-
VOLUME TWELVE NUMBER THREE FALL 2000
ORTHODONTIC FORCED ERUPTION IN MULTIDISCIPLINARY TREATMENT
-
the relationship between orthodontictooth movement and
infrabonyosseous defects. On the negative side,there was an
inability to predictablygain connective tissue attachmentwhen
bodily moving a tooth into aninfrabony defect.1,2 However, on
thepositive side, it had been demonstrat-ed in earlier studies that
favorableradiographic changes result whenmesially tipped second
molars areuprighted and extruded by orthodon-tic forces.3 These
findings were fur-ther expanded to include forcederuption for the
treatment of one-and two-walled infrabony defects4and forced
eruption for the treatmentof otherwise non-restorable
teeth.5Without forced eruption, these teethwere destined for
extraction or peri-odontal crown lengthening proce-dures, resulting
in long unestheticteeth with visible restorative margins.It has
been demonstrated that evenin the presence of advanced peri-odontal
disease, when teeth areorthodontically extruded, the bonycrest will
follow the direction of theforce.6,7 However, initial
periodontalpreparation to control gingivalinflammation prior to
orthodonticintervention is highly recommended.
Which of the following bestdescribes forced eruption?
(A) Drilling "venting" holes in the side of Vesuvius
(B) Uncorking a warm bottle of champagne
(C) Explaining to your office staff that you will be starting
evening hours for your patients
(D) Using orthodontic force to extrude teeth
(E) All of the above
If you answered positively to anyof the above, you are entitled
to con-tinue reading this issue. If you didnot, we hope you will
enjoy this issueof Orthodontic Dialogue anyway!
It has long been known that tensileforces placed on the
periosteum willcreate histological and structuralchanges in the
underlying bone.Forced eruption, a.k.a. orthodonticextrusion, is a
simple but quite effec-tive means of placing tension on
theperiodontal ligament (periosteum) inorder to precipitate
favorableanatomical changes in otherwiseunmanageable osseous
conditions.Over the last three decades, the den-tal literature has
been replete withstudies and clinical trials outlining
Finally, the literature has shown that forced eruption can be
utilizedto help prepare otherwise unsuitablesites for eventual
implant placement.8,9
Fixed appliances should be used toallow control of the
application of agentle, continuous force. This systemshould include
sufficient dental unitsto counteract the potential sideeffects of
the eruptive force. A reten-tion period, which may include
fixedstabilization for four to six months, isnecessary. Proper
retention maxi-mizes the esthetic result and/orensures adequate
bone maturationprior to definitive periodontal care.
Orthodontic forced eruption can be extremely useful as part of
themultidisciplinary treatment of thefollowing:
esthetic enhancement of the maxillary anterior periodontium;
recontouring infrabony peri-odontal defects in anterior and
posterior areas;
esthetic restoration of subgingival and subosseous dental
fractures, carious lesions,and resorbed areas;
maintenance of osseous integrity
You may wish to share this issue of Orthodontic Dialogue with
your hygienists and other staff members.
ORTHODONTIC FORCED ERUPTION IN MULTIDISCIPLINARY TREATMENT
A B C
D E
F
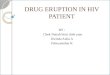
FIG. 2
Mesialosseousdefect onmaxillaryright canine
Leveling ofbony defectafter canineeruption andpreparationof
teeth #5, 6and 7
A
B
FIG. 3
Esthetic enhancement using orthodontic forced eruption following
placement of anautogenous free gingival graft
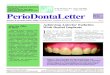
FIG. 1A B C D
E
Forced eruption followed by surgicalcrown lengthening to ensure
the gingi-val margin of the fractured maxillaryright central is in
esthetic harmonywith the unrestored left central
-
ORTH
ODO
NTIC
DIAL
OG
UE
in "early" trauma sites (for eventual implant replacements);
and
slow extrusion of hopeless peri-odontally involved teeth in
preparation for implant placement.
Case #1: A 30-year-old femalepatient was not pleased with
theappearance of her partially eruptedmaxillary left canine. The
tooth had alack of attached gingiva combinedwith a very fragile
mucosal attachmentoverlying an extremely thin plate ofbuccal
alveolar bone. As a precaution-ary move, a free gingival graft
wasplaced prior to orthodontic extrusion.The graft was expected to
prevent theoccurrence of adverse periodontal con-ditions in the
area. Orthodonticforced eruption was then used to bringthe canine
into function withimproved esthetics. The orthodonticextrusion
enhanced the success of thegraft, which resulted in the
desiredesthetic change. (See Fig. 1.)
Case #2: Tension applied viaperiodontal ligament as a result
offorced eruption led to radiographicevidence of improved osseous
archi-tecture. The crown may requireselective recontouring, or, in
severecases, the extruded tooth may requireendodontic therapy
followed by pros-thetic coverage. (See Fig. 2.)
Case #3: This patient presentedwith a hockey injury that
resulted ina subgingival fracture of his rightcentral incisor.
Forced eruption wasused to move gingival tissues andosseous crest
incisally. Periodontalsurgical intervention then enabledthe
restorative dentist to place a fullcoverage crown. The
traumatizedtooth was then stabilized by splintingto the adjacent
central incisor. (See Fig. 3.)
Case #4: A very young patient suf-fered a subgingival fracture
of theentire central incisor crown. Theplacement of a pin in the
crown followed root canal therapy. Thetooth was then extruded with
forcederuption so that a temporary crowncould be placed. This
multidiscipli-nary approach was used to preservethe root in order
to avoid atrophy ofthe surrounding bone that normallyaccompanies a
long-standingextraction site.
The preservation of bone willenhance the success of
eventualimplant replacement if it becomesnecessary at a later date.
(See Fig. 4.)
Case #5: Diagrammatic represen-tation of forced eruption of a
toothwith severe periodontal involvement.The bracket is placed
gingivally onthe involved tooth in order toextrude the tooth by
means of analignment arch wire. Bone and softtissue are moved
incisally as thetooth is forcibly erupted and thenstabilized for
four to six months.Subsequently, the affected tooth isextracted,
leaving significantlyenhanced hard and soft tissues in thearea for
eventual implant placement.Hard and soft tissues can be
furtherimproved with the placement of anautogenous or allogenic
bone graftcombined with gingival enhance-ment and/or recontouring
before orafter implant placement. (See Fig. 5.)
Evidence has shown that simpleextrusion of periodontally
involvedteeth, traumatized teeth, or normallynon-restorable teeth
can provide therestorative dentist with more favor-able conditions
for the placement offunctional and esthetically
pleasingrestorations. The inclusion of ortho-dontic forced eruption
as part of themultidisciplinary treatment approachhas the potential
to greatly enhanceesthetics, recontour periodontaldefects,
eliminate disfigurement fromdental injuries, and facilitate
dentalimplant placement.
ESTHETIC ENHANCEMENT
CONCLUSION
FIG. 4 FIG. 5AA B
C D
E F
B
C D
MAINTENANCE OF OSSEOUSINTEGRITY
EXTRUSION OF PERIODONTALLYINVOLVED TEETH
RECONTOURINGINFRABONY DEFECTS
Forced eruption of traumatized tooth in the mixed dentition
stage ofdevelopment. This procedure to retain this otherwise
unrestorable
root allowed the orthodontist to preserve the delicate
buccal-lingualplate around this tooth during this critical time in
development.
Premature loss of this tooth could result in atrophy of the bony
ridge,making future implant placement difficult or even impossible
with-
out extensive bone regeneration surgical procedures.
Forced eruption of a hopeless periodontally involvedtooth to
prepare this area for a more ideal implantplacement. After
eruption, the tooth must be stabi-
lized for four months prior to extraction.Periodontal
regeneration can then be accomplished
to facilitate placement of an implant with morefavorable length,
width and esthetics.
ESTHETIC RESTORATION
-
1. Polson, A.; Caton, J.; Polson,A.P.; Nyman, S.; Novak, J.;
Reed,B.: Periodontal response after toothmovement into intrabony
defects. J Periodontol. 1984;55:197-202.
2. Wennstrom, J.L.; Stokland,B.L.; Nyman, S.; Thilander,
B.:Periodontal tissue response to ortho-dontic movement of teeth
withinfrabony pockets. Am J OrthodDentofac Orthop.
1993;103:313-319.
3. Brown, I.S.: The effect of ortho-dontic therapy on certain
types ofperiodontal defects. J Periodontol.1973;44:742-56.
4. Ingber, J.S.: Forced Eruption:Part 1. A method of treating
isolatedone and two wall infrabony osseousdefects rationale and
case report. J Periodontol. 1974;45:199-206.
5. Ingber, J.S.: Forced Eruption:Part II. A method of treating
non-restorable teeth periodontal andrestorative considerations. J
Periodontol. 1976;47:203-216.
6. Ven Rooy, J.R.; Yukna, R.A.:Orthodontic extrusion of
single-root-ed teeth affected with advanced peri-
ORTHODONTIC DIALOGUEVOLUME TWELVE NUMBER THREE FALL 2000
The American Association ofOrthodontists is a national dental
specialtyorganization that was founded in 1900.The AAO is comprised
of more than13,500 members. Among its primary goalsare the
advancement of the art and the sci-ence of orthodontics; the
encouragementand sponsorship of research; and theachievement of
high standards of excel-lence in orthodontic instruction,
practiceand continuing education.
Orthodontic Dialogue is publishedto help communicate with the
dental pro-fession about orthodontics and patientcare. Unless
stated otherwise, the opin-ions expressed and statements made
inthis publication are those of the authorsand do not imply
endorsement by or official policy of the AAO. Reproductionof all or
any part of this publication is prohibited without written
permission ofthe AAO.
Correspondence is welcome and should be sent to: American
Association of Orthodontists, Council on Com-munications, 401 N.
Lindbergh Blvd., St. Louis, MO 63141-7816. Dr. Michael D. Rennert,
PresidentMontreal, QuebecDr. Frederick G. Preis, President-ElectBel
Air, MarylandDr. James E. Gjerset, Secretary-TreasurerGrand Forks,
North DakotaDr. John R. Barbour, ChairCouncil on
CommunicationsCarmel, IndianaDr. Robert P. Scholz, Chair
Orthodontic Dialogue SubcommitteeSan Leandro, CaliforniaRonald S.
Moen, Executive DirectorSt. Louis, MissouriContributors to this
issue:Dr. John BednarNashua, New HampshireDr. Roger WiseSwampscott,
Massachusetts
American Association of Orthodontists401 N. Lindbergh Blvd.St.
Louis, MO 63141-7816
The AAO recommends that every childshould have an orthodontic
screening nolater than age 7.
The AAO encourages you and yourpatients to visit the AAO Web
site,Orthodontics Online, to learn moreabout the AAO and
orthodontics.
www.braces.org
odontal disease. Am J OrthodDentofac Orthop. 1985;87:67-74.
7. Ven Rooy, J.R.; Vanarsdall,R.L.: Tooth eruption: correlation
ofhistologic and radiograph findings inthe animal model with
clinical andradiographic findings in humans. Int.J. Adult
Orthodontics andOrthognathic Surgery, Vol. 4. 1987;235-245.
8. Salema, H.; Salema, M.: Therole of orthodontic extrusive
remod-eling in the enhancement of hardand soft tissue profiles
prior toimplant placement. Int. J. Perio RestDent. 1993;
313-333.
9. Mantzikos, T.; Shamus I.:Forced Eruption and Implant
SiteDevelopment: An OsteophysiologicResponse. Am J Orthod
DentofacOrthop. 1999;115:583-91.
REFERENCES