Embed Size (px)
Citation preview

Forensic Implications of the Foot andAnkle
Jeremy Rich, DPM,1 Dorothy E. Dean, MD,2 and Yvonne Y. Cheung, MD3
To clinicians, forensic medicine and the foot and ankle complex may appear to have little connection.However, if decomposed, burned, fragmented, or skeletonized human remains are recovered, the footand ankle can provide information leading to identification and incident analysis. Furthermore, analysis ofdata collected at accidents can lead to safety modifications. This article reviews common elements offorensic medicine applied to the foot and ankle in 2 areas: establishing positive identification by usingradiographic comparisons and analyzing aviation incidents. An understanding of these cases will en-hance clinicians’ awareness of the potential forensic value of the foot and ankle. (The Journal of Foot &Ankle Surgery 42(4):221–225, 2003)
Key words: forensic science, forensic pathology, human identification, ankle, foot
Often, the examination of human remains in suspicious,unexpected, violent, and unattended deaths requires a mul-tidisciplinary approach, using forensic pathologists, radiol-ogists, anthropologists, odontologists, and other experts (1).The use of the foot and ankle complex in forensic investi-gations has been reported in the medical and forensic liter-ature (2–16). The infamous Ruxton case of 1935 matcheddismembered feet to footwear in a nonmetric effort toincrease the identification potential from 2 mutilated dece-dents (14,15). Reports have evaluated quantitatively the roleof foot and ankle bones in forensic medicine by anthropo-metric techniques from large skeletal collections (2,3,6,9).In certain cases, pre- and postsurgical radiographs of thefoot and ankle can assist in establishing either presumptiveor positive identification (16). Moreover, surgical interven-tion with subsequent soft tissue and bone healing does notpreclude positive identification, even if the only antemortemradiographs are those taken before surgery (16).
This article reviews forensic investigations involving thefoot and ankle in 2 areas: establishing positive identificationby using radiographic comparisons and the analysis of avi-ation incidents. An understanding of these cases will en-hance clinicians’ awareness of the potential forensic valueof the foot and ankle.
Identification of Human Remains From the Footand Ankle
Part of a forensic investigation may involve identifying adecedent. Identification can be particularly difficult whenhuman remains are decomposed, fragmented, or mutilatedwhen recovered. The most useful anatomic regions foridentification are the skull, teeth, chest, lumbar spine, andpelvis. When these elements are unavailable because theyhave been destroyed, are inconclusive, or are incomplete,the foot and ankle can be useful. Given their protectednature in footwear, the feet usually escape the trauma sus-tained by the rest of the body. Footwear not only slows thedisarticulation process but also aids in the retention of footand ankle bones (17). High-top boots may retard the disar-ticulation sequence between the leg and the foot in aqueousenvironments (17). Moreover, the short and stout architec-ture of the metatarsals offers an additional degree of pro-tection (9).
Animal or Human Remains?
Although morphologic distinctions between human andanimal remains should not mislead an experienced forensicexpert, hind bear paws remain an exception. At first glance,the human foot and hind bear paw are particularly difficultto distinguish. If the hide, hair, and claws are removed, thepaws often resemble human hands and feet (18,19). Thecircumstances surrounding the recovery, including the dis-posal site, manner of skinning, and time of year recovered,combined with examination of the osseous features, canhelp discern if the remains are indeed human (19).
Radiographs or defleshing techniques can help establishseveral skeletal differences between the hind bear paw andthe human foot. Paw calcanei are tapered from distal to
From the From Harvard Medical School, Boston, MA; Franklin CountyCoroner’s Office, Columbus, OH; and Dartmouth Medical School,Hanover, NH. Address correspondence to: Dorothy E. Dean, MD, 520King Ave, Columbus, OH 43201.
1Research Fellow, Harvard Medical School.2Forensic Pathologist and Deputy Coroner, Franklin County Coroner’s
Office.3Assistant Professor of Radiology, Dartmouth Medical School.
Copyright © 2003 by the American College of Foot and Ankle Surgeons1067-2516/03/4204-0009$30.00/0doi:10.1053/jfas.2003.50027
VOLUME 42, NUMBER 4, JULY/AUGUST 2003 221

proximal. The bear paw’s talus has an appreciably deeptrochlea. Moreover, the phalanges and metatarsals are moresculptured, lack distal tufts, and have numerous metatarsalsesamoids. The metatarsals are also reversed in robusticity.The first metatarsal of the human is largest in girth andlength, whereas the fourth metatarsal of the hind bear pawis the most robust.
Establishing Identification From RadiographicComparisons
Positive identification of human remains can be estab-lished by comparing postmortem radiographs with antemor-tem films (20–27). Radiographic observation of foreignbodies, congenital anomalies, pathological processes, andprior surgical intervention can contribute to positive iden-tification (20–27). Even if the region is anatomically intact,unique characteristics within and between the soft tissuesand bones may be present. These features may includeexostoses and trabecular bone patterns. Radiographic com-parisons, however, require procurement of medical recordsof the victim after a presumptive identification is made. Thisis usually performed by using the available personal effectsor location of death.
Presumptive Identification
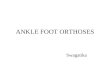
When only the postmortem radiographs are available, apositive identification cannot be made. However, presump-tive identification based on comparisons of postmortemradiographs with past medical information can be useful. Asmoldering car containing charred and calcined human re-mains was discovered in a wooded area. The distal righttibia and proximal bones of the right foot were fused to thevictim’s socks. Unfortunately, the bones of the left footwere too fragmented to be useful forensically. The medicalhistory of the vehicle’s owner included a fracture of hisright ankle 15 years before his absence (24). Postmortemradiographs of the right ankle showed a surgically per-formed tibiotalar fusion and a distal fibulectomy (Fig. 1).Presumptive identification was made on the basis of the pastmedical history and postmortem radiographs.
Surgical Intervention and Positive Identification
An isolated charred human foot was recovered from afarmyard (7). Before the foot was discovered, a middle-agedwoman was reported missing by her husband. Postmortemradiographs of the left foot showed surgically fused proxi-mal and distal interphalangeal joints, and were consistentwith an antemortem medical procedure. The missing indi-vidual had surgical intervention of her left foot, including an
arthrodesis of the interphalangeal joints. Antemortem radio-graphs were obtained for comparison. In addition to thesurgically modified phalanges, the trabecular patternsmatched without discrepancy and established positive iden-tification (7).
Surgical plates, screws, and pins can also be invaluablefor identity purposes (28,29). If antemortem information isavailable, the use of surgically implanted devices in the footand ankle may offer valuable identity data. For example,radiographic comparisons of a first metatarsophalangealjoint implant established identification of a decedent bycomparing the device with available medical records (BoydG. Stephens, MD, personal communication, February1998).
Anomalous Development and Positive Identification
Anomalous development of the foot and ankle accompa-nied by surgical intervention may also help establish posi-tive identification from decomposed human remains. Forexample, a markedly decomposed 79-inch man was foundin a locked, spartan apartment (30). Because the apartmentwas undisturbed and did not show forced entry, all initialindications were to an apparently natural death. Police pho-tographs of the decedent showed him wearing orthopedicfootwear. Physical examination of the decedent in the cor-oner’s office showed bilateral talipes equinovarus.
Several techniques were used to establish positive iden-tification; however, they were unsuccessful. Because of thedecomposed state of the remains, only 3 fingerprints could
FIGURE 1 Postmortem right ankle radiograph of a tibiotalar fusionthat established presumptive identification. (From Riddick L,Brogdon BG, Laswell-Hoff J, Demar B. Radiographic identificationof charred human remains through use of the dorsal defect of thepatella. J Forensic Sci 28:263–267, 1983. Copyright ASTM Interna-tional. Reprinted with permission.)
222 THE JOURNAL OF FOOT & ANKLE SURGERY

be obtained. The presumed decedent had been arrested forvagrancy, but there were no fingerprints in either local ornational databases.
There was no medical or dental information available,and the decedent was not reported missing by his relatives.Because the foot deformities were a distinctive anatomicfeature of the decedent, investigators contacted vendors ofcustom orthopedic footwear in the local area. A vendor hadconstructed shoes for a client fitting the decedent’s physicaldescription. Of note, a clinical diagnosis of bilateral talipesequinovarus was described.
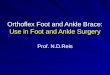
The most recent radiographs of each foot and the client’sname, social security number, and date of birth were thengiven to the coroner’s office. Radiographic comparisons ofthe feet and subsequent defleshing showed bilateral talipesequinovarus deformities (30) (Fig. 2). Positive identificationwas established on the basis of skeletal features present inthe radiographs. Skeletal features in both feet were consis-tent with antemortem surgical intervention, including cal-caneal osteotomies to correct the bony anomalies of talipesequinovarus.
Mass Fatality Incidents
Mass fatality incidents in which foot and ankle radio-graphs were used for identification purposes include theValujet flight 592 crash and the Oklahoma City bombing(25,26). A historical example of using foot and ankle radio-graphic comparisons for identification in multiple fatalitiesincludes the infamous Noronic disaster (31,32). On Septem-ber 17, 1949, the Toronto Great Lakes liner, the Noronic,caught fire and 119 of the 527 passengers died (31,32).Because the human remains were considerably mutilatedand distorted, antemortem radiographs of passengers wereobtained.
The torso and extremities of 1 disaster victim were all butdestroyed (31). The left foot was relatively intact yet plan-tarflexed at the ankle joint and arched at the midtarsal joint;these features were most likely caused by perimortem al-terations. An antemortem radiograph of the left foot of apassenger was obtained for postmortem comparison. Poste-rior bone spurs and articulations (tarsal and intertarsal)provided several matching points without any discrepancy.Additionally, the medial sesamoid bone beneath the firstmetatarsal matched perfectly with the antemortem radio-graphs (31). Therefore, positive identification was estab-lished from radiographic comparison.
Analysis of Aviation Incidents From the Foot andAnkle
Documentation of foot and ankle injuries sustained in anaviation incident can provide valuable forensic data and
offer safety modifications (33–39). These data can improvethe design of aircraft and prevent similar injuries in thefuture. An example is an investigation involving a DC-9aircraft incident in Toronto (36). In a failed effort to aborttake-off, the aircraft reached the end of the runway and fell50 feet into a ravine. The surviving passengers sustainedseveral foot and ankle injuries, including tibial, fibular, tali,calcanei, and cuboid fractures (36).
FIGURE 2 Lateral radiographic comparison of the left foot andankle shows matching skeletal features (noted by the arrows). (A)Antemortem. (B) Postmortem. (Copyright ASTM International. Re-printed with permission [30].)
VOLUME 42, NUMBER 4, JULY/AUGUST 2003 223

Evaluation of these injuries from clinical radiographs andtheir implications led to the introduction of improvements inaircraft design. For example, the crashed aircraft seats weremounted on longitudinally placed floor rails. A transversebar was placed under each seat and fixed to the floor rail.Many seats had left the mounting rails, and further scrutinyrevealed that the transverse bars remained firmly attached tothe floor rails. When the passengers were thrown forward onimpact, their feet were caught beneath these bars, therebycausing many foot and ankle injuries. If the bars had beenattached to the seats instead of the floor, these injuries mayhave been avoided (36). Recommendations in aircraft seatdesign were introduced, and modifications in seat construc-tion commenced.
Flail-Type Injury Patterns
In another forensic investigation, Brogdon reviewed theradiographs of 131 victims in the Air India flight 182 bombexplosion of 1985, which involved many dislocation andflail-type injuries in the foot and ankle (B. G. Brogdon, MD,personal communication, March 2001). Comminuted frac-tures at the distal aspects of the tibia and fibula are consis-tent with a flail-type injury in which a significant dorsallydirected force from a plantar location causes the foot andankle to flail outward because of the resultant dorsiflexoryforces. In these instances, multiple fractures to the metatar-sals and midtarsal joint occur, leaving the calcaneus intact(34,35). This fracture pattern is consistent with a high-intensity plantar force delivered to the midfoot before theleg and foot flail away on impact, as encountered in aviationincidents. These fractures also may be the result of the bodybeing thrown upward and through the seat belt in an aircraft,thereby causing impaction against the seatback in front. Inaddition, these injuries may be the result of a collision witha part of the aircraft.
Who Was Flying the Aircraft?
Of particular interest in forensic investigations is exam-ining injury patterns in fatally injured aircraft pilots todetermine who was flying the aircraft when the fatal inci-dent occurred (35). This question is particularly importantwhen several occupants are aboard and ejected from thecabin on impact. In these instances, commingled body partsmake identification and incident reconstruction challenging.In cases involving training missions, the question ofwhether the student or instructor was flying the aircraft atimpact can be paramount.
Characteristic soft tissue and skeletal injuries may occurif the pilot’s feet were resting on the cockpit structuresduring a crash. Because rudder pedals are angulated, thecalcaneus is subject to considerable dorsiflexory forces on
impact. Comminuted fractures of the tarsal bones also aresustained. Plantar soft tissue tears, stripe-shaped hemato-mas, and flail-type injuries occur as a result of the pilotplacing his or her foot onto the cockpit controls.
In aviation incidents, the most common fracture site inthe talus is located within the neck (38). Anderson (38)called this fracture pattern “aviator’s astragulus.” The frac-ture is produced when aviators rest the soles of their feet onthe rudder bar during an airplane crash in a position of fullplantarflexion (34,35). Aviator’s astragulus has also beenreported in falls from heights and in motorcycle incidents(39).
Documentation of the aviator’s astragulus used in con-junction with other forensic evidence can implicate 1 personover another as the pilot. Forensic experts are sometimesasked to distinguish between 2 people, 1 living and 1deceased, both of whom with blood ethanol levels above thelegal limit for driving. Being able to diagnose and forensi-cally evaluate the aviator’s astragulus may exculpate theliving person.
Conclusions
The potential forensic value of the lower extremity maybe great. For clinicians, correlating injury pattern with theclinical history is provocative and worthy of further study toprevent insurance fraud and to determine the mechanism oftrauma. Important forensic implications of the foot andankle will almost certainly provide insight into human iden-tification, incident reconstruction, and safety modifications.
Acknowledgment
The authors thank B. G. Brogdon, MD, and Barbara C.Wolf, MD, for their editorial suggestions.
References
1. DiMaio DJ, DiMaio VJM. Medicolegal investigative systems. In Fo-rensic pathology, p 1, Elsevier, New York, 1989.
2. Steele DG. The estimation of sex on the basis of the talus and thecalcaneus. Am J Phys Anthropol 45:581–588, 1976.
3. Smith SL. Attribution of foot bones to sex and population groups.J Forensic Sci 42:186–195, 1997.
4. Huxley AK. Comparison of gestational age values derived from di-aphyseal length and foot length from forensic foetal remains. Med SciLaw 38:42–51, 1998.
5. Batamanabane M, Malathis S. Identification of human second, third,and fourth metatarsal bones. Anat Rec 207:509–511, 1983.
6. Introna F Jr, Di Vella G, Campobasso CP, Dragone M. Sex determi-nation by discriminant analysis of calcanei measurements. J ForensicSci 42:725–728, 1997.
7. Sivaloganathan S, Butt WP. A foot in the yard. Med Sci Law 28:150–156, 1988.
224 THE JOURNAL OF FOOT & ANKLE SURGERY

8. Byers S, Akoshima K, Curran B. Determination of adult stature frommetatarsal length. Am J Phys Anthropol 79:275–279, 1989.
9. Robling AG, Ubelaker DH. Sex determination from the metatarsals.J Forensic Sci. 42:1062–1069, 1997.
10. Singh SS, Singh SP. Identification of sex from tarsal bones. Acta Anat93:568–573, 1975.
11. Gordon CC, Buikstra JE. Linear models for the prediction of staturefrom foot and boot dimensions. J Forensic Sci 37:771–782, 1992.
12. Giles E, Vallandigham PH. Height estimation from foot and shoeprintlength. J Forensic Sci 36:1134–1151, 1991.
13. Leonetti G, Signoli M, Pelissier AL, Champsaur P, Hershkovitz I,Brunet C, Dutour O. Evidence of pin implantation as a means ofverifying death during the great plague of Marseilles. J Forensic Sci42:744–748, 1997.
14. Rich J. Increasing the identification potential from human foot re-mains. J Forensic Sci. 45:505–506, 2000.
15. Glaister J, Brash JC. The feet and the shoes. In Medico-Legal Aspectsof the Ruxton Case, pp 138–143, William Wood, Baltimore, 1937.
16. Rich J, Tatarek NE, Powers RH, Brogdon BG, Lewis BJ, Dean DE.Using pre- and post-surgical foot and ankle radiographs for identifi-cation. J Forensic Sci 47:1319–1322, 2002.
17. Haglund WD. Disappearance of soft tissues and the disarticulation of humanbeings from aqueous environments. J Forensic Sci 38:806–815, 1993.
18. Mann RW, Owsley DW. Medicolegal investigation involving a bear-paw. J Am Podiatr Med Assoc 80:623–625, 1990.
19. Stewart TD. Essentials of Forensic Anthropology: Especially as De-veloped in the United States, pp 45–58, Charles C. Thomas, Spring-field, IL, 1979.
20. Murphy WA, Spruill FG, Gantner GE. Radiologic identification ofunknown human remains. J Forensic Sci 25:727–735, 1980.
21. Murphy WA, Gantner GE. Radiologic examination of anatomical partsand skeletonized remains. J Forensic Sci 27:9–18, 1982.
22. Mann RW. Use of the trabeculae to establish positive identification.Forensic Sci Int 98:91–99, 1998.
23. Evans KT, Knight B, Whittaker DK. Radiology in identification. InForensic Radiology, pp 3–46, Blackwell, Oxford, 1982.
24. Brogdon BG. Radiological identification of individual remains. InForensic Radiology, pp 149–187, edited by BG Brogdon, CRC Press,Boca Raton, 1998.
25. Nye PJ, Tytle TL, Jarman RN, Eaton BG. The role of radiology in theOklahoma City bombing. Radiology 200:541–543, 1996.
26. Franz N. APMA news. September:48–49, 1996.27. Lichtenstein JE, Madewell JE, McMeekin RR, Madewell JE. The role
of radiology in fatality investigations. Am J Roentgen 150:751–755, 1988.28. Ubelaker DH, Jacobs CH. Identification of orthopedic device manu-
facturer. J Forensic Sci 40:168–170, 1995.29. Bennett JL, Benedix DC. Positive identification of cremains recovered
from an automobile based on presence of an internal fixation device.J Forensic Sci 44:1296–1298, 1999.
30. Sudimack JR, Lewis BJ, Rich J, Dean DE, Fardal PM. Identification ofdecomposed human remains from radiographic comparisons of anunusual foot deformity. J Forensic Sci 47:218–220, 2002.
31. Singleton AC. The roentgenological identification of victims of the“Noronic” disaster. Am J Roentgenol Radiat Ther 66:375–384, 1951.
32. Brown TC, Delaney RJ, Robinson WL. Medical identification in the“Noronic” disaster. JAMA 148:621–627, 1952.
33. Simson LR Jr. Roentgenography in the human factors investigation offatal aviation accidents. Aerosp Med 43:81–85, 1972.
34. Mason JK. Reconstruction of a fatal aircraft accident from medicalfindings. Proc R Soc Med 61:1079–1084, 1968.
35. Krefft S. Who was at the aircraft’s controls when the fatal accidentoccurred? Aerosp Med 41:785–789, 1970.
36. Horne JG, Mowbray M. Ankle and foot injuries in an aircraft crash.Foot Ankle 1:110–111, 1980.
37. Mann RW, Holland TD. Perimortem calcaneal and talar fracturessustained in a military crash in Vietnam. J Am Podiatr Med Assoc88:446–450, 1998.
38. Coltart WD. Aviator’s astragulus. J Bone Joint Surg 34B:545–566,1952.
39. Penny JN, Davis LA. Fractures and fracture-dislocations of the neck ofthe talus. J Trauma 20:1029–1037, 1980.
VOLUME 42, NUMBER 4, JULY/AUGUST 2003 225