Embed Size (px)
Citation preview

FOR BHF USE IMPORTANT NOTICELL1 THIS AGENCY IS REQUESTING DISCLOSURE OF INFORMATION
THAT IS NECESSARY TO ACCOMPLISH THE STATUTORY
2008 PURPOSE AS OUTLINED IN 210 ILCS 45/3-208. DISCLOSURESTATE OF ILLINOIS OF THIS INFORMATION IS MANDATORY. FAILURE TO PROVIDE
DEPARTMENT OF HEALTHCARE AND FAMILY SERVICES ANY INFORMATION ON OR BEFORE THE DUE DATE WILLFINANCIAL AND STATISTICAL REPORT (COST REPORT) RESULT IN CESSATION OF PROGRAM PAYMENTS. THIS FORM
FOR LONG-TERM CARE FACILITIES HAS BEEN APPROVED BY THE FORMS MANAGEMENT CENTER.(FISCAL YEAR 2008)
I. IDPH License ID Number: 0025577 II. CERTIFICATION BY AUTHORIZED FACILITY OFFICER
Facility Name: Covenant Health Care Center-Batavia I have examined the contents of the accompanying report to the
Address: 831 North Batavia Avenue Batavia 60510 State of Illinois, for the period from 02/01/07 to 01/31/08Number City Zip Code and certify to the best of my knowledge and belief that the said contents
are true, accurate and complete statements in accordance withCounty: Kane applicable instructions. Declaration of preparer (other than provider)
is based on all information of which preparer has any knowledge.Telephone Number: (630) 879-4300 Fax # (630) 879-8483
Intentional misrepresentation or falsification of any informationHFS ID Number: 521115873002 in this cost report may be punishable by fine and/or imprisonment.
Date of Initial License for Current Owners: 5/9/1980 (Signed)Officer or (Date)
Type of Ownership: Administrator (Type or Print Name)of Provider
X VOLUNTARY,NON-PROFIT PROPRIETARY GOVERNMENTAL (Title)X Charitable Corp. Individual State
Trust Partnership County (Signed)IRS Exemption Code 501 c (3) Corporation Other (Date)
"Sub-S" Corp. Paid (Print Name Steven N. Lavenda, C.P.A.Limited Liability Co. Preparer and Title)TrustOther (Firm Name Frost, Ruttenberg & Rothblatt, P.C.
& Address) 111 Pfingsten Road, Suite 300 Deerfield, IL 60015
(Telephone) (847) 236-1111 Fax #(847) 236-1155 MAIL TO: BUREAU OF HEALTH FINANCE
In the event there are further questions about this report, please contact: ILLINOIS DEPT OF HEALTHCARE AND FAMILY SERVICESName:: Steve Lavenda Telephone Number: (847) 236-1111 201 S. Grand Avenue East
Email Address: Springfield, IL 62763-0001 Phone # (217) 782-1630SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 2Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
III. STATISTICAL DATA D. How many bed-hold days during this year were paid by the Department?A. Licensure/certification level(s) of care; enter number of beds/bed days, None (Do not include bed-hold days in Section B.) (must agree with license). Date of change in licensed beds N/A
E. List all services provided by your facility for non-patients. 1 2 3 4 (E.g., day care, "meals on wheels", outpatient therapy)
None Beds at Licensed Beginning of Licensure Beds at End of Bed Days During F. Does the facility maintain a daily midnight census? Yes Report Period Level of Care Report Period Report Period
G. Do pages 3 & 4 include expenses for services or1 99 Skilled (SNF) 99 36,135 1 investments not directly related to patient care?2 Skilled Pediatric (SNF/PED) 2 YES NO X3 Intermediate (ICF) 34 Intermediate/DD 4 H. Does the BALANCE SHEET (page 17) reflect any non-care assets?5 Sheltered Care (SC) 5 YES NO X6 ICF/DD 16 or Less 6
I. On what date did you start providing long term care at this location?7 99 TOTALS 99 36,135 7 Date started 05/06/1980
J. Was the facility purchased or leased after January 1, 1978?B. Census-For the entire report period. YES Date NO X
1 2 3 4 5 Level of Care Patient Days by Level of Care and Primary Source of Payment K. Was the facility certified for Medicare during the reporting year?
Medicaid YES X NO If YES, enter numberRecipient Private Pay Other Total of beds certified 99 and days of care provided 2,345
8 SNF 12,980 2,931 19,750 35,661 8 9 SNF/PED 9 Medicare Intermediary National Government Services 10 ICF 1011 ICF/DD 11 IV. ACCOUNTING BASIS12 SC 12 MODIFIED13 DD 16 OR LESS 13 ACCRUAL X CASH* CASH*
14 TOTALS 12,980 2,931 19,750 35,661 14 Is your fiscal year identical to your tax year? YES X NO
C. Percent Occupancy. (Column 5, line 14 divided by total licensed Tax Year: 01/31/2008 Fiscal Year: 01/31/2008 bed days on line 7, column 4.) 98.69% * All facilities other than governmental must report on the accrual basis.
SEE ACCOUNTANTS' COMPILATION REPORT
STATE OF ILLINOIS Page 3Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08V. COST CENTER EXPENSES (throughout the report, please round to the nearest dollar)
Costs Per General Ledger Reclass- Reclassified Adjust- Adjusted FOR BHF USE ONLY Operating Expenses Salary/Wage Supplies Other Total ification Total ments TotalA. General Services 1 2 3 4 5 6 7 8 9 10
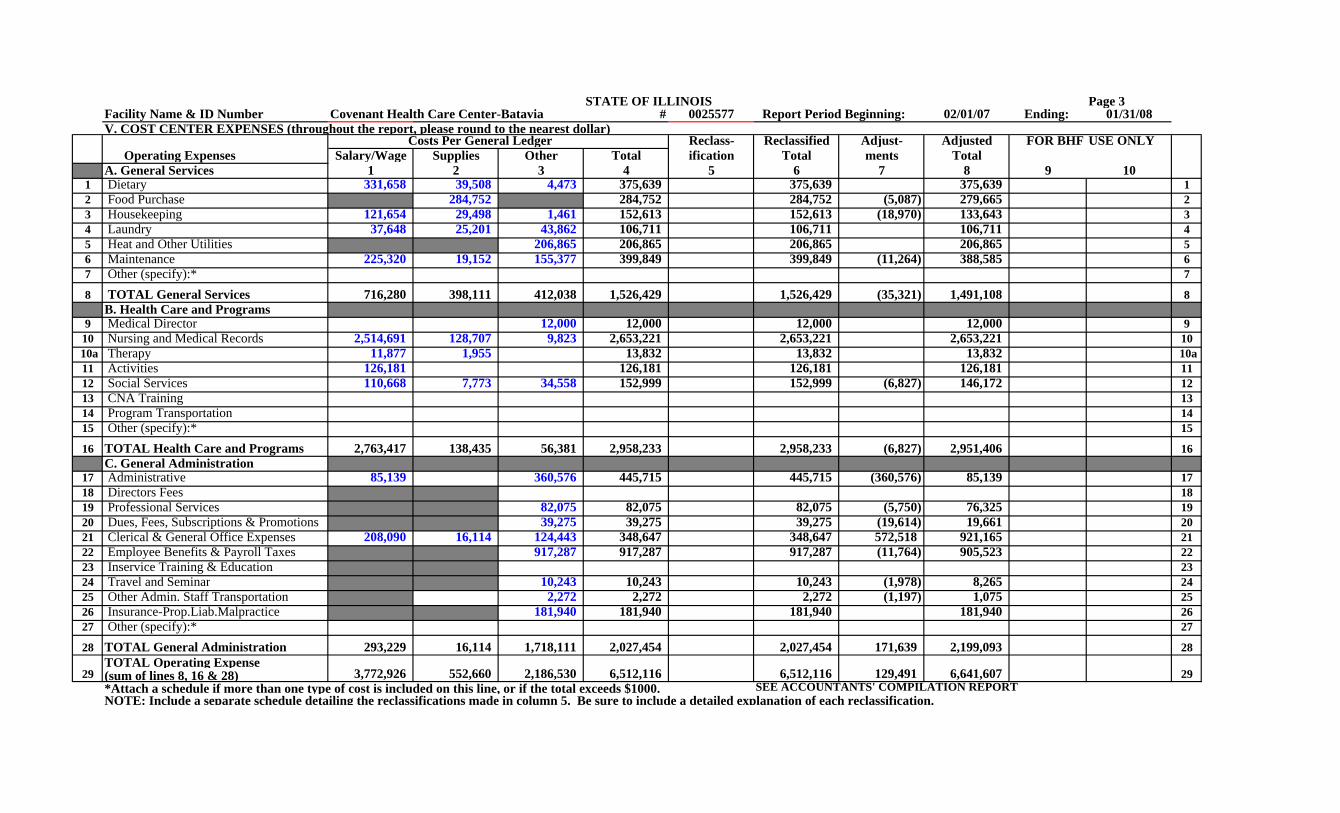
1 Dietary 331,658 39,508 4,473 375,639 375,639 375,639 12 Food Purchase 284,752 284,752 284,752 (5,087) 279,665 23 Housekeeping 121,654 29,498 1,461 152,613 152,613 (18,970) 133,643 34 Laundry 37,648 25,201 43,862 106,711 106,711 106,711 45 Heat and Other Utilities 206,865 206,865 206,865 206,865 56 Maintenance 225,320 19,152 155,377 399,849 399,849 (11,264) 388,585 67 Other (specify):* 7
8 TOTAL General Services 716,280 398,111 412,038 1,526,429 1,526,429 (35,321) 1,491,108 8B. Health Care and Programs
9 Medical Director 12,000 12,000 12,000 12,000 910 Nursing and Medical Records 2,514,691 128,707 9,823 2,653,221 2,653,221 2,653,221 10
10a Therapy 11,877 1,955 13,832 13,832 13,832 10a11 Activities 126,181 126,181 126,181 126,181 1112 Social Services 110,668 7,773 34,558 152,999 152,999 (6,827) 146,172 1213 CNA Training 1314 Program Transportation 1415 Other (specify):* 15
16 TOTAL Health Care and Programs 2,763,417 138,435 56,381 2,958,233 2,958,233 (6,827) 2,951,406 16C. General Administration
17 Administrative 85,139 360,576 445,715 445,715 (360,576) 85,139 1718 Directors Fees 1819 Professional Services 82,075 82,075 82,075 (5,750) 76,325 1920 Dues, Fees, Subscriptions & Promotions 39,275 39,275 39,275 (19,614) 19,661 2021 Clerical & General Office Expenses 208,090 16,114 124,443 348,647 348,647 572,518 921,165 2122 Employee Benefits & Payroll Taxes 917,287 917,287 917,287 (11,764) 905,523 2223 Inservice Training & Education 2324 Travel and Seminar 10,243 10,243 10,243 (1,978) 8,265 2425 Other Admin. Staff Transportation 2,272 2,272 2,272 (1,197) 1,075 2526 Insurance-Prop.Liab.Malpractice 181,940 181,940 181,940 181,940 2627 Other (specify):* 27
28 TOTAL General Administration 293,229 16,114 1,718,111 2,027,454 2,027,454 171,639 2,199,093 28TOTAL Operating Expense
29 (sum of lines 8, 16 & 28) 3,772,926 552,660 2,186,530 6,512,116 6,512,116 129,491 6,641,607 29*Attach a schedule if more than one type of cost is included on this line, or if the total exceeds $1000. SEE ACCOUNTANTS' COMPILATION REPORTNOTE: Include a separate schedule detailing the reclassifications made in column 5. Be sure to include a detailed explanation of each reclassification.
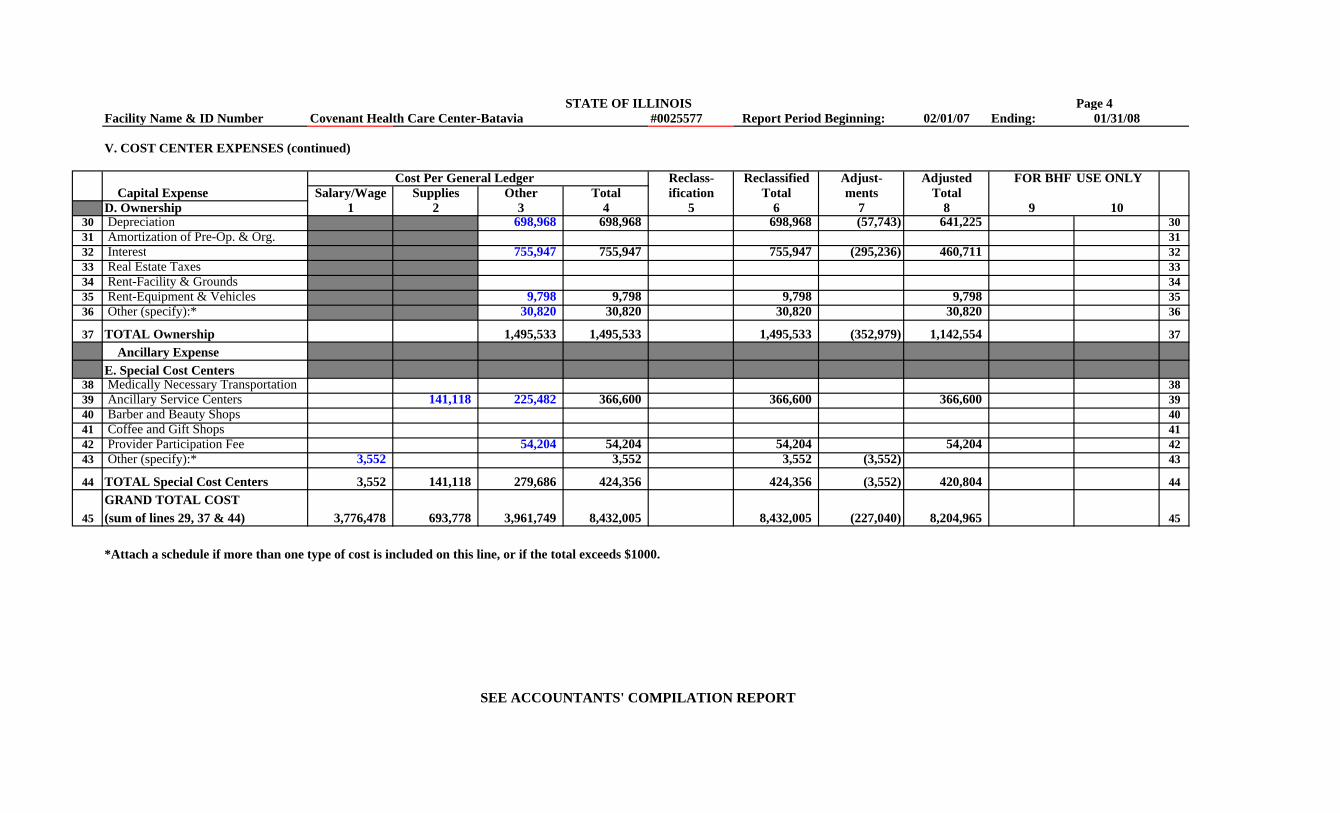
STATE OF ILLINOIS Page 4Facility Name & ID Number Covenant Health Care Center-Batavia #0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
#V. COST CENTER EXPENSES (continued)
Cost Per General Ledger Reclass- Reclassified Adjust- Adjusted FOR BHF USE ONLY Capital Expense Salary/Wage Supplies Other Total ification Total ments TotalD. Ownership 1 2 3 4 5 6 7 8 9 10
30 Depreciation 698,968 698,968 698,968 (57,743) 641,225 3031 Amortization of Pre-Op. & Org. 3132 Interest 755,947 755,947 755,947 (295,236) 460,711 3233 Real Estate Taxes 3334 Rent-Facility & Grounds 3435 Rent-Equipment & Vehicles 9,798 9,798 9,798 9,798 3536 Other (specify):* 30,820 30,820 30,820 30,820 36
37 TOTAL Ownership 1,495,533 1,495,533 1,495,533 (352,979) 1,142,554 37 Ancillary ExpenseE. Special Cost Centers
38 Medically Necessary Transportation 3839 Ancillary Service Centers 141,118 225,482 366,600 366,600 366,600 3940 Barber and Beauty Shops 4041 Coffee and Gift Shops 4142 Provider Participation Fee 54,204 54,204 54,204 54,204 4243 Other (specify):* 3,552 3,552 3,552 (3,552) 43
44 TOTAL Special Cost Centers 3,552 141,118 279,686 424,356 424,356 (3,552) 420,804 44GRAND TOTAL COST
45 (sum of lines 29, 37 & 44) 3,776,478 693,778 3,961,749 8,432,005 8,432,005 (227,040) 8,204,965 45
*Attach a schedule if more than one type of cost is included on this line, or if the total exceeds $1000.
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 5Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08VI. ADJUSTMENT DETAIL A. The expenses indicated below are non-allowable and should be adjusted out of Schedule V, pages 3 or 4 via column 7.
In column 2 below, reference the line on which the particular cost was included. (See instructions.) 1 2 3
Refer- BHF USE B. If there are expenses experienced by the facility which do not appear in the NON-ALLOWABLE EXPENSES Amount ence ONLY general ledger, they should be entered below.(See instructions.)
1 Day Care $ $ 1 1 22 Other Care for Outpatients 2 Amount Reference3 Governmental Sponsored Special Programs 3 31 Non-Paid Workers-Attach Schedule* $ 314 Non-Patient Meals (5,071) 02 4 32 Donated Goods-Attach Schedule* 325 Telephone, TV & Radio in Resident Rooms 5 Amortization of Organization &6 Rented Facility Space 6 33 Pre-Operating Expense 337 Sale of Supplies to Non-Patients 7 Adjustments for Related Organization8 Laundry for Non-Patients 8 34 Costs (Schedule VII) 237,445 349 Non-Straightline Depreciation (57,743) 30 9 35 Other- Attach Schedule 35
10 Interest and Other Investment Income (295,236) 32 10 36 SUBTOTAL (B): (sum of lines 31-35) $ 237,445 3611 Discounts, Allowances, Rebates & Refunds 11 (sum of SUBTOTALS12 Non-Working Officer's or Owner's Salary 12 37 TOTAL ADJUSTMENTS (A) and (B) ) $ (227,040) 3713 Sales Tax 02 1314 Non-Care Related Interest 14 *These costs are only allowable if they are necessary to meet minimum15 Non-Care Related Owner's Transactions 15 licensing standards. Attach a schedule detailing the items included16 Personal Expenses (Including Transportation) 16 on these lines.17 Non-Care Related Fees 1718 Fines and Penalties (15,000) 21 18 C. Are the following expenses included in Sections A to D of pages 319 Entertainment 19 and 4? If so, they should be reclassified into Section E. Please 20 Contributions (1,155) 20 20 reference the line on which they appear before reclassification.21 Owner or Key-Man Insurance 21 (See instructions.) 1 2 3 422 Special Legal Fees & Legal Retainers 22 Yes No Amount Reference23 Malpractice Insurance for Individuals 23 38 Medically Necessary Transport. $ 3824 Bad Debt (15,847) 21 24 39 3925 Fund Raising, Advertising and Promotional (16,599) 20 25 40 Gift and Coffee Shops 40
Income Taxes and Illinois Personal 41 Barber and Beauty Shops 4126 Property Replacement Tax 26 42 Laboratory and Radiology 4227 CNA Training for Non-Employees 27 43 Prescription Drugs 4328 Yellow Page Advertising 28 44 4429 Other-Attach Schedule (57,834) 29 45 Other-Attach Schedule 4530 SUBTOTAL (A): (Sum of lines 1-29) $ (464,485) $ 30 46 Other-Attach Schedule 46
47 TOTAL (C): (sum of lines 38-46) $ 47BHF USE ONLY
48 49 50 51 52 SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 5ACovenant Health Care Center-Batavia
ID# 0025577Report Period Beginning: 02/01/07
Ending: 01/31/08Sch. V Line
NON-ALLOWABLE EXPENSES Amount Reference1 Non-Allowable Travel $ (1,197) 25 12 Equipment Rental Income (11,052) 06 23 Vending Machine Revenue (16) 02 34 Telephone Revenue (334) 21 45 Replacement Badge Income (72) 21 56 Promotions & Public Relations (1,860) 20 67 Transportation Revenue (6,827) 12 78 Non-Allowable Seminar (1,978) 24 89 Housekeeping Revenue (18,970) 03 9
10 Maintenance Revenue (212) 06 1011 Employee Recognition (11,764) 22 1112 Marketing Salary (3,552) 43 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 2526 2627 2728 2829 2930 3031 3132 3233 3334 3435 3536 3637 3738 3839 3940 4041 4142 4243 4344 4445 4546 4647 4748 4849 Total (57,834) 49

STATE OF ILLINOIS Page 5BCovenant Health Care Center-Batavia
ID# 0025577Report Period Beginning: 02/01/07
Ending: 01/31/08Sch. V Line
NON-ALLOWABLE EXPENSES Amount Reference50 $ 151 252 353 454 555 656 757 858 959 1060 1161 1262 1363 1464 1565 1666 1767 1868 1969 2070 2171 2272 2373 2474 2575 2676 2777 2878 2979 3080 3181 3282 3383 3484 3585 3686 3787 3888 3989 4090 4191 4292 4393 4494 4595 4696 4797 4898 49

STATE OF ILLINOIS Summary AFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08SUMMARY OF PAGES 5, 5A, 6, 6A, 6B, 6C, 6D, 6E, 6F, 6G, 6H AND 6I
SUMMARY Operating Expenses PAGES PAGE PAGE PAGE PAGE PAGE PAGE PAGE PAGE PAGE PAGE TOTALSA. General Services 5 & 5A 6 6A 6B 6C 6D 6E 6F 6G 6H 6I (to Sch V, col.7)
1 Dietary 12 Food Purchase (5,087) (5,087) 23 Housekeeping (18,970) (18,970) 34 Laundry 45 Heat and Other Utilities 56 Maintenance (11,264) (11,264) 67 Other (specify):* 78 TOTAL General Services (35,321) (35,321) 8
B. Health Care and Programs9 Medical Director 9
10 Nursing and Medical Records 10 10a Therapy 10a11 Activities 1112 Social Services (6,827) (6,827) 1213 CNA Training 1314 Program Transportation 1415 Other (specify):* 15
16 TOTAL Health Care and Programs (6,827) (6,827) 16C. General Administration
17 Administrative (360,576) (360,576) 1718 Directors Fees 1819 Professional Services (5,750) (5,750) 1920 Fees, Subscriptions & Promotions (19,614) (19,614) 2021 Clerical & General Office Expenses (31,253) 603,771 572,518 2122 Employee Benefits & Payroll Taxes (11,764) (11,764) 2223 Inservice Training & Education 2324 Travel and Seminar (1,978) (1,978) 2425 Other Admin. Staff Transportation (1,197) (1,197) 2526 Insurance-Prop.Liab.Malpractice 2627 Other (specify):* 27
28 TOTAL General Administration (65,806) 237,445 171,639 28TOTAL Operating Expense
29 (sum of lines 8,16 & 28) (107,954) 237,445 129,491 29

STATE OF ILLINOIS Summary BFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
SUMMARY OF PAGES 5, 5A, 6, 6A, 6B, 6C, 6D, 6E, 6F, 6G, 6H AND 6I
SUMMARY Capital Expense PAGES PAGE PAGE PAGE PAGE PAGE PAGE PAGE PAGE PAGE PAGE TOTALSD. Ownership 5 & 5A 6 6A 6B 6C 6D 6E 6F 6G 6H 6I (to Sch V, col.7)
30 Depreciation (57,743) (57,743) 3031 Amortization of Pre-Op. & Org. 3132 Interest (295,236) (295,236) 3233 Real Estate Taxes 3334 Rent-Facility & Grounds 3435 Rent-Equipment & Vehicles 3536 Other (specify):* 36
37 TOTAL Ownership (352,979) (352,979) 37 Ancillary ExpenseE. Special Cost Centers
38 Medically Necessary Transportation 3839 Ancillary Service Centers 3940 Barber and Beauty Shops 4041 Coffee and Gift Shops 4142 Provider Participation Fee 4243 Other (specify):* (3,552) (3,552) 43
44 TOTAL Special Cost Centers (3,552) (3,552) 44GRAND TOTAL COST
45 (sum of lines 29, 37 & 44) (464,485) 237,445 (227,040) 45

STATE OF ILLINOIS Page 6Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES A. Enter below the names of ALL owners and related organizations (parties) as defined in the instructions. Attach an additional schedule if necessary.
1 2 3 OWNERS RELATED NURSING HOMES OTHER RELATED BUSINESS ENTITIES
Name Ownership % Name City Name City Type of BusinessCovenant Retirement Communities 100% See Attached See Attached
B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,management fees, purchase of supplies, and so forth. YES X NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)1 V $ $ $ 12 V 23 V 34 V 45 V 56 V 67 V 78 V 89 V 910 V 1011 V 1112 V 1213 V 1314 Total $ $ $ * 14
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6AFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. X YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V 21 Clerical and General Office Exp. $ Covenant Retirement Communities 100.00% $ 603,771 $ 603,771 1516 V 1617 V 17 Management Fees 360,576 Covenant Retirement Communities 100.00% (360,576) 1718 V 19 Cost Report Preparation 5,750 Covenant Retirement Communities 100.00% (5,750) 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ 366,326 $ 603,771 $ * 237,445 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6BFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6CFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6DFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6EFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6FFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT
STATE OF ILLINOIS Page 6GFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
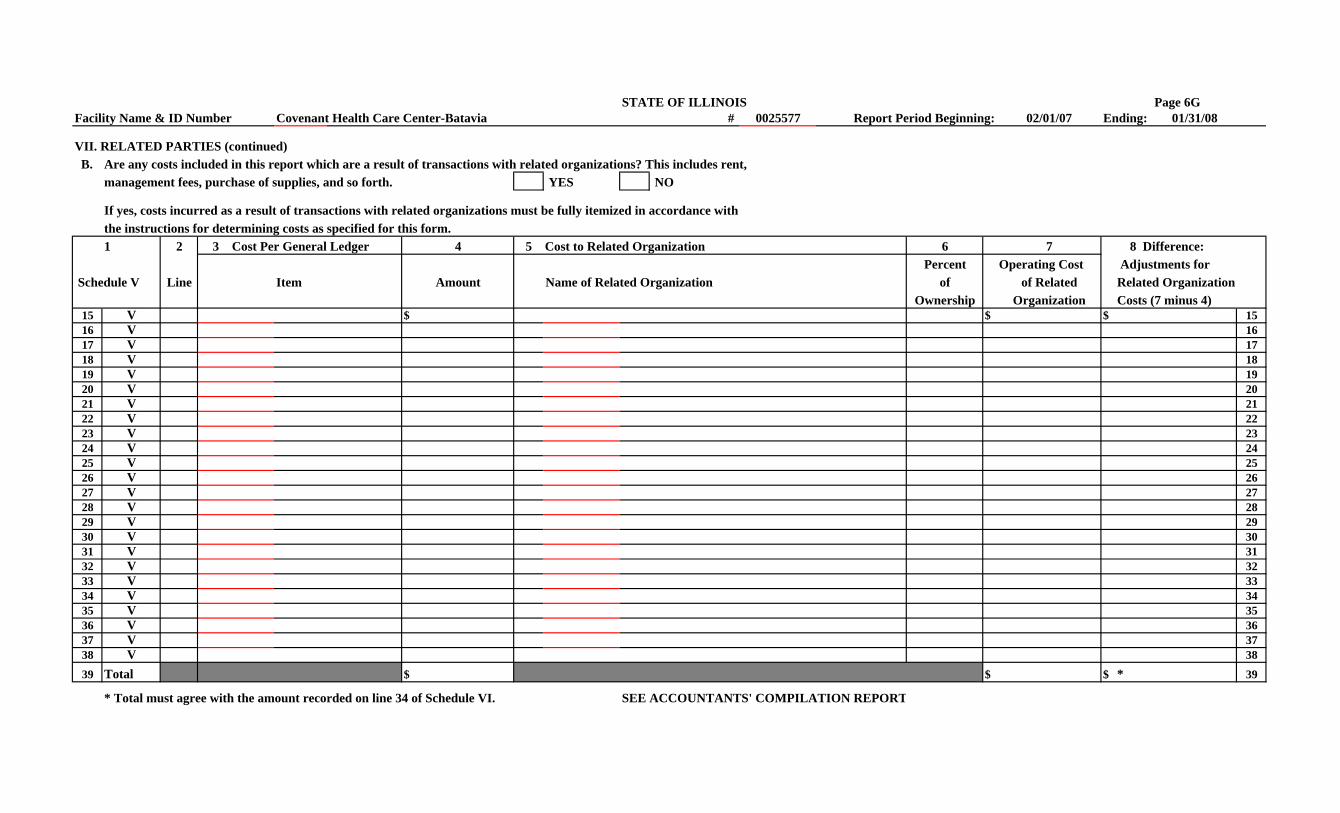
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6HFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 6IFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued) B. Are any costs included in this report which are a result of transactions with related organizations? This includes rent,
management fees, purchase of supplies, and so forth. YES NO
If yes, costs incurred as a result of transactions with related organizations must be fully itemized in accordance withthe instructions for determining costs as specified for this form.1 2 3 Cost Per General Ledger 4 5 Cost to Related Organization 6 7 8 Difference:
Percent Operating Cost Adjustments for Schedule V Line Item Amount Name of Related Organization of of Related Related Organization
Ownership Organization Costs (7 minus 4)15 V $ $ $ 1516 V 1617 V 1718 V 1819 V 1920 V 2021 V 2122 V 2223 V 2324 V 2425 V 2526 V 2627 V 2728 V 2829 V 2930 V 3031 V 3132 V 3233 V 3334 V 3435 V 3536 V 3637 V 3738 V 38
39 Total $ $ $ * 39
* Total must agree with the amount recorded on line 34 of Schedule VI. SEE ACCOUNTANTS' COMPILATION REPORT
STATE OF ILLINOIS Page 7Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VII. RELATED PARTIES (continued)C. Statement of Compensation and Other Payments to Owners, Relatives and Members of Board of Directors. NOTE: ALL owners ( even those with less than 5% ownership) and their relatives who receive any type of compensation from this home must be listed on this schedule.
1 2 3 4 5 6 7 8Average Hours Per Work
Compensation Week Devoted to this Compensation Included Schedule V.Received Facility and % of Total in Costs for this Line &
Ownership From Other Work Week Reporting Period** ColumnName Title Function Interest Nursing Homes* Hours Percent Description Amount Reference
1 See Attached Board of Directors $ 12 23 34 45 56 67 78 89 9
10 1011 1112 12
13 TOTAL $ 13
* If the owner(s) of this facility or any other related parties listed above have received compensation from other nursing homes, attach a schedule detailing the name(s)of the home(s) as well as the amount paid. THIS AMOUNT MUST AGREE TO THE AMOUNTS CLAIMED ON THE THE OTHER NURSING HOMES' COST REPORTS.
** This must include all forms of compensation paid by related entities and allocated to Schedule V of this report (i.e., management fees).FAILURE TO PROPERLY COMPLETE THIS SCHEDULE INDICATING ALL FORMS OF COMPENSATION RECEIVED FROM THIS HOME,ALL OTHER NURSING HOMES AND MANAGEMENT COMPANIES MAY RESULT IN THE DISALLOWANCE OF SUCH COMPENSATION.
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO X City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8AFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization Covenant Retirement Communities
A. Are there any costs included in this report which were derived from allocations of central office Street Address 5115 North Francisco Avenue or parent organization costs? (See instructions.) YES X NO City / State / Zip Code Chicago, Illinois 60625-3611
Phone Number ( (773) 878-2294 B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( (773) 878-2289
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 21 Clerical and General Office Exp. Total Expenses 603,771 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 603,771 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8BFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8CFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8DFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8EFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8FFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8GFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8HFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 8IFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
VIII. ALLOCATION OF INDIRECT COSTS Name of Related Organization
A. Are there any costs included in this report which were derived from allocations of central office Street Address or parent organization costs? (See instructions.) YES NO City / State / Zip Code
Phone Number ( ) B. Show the allocation of costs below. If necessary, please attach worksheets. Fax Number ( )
1 2 3 4 5 6 7 8 9Schedule V Unit of Allocation Number of Total Indirect Amount of Salary
Line (i.e.,Days, Direct Cost, Subunits Being Cost Being Cost Contained Facility AllocationReference Item Square Feet) Total Units Allocated Among Allocated in Column 6 Units (col.8/col.4)x col.6
1 $ $ $ 12 23 34 45 56 67 78 89 910 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 TOTALS $ $ $ 25
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 9 - SUPPLEMENTALFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
IX. INTEREST EXPENSE AND REAL ESTATE TAX EXPENSE - SUPPLEMENTAL SCHEDULE A. Interest: (Complete details must be provided for each loan - attach a separate schedule if necessary.)
1 2 3 4 5 6 7 8 9 10Reporting
Monthly Maturity Interest PeriodName of Lender Related** Purpose of Loan Payment Date of Amount of Note Date Rate Interest
YES NO Required Note Original Balance (4 Digits) ExpenseA. Directly Facility Related Long-Term
1 $ $ $ 12 23 34 45 56 67 TOTAL Long-Term 7
Working Capital8 $ $ $ 89 910 1011 1112 1213 1314 TOTAL Working Capital 14
B. Non-Facility Related*15 $ $ $ 1516 1617 1718 1819 1920 TOTAL Non-Facility Related 20
* Any interest expense reported in this section should be adjusted out on page 5, line 14 and, consequently, page 4, col. 7.(See instructions.) SEE ACCOUNTANTS' COMPILATION REPORT
** If there is ANY overlap in ownership between the facility and the lender, this must be indicated in column 2.(See instructions.)

STATE OF ILLINOIS Page 9Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
IX. INTEREST EXPENSE AND REAL ESTATE TAX EXPENSE A. Interest: (Complete details must be provided for each loan - attach a separate schedule if necessary.)
1 2 3 4 5 6 7 8 9 10Reporting
Monthly Maturity Interest PeriodName of Lender Related** Purpose of Loan Payment Date of Amount of Note Date Rate Interest
YES NO Required Note Original Balance (4 Digits) ExpenseA. Directly Facility Related Long-Term
1 Interest 1998 Tax EE X Refinance of Debt 1998 $ 898,564 $ 718,852 2015 0.0410 $ 36,841 12 Interest 2001 Tax EE X Building Construction 2001 22,000,000 8,758,200 2031 0.0588 514,544 23 Interest 2002 Tax EEX Bond X Refinance of Debt 2002 5,048,176 3,641,166 2028 0.0613 204,562 34 45 See Supplemental Schedule 5
Working Capital6 67 78 See Supplemental Schedule 8
9 TOTAL Facility Related $ 27,946,740 $ 13,118,218 $ 755,947 9B. Non-Facility Related*
10 Interest Income X (295,236) 1011 1112 1213 See Supplemental Schedule 13
14 TOTAL Non-Facility Related $ $ $ (295,236) 14
15 TOTALS (line 9+line14) $ 27,946,740 $ 13,118,218 $ 460,711 15
16) Please indicate the total amount of mortgage insurance expense and the location of this expense on Sch. V. $ N/A Line # N/A
* Any interest expense reported in this section should be adjusted out on page 5, line 14 and, consequently, page 4, col. 7.(See instructions.) SEE ACCOUNTANTS' COMPILATION REPORT
** If there is ANY overlap in ownership between the facility and the lender, this must be indicated in column 2.(See instructions.)

STATE OF ILLINOIS Page 10Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
IX. INTEREST EXPENSE AND REAL ESTATE TAX EXPENSE (continued) B. Real Estate Taxes
1. Real Estate Tax accrual used on 2007 report. $ 1
2. Real Estate Taxes paid during the year: (Indicate the tax year to which this payment applies. If payment covers more than one year, detail below.) $ 2
3. Under or (over) accrual (line 2 minus line 1). $ 3
4. Real Estate Tax accrual used for 2008 report. (Detail and explain your calculation of this accrual on the lines below.) $ 4
5. Direct costs of an appeal of tax assessments which has NOT been included in professional fees or other general operating costs on Schedule V, sections A, B or C. (Describe appeal cost below. Attach copies of invoices to support the cost and a copy of the appeal filed with the county.) $ 5
6. Subtract a refund of real estate taxes. You must offset the full amount of any direct appeal costs classified as a real estate tax cost plus one-half of any remaining refund. TOTAL REFUND $ For Tax Year. (Attach a copy of the real estate tax appeal board's decision.) $ 6
7. Real Estate Tax expense reported on Schedule V, line 33. This should be a combination of lines 3 thru 6. $ 7
Real Estate Tax History:
Real Estate Tax Bill for Calendar Year: 2003 8 FOR BHF USE ONLY2004 92005 10 13 FROM R. E. TAX STATEMENT FOR 2007 $ 132006 112007 12 14 PLUS APPEAL COST FROM LINE 5 $ 14
Facility does not pay real estate taxes due to its non-profit status.15 LESS REFUND FROM LINE 6 $ 15
16 AMOUNT TO USE FOR RATE CALCULATION $ 16
NOTES: 1. Please indicate a negative number by use of brackets( ). Deduct any overaccrual of taxes from prior year.
2. If facility is a non-profit which pays real estate taxes, you must attach a denial of an application for real estate tax exemption unless the building is rented from a for-profit entity. This denial must be no more than four years old at the time the cost report is filed.
SEE ACCOUNTANTS' COMPILATION REPORT
Important , please see the next worksheet, "RE_Tax". The real estate tax statement and bill must accompany the cost report.

2007 LONG TERM CARE REAL ESTATE TAX STATEMENTFACILITY NAME Covenant Health Care Center-Batavia COUNTY Kane
FACILITY IDPH LICENSE NUMBER 0025577
CONTACT PERSON REGARDING THIS REPORT Steve Lavenda
TELEPHONE (847) 236-1111 FAX #: (847) 236-1155
A. Summary of Real Estate Tax Cost
Enter the tax index number and real estate tax assessed for 2007 on the lines provided below. Enter only the portion of thecost that applies to the operation of the nursing home in Column D. Real estate tax applicable to any portion of the nursinghome property which is vacant, rented to other organizations, or used for purposes other than long term care must not beentered in Column D. Do not include cost for any period other than calendar year 2007.
(A) (B) (C) (D)Tax
Applicable toTax Index Number Property Description Total Tax Nursing Home
1. N/A N/A $ N/A $ N/A
2. $ $
3. $ $
4. $ $
5. $ $
6. $ $
7. $ $
8. $ $
9. $ $
10. $ $
TOTALS $ $
B. Real Estate Tax Cost Allocations
Does any portion of the tax bill apply to more than one nursing home, vacant property, or property which is not directlyused for nursing home services? YES X NO
If YES, attach an explanation & a schedule which shows the calculation of the cost allocated to the nursing home.(Generally the real estate tax cost must be allocated to the nursing home based upon sq. ft. of space used.)
C. Tax Bills
Attach a copy of the original 2007 tax bills which were listed in Section A to this statement. Be sure to use the 2007tax bill which is normally paid during 2008.
PLEASE NOTE: Payment information from the Internet or otherwise is not considered acceptable tax billdocumentation. Facilities located in Cook County are required to provide copies of their original second installment tax bill.
Page 10A
IMPORTANT NOTICE
TO: Long Term Care Facilities with Real Estate Tax Rates RE: 2007 REAL ESTATE TAX COST DOCUMENTATION
In order to set the real estate tax portion of the capital rate, it is necessary that we obtain additional information regarding your calendar 2007 real estate tax costs, as well as copies of your original real estate tax bills for calendar 2007.
Please complete the Real Estate Tax Statement below and forward with a copy of your 2007 real estate tax bill to Healthcare and Family Services, Bureau of Health Finance, 201 South Grand Avenue East, Springfield, Illinois 62763.
Please send these items in with your completed 2008 cost report. The cost report will not be considered complete and timely filed until this statement and the corresponding real estate tax bills are filed. If you have any questions, please call the Bureau of Health Finance at (217) 782-1630.

2007 LONG TERM CARE REAL ESTATE TAX STATEMENTFACILITY NAME Covenant Health Care Center-Batavia COUNTY Kane
FACILITY IDPH LICENSE NUMBER 0025577
CONTACT PERSON REGARDING THIS REPORT Steve Lavenda
TELEPHONE (847) 236-1111 FAX #: (847) 236-1155
A. Summary of Real Estate Tax Cost
Enter the tax index number and real estate tax assessed for 2000 on the lines provided below. Enter only the portion of thecost that applies to the operation of the nursing home in Column D. Real estate tax applicable to any portion of the nursinghome property which is vacant, rented to other organizations, or used for purposes other than long term care must not beentered in Column D. Do not include cost for any period other than calendar year 2000.
(A) (B) (C) (D)Tax
Applicable toTax Index Number Property Description Total Tax Nursing Home
1. $ $
2. $ $
3. $ $
4. $ $
5. $ $
6. $ $
7. $ $
8. $ $
9. $ $
10. $ $
TOTALS $ $
B. Real Estate Tax Cost Allocations
Does any portion of the tax bill apply to more than one nursing home, vacant property, or property which is not directlyused for nursing home services? YES NO
If YES, attach an explanation & a schedule which shows the calculation of the cost allocated to the nursing home.(Generally the real estate tax cost must be allocated to the nursing home based upon sq. ft. of space used.)
C. Tax Bills
Attach a copy of the 2000 tax bills which were listed in Section A to this statement. Be sure to use the 2000 tax bill whichis normally paid during 2001.
Page 10B
IMPORTANT NOTICE
TO: Long Term Care Facilities with Real Estate Tax Rates RE: 2007 REAL ESTATE TAX COST DOCUMENTATION
In order to set the real estate tax portion of the capital rate, it is necessary that we obtain additional information regarding your calendar 2007 real estate tax costs, as well as copies of your real estate tax bills for calendar 2007.
Please complete the Real Estate Tax Statement below and forward with a copy of your 2007 real estate tax bill to the Department of Public Aid, Office of Health Finance, 201 South Grand Avenue East, Springfield, Illinois 62763.
Please send these items in with your completed 2008 cost report. The cost report will not be considered complete and timely filed until this statement and the corresponding real estate tax bills are filed. If you have any questions, please call the Office of Health Finance at (217) 782-1630.
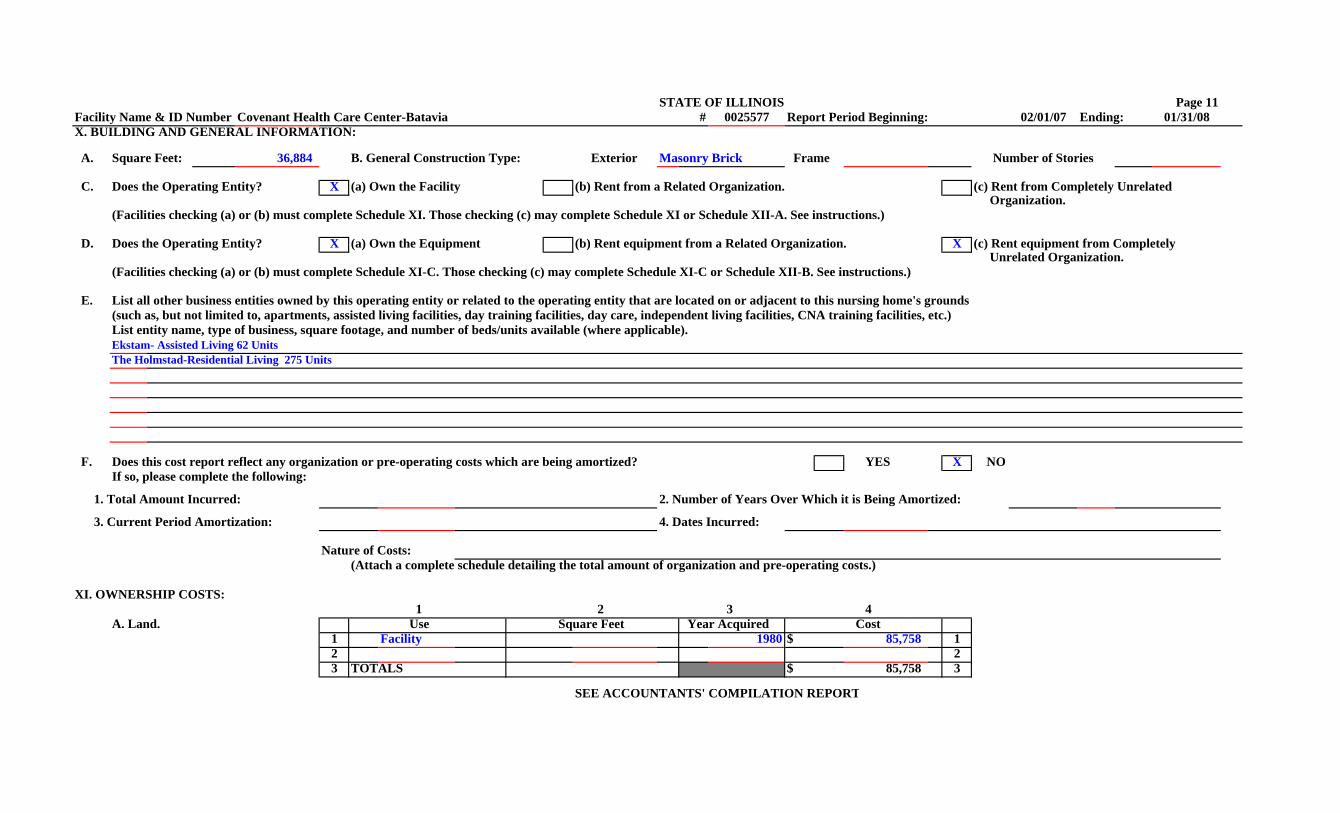
STATE OF ILLINOIS Page 11Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08X. BUILDING AND GENERAL INFORMATION:
A. Square Feet: 36,884 B. General Construction Type: Exterior Masonry Brick Frame Number of Stories
C. Does the Operating Entity? X (a) Own the Facility (b) Rent from a Related Organization. (c) Rent from Completely Unrelated Organization.
(Facilities checking (a) or (b) must complete Schedule XI. Those checking (c) may complete Schedule XI or Schedule XII-A. See instructions.)
D. Does the Operating Entity? X (a) Own the Equipment (b) Rent equipment from a Related Organization. X (c) Rent equipment from Completely Unrelated Organization.
(Facilities checking (a) or (b) must complete Schedule XI-C. Those checking (c) may complete Schedule XI-C or Schedule XII-B. See instructions.)
E. List all other business entities owned by this operating entity or related to the operating entity that are located on or adjacent to this nursing home's grounds(such as, but not limited to, apartments, assisted living facilities, day training facilities, day care, independent living facilities, CNA training facilities, etc.)List entity name, type of business, square footage, and number of beds/units available (where applicable).Ekstam- Assisted Living 62 UnitsThe Holmstad-Residential Living 275 Units
F. Does this cost report reflect any organization or pre-operating costs which are being amortized? YES X NOIf so, please complete the following:
1. Total Amount Incurred: 2. Number of Years Over Which it is Being Amortized:
3. Current Period Amortization: 4. Dates Incurred:
Nature of Costs:(Attach a complete schedule detailing the total amount of organization and pre-operating costs.)
XI. OWNERSHIP COSTS: 1 2 3 4
A. Land. Use Square Feet Year Acquired Cost1 Facility 1980 $ 85,758 12 23 TOTALS $ 85,758 3
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 12Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 2 3 4 5 6 7 8 9 FOR BHF USE ONLY Year Year Current Book Life Straight Line Accumulated
Beds* Acquired Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation4 99 1980 1980 $ 2,546,788 $ 40 $ 63,670 $ 63,670 $ 1,846,421 45 56 67 78 8
Improvement Type**1 9 Various 1982 4,706 20 4,706 92 10 Various 1983 16,662 20 16,662 103 11 Various 1984 832 20 832 114 12 Various 1986 14,644 20 14,644 125 13 Various 1987 12,021 20 12,021 136 14 Various 1988 9,128 20 9,128 147 15 Various 1990 15,226 20 761 761 14,465 158 16 Various 1991 40,083 20 2,004 2,004 36,075 169 17 Various 1992 18,354 20 918 918 15,601 17
10 18 Various 1993 18,931 20 947 947 15,145 1811 19 Various 1994 90,076 20 4,504 4,504 67,557 1912 20 Various 1995 56,935 20 2,847 2,847 39,855 2013 21 Various 1996 84,370 20 4,219 4,219 54,841 2114 22 Various 1997 9,674 20 484 484 5,804 2215 23 Various 1998 4,570 20 229 229 2,514 2316 24 Various 1999 41,323 20 2,066 2,066 20,662 2417 25 Various 2000 5,092 20 255 255 2,291 2518 26 Various 2001 9,810 20 491 491 3,924 2619 27 Various 2003 1,541 20 77 77 462 2720 28 Various 2004 33,456 20 1,673 1,673 8,364 2821 29 2922 30 3023 31 3124 32 3225 33 3326 34 3427 35 3528 36 36
*Total beds on this schedule must agree with page 2. See Page 12A, Line 70 for total**Improvement type must be detailed in order for the cost report to be considered complete. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 12AFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation29 37 $ $ $ $ $ 3730 38 3831 39 3932 40 4033 41 4134 42 4235 43 4336 44 4437 45 4538 46 4639 47 4740 48 4841 49 4942 50 5043 51 5144 52 5245 53 5346 54 5447 55 5548 56 5649 57 5750 58 5851 59 5952 60 6053 61 6154 62 6255 63 6356 64 6457 65 6558 66 66
67 Related Building Company (Pages 12-BLDG & 12A-BLDG) 6768 Related Party Allocations (Pages 12-REP & 12A-REP) 6869 Financial Statement Depreciation 608,963 (608,963) 6970 TOTAL (lines 4 thru 69) $ 3,034,222 $ 608,963 $ 85,142 $ (523,821) $ 2,191,973 70
SEE ACCOUNTANTS' COMPILATION REPORT**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12BFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12A, Carried Forward $ 3,034,222 $ 608,963 $ 85,142 $ (523,821) $ 2,191,973 1
1 2 Site Work 2005 511,923 20 25,596 25,596 102,385 22 3 Foundation / Slab On Grade 2005 352,412 20 17,621 17,621 70,482 33 4 Building Cost 2005 4,748,904 20 237,445 237,445 949,781 44 5 Job Services 2005 1,170,344 20 58,517 58,517 234,069 55 6 Construction Fee 2005 321,082 20 16,054 16,054 64,216 66 7 Fee And Permits 2005 62,348 20 3,117 3,117 12,470 77 8 Legal Fees 2005 15,062 20 753 753 3,012 88 9 Architect And Engineering Fees 2005 719,275 20 35,964 35,964 143,855 99 10 Property Development 2005 813,163 20 40,658 40,658 162,633 10
10 11 Opening In North Wall 2005 4,436 20 222 222 887 1111 12 Expansion 2Nd Floor Dining Room 2005 16,560 20 828 828 3,312 1212 13 New Sidewalks 2007 17,348 20 867 867 1,735 1313 14 New Storage Shed 2007 12,837 20 642 642 1,284 1414 15 Angle Ball Valves 2007 61 20 3 3 3 1515 16 Backflow Preventors For Bldgs. 2007 2,817 20 141 141 141 1616 17 Bathroom Refurb 2007 666 20 33 33 33 1717 18 Building Repairs 2007 315 20 16 16 16 1818 19 Cabinets 2007 13,752 20 688 688 688 1919 20 Carpet & Wallpaper For 1St Flo 2007 106,252 20 5,313 5,313 5,313 2020 21 Conduit For Pon Cabinets In Co 2007 9,737 20 487 487 487 2121 22 Construction Labor 2007 39,492 20 1,975 1,975 1,975 2222 23 Construction Labor & Materials 2007 3,571 20 179 179 179 2323 24 Counter Tops 2007 5,480 20 274 274 274 2424 25 Crash Bar And Key Pad Installa 2007 1,593 20 80 80 80 2525 26 Custom Countertop 2007 561 20 28 28 28 2626 27 Door Frames 2007 46 20 2 2 2 2727 28 Draperies Replaced From Water 2007 660 20 33 33 33 2828 29 Drapery Fabric 2007 83 20 4 4 4 2929 30 Drapery Installation 2007 42 20 2 2 2 3030 31 Drywall Supplies 2007 343 20 17 17 17 3131 32 Electrical Boxes 2007 15 20 1 1 1 3232 33 Electrical Supplies 2007 3 20 0 0 0 33
34 TOTAL (lines 1 thru 33) $ 11,985,405 $ 608,963 $ 532,701 $ (76,262) $ 3,951,367 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.
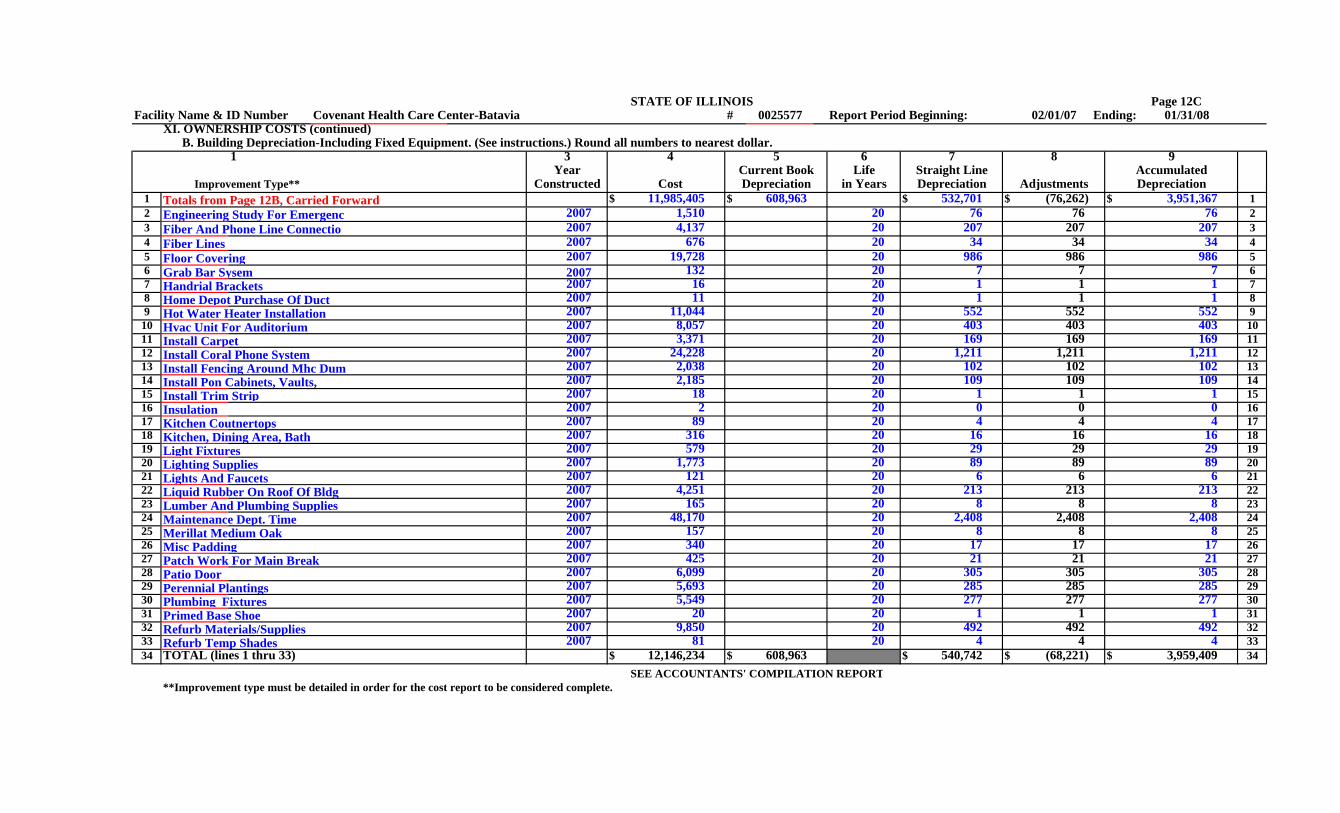
STATE OF ILLINOIS Page 12CFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12B, Carried Forward $ 11,985,405 $ 608,963 $ 532,701 $ (76,262) $ 3,951,367 1
33 2 Engineering Study For Emergenc 2007 1,510 20 76 76 76 234 3 Fiber And Phone Line Connectio 2007 4,137 20 207 207 207 335 4 Fiber Lines 2007 676 20 34 34 34 436 5 Floor Covering 2007 19,728 20 986 986 986 537 6 Grab Bar Sysem 2007 132 20 7 7 7 638 7 Handrial Brackets 2007 16 20 1 1 1 739 8 Home Depot Purchase Of Duct 2007 11 20 1 1 1 840 9 Hot Water Heater Installation 2007 11,044 20 552 552 552 941 10 Hvac Unit For Auditorium 2007 8,057 20 403 403 403 1042 11 Install Carpet 2007 3,371 20 169 169 169 1143 12 Install Coral Phone System 2007 24,228 20 1,211 1,211 1,211 1244 13 Install Fencing Around Mhc Dum 2007 2,038 20 102 102 102 1345 14 Install Pon Cabinets, Vaults, 2007 2,185 20 109 109 109 1446 15 Install Trim Strip 2007 18 20 1 1 1 1547 16 Insulation 2007 2 20 0 0 0 1648 17 Kitchen Coutnertops 2007 89 20 4 4 4 1749 18 Kitchen, Dining Area, Bath 2007 316 20 16 16 16 1850 19 Light Fixtures 2007 579 20 29 29 29 1951 20 Lighting Supplies 2007 1,773 20 89 89 89 2052 21 Lights And Faucets 2007 121 20 6 6 6 2153 22 Liquid Rubber On Roof Of Bldg 2007 4,251 20 213 213 213 2254 23 Lumber And Plumbing Supplies 2007 165 20 8 8 8 2355 24 Maintenance Dept. Time 2007 48,170 20 2,408 2,408 2,408 2456 25 Merillat Medium Oak 2007 157 20 8 8 8 2557 26 Misc Padding 2007 340 20 17 17 17 2658 27 Patch Work For Main Break 2007 425 20 21 21 21 2759 28 Patio Door 2007 6,099 20 305 305 305 2860 29 Perennial Plantings 2007 5,693 20 285 285 285 2961 30 Plumbing Fixtures 2007 5,549 20 277 277 277 3062 31 Primed Base Shoe 2007 20 20 1 1 1 3163 32 Refurb Materials/Supplies 2007 9,850 20 492 492 492 3264 33 Refurb Temp Shades 2007 81 20 4 4 4 33
34 TOTAL (lines 1 thru 33) $ 12,146,234 $ 608,963 $ 540,742 $ (68,221) $ 3,959,409 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12DFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12C, Carried Forward $ 12,146,234 $ 608,963 $ 540,742 $ (68,221) $ 3,959,409 1
65 2 Remove Shrubs 2007 821 20 41 41 41 266 3 Repair Ceiling Front Office 2007 1,006 20 50 50 50 367 4 Repair Damage To Willow Dining 2007 1,218 20 61 61 61 468 5 Repair Water Valve 2007 1,130 20 56 56 56 569 6 Repairs To Sprinkler System In 2007 1,140 20 57 57 57 670 7 Replace Dining Room Ac 2007 7,340 20 367 367 367 771 8 Replace Shower Cabinet- 1St Fl 2007 1,845 20 92 92 92 872 9 Restoration From Sprinkler Bre 2007 27,603 20 1,380 1,380 1,380 973 10 Roller Shades 2007 77 20 4 4 4 1074 11 Roof Repiars-Pm 2007 1,402 20 70 70 70 1175 12 Sd Purchase Sheers/Install 2007 409 20 20 20 20 1276 13 Sealcoating And Striping Park 2007 43,051 20 2,153 2,153 2,153 1377 14 Shelves 2007 6,331 20 317 317 317 1478 15 Sidesplashes 2007 413 20 21 21 21 1579 16 Tile And Plumbing Supplies 2007 13 20 1 1 1 1680 17 Vanity Tops 2007 929 20 46 46 46 1781 18 Water Valves 2007 22 20 1 1 1 1882 19 Zonelines 2007 867 20 43 43 43 1983 20 Concrete Patch Supplies 2008 2,988 20 149 149 149 2084 21 Menards Drywall/Siding/Glass 2008 846 20 42 42 42 2185 22 Refurb Labor 2008 2,320 20 116 116 116 2286 23 Security Camera Equipment 2008 1,288 20 64 64 64 2387 24 2488 25 2589 26 2690 27 2791 28 2892 29 2993 30 3094 31 3195 32 3296 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12EFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12D, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
97 2 298 3 399 4 4
100 5 5101 6 6102 7 7103 8 8104 9 9105 10 10106 11 11107 12 12108 13 13109 14 14110 15 15111 16 16112 17 17113 18 18114 19 19115 20 20116 21 21117 22 22118 23 23119 24 24120 25 25121 26 26122 27 27123 28 28124 29 29125 30 30126 31 31127 32 32128 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12FFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12E, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
129 2 2130 3 3131 4 4132 5 5133 6 6134 7 7135 8 8136 9 9137 10 10138 11 11139 12 12140 13 13141 14 14142 15 15143 16 16144 17 17145 18 18146 19 19147 20 20148 21 21149 22 22150 23 23151 24 24152 25 25153 26 26154 27 27155 28 28156 29 29157 30 30158 31 31159 32 32160 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12GFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12F, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
161 2 2162 3 3163 4 4164 5 5165 6 6166 7 7167 8 8168 9 9169 10 10170 11 11171 12 12172 13 13173 14 14174 15 15175 16 16176 17 17177 18 18178 19 19179 20 20180 21 21181 22 22182 23 23183 24 24184 25 25185 26 26186 27 27187 28 28188 29 29189 30 30190 31 31191 32 32192 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12HFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12G, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
193 2 2194 3 3195 4 4196 5 5197 6 6198 7 7199 8 8200 9 9201 10 10202 11 11203 12 12204 13 13205 14 14206 15 15207 16 16208 17 17209 18 18210 19 19211 20 20212 21 21213 22 22214 23 23215 24 24216 25 25217 26 26218 27 27219 28 28220 29 29221 30 30222 31 31223 32 32224 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12IFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12H, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
225 2 2226 3 3227 4 4228 5 5229 6 6230 7 7231 8 8232 9 9233 10 10234 11 11235 12 12236 13 13237 14 14238 15 15239 16 16240 17 17241 18 18242 19 19243 20 20244 21 21245 22 22246 23 23247 24 24248 25 25249 26 26250 27 27251 28 28252 29 29253 30 30254 31 31255 32 32256 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12JFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12I, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
257 2 2258 3 3259 4 4260 5 5261 6 6262 7 7263 8 8264 9 9265 10 10266 11 11267 12 12268 13 13269 14 14270 15 15271 16 16272 17 17273 18 18274 19 19275 20 20276 21 21277 22 22278 23 23279 24 24280 25 25281 26 26282 27 27283 28 28284 29 29285 30 30286 31 31287 32 32288 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12KFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12J, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
289 2 2290 3 3291 4 4292 5 5293 6 6294 7 7295 8 8296 9 9297 10 10298 11 11299 12 12300 13 13301 14 14302 15 15303 16 16304 17 17305 18 18306 19 19307 20 20308 21 21309 22 22310 23 23311 24 24312 25 25313 26 26314 27 27315 28 28316 29 29317 30 30318 31 31319 32 32320 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12LFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12K, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
321 2 2322 3 3323 4 4324 5 5325 6 6326 7 7327 8 8328 9 9329 10 10330 11 11331 12 12332 13 13333 14 14334 15 15335 16 16336 17 17337 18 18338 19 19339 20 20340 21 21341 22 22342 23 23343 24 24344 25 25345 26 26346 27 27347 28 28348 29 29349 30 30350 31 31351 32 32352 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12MFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12L, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
353 2 2354 3 3355 4 4356 5 5357 6 6358 7 7359 8 8360 9 9361 10 10362 11 11363 12 12364 13 13365 14 14366 15 15367 16 16368 17 17369 18 18370 19 19371 20 20372 21 21373 22 22374 23 23375 24 24376 25 25377 26 26378 27 27379 28 28380 29 29381 30 30382 31 31383 32 32384 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.
STATE OF ILLINOIS Page 12NFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12M, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
385 2 2386 3 3387 4 4388 5 5389 6 6390 7 7391 8 8392 9 9393 10 10394 11 11395 12 12396 13 13397 14 14398 15 15399 16 16400 17 17401 18 18402 19 19403 20 20404 21 21405 22 22406 23 23407 24 24408 25 25409 26 26410 27 27411 28 28412 29 29413 30 30414 31 31415 32 32416 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12OFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12N, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
417 2 2418 3 3419 4 4420 5 5421 6 6422 7 7423 8 8424 9 9425 10 10426 11 11427 12 12428 13 13429 14 14430 15 15431 16 16432 17 17433 18 18434 19 19435 20 20436 21 21437 22 22438 23 23439 24 24440 25 25441 26 26442 27 27443 28 28444 29 29445 30 30446 31 31447 32 32448 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12PFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12O, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
449 2 2450 3 3451 4 4452 5 5453 6 6454 7 7455 8 8456 9 9457 10 10458 11 11459 12 12460 13 13461 14 14462 15 15463 16 16464 17 17465 18 18466 19 19467 20 20468 21 21469 22 22470 23 23471 24 24472 25 25473 26 26474 27 27475 28 28476 29 29477 30 30478 31 31479 32 32480 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12QFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 Totals from Page 12P, Carried Forward $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 1
481 2 2482 3 3483 4 4484 5 5485 6 6486 7 7487 8 8488 9 9489 10 10490 11 11491 12 12492 13 13493 14 14494 15 15495 16 16496 17 17497 18 18498 19 19499 20 20500 21 21501 22 22502 23 23503 24 24504 25 25505 26 26506 27 27507 28 28508 29 29509 30 30510 31 31511 32 32512 33 33
34 TOTAL (lines 1 thru 33) $ 12,249,294 $ 608,963 $ 545,895 $ (63,068) $ 3,964,562 34SEE ACCOUNTANTS' COMPILATION REPORT
**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12-BLDGFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 2 3 4 5 6 7 8 9 FOR OHF USE ONLY Year Year Current Book Life Straight Line Accumulated
Beds* Acquired Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation1 4 $ $ $ $ $ 42 5 53 6 64 7 75 8 8
Improvement Type**1 9 92 10 103 11 114 12 125 13 136 14 147 15 158 16 169 17 17
10 18 1811 19 1912 20 2013 21 2114 22 2215 23 2316 24 2417 25 2518 26 2619 27 2720 28 2821 29 2922 30 3023 31 3124 32 3225 33 3326 34 3427 35 3528 36 36
SEE ACCOUNTANTS' COMPILATION REPORT**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12A-BLDGFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation29 37 $ $ $ $ $ 3730 38 3831 39 3932 40 4033 41 4134 42 4235 43 4336 44 4437 45 4538 46 4639 47 4740 48 4841 49 4942 50 5043 51 5144 52 5245 53 5346 54 5447 55 5548 56 5649 57 5750 58 5851 59 5952 60 6053 61 6154 62 6255 63 6356 64 6457 65 6558 66 6659 67 67
68 6869 6970 TOTAL (lines 4 thru 69) $ $ $ $ $ 70
SEE ACCOUNTANTS' COMPILATION REPORT**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12-REPFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 2 3 4 5 6 7 8 9 FOR OHF USE ONLY Year Year Current Book Life Straight Line Accumulated
Beds* Acquired Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation4 $ $ $ $ $ 45 56 67 78 8
Improvement Type**9 9
10 1011 1112 1213 1314 1415 1516 1617 1718 1819 1920 2021 2122 2223 2324 2425 2526 2627 2728 2829 2930 3031 3132 3233 3334 3435 3536 36
SEE ACCOUNTANTS' COMPILATION REPORT**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 12A-REPFacility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XI. OWNERSHIP COSTS (continued) B. Building Depreciation-Including Fixed Equipment. (See instructions.) Round all numbers to nearest dollar.
1 3 4 5 6 7 8 9Year Current Book Life Straight Line Accumulated
Improvement Type** Constructed Cost Depreciation in Years Depreciation Adjustments Depreciation37 $ $ $ $ $ 3738 3839 3940 4041 4142 4243 4344 4445 4546 4647 4748 4849 4950 5051 5152 5253 5354 5455 5556 5657 5758 5859 5960 6061 6162 6263 6364 6465 6566 6667 6768 6869 6970 TOTAL (lines 4 thru 69) $ $ $ $ $ 70
SEE ACCOUNTANTS' COMPILATION REPORT**Improvement type must be detailed in order for the cost report to be considered complete.

STATE OF ILLINOIS Page 13Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08XI. OWNERSHIP COSTS (continued)
C. Equipment Depreciation-Excluding Transportation. (See instructions.) Category of 1 Current Book Straight Line 4 Component Accumulated Equipment Cost Depreciation 2 Depreciation 3 Adjustments Life 5 Depreciation 6
71 Purchased in Prior Years $ 918,057 $ 84,033 $ 92,940 $ 8,907 10 $ 183,733 7172 Current Year Purchases 7273 Fully Depreciated Assets 7374 7475 TOTALS $ 918,057 $ 84,033 $ 92,940 $ 8,907 $ 183,733 75
D. Vehicle Depreciation (See instructions.)*1 Model, Make Year 4 Current Book Straight Line 7 Life in Accumulated
Use and Year 2 Acquired 3 Cost Depreciation 5 Depreciation 6 Adjustments Years 8 Depreciation 976 2008 Ford E-150 Wheelchair Van 2007 $ 11,944 $ 5,972 $ 2,389 $ (3,583) 5 $ 2,389 7677 7778 7879 7980 TOTALS $ 11,944 $ 5,972 $ 2,389 $ (3,583) $ 2,389 80
E. Summary of Care-Related Assets 1 2Reference Amount
81 Total Historical Cost (line 3, col.4 + line 70, col.4 + line 75, col.1 + line 80, col.4) + (Pages 12B thru 12I, if applicable) $ 13,265,053 8182 Current Book Depreciation (line 70, col.5 + line 75, col.2 + line 80, col.5) + (Pages 12B thru 12I, if applicable) $ 698,968 8283 Straight Line Depreciation (line 70, col.7 + line 75, col.3 + line 80, col.6) + (Pages 12B thru 12I, if applicable) $ 641,225 83 **84 Adjustments (line 70, col.8 + line 75, col.4 + line 80, col.7) + (Pages 12B thru 12I, if applicable) $ (57,743) 8485 Accumulated Depreciation (line 70, col.9 + line 75, col.6 + line 80, col.9) + (Pages 12B thru 12I, if applicable) $ 4,150,683 85
F. Depreciable Non-Care Assets Included in General Ledger. (See instructions.) G. Construction-in-Progress1 2 Current Book Accumulated
Description & Year Acquired Cost Depreciation 3 Depreciation 4 Description Cost86 $ $ $ 86 92 $ 9287 87 93 9388 88 94 9489 89 95 $ 9590 9091 TOTALS $ $ $ 91 * Vehicles used to transport residents to & from
day training must be recorded in XI-F, not XI-D.
SEE ACCOUNTANTS' COMPILATION REPORT ** This must agree with Schedule V line 30, column 8.

STATE OF ILLINOIS Page 14Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XII. RENTAL COSTSA. Building and Fixed Equipment (See instructions.) 1. Name of Party Holding Lease: N/A 2. Does the facility also pay real estate taxes in addition to rental amount shown below on line 7, column 4? If NO, see instructions. YES NO 00
001 2 3 4 5 6
Year Number Original Rental Total Years Total YearsConstructed of Beds Lease Date Amount of Lease Renewal Option*
Original 10. Effective dates of current rental agreement:3 Building: $ 3 Beginning4 Additions 4 Ending5 56 6 11. Rent to be paid in future years under the current7 TOTAL $ 7 rental agreement:
** 8. List separately any amortization of lease expense included on page 4, line 34. Fiscal Year Ending Annual Rent This amount was calculated by dividing the total amount to be amortized by the length of the lease . 12. /2009 $
13. /2010 $ 9. Option to Buy: YES NO Terms: * 14. /2011 $
B. Equipment-Excluding Transportation and Fixed Equipment. (See instructions.) 15. Is Movable equipment rental included in building rental? YES NO 16. Rental Amount for movable equipment: $ 9,798 Description: See Attached Schedule
(Attach a schedule detailing the breakdown of movable equipment)C. Vehicle Rental (See instructions.)
1 2 3 4Model Year Monthly Lease Rental Expense
Use and Make Payment for this Period * If there is an option to buy the building,17 $ $ 17 please provide complete details on attached18 18 schedule.19 1920 20 ** This amount plus any amortization of lease21 TOTAL $ $ 21 expense must agree with page 4, line 34.
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 15Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08XIII. EXPENSES RELATING TO CERTIFIED NURSE AIDE (CNA) TRAINING PROGRAMS (See instructions.)
A. TYPE OF TRAINING PROGRAM (If CNAs are trained in another facility program, attach a schedule listing the facility name, address and cost per CNA trained in that facility.)
1. HAVE YOU TRAINED CNAs YES 2. CLASSROOM PORTION: 3. CLINICAL PORTION: DURING THIS REPORT PERIOD? X NO IN-HOUSE PROGRAM IN-HOUSE PROGRAM
IN OTHER FACILITY IN OTHER FACILITY If "yes", please complete the remainder of this schedule. If "no", provide an COMMUNITY COLLEGE HOURS PER CNA explanation as to why this training was not necessary. HOURS PER CNA
B. EXPENSES C. CONTRACTUAL INCOMEALLOCATION OF COSTS (d)
In the box below record the amount of income your1 2 3 4 facility received training CNAs from other facilities.
FacilityDrop-outs Completed Contract Total $
1 Community College Tuition $ $ $ $2 Books and Supplies D. NUMBER OF CNAs TRAINED3 Classroom Wages (a)4 Clinical Wages (b) COMPLETED5 In-House Trainer Wages (c) 1. From this facility6 Transportation 2. From other facilities (f)7 Contractual Payments DROP-OUTS8 CNA Competency Tests 1. From this facility9 TOTALS $ $ $ $ 2. From other facilities (f)10 SUM OF line 9, col. 1 and 2 (e) $ TOTAL TRAINED
(a) Include wages paid during the classroom portion of training. Do not include fringe benefits. (e) The total amount of Drop-out and Completed Costs for(b) Include wages paid during the clinical portion of training. Do not include fringe benefits. your own CNAs must agree with Sch. V, line 13, col. 8.(c) For in-house training programs only. Do not include fringe benefits. (f) Attach a schedule of the facility names and addresses(d) Allocate based on if the CNA is from your facility or is being contracted to be trained in of those facilities for which you trained CNAs. your facility. Drop-out costs can only be for costs incurred by your own CNAs. SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 16Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XIV. SPECIAL SERVICES (Direct Cost) (See instructions.)1 2 3 4 5 6 7 8
Schedule V Staff Outside Practitioner SuppliesService Line & Column Units of Cost (other than consultant) (Actual or) Total Units Total Cost
Reference Service Units Cost Allocated) (Column 2 + 4) (Col. 3 + 5 + 6)1 Licensed Occupational Therapist 39 - 03 hrs $ $ 70,716 $ $ 70,716 1
Licensed Speech and Language2 Development Therapist 39 - 03 hrs 2,019 2,019 23 Licensed Recreational Therapist hrs 34 Licensed Physical Therapist 39 - 03 hrs 103,452 103,452 45 Physician Care visits 56 Dental Care visits 67 Work Related Program hrs 78 Habilitation hrs 8
# of9 Pharmacy prescrpts 9
Psychological Services (Evaluation and Diagnosis/
10 Behavior Modification) hrs 1011 Academic Education hrs 1112 Other (specify): 12
13 Other (specify): See Supplemental 49,295 141,118 190,413 13
14 TOTAL $ $ 225,482 $ 141,118 $ 366,600 14
NOTE: This schedule should include fees (other than consultant fees) paid to licensed practitioners. Consultant fees should be detailed on Schedule XVIII-B. Salaries of unlicensed practitioners, such as CNAs, who help with the above activities should not be listed on this schedule.
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 17Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XV. BALANCE SHEET - Unrestricted Operating Fund. As of 01/31/08 (last day of reporting year) This report must be completed even if financial statements are attached.
1 2 After 1 2 After Operating Consolidation* Operating Consolidation*
A. Current Assets C. Current Liabilities1 Cash on Hand and in Banks $ 150 $ 1 26 Accounts Payable $ 22,140 $ 262 Cash-Patient Deposits 1,318 2 27 Officer's Accounts Payable 27
Accounts & Short-Term Notes Receivable- 28 Accounts Payable-Patient Deposits 283 Patients (less allowance ) 507,008 3 29 Short-Term Notes Payable 294 Supply Inventory (priced at ) 4 30 Accrued Salaries Payable 234,749 305 Short-Term Investments 5 Accrued Taxes Payable6 Prepaid Insurance 6 31 (excluding real estate taxes) 12,172 317 Other Prepaid Expenses 7,327 7 32 Accrued Real Estate Taxes(Sch.IX-B) 328 Accounts Receivable (owners or related parties) 8 33 Accrued Interest Payable 230,014 339 Other(specify): See Attached Schedule 251,702 9 34 Deferred Compensation 34
TOTAL Current Assets 35 Federal and State Income Taxes 3510 (sum of lines 1 thru 9) $ 767,505 $ 10 Other Current Liabilities(specify):
B. Long-Term Assets 36 See Attached Schedule 61,502 3611 Long-Term Notes Receivable 11 37 3712 Long-Term Investments 12 TOTAL Current Liabilities13 Land 85,758 13 38 (sum of lines 26 thru 37) $ 560,577 $ 3814 Buildings, at Historical Cost 11,751,373 14 D. Long-Term Liabilities15 Leasehold Improvements, at Historical Cost 49,764 15 39 Long-Term Notes Payable 13,118,218 3916 Equipment, at Historical Cost 965,884 16 40 Mortgage Payable 4017 Accumulated Depreciation (book methods) (5,228,468) 17 41 Bonds Payable 4118 Deferred Charges 421,341 18 42 Deferred Compensation 4219 Organization & Pre-Operating Costs 19 Other Long-Term Liabilities(specify):
Accumulated Amortization - 43 See Attached Schedule 4320 Organization & Pre-Operating Costs 20 44 4421 Restricted Funds 21 TOTAL Long-Term Liabilities22 Other Long-Term Assets (specify): 22 45 (sum of lines 39 thru 44) $ 13,118,218 $ 4523 Other(specify): See Attached Schedule 5,673,610 23 TOTAL LIABILITIES
TOTAL Long-Term Assets 46 (sum of lines 38 and 45) $ 13,678,795 $ 4624 (sum of lines 11 thru 23) $ 13,719,262 $ 24
47 TOTAL EQUITY(page 18, line 24) $ 807,972 $ 47TOTAL ASSETS TOTAL LIABILITIES AND EQUITY
25 (sum of lines 10 and 24) $ 14,486,767 $ 25 48 (sum of lines 46 and 47) $ 14,486,767 $ 48
SEE ACCOUNTANTS' COMPILATION REPORT *(See instructions.)
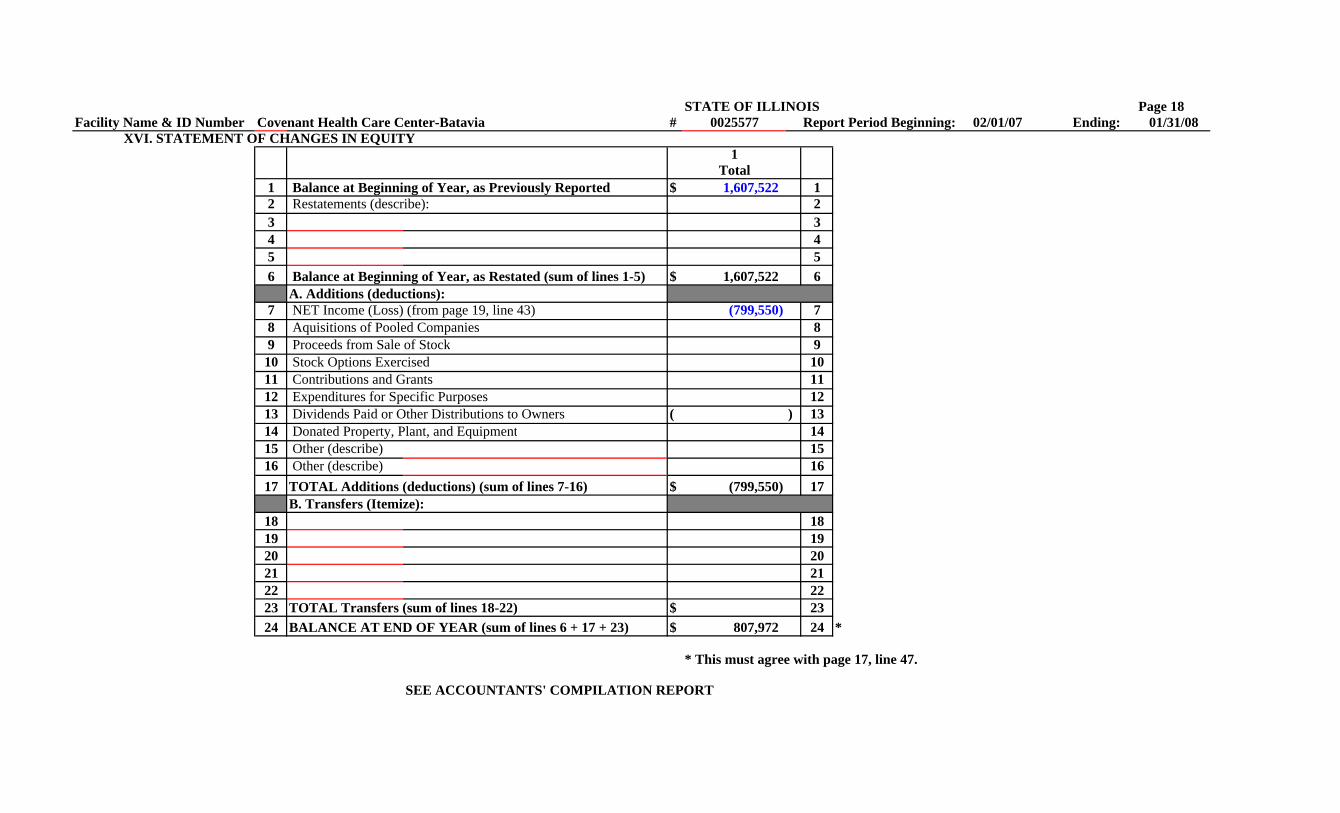
STATE OF ILLINOIS Page 18Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XVI. STATEMENT OF CHANGES IN EQUITY1
Total1 Balance at Beginning of Year, as Previously Reported $ 1,607,522 12 Restatements (describe): 23 34 45 56 Balance at Beginning of Year, as Restated (sum of lines 1-5) $ 1,607,522 6
A. Additions (deductions):7 NET Income (Loss) (from page 19, line 43) (799,550) 78 Aquisitions of Pooled Companies 89 Proceeds from Sale of Stock 910 Stock Options Exercised 1011 Contributions and Grants 1112 Expenditures for Specific Purposes 1213 Dividends Paid or Other Distributions to Owners ( ) 1314 Donated Property, Plant, and Equipment 1415 Other (describe) 1516 Other (describe) 1617 TOTAL Additions (deductions) (sum of lines 7-16) $ (799,550) 17
B. Transfers (Itemize):18 1819 1920 2021 2122 2223 TOTAL Transfers (sum of lines 18-22) $ 2324 BALANCE AT END OF YEAR (sum of lines 6 + 17 + 23) $ 807,972 24 *
* This must agree with page 17, line 47.
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 19Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XVII. INCOME STATEMENT (attach any explanatory footnotes necessary to reconcile this schedule to Schedules V and VI.) All required classifications of revenue and expense must be provided on this form, even if financial statements are attached. Note: This schedule should show gross revenue and expenses. Do not net revenue against expense.
1 2Revenue Amount Expenses Amount
A. Inpatient Care A. Operating Expenses1 Gross Revenue -- All Levels of Care $ 8,167,905 1 31 General Services 1,526,429 312 Discounts and Allowances for all Levels (1,719,795) 2 32 Health Care 2,958,233 323 SUBTOTAL Inpatient Care (line 1 minus line 2) $ 6,448,110 3 33 General Administration 2,027,454 33
B. Ancillary Revenue B. Capital Expense4 Day Care 4 34 Ownership 1,495,533 345 Other Care for Outpatients 5 C. Ancillary Expense6 Therapy 366,526 6 35 Special Cost Centers 370,152 357 Oxygen 642 7 36 Provider Participation Fee 54,204 368 SUBTOTAL Ancillary Revenue (lines 4 thru 7) $ 367,168 8 D. Other Expenses (specify):
C. Other Operating Revenue 37 379 Payments for Education 9 38 38
10 Other Government Grants 10 39 3911 CNA Training Reimbursements 1112 Gift and Coffee Shop 12 40 TOTAL EXPENSES (sum of lines 31 thru 39)* $ 8,432,005 4013 Barber and Beauty Care 48,586 1314 Non-Patient Meals 5,071 14 41 Income before Income Taxes (line 30 minus line 40)** (799,550) 4115 Telephone, Television and Radio 334 1516 Rental of Facility Space 16 42 Income Taxes 4217 Sale of Drugs 90,660 1718 Sale of Supplies to Non-Patients 18 43 NET INCOME OR LOSS FOR THE YEAR (line 41 minus line 42) $ (799,550) 4319 Laboratory 14,153 1920 Radiology and X-Ray 2021 Other Medical Services 227,774 2122 Laundry 62,020 2223 SUBTOTAL Other Operating Revenue (lines 9 thru 22)$ 448,598 23
D. Non-Operating Revenue24 Contributions 35,832 24 * This must agree with page 4, line 45, column 4.25 Interest and Other Investment Income*** 295,236 2526 SUBTOTAL Non-Operating Revenue (lines 24 and 25) $ 331,068 26 ** Does this agree with taxable income (loss) per Federal Income
E. Other Revenue (specify):**** Tax Return? N/A If not, please attach a reconciliation.27 Settlement Income (Insurance, Legal, Etc.) 2728 See Supplemental Schedule 37,511 28 *** See the instructions. If this total amount has not been offset
28a 28a against interest expense on Schedule V, line 32, please include a29 SUBTOTAL Other Revenue (lines 27, 28 and 28a) $ 37,511 29 detailed explanation. SEE ACCOUNTANTS' COMPILATION REPORT
30 TOTAL REVENUE (sum of lines 3, 8, 23, 26 and 29) $ 7,632,455 30 ****Provide a detailed breakdown of "Other Revenue" on an attached sheet.

STATE OF ILLINOIS Page 20Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08XVIII. A. STAFFING AND SALARY COSTS (Please report each line separately.) (This schedule must cover the entire reporting period.) B. CONSULTANT SERVICES
1 2** 3 4 1 2 3# of Hrs. # of Hrs. Reporting Period Average Number Total Consultant Schedule VActually Paid and Total Salaries, Hourly of Hrs. Cost for Line &Worked Accrued Wages Wage Paid & Reporting Column
1 Director of Nursing 1,876 2,115 $ 80,749 $ 38.18 1 Accrued Period Reference2 Assistant Director of Nursing 2 35 Dietary Consultant 61 $ 4,473 01-03 353 Registered Nurses 33,468 36,457 1,047,045 28.72 3 36 Medical Director Monthly 12,000 09-03 364 Licensed Practical Nurses 4,924 5,517 129,447 23.46 4 37 Medical Records Consultant Monthly 1,305 10-03 375 CNAs & Orderlies 80,614 88,367 1,234,027 13.96 5 38 Nurse Consultant Monthly 4,850 10-03 386 CNA Trainees 6 39 Pharmacist Consultant Monthly 1,104 10-03 397 Licensed Therapist 7 40 Physical Therapy Consultant 408 Rehab/Therapy Aides 664 752 11,877 15.79 8 41 Occupational Therapy Consultant 419 Activity Director 366 412 9,456 22.95 9 42 Respiratory Therapy Consultant 4210 Activity Assistants 7,928 8,821 116,725 13.23 10 43 Speech Therapy Consultant 4311 Social Service Workers 4,856 5,450 110,668 20.31 11 44 Activity Consultant 4412 Dietician 12 45 Social Service Consultant Monthly 100 12-03 4513 Food Service Supervisor 4,210 4,479 96,447 21.53 13 46 Other(specify) 4614 Head Cook 2,361 2,515 42,272 16.81 14 47 Chaplain Monthly 34,458 12-03 4715 Cook Helpers/Assistants 19,073 20,351 192,939 9.48 15 48 4816 Dishwashers 1617 Maintenance Workers 11,684 13,006 225,320 17.32 17 49 TOTAL (lines 35 - 48) 61 $ 58,290 4918 Housekeepers 10,153 11,187 121,654 10.87 1819 Laundry 3,083 3,426 37,648 10.99 1920 Administrator 1,811 1,926 85,139 44.21 2021 Assistant Administrator 21 C. CONTRACT NURSES22 Other Administrative 22 1 2 323 Office Manager 23 Number Schedule V24 Clerical 10,709 11,803 208,090 17.63 24 of Hrs. Total Line &25 Vocational Instruction 25 Paid & Contract Column26 Academic Instruction 26 Accrued Wages Reference27 Medical Director 27 50 Registered Nurses $ 5028 Qualified MR Prof. (QMRP) 28 51 Licensed Practical Nurses 5129 Resident Services Coordinator 29 52 Certified Nurse Assistants/Aides 103 2,564 10-03 5230 Habilitation Aides (DD Homes) 3031 Medical Records 1,190 1,378 23,423 17.00 31 53 TOTAL (lines 50 - 52) 103 $ 2,564 5332 Other Health Care(specify) 3233 Other(specify) See Supplemental 63 96 3,552 37.00 3334 TOTAL (lines 1 - 33) 199,033 218,058 $ 3,776,478 * $ 17.32 34 SEE ACCOUNTANTS' COMPILATION REPORT
* This total must agree with page 4, column 1, line 45. ** See instructions.

STATE OF ILLINOIS Page 21Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08XIX. SUPPORT SCHEDULES A. Administrative Salaries Ownership D. Employee Benefits and Payroll Taxes F. Dues, Fees, Subscriptions and Promotions
Name Function % Amount Description Amount Description AmountJeanne Heid-Grubman Administrator 0% $ 85,139 Workers' Compensation Insurance $ 129,843 IDPH License Fee $ 995
Unemployment Compensation Insurance 190 Advertising: Employee Recruitment 6,148 FICA Taxes 272,263 Health Care Worker Background Check 620Employee Health Insurance 397,840 (Indicate # of checks performed 62 )Employee Meals Patient Background Checks 94 940 Illinois Municipal Retirement Fund (IMRF)* Advertising and Public Relations 2,546Life & Disability Insurance 9,909 Subscriptions and Dues 8,072
TOTAL (agree to Schedule V, line 17, col. 1) Pension Plan Expense 85,433 Licenses 2,886(List each licensed administrator separately.) $ 85,139 Other Employee Benefits 9,010B. Administrative - Other Employee Physicals 1,035
Less: Public Relations Expense (909) Description Amount Non-allowable advertising (1,637)Covenant Retirement Communities $ 360,576 Yellow page advertising ( )
TOTAL (agree to Schedule V, $ 905,523 TOTAL (agree to Sch. V, $ 19,661 line 22, col.8) line 20, col. 8)
TOTAL (agree to Schedule V, line 17, col. 3) $ 360,576 E. Schedule of Non-Cash Compensation Paid G. Schedule of Travel and Seminar**(Attach a copy of any management service agreement) to Owners or EmployeesC. Professional Services Description Amount Vendor/Payee Type Amount Description Line # AmountDeloitte & Touche Accounting $ 13,404 $ Out-of-State Travel $Ult Pro Payroll Processing 19,219See Attached Legal 43,002Alan Pepa Architect Services 700 In-State TravelCovenant Retirement Comm. Cost Report 5,750
Seminar Expense 8,265
Entertainment Expense ( )TOTAL (agree to Schedule V, line 19, column 3) TOTAL $ (agree to Sch. V,(If total legal fees exceed $5,000, attach copy of invoices.) $ 82,075 TOTAL line 24, col. 8) $ 8,265
* Attach copy of IMRF notifications **See instructions.SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 22Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08
XIX-H. SUPPORT SCHEDULE - DEFERRED MAINTENANCE COSTS (which have been included in Sch. V, line 6, col. 3). (See instructions.)
1 2 3 4 5 6 7 8 9 10 11 12 13Month & Year Amount of Expense Amortized Per Year
Improvement Improvement Total Cost UsefulType Was Made Life FY2004 FY2005 FY2006 FY2007 FY2008 FY2009 FY2010 FY2011 FY2012
1 N/A $ $ $ $ $ $ $ $ $ $23456789
10111213141516171819
20 TOTALS $ $ $ $ $ $ $ $ $ $
SEE ACCOUNTANTS' COMPILATION REPORT

STATE OF ILLINOIS Page 23Facility Name & ID Number Covenant Health Care Center-Batavia # 0025577 Report Period Beginning: 02/01/07 Ending: 01/31/08XX. GENERAL INFORMATION:
(1) Are nursing employees (RN,LPN,NA) represented by a union? No (13) Have costs for all supplies and services which are of the type that can be billed tothe Department, in addition to the daily rate, been properly classified
(2) Are there any dues to nursing home associations included on the cost report? Yes in the Ancillary Section of Schedule V? Yes If YES, give association name and amount. LSN $4,881
(14) Is a portion of the building used for any function other than long term care services for(3) Did the nursing home make political contributions or payments to a political the patient census listed on page 2, Section B? No For example,
action organization? Yes If YES, have these costs is a portion of the building used for rental, a pharmacy, day care, etc.) If YES, attachbeen properly adjusted out of the cost report? Yes a schedule which explains how all related costs were allocated to these functions.
(4) Does the bed capacity of the building differ from the number of beds licensed at the (15) Indicate the cost of employee meals that has been reclassified to employee benefitsend of the fiscal year? No If YES, what is the capacity? N/A on Schedule V. $ Has any meal income been offset against
related costs? Yes Indicate the amount. $ 5,071(5) Have you properly capitalized all major repairs and equipment purchases? Yes
What was the average life used for new equipment added during this period? 10 Years (16) Travel and Transportationa. Are there costs included for out-of-state travel? No
(6) Indicate the total amount of both disposable and non-disposable diaper expense If YES, attach a complete explanation.and the location of this expense on Sch. V. $ 71,507 Line 10 b. Do you have a separate contract with the Department to provide medical transportation for
residents? No If YES, please indicate the amount of income earned from such a(7) Have all costs reported on this form been determined using accounting procedures program during this reporting period. $ N/A
consistent with prior reports? Yes If NO, attach a complete explanation. c. What percent of all travel expense relates to transportation of nurses and patients? 100% Ln14
d. Have vehicle usage logs been maintained? N/A(8) Are you presently operating under a sale and leaseback arrangement? No e. Are all vehicles stored at the nursing home during the night and all other
If YES, give effective date of lease. N/A times when not in use? N/Af. Has the cost for commuting or other personal use of autos been adjusted
(9) Are you presently operating under a sublease agreement? YES X NO out of the cost report? N/Ag. Does the facility transport residents to and from day training? No
(10) Was this home previously operated by a related party (as is defined in the instructions for Indicate the amount of income earned from providing suchSchedule VII)? YES NO X If YES, please indicate name of the facility, transportation during this reporting period. $ N/AIDPH license number of this related party and the date the present owners took over.N/A (17) Has an audit been performed by an independent certified public accounting firm? Yes
Firm Name: Deloite & Touche, LLP The instructions for the(11) Indicate the amount of the Provider Participation Fees paid and accrued to the Department cost report require that a copy of this audit be included with the cost report. Has this copy
during this cost report period. $ 54,204 been attached? No If no, please explain. Not Complete This amount is to be recorded on line 42 of Schedule V.
(18) Have all costs which do not relate to the provision of long term care been adjusted out(12) Are there any salary costs which have been allocated to more than one line on Schedule V out of Schedule V? Yes
for an individual employee? No If YES, attach an explanation of the allocation.(19) If total legal fees are in excess of $5,000, have legal invoices and a summary of services
SEE ACCOUNTANTS' COMPILATION REPORT performed been attached to this cost report? YesAttach invoices and a summary of services for all architect and appraisal fees.