Embed Size (px)
Citation preview

Jo ur nal o f Ca se s inOb st et ri cs &G ynec olog y
J Cases Obstet Gynecol, 2015;2(2):22-24
Case Report
Foix-Alajouanine Syndrome: Report of a case with spinal cord haemorrhage induced by normal vaginal delivery
A. Bruce Janati1, Naif ALGhasab2,*, Aboubaker Osman2, Afnan Mohammed Altamimi3, Amani Fahad Al-Thwainy3, Fazal Haq4 1Center for Neurology, Fairfax, VA, 22031, USA, 2Department of Medicine, King Faisal Hospital, Riyadh, Saudi Arabia, 3Medical Student, King Saud University, Riyadh, Saudi Arabia, 4General Practitioner, King Khaled Hospital, Haeil, Saudi Arabia
Abstract-
hemorrhage after a normal vaginal delivery in a 32-year-old primigravida with Foix-Alajouanine syndrome. During pregnancy the patient received subcu--
orrhagic transformation (presenting with acute compressive myelopathy) posed by normal vaginal delivery in patients with Foix-Alajouanine syndrome.
Key words:Foix Alajouanine syndrome, spinal arteriovenous malformation, vaginal delivery
Introduction
Fyoung men in 1926 [1]. It was thought to be a subacute myelopathy produced by a thrombotic process of the spi-nal cord that ultimately caused death [2]. At autopsy, they discovered necrosis of the spinal cord and numerous thick-ened tortuous vessels lying on the surface of the cord. In 1931, Lhermitte et al. associated this syndrome with spinal arteriovenous malformation (AVM) [3] and attributed the myelopathy to thrombosis of the abnormal vessels within the spinal canal. Over the years, several diagnostic rubrics have been used interchangeably with Foix-Alajouanine syndrome (FAS) including angiodysgenetic necrotizing myelopathy, subacute necrotizing myelopathy, and venous
Journal of Cases in Obstetrics & Gynecology22
Article history:Received 12 11 2014Accepted 30 01 2015
*Correspondence: Naif Saad ALGhasabDepartment of Neuroscience, King Faisal Hospital, Riyadh, Saudi Arabia Phone: 00966507886878 Email: [email protected]
congestive myelopathy [4]. The syndrome is generally believed to be irreversible with a poor prognosis [5,6]. In most patients with this condition, sensory symptoms and leg weakness are the most common initial symptoms [7-9].
-currence of intramedullary hemorrhage after nor-mal vaginal delivery (NVD) in a patient with FAS who had received anticoagulation therapy for pre-vention of deep vein thrombosis during pregnancy.
Case presentation
A 32- year-old primigravid Saudi female came to the emergency room of King Khalid Hospital on Feb 10, 2012 with a chief complaint of weakness of both legs and in-ability to void shortly after a normal vaginal delivery.
deep vein thrombosis of the left lower extremity in the -
ed on low molecular weight heparin (Enoxaparin) 0.6 ml subcutaneously twice a day which was continued until

April 2015www.jcasesobstetgynecol.com23
delivery. On examination the patient was conscious and alert. Her vital signs were as follows: blood pressure 111/76 mmHg, temperature 36.6 °C, pulse rate 92 per minute, res-piration rate 12 per minute. Oxygen saturation was 94%. The pre-labor obstetric examination prior to presentation to King Khaled Hospital had shown the uterus to be term size with a normal tone and a conceptional age of 38 weeks. A regular fetal heart rate of 150 beats per minute was pres-ent. Initially, vital signs were normal and there were no pal-lor, icterus or pedal edema. No skin rash or petechiae were present. Her routine blood tests and coagulation profile were normal. She delivered a 3.5 kg baby with an Apgar score of 7/10 and 9/10 in one and five minutes, respectively. However, under observation, she deteriorated neurological-ly, prompting her urgent transfer to King Khaled Hospital.
General physical examination was unremarkable at ad-mission except for a distended bladder. Neurological ex-amination showed a normal mental status. Cranial nerves were intact. Evaluation of the motor system showed normal
Jo ur nal o f Ca se s inOb st et ri cs &G ynec olog y
strength in the upper extremities. She had flaccid paraple-gia (0/5). Deep tendon reflexes were +2 in the upper ex-tremities and absent in the lower extremities. There was no Babinski sign. Cerebellar testing was normal. She had an L4 pinprick sensory level bilaterally. There were no crani-al or spinal bruits. There was a moderate nuchal rigidity.Laboratory tests showed a prothrombin time of 11.8, partial thromboplastin time of 22.6, international normalized ratio of 1 and platelet count of 247,000 per μl. Magnetic resonance imaging of thoracic spine showed intraspinal-dural arteriove-nous malformation with extramedullary and intramedullary components associated with cord haemorrhage (abnormal bright signal in the spinal cord at T5 level) (Figure 1). There was swelling of the cord from T5 to T10 level with multi-ple serpentine signal void structures presenting as heteroge-neous T1 and T2 hyperintense configurations pointing to-wards the hemorrhage within the cord (Figure 2). The patient was subsequently transferred to a tertiary-care facility for neurosurgical intervention. Later, she was lost to follow-up.
Discussion
The principal mechanism of progressive myelopathy in FAS is believed to be vascular thrombosis that leads to mul-tiple small infarcts, which can be hemorrhagic in cases of venous thrombosis [10]. Other complications of FAS in-clude subarachnoid hemorrhage, epidural hematoma, hema-tomyelia, and compressive myelopathy. In our patient, the presence of nuchal rigidity was consistent with the exten-sion of the cord hemorrhage into the subarachnoid space.It should be noted that Valsalva (bearing down during la-bor) maneuver may be a contributing factor in the patho-genesis of hemorrhagic complication in FAS, by raising the spinal venous pressure. Similarly, aneurysmal subarach-noid haemorrhage that occurs in adulthood is often tem-porally related to a Valsalva maneuver (e.g., physical ex-ertion, sexual activity, bowel movements, NVD). It should be noted that AVM can be a culprit behind “thunderclap” headaches associated with neurologic signs, commonly seen in cerebral aneurism. AVM most commonly presents in young adults, and typically occurs within the brain pa-renchyma, causing intracerebral hematomas (also known as parenchymal hematomas) [11]. Occasionally, these le-sions expand into the ventricular or subarachnoid space and produce meningeal signs. Non-complicated AVMs most commonly present with seizures and chronic headaches. In our patient hemorrhagic transformation of AVM occurred
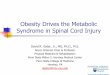
Figure 1.
MRI of thoracic spine showed intraspinal dural AVM with extra-medullary and intra-medullary components associ-ated with cord haemorrhage (abnormal bright signal in the spinal cord at T5 level)

References1. Foix CH, Alajouanine T. La myelite necrotique subaigue. Rev Neurol. 1926;46:1-42.2. Lhermitte J, Friboury-Blanc A, Kyriaco N. La glioseangéio-hyperthrophique de la mo-elleépinière (myélitenécrotique de Foix-Ala-jouanine). Rev Neurol (Paris) 1931;2:37-53.3. Rodriguez FJ, Crum BA, Krauss WE. Ve-nous congestive myelopathy: a mim-ic of neoplasia. Mod Pathol. 2005;18:710-8.4. Pia HW, VogelsangH. Diagnose und Therapie Spina-ler Angiome. DtschZ Nervenheilkd 1965;187:74-96.5. Wirth FP Jr, Post KD, Di Chiro G et al. Foix Ala-
jouanine disease. Spontaneous thrombosis of a spinal cord arteriovenous malformation: a case report. Neurology 1970;20:1114-1118.6. Tobin WD, Layton DD . The diagnosis and nat-ural history of spinal cordarteriovenous mal-formations.Mayo ClinProc 1976; 51:637-646.7. Criscuolo GR, Oldfield EH, Doppman JL et al. Reversible acute and subacute my-elopathy in patients with duralarteriove-nous fistulas: Foix-Alajouanine syndrome re-considered. J Neurosurg 1989;70:354-359.8. Van Dijk JMC, Ter Brugge KG, Willinsky RA, et al. Mul-tidisciplinary management of spinal dural arterove-nous fistulas: clinical presentation and long-term
follow-up in 49 patients. Stroke 2002;33:1578-15839. Jellinger K. Vascular malformations of the central nervous system: a morphologi-cal overview. Neurosurg Rev. 1986;9:177-216.10. Lewis P.R, Timothy A.P, eds. Merritt's textbook of neurology. 12th ed. USA: Lip-pincott and Williams; December 3, 2009.11. Aneurysm and intracranial haemorrhage. Surgery: A clinical approach. Marvin Bergs-neider. chapter 80 page 579 review, 1997.
Journal of Cases in Obstetrics & Gynecology24
from T5 to T10, presenting with compressive myelopathy. At this juncture, we would like to alert obstetricians to the risk of hemorrhagic transformation of AVM during vaginal delivery and a possible need for elective cesarean section. Further studies will be necessary to identify var-ious risk factors for hemorrhagic transformation in FAS. In conclusion, spinal arteriovenous malformation is associated with what has been known as Foix-Ala-jouanine syndrome (FAS), presenting with a clinical picture of sub-acute progressive myelopathy. We cau-tion obstetricians against vaginal delivery in patients with FAS because of a risk of hemorrhagic transfor-mation and abrupt onset of compressive myelopathy.
Conflict of InterestAuthors declare no conflict of interest
Figure 2.
There was swelling of the cord from T5 to T10 level with multiple serpentine signal void structures presenting as heterogeneous T1 and T2 hyperintense configurations pointing towards the hemorrhage within the cord
Janati et al.