Embed Size (px)
Citation preview
Deborah Carr, James S House, Randolph Nesse, and CamilleWortman
Forewarning of Spouse's Death and PsychologicalAdjustment to Widowhood among Older Adults
Report No. 00-462
Research Report
POPULATION STUDIES CENTERAT THE INSTITUTE FOR SOCIAL RESEARCH
UNIVERSITY OF MICHIGAN
PSC

PSC Publications Population Studies Center, University of Michiganhttp://www.psc.isr.umich.edu/pubs/ PO Box 1248, Ann Arbor, MI 48106-1248 USA
The Population Studies Center at the University of Michigan is one of the oldest population centers in theUnited States. Established in 1961 with a grant from the Ford Foundation, the Center has a rich history as themain workplace for an interdisciplinary community of scholars in the field of population studies. Today theCenter is supported by a Population Research Center Core Grant from the National Institute of Child Healthand Human Development (NICHD) as well as by the University of Michigan, the National Institute on Aging,the Hewlett Foundation, and the Mellon Foundation.
PSC Research Reports are prepublication working papers that report on current demographic researchconducted by PSC associates and affiliates. The papers are written by the researcher(s) for timelydissemination of their findings and are often later submitted for publication in scholarly journals. The PSCResearch Report Series was begun in 1981 and is organized chronologically. Copyrights are held by theauthors. Readers may freely quote from, copy, and distribute this work as long as the copyright holder andPSC are properly acknowledged and the original work is not altered.

Forewarning of Spouse’s Death and Psychological Adjustment toWidowhood Among Older Adults
Deborah CarrAssistant Professor of Sociology and Assistant Research Scientist, Population Studies Center and Survey
Research Center, University of Michigan
James S. HouseProfessor of Sociology, and Director, Survey Research Center, University of Michigan
Randolph NesseProfessor of Psychiatry and Faculty Associate, Survey Research Center, University of Michigan
Camille WortmanProfessor of Psychology, State University of New York at Stony Brook
Acknowledgements: This research was supported by Grants R01-AG15948 and P01-AG05561 from theNational Institute of Aging, and from the Nancy Pritzker Research Network. Address correspondence toDeborah Carr, Department of Sociology, University of Michigan, 500 S. State Street, Ann Arbor, MI48109. E-mail: [email protected].

ABSTRACT
Forewarning of Spouse’s Death and Psychological Adjustment toWidowhood Among Older Adults
This study examined: (1) whether psychological adjustment to widowhood is affected by the amount offorewarning prior to spouse’s death; (2) whether the effect of forewarning differs for men and women;and (3) the extent to which the effect of forewarning is mediated or suppressed by death contextcharacteristics (i.e., pre-death care giving, nursing home usage, spouse age at death and couplecommunication about the impending death). Analyses are based on data from The Changing Lives ofOlder Couples (CLOC) study, a probability sample of 1,532 married individuals age 65 and older forwhom baseline information was collected in 1987-88, with widows reinterviewed 6, 18, and 48 monthsafter spousal loss.
Overall, the effects of death forewarning (and sudden death) were quite limited; forewarning didnot significantly affect depression, anger, shock, or overall grief six or 18 months after the loss. Prolongedforewarning (i.e., more than six months warning) was associated with elevated levels of anxiety both sixand 18 months after the death. Sudden death was a positive and significant predictor of intrusive thoughtsat the six-month follow up only. Warning time had significantly different effects on men’s and women’syearning. At both six and 18 months after the loss, sudden death was associated with slightly higher levelsof yearning among women, but with significantly lower yearning among men. The findings call intoquestion the widespread belief that grief is more severe if the death was sudden. Understanding how deathforewarning affects diverse aspects of older widowed persons’ well-being is critically important today, aschronic diseases account for the majority of older adults’ deaths.
Dataset used: Changing Lives of Older Couples (CLOC) Study: United States, 1987-1994
Widowhood is characterized as among the most stressful of life events (Holmes & Rahe,1967). The psychological consequences of widowhood vary widely, however, based oncharacteristics of the survivor (Matthews, 1991; Stroebe & Stroebe, 1983; Umberson, Wortman &Kessler, 1992), the deceased (Parkes, 1985; Reed, 1998), and the marital relationship (Carr et al.,2000). The context of the death - including whether the death was sudden or the endpoint of a longand lingering illness - is also an important influence on patterns of grief (Ball, 1977; Carey, 1979-80;Lundin, 1984; O�Bryant, 1990-1991; Rando 1986; Smith, 1978; Vachon et al., 1982). Numerousstudies explore whether sudden or anticipated deaths are more distressing for bereaved spouses, butthis research is inconclusive and does not specifically address the unique circumstances of the elderlybereaved. Understanding the linkage between death forewarning and older widowed persons� well-being is critically important today as chronic diseases, or ongoing conditions for which there is nocure, account for the majority of older adults� deaths (McLeroy & Crump, 1994; Olshansky & Ault,1986). Furthermore, advances in medical technology which delay old-age mortality mean thatinterval between diagnosis and death is lengthening. It is thus critically important that scholars andpractitioners understand how the �living-dying interval� affects survivors� adjustment (Pattison,1977, 1978).
Theoretical Issues
The proposition that sudden deaths are more difficult for family members to cope with thananticipated deaths was first suggested in Lindemann�s (1944) classic article �Symptomatology andManagement of Acute Grief.� Lindemann found that spouses of the men serving in World War IIexperienced grief-like symptoms (or �anticipatory grief�) before their spouses actually died. Militarywives tended to emotionally detach in anticipation of their spouses� deaths, and thus did not appear tobe highly grief-stricken upon the actual death. In contrast, the relatives of the 500 persons killedsuddenly in a nightclub fire suffered more severe symptoms of grief. Building upon this work, manygrief scholars have concluded that individuals who anticipate their spouse�s death will use theforewarning period to make peace with their partner, to disengage from the relationship, and toprepare psychologically and practically for the transition to widowhood. Although spouses mayexhibit grief-like symptoms or �anticipatory grief� during the pre-death period, their adjustmentfollowing the death is believed to be better than those who experienced an unexpected and suddenloss (Gerber, 1974:27; Rando, 1986; Vachon et al.. 1982).
Empirical studies examining the effect of death forewarning on widowed persons�psychological adjustment to loss are inconclusive, however. A considerable body of researchsuggests that sudden death is associated with poorer psychological adjustment among spouses of thedeceased (Ball, 1977; Carey, 1979-80; Farberow, Gallagher-Thompson, Gilewski and Thompson,1992; Glick, Weiss & Parkes 1974; Hill, Thompson & Gallagher, 1988; Jacobs, Kasl & Ostfeld,1986; Lundin, 1984; O�Bryant, 1990-1991; Smith, 1978; Vachon et al., 1982; Wells & Kendig, 1997;Willis et al., 1987; Zisook, Schuchter & Lyons 1987). A smaller group of studies find the reverse -that forewarning is linked to poorer physical and mental health among widowed persons. (Fengler &Goodrich, 1979, Gerber et al., 1975; Sanders, 1982-83; Schwab et al., 1975). Others, still, find norelationship between death forewarning and survivors� psychological adjustment (Bowling &Cartwright, 1982; Clayton et al., 1973; Hill et al. 1988; Maddison & Walker, 1967; McGloshen &O�Bryant, 1988; Roach & Kitson 1989; Sanders 1982).
We believe that there are four reasons for these inconclusive findings. First, few studiesexplicitly acknowledge that the age of the deceased may condition the effects of forewarning onwidowed persons� well-being. For older adults, even �sudden� deaths may be anticipated and viewedas timely (Neugarten & Hagestad, 1976). Second, the larger context of the death is rarely considered(Sweeting & Gilhooly, 1990). Factors associated with forewarning, such as the stress of a spouse�s
ongoing illness, the physical and emotional strain of caregiving, social isolation, and the depletion ofeconomic resources may lead to poorer adjustment following the death, and thus may cancel out thegains presumably provided by the period of pre-death anticipation and preparation (Rando, 1986:7;Siegel & Weinstein, 1983). Third, a diverse set of outcome measures (e.g., depression, grief, andphysical health) and inconsistent definitions of �sudden� versus �anticipated� death have been usedin past studies, thus limiting the comparability of findings across studies. Finally, because most pastresearch has relied on cross-sectional rather than longitudinal data, baseline demographic andsocioeconomic characteristics which affect both death timing and psychological adjustment (e.g.,age, sex, income, respondent�s pre-widowhood psychological and physical health) may have beenomitted. Consequently, past studies have not always acknowledged the possibility of a spuriousrelationship between death forewarning and psychological adjustment.
Death Forewarning among Older Adults
Surprisingly few studies examine the effects of sudden versus anticipated death on olderwidowed persons� well-being; rather, most focus on sudden deaths which are also premature or �off-time� deaths to the young. Lindemann (1944) focused on the wives of World War II soldiers and thefamily members of undergraduates who died in a fire. In the 1950s and 1960s, studies typicallyfocused on the parents of young children suffering from terminal illnesses (Binger et al., 1969;Bozeman, Orbach & Sutherland, 1955; Chodoff, Friedman, & Hamburg, 1964; Natterson &Knudson, 1960; Richmond & Waisman, 1955). Studies of death forewarning and spousal loss havefocused overwhelmingly on young and midlife widowed persons� adjustment (Ball, 1977; Glick,Weiss & Parkes, 1974; Lundin, 1984; Parkes & Weiss, 1983; Sanders, 1982-83; Vachon et al., 1976).Other studies have focused solely on sudden deaths occurring under particularly horrificcircumstances such as murders (Rynearson, 1984) or suicides (Calhoun & Allen, 1991; Dunn &Morrish-Vidners, 1987; Reed, 1998; van der Wal, 1989-90). Thus, the effects of death forewarningmay be confounded with type of death. Because deaths of young people and violent deaths areconsidered the most difficult to cope with (Archer, 1999; Parkes & Brown, 1972; Reed, 1998; Roach& Kitson, 1989; Smith, 1978; Vachon et al., 1976), it is not clear whether the deleterious effects aredue to suddenness or life stage. Hence, sudden deaths to older adults which occur under fairly normalcircumstances may not be as traumatic as past research suggests.
For older adults (i.e., age 65 and older), even �sudden� deaths may be at least somewhatanticipated: �beyond a certain age, death is expected and viewed as timely� (Archer, 1999, p. 232).Given that predictable life events are presumed to be less stressful than unexpected life events(George, 1993; Pearlin, 1982; Pearlin & Lieberman, 1979; Thoits, 1983), sudden death may be nomore difficult for the elderly survivor than deaths following a long period of illness (DeSpelder &Strickland, 1992; Hyman, 1983). Moreover, sudden spousal deaths are more likely to be anticipatedby older women than older men. Because of men�s mortality disadvantage, women age 65 and olderoutnumber older men by roughly 1.5 to 1 (U.S. Bureau of the Census, 1996). Nearly half ofAmerican women age 65 and older are widowed, compared to 14 percent of men. Noting the gendergap in mortality, Neugarten & Hagestad (1976) observed that women may go through a �rehearsalfor widowhood� as they observe their peers experience the loss of spouse (Fooken 1985, p. 98).Consequently, sudden death may have a more deleterious effect on the well-being of men thanwomen, as older women are more likely to expect and prepare for the death of their spouse - even iftheir spouse is in reasonably good health (Hill et al., 1988, p. 795).
Death Context and Forewarning
A second reason for the inconclusive findings of past studies is that empirical analyses haverarely controlled important contextual factors related to the death. This omission is critical, as theeffects of death timing and other characteristics of the death may counteract one another. Forinstance, while prolonged forewarning periods are characterized as a time when spouses can preparepsychologically and practically for the loss (Kalish 1981; Rando 1986), the warning period may alsobe accompanied by difficult caregiving duties (Anashensel, Pearlin, Mullan, Zarit & Whitlach, 1995;George & Gwyther, 1986; Norris & Murrell, 1987; Wells & Kendig, 1997), emotional isolation fromfamily members and friends (Kramer, 1996-97), and the neglect of one�s own health (Fengler &Goodrich, 1979; Rosenblatt, 1983; Sanders, 1982-3; Siegel & Weinstein, 1983; Sweeting &Gilhooly, 1990). Stress related to the �extended death watch� period (Gerber et al., 1975) may beparticularly difficult for older adults due to their age and accompanying health problems (Averill &Wisocki, 1981; Fengler & Goodrich, 1979; George & Gwyther, 1986).
Factors correlated with death forewarning also might be associated with better spousaladjustment (O�Bryant, 1990-91). Caregiving may increase closeness with an ill relative (Hinrichsen,Hernandez & Pollack, 1992; Vachon et al., 1982; Wilson, 1990), and may provide a sense of purposeto the caregiver (O�Bryant, Straw & Meddaugh, 1990; Wright, 1991). Moreover, older individualssuffering prolonged illnesses are more likely to reside in nursing homes (Foner, 1994), and thus theirspouses may make a smoother transition to widowhood. The institutionalization process has beencharacterized as �quasi-widowhood,� because spouses have considerably reduced daily contact andcommunication, may emotionally separate from one another, and are spared the daily stresses ofdirect caregiving (DeSpelder & Strickland, 1992; Rosenthal & Dawson, 1993). Thus, our analysesinclude three important indicators of death context which may mediate (or suppress) the effect ofdeath timing on widowed persons� adjustment: age of spouse at death, whether the deceased wasliving in a nursing home prior to death, and whether the survivor provided care prior to their spouse�sdeath.
Knowledge about the impending death also may affect the couple�s interactions during the illspouse�s last days. Couples who anticipate a death may use the forewarning period to make practicalplans for the survivor�s economic and social adjustment, which may enable a smoother transition towidowhood (Rando, 1986). Moreover, couples who use the time between diagnosis and death toresolve emotional �unfinished business� (Blauner, 1966) may find their relationships strengthened inthe final days. Bereaved persons who were by their ailing spouse�s side at the moment they died havebeen found to cope better with the loss than those who did not reach such closure (Bennett & Vidal-Hall, 2000; Fiewiger & Smilowitz 1984-5; Hinds, 1985). Although theoretical writings and clinicalresearch suggest that individuals who anticipate their spouse�s death may use the pre-death period asa time to prepare emotionally for the loss, and to seek closure in their relationship, we know of nostudies which empirically assess whether these behaviors mediate the relationship between deathforewarning and psychological adjustment (Bennett & Vidal-Hall, 2000; Pattison, 1977;1978; Siegel& Weinstein, 1983). Thus, our analyses include indicators of whether the couple talked about howthe survivor would cope with being alone, and whether the survivor was with their spouse at themoment they died.
Measuring Death Forewarning and Adaptation to Loss
The discrepant results in past studies may reflect differences in the conceptualization andmeasurement of both independent and dependent variables (Sweeting and Gilhooly 1990). Theoperationalization of sudden versus anticipated death varies across studies. Some researchers definesudden deaths as those where the deceased was dead on arrival at the hospital (Carey, 1979-80),

while others consider sudden deaths those where the survivor had less than two hours (Lundin, 1984),one week (Sanders, 1982-83) or two weeks (Bowling & Cartwright, 1982) warning. As noted earlier,other studies consider sudden deaths to be synonymous with violent deaths such as suicides, murders,or accidents (Calhoun & Allen, 1991; Dunn & Morrish-Vidners, 1987; Rynearson, 1984; van derWal, 1989-90). Definitions of �prolonged� forewarning also vary, from one month (Bornstein et al.,1973; Clayton et al., 1973) or two months (Vachon et al., 1982; Gerber et al., 1975 ) up to six monthsor longer (Clayton et al., 1973).
The dependent variables used across studies also are diverse, ranging from self-report ofmedical symptoms (Gerber et al., 1975), to depressive symptomatology (Clayton et al., 1973) andsocial isolation (Parkes & Weiss, 1983). Although a handful of studies have focused on specificsymptoms, such as anger, guilt, and rumination (Sanders, 1982-83; Glick et al. 1974), most focus onglobal indicators of mental health such as depression, or broad grief scales (Carey, 1979-80; Fulton &Fulton, 1972; Clayton et al., 1968). Consequently, findings purported to characterize the general linkbetween forewarning and adjustment instead may be specific to particular outcomes.
We believe that psychological adjustment to loss encompasses a complex set of emotional,cognitive, and behavioral reactions. Thus, in this analysis we explore the effect of death forewarningand sudden death on five loss-related (i.e., shock, anger, yearning, intrusive thoughts, and overallgrief) and two general (i.e., depression and anxiety) dimensions of psychological adjustment both sixand 18 months after the death. Moreover, rather than operationalizing �sudden death� and �prolongedforewarning� a priori, we empirically evaluate diverse measures of each construct, in order toascertain the specific nature of the relationship between death forewarning and adjustment of olderadults. Drawing on past research and theory, we evaluate three possible relationships; sudden deatheffects only, linear effects of warning time, and curvilinear effects of warning time. Thus, ouranalyses will evaluate whether a particular parameterization of forewarning better predicts widowedpersons� psychological adjustment.
Other Influences on Psychological Adjustment and Spousal Loss
Finally, our research acknowledges that pre-death characteristics might affect both thesuddenness and context of spousal death, as well as adjustment to the loss. To address the possibilityof a spurious relationship between forewarning and psychological adjustment, we control importantbaseline (i.e., pre-widowhood) characteristics. First, we control mental health prior to loss, to helpdistinguish one�s affective state prior to the death and change in affective state that occurredfollowing the death (Jacobs, 1993; Zisook & Schucter, 1991). Second, we control demographiccharacteristics (age and sex) and socioeconomic status (education, income, and home ownership) atbaseline, as these characteristics have been linked both to death context (e.g., younger persons andwomen are more likely to have their spouses die suddenly) and later psychological adjustment.Finally, respondent�s physical health at baseline is controlled; past research suggests that survivors ofsudden deaths tend to have been healthier prior to the death due to the advanced age of spouses dyingof long-term illnesses, and the fact that husbands with long-term illnesses tend to have somewhatunhealthy wives (Lopata, 1996, p. 74; Stroebe & Stroebe 1987, p. 206-8). Moreover, baseline healthmay influence both how one manages stressors related to the death timing and psychologicaladjustment following the death (George & Gwyther, 1984).
In sum, our research has three objectives: first, to identify the relationship between deathforewarning (in various parameterizations) and widowed persons� psychological adjustment six and18 months after the loss; second, to assess whether and how the relationship between deathforewarning and widowed persons� well-being differs for men and women, since most of thepotential sources of variability discussed above vary by gender; and third, to evaluate the extent towhich the effect of death forewarning is mediated or suppressed by death context characteristics (i.e.,
pre-death care giving, nursing home usage, spouse age at death and couple communication prior tothe death). Analyses are based on data from the Changing Lives of Older Couples (CLOC) survey, aprospective study of a sample of married individuals age 65 and older. The CLOC allows evaluationof the effects of many pre-death contextual factors that are potentially confounded with forewarningin prior research.
METHODS
Sample
The Changing Lives of Older Couples (CLOC) study is a prospective study of a two-stagearea probability sample of 1,532 married individuals from the Detroit Standardized MetropolitanStatistical Area (SMSA). To be eligible for the study, respondents had to be English-speakingmembers of a married couple where the husband was age 65 or older. All sample members were non-institutionalized and were capable of participating in a two-hour long interview. Approximately 65%of those contacted for an interview participated, which is consistent with the response rate from otherDetroit area studies in that period. Baseline face-to-face interviews were conducted from June 1987through April 1988.
Spousal loss was monitored using monthly death record tapes provided by the State ofMichigan and by reading the daily obituaries in Detroit-area newspapers. The National Death Index(NDI) and direct ascertainment of death certificates were used to confirm deaths and obtain causes ofdeath. Of the 319 respondents who lost a spouse during the study, 86% (n=276) participated in atleast one of the three follow-up interviews which were conducted six months (Wave 1), 18 months(Wave 2) and 48 months (Wave 3) after the spouse�s death. The primary reasons for non-responsewere refusals to participate (38 percent of nonparticipants) and ill health or death at follow-up (42percent). Our analyses are based on the 210 widowed persons (59 men and 151 women) interviewedat the six-month follow up, or roughly 66 percent of the 319 respondents who lost a spouse, as wellas the 155 widowed persons (110 women and 45 men) who were also interviewed at the 18-monthfollow up.
The issue of selective attrition deserves a brief mention. Although the sample size declinesby roughly 20 percent between waves 1 and 2 (from 210 to 155), we do not believe that this attritionbiases our results. In order to ascertain whether the 20 percent of CLOC participants who dropped outbetween Waves 1 and 2 differs significantly from those who remain in the sample, logistic regressionmodels were estimated to predict sample attrition. Sudden death, months forewarning, baselinedemographic, physical and mental health, and Wave 1 levels of grief were evaluated as predictors.Only one variable was a significant predictor of sample attrition: age. Each additional year of ageincreased the risk of attrition by 7 percent, although this effect was only marginally significant (p <.10). Thus, straightforward OLS regression models, rather than two-stage selection models are usedto predict Wave 2 outcomes.
Measures
Dependent Variables. Two general (i.e., depression and anxiety) and five loss-related (i.e.,shock, anger, yearning, intrusive thoughts, and overall grief) dimensions of psychological adjustmentat the 6-month and 18-month follow-ups are considered. Depression (α = .83) is assessed with asubset of nine negative items from the 20-item Center for Epidemiologic Studies depression (CES-D)scale (Radloff, 1977). Respondents are asked to indicate how often they experienced each symptomin the week prior to interview. Response categories are: hardly ever, some of the time, or most of thetime. The nine symptoms are: (1) I felt depressed; (2) I felt that everything I did was an effort; (3) My
sleep was restless; (4) I felt lonely; (5) People were unfriendly; (6) I did not feel like eating. Myappetite was poor; (7) I felt sad; (8) I felt that people disliked me; and (9) I could not �get going.�
Anxiety (α=.86) is assessed with 10 items from the Symptom Checklist 90 Revised (Derogatis& Cleary, 1977). Respondents are asked to indicate how often they have experienced each of tensymptoms in the week prior to interview. Symptoms include being bothered by: (1) nervousness orshakiness; (2) trembling; (3) feeling suddenly scared for no reason; (4) feeling fearful; (5) heartpounding or racing; (6) feeling tense and keyed up; (7) spells of terror and panic; (8) feeling sorestless you couldn�t sit still; (9) feeling that something bad is going to happen to you; and (10)thoughts and images of a frightening nature. Response categories are: not at all, a little bit,moderately, quite a bit, and extremely.
Psychological reactions specific to the loss, as well as an overarching grief scale, are alsoconsidered. The four aspects of grief considered here are shock, anger, yearning, and intrusivethoughts. Shock (α=.77) is evaluated with three questions: In the last month, (1) have you felt asthough you were in a state of shock; (2) have you felt as though you couldn�t believe what washappening; and (3) have you felt emotionally numb. Anger (α=.68) is assessed with three questions:In the past month, (1) have you felt resentful or bitter about your spouse�s death; (2) have you feltthat the death of your spouse was unfair; and (3) have you felt anger toward God? Yearning (α=.75)is assessed with four questions: In the last month, (1) have you found yourself longing to have yourspouse with you; (2) have you had painful waves of missing your spouse; (3) have you experiencedfeelings of intense pain or grief over the loss of your spouse; and (4) have you experienced feelingsof grief, loneliness, or missing your spouse. Intrusive thoughts (α=.66) is based on three questions: Inthe past month, (1) have you had difficulty falling asleep because thoughts about your spouse keptcoming into your mind; (2) have you tried to block out memories or thoughts of your spouse; and (3)have you been unable to get thoughts about your spouse out of your mind? Grief (α=.85) is theaverage of the four subscale scores.
Response categories for all grief scale items are: no, never; yes, but rarely; yes, sometimes;and yes, often. Items were drawn from widely used grief scales including the Bereavement Index(Jacobs, Kasl & Ostfeld, 1986), Present Feelings About Loss (Singh & Raphael, 1981), and TexasRevised Inventory of Grief (Zisook, Devaul & Click, 1982). Each of the dependent variables isstandardized for ease of interpretation and comparison across indicators.
Independent variables. The central independent variable in the analysis is warning time priorto death, evaluated retrospectively at the Wave 1 interview with the question: �How long before yourspouse�s death did you realize that s/he was going to die?� Respondents could report the duration inhours, days, weeks, months, years or �no warning/minutes.� The number of months warning times isused as the independent variable. Months are top-coded at 24, as more than 90 percent of widowedpersons said that they had less than two years warning. The variable was top-coded because outliersranged as high as 36 years warning. Sudden death is a dummy variable set equal to one forrespondents who indicated that they had �no warning/minutes� prior to their spouse�s death (33percent of sample). We do not separately consider the effects of violent sudden deaths (e.g., suicideor murder), as fewer than two percent died in this manner.
Death Context. Both the psychological consequences of loss and warning time may beassociated with other conditions of the death, thus three additional characteristics of the spouse�sdeath are controlled: spouse’s age at death (in years), and dichotomous variables indicating whetherthe respondent was providing care to his/her spouse in the six months prior to the death, and whetherthe spouse was residing in a nursing home prior to death.
Communication about death was evaluated at Wave 1 with the question: �Did you and [your

spouse] talk about how you would deal with being on your own once she or he was gone?� Thevariable is set equal to �1" for those who responded yes. Closure is evaluated with the question:�Were you there with your [husband/wife] at the moment when [she/he] died?�
Confounding Factors. Depression and anxiety at baseline are measured exactly the same wayas the follow up measures (Derogatis & Cleary, 1977; Radloff, 1977). Respondent�s physical healthat baseline is assessed with the question: �How would you rate your health at the present time?Would you say it is excellent, very good, good, fair or poor?� Responses of �fair� and �poor� arecoded 1, all others are coded as 0.
Demographic Variables. Control variables include age; sex (1=female); home ownership atbaseline (1=owns home), total household income at baseline (natural log of income), and education(a continuous measure ranging from 3 to 17 or more years of completed schooling). The totalhousehold income variable was originally measured by having respondents indicate which of tenincome categories most accurately characterized their economic status. A continuous measure ofincome was derived by taking the midpoint of each of the ten income categories, with Paretoestimation of the mean for the top income category. The natural log of income is used because therespondents� income distribution was skewed toward the lower income categories.
Finally, the analyses control for the duration (in months) between the Baseline and Wave 1interviews. Although all Wave 1 interviews were conducted six months following spousal death, theduration between the Baseline and Wave 1 interviews ranges from nine to 76 months due to variationin the timing of spouse�s death. Thus, baseline assessments are more temporally distant for those wholost their spouses at later dates.
RESULTS
Sample Characteristics
Descriptive statistics and t-tests comparing means for men and women are presented in Table1. Men and women do not differ from one another in terms of anxiety, yearning or intrusive thoughtssix or 18 months following their loss. Death forewarning does not differ significantly by gender;roughly one-third of widowed persons experienced no forewarning of their spouse�s death, whileanother one-third reported more than six months forewarning. The warning times ranged from �notime� to 35 years. The average warning time was five to six months.
Men and women do differ in terms of the context surrounding their spouse�s death.Husbands were significantly older than wives at death (ages 77 versus 73). Men are significantlymore likely than women to report that their spouse was residing in a nursing home prior to death (14versus 2 percent) and that they were with their spouse at the exact moment they died (54 versus 40percent). One-fifth of women and 12 percent of men report that they had discussed with their spousehow they would cope with being on their own. Similar proportions of men and women (44 and 50percent, respectively) reported providing care to their spouse in the months prior to their death. Fewdemographic characteristics differ by gender; men in the CLOC are significantly older than thewomen, and are also slightly more likely to own their own homes. At baseline, women havesignificantly higher levels of anxiety than men.
To provide a fuller portrait of the CLOC participants and their spouses, several characteristicswhich are not used in the multivariate analyses (and thus not presented in Table 1) deserve mention.The leading causes of death among the CLOC spouses are cancer (51 percent) and heart disease (34percent). A significantly larger portion of husbands than wives died of heart disease (49 versus 28percent). Men and women are equally likely to report that their spouse was in a great deal of pain
prior to death (37 versus 35 percent, respectively). Although similar proportions of men and womenprovided care to their spouse during the six months prior to the spouse�s death, women providedmore hours care per week, and are more likely to report that caregiving duties are stressful andprevent them from meeting other obligations.
Intercorrelations are displayed in Table 2. Death context and death timing are associated inexpected ways. Caring for one�s spouse, having placed one�s spouse in a nursing home, and havingdiscussed how one would cope after death are positively correlated with prolonged forewarning andnegatively correlated with sudden death.
Influence of Death Forewarning on Mental Health
The first two objectives of the multivariate analysis are: (1) to specify the relationshipbetween death forewarning and widowed persons� psychological adjustment six and 18 months aftertheir loss; and (2) to assess whether these patterns differ by gender. To address the first objective, weregressed each of four different measures of forewarning on two general (i.e., depression andanxiety), and five loss-related (yearning, shock, anger, intrusive thoughts, and a composite griefmeasure) indicators of psychological adjustment at both six and 18 months after the death. The fourmodels evaluated were: (1) sudden death effects only, measured with a dichotomous indicator ofsudden death; (2) linear effects of warning time, measured with a continuous indicator of monthswarning time (from 1 to 24 months) and a dichotomous indicator of sudden death; (3) curvilineareffects of warning time, measured with a continuous indicator of months warning time, monthswarning time squared, and a dichotomous indicator of sudden death; and (4) effects of sudden andvery prolonged warning time, measured with dichotomous indicators representing sudden death, andwarning time of more than six months. (In preliminary analyses, more fine-grained cutpoints wereevaluated: no warning time, less than 1 month warning, 1-6 months warning, 6-12 months warning,more than 12 months warning. However, the model including just two indicators for no warningversus more than six months warning best fit the data). To achieve the second objective, all modelswere estimated including interaction terms of sex by death forewarning. All models controlleddemographic characteristics and respondent�s baseline physical and mental health (Complete modelsare not shown but are available from the author). Models with significant effects of forewarning arepresented in Tables 3 through 5.
Three main findings emerged from the regression results. First, the effect of deathforewarning on survivors� well-being is far weaker than past research suggests. Considering onlythose models which parameterized forewarning with two dummy variables, we tested 14 models (i.e.,seven dependent variables each at two follow-ups) with two forewarning indicators in each model. Ofthese, only two models produced significant effects - each including one of the forewarning dummyvariables. These effects are probably greater than expected by chance, but indicate very limitedeffects of forewarning on reactions to widowhood among older adults.
Second, when death forewarning does significantly affect widowed persons� psychologicaladjustment, its effect differs across outcomes. Death forewarning - regardless of how operationalized- is unrelated to four (i.e., depression, overall grief, shock, and anger) out of the seven possibleoutcomes at both the six- and 18-month follow up. Even when potential suppressor variables wereadded to the regression equation (i.e., death context and communication), warning time is not asignificant predictor of any of the four outcomes. Sudden death significantly increases levels ofintrusive thoughts six months after the loss, although the effect is no longer significant at the 18-month follow up (Table 3). Prolonged forewarning (i.e., more than six months forewarning) isassociated with elevated anxiety both six and 18 months after the loss.
Third, gender differences in the effect of forewarning are significant for just one of the sevenoutcomes: yearning. At both the six and 18 month follow-ups, sudden death (compared to anticipated

death) is associated with slightly higher yearning scores among women and considerably loweryearning scores among men at both interviews (Table 5).
Death Context and Communication as Mediators of Death Forewarning Effects
To more fully understand the linkages between death forewarning and anxiety, yearning, andintrusive thoughts, baseline models (Model 1) were expanded to include two sets of possiblemediator (or suppressor) variables: death context (Model 2) and communication variables (Model 3).Tables 3 through 5 display regression results for intrusive thoughts (Table 3), anxiety (Table 4), andyearning (Table 5). Models are estimated separately for the six- and 18-month outcomes.
Intrusive Thoughts
Sudden death is associated with elevated levels of intrusive thoughts six months after theloss. However, the effect of sudden death on intrusive thoughts increases when death context andcommunication indicators are controlled. When only demographic and baseline health characteristicsare controlled (Model 1), sudden death is associated with a .316 standard deviation increase inintrusive thoughts (p < .05). When death context variables are adjusted, the effect of sudden deathincreases by nearly 25 percent, to .39 standard deviations. Few of the death context variables havedirect effects on intrusive thoughts, although having been with one�s spouse at the moment of deathprotects against high levels of intrusive thoughts (b=-.389, p<.001).
Intrusive thoughts at the 6-month follow-up are not related to any of the baselinedemographic or social class variables. Of baseline variables, only anxiety is positively andsignificantly related to intru-sive thoughts; those with higher levels of anxiety prior to their spouse�sdeath have elevated levels of intrusive thoughts six months after the death. In general, deathforewarning, context, and demographic factors are relatively weak predictors of intrusive thoughts;the final model explains only 6 percent of the variance in wave 1 intrusive thoughts. By wave 2,intrusive thoughts are no longer significantly linked to sudden death, although other death contextvariables are significantly associated with intrusive thoughts 18 months after the loss. Those whodiscussed death with their spouse and whose spouse resided in a nursing home have significantlylower levels of intrusive thoughts.
Anxiety
Having more than six months forewarning - is a positive and significant predictor of anxietylevels both six and 18 months after the death. However, the effect of sudden death on anxiety is notsignificantly different from the effect of having less than six months warning. The effect ofprolonged forewarning also is not mediated by death context or communication variables; rather, thiseffect also is suppressed by these factors. By and large, the linkages between death forewarning,death context, and demographic factors on anxiety are the same at both the six and 18 months follow-ups, and the amount of variance explained is the same at both time points.
The baseline model (Model 1) reveals that prolonged forewarning is associated with a .37standard deviation increase in anxiety levels at Wave 1, and this effect increases by 27 percent whendeath context variables are considered. The baseline model predicting Wave 2 anxiety shows apositive (though not statistically significant) effect of prolonged death on anxiety. However, whendeath context factors are considered, the effect of prolonged death increases by 32 percent and issignificant at the p<.05 level. Individuals whose spouses resided in a nursing home prior to death hadsignificantly higher anxiety levels at both waves. Communication about the death and being withone�s spouse at death are unrelated to anxiety levels both six and 18 months after the death.

Yearning
Sudden deaths are associated with reduced yearning among men and somewhat elevatedyearning among women at both the six- and 18-month interviews. Gender interaction terms forModel 1 (effects of forewarning, net of demographic and health characteristics) and Model 3 (fullmodel, including indicators of death context and communication) are plotted in Figure 1 (for wave 1yearning levels), and Figure 2 (for wave 2 yearning levels).
When only demographic and health variables are controlled (Model 1), sudden death isassociated with a .67 standard deviation reduction in men�s yearning levels and a .102 standarddeviation increase in women�s yearning levels at the six-month follow-up (compared to those whosespouses died after a warning period). Interestingly, the effect of sudden death on men�s yearning ismediated by death context and communication characteristics, yet the effect of sudden death onwomen�s yearning is suppressed by these factors. When death context factors are controlled, theeffect of sudden death on men�s yearning declines while its effect on women�s yearning increasesslightly. Of the three death context variables, only one is (marginally) significant: having providedcare for one�s spouse prior to death is associated with an increase (b=.27) in yearning six monthsafter the loss. Caregiving is widely believed to be a more stressful (and unanticipated) role for menthan women, and thus may partially account for the slightly better adjustment of men whose wivesdie suddenly.
By the 18 month follow-up, the general patterns documented at wave 1 persist althougheffects tend to be weaker. At wave 2, men whose wives died suddenly continue to have yearningscores roughly one-half standard deviations lower than men whose wives died after a warning period.Women whose spouses died suddenly have yearning levels which are roughly .2 standard deviationshigher than women whose spouses died after a forewarning period. The gender difference in theeffect of forewarning continues to be significant at the p<.05 level.
DISCUSSION
Abundant research has tried to determine whether sudden or anticipated deaths are moredistressing to the bereaved. Although findings are inconsistent across studies, the majority of suchwork concludes that sudden deaths are more difficult for the survivor than anticipated deaths (Ball,1977; Carey, 1979-80; Glick, Weiss & Parkes, 1987; Hill, Thompson & Gallagher, 1988; Jacobs,Kasl & Ostfeld, 1986; Lundin, 1984; O�Bryant, 1990-1991; Smith, 1978; Vachon et al., 1982; Wells& Kendig, 1997; Willis et al., 1987; Zisook, Schuchter & Lyons, 1987). In the case of widowhood,forewarning of a spouse�s death has been thought to provide the survivor with time to resolveconflicts and �unfinished business� with their partner, to support and assist their ailing partner duringtheir final days, to make sense of the dying process, to prepare practically and psychologically for thetransition to widowhood, and to say �goodbye� (Blauner, 1966; Rando, 1986).
Our study of grief among the elderly widowed has shown that the protective effects of deathforewarning on survivors� mental health - found in earlier research - may be overstated. Our findingsalso suggest that researchers should no longer ask the question: �does death forewarning affectpsychological adjustment among widowed persons?� Rather, the more appropriate question is �whichdimensions of psychological adjustment are affected by death forewarning�?
First, our analyses revealed that death forewarning is not a significant predictor of broadmental health outcomes such as depression and overall grief, either six or 18 months following theloss. These findings are consistent with work of O�Bryant (1990-91) and others (e.g. Ball, 1977;Bornstein et al., 1973; Bowling & Cartwright, 1982) who find that broad measures of negative affect
such as depression are unrelated to death forewarning. It is not surprising that forewarning does nothave a significant effect on these broad scales. As noted earlier, depression and grief comprisedistinctive emotional, cognitive, physiological and behavioral symptoms, and these distinctsymptoms may respond in very different ways to death forewarning. For instance, our subscaleanalyses revealed that sudden death is associated with elevated intrusive thoughts, yet reducedanxiety. Consequently, these competing effects may cancel out one another when an aggregate scalesuch as grief is considered as a dependent variable.
Our analyses also show that death forewarning is not a significant predictor of the specificoutcomes of shock and anger. Because shock and anger are believed to be more immediate reactionsto loss (Glick et al., 1974; Parkes, 1970; Zisook et. al., 1987), measurements obtained six monthsafter the death may be too late to evidence effects. It is also possible that death forewarning isunrelated to shock and anger in an older population. As noted earlier, members of the CLOC samplemay not be shocked by even a sudden death, given that death is a normative and anticipated transitionamong older adults (Neugarten & Hagestad, 1976).
Second, sudden deaths are associated with elevated levels of intrusive thoughts. Survivorswhose spouses died suddenly had elevated levels of intrusive thoughts six months after the loss,although the effect faded by the eighteen-month follow up. These findings are consistent with recentresearch examining symptoms of post-traumatic stress disorder (PTSD) among the bereaved.(Intrusive thoughts are believed to be similar conceptually to post-traumatic stress disorder, whereunprovoked painful thoughts about the deceased plague the survivor of a sudden or shocking loss(Archer, 1999, p. 133)). Recent studies have revealed that individuals who lost family members toviolent deaths (accident, suicide or homicide) were much more likely to meet the criteria for PTSDthan those whose relatives died of other conditions (Zisook, Chenstova-Dutton, & Shuchter, 1998;Kaltman & Bonnano, 1999). Likewise, family members of murder victims report higher levels ofintrusive thoughts than relatives of persons who died naturally (Rynearson & McCreery, 1993). Ouranalysis shows further that the effect of sudden death on intrusive thoughts is no longer significant bythe 18-month follow up, a finding which is consistent with the view of Parkes and colleagues (1972,1985) and others that intrusive thoughts will fade over time, as the widowed person becomesenmeshed in other activities and relationships.
Third, prolonged forewarning is linked to elevated of anxiety. Deaths which occurred after afairly long period of anticipation (i.e., more than six months) are linked to higher levels of men�s andwomen�s anxiety both six and 18 months following the death. The harmful effects of advancedforewarning are suppressed by death context and communication characteristics, thus past studieswhich omitted controls for death context characteristics may have underestimated the effect ofadvanced forewarning on elderly survivors� anxiety. Yet this finding also means that the harmfuleffects of advanced forewarning cannot be explained away by caregiving, couple communication,spouse�s age at death, or whether one�s spouse resided in a nursing home prior to death. Griefscholars thus face the task of identifying why and how prolonged forewarning periods lead toelevated anxiety among older adults.
Sociological research on chronic stressors may provide a starting point for this inquiry.Chronic stressors, such as caregiving or watching a spouse suffer from a debilitating illness, arebelieved to be more difficult for psychological adjustment than stressors of shorter duration (Avison& Turner, 1988; Also see Pearlin & Skaff, 1995 for a review). Moreover, the psychological effects ofa chronic stressor may be compounded when experienced in conjunction with concurrent orsuccessive stressors (Holmes & Rahe, 1967; Johnson & Catalano, 1983). Spouses who spend periodsof six months or longer anticipating their spouse�s death are presumably at a greater risk ofexperiencing concurrent stressors (such as caregiving and economic stress) than those whoseanticipation periods are confined to a shorter time frame. By incorporating indicators of other pre-

widowhood stressors into future analyses, the pathways linking prolonged forewarning andsurvivors� elevated anxiety levels may become more apparent.
Fourth, the relationship between sudden death and yearning differs starkly for men andwomen. Sudden death predicts a slight increase in women�s yearning, a finding which is generallyconsistent with past clinical research revealing that sudden death is linked to poor adjustment to loss(Lindemann, 1944; Rando, 1986). It is not surprising that past research is more applicable incharacterizing the experiences of women rather than men, given that the overwhelming majority ofstudies examining the psychological consequences of late life widowhood focus on samples ofwomen only (e.g. Lopata, 1973; O�Bryant, 1990-91).
However, it is surprising that sudden death is more distressing to women than men. We hadexpected the reverse: because women are more likely than men to be widowed, they may have�rehearsed� and mentally prepared for the transition (Neugarten & Hagestad, 1976). The harmfuleffects of death forewarning on men�s yearning may reflect gender differences in how individualsrespond to their partner�s end of life experiences. For instance, the caregiving duties that oftenaccompany death forewarning may prove more difficult for men, given that men of the CLOC cohorthave less experience with performing the role of caregiver over the life course (see Hatch 2000 for areview). Consistent with this interpretation, our empirical analyses reveal that the effect of suddendeath on men�s yearning attenuates somewhat when caregiving is controlled.
Past research also suggests that for men, the forewarning period may be associated withincreased closeness to the spouse and increased isolation from others. During this time, men maybecome even closer to and more emotionally bonded to their spouse, at the expense of relationshipswith others. Moreover, given gender differences in mortality, men may have few same-sex peers whoare also awaiting an ill wife�s death. In contrast, during the period prior to spousal death, women mayrely on their social networks and their female friends� direct experience with spousal illness to helpthem through the difficult period (Fooken, 1985, p. 98).
Why do the effects of forewarning differ by sex for yearning only? This pattern may reflectthe fact that yearning is the only subdimension of grief which is explicitly relational and thus mayreflect gender differences in how spousal relationships unfold during the pre-death period. Intrusivethoughts, in contrast, reflect the cognitive process of �stimulus-independent thoughts�(Archer, 1999,p. 65), and anxiety reflects worries about coping with daily experiences.
In sum, our findings suggest that among older couples, sudden spousal death does not havedeleterious effects on mental health, except for increasing intrusive thoughts during the first sixmonths after widowhood. Prolonged periods of anticipating a spouse�s death are also not generallydeleterious, but do seem to increase anxiety for both men and women, and yearning among men only.These gender-specific effects appear to be due to the different experiences of men and women incaring for and relating to a dying spouse. Future research is needed to more adequately understandthe limited but real effects found here, and to explore the degree to which other characteristics of thedeceased, the surviving spouse, the marital relationship, and the social context condition the ways inwhich older adults respond to widowhood and its forewarning.

17
REFERENCES
Anashensel, C.S., Pearlin, L.I., Mullan, J.T., Zarit, S. & Whitlach, C. (1995). Profiles in care giving: theunexpected career. New York: Academic Press.
Archer, J. (1999). The nature of grief: the evolution and psychology of reactions to loss. London:Routledge Press.
Averill, J.R., & Wisocki, P.A. (1981).Some observations on behavioral approaches to the treatment ofgrief among the elderly. Pp. X-x in Behavioral Therapy in Terminal Care, edited by H.J. Sobel.Cambridge: Ballinger Publishing.
Avison, W.R. & Turner, R.J. (1988). Stressful life events and depressive symptoms: Disaggregating theeffects of acute stressors and chronic strains. Journal of Health and Social Behavior, 29, 253-64.
Ball, J.F. (1977). Widows’ grief: the impact of age and mode of death. Omega: The Journal of Death andBereavement, 7, 307-33.
Bennett, K.M., & Vidal-Hall, S. (2000). Narratives of death: a qualitative study of widowhood in laterlife. Ageing and Society, 20, 413-28.
Binger, C.M., Ablin, A.R., Feurstein, M.D., Kushner, J.H., Zoger, S. & Middelsen, C. (1969). Childhoodleukemia: emotional impact on patient and family. New England Journal of Medicine, 280, 414-18.
Blanchard, C.G.,. Blanchard, E.B. & Becker, J.N. (1976). The young widow: depressive symptomatologythroughout the grief process. Psychiatry, 39, 394-99.
Blauner, R (1966). Death and social structure. Psychiatry, 25, 378-399.Bornstein, P.E., Clayton, P.J., Halikas, J.A., Marucie, W.L. & Robins, E. (1973). The depression of
widowhood after thirteen months. British Journal of Psychiatry, 122, 561-66.Bowling, A., & Cartwright, A. (1982). Life after death: a study of the elderly widowed. London:
Tavistock.Bozeman, M.F., Orbach, C.E., & Sutherland, A.M. (1955). Psychological impact of cancer and its
treatment: adaptation of mothers to threatened loss of their children through leukemia. Cancer, 8,1-9.
Calhoun, L.G. & Allen, B.G. (1991). Social reactions to the survivor of a suicide in the family: a reviewof the literature. Omega: Journal of Death and Dying, 20, 265-72.
Carey, R.G. (1979-80). Weathering widowhood: problems and adjustment of the widowed during the firstyear. Omega, 10, 163-174.
Carr, D., House, J.S., Kessler, R.C., Nesse, R.M., Sonnega, J. & Wortman, C. (2000). Marital quality andpsychological adjustment to widowhood among older adults: a longitudinal analysis. Journal ofGerontology: Social Sciences 55B, 4, S197-207.
Chodoff, P., Friedman, S.B., & Hamburg, D.A. (1964). Stress, defenses and coping behavior: observa-tions in parents of children with malignant disease. American Journal of Psychiatry, 120, 743-9.
Clayton, P., Desmarais, L. & Winokur, G. (1968). A study of normal bereavement. American Journal ofPsychiatry, 125, 168.
Clayton, P.L., Halikas, J.A., Maurice, W.L. & Robins, E. (1973). Anticipatory grief and widowhood.British Journal of Psychiatry, 122, 47-51.

18
Deimling, G.T., Bass, D.M., Townsend, A.T., & Noelker, L.S. (1989). Care-related stress: a comparisonof spouse and adult child caregivers in shared and separate households. Journal of Aging andHealth, 1, 67-82.
Derogatis, L.R. & Cleary, P.A. (1977). Confirmation of the dimensional structure of the SCL-90: a studyin construct validation. Journal of Clinical Psychology, 33, 981-989.
DeSpelder, L.A. & Strickland, A.L. (1992). The last dance: encountering death and dying, 3d ed.Mountain View, CA: Mayfield.
Dunn, R.G. & Morrish-Vidners, D. (1987). The psychological and social experience of suicide survivors.Omega: Journal of Death and Dying, 18, 175-215
Farebrow, N.L., Gallagher-Thompson, D., Gilewski, M. & Thompson, L. (1992). Changes in grief andmental health of bereaved spouses of older suicides. Journal of Gerontology, 47, 357-66.
Fengler, A.P. & Goodrich, R. (1979). Wives of elderly, disabled men: the hidden patients. TheGerontologist, 19, 2, 175-83.
Fiewiger, M. & Smilowitz, M. (1984-85). Relational conclusion through interaction with the dying.Omega, 15, 161-72.
Fooken, I. (1985). Old and female: psycho social concomitants of the aging process in a group of olderwomen. In J. Munniches, P. Mussen, E. Olbrich & P.G. Coleman. (Eds.), Life span and change ina gerontological perspective (pp. 7-101). Orlando, FL: Academic Press.
Foner, N. (1994). The caregiving dilemma: work in an American nursing home. Berkeley, CA: Universityof California Press.
Fulton, R. & Fulton, J. (1972). Anticipatory grief: a psycho social aspect of terminal care. In B.Schoenberg et al. (Eds.), Psychosocial aspects of terminal care (pp. X-x). , New York: ColumbiaUniversity.
George, L., K. (1993). Sociological perspectives on life transitions. Annual Review of Sociology, 19,353-73.
George, L. & Gwyther, L. (1984). The dynamics of caregiving burden: changes in caregiver well-beingover time. The Gerontologist, 26, 253-9.
Gerber, I. (1974). Anticipatory bereavement. In B. Schoenberg, A.C. Carr, A.H. Kutscher, D. Peretz &I.K. Goldberg (Eds.) . Anticipatory Grief (pp. 26-31). New York: Columbia University Press.
Gerber, I., Rusalem, R., Hannon, N., Battin, D. & Arkin, A. (1975). Anticipatory grief and to agedwidows and widowers. Journal of Gerontology, 30, 225-9.
Glick, I.O., Weiss, R. S., & Parkes, C.M. (1974). The first year of bereavement. New York: Wiley.Hill, C.D., Thompson, L.W. & Gallagher, D. (1988). The role of anticipatory bereavement in older
women’s adjustment to widowhood. The Gerontologist 28, 6, 792-6.Hinds, C. (1985). The needs of families who care for patients with cancer at home: are we meeting them?
Journal of Advanced Nursing, 10, 575-81.Hinrichsen, G.A., Hernandez, N.A., and Pollack, S. (1992). Difficulties and rewards in family care of the
depressed older adult. The Gerontologist, 32, 486-92. Holmes, J.H. & Rahe, R.H. 1967. The social readjustment scale. Journal of Psychosomatic Research, 11,
213-28.Hyman, H.H. (1983). Of time and widowhood: nationwide studies of enduring effects. Durham, NC: Duke
University Press.
19
Jacobs, S. (1993). Pathologic grief: maladaptation to loss. Washington, D.C.: American PsychiatricPress.
Jacobs, S., Kasl, S. & Ostfeld, A. (1986). The measurement of grief: bereaved versus non-bereaved. TheHospice Journal, 2, 21-36.
Johnson, C.L. & Catalano, D.J. (1983). A longitudinal study of family supports to impaired elderly. TheGerontologist, 23, 612-8.
Kalish, R.A. (1981). Death, grief, and caring relationship. Monterey, CA: Brooks/Cole.Kaltman, S., & Bonanno, G. (1999). Trauma and bereavement: examining the role of sudden and violent
deaths. Unpublished manuscript.Kramer, D. (1996-97). How women relate to terminally ill husbands and their subsequent adjustment to
bereavement. Omega, 34, 93-106.Lindemann, E. (1944). Symptomatology and management of acute grief. American Journal of Psychiatry,
151, 155-60.Lopata, H.Z. (1973). Widowhood in an American city. Cambridge, MA: Schenkman.Lopata, H.Z. (1996). Current Widowhood: Myths and Realities. Thousand Oaks, CA: Sage Publications.Lundin, T. (1984). Long-term outcome of bereavement. British Journal of Psychiatry, 145, 424-8.Lundin, T. (1984). Morbidity following sudden and expected bereavement. British Journal of Psychiatry,
144, 84-88.Maddison, D. & Walker, W. (1967). Factors affecting the outcome of conjugal bereavement. British
Journal of Psychiatry, 113, 1057-67.Matthews, A. M. (1991 ). Widowhood in late life. Toronto: Buttersworth.McGloshen, T.H. & O’Bryant, S.L. (1988). The psychological well-being of older, recent widows.
Psychology of Women, 12, 99-116.McLeroy, K. & Crump, C. (1994). Health promotion and disease prevention: a historical perspective .
Generations, Spring, 9-17.Natterson, J.M., & Knudson, A.G. (1960). Observations concerning fear of death in fatally ill children
and their mothers. Psychosomatic Medicine, 22, 456-65.Neugarten, B. & G.O. Hagestad. (1976). “Age and the Life Course.” In G. Binstock and E. Shanas (Eds).
Handbook of Aging and the Social Sciences (pp. 35-55). New York: Van Nostrand Reinhold.Norris, F.H. & Murrell, S.A. (1990). Social support, life events and stress as modifiers of adjustment to
bereavement by older adults. Psychology and Aging, 5, 429-36.O’Bryant, S.L. (1991). Forewarning of husband’s death: does it make a difference? Omega 22, 3, 227-39.O’Bryant, S.L., Straw, L.B., & Meggaugh, D.I. (1990). Contributions of the caregiving role to women’s
development. Sex Roles, 23, 645-58.Olshansky, S. J. & Ault, A.B. (1986). The fourth stage of the epidemiologic transition: the age of delayed
degenerative diseases. The Millbank Memorial Fund Quarterly, 64, 355-91.Parkes, C. M. (1985). Bereavement. British Journal of Psychiatry, 146, 11-17.Parkes, C.M. & R.S. Weiss. (1983). Recovery from bereavement. New York: Basic Books.Pattison, E.M.(1977). The experience of dying. Englewood Cliffs, NJ: Prentice-Hall.Pattison, E.M. 1978. The living-dying process. In C.A. Garfield (Ed.), Psychosocial care of the dying
patient, (pp. 133-68). New York: McGraw-Hill.
20
Parkes, C.M. (1970). The first year of bereavement: a longitudinal study of the reaction of Londonwidows to the death of their husbands. Psychiatry, 33, 444-467.
Parkes, C.M. & Brown, R. (1972). Health after bereavement: a controlled study of young Boston widowsand widowers. Psychosomatic Medicine, 34, 449.
Pearlin, Leonard I. (1982). .The social contexts of stress. In L. Goldberger & S. Breznitz. (Eds.),Handbook of Stress, (pp. 367-79). New York: Free Press.
Pearlin, L.I, & Lieberman, M. (1979). Social sources of emotional distress. In R. Simmons. (Ed.),research in community and mental health, (pp. 217-48). Greenwich, CT: JAI Press.
Pearlin, L.I., & Skaff, M.M. (1995) Perspectives on the family and stress and late life. In J. Loranz (Ed.)Pp.323-340 in Handbook of aging and mental health: an integrative approach, (pp. 323-40). NewYork: Plenum Press.
Radloff, L. (1977). The CES-D scale: a self-report depression scale for research in the general population.Applied Psychological Measurement, 1, 381-401.
Rando, T.A. (1986). A comprehensive analysis of anticipatory grief: perspectives, processes, promisesand problems. In T.A. Rando. (Ed.) Loss and anticipatory grief, (pp. 3-38). Lexington, MA:Lexington Books.
Reed, M.D. (1998). Predicting grief symptomatology among the suddenly bereaved. Suicide & Life-Threatening Behavior, 28, 285-301.
Richmond, J.B. & Waisman, H.A. (1955). Psychologic aspects of management of children with malignantdiseases. American Journal of Diseased Children, 89, 42-47.
Roach, M.J. & Kitson, C. (1989). Impact of forewarning on adjustment to widowhood and divorce. InD.A. Lund (ed.)., Older Bereaved Spouses: Research with Practical Applications, (pp. 185-200).New York: Hemisphere Publishing.
Rosenblatt, P. (1983). Bitter, bitter tears: nineteenth century diarists and twentieth century grief theories.Minneapolis: University of Minnesota.
Rosenthal, C.J. & Dawson, P. (1993). Families and the Institutionalized Elderly.” In G. Jones & B.Miesen (Eds.) Caregiving and dementia: convergence of research models and empiricalreflections. London: Routledge.
Rynearson, E.K. (1984). Bereavement after homicide: A descriptive study. American Journal ofPsychiatry, 141, 1452-54.
Rynearson, E.K. & McCreery, J.M. (1993). Bereavement after homicide: a synergism of trauma and loss.American Journal of Psychiatry, 150, 258-261.
Sanders, C.M. (1982-83). Effects of sudden vs. chronic illness on bereavement outcome. Omega: Journalof Death and Dying, 13, 227-41.
Schwab, J.J., Chalmers, J.M.,. Conroy, S.J., Farris, P.N., & Markush, R.E. (1975). Studies in grief: apreliminary report. In B. Schoenberg, A.C. Carr, A.H. Kutscher, D. Peretz & I.K.Goldberg.(Eds.), Anticipatory grief. (pp. 78-87). New York: Columbia University Press.
Siegel, K., & Weinstein, L. (1983). Anticipatory grief reconsidered. Journal of Psycho social Oncology,1, 61-73.
Singh, B., & Raphael, B. (1981). Postdisaster morbidity of the bereaved: a possible role for preventivepsychiatry? The Journal of Nervous and Mental Disease, 169, 203-212.

21
Smith, W.J. (1978). The etiology of depression in a sample of elderly widows. Journal of GeriatricPsychiatry, 11, 81-3.
Stroebe, M.S. & Stroebe, W. (1983). Who suffers more? Sex differences in health risks of the widowed.Psychological Bulletin, 93, 279-301.
Stroebe, W. & Stroebe, M.S. (1987). Bereavement and health: the psychological and physicalconsequences of partner loss. New York: Cambridge University Press.
Sweeting, H. N., & Gilhooly, M.L.M. (1990). Anticipatory grief: a review. Social Science and Medicine,30, 1073-80.
Stone, R., Cafferata, G. & Sangl, J. (1987). Caregivers of the frail elderly: a national profile. TheGerontologist, 27, 616-26.
Thoits, P.A. (1983). Dimensions of life events that influence psychological distress: An evaluation andsynthesis of the literature. In H.B. Kaplan (Ed.), Psychsocial stress: trends in theory andresearch, (Pp. 33-103). New York: Academic Press.
Umberson, D., Wortman, C. & Kessler, R.C. (1992). Widowhood and depression: explaining long-termgender differences in vulnerability. Journal of Health and Social Behavior 33, 10-24.
U.S. Bureau of the Census. (1996). Statistical abstract of the United States: 1996 (116th ed.). Washington,D.C.: U.S. Government Printing Office.
Vachon, M.L., Formo, S.A., Freedman, K., Lyall, A., Rogers, J. & Freeman, S.J. (1976). Stress reactionsto bereavement. Essence: Issues in the Study of Aging, Dying and Death, 1, 23-33.
Vachon, M.L., Rogers, J., Lyall, W.A., Lances, W.J., Sheldon, A.R., & Freeman, S.J. (1982). Predictorsand correlates of adaptation to conjugal bereavement. American Journal of Psychiatry, 139, 998-1002.
Van der Wal, J. (1989-90). The aftermath of suicide: a review of empirical evidence. Omega: Journal ofDeath and Dying, 20, 149-71.
Wells, Y. D. & Kendig, H.L. (1997). Health and well-being of spouse caregivers and the widowed. TheGerontologist, 37, 5, 666-74.
Willis, L., Thomas, P, Garry, P.J., & Goodwin, J. (1987). A prospective study of response to stressful lifeevents in initially healthy elders. Journal of Gerontology, 42, 6, 627-30.
Wilson, V. (1990). The consequences of elderly wives caring for disabled husbands: Implications forpractice. Social Work, 35, 417-21.
Wright, L.K. (1991). The impact of Alzheimer’s disease on the marital relationship. The Gerontologist,31, 224-37.
Zisook, S., Chentsova, Y. & Schucter, S.R. (1998). Post-traumatic stress disorder following bereavement.Annals of Clinical Psychiatry, 10, 157-63.
Zisook, S., DeVaul, R. & Click, N. (1982). Measuring symptoms of grief and bereavement. AmericanJournal of Psychiatry, 139, 1590-1593.
Zisook, S. & S.R. Shuchter. (1991). Early Psychological Reaction to the Stress of Widowhood.Psychiatry, 54, 320-332.
Zisook, S., Schucter, S.R. & Lyons, L.E. (1987). Adjustment to widowhood. In S. Zisook (Ed.).Biopsychosocial aspects of bereavement. Washington, DC: American Psychiatric Press.
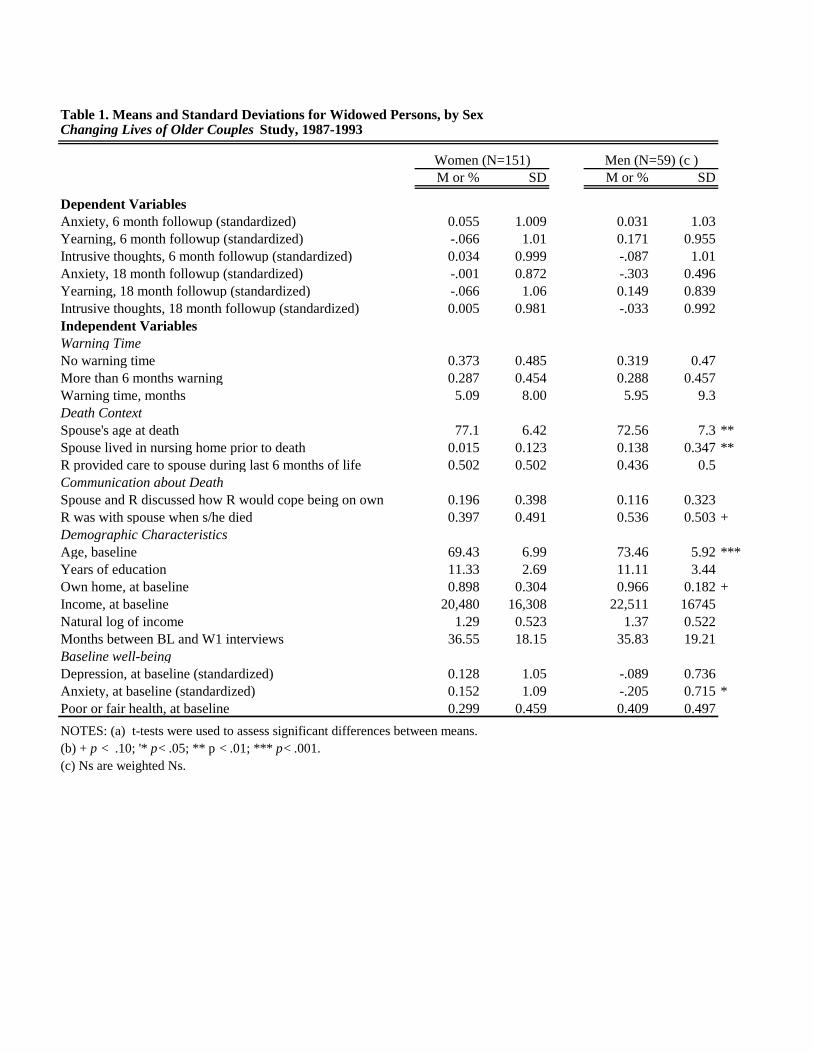
Table 1. Means and Standard Deviations for Widowed Persons, by SexChanging Lives of Older Couples Study, 1987-1993
M or % SD M or % SD
Dependent VariablesAnxiety, 6 month followup (standardized) 0.055 1.009 0.031 1.03Yearning, 6 month followup (standardized) -.066 1.01 0.171 0.955Intrusive thoughts, 6 month followup (standardized) 0.034 0.999 -.087 1.01Anxiety, 18 month followup (standardized) -.001 0.872 -.303 0.496Yearning, 18 month followup (standardized) -.066 1.06 0.149 0.839Intrusive thoughts, 18 month followup (standardized) 0.005 0.981 -.033 0.992Independent VariablesWarning TimeNo warning time 0.373 0.485 0.319 0.47More than 6 months warning 0.287 0.454 0.288 0.457Warning time, months 5.09 8.00 5.95 9.3Death ContextSpouse's age at death 77.1 6.42 72.56 7.3 **Spouse lived in nursing home prior to death 0.015 0.123 0.138 0.347 **R provided care to spouse during last 6 months of life 0.502 0.502 0.436 0.5Communication about DeathSpouse and R discussed how R would cope being on own 0.196 0.398 0.116 0.323R was with spouse when s/he died 0.397 0.491 0.536 0.503 +Demographic CharacteristicsAge, baseline 69.43 6.99 73.46 5.92 ***Years of education 11.33 2.69 11.11 3.44Own home, at baseline 0.898 0.304 0.966 0.182 +Income, at baseline 20,480 16,308 22,511 16745Natural log of income 1.29 0.523 1.37 0.522Months between BL and W1 interviews 36.55 18.15 35.83 19.21Baseline well-beingDepression, at baseline (standardized) 0.128 1.05 -.089 0.736Anxiety, at baseline (standardized) 0.152 1.09 -.205 0.715 *Poor or fair health, at baseline 0.299 0.459 0.409 0.497NOTES: (a) t-tests were used to assess significant differences between means.(b) + p < .10; '* p< .05; ** p < .01; *** p< .001.(c) Ns are weighted Ns.
Women (N=151) Men (N=59) (c )
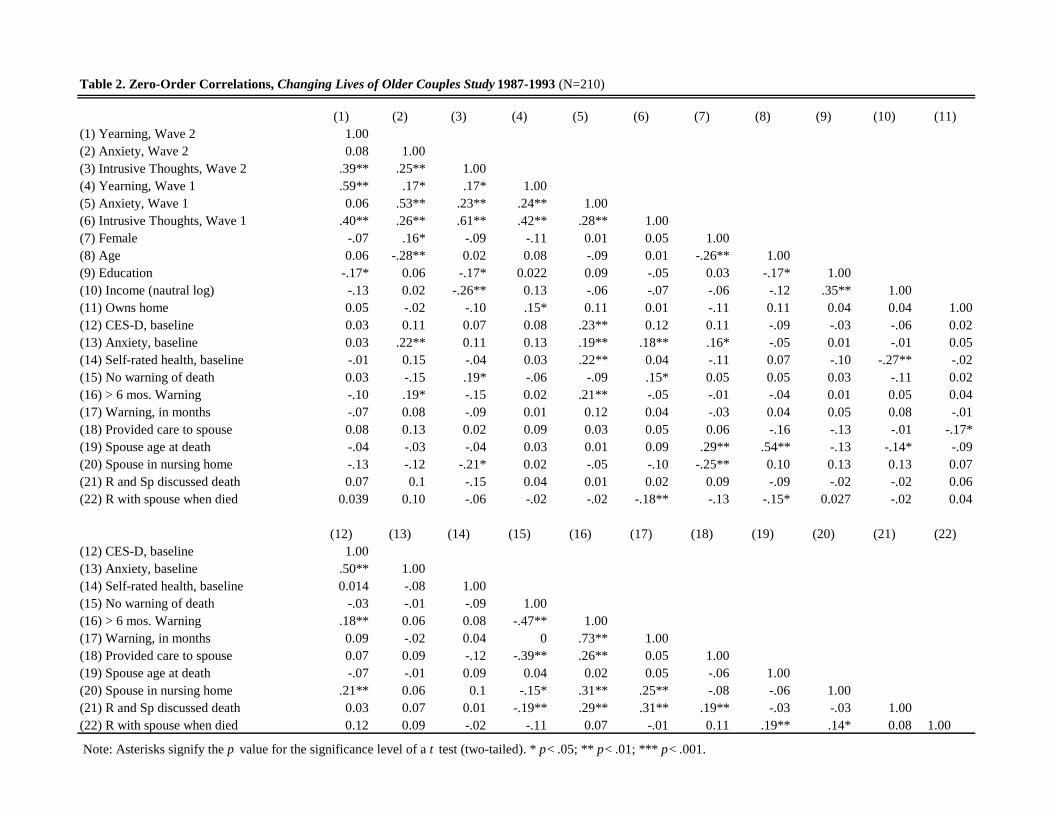
Table 2. Zero-Order Correlations, Changing Lives of Older Couples Study 1987-1993 (N=210)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11)(1) Yearning, Wave 2 1.00(2) Anxiety, Wave 2 0.08 1.00 (3) Intrusive Thoughts, Wave 2 .39** .25** 1.00(4) Yearning, Wave 1 .59** .17* .17* 1.00(5) Anxiety, Wave 1 0.06 .53** .23** .24** 1.00(6) Intrusive Thoughts, Wave 1 .40** .26** .61** .42** .28** 1.00(7) Female -.07 .16* -.09 -.11 0.01 0.05 1.00(8) Age 0.06 -.28** 0.02 0.08 -.09 0.01 -.26** 1.00(9) Education -.17* 0.06 -.17* 0.022 0.09 -.05 0.03 -.17* 1.00(10) Income (nautral log) -.13 0.02 -.26** 0.13 -.06 -.07 -.06 -.12 .35** 1.00(11) Owns home 0.05 -.02 -.10 .15* 0.11 0.01 -.11 0.11 0.04 0.04 1.00(12) CES-D, baseline 0.03 0.11 0.07 0.08 .23** 0.12 0.11 -.09 -.03 -.06 0.02(13) Anxiety, baseline 0.03 .22** 0.11 0.13 .19** .18** .16* -.05 0.01 -.01 0.05(14) Self-rated health, baseline -.01 0.15 -.04 0.03 .22** 0.04 -.11 0.07 -.10 -.27** -.02(15) No warning of death 0.03 -.15 .19* -.06 -.09 .15* 0.05 0.05 0.03 -.11 0.02(16) > 6 mos. Warning -.10 .19* -.15 0.02 .21** -.05 -.01 -.04 0.01 0.05 0.04(17) Warning, in months -.07 0.08 -.09 0.01 0.12 0.04 -.03 0.04 0.05 0.08 -.01(18) Provided care to spouse 0.08 0.13 0.02 0.09 0.03 0.05 0.06 -.16 -.13 -.01 -.17*(19) Spouse age at death -.04 -.03 -.04 0.03 0.01 0.09 .29** .54** -.13 -.14* -.09(20) Spouse in nursing home -.13 -.12 -.21* 0.02 -.05 -.10 -.25** 0.10 0.13 0.13 0.07(21) R and Sp discussed death 0.07 0.1 -.15 0.04 0.01 0.02 0.09 -.09 -.02 -.02 0.06(22) R with spouse when died 0.039 0.10 -.06 -.02 -.02 -.18** -.13 -.15* 0.027 -.02 0.04
(12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22)(12) CES-D, baseline 1.00(13) Anxiety, baseline .50** 1.00(14) Self-rated health, baseline 0.014 -.08 1.00(15) No warning of death -.03 -.01 -.09 1.00(16) > 6 mos. Warning .18** 0.06 0.08 -.47** 1.00(17) Warning, in months 0.09 -.02 0.04 0 .73** 1.00(18) Provided care to spouse 0.07 0.09 -.12 -.39** .26** 0.05 1.00(19) Spouse age at death -.07 -.01 0.09 0.04 0.02 0.05 -.06 1.00(20) Spouse in nursing home .21** 0.06 0.1 -.15* .31** .25** -.08 -.06 1.00(21) R and Sp discussed death 0.03 0.07 0.01 -.19** .29** .31** .19** -.03 -.03 1.00(22) R with spouse when died 0.12 0.09 -.02 -.11 0.07 -.01 0.11 .19** .14* 0.08 1.00
Note: Asterisks signify the p value for the significance level of a t test (two-tailed). * p< .05; ** p< .01; *** p< .001.
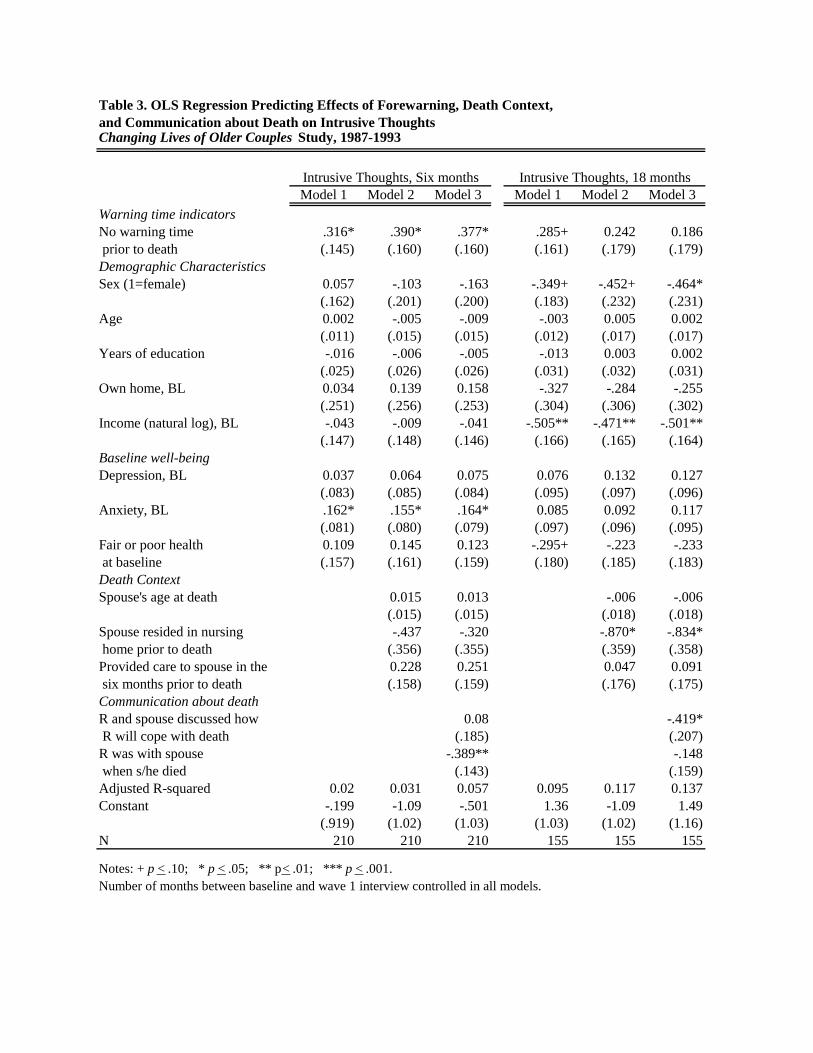
Table 3. OLS Regression Predicting Effects of Forewarning, Death Context,and Communication about Death on Intrusive Thoughts Changing Lives of Older Couples Study, 1987-1993
Model 1 Model 2 Model 3 Model 1 Model 2 Model 3Warning time indicatorsNo warning time .316* .390* .377* .285+ 0.242 0.186 prior to death (.145) (.160) (.160) (.161) (.179) (.179)Demographic CharacteristicsSex (1=female) 0.057 -.103 -.163 -.349+ -.452+ -.464*
(.162) (.201) (.200) (.183) (.232) (.231)Age 0.002 -.005 -.009 -.003 0.005 0.002
(.011) (.015) (.015) (.012) (.017) (.017)Years of education -.016 -.006 -.005 -.013 0.003 0.002
(.025) (.026) (.026) (.031) (.032) (.031)Own home, BL 0.034 0.139 0.158 -.327 -.284 -.255
(.251) (.256) (.253) (.304) (.306) (.302)Income (natural log), BL -.043 -.009 -.041 -.505** -.471** -.501**
(.147) (.148) (.146) (.166) (.165) (.164)Baseline well-beingDepression, BL 0.037 0.064 0.075 0.076 0.132 0.127
(.083) (.085) (.084) (.095) (.097) (.096)Anxiety, BL .162* .155* .164* 0.085 0.092 0.117
(.081) (.080) (.079) (.097) (.096) (.095)Fair or poor health 0.109 0.145 0.123 -.295+ -.223 -.233 at baseline (.157) (.161) (.159) (.180) (.185) (.183)Death ContextSpouse's age at death 0.015 0.013 -.006 -.006
(.015) (.015) (.018) (.018)Spouse resided in nursing -.437 -.320 -.870* -.834* home prior to death (.356) (.355) (.359) (.358)Provided care to spouse in the 0.228 0.251 0.047 0.091 six months prior to death (.158) (.159) (.176) (.175)Communication about deathR and spouse discussed how 0.08 -.419* R will cope with death (.185) (.207)R was with spouse -.389** -.148 when s/he died (.143) (.159)Adjusted R-squared 0.02 0.031 0.057 0.095 0.117 0.137Constant -.199 -1.09 -.501 1.36 -1.09 1.49 (.919) (1.02) (1.03) (1.03) (1.02) (1.16)N 210 210 210 155 155 155
Notes: + p < .10; * p < .05; ** p< .01; *** p < .001.Number of months between baseline and wave 1 interview controlled in all models.
Intrusive Thoughts, Six months Intrusive Thoughts, 18 months
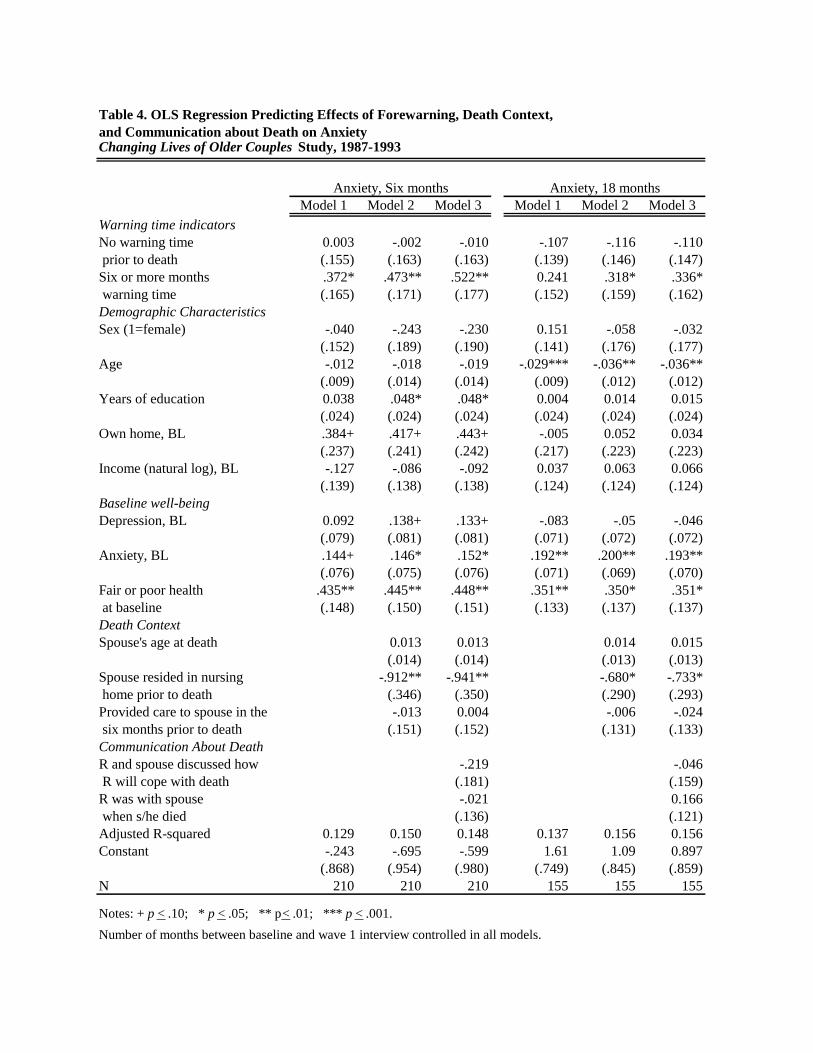
Table 4. OLS Regression Predicting Effects of Forewarning, Death Context,and Communication about Death on AnxietyChanging Lives of Older Couples Study, 1987-1993
Model 1 Model 2 Model 3 Model 1 Model 2 Model 3Warning time indicatorsNo warning time 0.003 -.002 -.010 -.107 -.116 -.110 prior to death (.155) (.163) (.163) (.139) (.146) (.147)Six or more months .372* .473** .522** 0.241 .318* .336* warning time (.165) (.171) (.177) (.152) (.159) (.162)Demographic CharacteristicsSex (1=female) -.040 -.243 -.230 0.151 -.058 -.032
(.152) (.189) (.190) (.141) (.176) (.177)Age -.012 -.018 -.019 -.029*** -.036** -.036**
(.009) (.014) (.014) (.009) (.012) (.012)Years of education 0.038 .048* .048* 0.004 0.014 0.015
(.024) (.024) (.024) (.024) (.024) (.024)Own home, BL .384+ .417+ .443+ -.005 0.052 0.034
(.237) (.241) (.242) (.217) (.223) (.223)Income (natural log), BL -.127 -.086 -.092 0.037 0.063 0.066
(.139) (.138) (.138) (.124) (.124) (.124)Baseline well-beingDepression, BL 0.092 .138+ .133+ -.083 -.05 -.046
(.079) (.081) (.081) (.071) (.072) (.072)Anxiety, BL .144+ .146* .152* .192** .200** .193**
(.076) (.075) (.076) (.071) (.069) (.070)Fair or poor health .435** .445** .448** .351** .350* .351* at baseline (.148) (.150) (.151) (.133) (.137) (.137)Death ContextSpouse's age at death 0.013 0.013 0.014 0.015
(.014) (.014) (.013) (.013)Spouse resided in nursing -.912** -.941** -.680* -.733* home prior to death (.346) (.350) (.290) (.293)Provided care to spouse in the -.013 0.004 -.006 -.024 six months prior to death (.151) (.152) (.131) (.133)Communication About DeathR and spouse discussed how -.219 -.046 R will cope with death (.181) (.159)R was with spouse -.021 0.166 when s/he died (.136) (.121)Adjusted R-squared 0.129 0.150 0.148 0.137 0.156 0.156Constant -.243 -.695 -.599 1.61 1.09 0.897 (.868) (.954) (.980) (.749) (.845) (.859)N 210 210 210 155 155 155
Notes: + p < .10; * p < .05; ** p< .01; *** p < .001.Number of months between baseline and wave 1 interview controlled in all models.
Anxiety, Six months Anxiety, 18 months
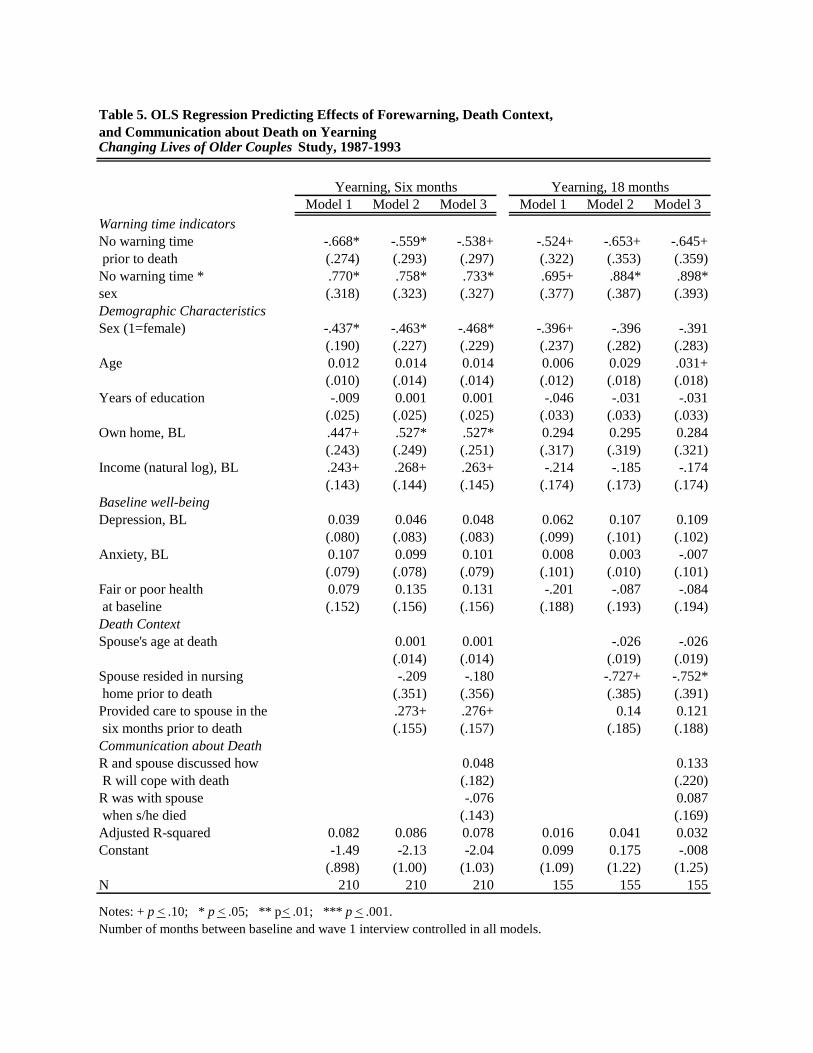
Table 5. OLS Regression Predicting Effects of Forewarning, Death Context,and Communication about Death on YearningChanging Lives of Older Couples Study, 1987-1993
Model 1 Model 2 Model 3 Model 1 Model 2 Model 3Warning time indicatorsNo warning time -.668* -.559* -.538+ -.524+ -.653+ -.645+ prior to death (.274) (.293) (.297) (.322) (.353) (.359)No warning time * .770* .758* .733* .695+ .884* .898*sex (.318) (.323) (.327) (.377) (.387) (.393)Demographic CharacteristicsSex (1=female) -.437* -.463* -.468* -.396+ -.396 -.391
(.190) (.227) (.229) (.237) (.282) (.283)Age 0.012 0.014 0.014 0.006 0.029 .031+
(.010) (.014) (.014) (.012) (.018) (.018)Years of education -.009 0.001 0.001 -.046 -.031 -.031
(.025) (.025) (.025) (.033) (.033) (.033)Own home, BL .447+ .527* .527* 0.294 0.295 0.284
(.243) (.249) (.251) (.317) (.319) (.321)Income (natural log), BL .243+ .268+ .263+ -.214 -.185 -.174
(.143) (.144) (.145) (.174) (.173) (.174)Baseline well-beingDepression, BL 0.039 0.046 0.048 0.062 0.107 0.109
(.080) (.083) (.083) (.099) (.101) (.102)Anxiety, BL 0.107 0.099 0.101 0.008 0.003 -.007
(.079) (.078) (.079) (.101) (.010) (.101)Fair or poor health 0.079 0.135 0.131 -.201 -.087 -.084 at baseline (.152) (.156) (.156) (.188) (.193) (.194)Death ContextSpouse's age at death 0.001 0.001 -.026 -.026
(.014) (.014) (.019) (.019)Spouse resided in nursing -.209 -.180 -.727+ -.752* home prior to death (.351) (.356) (.385) (.391)Provided care to spouse in the .273+ .276+ 0.14 0.121 six months prior to death (.155) (.157) (.185) (.188)Communication about DeathR and spouse discussed how 0.048 0.133 R will cope with death (.182) (.220)R was with spouse -.076 0.087 when s/he died (.143) (.169)Adjusted R-squared 0.082 0.086 0.078 0.016 0.041 0.032Constant -1.49 -2.13 -2.04 0.099 0.175 -.008 (.898) (1.00) (1.03) (1.09) (1.22) (1.25)N 210 210 210 155 155 155
Notes: + p < .10; * p < .05; ** p< .01; *** p < .001.Number of months between baseline and wave 1 interview controlled in all models.
Yearning, Six months Yearning, 18 months

Figure 1. Yearning (Wave 1) by Gender and Death Forewarning
-0.4
-0.2
0
0.2
0.4
S udde n D e a th F o re warne d
(N o t e : M o d e l 3 c o nt r o ls d e m o g r a p h ic a nd h e a lt h c h a r a c t e r ist ic s;
Yea
rnin
g, W
ave
1(S
tand
ardi
zed)
Men, Model 1Women, Model 1Men, Model 3Women, Model 3
Figure 2. Yearning (Wave 2) by Gender and Death Forewarning
-0.4
-0.2
0
0.2
0.4
Sudden Death Forewarned
Yea
rnin
g, W
ave
2 (S
tand
ardi
zed) Men, Model 1
Women, Model 1
Men, Model 3
Women, Model 3











![005014910 00293 - National Archives of Ireland · 2013-06-18 · Dublin to Julian G. W. Butler of 2 Garscube Murryfield Edinburgh Esquire Effects £1,532 163. 4d. ... Joseph [337]](https://img.pdfslide.us/doc/110x75/5fa3e614d9fd142da16a112d/005014910-00293-national-archives-of-2013-06-18-dublin-to-julian-g-w-butler.jpg)
















