Embed Size (px)
Citation preview
1
APPLICATION DOCUMENT
FOR
Empanelment of Suppliers
For
Medical Store Items
(1st April 2016 – 31st March 2019)
Medical Stores,
Kasturba Hospital, Sevagram
Distt. Wardha (M.S.)
India – 442102
Phone :- 07152 – 284341 Ext. 243

2
INDEX
Sr.No. CONTENT
1. About Kasturba Hospital, Sevagram
2. General Information & Instructions
3. Eligibility for empanelment
4. Documents to be submitted
5. Submission of documents
INFORMATION TO BE FURNISHED BY THE
APPLICANT
PART – I : Basic Information
PART – II : Financial Information
PART – III : Enclosures
Undertaking (Annexure-A)
Details of Orders/ Completed during the Last Three years (
Annexure – B)
Abbreviations:
KHS Kasturba Health Society
KH Kasturba Hospital
MGIMS Mahatma Gandhi Institute of Medical Sciences

3
1.0 About Kasturba Hospital, Sevagram
Kasturba Hospital (KH) Sevagram is a nearly 1000 bedded hospital affiliated to Mahatma
Gandhi Institute of Medical Sciences (MGIMS) which is a teaching Medical College, located
in Wardha district of Maharashtra. KH & MGIMS are run by Kasturba Health Society
(KHS), which is an autonomous, government funded organization, established in 1969.
Kasturba Hospital provides medicines, surgical items, disinfectants and diagnostics for
patients through its Medical Stores. During 2015-2016 Medical Stores made total purchase
worth around Rs. 13.00 crores, and it is anticipated that the values will grow by at least 10%
annually.
2.0 General Information & Instructions :-
Category Category Name Sub-Categories Item Description A Oral Drugs Tablets All Tablets for oral use
Capsules All Capsules for oral use
Syrups All Syrups / Suspension
for oral use
Powders All Powders for oral use
Category Category Name Sub-Categories Item Description B Parental Drugs Injections All Injections for
Parenteral use.
Intra-Venous (IV)
Intra-Muscular (IM)
Subcutaneous (SC)
Intradermal ( ID ) Intra
spinal route
Category Category Name Sub-Categories Item Description C Topical Drugs Eye-Ear-Nose Drops EEN Drops
Sprays Local/ Oral/Mucosal
Ointments Local/ Oral/Mucosal
Local Applicants Suppositories
Creams Local / Oral /Mucosal
Respiratory Solution Nebulizer Solutions
Inhalers Inhalers, Respules
Transdermal Patch Analgesic
Category Category Name Sub-Categories Item Description
D General Surgical 1 CSSD items Cotton, Gauze,
Bandage, Gloves,
Syringes, IV fluids

4
Category Category Name Sub-Categories Item Description E General Surgical
items- 2
Needles All sizes for parenteral
use
Syringes Disposable / Glass
Tubings & Catheters All catheters Ryle’s
tube, feeding tubes,
Catheter, O2 mask
Endotracheal etc.
Infusion devices All I.V. Sets, Blood
bag
Urology Stents All tubed Medical
devices for intra
operative use
Category Category Name Sub-Categories Item Description
F Suture Materials Sutures/Mesh/
Staplers
Surgical sutures, mesh
and staplers/Devices
Category Category Name Sub-Categories Item Description G Diagnostic Agents Imaging films CT/MRI/X-Ray Films
Radiology
Solutions
Any Chemical used in
processing of Radiology
films
Testing – Strips E.g. Glucometer strips
used with a testing device
Testing – Kit A testing kit used without
any instrument for
diagnostic purpose
Category Category Name Sub-Categories Item Description
H Chemicals and
Anesthetic Gases
Antiseptic,
Disinfectants,
Dialysis solution
Plaster material
Halothane,
Sevoflurane,
Isoflurane
Phenyl, POP, Pt.
related and Hospital
disinfectant
Category Category Name Sub-Categories Item Description I INTERVENTIONAL Cardiology
Radiology
Stents, guide wires,
related consumables for
cath lab and
Interventional
procedures
5
Category Category Name Sub-Categories Item Description
J IMPLANTS and
DEVICES Implants and Devices related to Orthopedics, Dental and Physiotherapy
Screw, plates,
prosthesis, Hip and
Knee replacement, K-
wires and other
orthopedic consumables.
Dental appliances and
consumables.
Physiotherapy kits,
appliances
ii) Suppliers need to indicate on the enclosed proforma, the groups for which
empanelment is sought.
iii) Kasturba Hospital will call for tenders for the items in each group from empanelled
suppliers of that group. This procedure will be followed every year in April. It will
ensure that all suppliers of particular group item receive the Tender notification.
iv) Empanelment does not guarantee any other favorable treatment and neither does
assure receipt of orders. Tenders and / or quotations will be processed as per
procurement rules framed by Kasturba Health Society.
v) Empanelment applications will be received throughout the year. Any new suppliers
can register themselves, at any time of the year. Existing empanelled suppliers can
add more groups at any time by filling up modification form and paying requisite
fees. However if registration is done after last closing date of said year Tender, then
he will not be considered in current comparative list. Tenderer will be eligible for any
Tender which is released after successful registration.
vi) Kasturba Hospital will charge an empanelment fees of Rs. 1000/- only with
REFUNDABLE SECURITY AMOUNT of Rs 10,000/- per group. Empanelment fees
can be paid by Demand Draft drawn in favor of “Kasturba Health Society, Sevagram”
or by cash deposition in Account office, KHS. Any unpaid dues will be deducted from
the security amount. In event of supplier being blacklisted/found guilty of
malpractice, the security amount will be forfeited.
vii) All information called for in the enclosed Proforma should be furnished against the
relevant columns. Please attach separate sheet if the space provided is insufficient. All
columns in the form are to be filled up. If applicant has no information to be filled in a
particular column, “Nil” may be mentioned. In case of columns not relevant in the
applicant’s case, it should be stated as ‘Not-Applicable’. No column should be left

6
blank. Applications can also be sent by registered post. However it is the
responsibility of Tenderer to follow-up and ensure registration till the last step. It is
advisable to send authorized personal for completing the formalities.
viii) The application should be typewritten/printed. Overwriting should be avoided.
Correction, if any, should be made by neatly crossing out, initialing, dating and
rewriting.
ix) All sheets of the form are to be signed by the authorized signatory.
x) The application should invariably be accompanied by the “Undertaking” on the
prescribed format (Annexure –A) on a Rs 100/- stamp paper.
xi) Suppliers should furnish list of five largest orders executed in past three years in the
prescribed format (Annexure – B)
xii) The complete application document will be available as a hard copy from Medical
Stores, Kasturba Hospital Sevagram. This application form is available free of cost .
A soft copy of the application form can be sent by E-mail to suppliers on request.
Please make all such requests by E-mail, by sending a mail to
[email protected] or [email protected] with subject heading
“Request for Empanelment Form”
xiii) KH, Sevagram reserves the right to verify the performance of Vendors and to call for
any further information. Any information / clarification required during evaluation
must be given expeditiously. Failure to cooperate may affect registration.
xiv) Empanelment will be for a period of three years (April 2016 – 31st March 2019)
IRRESPECTIVE of date of empanelment, subject to satisfactory service. If the
service provided by the vendor is found to be unsatisfactory or if at any time it is
found that information furnished by the vendor is incorrect, then KH, Sevagram
reserves the right to remove such vendors from the empanelled list without giving any
notice to the vendor in advance.
xv) KH, Sevagram will evaluate the applications based on the set criteria and will choose
to short list qualified suppliers.
xvi) Decision of KHS, Sevagram with regard to preparation of panel of the Suppliers shall
be final. KHS, Sevagram is not bound to assign any reasons thereof.
xvii) KHS, Sevagram reserves the right to accept or reject any or all the applications
without assigning any reasons thereof and no correspondence in this regard shall be
entertained.

7
xviii) KHS, Sevagram shall not be responsible for any postal delay or loss in transit.
Incomplete applications may be rejected summarily.
3.0 Eligibility for Empanelment
i) Should be a reputed wholesaler and possess wholesale drug license from concerned
drug controller.
ii) Supplier should be registered and authorized stockiest/distributor/ dealer. In support,
the supplier should submit evidentiary proof along with the application document.
iii) The supplier should preferably be in existence for the last three years. In support,
the supplier should submit evidentiary proof along with the application document.
iv) The supplier should be registered with Central sale tax / State Sale tax/ VAT
registration number/ any other bodies, as applicable (Please attach documentary
proof).
v) An applicant should have neither failed to perform on any agreement nor should have
been expelled/debarred/black listed or banned during the last three years with KH,
Sevagram or Kasturba Health Society.
vi) Should be financially sound and the total annual turnover be adequate enough to
maintain uninterrupted supply. He should supply goods at Institutional rates
vii) Should have adequate storage facility and capability of bulk supplies including cold
storage as applicable.
viii) Manufacturers need not have Dealership certificate. It is always preferable and
advised that manufacturers should quote directly to our charitable Institution for
ensuring uninterrupted supply and cost-benefit to the patients.
ix) Acceptance of payment by Cheque.
x) Quality assurance protocol followed in manufacturing and/or supply of goods.
4.0 Documents to be submitted
The following documents duly attested & certified should be enclosed along with the
application :
i) Attested photocopy of registration certificates with Food and Drug Administrator
(FDA).
ii) Audited financial statements / balance Sheet for the past three years along with last
three years Income Tax and Sales Tax Returns.

8
iii) Attested Photocopy of registration with relevant tax authorities i.e. Income Tax
(PAN) No. : Service Tax No. : VAT Registration No. etc.
iv) Any Dealership authorization letters from pharmaceutical companies. This document
should be submitted in ORIGINAL on company letter head clearly showing outward
no. along with sign & name of competent authority.
5.0 Submission of Documents
The application form duly filled in shall be submitted in a sealed envelope super
subscribing “ Expression of Interest for Empanelment” addressed to
Incharge, Medical Stores
Dean Office complex
Kasturba Hospital, Sevagram
Dist: Wardha, Maharashtra – 442 102
Monday to Friday 9.00am to 4.00pm
Saturday 9.00am to 12.00pm
(Excluding Sunday and Holidays)

9
KASTURBA HOSPITAL, SEVAGRAM
SUPPLIER EMPANELMENT FORM
VALID FOR 2016 - 2019
Part – I Basic Information
1. Name of Firm :
Sole proprietor / Partnership: …...……………………………………
2. Name of owner/ Partners Signature
1. …...…………………………………….. …...……………………………………
2. …………………..…………………...… …...……………………………………
3………………….…………………...…… …...……………………………………
Recent passport size Photo (Sole / All Partners)
3. Contact Details
Address …………………………………………………………….……………….
Landmark……………..……………… City / Place……………….……………….
District………..………………..…………… State……………………….………
.
Pin ……………………………………..…
Phone (Land Line)………….………...………….
Mobile no. ….…………………….…………….
10
….…………………….…………….
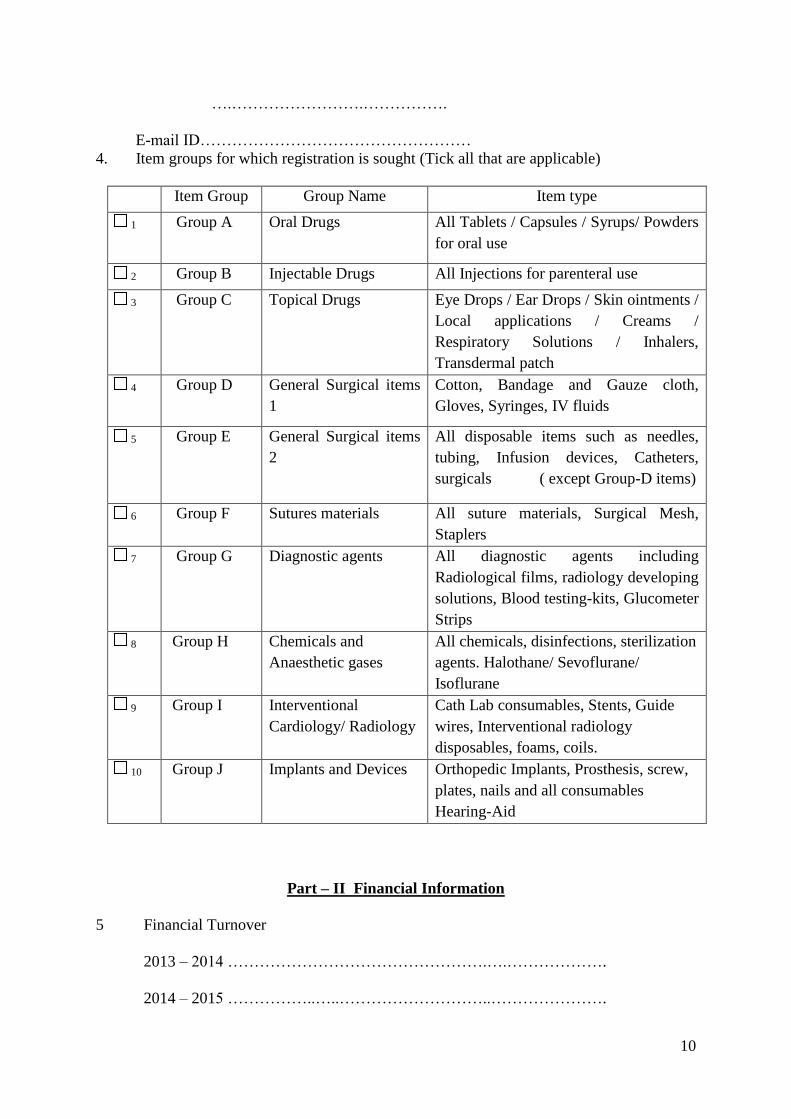
E-mail ID……………………………………………
4. Item groups for which registration is sought (Tick all that are applicable)
Item Group Group Name Item type
1 Group A Oral Drugs All Tablets / Capsules / Syrups/ Powders
for oral use
2 Group B Injectable Drugs All Injections for parenteral use
3 Group C Topical Drugs Eye Drops / Ear Drops / Skin ointments /
Local applications / Creams /
Respiratory Solutions / Inhalers,
Transdermal patch
4 Group D General Surgical items
1
Cotton, Bandage and Gauze cloth,
Gloves, Syringes, IV fluids
5 Group E General Surgical items
2
All disposable items such as needles,
tubing, Infusion devices, Catheters,
surgicals ( except Group-D items)
6 Group F Sutures materials All suture materials, Surgical Mesh,
Staplers
7 Group G Diagnostic agents All diagnostic agents including
Radiological films, radiology developing
solutions, Blood testing-kits, Glucometer
Strips
8 Group H Chemicals and
Anaesthetic gases
All chemicals, disinfections, sterilization
agents. Halothane/ Sevoflurane/
Isoflurane
9 Group I Interventional
Cardiology/ Radiology
Cath Lab consumables, Stents, Guide
wires, Interventional radiology
disposables, foams, coils.
10 Group J Implants and Devices Orthopedic Implants, Prosthesis, screw,
plates, nails and all consumables
Hearing-Aid
Part – II Financial Information
5 Financial Turnover
2013 – 2014 ………………………………………….….……………….
2014 – 2015 ……………..…..………………………..………………….

11
2015 – 2016 ………………………………………………………………
6. PAN/TIN Number ………………………………………………………..
7. CST/ST Number ……………………………….…………………………
8. VAT Registration ………………………………………………………..
9. VAT clearance upto ………………………………………………………
Part – III Enclosures
Enclosed documents (attach in following order)
1. Demand Draft amount Rs. ……………… No. …………………
dated ………………….. drawn on Bank …………………………… in favor of
KASTURBA HEALTH SOCIETY, SEVAGRAM. ( OR Cash payment at
“Accounts Dept., KHS, Sevagram)
2. Attested copy of Registration certificate with FDA
3. Copy of PAN Card of supplier
4. Audited financial statement / balance sheet for past three years along with last
three year sales tax + Income tax returns.
5. Copy of Sales Tax, VAT Registration. True copies of Sales Tax, VAT Clearance
certificate UPTO 31/03/2015.
6. Certified copy of deed of partnership and if required C&F Agreement from
manufacturer, power of attorney, if applicable.
7. Any dealership authorization letters from pharmaceutical companies. SUBMIT
ORIGINAL on manufacturing co. letter head duly signed by competent authority
displaying his name and designation with stamp along with outward no.
FOR OFFICE USE ONLY
The following items were checked and found to be in order.
1 Items and Empanelment fees amount Yes / No
2 Demand Draft / Cash receipt Yes / No
3 FDA Registration Yes / No
4 Tax assessment documents Yes / No
5 PAN Card Yes / No
6 Sales Tax documents Yes / No
7 VAT registration Yes / No
8 VAT clearance upto 31st March 2015 Yes / No
9 Others (specify)-
__________________________________________________________

12
__________________________________________________________
All certificates in order –
All mandatory license attached –
Fine due (if Any) -
Checked and found all clear.
Checked by ………………. ……………Ritesh Ambulkar………..Date …………..…….
(Signature) (Name)
All certificates in order –
All mandatory license attached -
Fine due (if Any) -
Dues – Paid / Unpaid
Checked and found all clear. No dues pending.
Incharge pharmacist
All certificates in order –
All mandatory license attached -
Fine due (if Any) -
Dues – Paid / Unpaid
Checked and found all clear. No dues pending.
Medical Officer Incharge

13
All Finance related certificates in order – Yes / No
Sales tax/VAT / Income tax related documents - Approved / Not approved
Remarks (in any) :
Checked and found all clear. No dues pending.
All finance/ Audit related documents are clear.
Incharge Accounts section
Registration Approved / Not approved
Remarks (if any)
Medical Superintendent
Complete details saved electronically in “SUPPLIER DATA BASE”
Correct and complete information entered in E-mail account of [email protected]
Demand Draft received and forwarded to accounts section
Mr. Pravin Wankhede
Pharmacist and Data operator

14
REGISTRATION PROCESS COMPLETED
ANNEXURE – A
(To be submitted on Rs. 100/- stamp paper)
UNDERTAKING
I/We have read, understood and accept Kasturba Hospital, Sevagram’s General Terms and
conditions contained in the application form. I/we do hereby declare that all the details
provided in this application form are true to the best of my / our knowledge and belief and
any misrepresentation of facts will render me/us liable to any action as may be deemed fit by
Kasturba Hospital, Sevagram
I/We, do hereby also accept that Kasturba Hospital has the right to accept or reject this
application and not to issue invitation to Tender/ Quotation to me/us.
I/We undertake to communicate promptly to Kasturba Hospital, Sevagram any changes in the
condition or working of the firm. It is certified that my/our Firm has NOT been found guilty
of malpractice, misconduct, nor blacklisted/ debarred by Public Health Department, Govt. of
Maharashtra / any local authority / other State Government, Central Government's
organizations. Also there are no police cases pending against us or our business in the country
which would render our firm as disqualified. The undersigned is fully authorized to sign and
submit this application, form on behalf of our organization. We authorize Kasturba Hospital,
Sevagram to approach individuals, employers, firms and corporations and any other as may
be deemed necessary to verify our competence and general reputation.
Signature _____________
Name _____________
Designation _____________
Address _____________
Seal _____________
Place _____________
Date _____________
Note: In partnership firms, all partners should sign

15
ANNEXURE – B
List of Largest Orders / Contracts Completed during the Last three years
Signature:
Name (in Block Letters):
Designation:
Seal of Company/ Supplier:
S.No
.
Name of the Product(s)
Name of
Client
Total cost of the
Project (In Rs.)
Completion Period
Scheduled Actual
Date
Date
i)
II)
III)
iv)
v)






















![[Mikrobiologi] It 5 - Coccus - Khs](https://img.pdfslide.us/doc/110x75/55cf920d550346f57b930bd5/mikrobiologi-it-5-coccus-khs.jpg)





