Embed Size (px)
Citation preview

Archives of Disease in Childhood, 1989, 64, 1394-1402
Personal practice
Follow up studies: design, organisation, and analysisL M M MUTCH,* M A JOHNSON,t AND R MORLEYt
*Social Paediatric and Obstetric Research Unit, University of Glasgow, tOxford Region Child DevelopmentProject, John Radcliffe Hospital, Oxford, and *Medical Research Council Dunn Nutrition Unit, Cambridge
The follow up of infants who were exposed toadverse perinatal events is an important componentof perinatal audit. We need to know whether thechanges in perinatal care that have undoubtedlyresulted in their improved survival have altered theincidence of impairments in their long term health,growth, or neurodevelopmental state. Moreover,recent improvements in diagnostic imaging tech-niques carried out in the neonatal period may con-siderably enhance our ability to predict longer termoutcome.1-3 Their importance lies not only in theiruse to monitor the eventual outcome for individualchildren, but because therein could lie some ex-planation of the mechanisms linking clinical patho-logical entities to the lesions visualised.4
In the absence of reliable validated routine healthsurveillance of all children, special studies arerequired to monitor the effects of rapidly changingperinatal practice and to evaluate specific com-ponents of care. Studies from any one centre areoften too small to answer the questions being posed.The purpose of this paper is to discuss ways in whichthe design of following studies could be madecompatible to enable multicentre collaboration, andthus provide more rapid feedback to neonatalpaediatricians on current issues.
Background
In 1981, Kiely and Paneth outlined some of thetheoretical problems that beset the design andreporting of follow up studies.5 In the same year,Sinclair et al expanded on the methodologicalrequirements for a proper evaluation of neonatalintensive care.6 This included testing of the efficacyof particular treatments, their effectiveness in thefield, the efficiency of these treatments in relation toother calls on resources, and the implications(economic and otherwise) of making them availableto all who need them. In this paper we discuss some
of the other issues and practical problems en-countered in mounting follow up studies and suggestsome solutions, but our main aim is to stimulatefurther discussion that will eventually encouragemore effective use of the vast amount of resourceand expertise expended in the name of 'follow up'.
How is the information derived from follow upstudies used?
Most reported follow up studies based on hospitalpopulations are descriptive or observational; that is,information is collected on the outcome of cohortsof children with particular characteristics-forexample birthweight groups, infants who wereventilated, infants with seizures, and so on. Thisinformation tends to be misused in two ways.Firstly, associations between perinatal variables andoutcome are observed, and there is then a tendencyto ascribe-erroneously-a causal relationshipbetween the two. Descriptive follow up studies can,however, only generate hypotheses that need to betested in a new cohort. Causal relationships can bedetermined only by a randomised study design.Secondly, the information collected is comparedwith other similar observations made in previousyears or in other centres. Differences in outcomeare ascribed to differences in care, but they maymerely reflect differences in the study population(either over time or between centres), or a lack ofuniformity in the way outcomes have been definedor ascertained.
How can we improve on study design?
The design of the study must be prospective, withthe aims, the population, and the outcomes definedbefore collection of data starts. The selection of acomparison group must also be considered.
1394
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

Follow up studies: design, organisation, and analysis 1395
DEFINITION OF THE AIMSThe aim of the study should be defined at the outsetand usually falls into one of the following categories:to estimate the incidence of disease, disorder, or
impairment in a defined cohort followed up for a
specific period; to evaluate the effectiveness orotherwise of a particular therapeutic intervention;or to test a specific aetiological hypothesis.A descriptive follow up study of the first type can
provide important information on the naturalhistory and prognosis of a condition, and can
identify the presence or absence of associationsbetween perinatal events and outcome. The evalua-tion of specific treatments is best achieved byrandomised clinical trials with predefined measure-
ments of outcome made by investigators who are
preferably 'blind' to the original treatment. The roleof each type of study is illustrated in the followingexample.A study of the natural history and prognosis of a
group of infants with neonatal seizures identified a
subgroup of infants born at full term whose seizuresoccurred in the first 48 hours of life and who had sus-tained an intrapartum insult.7 This gave rise to theaetiological hypothesis that changes in intrapartummanagement might reduce the number of infantsborn at full term with early seizures. It was thenpostulated that the rate of such seizures mightprovide a useful marker of the quality of intra-partum care.8 Two case control studies were set upto investigate the relationship between variousadverse outcomes of pregnancy including earlyneonatal seizures and the quality of care in preg-
nancy and labour; both showed that there was astrong association between suboptimal care andearly seizures.9 10 The hypothesis was sustained in alarge randomised controlled trial of intrapartumelectronic fetal heart rate monitoring.11
DEFINITION OF THE STUDY COHORTThe criteria by which the study cohort is selectedshould be clearly defined and will be determined bywhether the study is investigating prevalence, or theeffects of an intervention, or testing a specificaetiological hypothesis.
In a study of the prevalence of morbidity, thepopulation should be geographically defined. Thispermits evaluation of care to a total populationwhose characteristics can be defined, and hence thefindings can be compared with other populations forwhich reference statistics are available, takingaccount of any differences in these variables.Results from tertiary referral centres are difficult tointerpret, because they are confounded by thetransfer of mothers and infants between units. Anexample of the importance of this source of bias was
described by Horwood et al who showed that 28% ofthe reduction in mortality experienced after theopening of a new intensive care centre wasaccounted for by the transfer in from outside thegeographical region of mothers who had beenthought, incorrectly, to be at high risk of a pooroutcome. 12Enrolment in such a study can be on the basis of
all births, or all live births. It is, however, importantto ensure that a birth is also defined by some othervariable such as-for example, all births over500 g-because there is marked variation in thedefinition of live birth both internationally andwithin countries. 13 For the purposes of internationalcomparison, it is preferable to use standard cate-gories such as those recommended by the WorldHealth Organisation for birthweight groupings.'4
In the United Kingdom, information on all birthsto women resident in a defined geographical areacan be obtained through statutory birth notificationsthat are held by district medical officers in Englandand Wales, and chief administrative medical officersin Scotland and Northern Ireland. In most districtgeneral hospitals outside the big conurbations, thedifference between the hospital based populationand the geographically based one is not large. Thoseinfants who are in the geographical cohort, but whowere not included in the hospital population, can beeasily identified and included. In large cities whereinfants could be cared for in a wide range of tertiarycare centres dictated by the availability of an inten-sive care cot, it is not possible to evaluate the qualityof care from information on the outcome of infantstreated in a single unit.
In conducting studies to test aetiological hypo-theses, or intervention studies, it is not necessary touse a geographically defined population. Once thestudy cohort has been defined it is important that allare accounted for in the analysis. In the special caseof an antepartum or intrapartum intervention study,the women entered into the study and all the infantsborn to those women should be included in theevaluation of the intervention. For example, in atrial of a tocolytic agent to prevent preterm labour,the condition of all the infants resulting from all thepregnancies being studied needs to be compared,whether they are born prematurely or not. Itcould-for example-be argued that postponingdelivery might subject the fetus to additionalunsuspected hazards.
DETERMINATION OF SAMPLE SIZEThe sample should be large enough to provide ananswer, either on its own or in conjunction withother similarly structured studies, to the mainquestion being asked in the study. The involvement
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

1396 Mutch, Johnson, and Morley
of parents and children in a follow up study that haslittle chance of producing an answer to the questionposed should be regarded as unethical.
In a study of prevalence in a defined population,the study size is obviously constrained by theavailable eligible entrants. In testing a hypothesis itis important that the sample size is big enough topermit identification of enough subjects with thepredefined outcome. For example, there is littlepoint in examining 100 infants for the incidence ofan outcome that occurs in only 1/1000. Furthermore,the sample needs to be large enough to detectintergroup differences that are also biologicallyimportant.
It is difficult to give general advice because eachstudy has a different perspective; a statisticianshould be consulted to advise on the necessarycalculations based on the reported frequency of agiven dichotomous outcome, or some measure ofcentral tendency and dispersion such as the meanand standard deviation of a continuous outcomemeasure such as growth or a developmental score. 15It should be borne in mind that the standarddeviation for a developmental score is likely to begreater in a 'high risk' population than in thestandardisation sample for the test.
In order to study infrequent outcomes (such asretinopathy of prematurity) or a limited population(such as infants weighing less than 1000 g at birth)within a reasonable time span, multicentre collabor-ation is essential to achieve sufficient numbers. Forthis to be successful, standard methods for identifyingand reporting those outcomes are needed.
DEFINITION OF OUTCOMESThe outcomes to be measured will depend on theaim of the study, but whatever they are they must bespecified and clearly defined before the start of thestudy. The outcome should be relevant to the childor family, or likely to improve our understanding ofthe aetiology or treatment of the condition beingstudied. The availability of funds or personnel, orboth, may impose constraints on the study, makingthe choice of the most important and valid outcomemeasures even more essential.Commonly reported outcomes are death, neuro-
developmental state, sensory impairment, mor-bidity, growth, behavioural attributes, and learningability. It is important that the outcome to bemeasured can be defined accurately. In the case ofdeath, for example, the definition is simple, whereasneurodevelopmental impairment or emotionalproblems would require careful definition before astudy was undertaken.
In making a full evaluation of the effects of anytreatment it is important to consider outcomes that
have economic implications. Measures such as theneed for hospital admission, length of stay, the needfor increased primary health care contacts, and theuse of ancillary services are important factors thatcould influence whether recommendations based onthe findings of a particular study are accepted.
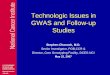
Measuring outcomesThe tests (tools) used in measuring outcome shouldhave both reproducibility and validity. These termsare illustrated in the figure (JC Sinclair, personalcommunication).Even with standardised 'tests' inaccuracies, im-
precision, and biases can arise. There is a realchance of interobserver variation-and also intra-observer variation-and these need to be tested in apilot study. It has been shown that further trainingcan help to improve the level of agreementbetween observers.'6 The problem is accentuatedwhen non-standardised tests, sometimes devised bythe examiner, are used before being subjected torigorous evaluation. There is a large number oftests currently in use for assessing a wide variety offunctions at differing ages and we do not intend todiscuss specific ones here. There is, however, a needfor some consensus on the optimal ages for testingchildren and the most appropriate tests at each agein order to achieve comparability between studies.Outcome measures that require intensive assess-
ment by highly trained personnel are not feasible ifthe study population is large. Conversely, smallerstudies on their own, or 'nested' in large trials, mayprovide the opportunity for in depth examination ofunsuspected effects of the treatments being com-pared.
Other sources of outcome informationIn addition to data collected in the study there areseveral other sources which can be used to find outabout the longer term health and development ofchildren. Information on deaths in the study cohortcan usually be obtained from routinely collecteddata held by districts on the child health register, asthe death of a child is entered immediately to ensurethat parents are not contacted for routine appoint-ments.Where appropriate, for a small cost, the National
Health Service record of individuals held by theOffice of Population Censuses and Surveys can be'flagged' so that the researcher will be informed ofthe death or emigration of study children, or theirmovement from one family practitioner committeearea to another.
Parents, health visitors, general practitioners,community child health doctors, hospital paediatri-cians, and teachers as well as research workers
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

Follow up studies: design, organisation, and analysis 1397
0
0-a0
- 0, -0_
0
DI. )
'@$0
Figure Reproducibility and validity: (a) the shot is valid (it hit the target) and reproducible (it hit the target everytime); (b) one shot is valid, but the others went wide (not reproducible); (c) shots all hit the same spot(reproducible), but missed the target (not valid); and (d) shots neither valid nor reproducible.
committed to the study can all provide their ownperspectives on the child. The ideal, but expensive,situation would be to draw on all these sources,using them to validate each other. The advantagesand disadvantages of the various sources aresummarised in table 1. There is a need for validationof inexpensive methods of obtaining information onchildren's health and development. Such validationstudies should be incorporated in more detailed andcostly studies.
Reporting outcomesIn order to compare outcomes of studies fromdifferent centres the diseases, disorders, or impair-ments should be defined in a standard way.
It is helpful to consider outcomes in the waydescribed in the International Classification ofImpairments, Disabilities and Handicap. 7 A diseaseor disorder causes an impairment, which is definedas '. . . any loss or abnormality of psychological,
physiological or anatomical structure or function'. Adisability resulting from this impairment is '. . . anyrestriction or lack of ability to perform an activity inthe manner or within the range considered normalfor a human being'. Handicap is the disadvantageresulting from an impairment or disability that'. . . limits or prevents the fulfilment of a role that isnormal (depending on age, sex, and social andcultural factors) for that individual'.
Impairments-Of these three terms, impairmentsare the most amenable to definition. For example,consensus has been reached on the standard descrip-tion and reporting of the grades of retinopathy ofprematurity.'l A working group has developed astandard format for the recording and reporting ofthe motor deficit in cerebral palsy.19 An attempt toprovide uniformity in describing and identifyingneurological impairments has been proposed byAmiel-Tison and Stewart.20
l0
0
0*0t 0 0 -
- .0 0 0
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

1398 Mutch, Johnson, and Morley
Table 1 Summary of methods of follow up
Sources of information
Routinely collected data (available in UK):
Preschool health (school health) systemHospital activity analysis
Parents:Parental questionnaires
Health diaries
Inexpensive
Accommodate large study populations
InexpensiveAccommodate large study populationsUnique knowledge of child's abilities and
disabilities and social and behaviouralattributes
Improved accuracy of recall
Lack of uniformity between districtsin child health surveillance
Limited detail
Inaccuracy of recall'Subjectivity' biasInadequately validated
'Subjectivity' biasInadequately validated
No additional funding if part of routinesurveillance
Can accommodate quite large numbersSpecific training feasible
No additional funding if part of routineCan accommodate quite large numbersUse of standardised testsExplores cognitive development
Additional workloadUnstandardised 'tools'Interobserver variation
Additional workload
Hospital based personnel:Routine outpatient
Special study personnel:Standard protocol
Multiple observersSingle observer
No additional visits
Longer time for assessmentCan be seen in own surroundingsIn depth study possibleLarger numbers possibleRelative consistency in observationIn depth study possibleFiner discrimination possible between
groups
Lack of uniformity in testingInterobserver variationLimited time for assessmentClinical environment
Additional appointmentsCost
Interobserver variationSmall numbers onlyCostUndetected systematic error
Disability-Assigning grades of severity to thedisability arising from impairments is fraught withproblems. In prevalence studies it is important thatthe 'cut off' point for ascertaining the conditionunder review is predefined for comparative pur-
poses, as children with minimal problems may wellnot be universally recognised, and the reader needsto know the threshold of inclusion.The description of disability needs to be related to
a particular task and the developmental age of thechild and must take account of the use andusefulness of aids.2' In most currently reportedstudies, however, there is a lack of uniformity indescribing disability in children and this is com-pounded by the arbitrary categorisation of disabilitiesinto grades of 'mild', 'moderate', and 'severe',which may have different meanings in differentstudies. Furthermore, a physician's perception of
the severity of a disability will depend on his or herclinical experience.
In a population based study in the Northernregion of England a system was developed to cate-gorise the degree of disability in a group of childrenwith established cerebral palsy in which aspects ofmobility, physical dependence, social and economicimplications and resource use were summed toprovide an overall measure of disability.22
In a recent study of disabilities in children by theSocial Survey Division of the Office of PopulationCensuses and Surveys, considerable attention waspaid to all these points; it will be a useful referencesource. 23
One possible way forward would be the develop-ment of a 'minimum data set' incorporating standardways of categorising death, accepted definitions ofimpairments, and guidelines on assigning grades of
Advantages Disadvantages
Health visitors:Assessment
Teachers:Assessment
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

Follow up studies: design, organisation, and analysis 1399
severity. This would permit meaningful accuratecomparisons between studies.
Handicap-This is a particularly difficult outcomefor comparative use, as it depends heavily onsubjective factors and is a reflection of the attitudeswithin the family and society as a whole to peoplewith disabilities. It is best avoided in the types ofstudy described here.
CHOICE OF A COMPARISON GROUPIn a controlled trial the control group should berandomly chosen from those eligible for entry to thestudy and therefore should be comparable with theindex group in every respect other than the inter-vention being studied.
In an observational study there is no easy answer
to the choice of a comparison group.5 As previouslystated, comparison of the outcome of hospitalpopulations either over time (historical controls) or
between centres may result in misleading inferences.The choice of a comparison group depends on the
question being asked. The choice must be betweenmatched and 'unmatched' controls; if the preferenceis for matched controls, then subjects could bematched on antecedent factors such as maternal age,
parity, birth weight, or gestational age, dependingon the design of the study. In considering develop-mental outcomes, however, the over-riding deter-mining factors are sex, social class,24 and preschool
25experience, so there is a rational basis formatching on those variables. Often it is better tomatch for only exceptional factors and adjust forothers in the analysis. Overmatching can introducedifficulties in interpretation by taking out of con-sideration the very factor being investigated.
In a prevalence study in, for example, a very lowbirthweight population where the outcome to bemeasured is relatively uncommon, more than onecontrol for each index case may be necessary toprovide more accurate estimates of the increasedrelative risk experienced by the study subjects. Butthe advantage to be gained by increasing the numberof controls soon falls off15; statistical advice isneeded on this point.The use of siblings as a comparison may have the
advantage that socioeconomic variables and experi-ence of parenting are likely to be the same. In somefamilies, however, there will be no siblings and anyfinding limited to those cases who had a siblingwould not necessarily be relevant for the one childfamily. Birth order in itself has been shown to have a
significant effect on developmental score almostequal to that of the sex of the child.26At an older age group, classroom controls of the
same sex and social class are an attractive alterna-
tive, but this necessarily excludes children notable to attend school who may be represented to agreater extent in the index group.
If a concurrent comparison is carried out betweentwo geographically defined populations with thesame ascertainment criteria for measures of out-'come, observed differences may indeed reflectdifferences in care; these may, however, also be theresults of known differences in the sociodemo-graphic structure of the populations, or to some asyet unidentified confounding factor. Informationshould be collected on factors known to be relatedto the outcome being measured, so that adjustmentcan be. made in the analysis for any markedimbalance.
TRACING CHILDRENTracing children can be time consuming, and severalsources may need to be tapped.27 High ascertain-ment rates are extremely important, because biasesarise when follow up rates are low and it should berecognised that the lower the follow up rate themore inaccurate the estimate of the true rate ofimpairment. There is, furthermore, some evidencethat children who are difficult to trace may be at ahigher risk of an abnormal outcome. The extent towhich this is true has recently been quantified in astudy of very low birthweight children in theNorthern region of England; children not seen onthe first attempt had a sevenfold increased risk ofimpairment compared with those who were easilytraced.28
If parents are aware from the time of birth or soonafter that their children will form part of a study,contact can be maintained in a number of ways. Inthe 1946 British cohort used to study child health,birthday cards are used to keep in touch.29 Assess-
Table 2 Information required to tap sources helpful intracing children
Child:
Mother:
Full name, date of birth, last address,National Health Service number,telephone number
Full name, maiden name, National HealthService number
Father: First name or initialsGeneral practitioner: Name, addressGrandparents: Name, address, telephone numberUseful sources:
Child health registers held by districtsFamily practitioner committees - registration departmentsNational Health Service Central Registry in Southport (England),
in Edinburgh (Scotland), and in Belfast (Northern Ireland)Telephone directoriesLocal education authorities for children of school ageLocal post offices and electoral rolls
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

1400 Mutch, Johnson, and Morley
ments in the early months of life can help inestablishing rapport with the family. The informa-tion that can be helpful in tracing children within theUnited Kingdom, and agencies and other sourcesthat can be used, are outlined in table 2.
In most follow up studies there are a few childrenwho cannot be traced. Every effort should be madeto restrict their number as much as possible. It isimportant to record the number of untraced childrenand to compare their known characteristics withthose of the children assessed.
Analysis and reporting of results
The selected study groups form the basis for theanalysis. Statistical advice should be sought toensure that the analysis of the data and interpreta-tion of the results are appropriate, and this shouldbe a stated part of the initial design of the study.There are several circumstances that deserve specialconsideration.
REFUSAL BY PARENTS TO PARTICIPATEParents may refuse because they suspect the motivesof the assessor, particularly if their child is alreadythe subject of concern on the part of the welfareauthorities. A further explanation of the aims of thestudy will often secure their cooperation. In othercases parents may suspect that their child is notdeveloping normally and do not welcome confirma-tion of their suspicions. It is also understandablethat assessments may be unwelcome when familydynamics are disturbed, or where a child is severelyimpaired and already having regular assessments.Information from general practitioners and paedia-tricians may assist in these cases.
REFUSAL OF CHILDREN TO PARTICIPATESome children refuse to comply with testing. Thereis evidence that they do so because they are unableto do a test.30 For those testing small children, it isoften difficult to decide whether a child is failing todo a test or refusing to try it. Experience gained in apilot study will help in defining a 'refusal'. Ounstedet al recommend exclusion of such children fromthe analysis of the variable concerned with a clearstatement about their numbers and characteristics, 30and Stewart (AL Stewart, personal communication)recommends assigning them to a grade above failurebut below pass (for example, the 'suboptimal range'in the McCarthy test31).
EXCLUSIONS AFTER ASSESSMENTIt is difficult-to make a general statement about thisissue. In a randomised trial, once subjects have beenassigned to a treatment they should all be included
in the analysis. In an observational study of thedevelopmental outcome of for example, childrenwhose mothers had had some late onset pregnancycondition, then the inclusion of a child with agenetically determined syndrome would be inappro-priate. When language development is a principaloutcome of interest, then children whose firstlanguage differs from that of the tester are at adisadvantage, and not only in the sphere of language.Decisions about how to deal with these situationsshould be discussed at the outset of the study.
DISTRIBUTION OF CONFOUNDING VARIABLESThe first priority is to determine the distribution inthe study group, and in the population from whichthe study sample was derived, of characteristics thatmight affect outcome such as birth weight, gesta-tional age, sex, social class, birth order, and pre-school experience.
DESCRIPTION AND CLASSIFICATION OF OUTCOMEVARIABLESThe distribution of the outcome variables in thewhole study group and separately in the comparisongroups should be examined first. If the results ineach group are normally distributed and have thesame variance, comparison of means and standarddeviations will be appropriate. Information on thenumber of subjects whose results fall below the10th centile can be a useful additional way todescribe the results especially if they are variableslike developmental quotients or anthropometricmeasures. By itself, comparing groups of childrenfalling below the 10th centile for a test may be acrude measure, and it is analogous to measuring theheight of a group of people by placing a bar at thestrategic height and seeing how many people couldwalk under it. Nevertheless, using cut off points ofthis type can also serve to increase the chance ofdata dependent choices to highlight or minimiseapparent differences.Where the results are skewed (that is, not
normally distributed) statistical advice on the bestand most informative approach should be sought. Inthe absence of a comparison group the findings canbe described in terms of both means and standarddeviations, and the numbers falling below the 10thcentile.
Costing and funding
Follow up studies that do not use routine sources ofinformation are usually costly to mount; they areusually project funded and estimates of their truecost are difficult to come by. It would be valuablefor future researchers to have information on how
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

Follow up studies: design, organisation, and analysis 1401
Table 3 Costing a follow up study
Personnel costs:Study design, including statistician's timeTracing childrenTraining of personnelConducting a pilot studyTesting interobserver variationOrganising appointments or questionnairesAssessing childrenCommunicating findings to those responsible for clinical careData entry and processingData analysis (with computing and statistical advice)Writing up time
Administrative and clerical costs:Preparation of assessment protocolsStationeryPhotocopying, telephone, and postage
Equipment costs:Weighing and measuring equipmentKits for developmental testsStandard test recording formsComputer and other office equipment
Travel costs:Costs for either parents or study personnel
much a study has cost available as part of anappendix to publication. The items to be consideredare outlined in table 3.
Estimates of travel costs depend on local circum-stances and how far removed in age the subjects arefrom the age at entry into the study. For example, ofa birth cohort contacted first at the age of 4 years,80% were still living within 25 miles of the districtgeneral hospital in which they were born, 12% werebetween 25 and 100 miles away, and 1% were morethan 200 miles away25 (unpublished data).
Ethical perspective on follow up studies
It could be said that a physician has a responsibilityto monitor the outcome of any treatment prescribedas part of routine health care: to ensure-forexample-that a child's hearing is intact aftertreatment for an ear infection. The responsibility isperhaps less well defined in the perinatal periodwhere the effectiveness of treatment for the motheris not always interpreted in the light of possibleeffects on the child.The follow up systems developed by most special
care nurseries provide a continuing clinical servicefor patients and their parents and have a counsellingand supportive role as well as being a means ofassessing overall health and development. Carefullydesigned follow up studies can be incorporatedwithin these systems, but a fine balance needs to be
achieved between fulfilling the needs of individualpatients and meeting the rather stringent require-ments of a research study.
Ethical approval must be sought for follow upwhere this is not considered an integral part ofcontinuing clinical care. This is particularly impor-tant if a 'normal' control group is enrolled. Parents'consent should be sought after an explanation of thepurpose of the study and what is entailed in thefollow up assessment. This can be done orally or byletter, and parents can consent either by opting in oropting out.32 General practitioners should beinformed that their patient has consented to takepart in a study. Results should be communicatedpromptly so that they are as relevant as possible tocurrent practice; parents and general practitionersare entitled to receive the reports of assessments.
If we are concerned to monitor the effects ofchanging perinatal practice, then it must also beappreciated that the effect of follow up studies inthemselves has never been evaluated fully. On theone hand, benefits may accrue from the earlyidentification of-for example-sensory deficit andthe implementation of treatment; on the other handit may be that the identification of other problems ofdevelopment, some of which cannot be 'cured',might cause unnecessary anxiety to parents andchildren. It is therefore important that studiesshould not be undertaken unless they are properlydesigned and of sufficient size to answer specificquestions.33 This counsel of perfection could welllimit the number of studies but would undoubtedlyincrease their usefulness.
We acknowledge with thanks the helpful advice of Professor EAlberman and Dr G Escobar who commented on a later draft, andcolleagues in the National Perinatal Epidemiology Unit who readearlier drafts; also the help of the department of medical illustra-tion at the University of Edinburgh.
References
Stewart AL, Thorburn RJ, Hope PL, Goldsmith M, LipscombAP, Reynolds EOR. Ultrasound appearance of the brain in verypreterm infants and neurodevelomental outcome at 18 monthsof age. Arch Dis Child 1983;58:598-604.
2 de Vries LS, Dubowitz LMS, Dubowitz V, et al. Predictivevalue of cranial ultrasound in the newborn baby: a reappraisal.Lancet 1985;ii:137-40.
3 Stewart AL, Reynolds EOR, Hope PL, et al. Probability ofneurodevelopmental disorders estimated from ultrasoundappearance of brains of very preterm infants. Dev Med ChildNeurol 1987;29:3-11.
4 Bax MO. Forward from neonatology. Dev Med Child Neurol1987;29:1-2.
5 Kiely JL, Paneth N. Follow up studies of low birthweightinfants: suggestions for design, analysis and reporting. Dev MedChild Neurol 1981 ;23:96-9.
6 Sinclair JC, Torrance GW, Boyle MH, Horwood SP, Saigal S,Sackett DL. Evaluation of neonatal intensive care programs. NEngl J Med 1981;305:489-94.
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from

1402 Mutch, Johnson, and Morley
7 Dennis J. Neonatal convulsions: aetiology, late neonatal statusand long term outcome. Dev Med Child Neurol 1978;20:143-58.
8 Dennis J, Chalmers I. Very early neonatal seizure rate: apossible epidemiological marker of the quality of perinatal care.Br J Obstet Gynaecol 1982;89:418-26.
9 Niswander K, Elbourne D, Redman C, Henson G, Chalmers I,Macfarlane A. Adverse outcome of pregancy and the quality bfobstetric care. Lancet 1984;ii:827-31.
10 Minchom P, Niswander K, Chalmers I, et al. Antecedents andoutcome of very early neonatal seizures in infants born at orafter term. Br J Obstet Gynaecol 1987;94:431-9.MacDonald D, Grant A, Sheridan-Pereira M, Boylan P,Chalmers I. The Dublin randomised controlled trial of intrapar-tum fetal heart rate monitoring. Am J Obstet Gynecol 1985;152:524-39.
12 Horwood SP, Boyle MH, Torrance GW, Sinclair JC. Mortalityand morbidity of 500-1499 g birthweight infants liveborn toresidents of a defined geographic region before and afterneonatal intensive care. Pediatrics 1982;69:o13-20.
13 Mugford M. International comparisons of definitions of vitalevents. World Health Stat Q 1983;36:201-12.
14 World Health Organisation. International classification ofdiseases. 9th Revision. Geneva: WHO, 1970.
15 Gore SM, Altman DG. Statistics in practice. London: BritishMedical Association, 1982.
16 Blair E, Stanley FJ. Interobserver agreement in the classifica-tion of cerebral palsy. Dev Med Child Neurol 1985;27:615-22.
17 World Health Organisation. International classification ofimpairments, disabilities and handicaps. Geneva: WHO, 1980.
18 International Committee for the Classification of Retinopathy ofPrematurity. An international classification of retinopathy ofprematurity. Pediatrics 1984;74:127-33.
19 Evans P, Johnson A, Mutch L, Alberman E. A standard formfor recording clinical findings in children with a motor deficit ofcentral origin. Dev Med Child Neurol 1989;31:119-27.
20 Amiel-Tison C, Stewart A. Follow up studies during the firstfive years of life: a pervasive assessment of neurologicalfunction. Arch Dis Child 1989;64:496-502.
21 Saigal S, Rosenbaum P, Stoskopf B, Milner R. Follow-up of
infants 501-1500 g birthweight delivered to residents of ageographically defined region with perinatal intensive carefacilities. J Pediatr 1982;100:606-13.
22 Jarvis S, Hey E. Measuring disability and handicap due tocerebral palsy. In: Stanley F, Alberman E, eds. The epidemio-logy of the cerebral palsies. Clinics in Developmental MedicineNo 87. Spastics International Medical Publications. London:Heinemann Medical Books, 1984.
23 OPCS Surveys of Disability in Great Britain. Report No 3. Theprevalence of disability among children. London: HMSO, 1989.
24 Ounsted MK, Osborn ML, Sleigh G, Good FJ. A method ofdevelopmental assessment at 4 years and some associatedfindings. Early Hum Dev 1979;3:1-19.
25 Dennis J, Johnson A, Mutch L, Yudkin P, Johnson P. Acid-basestatus at birth and neurodevelopmental outcome at four and ahalf years. Am J Obstet Gynecol (in press).
26 Morley R, Cole TJ, Powell R, Lucas A. Mother's choice toprovide breast milk and developmental outcome. Arch DisChild 1988;63:1382-5.
27 Hewitt A. In: Illsley R, Mitchell R, eds. Low birth weight: amedical, psychological and social study. Chichester: John Wiley,1984:105-32.
28 Wariyar U, Richmond S. Morbidity and preterm delivery:importance of 100% follow up. Lancet 1989;i:387-8.
29 Douglas JWB, Blomfield JM. Children under five. London:Allen and Unwin, 1958.
30 Ounsted MK, Cockburn J, Moar VA. Developmental assess-ment at four years: are there differences between children whodo or do not cooperate? Arch Dis Child 1983;58:280-9.
31 McCarthy scales of children's abilities. New York: PsychologicalCorporation, 1970.
32 Mutch L, King R. Obtaining parental consent - opting in oropting out? Arch Dis Child 1985;60:979-80.
33 Aylward GP. Developmental assessment: caveats and a cry forquality control. J Pediatr 1987;110:253-254.
Correspondence to DrLMM Mutch, Social Paediatric and ObstetricResearch Unit, University of Glasgow, 1 Lilybank Gardens,Glasgow G12 8RZ.
copyright. on M
arch 9, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.64.10_Spec_N
o.1394 on 1 October 1989. D
ownloaded from