluation section above that explains the applications of the Most Economically Advantageous Tender principle(see 3.30, on page 54).
G 5 Contingency Arrangements; procedures to be put in place to address what actions should be taken for
unforeseen events e.g. if someone was out on unplanned leave and departure from regulations were required.
G 6 Nominated Receipting Location; This refers to the physical location where it has been agreed that goods are delivered. This could be a Stores location, direct delivery to a client, or delivery to the requester. G 7 Prompt Payment Interest. The HSE is required to calculate and pay late payment interest for every commercial transactions not paid within the Relevant Payment Date. Amounts of late payment interest less than €5 are not payable. Ref 1997 Prompt Payment Act and 2002 Statutory Instrument No.388. See ‘Links’ on page 170.
G 8 Routine versus Non Routine Expenditure – Routine expenditure relates to good/services consumed by the HSE on a daily basis to support the provision of services. In general terms it can be considered all non pay expenditure except that excluded. Note that expenditure approval is not the same as Contract approval where a procurement contract may be put in place for a number of years.
Routine expenditure excludes; (i) Capital Projects – Capital funded expenditure plus non routine Revenue funded expenditure above €500k should be
dealt with in accordance with the Capital Approvals Protocol. (ii) Property Transactions – dealt with under Property Transactions Protocol. (iii) Non Routine Expenditure Non Routine expenditure - primarily relates to ; (i) Commissioning new or expanded Service within HSE and from other Public/private or voluntary providers (ii) Purchase of new equipment that is paid out of Revenue funds (iii) Construction type work (building/extension/repairs/ refurbishment) paid for out of revenue funds which goes beyond
ordinary day to day maintenance /repairs. Above €500k revenue funded works should be dealt with in accordance with the Capital Approvals Protocol
Examples of Routine Expenditure; (a) Existing level of service (b) Renewal of Voluntary Provider / s.65 etc budget / SLA for existing level of services (c) Amendments to Voluntary Provider / s.65 budget for pay awards, non pay inflation etc (d) Approval of price increases for existing home help hours, home care packages, foster care places, private nursing home beds etc. (e) Repairs / servicing of equipment (f) Normal maintenance (g) Stock (normal) (h) Demand Led Schemes (Community Drugs Schemes, Aids / Appliances, Chiropody, Optical, Maternity, DTSS, Immunisation, Allowances)
Examples of NON Routine Expenditure; (1) Provision of a new service (direct or via voluntary / s.65 etc) , (2) Expansion of a service (direct or via voluntary / s.65 etc) (3) Additional Home help hours, home care packages, foster care places, private nursing home beds etc. (4) Purchase of Equipment (5) Construction / Refurbishment / Backlog Maintenance beyond the limits of routine expenditure (6) Expenditure which acquires or creates an asset or significantly enhances the value and / or useful economic life of an existing asset
G 9 Good Received Note (GRN) ; A goods received note is a record that documents the receipt of Goods or Services received from external sources. A goods receipt note may be a manual (hardcopy) record or entry within the Financial Information System. A GRN record should be supported by a supplier’s ‘Proof of Delivery’, Professional Valuation/Certification.
G 10 Accrual (s) – A financial record of the value of expenditure for goods or services incurred (but not necessarily invoiced by the supplier) within the period to which it relates. For example if someone received and used goods in January, this ‘consumption’/expense should be recorded in the Financial Information System irrespective as to whether the invoice has been received from the supplier and processed in the system.
G 11 Proof of Delivery (POD) is a notification (normally paper based) of advice or other document generated by the vendor that records the delivery of goods. In recent time, some suppliers rely on Couriers to deliver and record evidence of receipt of Goods – the advis/POD may be in the form of an electronic tracking number. The POD is a key document which, when properly signed provides evidences receipt of Goods or Services.
G 12 Prior Indicative Notice is an EU Tender procedure relating to publication of information in advance of Actual Tender publication. PIN can be published (normally at the beginning of financial period) either on the OJEU or E-Tenders website, setting out categories of products/services. Publication of a PIN reduces the minimum time required for tendering.
G 13 A Petty Cash ‘Imprest’ refers to the amount at which a petty cash balance has been set and for which a individual location is accountable.