Embed Size (px)
Citation preview

Cristina Fuss, M.D., Joseph L. Whetstone, M.D., Dianna M. E. Bardo M.D. Department of Radiology
Oregon Health & Science University – Doernbecher Children’s Hospital
Common Surgical Procedures
for Congenital Heart
Disease

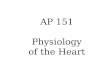
All structures of the L heart, LA, MV, LV, and AoV as well as the AAo (arrow) are small. In utero & in early postnatal period systemic and coronary blood supply is through the PDA. Surgical repair consists of a Norwood 3-staged palliation beginning as a neonate, usually ending by 5 years of age. High neonatal pulmonary pressures preclude definitive surgical management in infancy.
Hypoplastic left heart syndrome

1 – (neonate) Aorta reconstruction uses the MPA – the RV then pumps systemic blood (dotted line); pulmonic blood flow is via systemic arterial-to-branch PA, BT shunt (green). 2 – (around 6 months) BT shunt is closed and a bidirectional cavopulmonary (SVC-to-branch PA), aka Glenn shunt, (arrow) is created. 3 – (age 3-5 years) A modified Fontan circuit completes separation of pulmonary & systemic circulations with addition of an IVC to PA shunt (arrow).
Norwood Procedure
2 3 1

DAMUS-KAYE-STANSEL End-to-side anastomosis of the AAo to the MPA (circle). A BT shunt or RV to PA conduit is used to maintain pulmonary flow. SANO MODIFICATION An RV to PA conduit (green), helps maintain better diastolic perfusion pressure to the coronary arteries than is seen in patients with BT shunts. HYBRID PROCEDURE A combined surgical and interventional procedure eliminates the need for cardiopulmonary bypass; involves MPA or branch PA banding (arrows) and stenting the PDA (green) so it remains patent.
Norwood alternatives

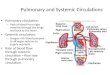
Temporary shunt designed to palliate low pulmonary blood flow (TOF, tricuspid or PA atresia, DORV, & single ventricle forms of CHD). Directs arterial pressure blood flow from the subclavian artery to the PAs (green & arrow) until pulmonary perfusion pressure declines. • Classic BT shunt – subclavian artery was ligated and sewn to the PA • Modified BT shunt – uses synthetic graft material (green & arrow)
Blalock-Taussig shunt

SVC is connected to confluent branch PAs; cerebral & upper extremity venous return to the lungs bypasses the heart. Pulmonary blood flow is often asymmetric (black arrows). If bilateral SVCs, bilateral shunts Are required (dotted lines).
Bidirectional cavopulmonary shunt
The SVC is anastomosed to the right PA (red arrow); branch PAs are not necessarily confluent.
Glenn shunt

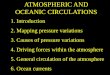
Due to anterior, superior & leftward displacement of the infundibular septum 4 features of TOF are: • RVOT obstruction subpulmonary muscle bundles (black arrows), valvar or supravalvar stenosis • RV hypertrophy • VSD • Aorta overrides VSD (red arrow) Depending on the severity of pulmonary stenosis, pulmonary blood flow may be temporized with a BT shunt or definitive palliation, with VSD closure & augmentation of the RVOT with transannular patch or pulmonary valvotomy, can be performed around the age of 6 months.
Tetralogy of Fallot

ALTERNATIVE SURGICAL PROCEDURES The VSD is closed, directing LV blood flow to the aorta (arrow). The pulmonary outflow tract is reconstructed using a valved homograft conduit (green). Also used to correct PA atresia w/ VSD, TGA with VSD and LVOT obstruction, & DORV.
Transannular patch RVOT using pericardium or artificial graft material (green). Used in TOF or in patients with a small PV annulus which precludes valve-sparing palliation. The patch enlarges the MPA (green & *). The patched RVOT segment is akinetic and pulmonic insufficiency leads to RV dilation & dysfunction.
Rastelli procedure RV –PA conduit
*
*

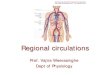
Fontan
*
A conduit connects the IVC to branch PAs, in patients who usually have a BCPS or Glenn shunt, completing delivery of all systemic venous return to the lungs, bypassing the heart. The systemic & pulmonary circulations are completely separated & a single ventricle pumps to the systemic circulation. Postop complications include thrombosis (*), chylous pleural effusions, and ascites.

INTRACARDIAC / EXTRACARDIAC A tunnel is constructed within the lateral aspect of the RA (white arrows), or a conduit adjacent to RA (*), directing blood flow from the IVC to the PAs. FENESTRATED A small opening or communication is often left between the conduit and RA and acts as a pop-off valve if pulmonary pressure is high. It may be closed with a device at later date. • Classic Fontan – The RA is sewn to the branch PAs. No longer used as the RA acts as a reservoir with risks of arrhythmia & mural thrombi.
Fontan
*

Transposition of the great arteries D-TGA D –TGA: AV concordance/VA discordance Aorta arises from RV & MPA from LV, results in separate, parallel pulmonary & systemic circulations, mixing/shunt (ASD / VSD / PDA) for early survival. JATENE – ARTERIAL SWITCH Physiologic correction of D-TGA involves switching the aorta & MPA (circle) along with coronary artery reimplantation to the neo-aorta (arrow).

L –TGA: AV discordance/VA discordance results in a “congenitally corrected” TGA • lungs – pulmonary veins –
LA – RV – aorta
• SVC/IVC – RA – LV – pulmonary arteries
Though “corrected”, the morphologic RV supplies systemic circulation, eventually resulting in RV failure.
Transposition of the great arteries L-TGA

Intra-atrial baffle corrects TGA at the atrial level by redirecting pulmonary venous return to the atrium (arrows) connected to the systemic ventricle & systemic venous return toward the pulmonary ventricle. The baffle is created using pericardial (Mustard) or atrial (Senning) tissue. The disadvantage of this procedure in D-TGA is that the morphologic RV (arrow, moderator band) supplies the systemic circulation & will eventually fail. JATENE VARIATION Le Compte Maneuver If there is tension on the coronary arteries during a Jatene surgery the Le Compte maneuver alleviates this by placing the AAo posterior and draping the PAs (*) over the aorta.
*
Mustard & Senning

Ross procedure To treat severe AV stenosis, the PV is moved to the aortic position to alleviate severe aortic stenosis (arrow). The coronary arteries are reimplanted into the PV autograft. A valved conduit or cadaveric homograft (green) replaces the pulmonic valve.
Ross – Konno operation In multilevel aortic stenosis which cannot be effectively treated by valvotomy alone, a PV autograft with RVOT and/or septal tissue replaces the AV & augments the LVOT, the coronary arteries are reimplanted & conduit used for the RVOT.
*

abbreviations AAo ascending aorta AoV aortic valve ASD atrial septal defect AV atrioventricular BCPS bidirectional cavopulmonary shunt BT Blalock-Taussig shunt CHD congenital heart disease DKS Damus-Kaye-Stansel DORV double outlet right ventricle HLHS hypoplastic left heart syndrome IVC inferior vena cava LA left atrium LPA left pulmonary artery LV left ventricle LVOT left ventricular outflow tract
MPA main pulmonary artery MV mitral valve PA pulmonary artery PDA patent ductus arteriosus PV pulmonary valve RA right atrium RPA right pulmonary artery RV right ventricle RVH right ventricle hypertrophy RVOT right ventricular outflow tract SVC superior vena cava TGA transposition of the great arteries TOF tetralogy of Fallot VA ventriculoarterial VSD ventricular septal defect