Embed Size (px)
Citation preview

Follow-Up Results of Surgical Treatment
For Chronic Pancreatitis
Present Status in Japan
Toshio Sato, MD, FACS, Sendai, Japan
Noboru Noto, MD, Sendai, Japan
Seiki Matsuno, MD, Sendai, Japan
Kikuo Miyakawa, MD, Sendai, Japan
In the symposium of the 13th General Meeting of the Japanese Society of Gastroenterological Surgery held in February 1979, the subject “Surgical Treatment of Chronic Pancreatitis” was taken up. One of the present authors (TS) collected the follow-up results of surgery for chronic pancreatitis from the eight institutions that participated in the symposium. This study reports the follow-up results of the authors’ cases and those of the patients collected from these institutions and presents a general view of the current status of surgical treatment for chronic pancreatitis in Japan.
Material and Methods
From 1960 to December 1979, a total of 114 patients with chronic pancreatitis were treated in our clinic. Of these, 87 patients were male and 27 were female. Their ages ranged from 11 to 72 (average 45). The cause was abuse of alcohol in 48 patients (42 percent), gallstones in 12 (11 percent), acute pancreatitis in 13 (11 percent) and pancreatic injury in 6 (5 percent); the cause was unknown in 35 patients (31 percent). Pancreatic calculi were found in 67 patients (59 percent) and diabetes in 35 (31 percent). Of these 114 pa- tients, 103 underwent a total of 110 operations. Among these patients, 82 who had survived more than 6 months after operation were followed up for an average of 6.5 years (range 6 months to 18 years). From the eight institutions including our Tohoku University Hospital, 328 patients with chronic pancreatitis who had survived more than 6 months after operation were subjected to the follow-up study. The institutions which provided the present data are University Hospitals of Hirosaki, Tokyo, Kanazawa, Kumamoto, Nagasaki, the Juntendo, and Hospital of Tokyo Women’s Medical College.
From the Department of Surgery, Tohoku University School of Medicine, Sendai, Japan.
Requests for reprints should be addressed to Toshio Sate, MD. Department of Surgery, Tohoku University School of Medicine, Sendai 980. Japan.
Volume 142, September 1981
Results in the Authors’ Cases
Of our 114 patients, 103 underwent a total of 110 operations. Operative procedures included 19 distal pancreatectomies, 12 pancreaticoduodenectomies, 1 total pancreatectomy, 40 side-to-side pancrea- ticojejunostomies, 9 sphincteroplasties of termina- tion of both the bile and pancreatic ducts, 5 cysto- digestive anastomoses, 13 biliary tract operations, and others. Postoperative death within 30 days was encountered in five patients.
Effect on pain: The effect of operation on ab- dominal pain could be surveyed in 82 patients (Table I). Disappearance and alleviation of pain at the time of follow-up were observed in 67 and 22 percent, re- spectively, of the patients with pancreaticoduode- nectomy, 79 and 21 percent of those with distal re- section, and 68 and 21 percent of those with side- to-side anastomosis. There was no significant dif- ference in the results for the different types of oper- ations. As a whole, disappearance and alleviation of pain were observed in 67 and 26 percent of the pa- tients, respectively, showing a favorable effect of operation in about 90 percent. Of the six patients who underwent sphincteroplasty, only one had elimina- tion of pain.
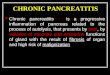
Exocrine function of the pancreas: Pre- and postoperative pancreozymin-secretin tests could be performed under the same conditions in patients with limited types of operations such as distal re- section and biliary tract operation. In our present series, the results of these tests could be compared before and after the operation in only 11 patients, revealing postoperative improvement in 4, no change in 5 and aggravation in 2 (Figure 1). Fat absorption tests performed at the time of follow-up showed that of patients with side-to-side anastomosis, only 2 had
317

Sat0 et al
I I
Preop. Postop.
30
‘day)
Preop. Postop.
PS Test Fat Absorption Test
Postop.
BTPABA Test
0 Cases of Pancreatectomy 0 Cases of Puestow’s Op.
0 Cases of Cholecystectomy and Others EZ Level within Normal Limits
Figure 1. Results of exocrine pancreatic function tests. BTPABA test = test by a syn- thetic peptide ( N-benzoyl-L- tyrosyl-p-amtnoberuotc acid); PS test = pancreozymin-se- cretin test; -I- = mildly im- paired; ++ = moderately im- paired; +++ = marked/y im- paired.
daily excretion of less than 5 g of fecal fat while the remaining 18 had daily excretion of over 5 g. In 13 patients, comparison of fecal fat excretion before and after the operation revealed a postoperative decrease in only 1 and a remarkable increase in 7, while the remaining 5 had almost no change. Two patients who underwent side-to-side anastomosis had fecal fat ievels as high as 60 and 36 g at the time of follow-up. Both had diffuse calcification of the pancreas with severe disturbance of exocrine and endocrine func- tion, and continued to drink alcohol postoperatively. Among those subjected to pancreatectomy of chole- cystectomy, seven patients were available for com- parison of fecal fat levels before operation and at the time of follow-up; the follow-up levels were remark- ably low in one and remarkably high in three patients compared with the preoperative levels. Of the 14 patients available for determination of fecal fat levels at the time of follow-up, a daily level below 5 g was found in only 3 patients, and the remaining 11 had
a level below 10 g. In no patient were the results of exocrine pancreatic function test by a synthetic peptide [1] compared before operation and at the time of follow-up. In 33 patients available for this test at the time of follow-up, a normal level (75 to 95 percent) was seen in only three with pancreatectomy and in one with cholecystectomy. A level of 50 to 74 percent was found in 21 patients (64 percent), in- cluding 10 (71 percent) of 14 patients with side-to- side anastomosis.
Endocrine function of the pancreas: Glucose tolerance tests performed in 53 survivors showed improved results in 7 patients, no change in 13, and worse results in the remaining 33 at the time of fol- low-up. Improvement in glucose tolerance was ob- served in 4 of the 29 patients with side-to-side anas- tomosis, but in none of the patients who underwent resection (Table II).
Postoperative changes in body weight: Changes in body weight between preoperative and follow-up
TABLE I Effect of Operation on Abdominal Pain
Patients Pain at Follow-Up Tvoe of Ooeration (n) Disaooeared Alleviated Persisted
Pancreaticoduodenectomy Distal pancreatectomy Side-to-side pancreaticojejunostomy Sphincteroplasty Cystodigestive anastomosis Wary tract operation Pancreaticolithotomy Left splanchnicectomy Gastrectomy with vagotomy
Total
Numbers in parentheses indicate percentages.
9 14 38
6 2
10 1 1 1
6 (67) 11 (79) 26 (68)
1 1 8 . . . 1 1
82 55 (67)
2 (22) 1 3 (21) 8 (21) 4 4 1 1 . 2 1 . . .
. 21 (26) 6 (7)
318 The American Journal of Surgery

Surgery for Chronic Pancreatitis
TABLE II Postoperative Change in Glucose Tolerance
Type of Operation Patients Glucose Tolerance at Follow-Up (f-3) Improved Unchanged Aggravated
Pancreaticoduodenectomy 7 0 2 5 Distal pancreatectomy 8 0 1 7 Side-to-side pancreaticojejunostomy 29 4 5 20 Miscellaneous 9 3 5 1
Total 53 7 13 33
TABLE Ill Postoperative Change in Body Weight
Type of Operation
Pancreaticoduodenectomy Distal pancreatectomy Side-to-side pancreaticojejunostomy Miscellaneous
Tntal
Patients Body Weight at Follow-Up (n) Gained Unchanged Lost
8 2 1 5 11 2 4 5 32 12 13 7 18 5 10 3
69 21 28 20
determinations were investigated in 69 survivors. A gain of more than 5 percent at the time of follow-up was observed in 25 percent of the patients with pancreaticoduodenectomy, 18 percent of those with distal resection and 38 percent of those with pan- creaticojejunostomy, while the body weight remained unchanged in 36 percent of the patients with distal resection and 41 percent of those with side-to-side anastomosis (Table III). Overall, a gain in body weight was observed in 30 percent, a loss in 29 per- cent and no change in 41 percent.
Follow-up results (Table IV): “Good” indicates that pain was alleviated and the patient had resumed normal activity. “Fair” means that the patient had some alleviation of pain but needed continued treatment, or had changed his job to the light labor category. “Poor” indicates that the pain remained and the patient remained under treatment because of severe complications. Good results were confirmed in 56 percent of the patients with pancreaticoduo-
TABLE IV Follow-Up Results
denectomy, 64 percent of those with distal resection and 80 percent of those with biliary tract operation. Late deaths were observed in 13 patients (16 per- cent), including 2 with pancreaticoduodenectomy, 2 with distal resection, 8 with side-to-side anasto- mosis and 1 with biliary tract operation.
Results in the Collected Cases
Follow-up results were reviewed in patients from the eight institutions. In this study, one type of op- eration which was considered the main procedure was selected from each institution. The types of operation used in the total of 328 cases were pancreatectomy in 91 (28 percent), pancreaticojejunostomy in 141 (43 percent), sphincteroplasty of the termination of both the bile and pancreatic ducts in 21 (6 percent), biliary tract operation in 49 (15 percent), nerve-cutting operation in 9 (3 percent) and others in 17 (5 per- cent). The results of these operations were re- viewed.
Type of Operation (n)
Pancreaticoduodenectomy Distal pancreatectomy Side-to-side pancreaticojejunostomy Sphincteroplasty Cystodigestive anastomosis Biliary tract operation Pancreaticolithotomy Left splanchnicectomy Gastrectomy with vagotomy
Total
Numbers in parentheses indicate percentages.
Good Results
Fair Poor Death
9 14 38
6 2
10 1 1 1
82
5 (56) 1 1 9 (64) 2 1
19 (50) 7 4 1 4 1 :, 1 1
(80) . 1
2 2 8
1
; 45 (55) 17 (21) 7 (8) 13 (16)
Volume 142, September 1981 319

Sat0 et al
TABLE V Effect of Operation on Abdominal Pain in Collected Cases
Patients Pain at Follow-Up Type of Operation (n) Disappeared Alleviated Unchanged
Pancreaticoduodenectomy 28 21 (75) 5 (18) 2 Distal pancreatectomy 56 43 (77) 12 (21) 1 Side-to-side pancreaticojejunostomy 111 79 (71) 25 (23) 7 Distal pancreaticojejunostomy 13 8 (62) 3 (23) 2 Sphincteroplasty 17 7 (41) 9 (53) 1 Cystodigestive anastomosis 9 4 4 1 Biliary tract operation 56 41 11 4 Nerve-cutting operation 9 4 2 3 Miscellaneous 16 9 2 5
Total 315 216 (69) 73 (23) 26 (8)
Numbers in parentheses indicate percentages.
Effect on pain: In 315 patients available for the study, the effect of operation on abdominal pain was examined (Table V). Disappearance and alleviation of pain at the time of follow-up were found in 75 and 18 percent, respectively, of the patients with pan- creaticoduodenectomy, in 77 and 21 percent of those with distal resection and in 70 and 23 percent of those with pancreaticojejunostomy. There was no signifi- cant difference in the results for the three types of operations. On the whole, disappearance and alle-
viation of abdominal pain were observed in 67 and 23 percent of the patients, respectively. On the other hand, nerve-cutting operations performed in nine patients resulted in the disappearance of pain in only four.
Postopekative changes in body weight: In 274 patients available for the study, a gain of more than 5 percent at the time of follow-up compared with preoperative levels was observed in 22 percent of the patients with pancreaticoduodenectomy, 16 percent
TABLE VI Postoperative Change in Body Weight in Collected Cases
Patients Type of Operation (n) Gained
Body Weight at Follow-Up Unchanged Lost
Pancreaticoduodenectomy 27 6 (22) 10 (37) Distal pancreatectomy 46 12 (26) 22 (48) Side-to-side pancreaticojejunostomy 99 43 (43) 38 (38) Distal pancreaticojejunostomy IO 3 7 Sphincteroplasty 19 6 9 Cystodigestive anastomosis 7 4 2 Biliary tract operation 41 13 22 Nerve-cutting operation 8 3 2 Miscellaneous 17 4 5
11 12 18
4 1 6 3 8
Total 274 94 (34) 117 (43) 63 (23)
Numbers in parentheses indicate percentages.
TABLE VII Follow-Up Results in Collected Cases
Type of Operation Patients
(n) Good Results
Fair Poor Death
Pancreaticoduodenectomy 31 19 (61) 5 (16) Distal pancreatectomy 60 40 (67) 8 (13) Side-to-side pancreaticojejunostomy 117 66 (56) 24 (21) Distal pancreaticojejunostomy 14 8 (57) 3 (21) Sphincteroplasty 21 10 6 Cystodigestive anastomosis 10 4 4 Biliary tract operation 49 33 6 Nerve-cutting operation 9 4 2 Miscellaneous 17 8 1
5 6
19 . .
1 1 5
6
Total 328 192 (59) 59 (18) 34 (10) 43 (13)
Numbers in parentheses indicate percentages.
320 The American Journal of Surgery

Surgery for Chronic Pancreatitis
of those with distal resection and 42 percent of those with pancreaticojejunostomy. Only 33 percent of the patients who underwent biliary tract operations gained weight (Table VI).
Follow-up results: Follow-up results judged from our criteria were studied in relation to various types of operations in the 328 patients (Table VII). Good results were observed in 61 percent of the patients with pancreaticoduodenectomy, 67 percent of those with distal resection, 57 percent of those with pan- creaticojejunostomy and 67 percent of those with biliary tract operation. There was no significant difference in the results for the various types of op- erations. Thus, good results were observed in 59 percent, fair in 18 percent and poor in 10 percent of all the patients. Of the nine patients who underwent nerve-cutting operations, only four showed good re- sults. Late deaths were observed in 43 patients (13 percent), including 5 with pancreaticoduodenectomy, 6 with distal resection and 19 with side-to-side anastomosis. ‘I’he main causes of death were diabetes in seven patients, liver cirrhosis, apoplexy and heart failure in three patients each, fulminant hepatitis, uremia and gastric bleeding in two each, and pan- creatic cancer in one.
Pancreatic Ductal Drainage Operation
The effects on abdominal pain, changes in body weight and follow-up results were reviewed in rela- tion to different procedures for pancreatic ductal decompression such as sphincteroplasty of the ter- mination of both the bile and pancreatic ducts (Nardi’s operation), distal pancreaticojejunostomy (DuVal’s operation) and side-to-side pancreaticoje- junostomy (Puestow’s operation), excluding cysto- digestive anastomosis.
Effects on pain: Among patients who survived for more than 6 months, disappearance of pain was identified in 41 percent of those with Nardi’s oper- ation, in 62 percent of those with DuVal’s operation and in as many as 71 percent of those with Puestow’s operation, revealing a significantly higher rate with Puestow’s than with Nardi’s operation (Table V). However, when patients with alleviation of pain were included, the rate of relief of abdominal pain was about 90 percent with all three of these operations, indicating no significant difference among them.
Postoperative changes in body weight: A gain of more than 5 percent in body weight at the time of follow-up was identified in 32 percent of the patients with Nardi’s operation and 30 percent of those with DuVal’s operation. The highest rate of gain, 43 per- cent, was seen in patients with Puestow’s operation, although the difference was insignificant (Table VI). No patient who underwent DuVal’s operation showed a loss in body weight.
Follow-up results: Follow-up results were re- viewed according to our criteria in the patients who survived for more than 6 months (Table VII). Good results were observed in 48 percent of the patients
with Nardi’s operation, 57 percent of those with DuVal’s operation and 56 percent of those with Puestow’s operation, showing the results of the latter two procedures superior to those of Nardi’s opera- tion. Among the patients with fair results, there was no significant difference in the results for the three types of operation.
Comments
As previously reported [2], the indications for operation in our patients with chronic pancreatitis were (1) intractable pain uncontrollable by medical treatment, (2) complications such as pancreatic cyst, abscess or fistula, bile duct stricture and other biliary tract disease, and (3) suspected carcinoma of the pancreas.
According to the collective review of Jordan et al 131, pancreatectomy for chronic pancreatitis was carried out in 27 percent of 1,558 patients, pancrea- ticojejunostomy in 20 percent, biliary tract operation in 18 percent, sphincteroplasty in 17 percent and others in 17 percent. No type of operation predomi- nated, In contrast, the types of operation adopted by the eight institutions of the present series were as follows: pancreaticojejunostomy was most predom- inantly used, in 43 percent of the cases, followed by pancreatectomy in 28 percent, and biliary tract op- eration in 15 percent. Pancreatic ductal drainage was performed in 162 patients, with pancreaticojeju- nostomy in 141 and sphincteroplasty in 21. Of the 141 pancreaticojejunostomies, side-to,-side anastomosis was used most frequently, in 117 patients (72 per- cent), and distal pancreaticojejunostomy was used in only 14 patients (9 percent).
Pancreaticoduodenectomy is recommended by most investigators for patients with advanced chronic pancreatitis with multiple strictures, cysts or pan- creatic calculi localized in the head of the pancreas, evidence of stricture of the bile duct or duodenum, or unsatisfactory results after an operation other than resection. Longmire et al 141, considering that the region of the head of the pancreas functions as a pacemaker of chronic pancreatitis, make it a rule to incise the pancreatic duct in pancreaticojejunostomy as far proximally in the head of the pancreas as pos- sible, and to clear the proximal ductal system of calculi through the papilla of Vater. However, be- cause of the difficulty of removing all pancreatic calculi completely, even with t.hese procedures, they have been carrying out extended proximal pancrea- ticoduodenectomy and preserving 5 to 15 percent, of the tail of the pancreas in an attempt to prevent di- abetes. In a recent report, Traverso et al 151 empha- size the rationale of this operation as a resectional procedure for chronic pancreatitis.
For patients with chronic pancreatitis, Frey et al first advocated 95 percent distal pancreatectomy. However, according to their recent report [6], com- parison of 40 to 80 percent. and 80 to 95 percent distal resection of’ the pancreas apparently disclosed that
Volume 142, September 1991 321

Sat0 et al
endocrine and exocrine insufficiency and their complications occurred more frequently after 80 to 95 percent than after 40 to 80 percent distal pancre- atectomy. That finding led them to recommend that distal resection be limited to 80 percent of the pan- creas whenever possible. On the other hand, there are very few reports on total pancreatectomy in patients with chronic pancreatitis. According to Braasch et al [7], a total of 53 patients with chronic pancreatitis throughout the world’have undergone total pancre- atectomy so far. In the Lahey Clinic, total pancrea- tectomy was performed in 26 patients with end-stage chronic pancreatitis up to 1976. Total pancreatec- tomy, they insist, should be performed as the last resort in patients in whom pancreatic ductal drainage or other types of pancreatectomy have proved un- satisfactory.
With regard to surgical procedures for patients with chronic pancreatitis, most workers lately maintain the following policy: Patients with evidence of stricture of the pancreatic duct showing distal di- latation should first undergo decompression of the pancreatic duct. In patients with severe symptoms despite the absence of ductal dilatation, or in those with no effect from a decompression procedure, some type of pancreatectomy is indicated. Various nerve- cutting operations are generally regarded as inef- fective. In a recent report, White and Slavotinek [8] also reported that celiac ganglionectomy used in 22 patients was less effective in relieving symptoms than the other procedures.
In our own patients who survived more than 6 months after operation, we found disappearance of pain in 67 percent and alleviation in 26 percent, with overall favorable results in more than 90 percent of all patients. There was no significant difference in the results for the three main types of operations: pan- creaticoduodenectomy, distal resection and side- to-side anastomosis. Among the collected patients from the eight institutions who survived more than 6 months after operation, 69 percent had disap- pearance of pain and 23 percent had alleviation of pain. As in our cases, the three types of operations showed no significant difference in the effect on pain. Traverso et al [5] also pointed out that there was no statistical difference in the follow-up results in the groups with resection and ductal drainage. In the patients from the eight institutions, pancreatic ductal drainage procedures showed the best results in terms of disappearance of pain in patients who underwent side-to-side anastomosis. Jordan et al [3], comparing 24 patients with side-to-side anastomosis and 6 pa- tients with DuVal’s operation at the time of follow- up, found a favorable effect on pain in 70 percent of the former and 50 percent of the latter. Thirty per- cent of our patients, predominantly those with anastomosis, gained weight postoperatively. Of the patients collected from the eight institutions, 34 percent gained weight, and the largest proportion of
them had pancreatic ductal drainage. A weight gain was predominantly linked to Puestow’s operation. Using our criteria, 55 percent of our patients had good and 21 percent fair follow-up results. In the collected patients, the follow-up results were good in 59 percent and fair in 18 percent.
The question of interest is whether or not pan- creatic ductal drainage can improve pancreatic function. In our patients, evidence has hardly con- firmed that pancreatic ductal drainage can improve pancreatic exocrine function. Nevertheless, a weight gain at the time of follow-up was observed in 38 percent of the patients with Puestow’s operation. A weight gain may be explained by the increased food intake due to postoperative relief of pain. On the other hand, of our 29 patients available for the glu- cose tolerance test at the time of follow-up, 20 showed aggravated glucose tolerance compared with preop- erative levels. Prinz et al [9] reported that diabetes developed in 30 percent of nondiabetic patients some time after direct drainage of the pancreatic duct. They pointed out that the postoperative diabetes seen in these patients might reflect improved nutri- tion due to increased caloric intake rather than pro- gression of chronic pancreatitis.
Dixon and Englert [IO] recommend early surgical treatment for chronic pancreatitis on the basis that any delay is likely to aggravate the disease. Many surgeons insist on early drainage of the pancreatic duct on the basis that some patients with mild dis- orders show postoperative improvement in pancre- atic function. On the other hand, Hayakawa and Kondo [11], from the viewpoint of internal medicine, reported their experience with conservative treat- ment of 66 patients with pancreaticolithiasis for an average of 10 years since the onset of symptoms, and observed that the pain disappeared, was alleviated or was absent throughout the course in 83 percent of the patients. Along with the similar process in pa- tients with noncalcification, they pointed out that nearly 80 percent of patients with noncomplicated chronic pancreatitis could be controlled conserva- tively, and early detection and adequate treatment of the disease might be able to prevent progression of pancreatitis.
From the surgical standpoint, “early” in the course of pancreatitis indicates the stage of the disease in which pancreatic duct dilatation is not so severe and pancreatic dysfunction is still mild. The internists maintain that in this stage patients can be treated conservatively. However, there remains doubt whether any conservative treatment can diminish the diameter of a once-dilated pancreatic duct. Dixon and Englert [IO] advocate early operation for chronic pancreatitis and insist that their “early” stage should coincide with progressive aggravation of the patient’s condition, accompanied by at least one complication. Where to draw the limit of conservative treatment is an extremely difficult problem. At present, no
322 The American Journal of Surgery

Surgery for Chronic Pancreatitis
chance of recovery with conservative treatment is defined as one of the indications for operation. We must, for the time being, subject to surgical treat- ment those patients whose condition shows aggra- vation to some extent. We hold the view that for pa- tients with persistent pain and beginning weight loss, operations should be carried out before the devel- opment of diabetes or calcification if the pancreatic duct is dilated.
In surgical treatment for chronic pancreatitis, it is necessary to evaluate beforehand the condition of each individual patient accurately and thoroughly. As we reported, pancreatic ductal drainage can bring relief of abdominal pain in about 90 percent of pa- tients, but it cannot be expected to help improve impaired function of the pancreas. This demon- strates the need for postoperative supervision of the patients; especially, resumption of drinking must be strictly prohibited. The advice of Frey et al [6] that surgeons who are interested only in the technical aspects of pancreatic surgery should not operate on patients with chronic pancreatitis emphasizes the importance of long-term follow-up care of the pa- tients. Surgeons, even more than internists, must have a thorough knowledge and understanding of chronic pancreatitis.
Summary
The results of surgical treatment for chronic pancreatitis at our clinic and in the eight leading institutions of Japan were reviewed in a total of 328 cases. Abdominal pain disappeared or was alleviated in about 90 percent of the patients who survived more than 6 months after operation, There was no signif- icant difference in the effect on pain among the three main types of operations: pancreaticoduodenectmy, distal resection and pancreatic ductal drainage. In
the collected cases, however, complete disappearance of pain was reported more often in patients subjected to Puestow’s operation than in those who underwent Nardi’s operation. The patients who underwent pancreatic ductal drainage had a greater postoper- ative weight gain than those without drainage, in both our patients and the collected cases. In the collected cases, Puestow’s operation was predomi- nantly linked to postoperative weight gain. Evidence of pancreatic functional improvement, either in en- docrine or in exocrine, was very meager.
References
1. Arvanitakis C, Greenberger NJ. Diagnosis of pancreatic disease by a synthetic peptide. A new test of exocrine pancreatic function. Lancet 1976;1:663.
2. Sato T, Saitoh Y, Noto N. Appraisal of operative treatment for chronic pancreatitis. Am J Surg 1975;129:621.
3. Jordan GL, Strug BS, Crowder WF. Current status of pancrea- ticojejunostomy in the management of chronic pancreatitis. Am J Surg 1977;133:46.
4. Longmire WP Jr, Tompkins RK, Traverso LW, Forrest JF. The surgical treatment of pancreatic disease. Jpn J Surg 1978;8:249.
5. Traverso LW, Tompkins RK, Urrea PT, Longmire WP Jr. Surgical treatment of chronic pancreatitis. Ann Surg 1979;190: 312.
6. Frey CF, Child CG III, Fry W. Pancreatectomy for chronic pan- creatitis. Ann Surg 1976;184:403.
7. Braasch JW, Vito L, Nugent FW. Total pancreatectomy for end-stage chronic pancreatitis. Ann Surg 1978; 188:317.
8. White TT, Slavotinek AH. Results of surgical treatment of chronic pancreatitis. Ann Surg 1979; 189:217.
9. Prinz RA, Kaufman BH, Folk FA, Greenlee HB. Pancreaticoje- junostomy for chronic pancreatitis. Arch Surg 1978;113: 520.
10. Dixon JA, Englert E Jr. Growing role of early surgery in chronic pancreatitis-a practical clinical approach. Gastroenterology 1971;61:375.
11. Hayakawa T, Kondo T. Surgical indication for chronic pan- creatitis evaluated from the natural history of the disease. Jpn J Gastroenterol Surg 1979;12:647 (Jpn).
Volume 142, September 1991 323