Embed Size (px)
Citation preview

I''=--- -
DOC BC 5458 D:H42:3 1995 c.1 v.1
FOR REFERENCE DO NOT REMOVE FROM
LIBRARY

m~~~11~~~1~mmi11m1r 3 3298 00050 2816
Health Sector Labour Relations Commission
. . ea ec or ....... . Appropriate Bargaining Units
Report and Recommendations
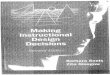
RESIDENTS 500
NURSES 26,000
PARAMEDICAL PROFESSIONALS 13,000
HEALTH SERVICES HEALTH SERVICES &SUPPORT &SUPPORT
(Facilities) (Community)
43,000 14,000
• James E. Dorsey, Commissioner
LEGf3L/\Tf\T Ll.3L\RY \ '/ICJ()};~~A., hC \18'\/ 1):~1 June 30, 1995

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Jame1 E. Doney, Comml11loner Karen E. Jewell, Counsel Dave MacKinnon, Facilltator I..ouile J. Stuart, Oftice Manager
June 30, 1995
The Honourable Dan Miller, Minister, Skills, Training & Labour, Room I 09 - Parliament Buildings, Victoria, B.C. VSV 1X4
Dear Mr. Minister:
212 - 865 HORNBY STREET
VANCOUVER, B.C. V6Z. 2GJ
PHONE: (604) 775-2845 FAX: (604) 775-2799
My final report with recommendations is enclosed. I thank you for having entrusted this challenge and important responsibility to my competence.
Your government and the Labour Relations Board provided every assistance and cooperation ~o the Commission. The affected Unions participated vigorously and cooperatively in the process. The B.C. Federation of Labour, Health Employers Association of British Columbia, Public Sector Employers' Council, Public Service Employee Relations Commission, Greater Vancouver Regional District and Capital Regional District provided valuable information, assistance and representations.
A small Commission team assisted me to achieve the successes in the process and recommendations. Any of the solutions recommended today that become tomorrow's problems are my sole responsibility.
The recommendations reduce bargaining units from 888 to I 0 by utilizing multi-employer unit structures. The effect is a change in union membership by 5% of the 96, 700 unionized employees.
, This includes 8,200 employees who will change employers from the Ministry of Health, Riverview Hospital, Glendale and Oak Bay Lodge Societies ·and six municipalities.
The change in union membership is less than 3% if membership transfers between affiliated unions, like Hospital Employees' Union and Canadian Union of Public Employees, are excluded.
Through mandating associations of trade union bargaining agents, the accompanying number of collective agreements and incidence of collective bargaining can be reduced from 200 to 5.
The recommendations set out how this can be achieved while protecting employee seniority, without prematurely terminating any collective agreements and without incurring additional costs to the taxpayer.

The Honourable Dan Miller June 30, 1995
Page2
The recommended bargaining unit structure and accompanying collective bargaining structure will enable the parties to address the foreseeable issues confronting health care service delivery and unionized health care employees who deliver the services.
Yours very truly,
•

HEALTH SECTOR LABOUR RELATIONS COMMISSION
ACKNOWLEDGMENT
When a group of strangers come together to do a task in a limited time, there is a risk that they will not develop the spirit necessary to succeed. For the commission's project, the spirit was there. We became a team and supported one another to our goal.
I am proud to have led such a dedicated, hard working and quick to laugh group of people.
Dave MacKinnon has been a loyal first mate for whom no task was too menial and no challenge too great. His hard work, good humour, insight and challenging approach were invaluable assistance. His cast iron briefcase, stories and expressions ....
Karen Jewell married her duties at the Labour Relations Board and the commission in her good natured and hardworking way. Her experience in health care and law and her insight into current administration at the Labour Relations Board were invaluable.
Louise Stuart gave much of herself during the past four months. She also benefited from our health care system. No matter how frustrating the administrative obstacle, she took charge and thought of the needs of the commission. We are indebted to her dedication.
George Bryce willingly shared his experience in government, health administration, law and with the Royal Commission on Health Care and Costs and other commissions. With enthusiasm, he pursued data and detail.
Betty McDonell and Sherry Crowther, respectively, got the commission up and running and closed down and archived. Their positive attitude, willingness to take on any task and commitment made · much of the work happen.
To each of them and the many others in the Ministries of Skills, Training and Labour and Health who helped, thank you.
Most importantly, to the union officers and representatives, and to the leadership ofHEABC, sincere gratitude for the patience, participation, assistance and support extended to the commission. I hope that what we have fashioned and I have proposed serves the best interests of the public and their best interests.
Jim Dorsey
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995

HEALTH SECTOR LABOUR RELATIONS COMMISSION
FULL APPENDICES TO THIS REPORT ARE PUBLISHED IN A SEPARATE VOLUME.
FOR CONVENIENCE, APPENDICES (e), (i) and (j) ARE ALSO ( INCLUDED HERE.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
<if I '

· HEALTH SECTOR LABOUR RELATIONS COMMISSION
TABLE OF CONTENTS
Page
Acknowledgment
Abbreviations
Report ............. · ...... ·..... .. . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Introduction
In Advance of the Commission
Commission Process and Parties
Public Sector Collective Bargaining Reform
Health Care Reform
Appropriate Bargaining Unit Reshaping
Organization of Health Care Work
Change and Future Resource Allocation Competition
Integration of Health Care Delivery
Provincial Consistency Over Time
History of Union Representation
Province Wide, Multi-Employer Units Recommended
Ten Bargaining Units Recommended
Other Recommendations: Change Management
Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Charts
1. Current Union Representation: All Health Employees
2. Incongruence of Health Bargaining UnitStructures
3. Unionized Employees By Health Subsector
4. Representation of Recommended Bargaining Units
Appendices
a) Bill 45: Health Authorities Act, S.B.C. 1993, c.47 Bill 48: Miscellaneous Statutes Amendment Act (No. 2), S.B.C. 1994, c.50 Bill 40: Health Authorities Amendment Act; 1995
b) New Directions for a Healthy British Columbia
c) LRB Health Care Bargaining Unit Proceedings
d) Ministerial Correspondence
e) Trade Unions in Health Sector
t) Employee Associations in Health Sector
g) HEABC Unionized Membership Profile
h) HEABC Collective Agreement Status Report
i) Devolving Government or Public Agency Unionized Health Care
Employees : Trade Union By Sector
j) Estimated Number of Unionized Health Care Employees in B.C. : Sector By Trade Union
k) First Progress Statement, February 27, 1995
1) Second Progress Statement, April 28, 1995
m) Denominational Facilities Master Agreement
n) May 24, 1995 Proposed Restructuring Plan and Recommendations
o) Inventory of Documents
p) Update Newsletters
q) The Evolution of Professionalism
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
I

HEALTH SECTOR LABOUR RELATIONS COMMISSION
ABBREVIATIONS
BCGEU B.C. Government & Service LPN Licensed Practical Nurse Employees Union
PAR-BC Professional Association of Residents BCMA B.C. Medical Association ofB.C.
BCNU B.C. Nurses' Union PEA Professional Employees Association
BP LEA Broadway Pentecostal Lodge PRICARE B.C. Association of Private Care Employees' Association
PSEC Public Sector Employers' Council CCERA Continuing Care Employee Secretariat
Relations Association PSERC Public Service Employee Relations
CGWU Construction & General Workers Commission Union, Local 602
RN Registered Nurse CHC Community Health Council
RHB Regional Health Board CRD Capital Regional District
RPN Registered Psychiatric Nurse CUPE Canadian Union of Public Employees
UA United Assoc. of Journeymen & HEABC Health Employers Association ofB.C. Apprentices of the Plumbing &
HEU Hospital Employees' Union Pipefitting Industry of U.S. & Canada, Local 324
HLRA Health Labour Relations Association UBCJA United Brotherhood of Carpenters &
HSA Health Sciences Association ofB.C. Joiners of America, Local 1598
IBEW International. Brotherhood of UFCW United Food & Commercial Workers' Electrical Workers, Local 230 International Union, Local, 1518
IBPAT International Brotherhood of Painters UPN Union of Psychiatric Nurses & Allied Trades, Local 1163
USWA United Steelworkers of America, ICBC Insurance Corporation ofB.C. Local, 9705
IUOE International Union of Operating VMREU Vancouver Municipal & Regional Engineers, Local 882 Employees Union
IWA !WA-Canada WCB Workers' Compensation Board
LGN Licensed Graduate Nurse
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995

j
CURRENT UNION REPRESENTATION: ALL HEALTH EMPLOYEES
PLUMB* IWA*
PNTR*
* less than 100 members ** 101 - 500 members
BCNU BCGEU BPLEA CGWU CUPE HEU HSA
B.C. Nurses' Union B.C. Government & Service Employees Union Broadway Pentecostal Lodge Employees' Association Construction & General Workers Union, Local 602 Canadian union of Public Employees Hospital Employees' Union Health Sciences Association ofB.C.
IBEW IUOE IWA PAR
PEA** UPN
International Brotherhood of Electrical Workers International Union of Operating Engineers IW A - Canada . Professional Association of Residents of B. C.
PEA Professional Employees Association
UFCW USWA*
CUPE I BEW*
IUOE
BCGEU
HEU
CGWA** PAR** VMREU UBCJ* BPLEA*
PNTR International Brotherhood of Painters & Allied Trades UBCJ United Brotherhood of Carpenters & Joiners of America UFCW United Food & Commercial Workers' International
Union, Local, 1518 PLUMB United Assoc. Of Journeymen & Apprentices of the
Plumbing & Pipefitting Ind. of U.S. & Canada UPN Union of Psychiatric Nurses USWA United Steelworkers of America VMREU Vancouver Municipal·& Regional Employees Union
Chart 1
~

HEALTH SECTOR LABOUR RELATIONS COMMISSION
INTRODUCTION
"In general, we support a move toward one independent agent bargaining for management, and a significantly reduced number of bargaining units acting for the unions. Such a move would increase the flexibility of the system as it places greater emphasis on providing services in the home and in the community. A myriad bargaining agents do not foster mobility and multi-skilled services. Nor does a number of associations bargaining on behalf of employers encourage uniformity of working conditions. Therefore, the commission recommends that: both employers and unions move to reduce the numbers of bargaining agents and units." (Closer To Home, The Report of the British Columbia Royal Commission on Health Care and Costs, (1991) Vol. 2, p. D-27)
Against the background of health care delivery restructuring arising from the Royal Commission Report, this commission has been asked to make recommendations regarding the composition of the appropriate bargaining units in health care in B.C. Commission recommendations can be implemented by the Lieutenant Governor in Council through regulations that will have the same force and effect as a decision by the Labour Relations Board.
The legal rights of workers and their trade unions and the obligations of employers will be altered to the extent that the recommendations and regulations alter existing bargaining units, which were established by past Labour Relations Board decisions and voluntary employer recognition.
The fundamental purpose of the Commission's recommendations are to facilitate and anticipate changes in health care service delivery. Existing bargaining units and the resultant trade union representation and collective bargaining relationships are to be realigned for this overriding public interest purpose.
To the extent that this commission is to place the larger public interest ahead of employee wishes -for association, trade union acquired representational rights and employer or union strategic interests in bargaining unit structures, the task of the commission is a departure from the narrower focus that is usually brought to appropriate bargaining unit determination in a contest before the Labour Relations Board between one or several trade unions and an employer.
This departure is reinforced by two aspects of the governing legislation. The first is the mandatory considerations for the commission's recommendations.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
1
I

HEALTH SECTOR LABOUR RELATIONS COMMISSION
(2) "The commissioner must consider the following:
(a) the new employment relationships that will be established as a result of restructuring under this Act
(b) the need to promote integration of health care delivery and to enable the development over time of Provincial consistency in terms and conditions of employment
( c) the history of union representation in the health sector"
(3) The commissioner must make recommendations regarding the composition of appropriate bargaining units that would address the considerations set out in subsection (2) and may make other recommendations the commissioner considers appropriate
(6) If there is an agreement between 2 or more trade unions with respect to jurisdiction in the hei;i.lth sector and, in the opinion of the commissioner, the agreement addresses appropriately the considerations set out in subsection (2), the commissioner, after providing an opportunity to be heard for trade unions that may be affected and for the Health Employers' Association of British Columbia, may include the agreement as a recommendation." Health Authorities Act, S. 1 Ll (2), (3) and (6)
The second aspect is granting the commission a wider latitude in creating bargaining unit and representational structures than is given to the Labour Relations Board.
"The recommendations under subsection (3) may include, without limitation, recommendations regarding multi-employer certification and councils of trade unions for the health sector" Health Authorities Act, S. 11.1 ( 4)
The wide range of options available to the commission, the investigatory nature of the commission's mandate and the considerations that the commission must take into account, recognize that the task is to reshape existing bargaining units and structures on a broad industry wide scale.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
2

HEALTH SECTOR LABOUR RELATIONS COMMISSION
This task is unlike applications before the Labour Relations Board where the issue is usually either determining the boundaries for new bargaining units for trade unions seeking to represent previously unorganized employees, or determining the consequences on existing bargaining units and trade union rights when there is an amalgamation of units following employer organizational change because of a change in business or integration of employers in some manner.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
3

. HEALTH SECTOR LABOUR RELATIONS COMMISSION
IN ADVANCE OF THE COMMISSION
"In carrying out this mandate, the Commissioner should work with the affected and interested trade unions and the employer organization, to the extent possible, to achieve and bring forward recommendations that are in the longer term best interests of the health sector and employees working within this sector." (Honourable Dan Miller, Minister of Skills, Training and Labour, January 24, 1994)
Applications to the Labour Relations Board anticipating new organizational structures for health care delivery led the Board to convene a policy hearing to review bargaining unit structure in the health sector. A panel of the chair, two vice-chairs and two members of the Board held hearings from May 16 to 27, 1994 attended by many parties and their lawyers. The Board asked the parties to address ten issues. Five were directed to long term care facilities and the other five had potentially broader implications.
July, 1994 amendments to the Health Authorities Act enabled the appointment of this commission of inquiry into trade union representation and jurisdiction in the health sector in the context of transition to boards and councils under the Act. The appointment was made on January 24, 1995.
The Labour Relations Board has deferred rendering a decision pending the appointment and work of this commission.
In advance of appointing the commission, the Minister of Health appointed Industrial Relations Officer Dave MacKinnon on September 6, 1994 to act as facilitator with the parties. His research, analysis and insight into the issues served as the foundation for the commission's work and enabled the preparation of a work plan that expedited the work of the commission.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
4

HEALTH SECTOR LABOUR RELATIONS COMMISSION
COMMISSION PROCESS AND PARTIES
"The Commission should .structure hearings and meetings with interested parties in a manner which ensures that: (a) there is complete transparency regarding the information used by the Commission and his rationale for all recommendations (b) there is an opportunity for a candid/frank exchange of views between the Commissioner and interested parties regarding the difficult issues raised by Bill 48 i.e. to permit discussions to take place in a problem solving manner as opposed to the more positional/adversarial approach normally required in formal hearings." (Dennis Blatchford on behalf ofB.C. Federation Expanded Health Reform Committee, February 28, 1995)
On appointment, the commission set out to establish a project team and a plan to fulfil the mandate in a timely manner. The commission determined that it should strive to act openly, fairly, impartially, independently, with integrity, respectfully, economically, efficiently, effectively and pragmatically. The process would be a mixture of private meetings with parties to understand their point of view, research and public gatherings. There was neither the time nor the budget to undertake original or extensive directed research. Materials presented to the commission would be available to all.
To keep all parties informed of the issues being considered and the activities of the commission, a newsletter was prepared and periodically distributed by fax. At ~he request of the Minister of Skills, Training and Labour, interim progress statements were delivered on February28 and April 28, 1995.
The stages and timeline of the commission's work were as follows:
1. Appointment January 24, 1995
2. Recruit team and open office February 1, 1995
3. First meeting with all parties February 3, 1995
4. Ministry ofHeaithpresents detailed transition plan February 25, 1995
5.
6.
First progress statement February 28, 1995
Conclude first round of consultation April 1, 1995
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
5

HEALTH SECTOR LABOUR RELATIONS COMMISSION
7. Second progress statement April 28, 1995
8. Conclude public meetings to receive submissions April 28, 1995
9. Conclude research May 1, 1995
10. Present proposed recommendations May 24, 1995
11. Consult on proposed recommendations and finalize June 30, 1995
12. Close commission office July 13, 1995
13. Termination of commission September 28, 1995
The commission has been constantly aware that the process is an extraordinary substitute for both administrative tribunal and direct legislative decision making. One commission goal has been to fulfil the mandate with the overall least invasive treading on established bargaining rights.
The state can always dictate and .expropriate through legislation within its constitutional authority. Before it does so, it can seek consent or permission from its citizenry. The commission's processes sought consent or permission from potentially affected unions and the employers' organization, knowing that some could never give either to outcomes that took away or diminished their members or their acquired rights.
Trade unions are not emanations of the state or industry. While they may make political alliances for social gains for their members, they are autonomous organizations with distinct cultural and philosophical identities which speak with fiercely independent voices for the workers they represent.
The task of having trade unions relinquish or submerge their hard earned and jealously guarded bargaining rights for the greater public good, as determined by the state, is daunting. While the state has given itself the authority to eliminate or otherwise impact these rights, it should be certain that it is doing so for good reason and with proportionate impact.
(
The unions are understandably suspicious. The motivation behind the forced change is not industrial instability or some other labour relations crisis. It is a long term public interest goal and a health care services affordability crisis.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
6

HEALTH SECTOR LABOUR RELATIONS COMMISSION
The unions suspect that the focus on cost effectiveness invites all managerial decision makers to_ examine contracting out to nonunion suppliers or entering into joint ventures, alliances and other arrangements in which the entire chain of costs leading to acceptable pricing is contained and controlled. Even though labour and knowledge resources are the greatest asset in the system, they are also the highest cost in the system. It is an understandable union concern that cheaper labour may be the vehicle by which some will seek to achieve the desired cost containment.
The highly centralized employer structures for collective bargaining that have been put in place mean that the employer bargaining agent, Health Employers Association of British Columbia, will earnestly take cost containment and reduction issues to the bargaining table. The unions will be asked to help maintain the viability of the public delivery of health services by assisting in eliminating redundancy, improving efficiency and enabling health services to move where they can be delivered most cost effectively without compromising quality.
The unions will be asked to make this commitment despite the disparate impacts it will have on differing groups of employees; may not impact on others benefiting from the expenditure of public resources, such as fee for service providers; and in the face of the threat that some decision makers will favour cheaper labour, which may be nonunion labour, as the most expeditious route to cost containment and cost reduction.
This realistic appraisal of what lies ahead has challenged the unions to question why they should participate in a process that can adversely affect some, diminish the bargaining leverage of others and provide the employer with the forums to more effectively attain its cost goals at the expense of employees.
This background required that the process fashioned for the . commission's inquiry and recommendations be sensitive to the ability of the unions to refuse to participate and their understandable distrust and suspicion of the government's intent to modify or expropriate their bargaining rights.
Counting the two IW A locals as separate unions, the 18 CUPE locals as one union and not including an ICTU local, there were 19 trade unions with rights that may be directly affected. A twentieth union was certified for the first time on June 9, 1995 as the Commission was concluding its work.
Not all of them are affiliates of the B.C. Federation of Labour, which had established an Expanded Health Reform Committee in advance of the appointment of the commission for all affected trade
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
7

HEALTH SECTOR LABOUR RELATIONS COMMISSION
unions to consider the issues which were to become the work of the commission. Until the appointment of the commission, not all of the unions were participating or had elected or staff persons assigned to work on the issues. Shortly after the appointment of the commission, all unions assigned persons to deal with the commission and to establish ways to participate in the process.
In addition, the commission learned that there are 24 employee associations with whom members of the Health Employers Association of British Columbia have agreements referred to as collective agreements. None had been certified or determined to be a trade union. Each was notified of the commission's work and asked if it considered itself to be trade union. One was unsure. Six replied that they are not trade unions. One said that it was. The commission requested that the Labour Relations Board make that determination. On June 23 the Board determined that the association in question was not a trade union.
Identifying the employer spokesperson was as simple as making contact with the Health Employers Association of British Columbia.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
8

HEALT~ SECTOR LABOUR RELATIONS COMMISSION
PUBLIC SECTOR COLLECTIVE BARGAINING REFORM
"The health care system in BC is currently undergoing significant change as a result of the implementation of the recommendations of the Royal Commission on Health Care and Costs. Furthermore, the system continues to be constrained by increasing costs and public demands for health care in an era of economic restraint. Given these conditions, and the crucial nature of the services provided by the sector, it is absolutely necessary that human resource matters are managed in such a way so as to enable an efficient and effective provision of services. At the same time we must ensure that health care providers are treated fairly and equitably. The commission was asked specifically by the Minister of Health to review how to best manage all human resource matters in the sector and to include an examination of labour adjustment in its report.
In its interim report, the commission concluded that the best way to create the structural reform necessary in the health sector would be through the creation of a single employer organization in health care responsible for coordinating all human resource and labour relations matters in the province.
The issues that emerged from the consultations with the health care sector as the most urgent were those of administrative waste, compensation inequities, and the duplication of functions. One of the major impediments to addressing these problems has been the absence of a coordinated approach to human resource management across the entire health care sector." (The Report of the Commission oflnquiry into the Public Service and Public Sector, Final Report Vol. 2 (1993) pp. Dl and D3)
Direct and indirect labour costs in the public sector, including employees engaged in the delivery of health care, constitute almost 60% of the provincial budget. For many of the same public policy goals of attaining effective utilization of resources and the best outcomes that were recommended in 1991 by the Royal Commission on Health Care and Costs, the government struck a Commission of Inquiry Into the Public Service and the Public Sector in March 1992. One of the terms of reference related to public sector collective bargaining structures. Commissioner Judi Korbin made an interim report in December, 1992 and a final report in June, 1993.
Its recommendations led to the establishment of the Public Sector Employers' Council and to the creation of the Health Employers Association of British Columbia in December, 1993 as the exclusive bargaining agent for employers in the health sector. Membership in HEABC is mandatory on criteria developed by the Public Sector Employers' Council and includes employers in all service subsectors, including for shareholder profit employers. Its board of directors includes three government appointees from among the public service as well as representatives of member employers.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
9

· HEALTH SECTOR LABOUR RELATIONS COMMISSION
HEALTH CARE REFORM
"Mastering health policy imposes one of the steepest learning curves imaginable. We know of no other policy area more complex than health and its relationship to health care .. And we know of no system more complex to comprehend than the intricate inner workings of health care financing and health care delivery." (Michael Rachlis and Carol Kushner, Strong Medicine: How to Save Canada's Health Care System, (1994) Harper Collins, p.344)
Health care reform initiatives in B.C., under the 1993 New Directions For A Healthy British Columbia, are intended to effect social objectives that were generally identified in the 1992 Royal Commission Report on Health Care and Costs, Closer To Home. The Royal Commission report and this subsequent government policy agenda have a foundational goal of attaining healthier citizens and healthier communities in B.C.
The Royal Commission proposed an extensive overhaul of health care. It recommended a reduction in the number of acute care beds; a shift of services into the community; redistributing rather than increasing funding; and decentralizing health care administration to regional decision makers. The constant theme is public participation in health care policy planning and decision making.
Starting with the premise that the health status of our community is much more than the negative absence of illness, the New Directions are toward improvement bf illness prevention and enhanced quality of life, as well as more effective curative treatments.
The general directions are assurance of equality in access to health services; greater inclusiveness in the decision making processes that decide priorities, resources allocation and service direction; objective, fact based, and not just peer, assessment of the efficiency and effectiveness of services, treatment and resource allocation; and an overall coherent, logical structure within which an integrated, provincial health care system can efficiently and effectively operate.
The government's policy agenda sets action priorities in attaining better health; greater public participation and responsibility; bringing health care closer to home; respecting the care provider; and establishing effective management of the new health system.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
10
.1

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Much of the beginning phase of the change process is devoted to creating the overall structure that will serve and facilitate health outcome and resource utilization goals. The wrong organizational and operational structures can impede and frustrate the goals. The right structures can facilitate and assist in effecting the goals.
At the local community level, the intent is to reduce duplication of services and its attendant competition for limited public resources. Consolidation of services through integration and coordination at the community level is directed to achieving the highest possible health return for the shrinking available dollars.
Elimination of duplication and consolidation is directed at enabling the community to see and choose where the best outcomes are attained and what are to be the priority services. The desire is to have resource allocation that is price/outcome, and not cost, driven.
Costs led by pricing cannot continue to be practised, as it has been, when the price is continually escalating. There is a need to move to more cost driven pricing for goods and services in the health system and a broader range of controls and decision making to that end all the way from system design to service delivery.
"In publicly funded health care systems such as Canada's, where. a consumer price system is not used to determine the overall size of the system, management of the system's capacity to produce health care services and management of the cost of inputs is tantamount to management of total health care costs. Say's Law [economist Jean-Baptiste Say - 1767-1832], which posits that 'supply creates its own demand,' drives health care system costs when needs are ill-defined, the effectiveness of alternative treatments is difficult to measure, evidence of comparative costeffectiveness is scarce, and the propensity to utilize service is governed by the degree of convenience to patients tempered by micro-rationing decisions of health care providers. In such systems, the increased capacity to provide health care services results in increased utilization at both the extensive and intensive boundaries of health care needs." (Murray G. Brown, "Rationing Health Care in Canada"(l993), 2 Annals of Health Law 101 at p. 113)
The creation of a structure that will facilitate inclusive local decision making, cost containment, shifts towards community based services and the new directions requires substantial change across the entire spectrum of health care organizations. The roles of municipalities and the provincial government, through its various ministries and agencies, in community health care are being ·redefined.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
11

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Autonomous health care organizations are to be integrated into an overall system directed by community planning. Many publicly funded and supported organizations are to be amalgamated or required to cooperate with others in planning and service delivery. Decisions are being made about how far to go in compelling change within autonomous organizations established to service a specific population as defined by disease, age, disability, religion, ethnic origin and so on.
All of these decisions have consequences for those who have voluntarily served and strived to establish organizations, maintain their viability and fulfil their mandate. The decisions have consequences for those who depend upon the organjzations for a profit, a salary and a future career. They have consequences for the organizations that represent the health care providers who will be impacted by organizational, service and operational changes.
The July, 1993 Health Authorities Act is the vehicle by which the government established the transitional phase for the initial organizational changes to effect the New Directions. It "creates the first stage in the establishment of regional health boards and community health councils across British Columbia." (s. 2)
As the changes began to take effect and were more broadly anticipated, the government saw the need in 1994 to address the impact of the changes and the New Directions on trade union representation and jurisdiction among health care workers across the province·.
It had already anticipated that restructuring creates a need for worker mobility and a labour adjustment strategy to facilitate redeployment and retraining of dislocated workers. It negotiated with the HEU, BCNU and HSA a Framework Agreement on March 12, 1993 known as the Health Accord . This agreement was later extended beyond the original group of HLRA employer members to those represented by CCERA and PRICARE.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
12
-,.-1

BCNU
UPN
PEA
BCGEU
INCONGRUENCE OF HEALTH BARGAINING UNIT STRUCTURES
Ministry of Health and Public Agencies
~ RNs 1,880 I --------------------
RPNsn1
Paramedical I Professionals 168
Other Paramedical Professionals 560
--------------------
Health Services and Support
2,935
6,264
c::D
BCNU I
HSA
HEU/ BCGEU/
CUPE/ IUOE/ etc.
c::D
Health Sector
RNs 24,890 I
Paramedical Professionals
9,851
---------~-~-~-----
Health Services and Support
53,368
88,449
Chart 2
Municipal Government
BCNU I RNs 925
~
CUPE/ VMREU/
HSA
~
Paramedical Professionals
211
~--------------------
Health Services and Support
833
1,969
-~

I !
HEALTH SECTOR LABOUR RELATIONS COMMISSION
APPROPRIATE BARGAINING UNIT RESHAPING
"The internal labour force in the health sector is intricate and multifaceted. Employees range from highly skilled to unskilled. There is also a large array of specialist professions, semiprofessions and occupations, e.g. doctors, nurses, technologists, and therapists of all descriptions, with their own associations, vying for power, influence, and remuneration in the medical division of labour. Many of these groups are represented not only by professional associations but by trade unions as well. Separate 'community of interest' provide for a proliferation of bargaining units into which these groups can be organized." (Larry Haivan, "Industrial Relations in Health Care: Regulation, Conflict and Transition to the 'Wellness Model"' in Swimmer and Thompson, ed., Public Sector Collective Bargaining in Canada: Beginning of the End or End of the Beginning? (1995) IRC Press, Queen's University, p.236)
Bargaining unit reshaping is the final major phase of the organizational restructuring in this initial preparation for substantive health care reform.
Reshaping bargaining units and the consequent collective bargaining relationships is an entirely different issue than reorganizing government departments and agencies, statutory hospital boards and societies dependant on government funding.
Grounded in employee choice and continuing support, the foundational representational structure for union legitimacy, rights and jurisdiction is the bargaining unit. This is the constituency of employees who choose union representation and for whom the union acts. Over time its boundaries may grow or shrink. Several units may be combined to form a broader base for the application of collective agreements to many operational locations of one or more employers either by union and
. employer agreement or, with more frequency recently in Canada, by labour relations board consolidation.
In the absence of legislative and administrative tribunal definition, a bargaining unit may take any shape or size that a trade union and one or more employers may agree. Before the enactment of legislation regulating collective bargaining rights and their acquisition, bargaining unit composition and scope could be the subject of a recognition dispute between the union and employer.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
13

HEALTH SECTOR LABOUR RELATIONS COMMISSION
With the advent of collective bargaining legislation, the unit in which there is a grouping of one or more employees must be "appropriate" for collective bargaining. It may be a craft unit, technical unit, plant unit, employer unit or another unit "whether or not the employees in it are employed by one or more employers." (Labour Relations Code, s.1(1) "unit")
For almost fifty years, the important determinations about the appropriateness of proposed units have not been made through economic conflict between the union and employer, but by labour relations boards.
The appropriate bargaining unit supports the statutory, exclusive, representational rights of the trade union as bargaining agent. It is also the public policy tool that addresses the competing interests of employee wishes, self imposed trade union membership limitations, employer operational needs and public social order concerns.
Over the five decades of collective bargaining legislation, an appropriate bargaining unit has been legislatively defined at various times to be a minimum group of two or more employees or just one employee. The scope of the definition of employee, and therefore access to legislatively sanctioned collective bargaining, has evolved.
Social attitudes about collective action and trade union represen~ation have also changed. As a consequence, new occupational groups and their trade or professional associations and, later, trade unions have asserted representational rights.
Extension of collective bargaining rights to provincial government employees followed the establishment of those rights in hospitals, municipalities and non-government employers. New trade unions emerged to represent each of these employee groups.
The administrative decisions by labour relations boards about appropriateness have evolved and changed with the craft, industrial, technical, professional and other basis of trade union philosophies, structures and organizing efforts. Over the years, labour relations tribunals have been more or less supportive of craft, industrial, technical, professional and other sorts of bargaining units. The decision making has almost always been on a case by case basis with any change in approach operating prospectively, but not changing established units unless they become the subject of a specific proceeding.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
14
---------------- .. -,,

HEALTH SECTOR LABOUR RELATIONS COMMISSION
The determination of appropriate bargaining units has also been consciously influenced by whether the request for determining the unit is to enable employee access to collective representation at the · time of initial organizing; to consolidate established units for ease of administration; to alter or clearly define the employee constituency for purposes of an application for decertification or to change bargaining agents; or to further some collective bargaining goal.
The appropriate bargaining unit has, in turn, been the basis for asserting and negotiating exclusive work jurisdiction for one group of employees or another as unions seek to gain and maximize labour market security for those they represent.
Fifty years after the first collective bargaining legislation and the first union certifications for exclusive bargaining rights for a unit found to be appropriate, the unit boundaries in any industry can be a patchwork quilt. With varying degrees of success, inter-union processes exist to resolve boundary and work jurisdictional disputes between unions.
Labour relations board processes to clarify or redefine units are invoked by unions, employers and employees to record organizational changes, to achieve changes that address the emergence of new occupations or gain advantages that are seen as desirable by the initiator of the process
Labour relations boards have sought to contain the proliferation of units. In the health sector, a 1970's decision limited bargaining units in hospitals. (Kelowna Hospital Society [1977] 2 Can LRBR 58) When a situation presents itself, the board has said that it will actively reconstruct units to reduce fragmentation. (Island Medical Laboratories Ltd (1993), 19 CLRBR (2d) 161)
There are 888 bargaining units that form the basis for the representational rights of the 38 trade unions holding Labour Relations Board certified bargaining rights in the B.C. health sector. The debates over the decades about the boundaries of these units and trade union jurisdiction reflect all aspects of trade union, legislative and administrative bargaining unit policy, its evolution and disparate, often competing, philosophies and approaches to the representation of employees.
This commission is the means to review, revise and reshape bargaining units because of the imminent changes in health care management structures and the anticipated affordability crunch in health care. The work of the commission is a specially designed approach outside the legislature and apart from the adjudicative processes of the Labour Relations Board.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
15

HEALTH SECTOR LABOUR RELATIONS COMMISSION
ORGANIZATION OF HEALTH CARE WORK
11 ••• exclusive scopes of practice should be narrowed to focus on preventing harm, as has
been initiated recently in Ontario. We believe that more cost-effective and timely health care could be provided to more patients if BC were to follow the Ontario initiative .
. . . it is important to examine the existing scope of practice of the health care professions before granting any more. To do otherwise would further complicate an already complicated patchwork of prohibitions and exemptions. 11 (Closer to Home, The Report of the British Columbia Royal Commission on Health Care and Costs (1991) Vol. 2, p. D-33)
Broadly speaking there is a dizzying array of occupations in health care clustered around two general cultures vying for recognition, influence and compensation in the division of labour and resources. The occupations range from the highly skilled to the unskilled.
There is a potpourri of specialists granted degrees of exclusive or qualified scope of practice. They, and those seeking similar status, clothe themselves in arguments based on the threat to quality of care and the dire consequences that will follow from having someone else do the work that they have
' done. The fiercest debates are among those who have or are seeking access to the right to diagnose and treat. All groups are aided in advancing their interests by health industry manufacturers and suppliers of pharmaceutical, diagnostic and other goods and services which benefit from the advancement of the group interest. ·
The two broad cultures are, first, the medical model culture that we have embraced in recent decades and that has been generously supported by universal Medicare and, secondly, a community health culture that sees the determinants of health as much broader than physical health services dominated by physicians, hospitals and technology.
The community health culture sees health as more than the absence of disease. Its view is captured by such definitions of health as that of the 1984 World Health Organization (European Region), adopted by the New Direction policy agenda: "The extent to which an individual or group is able, on the one hand to develop aspirations and satisfy needs; and, on the other hand, to change or cope with the environment. Health is therefore seen as a resources for everyday life, not the objective of living; it is seen as a positive concept emphasizing social and personal resources, as well as physical capacities." Or that of Pericles (495-429 B.C.): "Health is a state of moral, mental, and physical well being which enables a person to face any crisis in life with the utmost grace and facility. II
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
16
. --,-.

. HEALTH SECTOR LABOUR RELATIONS COMMISSION
The two differing foci, absence of physical disease and resources for daily living - sickness or wellness - vie for attention, priority, influence and money in the highly competitive environment of public health care resource allocation.
The organization of work differs in the environments where these cultures predominate. The medical model culture is rigidly hierarchical with doctors, hospitals, nurses, drugs and technology critically central to the care of the sick and injured. The "patient" is more passive than active in the process. The emphasis is on treating and curing. The division of labour is along lines supported by credentials with authority and responsibility regulated by tradition, licensing authorities, accreditation standards and so on.
In the community care culture or wellness model, the determinants of health are assigned an order of importance - individual and collective wealth, the environment, inherited genetic endowment, individual choice or lifestyle, decisions by governments and others in power able to affect individual lives, and health care. "Consumer" support or caring is the focus. Relationships between care provider and consumer are emphasised. The community care culture is more accepting of the role and importance of the non-physician - chiropractors, midwives, social workers, nurse practitioner, etc. Work is less strictly divided. Regardless of the streams of their education or training, workers may and do perform interchangeable roles.
Our provincial system and resource allocation is heavily weighted in favour of the medical model. This is also where there is the longer history of trade union representation. In those subsectors of the industry where this model predominates, employees have chosen and have been grouped for bargaining unit and trade union representation purposes by occupations on a hierarchical order -residents, nurses, paramedical professionals, health services and support, and maintenance trades.
As you move away from acute and extended care and diagnosis and treatment, into long term care and mental health the number of groupings diminishes and some of the rigidity of the medical model disappears. For example, registered psychiatric nurses are not in the same bargaining unit as registered and licensed graduate nurses in hospitals and extended care facilities. They are in long term care facilities. In some long term care facilities nurses are in the same bargaining unit as other employees.
As you move out of the facilities setting and into the community services - adult daycare, home support, child development centres, drug and alcohol counselling and so on - the number of employees significantly diminishes and the groupings of employees tend to be more integrated.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
17

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Credentials are often based on work or life experience rather than formal educational training. Frequently, one union will represent all employees in one bargaining unit, regardless of occupation or classification. Many employees are represented by trade unions that do not have exclusively a health industry focus - CUPE, BCGEU, UFCW, IWA, USW A. These unions have a municipal or provincial government, community or multi-industry focus.
The New Directions policy agenda, following the lead of the Royal Commission, is toward integration and less rigidity. There is a shift toward a community care culture or wellness model of health. The clear challenge in the workplace will be to face and question the need and limits of work practices, divisions of labour and expectations based on the past credentialization of treatment and care procedures. Change will be difficult. Health worker education and training, established procedures, entrenched work practices and classification structures, collective agreement terms, occupational turf, ingrained attitudes and beliefs, and public expectations and conditioning are only a few of the hurdles.
The expectation is that there will be a shift in focus and resources, including employees, toward integrated service and that the existing hospital, extended and long term care facilities will become more versatile and diverse in their use. The hierarchical medical model culture of work organization will have to interact with, rather thi;tn stand in isolation from, the more integrated community care culture.
The effort, as recommended by the Royal Commission, will be to achieve greater congruence between the skills required to give high quality care and the education, training and credentials of the care provider to whom the task is assigned.
Another feature of the current work organization is the dedication of support, administrative and other services to single sites, programs or organizations. Some are relatively rich in talent and resources. Others are struggling to firid or develop the necessary skills. The result is duplication and inefficiencies.
Whether it is laundry, food preparation, materiel management, procurement, property management, payroll service, administration, preventative and emergency maintenance, pharmaceutical, laboratory or medical records services there are opportunities for one agency or organization to share its physical plant and resource capacity to provide a service to others in the system. Regional planning and management should enable these economies to be identified and implemented through shared services.
RESHAPING B.C. HEALTHSECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
18

HEALTH SECTOR LABOUR RELATIONS COMMISSION
CHANGE AND FUTURE RESOURCE ALLOCATION COMPETITION
"Most people know that health care consumes one quarter to more than one third of all the money spent by provincial governments, and that spending levels have risen steadily for 30 years. Most people know that all provinces are trying very hard to control spending on health care, and many support these efforts.
Health care is only one of the many things which affect our health. If too much is spent on health care there will be less left for all the other things which matter to our health, such as education, safe roads, safe communities and healthy environments. There may not be agreement on how much should be spent on health care, or which health care spending should have highest priority, but there is broad agreement that government spending on health care does need to be controlled." (Ralph Sutherland and Jane Fulton, Spending Smarter and Spending Less (1994) The Health Group, p.1)
The provincial health care system is mainly built around the role of the physician, who is a fee for service care provider receiving fees from Medicare, private insurers, the Insurance Corporation of B.C., the Workers' Compensation Board, litigants and others. Some physicians also own, operate and profit from clinics, the work of employed physicians, laboratories and various private diagnostic and treatment services from which Medicare and other payors purchase goods and services.
Collectively they negotiate their medical fee rates, allowances for costs and the nature and extent of their influence in health care through their mutual advancement/protection and political action organization, the British Columbia Medical Association. The BCMA also negotiates collectively for fee rates and related service remuneration with the WCB, ICBC and other non-Medicare providers. It bargains collectively for salaried physicians with employers such as the WCB. Although never determined to be a trade union by the Labour Relations Board, the BCMA asserted on June 28 that it is a trade union and party to collective agreements covering various groups of physicians employed in the health sector. It says physicians should have a separate bargaining unit.
In their negotiations with the province and others, the physicians make all the usual arguments, threats, public appeals, political manoeuvres and limited withdrawal of services that large interest groups do when negotiating to advance their interests in the public domain. The Royal Commission adjudged this strong physician voice to serve the interests of all British Columbians. It recommended that mandatory financial support of the BCMA be guaranteed through compulsory payment of dues by all physicians, but not compulsory membership, on the basis of the trade union Rand Formula. (Closer To Home, Vol.2, p. D-10)
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
19
~ 1,,I Ii !I I

HEALTH SECTOR LABOUR RELATIONS COMMISSION
During their residency, physicians working toward specialist credentials, are represented by the Professional Association of Residents of B.C. PAR-BC is a trade union holding certification and bargaining rights like any other trade union. Virtually all residents in B.C. are represented by PARBC, which has a single industry-wide collective agreement that covers them regardless of where they work - acute care hospitals, community health facilities, physicians offices.
There are more registered nurses than physicians in B.C. (30, 728 vs. 8,220). Nurses constitute about 28.5% of all unionized employees in the health sector. Unlike most physicians and some other credentialed care givers, nurses are salaried rather than fee for service providers. Like physicians, they have both their professional association (Registered Nurses Association of British Columbia/Registered Psychiatric Nurses of British Columbia and College of Physicians and Surgeons) and their bargaining organization (British Columbia Nurses Union, Union of Psychiatric Nurses and BCMA).
Like physicians, they negotiate collectively for provincial terms and conditions of employment with their main payors or employers. There is one collective agreement covering nurses in the hospitals; one covering nurses in long term care; one with the provincial government covering nurses employed in the public service under the Public Service Labour Relations Act;. and effectively, one for nurses employed in municipal health departments. In large measure, these agreements are very similar in their terms.
As you move way from these two occupations, there are larger numbers of employees and occupations that are more fragmented and less well positioned to be heard and influence. However, they are equally competitive for a larger share of the available health care dollars and influence in the system.
These employees are organized on an enterprise basis and, to varying degrees, negotiate on a provincial, industry, health subsector, single employer or single location basis. The smaller the basis, the further they are away from the public funding source that everyone relies upon.
The result of these structures is 203 collective agreements and negotiations chasing the same resources.
And these resources are shrinking on a per capita basis as the population expands. They will continue to shrink as the federal government reduces transfer payments and as the need and priority for deficit and debt reduction claim available dollars. There will be $375 million less for health care
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
20
-n

\
HEALTH SECTOR LABOUR RELATIONS COMMISSION
in fiscal year 1997/98 coming to the province from the federal government than in 1994/95. The reductions are $16 million in 1995/96, $203 million in 1996/97, and $156 million in 1997/98. The introduction of federal block funding does allow health care costs to expand to maintain the status quo. However, this expansion would be at the expense of other public services.
The foreseeable funding results are seen by some as catastrophic with the health care system imploding and legislated controls replacing collective bargaining. Some see an increase in for profit service providers, user fees, decreased services and blame and cost shifted to persons who are ill, injured and disabled. Some see the largest burden of care shifting from shared community responsibility through taxation and public care providers to family members - in short the women of B.C. Others see an opportunity in the situation to compel resource allocation and priorities decisions on the basis of cost and outcome rather than price and supply.
Throughout the range of opinions, there is a common expectation that there will be greater dependence on individual citizen self reliance and a need for policy choices and funding decisions that more clearly show that various types of services are being rationed. Those macro-rationing decisions at the provincial, regional or community level will influence micro-rationing decisions in physicians' offices, in hospital wards and so on.
"Societies ration health care resources in ways that reflect their own societal values, beliefs, institutions, and history. In pure price-rationing systems, market forces determine who has access to health care services, with rationing detennined by the distribution. of purchasing power. Non-price-rationing systems adopt other entitlement criteria to determine who has access to available health care services while relying on charitable donations or public taxation to fund health care services. Hybrid rationing systems combine non-price entitlement criteria with user co-payment pricing policies.
Decisions that 'ration' health care resources within a publicly funded health care system, such as Canada's, occur at many levels. Rationing at the macro (managerial) level is implicit in government decisions about the overall size of health care budgets and allocations to Medicare and competing health programs. Macro-rationing decisions at each successive level of management set the stage for micro-level rationing decisions involving individual patients and health care providers.
At the macro level, rationing is performed in the abstract: governments allocate scarce resources among competing uses and users. At the micro level, patients and providers are usually unaware of the many macro management decisions that indirectly affect patient/provider behaviours and utilization of Medicare services. Neither patients nor providers show much interest in macro allocation issues when patient access to non-urgent
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
21

HEALTH SECTOR LABOUR RELATIONS COMMISSION
health care services and provider workloads are reasonable. However, in more dramatic cases, micro rationing at the patient/provider level involves highly emotive and value-laden decisions about who gets access to scarce services that may be vitally important to either the length or quality of the patient's life." (Murray G. -Brown, " Rationing Health Care in Canada" (1993), 2 Annals of Health Law 101 at pp. 107-8)
Regardless whether one is pessimistic or sees an opportunity, a situation of limited and shrinking resources accompanied by more difficult and controversial rationing decisions will heighten the will of the more powerful to pursue their interests more vigorously. This wiHnot foster a situation where the compensation inequities across the system can be addressed in a planned and measured fashion.
Integration of services and direct interchange between employees from different past employers will underscore the existing inconsistencies and inequities. To have integration, the inequities among the 203 collective agreements must be addressed.
However, there are insufficient resources to immediately address inequities if it means increasing compensation to the highest common denominator that has resulted from the past negotiations. For this reason, the legislation tells this commission to seek to "promote integration of health care delivery" while enabling the "development over time of Provincial consistency in terms and conditions of employment."
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
22
---~--------~-~- --...-.

HEALTH SECTOR LABOUR RELATIONS COMMISSION
INTEGRATION OF HEALTH CARE DELIVERY
"The Ministry of Health is of the view that these and other powers of the commission should be used to the fullest extent to create the broadest possible bargaining structure. Integration of health care delivery and development of health care consistency in terms and conditions of employment are impossible to achieve within a fragmented collective bargaining and certification base.
In examining the criteria set out in section 11.1 (2) of the Health Authorities Act, we urge the Commissioner to recognize and reflect in his recommendations that the changing employment relationships flowing from restructuring can only be accommodated across a broad collective bargaining and certification base." (Lawrie Mcfarlane, Deputy Minister of Health, February 25, 1995 presentation)
At the heart of the Royal Commission recommendations, the New Directions policy agenda and so much of the national and international health care reform movement is "redistributing" not increasing resources; "shifting" from one type and provider of service to another; and "decentralizing" decision making. It seeks a change in the priorities in the rationing process and a change in who and, therefore, what values and beliefs will guide the rationing.
Among health care providers, credentialization, which the Royal Commission recommended be restrained and reduced in the future, and bargaining competition. have a large part to play in directing resource allocation and, consequently, health care rationing decisions.
If there are to be shifts and redistribution, then system managers must be able to redirect all resources, including health care providers. Barriers to change must be removed and lessened.
This concept is captured in the direction that this commission consider "the need to promote integration of health care delivery."
"Integration" is the shorthand for seamless service across the continuum of care that will allow the citizen to receive the level of quality care required from the appropriately trained and experienced care provider in the most cost effective setting. To achieve seamless service the system must allow ease of mobility of both citizen and health care provider.
Hospitals may become wall-less so that hospital based workers can give post-operative or other care following a brief stay in the hospital outside its walls in a community health centre, long term care
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
23

HEALTH SECTOR LABOUR RELATIONS COMMISSION
facility or through home support. Community services must be available within the walls of hospitals where beds have been closed and space is available. These large expensive modem cathedrals within our communities will become more multi-purpose community resources.
Long term care facilities are becoming multi-level care centres as the acuity of their "residents" rises with shortened "patient" stays and rising acuity in hospitals. They are opening their doors and programs to "clients" who live in their own home but require support through adult day care or some other service. Community clients come to the facility and share services, support and friendship with its residents.
Integration means that health services and support workers will provide services and support beyond the site to which they are attached. For example, meals on wheels may be prepared in hospital kitchens. The focus can be the community or region or province when the services are administrative, information, accounting, planning, budgeting, purchasing, medical records, personnel and labour relations, communication and public education, laundry, food preparation, preventive and emergency maintenance, and so on. It can be beyond a single service subsector such as acute, extended, long term care, drug and alcohol, mental health, adult day care, child development, home support and so on.
Boundaries generated by funding policies, credentials creating exclusive areas of practice, professional rivalries and other turf issues, trade union representation and jurisdiction, bargaining unit boundaries and so on, all create present or potential interruptions or breaks in seamless service. Each requires some bridge that, in tum, requires resources (money, people and time) to build and maintain - sometimes until no one clearly remembers why it was constructed in the first place.
Bargaining unit boundaries encircling groups of employees, create turf and invite employees, employers, managers and union representatives to jockey to be on one side or the other of them for some reason in one situation or other and to distinguish why one side is appropriate in one situation and the opposite side in another situation.
Removing barriers enables integration. Reducing the number of bargaining units removes barriers. Promoting integration for this commission means reducing the number of bargaining units, which is what the Royal Commission recommended. Reducing the number of bargaining units will also mean a reduction in the incidence of collective bargaining and the number of collective agreements in the industry being funded by health care resources.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
24

HEALTH SECTOR LABOUR RELATIONS COMMISSION
PROVINCIAL CONSISTENCY OVER TIME
"Doctors may exert the most influence over our health care system, and the costs it generates, but they aren't the only players in the field. A host of other providers from as many as 40 occupational groups are constantly jockeying for position." (Michael Rachlis and Carol Kushner, Second Opinion, 1994 Harper Collins, p.43)
Collective bargaining, dependent upon funding allocations to different subsectors of health care, has produced different and inequitable results in terms and conditions of employment for health care providers doing the same or similar work in the province. These differences also act as barriers to integration.
As a community, we cannot afford to move to provincial consistency if it is to be the highest set of terms and conditions of employment. As a society, we have not been able to decide that we should reallocate from those who receive the most from the available funds - physicians, pharmacists, suppliers, nurses, paramedical professionals, hospital administrators, hospital health services and support workers - and give it to care providers in mental health, home support, social and other services.
One result is that this commission is to seek to enable the development over time of provincial consistency in terms and conditions of employment.
Fewer and broader based bargaining units will bring more of the disparate situations to the.same set of negotiations and decision making. This will, at least, enable the parties to those negotiations to make decisions on resource allocation that place a priority on addressing inequities and removing barriers to integration ahead of meeting the aspirations of those who have achieved the superior benefits because of their preferred or critical place in the system, the sheer volume of their voice or· their influence in the system. Their continued gains maintain inconsistency.
A reduction in the number of bargaining units will not directly address the government allocation decisions among unionized wage earners, nonunion workers, management, physicians, other fee for service providers, suppliers and others.
r-·--------
RESHAPING B.C. HEAL TH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
25

HEALTH SECTOR LABOUR RELATIONS COMMISSION
The economic realities of shrinking resources for health care dictate that negotiators firmly address. demands and that the parties to collective bargaining, including the provincial funder, move toward affordable standardization or commonality in a measured fashion. We simply cannot afford to jump to consistency on the basis of the highest terms and conditions of employment.
HEABC presented that a reasonable time line for achieving provincial consistency is seven or so years. That is two to three rounds of bargaining.
Maintaining several subsector based bargaining units, as some represent to the commission, may delay achieving consistency. It will also be a barrier to integration.
Some urge unit boundaries which fence in the collective agreements and unions with higher terms to avoid their migration into the lower paid areas. They fear the prospect of making the powerful more powerful - especially the Hospital Employees' Union - by increasing their base. Seldom do they represent the same solution for the nurses or paramedical professionals, who also have powerful bases in the system.
These powerful bases currently exist. Excluding them from participation in how consistency is to be achieved, denies the possibility that they contribute to that goal by having some responsibility for representing the employees who currently have the lesser terms.and conditions of employment at the same time as they bargaining for those who have the superior terms and conditions of employment.
One real life situation that we confront is significant fiscal pressure on the government; demands for deficit and debt reduction; no ability to increase taxes; and reduced transfer payments from the federal government. When 1 % of the wage bill is $27 million, a $375 million cut is most significant.
The Public Sector Employers' Council presented that within the health wage earning groups, the high group receives $310 million of the wages. The typical group receives $2.055 billion. The low paid group receives $262 million. By comparison the low paid group in social services is much larger with $485 million of a smaller budget going to them. While the commission's focus must be toward consistency within the sector, the fact of inter,..sectoral inconsistency must not be forgotten, especially when the distinctions between what constitutes some health or social services are not easily determined. An example is child development centres providing the same service in both sectors.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
26
~~~------,,,,---"I

HEALTH SECTOR LABOUR RELATIONS COMMISSION
"A society that spends so much on health care that it cannot or will not spend adequately on other health enhancing activities may actually be reducing the health of its population" (R.G. Evans and G.L. Stodart, "Producing Health, Consuming Health Care" in Evans, Barer and Marmor, ed. Why Are Some People Healthy and Others Not? The Determinants of Health of Populations (1994) Aldine de Gruyter at p. 55)
Collective bargaining with data scrutinized by spirited advocacy between strong, well informed opposing forces is the best vehicle for finding the balance that moves toward provincial consistency while maintaining a viable public health system within our fiscal limitations.
In the short term, during the transition to the reshaped bargaining units and upcoming collective bargaining, maintaining existing collective agreements until their expiry term will delay attaining consistency.
Provincial consistency in terms and conditions of employment and integration of health care delivery are interrelated; In many respects, each is needed to achieve the other or each is. the price that a bargaining party must pay to achieve the other.
Each party emphasizes the dire consequences of too much consistency too soon or . too much integration before consistency. Using the acute care wage and benefit structure the cost of moving to that level is variously guessed to be $400 to $800 million p~r year at today's costs, more if there were increases in acute as a result of pay equity adjustments or general increases.
Everyone accepts that no one has a credible estimate. But the interim guesses demonstrate the enormous challenge ahead, and that achieving it must necessarily be a protracted exercise.
There are options. Consistency can be achieved in a planned fashion by legislative action. We have seen public sector wage guidelines in recent decades.
But the choice is to support collective bargaining, through bargaining unit reshaping, as the preferred decision making process. It has the best potential for unions and employers to shape compromises that accommodate their competing and common interests in the context of health care restructuring.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
27

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Collective bargaining is not a perfect decision making process. Many of the current problems, for example wage and benefit inequities, or agreement provisions limiting flexibility without being necessary to preserve job opportunities or security, are the result of collective bargaining. Its efficacy in this sector has been challenged in light of the history of disputes, settlements and the perceived convergence of interests of unions and public sector management in a highly political setting.
The new period of government seeking to manage demand for services by limiting supply and of public sector employer coordination and partnership with government challenges HEABC to take a different path than its predecessors.
It has the resources, legal authority, connection to government and mandate to take leadership. It has for profit members whose beliefs, values, style and entrepreneurial spirit must be reflected at the bargaining table.
Regardless of the judgment about collective bargaining in the health sector in the past fifteen years, the parties under a centralized bargaining unit structure are neither helpless, nor incapable of using collective bargaining to strike the appropriate balance between integration and consistency over time.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
28
----------- ~----------- -YI

LEGEND
AC Acute Care LT Long Term Care HS Home Support EC Extended Care MoH Ministry of Health MG Municipal Gov't R Riverview MH Mental Health RC Red Cross D& T Diagnotic &
Treatment D&A Drug & Alcohol CDC Child Dvlpmt
Centre CS Community
Services ADC Adult Day Care
60000
50000
40000 "' ~ l-o 30000 u Q)
"' .c ~ 20000
10000
----- ------------
Unionized Employees By Health Subsector
0-"--.------.-~,----,---,~-.-----.~-.---,-~-,------.-~..------.---.~
AC LT HS EC MoH MG R MH RC D&TD&ACDC CS ADC Subsector
Chart 3

HEALTH SECTOR LABOUR RELATIONS COMMISSION
HISTORY OF UNION REPRESENTATION
"Decision making by majority choice is an accepted tenet of democratic society, but not all organizations in a democratic community decide by majority choice. Although employers in virtually all private sector enterprises and most publicly sponsored institutions make decisions by various means ranging from autocracy to committee consensus, they are an accepted part of a democratic society. Why then is majority rule required for trade unions?
There are different social expectations about the behaviour of trade unions. They are not profit-motivated entities. They are organizations intended and accepted for the purpose of expressing and implementing the principle of freedom of association, through which employees may strive for objectives of social justice for themselves and fellow employees. Trade unions are expected not to be autocratic or dictatorial, no matter how efficient these forms of decision making may be. They are expected to reflect in themselves the principles of the social order they seek to achieve.
In the 1980's Canadian trade unions confront challenges from a vast array of baffling forces: an unsettling economic climate, post-war baby boom expectations and frustrations, polarizing opinions about public sector collective bargaining, a drastically changing work force demography, a rising wave of conservatism and rapidly advancing technology. All of these forces will tug at the political fibre of the country. One of the binding forces of that fibre is the freedom to associate which is manifested in our trade unions. For their role to be maintained and strengthened they must be seen as the organs of democracy they are." (James E. Dorsey, "Individuals and Internal Union Affairs: The Right to Participate", Swan & Swinton, ed. Studies in Labour Law, (1983) Butterworths, p. 193 at 196 and 220)
· The history of trade union representation in the health sector can be assessed as a matter of longevity, quality of representation, pattern of growth or stagnation, breadth of representation in various subsectors, percentage of unionized employees in a service subsector or occupation or of all
. unionized employees, or record of workplace and social achievement.
Some of the smallest, like the four craft unions at the Royal Jubilee Hospital, have almost the greatest longevity. Some, like CUPE, have longevity and multi-sector and occupational representation. Some narrowly focused unions, like UPN and IUOE, have a lengthy history in several sectors and all or most of their members employed in health care, but they are small in the overall scheme of the health sector.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
29

HEALTH SECTOR LABOUR RELATIONS COMMISSION
This consideration directs that the commission's recommendations are not to be based on size alone within or without the health sector, but respect the organizational attachment of the union to the health sector.
Unions which have organized the unorganized, like the UFCW in home support, deserve to have value placed on that history of representation even if it is relatively recent. Unions that have organized in other sectors, like the IUOE in long term care, after it was frozen by the labour relations board in the acute sector deserve to have its majority health care membership respected. Its continuance in acute care is a result of the Labour Relations Board creating for it an exception to acute care bargaining unit structures for "compelling historical reasons." (Kelowna Hospital Society [1977]
12 Can LRBR 58 a,t p. 61]
This commission's recommendations should not threaten the continued existence of a trade union, even if its representation of health care workers is small in the larger picture. No union's history of representation should be discounted or demeaned. The nature of a union's history of representation in the health sector directs the extent to which measures must be taken to accommodate its continued representation in the health sector.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
30

HEALTH SECTOR LABOUR RELATIONS COMMISSION
PROVINCE WIDE, MULTI-EMPLOYER UNITS RECOMMENDED
"If the Health Ministry were operating with a blank sheet, without the weight of history and the specific provisions of the Health Authorities Act, our task would be simple - one bargaining unit and one trade union." (Lawrie Mcfarlane, Deputy Minister of Health, February 25, 1995)
Even with a blank piece of paper, one bargaining unit represented by one union is not necessarily the optimum solution. Some of the disparate interests at this stage of the evolution of the industry are too divergent to be addressed in one set' of collective bargaining.
The commission publicized a proposed recommended optimum bargaining unit structure on May 24, 1995. Since then the commission has had the benefit of many hours of representation from many potentially affected parties on the advantages and disadvantages of the proposal as it affected them or health care service delivery generally. The final commission recommendations are a modification of that proposal.
Generally, the commission has concluded that the bargaining unit structure which will enable integration of services and facilitate greater efficiency and effectiveness is province wide and multiemployer bargaining units. To varying degrees, some of the larger unions are already in this position for the employees that they represent.
Like the situation of most physicians, there will continue to be major payors/employers still outside the structure - Ministry of Health, Ambulance Service, Forensic Psychiatric Services, Centre For Disease Control. The purely private, not taxpayer funded, dollars will be outside. Mixed funded employers who are members of HEABC will be included whether they raise money through house lotteries, auctions, telethons, denominational community support, provision of services to WCB, ICBC, the federal government, private insurers, out of country patients or other sources.
The multi-employer base for each bargaining unit is the same. It is all current and future members of HEABC. This includes employers who will cease to exist because of amalgamation; some who do not yet employ employees, like regional health boards and community health councils; some who will continue to exist because they are denominational employers and covered by the master agreement between the province and The Denominational Health Care Facilities Association; some who employ employees in other sectors and will have collective agreements with other unions for other employees outside the health sector; societies which finance other social purpose aims out of
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
31

. HEALTH SECTOR LABOUR RELATIONS COMMISSION
surplus or non-shareholder profit from health care funded services; and companies, partnerships, proprietorships and other entities that are in the health care business for shareholder or personal profit.
The key to membership in this group is voluntary or mandatory membership in HEABC as a result of the Public Sector Employers' Act and its administration. By virtue of this statute, HEABC is the exclusive bargaining agent for collective bargaining purposes for its members.
This multi-employer group speaks with one voice through HEABC. It is mandated to reconcile the competing interests among its membership. Segregating its employer members into various groups would likely make it easier for HEABC to respond to and advance the interests of its groups. At the same time, it would accentuate their differences and not emphasize their common interests and the public's interest in their integration of service and establishment of provincial consistency in terms and conditions of employment.
All publicly funded entities delivering health care services strive to have financial surpluses at the end of their fiscal years to make improvements, finance the future or increase shareholder return. When revenues are less than planned, they must find ways to reduce costs or to finance or generate the difference. With shrinking public resources this has been, is and will be an ever increasing challenge for all managers.
Including for shareholder profit and not for shareholder profit employers in the same multi-employer bargaining unit is highly unusual, if not unique. So is the publicly funded Canadian health care system with its provincial, and now more sub-provincial, planning and policy decision making; government mental health institutions and social sector public hospitals; social sector service delivery agencies; and for profit services.
The same public policy goals that include the employers under the public sector umbrella of the Public Sector Employers' Act and compel their membership in HEABC direct the inclusion of their employees in the same bargaining unit as the employees of other employers competing for the same public resources.
The crux of the concern about inclusion expressed by the for profit employers is twofold. First, that they will not have adequate voice and control within the internal HEABC decision making processes. This is the same concern expressed by groups of employees who do not wish to be included with larger or any other group because they lose their autonomy or their influence
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
32
---~~------~----.I

HEALTH SECTOR LABOUR RELATIONS COMMISSION
diminishes. Procedures and mechanisms can be developed within HEABC so that decision making processes are responsive to the special needs of all of its members with all of their many special concerns. (As an employers' organization HEABC has a statutory duty not to act arbitrarily, discriminatory or in bad faith in representing any of the employers.)
If this cannot be done then, the wisdom of the underlying policy to have them included in HEABC may have to be revisited. If there is a future change, the Labour Relations Board can apply successorship and other legislation to create employer, enterprise or single location units.
Collective bargaining in the health sector is criticized for its record of work stoppages, third party resolution of disputes, some of the outcomes, confrontational culture in some quarters and the locked step relationship between union gains and most managerial terms and conditions of employment. Entrepreneurial voices in the employer mix within HEABC should not be segregated out if there is to be change. Their voices should be heard and added to the other managerial voices if collective bargaining is to meet fully the challenges of public sector organizational and care delivery restructuring.
Second, the for profit employers say that are not treated equitably under the existing funding policies and fear that funding will not be made available for any future costs. HEABC and all of its members will have to listen to these concerns as HEABC develops its collective bargaining goals and strategy and undertakes negotiations. Those setting funding policy will have to listen to and assess these concerns.
HEABC argues that the commission does not have the legislative jurisdiction to reshape, in any way, the bargaining units of the for profit employer members of HEABC. Legal opinions limiting and extending the commission's jurisdiction were filed.
The pivotal interpretive issue is whether the commission's jurisdiction to make bargaining unit and other recommendations considered appropriate under s.11.1 (3 ), after exercising the inquiry authority under s.11.1(1), is to be narrowly constructed in light of one mandatory consideration or more purposively constructed in light of all of the mandatory considerations in s.11.1 (2). For the reasons generally stated in the Second Interim Progress Statement to the Minister of Skills, Training and Labour on April 28, 1995, the commission concludes that it has the jurisdiction.
The narrower construction reads the purpose of the statute and the purpose of the commission too restrictively. It excludes all employers that do not amalgamate with a regional health board or
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
33

HEALTH SECTOR LABOUR RELATIONS COMMISSION
community health council and assigns an unnecessary task to the commission. There is very well established and comprehensive law and Labour Relations Board policy on employer successorships. The considerations in s.11.1 (2)(b) are rendered essentially ineffectual with the narrower construction
Since the Second Interim Progress Statement, reliance has been placed on extra-le$islative statements by the Minister of Health and Ministry officials as well as certain statements during the legislative debates. The former are irrelevant to the commission's interpretation of its statutory jurisdiction. The latter do not compel any conclusion. In any event, the statements as reported.are not incompatible with the broader, purposive interpretation of jurisdiction that the commission has adopted.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
34
--~~------~----I

~ ~-
REPRESENTATION OF
RECOMMENDED l;IARGAINING UNITS
RESIDENl'S
NURSES
PARAMEDICAL PROFESSIONALS
26,000
13,000
HEALTII SERVICES
& SUPPORT (Facilities)
43,000
Chart4
®
©
HEALTII SERVICES
&SUPPORT (Community)
14,000
LEGEND
HEU BCNU HSA BCGEU UFCW PAR-BC IUOE
© CJ) (3) © ® ® ®

HEALTH SECTOR LABOUR RELATIONS COMMISSION
TEN BARGAINING UNITS RECOMMENDED
"Many submissions to the commission reflected the persistence of territorial disputes between different occupational groups in and out of hospitals. Health care seems to be particularly plagued with struggles over who shall be entitled to hold certain jobs or perform certain functions. The advantage in these conflicts always appears to be held by those groups with more extensive training or higher credentials, and academic degrees bring exceptional power. Demonstrated capability to perform a function seems to play a minor role, if any, in these disputes.
The advantage conferred by higher training distorts the whole educational process. The need for education - formal, credential-granting programs in particular - is often determined by the pressures of inter-occupational rivalry and aspirations for professional status, rather than by the requirements of the job." (Closer to Home, The Report of the Royal Commission on Health Care and Costs, (1991) Vol. 2, pp. C-144-145)
The commission recommends establishing ten multi-employer bargaining units based on five appropriate unit descriptions: ( 1) residents, (2) nurses, (3) paramedical professionals, ( 4) health services and support - facilities, and (5) health services and support - community.
Residents
Residents are physicians in post-graduate training. Internship was eliminated in favour of specialty training immediately following medical school under licensing legislation in July, 1993. The Professional Association of Residents ofB.C. represents 512 residents.
Residency is a unique form of apprenticeship with 60 to 80 hour weeks the norm and weeks in excess of 100 hours not unusual. Upon completion of residency, the employment relationship with the hospital and membership in PAR-BC are terminated.
While residents are appointed to a base hospital, they rotate through various hospitals. Those undertaking training in family medicine may be placed in rural hospitals, community health clinics and offices of private practitioners for portions of their training. Because of this movement, the B.C. Paying Agency was established in 1982 to administer their salary and working conditions on behalf of the teaching hospitals which employ them.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
35

HEALTH SECTOR LABOUR RELATIONS COMMISSION
PAR-BC was first certified in 1976 following a strike at seven hospitals. Today, it is certified to represent residents in 13 separate hospital bargaining units. There is one collective agreement covering all 13 units between PAR-BC and HEABC.
This group of employees has a distinct community of interest. Any new employment relationships, the promotion of integration of health care delivery and the maintenance of existing consistency in terms and conditions of employment can be met by determining that a single health sector bargaining unit for residents is appropriate.
Nurses
Registered, licensed graduate, registered psychiatric and licensed practical nurses are variously represented in many bargaining units by several trade unions.
Registered nurses (RN) and licensed graduate nurses (LGN) are in the same unit and generally represented by the British Columbia Nurses Union, except in some employment places where they are included in all employee units.
Licensed practical nurses (LPN) are represented by the HEU in its bargaining units. The HEU and BCNU have a 1991 jurisdictional agreement to this effect. No submissions were invited on the appropriateness of including the LPNs in the same bargaining unit as the RNs and LGNs. Although there is logic to having these nursing occupations in the same bargaining unit, no one has suggested that this history of representation should be changed at this time.
The BCNU represents 26,000 employees, all but 20 of whom are nurses. It is certified for 266 bargaining units and has 21 collective agreements. Four master or standard agreements cover 242 of the units. This is one example of the extent to which centralization of bargaining has evolved in the health industry.
The BCNU represents RNs and LGNs in acute and community care. In long term care, it also represents registered psychiatric nurses (RPNs). Other unions represent nurses in long term care and some other service subsectors where the unions hold all employee certifications.
Nurses have a community of interest and, despite the fact it is a single occupation, the history of representation directs that they should continue as a separate bargaining unit.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
36
---~--------,_~~1

HEALTH SECTOR LABOUR RELATIONS COMMISSION
The recommended unit description of "all practising registered, licensed graduate or dual registered psychiatric nurses" does not include LPNs or singly registered psychiatric nurses. It does riot anticipate into which unit midwives or other occupations should be included. It is based on registration being a mandatory prerequisite to performing the duties of the job and does not include nurses who are working in other occupations or classifications where being a nurse is not a mandatory prerequisite to employment.
There will likely be a need for the Labour Relations Board to explore and articulate the limits of this · bargaining unit's boundaries.
The anomalous group, about which the commission has heard much, is the RPN. They are represented by HSA in acute care, BCNU in long term care and UPN in mental health and provincial government employment. Some nurses are dual registered as RN and RPN.
Sometimes there is unbecoming professional competition between RN and RPN organizations rooted in history and personalities. Professional and organizational egos came to the fore in many of the statements to the commission.
The BCNU and UPN are dysfunctional partners in their joint certification for the provincial government nurses' unit. In the midst of the commission's work the BCNU mounted a raid campaign on the provincial government unit.
In the absence of this history, there are compelling reasons to have the RPN and RN in the same bargaining unit. Another option is to have the RPN s in the nurse unit in community and long term care, but in the paramedical professional unit in acute and extend care. This does not confront the issue squarely and does not foster the integration intended for health care service delivery.
The commission recommends that the choice whether to be in the paramedical unit or the nurse unit be given to the RPNs in the health sector by way of representational vote.
The Labour Relations Board may vary a bargaining unit established by regulation implementing a recommendation of the commission. As events unfold and any application arising out of the raid campaign on the public sector RPN group is decided, the Board may consider, at that time, if it appropriate to vary the bargaining unit assignment ofRPNs in the health sector.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
37

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Paramedical professionals
The exclusive scopes of practice and occupational structure of work in the health industry fosters work function separation rather than integration. Professional group identity, association and self advancement represents a modem form of craft unionism since the professions embraced collective bargaining in the 1960's and 70's. Some other trade unionists see it as a culture of crafts and class distinctions that many unions have overcome and that unions that did not are no longer prominent.
Under the Labour Relations Board's leadership, B.C. has escaped the proliferation of technical and maintenance units that exist in the industry in other jurisdictions. It allowed the paramedical professional unit in the 1970's as an exception to the established bargaining units for much the same rationale as the licensed professional unit was adopted under the Public Service Labour Relations Act.
However, while the latter has been restrictively maintained the paramedical professional unit has expanded to include more groups of employees. Several other groups are actively aspiring and manoeuvring to be included in its ranks. The rationale for its separate community of interest is not as defensible when the same occupations are included in other bargaining units in municipal health departments and the provincial government bargaining unit structure.
In the commission's work the incongruence among the bargaining unit membership of paramedical professionals has created a situation where more unions represent some of this group than any other group of employees. There is one union, HSA, that began as an association of associations and represents a majority of the paramedical professionals in the health sector.
Another union, BCGEU, has a history of representation of health paramedical professionals and represents a significant number of employees. It has experience representing both paramedical professionals and others and may be able to assist in achieving some future further integration of units.
Other unions, like HEU/CUPE, also represent paramedical professionals in lesser numbers. The commission's judgment is that history does not compel and the nature of the group militates against more than two Paramedical Professionals units.
The UPN has potentially significant numbers in the health sector, but only in a single occupational focus.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
38
T

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Despite the organizational choices that will be forced upon the UPN, the commission does not recommend that it be certified for a single occupational unit. The RPNs will be able to choose between the BCNU and HSA and the Nurses or Paramedical Professionals units.
The commission is recommending the establishment of two Paramedical Professionals units that will be associated for collective bargaining purposes.
The establishment of Paramedical Professionals units will require the Labour Relations Board to sharply define and attentively superintend its boundaries. The forces to promote professional status for technicians, certified and licensed groups and others in workplaces where knowledge work is expanding and increasingly specialized, come from within the groups and many others who want to create wage differentials for whatever reason for a particular group or want them to be represented by another union.
The Labour Relations Board has been clear that in deciding what is an appropriate unit, it will not "cut across classification lines." (Island Medical Laboratories Ltd. (1993), 19 CLRBR (2d) 161 at 184)
Currently biomedical engineering technologists are in this situation and HSA and HEU have agreed to maintain the status quo. The commission finds that this agreement (presented under s. 11.1 (6)) does not address appropriately the considerations of the need to promote integration of health care delivery and to enable the development over time of provincial consistency in terms and conditions of employment. Therefore, the agreement is not included as a recommendation. ·
The question of which unit is appropriate for all biomedical engineering technologists is to be determined by the Labour Relations Board if HSA and HEU cannot reach an agreement, which is likely given the history of the current situation.
This case presents an early opportunity to the Board to examine the issue and decide in the context of health reform and against the background of the Royal Commission, New Directions and recent health professions legislation if it wishes to anchor this and future determinations in its past criteria or establish new criteria for determining paramedical professional status.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
39

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Health services and support
The diversity of this group extends from hands on patient care to the most remote support service. This group is representationally fragmented among several unions, many of which have very small membership.
The commission recommends two appropriate units - one in facilities care and one in community care. There are three units of each and each grouping of three are to be represented for collective bargaining purposes by an association of bargaining agents. In those associations the HEU and BCGEU have· interlocking memberships with each being the majority participant in one and a minority participant in the other. The interlocking membership of the HEU and the BCGEU in the two associations should enable the establishment of easy transition for employees from one unit to the other. The two units are Health Services and Support - Facilities and Health Services and Support -Community. The former is about three times the size of the latter and is based in the acute, extended and long term care services. The latter is based in community care. The third union in each is IUOE in Facilities and UFCW in Community. Each will have an important role to play in their association.
Health services and support workers are the greatest number of employees with the greatest occupational diversity. The cultural differences between the hierarchical medical model and the community model in the organization of work are greater to overcome when there is a wider range of occupations.
The challenges within the Nurses unit and the Paramedical Professionals units exist and will have to be overcome by the employees and their bargaining agents. Their occupational credentials provide a basis for mobility and demand for their skills. Their job security threats are technological change, reduced resources and substitution by other occupations.
Among health services and support workers their work culture differences are accentuated by the diversity of their current trade union representation. They face the challenge of health care reform from very different perspectives.· Integration and development over time of provincial consistency in terms and conditions of employment is overlaid on many different collective agreements and approaches by employers, trade unions and employees.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
40
,..... I I
-----------~ l

HEAL TH SECTOR LABOUR RELATIONS COMMISSION
It is the commission's assessment that orderly change management directs that there be two units for collective bargaining: one encompassing acute, extended and long term care called Facilities; and another encompassing all other service subsectors called Community.
The administrations of the new public employer are included in the latter. The RHB and CHC regional and community administration is intended to be the direct support for the planning and coordinating role of Boards and Councils - not service delivery. It is not intended to be any and all shared services.
If health care service subsectors were placed on a continuum of care from acute to home support, the trade union representation is overwhelmingly HEU from the acute to long term care subsectors. From home support to long term care, representation is dispersed and BCGEU has been the majority trade union.
These two unions have the experience to lead all health support and service workers - through integration and toward provincial consistency. Each will have a Facilities and Community unit. Out of respect for their different history of representation, the IUOE and UFCW each have a unit. The former in Facilities and the latter in Community.
These four unions with their six bargaining units can effectively represent and resolve the competing cultural concerns. In the Facilities group, HEU has one unit encompassing over 99% of its current
. membership. In the Community group BCGEU has one unit encompassing over 70% of its current health services and support membership. They each have the base to provide leadership on all sides of integration.
While the recommendations do not integrate Facilities and Community into one bargaining unit, they do enable service delivery and organizational integration.
"Bargaining centralization is a fact of life, but just how much centralization is appropriate is a conundrum that still bedevils the parties" (Larry Haivan, "Industrial Relations in Health Care:. Regulation, Conflict and Transition to the 'Wellness Model"' in Swimmer and · Thompson, ed., Public Sector Collective Bargaining in Canada: Beginning of the End or End of the Beginning? (1955) IRC Press, Queen's University, p. 236)
To achieve the consolidation of these six units as the foundation for manageable associations of bargaining agents,. it is considered necessary to end the representational rights of several unions.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
41

· HEAL TH SECTOR LABOUR RELATIONS COMMISSION
This is where the recommendations tread on established rights as an imperative of change. No one takes any satisfaction in this outcome.
The most resentful are the private sector community and craft trade unions - IW A, USW A, IBEW, Carpenters, Painters, Plumbers and Labourers. The recommendations exclude them from the health sector without similar restrictions on unions in their industrial sector. It takes what they earned and what their members chose for a greater purpose without extending to accommodate or grandparent them.
The recommendations do afford limited union agreements or employee choice for all but 40 employees in four bargaining units represented by four unions. In their case, the employees have their current union membership rights continued if they wish.
The concern of the four construction trades is that the industry and its unions rely upon them, their members and their apprenticeship and training programs to produce and supply qualified trades employees on a temporary or permanent basis. Yet the industry does not actively support trades training through apprenticeships or assured demand through agreement to call on the trades unions for qualified persons when work or vacancies become available. This is an issue that will have to be addressed as a matter of employer policy or at collective bargaining.
The Broadway Pentecostal Lodge Employees' Association received its first recognition as a trade union and first certification on June 9 for a unit of 99 employees .. The commission learned of this on June 26. The same principles that were applied to transfer representation from other trade unions, with as many or more members and a history of representation, were applied to the BPLEA.
Jurisdictional Agreements
The commission received a jurisdiction agreement between HEU and HSA concerning biomedical engineering technologists. For reasons stated earlier, it is not being recommended. The HEU, CUPE and BCNU presented a wide ranging agreement addressing their and other unions' jurisdiction. Some parts, but not all, have been incorporated into the recommendations.
CUPE presented that, in the spirit of its organizing protocol with HEU establishing HEU as the "Service division of CUPE in British Columbia covering acute care, long-term care services workers", it took one position with HEU. The recommendations build on this relationship to enable more rapid consolidation than the two unions may have originally planned.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
42
---------.--f I

HEALTH SECTOR LABOUR RELATIONS COMMISSION
As the commission prepared its report, members ofVMREU (a 76 year old union) were to vote on merging with CUPE. Other unions were considering how they sustain their viability in the new environment and if they should merge with another union. The recommendations provide latitude for inter-union agreements on jurisdiction.
OTHER RECOMMENDATIONS: CHANGE MANAGEMENT
The commissioner "may make other recommendations the commissioner considers appropriate." (Health Authorities Act, S. 11.1 (3))
It is necessary to act on recommendations implemented by regulation in an expeditious manner in order to facilitate health care delivery restructuring. The recommendations therefore include times within which unions may agree and after which the Labour Relations Board must act.
The overall plan for reshaping bargaining units is broadly to facilitate health care reform. The approach is to consolidate the health sector bargaining units in advance of Regional Health Boards and Community Health Councils starting to assume responsibility this fall.
As organizational amalgamation occurs among employers and municipal and provincial government employees are transferred into the health sector, the composition ofthe bargaining units will be known in advance of amalgamation and integration. The immediacy for preparing that structure is the known fund reduction the province will face in 1996 and 1997 and the impending organizational changes.
"Change is stressful. Pace of change is a real issue. A lot of health care leaders and providers are wearied by the pace of change and wish everything couldjust decelerate. Circumstances won't allow it. People are going to have to continue a juggling act of doing a superb job of managing their existing programmes while being involved in innovative redirection of programmes. That is stressful.
This overwhelming feeling is felt all the way up and down the line. We will need to be skilful in managing the 750,000 of us who work in the delivery of care and in the promotion of health in Canada, to arrive at a new and better place. We will need to support each other. This is a real opportunity to make change in a constructive way, while being aware of the mounting pressure to move rapidly. We are in the early stages of a major transformation of health work. Our working lives in health will be irreversibly altered and, if we are able to balance efficiency with compassion, improved." (Michael B. Decker, Healing Medicare: Managing Health System Change The Canadian Way (1994) McGilligan Books, p. 95)
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
43

HEAL TH SECTOR LABOUR RELATIONS COMMISSION
Change is intimidating and most often resisted, either actively or passively. To facilitate change, service integration and worker mobility, the commission recommends portability of seniority and service recognition as a necessary companion to bargaining unit restructuring. The recommended disputes resolution process is grievance arbitration.
Some measure of disorder, inconsistency and illogic is part of transition in change. Maintaining all current collective agreements until their expiration will create some of this during the transition. However, it will also provide familiarity for most, delay the urgency to rationalize and assure there are no immediate cost impacts to employees through collective agreement stripping or to employers through leapfrogging or levelling up .. Continuance of all collective agreements until their expiration is recommended.
The change process in health reform requires some elements of stability. Assuring the current bargaining agents that their bargaining units will not be subject to a raiding campaign by another union, provides some measure of stability. This is recommended.
Bargaining unit reshaping addresses the existing bargaining units. To address the future, it is recommended that all new groups of employees who chose union representation are included as an accretion to an existing bargaining unit. This avoids future proliferation of bargaining units.
Major change initiatives have to be evaluated. Information is necessary to make the evaluation. It is recommended that the Labour Relations Board provide that information in its annual report for three years. Of course, it may choose to report longer.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
44

HEALTH SECTOR LABOUR RELATIONS COMMISSION
RECOMMENDATIONS FOR RESHAPING HEALTH SECTOR BARGAINING UNITS
Phase One: Initial Consolidation
1.1 The "health sector" consists of all current and future members of the Health Employers Association of British Columbia or its successor, while members, and all their unionized health care employees.
1.2 With transitional exceptions, all appropriate bargaining units in the health sector will be multi-employer bargaining units.
1.3 There are to be five appropriate multi-employer bargaining units in the health sector: (1) Residents, (2) Nurses, (3) Paramedical Professionals, (4) Health Services and Support - Facilities, and (5) Health Services and Support - Community.
1.4 Where there is more than one bargaining agent for similar appropriate multi-employer bargaining units the bargaining agents will form an association of bargaining agents.
1.5 To establish a Residents unit, the existing resident bargaining units represented by PAR-BC are consolidated into one health sector bargaining unit to be represented by PAR-BC.
1.6 As a preparatory step to establish the other appropriate bargaining units in the health sector, all of the existing bargaining units of the following trade unions are consolidated into one bargaining unit for each trade union in each of the following groupings of health care delivery subsectors:
Health Sector: Nurses BCNU
Health Sector: Paramedical Professionals HSA
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
45

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Acute. Extended & Long Term Care: Health Services and Support - Facilities (Acute, Extended and Long Term Care, The Arthritis Society, Canadian Red Cross Society, British Columbia Cancer Agency, Cumberland and Tilbury Laundries, and Diagnostic and Treatment Centres) HEU BCGEU IUOE
Community Care: Health Services and Support - Community (includes Adult Day Care, Child Development Centres, Community Service Agencies, Drug and Alcohol, Home Support, Mental Health, and RHB and CHC regional and community administration) UFCW BCGEU HEU
1. 7 The trade unions are to be certified for these consolidated bargaining units by the Labour Relations Board within thirty days after ·the making of regulations to implement these recommendations.
Implications:
• The multi-employer units include Regional Health Boards, Community Health Councils, denominational employers, for profit and not for profit corporations, · societies and agencies, and hospitals ..
• First bargaining unit - Residents - is established.
• Bargaining units of trade unions that will continue to h:ive representational rights are consolidated.
• Bargaining units of trade unions whose representational rights will be merged or transferred are unaffected in this phase.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
46

HEALTH SECTOR LABOUR RELATIONS COMMISSION
• The preparatory consolidation, and final consolidation in the case of the residents, of certified bargaining units is to be an administrative matter handled expeditiously by the Labour Relations Board.
• The Community Care grouping is an inclusive grouping that will include any new or unspecified health care delivery subsector.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
47

HEALTH SECTOR LABOUR RELATIONS COMMISSION
· Phase Two: Consolidate Nurses Unit
2.1 All practising registered, licensed graduate and dual registered psychiatric nurses in the health sector are to be included in the consolidated BCNU Nurses unit within ninety days after the making of regulations to implement these recommendations.
2.2 A nurse is a "practising" registered, licensed graduate or dual registered psychiatric nurse when registration is a mandatory prerequisite to performing the duties of the job as required by statute, regulation, program accreditation or by the employer.
2.3 By agreement between the BCNU and other unions or, if no agreement, by representational vote, the 20 or so remaining employees in the BCNU unit who are not registered, licensed graduate or registered psychiatric nurses vote, on an employer by employer basis, to be represented by HEU, BCGEU, IUOE or UFCW in their applicable Health Services and Support - Facilities or Community unit.
2.4 Notice of all agreements must be given to the Labour Relations Board not later than forty five days after the making of regulations to implement these recommendations.
2.5 Any representation votes are to be conducted within ninety days after the making of regulations to implement these recommendations.
Implications:
• Up to 420 nurses may change union representation to the BCNU.
• Second bargaining unit - Nurses - is established.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
48
______________ , ___ ·1

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Phase Three: Associate Paramedical Professionals Units
3 .1 The 680 or so paramedical professional employees represented by BCGEU in both its Health Services and Support - Facilities and Community units are to be included in a new Paramedical Professionals unit to be represented by BCGEU.
3 .2 All paramedical professional employees in the health sector, except those represented by BCGEU and HSA, are to be included in either the HSA or BCGEU Paramedical Professionals unit by agreement between the currently certified trade union and HSA or BCGEU. If there is no agreement, the employees vote, on an employer by employer basis, to be represented by HSA or BCGEU in their Paramedical Professionals unit.
3 .3 By agreement between HSA and HEU, all 13 5 or so biomedical engineering technologists in the health sector (represented by HEU, HSA, IUOE, and BCGEU) are to be included in either the HEU Health Services and Support - Facilities unit or the HSA Paramedical Professionals unit. If there is no agreement within thirty · days after the making of regulations to implement these recommendations, the Labour Relations Board schedule a hearing to commence within ninety days after the making of regulations to decide which is the appropriate unit to include all biomedical engineering technologists.
3 .4 All singly registered psychiatric nurses in the health sector, represented by any trade union, vote as one constituency to be included in the BCNU Nurses unit or in the HSA Paramedical Professionals unit. The outcome will determine for all singly registered psychiatric nurses employed in the health sector whether they will be included·in the Nurses or HSA Paramedical Professionals unit.
3.5 By agreement between HSA and HEU, BCGEU, IUOE or UFCW or, if no agreement, by representational vote, the 400 or so employees in the HSA Paramedical Professionals unit who are not paramedical professionals vote, on an employer by employer basis, to be represented by HEU, BCGEU, IUOE or UFCW in their applicable Health Services and Support - Facilities or Community unit.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
49

HEALTH SECTOR LABOUR RELATIONS COMMISSION
3.6 Notice of all agreements must be given to the Labour Relations Board not later than forty five days after the making of regulations to implement these recommendations.
3. 7 Any representation votes are to be conducted within ninety days after the making of regulations to implement these recommendations.
3.8 For all collective bargaining purposes, HSA and BCGEU are to form an association of bargaining agents to negotiate one collective agreement covering the employees in both Paramedical Professionals units, including means to promote integration of health care delivery and to enable the development over time of provincial consistency in terms and conditions of employment.
3 .9 While HSA and BCGEU will be the certified bargaining agents for their respective Paramedical Professional units, the Labour Relations Board will certify their association of bargaining agents for collective bargaining purposes and all procedures under Parts 4 to 7, inclusive, of the Labour Relations Code.
3.10 IfHSA and BCGEU have not agreed upon the articles of association by January 1, 1996, the Labour Relations Board will, before March 31, 1996, decide the articles of association that fulfil the purposes for which the association is to be formed and certify the association of bargaining agents.
Implications:
• Third bargaining unit - Paramedical Professionals - is established.
• An estimated 340 paramedical professionals will change trade unions.
• Approximately 600 singly registered psychiatric nurses would participate m the representation vote.
·• Trade unions may voluntarily form an association of bargaining agents or have the
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
50
--- ---~~-----------"--I

r
HEALTH SECTOR LABOUR RELATIONS COMMISSION
Labour Relations Board decide the articles of association after hearing from all parties, including the employer, with the ability to reconsider its decision in the future.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
51

HEAL TH SECTOR LABOUR RELATIONS COMMISSION
Phase Four: Directed Transfers. Representation Votes and Board Decisions
4.1 Unless there are agreements to merge or transfer jurisdiction between the currently certified trade union and one of the trade unions identified to be a choice in a representational vote, the Labour Relations Board will conduct the following representational votes:
1. The 4 7 5 or so remaining employees represented by a local of CUPE vote, on an employer by employer basis, to be represented by HEU, BCGEU or IUOE in their Health Services and Support - Facilities unit.
2. The 330 or so remaining employees represented by a local of CUPE vote, on an employer by employer basis, to be represented by HEU, BCGEU or UFCW in their Health Services and Support - Community unit.
3. The 259 or so remaining employees represented by CGWU, Local 602 at Clovelly Terrace Hospital Ltd., Decker Management (Sandringham Hospital), Preferred Care Corporation (James Bay Lodge) and Vancouver Island Housing Association for the Physically Disabled ( 197 6) (Nigel Home) vote, on an employer by employer basis, to be represented by HEU, BCGEU or IUOE in their Health Services and Support - Facilities unit.
4. The 80 or so remaining employees represented by IW A, Local 1-425 at Central and South Cariboo Home Support Services Associations vote to be represented by UFCW, BCGEU or HEU in their Health Services and Support - Community unit.
5. The 20 or so remaining employees represented by IW A, Local 1-71 at Prince Rupert Home Support Society vote to be represented by UFCW, BCGEU or HEU in their Health Services and Support - Community unit.
6. The 59 or so remaining employees represented by Broadway Pentecostal Lodge Employees' Association vote to be represented by HEU, BCGEU or IUOE in their Health Services and Support - Facilities unit.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
52

HEALTH SECTORLABOUR RELATIONS COMMISSION
7. The 34 or so remaining employees represented by IUOE at C.L. Antonio Inc. (Katalin House) Crestlene Lodge Ltd. (Crestlene Lodge) and Haven Guest Home vote, on an employer by employer basis, to be represented by HEU, BCGEU or UFCW in their Health Services and Support - Community unit.
8. The 13 or so remaining employees represented by USWA, Local 9705 at McBride Manor Society vote to be represented by HEU, BCGEU or UFCW in their Health Services and Support - Community unit.
9. The 8 or so remaining employees represented by USW A, Local 9705 at the Trail Regional Hospital Society vote to be represented by HEU or IUOE in their Health Services and Support - Facilities unit.
10. The 45 or so remaining employees represented by VMREU at Vancouver Mental Patient's Association Society vote to be represented by HEU, BCGEU or UFCW in the Health Services and Support - Community unit.
11. The 210 or so remaining employees represented by the PEA at the Greater Vancouver Mental Health Services Society vote to be represented by HEU, BCGEU or UFCW in the Health Services and Support - Community unit.
4.2 Notice of all agreements must be given to the Labour Relations Board not later than forty five days after the making of the regulations to implement these recommendations.
4.3 Any representation votes are to be conducted within ninety days after the making of regulations to implement these recommendations.
4.4 Include the employees represented by the following trade unions at Royal Jubilee Hospital into the HEU Health Services and Support - Facilities unit within ninety days after the making of regulations to implement these recommendations:
• the 16 or so employees represented by the IBEW, Local 230;
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
53

HEALTH SECTOR LABOUR RELATIONS COMMISSION
• the 10 or so employees represented by the Carpenters, Local 1598;
• the 8 or so employees represented by the Painters, Local 1163; and
• the 6 or so employees represented by the Plumbers, Local 324.
4.5 The employee members of IBEW, Local 230, Carpenter, Local 1598, Painters, Local 1163 and Plumbers, Local 324, who are transferred into the HEU Health Services and Support - Facilities unit, may choose to retain their membership in these trade unions and exercise all of the attendant rights, including continued participation in trade union pension plans, despite the fact that they will become members of the HEU.
Implications:
• An estimated 1453 health services and support employees will change trade unions.
• Employees who are not given any choice through their trade union or by representation vote have their current trade union membership rights continued.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
54
-------------r--J

I I
HEALTH SECTOR LABOUR RELATIONS COMMISSION
Phase Five: Associate Facilities and Community Care Health Services and Support Units
5.1 For all collective bargaining purposes, HEU, BCGEU and IUOE are to form an association of bargaining agents to negotiate one collective agreement covering the employees in their Health Services and Support-Facilities units, including means to promote integration of health care delivery and to enable the development over time of provincial consistency in terms and conditions of employment.
5 .2 While HEU, BCGEU and IUOE will be the certified bargaining agents for their respective Health Services and Support-Facilities units, the Labour Relations Board will certify their association of bargaining agents for collective bargaining purposes and all procedures under Parts 4 to 7, inclusive, of the Labour Relations Code.
5 .3 If HEU, BCGEU and IUOE have not agreed upon the articles of association by January 1, 1996, the Labour Relations Board will, before March 31, 1996, decide the articles of association that fulfil the purposes for which the association is to be formed and certify the association of bargaining agents.
5.4 For all collective bargaining purposes, BCGEU, UFCW and HEU are to form an association of bargaining agents to negotiate a collective agreement covering the employees in their Health Services and Support-Community units, including means to promote integration of health care delivery and to enable the development over time of provincial consistency in terms and conditions of employment.
5.5 While BCGEU, UFCW and HEU will be the certified bargaining agents for their respective Health Services and Support-Community units, the Labour Relations Board will certify their association of bargaining agents for collective bargaining purposes and all procedures under Parts 4 to 7, inclusive, of the Labour Relations Code.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
55

HEALTH SECTOR LABOUR RELATIONS COMMISSION
5.6 If BCGEU, UFCW and HEU have not agreed upon the articles of association by. January 1, 1996, theLabour Relations Board will, before March 31, 1996, decide the articles of association that fulfil the purposes for which the association is to be formed and certify the association of bargaining agents.
Implications:
• Fourth bargaining unit-Health Services and Support-Facilities - and Fifth bargaining unit - Health Services and Support-Community- are established.
• Trade unions may voluntarily form an association of bargaining agents or have the Labour Relations Board decide the articles of association after hearing from all parties, including the employer, with the ability to reconsider its decision in the future.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
56
~~~------------~ l

HEALTH SECTOR LABOUR RELATIONS COMMISSION
Phase Six: Integrate Ministry of Health, B.C. Mental Health Society (Riverview Hospital), Glendale Lodge Society (Broadmead Lodge and Glendale Lodge) and Oak Bay Lodge Society (Oak Bay Lodge)
6.1 The 1,880 or so registered, licensed graduate and dual registered psychiatric nurses be included in the BCNU Nurses unit.
6.2 The 168 or so paramedical professionals represented by the PEA be included in the Paramedical Professional unit represented by either HSA or BCGEU as agreed between PEA and HSA or BCGEU.
6.3 Notice of an agreement must be given to the Labour Relations Board not later than forty five days after the making of regulations to implement these recommendations.
6.4 If notice is not given, the Labour Relations Board conduct a representation vote among the paramedical professional employees. represented by PEA at each of these four employers; on an employer by employer basis. The vote is to be held within thirty days after the employer, in the case ofB.C. Mental Health Society, Glendale Lodge Society and Oak Bay Lodge Society, becomes an employer in the health sector. In the case of the Ministry of Health, the vote will be held within thirty days after fifteen percent of the paramedical professional employees are transferred to employment by an employer in the health sector.
6.5 The paramedical professional employees represented by the BCGEU be included in the Paramedical Professionals unit represented by BCGEU.
6.6 The health services and support employees represented by the BCGEU continue to be represented by the BCGEU in its Health Services and Support-Facilities unit in the case of Riverview Hospital, Glendale Lodge Society and Oak Bay Lodge Society and in the its Health Services and Support-Community unit in the case of the Ministry of Health.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
57

· HEALTH SECTOR LABOUR RELATIONS COMMISSION
6. 7 Singly registered psychiatric nurses represented by VPN be included in the BCNU Nurses unit or the HSA Paramedical Professionals unit as determined by the outcome of the representational vote in 3.4.
Implications:
• Singly registered psychiatric nurses are in one unit.
• As provincial government employees transfer to health sector employees they transfer into an appropriate bargaining unit.
• Provincial government employees may transfer to the health sector over time knowing into which bargaining unit they will be included.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS
June 30, 1995
58
.~. ~,.,,,...,,,...,_~---·--·---------------
r

HEALTH SECTOR LABOUR RELATIONS COMMISSION ·
Phase Seven: Integrate Municipal Government and Pender Detox Employees Represented by VMREU
7 .1 The 940 or so registered, licensed graduate and dual registered psychiatric nurses be included in the BCNU Nurses unit
7 .2 The 260 or so paramedical professional employees represented by VMREU and CUPE at the Capital Regional District, North Shore Health, four Lower Mainland municipalities and the Governing Council of the Salvation Army in Canada (Pender Detox) be included in the HSA or BCGEU Paramedical Professionals unit by merger or transfer of jurisdiction agreement between VMREU or CUPE and HSA or BCGEU on an employer by employer basis. Where there is no agreement, then the employees represented by VMREU and CUPE vote, on an employer by employer basis, to be represented by HSA or BCGEU.
7 .3 The 420 or so remaining health services and support employees repre~ented by VMREU be included in the HEU, BCGEU or UFCW Health. Services and Support-Community unit by agreement betweep VMREU and HEU, BCGEU or UFCW or, in the absence of an agreement, by representation vote among the employees. The VMREU health services and support employee portion of the unit at Pender Detox be represented by whatever union is agreed or successful in the vote.
7.4 If CUPE and HEU have not transferred jurisdiction by agreement, any health services and support employees represented by CUPE at the Capital Regional District, North Shore Health and Lower Mainland municipalities be included in the HEU, BCGEU or UFCW Health Services and Support-Community unit and represented by HEU, BCGEU or UFCW by a representational vote among each group of employees at North Shore Health and each municipality.
7.5 The 40 or so paramedical professional employees represented by HSA at North Shore Health be included in the Paramedical Professionals unit represented by HSA.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
59

HEAL TH SECTOR LABOUR RELATIONS COMMISSION
7.6 The 50 or so remaining health services and support employees represented by RSA at North Shore Health be included in the HEU, BCGEU or UFCW Health Services and Support - Community unit by agreement between HSA and HEU, BCGEU or UFCW or, in the absence of an agreement, by representation vote among the employees.
7. 7 Notice of an agreement must be given to the Labour Relations Board not later than forty five days after the making of regulations to implement these recommendations.
7 .8 Any representational votes are to be conducted within ninety days after the making of regulations to implement these recommendations.
Implications:
• As municipal government employees transfer to health sector employers they are included in an appropriate bargaining unit.
• Municipal government employees may transfer to the health sector over time knowing into which bargaining unit they will be included.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
60
r
-----------------------··~ l

HEAL TH SECTOR LABOUR RELATIONS COMMISSION
OTHER RECOMMENDATIONS
8.1 Seniority and service recognition will be portable for any employee who changes bargaining unit, bargaining agent or collective agreement as a result of any aspect of bargaining unit reshaping in the next five years.
8.2 All disputes about the interpretation, application and operation of the portability of seniority and service recognition and any consequence whatsoever of portability are to be finally resolved by the arbitration procedures in Part 8 of the Labour Relations Code.
8.3 Unless otherwise agreed by HEABC and a bargaining agent or association of bargaining agents, all collective agreements and all their terms and conditions of employment continue to apply . until their expiration to employees transferred between bargaining units or employers under these recommendations.
8.4 To foster certainty during implementation of the bargaining unit reshaping, no trade union may apply for certification for any pargaining unit or constituent unit of an association of bargaining agents during the three years following the making of regulations to implement these recommendations.
8.5 All unrepresented employees who choose trade union representation in the future will be included in one of the ten appropriate multi-employer bargaining units represented by the applicant trade union.
8.6 The Labour Relations Board include a report on the implementation of these recommendations in its annual report under s.157 of the Labour Relations Code in each of the three years subsequent to making regulations implementing these recommendations.
8.7 All circumstances unanticipated by these recommendations are to b~ resolved by the Labour Relations Board in accordance with the principles of these recommendations.
RESHAPING B.C. HEALTH SECTOR APPROPRIATE BARGAINING UNITS June 30, 1995
61

APPENDIX E llllll
Trade Unions in Health Sector

BCGEU
BCNU
BP LEA
CGWU
CUPE
TRADE UNIONS IN HEAL TH SECTOR
B.C. Government & Setvice Employees Union
B.C. Nurses' Union
Broadway Pentecostal Lodge Employees• Association
Construction & General Workers Union, Local 602
Canadian Union of Public Employees
-Local 3495-02 - Pioneer Community Living Association
-Local 3495-03 - Coast Foundation Society
-Local 3495-04 - Canadian Mental Health Association Vancouver/Burnaby Branch
-Local 3495-05 - Chown Adult Day Care Centre
-Local 3495-07 - St. James Social Setvice Society
-Local 3495-12 - Marine View Housing Society
-Local 3495-14 - B.C. Persons with Aids Society
-Local 3495-19 - Mount View Lodge
-Local 3495-20 - Grouse View Care Home
-Local 608 - Okanagan Similkameen Housing Society for Handicapped Citizens
-Local 608 - Country Squire Retirement Villa Limited (Country Squire Villa)
-Local 608 - A.C.M.C.J. Holdings Limited (Haven Hill Retirement Centre)
-Local 1136 - Summerland Lodge
-Local 1136 - Parkdale Place Housing Society
-Local 1731 - New England Hospitals
-Local 1731 - Napier Intermediate Care Home
-Local 3238 - Parksville & District Home Support Society
-Local 2516 - Prince George Regional Community Care Society
-Local 2254 - Boundary Lodge
-Local 2209 - Bradden Private Hospital
-Local 2093-A-The Tom Uphill Memorial Home Society
-Local 1978 - Victoria Capital Regional District
-Local 1311 - Central Park Lodges Limited
-Local 1267 - Pleasant View Housing Society
I
I I
I. I

HEU
HSA
IBEW
IBP AT
IUOE
IWA
PAR-BC
PEA
UA
UBCJA
UFCW
VPN
USWA
VMREU
-Local 900 - Kamloops Home Support Services Association
-Local 718 - Richmond Civic Employees
-Local 389 - North Vancouver Civic Employees
-Local 387 - New Westminster Civic Employees
-Local 338 - Central Okanagan Health Care Society (David Lloyd Jones Home)
-Local 23 - Burnaby Civic Employees
Hospital Employees' Union
Health Sciences Association ofB.C.
International Brotherhood of Electrical Workers, Local 230
International Brotherhood of Painters & Allied Trades, Local 1163
International UnionofOperating Engineers, Local 882
IW A - Canada - Local 1-71
- Local 1-425
Professional Association of Residents ofB.C.
Professional Employees Association
United Association of Journeymen & Apprentices of the Plumbing & Pipefitting
Industry of U.S. & Canada, Local 3 24
United Brotherhood of Carpenters & Joiners of America, Local 1598
United Food & Commercial Workers' International Union, Local, 1518
Union of Psychiatric Nurses
United Steelworkers of America, Local, 9705
Vancouver Municipal & Regional Employees Union
-,

APPENDIX I
Devolving Government or Public Agency
Unionized Health Care Employees:
Trade Union By Sector
111111

DEVOLVING GOVERNMENT OR PUBLIC AGENCY UNIONIZED HEALTH CARE EMPLOYEES : UNION BY SECTOR (Prepared by: George K. Bryce for the Health Sector Labour Relations Commission, current to June 24, 1995) COMMENT: This table sets out the number of unionized health care workers working for various governments and public agencies who are not members of the HEABC. It is the bestavailable data, current as of June 1, 1995. It is assumed that each cell in this table represents a separate but active certification.
UNION BCGEU BCNU CUPE HSA PEA UPN VMREU Total
MUNICIPAL AND REGIONAL GOVERNMENTS
North Shore Health 104 8 91 203
City of Vancouver 431 542 973
City of Richmond 82 76 158
City of New Westminster 12 15 27
City of Burnaby 105 106 211
Capital Regional District 191 206 397
Municipal Subtotal 925 411 91 542 1,969
PROVINCIAL GOVERNMENT
Ministry of Health 1,893 1,654 138 202 3,887
BC Mental Health Soc (Riverview Hospital) 1,069 152 27 487 1,735
Glendale Lodge Society (Broadmead and Glendale Lodges) 324 37 3 27 391
Oak Bay Lodge Society (Oak Bay Lodge) 209 37 5 251
Provincial Subtotal 3,495 1,880 168 721 6,264
Total Members 3,495 2,805 411 91 168 721 542 8,233
Total Certifications 4 10 5 I 3 4 1 28
I

APPENDIX J
Estimated Number of Unionized
Health Care Employees in B.C.:
Sector By Trade Union 1!1111

ESTIMATED NUMBER OF UNIONIZED HEALTH CARE EMPLOYEES IN BC: SECTOR BY TRADE UNION Prepared by: George K. Bryce for the Health Sector Labour Relations Commission, current to June 24, 1995 COMMEITT: This table sets out the number of unionized health care workers working for members of the HEABC (current as of June 23, 1995) and for various governments and public agencies who are not members of the HEABC (current as of June I, 199.5). The numbers in brackets and italic /0111 arc the estimated number of certifications held by that union.
SECTOR Acute Care fa.tended Brdmead, Diagno Rat Long Tenn Adult Child Comly Drug Mental GnrVon Ri\'Cr- llume Devolv111 Devolvne with Can: Glendale slicnnd Cross Can: Dny [h'lpmt Ser\·c:c mt Health Mental view Support Ministry Municipl Evmded (stand &O.k Treaunt ®nl Can: Centres A gens Alcohol Health Hospital Aaenc:Y of Health & Reenl
UNION Can: alone) Bay Ldgs lmlll<h' Ser Soc Total UNION HEU 27895f941 3.053 f/51 146(81 395 fJ) 8714 fl261 13 (}) -1.2 (/) 31 (2) 125 flOI 10 (/) 40.424 (2611 OCNU 21 566(96) 852 f/61 7-1. (2) 64(/01 48 (/) 2,25711291 15(/) 9121 15(}) 152'/l 4 (/) 1654fll 925(6) 27 695(267) OCOEU 392 ti) 533 f2) 1.-1.09 f241 1912) 67 (}) ff7121 180 (IQ) 378 (/0) I 069(/) 4q;J(J4) I 893 fl) 10588(88) HSA 8630 f9JI -l.60 ( /2l 14919) 56 (/) 6318) 4091121 39121 19 (/) 26 (2) 91 (/) 9.942 (1411 UR:.'W 2 737 (35) 2 737 fJSJ CUPE 616 fl21 12 (}) 61/l 471 f7) 121 f21 411 (j) I 637 fJOJ
· UPN 32 (21 9 (/) 73 (/) 487 (JI 202 (/) 803 (6)
IUOE 176 ( /9) 534(8) 34 {]) 744 (JO) VMREI.J 62 {/) 542 (1) 604 f2J PAR 509 (//) (/) 509(]2) l'J;A ~ (/) 312 ( /) 27 (/) 138 {/) 480(4) <.UWU 259(4) 259"" IWA 100 {j) 100 fJI BPU'.A 99(/) 99(/)
USWA 8 (/) 13 (/) 21 f21 IBEW 16 {/) 16 (}) UBCJ 10 (/) 10 (J PNTR 8 (/) 8 fl' PLUMB 6 (/) 6 (J
Toi al 511.824 -1.,757 642 359 49') 13,960
"""" -1.76 1119 230 1,118 460 1,735 7,533 3,8ff7 1,969 96,612 mcmbcra
TOllll 318
"""" 7 27 5 314 "' 13 7 13 36 3 4 76 4 13 Ill cerlifictns
Total 89 13 2 12 3 160 ~ 12 6 13 31 1 1 63 l 6 • 416
employers
I •Some employers operate in more than one sector, so this total may be somewhat greater than the trne total. Unfortunately, it was not possible to adjust this figure downward to account for those few employers who operate in more than one sector.
HEU eoru BCOEU HSA UR:\V CUPE UPN IOOE VMREI.J PAR PEA cnwu IWA BPUlA USWA lBEW UBCJ PNrR PUJMB
1