Embed Size (px)
Citation preview

7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 1/19

7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 2/19
P R E P A R E D B Y : N U R U L S Y A Z W A N I R A M L I
Foreign Bodies of Air Passages
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 3/19
Foreign Bodies of Air Passages
A foreign body (FB) aspirated into air passage canlodge in the larynx, trachea, or bronchi (depend onsize and nature of FB).
Large FB = can’t pass thru glottis lodge insupraglottic area.
Smaller FB = pass down thru larynx into trachea or bronchi.
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 4/19
Aetiology
Vegetable
Peanut (most common)
Almond seed
Peas
Beans
Wheat seed
Water melon seed
Piece of carrot or apple, etc
Nonvegetable
Plastic whistle
Plastic toys
Safety pins
Nails / Screws
Coins
Bones
Buttons
Hair clips
Marble, etc
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 5/19
Nature of Foreign Body
Non-irritating type
Eg: plastic, glass, metallic FB
Relatively non- irritating
May remain symptomless for a long time
Irritating type
Eg: vegetable (peanuts, beans, seeds, etc)
Set up diffuse violent reaction congestion and oedema of tracheobronchial mucosa ( vegetal bronchitis)
swell up with time causing airway obstruction and latersuppuration in the lung.
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 6/19
Clinical Features
Symptomatology of FB is divided into 3 stages:1) Initial period of choking, gagging and wheezing
Last for a short time
FB may be coughed out or it may lodged in the larynx or further
down in tracheobronchial tree
2) Symptomless interval
Resp. mucosa adapts initial symptoms dissappear
3) Later symptoms
Caused by obstruction to the airway, inflammation or traumainduced by FB and would depend on site of its lodgement.
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 7/19
Cont. Clinical Features
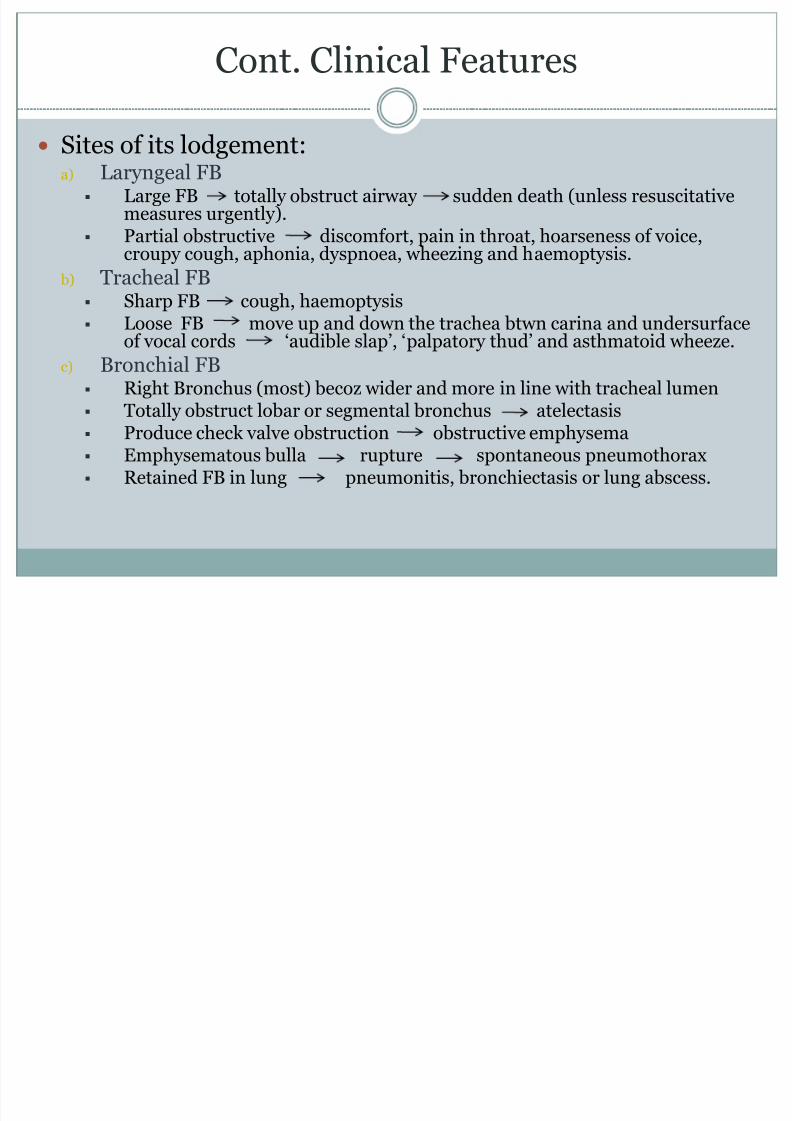
Sites of its lodgement:a) Laryngeal FB
Large FB totally obstruct airway sudden death (unless resuscitativemeasures urgently).
Partial obstructive discomfort, pain in throat, hoarseness of voice,croupy cough, aphonia, dyspnoea, wheezing and haemoptysis.
b) Tracheal FB Sharp FB cough, haemoptysis Loose FB move up and down the trachea btwn carina and undersurface
of vocal cords ‘audible slap’, ‘palpatory thud’ and asthmatoid wheeze.
c) Bronchial FB Right Bronchus (most) becoz wider and more in line with tracheal lumen
Totally obstruct lobar or segmental bronchus atelectasis Produce check valve obstruction obstructive emphysema Emphysematous bulla rupture spontaneous pneumothorax Retained FB in lung pneumonitis, bronchiectasis or lung abscess.
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 8/19
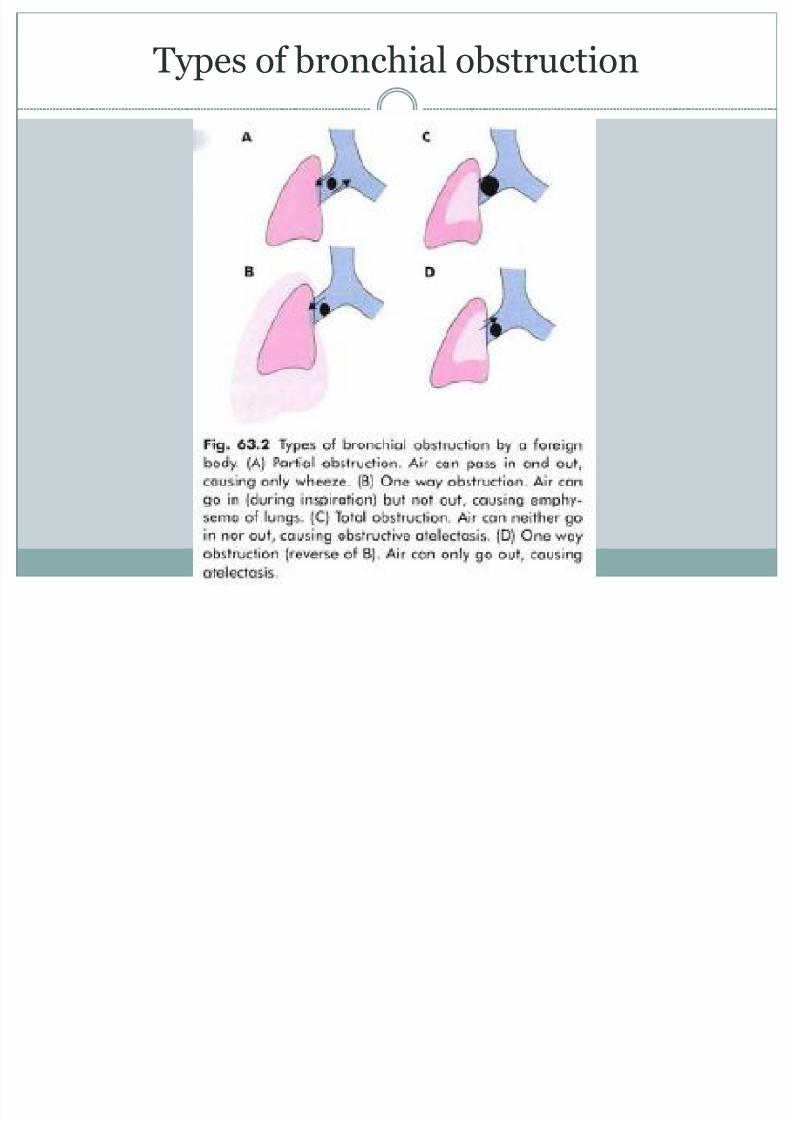
Types of bronchial obstruction
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 9/19
Diagnosis
Detailed Hx (FB ingestion)
PE of neck and chest Classical triad
Sudden onset of coughing
Wheezing Diminished air entry
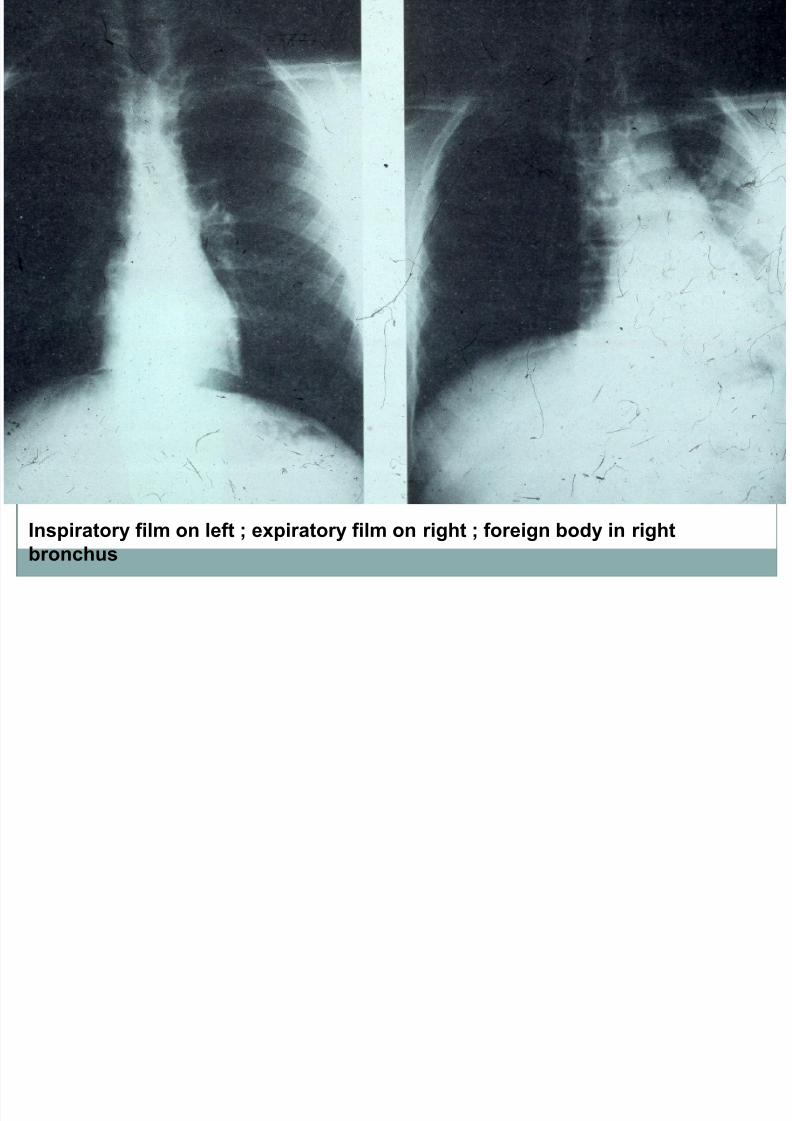
Radiology: Plain X-Ray
CXR at end of inspiration and expiration Fluoroscopy/videofluoroscopy
CT chest
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 10/19
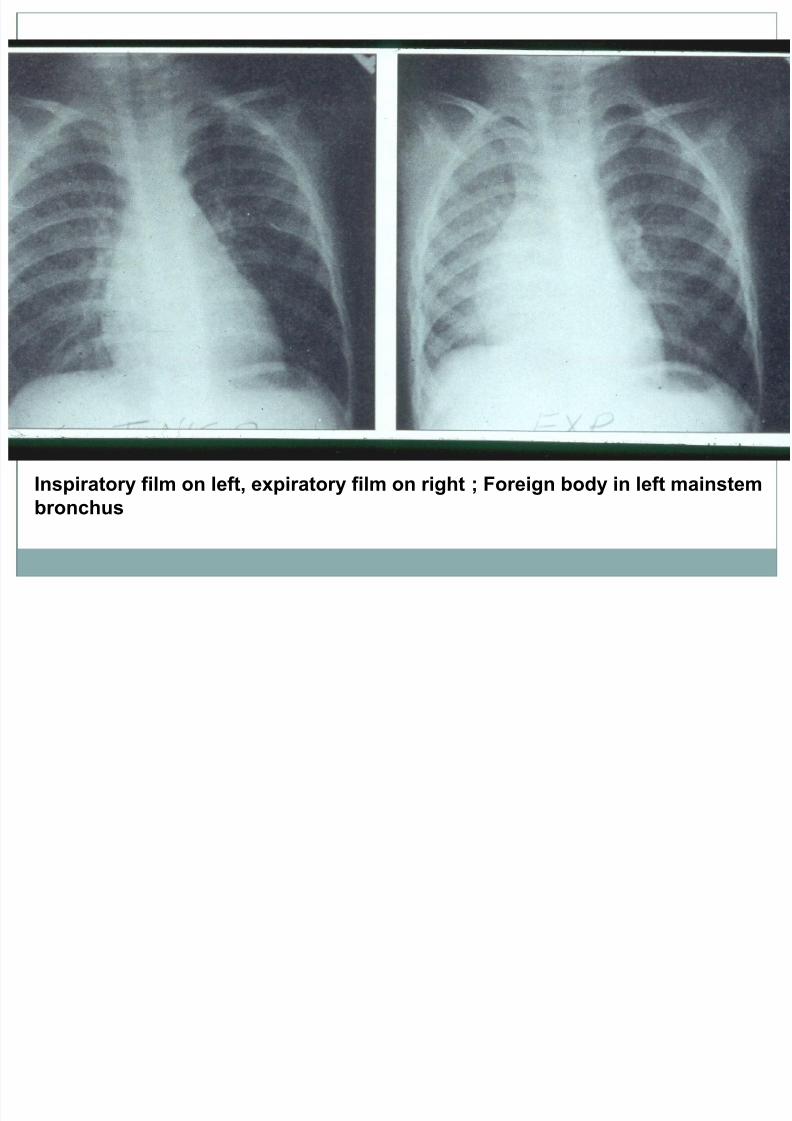
Inspiratory film on left, expiratory film on right ; Foreign body in left mainstem
bronchus
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 11/19
Inspiratory film on left ; expiratory film on right ; foreign body in right
bronchus
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 12/19
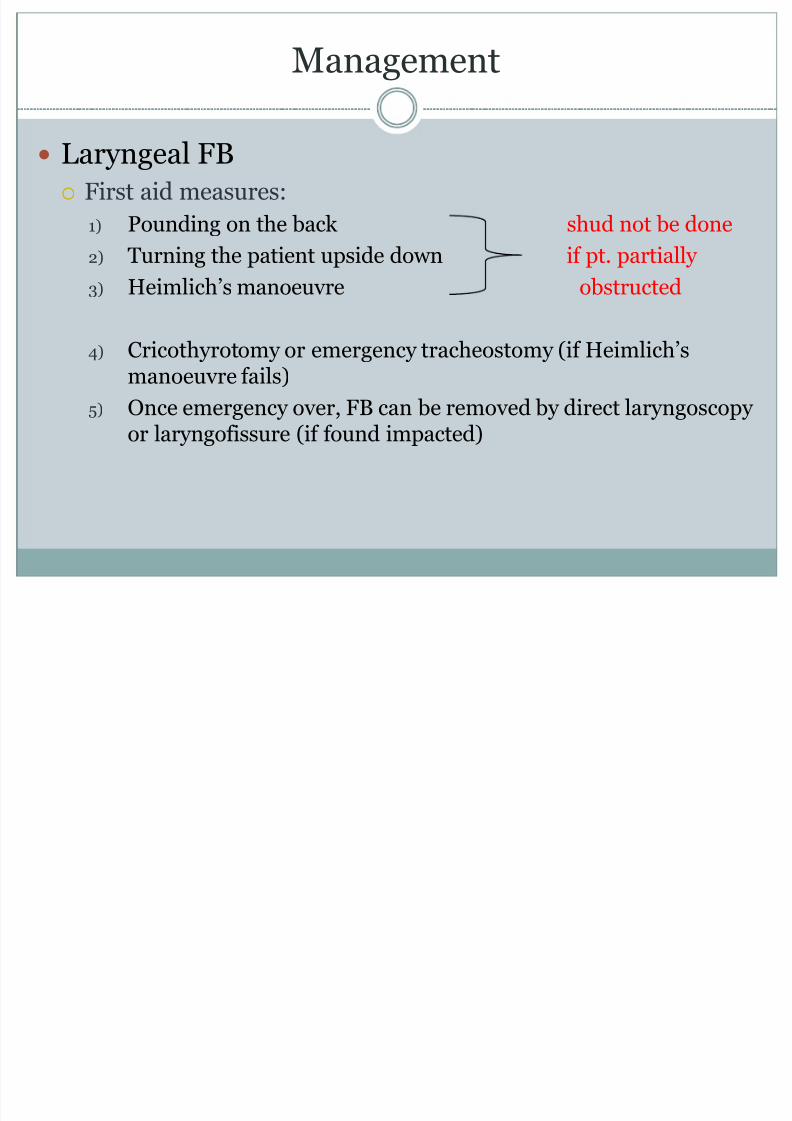
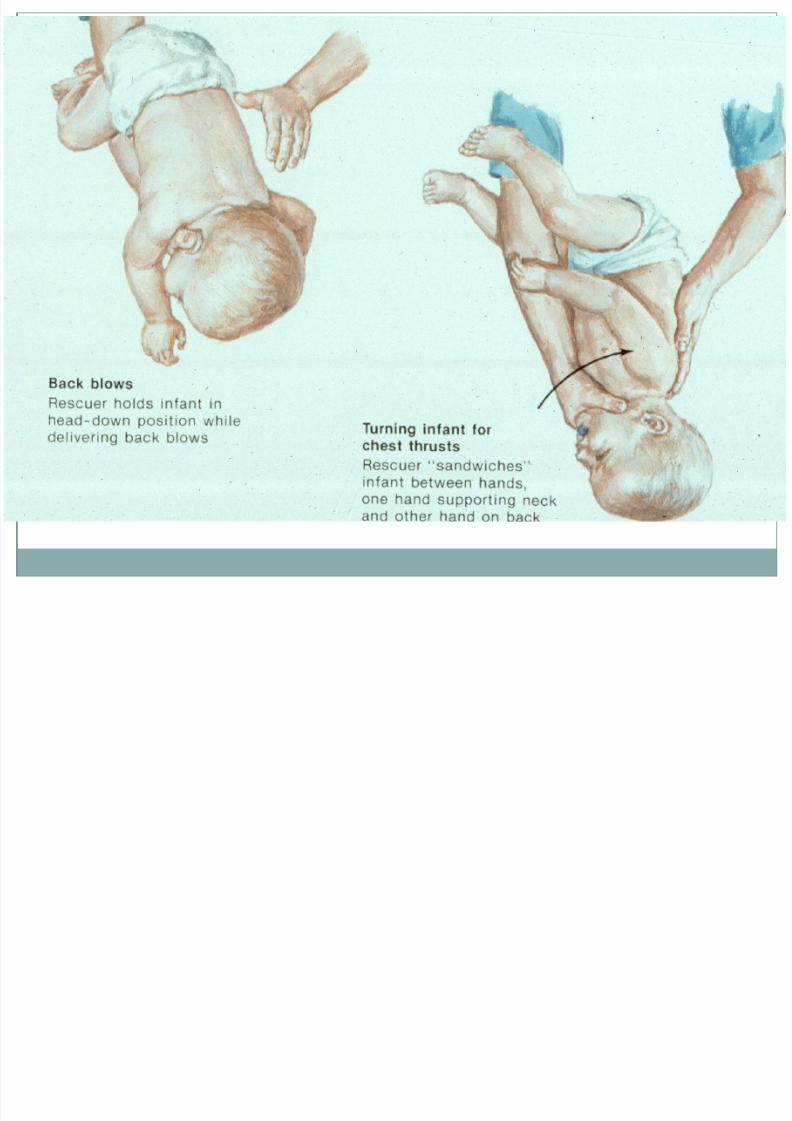
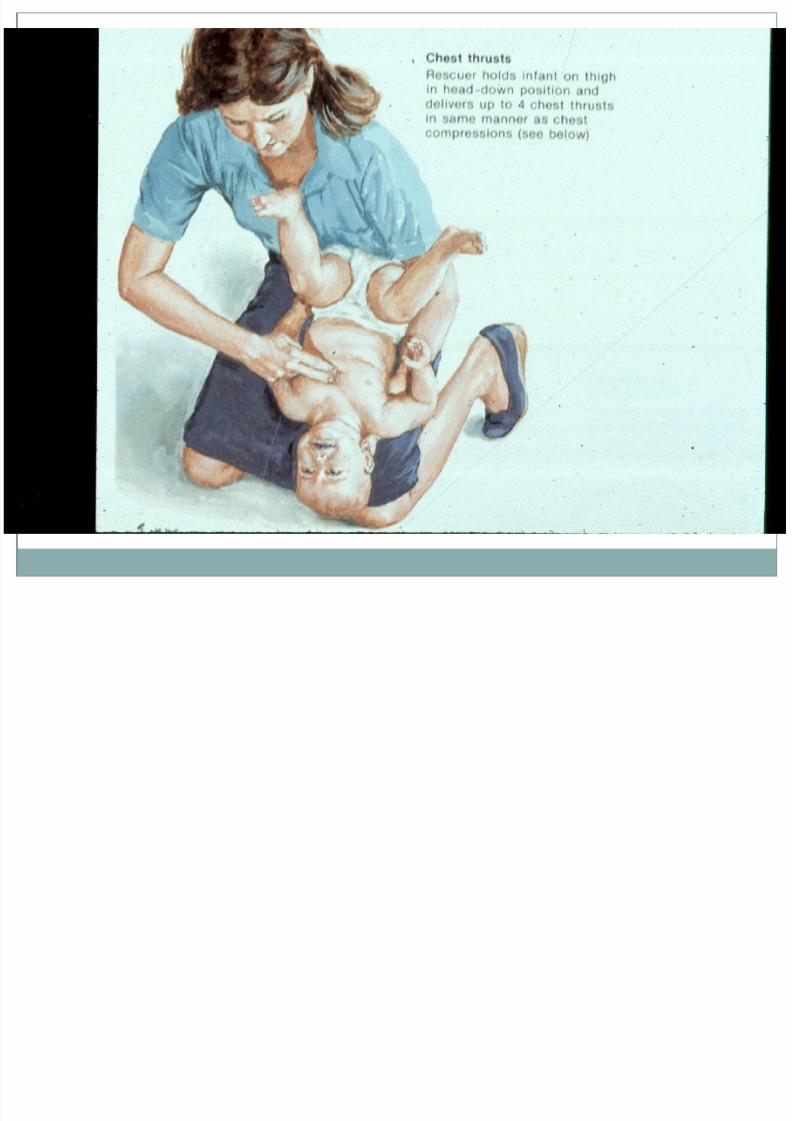
Management
Laryngeal FB
First aid measures:
1) Pounding on the back shud not be done
2) Turning the patient upside down if pt. partially
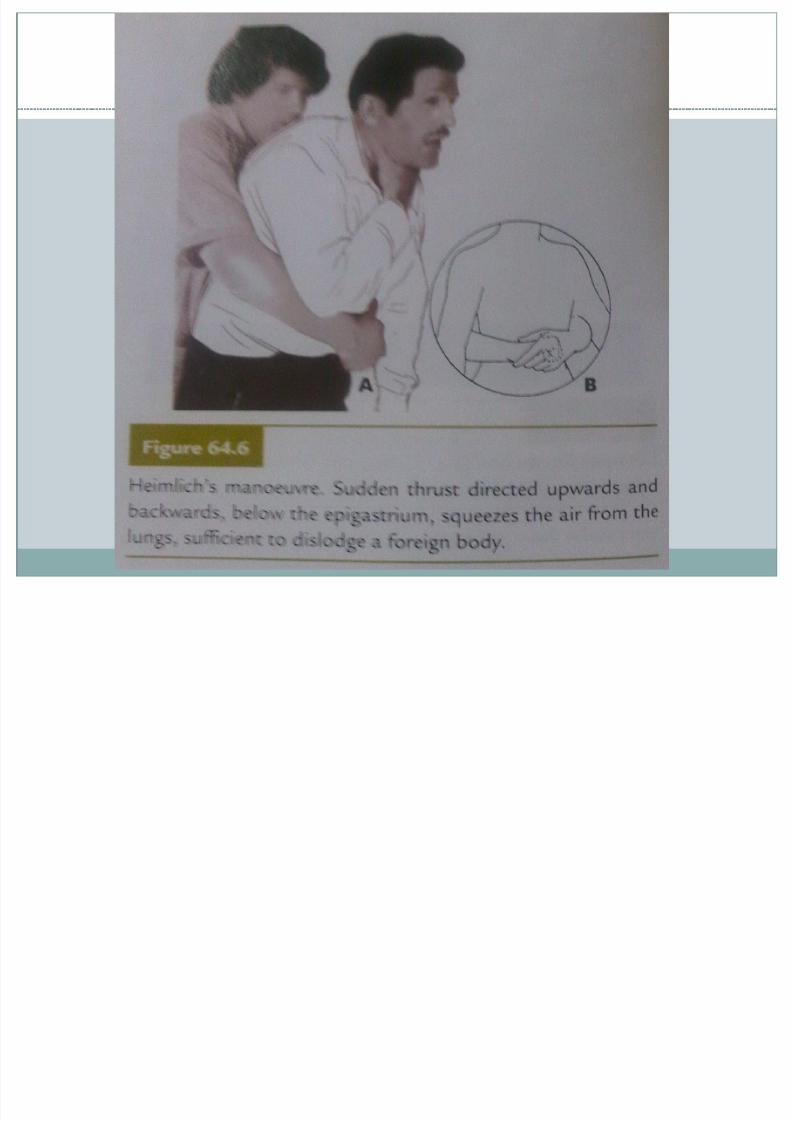
3) Heimlich’s manoeuvre obstructed
4) Cricothyrotomy or emergency tracheostomy (if Heimlich’s manoeuvre fails)
5) Once emergency over, FB can be removed by direct laryngoscopy or laryngofissure (if found impacted)
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 13/19
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 14/19
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 15/19

7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 16/19
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 17/19
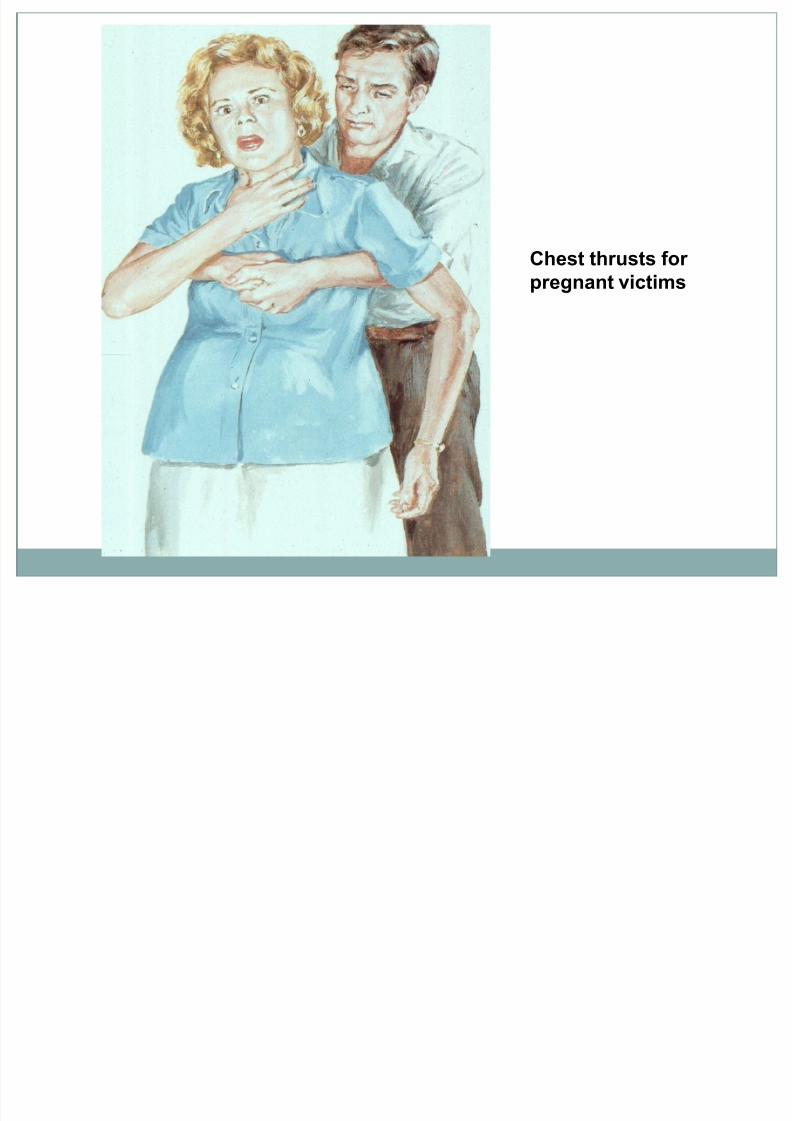
Chest thrusts for
pregnant victims
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 18/19
Cont. Management
Tracheal and Bronchial FBs Can be removed by bronchoscopy with full preparation and
under GA
Emergency removal not indicated unless there’s airway
obstruction or vegetable nature and likely to swell up. Methods to remove tracheobronchial FB:
1) Conventional rigid bronchoscopy
2) Rigid bronchoscopy with telescopic aid
3) Bronchoscopy with C-arm fluoroscopy
4) Use of Dormia basket or Fogarty’s balloon for rounded objects 5) Tracheostomy 1st and then bronchoscopy thru the tracheostome
6) Thoracotomy and bronchotomy for peripheral FBs
7) Flexible fibre optic bronchoscopy in selected adult pt.
7/29/2019 Foreign Body of Air Passage
http://slidepdf.com/reader/full/foreign-body-of-air-passage 19/19
Thank You





























