Embed Size (px)
Citation preview

9/22/15
1
Foot and Ankle in the
Primary Care Setting
“Feets don’t fail me now”
John S. Early, M.D. Texas Orthopaedic Associates, L.L.P.
Dallas, Texas
The Role of the Foot / Ankle Complex
! To provide a stable, weight bearing platform for smooth weight transfer during single limb stance
Foot function in the Role of Ambulation
! Static component – Bones and Ligaments
! Dynamic component – Muscles
Anatomy of Foot Ankle Complex
! 28 Bones
! 30 articular surfaces
! 7 major motor units
Functional Issues
! Static Control – Bones and Ligaments – Mechanical integrity for
motor function – Static foot structure not
dependent on motor function
Anatomy: Ligamentous
Dorsolateral
Plantar

9/22/15
2
Stability: Foot and Ankle
! Tripod balance of talus
! Smooth contours
! Motor control of major functioning joints
Stability Modelling
“3-legged” stool
Talus
• Stability of stool depends on leg position
Foot Function
! Depends on: – Stable structure – Shock absorption – Adaptability to surface
contours ! Determination of Foot
function – Hindfoot – Midfoot – Forefoot
Hindfoot Motion
Hindfoot Mechanics
! Ankle joint controls stride length
! Pivot point for lever arm of foot
Hindfoot Motion

9/22/15
3
Hindfoot Mechanics ! Calcaneal position: Controls gross forefoot
alignment
! Varus hindfoot restricts chopart motion ! Valgus hindfoot increases chopart motion
Midfoot Mechanics
! Rigid link – Minimal joint motion within section
! Shock absorption – Dissipates forces – Strong ligaments
! No bony ground contact – Distributes load
Forefoot Mechanics
! 6 weight bearing bones ! Varied mobility at Tarsometatarsal joints
– Minimal motion at 2 and 3 – 1st ~ 2x greater than middle two – 4th & 5th ~3x greater than 1st
Columnar Approach
Lateral Column Medial column
Central Column
- Normal foot position depends on equal column lengths
Varus hindfoot: Lateral column long
Valgus hindfoot: Medial column long
Foot “Types”
! Weight bearing shape
! No relation to pathology
! No pain…. No problem
Role of Joint Motion
! Create a level platform for gait – Subtalar complex
! Allows foot to conform to ground
! Minimize energy expenditures – Ankle
! Allows transfer of weight to forefoot ! Advances point of contact from heel to toes ! Without ankle greater vertical rise of pelvis and
shorter stride

9/22/15
4
Gait and the Foot
! “Normal Gait” – Minimize energy use – Minimize discomfort
! Important points – Motor function Eccentric in
stance – 10° ankle dorsiflexion for
gait – Use of ligamentous support
allows muscle rest
Functional Issues ! Dynamic Control
– Dependant on motor function
– Stability and mobility of joints
– Allow smooth progression of body weight to next foot ! The less vertical displacement of body mass the better
Motor Balance ! 7 motor units
– Posttib muscles plantarflex
– Pretibial muscles dorsiflex
! Dynamic stability dependent on antagonist pairs
! Strength disparity balanced by mechanical lever arm
Ankle dorsiflexors
! Eccentric work
! Concentric during swing
Ankle Plantarflexors
! Eccentric work
Foot Function: Simple Truths
! The muscles are designed to dissipate the load away from the ligaments that hold the bones together
! The ligaments and bones have a resting stability that is supposed to allow the muscles to rest occasionally
! Failure of one will lead to dysfunction of the other

9/22/15
5
My Foot Hurts and I Can’t do Anything
Everything is a 10 when your foot hurts
Classifying Foot Pain for Medical Urgency
! “I can’t put weight on it” : Unstable injury ! “It hurts to stand” : stable injury hindfoot ! “It hurts to walk” : stable injury midfoot
forefoot ! “It Hurts when I exercise” : chronic instabilty ! “It hurts when run marathons or compete”
Clinical Evaluation
! Observe weight bearing function and position
! Test motor strength with patient’s body weight
! Carefully palpate the foot for pain location ! Move joints to assess pain and stability
Motor Testing
! Observe gait for symmetry / upper body sway
! Single limb stance: balance coordination
! Toe walk: extensor muscle function
! Heel walk: flexor muscle function
Examine the Foot
! Let foot hang to gravity – Best way to see deformity or assymetry – Gravity will allow muscles to relax – Gravity will many times help reduce fractures
or dislocations
Examine the foot
! Examine the “good foot” first – See what “normal” is; relax patient
! Observe deformity: – Supple or stiff? Does it change with weightbearing
! Observe skin
! Palpate all anatomical structures – Bones and tendons

9/22/15
6
Corns and Callous
! Marker of high pressure
! Reaction of skin between bone and shoe
! Callous: broad tissue change
! Corn: deep, localized ! Analogous to splinter
Corns and Callous
! Treatment – Debride thick
tissue
! Daily pumice stone
! Daily skin softener – Alter plantar
pressure
Neuroma
! Damaged nerve – Between metatarsal
heads – Burning, stinging
pain – Distinct area of pain
Neuroma Treatment
! Shoewear
! In shoe orthotics
! Steroid injection
! Transverse ligament release
! Neuroma excision
Neuroma vs Metatarsalgia ! Burning pain ! Pain in shoes ! Between metatarsals ! No toe instability
! Achy pain ! Pain barefoot ! Metatarsal head ! Toe instability
Metatarsalgia
! Local pressure overload
! Uneven metatarsal heads
! Tight heel cord
! Toe deformities
9/22/15
7
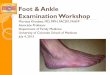
Lesser toe Deformities ! PIP flexion ! Supple MTP joint
! MTP subluxation ! PIP and DIP flexion
Metatarsalgia
! Plantar plate instability
! Progressive deformity ! Raised toe ! Instability test
• Requires operative care
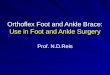
Combinations ! Crossover toes ! Hammer / mallet
Metatarsalgia Treatment
! Heel cord stretch
! In shoe orthotics
! Cushioned shoes
! Correction of toe deformities
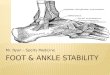
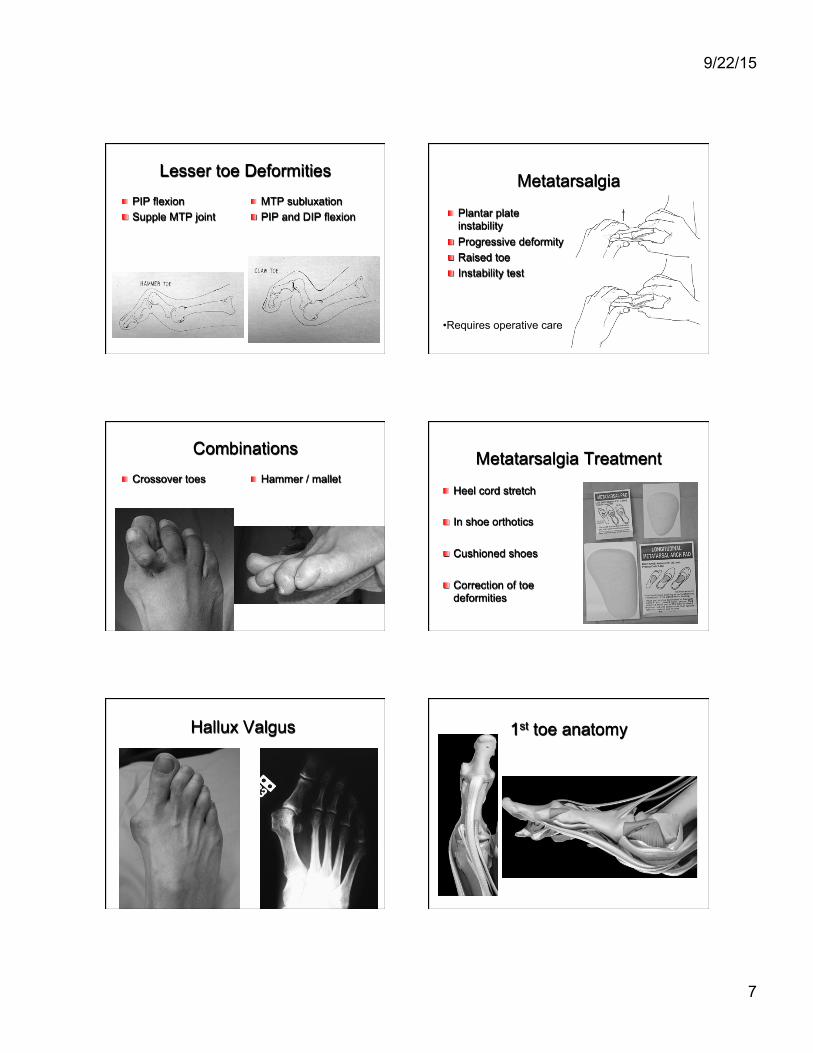
Hallux Valgus 1st toe anatomy

9/22/15
8
Hallux Rigidus Forefoot Treatment
! Motor / soft tissue driven deformities
! Nonoperative: Extra depth wide toed shoes
! Operative: – Bony realignment – Soft tissue realignment
HEEL PAIN
! Plantar Fasciitis: 90% ! Nerve Entrapment: 2% ! Soft Tissue Contusion: 8%
PLANTAR FASCIITIS
! Bow string of foot arch – Supports arch shape
! Pain in am and after rest
! Worse with flat heels ! Tight Gastrocnemius ! No relation to
radiographic spur
Plantar Fasciitis
! 95% improve with non operative treatment ! Resolution can take 12 months ! Treatment consists of:
– Heel lift / cushion – gastrocnemius stretching – NSAIDS – Reassurance – Ice massage
Gastrocnemius Tightness ! Found with knee
extension – Loss of dorsiflexion
! Root of all evil in the foot – Forefoot pain
! Metatarsalgia
– Midfoot pain ! Posterior tibial dysfunction
– Hindfoot pain ! Plantar fasciitis
Achilles Insertion
Gastrocnemius Origin
Soleus Origin

9/22/15
9
Patient Evaluation ! Foot mobility
– Subtalar mobility – Achilles contracture
! gastrocnemius ! gastrosoleus
Gastrocnemius Tightness
! Technique – Internal rotation of foot – No pain in heel – Knee extended – Hold for 30 seconds – 5 or more times daily
Toe Fractures
! Usually isolated ! Usually stable ! Pain with weight ! Treatment
– Correct deformity – Buddy tape – Hard sole shoe
! Up to 3 months recovery
Toe Fractures The exceptions
Metatarsal Fractures
! Acute Trauma ! Repetitive Trauma ! Dorsal pain with
weight ! Point tender ! Initial Radiograph
may be normal
Metatarsal Fracture
! Treatment – Hard sole shoe – Analgesics – Weightbearing as tolerated
! 8 -12 weeks recovery ! Achilles stretch if stress induced

9/22/15
10
Stress Fractures
If tender on bone, treat As fracture till pain gone
7 days 4 weeks
Metatarsal Fractures Operative Care
First Metatarsal Multiple Metatarsals
Achilles Tendon Rupture
! Sudden movement ! Usually a pop felt ! Unable to walk
normally – short step – knee behind ankle
! No single heel lift
Achilles Tendon Rupture
! Asymmetric function ! Gravity check ! Thompson test
– Foot over table – Squeeze calf – No movement foot – Achilles
compromised
Achilles Tendon Treatment ! Immobilize immediately
– Keep tendon from retracting further
! Functional tx: nonoperative
! Operative tx: sew ends back together
! Successful treatment depends on tendon growing together – LONG RECOVERY

9/22/15
11
“ANKLE SPRAINS” “ANKLE SPRAIN” ! Ankle ligament stretch
– Lateral ! Anterior talofibular ligament ! Calcaneal fibular ligament ! Syndesmosis ligament; High ankle
– Medial ! Deltoid ! Spring ligament
“ANKLE SPRAIN” ! Fracture
– Lateral Malleolus – Medial Malleolus – Talus
! Osteochondral lesion ! Lateral process ! Os Trigonum
– Calcaneus: anterior process
“ANKLE SPRAIN” ! Tendon Injury: tear or
subluxation – Medial side
! Tibialis Posterior – Lateral side
! Peroneus Brevis ! Peroneus Longus
“ANKLE SPRAIN” ! Anterior Lateral Pain
– Not on bone; in front
! Get an xray – Lateral and mortise view ankle – AP view of foot

9/22/15
12
High Ankle Sprain
! On field evaluation – Location of pain
! Malleolar tip / syndesmosis
– Anterior drawer ?
– External rotation pain ! Ankle in neutral
Clinical Evaluation of Syndesmotic Injury
! A) Squeeze test
! B) External stress tests – (shown) Keep knee
flexed to 90 degrees – Standing version -
single limb stance with external rotation of body causes pain at syndesmosis
Clinical Evaluation
! Weight bearing stress
Ankle Sprain: Treatment In General
R - Rest I - Ice I - Immobilize C - Compress E - Elevate
Ankle Sprain: Treatment ! Can walk on ankle without instability
– Lace up brace and balance therapy
! Can Not bear weight – Cast in dorsiflexion 7-10 days – Allow weight bearing as comfort allows – Begin bracing and therapy when able to walk
Surgical Candidates ! Bony instability at exam ! Chronic joint laxity ! Failed Rehab ! Be sure no other pathology

9/22/15
13
Joint Sprains: foot
! From stretch to complete dislocation
– Restore anatomical alignment
– Immobilize non weight bearing till pain gone and able to bear weight (6 weeks)
– Balance therapy
Anatomy: Ligamentous
! Lisfranc ligament – Thickest of ligaments in midfoot – Lateral plantar base of medial
cuneiform – Plantar base of 2nd metatarsal – Rotates on its long axis
clockwise ! plantar from cuneiform to lateral
base metatarsal
Anatomy: Function
! Shock absorption mechanism for weight bearing
! joint motion at joints vary – 2nd tarsometatarsal stiffest – 1st and 3rd similar – 4th and 5th with 3 times the motion of
medial joints
Lisfranc: Mechanism of Injury
! Direct loading – Load parallel to joint
surfaces – Significant soft tissue
disruption ! Indirect loading
– Axial load along metatarsals
– Variable bony fracture involved
Lisfranc: Diagnosis
! Tender, swollen midfoot
! Pain with weight bearing
! Plantar ecchymosis
Lisfranc: Stress test No Stress Stress View

9/22/15
14
Tendons about the ankle
! Treatment – Acute Injury / laceration
! Operative repair
– Chronic degeneration ! Bracing for stability ! Surgical reconstruction
– May require bony realignment if deformity present
Posterior Tibial Insufficiency ! Asymmetry in weight bearing foot position ! Unable to single heel rise ! Medial pain and swelling progressing to lateral
pain
Tibialis Posterior Insufficiency
• Surgery: If Painful • Rigid deformity • Uncomfortable bracing • Patient activity level
Posterior Tibial Insufficiency ! Bracing
– For supple deformity – UCBL insert – AFO
Peroneal Subluxation

9/22/15
15
Diabetes and Feet
A Disaster Waiting to Happen
Diabetes
! Prevention is the key to foot preservation ! Constant education of patient necessary ! Diabetic neuropathy major complication
– unable to detect bone stress ! Diabetic vasculopathy major issue in
treatment – No blood flow… no healing
! A warm swollen foot without wound is foot fracture not infection
Diabetic Foot: Risk Factors
! Neuropathy
! Foot deformity
! Ulceration
! Infection
! Amputation
! Vasculopathy
! Amputation to viable level
Extra depth Wide Toed Shoes
! “Ugly Shoe” ! Provides extra room
for forefoot deformity ! Room for insert ! For low demand
patients ! For poor surgical
risk patients
Charcot Foot ! Bony instability ! Repetitive injury ! Warm, swollen
foot ! Bony
destruction ! Intact soft
tissue

9/22/15
16
Charcot Arthropathy ! Ligamentous instability is not Charcot disease
but the start of the process
Charcot: Treatment
! Total Contact cast during active phase – Change 1-3 weeks – Initial non weight
bearing – Continue till coalesence – Attempt to minimize
deformity
! Surgical considerations – Acute injury
! Ligamentous injury
– Complications from deformity ! instability ! ulcer
Simple Treatment Truths
! With foot use: “IF IT HURTS…DON’T DO IT!” ! If it hurts to use immobilize it ! If a motor unit is tender, protect it
! Gait is all about bony stability and motor balance