Embed Size (px)
Citation preview

For Easier Navigation Activate the “Previous View” tool on the Adobe “Page Navigation Toolbar.” To do this: 1. Right click on the toolbar. 2. In the drop down menu that appears, left click “More Tools.” 3. Scroll down to “Page Navigation Toolbar.” 4. Select the checkbox beside to “Previous View.” 5. Click “OK.”

Module: Perioperative assessment and care Topic: postoperative delirium and cognitive dysfunction Case #1: A 79-year-old man presents for elective open-repair of an asymptomatic 5 × 6 cm suprarenal abdominal aortic aneurysm. He has coronary artery disease with chronic stable angina of moderate severity (Canadian Heart Association Class III), hypertension, hyperlipidemia, anxiety, and ongoing tobacco use (1 PPD for 50 years). He drinks 2 highballs every night at dinner and a glass of wine at bedtime. He has no prior surgical history. He lives alone and states that he is able to perform routine house chores and push-mow his lawn. Medications include mirtazapine 7.5 mg qhs, trazodone 100 mg tid, quetiapine 25 mg q am and 50 mg qhs, bupropion 150 mg tid, simvastatin 40 mg qhs, HCTZ 25 mg q am, metoprolol 100 mg bid, and NTG sl 0.4 mg prn. On physical examination, the heart rate is 55 bpm. The blood pressure is 142/90 mmHg on the left and 170/77 mmHg on the right. Mild expiratory wheezing is present, but the remainder of the exam is unremarkable. The hemoglobin is 15.5 g/dl, serum urea nitrogen (SUN) 36 mg/dl, and creatinine 1.2 mg/dl. Other laboratory findings are normal. Question #1: Postoperatively in the intensive care unit, this patient is at highest risk for developing:
A. Delirium B. Myocardial infarction C. Deep venous thrombosis D. Atrial fibrillation E. Pneumonia
Answer A This patient has multiple risk factors for the development of postoperative delirium, including age >70 yrs, preexisting neuropsychological disorders, polypharmacy, SUN/creatinine ratio >18, vascular surgery, and potentially alcohol withdrawal (slide 1). Myocardial ischemia and infarction, arrhythmias, and pneumonia are also among the more frequent postoperative complications in older patients, particularly in those with preexisting cardiorespiratory disease. Although older patients with CAD undergoing major vascular surgery are at increased risk for perioperative cardiac events (slides 2-6), the risk is lower in this patient because he has a >4 METS symptom-free activity level and he is on high dose beta-blocker therapy (slide 7). In addition, the presence of uncontrolled hypertension is considered to be only a minor predictor of cardiac risk. While history of smoking, COPD, and upper abdominal surgery are independent risk factors for postoperative pulmonary events, the incidence of postoperative delirium (15-53% in older patients undergoing general surgery; 70-87% in those requiring admission to an ICU following surgery; Inouye et al) far exceeds the incidence of pneumonia (5.5-7%). Stasis of blood, decreased flow in the iliofemoral venous system, and a hypercoagulable state as a result of surgery, anesthesia and immobility in the postoperative period predispose the patient to deep venous thrombosis (DVT). However, prophylactic use of graded pneumatic compression boots and either unfractionated heparin or low molecular weight heparin in the ICU serve to lower the risk of thromboembolic complications. In the past, rates of asymptomatic DVT in patients undergoing general surgical procedures without thromboprophylaxis varied between 15% and 30%, while the rates of fatal pulmonary embolism ranged between 0.2% and 0.9%. The risk of venous thromboembolism (VTE) in contemporary general medical and surgical patients remains around 10% despite thromboprophylaxis. Other factors that may reduce the risk of VTE in current patients include improvements in general perioperative care, more rapid mobilization, and greater use of regional anesthesia. Although the performance of more extensive surgical procedures in older and sicker patients, as well as the use of preoperative chemotherapy and shorter lengths of stay in the hospital (leading to shorter durations of

thromboprophylaxis), may contribute to an increased risk for VTE in contemporary patients, this risk is still substantially less than the risk of postoperative delirium in elderly patients.
• Liu LL, Leung JM. Predicting adverse postoperative outcomes in patients aged 80 years or older. J Am Geriatr Soc 2000;48:405-12. This study looks at the importance of intraoperative versus preoperative risk factors in predicting adverse postoperative events in geriatric patients.
• Hamel MB, Henderson WG, Khuri SF, Daley J. Surgical outcomes for patients aged 80 and older: morbidity and mortality from major noncardiac surgery. J Am Geriatr Soc 2005;53:424-9.This is a large prospective study looking at morbidity and mortality in old and very old veterans’ postoperatively. They found that postoperative mortality at 30 days was greater in very old (over 80 years) vs. younger old patients; 8% vs. 3%. However for minor operations such as hernia repair or TURP the mortality rate was low (<2%) even in the oldest patients. Postoperative complications in the oldest patients were associated with a higher 30 day mortality.
• Leung JM, Dzankic S. Relative importance of preoperative health status versus intraoperative factors in predicting postoperative adverse outcomes in geriatric surgical patients. J Am Geriatr Soc 2001;49:1080-5. Age was not found to be a significant predictor of postoperative adverse events in this elderly population who were followed in the hospital after surgery, (not outpatients). The severity of preoperative comorbidities and ASA classification, need for emergency surgery, and intraoperative tachycardia were predictive.
• Prevention of Venous Thromboembolism*American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) William H. Geerts, MD, et al. Chest. 2008; 133:381S-453
• Inouye SK. Delirium in older persons. N Engl J Med 2006;354:1157-65. A recent review of delirium in medical and surgical patients. It provides a general overview of severity of the problem, its consequences and predictors, as well as strategies for its prevention and treatment.
• Dasgupta M, Dumbrell AC. Preoperative risk assessment for delirium after noncardiac surgery: a systematic review. J Am Geriatr Soc 2006;54:1578-89. An excellent systematic review of the risk factors for postoperative delirium.
• Cook D, Crowther M, Meade M, Deep venous thrombosis in medical-surgical critically ill patients. Prevalence, incidence, and risk factors. Crit Care Med 2005; 33: 1565-71.
Case 1 continued Two days following an uneventful surgical procedure performed under general anesthesia, the patient although hemodynamically stable becomes disoriented, pulls out his intravenous lines, and tries to get out of bed. His heart rate is 82/min and blood pressure 142/68 mmHg. The cardiopulmonary and neurological examinations are unremarkable. Question #2. The most likely cause of postoperative delirium in this patient is:
A. impaired central nervous system perfusion due to cross-clamping of the aorta during surgery
B. alcohol withdrawal C. preoperative use of multiple psychotropic medications D. inadequate pain control E. general anesthesia
Answer C The most likely cause of this patient’s delirium is polypharmacy and drug interactions (slide 8). Underlying depression and anxiety are also among the most likely factors that predispose this patient to perioperative delirium (slides 1 and 9). Given his hyperactive presentation, alcohol withdrawal and inadequate pain control should also be suspected. However, the lack of hemodynamic signs of sympathetic arousal (i.e. tachycardia, hypertension) makes these causes less likely. Vascular surgery

is associated with an increased risk for delirium due to hypoperfusion related to cross-clamping of the aorta or atherosclerotic emboli, but these factors are less frequently the cause of delirium than drug-related side effects. Importantly, choice of anesthesia, i.e. general or regional, does not affect the predisposition to postoperative confusion in older patients.
• Lepouse C, Lautner CA, Liu L, Gomis P, Leon A. Emergence delirium in adults in the post-anaesthesia care unit. Br J Anaesth 2006;96:747-53. This is a prospective study addressing the incidence of and risk factors for emergence delirium in elderly patients. The authors enrolled over 1200 patients and found that preoperative benzodiazepines, and long surgeries were two of several risk factors for emergence delirium.
• Marcantonio ER, Goldman L, Orav EJ, Cook EF, Lee TH. The association of intraoperative factors with the development of postoperative delirium. Am J Med 1998;105:380-4.
• Marcantonio ER, Juarez G, Goldman L, Mangione CM, Ludwig LE, Lind L, Katz N, Cook EF, Orav EJ, Lee TH. The relationship of postoperative delirium with psychoactive medications. JAMA 1994;272:1518-22.
• Williams-Russo P, Sharrock NE, Mattis S, et al. Randomized trial of hypotensive epidural anesthesia in older adults. Anesthesiology 1999; 91(4):926-935.
• Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validated and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA 2001;286(21):2703-2710.
Question #3: Which statement about cognitive dysfunction following major noncardiac surgery in older patients is true?
A. The Mini-Mental State Examination is recommended for detecting postoperative cognitive dysfunction. B. Up to 25% of older patients develop cognitive dysfunction within one week after surgery. C. Postoperative cognitive dysfunction is more common in women than in men. D. Compared to general anesthesia, regional anesthesia reduces the risk of postoperative cognitive dysfunction. E. Up to 50% of patients who demonstrate early postoperative cognitive dysfunction (within one week) have persistent cognitive dysfunction at 6 months.
Answer B It is important to distinguish between an acute confusional state (i.e. delirium), a reversible state associated with injury or surgery (e.g. postoperative cognitive dysfunction or POCD) and a chronic brain syndrome, such as dementia (slide 10). The latter exists before surgery but may be exacerbated by the procedure. The most important risk factor for POCD is advancing age (slide 11). Among octogenarians undergoing general anesthesia, the incidence of POCD at 1 week has been reported to be as high as 25%, compared to 3% in octogenarians who did not receive a general anesthetic. At 3 months follow-up, 10% of these patients have persistent cognitive impairment (slide 12). In most patients neurocognitive function returns to baseline or near baseline by 6 months after surgery. In addition to older age, risk factors for early POCD (within 1 week of major noncardiac surgery) include increased duration of anesthesia, lower education level, re-operation, and respiratory complications (slide 11). At 3 months, older age is the only significant risk factor for persistent POCD. While major surgery increases the risk of POCD in older patients, general anesthesia alone does not. Specifically, studies have shown that cognitive function between 1 and 6 months after surgery is similar in patients undergoing general or regional (i.e. spinal or epidural) anesthesia. Mental status screening instruments, such as the Mini-Mental State Examination (MMSE; link to MMSE and Mini-Cog), are useful for assessing cognitive function in the general population, but are insensitive for detecting subtle changes in cognition that may occur in the perioperative setting. Accurate evaluation for POCD requires a

battery of neuropsychological tests at baseline and again following surgery. In most cases, such testing is not clinically indicated, so that the diagnosis of POCD is largely empiric based on physician assessment with input from the patient’s family.
• Williams-Russo P, Sharrock NE, Mattis S, Szatrowski TP, Charlson ME. Cognitive effects after epidural vs general anesthesia in older adults. A randomized trial. JAMA 1995;274:44-50. A classic article addressing cognitive dysfunction in elderly patients undergoing knee replacement surgery. The authors found no difference between the two groups.
• Morley JE, Haren MT, Rolland Y, Kim MJ. Frailty. Med Clin North Am 2006;90:837-47. This is a landmark international prospective study investigating the effects of general anesthesia and general surgery on long term cognitive performance in elderly patients using neuropsychometric testing.
• Silverstein JH, Timberger M, Reich DL, Uysal S. Central nervous system dysfunction after noncardiac surgery and anesthesia in the elderly. Anesthesiology 2007;106:622-8. An outstanding summary of the broad topic of postoperative central nervous system dysfunction.
• Bass DS, Attix DK, Phillips-Bute B, Monk TG. An efficient screening tool for preoperative depression: the Geriatric Depression Scale-Short Form. Anesth Analg. 2008 Mar;106(3):805-9.
• Monk TG, Weldon BC, Garvan CW, Dede DE, et al. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology. 2008 Jan;108(1):18-30.
• Price CC, Garvan CW, Monk TG. Type and severity of cognitive decline in older adults after noncardiac surgery. Anesthesiology. 2008 Jan;108(1):8-17.
• Rudolph JL, et al. Delirium is associated with early postoperative cognitive dysfunction. Anaesthesia. 2008
Sep;63(9):941-7 Key Point: Older patients with multiple comorbid illnesses, functional limitations, cognitive impairment, and/or frailty are at increased risk for perioperative morbidity and iatrogenic complications, and these factors should be considered in assessing the overall operative risk. Key Point: Postoperative delirium occurs in 15-53% of older surgical patients, including 70-87% of those in the intensive care unit, and it is associated with increased postoperative morbidity, mortality, and length of hospital stay. Key Point: Patients with known coronary artery disease or major cardiovascular risk factors should receive perioperative beta-blockade, but preoperative cardiac testing and prophylactic coronary revascularization are generally not recommended in the absence of worsening symptoms or hemodynamic instability. Key Point: Age-related changes in the cardiovascular system, lungs, kidneys, and central nervous system diminish reserve capacity and greatly increase the risk of perioperative complications, both cardiac and noncardiac, especially in patients over 80 years of age. ---------------------------------------------------------------------------------------------------------- Additional Content (corresponding slides in “blue”) The safety of surgery has been improving steadily and the risk for complications and mortality has been declining steadily over the past 30 years as anesthetic and surgical techniques and hospital care have improved. Nonetheless, with increasing age and accumulated chronic diseases, physiologic reserves decline, leaving older individuals at greater risk for adverse clinical outcomes under conditions of stress. The stress of surgery and anesthesia is great and can have profound effects on high-risk elders. Even though mortality and complication rates increase dramatically with age in patients undergoing

noncardiac surgery (slides 4 and 5), coexisting diseases and surgical urgency are the most significant factors associated with poor outcome (slides 5 and 6). Postoperative delirium is one of the most common adverse outcomes in the older surgical patient. Delirium is a syndrome of disturbed consciousness, attention, and cognition or perception, which develops acutely and fluctuates during the course of the day (slides 13-16). Delirium is present in 22% to 31% of elderly, hospitalized patients; 15% to 53% of postoperative geriatric patients and in 70% to 87% of those in intensive care (slides 18 and 19). There are many preoperative, intraoperative and postoperative precipitating factors for postoperative delirium (slides 9, 17, 20, 21). Delirium usually presents during postoperative days 1-4, often following a lucid interval. Postoperative delirium presents in three forms: hyperactive, hypoactive and mixed (slide 24). Roughly 25% will present as the readily apparent hyperactive delirium with confusion, agitation, and combative behavior. Another quarter will present as hypoactive delirium, which is characterized by calm and withdrawn appearance, clouded attention, and reduced mobility. About half will demonstrate a combination of both hyperactive and hypoactive features. Postoperative delirium has traditionally been considered a temporary or transient phenomenon but it can last for days to weeks after the procedure, extend hospital length of stay, increase costs, and may even be a marker for subsequent cognitive deterioration and a predictor for mortality (slides 22, 23, 25). Identify precipitants of delirium • Preoperative factors associated with postoperative delirium include age >70 yrs, preexisting
cognitive impairment, a history of delirium, depression, visual impairment, diabetes, poor nutritional and functional status, polypharmacy (more than six medications or 3-4 new inpatient medications), and drugs with anti-cholinergic properties that cross the blood brain barrier.
The Mini-Mental Status Examination (MMSE; LINK to MMSE) is a widely accepted instrument to screen for dementia; however, it is often too time-consuming for use in busy preoperative clinics. The Mini-Cog (slide 26) is a more recently developed tool used to screen for dementia that can be performed in less than 5 minutes. While it has a sensitivity and specificity similar to the MMSE and to formal neuropsychological tests for detecting dementia, the Mini-Cog has not been used in a surgical population. In brief, it consists of three-item recall and a clock-drawing test.
Mini-Cog ↓ 3-item recall=0 3-item recall=1-2 3-item recall=3 Recalls none of the words Recalls 1-2 of words Recalls all 3 words
Demented Not-Demented
Abnormal Clock Draw Test (CDT) Normal Clock Draw Test Mini-Cog scoring algorithm (Borson, et al, p 1024). From Borson, S., Scanlan, J., Brush, M., Vitallano, P., & Dokmak, A. (2000). The Mini-Cog: A cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psych; 15(11), 1021-1027. Copyright John Wiley & Sons Limited. Reproduced with permission. http://www.hospitalmedicine.org/geriresource/toolbox/pdfs/clock_drawing_test.pdf),

• Intraoperative factors affecting postoperative delirium include type of surgical procedure (orthopedic, cardiac, thoracic, major vascular, emergency, and organ transplantation operations), excessive blood loss, excessive fluid administration, and hypotension. Importantly, there is no relationship between anesthetic technique and incidence of postoperative delirium.
• Postoperative factors associated with delirium include use of physical restraint, bladder catheterization, more than three new (and precipitative initiation) medications during hospitalization, uncontrolled pain, anemia, prolonged bed rest, poor fluid or glycemic status, sleep deprivation or sensory overload (Intensive Care Unit)
Diagnosis of delirium Given that the presentation of postoperative delirium is heterogenous, it is often misdiagnosed or not identified. The hypoactive form is more common in elderly patients, in whom it is often misdiagnosed as dementia. Thus, enhanced awareness of the variable presentation and fluctuating course should improve diagnostic sensitivity. A widely used diagnostic tool for delirium is the Confusion Assessment Method (CAM) (slide 16). However, this tool was developed for use in patients in a general medicine ward or outpatient setting, thus its interpretation in context of surgery and anesthesia may be difficult. For example, using it in the early postoperative period may identify patients as delirious when they are still under the influence of anesthetic agents. Whether delirium in that circumstance is prognostic of outcome in the same way as delirium that occurs after the effects of anesthetics have subsided remains unclear. Interestingly, there is evidence that, in hip fracture surgery patients, a positive CAM 60 minutes after discontinuation of volatile anesthesia predicts later postoperative delirium (Sharma Anesth Analg 2005; 101:1215). Another variant of the CAM, the CAM-ICU, has been validated for delirium assessment of intubated, nonverbal patients in an intensive care unit. Management (slides 27 and 28).
• Prevention: Among the modifiable factors, type of anesthesia has not been shown to affect delirium risk. Specifically, there is no benefit of regional or neuraxial (spinal or epidural) anesthesia over general anesthesia on risk of postoperative neurologic dysfunction. However, certain anesthetic adjuvants such as benzodiazepines and anticholinergic drugs may increase the risk of delirium. Anticholinergic drugs that cross the blood brain barrier, such as atropine and scopolamine, are thought to reduce cholinergic neurotransmission in the already compromised elderly brain. Pain is another contributing factor to postoperative delirium. Elderly patients with undertreated postoperative pain are nine times more likely to develop delirium than those adequately treated. The specifics of pain treatment, except for use of meperidine, are less important as long as pain is controlled. Meperidine should be avoided as accumulation of toxic metabolites and/or its anticholinergic activity has been associated with delirium. Because there is a possibility that the way we interpret pain in elderly patients may be deficient, a robust and objective way of evaluating pain is needed to deliver good perioperative care. When words fail to describe pain, nonverbal cues, such as facial expression or behavior, become important.
• Treatment of delirium:
Nonpharmacologic Once diagnosed, the focus should be on treatment of underlying medical conditions and/or discontinuation of toxic medications. Attention should also be directed at creating a calm environment populated with familiar faces, provide a board with names of care-team members, and reorient frequently to surroundings. Minimal use of immobilizing equipment is essential. Also ensure that glasses and hearing aids are worn. Further, pre- and postoperative geriatric consultations have been shown to decrease the incidence of delirium by as much as 30%.

Pharmacologic Pharmacotherapy has a place in the management in agitated delirium in the elderly postsurgical patient but one should resort to it only after seeking and treating remediable medical or pharmacologic causes of delirium. Abiding by the geriatrician’s rule to “start low and go slow”, low-dose haloperidol (starting dose, 0.5 mg b.i.d.) can be considered. Risperidone (0.25 mg q day) or olanzapine (2.5 mg q day) have also been used but lack clinical studies to demonstrate superiority. As discussed previously, three or more new inpatient medications are an independent factor for precipitating delirium. Accordingly, discontinuation of medications should be considered, if feasible. Also, sedatives prescribed for sleep, such as diphenhydramine, can increase the risk of delirium. Meperidine, but not other opioids, triples the risk. Lorazepam and other benzodiazepines used for anxiolysis can further lead to a disinhibition and a paradoxical agitated state.
LINK TO: Merck Manual of Geriatrics. Chapter 39 Delirium http://www.merck.com/mkgr/mmg/sec5/ch39/ch39a.jsp LINK TO: http://www.americangeriatrics.org/specialists/NewFrontiers/chapter.asp?ch=15 Additional Content for POCD To establish a preoperative diagnosis of cognitive impairment, there should be a corroborative history from the patient’s primary physician or nursing home. While mental status exams are useful for detecting baseline dementia, they are usually not sensitive enough to detect some of the subtle cognitive changes that can occur after surgery. Nonetheless, the existence of mild cognitive impairment at baseline, evidenced by minor abnormalities on the MMSE or Clock Drawing Test, are important to note because such patients are prone to develop acute confusion or delirium after surgery/anesthesia. http://www.hospitalmedicine.org/geriresource/toolbox/pdfs/clock_drawing_test.pdf), http://www.merck.com/mkgr/mmg/tables/39t2.jsp

Independent Predictors andPostoperative Delirium FoPostoperative Delirium Fo
Marcantonio. JAMA 1994;271:134-139Variable Odd
Age ≥ 70 yrs 3.3 (
Alcohol ab se 3 3 (Alcohol abuse 3.3 (
TICS score <3* 4.2 (
SAS class IV* 2.5 (
Markedly abnormal preop 3.4 (Markedly abnormal preop Na+, K+, glucose
3.4 (
Aortic aneurysm surgery 8.3 (
Noncardiac thoracic surgery 3.5 (
P ti t ith 0 1 2 d ≥ 3 i t h 2% 11%Patients with 0, 1-2, and ≥ 3 points have a 2%, 11%,indicates Telephone Interview for Cognitive Status (indicates specific activity level (class IV represents sor > 150mmol/L; K+ <3.0 or >6.0 mmol/L, glucose
d Clinical Prediction Rule for llowing Noncardiac Surgeryllowing Noncardiac Surgery
ds Ratio (95% C.I.) Points
(1.9-5.9) 1
(1 4 8 3) 1(1.4-8.3) 1
(2.4-7.3) 1
(1.2-5.2) 1
(1.3-8.7) 1(1.3 8.7) 1
(3.6-19.4) 2
(1.6-7.4) 1
d 50% i k f d li i ti l TICS and 50% risk of delirium, respectively. TICS (scores < 30 suggest cognitive impairment). SAS severe physical impairment). Abnormal Na+ (<130 <60 or >300 mg/dl)

Revised Cardi
Independent predictors of carLee TH, et al. Circulation
● Independent predictors of car(MI, pulmonary edema, Vfib, card
Hi h i k *– High risk surgery*– History of ischemic HD
History of CHF*– History of CHF*– History of Cerebrovascular ds– Insulin therapyInsulin therapy– Serum creatinine > 2.0 mg/dL
● 0, 1, 2, or > 2 predictors assorates of 0.5%, 1.3%, 3.6%, 9
iac Risk Index
rdiac complications1999;100:1043-1049
rdiac complicationsdiac arrest, complete heart block)
ociated with cardiac complication .1%, respectively

Surgery-Specific Cardiac Ris(2007 AHA/AC(2007 AHA/AC
High (risk > 5%)Emergent major surgery, particulaAortic and other major vascular (sPeripheral vascularPeripheral vascular
Intermediate (risk 1 to 5%)Carotid endarderectomyHead and neck Intraperitoneal and intrathoracicOrthopedicOrthopedicProstate
Low (risk < 1%)( )Endoscopic proceduresSuperficial proceduresCataract surgeryBreast surgery
k for Noncardiac Procedures CC guidelines)CC guidelines)
arly in elderly (2002 AHA/ACC guidelines)uprainguinal, abdominal or thoracic)

Major postoperative compmortality in patients un
surg
Polanczyk, C. A. et. al. Ann I
plications and in-hospital ndergoing noncardiac gery
ntern Med 2001;134:637-643

Preoperative clinical corrcomplicompli
Polanczyk, C. A. et. al. Ann
relates and postoperative cationscations
n Intern Med 2001;134:637-643
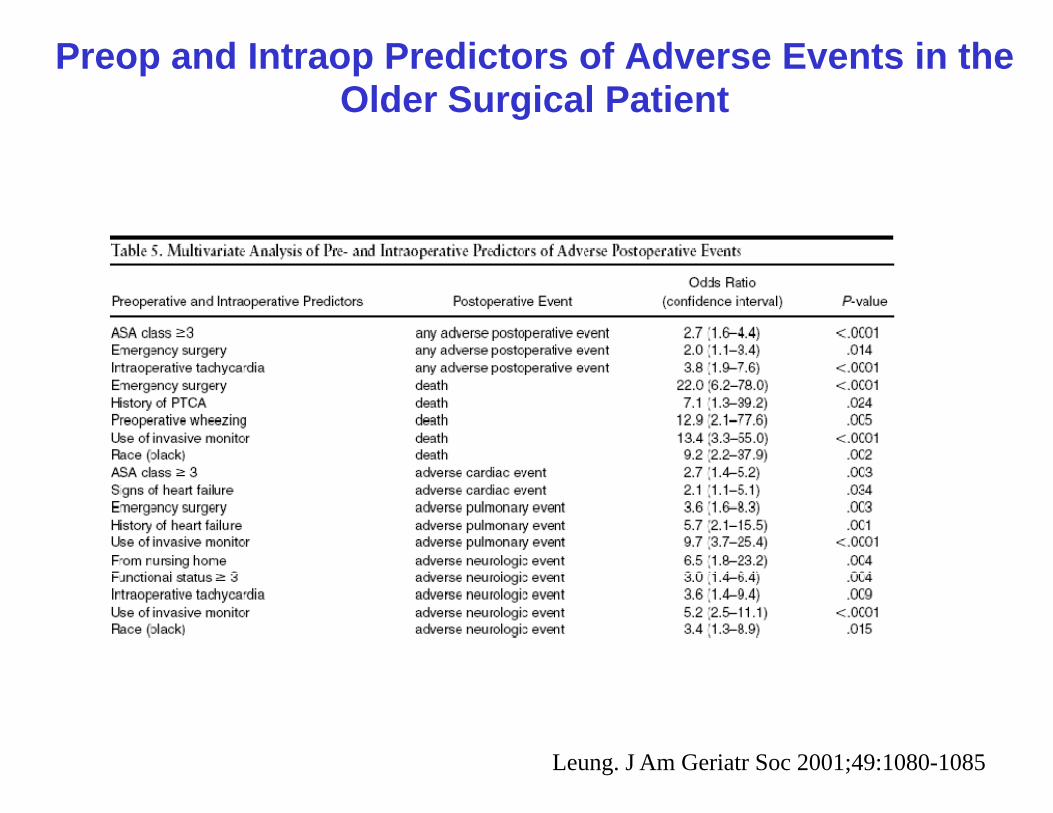
Preop and Intraop PredictoOlder SurgOlder Surg
ors of Adverse Events in the gical Patientgical Patient
Leung. J Am Geriatr Soc 2001;49:1080-1085

Perioperative Beta Blocafter noncarafter noncar
ckade and Cardiac Risk rdiac surgeryrdiac surgery
J Am Coll Cardiol. 2008 May 20;51(20):1913-24

Selected Drugs
http://www.merck.com/mkgr
s and Delirium
r/mmg/sec5/ch39/ch39a.jsp

PREDISPOSIN
● Advanced age
● Dementia, Anxiety, De
● Functional impairmen● Functional impairmen
● Medical comorbidity
● History of alcohol abu
● Male sex
↓● Sensory impairment (↓
From Delirium. GRS 6th edition. Am Geriat
NG FACTORS
epression
t in ADLst in ADLs
use
↓ ↓↓ vision, ↓ hearing)
tr Soc.

Predisposing factors/vulnerabilityvulnerability
High vulnerabilityS d tiSevere dementia
Severe illness
Multi-sensoryimpairment
Healthy, fit elderWithout chronic
conditionsLow vulnerability
conditions
Inouye, SK. J Geriatr Psychiatry Neurol 1998;11
Precipitating factors/insultsinsults
Noxious insultMajor s rgerMajor surgeryICU stay
M l i h iMultipe psychoactivemedications
Sleep deprivation
One dose of sleepingmedication
Not noxious insult:118

Delirium vsDelirium vs
http://www.merck.com/mkgr
s. Dementias. Dementia
r/mmg/sec5/ch39/ch39a.jsp
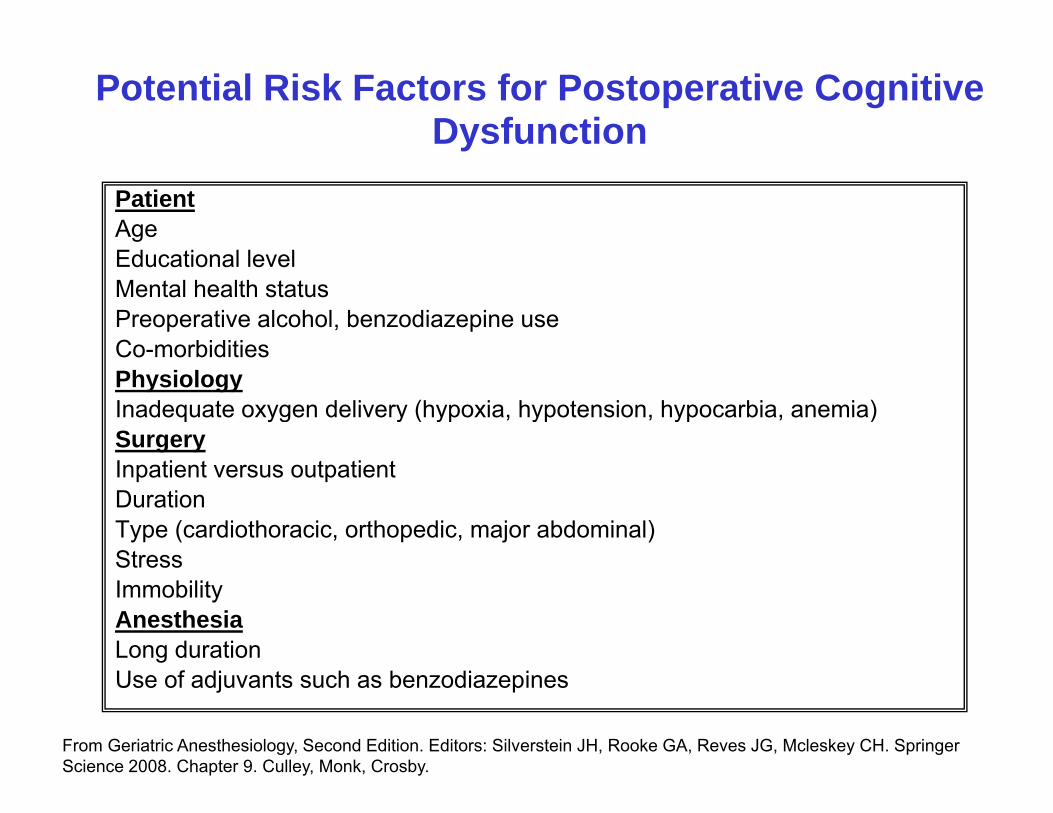
Potential Risk Factors foDysfu
PatientAgeEducational levelMental health statusPreoperative alcohol, benzodiazepine uCo-morbiditiesPhysiologyInadequate oxygen delivery (hypoxia hInadequate oxygen delivery (hypoxia, hSurgeryInpatient versus outpatientDurationDurationType (cardiothoracic, orthopedic, majorStressImmobilityAnesthesiaLong durationUse of adjuvants such as benzodiazepi
From Geriatric Anesthesiology, Second Edition. Editors: SilveScience 2008. Chapter 9. Culley, Monk, Crosby.
or Postoperative Cognitive unction
use
hypotension hypocarbia anemia)hypotension, hypocarbia, anemia)
r abdominal)
ines
erstein JH, Rooke GA, Reves JG, Mcleskey CH. Springer

International Study of PyDysfunctio
Cognitive Deficit in older surgsurg
• 25% of patients > 60 yrs, p y ,
• 10% of patients > 60 yrs,
• 14% of patients > 70 yrs,
L t 1998 351(9106) 857 61Lancet 1998;351(9106):857-61.Acta Anaesthesiol Scand 2000;44(10)
Post-Operative Cognitive p gn (ISPOCD)
persons after non-cardiac gerygery
1 week after surgeryg y
3 months after surgery
3 months after surgery
):1246-51

DiagnosinDSM-IV DIAGNO
Dist rbance of conscio sne● Disturbance of consciousnefocus, sustain, or shift atten
● Change in cognition (eg, melanguage disturbance) or a pbetter acco nted for b e isbetter accounted for by exis
● Development over a short ti● Development over a short tifluctuation during the day
● Evidence from history, physdisturbance is a direct physmedical condition or a drugmedical condition or a drug
From Delirium. GRS 6th edition. Am Geriat
g DeliriumOSTIC CRITERIA
ess ith red ced abilit toess with reduced ability to ntion
emory deficit, disorientation, perceptual disturbance not sting dementiasting dementia
me (hours to days) andme (hours to days) and
sical, or labs that the iologic consequence of a
tr Soc.

CONFUSION ASSECONFUSION ASSE
1 A t h i1. Acute change in fluctuatin
+2. Ina
+
3. Disorganized gthinking
Diagnosis of delirium requires feaDiagnosis of delirium requires fea
Inouye SK. Ann Intern Med. 1990;113:941
ESSMENT METHODESSMENT METHOD
t l t t ithmental status with ng course
+ttention
+
4. Altered level of consciousness
atures 1 and 2 as well as 3 or 4atures 1 and 2 as well as 3 or 4
Ely EW. JAMA 2001;286:2703

Confusing AssessFeature Question
1 Acute onset or fluctuating course
Evidence of astatus from t
Did the behaDid the behapast 24 hour
2 Inattention Did the patieattention?attention?
3 Disorg. Thinking
Is the patientincoherent?
4 Altered level of Overall how4 Altered level of consciousness
Overall, howpatient’s leve
Not alert BUTor comaor coma.
The Confusion Assessment Method li i Th di i f d li idelirium. The diagnosis of deliriumeither 3 or 4. (Inouye SK, et al. ClaAssessment Method: A New MethoIntern Med 1990;113:941-48)
sment Method (CAM)Present
an acute change in mental the baseline?
avior fluctuate during the
Y or N
avior fluctuate during the rs?ent have difficulty focusing Y or N
t’s thinking disorganized or Y or N
w would you rate the Y or Nw would you rate the el of consciousness?
T vigilant, lethargic, stupor
Y or N
d is a protocol for identifying i f t 1 d 2 lm requires features 1 and 2 plus
arifying Confusion: The Confusion od for Detection of Delirium. Ann

Potential History
Evaluatioo e
precipitants o y
Drug toxicity Review all current medications
Drug withdrawal Ask about alcohol or benzodiazepine or opioid misuse
Urinary retention/catheterization
Review ‘ins and outs’
Volume depletion or Review ‘ins andVolume depletion or overload
Review ins and outs’
Hypoxia
Hypoperfusion
Infection
Electrolyte/Metabolic imbalance
Adapted from Aging Issues in Cardiology. Edited by I.D. Turpie and G.A. Cardiac Patients. 2004.
Physical exam Lab
n of Deliriumys c e b
tests/imaging
Look for signs of sympathetic arousal
Suprapubic mass? In/out catheterization/ flush foley
Assess volume status BUN creatinineAssess volume status BUN, creatinine, electrolytes, CVP, LVEDP, echo
Pulse oximetry ABG
VS, cool extremities, urine output
Hemodynamics, ECG
Temperature CBC, U/A, CXR
Electrolytes, glucose
Heckman. Kluwer Academic Publishers. Chapter 2. Delirium in Elderly

INCIDENCE OF DELDERLY PAT
1/3 of older patien
ELDERLY PAT
● 1/3 of older patienthe ED
● 1/3 of inpatients apmedical units, hadelirious on admi
From Delirium. GRS 6th edition. Am Geriat
DELIRIUM AMONG TIENTS IS HIGH
nts presenting to
TIENTS IS HIGH
nts presenting to
aged 70+ on general g glf of whom are ission
tr Soc.

INCIDENCE & RISKS FDELIRDELIR
50%50%
15%
Noncardiacsurgery
Cardiac s
From Delirium. GRS 6th edition. Am Geriat
FOR POSTOPERATIVE RIUMRIUM
% 50%% 50%
surgery Hip fracturerepair
tr Soc.

INCIDENCE & RISKS FDELIRDELIR
Increased risk with preoperativrisk factors:
AgeCognitive impairmentCognitive impairmentPhysical functional impairmentHistory of alcohol abuseAbnormal serum h i t i
1chemistriesIntrathoracic and aortic aneurysm surgeryaneurysm surgery
Fro
FOR POSTOPERATIVE RIUMRIUM
50%
ve
50%
10%
or 2 risk factors 3+ risk factors
om Delirium. GRS 6th edition. Am Geriatr Soc.

PRECIPITATINAcute cardiac events• Acute cardiac events
• Acute pulmonary eventsevents
• Bed rest• Drug withdrawal• Drug withdrawal
(sedatives, alcohol)• Fecal impactionp• Fluid or electrolyte
disturbances• Indwelling devices
From Delirium. GRS 6th edition. Am Geriat
NG FACTORSI f ti (• Infections (esp. respiratory, urinary)M di ti• Medications
• Restraints • Severe anemia• Uncontrolled pain• Urinary retention
tr Soc.
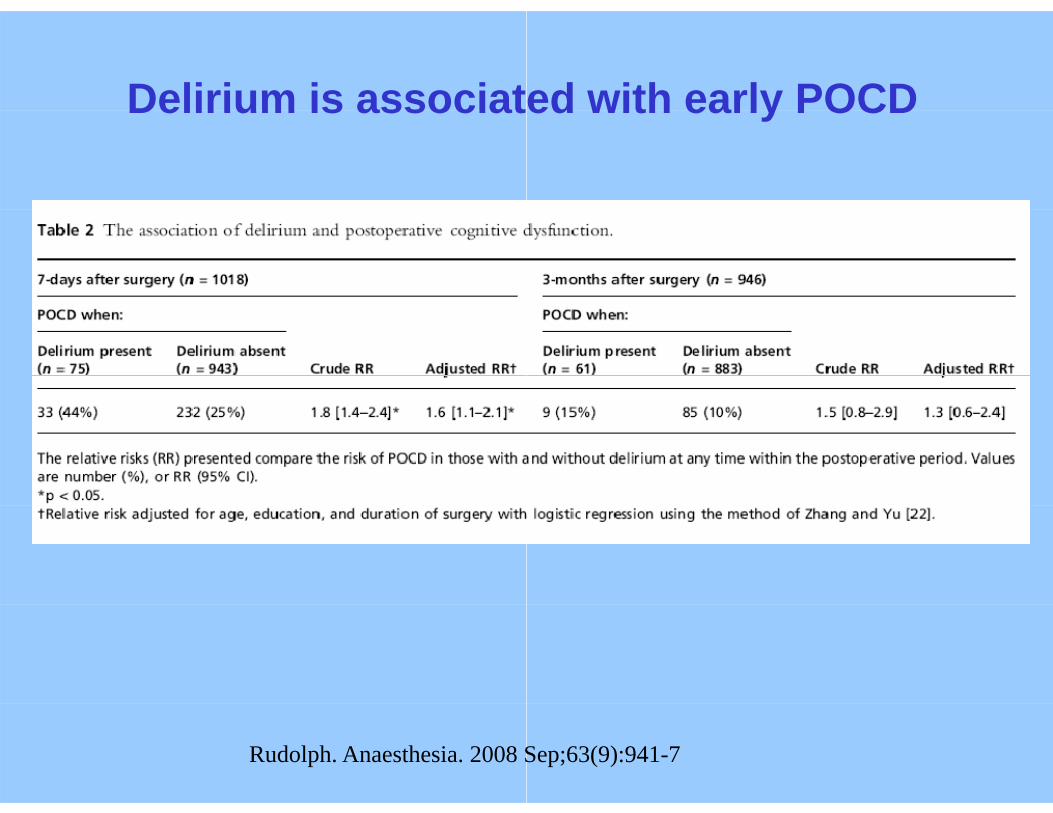
Delirium is associatDelirium is associat
Rudolph. Anaesthesia. 2008 S
ed with early POCDed with early POCD
Sep;63(9):941-7

Duration of DeliriumDuration of Delirium
Rudolph.Anaesth
m and early POCDm and early POCD
hesia. 2008 Sep;63(9):941-7

DELIRIUM TAKES
• Hyperactive or agitatecases
• Mixed
• Hypoactive delirium =less recognized and a
• Additional features incpsychosis, hallucinatip y ,
From Delirium. GRS 6th edition. Am Geriat
VARIOUS FORMS
ed delirium = 25% of all
= ≥50% of all cases, but appropriately treated
clude emotional lability, ions
tr Soc.

MORBIDITY AWITH DEWITH DE
• 10-fold risk of death in ho
• 3 to 5 fold ↑ risk of nosoc• 3- to 5-fold ↑ risk of nosocprolonged stay, postacute
• Poor functional recovery years following discharge
• Persistence of delirium →
From Delirium. GRS 6th edition. Am Geriat
ASSOCIATEDELIRIUMELIRIUM
ospital
comial complicationscomial complications, e nursing-home placement
and ↑ risk of death up to 2 e
→ poor long-term outcomes
tr Soc.

Mini -ADMINISTRATION
The test is administered as follows:
Mini
The test is administered as follows:1. Instruct the patient to listen carefully to and
the words.
2 I t t th ti t t d th f f l2. Instruct the patient to draw the face of a clocwith the clock circle already drawn on the paclock face, ask him or her to draw the hands
3. Ask the patient to repeat the 3 previously sta
SCORING
• Give 1 point for each recalled word after the• Patients recalling none of the three words ar• Patients recalling all three words are classif• Patients with intermediate word recall of 1-2Patients with intermediate word recall of 1 2
= demented;• Normal = non-demented)• Note: The CDT is considered normal if all nu
position and the hands display the requesteposition, and the hands display the requeste
- CogCog
remember 3 unrelated words and then to repeat
k ith bl k h t f h tck, either on a blank sheet of paper or on a sheet age. After the patient puts the numbers on the s of the clock to read a specific time.
ated words.
CDT distractor.re classified as demented (Score = 0).ied as non-demented (Score = 3)
2 words are classified based on the CDT (Abnormal2 words are classified based on the CDT (Abnormal
umbers are present in the correct sequence and ed timeed time.

Keys to Prevention
● Treat the underlying disea
● Address contributing fact
● Avoid the complications oRemove indwelling deviPrevent or treat constipEvaluate and treat painEncourage proper sleep
● Optimize medication regim
From Delirium. GRS 6th edition. Am Geriat
n and Management
ase
tors
of delirium:ices ASAPation and urinary retention
p hygiene, avoid sedatives
men (avoid polypharmacy)
tr Soc.

Nonpharmacolop
Use orienting stim li (clocks● Use orienting stimuli (clocks
● Provide adequate socializati● Provide adequate socializati
● Use eyeglasses and hearing
● Mobilize patient as soon as
● Ensure adequate intake of nfeeding if necessaryfeeding if necessary
● Educate and support the pat
From Delirium. GRS 6th edition. Am Geriat
ogic Managementg g
s calendar radio)s, calendar, radio)
ionion
g aids appropriately
possible
nutrition and fluids, by hand
tient and family
tr Soc.