-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
1/56
Foot and Ankle Fractures
Foot and AnkleFoot and Ankle
FracturesFractures
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
2/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
3/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
4/56
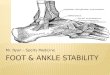
Anatomy
2)Medial
-deltoid ligament (group of four ligaments)
-anterior and posterior tibiotalar
-tibionavicular
-tibiocalcaneal
-stabilize the joint during eversion and
prevent talar subluxation
-20-50% stronger than lateral ligaments
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
5/56
History
History
-mechanism of injury
-ankle and foot position during the injury
-any sounds heard at the time injury
-previous history of ankle injury, any kneeor foot pain
-degree of function after the event.
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
6/56
Physical Exam
Inspection
-deformity, ecchymosis, swelling, perfusion
ROM (normal)
-30 to 50 degrees plantar flexion
-20 degrees dorsiflexion
-25 degrees inversion and eversion
-15 degrees of adduction
-30 degrees of abduction
Palpation
-individual ligaments (MCL,LCL, syndesmotic) and tendons-the
joints above and below the ankle
-important: proximal fibula (Maisonneuve fracture) and the base
of the fifth metatarsal("dancer's fracture").
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
7/56
Special Tests
Anterior Drawer
-integrity of the ATFL
-grasp the heel with one hand and apply a posterior force to the
tibia with theother hand, while drawing the heel forward.
-laxity is compared with the opposite (uninjured) ankle.
-positive test: a difference of 2 mm subluxation compared with
the opposite side
or a visible dimpling of the anterior skin of the affected ankle
(suction sign)
Squeeze Test-tests the integrity of the syndesmotic
ligaments
-examiner places his hand 6 to 8 inches below the knee and
squeezes the tibiaand fibula together
-positive test: results in pain in the ankle, which indicates
injury of thesyndesmotic ligament
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
8/56
X-rays
X-rays
-approx. 10-15% of all traumatic radiographs are of the
ankle
-80% of all ankle injuries get an x-ray, fewer than 15% have
a
significant fracture
Views
-AP, lateral, mortise view (15-20 degrees of internal
rotation)
-AP : malleoli, plafond, talar dome, lateral process of the
talus
-Lateral : ant/post tibial margins, talar neck, post, talar
process andcalcaneus
-Mortise : most important view, medial clear space should
not
exceed 4mm
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
9/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
10/56
Xray Measurments
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
11/56
Ankle Fractures
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
12/56
Classification
Danis-Weber
-based on mechanism of injury
-three fracture types (i.e., A, B, C ),
defined by the location of the fibularfracture
-A - below the tibiotalar joint
-B - at the level of the tibiotalar joint
-C - above the tibiotalar joint
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
13/56
Unimalleolar Fractures
Lateral
-any avulsion
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
14/56
Unimalleolar Fractures- Lateral
Stability depends on the location of the fracture
-Type A (below tibiotalar joint)
-no medial tenderness-BN walking cast
-f/u 1wk to ensure no displacement
-non-wt bearing x3wks then wt bearing for another
3-5 wks-medial tenderness (check mortise for displacement)
-ortho consult
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
15/56
Unimalleolar Fractures- Lateral
Type B and C (at or above the tibiotalar
joint)
-orthopedic consult ?ORIF
-type B : 50% associated with
tibiofibular disruption
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
16/56
Unimalleolar Fractures-Medial
Medial
-commonly associated with lateral and posterior
malleolar disruption-need to examine entire length of the
fibula
(Maisonneuve #)
Isolated medial fracture (nondisplaced)
-non wt bearing x3 wks, f/u after 1 wk
-wt bearing another 3-5 wks
-if very active can ORIF initially!!!
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
17/56
Bimalleolar Fractures
Management
-disruption of two elements of the ring
-ortho consult
-management controversial (ORIF vs closed
reduction and close f/u)
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
18/56
Trimalleolar Fractures
(Cottons fracture)
Management
-disruption of three parts of the ring
(medial/lateral/posterior)
-ortho consult
-ORIF
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
19/56
Pilon #?
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
20/56
Pilon Fractures (Bad!)
Mechanism
-axial compression
-talus driven into the plafond-usually comminuted and displaced
with extensive softtissue swelling
-look for associated injuries
-calcaneus, femoral neck, acetabulum, lumbar
vertebraeManagement
-emergent ortho consult
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
21/56
Tillaux #?
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
22/56
Tillaux fracture (Pediatric)
SH type III of the lateral tibial epiphysis
-extreme eversion and lateral rotation
-adolescence
-medial aspect of epiphysis is closed
-fracture of the lateral aspect and into jointManagement
-ortho consult ORIF
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
23/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
24/56
Foot Fractures
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
25/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
26/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
27/56
X-rays
Xrays
-AP, lateral, oblique(45 degrees of internal
rotation)
-AP and oblique
-best image for the forefoot and midfoot
-Lateral
-best image for the hindfoot and soft tissues
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
28/56
Foot Fractures
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
29/56
Talar #
Talus
General
-second most common fractured tarsal
-3 parts : head, neck, body
-prone to dislocation with foot in plantar
flexion-tenuous blood supply risk ofavascular necrosis
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
30/56
Fractures - Talus
Minor
-chip #s treated like sprains
Treatment
-as above tx as sprain
-fragments >5mm may need excision
Major
-involve head (5-10% of all talar #s), neck (50% of all
major
#s) and body (23% of all talar #s)-high energy mechanism
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
31/56
Fractures Talus
Classification
Classification (Hawkins)Type I fractures
-nondisplaced and lack joint involvement
risk AVN : approx. 10%Type II fractures
-displacement of the talar neck with subluxation or dislocation
of the subtalarjoint and preservation of the ankle joint
Type III fractures
-displaced with dislocation of the talus from both the subtalar
and ankle joints
-risk AVN : >70%
Type IV fracture
-type II injury with associated talar head dislocation
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
32/56
Fractures - Talus
Treatment
-all require ortho consult
-any significant displacement/dislocation,
attempt closed reduction in the ED
-grasp midfoot and apply longitudinal
traction while plantar flexing the foot
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
33/56
Calcaneus (Lovers #)
General
-5x more common in men
-largest and most frequently fractured tarsal bone
-falls (axial load) or twisting mechanisms
-extra-articular (25-35%) good prognosis
-intra-articular (70-75%) not so good prognosis!
-look for associated fractures
->50 % cases have associated other extremity or spinal
fractures
-7% bilateral
-50% will have long-term disability
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
34/56
Calcaneus #s
X-ray
-Boehlers angle (20-40
degrees)
-suspect fracture if
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
35/56
Navicular
General
-most common midfoot #
-blood supply tenuous, risk AVN
-classification: dorsal avulsion # (47% allnavicular #s),
tuberosity and body #s
-mechanism usually eversion injury-pain over the dorsal and
medial aspect offoot with swelling
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
36/56
Navicular
Treatment
Avulsion
-walking cast 4-6wks and ortho f/u
Tuberosity and body
-not displaced, cast (non wt bearing
initially) with close f/u-if displaced or >20% articular
surface
area will require ORIF
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
37/56
LisFranc ?
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
38/56
Lisfranc Injury (tarsometatarsal
fractures/dislocations)
General
-damage to the tarsometatarsal joint (any # or dislocation to
this area istermed a Lisfranc injury)
-commonly missed injury-4% incidence per year of tarsometatarsal
injuries in collegiate footballplayers
-early recognition and anatomical alignment with internal
fixation isnecessary for satisfactory results
-mechanism : high-energy needed to disrupt ligament,
rotationalforce( e.g MVA)
-clinical: severe midfoot pain, significant swelling and
ecchymosis,inability to wt bear
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
39/56
Classification
Classification
1)Total Incongruity
2)Partial Incongruity
3)Divergent
(Homolateral/Divergent, Type A,B,C)
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
40/56
X-ray Findings
1. The medial shaft of the second metatarsal should be aligned
withthe medial aspect of the middle cuneiform on the
anteroposteriorview.
2. The medial shaft of the fourth metatarsal should be aligned
with
the medial aspect of the cuboid on the oblique view.
3. The first metatarsal cuneiform articulation should have
noincongruency.
4. A "fleck sign" should be sought in the medial
cuneiform-secondmetatarsal space. This represents an avulsion of
the Lisfranc ligament.
5. The naviculocuneiform articulation should be evaluated
forsubluxation.
6. A compression fracture of the cuboid should be sought.
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
41/56
Lisfranc - Treatment
Treatment
The key to successful outcome in the Lisfranc
injuries is anatomical alignment-Nondisplaced
-treated with a non-weight-bearing cast for 6 weeks
followed by a weight-bearing cast for an additional
4 to 6 weeks.
-Displaced fractures (>2mm) ORIF
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
42/56
Metatarsal #s
Treatment
-2nd 4th conservative with well padded
shoe
-1st - ORIF
Exception
-displaced (>3mm or angulated-plantar direction >10
degrees)
-closed reduction
-+/- pinning if unstable-non wt bearing cast 4-6 wks
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
43/56
Jones #
Jones #
-transverse # >15mm from the proximal end
of the bone (high rate delayed/nonunion)-occur in >50% pts
with conservative therapy)
Treatment
-ortho f/u-non-wt bearing cast 6-8 weeks or ORIF
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
44/56
X-Rays
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
45/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
46/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
47/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
48/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
49/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
50/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
51/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
52/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
53/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
54/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
55/56
-
8/6/2019 Foot and Ankle Fractures2.Ppt 0
56/56